Embed Size (px)
Citation preview
Arthroscopic-Assisted Allograft Anterior Cruciate Ligament Reconstruction in Patients With Symptomatic Arthrosis
Frank R. Noyes, M.D., and Sue D. Barber-Westin, B.S.
Summary: We reviewed the results of arthroscopic-assisted anterior cruciate liga- ment (ACL) allograft reconstructions in 40 patients who had advanced articular cartilage deterioration documented by arthroscopy during the reconstruction. A mean of 7 years had elapsed between the original injury and the reconstruction, and 102 prior operative procedures had been done in 34 of the 40 patients. A total of 64 articular cartilage lesions were noted; 34 knees had lesions in the medial or lateral tibiofemoral compartment. Postoperatively, all had immediate motion and early functional rehabilitation. The results were assessed using the Cincinnati Knee Rating System. At follow-up (mean, 37 months), significant improvements were found for pain, giving-way, and functional limitations with daily and sports activi- ties (P < .01). Fifty-five percent had returned to mostly light athletics (avoiding high impact sports) based on our advice and were asymptomatic. The mean overall rating scores significantly improved (P < .0001, mean improvement 22 points). We concluded that the majority of patients in this study with chronic ACL rupture and post-tranmatic arthrosis benefited short-term from arthroscopic-assisted ACL reconstruction. Key Words: Anterior cruciate ligament--Articular cartilage-- Allograft--Immediate motion.
W hile the English literature abounds with reports of results of anterior cruciate ligament (ACL)
reconstruction in patients with chronic deficiency, few have presented data on patients who have had this operation and who also had advanced articular carti- lage deterioration determined by direct arthroscopic visualization. 16 Some authors have provided results of ACL reconstruction in patients in whom the amount of articular cartilage deterioration was determined by radiographsT9; however, this method does not provide a true indication of the extent of patellofemoral or tibiofemoral compartment damage. 1°~1 Few studies on ACL reconstruction have separately assessed results between individuals with no or only mild deterioration
From the Cincinnati Sportsmedicine and Orthopaedic Center and the Deaconess Hospital, Cincinnati, Ohio.
Research funded by the Cincinnati Sportsmedicine Research and Education Foundation.
Address correspondence and reprint requests to: Frank R. Noyes, M.D., Deaconess Hospital, Sportsmedicine Research Dept., 311 Straight Street, Cincinnati, OH 45219, U.S.A.
© 1997 by the Arthroscopy Association of North America 0749-8063/97/1301-145253.00/0
and those with advanced damage determined from arthroscopic visualization, or have attempted to corre- late the amount of joint deterioration with residual symptoms and functional limitations experienced post- operatively. 4 Although we have previously performed these analyses on small subgroups of patients within large populations of knees that have had ACL allograft reconstruction, 13 the number of individuals with ad- vanced deterioration has been too small for valid con- clusions to be reached on the efficacy of the reconstruc- tion in these individuals.
Patients with chronic ACL deficiency and advanced articular cartilage deterioration often present with pain and swelling as their major complaints. Full giving- way of the knee may be infrequent because the major- ity of these individuals have modified their activities, although partial giving-way may still occur with daily or light recreational activities. Therefore, the surgeon may be reluctant to perform an ACL reconstruction because instability is not the primary problem. Opera- tive procedures designed to treat symptoms of pain and swelling (meniscectomy, chondroplasty, abrasion arthroplasty) may provide short-term relief, however,
24 Arthroscopy: The Journal o f Arthroscopic and Related Surgery, Vol 13, No 1 (February), 1997: pp 24-32

ACL RECONSTRUCTION AND KNEE ARTHROSIS 25
they do not correct the inherent problem of abnormal knee kinematics. The sequela of chronic ACL defi- ciency in the young athletically active patient, includ- ing recurrent giving-way episodes, loss of secondary restraints, meniscal tears, and eventual chondral deteri- oration, is well known. 9'1~ What has not been clearly addressed is the role of ACL reconstruction in knees with advanced articular cartilage deterioration. Is a lig- ament reconstructive procedure and added rehabilita- tion period warranted in these individuals? Should sim- pler procedures, such as arthroscopic debridement and chondroplasty, be performed with the objective of buy- ing time until the patient reaches the appropriate age for arthroplasty? We believe that in active patients, arthroscopic-assisted ACL reconstruction followed by immediate knee motion is warranted to correct abnor- mal knee displacements and potentially provide relief or a decrease in instability, pain, and swelling symp- toms, as well as an increase in activity level.
The purpose of this study was to determine the ability of an arthroscopic-assisted ACL allograft reconstruction, perfomaed in knees with advanced articular cartilage de- terioration, to decrease or alleviate pain, swelling, giving- way, and functional limitations incurred during sports and daily activities. Advanced deterioration was determined during the ACL reconstruction, and was defined as gross fissuring or fragmentation of a cartilage surface extending into greater than one-half of the depth of the cartilage and over an area of at least 15 ram, or subchondral bone exposure.
