Embed Size (px)
Citation preview

167
Abstract: Despite a body of compelling evidence pertaining to the root canal accessibility of primary teeth, the number of referrals for inaccessibility of primary molars is considerable. The aim of the present study was to evaluate the prevalence of true and false primary molar inaccessibility among subjects who had been referred by general and pediatric dentists. We examined 199 primary molars in 156 patients (87 males, 69 females) aged 3-7 years who were referred by 215 general and 35 pediatric dentists. Problems related to inaccessibility were recorded for each tooth and any individual canal. One hundred seventy-five inaccessible teeth (87.9%) were successfully rehabilitated to accessible status (P < 0.001). The most frequent cause of inaccessibility was an inappropriate access cavity (42.3%), followed by difficult canals (32.6%) and orifice calcification (25.2%). The tooth most frequently reported as inac-cessible was the maxillary first molar (40.2%), and that least frequently reported was the mandibular second molar (11.6%). The distobuccal canal of the maxillary first molar and the mesiolingual canal of the mandibular first molar were the most commonly inaccessible canals (P < 0.001). Only 1 out of 8 teeth referred as inaccessible was truly inaccessible. It seems that root canal inaccessibility is mostly attributable to lack of expertise among individual practitioners.(J Oral Sci 55, 167-173, 2013)
Keywords: root canal inaccessibility; primary teeth; pulpectomy.
IntroductionEndodontic procedures for the treatment of primary teeth are indicated if the canals are accessible and there is evidence of essentially normal supporting bone. However, the bizarre and tortuous morphology of the root canals and difficulty in cleaning and shaping them has led to negative attitudes toward root canal therapy for primary teeth (1-4). Arduous preparation of primary root canals with complex and variable morphologic geometry, the ambiguous influence of instrumentation, medication and filling materials on developing permanent teeth, and the problems associated with children’s behavior in dental offices have led to a reluctance among dentists to perform such treatment. Accordingly, some studies have suggested that clinical indications for this kind of treat-ment are limited, whereas others have ignored the issue
or totally dismissed it (1,2).It is evident that successful root canal therapy for
primary teeth requires a thorough knowledge of the size, morphology and variation of the root canals. This makes pulp treatment of primary teeth different from that of permanent teeth, and has the potential to greatly improve the effectiveness and outcome of pulp therapy for primary teeth (5,6).
Although the essential facts have not changed, more recent studies have provided substantial insights into our understanding of the complexities of the root canals of primary teeth (7,8). Moreover, some recent studies have shown that primary molars have accessible canals, and
Correspondence to Dr. Naser Asl Aminabadi, Daneshgah St, Golgasht St, Tabriz, IranFax: +98-4113346977 E-mail: [email protected]
Journal of Oral Science, Vol. 55, No. 2, 167-173, 2013
Original
Are referred inaccessible human primary molar teethreally inaccessible?
Naser Asl Aminabadi1), Alireza Sighari Deljavan1), Mohammad Samiei2),and Zahra Jamali3)
1)Department of Pediatric Dentistry, Faculty of Dentistry, Tabriz University of Medical Sciences, Tabriz, Iran2)Department of Endodontics, Tabriz University of Medical Sciences, Tabriz, Iran3)Department of Oral Science, Tabriz University of Medical Sciences, Tabriz, Iran
(Received December 17, 2012; Accepted May 9, 2013)

168
that root canal treatments may not necessarily be lengthy or complicated (9). In addition, large numbers of clinical studies have demonstrated an overall success rate of 90% for pulpectomy techniques in primary teeth, with a wide variation of study design (10-15).
Even though decision-making about the potential success of pulpectomy procedures and the root canal accessibility of human primary teeth does not seem to be especially difficult, concerns still remain and issues continue to be raised in the literature. In addition, clinicians still face a considerable number of referrals because of the attitudes of dental practitioners, who harbor unnecessary misgivings about the feasibility of pulpectomy for primary molars. Therefore a question has arisen as to whether the root canals of primary teeth are, in fact, accessible.
