Embed Size (px)
Citation preview
The Chief ’s Corner
Who was the first … ?
A common question to historians is who was the first something – per-
haps the first person to be something or the first person to do something.
Depending on how the question is framed can change the answer. The
first president of the United States was:
* George Washington (first President under the current Constitution), or
* Peyton Randolph (President of the Continental Congress), or
* John Hanson (President of the United States under the Articles of
Confederation).
Who was the first… ? 1-2
Christmas Letters Home 2-3
Enlisting Amputees 3-4
The Army Prosthetics Lab 5-7
Bolko Zimmer and “White
Elephants”
8
Punji Stakes 9
AMEDD Expeditions in
Russia
10-
11
Numbered medical regiments 12-
13
AMEDD Center of History and
Heritage
Director, Mr Robert Driscoll
AMEDD Museum
ameddmuseum.amedd.army.mil/
210-221-6358
Office of Medical History
history.amedd.army.mil
210-295-0977
Office of the AMEDD Regiment
ameddregiment.amedd.army.mil/
210-221-8160
http://history.amedd.army.mil/
http://
ameddregiment.amedd.army.mil/
http://
ameddmuseum.amedd.army.mil/
History teaches each and every one of us. We have received many emails
from you saying how much you are enjoying reading the AMEDD Histo-
rian, and how much you have learned about our history and heritage, and
this issue will be no different.
Improvised explosive devises (IED) have caused loss of limbs and other
devastating injuries to our Soldiers. Historian Lew Barger has written an
article on the Army Prosthetics Research laboratory which began in World
War II. This lab conducted basic research on limb prosthetics, which is to-
day’s foundation of prosthetics for our wounded warriors. Retaining
wounded warriors on active duty is not new; Dr. Sanders Marble has writ-
ten a piece retaining amputees on duty in 1946.
History can also be the three dimensional artifact that tells a story, in this
issue, Chuck Franson and Paula Ussery have written two articles about arti-
facts that are on display at the AMEDD Museum. For some Doughboy’s
World War I didn’t end on the 11th hour of the 11th day of November
1918. Bob Ampula writes about the United States forces sent to Northern
Russia and Siberia in 1917 to 1920, and where six AMEDD Soldiers would
earn the newly created Distinguished Service Cross (DSC) for valor. As we
approach the holiday season, let’s not forget our Soldiers deployed around
the world. Andy Watson remembers “Christmas Letters Home,” in his arti-
cle from past AMEDD Soldiers away from home on Christmas.
Remember this on-line journal is yours, and we are seeking articles from
you. If you have an interest in AMEDD history and need some encourage-
ment, contact us as we would enjoy helping you research your history, then
publishing to educate fellow Soldiers.
Army Medical Department Center of History and Heritage, Fort Sam Houston, Texas Number 4 Autumn 2013

Page 2 The AMEDD Historian
The first Medal of Honor recipient was:
* Assistant Surgeon Bernard J.D. Irwin (his gallant actions were on 13-14 February 1861, but the medal was awarded in
1894), or
* Private Francis E. Brownell, whose medal citation states “first Civil War deed to merit Medal of Honor,” at a time when
the law restricted awarding the Medal to events “during the present insurrection,” or
* the six men who actually received their medals on 25 March 1863.
In fact, the Army’s Center of Military History avoids ‘firsts’: “As a matter of policy, unless an official announcement of known facts
is issued, the Center of Military History refrains from sanctioning claims involving ‘firsts’ or the ‘most’ because they often are diffi-
cult to substantiate and frequently are contested by other claimants.”
So we’ve got a poll for you. When was the Army’s first kidney transplant? We’ve got two contenders, and have tried to make the
nominations balanced.
There’s no right answer, but go to our Facebook page (https://www.facebook.com/medhistory), look at the two contenders, and ‘like’
the option you think was first. Of course you can vote for both!
Christmas Letters Home Andy Watson, AMEDD Regimental Historian
One challenge that many Soldiers face is separation from friends and family during the holidays. Christmas, in particular,
stands out as a time when their thoughts are concentrated on home. Although dedicated to their mission, holiday activities often
serve as a welcome diversion. Conversely, other Soldiers delve into their job, staying extremely busy. Here are some reminisces of
troops from our past that provide glimpses into their service away from home.
MAJ William Watson was the Regimental surgeon for the 105th Regiment of Pennsylvania Volunteers during the Civil
War. Although geographically close, his Christmas was still away from home. MAJ Watson was disappointed by the lack of an an-
ticipated feast, and hopeful for it to distract him from the recent Fredericksburg battle.
28 Dec 1862. “I spent a very dull and dry old Christmas. My bill of fare for dinner consisted of hard tack, corned beef,
beans, and coffee.”
Elizabeth Lewis served with the American Expeditionary Forces during World War I as a member of the Army Nurse Corps with
Base Hospital 115 in Vichy, France. She continued to serve overseas and looked forward to the New Year without war.
24 December 1918 “…Wish I could be home this Christmas but as I can’t I will have to make the best of it. There is a lot to
be thankful for even if I am so far away…When I think of where I would have been if the war continued and now to think
of being back and sending patients home, and knowing when these are home there won’t be any more to get wounded and
take their place...”
Iva Lehman was a nurse from Whitley County, Indiana.
Christmas of 1918 in France was very interesting. All did what they could to make it a merry one, as there were prospects of
our soon going home, but Quartermaster issued us a 100 lb. sack of sugar to be made into candy. We were busy every
minute when off-duty, for several days, on this job, as we only had an upright heating stove in our quarters, and much of the
candy was cooked there. Fuel was very scarce, which added to our difficulties, but we finally accomplish our purpose, and
made the candy go was far as possible among the boys. Mistletoe grew in abundance, and this was used to decorate the
wards. We also had Christmas trees in the wards and at the nurse's home. The Red Cross filled home knitted socks for all
the patients with cigarettes, oranges, nuts and candy. All patients who were able went to Christmas Eve services held at the
Red Cross hut. To accommodate the crowds, three services were held, the last at midnight. We attended this one and then
went to bed at 4 AM, then many of us put on our white uniforms, which were seldom worn, our caps and capes, and
marched through all the wards carrying candles and singing Christmas carols. Later, there was a very nice dinner for the
boys, and each ward had a little party of his own.