MATERIALS AND METHODS
Subjects The criteria for inclusion in this study were: 1)
chronic ACL rupture (greater than 12 weeks from in- jury to reconstruction); 2) pain and swelling with sports or daily activities; 3) advanced articular cartilage dete- rioration detected during the arthroscopic examination at ACL reconstruction; 4) no concomitant reconstruc- tion to the medial or lateral collateral ligament or poste- rior cruciate ligament; 5) normal valgus lower osseous alignment with no prior correcting procedure (high tib- ial osteotomy); and 6) ACL reconstruction performed with a bone-patellar ligament-bone allograft. Forty pa- tients met the criteria over a 6-year period (1986 to 1992) and were followed a mean of 37 months (range, 22 to 74 months) postoperatively. Twenty-three pa- tients were followed between 2 and 3 years postopera- tive; 12 patients, between 3 and 4 years postoperative; and 5 patients, greater than 4 years postoperatively. These patients were part of a large prospective study on ACL allografts which has been previously reported. 1-3
There were 30 males and 10 females whose mean age at operation was 29 years (range, 15 to 49). The major- ity were athletically active, as 34 (85%) had sustained the original knee injury during a sporting event. The mean time from the original knee injury to the index operation was 83 months (range, 5 to 281). A total of 102 prior operative procedures (Table 1) had been performed in 34 of the 40 patients (85%), including 16 prior failed ACL reconstructions in 12 patients. The average number of prior operative procedures was 3 (range, 0 to 7).
Evaluation Knee displacement testing was performed with a
KT-2000 (MEDMetric, San Diego, CA) at 89 N of anterior-posterior (AP) at 25 ° of flexion preoperatively, and at 89 and 134 N at follow-up. One examiner per- formed the arthrometer testing in a previously de- scribed manner. 12 This method has previously been found to be reliable. 13 Five knees were excluded from the analysis of the arthrometer testing due to ACL ruptures on the contralateral limb.
A previously described X classification system for de- termining ACL function using arthrometric testing was employed to categorize the knees into either a func- tional, partially functional, or failed category. Knees in which the ACL reconstruction was considered func- tional had less than 3 mm of increased AP displace- ment over the contralateral knee. Partial function was assigned to knees that had between 3 mm and 5.5 mm of increased displacement at follow-up, a correction of 50% or more, and an improvement of 3 mm or more compared with the preoperative difference in AP dis- placement between knees. The ACL reconstruction was considered a failure in knees that had a follow-up test result of greater than 5.5 mm, a correction of less than 50%, or an improvement of less than 3 mm com- pared with the preoperative value.
A comprehensive clinical examination of the knee was performed, with rating of effusion, range of knee motion, and tibiofemoral and patellofemoral crepitus.ll Subluxation was recorded in millimeters for all too-
T A B L E 1. Operations Before the Index Procedure
Operations Number
Arthroscopy, debridement 38 Medial meniscectomy (partial or total) 24 Lateral meniscectomy (partial or total) 18 Anterior cruciate ligament reconstruction 16 Meniscus repair 3 Other 3 Total 102

26 F. R. NOYES AND S.D. BARBER-WESTIN
tions of both knees] 4 The results of the pivot shift test were recorded on a scale of 0 to 3: 0, no pivot; grade 1, a slip; grade 2, a jerk with gross subluxation; and grade 3, gross subluxation with impingement of the posterior aspect of the lateral tibial plateau against the femoral condyle. Medial and lateral joint openings were assessed at 0 ° and 25 ° of knee flexion. Posterior displacement was measured at 90 ° of flexion.
Radiographic analyses were conducted on all knees and included assessment of patellofemoral and tibio- femoral joint space using anteroposterior views, lateral views with the knee flexed 30 °, and patellofemoral axial views.
During the ACL reconstruction, the appearance of the articular cartilage was classified according to our previously described systemJ 5 Surface abnormalities were categorized as grade I (softening), grade II (fis- suring and fragmentation), or grade III (exposed bone). Each category was then divided into subtype A or B depending on whether the depth of the lesion was less than or more than one half the depth of the articular surface. For this study, only grade IIB, IIIA, and IIIB lesions with an area of at least 15 mm were classified as abnormal, or as having advanced deterioration.
The rating system used to evaluate symptoms, func- tional limitations during sports and daily activities, and changes in the level of activity has been previously described in detail. 2'~6 The overall rating, which as- sessed 20 factors, was calculated as the difference in the total number of points from preoperative to follow- up examination on a 100-point scale. Thirty-eight pa- tients completed an overall rating of the knee condition based on a 1-10 point scale, where 1-2 points indicated a poor knee; 3-4 points, a fair knee; 5-6 points, a good knee; 7-8 points, a very good knee; and 10 points, a normal knee.
