Embed Size (px)
Citation preview

O
Aa
PPa
7b
c
Fd
e
f
ARA
KAASML
1
Orthopaedics & Traumatology: Surgery & Research 101 (2015) 895–901
Available online at
ScienceDirectwww.sciencedirect.com
riginal article
rthroscopic treatment of acute acromioclavicular dislocations using double button device: Clinical and MRI results
. Loriauta,∗,b, L. Casabiancaa, J. Alkhaili c, B. Dallaudièred,e, E. Desportes f, R. Rousseaua,
. Massinc, P. Boyerc
Service de chirurgie orthopédique et de traumatologie, hôpital de la Pitié-Salpêtrière, université Pierre-et-Marie-Curie, 47, boulevard de l’Hôpital,5013 Paris, FranceInstitut de chirurgie orthopédique, clinique des Lilas, 41-49, avenue du Maréchal-Juin, 93260 Les Lilas, FranceService de chirurgie orthopédique et de traumatologie, hôpitaux universitaires Paris Nord – Val-de-Seine, 46, rue Henri-Huchard, 75877 Paris cedex 18,ranceService de radiologie, clinique du sport, Bordeaux-Mérignac, 2, rue Negrevergne, 33700 Mérignac, FranceService de radiologie, hôpital Pellegrin, Bordeaux, place Amélie-Raba-Léon, 33076 Bordeaux, FranceService de radiologie, hôpitaux universitaires Paris Nord – Val-de-Seine, 46, rue Henri-Huchard, 75877 Paris cedex 18, France
a r t i c l e i n f o
rticle history:eceived 10 December 2014ccepted 8 September 2015
eywords:cromioclavicular joint dislocationrthroscopyhoulder surgeryRI
igament healing
a b s t r a c t
Introduction: Arthroscopic treatment of acute grade 3 and 4 acromioclavicular dislocation is controversial,due to the risk of recurrence and of postoperative reduction defect. The purpose of the present study wasto investigate whether the healing of the acromioclavicular (AC) and coracoclavicular (CC) ligamentsand the accurate 3D positioning parameters of the AC joint using MRI were correlated with satisfactoryfunctional outcome.Material: Thirty-nine patients were enrolled from 2009 to 2011 and managed arthroscopically by CClacing using a double-button device.Methods: Clinical assessment included the Shoulder and Hand (QuickDash) score, Constant-Murley scoreand visual analog scale (VAS) for residual pain. Time and rate to return to work and return to sport wereassessed according to type of sport and work. Postoperative complications were recorded. Radiologicalexamination consisted of anteroposterior clavicle and lateral axillary radiographs. AC ligament healingand 3D joint congruency were assessed on MRI and correlated to the clinical results.Results: Mean patient age was 35.7 years (range, 20–55). Mean follow-up was 42.3 ± 10.6 months (range,24–60). At final follow-up, mean QuickDash score, Constant score and VAS were respectively 1.7 ± 4(range, 0–11), 94.7 ± 7.3 (range, 82–100) and 0.5 ± 1.4 (range, 0–2). Thirty-five (90%) patients were ableto resume work, including heavy manual labor, and sport. Radiology found accurate 3D joint congruencyin 34 patients (87%) and CC and AC ligament healing in 36 (93%). Complications included reduction lossat 6 weeks in 3 patients, requiring surgical stabilization. Satisfactory functional results were associatedwith accurate AC joint congruency in the coronal and axial planes (P < 0.05) and good AC and CC ligamenthealing (P < 0.04). An initial 25% reduction defect in the coronal plane was not associated with poor
functional results (P = 0.07).Conclusion: Arthroscopic treatment by CC lacing satisfactorily restored ligament and joint anatomy inthe present series. These satisfactory anatomic results correlated with good clinical outcome encouragecontinuing with this technique.Level of evidence: Level IV, therapeutic case series.© 2015 Elsevier Masson SAS. All rights reserved.
