Embed Size (px)
Citation preview

10
Friday General Session
Arthropod‐borneInfectionsinFamilyMedicine
JonathanMacClements,MDAssociate Dean and DIO of Graduate Medical Education, Department of Medical Education UT Austin Dell Medical School Austin, Texas EducationalObjectivesBy completing this educational activity, the participant should be better able to:
1. Describe various arthropod-borne infections that may affect patients. 2. Discuss the epidemiology of Rocky Mountain Spotted Fever, Lyme Disease,
West Nile Virus, Dengue, Chikungunya, Ricketts, and Zika Virus. 3. Recognize the signs and symptoms of various arthropod-borne infections.
SpeakerDisclosure Dr. MacClements has disclosed that he has no actual or potential conflict of interest in relation to this topic.

1
Jonathan MacClements, MD, FAAFPProfessor of Family Medicine, UT Austin Dell Medical School
CAQ Adolescent MedicineCAQ Hospice and Palliative Medicine
ASTMH Certificate of Knowledge in Tropical Medicine and Travelers’ Health
Arthropod‐borne Infections and Conditions
Disclosures
• Nothing to disclose.
• I have or my spouse has no relevant financial interest/arrangement, or affiliation with one or more commercial interest that could be perceived as a real or apparent conflict of interest in the context of this activity.
EDUCATIONAL OBJECTIVES
By the end of this educational activity, participants should be better able to:
• Describe various arthropod‐borne infections that may affect patients.
• Discuss the epidemiology of Rocky Mountain Spotted Fever, Lyme Disease, West Nile Virus, Dengue, Chikungunya, Ricketts, and Zika Virus.
• Recognize the signs and symptoms of various arthropod‐borne infections.
Arthropods
Vast invertebrate phylum:
– Arachnids (those with eight legs, such as spiders, mites, and ticks) and
– Insects (those with six legs [subphylum Hexapoda], such as mosquitoes, gnats, and flies)
WHO Key Factshttps://www.who.int/en/news‐room/fact‐sheets/detail/vector‐borne‐diseases
• Vector‐borne diseases account for more than 17% of all infectious diseases, causing more than 700,000 deaths annually.
• More than 3.9 billion people in over 128 countries are at risk of contracting Dengue, with 96 million cases estimated per year.
• Malaria causes more than 400,000 deaths every year globally, most of them children under 5 years of age.
• Other diseases such as Chagas disease, leishmaniasis and schistosomiasis affect hundreds of millions of people worldwide.
• Many of these diseases are preventable through informed protective measures.
WHO Key Facts
• Vector‐borne diseases are human illnesses caused by: parasites, viruses and bacteria
• Transmitted by: Mosquitoes, sandflies, triatomine bugs, blackflies, ticks, tsetse flies, mites, snails and lice.
• More than 700,000 deaths per years from diseases such as malaria, dengue, schistosomiasis, human African trypanosomiasis, leishmaniasis, Chagas disease, yellow fever, Japanese encephalitis and onchocerciasis, globally.
1 2
3 4
5 6

2
WIDOW SPIDERS
• Red coloration on the underside of their abdomen.
• Workplaces containing undisturbed areas.
• Two puncture marks in the skin.• The venom is a neurotoxin that
produces pain at the bite area and then spreads to the chest, abdomen, or the entire body.
BROWN RECLUSE SPIDERS• Brown in color with a characteristic dark violin‐shaped (or fiddle‐shaped) marking on its head and has six equal‐sized eyes (most spiders have eight eyes).
• Brown recluse spiders are usually found in workplaces with secluded, dry, sheltered areas
• Bites may cause a stinging sensation with localized pain.
• A small white blister usually develops at the site of the bite.
• Severe lesion with skin necrosis
• Generic sketch for transmission of diseases by ectoparasites (vectors). • Blocking of transmission can in principle occur at every stage, but most drugs aim to interfere during “Attachment” phase and/or “Feeding & Transmission” phase.
Int J Parasitol Drugs Drug Resist. 2017 Apr; 7(1): 90–109. Published online 2017 Jan 30. doi: 10.1016/j.ijpddr.2017.01.004
Ticks That Commonly Bite Humans
Ticks
• Lyme disease
• Rickettsial diseases (spotted fever and Q fever)
• Anaplasmosis
• Ehrlichiosis
• Relapsing fever (borreliosis)
• Tularemia
• Tick‐borne encephalitis
• Crimean‐Congo hemorrhagic fever
Selected Tick‐borne Diseases Reported to
CDC, U.S., 2016
https:/www.cdc.gov/ticks/tickbornediseases/overview.html/
7 8
9 10
11 12

