Embed Size (px)
Citation preview

VOLUME 46 • NUMBER 6 • 2019
ARCHIVES OF
Revista de Psiquiatria Clínica Online version: www.archivespsy.comiPad edition: APPSTORE/categoria MEDICINA/Psiquiatria Clinica

Editor-in-Chief: Wagner F. Gattaz (São Paulo, Brazil)
Co-Editor-in-Chief: José Alexandre de Souza Crippa (Ribeirão Preto, Brazil)
Assistant Editor: João Paulo Machado de Sousa (Ribeirão Preto, Brazil)
Regional Editor USA: Rodrigo Machado Vieira (Bethesda, USA)
Regional Editor Europe: Wulf Rössler (Zürich, Switzerland)
Child and Adolescent Psychiatry Editors: Guilherme Vanoni Polanczyk (São Paulo, Brazil) Maria Beatriz Linhares (Ribeirão Preto, Brazil) Assistant Editor: Cláudia Maria Gaspardo (Ribeirão Preto, Brazil) Luisa Sugaya (São Paulo, Brazil)
Clinical Psychiatry Editors: Jaime E. C. Hallak (Ribeirão Preto, Brazil) Tânia C. F. Alves (Sao Paulo, Brazil) Assistant Editor: Marcus V. Zanetti (São Paulo, Brazil)
Instruments and Scales Editors: Elaine Henna (Sao Paulo, Brazil) Flávia de Lima Osório (Ribeirão Preto, Brazil) Assistant Editor: Juliana Teixeira Fiquer (São Paulo, Brazil)
Neurosciences Editors: Marcos H. N. Chagas (Ribeirão Preto, Brazil) Andre Russowsky Brunoni (São Paulo, Brazil) Assistant Editor: Leandro da Costa Lane Valiengo (São Paulo, Brazil) Rafael T. de Sousa (São Paulo, Brazil)
Psychology and Psychotherapy Editors: Clarissa M. Corradi-Webster (Ribeirão Preto, Brazil) Julio Peres (Sao Paulo, Brazil) Assistant Editors: Felipe D’Alessandro F. Corchs (São Paulo, Brazil) Paulo Clemente Sallet (São Paulo, Brazil)
Former Editors Antonio Carlos Pacheco e Silva (1972-1985)Fernando de Oliveira Bastos (1972-1985)João Carvalhal Ribas (1980-1985)José Roberto de Albuquerque Fortes (1985-1996)Valentim Gentil Filho (1996-2010)
Editors
ALEXANDER MOREIRA-ALMEIDA ( Juiz de Fora, Brazil)ALEXANDRE ANDRADE LOCH (São Paulo, Brazil)ALMIR RIBEIRO TAVARES JR. (Belo Horizonte, Brazil)ANDRÉ F. CARVALHO (Fortaleza, Brazil)ANDRÉ MALBERGIER (São Paulo, Brazil)ANDRÉ RUSSOWSKY BRUNONI (São Paulo, Brazil)ANDRÉA HORVATH MARQUES (São Paulo, Brazil)ANDREA SCHMITT (Göttingen, Germany)BENEDICTO CREPO-FACORRO (Santander, Spain)CARMITA HELENA NAJJAR ABDO (São Paulo, Brazil)CHRISTIAN COSTA KIELING (Porto Alegre, Brazil)DANIEL MARTINS DE SOUZA (São Paulo, Brazil)DORIS HUPFELD MORENO (São Paulo, Brazil)EDUARDO IACOPONI (London, UK)ELIDA PAULA BENQUIQUE OJOPI (São Paulo, Brazil)EMMANUEL DIAS NETO (São Paulo, Brazil)ÊNIO ROBERTO DE ANDRADE (São Paulo, Brazil)
ESTER NAKAMURA PALACIOS (Vitória, Brazil)FREDERICO NAVAS DEMETRIO (São Paulo, Brazil)FULVIO ALEXANDRE SCORZA (São Paulo, Brazil)GUNTER ECKERT (Frankfurt, Germany)HELENA MARIA CALIL (São Paulo, Brazil)HELENA PAULA BRENTANI SAMAIA (São Paulo, Brazil)HÉLIO ELKIS (São Paulo, Brazil)HOMERO PINTO VALLADA FILHO (São Paulo, Brazil)IRISMAR REIS DE OLIVEIRA (Salvador, Brazil)JAIR CONSTANTE SOARES (Texas, USA)JERSON LAKS (Rio de Janeiro, Brazil)JOÃO LUCIANO DE QUEVEDO (Criciúma, Brazil)JORGE OSPINA DUQUE (Medellín, Colombia)LIGIA MONTENEGRO ITO (São Paulo, Brazil)LILIANA RENDÓN (Assunção, Paraguai)LUIS VALMOR CRUZ PORTELA(Porto Alegre, Brazil)MARCO AURÉLIO ROMANO SILVA (Belo Horizonte, Brazil)
MARCOS HORTES NISIHARA CHAGAS(Ribeirão Preto, Brazil)MARISTELA SCHAUFELBERGER SPANGHERO(Ribeirão Preto, Brazil)MÔNICA SANCHES YASSUDA (São Paulo, Brazil) OSVALDO PEREIRA DE ALMEIDA (Crawley, Australia)PAULO EDUARDO LUIZ DE MATTOS (Rio de Janeiro, Brazil)PAULO RENATO CANINEU (São Paulo, Brazil)PAULO ROSSI MENEZES (São Paulo, Brazil)PAULO SILVA BELMONTE ABREU (Porto Alegre, Brazil)RAFAEL TEIXEIRA DE SOUSA(Bethesda, USA)RENATO TEODORO RAMOS (São Paulo, Brazil)RENÉRIO FRAGUÁS JUNIOR (São Paulo, Brazil)RONALDO RAMOS LARANJEIRA (São Paulo, Brazil)SANDRA SCIVOLETTO (São Paulo, Brazil)TÁKI ATHANASSIOS CORDÁS (São Paulo, Brazil)TENG CHEI TUNG (São Paulo, Brazil)ZACARIA BORGE ALI RAMADAM (São Paulo, Brazil)
INSTRUCTIONS FOR AUTHORS Available on the journal’s website (www.archivespsy.com) and published in the last issue every year (number 6).
Editorial Board

We would like to thank the artist Laila Gattaz, who gently allowed, for exclusive use on the covers of the Archives of Clinical Psychiatry, the series of art works named “Imagens de São Paulo”.
CATALOGUING IN PUBLICATION (CIP) DATA
Archives of Clinical Psychiatry / University of São Paulo Medical School. Institute of Psychiatry - vol. 46, n. 6 (2019). – São Paulo: /IPq-USP, 2011- Fromvolume29(2001),thearticlesofthisjournalareavailableinelectronicformintheSciELO(ScientificElectronicLibraryOnline)database. 1.1. Clinical Psychiatry. University of São Paulo Medical School. Institute of Psychiatry. ISSN : 0101-6083 printed version ISSN : 1806-938X online version
CDD 616.89
Indexing Sources
• ISI (Institute for Scientific Information) - Science Citation Index Expanded (SciSearch®) - Journal Citation Reports/Science Edition• EMBASE - Excerpta Medica Database• LILACS - Literatura Latino-Americana e do Caribe de Informação em Ciências
da Saúde• PERIODICA - Índice de Revistas Latino-Americanas em Ciências
• SciELO - Scientific Eletronic Library Online• SIIC - Sociedad Iberamericana de Información Científica• Scopus (www.scopus.com)• Gale Cengage Learning• DOAJ - Directory of Open Access Journals• HINARI - World Health Organization
Advertisers bear full responsibility for the content of their advertisements. There is no commercial involvement by advertisers in the development of the content or in the editorial
decision-making process for the Archives of Clinical Psychiatry.
This journal is printed on acid-free paper.
Rua Anseriz, 27, Campo Belo – 04618-050 – São Paulo, SP. Fone: 11 3093-3300 • www.segmentofarma.com.br • [email protected]
Cód. da publicação: 23725.11.19
Todos os anúncios devem respeitar rigorosamente o disposto na RDC nº96/08
Financial Support
INDEX
VOLUME 46 • NUMBER 6 • 2019
Editorial
Residency training: a period of risk for mental health? .......................................................................................... 143Ricard Navinés, Victoria Olivé, Rocio Martín-Santos
Original articles
The relationship between coping styles and depression among caregivers of children with cerebral palsy in Nigeria, West Africa .................................................................................................................................................. 145Olajide Benjamin Obembe, Suraju Adeyemo, Oluwayemi Cecilia Ogun, Grace Temitayo Ijarogbe
Frailty and cognitive performance in older adults living in the community: a cross-sectional study ........... 151Daiene de Morais Fabrício, Tiago da Silva Alexandre, Marcos Hortes Nisihara Chagas
Does psychotherapy improve alexithymia? A comparison study among patients with mild or moderate depression ....................................................................................................................................................................... 156Onur Yilmaz, Ali Barlas Mirçik, Merve Kunduz, Müge Çombaş, Ahmet Öztürk, Erdem Deveci, Ismet Kirpinar
Review article
The role of NMDA receptor antagonists, amantadine and memantine, in schizophrenia treatment: a systematic review ...................................................................................................................................................... 165Bruno Terra Junho, Victor Fernandes de Oliveira
Letters to the editor
Primary hyperparathyroidism presenting as major depression with psychotic features ................................ 169Joseph Kuo, Yone-Han Mah, Jui-Teng Wu, Chih-Chung Shiao
Complex drug interaction of carbamazepine, fluvoxamine and clozapine in a patient with bipolar depression ......................................................................................................................................................... 171Wei-Yuan Chen, Yu-Chih Shen