∗ Corresponding author. Tel.: +33 6 19 53 52 07; fax: +33 1 42 17 70 53.E-mail address: [email protected] (P. Loriaut).
http://dx.doi.org/10.1016/j.otsr.2015.09.024877-0568/© 2015 Elsevier Masson SAS. All rights reserved.
1. Introduction
Acromioclavicular (AC) dislocation is a very common shoulder
injury. Incidence is 1.8 per 10,000 per year [1]. Several classificationsystems have been proposed to describe AC dislocation morphol-ogy. The Allman and Tossy and Rockwood classifications are themost common ones [2,3]. These classifications, initially based on
8 ology:
pit
chs
pbiarurof
MaNwfa
2
t2rr6otFdgswo
Fop
96 P. Loriaut et al. / Orthopaedics & Traumat
lain radiographs, were recently updated with magnetic resonancemaging (MRI). Thus, MRI provides better imaging of AC joint struc-ures and of AC and coracoclavicular (CC) ligament injuries [4–7].
The surgical treatment of acute type 3 and 4 AC dislocation is stillontroversial [8–12]. Several open surgical techniques for fixationave been described, but most are associated with complicationsuch as infection, correction loss or implant migration [13–18].
Recently, arthroscopic techniques have been successfully pro-osed to treat AC joint instability [19–22]. However, despiteetter understanding of AC pathophysiology and continuous
mprovement in surgical management, current techniques remainssociated with many significant complications [23]. Some authorseported under-correction leading to loss of congruency and resid-al horizontal and vertical instability [24,25]. To date, routineadiographs remain the most widespread method of assessmentf AC dislocation treatment; only a few studies used MRI, and onlyor diagnostic purposes.
The purpose of the present study was to assess clinical andRI outcome of arthroscopically assisted treatment of acute type 3
nd 4 AC dislocation using a double button (TightRopeTM: Arthrex;aples, FL) at a minimum follow-up of two years. The hypothesisas that this technique could be effective, providing satisfactory
unctional outcome correlated with AC and CC ligament healingnd accurate AC joint congruency.
. Material and methods
Eighty-seven patients diagnosed with acute AC dislocation werereated in our department between January 2009 and October011. Data were recorded prospectively and then analyzed ret-ospectively by an independent observer. Patient records wereeviewed for the following inclusion criteria: patient aged 18 to0 years, with radiological evidence of isolated Rockwood type 3r 4 acute AC dislocations, receiving arthroscopically assisted fixa-ion using a double button device (TightRopeTM: Arthrex; Naples,L) and with minimum follow-up of two years. Patients with otherislocation types (1, 2 or 5), with associated rotator cuff, labral,
lenohumeral or biceps tendon injury diagnosed during the arthro-copic procedure or with incomplete evaluation at final follow-upere excluded. This series has some patients in common with thatf Cohen et al. [19].
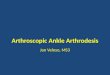
ig. 1. A: The base of the coracoid process was cleaned using a radiofrequency ablator; B: Af the base of the coracoid process; C: A 2 mm K-wire was inserted through the guide, whrocess; D: The TightRopeTM system was then inserted through the tunnels using a wire
Surgery & Research 101 (2015) 895–901
2.1. Surgical technique
The surgical procedures were performed by a single seniororthopedic surgeon. The patient was placed in the beach chairposition, without any traction, and operated on under general anes-thesia. First, a posterior portal was created for joint exploration.Then, an anterior working portal was created using an outside-in technique. A finger depressed the skin to identify the rotatorinterval. A spinal anesthesia needle was then used to locate the cor-rect position for skin incision. The subscapularis bursa was resectedusing a radiofrequency ablator until the base of the coracoid pro-cess could be visualized (Fig. 1A). A drill guide (Arthrex; Naples, FL)was introduced by the anterior portal and centered on the under-surface of the base of the coracoid process (Fig. 1B). A 3 cm incisionwas made over the clavicle and the drill guide was positioned in thecenter of the clavicle. Good positioning is critical because an anteri-orly or posteriorly placed tunnel may break through the remainingcortex of the clavicle and lead to implant loosening or loss. Usingarthroscopy, fluoroscopy and the guide, a 2 mm K-wire was insertedfrom the clavicle toward the coracoid, and a 4 mm hole was cre-ated following the K-wire through the clavicle and the coracoidprocess with a cannulated drill, with 4 passages through the cor-tex (Fig. 1C). The K-wire was withdrawn, leaving the drill in place,and replaced by a guide, which was retrieved through the ante-rior portal. The TightRopeTM system (Arthrex; Naples, FL) was theninserted through the tunnels using a wire passer through the can-nulated mesh, from the clavicle to the coracoid, and the buttonwas flipped so as to fix under the surface of the coracoid process(Fig. 1D). Finally, the dislocation was reduced under fluoroscopicvisualization with a downward pressure on the proximal fragmentof the clavicle, associating a shoulder abduction maneuver to helpreduction. The sutures were then tightened and tied at the clavi-cle. Fluoroscopic control was performed to confirm reduction of thejoint and positioning of the implants.