The aim of the present study was to determine the frequency, location and type of false and true inacces-sibility of root canals of primary teeth, and also the frequency distribution of false and true inaccessibility of these canals among general dentists (GDs) and pediatric dentists (PDs).
Materials and MethodsStudy designThis quasi-experimental study was conducted at the Department of Pediatric Dentistry, Tabriz University of Medical Sciences, during the period from March 2011 to July 2012. The participants were referred to the Department of Pediatric Dentistry by practitioners who had practices in the area. The subjects were enrolled by simple sampling, in which a postcard survey containing two sets of questions was mailed to all of 250 local practitioners (GD = 215 and PD = 35). The first set of questions covered each practitioner’s demographic char-acteristics and experience. The second set of questions were intended to identify the best explanation of failure to access the root canals, and which canals were not accessible in the corresponding teeth.
Of the 210 subjects who were referred as inaccessible cases, a total of 199 primary molars in 156 patients (87 males, 69 females) aged 3-7 years were included in the present study. The selected carious molars were candi-dates for partial or complete pulpectomy. The subjects had been referred because practitioners had been unable to locate and/or properly debride the canal(s) of the primary molars. A comprehensive medical and dental history was taken and a treatment plan was established for each patient. The following signs and symptoms were ruled out by clinical and radiographic examinations:
• Any confounding medical history
• Teeth presenting a serious challenge to crown resto-ration
• Teeth with evidence of pulpal floor perforation.• Teeth with extensive pathologic (non-physiologic)
root resorption.• Teeth with inadequate bone support.• Teeth at a stage of development for which preserva-
tion was not important.• Parents who were unwilling to agree to the therapy
and were not prepared to bring their children for follow-up examinations.
Eleven cases were excluded from the study because of pulpal floor perforation and extensive pathologic root resorption. The study procedure, probable risks, and discomfort and as well as benefits were explained to the parents of the children, and all of them signed written informed consent. This study was approved by the ethical and medical research committee of Tabriz University of Medical Sciences (90/16, 2011).
Therapeutic protocolThe study procedure was performed by a single experienced pediatric specialist. Initially, periapical radiographs of the selected teeth were taken using the standard parallel technique. Local anesthesia was induced using inferior alveolar nerve/lingual nerve block for mandibular primary molars and infiltration and superior alveolar nerve block anesthesia (palatal/buccal) for maxillary primary molars using 2% lidocaine with 1:100,000 epinephrine. Standard isolation of the operation site was accomplished by placement of a rubber dam. After removal of the temporary restoration, preliminary assessment of the previous access cavities was done. Thereafter, the likely problems related to the access cavity design (Figs. 1 and 2) were recorded and rectified in order to gain proper access to the orifices and canals. Prior to the access cavity preparation, all of the remaining dental caries as well as undermined enamel structures were eliminated. The remaining roof of the pulp chamber and dentinal remnants overhanging the pulp horns were removed, and a funnel-shaped access to the entrance of the root canals was prepared. After extir-pation of the remaining coronal pulp, the pulp chamber was irrigated with a light flow of sterile 0.9% normal saline solution (16,17).
After preparing the appropriate access cavity, the pulp chamber and the orifice of the canals were assessed using a sharp standard dental explorer (Kohler Mediz-intechnik GmbH & Co., Neuhausen, Germany) and then the root canals were explored using a size 10 K-type file (Dentsply/Maillefer, Ballaigues, Switzerland) in order

169
to determine the number and configuration of the root canals while evaluating the overall accessibility status. One of the characteristics of the root canal anatomy in primary teeth is continuing dentin deposition in the root canal after root length completion (Fig. 2). This
phenomenon can create highly calcified canals and may change the number, size, and shape of the root canals. Moreover, canal entrances may also become obstructed by pulp stones and other dystrophic calcifications that make it more difficult to locate the root canal entrances (16,17). During the present study, canals that were diffi-cult to access were mainly divided into two categories: the first group included root canal-related problems such as calcified canals, unusual root curvatures, and roots with complex anatomies, whereas the second category included amorphous pulp chambers and orifice calcifica-tions such as pulp stones in the pulp chambers (18,19).