INSTRUCTIONS FOR AUTHORS
General information
The Archives of Clinical Psychiatry is a peer-reviewed journal with six issues per year, published bimonthly. Consonant with its broad access policy, the Journal charges no publication fees, article processing charges, or access fees.
The Journal follows the recommendations of the International Committee of Medical Journal Editors (ICMJE), available at www.icmje.org.
SubmissionsThe Archives of Clinical Psychiatry receives submissions exclusively through
ScholarOne Manuscripts. To start a new submission or check the status of an existing submission, please visit https://mc04.manuscriptcentral.com/rpc-scielo.
All submissions must be accompanied by a cover letter, to be uploaded as a supplementary file under this name during the submission process. The cover letter should summarize the essence of the work, describing main results and potential impact for the field of research. For additional information about the contents of an adequate cover letter, please click here.
In addition to the cover letter, submissions (except letters to the editor) must include an abstract. Both the cover letter and the abstract should respond to the following questions: (i) Why this study has been done?; (ii) How this study has been done? (literature reviews: consulted databases, number of articles found, number of articles included, inclusion and exclusion criteria, meta-analysis or descriptive work; original articles: study design, number of subjects included, study duration, etc.); (iii) What are the key findings?; and (iv) What significance do your results have for the field and for the broader community?
The abstract must not exceed 200 words and should be structured as follows: Background, Objectives, Methods, Results, and Discussion/Conclusion.
NOTE: The Archives of Clinical Psychiatry only accepts submissions in English. Both British and American English variations are acceptable, but not a mix of the two.
Conflicts of interestSubmissions to the Archives of Clinical Psychiatry must include a conflict of interest
statement listing any possible sources of influence on the authors’ capacity to deal with each of the steps of research conduction or reporting; especially – but not limited to – financial and personal interests. When no competing interests exist, this should be clearly stated in this section.
For further information, please visit section “Author Responsibilities” of ICMJE’s recommendations.
EthicsSubmissions reporting results from human studies must have been approved by a
competent review board to certify that the study has been conducted in accordance with the Declaration of Helsinki and its latest revision. Studies with human volunteers must have obtained informed consent from all participants and this should be stated in the Methods section of the manuscript.
Likewise, reports of animal studies should bring information about the approval by competent review boards of ethics in animal research.
For detailed information on the protection of research subjects, please visit http://www.icmje.org/recommendations/browse/roles-and-responsibilities/protection-of-research-participants.html.
Peer reviewUpon receipt, manuscripts are evaluated by the journal editor and/or assistant editors
for their originality, structure, and relevance of contents and conclusions. Manuscripts with insufficient quality or priority for publication are promptly rejected at this point.
After the initial evaluation, submissions are forwarded to an area editor according to their field of knowledge. The area editor then assigns at least two independent reviewers for the submission. In special cases, the area editor may increase or decrease the number of reviews or make a recommendation to the Editor-in-chief based on his own appraisal of the submission. Once all reviews have been received, the area editor makes a recommendation to the editor-in-chief. The area editors’ recommendations are standardized and include the options “Accept”, “Reject”, Minor Review”, and “Major Review”. The editor-in-chief receives the recommendation and has the last word on all submissions.
Copyright Notice: Once accepted for publication, the manuscript becomes permanent property of the Archives of Clinical Psychiatry. This copyright transfer subsumes exclusive and unlimited entitlement of the Archives of Clinical Psychiatry to publish and distribute the full contents of articles in whichever publishing medium, including press and electronic media, in Brazil and abroad.
Manuscript typesThe Archives of Clinical Psychiatry publishes (a) original articles; (b) brief
communications; (c) review articles; and (d) letters to the editor. Case reports will be considered for publication if submitted according to the guidelines for letters to the editor (below).
ORIGINAL ARTICLESTypically, original articles contain new data derived from a sizable and representative
sample of patients or subjects.Original articles should not exceed 3,500 words and include a maximum of 6 tables and/
or figures and 30 references. The word count includes only the main body of the text (i.e., not tables, figures, abstracts or references).
The main text should follow the typical structure of scientific articles, namely, Introduction, Methods, Results, Discussion, Conflicts of interest statement, Acknowledgments (if available), and References.
BRIEF REPORTSBrief reports are short manuscripts with a maximum of 1,500 words, organized according
to the same structure of original articles and with a maximum of 2 tables and/or figures and 15 references.
REVIEW ARTICLESThe Archives of Clinical Psychiatry publishes mainly systematic reviews and meta-
analyses performed according to well-established guidelines such as PRISMA and Cochrane. Non-systematic reviews may be accepted in exceptional occasions.
Reviews should contain a maximum of 5,000 words and 6 tables and/or figures and there is no limit for references.
LETTERS TO THE EDITORLetters to the editor are considered for publication if they do not contain material
submitted to other publications. They should not exceed 500 words, contain a maximum of 1 figure or table, and 10 references. Letters with comments on previous publications of the Archives of Clinical Psychiatry should be submitted within three months of the original publication.
Case reports can be submitted as letters to the editor and should follow the same instructions.
Preparation of ManuscriptsI. TITLE PAGE: The first page should include only the title of the manuscript.II. AUTHORS AND AFFILIATIONS: The second page, which will not be sent to the
reviewers, should include: (a) full authors’ names (first name, middle initials, and family name) and main affiliations (no academic titles); (b) name and address of the institution where the study was conducted; (c) complete address of the corresponding author, including phone, fax, and e-mail.
III. ABSTRACT: The third page should include the abstract, followed by up to five relevant key words.
IV. REFERENCES: Citations in the text should be organized in the Vancouver style, i.e., followed by the appropriate reference Arabic number in parentheses. References should be numbered and listed by their order of appearance in text. Reference lists should be double-spaced.
V. TABLES: Tables should be restricted in size, consecutively numbered with Arabic numbers in the text, and presented in separate pages after the reference list (one page for each table). Refer to every table in the text in numerical order. Indicate within angle brackets < > its preferred location in the main text. Legends should provide a complete understanding of the tables without the need to go back to the text. Tables should be restricted to information that has not been already included in the text.
VI. FIGURES: Figures should be restricted both in number and size to the strictly necessary in order to clarify the text contents. Color illustrations are accepted, but additional costs may have to be covered by authors. Figures should be presented after the reference list in separate pages (one page for each figure). Refer to every figure in the text in numerical order. Indicate within angle brackets < > its preferred location.
VII. LEGENDS: Each table and figure should include a legend with the necessary information for its thorough understanding. For that purpose, a short title followed by a concise explanation of the table or figure should be provided. However, legends should not replicate contents in the text. Abbreviations and symbols that appear in tables or figures should be referred to, even though already cited in the text.
VIII. PATIENT PHOTOGRAPHY: The Archives of Clinical Psychiatry does not encourage the publication of photography of patients. Whenever indispensable for the comprehension of the article, written informed consent must be signed by the patient or respective caregiver, and patient details must be removed from the illustration.

Editorial
Address for correspondence: Ricard Navinés. Hospital Clínic, Universidad de Barcelona, IDIBAPS y CIBERSAM. Villarroell, 170. 08036 – Barcelona, Spain. Telephone: +34 93 2275494. Email: [email protected]
Residency training: a period of risk for mental health?RicaRd NaviNés1https://orcid.org/0000-0002-6999-7510
victoRia olivé2https://orcid.org/0000-0002-2015-4678
Rocio MaRtíN-saNtos1,3 https://orcid.org/0000-0003-4150-4726
1 Servicio de Psiquiatría y Psicología, Hospital Clínic, Instituto de Investigación Biomédica August Pi i Sunyer (IDIBAPS), Departamento de Medicina, Universidad de Barcelona (UB), y Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Barcelona, España. 2 Servicio de Prevención de Riesgos Laborales, Hospital Clínic, y Departamento de Medicina, Universidad de Barcelona (UB), Barcelona, España.3 National Institute for Translational Medicine (INCT-TM), CNPq, Ribeirão Preto, SP, Brazil.
Received: 10/24/2019 – Accepted: 10/28/2019DOI: 10.1590/0101-60830000000214
Navinés R et al. / Arch Clin Psychiatry. 2019;46(6):143-4
There is currently a wide-ranging international debate1-3 on whether the residency period constitutes a health risk for resident physicians. The importance of this debate is reflected in the rise of resident associations in national and international scientific societies4, the programming of seminars, workshops and presentations at national and international conferences5 and the creation of specific care programs for professionals with health problems, including mental health problems3,6.
For most residents, the period of training in their speciality involves a general level of activation that is stimulating and profitable, and they manage to adapt progressively to the professional environment without major problems. However, in some residents the training period may trigger their stress response, which, if prolonged in time and intensity, prevents adequate adaptation and may lead to psychobiological exhaustion or burnout1,3.
The term “stress” refers to the state of anti-homeostatic biological activation that occurs when the organism fails to adapt to the demands of its immediate environment7. Certain occupations, among them the healthcare professions, are considered “highly stressful” and are associated with elevated sick leave rates2. Several studies of stress in resident physicians indicate that this group of professionals is especially vulnerable2,6. The risk factors that have been detected in health practitioners are related either to the profession itself, such as attention to serious pathologies, difficulties in communicating with patients/family, long working hours, or to its organization: excessive workload, lack of supervision, lack of participation in organization, lack of incentives, and the difficulty of combining work with family and social life2. It is also known that repeated or prolonged stress tends to precede the burnout syndrome, described as a state of dissatisfaction with one’s job due to the working conditions2,7.
Recently, the WHO resolved to include burnout syndrome as an occupational phenomenon in the new version of the international diagnostic classification (ICD-11) (https://www.who.int/mental_health/evidence/burn-out/en/). However, the DSM-V does not consider it as a specific syndrome. Traditionally, burnout has been evaluated at the clinical level using the Maslach Burnout Scale, which measures the three main dimensions of the syndrome: emotional exhaustion, depersonalization, and personal accomplishment. Emotional exhaustion refers to the experience of being emotionally exhausted by the demands of work. Depersonalization values the degree to which respondents recognize attitudes of coldness and distancing from people. Finally, the personal accomplishment dimension evaluates feelings of self-efficacy and personal achievement at work8.
In a recent systematic review and meta-analysis9 of 61 cross-sectional and cohort observational studies including more than 22,000 residents from different specialties and countries in America, Asia and Europe, the overall prevalence of burnout evaluated using the Maslach questionnaire was 51.0% (95% CI: 45.0%-57.0%). This prevalence was higher than the rate reported in a previous systematic review and meta-analysis10 of 26 cross-sectional studies from different countries including almost 5,000 medical and surgical residents evaluated with the same questionnaire, which showed an overall prevalence of 35.7% (95% CI: 26.8%-43.5%).
A wide variety of individual and psychosocial factors can affect burnout rates in resident physicians. Regarding gender and age, the results are contradictory. In the systematic review by Low et al.9 male gender was a risk factor, as was older age, but in the review by Rodrigues et al.10 female gender and younger age were reported to be risk factors. Being married or with a partner seems to protect against burnout11. Childcare responsibilities may have a humanizing effect, lowering depersonalization scores rather than adding stress11. Moreover, it seems that residents in certain cultures experience a lower level of burnout and less emotional exhaustion and depersonalization than others11. With regard to personality traits, neurotic and introverted personalities appear to be at the highest risk, and extroversion appears to be a protective factor12; residents with “high cooperation” were more prone to emotional exhaustion and those with high “harm avoidance” and “low self-direction” were significantly more prone to depressive states13. Several studies have found emotional intelligence to be a strong predictor of well-being during residency and to protect against burnout14. The main psychosocial risk factors for the appearance of burnout are excessive work pressure, long hours, feeling of lack of control at work, and lack of supervision1.
Another widely discussed issue is the difference between specialities, since burnout is more prevalent in surgery and emergency care than in medical specialities10. One study that included residents of psychiatry showed a prevalence of 43%9. In general, the main factors influencing burnout are first year residency, recent family stressors, and dissatisfaction with the speciality chosen. In the case of residents in psychiatry, the two situations that cause the highest levels of stress are coping with patients’ suicidal ideation and aggressiveness11.
There is also increasing evidence of the benefit for general and mental health of leading a healthy lifestyle, with a certain amount of physical exercise and socialization. One of the factors seen to influence and even predict the appearance of stress and burnout is

144 Navinés R et al. / Arch Clin Psychiatry. 2019;46(6):143-4
the decrease in sleep hours, which has been related to an increase in the number of hours of work15. In addition, rates of physical exercise tend to fall during residency, even though physical activity has been associated with lower physician burnout and improved personal and professional quality of life2.
The in-work activities that residents associate with relaxation are the possibility of having time to review clinical notes, to chat with patients, and to study and review articles. Also, spaces where to relax (i.e., offices) and time to talk or comment on patients have been found to lower levels of stress among professionals16. Unfortunately, these spaces (both physical and temporal) tend to be in short supply in the workplace. For its part, developing mindfulness skills has been shown to be an important protective factor in several recent studies is2,10.
In summary, the prevalence of stress and burnout during residence is high. The risk depends on individual factors regarding styles for coping with stressful stimuli, although the most decisive factor appears to be the resident’s working conditions. Although the training plan tries to combine the acquisition of clinical, teaching and research skills, it is often very difficult to implement in everyday practice, with high workloads, poor control and supervision, lack of free time and reduced hours of sleep which all make the development of maladaptive responses in residents more likely.
The prevention of burnout symptoms during residency is an issue that remains largely unaddressed, despite its enormous repercussions both at the individual level and in the provision of adequate care to the patients treated.
References
1. Ironside K, Becker D, Chen I, Daniyan A, Kian A, Saheba N, et al. Resident and faculty perspectives on prevention of resident burnout: A focus group study. Perm J. 2019;23. doi: 10.7812/TPP/18-185.
2. Sharp M, Burkart KM. Trainee wellness: Why It matters, and how to promote It. Ann Am Thorac Soc. 2017;14(4):505-12.
3. Meeks LM, Ramsey J, Lyons M, Spencer AL, Lee WW. Wellness and work: mixed messages in residency training. J Gen Intern Med. 2019l;34(7):1352-5.
4. Carrion DM, Gómez Rivas J, Esperto F, Patruno G, Vasquez JL. Current status of urological training in Europe. Arch Esp Urol. 2018;71(1):11-7.
5. Bitran M, González M, Nitsche P, Zúñiga D, Riquelme A. Concern for residents’ wellbeing, an issue discussed at the latin american conference on resident education (LACRE) 2017. Rev Med Chil. 2017;145(10):1330-5.
6. Zabar S, Hanley K, Horlick M, Cocks P, Altshuler L, Watsula-Morley A, et al. “I cannot take this any more!” Preparing interns to identify and help a struggling colleague. J Gen Intern Med. 2019;34(5):773-7.
7. Navinés R, Martín-Santos R, Olivé V, Valdés M. Work-related stress: Implications for physical and mental health. Med Clin (Barc). 2016;146(8):359-66.
8. Maslach C, Jackson SE. The measurement of experienced burnout. J Occup Behav 1981;2:99-113.
9. Low ZX, Yeo KA, Sharma VK, Leung GK, McIntyre RS, Guerrero A, et al. Prevalence of burnout in medical and surgical residents: A Meta-Analysis. Int J Environ Res Public Health. 2019;16(9). pii: E1479.
10. Rodrigues H, Cobucci R, Oliveira A, Cabral JV, Medeiros L, Gurgel K, et al. Burnout syndrome among medical residents: A systematic review and meta-analysis. PLoS One. 2018 12;13(11):e0206840.
11. Ishak WW, Lederer S, Mandili C, Nikravesh R, Seligman L, Vasa M, et al. Burnout during residency training: a literature review. J Grad Med Educ. 2009;1(2):236-42.
12. Prins DJ, van Vendeloo SN, Brand PLP, Van der Velpen I, de Jong K, van den Heijkant F, et al. The relationship between burnout, personality traits, and medical specialty. A national study among Dutch residents. Med Teach. 2019;41(5):584-90.
13. Miyoshi R, Matsuo H, Takeda R, Komatsu H, Abe H, Ishida Y. Burnout in Japanese residents and its associations with temperament and character. Asian J Psychiatr. 2016;24:5-9.
14. Cofer KD, Hollis RH, Goss L, Morris MS, Porterfield JR, Chu DI. Burnout is associated with emotional intelligence but not traditional job performance measurements in surgical residents. J Surg Educ. 2018;75(5):1171-9.
15. Söderström M, Jeding K, Ekstedt M, Perski A, Akerstedt T. Insufficient sleep predicts clinical burnout. J Occup Health Psychol. 2012;17(2):175-83.
16. Benson NM, Chaukos D, Vestal H, Chad-Friedman EF, Denninger JW, Borba CPC. A qualitative analysis of stress and relaxationt contributing to burnout in first-year psychiatry and medicine residents. Acad Psychiatry. 2018;42(5):630-5.