Surgical Procedure and Rehabilitation The arthroscopic-assisted ACL allograft operative
procedure has been previously described in detail. 16 All allografts were obtained from tissue banks certified by the American Association of Tissue Banks and 32 (80%) received 2.5 Mrads of gamma irradiation prior to implantation. The others received no secondary ster- ilization, as they were implanted prior to the initiation of our irradiation protocol which began in mid-1987. There was no statistically significant difference be- tween knees that had grafts which had been secondarily sterilized with irradiation and those that had not re- ceived sterilization in AP displacement testing or the overall rating scores at follow-up. Additional operative procedures performed with the ACL reconstruction in-
cluded four partial meniscectomies and nine arthros- copically-assisted meniscal repairs. 17
The postoperative program included immediate knee motion for all patients and has been described in detail elsewhere. 16 Partial weight bearing was begun on the 7th postoperative day and was slowly progressed to full by the 8th postoperative week. Immediately post- operatively, all patients were allowed a range of motion of 0 ° to 90 °. The range of flexion was advanced to 120 ° by the 2nd postoperative week and to 135 ° by the 3rd postoperative week. Any patient who had dif- ficulty in regaining a normal range of knee motion (0 to 135 °) was placed in a specific program of treatment as described previously. TM
Exercises were begun the day after the operation in all patients and included mobilization of the patella, straight-leg raises, isometric exercises, closed-chain exercises (mini-squats), and electrical muscle stimula- tion. A swimming program was initiated at the 3rd postoperative month. Modifications to our standard program were made for these patients in an attempt to avoid further damage to the articular cartilage surfaces. These included the avoidance of stationary bicycling, stair machines, progressive resistance quadriceps exer- cises in the 0 ° to 30 ° range, and a delay or avoidance of return to running and athletic activities that involved jumping, twisting, and turning. Patients who wished to return to strenuous sports activities were advised of the risk of further cartilage deterioration, and were only given medical consent to participate when muscle strength tests showed that the strength of the quadri- ceps on the involved limb was at least 70% of that of the contralateral limb, and no pain or swelling was incurred with or after the activities. We strongly rec- ommended, in the majority of these patients, a return to light recreational sporting pursuits and to avoid high- impact athletic activities.
Articular Cartilage Findings A total of 64 advanced articular cartilage lesions
were found in the 40 knees. The medial tibiofemoral compartment was affected in 22 patients (55%); the lateral tibiofemoral compartment, in 17 patients (43%); and the patellofemoral compartment, in 16 patients (40%). Twenty-four patients (60%) had one advanced lesion, l0 patients (25%) had two lesions each, four patients (10%) had three lesions each, and two patients (5%) had four lesions each.
Fifteen knees (38%) had subchondral bone exposure in at least one compartment and 25 knees (62%) had fissuring and fragmentation extending into greater than one-half of the depth of the cartilage and over an area of at least 15 mm in at least one compartment.

ACL RECONSTRUCTION AND KNEE ARTHROSIS 27
Thirty-four knees had at least one advanced articular cartilage lesion in the medial or lateral tibiofemoral compartment; 27 (79%) of these had previously had a meniscectomy in the corresponding tibiofemoral com- partment.
Statistical Analysis All statistical analyses were conducted on StatView
II software (Brainpower, Calabases, California). Paired two-tailed Student t tests and chi-square tests were used to determine significant differences for the vari- ables that were rated preoperatively and at follow-up. The level of significant was P < .05. A second analysis was performed on the difference in results between the 15 patients in whom grade IIIA or IIIB (subchondral bone exposure) articular cartilage deterioration was noted and the 25 patients in whom grade IIB (fissuring and fragmentation extending greater than one-half of the depth of the cartilage) cartilage lesions were found.
% of Knees
45
40
35
30
25
20
15
10
5
0 Pain with ADL
Daily activities
38%
Light Moderate Strenuous sports sports sports
Pain Scale*
• Preoperative
[ ] Follow-up
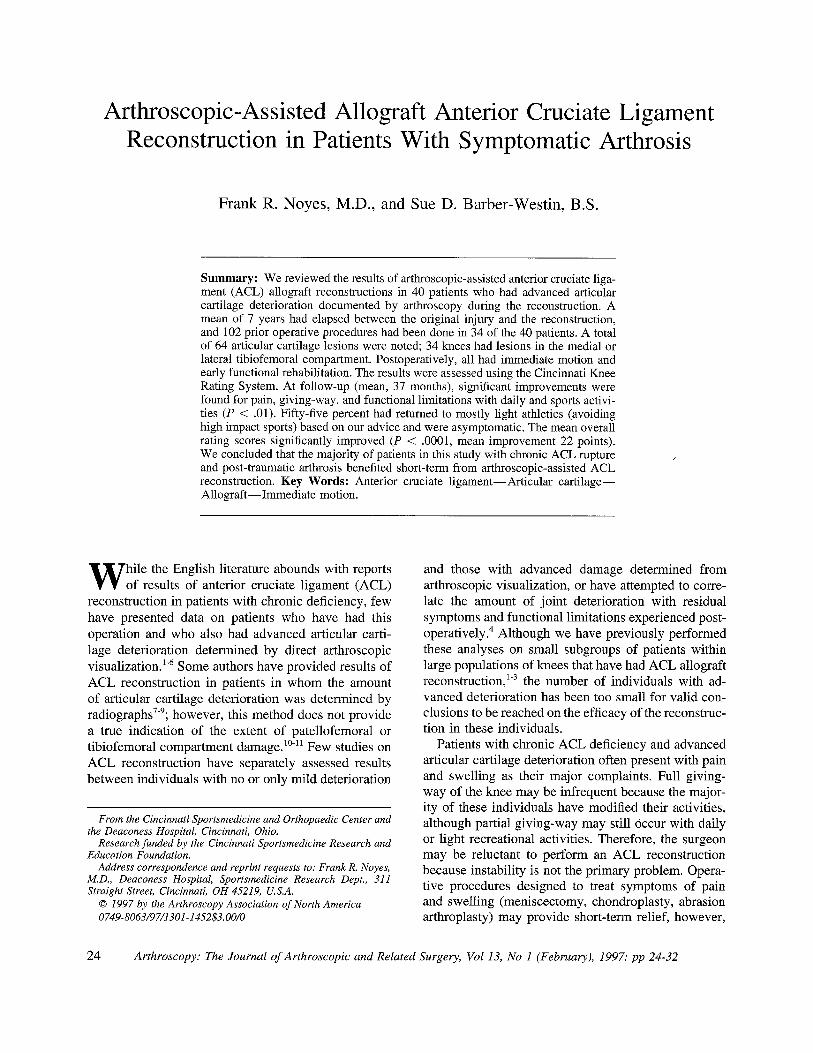
FIG 1. The distribution of the patient responses to the pain scale are shown preoperatively and at follow-up. The improvement was significant (P < .01). Light sports = swimming, bicycling; moderate sports = running, twisting, turning; and strenuous sports = jumping, hard pivoting, cutting.