2.2. Postoperative rehabilitation
Patients were given a standard surgical corset immediately aftersurgery. Passive range of motion and pendulum exercises werestarted one week postoperatively, and conducted over a period ofsix weeks. Then the corset was removed and patients started active
drill guide was introduced by the anterior portal and centered on the undersurfaceich was withdrawn and replaced by a 4 mm drill through the clavicle and coracoid
passer, and the button was flipped to fix under the surface of the coracoid process.

ology:
rfa
2
caCcpoh
a“
aR
bll6f
adTwwp2tchiMtI
oprih
P. Loriaut et al. / Orthopaedics & Traumat
ange of motion and strength exercises. They were told to abstainrom lifting, carrying, pushing and pulling on the operated side for
period of three months after the surgery.
.3. Clinical and radiological assessment
Clinical assessment included the following data: demographics,ause of injury, associated injuries, handedness, time to surgery,nd range of motion. The Shoulder and Hand (QuickDash) [26] andonstant-Murley score [27] and visual analog pain scale (VAS) wereompleted at final follow-up. Values were reported to one decimallace. Type of sport activity was classified according to Allain [28];ccupation was categorized as sedentary, clerical, light manual oreavy manual.
Time to and rate of return to work and to sport were alsossessed, as well as global satisfaction with surgery: “satisfied” ornot satisfied”.
Radiological examination consisted of bilateral X-ray and lateralxillary radiographs. Dislocations were graded according to theockwood classification. [2].
Postoperative complications or failure were recorded: implantreakage, secondary displacement, infection, clavicle erosion, CC
igament ossification or early AC arthropathy. Clinical and radio-ogical follow-up was performed at 1 week, 6 weeks, 3 months,
months and then every 6 months postoperatively until finalollow-up.
MRI assessment of the operated shoulder was performed at 3nd 24 months’ follow-up. Patient positioning during MRI was stan-ardized: supine, arm along the body with elbow in extension.1-weighted fast spin echo (TR 560; TE 12) and fat-saturated T2-eighted gradient echo (TR 2920; TE 70) sequences were acquiredith a 1.5 T Signa HDx apparatus (GE Healthcare). The other MRIarameters were: field of view 160 mm, matrix size 320 × 256 or56 × 512, and 4 mm section thickness. Images were transferredo a PACS workstation. Two radiologists specialized in osteoarti-ular pathology assessed the images blinded to clinical outcome,aving undergone prior dedicated training sessions to familiar-
ze themselves with the measurement methods and classifications.easurements were made using the digitized tools of the PACS sys-
em, Impax (Agfa, Gevaert N.V), and repeated at a 2 week interval.nterobserver and intraobserver reliability were evaluated.
