Embed Size (px)
Citation preview

209
Received:April 2, 2015, Revised:April 20, 2015, Accepted:April 20, 2015
Corresponding to:Yong-Gil Kim, Division of Rheumatology, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 138-736, Korea. E-mail:[email protected]
pISSN: 2093-940X, eISSN: 2233-4718Copyright ⓒ 2015 by The Korean College of Rheumatology. All rights reserved.This is a Free Access article, which permits unrestricted non-commerical use, distribution, and reproduction in any medium, provided the original work is properly cited.
Clinical Image
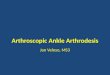
Figure 1. (A) T-spine X-ray, lateral. (B) Spinemagnetic reso-nance imaging: Newly ap-peared compression fracture at T9 and segmental cord signal change at T9 level (white arrow head). Posterolateral fusion masson T7-L1 that was misinterpreted as bony bridge were shown (white arrows). Additionally, bulging disc and facet arthrosis were shown at multiple level of spine.
Journal of Rheumatic Diseases Vol. 22, No. 3, June, 2015http://dx.doi.org/10.4078/jrd.2015.22.3.209
Arthrodesis Radiologically Mimicking Ankylosing Spondylitis
Yunkyoung Lee1, Yong-Gil Kim1, Myung Jin Shin2
Departments of 1Internal Medicine and 2Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
A 73-year-old male with back pain was hospitalized for managing new onset T9 compression fracture. The initial radiograph of T-spine showed kyphotic angulation of low-er thoracic spine with syndesmophyte formations ante-riorly and bridging bony lesions posteriorly (Figure 1), which was reported as suggestive of ankylosing spondyli-tis (AS) by radiologist. So he was consulted to rheumatol-ogist to rule out AS.His back pain has been persistent for several decades
and tended to be relieved by rest. The range of motion in thoracic and lumbar spine was not checked fully because of severe back pain, however, the movement of cervical spine was perfectly saved. In laboratory data, erythrocyte
sedimentation rate and C-reactive protein was 71 mm/h and 1.1 mg/dL. However, human leukocyte antigen-B27 allele was absent. We discussed again with senior musculoskeletal radiol-
ogist about the radiologic findings, because clinical fea-tures and radiographic findings were not consistent. An incision scar on his back was found on spine magnetic res-onance imaging (Figure 2A) and large bony defect with deformity on both iliac crest was identified on pelvic sim-ple X-ray as a sequelae of previous bone harvest site (Figure 2B). We repeatedly done a history taking then we confirmed his history of total laminectomy with posterior lumbar fusion operation using a bone-graft [1] for certain

Yunkyoung Lee, et al.
210 J Rheum Dis Vol. 22, No. 3, June, 2015
Figure 2. (A) Incision line for posterior lumbar fusion oper-ation (white arrow). (B) Irregular postoperative change at alar of both ilium (white arrows) due to bone harvest. There was no evi-dence of sacroiliitis.
spine fracture more than 40 years ago. Finally, we con-cluded that the spinal ankylosis was not a result of AS.The case was initially suspected as AS due to insufficient
history taking and lack of experience of a young radiologist.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCE
1. Hutter CG. Posterior intervertebral body fusion. A 25-year study. Clin Orthop Relat Res 1983;(179):86-96.