RESULTS
Objective Evaluation and Examination of the Knee
Before the operation, all patients had 4.5 mm or more increased AP displacement on the involved knee compared with the contralateral limb. The mean preop- erative difference in AP displacement between the in- volved and contralateral limb at 89 N was 9.9 _+ 3.2 ram. At follow-up, 40% (14 of the 35 patients tested) had less than 3 mm of increased AP displacement at 89 N of force; at 134 N, 44% were within this range (Table 2). Eighteen grafts (45%) were classified as functional; 10 (25%), as partially functional; and 12 (30%), as failed. Patients who had articular cartilage lesions with subchondral bone exposure had signifi- cantly greater mean AP displacements (6.6 _+ 5.2 ram) at 134 N at follow-up than those who had lesions of fissuring and fragmentation (2.7 +_ 3.9 ram, P = .05). There was no significant difference in mean AP dis- placements between these subgroups at 89 N.
Preoperatively, all patients had a grade 2 or grade
TABLE 2. Results of Arthrometer Testing at Follow-up
Difference Involved- Noninvolved
(mm) 89 Newtons 134 Newtons
<3 40% 44% 3-5.5 37% 32% ->6 23% 24% Mean _+ SD 3.6 _+ 3.2 4.3 _+ 4.8
3 pivot shift test. At follow-up, 31 patients (78%) had a grade 0 or 1 pivot shift; 7 patients (18%), a grade 2; and 2 patients, a grade 3.
Preoperatively, two patients had 5 mm of increased medial joint opening to valgus stress at 25 ° of knee flexion and the remainder had no increase in this test. At follow-up, no patient had an increase in medial joint opening. Preoperatively, five patients had 5 mm of increased lateral joint opening to varus stress at 25 ° of knee flexion preoperatively and the remainder had no increase. At follow-up, two patients had 5 m m of in- crease in lateral joint opening. No patient had an in- crease in posterior displacement either before or after the reconstruction.
Preoperatively, 11 patients had palpable moderate patellofemoral crepitus and the remainder had no or only mild crepitus. At follow-up, three patients had moderate patellofemoral crepitus that was not detected preoperatively. The conversion rate for increased crep- itus over the preoperative condition was 10% (3 of 29 knees).
Subjective Evaluation and Return to Activities Statistically significant improvements were found
between the preoperative and follow-up scores for the symptoms of pain, partial giving-way, and full giving- way (P < .01 for all comparisons). The distributions of the patient responses to pain and full giving-way questions before the operation and at follow-up are shown in Figs 1 and 2 respectively. Before the opera- tion, 12 patients (30%) had pain with daily activities. At follow-up, 7 of these patients (18%) continued to have pain with daily activities.