Original article
Address for correspondence: Suraju Adeyemo. Synapse Services, 60 Babapomile Street, Onipetesi Estate, Mangoro, Lagos, Nigeria. E-mail: [email protected]
The relationship between coping styles and depression among caregivers of children with cerebral palsy in Nigeria, West Africaolajide BeNjaMiN oBeMBe1https://orcid.org/0000-0001-7563-1147
suRaju adeyeMo2https://orcid.org/0000-0002-0395-610X
oluwayeMi cecilia oguN1https://orcid.org/0000-0002-3922-0399
gRace teMitayo ijaRogBe1https://orcid.org/0000-0002-4131-6728
1 Federal Neuropsychiatric Hospital Yaba, Lagos State, Nigeria.2 Synapse Services, Onipetesi Estate, Mangoro, Lagos, Nigeria.
Received: 05/05/2018 – Accepted: 09/10/2019DOI: 10.1590/0101-60830000000215
Abstract Background: Caring for a child with cerebral palsy (CP) is an arduous task and the over-reliance on specific coping strategies may predispose caregivers to depression. Objective: The aim of this study was to determine the relationship between the different types of coping strategies and presence of depression in caregivers of children with CP. Methods: One hundred and thirty two participants were recruited into the study. Their coping styles were measured using the Brief COPE inventory while depression was assessed with Mini International Neuropsychiatric Interview. Results: The prevalence of current depressive episodes among the participants was 20.5%. Depression had a strong negative correlation with active coping (r = -0.415), planning (r = -0.432), and positive reframing (r = -0.594), and a weak negative correlation with humor (r = -0.239). But a strong positive correlation with use of instrumental support (r = 0.421) and self-blame (r = 0.448), and a moderate positive correlation with denial (r = 0.313), and behavioral disengagement (r = 0.308). Both emotion–focused (r = -0.361) and problem-focused (r = -0.576) coping style had a strong negative correlation with depression. While dysfunctional coping style had a strong positive correlation with depression (r = 0.489). Discussion: Emotional and problem focused coping style were found to more protective against depression than dysfunctional coping styles among care givers of children with CP.
Obembe OB et al. / Arch Clin Psychiatry. 2019;46(6):145-50
Keywords: Caregiver, children, coping style, depression, cerebral palsy.
Introduction
Caregiving is a normal part of parenting a young child, but managing the child with cerebral palsy can be very exhausting for caregivers1. Studies have shown that taking care of children with impairments often causes detrimental effect on caregivers’ mental health2. Cerebral palsy (CP) describes a set of conditions that is associated with major physical deficits which arise in the early stages of brain development. It results from a non-progressive brain lesion occurring pre-, peri- or post-natally before the second year3. A major characteristic of cerebral palsy is impaired motor function, but many patients also suffer communicative, sensory and intellectual impairments and subsequently experience severe limitations in basic self-care activities such as feeding and dressing3. The overall Prevalence estimates from High Income Countries range from 1.5-3.3 per 1,000 live births4,5, while those in Africa are less precise with limited information depicting wide range figures from 2-10 per 1,000 live births6,7. Cerebral palsy has substantial lifelong effects on daily function, societal participation and quality of life (QOL) for children and their families. Caregiving therefore is often lifelong with the attendant impact on the caregivers (parents).
There is strong evidence that the prevalence of mental health problems, particularly depressive disorders, is higher among the parents of children with disabilities8. On the average, a number of studies put depression in caregivers of children with CP to range from 30%-61.2%9,10. Children with CP are at increased risk of behavioral and emotional problems and subsequently their parents experience increased parental stress. In fact, studies showed that Child behavioral problems uniquely predict parental psychological
symptoms and impaired adjustment11. Although not all parents of children with cerebral palsy develop mental health problems12. Studies have associated different parental coping styles with either positive or negative psychological outcomes in parents of children with cerebral palsy13,14. Coping refers to the cognitive and behavioral efforts made to manage stress15. Specific coping strategies serve to manage or alter the source of stress (problem-focused coping) or to regulate stressful emotions (emotion-focused coping)15.
Previous African study have shown that the task of caring for children with cerebral palsy have a stressful impact on the caregivers which may lower their qualities of life and thus contribute to psychiatric morbidity16. However, in our environment records show a dearth of studies on the types of coping strategies used by the caregivers of children with cerebral palsy, the prevalence of depression in them and the relationship between their coping styles and level of depression. Hence, this study aims to investigate the association between the types of coping strategies used and the development of depression in the of primary care-givers of children with cerebral palsy attending two health facilities in Nigeria. The result will add to the knowledge base about cerebral palsy in Africa and also help bring problems to the fore, and identify caregivers at risk of developing mental illness due to caregiving
Methods
This study was conducted between January and June 2017 in two Federal government owned tertiary hospitals; Child and Adolescent Mental Health Services Centre (CAMHSC) of the Federal Neuro-psychiatric Hospital Lagos, and Lagos University Teaching Hospital

146 Obembe OB et al. / Arch Clin Psychiatry. 2019;46(6):145-50
(LUTH) Idi-Araba, with 138 and 36 registered children and adolescents with cerebral palsy respectively.
The study design was a cross-sectional descriptive study and the participants were recruited through a convenient sampling method. The calculated sample size of 132, with desired degree of confidence set at 0.05 and normal deviate for two-tailed null hypothesis at 95% (1.96).
Data were collected using:
1. Socio-demographic questionnaire: a semi-structured ques-tionnaire which was used to determine socio-demographic variables such as ages of caregiver and child, gender of caregi-ver and child, relationship to child, marital and employment status of the caregiver, number of children and their ages, ethnicity, highest level of education completed, duration of being the primary care-giver, and level of social supports.
2. Brief COPE Questionnaire: a self-report questionnaire used to assess a number of different coping behaviors and thoughts a person may have in response to a specific situa-tion. It is made up of 14 subscales (self-distraction, active coping, denial, substance use, use of emotional support, use of instrumental support, behavioral disengagement, venting, positive reframing, planning, humor, acceptance, religion, and self-blame) with internal consistencies that range from α = 0.57-0.90. These are further grouped into three composite subscales measuring emotion-focused (acceptance, use of emotional support, positive reframing, humour, and religion), problem-focused (active coping, use of instrumental support and planning), and dysfunctional coping (venting, self-dis-traction, denial, behavioural disengagement, self-blame and substance use)17. The instrument has been successfully used in health-relevant studies in Nigeria18.
3. Mini international neuropsychiatric interview; is a short, structured diagnostic interview developed for DSM-IV and ICD-10 psychiatric disorders19. It has a sensitivity is 0.70 and specificity of 0.85, the inter-rater and retest reliabilities are 0.75. MINI has also been widely used in health related studies in Nigeria20. The depression module was used in the study to assess for depressive disorder.
Procedure
Ethical consideration
The permission to carry out this study was obtained from the Research and Ethical committee of the Federal Neuro-Psychiatric Hospital, Yaba, Lagos, and the Research and Ethical committee of the Lagos University Teaching Hospital, Idi-Araba, Lagos. The participants gave a voluntarily written informed consents indicating their willingness to participate in the study after the details of the study had been explained to them. They were also informed of their freedom to opt out of the study and that such decision would not be used against them in any way. High level of confidentiality and anonymity was assured.
Recruitment of participants and data collection
At the out-patient clinics of the study centers, all consecutive caregivers of children and adolescents previously diagnosed with cerebral palsy who met the inclusion criteria and who gave a written informed consent were recruited in to the study. The participants fill the Socio-demographic questionnaire and Brief COPE inventory, which are both self-administered questionnaire, while the depression sections of MINI questionnaire was administered by the researcher. The interview was carried out in a consulting room at the out-patient clinic on a one on one basis. About 6-10 participants were recruited per week and data collection lasted for about five months.
Data management and statistical analysis
The statistical package for social sciences (SPSS) software 20th edition was used for the statistical analysis of the generated data. Chi-square test was used to determine the association between categorical variables while the t-test was used to assess significant difference between two mean values. Regression analyses examined the strength of relationship between type of coping strategy used and depression.
Results
A total of one hundred and thirty-two (132) adult caregivers of children with cerebral palsy participated in this study.
The ages of the participants ranged from 26 to 68 years, with a mean age of 37.57 (±6.96) years (Table 1). Majority (96.2%) of the participants were female, employed (89.4%), married (91.7%) and were mothers (93.2%). Caregivers who had tertiary level of education were 49.2% of the participants, 38.6% had secondary level of education while 12.1% had primary level of education.
Table 1. Socio-demographic characteristics of primary caregivers and their children – N = 132Variables Frequency (n) Percentage (%)Age of caregiver in years
< 30 16 12.130-39 62 47.040-49 47 35.6≥ 50 7 5.3
Gender of caregiversMale 5 3.8Female 127 96.2ReligionChristianity 72 54.5Islam 60 45.5
Employment statusUnemployed 14 10.6Self-employed 76 57.6Paid employment 42 31.8
Absence from work due to caregiving of child No 26 22.0Yes 92 78.0
Marital status of caregiverSingle 3 2.3Married 121 91.7Separated 2 1.5Divorced 1 0.8Widowed 5 3.7
Relationship to childFather 5 3.8Mother 123 93.2Others 4 3.0Level of educationPrimary 16 12.1Secondary 51 38.6Tertiary 65 49.3
Age of caregivers children≤ 5 85 64.46-10 37 28.0> 10 10 7.6
Gender of caregivers childrenMale 87 65.9Female 45 34.1