Page 3 Number 4, Autumn 2013
SGT George E. Hubbard served as medic during the Korean War and was assigned to an ambulance company of 25th Infantry Divi-
sion’s 25th Medical Battalion.
25 December 1951 “They sent me to follow a convoy to the east coast on Christmas Day. The snow was very deep over
there, and it was cold. Cox (my assistant driver) and I would swap driving every hour. I would drive for an hour until my
feet and hands were frozen and felt like stumps, then I would get in the back of the ambulance where the heater was and
thaw out. For Christmas dinner that day, I got some communication wire that was strung all along the road. I took a couple
of C-rations and tied them to the exhaust manifold on the engine. When my hour of driving was up, I took the cans off and
had a good hot meal.”
More recently deployments such as Operation Uphold Democracy in Haiti (1994-1995), were shorter but spanned several holidays
away from home. Mary Sarnecky author of A Contemporary History of the U.S. Army Nurse Corps writes,
“To counteract melancholy the nurses held parties, staged talent shows, listened to concerts, and derived solace from their
patriotic service and the knowledge that in the next year, the holiday season would be even more special.”
These reminisces demonstrate that we still have similar concerns, and also that there is generally some optimism for the coming year.
Fellowship and activities that change the routine are very much appreciated, even if not always acknowledged. During this holiday
season please remember our service men and women serving and recovering away from home.
Sources
Elizabeth Lewis, diary entries, found in Army Nurses of World War I: Service Beyond Expectations, edited by Lorraine Luciano and
Casandra Jewell
George E. Hubbard, memoirs, submitted to http://www.koreanwar-educator.org
William Watson, compiled letters, Letters of a Civil War Surgeon, edited by Paul Fatout
A Contemporary History of the U.S. Army Nurse Corps, by Mary Sarnecky
http://www.wwvets.com/MedicalCorps.html
Enlisting Amputees Sanders Marble, Senior Historian, Office of Medical History
In 1946 the Army was in the midst of an enormous demobilization. From a peak of 8 million men and women in 1945, by mid-1946
it was down to under 2 million with further cuts planned. While the threat from Germany, Italy, and Japan was over, maintaining
effective units was increasingly difficult as experienced personnel were discharged.
That summer a discharged master sergeant, Richard Montgomery, wrote to Army Chief of Staff Eisenhower. Montgomery had been
a radio operator in an Army Air Forces B-29 that was shot down by the Japanese. His left hand was nearly amputated in bailing out
of the aircraft, and gangrene developed in his forearm; a British doctor in the POW camp amputated Montgomery’s arm. Montgom-
ery had gone through Army hospitals, recuperated, been issued a prosthesis, and learned how to use it. On 24 January 1946 he was
discharged from hospital and from the Army. Montgomery had enlisted in February 1940
and wanted to make the Army a career; he thought he was as effective a radio operator as
he had been before, and he did not like being “turned out to pasture.” He asked General
Eisenhower why he could not rejoin the Army, pointing out the Army had already in-
vested thousands of dollars in his training. He had gone to several recruiting stations and
been told he did not meet the physical standards, and had previously written to The Adju-
tant General without results.
Eisenhower liked the idea: it would gain experienced, motivated leaders. He had the
General Staff study how to make it happen. With the personal interest of the Chief of
Staff, the paperwork moved rapidly: between Montgomery’s letter to Eisenhower on 28
August and 1 November 1946 a program was established. Now combat-disabled men
could apply for reenlistment. This was remarkable: at the time, enlisted men who were
discharged for disability had been ruled flatly unfit for service. Now those who wanted
to, and met strict criteria, could return to duty. They did have to meet all physical stan-
dards with the exception of things related to their wound, they had to be able to take care
of themselves, and they would not need further medical care for their wound.

(The careful medical examination and deliberation on each individual would be a burden on the Medical Department.)
The Army opened 103 specialties to the men. It would take care of them by only assigning them to duty in the US, and not to tactical
units. They were expected to be effective leaders for the inexperienced troops who were rapidly replacing the veteran troops still
being discharged. Up to 5,000 volunteers were expected.
Eisenhower’s aides coordinated with Montgomery to be the standard-bearer for the new program: he was issued invitational travel
orders to be re-examined for enlistment and then to the Pentagon. On 8 November The Adjutant General personally swore Montgom-
ery back into the Army, with other dignitaries (including the director of the VA’s Retraining and Reemployment Administration) in
attendance. This helped draw the desired publicity, and both Army publications and civilian newspapers (including the VFW maga-
zine) picked up the story about Montgomery and the opportunity to re-enlist. It also helped the Army avoid criticism at a time when
the American Legion was strongly pushing a nationwide “Employ The Handicapped Veteran” campaign, and Montgomery was also
used as an example of how hiring the “handicapped” was sensible.
In the next few years the program expanded its criteria: officers and warrant officers could come back on duty; men could reenlist for
longer periods (up to six years); and non-combat disabled could rejoin. There is no evidence that women were allowed to re-enlist,
while there would have been few who would have been wounded in combat, more would have been disabled outside combat.
The personnel system of the time was quite different. Enlisted men could be discharged on the signature of a single physician, while
officers, no matter how junior, had to be retired if they were injured. The Medical Evaluation Board/Physical Evaluation Board proc-
ess did not exist, and even physical profiles were relatively new and incomplete. The Career Compensation Act of 1949, which sub-
stantially changed physical disability retirements, did not yet exist.
When the Korean War erupted in June 1950, the program was opened to men recovered from Korean War wounds, and later Korean
War injuries. Men were also allowed to stay in the Army who would have otherwise been discharged, as long as they could render
satisfactory service in another MOS, similar to today’s MEB process.
In 1953 the Army studied the program. Two-thirds of the men involved had been wounded, three-quarters were enlisted men. The
most common position for officers was commanding training units, followed by staff positions and miscellaneous. The most com-
mon positions for enlisted men were in administrative/supervisory jobs. However, there were only 630 personnel in the program.
Whatever its fairness (Master Sergeant Montgomery and his comrades were not “turned out to pasture”) the program came nowhere
close to producing 5,000 experienced men for the Army. The Army continued the program through at least 1962, perhaps because
the numbers were small enough to give individual attention. The developing MEB process also identified MOSs where individuals
could continue to serve. Today’s amputees continuing on active duty have paid a price for their service, and have skills, character
and dedication to offer today’s and tomorrow’s Army, but others broke the ground for them to continue serving in uniform.