3
Lyme Disease Reported Cases of Lyme Disease –United States, 2017
Spirochete: Borrelia burgdorferi • Ixodes scapularis or deer tick: Midwestern and Eastern United States
• Ixodes pacificus or Western black‐legged tick on the West Coast
• Lone star ticks (Amblyomma americanum) in the South
Early Signs and Symptoms (3 to 30 days after tick bite)
• Fever, chills, headache, fatigue, muscle and joint aches, and swollen lymph nodes
• Erythema migrans (EM) rash: – Occurs in approximately 70 to 80 percent of infected persons– Begins at the site of a tick bite after a delay of 3 to 30 days (average is about 7
days)– Expands gradually over a period of days reaching up to 12 inches or more (30
cm) across– May feel warm to the touch but is rarely itchy or painful– Sometimes clears as it enlarges, resulting in a target or “bull’s‐eye” appearance– May appear on any area of the body
https://www.cdc.gov/lyme/signs_symptoms/index.html
• Severe headaches and neck stiffness• Additional EM rashes on other areas of the body• Arthritis with severe joint pain and swelling, particularly the knees and other large
joints.• Facial palsy (loss of muscle tone or droop on one or both sides of the face)• Intermittent pain in tendons, muscles, joints, and bones• Heart palpitations or an irregular heart beat (Lyme carditis)• Episodes of dizziness or shortness of breath• Inflammation of the brain and spinal cord• Nerve pain• Shooting pains, numbness, or tingling in the hands or feet• Problems with short‐term memory
Later Signs and Symptoms (Days to Months After Tick Bite)
13 14
15 16
17 18

4
Variations of Rash
Post‐Treatment Lyme Disease Syndrome
• Non‐specific symptoms (like fatigue, pain, and joint and muscle aches) after the treatment of Lyme disease as having post‐treatment Lyme disease syndrome (PTLDS) or post Lyme disease syndrome (PLDS).
• The cause of PTLDS is not known.
• The term “chronic Lyme disease” (CLD) has been used to describe people with different illnesses:– In many occasions it has been used to describe symptoms in people who have no
evidence of a current or past infection with B. burgdorferi (Infect Dis Clin N Am.22:341‐60, 2008).
– Because of the confusion of term CLD experts do not support its use (New Engl J Med. 357:1422‐30, 2008).
Rocky Mountain Spotted Fever (RMSF)
• Agent: Rickettsia rickettsii• RMSF:
– American dog tick in the Eastern, Central and Western United States
– Rocky Mountain wood tick in the Rocky Mountain states– Brown dog tick in the Southwestern United States, along the U.S.‐Mexico border.
• Rapidly fatal if not treated within the first 5 days of symptoms.
• Before tetracycline antibiotics were available, case fatality rates ranged from 20–80%
• Incubation Period: 3–12 days
Signs and Symptoms
Early (1–4 Days)• High fever• Severe headache• Malaise• Myalgia• Edema around eyes and on the back of hands• Gastrointestinal symptoms (nausea, vomiting, anorexia)Late (5 Days and Beyond)• Altered mental status, coma, cerebral edema• Respiratory compromise (pulmonary edema, ARDS)• Necrosis, requiring amputation• Multi‐organ system damage (CNS, renal failure)
19 20
21 22
23 24