The initial endodontic K-file was introduced up to the estimated working length, and a second radiograph was taken. The endodontic file that could be passed along the estimated working length while fitting closely into the canal was used as the initial endodontic file. Subsequently, the corrected working length was determined by radiog-raphy. The estimated working length was considered to be 2 mm short of the primary diagnostic radiographic length. Cleaning of the canals was started from the initial file for the corrected working length and the canals were enlarged three sizes beyond the initial file to eliminate any organic remnants (9,16). Copious irrigation was implemented throughout the preparation. Thereafter, the canals were dried and then filled with zinc oxide-eugenol paste (Dentsply, Petrópolis, RJ, Brazil). The remainder of the pulp chamber was filled with restorative glass ionomer (Dentsply, Weybridge, UK) and a stainless steel crown (Unitek SS Crown-3M Co, Monrovia, CA, USA) was placed (16,17). Information about the number and location of canal orifices and the initial files was recorded for each tooth and any individual canal.
On a random basis, 50 cases were assessed and rated by the second examiner independently and systematically during the stages of treatment to allow for estimation of inter-examiner data agreement.
Statistical analysisAll data are presented as mean ± standard deviation (SD) and n (%). Chi-squared or Fisher’s exact test and Mantel-Haenszel test were used to evaluate the association of qualitative variables including type of inaccessibility, cause of inaccessibility, type of practitioner, type of tooth and root canal. The kappa statistic was calculated for inter-rater reliability assessment. Statistical analysis was performed using the SPSS statistical software package version 15. In the present study P < 0.05 was considered to indicate statistical significance.
Fig. 1 Inappropriate access cavity preparation in maxillary first molar.
Fig. 2 Inappropriate access cavity preparation in mandibular first molar.
Fig. 3 The Stereomicroscope images (16×) of the accessible canal (A) and different types of inaccessibility (B, C, D) in extracted teeth that embedded in methylene blue dye for 48 h.

170
ResultsOf the 210 returned questionnaires, 199 teeth in 156 patients (87 males, 69 females) aged 3-7 years were included in the data analysis, yielding a response rate of 94.8%. Of these, 113 were maxillary molars (first molar: 80, second molar: 33) and 86 were mandibular molars (first molar: 63, second molar: 23). The majority of the participants were GD (n = 125, 80.1%) and the rest were PD (n = 31, 19.9%).
The agreement between the examiners was very good and significant (κ = 0.92, P < 0.001), indicating good agreement.
The findings showed that 175 (87.9%) of the teeth that had been referred as inaccessible were rehabilitated to accessible status, and only 24 teeth (12.1%) were truly inaccessible. It is noteworthy that a significantly high proportion of inaccessibility was false (P < 0.001). The most frequent reason for inaccessibility was inap-propriate access cavity preparation (42.3%), followed by difficult canals (32.6%) and orifice calcification (25.2%).
After the second intervention, true inaccessibility rates among the cases referred by the PD and the GD were 38.2% and 6.7%, respectively. This difference was statistically significant (P < 0.001). Conversely, false root canal inaccessibility was significantly more frequent among GDs compared to PDs (P < 0.001). The difference in the recovery rate for inaccessible teeth, considering different levels of experience among GDs, was not statistically significant, whereas it reached a significant level among PDs with different levels of experience (P < 0.001; Table 1).
Considering the practitioners’ experience, there was no significant change in the frequency of teeth being deemed inaccessible as the years of experience increased among GDs (P > 0.05); however, this rate was significant for PDs (P < 0.05; Table 2).