Persistent superior displacement in the coronal oblique viewr posterior displacement in the axial view were quantified as
ercentage translation of the anterolateral edge of the clavicle inelation to the anteromedial edge of the acromion and classifiedn five categories: zero, 25%, 50%, 75% or 100% displacement. Anyyper-reduction was also noted.Fig. 2. A and B. Postoperative AP and axillary radiograph at two years’ follow
Surgery & Research 101 (2015) 895–901 897
AC and CC ligament healing was defined as the formation ofcontinuous scar tissue, and was assessed on sagittal oblique andcoronal oblique images. AC osteoarthritis, CC ligament calcification,subacromial bursitis or rotator cuff tear were also noted.
2.4. Statistical analysis
Calculations and the statistical analysis were done using SPSS forWindows (Version 20; SPSS Inc., Chicago, Illinois). Mann-WhitneyU test was performed for qualitative variables (satisfaction, dissat-isfaction), and Fisher’s exact test for quantitative variables. A P valueof < 0.05 was considered to be significant. The intra- and interob-server reliability values were calculated using Cohen’s weightedkappa and strength of agreement was interpreted according to thecriteria of Landis and Koch.
Informed consent was obtained from all patients according tothe Declaration of Helsinki. The IRB classified the study as “standardcare”.
3. Results
Forty-eight patients were excluded from the study: 40 withother dislocation types and 5 with type 3 or 4 AC dislocation andassociated shoulder injury (4 rotator cuff injuries and one labraltear requiring arthroscopic repair). Three of the 42 patients withisolated type 3 or 4 AC dislocation didn’t have sufficient follow-up.Thus, outcome was determined for 39 patients (26 male and 13female).
Mean age was 35.7 years (range 20–55). Traffic accidents (n = 21)were the predominant cause of injury, followed by sport injuries(n = 15) and other trauma (n = 3). The dominant arm was affectedin 31 patients. All but 4 patients had recreational sport activities;the distribution of sport activities was: G1, 11%; G2, 34%; G3, 40%;and G4, 15%. The distribution of occupations was: sedentary, 21%;clerical, 15%; light manual, 23%; and heavy manual, 41%. Meanfollow-up was 42.3 ± 10.6 months (range, 24–60). According to theRockwood classification, there were 28 type 3 and 11 type 4 dis-locations. Mean time to surgery was 3 days (range, 1–10). Meanoperative time was 40 min (range, 30–80).
At final follow-up, mean QuickDash score, Constant score andVAS were respectively 1.7 ± 4 (range, 0–11), 94.7 ± 7.3 (range,82–100) and 0.5 ± 1.4 (range, 0–2).
Thirty-five patients (90%) showed complete functional recoverywith full range of motion and pain relief. Patients with seden-
tary, clerical and light manual jobs returned to work at a mean11 weeks and those with heavy manual jobs at a mean 20 weeks.Three patients (heavy manual) were unable to resume previouswork. One patient was retired. Thirty-four patients resumed their-up, showing a complete reduction of a Rockwood type 4 dislocation.

8 ology:
rlwo
r3T
r1OwatU
p
cri0
t
lia
Fn
98 P. Loriaut et al. / Orthopaedics & Traumat
ecreational sport activities, at a mean 21 weeks: 30 at the sameevel as before trauma and 4 at a lower level. Thirty-five patients
ere satisfied with the cosmetic appearance and functionalutcome.
Immediate postoperative radiographs showed an accurate ACeduction in 37 patients (Figs. 2A and B). Two patients with type
dislocation presented initial 25% lack of reduction on AP view.here was no AC hyper-reduction or coracoid process fracture.
Despite complete initial reduction, 3 patients presented recur-ence, at a mean 6 weeks postoperatively, due to implant failure in
patient and tunnel misplacement in 2 patients (Figs. 3A and 3B).wing to persistent functional discomfort, these patients under-ent surgical revision at 6 months, with arthroscopic AC joint
ugmentation with transacromial gracilis tendon loop associatedo synthetic ligament stabilization (GraftRope, Arthrex, Naples, FL,SA).
No hardware-related discomfort was reported, except for 1atient, in whom material was removed.