147Obembe OB et al. / Arch Clin Psychiatry. 2019;46(6):145-50
Age of participants’ children with cerebral palsy ranged from 2 to 16 years with a mean age of 5.22 (±2.92). Most (64.4%) of the participants children were within ages 5 years and below, and of the male (65.9%) gender (Table 1).
Most (65.9%) of the participants had been primary caregivers for less than 5 years, 27.3% for between 6 to 10 years, while 6.8% were caregivers for between 11 to 15 years. Eight out of every ten participants (80.3%) had other children to also care for while 19.7% did not have other children. A quarter of the participants (25.8%) reported to have been blamed for the child’s disability while the prevalence of current depressive episode among primary care givers of children with cerebral palsy was 20.5% (Table 2).
Caregivers of children within the ages 6 and 10 years have a statistically higher rate of depression (32.4% had depression) compared to caregivers of children less than 5 years (17.6%) and caregivers of children above 10 years (0.0%) (p = 0.044). Also, participants who had been caregivers for between 6 to 10 years were more likely to be depressed than those who were caregivers for less than 5 years (17.2%) or more than 10 years (0.0%) (p = 0.038). Similarly, participants who had been blamed for child’s disability (44.1%) had a statistically higher rate of depression than those who had not been blamed (12.2%) in the past. (p ≤ 0.001). Among participants who had been blamed for child’s disability, those who were blamed by their relatives (64.3%) were statistically more likely to have higher rate of depression than those who were blamed by their spouses (33.3%) and others (friends, neighbor) (25.0%), (p ≤ 0.001) (Table 3).
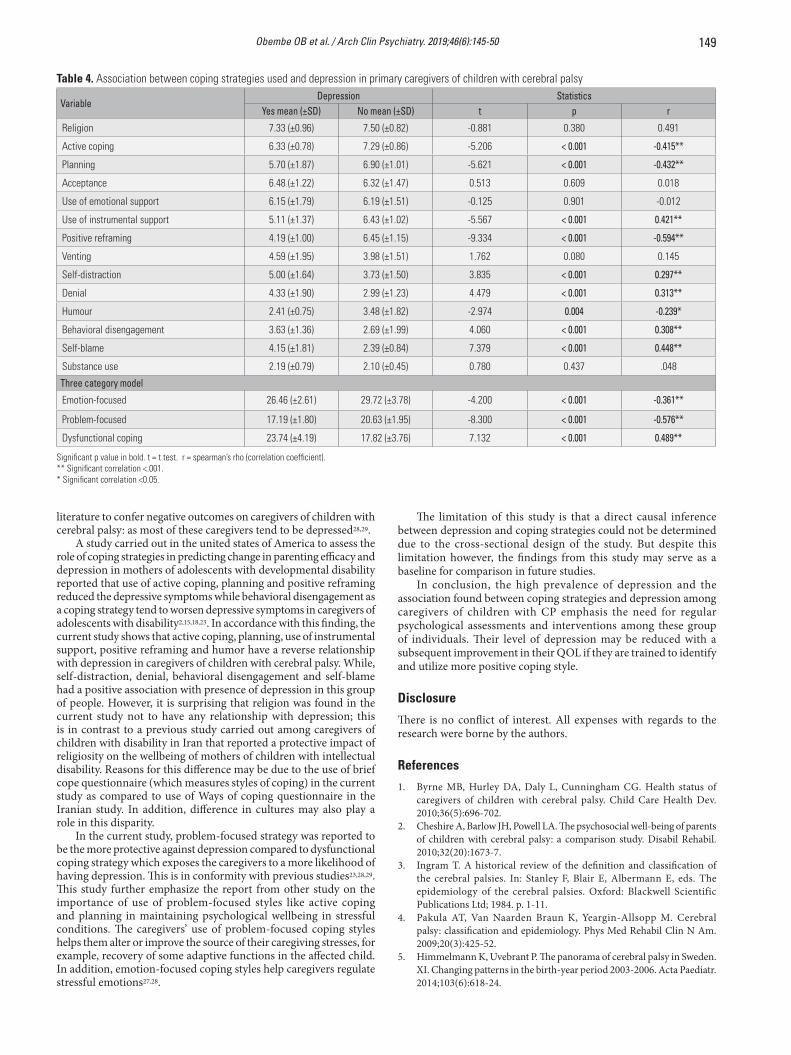
The mean score of active coping was significantly (p ≤ 0.001) lower in participants with depression (6.33 ± 0.78) as compared to those without depression (7.29 ± 0.86). Similarly, planning as a coping style has a statistically (p ≤ 0.001) lower mean score (5.70 ± 1.87) in depressed participant compared to those without depression 6.90 (±1.01) (Table 4).
Use of instrumental support (p ≤ 0.001), positive reframing (p ≤ 0.001), self-distraction (p ≤ 0.001) and denial (p ≤ 0.001) as coping styles were also found to have statistically significant relationships with depression. Participants with depression had lower mean score in use of instrumental support 5.11 (±1.37) and positive reframing 4.19 (±1.00) compared to those without depression who had a higher mean score of 6.43 (±1.02) and 6.45 (±1.15) respectively. On the contrary, participants with depression had a significantly higher
mean score in self-distraction 5.00 (±1.64) and denial 4.33 (±1.90) compared to those without depression who had a lower mean score of 3.73 (±1.50 and 2.99 (±1.23) respectively.
The mean score of humor in participants with depression was 2.41 (±0.75); this was statistically lower than the mean score in those without depression 3.48 (±1.82) (p = 0.004). Conversely, behavioural disengagement (p ≤ 0.001) and self-blame (p ≤ 0.001) have a statistically significant higher mean scores in participants with depression (3.63 ± 1.36 and 4.15 ± 1.81 respectively). There was no statistically significant relationship between depression and religion (p = 0.380), acceptance (p = 0.609), use of emotional support (p = 0.901), venting (p = 0.080), and substance use (p = 0.437).
Depression had a strong negative correlation with active coping (r = -0.415), planning (r = -0.432), and positive reframing (r = -0.594), and a weak negative correlation with humor (r = -0.239). But a strong positive correlation with use of instrumental support (r = 0.421) and self-blame (r = 0.448), and a moderate positive correlation with denial (r = 0.313), and behavioral disengagement (r = 0.308).
Emotion-focused (p ≤ 0.001), problem focused (p ≤ 0.001) and dysfunctional coping (p ≤ 0.001) were found to have statistically significant relationships with depression. Both emotion–focused (r = -0.361) and problem-focused (r = -0.576) coping style had a strong negative correlation with depression. While dysfunctional coping style had a strong positive correlation with depression (r = 0.489) (Table 4).
Discussion
The general aim of this study was to determine the relationship between the different types of coping strategies and presence of depression in caregivers of children with cerebral palsy.
Caregivers of children with cerebral palsy have been reported in previous studies to be more prone to psychological disturbances when compared to caregivers of normally developing children, and majority of them have symptoms of depression. This has been attributed to greater parenting stress and lower satisfaction with life found in these group of caregivers2. The prevalence of depression in the current study was 20.5%. This is lower than prevalence of depression reported in caregiver of children with cerebral palsy in previous studies9,21,22. A prevalence of 45.2% was reported in Tunisia and 31% in Brazil22,23. The difference in prevalence between the previous studies and the current study can be due to cultural differences, and may also be due the use of Hospital Anxiety and Depression Scale which is a self-administered rating instrument in the Tunisian and Brazilian study as compared to MINI, an interviewer administered diagnostic instrument was used in the current study. In addition, the sample size in the Tunisian study was 62 and that of Brazil was 82 while the sample size in the current study was 132.
The current study shows that the age of the caregivers children and duration of caregiving has a great impact on the psychological state of caregivers; those whose children were within the ages of 6-10 years had higher rate of depression and also, caregivers who have been caring for children with cerebral palsy for more than 5 years but less than 11 years were more likely to be depressed than those of lower or higher durations. This may be explained by the fact that reactions to the birth or diagnosis of a disabled child usually progress gradually from an initial feelings of shock and numbness, and then over time leads to a period of helplessness, periods of indifference and anger, at which time they face nearly overwhelming apathy, bitterness and depression10,24.
According to report from previous study, participants with poor marital relationship, inadequate social interaction, isolation and problems with the extended family had a higher rate of depression compared to those without such experiences14,25. The current study shows that caregivers who have been blamed for the child’s condition; especially those who were blamed by their relatives (family member) had a higher rate of depression compared to those who had never been blamed. This finding further emphasis the importance of the need for relatives of caregivers of these group of children to avoidance the use of negative comment or ascribing blames.
Table 2. Frequency table of care giving related characteristics and depres-sion – N = 132Variables Frequency (n) Percentage (%)Duration of caregiving in years
1-5 87 65.96-10 36 27.311-15 9 6.8
Presence of other childrenNo 26 19.7Yes 106 80.3
Presence of social supportNo 19 14.4Yes 113 85.6
Have you been blamed for your child’s disability?No 98 74.2Yes 34 25.8
If blamed, by who? (n = 34)Spouse 12 35.3Relatives 14 41.2Others 8 23.5
DepressionPresent 27 20.5Absent 105 79.5

148 Obembe OB et al. / Arch Clin Psychiatry. 2019;46(6):145-50
Table 3. Association of socio-demographic variable and caregiving characteristics with depression in care giver of children with cerebral palsy – N = 132
Variable Depression
TotalStatistics
Yesn (%)
Non (%) x2 df p
Age of caregiver in years <30 3 (18.8 ) 13 (81.2) 16 0.350 3 0.95030-39 13 (21.0) 49 (79.0) 6240-49 9 (19.1) 38 (80.9) 47≥50 2 (28.6) 5 (71.4) 7
Age of child in years≤5 15 (17.6) 70 (82.4) 85 6.246 2 0.0446-10 12 (32.4) 25 (67.6) 37>10 0 (0.0) 10 (100) 10
Gender of childMale 19 (21.8) 68 (78.2) 87 0.301 1 0.583Female 8 (17.8) 37 (82.2) 45
Employment statusUnemployed 5 (35.7) 9 (64.3) 14 4.524 2 0.104Self-employed 11 (14.5) 65 (85.5) 76Paid employment 11 (26.2) 31 (73.8) 42
Marital status of caregiverMarried 24 (19.8) 97 (80.2) 121 0.695*Others 3 (20.5) 8 (72.7) 11
Level of education Primary 3 (18.8) 13 (81.2) 16 4.488 2 0.106Secondary 6 (11.8) 45 (88.2) 51Tertiary 18 (27.7) 47 (72.3) 65
Relationship to childFather 0 (0.0) 5 (100) 5 2.372 2 0.305Mother 26 (21.1) 97 (78.9) 123Others 1 (25.0) 3 (75.0) 4
Absence from work due to caregivingNo 5 (12.5) 35 (87.5) 40 2.232 1 0.135Yes 22 (23.9) 70 (76.1) 92
Duration of caregiving 1-5 years 15 (17.2) 72 (82.8) 87 6.536 2 0.0386-10 years 12 (33.3) 24 (66.7) 36 11-15 years 0 (0.0) 9 (100.0) 9
Presence of other childrenNo 3 (11.5) 23 (88.5) 6 0.282*Yes 24 (22.6) 82 (77.4) 106
Presence of social supportNo 2 (10.5) 17 (89.5) 19 0.361*Yes 25 (22.1) 88 (77.9) 113
Have you been blamed? No 12 (12.2) 86 (87.8) 98 15.760 1 < 0.001Yes 15 (44.1) 19 (55.9) 34
If blamed, by who? (n = 34)Spouse 4 (33.3) 8 (87.8) 12 18.360 2 < 0.001Relatives 9 (64.3) 5 (35.7 ) 14 Others 2 (25.0) 6 (75.0 ) 8
Significant P value in bold.*Fishers exact test (used where observed cell values were small)
Caregivers of children with Cerebral palsy may face many decades of stressful caregiving responsibility; they encounter a variety of challenges such as overcoming the disappointments attendant to the diagnosis, learning to negotiate a system of health and educational networks and developing strategies for guiding the child’s overall success11,26. Coping strategies have been postulated as one mechanism
by which parents adapt to the stresses associated with raising a child with a disability. Previous studies have reported an association between better caregiver wellbeing and higher level of problem-focused coping style, while those who used dysfunctional coping style were associated with regular emotional distress like depression15,27. Coping styles like denial and avoidance have also been shown in
149Obembe OB et al. / Arch Clin Psychiatry. 2019;46(6):145-50
Table 4. Association between coping strategies used and depression in primary caregivers of children with cerebral palsy
VariableDepression Statistics
Yes mean (±SD) No mean (±SD) t p r
Religion 7.33 (±0.96) 7.50 (±0.82) -0.881 0.380 0.491
Active coping 6.33 (±0.78) 7.29 (±0.86) -5.206 < 0.001 -0.415**
Planning 5.70 (±1.87) 6.90 (±1.01) -5.621 < 0.001 -0.432**
Acceptance 6.48 (±1.22) 6.32 (±1.47) 0.513 0.609 0.018
Use of emotional support 6.15 (±1.79) 6.19 (±1.51) -0.125 0.901 -0.012
Use of instrumental support 5.11 (±1.37) 6.43 (±1.02) -5.567 < 0.001 0.421**
Positive reframing 4.19 (±1.00) 6.45 (±1.15) -9.334 < 0.001 -0.594**
Venting 4.59 (±1.95) 3.98 (±1.51) 1.762 0.080 0.145
Self-distraction 5.00 (±1.64) 3.73 (±1.50) 3.835 < 0.001 0.297**
Denial 4.33 (±1.90) 2.99 (±1.23) 4.479 < 0.001 0.313**
Humour 2.41 (±0.75) 3.48 (±1.82) -2.974 0.004 -0.239*
Behavioral disengagement 3.63 (±1.36) 2.69 (±1.99) 4.060 < 0.001 0.308**
Self-blame 4.15 (±1.81) 2.39 (±0.84) 7.379 < 0.001 0.448**
Substance use 2.19 (±0.79) 2.10 (±0.45) 0.780 0.437 .048
Three category model
Emotion-focused 26.46 (±2.61) 29.72 (±3.78) -4.200 < 0.001 -0.361**
Problem-focused 17.19 (±1.80) 20.63 (±1.95) -8.300 < 0.001 -0.576**
Dysfunctional coping 23.74 (±4.19) 17.82 (±3.76) 7.132 < 0.001 0.489**
Significant p value in bold. t = t test. r = spearman’s rho (correlation coefficient). ** Significant correlation <.001.* Significant correlation <0.05.
literature to confer negative outcomes on caregivers of children with cerebral palsy: as most of these caregivers tend to be depressed28,29.
A study carried out in the united states of America to assess the role of coping strategies in predicting change in parenting efficacy and depression in mothers of adolescents with developmental disability reported that use of active coping, planning and positive reframing reduced the depressive symptoms while behavioral disengagement as a coping strategy tend to worsen depressive symptoms in caregivers of adolescents with disability2,15,18,23. In accordance with this finding, the current study shows that active coping, planning, use of instrumental support, positive reframing and humor have a reverse relationship with depression in caregivers of children with cerebral palsy. While, self-distraction, denial, behavioral disengagement and self-blame had a positive association with presence of depression in this group of people. However, it is surprising that religion was found in the current study not to have any relationship with depression; this is in contrast to a previous study carried out among caregivers of children with disability in Iran that reported a protective impact of religiosity on the wellbeing of mothers of children with intellectual disability. Reasons for this difference may be due to the use of brief cope questionnaire (which measures styles of coping) in the current study as compared to use of Ways of coping questionnaire in the Iranian study. In addition, difference in cultures may also play a role in this disparity.
In the current study, problem-focused strategy was reported to be the more protective against depression compared to dysfunctional coping strategy which exposes the caregivers to a more likelihood of having depression. This is in conformity with previous studies23,28,29. This study further emphasize the report from other study on the importance of use of problem-focused styles like active coping and planning in maintaining psychological wellbeing in stressful conditions. The caregivers’ use of problem-focused coping styles helps them alter or improve the source of their caregiving stresses, for example, recovery of some adaptive functions in the affected child. In addition, emotion-focused coping styles help caregivers regulate stressful emotions27,28.
The limitation of this study is that a direct causal inference between depression and coping strategies could not be determined due to the cross-sectional design of the study. But despite this limitation however, the findings from this study may serve as a baseline for comparison in future studies.
In conclusion, the high prevalence of depression and the association found between coping strategies and depression among caregivers of children with CP emphasis the need for regular psychological assessments and interventions among these group of individuals. Their level of depression may be reduced with a subsequent improvement in their QOL if they are trained to identify and utilize more positive coping style.
Disclosure
There is no conflict of interest. All expenses with regards to the research were borne by the authors.
References
1. Byrne MB, Hurley DA, Daly L, Cunningham CG. Health status of caregivers of children with cerebral palsy. Child Care Health Dev. 2010;36(5):696-702.
2. Cheshire A, Barlow JH, Powell LA. The psychosocial well-being of parents of children with cerebral palsy: a comparison study. Disabil Rehabil. 2010;32(20):1673-7.
3. Ingram T. A historical review of the definition and classification of the cerebral palsies. In: Stanley F, Blair E, Albermann E, eds. The epidemiology of the cerebral palsies. Oxford: Blackwell Scientific Publications Ltd; 1984. p. 1-11.
4. Pakula AT, Van Naarden Braun K, Yeargin-Allsopp M. Cerebral palsy: classification and epidemiology. Phys Med Rehabil Clin N Am. 2009;20(3):425-52.
5. Himmelmann K, Uvebrant P. The panorama of cerebral palsy in Sweden. XI. Changing patterns in the birth‐year period 2003-2006. Acta Paediatr. 2014;103(6):618-24.