5
Rash• 2–5 days after onset of symptoms
• 10% never develop a rash
• Decision to treat should not be based on presence of rash
Early Rash
• Maculopapular: Small, flat, pink, non‐itchy spots (macules) initially
appear on the wrists, forearms, and ankles then spread to the trunk and
sometimes palms and soles
Late Rash
• Petechial: Red to purple spots (petechiae) are usually not seen until day 6
or later after onset of symptoms
• Petechial rash is considered a sign of progression to severe disease. Every
attempt should be made to begin treatment before petechiae develop
DiagnosisGeneral Laboratory Findings• Thrombocytopenia• Elevated hepatic transaminases• Hyponatremia• NOTE: Laboratory values are often within normal limits in early illness.Laboratory Diagnosis• Four‐fold change (typically rise) in IgG‐specific antibody titer by indirect immunofluorescence
antibody (IFA) assay in paired serum samples.• Detection of DNA in a skin biopsy specimen of a rash lesion by PCR assay or in an acute phase
whole blood specimen. Immunohistochemical (IHC) staining of organism from skin or tissue biopsy specimen.
• NOTE: Antibody titers are frequently negative in the first 7–10 days of illness. • NOTE: IgM antibodies are less specific than IgG antibodies and are more likely to generate false
positives. IgM results alone should not be used for laboratory diagnosis.
Rocky Mountain Spotted Fever Treatment Regimen
Age Category Drug Dosage Maximum Duration (Days)
Adults Doxycycline100 mg twice per
day, orally or IV100 mg/dose
Patients should be
treated for at least
3 days after the
fever subsides and
until there is
evidence of clinical
improvement.
Minimum course of
treatment is 5‐7
days.
Children
weighing <100
lbs. (45.4 kg)
Doxycycline
2.2 mg/kg per
dose twice per
day, orally or IV
100 mg/dose
.
Rickettsia parkeri Rickettsiosis
• Agent
• Rickettsia parkeri
• Gulf Coast ticks in the Southeastern and Mid‐Atlantic states, as well as parts of Southern Arizona
Babesiosis
nymphal stage of Ixodes scapularis ticks
Anaplasmosis
• Agent Anaplasma phagocytophilum
• Formerly known as Human Granulocytic Ehrlichiosis (HGE), and A. phagocytophilum was Ehrlichia phagocytophilum.
• Severe and life‐threatening illness is less common compared to other rickettsial diseases, such as Rocky Mountain spotted fever (RMSF) or E. chaffeensis ehrlichiosis.
25 26
27 28
29 30
6
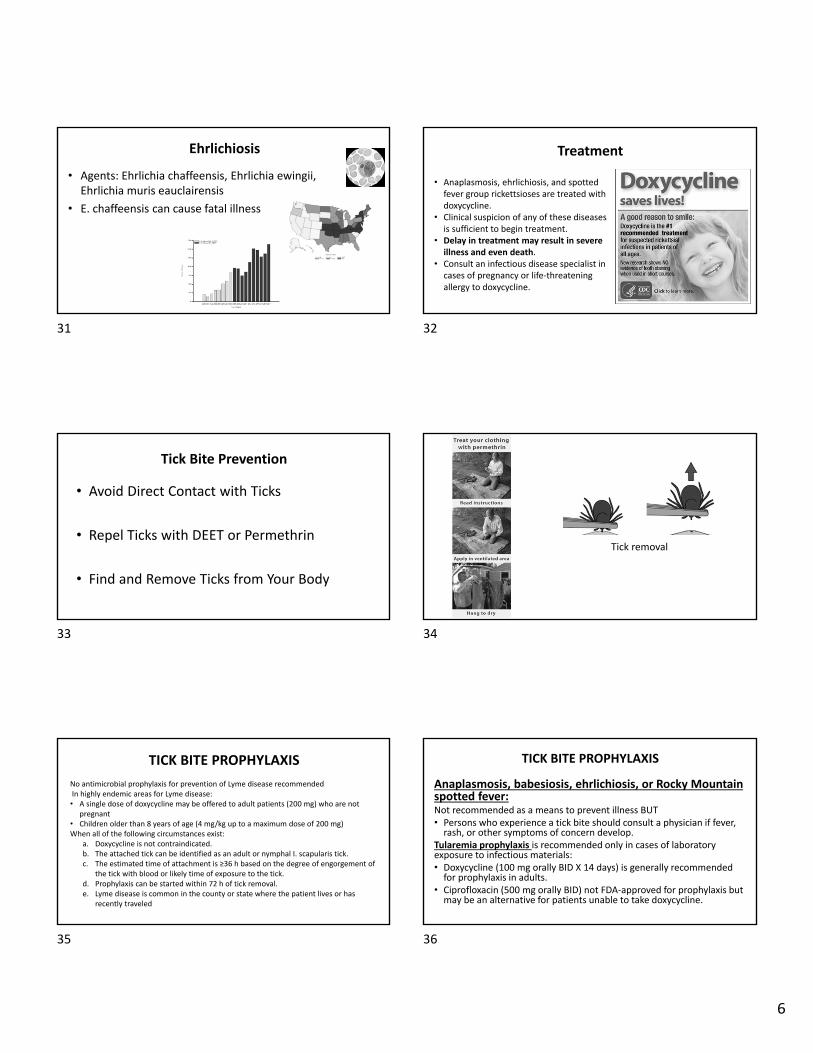
Ehrlichiosis
• Agents: Ehrlichia chaffeensis, Ehrlichia ewingii, Ehrlichia muris eauclairensis
• E. chaffeensis can cause fatal illness
Treatment
• Anaplasmosis, ehrlichiosis, and spotted fever group rickettsioses are treated with doxycycline.
• Clinical suspicion of any of these diseases is sufficient to begin treatment.
• Delay in treatment may result in severe illness and even death.
• Consult an infectious disease specialist in cases of pregnancy or life‐threatening allergy to doxycycline.
Tick Bite Prevention
• Avoid Direct Contact with Ticks
• Repel Ticks with DEET or Permethrin
• Find and Remove Ticks from Your Body
Tick removal
TICK BITE PROPHYLAXIS
No antimicrobial prophylaxis for prevention of Lyme disease recommendedIn highly endemic areas for Lyme disease:• A single dose of doxycycline may be offered to adult patients (200 mg) who are not
pregnant • Children older than 8 years of age (4 mg/kg up to a maximum dose of 200 mg) When all of the following circumstances exist:
a. Doxycycline is not contraindicated.b. The attached tick can be identified as an adult or nymphal I. scapularis tick.c. The estimated time of attachment is ≥36 h based on the degree of engorgement of
the tick with blood or likely time of exposure to the tick.d. Prophylaxis can be started within 72 h of tick removal.e. Lyme disease is common in the county or state where the patient lives or has
recently traveled
TICK BITE PROPHYLAXIS
Anaplasmosis, babesiosis, ehrlichiosis, or Rocky Mountain spotted fever:Not recommended as a means to prevent illness BUT• Persons who experience a tick bite should consult a physician if fever, rash, or other symptoms of concern develop.
Tularemia prophylaxis is recommended only in cases of laboratory exposure to infectious materials:• Doxycycline (100 mg orally BID X 14 days) is generally recommended for prophylaxis in adults.
• Ciprofloxacin (500 mg orally BID) not FDA‐approved for prophylaxis but may be an alternative for patients unable to take doxycycline.
31 32
33 34
35 36