At the 24 months follow-up, MRI confirmed accurate 3D jointongruency in 34 patients (87%) (Figs. 4A and B) and 25% lack ofeduction on coronal view in 2 patients (Figs. 5A and B). Overallnter- and intraobserver variability kappa values were 0.81 and.85, respectively, indicating very good agreement.
MRI found anatomic AC and CC ligament tissue healing. Scarissue was found in 36 patients (93%) (Figs. 6A, B and C).
At final follow-up, no AC osteoarthritis was reported. CC-igament calcification was visible in 4 patients. There was nomplant migration or bone resorption. Two patients developed sub-cromial bursitis and symptomatic supraspinatus tears.
ig. 3. A and B. Postoperative radiograph showing implant failure with secondary dison-healing of the AC ligaments.
Surgery & Research 101 (2015) 895–901
In summary, postoperative complications were reported in 6patients: 1 implant failure, 2 tunnel misplacements, 1 implantremoval due to discomfort, and 2 cases of subacromial bursitisassociated with supraspinatus tear.
3.1. Statistical analysis
Satisfactory functional results were associated with accurateacromioclavicular joint (ACJ) congruency in the coronal and axialplanes (P < 0.05) and with good AC and CC ligament healing(P < 0.04).
Initial 25% lack of reduction on coronal view was not associatedwith poor functional results or dissatisfaction (P = 0.07).
CC ligament calcification was not associated with poor func-tional outcome (P = 0.09).
4. Discussion
The main finding of this study was that arthroscopic stabiliza-tion of type 3 and 4 acute AC dislocation achieves satisfactoryoutcome, associated with accurate AC congruency and ligamenthealing. Patient satisfaction and functional recovery rates werehigh and the complications rate was acceptable.
Several techniques for fixation of AC dislocations have been
described. However, most techniques (coracoacromial ligamenttransfer, hook plate fixation, wire fixation, suture or screw fixa-tion) do not restore the AC joint anatomically, and are associatedwith many complications [13–18].placement. Coronal T2 FS MR image at 3 months showing lack of reduction and

P. Loriaut et al. / Orthopaedics & Traumatology: Surgery & Research 101 (2015) 895–901 899
F owin
rItcc
ws
id
mudtc
lowftfi
n
ig. 4. A and B. Fat-saturated T2-weighted gradient echo MR image at follow-up, sh
More recent techniques have focused on anatomic CC ligamenteconstruction, such as the TightRopeTM device technique [19–22].n this procedure, the CC ligaments are expected to heal along theightrope, providing guided healing. Restoring accurate AC jointongruency, the AC and CC ligament remnants are brought intoontact to facilitate healing.
Furthermore, this arthroscopic procedure required no hard-are removal in most cases and allowed treatment of concomitant
houlder injuries in the same step [29].Our findings are consistent with several authors reporting sat-
sfactory functional outcome using the same technique and sameevice [30–32].
Some authors observed recurrent posterior or superior displace-ent of the clavicle after a procedure for type 3 or 4 dislocation
sing this technique. They reported good functional outcomeespite partial loss of reduction [21] or partial initial lack of reduc-ion [33]. In the present study, an 25% initial lack of reduction onoronal view was not predictive of poor functional outcome.
In the present series, no posterior secondary displacement orack of reduction was observed in type 4 dislocations. To the bestf our knowledge, no persistent posterior or superior instabilityas associated with poor functional outcome using this procedure
or type 3 and 4 dislocations in previous studies. Gerhardt showedhat loss of reduction or initial lack of reduction was responsible
or persistent posterior instability and poorer clinical results onlyn high-grade type 5 dislocation [24].According to Andreani et al., comparing the results of two tech-iques (TightRopeTM and hook plate), mean Constant score was
Fig. 5. A and B. Incomplete reduction of a type 3 dislocation (2
g accurate reduction of the type 4 dislocation in both coronal and axial planes.
significantly higher in the TightRopeTM group. Two the fixationsystem breakages were reported. [34].