Sources
Marginal Man and Military Service: A Review (Department of the Army, December 1965)
COL George Evans, “Not So Disabled” Army Information Digest 1/8 (December 1946)
“Retention and Utilization of Partially Disabled Personnel” Health of the Army July 1953.
“Amputees Enlist Under New Policy” Bulletin of the U.S. Army Medical Department 7/1 (January 1947)
Fairfax Downey, “Our Not-So-Invalid Corps,” Infantry Journal 60/4 (April 1947), 68-69.
Howard A. Rusk, “Army Enlists First Disabled Veteran for Its Post-War Set-Up – 5,000 Such Men From the War Will Be Sought”,
New York Times, 1 December 1946.
Louis Galambos, ed., The Papers of Dwight David Eisenhower: VIII, The Chief of Staff. Johns Hopkins University Press, 1978.
Page 4 The AMEDD Historian

Page 5 Number 4, Autumn 2013
The Army Prosthetics Research Laboratory Lewis Barger, Historian, Office of Medical History
Men and women may lose limbs for many reasons, but warfare can generate large numbers of amputees and spur official interest
in finding (and funding) technological replacements for missing limbs. During World War II many agencies were organized to inte-
grate new technologies, engineering, and manufacturing techniques into the field of prosthetics. The Army, at the direction of the
Secretary of War, had opened seven laboratories to study improvements in prosthetics, including the Army Hand Laboratory at Wal-
ter Reed. Army Surgeon General Norman T. Kirk petitioned the National Academy of Sciences to investigate opportunities to im-
prove prosthetics, which ultimately led to establishing the Prosthetic Research Board. The Office of Scientific Research and Devel-
opment funded prosthetics research during the war, but it was disbanded in 1947 and responsibility for coordinating prosthetics re-
search was transferred to the Veterans Administration, which was also responsible for supplying artificial limbs to amputee veterans.
In 1948 Congress authorized $1M per year (nearly $10M in 2013 dollars) “to aid in the development of improved prosthetic appli-
ances” (PL 80-729) and placed the VA in charge of distributing the funds. At the end of WWII the Army reorganized its prosthetics
laboratories, consolidating them all at Walter Reed as the Army Prosthetics Research Laboratory (APRL).
Amputee veterans were dissatisfied with the
prostheses available to them at the time. Lower limb
replacements provided a basic level of mobility but
could be painful to wear and upper limb replacements
had very limited functionality. As prosthetics research
progressed, research efforts divided into three major
areas. Lower limb research was centered at the Univer-
sity of California – Berkeley campus with participation
by the Oakland Naval Hospital Artificial Limb Depart-
ment. Research into the more complex problem of
replacing upper limbs was undertaken by the Univer-
sity of California at Los Angeles with assistance from
the APRL. Finally, New York University and the VA
Prosthetic Testing and Development Laboratory in
New York tested new devices for acceptance and inte-
gration into the VA prosthetic replacement program.
Captain Maurice J. Fletcher was temporarily assigned to the APRL in
1945, shortly after its establishment. Fletcher had a diverse background.
After receiving a reserve commission from the University of Iowa where he
received a degree in architectural engineering Fletcher spent time as a barn-
stormer, commanded a Civilian Conservation Corps camp during the De-
pression, and eventually became a patent attorney and inventor. Shortly
before the war he was commissioned in the Army where his technical exper-
tise and interest in mechanical items served him well in the Ordnance
branch. Those same interests were useful at the APRL, where his temporary
assignment became permanent; he took command of the organization in
1946 and branch transferred to the Medical Service Corps. Fletcher would
command the APRL until his retirement as a Colonel in 1961.
APRL staff and patients.
Photo courtesy National Museum of Health and Medicine.
Patent drawing for the APRL hand.
Photo courtesy U.S. Patent Office.

When Fletcher first arrived at the APRL much of the wartime staff was demobilizing and returning to civilian life. He gradually
built the organization up to two other officers, eight enlisted soldiers, and twenty-seven civilian technicians. At the same time he
also tackled developing an improved artificial hand. The result was the ‘APRL hook,’ a split-hook device that improved on older
designs by incorporating a voluntary closing action so wearers could apply levels of grasping pressure appropriate to the object they
were holding. This was followed by the APRL hand which lacked some of the hook’s functionality but included a cosmetic glove
color-matched for skin tone and incorporated realistic touches like skin lines and individually implanted hairs. The ‘F-M wrist,’ de-
veloped jointly by Fletcher and Gilbert M. Motis of Northrop Aircraft, enabled the prosthetics wearer to quickly switch the terminal
appliance to meet the needs of the wearer.
Both the hand and the hook were controlled by a harness worn on the
opposite shoulder. Trying to get better control the APRL, working with sur-
geons at Walter Reed, explored cineplasty. Cineplasty is the surgical crea-
tion of a tunnel through a muscle, covered by skin, which provides an attach-
ment point for an artificial limb control mechanism. The biceps proved an
ideal muscle for this purpose, and in cases of higher amputations the pector-
alis major was used. Once the surgery healed a pin or a detachable plastic
ring connected the prosthetic control mechanism to the tunnel, and the ampu-
tee was taught to manipulate the device. A 1957 review of 78 biceps cine-
plasties and 29 pectoral cineplasties found that 73 percent of the first group
continued to wear their prostheses after a one-year period, but that only 31
percent of pectoral cineplasty recipients continued to do so. The study deter-
mined that cineplasty was an appropriate procedure for male patients (female
recipients reacted unfavorably for cosmetic reasons) with below-the-elbow
and long above-the-elbow amputations. A ten-year follow-up discovered
that none of the original pectoral cineplasty patients continued to wear their
prosthesis, but 73 percent of the biceps cineplasty respondents continued to
wear their appliance and 88 percent would recommend the procedure to
other amputees. Cineplasty fell out of favor as a routine procedure by the
1970s – fewer cineplasty patients had long term success with their appli-
ances than conventional harness patients, the surgical sites would occasion-
ally reclose or become otherwise unusable, and although direct connection to
muscles provided sensory feedback, it didn’t always provide sufficient
power to control the prosthesis.