7
Leishmaniasis
Sand fly
Cutaneous leishmaniasis
Visceral leishmaniasis. Sleeping Sickness
African trypanosomiasis
Tsetse flies
Chagas Disease
Triatomine bugs
Chagas disease (American trypanosomiasis)
Filariasis
37 38
39 40
41 42

8
Fleas and ChiggersPlague (Yersinia pestis from rats to humans)
Scrub typhusOrientia tsutsugamushi
Black Flies
• Onchocerciasis (river blindness)
• O. volvulus
Body Lice
• Spread:– Epidemic typhus,
– Trench fever, and – Epidemic relapsing fever
• Close person‐to‐person contact – Limited to persons who live under conditions of crowding and poor hygiene.
Tularemia‐F. tularensis bacteria
Mosquito‐transmitted Diseases
• Malaria• Dengue fever• Chikungunya fever• Zika virus• Yellow fever (best prevented by vaccination)• Filariasis• Viral encephalitis (e.g., Japanese encephalitis, Venezuelan equine encephalitis)
• Miscellaneous viral illnesses‐Rift Valley fever, West Nile fever, and Sindbis fever
Mosquitoes• Aedes– Chikungunya– Dengue fever– Lymphatic filariasis– Rift Valley fever– Yellow fever– Zika
• Anopheles– Malaria– Lymphatic filariasis
• Culex– Japanese encephalitis– Lymphatic filariasis– West Nile fever
https://en.wikipedia.org/wiki/Mosquito
43 44
45 46
47 48