According to Jensen et al., in a study comparing techniques usinghook plate (HP) versus TightRopeTM (TR) in a series of 56 patients,63% of the patients in the HP group had hypertrophic scars. 46% ofthe TR group reported mild pain and paresthesia over the clavicu-lar buttons. Four CC ligament calcifications were reported in eachgroup. AC arthropathy was found in 28% of the patients in the HPgroup and 19% in the TR group. 12% of the patients required revi-sion surgery due to recurrent vertical and horizontal instability inthe TR group. In the HP group, 13% required revision surgery forposttraumatic stiffness [35].
Horst et al. compared the TightRopeTM technique (TR) to K-wire(KW) fixation in a series of 41 patients with type ≥ 3 AC joint dislo-cation. The TR technique was associated with shorter surgery timeand lower costs.
Material costs were significantly higher for using the TR tech-nique, but patients were discharged earlier.
In the TR group, there was early loss of reduction in 1 patientand delayed wound healing in 2. In the KW group, there was screwmigration in 4 patients, early reduction loss in 1, and impingementsyndrome in 1 [36].
According to Scheibel et al., recurrent partial vertical insta-bility was not associated with poorer clinical results. However,
patients with recurrent horizontal instability did present signif-icantly poorer results. It was concluded that the TightRopeTMtechnique provides sufficient biomechanical stability at time zerobut, in some cases, the healing potential of the ligaments seems to
5%) in the coronal view, with ligament healing achieved.

900 P. Loriaut et al. / Orthopaedics & Traumatology: Surgery & Research 101 (2015) 895–901
l T2 F
bsb
spa1l
ksTahra
ttsl
5
ucc
[
Fig. 6. A, B, C, D. Coronal T2 FS, Sagittal T1 SE and Axia
e limited, and anatomic scar formation was not always possible,o that reduction depended on the implant, leading to failure eithery initial migration or by suture breakage [37].
Di Francesco was the first to report clinical and MRI results forurgical treatment of type III and V AC dislocation using hooklate [38]. In a series of 42 patients, acceptable joint alignment waschieved in all cases after surgery; 1 year after plate removal, a2% rate of dislocation recurrence was reported. MRI showed CC
igament healing in the remaining cases (88%) [38].The present study has some strong points. To the best of our
nowledge, it is the first prospective study to investigate arthro-copic treatment of type 3 and 4 acute AC dislocation using theightRopeTM system, with medium-term clinical (clinical scores)nd radiologic follow-up AC joint position on MRI, and ligamentealing), with good correlation between clinical and radiologicalesults. It has also some limitations: the absence of a control groupnd relatively small number of cases.
The clinical interest of this study lies in the finding that theechnique can be used as a first-choice method for the surgicalreatment of acute type 3 and 4 AC dislocation, as it provides aatisfactory functional outcome and allows treatment of associatedesions in the same step, without requiring later hardware removal.
. Conclusions
The present study demonstrated that arthroscopic treatmentsing a double button device provides satisfactory functional out-ome associated with good AC ligament healing and accurate ACJongruency in patients with acute type 3 and 4 AC dislocation.
[
S images showing healing of the AC and CC ligaments.
Disclosure of interest
The authors declare that they have no competing interest.
References
[1] Franceschini V, Dei Giudici L, Alibardi A, Salate Santone F, Ramos Alday LJ, et al.Epidemiology of isolated acromioclavicular joint dislocation. Emerg Med Int2013;2013:171609.
[2] Nguyen V, Williams G, Rockwood C. Radiography of acromioclavicular disloca-tion and associated injuries. Crit Rev Diagn Imaging 1991;32:191–228.
[3] Tossy JD, Mead NC, Sigmond HM. Acromioclavicular separations: useful andpractical classification for treatment. Clin Orthop Relat Res 1963;28:111–9.
[4] Alyas F, Curtis M, Speed C, Saifuddin A, Connell D. MR imaging appearances ofacromioclavicular joint dislocation. Radiographics 2008;28(2):463–79.