Among the causes of false inaccessibility, the most frequent pitfall for GDs was an inappropriate access cavity design (45.5%) while that for PDs was difficult canals (42.9%). In addition, primary first molars had a
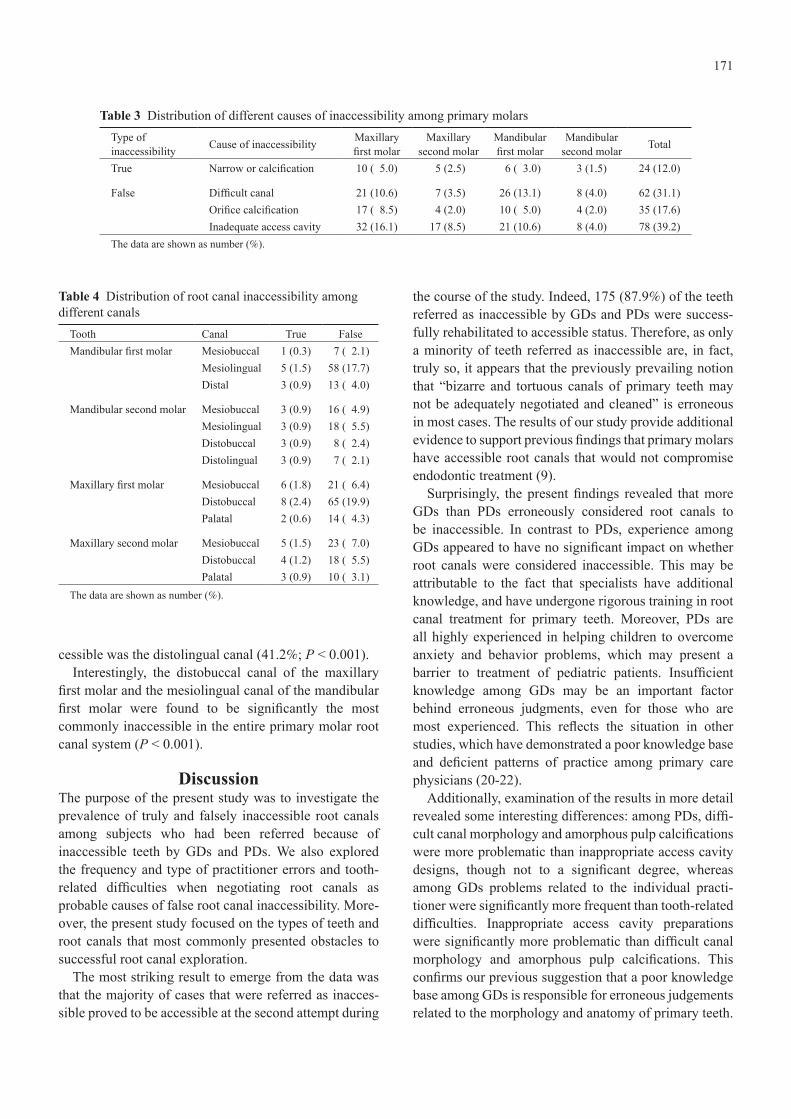
significantly higher rate of inaccessibility than primary second molars (P < 0.001). The tooth most commonly referred as inaccessible was the maxillary primary first molar (40.2%), and that least commonly referred was the mandibular primary second molar (11.6%; Table 3), the rates showing no significant difference between PDs and GDs (P > 0.05).
For PDs, the maxillary and mandibular first primary molars were the teeth most frequently deemed inacces-sible (72.7%), whereas the mandibular primary second molar was the tooth least frequently deemed inaccessible (12.1%). Similarly, among GDs, the most commonly inaccessible teeth were the maxillary and mandibular first primary molars (68.7%), and the least frequently inaccessible tooth was the mandibular primary second molar (11.44%).
The most frequently inaccessible (truly or falsely) root canal in the maxillary primary first molar was the distobuccal canal (62.9%), and the least inaccessible was the palatal canal (13.8%; P < 0.001). The most frequently inaccessible root canal in the maxillary primary second molar was the mesiobuccal canal (44.4%), and the least inaccessible was the palatal canal (20.6%) (P < 0.001; Table 4).