After the development of the APRL hook and APRL hand, Fletcher
turned his attention to the material that prosthetic sockets were made from.
Sockets had a tendency to collect perspiration which, over time, would irri-
tate the stump. The APRL developed a porous laminate socket that allowed
moisture to be wicked away yet still provided a solid connection to the
stump. The APRL staff also developed “improved control cables, harness-
ing materials, fittings, locks, and techniques of application [that] have
proved invaluable to limb-fitters everywhere.” APRL staff were able to ap-
ply their experience working with those materials to develop cosmetic replacements for ears and noses. They even experimented
with replacements for internal structures like heart valves, arteries, and tracheas.
The APRL’s work was part of a much larger coordinated effort to improve the lives of amputee veterans. Beginning in January
1945, the government brought together manufacturers, academic and industry researchers, surgeons, prosthetists, and government
organizations and established a multi-disciplinary working group to improve prosthetics. The military and civilian staff of the APRL
did not work in isolation but benefitted from and contributed to a systemic approach that encompassed research and development,
testing, manufacturing, and training. New studies of human body motion were undertaken and new techniques in surgery were de-
veloped in addition to developing new prosthetics.
When Colonel Fletcher retired from the Army in 1961 he was honored by the Academy of Achievement as one of the first class
of recipients of the Golden Plate award. He shared the honor with other leading Americans including Charles Mayo, Douglas Mac-
Arthur, and Edwin Teller. Fletcher, who used to joke that he’d originally been assigned to the APRL “because somewhere in his
Ordnance Corps records he was designated as a ‘small arms’ expert,” continued after his retirement as a highly respected member of
the Committee on Prosthetics and Orthotics of the International Society for the Rehabilitation of the Disabled.
Page 6 Number 4, Autumn 2013
A below-elbow amputee with his prosthesis, showing the
cineplasty area.
Photo courtesy National Museum of Health and Medicine.

Page 7 The AMEDD Historian
Shortly after Fletcher’s retirement the APRL, which had been placed under Medical Research and Development Command in 1958, was re-
named the US Army Medical Biomechanical Research Laboratory (USAMBRL). In 1972-3 the USAMBRL and the US Army Medical Depart-
ment Equipment Research and Development Laboratory were both relocated to Fort Detrick, Maryland and merged with the US Army Environ-
mental Engineering Research Unit, which remained at Aberdeen Proving Ground, Maryland. The new organization was renamed the US Army
Medical Bioengineering Research and Development Laboratory (USAMBRDL). In 1986 the name changed again to the US Army Biomedical
Research and Development Laboratory. This would be the last redesignation for the organization, which was identified for closure in 1991’s Base
Realignment and Closure legislation. The missions that were retained – “medial materiel development, occupational health, and environmental
quality” were reallocated to the Air Force’s Armstrong Aerospace Medical Research Laboratory in Dayton, Ohio.
Fletcher’s and the ARPL’s accomplishments were significant contributions to the field of prosthetics, but they were part of the government-led
coordinated effort that included civilian and governmental research institutions, professional societies, and industry. The next significant improve-
ment to prosthetic devices would have to wait for new technologies. Microprocessors and high density batteries for power supplies have led to
artificial legs like the C-Leg® and the Defense Advanced Research Projects Agency (DARPA) Autonomous Robotic Manipulation (ARM) pro-
gram. The DARPA-funded modular prosthetic limb is currently under development by the Johns Hopkins Applied Physics Laboratory as a
“neutrally controlled artificial limb that will restore near-natural motor and sensory capability to upper-extremity amputee patients.” Most of the
devices developed at the APRL have now been supplanted by newer designs, but Colonel Fletcher would have been pleased to see his commitment
to excellence in prosthetics being carried forward.
Sources
Brav EA, et al. Cineplasty – Ten Years Later. J Bone Joint Surg Am, 1965 Jul 01; 46(5): 1137-
1138.
Childress DS. Presentation Highlights: Tunnel cineplasty. J Rehab Res Dev, 2002 May/June; 39
(3, Supplement): 9-10.
Colonel Fletcher Honored. JAMA, 1961 Oct 21; 178(3): 338.
Fletcher MJ. Some Human Factors Engineering Implications from Design of Prosthetics. Report:
Third Annual Army Human Factors Engineering Conference, 2-4 OCT 1957. Natick, Mass: Quar-
termaster Research and Engineering Command; 32-34.
Gailey R. Guest Editorial: As history repeats itself, unexpected developments move us forward. J
Rehabil Res Dev. 2007; 44(4): vii-xiv.
Johns Hopkins Applied Physics Laboratory. Revolutionizing Prosthetics. JHAPU website. http://
www.jhuapl.edu/prosthetics/. Accessed 18 September 2013.
Notes and News. Bull Prosth Res. 1980 Fall; 17(2): 226-233.
Prosthetics Pioneer Hailed for 16 Years of APRL Progress. Army Research and Development
Newsmagazine. 1961 Oct; 2(10): 6.
Strong FS. Artificial Limbs – Today and Tomorrow. Artificial Limbs: A Review of Current De-
velopments. 1954 Jan; 13: 1-3. National Academy of Sciences, National Research Council, Advi-
sory Committee on Artificial Limbs, Division of Engineering and Industrial Research.
USAMRMC: 50 Years of Dedication to the Warfighter, 1958-2008. Available online at: http://
technologytransfer.amedd.army.mil/assets/docs/marketing/USAMRMC_history.pdf.
A DARPA “neurally integrated” modular
prosthetic limb developed by the Johns
Hopkins University Applied Physics
Laboratory.
Photo courtesy Johns Hopkins University
Applied Physics Laboratory
Michelle Ufner, a civilian employee, visits with an
injured U.S. Soldier while carolers sing at Craig
Hospital at Bagram Airfield, Afghanistan, Dec. 6,
2009. U.S. Army Maj. Doug McInvale, Depart-
ment of the Army civilian Henry McEnery, U.S.
Army Maj. Jeff Boldt, and Army Sgt. Maj. Cecil
Edwards formed a quartet to provide morale sup-
port to military and civilian audiences at Bagram
Airfield, Afghanistan. (U.S. Army photo by 1st Lt.