9
West Nile Virus
https://www.cdc.gov/westnile/statsmaps/preliminarymapsdata2018/activitybystate2018.html
West Nile Virus Activity by State 2018
West Nile Virus Neuroinvasive Disease Incidence by State –United States, 2018 (as of January 8, 2019)
https://www.cdc.gov/westnile/statsmaps/preliminarymapsdata2018/incidencestate‐2018.html
Clinical Signs & Symptoms
• The incubation period is 2 to 6 days• 70‐80% subclinical or asymptomatic• Acute systemic febrile illness with:– Headache– Weakness– Myalgia, or arthralgia– Gastrointestinal symptoms– Transient maculopapular rash
Neuroinvasive Disease
• Less than 1% have meningitis, encephalitis, or acute flaccid paralysis.
• WNV meningitis is clinically indistinguishable from viral meningitis
• WNV encephalitis is a more severe clinical syndrome that usually manifests with fever and altered mental status, seizures, focal neurologic deficits, or movement disorders such as tremor or parkinsonism.
• Most women known to have been infected with WNV during pregnancy have delivered infants without evidence of infection or clinical abnormalities
• Routine clinical laboratory studies are generally nonspecific.
• In patients with neuroinvasive disease, CSF examination generally shows lymphocytic pleocytosis
• Brain magnetic resonance imaging is frequently normal
– Signal abnormalities in the basal ganglia, thalamus, and brainstem may be seen in patients with encephalitis, and in the anterior spinal cord in patients with poliomyelitis.
49 50
51 52
53 54

10
WNV Diagnosis
• Serum or cerebrospinal fluid (CSF) to detect WNV‐specific IgM antibodies.
• WNV‐specific IgM antibodies are usually detectable 3 to 8 days after onset of illness and persist for 30 to 90 days
• WNV IgG antibodies generally are detected shortly after IgM antibodies and persist for many years following a symptomatic or asymptomatic infection
• Viral cultures and tests to detect viral RNA (e.g., reverse transcriptase‐polymerase chain reaction [RT‐PCR]) can be performed on serum, CSF, and tissue specimens.
Treatment
• No vaccine or specific antiviral treatments for West Nile virus infection are available.
• Over‐the‐counter pain relievers can be used to reduce fever and relieve some symptoms.
• In severe cases, patients often need to be hospitalized to receive supportive treatment, such as intravenous fluids, pain medication, and nursing care.
Chikungunya
Aedes mosquitoes
Where Has Chikungunya Virus Been Found?
• Prior to 2013, chikungunya virus cases and outbreaks had been identified in countries in Africa, Asia, Europe, and the Indian and Pacific Oceans.
• In late 2013, the first local transmission of chikungunya virus in the Americas was identified in Caribbean countries and territories. Local transmission means that mosquitoes in the area have been infected with the virus and are spreading it to people. The virus then spread throughout most of the Americas.
Transmission
• Most often spread to people by Aedes aegypti and Aedes albopictus mosquitoes.
• Mosquitoes become infected when they feed on a person already infected with the virus.
• Infected mosquitoes then spread the virus to other people through bites.
• Rarely, from mother to child inutero
• Rarely, through infected blood
Symptoms
• Most will develop some symptoms• Symptoms usually begin 3–7 days after being• Most common symptoms are fever and joint pain• Other symptoms may include headache, muscle pain, joint swelling,
or rash• Does not often result in death, but the symptoms can be severe and
disabling• Most patients feel better within a week• In some people, the joint pain may persist for months• Once infected, protected from future infections
55 56
57 58
59 60