The scenario for mandibular primary molars showed a pattern similar to that of the maxillary primary molars; the most inaccessible root canal in mandibular primary first molar was the mesiolingual canal (72.4%), and the least inaccessible was the mesiobuccal canal (9.2%; P < 0.001). In the same context, the most frequently inacces-sible root canal in the mandibular primary second molar was the mesiolingual canal (16.4%), and the least inac-
Table 1 Frequency of different types of inaccessibility referred from general and pediatric dentistsType of inaccessibility Cause of inaccessibility General dentist
(n = 165)Pediatric dentist
(n = 34) Total P value*
True Narrow or calcified canal 11 ( 6.7) 13 (38.2) 24 (12.1)
< 0.001False Difficult canal 53 (32.1) 9 (26.5) 62 (31.2)Orifice calcification 31 (18.8) 4 (11.8) 35 (17.6)Inadequate access cavity 70 (42.4) 8 (23.5) 78 (39.2)
The data are shown as number (%).Mantel-Haenszel test
Table 2 Frequency of inaccessible teeth considering the practitioner’s experience
DegreeYears of experience
P value0-5 5-10 > 10
General dentist 37 (29.6) 43 (34.4) 45 (36.0) > 0.05Pediatric dentist 19 (61.2) 8 (25.8) 4 (12.9) < 0.05The data are shown as number (%).
171
cessible was the distolingual canal (41.2%; P < 0.001).Interestingly, the distobuccal canal of the maxillary
first molar and the mesiolingual canal of the mandibular first molar were found to be significantly the most commonly inaccessible in the entire primary molar root canal system (P < 0.001).
DiscussionThe purpose of the present study was to investigate the prevalence of truly and falsely inaccessible root canals among subjects who had been referred because of inaccessible teeth by GDs and PDs. We also explored the frequency and type of practitioner errors and tooth-related difficulties when negotiating root canals as probable causes of false root canal inaccessibility. More-over, the present study focused on the types of teeth and root canals that most commonly presented obstacles to successful root canal exploration.
The most striking result to emerge from the data was that the majority of cases that were referred as inacces-sible proved to be accessible at the second attempt during
the course of the study. Indeed, 175 (87.9%) of the teeth referred as inaccessible by GDs and PDs were success-fully rehabilitated to accessible status. Therefore, as only a minority of teeth referred as inaccessible are, in fact, truly so, it appears that the previously prevailing notion that “bizarre and tortuous canals of primary teeth may not be adequately negotiated and cleaned” is erroneous in most cases. The results of our study provide additional evidence to support previous findings that primary molars have accessible root canals that would not compromise endodontic treatment (9).
Surprisingly, the present findings revealed that more GDs than PDs erroneously considered root canals to be inaccessible. In contrast to PDs, experience among GDs appeared to have no significant impact on whether root canals were considered inaccessible. This may be attributable to the fact that specialists have additional knowledge, and have undergone rigorous training in root canal treatment for primary teeth. Moreover, PDs are all highly experienced in helping children to overcome anxiety and behavior problems, which may present a barrier to treatment of pediatric patients. Insufficient knowledge among GDs may be an important factor behind erroneous judgments, even for those who are most experienced. This reflects the situation in other studies, which have demonstrated a poor knowledge base and deficient patterns of practice among primary care physicians (20-22).
Additionally, examination of the results in more detail revealed some interesting differences: among PDs, diffi-cult canal morphology and amorphous pulp calcifications were more problematic than inappropriate access cavity designs, though not to a significant degree, whereas among GDs problems related to the individual practi-tioner were significantly more frequent than tooth-related difficulties. Inappropriate access cavity preparations were significantly more problematic than difficult canal morphology and amorphous pulp calcifications. This confirms our previous suggestion that a poor knowledge base among GDs is responsible for erroneous judgements related to the morphology and anatomy of primary teeth.
Table 3 Distribution of different causes of inaccessibility among primary molarsType ofinaccessibility Cause of inaccessibility Maxillary
first molarMaxillary
second molarMandibular first molar
Mandibular second molar Total
True Narrow or calcification 10 ( 5.0) 5 (2.5) 6 ( 3.0) 3 (1.5) 24 (12.0)
False Difficult canal 21 (10.6) 7 (3.5) 26 (13.1) 8 (4.0) 62 (31.1)Orifice calcification 17 ( 8.5) 4 (2.0) 10 ( 5.0) 4 (2.0) 35 (17.6)Inadequate access cavity 32 (16.1) 17 (8.5) 21 (10.6) 8 (4.0) 78 (39.2)
The data are shown as number (%).