Rock Stevens/Released)

Bolko Zimmer and the “White Elephants” Chuck Franson, Registrar, AMEDD Museum
When they first arrived in Vietnam Army aviators wore cotton fatigue uniforms, but due to the danger of fire in a crash, the Army
sought to find a flame-proof replacement. Early experiments of treating uniforms with a Borax solution proved unsatisfactory. The
answer lay in uniforms made of DuPont Nomex, a fabric originally designed for auto racing suits in the 1960s. The Army procured
both one-piece coveralls and two-piece (jacket and pants) Nomex uniforms.
The AMEDD Museum is fortunate to have a Nomex uniform worn by 1LT Bolko Zimmer in Vietnam. His jacket, worn during his
service in 1971, has two theater made patches from the 54th Air Ambulance and the 236th Medical Detachments, the units he served
with while in Vietnam. While in Vietnam, LT Zimmer participated in
missions flying “White Elephants”, or white-painted UH-1 helicop-
ters.
During the later years of the US involvement in Southeast Asia, the
Army sought to gain support for the military. One of the ways this
was accomplished was through a program called MAST, Military As-
sistance to Safety and Traffic. The idea was for Army Medevac assets
to assist civilian authorities in transporting seriously injured persons,
such as traffic accident victims. The MAST helicopters flown at Fort
Sam Houston and Fort Rucker were painted white with red crosses, as
opposed to the Olive Drab paint scheme on regular operational air-
craft. Due to the high percentage of losses of DUSTOFF aircraft, the
Army decided to experiment with using the white helicopters in Viet-
nam; the rationale was that the higher visibility of a white helicopter
would better identify them as non-combatant and the enemy would not
fire upon them. The aviators referred to the newly painted birds as
“White Elephants”.
Bolko Zimmer later reminisced:
“In the summer of 1971, someone with a higher pay grade than me
decided we should fly white helicopter to demonstrate our commit-
ment to the Geneva Convention. So, all of our helicopters were
painted white with superimposed red crosses on the belly of each air-
craft. What someone failed to consider was that the Viet Cong didn’t
think much of that document or any other international document.
Shortly after our six aircraft were given the ‘new look,’ one was dispatched to pick up wounded South Vietnamese soldiers just south
of Chu Lai. We soon heard from our operations officer that the Viet Cong had shot up the aircraft and severely wounded the copilot.
Yet, the helicopter made it back to Chu Lai and the mechanics were able to repair it.
At the end of 1971, I was reassigned to the 236th Medical Detachment based in
DaNang because all of the military units in Chu Lai had stood down and were being
redeployed to the U.S. The white helicopters, though, followed me to DaNang like a
mother duck with her six ducklings. Shortly after my arrival, we were given the mis-
sion to evacuate a wounded South Vietnamese soldier not far from our base of op-
erations. I had a flashback of what had happened in Chi Lai and wondered if this
was going to be déjà vu all over again. We took off at dusk and soon arrived at the
pickup point to get the wounded soldier. Once in the air, our helicopter was hit by
several rounds, but nobody received injuries. Fortunately, the darkness had provided
enough concealment so the enemy could hear us but not see us.”
LT Zimmer’s Nomex jacket, as currently featured in the AMEDD Museum’s tempo-
rary exhibit “The DUSTOFF Legacy.”
Page 8 Number 4, Autumn 2013
LT Zimmer with his aircraft.
Photo courtesy AMEDD Museum.

Punji Stakes Paula Ussery, Museum Specialist, AMEDD Museum
The irregular nature of the warfare in Vietnam included a variety of booby traps designed to harass, demoralize, maim and/or kill American soldiers
and our allies. These concealed devices slowed American advances, created a constant state of tension for American soldiers and wounded many
soldiers.
The People’s Army of Vietnam and Viet Cong booby traps can be divided into two broad categories, explosive and non-explosive. The explosive
booby traps included cartridges positioned over a firing pin so that when a soldier stepped on the trap the cartridge detonated against his foot, and
traps that used grenades rigged to explode on impact.
On the very low tech end of the spectrum were booby traps that utilized sharpened stakes of either bamboo or steel. These “punji” stake traps were
the most common form of booby trap encountered. They caused numerous penetrating, perforating or lacerating injuries to foot, ankle, leg, chest, or
other body areas. The simplest trap consisted of a piece of scrap lumber with one of more sharpened bamboo or steel stakes sticking up from the
horizontal wooden base. The steel stakes frequently had flattened tips or “barbs” to create a larger wound. Stakes were frequently covered in human
or animal excrement to increase the chances of infecting the wound. Punji stake traps were hidden under water in swampy areas or in or under the
jungle floor litter and in tall grass. A soldier’s own weight drove the stakes into his foot or ankle.
There were a number of varieties of punji stake traps. One variation was the Pit Trap. As the name implies, a pit was dug into the ground and the
bottom lined with punji stakes. The opening was concealed. The soldier stepping onto the camouflage fell onto the stakes, causing multiple wounds.
The punji stake was also used effectively in mobile traps. The Mace Trap consisted of a concrete or mud ball, or a steel drum studded with punji
stakes. When the soldier stumbled into the trip wire, the mace swung down from an elevated position, inflicting numerous wounds on its victims.
So common were punji stake booby traps that the Army altered its jungle combat boot. The boot, as issued prior to 1966 had a black composition
sole and nylon webbing upper, but there was no protection for the sole of the foot. In 1966 the Army introduced a jungle boot with a “Spike Resis-
tant Sole Shield,” a steel shank embedded into the sole. The Viet Cong and North Vietnamese countered this improved boot by creating more-side
closing punji traps that grabbed both sides of the ankle.
In 1966 the 2d Surgical Hospital studied 342 wounds in 324 patients. Punji wounds accounted for 16% of total hospital admissions and 38.1% of
the 850 wounds treated between January and September. The highest rate of punji wounds was 65 patients in a 72-hour period. The typical wound
was shallow, measuring .5-2 cm. The depth varied, including some through-and-through wounds and 14 wounds with joint penetration. The leg
accounted for the most injuries with 206, the foot 38 cases, and the thigh in 29 cases. One palate wound resulted from a soldier falling with his
mouth open onto a punji stick. Eight patients were admitted with infected wounds.