28 F. R. NOYES AND S.D. BARBER-WESTIN
% of Knees
80 78%
70
60 ,~ 66 ,~
46
30 30% 27o/,0
° o lrL 2°Lo 10
G-W Daily Light Moderate Strenuous with activities sports sports sports ADL
• Preoperative
[ ] Follow-up
Full Giving-Way Scale*
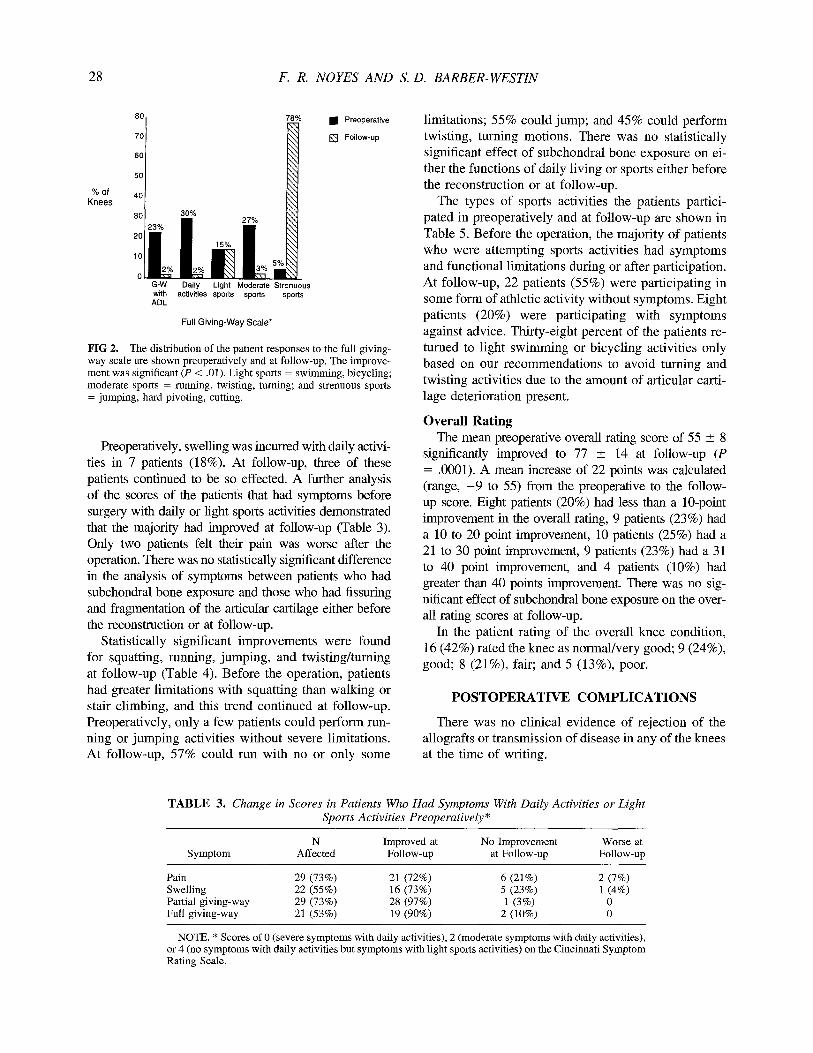
FIG 2. The distribution of the patient responses to the full giving- way scale are shown preoperatively and at follow-up. The improve- ment was significant (P < .01). Light sports = swimming, bicycling; moderate sports = running, twisting, turning; and strenuous sports = jumping, hard pivoting, cutting.
Preoperatively, swelling was incurred with daily activi- ties in 7 patients (18%). At follow-up, three of these patients continued to be so effected. A further analysis of the scores of the patients that had symptoms before surgery with daily or light sports activities demonstrated that the majority had improved at follow-up (Table 3). Only two patients felt their pain was worse after the operation. There was no statistically significant difference in the analysis of symptoms between patients who had subchondral bone exposure and those who had fissuring and fragmentation of the articular cartilage either before the reconstruction or at follow-up.
Statistically significant improvements were found for squatting, running, jumping, and twisting/turning at follow-up (Table 4). Before the operation, patients had greater limitations with squatting than walking or stair climbing, and this trend continued at follow-up. Preoperatively, only a few patients could perform run- ning or jumping activities without severe limitations. At follow-up, 57% could run with no or only some
limitations; 55% could jump; and 45% could perform twisting, turning motions. There was no statistically significant effect of subchondral bone exposure on ei- ther the functions of daily living or sports either before the reconstruction or at follow-up.
The types of sports activities the patients partici- pated in preoperatively and at follow-up are shown in Table 5. Before the operation, the majority of patients who were attempting sports activities had symptoms and functional limitations during or after participation. At follow-up, 22 patients (55%) were participating in some form of athletic activity without symptoms. Eight patients (20%) were participating with symptoms against advice. Thirty-eight percent of the patients re- turned to light swimming or bicycling activities only based on our recommendations to avoid turning and twisting activities due to the amount of articular carti- lage deterioration present.
Overall Rating The mean preoperative overall rating score of 55 _+ 8
significantly improved to 77 _+ 14 at follow-up (P = .0001). A mean increase of 22 points was calculated (range, - 9 to 55) from the preoperative to the follow- up score. Eight patients (20%) had less than a 10-point improvement in the overall rating, 9 patients (23%) had a 10 to 20 point improvement, 10 patients (25%) had a 21 to 30 point improvement, 9 patients (23%) had a 31 to 40 point improvement, and 4 patients (10%) had greater than 40 points improvement. There was no sig- nificant effect of subchondral bone exposure on the over- all rating scores at follow-up.
In the patient rating of the overall knee condition, 16 (42%) rated the knee as normal/very good; 9 (24%), good; 8 (21%), fair; and 5 (13%), poor.
POSTOPERATIVE COMPLICATIONS
There was no clinical evidence of rejection of the allografts or transmission of disease in any of the knees at the time of writing.