Table 4 Distribution of root canal inaccessibility among different canals
Tooth Canal True False Mandibular first molar Mesiobuccal 1 (0.3) 7 ( 2.1)
Mesiolingual 5 (1.5) 58 (17.7)Distal 3 (0.9) 13 ( 4.0)
Mandibular second molar Mesiobuccal 3 (0.9) 16 ( 4.9)Mesiolingual 3 (0.9) 18 ( 5.5)Distobuccal 3 (0.9) 8 ( 2.4)Distolingual 3 (0.9) 7 ( 2.1)
Maxillary first molar Mesiobuccal 6 (1.8) 21 ( 6.4)Distobuccal 8 (2.4) 65 (19.9)Palatal 2 (0.6) 14 ( 4.3)
Maxillary second molar Mesiobuccal 5 (1.5) 23 ( 7.0)Distobuccal 4 (1.2) 18 ( 5.5)Palatal 3 (0.9) 10 ( 3.1)
The data are shown as number (%).

172
Small access cavity size hinders the operator’s vision of the root canal system, resulting in limited accessibility, a higher frequency of missed canals, and an insufficient area for adequate instrumentation (23). A small access cavity also lengthens the time needed for the procedure and compromises the quality of the treatment (24-26).
In accordance with previous studies, the present find-ings indicate that the accessibility of mandibular primary first molars is significantly lower than that of primary second molars, and that a single canal in the entire root canal system has significantly lower accessibility than other canals (9). Similarly, Zoremchhingi et al. have reported that the mesiolingual canal has the smallest diameter (5).
The scenario for maxillary primary molars follows the pattern described previously: in the maxillary first molar, low accessibility of the distobuccal canal substantially decreases the accessibility of the maxillary first molar relative to the second molar. Accordingly, previous studies have demonstrated that the distobuccal canal has the smallest diameter and that its accessibility is limited compared to other root canals (5,9).
Overall, the present study has shown that almost 7 out of 8 teeth referred as inaccessible cases were rehabilitated to accessible status, and therefore it can be concluded that the “inaccessibility” of primary molar root canals is mostly the result of practitioner-related shortcomings. It is reasonable to assume that practitioner-related failure is related to insufficient knowledge and skill. However, this inference should be weighed against other factors sich as a child’s limited capacity to cooperate during the proce-dure, the limited area of operation, small tooth size, and at risk of being charged with primary molar. In addition, one should be aware of the possibility of undiagnosed cases that are treated without filling and obturation of the missed canals. Root canal treatment for primary molars requires more pertinent and meticulous work than that for permanent teeth and older patients.
The authors acknowledge some limitations of this study, including the small sample size for the PD group, which made it difficult to make conclusive judgements regarding the differences in accessibility observed after intervention. We also consider that broader generalization of the present findings would require further investiga-tion, particularly with regard to practitioner knowledge and skill.
Most of the teeth referred as inaccessible were reha-bilitated to accessible status, and only one in eight were truly inaccessible. It is recommended that dental students should be made more aware of the pitfalls of pulp treat-ment for primary teeth, and encouraged to develop more
effective skills. Academic institutions should actively highlight this issue and place more emphasis on all of its aspects through special training courses and other educational events.
References 1. Hibbard ED, Ireland RL (1957) Morphology of the root canals
of the primary molar teeth. ASDC J Dent Child 24, 250-257. 2. American Academy of Pediatric Dentistry (2009) Guideline
on pulp therapy for primary and young permanent teeth. Pediatr Dent 30, Suppl 7, 170-174.
3. Edgar HJ, Lease LR (2007) Corrections between deciduous and permanent tooth morphology in a European American sample. Am J Phys Anthropol 133, 726-734.