Treatment at the 2d Surgical involved a standard protocol of debridement and creating an open wound. Delayed primary closure was usually per-
formed on the fifth postoperative day. Patients were treated with intramuscular penicillin and streptomycin. Patients with deep wounds or wounds
involving a joint were initially given intravenous penicillin. Any patient who had not been given tetanus toxoid prior to admission was given one at
the hospital. Careful debridement, especially for punji stakes made from bamboo, was critical as X-ray was ineffective in finding these bamboo
fragments. The average length of hospital stay was 12.3 days with a seven to ten day convalescent period following a soldier’s return to his unit.
Punji stakes had a high return on investment for the
enemy.
Booby traps were manufactured until the end of the
Vietnam War. It is estimated that 11% of the deaths
and 17% of the injuries suffered by Army personnel
between January 1965 and June 1970 were caused
by booby traps and mines.
The U.S. Army Medical Museum is fortunate in-
deed to have in its collection four punji traps cap-
tured in Vietnam in 1962. These traps were cap-
tured in the Mekong Delta area of Vietnam, and are
on display in Gallery 1 that traces the Medical De-
partment from the Vietnam War to the present day.
Punji stakes from the AMEDD Museum collection.
Page 9 The AMEDD Historian

The Nor th Russian And Siberian Expeditions Robert L. Ampula, Administrative Officer, AMEDD Regiment
Everyone remembers the 11th hour of the 11th day of November 1918 as the day that hostilities ceased in Europe and think US in-
volvement in World War I ended then. With the end of the war most Soldiers returned home, but in 1918 America sent two fighting
forces into Russia that would not return with the rest of the doughboys. To understand these expeditions it is necessary to delve
briefly into Russian history. In February 1917 Russia’s government collapsed, and a civil war broke out between socialist/communist
forces (the Reds, led by Vladimir Lenin) and various other factions, collectively called the Whites. The Germans occupied much of
Russia, and with Russians fighting each other the Germans were able to move further east and seize economic resources.
Since 1914 the Allies had been sending military supplies to Russia, using the ports of Arkhangelsk (Archangel), Murmansk, and
Vladivostok. When the Russians made peace with the Germans, the Allies became increasingly concerned that the Germans would
occupy more Russian territory and possibly capture the supply dumps. The British and French backed the loyalist Whites, hoping
they would end the Bolshevik revolution, resurrect the Eastern Front, and pressure the Germans. The Allies also wanted to rescue the
Czechoslovak Legion, which was fighting the Germans in hopes of creating an independent homeland. The Czech Legion numbered
40,000—70,000 troops; many were trapped in Siberia along the Trans-Siberian Railroad.
For these reasons the Allies decided to intervene on behalf of the anti-Bolshevik forces, but
had few troops to spare and sought American troops as well. In June 1918 President Wood-
row Wilson, despite objections from the War Department, decided to send a limited contin-
gent of American troops to Archangel and Vladivostok to increase the Allied presence in
Russia during this period of extreme turbulence. Although the two expeditionary forces were
deployed under the same auspices, they were thousands of miles apart, did not interact during
their time in Russia, and their experiences were markedly different. In addition, their missions
were poorly defined and poorly understood.
The American Expeditionary Force Siberia was the first to deploy and arrived at Vladivostok
in mid-August 1918 from the Philippines. Their ranks included the 27th Infantry Regiment
and the 31st Infantry Regiment as well as various units from the 8th Division and would
eventually grow to around 8,000 troops. The medical units included Evacuation Hospital
number 17 from Fort Sam Houston, Texas, and both Field Hospital number 4 and Ambulance
Company number 4 from Camp Lewis, Washington.
Shortly after their arrival, the American 27th Infantry Regiment found themselves supporting
the Japanese who were attacking the Bolsheviks along the Trans-Siberian Railroad. It was
here the Regiment earned its now famous ‘Wolfhound’ nom de guerre. (A Japanese com-
mander commended them for a fast march, as fast as Russian wolfhounds.) When the expedition commander, MG William S.
Graves, arrived at the beginning of September, he halted American involvement in offensive operations, to the chagrin of the other
allies. His understanding of the mission was to
rescue the Czech Legion and safeguard Allied
supplies and interests in Vladivostok. The Czech
Legion was actually controlling Vladivostok at
the time of the American arrival and so the mis-
sion evolved into safeguarding allied interests.
From a medical standpoint, the Americans from
that point mainly dealt with illness (including the
pandemic influenza) and cold injuries. In addi-
tion, one of the main obstacles they faced in pro-
viding health care was sanitation. Virtually no
latrines existed and human waste accumulated in
large quantities. Water supplies were also con-
taminated, contributing to a large variety of ill-
nesses.
Page 10 Number 4, Autumn 2013
Interior of surgical ward, Evacuation Hospital No. 17, Siberia.
From: Medical Department of the United States Army in the World War, vol. VIII, p. 959
An American medic bandages a Cossack.
From: Ernest Dupuy, Perish by the
Sword: The Czechoslovakian Anabasis
and our Supporting Campaigns in North
Russia and Siberia 1918-1920
The American Expeditionary Force North
Russia was made up of elements of the 85th
Division which was comprised of men mainly
from Wisconsin and Michigan. The 85th was
preparing to depart England for France when
General John J. Pershing diverted a portion of
the division to Archangel aboard British ships.
This 5,000-man expeditionary force was made
up of the 339th Infantry Regiment and the
310th Engineer Regiment. The medical com-
ponents were the 310th Sanitary Train, the
337th Field Hospital, the 337th Ambulance
Company, and the Medical Detachments of the
339th Infantry Regiment and the 310th Engi-
neer Regiment. All units were placed under
British control which created unique problems.
When they arrived in Archangel at the begin-
ning of September 1918, the force was experi-
encing a severe outbreak of influenza, and
many were stricken seriously. Reports put
deaths near 70. Sanitary conditions matched
those encountered by American forces in Sibe-
ria, complicating the care of those afflicted. Soldiers that were not ill immediately went into action to try and rescue the Czech Le-
gion – which in turn entailed fighting the Bolsheviks. After about a month, and with winter setting in, it became apparent the Ameri-
cans would not reach the Legion, and the Americans set up defensive positions. In contrast, the Bolsheviks, seemingly unaffected by
the severe winter weather, stepped up their attacks, inflicting numerous casualties.