[5] Antonio GE, Cho JH, Chung CB, Trudell DJ, Resnick D. MR imaging appear-ance and classification of acromioclavicular joint injury. AJR Am J Roentgenol2003;180(4):1103–10.
[6] Fialka C, Krestan CR, Stampfl P, Trieb K, Aharinejad S, Vécsei V. Visualizationof intra articular structures of the acromioclavicular joint in an ex vivo modelusing a dedicated MRI protocol. AJR Am J Roentgenol 2005;185(5):1126–31.
[7] Izadpanah K, Winterer J, Vicari M, Jaeger M, Maier D, Eisebraun L, et al.A stress MRI of the shoulder for evaluation of ligamentous stabilizers inacute and chronic acromioclavicular joint instabilities. J Magn Reson Imaging2013;37(6):1486–92.
[8] Beitzel K, Cote MP, Apostolakos J, et al. Current concepts in the treatment ofacromioclavicular joint dislocations. Arthroscopy 2013;29(2):387–97.
[9] Calvo E, Lopez-Franco M, Arribas IM. Clinical and radiologic outcomes of sur-gical and conservative treatment of type III acromioclavicular joint injury. JShoulder Elbow Surg 2006;15:300–5.
10] Reid D, Polson K, Johnson L. Acromioclavicular joint separations grades I-III:a review of the literature and development of best practice guidelines. Sports
Med 2012;42(8):681–96.11] Smith TO, Chester R, Pearse EO, Hing CB. Operative versus non-operativemanagement following Rockwood grade III acromioclavicular separa-tion: a meta-analysis of the current evidence base. J Orthop Traumatol2011;12(1):19–27.

ology:
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
2011;39(7):1507–16.
P. Loriaut et al. / Orthopaedics & Traumat
12] Tauber M. Management of acute acromioclavicular joint dislocations: currentconcepts. Arch Orthop Trauma Surg 2013;133(7):985–95.
13] Greiner S, Braunsdorf J, Perka C, Herrmann S, Scheffler S. Mid to long-termresults of open acromioclavicular-joint reconstruction using polydioxansulfatecerclage augmentation. Arch Orthop Trauma Surg 2009;129(6):735–40.
14] Kienast B, Thietje R, Queitsch C, Gille J, Schulz AP, Meiners J. Mid-term resultsafter operative treatment of rockwood grade III-V acromioclavicular joint dis-locations with an AC-hook-plate. Eur J Med Res 2011;16(2):52–6.
15] Lyons FA, Rockwood CA. Migration of pins used in operations on the shoulder.J Bone Joint Surg Am 1990;72:1262–7.
16] Nadarajah R, Mahaluxmivala J, Amin A, Goodier DW. Clavicular hook-plate:complications of retaining the implant. Injury 2005;36(5):681–3.
17] Salem KH, Schmelz A. Treatment of Tossy III acromioclavicular joint injuriesusing hook plates and ligament suture. J Orthop Trauma 2009;23(8):565–9.
18] Sandmann GH, Martetschläger F, Mey L, Kraus TM, Buchholz A, Ahrens P, et al.Reconstruction of displaced acromio-clavicular joint dislocations using a triplesuture-cerclage: description of a safe and efficient surgical technique. PatientSaf Surg 2012;6(1):25.
19] Cohen G, Boyer P, Pujol N, Hamida Ferjani B, Massin P, Hardy P. Endoscopi-cally assisted reconstruction of acute acromioclavicular joint dislocation usinga synthetic ligament. Outcomes at 12 months. Orthop Traumatol Surg Res2011;97(2):145–51.
20] Lafosse L, Baier GP, Leuzinger J. Arthroscopic treatment of acute and chronicacromioclavicular joint dislocation. Arthroscopy 2005;21:1017.
21] Murena L, Vulcano E, Ratti C, Cecconello L, Rolla PR, Surace MF. Arthroscopictreatment of acute acromioclavicular joint dislocation with double flip button.Knee Surg Sports Traumatol Arthrosc 2009;17(12):1511–5.