150 Obembe OB et al. / Arch Clin Psychiatry. 2019;46(6):145-50
6. El Tallawy HN, Farghaly WM, Rageh TA, Shehata GA, Metwaly NA, Abo Elfto N, et al. Epidemiology of major neurological disorders project in Al Kharga District, New Valley, Egypt. Neuroepidemiol. 2010;35(4):291-7.
7. Couper J. Prevalence of childhood disability in rural KwaZulu-Natal. S Afr Med J. 2002;92(7):549-52.
8. Singer GH. Meta-analysis of comparative studies of depression in mothers of children with and without developmental disabilities. Am J Ment Retard. 2006;111(3):155-69.
9. Basaran A, Karadavut KI, Uneri SO, Balbaloglu O, Atasoy N. The effect of having a children with cerebral palsy on quality of life, burn-out, depression and anxiety scores: a comparative study. Eur J Phys Rehabil Med. 2013;49(6):815-22.
10. Unsal-Delialioglu S, Kaya K, Ozel S, Gorgulu G. Depression in mothers of children with cerebral palsy and related factors in Turkey: a controlled study. Int J Rehabil Res. 2009;32(3):199-204.
11. Ketelaar M, Volman MJ, Gorter JW, Vermeer A. Stress in parents of children with cerebral palsy: what sources of stress are we talking about? Child Care Health Dev. 2008;34(6):825-9.
12. Whittingham K, Wee D, Sanders MR, Boyd R. Predictors of psychological adjustment, experienced parenting burden and chronic sorrow symptoms in parents of children with cerebral palsy. Child Care Health Dev. 2013;39(3):366-73.
13. Rentinck IC, Ketelaar M, Jongmans MJ, Gorter JW. Parents of children with cerebral palsy: a review of factors related to the process of adaptation. Child Care Health Dev. 2007;33(2):161-9.
14. Glenn S, Cunningham C, Poole H, Reeves D, Weindling M. Maternal parenting stress and its correlates in families with a young child with cerebral palsy. Child Care Health Dev. 2009;35(1):71-8.
15. Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: a theoretically based approach. J Pers Soc Psychol. 1989;56(2):267-83.
16. Hamzat TK, Mordi EL. Impact of caring for children with cerebral palsy on the general health of their caregivers in an African community. Int J Rehabil Res. 2007;30(3):191-4.
17. Cooper C, Katona C, Livingston G. Validity and reliability of the brief COPE in carers of people with dementia: the LASER-AD Study. J Nerv Ment Dis. 2008;196(11):838-43.
18. Yussuf AD, Issa BA, Ajiboye PO, Buhari OI. The correlates of stress, coping styles and psychiatric morbidity in the first year of medical
education at a Nigerian University. Afr J Psychiatry (Johannesbg). 2013;16(3):206-15.
19. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59 Suppl 20:22-33;quiz 34-57.
20. Adewuya AO, Ola BA, Aloba OO, Mapayi BM, Oginni OO. Depression amongst Nigerian University students. Prevalence and sociodemographic correlates. Soc Psychiatry Psychiatr Epidemiol. 2006;41(8):674-8.
21. Marx C, Rodrigues EM, Rodrigues MM, Vilanova LC. Depression, anxiety and daytime sleepiness of primary caregivers of children with cerebral palsy. Rev Paul Pediatr. 2011;29(4):483-8.
22. Toulgui E, Jemni S, Samia F, Lazreg N, Mtaouaa S, Khachnaoui F. Depression and anxiety in mothers of children with cerebral palsy: Comparative study. Ann Phys Rehabil Med. 2016;59(Suppl):e9.
23. Woodman AC, Hauser‐Cram P. The role of coping strategies in predicting change in parenting efficacy and depressive symptoms among mothers of adolescents with developmental disabilities. J Intellect Disabil Res. 2013;57(6):513-30.
24. Parkes J, McCullough N, Madden A, McCahey E. The health of children with cerebral palsy and stress in their parents. J Adv Nurs. 2011;65(11):2311-23.
25. Badaru UM, Ogwumike OO, Adeniyi AF, Kaka B. Psychosocial adversities and depression in mothers of children with cerebral palsy in Nigeria. J Pediatr Neurol. 2013;11(1):1-7.
26. Saloviita T, Italinna M, Leinonen E. Explaining the parental stress of fathers and mothers caring for a child with intellectual disability: a Double ABCX Model. J Intellect Disabil Res. 2003;47(Pt 4-5):300-12.
27. Folkman S, Lazarus RS. Coping as a mediator of emotion. J Pers Soc Psychol. 1988;54(3):466-75.
28. Kim HW, Greenberg JS, Seltzer MM, Krauss MW. The role of coping in maintaining the psychological well‐being of mothers of adults with intellectual disability and mental illness. J Intellect Disabil Res. 2003;47(4‐5):313-27.
29. Gavidia-Payne S, Stoneman Z. Marital adjustment in families of young children with disabilities: associations with daily hassles and problem-focused coping. Am J Ment Retard. 2006;111(1):1-14.

Original article
Frailty and cognitive performance in older adults living in the community: a cross-sectional studydaieNe de MoRais FaBRício1https://orcid.org/0000-0001-8609-1190
tiago da silva alexaNdRe2https://orcid.org/0000-0003-3791-9793
MaRcos HoRtes NisiHaRa cHagas1,2https://orcid.org/0000-0003-3752-7984
1 Department of Psychology, Federal University of São Carlos, São Carlos, SP, Brazil.2 Department of Gerontology, Federal University of São Carlos, São Carlos, SP, Brazil.
Institution where the study was conducted: Federal University of São Carlos (UFSCar), São Carlos, SP, Brazil.
Received: 11/29/2018 – Accepted: 08/12/2019DOI: 10.1590/0101-60830000000216
AbstractBackground: Cognitive impairment and frailty are important problems affecting the elderly population. Frail elderly present worse overall cognitive performance. Objective: The aim of this study was to investigate general and domain-specific cognitive performance among non-frail, pre-frail, and frail elderly persons. Methods: This is a cross-sectional study in which 267 elderly persons living in São Carlos, SP were divided into three groups according to the frailty criteria defined by Fried et al. Cognitive performance was evaluated with a battery of cognitive tests covering domains such as memory, attention, language, and executive functioning. A multinomial logistic regression analysis adjusted for age, gender, and education was performed to evaluate the association between performance in cognitive domains and levels of frailty. Results: Frailty was significantly associated with lower scores on the global cognitive test (RRR = 0.86; IC 95% 0.78-0.96; p < 0.01), word list memory (RRR = 0.92; IC 95% 0.86-0.99; p = 0.02), and figure list recognition (RRR = 0.78; IC 95% 0.62-0.99; p = 0.04). Pre-frailty was associated with lower scores on the word list memory (RRR = 0.92; IC 95% 0.86-1.00; p = 0.04) and naming test (RRR = 0.82; IC 95% 0.69-0.99; p = 0.03). Discussion: Frailty syndrome can influence general cognition and specific domains such as memory and language. Prospective studies will be fundamental to evaluate the causal relation between frailty and cognition.
Fabrício DM et al. / Arch Clin Psychiatry. 2019;46(6):151-5
Keywords: Cognition, elderly, frailty, mental health.
Address for correspondence: Daiene de Morais Fabrício. Federal University of São Carlos – Department of Psychology. Rodovia Washington Luís, km 235, Jardim Guanabara – 13565-905 – São Carlos, SP, Brazil. Telephone: +55 (16) 99230-3366. E-mail: [email protected]
Introduction
Cognitive impairment is becoming more prevalent in older persons, and the consequences of dementia for this population are an increasingly worrying public health issue1. Thus, the study of diseases and syndromes most present in the elderly population is critical in order to contribute to the promotion and restoration of their health and quality of life2. As well as leading to reduced cognitive capacity and overload of homeostatic control mechanisms, the aging process can also result in frailty3.
The frailty syndrome is a complex concept with many definitions and screening methods. It is estimated that the prevalence of the frailty syndrome varies from 5% to 58%4. Fried et al.5 defined frailty as a state of physiological vulnerability associated with aging, which results from a reduced homeostatic reserve and difficulty for the body to adequately respond to stressful events5. Thus, clinical manifestations of this syndrome would be linked to impairment of the functional reserve of important organic systems in charge of hormonal, immunological, inflammatory, and neurological processes5. Therefore, a frail individual’s organism may not develop adaptive responses to stressors, such as intense physical activity, extreme temperatures, or acute diseases5. According to the definition by Fried et al.5, the frail individual has three or more of the following biological features: unintentional weight loss (greater than 4.5 kg or 5% of the body weight in the previous year); self-reported fatigue; muscle weakness; low level of physical activity; and slow walking speed5. On the other hand, other definitions of frailty include social, psychological, and cognition factors. Regardless of the diagnostic method, frailty is associated with aggravation of diseases, cognitive and functional decline, hospitalization, and death6.
Clinically, cognitive decline progresses in tandem with functional decline7. However, the way physical frailty contributes to the cognitive deficit is not fully established in the literature7. Scientific evidence suggests that the frailty syndrome can be a significant risk factor for dementia in elderly persons8,9, with higher levels of frailty being associated with lower scores of cognitive tests5,10. Environmental and genetic factors may also influence the relation between physical frailty and cognitive functions. Moreover, a hypothetical model proposes that oxidative stress, mitochondrial dysfunction, possible damage to DNA, and inflammation may cause impairment in both systems7.
The close link between frailty and cognition helped create a new term to describe individuals with both characteristics. Thus, cognitive frailty is a syndrome defined by physical frailty and cognitive impairment in elderly persons without a diagnosis of dementia11. Frail elderly persons suffering from cognitive impairment are prone to deleterious effects; consequently, understanding the association between these two variables may contribute to planning early and effective interventions12.
A review article examining the current evidence on the relation between frailty and cognition13 found that the vast majority of the studies evaluated the frailty syndrome using the components defined by Fried et al.5, since the objective was to analyze the physical dimension of the syndrome13. As for cognitive evaluation, the studies mainly used brief screening scales, such as the Mini-Mental State Examination (MMSE)13. These findings suggest the need to use more complex batteries for cognitive evaluation to determine the domains most altered by frailty.
Interest in how different cognitive domains are altered in the presence of the frailty syndrome is recent. Studies suggest that the memory domain is less affected in frail persons than the executive function14,15. On the other hand, a study conducted with 761 elderly persons with no cognitive