11
Laboratory Diagnosis
• Serum or plasma to detect virus, viral nucleic acid, or virus‐specific immunoglobulin (Ig) M and neutralizing antibodies.
• Viral culture may detect virus in the first 3 days of illness; however, chikungunya virus should be handled under biosafety level (BSL) 3 conditions.
• During the first 8 days of illness, chikungunya viral RNA can often be identified in serum.
Treatment
• There is no vaccine to prevent or medicine to treat virus
• Treat the symptoms:
– Rest
– Drink fluids to prevent dehydration
– Take medicine such as acetaminophen or paracetamol to reduce fever and pain
– NO aspirin and other non‐steroidal anti‐inflammatory drugs (NSAIDS until dengue can be ruled out to reduce the risk of bleeding)
• Prevent mosquito bites for the first week of illness
– During the first week of infection, chikungunya virus can be found in the blood and passed from an infected person to a mosquito through mosquito bites
– An infected mosquito can then spread the virus to other people
Zika
• Aedes species mosquito
– Aggressive daytime biters.
– Also bite at night.
• Zika can be passed from a pregnant woman to her fetus.
• Infection during pregnancy can cause certain birth defects.
• There is no vaccine or medicine.
https://www.nbcnews.com/storyline/zika‐virus‐outbreak/zika‐still‐emergency‐just‐different‐kind‐who‐says‐n686061
All Countries & Territories with Active Zika Virus Transmissionhttp://www.cdc.gov/zika/geo/active‐countries.html
Modes of Transmission
• Single‐stranded RNA virus of the Flaviviridae family, genus Flavivirus. Zika
• Bite of an infected Aedes species mosquito (Ae. aegypti and Ae. albopictus). T
• Nonhuman and human primates are likely the main reservoirs of the virus, and anthroponotic (human‐to‐vector‐to‐human) transmission occurs during outbreaks.
• Perinatal, in utero, and possible sexual and transfusion transmission events have been reported.
• Identified in asymptomatic blood donors during an ongoing outbreak.
61 62
63 64
65 66

12
Clinical Signs & Symptoms
• Most asymptomatic• Acute onset of
– Fever with– Maculopapular rash– Arthralgia, myalgia– Or conjunctivitis– And headache
• Severe disease requiring hospitalization is uncommon and case fatality is low• Cases of Guillain‐Barré syndrome • Pregnancy ‐microcephaly and other severe fetal brain defects
Diagnosis
• Clinical features, places and dates of travel, and activities.
• Testing whole blood, serum, or plasma to detect virus, viral nucleic acid, or virus‐specific immunoglobulin M and neutralizing antibodies.
Treatment
• No specific antiviral treatment • Supportive and can include rest, fluids, and use of analgesics and antipyretics.
• Evaluated and managed for possible dengue or chikungunya virus infection.
• Aspirin and other non‐steroidal anti‐inflammatory drugs (NSAIDs) should be avoided until dengue can be ruled out to reduce the risk of hemorrhage.
• Should be protected from further mosquito exposure during the first few days of illness to prevent other mosquitoes from becoming infected and reduce the risk of local transmission.
Dengue Fever
Dengue: Classic Dengue Fever, or “Break Bone Fever”
female Aedes aegypti mosquito
Acute onset of high fever 3–14 days Symptoms:• Anorexia and nausea• Frontal headache, retro‐orbital pain • Myalgias, arthralgias• Hemorrhagic manifestations• Rash
Low white blood cell count
Dengue Hemorrhagic Fever (DHF)
Fever lasts from 2 to 7 days consistent with dengue fever.
When the fever declines, warning signs develop. This marks the beginning of a 24 to 48 hour period capillaries become excessively leaky:
• Ascites• Pleural effusions• Shock• Possibly death
Low platelet count and hemorrhagic manifestations
Rose W, Jacob J E, Adhikari DD, Verghese VP. Dengue illness in children. Curr Med Issues 2017;15:95‐105
67 68
69 70
71 72