TABLE 3. Change in Scores in Patients Who Had Symptoms With Daily Activities or Light Sports Activities Preoperatively*
N Improved at No Improvement Worse at Symptom Affected Follow-up at Follow-up Follow-up
Pain 29 (73%) 21 (72%) 6 (21%) 2 (7%) Swelling 22 (55%) 16 (73%) 5 (23%) 1 (4%) Partial giving-way 29 (73%) 28 (97%) 1 (3%) 0 Full giving-way 21 (53%) 19 (90%) 2 (10%) 0
NOTE. * Scores of 0 (severe symptoms with daily activities), 2 (moderate symptoms with daily activities), or 4 (no symptoms with daily activities but symptoms with light sports activities) on the Cincinnati Symptom Rating Scale.

ACL RECONSTRUCTION AND KNEE ARTHROSIS 29
TABLE 4. Subjective Assessment of Functional Limitations With Daily Activities and Sports Activities
Preoperative Follow -up
Function* Number Percent Number Percent P Value
Walking 30-40 points 34 84% 38 95% 0.18 20 points 3 8% 0 - - 0 points 3 8% 2 5%
Stair Climbing 30-40 points 32 79% 36 89% 0.23 20 points 5 13% 1 3% 0 points 3 8% 3 8%
Squatting/kneeling 30-40 points 16 40% 28 70% 0.03 20 points 8 20% 4 10% 0 points 16 40% 8 20%
Running 80-100 points 10 25% 23 57% 0.009 60 points 12 30% 9 23% 40 points 18 45% 8 20%
Jumping 800-100 points 6 15% 22 55% 0.0001 60 points 6 15% 9 22% 40 points 28 70% 9 22%
Twisting/turning 80-100 points 3 7% 18 45% 0.0001 60 points 8 20% 11 28% 40 points 29 73% 11 28%
NOTE. *30-40 points, unlimited or only some limitations; 20 points, only a few blocks possible walking, only 11-30 steps possible stair climbing, only 6-10 squats possible; 0 points, cane, crutch or cannot do. 100-80 points, fully competitive or some limitations; 60, half speed; 40, cannot do.
A normal range of knee mot ion (0 ° to 135 °) was
restored within the first postoperative year in all knees
except one that had a mild l imitat ion of extension (1 °
to 5°). No patient in this series required a manipulat ion or arthroscopic lysis of adhesions for a knee motion
complication.
Two patients developed saphenous neuralgia of the sympathet ical ly-maintained type postoperatively. In
both, a series of saphenous nerve blocks were per-
formed. At follow-up, these individuals continued to
complain of discomfort with daily activities.
Twenty-n ine patients had operations done after the
index procedure. Of these, 26 had arthroscopy and
removal of the tibial interference screws and two had removal of the screws without arthroscopy; this com-
plication after allograft ACL reconstruction has been
TABLE 5. Sports Activities
Preoperative Follow up
Number Percent Number Percent
Type of Sport Jumping, hard pivoting, cutting Running, twisting, turning Swimming, bicycling only None
Change from preoperative levels Increased level, no symptoms Same level, no symptoms Decreased level, no symptoms Playing with symptoms No participation due to knee
condition
2 5% 10 25% 6 15% 5 12% 7 17% 15 38%
25 63% 10 25%
15 38% 3 7% 4 10% 8 20%
10 25%

30 F. R. NOYES AND S.D. BARBER-WESTIN
discussed previously. 2 Two patients had new meniscal injuries which required partial meniscectomy, and one patient had an arthroscopic-assisted implantation of a whole meniscus allograft. 19 Diagnostic arthroscopy and articular cartilage surface rating was done in 24 patients a mean of 15 months (range, 7 to 46 months) postoperatively. In six knees, surfaces which had ap- peared normal during the index procedure showed noteworthy fissuring and fragmentation during follow- up arthroscopy. None of the advanced lesions which had been noted during the index procedure showed significant deterioration at follow-up arthroscopy.
DISCUSSION
The results of this study showed that the ACL recon- structive procedure was effective in reducing symp- toms and functional limitations, and in allowing the majority of patients to return to light recreational or daily activities asymptomatically. We were encouraged by the early results of this ACL stabilization procedure performed in knees which represented, for many, worst case scenarios for the clinician. The majority of pa- tients (34 of 40, 85%) had already had operative proce- dures before the ACL reconstruction. A mean of 7 years had elapsed between the original knee injury and the stabilization procedure. During this time, 34 patients (85%) had suffered at least one additional full giving-way reinjury. Additionally, 29 patients (73%) had suffered meniscal damage and lost some, if not all, meniscal function prior to the reconstruction. These conditions, and the resultant knee with ACL-defi- ciency, meniscal loss, severe articular cartilage deterio- ration, and gross instability due to loss of secondary restraints, represent a tremendous challenge in terms of treatment decision criteria. 2° While the data showed improvement in the subjective variables of pain and giving-way and ability to perform daily activities, opti- mal results are expected in knees which undergo stabi- lization prior to the development of advanced cartilage surface deterioration. ACL reconstruction should, therefore, be seriously considered early after injury in athletically active patients 1~'2° and, as well, should be considered early in the course of treatment in the chronically-deficient knee which begins to demonstrate early signs of cartilage deterioration where instability symptoms are present. Although the majority of pa- tients in the present study were able to return to some form of activity, 38% (15 of 40) were swimming or bicycling only. We counseled all of the patients in this study regarding realistic goals of the stabilization procedure in terms of future athletic activity, and advo- cated avoidance of sports involving jumping, cutting,
and pivoting which we believe may be deleterious to the joint over the long-term. Patients who choose con- servative treatment should be made aware that, if artic- ular cartilage deterioration develops, changes in the goals of ACL reconstruction occur and usually do not include the return to more strenuous occupational or sports activities.