152 Fabrício DM et al. / Arch Clin Psychiatry. 2019;46(6):151-5
impairment at baseline found that physical frailty was associated with a risk higher than 60% of developing mild cognitive impairment, and this association was maintained after adjusting for depression and cardiovascular disease symptoms16. The frailty syndrome was linked to a faster decline in four cognitive domains (semantic memory, working memory, perceptive speed, and visuospatial capacity)16.
A study evaluating 4,317 individuals from the age of 50 found that pre-frailty and frailty are associated with lower scores in the attentional domain in regression analyses17. Complementing these data, Han et al.18 evaluated 10,388 aged 65 years or older and found that frail elderly had worse scores on the MMSE. The regression analyses showed that cognitive impairment was associated with a higher risk of the syndrome in men, as well as the orientation and attention domains were associated with a higher probability of occurrence of the syndrome in both sexes18.
Corroborating the study cited above, Chen et al.19 investigated the association between global cognition and frailty in the elderly without dementia. Lower scores on cognitive tests, as well as on their specific domains, were associated with higher likelihood of frailty19. These studies reaffirm the close relationship between global cognition, specific cognitive domains, and frailty in the elderly. In this sense, detailed information about both variables can contribute to effective interventions in the clinical context.
In the Brazilian context, few studies have sought to explore the most altered cognitive domains in the presence of the syndrome. To evaluate the frailty syndrome in Brazilian elderly and its related factors, the FIBRA-BR study found that there were more frail and pre-frail elderly with cognitive deficits than elderly classified as non-frail in seven Brazilian cities14,20. Components such as muscle strength and slow gait were associated with performance in the MMSE, the verbal fluency test, and the clock drowning test20. Besides, the frail elderly showed worse performance in temporal orientation and immediate memory14. In this way, continuing to explore the most altered cognitive domains in the presence of frailty through broader batteries of cognitive screening may contribute to uncovering new domains that could be altered in the presence of the syndrome. Thus, the objective of the present study was to investigate the differences in general and domain-specific cognitive performance between non-frail, pre-frail, and frail elderly persons.
Methods
Setting and participants
The study was carried out in the city of São Carlos, a municipality located in the interior of the state of São Paulo, Brazil. The city has 28,696 inhabitants with more than 60 years of age, corresponding to 12.9% of the total population21. The study was carried out in a catchment area covered by a family health program, in which 317 individuals aged over 60 years were registered as dwellers. During home visits, 28 individuals were not found in their homes or no longer lived at the address, 5 refused to participate in the study, 2 were bedridden, and 15 did not complete the frailty scale. Thus, the final sample consisted of 267 participants. The data were collected between March 2016 and February 2017.
Procedures
This study was approved by the ethics committee of the Federal University of São Carlos (CAAE: 48602515.5.0000.5504), and all participants signed the informed consent form prior to participation. Five trained gerontologists conducted the interviews at the participants’ homes. Sociodemographic data were also collected.
The participants were divided into frail, pre-frail, and non-frail groups, according to the criteria adopted by Fried et al.5 A self-report instrument of frailty validated for the Brazilian context was used22. The instrument is composed of five biological components: unintentional weight loss, manual grip strength, self-reported fatigue, reduced walking speed, and low level of physical activity22. The classification of frailty follows the criteria of Fried et al.5: “frail” individuals score
positively on three or more components, “pre-frail” score positively on one or two components, and “non-frail” do not score positively on any component5,22. In this instrument, the elderly respond “yes” or “no” to each one of the biological components: (1) unintentional weight loss – “In the last 12 months, did you lose weight without going on any diet?”; (2) manual grip strength – “In the last 12 months, do you feel weaker or think your strength has decreased?”; (3) reduced walking speed – “Do you think that you are walking more slowly than you did 12 months ago?”; (4) low level of physical activity – “Do you think that you are currently performing less physical activity than you did 12 months ago?”, and (5) fatigue – “In the past week, how often did you feel that you could not perform daily activities (you started something but could not finish)?” and “In the past week, how often did the performance of your routine activities require a major effort?”22.
As for the cognitive evaluation, the following instruments were used:– MMSE: This is a screening tool widely used for evaluation
of general cognition with a score ranging from 0 to 30. It evaluates temporal and spatial orientation, memory (fixation and evocation), language, attention, and calculation23;
– Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) neuropsychological battery: This battery is compo-sed of the following cognitive tests: verbal fluency (animals), Boston naming test of 15 items, MMSE, word list memory, constructional praxis, delayed word list recall, word list recog-nition, and delayed praxis recall24. In the memory evaluation of this battery, the word list memory, a list of 10 words is presented to the participant, who should remember as many words as possible for a maximum period of 90 seconds (free recall). The procedure is repeated another two times, and the score is calculated as the sum of the words remembered in the three attempts. Subsequently, constructional praxis is evaluated by copying four figures. The delayed recall of the previously presented word list is performed for a maximum of 90 seconds. The 10 initial words are presented along with 10 distracters, and the participant must recognize which words belong to the previously presented list. Finally, the four previously copied drawings are reproduced24;
– Brief Cognitive Screening Battery (BCSB): This battery inclu-des verbal fluency (animals), clock drawing test, and figure memory test (incidental, immediate, learning, delayed, and of recognition). It is used with good accuracy in populations with high illiteracy rates or low levels of education25. The evaluation of memory of this battery involves the presentation of 10 figures (shoe, spoon, comb, tree, turtle, key, airplane, house, book, and bucket), which should be named aloud immediately by the individual. Then the figures are presen-ted another two times, followed each time by an immediate recall. After performing the verbal fluency test and the clock drawing test, the 10 figures should be remembered in the delayed memory test, followed by a final recognition test (10 target figures with 10 distracting figures)25;
– Subtest of similarity of the Cambridge Mental Disorders Examination of the Elderly (CAMDEX): This test consists of four questions that evaluate the abstraction ability of the par-ticipants from the similarity between two things or objects, for instance, “What do an apple and a banana have in common?”26;
– Digit span test (backward and forward) of the Wechsler Me-mory Scale-Revised: Consisting of seven pairs of numerical sequences with different amounts of digits, this test is applied in backward and forward order. In the forward span, the sequences have 3 to 9 numbers, and in the backward span, 2 to 8 numbers27. The test ends after error in two consecutive sequences. The maximum quantity of repeated numbers without error is registered for each version27.
Statistical analyses
A descriptive analysis was performed for the independent variables considering the total sample and the three frailty groups (non-frail,

153Fabrício DM et al. / Arch Clin Psychiatry. 2019;46(6):151-5
pre-frail, and frail). Pearson’s chi-square test, analysis of variance (ANOVA), or Kruskall-Wallis test were used to assess differences between the groups according to the sample distribution and variable type. The association between frailty and cognitive performance was analyzed using multinomial logistic regression. The relative risk ratio (RRR) and their respective 95% confidence intervals (IC 95%) were calculated for each cognitive test, adjusting for age, gender, and education. The “non-frail” group was considered as the reference in the regression models. The analyses were performed using the STATA 15.1, and the significance level considered was 5%.
Results
The participants were classified as non-frail (n = 36), pre-frail (n = 71), and frail (n = 160). Sociodemographic data (gender, age, and education), as well as the average scores on the cognitive tests in
each frailty group, are shown in Table 1. The frail group had a higher number of women (63.8%) than men. The average age was 71.5 years old (±8.6), and the sample had low levels of schooling (63.8% with less than 4 years of schooling). The frail group presented a lower mean in all cognitive test scores. Nevertheless, the tests with statistically significantly differences were the MMSE, the CERAD battery word list, and the BCSB recognition item, the Boston naming test, and the backward digit span test.
The multinomial logistic regression results are shown in Table 2. Frailty was significantly associated with lower scores on the MMSE (RRR = 0.86; IC 95% 0.78-0.96; p < 0.01), CERAD word list memory (RRR = 0.92; IC 95% 0.86-0.99; p = 0.02), and BCSB figure list recognition (RRR = 0.78; IC 95% 0.62-0.99; p = 0.04). The pre-frail level was associated with lower scores on the CERAD word list memory (RRR = 0.93; IC 95% 0.86-1.00; p = 0.04) and Boston naming test (RRR = 0.82; IC 95% 0.69-0.99; p = 0.03).
Table 1. Sociodemographic variables and battery of cognitive tests in the three groups of frailty (non-frail, pre-frail and frail)Variable Total (n = 267) Non-frail (n = 36) Pre-frail (n = 71) Frail (n = 160) pAge 70.2 (±7.7) 68.0 (±5.9) 68.6 (±5.5) 71.5 (±8.6) 0.04Sex
FM
61% 39%
36.1% 63.9%
60.6% 39.4%
63.8%36.3%
<0.01
Education ≥4 year<4 year
43.8%56.2%
52.8%47.2%
56.3%43.7%
36.3%63.8%
<0.01
MMSE 22.2 (±5.0) 24.6 (±4.0) 23.0 (±4.7) 21.2 (±5.1) <0.01Word list memory (CERAD) 12.1 (5.8) 14.7 (±6.0) 12.5 (±5.4) 11.5 (±5.8) <0.01Delayed recall (CERAD) 3.0 (±2.5) 3.5 (±2.4) 3.1 (±2.5) 2.9 (±2.5) 0.32Recognition (CERAD) 7.2 (±3.1) 7.9 (±3.2) 7.3 (±3.0) 7.0 (±3.0) 0.07Constructional praxis (CERAD) 5.3 (±3.3) 5.7 (±3.4) 5.8 (±3.0) 5.0 (±3.4) 0.30Figures list memory (BCSB) 19.8 (6.3) 20.2 (±5.8) 20.9 (±6.3) 19.3 (±6.4) 0.10BCSB (Delayed recall) 6.5 (±2.7) 6.5 (±2.3) 7.0 (±2.8) 6.3 (±2.8) <0.01BCSB (Recognition) 8.4 (±2.7) 9.3 (±1.6) 8.5 (±2.6) 8.1 (±2.8) <0.01Abstraction subtest (CAMDEX) 2.7 (±2.2) 3.3 (±2.6) 2.8 (±2.0) 2.4 (±2.2) 0.11Clock Drawing Test 4.8 (±3.6) 5.0 (±3.5) 5.2 (±3.6) 4.7 (±3.6) 0.32Verbal fluency 10.4 (±4.0) 10.9 (±4.4) 10.7 (±4.1) 10.1 (±3.7) 0.68Boston Naming test 11.2 (±2.9) 12.4 (±2.3) 11.0 (±3.0) 11.0 (±2.8) 0.04Digit extension test (Forward) 4.3 (±1.4) 4.5 (±1.2) 4.6 (±1.4) 4.2 (±1.4) 0.14Digit extension test (Backward) 2.3 (±1.2) 2.7 (±0.9) 2.4 (±1.1) 2.1 (±1.3) 0.03
MMSE: Mini-Mental State Examination; CERAD: Consortium to Establish a Registry for Alzheimer’s disease neuropsychological battery; BCSB: Brief Cognitive Screening Battery.
Table 2. Multivariate regression analysis of cognitive domains in relation to frailty (n = 267)
VariableReference group (non-frail)
GroupsPre-frail Frail
RRR p RRR pMMSE 0.90 (0.80-1.00) 0.06 0.86 (0.78-0.96) < 0.01Word list memory (CERAD) 0.93 (0.86-1.00) 0.04 0.92 (0.86-0.99) 0.02Delayed recall (CERAD) 0.91 (0.76-1.07) 0.25 0.92 (0.79-1.07) 0.28Recognition (CERAD) 0.91 (0.77-1.06) 0.22 0.93 (0.81-1.08) 0.35Constructional praxis (CERAD) 1.01 (0.88-1.17) 0.84 1.00 (0.87-1.13) 0.91Figures list memory (BCSB) 1.01 (0.94-1.09) 0.78 0.98 (0.92-1.05) 0.67Delayed recall (BCSB) 1.03 (0.88-1.22) 0.69 0.97 (0.84-1.13) 0.70Recognition (BCSB) 0.79 (0.62-1.01) 0.06 0.78 (0.62-0.99) 0.04Abstraction subtest (CAMDEX) 0.87 (0.72-1.06) 0.17 0.88 (0.73-1.05) 0.15Clock Drawing Test 1.00 (0.88-1.14) 0.93 1.02 (0.90-1.15) 0.75Verbal fluency 1.00 (0.90-1.10) 0.93 0.99 (0.90-1.09) 0.81Boston Naming test 0.82 (0.69 -0.99) 0.03 0.89 (0.75-1.06) 0.19Digit extension test (Forward) 1.15 (0.84-1.56) 0.39 1.01 (0.76-1.34) 0.94Digit extension test (Backward) 0.89 (0.61-1.31) 0.57 0.80 (0.57-1.13) 0.21
Adjusted for age, sex and education. RRR: Relative Risk Ratio; MMSE: Mini-Mental State Examination; CERAD: Consortium to Establish a Registry for Alzheimer’s disease neuropsychological battery; BCSB: Brief Cognitive Screening Battery.