13
Malaria
Malaria Species
• Plasmodium
– Falciparum
– Malariae
– Vivax
– Ovale
Malaria
Symptoms• Fever• Chills• Headache• Nausea and vomiting• Muscle pain and fatigue
Other signs and symptoms may include:• Sweating• Chest or abdominal pain• Cough
73 74
75 76
77 78
14
Malaria Species Malaria Prevention
• Personal protective measures
– Transmissions (dusk to dawn)
– Insect repellent• Permethrin
• DEET 30‐35%
– Long sleeves, pants
– Bed nets & screens
• Chemo‐suppression
Principles of Malaria Chemo‐prophylaxis
• Inhibits parasite development – most do not prevent infection
• Take regardless of duration of stay in malaria endemic area
• Start 1‐3 weeks before travel for chloroquine and mefloquine
• Start 48 hrs. before travel for atovaquone/proguanil & doxycycline
Principles of Malaria Chemo‐prophylaxis
• Continue during travel & for 4 ‐6 weeks after leaving malaria area. (Malarone for 1 week)
• Numerous regimens. Do not change or abandon regimen
• May contract malaria despite prophylaxis
FEVER = MALARIA until proven otherwise up to 3 yrs. on returning
Anti‐Malarial Prophylaxis
1. Mefloquine
2. Doxycycline
3. Chloroquine phosphate
4. Hydroxy‐ chloroquine sulphate
5. Atovaquone/Proguanil
Emergency Self‐ Treatment
• Atovaquone/proguanil
Sig: 4 tablets daily for 3 days
79 80
81 82
83 84

15
Malaria Drug Resistance
• CRPF–All except Central America, Hispania & the Middle East
• MRPF –Borders of Thailand
• CRPV– Indonesia, Guyana, Brazil, Columbia, India
• PRPV– S.E. Asia, Somalia
Malaria Drugs in Pregnancy
• Recommended NO travel to chloroquine resistant area
• Chloroquine – Safe in all trimesters
• Mefloquine – Pregnancy category: B
• Atovaquone/Proguanil – cannot be used by pregnant or breastfeeding women.
• Contraindicated– Doxycycline
– Primaquine
Drugs in Children
• Chloroquine (Aralen)
• Mefloquine (Lariam)
• Atovaquone/Proguanil (Malarone)
• Doxycycline > 8yrs of age
• Primaquine caution in G6PD deficiency
Malaria: Future
• New diagnostic tools
• Vaccine
• New drugs
Yellow Fever
Aedes mosquito
The picture can't be displayed.
85 86
87 88
89 90

16
Vaccination Record
• Single dose lifelong immunity• Live virus vaccine• Recommended for people aged 9 months or older and who are traveling to or living in areas at risk for yellow fever virus in Africa and South America
• May be required for entry into certain countries
Insect Repellant
* Insect repellent brand names are provided for your information only. The Centers for Disease Control and Prevention and the U.S. Department of Health and Human Services cannot recommend or endorse any name brand products.
Personal Protective Measures
• Transmissions:– Malaria (dusk to dawn)– Zika (anytime but aggressive daytime)
• Insect repellent• Long sleeves, pants• Bed nets & screens
91 92
93 94
95 96

17
https://wwwnc.cdc.gov/travel/page/yellowbook‐home
Questions? References• https://wwwnc.cdc.gov/travel/page/yellowbook‐home• Arthropod Bites. GREGORY JUCKETT, MD, MPH, Am Fam Physician. 2013 Dec 15;88(12):841‐847.• https://www.cdc.gov/lyme/resources/TickborneDiseases.pdf• https://www.cdc.gov/dengue/resources/DengueDHF‐Information‐for‐Health‐Care‐
Practitioners_2009.pdf• Strickland: Hunter’s Tropical Medicine and Emerging Infectious Diseases, Eight ed. W.B. Saunders
Company, 2000.• Peters W, Gilles H. Tropical Medicine and Parasitology, Fourth Edition, Mosby‐Wolfe, 1997• The Sanford Guide to Antimicrobial Therapy, Sanford Guide, 2018• Chin J, Control of Communicable Diseases Manual, 17th Edition, American Public Health
Association, 2000• Edmond R, Rowland H. A Color Atlas of Infectious Diseases, Second Edition, Year Book Medical
Publishers, 1987• http://www.travax.com• http://www.who.org• http://www.astmh.org
97 98
99 100

Notes






