In mid winter, word reached the Soldiers in both theaters of the end of hostilities in Europe and they assumed they would soon head
home. When they didn’t depart and their mission remained the same, morale in North Russia plummeted and to a lesser extent, in
Siberia as well. While the reports of discontent in North Russia are well documented, the force could not leave by this point even if
given the order because the port at Archangel had now frozen over.
At home, public sentiment wanted the soldiers returned home. Newspapers and congressmen were notified and took up the cause.
President Wilson decided to bring the North Russian Expedition home and directed the War Department to plan for their departure.
In late May of 1919, the force started departing Russia. The men of the force (339th Infantry Regiment) decided to call themselves
the Polar Bears. The Polar Bear Expedition is now synonymous with the North Russian Expedition. By the end of July 1919, the
whole force had been extracted.
Not so in Siberia, where their presence would continue for another year after the departure of the Polar Bear Expedition. The Russian
civil war wreaked havoc on their mission of protecting the railroad and their directions to support all Russians equally. The railway
was mainly used by the anti-Bolshevik Whites while the local populace supported the Bolsheviks. The conflicting mission would
only become worse as time progressed. By the winter of 1919-1920, the Whites were virtually defeated and the American troops
were now in danger of direct assault from the Bolsheviks. President Wilson realized the cause was lost and directed that the Ameri-
can forces leave Siberia. The last of the force left Siberia at the beginning of April
1920. Interestingly, the 31st Infantry Regiment also adopted the name Polar Bears.
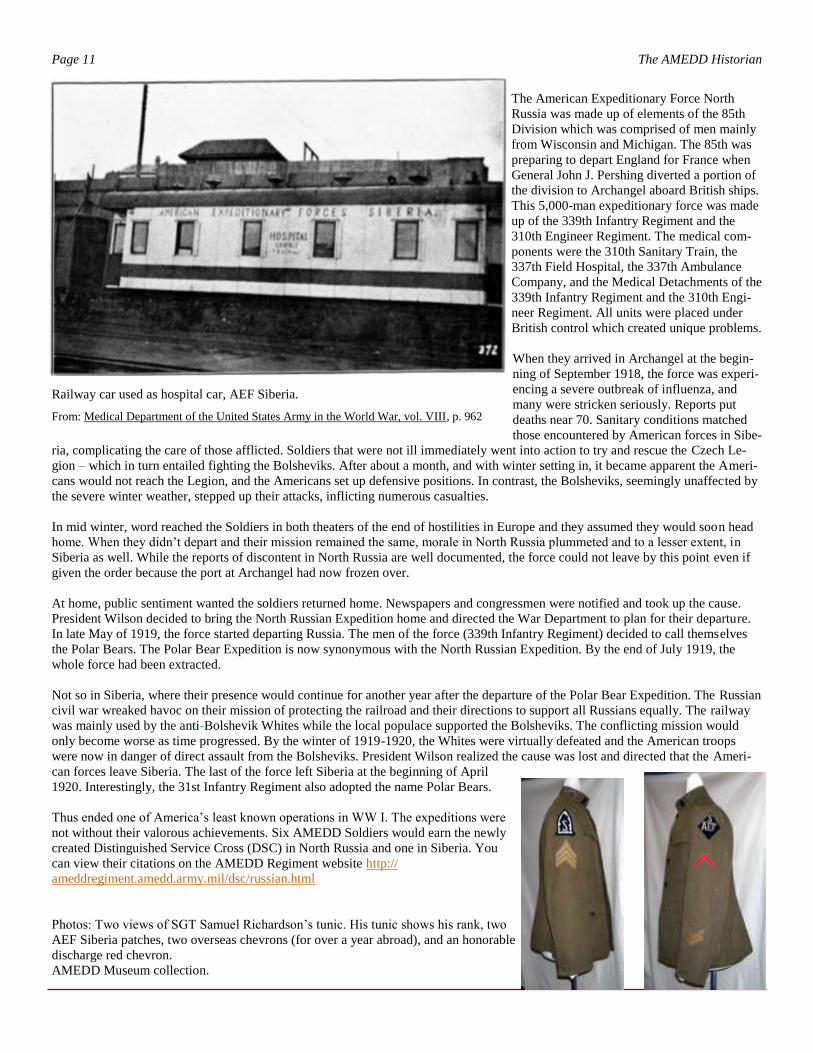
Thus ended one of America’s least known operations in WW I. The expeditions were
not without their valorous achievements. Six AMEDD Soldiers would earn the newly
created Distinguished Service Cross (DSC) in North Russia and one in Siberia. You
can view their citations on the AMEDD Regiment website http://
ameddregiment.amedd.army.mil/dsc/russian.html
Photos: Two views of SGT Samuel Richardson’s tunic. His tunic shows his rank, two
AEF Siberia patches, two overseas chevrons (for over a year abroad), and an honorable
discharge red chevron.
AMEDD Museum collection.