154 Fabrício DM et al. / Arch Clin Psychiatry. 2019;46(6):151-5
Discussion
In the present study, most participants were classified as frail (59.9%) and pre-frail (26.6%). Participants in the frail group were more likely to be women and have advanced age and low education level. This result is compatible with those from other studies evaluating the frailty syndrome in elderly persons28,29. This profile of frail elderly persons may be explained by the feminization of ageing and a significant physiological loss following this process, which may contribute to the emergence of the frailty syndrome in this population5. Furthermore, although low schooling is not directly considered as a risk factor for frailty, it can consequently decrease the quality of life of aging individuals, thus influencing the occurrence of the syndrome30.
A review of the literature examining the mechanisms involved in the relation between the frailty syndrome and cognitive performance found that few studies tried to answer in an experimental way the effect of the frailty syndrome on the decline of cognitive functions31. However, longitudinal studies indicate that frailty and cognitive decline are mutually related, since the presence of frailty increases the risk of cognitive decline and the presence of cognitive decline increases the risk of frailty. A meaningful discussion to be held is the role of cognitive decline in the frailty syndrome. Sternberg et al.4 found that the cognitive domain was present in 50% of the syndrome definitions4. Thus, the central aspect of this debate lies in the frailty construct.
In this study, the biological model proposed by Fried et al.5 was used to evaluate the association of frailty with cognitive aspects, since using a model that included cognition could erroneously increase the association because of collinearity between the variables. Moreover, the model by Fried et al.5 is the most frequently used in the current literature. However, it must be pointed out that other frailty models include cognition among the possible domains that may be altered in the syndrome. This study found significant differences between the frail and non-frail groups in global cognition, BCSB figure recognition, and CERAD word list. Additionally, we found differences between the non-frail and pre-frail groups in the Boston naming test. The tests used to evaluate these domains are traditionally used in the neuropsychological evaluation of dementias, especially Alzheimer’s disease (AD). Buchman et al.32 examined the relation between frailty, cerebral infarcts, dementia with Lewy bodies, and AD, and found that the frailty syndrome was associated only with AD (β = 0.252, SE = 0.077, p = 0.001)32. The authors raised the hypothesis that the frailty syndrome could be a non-cognitive manifestation of AD32. In this context, the introduction of frailty assessment in individuals with dementia, especially those with the AD, seems fundamental. Research and public policies should increasingly focus on developing strategies to maintain cognitive and physical health during the aging process.
Bunce et al.33 assessed associations between specific cognitive domains and the frailty syndrome33. At baseline, the frail elderly persons showed poorer cognitive performance in processing speed, word and face recognition, episodic memory, verbal fluency, and reaction time33. However, there were no significant changes throughout the 12 years of study for any of the cognitive variables33. Our findings also showed a higher association between the memory domain and frailty, so that each figure that was recognized in the BCSB decreased the risk of the elderly person being in the frail group by 22%, just as each word remembered in the list reduced the risk by 8%.
In addition, we found that the Boston naming test was more altered in pre-frail elderly persons. Since pre-frailty is an intermediate state of the syndrome, we hypothesized that language impairment could contribute to a more rapid impairment of other cognitive domains and, consequently, the progression of the syndrome. However, we did not find any studies specifically analyzing the language domain in the presence of frailty. Thus, our findings point to a cognitive domain that may also be altered in the presence of the syndrome and call for new studies assessing the relationship between these two variables more specifically.
Another study that explored the relation between frailty and functioning in cognitive domains found significant differences when comparing frail and non-frail elderly in executive functions and processing speed, but no significant differences in global cognition15. When comparing this finding with our results, the methodological differences of the studies may explain the differences found in cognitive domains. For example, the methods for screening the syndrome and defining the frailty groups were different in the two studies. The authors of the former study also prioritized instruments that assessed processing speed and executive functions, e.g., the Wechsler Adult Intelligence Scale (WAIS-III), the Trail Making Test (part A), and the Stroop color-word test15.
In an attempt to explore the frailty and cognitive performance of Brazilian elderly through the BCSB, Yassuda et al.20 found an association of gait speed and reduced strength to cognitive test performance in regression analysis20. In this sense, the evidence suggests that impaired motor skills may be related to cognitive impairment. Sternäng et al.34 examined the relationship between grip strength and cognitive performance by assessing 708 participants over 20 years. The authors used instruments that assessed verbal skills, spatial abilities, processing speed and memory34. The results evidenced an association between decreased grip strength and decreased performance in all cognitive tests34. The evidence presented here along with the results found in our study reaffirm that motor and cognitive abilities share common mechanisms. Thus, new studies should explore these variables more specifically.
The present study has some limitations. Firstly, more instruments assessing the memory domain were used, and this choice may have contributed to the obtained results since more specific tests to assess other domains, mainly functions related to the frontal lobe, may be essential to detect differences between the groups. Secondly, other potential confounders such as alcohol use and smoking were not considered in the analyzes and individuals with dementia, Parkinson’s disease, or severe depression were not excluded from the final sample. Lastly, the cross-sectional study does not allow to establish causal relationships between the frailty syndrome and decline in the cognitive domains evaluated, which would be possible in longitudinal designs.
Conclusion
The prevalence of frailty syndrome is a phenomenon that deserves attention from health professionals and researchers. In this study, we found a large number of elderly individuals classified as frail according to their self-perception. Moreover, we found an association between frailty and poor global cognitive performance, memory, learning, and language. New prospective studies are fundamental to evaluate the relation between frailty and cognitive functioning in specific domains, especially those related to the frontal lobe.
Acknowledgment
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (Capes) – Finance Code 001; and by the Brazilian fostering agency Fapesp (grant #: 2015/16412-1). Daiene de Morais is a recipient of a scholarship from the National Council for Scientific and Technological Development/CNPq, Brazil (grant: # 132257/2017-3).
Disclosure
We have no conflict of interest to declare.
References
1. Wang C, Ji X, Wu X, Tang Z, Zhang X, Guan S, et al. Frailty in rela-tion to the risk of Alzheimer’s disease, dementia, and death in older Chinese adults: A seven-year prospective study. J Nutr Health Aging. 2017;21(6):648-54.