We have previously reported 3 significant differences in symptoms and functional limitations following ACL allograft reconstruction between patients with normal or only slightly damaged articular cartilage and pa- tients with abnormal surfaces (as defined in the present study). Additionally, we 2 and others 4 have noted sig- nificant correlations between the presence of abnormal cartilage surfaces and increased pain and difficulties with activities of daily living. Tria et al. followed 29 patients between 2 and 4 years following central one- third patellar tendon ACL reconstruction, 17 of whom demonstrated articular cartilage deterioration on the medial femoral condyle and 7 of whom had similar changes in the patellofemoral region. 4 The overall rat- ing, which assessed symptoms and functional limita- tions, showed significant differences between knees with cartilage deterioration and those with normal sur- faces. The authors concluded that changes on the me- dial femoral condyle or patellofemoral joint compro- mise the results of ACL reconstruction.
In a study similar to ours, Shelbourne and Wilckens assessed the results of ACL bone-patellar ligament- bone autograft reconstruction performed in 33 young patients whose articular cartilage condition was as- sessed radiographically. 9 A broad spectrum of patients were included in the study whose knee joint arthrosis was rated from mild degeneration (decreased joint space) to severe degeneration (severe joint space loss). No data was provided on the actual condition of the articular cartilage during the ACL reconstruction. Im- mediate knee motion was emphasized and rehabilita- tion was modified to provide adequate muscle strength for daily activities. Significant improvement in pain and functional impairment and an increase in activity level postoperatively were reported. We agree with these authors' conclusions that ACL reconstruction and immediate knee motion are valid treatment options in the ACL deficient knee with mild to moderate arthro- sis, assuming functional limitations exist. We also agree with these investigators that a trial of function in a functional knee brace in patients who have pain and instability is an option to consider in selecting those who would benefit from ACL reconstruction. Functional braces can provide stability and pain relief under low forces involved with daily activities. Pa- tients may determine if ACL reconstruction is war-

A C L R E C O N S T R U C T I O N A N D K N E E A R T H R O S I S 31
ranted based on the resultant effect of the brace in reducing pain and instability symptoms. These braces may not be effective, however, under high loading conditions (athletics), and their long-term ability to delay ACL reconstructions in these knees is unknown.
Zaricznyj reported pain relief in a small subgroup of individuals (9 of 27) with arthritic changes documented on radiographs and at surgery following semitendinosus tendon graft ACL reconstruction. 5'6 Following patients between 2 and 9 years postoperatively, this author con- cluded that the restoration of stability delayed further deterioration of the joint. However, none of the patients with pre-existing arthritic changes had actual measures or visualization of the condition of the articular cartilage postoperatively such as follow-up arthroscopy or mag- netic resonance imaging. Even so, the majority of these patients benefited from the procedure and had returned to light sports or moderate work activities. Shino, et al provided arthroscopic documentation of articular carti- lage surfaces in 49 of 201 patients (24%) who received allograft ACL reconstruction a mean of 30 months post- operatively. 21 Patients who had pre-existing articular car- tilage deterioration in the tibiofemoral joint, loss of the corresponding meniscus, and who had returned to strenu- ous activities showed continued deterioration of the carti- lage surfaces. The authors concluded that ACL recon- struction in these knees is only indicated when giving- way occurs with daily activities.
What remains in question is the ability of an ACL reconstructive procedure to prevent or delay worsening of the existing articular cartilage changes. In our study, evidence was shown of further joint deterioration in a small number of patients. Twenty-four of the 40 pa- tients (60%) had follow-up arthroscopy a mean of 15 months postoperatively. None of the articular cartilage lesions which had been noted during the ACL recon- struction demonstrated further deterioration. However, in six of these knees, deterioration was found in sur- faces other than those recorded during the first arthros- copic procedure. Three of these patients had returned to sports involving jumping, pivoting and cutting post- operatively with symptoms against our advice, one had returned to light recreational activities with no prob- lems, and two had not returned to any type of athletic activities.
Historically, the presence of moderate to severe ar- ticular cartilage deterioration has been viewed as a relative contraindication to ACL reconstruction. A marked reduction in activity level and even giving- way have been tolerated due to the opinion that it is too late for reconstructive intervention in these pa- tients. This study has shown, using modern arthros- copic techniques, immediate knee motion and early
protected activity, that ACL reconstruction benefits these patients by increasing activity levels and decreas- ing symptoms without apparently further accelerating the joint destruction, at least in the short-term. It is our goal to provide at least a decade or more of added time to these knees prior to the requirement of total knee arthroplasty or other major operative intervention. A contraindication for ACL reconstruction in knees with severe articular cartilage deterioration is the presence of subchondral bone exposure on two opposing articu- lar cartilage surfaces, or severe bone concavity. Knees which have deteriorated to the extent where secondary osseous changes provide stability and symptoms relate to the arthrosis rather than true instability are also not candidates for ACL reconstruction. These demonstrate a negative pivot shift test, a mildly positive Lachman test, and radiographic evidence of intercondylar osteo- phytes, flattening of the femoral condyles, and a pe- ripheral osteophyte ring of the lateral tibial plateau. 11
The failure rate calculated for the allografts in this study is consistent with our prior report 1 on allografts used for chronic ACL deficiency alone (failure rate, 29%) and combined with a ligament augmentation de- vice (failure rate, 30%). Currently, bone-patellar ten- don-bone autografts are our preferl"ed graft of choice for ACL reconstruction. Allografts are reserved for revision procedures s where suitable autogenous tissues have been previously compromised.