22] Sobhy MH. Midterm results of combined acromioclavicular and coracoclavic-ular reconstruction using nylon tape. Arthroscopy 2012;28(8):1050–7.
23] Milewski MD, Tompkins M, Giugale JM, Carson EW, Miller MD, Diduch DR. Com-plications related to anatomic reconstruction of the coracoclavicular ligaments.Am J Sports Med 2012;40(7):1628–34.
24] Gerhardt C, Kraus N, Pauly S, Scheibel M. Arthroscopically assisted stabiliza-tion of acute injury to the acromioclavicular joint with the double TightRopeTM
technique: One-year results. Unfallchirurg 2013;116(2):125–30.
25] Thiel E, Mutnal A, Gilot GJ. Surgical outcome following arthroscopic fixationof acromioclavicular joint disruption with the tightrope device. Orthopedics2011;34(7):267–74.
26] Beaton DE, Wright JG, Katz JN. Development of the QuickDASH: comparison ofthree item-reduction approaches. J Bone Joint Surg Am 2005;87:1038–40.
[
Surgery & Research 101 (2015) 895–901 901
27] Constant CR, Murley AHG. A clinical method of functional assessment of theshoulder. Clin Orthop Relat Res 1987;214:160–4.
28] Allain J, Goutallier D, Glorion C. Long-term results of the Latarjet procedurefor the treatment of anterior instability of the shoulder. J Bone Joint Surg Am1998;80(6):841–52.
29] Pauly S, Kraus N, Greiner S, Scheibel M. Prevalence and pattern of glenohumeralinjuries among acute high-grade acromioclavicular joint instabilities. J Shoul-der Elbow Surg 2013;22(6):760–6.
30] Beris A, Lykissas M, Kostas-Agnantis I, Vekris M, Mitsionis G, Korompilias A.Management of acute acromioclavicular joint dislocation with a double-buttonfixation system. Injury 2013;23:288–92.
31] El Sallakh SA. Evaluation of arthroscopic stabilization of acute acromio-clavicular joint dislocation using the TightRope system. Orthopedics2012;35(1):18–22.
32] Patzer T, Clauss C, Kühne CA, Ziring E, Efe T, Ruchholtz S, et al. Arthroscopicallyassisted reduction of acute acromioclavicular joint separations: comparison ofclinical and radiological results of single versus double TightRopeTM technique.Unfallchirurg 2013;116(5):442–50.
33] Defoort S, Verborgt O. Functional and radiological outcome after arthroscopicand open acromioclavicular stabilization using a double-button fixation sys-tem. Acta Orthop Belg 2010;76(5):585–91.
34] Andreani L, Bonicoli E, Parchi P, Piolanti N, Michele L. Acromio-clavicularrepair using two different techniques. Eur J Orthop Surg Traumatol2014;24(2):237–42.
35] Jensen G, Katthagen JC, Alvarado LE, Lill H, Voigt C. Has the arthroscopicallyassisted reduction of acute AC joint separations with the double tight-ropetechnique advantages over the clavicular hook plate fixation? Knee Surg SportsTraumatol Arthrosc 2014;22(2):422–30.
36] Horst K, Dienstknecht T, Pishnamaz M, Sellei RM, Kobbe P, Pape HC. Operativetreatment of acute acromioclavicular joint injuries graded Rockwood III and IV:risks and benefits intight rope technique vs. k-wire fixation. Patient Saf Surg2013;7(1):18.
37] Scheibel M, Dröschel S, Gerhardt C, Kraus N. Arthroscopically assisted stabiliza-tion of acute high-grade acromioclavicular joint separations. Am J Sports Med
38] Di Francesco A, Zoccali C, Colafarina O, Pizzoferrato R, Flamini S. The use ofhook plate in type III and V acromio-clavicular Rockwood dislocations: clini-cal and radiological midterm results and MRI evaluation in 42 patients. Injury2012;43(2):147–52.