Page 11 The AMEDD Historian
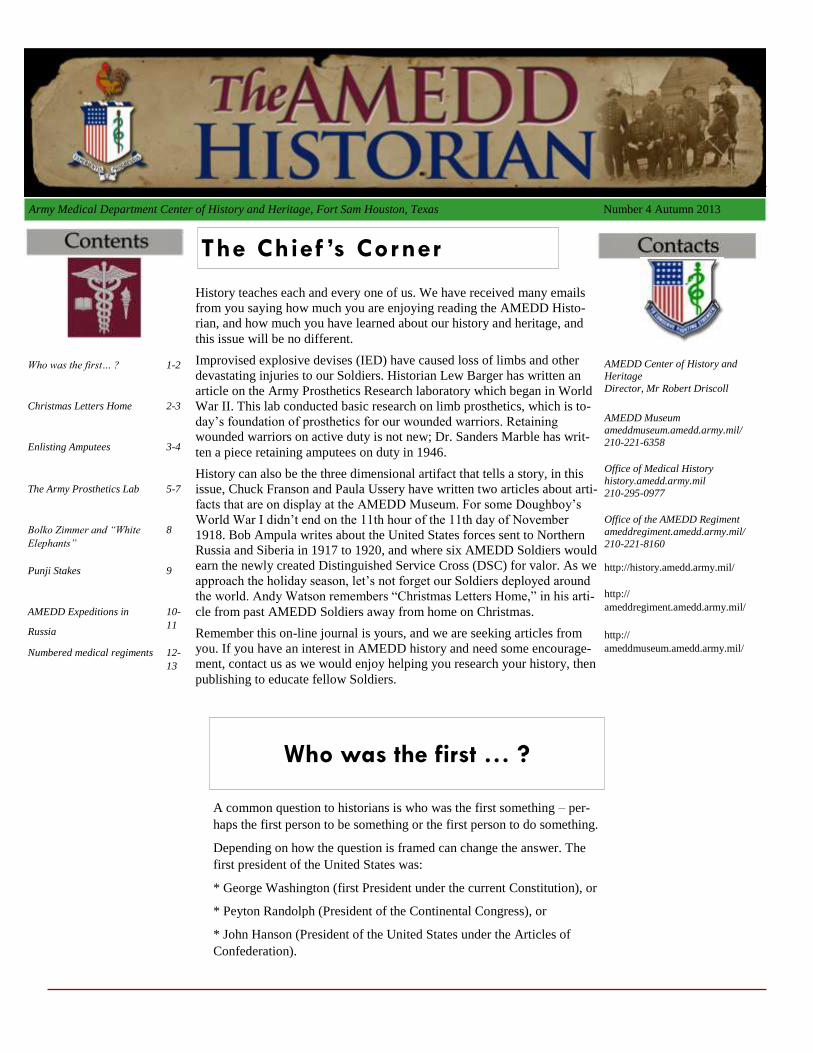
Railway car used as hospital car, AEF Siberia.
From: Medical Department of the United States Army in the World War, vol. VIII, p. 962

Numbered Medical Regiments 1919-1940 Robert S. Driscoll, Chief, ACHH
In the last issue of the AMEDD Historian, Bob Ampula wrote about the establishment of the U.S. Army Medical Department Regi-
ment in July 1986. However, before 1986 the AMEDD had numbered Medical Regiments between 1919 and 1940. The regiment as
we know it today is ceremonial but the earlier one were functional.
When the United States entered World War I in April 1917, each division was supported by a “sanitary train.” These numbered
“trains” (i.e. 101st Sanitary Train) consisted of a headquarters, four ambulance companies, four field hospitals, eight camp infirma-
ries, plus a divisional medical supply section, and attached Veterinary personnel.
After World War I the Army reorganized its division structure and the AMEDD reorganized and established numbered medical regi-
ments as successors to the sanitary trains. The medical regiment was an organic part of the infantry division, with the mission “to
assist in the maintenance of the health of the division, to assure the mobility of the division by promptly and systematically relieving
it of its noneffectives, to provide it with all necessary medical material and supplies, and to supplement and complete the medical
service of the division initiated by medical detachments attached to the combatant and service units in the division.” The regiment
consisted of 60 officers, 1 warrant officer, and 882 enlisted personnel. Medical regiments existed up to the beginning of World War
II, and then reorganized to medical battalions.
There were two types of numbered medical regiments. The first type was allocated to armies and corps for area support. The second
type of medical regiment supported infantry divisions. The only difference between the two was the divisional medical regiment had a supply sec-
tion plus a laboratory section.
Page 12 Number 4, Autumn 2013
Medics of a collecting company of the 1st Medical Regiment
set up a demonstration aid station in Washington, DC, May
1927.
Author’s collection.

Page 13 The AMEDD Historian
Initially, each regiment was organized into three
battalions (collecting, ambulance, and hospital) of
three companies. Initially, companies were num-
bered and each regiment had companies with the
same numbers, such as 101st Collecting Com-
pany, 101st Ambulance Company, and 101st
Hospital Company. In 1936 battalions were re-
designated 1st, 2d, and 3d Battalion, and compa-
nies were lettered A to I. Each battalion was still
single-purpose, collecting, ambulance, or hospi-
tal.
Due to Regular Army manpower restrictions,
active-duty regiments were severely under-
strength. Even so, there were not enough regulars
to go around and “Regular Army – Inactive” units
were created. These had no more than a unit flag
with a cadre staff that would be filled out with
men and equipment when needed. However,
much of the AMEDD force structure was in the
Reserve components. The table below provides a
breakdown:
Today the lineage of numbered medical regiments lives on in such units as the 1st Medical Brigade and the 111th Multifunctional
Medical Battalion, Texas Army National Guard.
Source The Army Medical Department Bulletin #13, 1925.
Organization Army/Corps Med. Regts Divisional Med. Regts
Regular Army 0 5
Regular Army, Inactive 11 7
Army National Guard 14 19
Organized Reserve 33 27
Totals 58 58
PFC Edward Gosse
and PFC Robert Seal-
bach of the 310th
Medical Detachment,
310th Infantry Regi-
ment, 78th Infantry
Division, demonstrate
pulling a litter
mounted on skis, out-
side Lammersdorf,
Germany, 22 January
1945.
Source:
National Archives

Upcoming History Conference
On 6-8 March 2014 the AMEDD Center of History and Heritage and the
Uniformed Services University of the Health Sciences will be co-
sponsoring a conference on medicine and World War II.
More details will be coming out through http://history.amedd.army.mil/
Send questions to: usarmy.jbsa.medcom.mbx.hq-medcom-office-of-
Page 14 The AMEDD Historian
Writing for The AMEDD Historian
We are seeking contributions! We believe variety is the way to attract a variety of audiences, so we can use:
Photos of historical interest, with an explanatory caption
Photos of artifacts, with an explanation
Documents (either scanned or transcribed), with an explanation to provide context
Articles of varying length (initially we will try a 500 word minimum), which must have sources listed if not footnotes/
endnotes
Book reviews and news of books about AMEDD history Technical requirements:
Photos will need to be at least 96dpi; contact us about file format.
Text should be in Microsoft Word (.doc or .docx) format. Please do NOT send text with footnotes/endnotes in .pdf format.
Scans should be in Adobe Acrobat (.pdf) format.
Material can be submitted to usarmy.jbsa.medcom.mbx.hq-medcom-office-of-medical-history@mail.mil





