REFERENCES
1. Noyes FR, Barber SD. The effect of a ligament-augmentation device on allograft reconstructions for chronic ruptures of the anterior cruciate ligament. J Bone Joint Surg Am 1992;74:960- 973.
2. Noyes FR, Barber SD. The effect of an extra-articular procedure on allograft reconstructions for chronic ruptures of the anterior cruciate ligament. J Bone Joint Surg Am 1991;73:882-892.
3. Noyes FR, Barber-Westin SD, Roberts CS. Use of allografts after failed treatment of rupture of the anterior cruciate ligament. J Bone Joint Surg Am 1994;76:1019-1031.
4. Tria AJ, Alicea JA, Cody RP. Patella baja in anterior cruciate ligament reconstruction of the knee. Clin Orthop 1994; 299:229- 234.
5. Zaricznyj B. Reconstruction of the anterior cruciate ligament of the knee using a doubled tendon graft. CIin Orthop 1987;220: 162-175.
6. Zaricznyj B. Reconstruction of the anterior cruciate ligament using free tendon graft. Am J Sports Med 1983; 11:164-176.
7. Aglietti P, Buzzi R, D'Andria S, Zaccherotti G. Long-term study of anterior cruciate ligament reconstruction for chronic instabil- ity using the central one-third patellar tendon and a lateral extra- articular tenodesis. Am J Sports Med 1992;20:38-45.
8. Buss DD, Warren RF, Wickiewicz TL, Galinat B J, Panariello R. Arthroscopically assisted reconstruction of the anterior cruciate ligament with use of autogenous patellar-ligament grafts. J Bone Joint Surg Am 1993;75:1346-1355.
9. Shelbourue KD, Wilckens JH. Intraarticular anterior cruciate ligament reconstruction in the symptomatic arthritic knee. Am J Sports' Med 1993;21:685-689.

32 F. R. NOYES AND S .D. BARBER-WESTIN
10. Lysholm J, Hamberg P, Gillquist J. The correlation between osteoarthrosis as seen on radiographs and on arthroscopy. Arthroscopy 1987; 3:161-165.
11. Noyes FR, Mooar PA, Matthews DS, Butler DL. The symptom- atic anterior cruciate-deficient knee. Part I. The long-term func- tional disability in athletically active individuals. J Bone Joint Surg Am 1983;65:154-162.
12. Daniel DM, Malcom LL, Losse G, Stone ML, Sachs R, Burks R. Instrumented measurement of anterior laxity of the knee. J Bone Joint Surg Am 1985;67:720-726.
13. Wroble RR, Van Ginkel LA, Grood ES, Noyes FR, Shaffer BL. Repeatability of the KT-1000 arthrometer in a normal popula- tion. Am J Sports Med 1990; 18:396-399.
14. Noyes FR, Grood ES. Diagnosis of knee ligament injuries: Clin- ical concepts. In: Feagin JA Jr, ed. The crucial Ligaments. Diag- nosis and treatment of Ligamentous injuries about the knee. New York: Churchill Livingstone, 1988;261-285.
15. Noyes FR, Stabler CL. A system for grading articular cartilage lesions at arthroscopy. Am J Sports Med 1989; 17:505-513.
16. Noyes FR, Barber SD, Mangine RE. Bone-patellar ligament- bone and fascia lata allografts for reconstruction of the anterior cruciate ligament. J Bone Joint Surg Am 1990;72:1125-1136.
17. McLanghlin JR, Noyes FR. Arthroscopic meniscus repair: rec- ommended surgical techniques for complex meniscal tears. Tech Orthop 1993;8:129-136.
18. Noyes FR, Mangine RE, Barber SD. The early treatment of motion complications after reconstruction of the anterior cruci- ate ligament. Clin Orthop 1992;277:217-228.
19. Noyes FR, Barber-Westin SD. Irradiated meniscus allografts in the human knee. A two to five year follow-up study. Orthop Trans 1995; 19:417.
20. Noyes FR, Matthews DS, Mooar PA, Grood ES. The symptom- atic anterior cruciate-deficient knee. Part II. The results of reha- bilitation, activity modification, and counseling on functional disability. J Bone Joint Surg Am 1983;65:163-174.
21. Shino K, Inoue M, Nakamura H, Hamade M, Ono K. Arthros- copic follow-up of anterior cruciate ligament reconstruction us- ing allogenec tendon. Arthroscopy 1989;5:165-171.





