4. Koora K, Sriram CH, Muthu MS, Chandrasekhar Rao R, Sivakumar N (2010) Morphological characteristics of primary dentition in children of Chennai and Hyderabad. J Indian Soc Pedod Prev Dent 28, 60-67.
5. Zoremchhingi, Joseph T, Varma B, Mungara J (2005) A study of root canal morphology of human primary molars using computerised tomography: an in vitro study. J Indian Soc Pedod Prev Dent 23, 7-12.
6. Bagherian A, Kalhori KA, Sadeghi M, Mirhosseini F, Parisay I (2010) An in vitro study of root and canal morphology of human deciduous molars in an Iranian population. J Oral Sci 52, 397-403.
7. Goerig AC, Camp JH (1983) Root canal treatment in primary teeth: a review. Pediatr Dent 5, 33-37.
8. Mani SA, Chawla HS, Tewari A, Goyal A (2000) Evaluation of calcium hydroxide and zinc oxide eugenol as root canal filling material in primary teeth. ASDC J Dent Child 67, 142-147.
9. Aminabadi NA, Farahani RM, Gajan EB (2008) Study of root canal accessibility in human primary molars. J Oral Sci 50, 69-74.
10. Petersson K, Hasselgren G, Petersson A, Tronstad L (1982) Clinical experience with the use of dentine chips in pulpecto-mies. Int Endod J 15, 161-167.
11. Oliet S (1983) Single-visit endodontics: a clinical study. J Endod 9, 147-152.
12. Pekhrun RB (1986) The incidence of failure following single-visit endodontic therapy. J Endod 12, 68-72.
13. Coll JA, Sadrian R (1996) Predicting pulpectomy success and its relationship to exfoliation and succedaneous dentition. Pediatr Dent 18, 57-63.
14. Guelmann M, McEachern M, Turner C (2004) Pulpectomies in primary incisors using three delivery systems: An in vitro study. J Clin Pediatr Dent 28, 323-326.
15. Wisithphrom K, Murray PE, About I, Windsor LJ (2006) Interactions between cavity preparation and restoration events and their effects on pulp vitality. Int J Periodontics Restorative Dent 26, 596-605.
16. Ingle JI, Bakland LK, Baumgartner JC (2008) Endodontic therapy for primary teeth. In: Ingle’s endodontics, 6th ed, Milledge JT ed, BC Decker, Hamilton, 1400.
17. McDonald RE, Avery DR, Dean JA (2011) Dentistry for the

173
child and adolescent. 9th ed, Mosby, St Louis, 354, 403.18. Patel S, Rhodes J (2007) A practical guide to endodontic access
cavity preparation in molar teeth. Br Dent J 203, 133-140. 19. Tang L, Sun TQ, Gao XJ, Zhou XD, Huang DM (2011) Tooth
anatomy risk factors influencing root canal working length accessibility. Int J Oral Sci 3, 135-140.
20. Kausz AT, Levey AS (2002) The care of patients with chronic kidney disease: what must we do and who should do it? J Gen Intern Med 17, 659-663.
21. Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW et al. (2003) National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med 139, 137-147.
22. Hsu CY, Vittinghoff E, Lin F, Shlipak MG (2004) The inci-dence of end-stage renal disease is increasing faster than the
prevalence of chronic renal insufficiency. Ann Intern Med 141, 95-101.
23. Walton RE (1976) Histologic evaluation of different methods of enlarging the pulp canal space. J Endod 2, 304-311.
24. Marlin J, Schilder H (1973) Physical properties of gutta percha when subjected to heat and vertical condensation. Oral Surg Oral Med Oral Pathol 36, 872-879.
25. Zoremchhingi, Joseph T, Varma B, Mungara J (2005) A study of root canal morphology of human primary molars using computerised tomography: an in vitro study. J Indian Soc Pedod Prev Dent 23, 7-12.
26. Gupta D, Grewal N (2005) Root canal configuration of deciduous mandibular first molars – an in vitro study. J Indian Soc Pedod Prev Dent 23, 134-137.





