155Fabrício DM et al. / Arch Clin Psychiatry. 2019;46(6):151-5
2. Ng TP, Ling LHA, Feng L, Nyunt MSZ, Feng L, Niti M, et al. Cognitive effects of multi-domain interventions among pre-frail and frail commu-nity-living older persons: randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2018;73(6):806-12.
3. Panza F, Seripa D, Solfrizzi V, Tortelli R, Greco A, Pilotto A, et al. Targe-ting cognitive frailty: clinical and neurobiological roadmap for a single complex phenotype. J Alzheimers Dis. 2015;47(4):793-813.
4. Sternberg SA, Schwartz AW, Karunananthan S, Bergman H, Mark Clar-field A. The identification of frailty: a systematic literature review. J Am Geriatr Soc. 2011;59(11):2129-38.
5. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al.; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146-57.
6. Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood K. Validity and reliability of the Edmonton Frail Scale. Age Ageing. 2006;35(5):526-9.
7. Halil M, Kizilarslanoglu MC, Kuyumcu ME, Yesil Y, Jentoft AC. Cogni-tive aspects of frailty: mechanisms behind the link between frailty and cognitive impairment. J Nutr Health Aging. 2015;19(3):276-83.
8. Song X, Mitnitski A, Rockwood K. Age-related deficit accumulation and the risk of late-life dementia. Alzheimers Res Ther. 2014;6(5-8):54.
9. Searle SD, Rockwood K. Frailty and the risk of cognitive impairment. Alzheimers Res Ther. 2015;7(1):54.
10. Neri AL, Yassuda MS, Araújo LFD, Eulálio MDC, Cabral BE, Siqueira MECD, et al. Metodologia e perfil sociodemográfico, cognitivo e de fragilidade de idosos comunitários de sete cidades brasileiras: Estudo FIBRA. Cad Saúde Pública. 2013;29(4):778-92.
11. Kelaiditi E, Cesari M, Canevelli M, Van Kan GA, Ousset PJ, Gillette--Guyonnet S, et al.; IANA/IAGG. Cognitive frailty: rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J Nutr Health Aging. 2013;17(9):726-34.
12. Butler A, Gallagher D, Gillespie P, Crosby L, Ryan D, Lacey L, et al. Frailty: a costly phenomenon in caring for elders with cognitive impairment. Int J Geriatr Psychiatry. 2016;31(2):161-8.
13. Canevelli M, Cesari M, Vankan GA. Frailty and cognitive decline: how do they relate? Curr Opin Clin Nutr Metab Care. 2015;18(1):43-50.
14. Macuco CRM, Batistoni SST, Lopes A, Cachioni M, da Silva Falcão DV, Neri AL, et al. Mini-Mental State Examination performance in frail, pre-frail, and non-frail community dwelling older adults in Ermelino Matarazzo, São Paulo, Brazil. Int Psychogeriatrics. 2012;24(11):1725-31.
15. Langlois F, Vu TTM, Kergoat MJ, Chassé K, Dupuis G, Bherer L. The multiple dimensions of frailty: physical capacity, cognition, and quality of life. Int Psychogeriatrics. 2012;24(9):1429-36.
16. Boyle PA, Buchman AS, Wilson RS, Leurgans SE, Bennett DA. Physical frailty is associated with incident mild cognitive impairment in commu-nity‐based older persons. J Am Getriatr Soc. 2010;58(2):248-55.
17. O’Halloran AM, Finucane C, Savva GM, Robertson IH, Kenny RA. Sustained attention and frailty in the older adult population. J Gerontol B Psychol Sci Soc Sci. 2013;69(2):147-56.
18. Han ES, Lee Y, Kim J. Association of cognitive impairment with frailty in community-dwelling older adults. Int Psychogeriatrics. 2014;26(1):155-63.
19. Chen S, Honda T, Narazaki K, Chen T, Nofuji Y, Kumagai S. Global cognitive performance and frailty in non‐demented community‐dwelling older adults: findings from the Sasaguri Genkimon Study. Geriatr Ge-rontol Int. 2016;16(6):729-36.
20. Yassuda MS, Lopes A, Cachioni M, Falcao DVS, Batistoni SST, Guimaraes VV, et al. Frailty criteria and cognitive performance are related: Data from the FIBRA study in Ermelino Matarazzo, São Paulo, Brazil. J Nutr Health Aging. 2012;16(1):55-61.
21. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo 2010. Disponível em: https://censo2010.ibge.gov.br/sinopse/index.php?dados=26&uf=35#topo_piramide. Acesso em: 3 maio 2018.
22. Nunes DP, Duarte YADO, Santos JLF, Lebrão ML. Screening for frailty in older adults using a self-reported instrument. Rev Saúde Pública. 2015;49(2).
23. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-98.
24. Bertolucci PHF, Okamoto IH, Brucki SMD, Siviero MO, Toniolo Neto J, Ramos LR. Applicability of the CERAD neuropsychological battery to Brazilian elderly. Arq Neuro-psiquiatr. 2001;59(3):532-6.
25. Nitrini R, Caramelli P, Herrera E, Porto CS, Charchat-Fichman H, Carthery MT, et al. Performance of illiterate and literate nondemented elderly subjects in two tests of long-term memory. J Int Neuropsychol Soc. 2004;10(4):634-8.
26. Roth M, Tym E, Mountjoy CQ, Huppert FA, Hendrie H, Verma S, et al. CAMDEX: a standardised instrument for the diagnosis of mental disorder in the elderly with special reference to the early detection of dementia. Br J Psychiatry. 1986;149(6):698-709.
27. Roth MTYME, Tym E, Mountjoy CQ, Huppert FA, Hendrie H, Verma S, Goddard R. A compendium of neuropsychological tests: administration, norms, and commentary. American Chemical Society; 2006.
28. Ge L, Yap CW, Heng BH. Prevalence of frailty and its association with depressive symptoms among older adults in Singapore. Aging Ment Health. 2019;23(3):319-24.
29. Nóbrega PVDN, Maciel ÁCC, De Almeida Holanda CM, Oliveira Guerra R, Araújo JF. Sleep and frailty syndrome in elderly residents of long‐stay institutions: a cross‐sectional study. Geriatr Gerontol Int. 2014;14(3):605-12.
30. Franse CB, Van Grieken A, Qin, L, Melis RJ, Rietjens JA, Raat H. Socioeconomic inequalities in frailty and frailty components among community-dwelling older citizens. PloS One. 2017;12(11):e0187946.
31. Robertson DA, Savva GM, Kenny RA. Frailty and cognitive impairment – a review of the evidence and causal mechanisms. Ageing Res Rev. 2013;12(4):840-51.
32. Buchman AS, Schneider JA, Leurgans S, Bennett DA. Physical frailty in older persons is associated with Alzheimer disease pathology. Neurology. 2008;71(7):499-504.
33. Bunce D, Batterham PJ, Mackinnon AJ. Long-term associations between physical frailty and performance in specific cognitive domains. J Gerontol B Psychol Sci Soc Sci. 2019;74(6):919-26.
34. Sternäng O, Reynolds CA, Finkel D, Ernsth-Bravell M, Pedersen NL, Dahl Aslan AK. Grip strength and cognitive abilities: associations in old age. J Gerontol B Psychol Sci Soc Sci. 2016;71(5):841-8.

Original article
Address for correspondence: Onur Yilmaz. Bezmialem Foundation University Medical Faculty Department of Psychiatry, Adnan Menderes Boulevard (Vatan Road) Fatih/Istanbul. Postal Code: 34093. Phone: +90 533 658 0934, Office Phone: +90 212 253 1818. Fax Number: +90 212 253 1883. E-mail: [email protected]. Alternate e-mail: [email protected]
Does psychotherapy improve alexithymia? A comparison study among patients with mild or moderate depressionoNuR yilMaz1https://orcid.org/0000-0002-8270-7354
ali BaRlas MiRçik1https://orcid.org/0000-0001-8192-9249
MeRve kuNduz1https://orcid.org/0000-0003-4161-4773
Müge çoMBaş1https://orcid.org/0000-0003-1536-0458
aHMet ÖztüRk1https://orcid.org/0000-0002-9854-7586
eRdeM deveci1https://orcid.org/0000-0002-9661-8344
isMet kiRpiNaR1https://orcid.org/0000-0001-9816-3438
1 Bezmialem Foundation University Medical Faculty, Department of Psychiatry, Istanbul, Turkey.
Institution where the study was conducted: Bezmialem Foundation University Medical Faculty, Department of Psychiatry, Istanbul, Turkey.
Received: 02/10/2019 – Accepted: 09/04/2019DOI: 10.1590/0101-60830000000217
Abstract Background: Alexithymia is reported to be a risk factor for depression. Psychotherapy is efficient for treatment of depression. Yet, the effect of psychotherapies on alexithymia is poorly understood. Objectives: We aimed to compare Cognitive Behavioral Therapy (CBT), Existential Psychotherapy (ExP) and Supportive Counseling (SUP) for therapeutic efficacy and effect on alexithymia in depression. Methods: There were 22 patients for each patient group. Sessions were performed as eight consecutive weekly and following two monthly boosters. Sixty six healthy controls were added. Prior to the sessions, patients received Sociodemographic Data Form, the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-1), Hamilton Depression Rating Scale (HDRS) and 20-item Toronto Alexithymia Scale (TAS-20). The control group received Sociodemographic Data Form, SCID-1 and TAS-20. Patients additionally received HDRS and TAS-20 after their weekly and booster sessions. Results: Patients’ mean TAS-20 score was greater than of controls, however, it did not have a significant change throughout the study. Mean HDRS scores of ExP and CBT groups were lower than SUP group at the end. Discussion: Alexithymia did not improve with psychotherapy. The exception was effect of ExP on externally oriented thinking. Psychotherapies all improved depression. CBT and ExP were more helpful than SUP.
Yilmaz O et al. / Arch Clin Psychiatry. 2019;46(6):156-64
Keywords: Alexithymia, cognitive behavioral therapy, depression, existential psychotherapy, supportive counselling.
Introduction
The word alexithymia was suggested by Sifneos, from the Greek (a = lack, lexis = work, thymos = mood or emotion)1. Alexithymic individuals have difficulty in recognizing their emotions, expressing them and manifesting them by linking emotions and thoughts. People with alexithymia were reported to prominently be unable to benefit from social support because of their cognitive deficits of emotion2. In furtherance, alexithymia was reported to be connected to MDD3. Alexithymia is not only seen in MDD or other psychiatric disorders, but also in psychosomatic disorders4 and systemic disorders like hypertension5. It should be noticed that, alexithymic signs are not absolutely pathological. They may also be seen in general population to some extent6,7. Various research reported the prevalence of alexithymia (TAS-20 total score ≥ 61) to be between 12 and 18%, besides, results about gender differences were contradictory8,9.
Depression is the most frequent type of mood disorders. It may cause significant burden of life and mortality10. Major depressive disorder (MDD) is estimated to reach the second rank among causes of disability by the year 202011.
Cognitive behavioral therapy (CBT) is one of the widely and successfully used psychotherapy models for MDD. CBT is
developed and put into practice firstly by Beck et al.12. As time goes by, retrospective studies and reviews about CBT for depression have been added to literature13,14. Several trials reported enduring effects of CBT delivered during acute phase of MDD, which was unlikely with antidepressants (AD)15. While traditional CBT is not beneficial enough in some cases, relatively new approaches on the field, called third wave CBT, have come to the scene. Several third wave CBT methods have been declared and empirically supported to be helpful for particular forms of depression16. The terms acceptance and mindfulness, which are closely related to existential phylosophy, are widely used among third wave CBT literature and practice17,18.
Existential philosopy focuses mainly on meaning of life, freedom, authenticity and responsibility19-22. Existential Psychotherapy (ExP)* is based on existential philosophy. That is to say, a psychotherapy model is called existential therapy only if it is based on phylosophy, rather than psychologic theories. The interview between the therapist and the patient in an existential psychotherapy session is based on
* There are no declared generic names or abbreviations for existential psychotherapies as a whole. Therefore, we named an abbreviation on our own behalf.

157Yilmaz O et al. / Arch Clin Psychiatry. 2019;46(6):156-64
the method called phenomenology23. Phenomenologic dialogue is a kind of invitation to the individual to let happenings and things to demonstrate themselves just like what actually they are24. Existential philosophy has an ancient course. Australian psychiatrist and psychotherapist Viktor Emile Frankl is generally accepted to be the first therapist who performed his work on the basis of existential philosophy. While it is roughly accepted that each existential therapist has his/her own way of performing ExP, Frankl’s approach on existential psychotherapy has a particular name, logotherapy (LT)25. LT is generally understood as “meaning therapy” and has been practiced by a large number of psychotherapists. There are also many other schools of existential psychotherapy, some of which are entitled as Dasein Analysis26, Existential Group Therapy27 and Existential Couple Therapy28. However, LT or other ExP echoles did not take part in guidelines for depression treatment yet.
A group of researchers performed unstructured forms of psychotherapy which does not help through specific psychological techniques. These nondirective therapies are commonly described in the literature as either counselling or supportive therapy. Though less effective than other therapies, nondirective supportive therapies were reported to be helpful for depressed patients29,30.
Given alexithymia is a potent risk factor for MDD and various psychotherapy echoles are proven to improve MDD significantly, we investigated effects of psychotherapies on alexithymia among MDD patients. We also compared the therapeutic effects of CBT, ExP and SUP against MDD. To the best of our knowledge, no previous study comparing CBT and ExP for treatment of MDD was performed.
Methods
Our study was performed at Bezmialem Foundation University Psychiatry Clinics. The study protocol was approved by Bezmialem Foundation University Ethics Committee for Interventional Studies (approval date: 07.02.2017; approval number: 3/21).
Subjects
One hundred two patients in total, who were diagnosed with mild or moderate MDD were selected throughout the study. Sixty-six patients (64,7%) completed the whole protocol. The control group consisted of 66 healthy volunteers, matched with the patient group for age, education and gender. All subjects were selected from individuals aged between 18 and 65 years. Patients who had comorbid psychiatric disorders such as obsessive compulsive disorder (OCD), severe personality disorders, post traumatic stress disorder (PTSD), substance-related and addictive disorders; patients who have bipolar affective disorder (BPD) and patients who had been on psychiatric medication from two months before the evaluation date for the study were not included. Individuals hard to communicate, such as patients with dementia, blindness and deafness were not included either.
Seventy-three individuals were selected for healthy control group throughout the process. Seven out of them were excluded, due to axis-1 psychiatric disorders, identified by performing The Structured Clinical Interwiev for DSM-IV TR Axis-1 Disorders (SCID-I) and psychiatric examination. Employees working at Bezmialem Foundation University Hospital were not included, for avoiding an unfavorable situation concerning ethics. After making necessary explanations about the study, subjects who agreed to participate, have signed voluntary informed consent forms.
Among 66 patients who completed the whole study protocol, 22 (33,3%) got CBT, 22 (33,3%) got ExP and the rest 22 (33,3%) got SUP for eight consecutive weekly sessions and the following two monthly booster sessions. Selection of patients and therapy models were made by two separate psychiatrists who were not on the therapist list. The selection model was randomisation, in which the subjects were directed to groups one by one, in order of CBT, ExP and SUP, till the number of subjects completed the study reached to the amount targetted. When necessary number was fulfilled, psychiatrists who select cases were informed by the therapists, in order not to direct any more patients.
Duration of sessions were 45 to 50 minutes. Ten patients selected for CBT (31,2%), 12 selected for ExP (35,3%) and 14 selected for SUP (38,9%) did not complete the whole study. Three patients selected for CBT, four for ExP and five for SUP did not start sessions. Thus, 66 out of 90 starters (73,3%) finished the trial. Two patients in CBT group, three in ExP group and two in SUP group did not continue after their first sessions. Throughout weekly sessions, one patient in CBT group, two in ExP group and one in SUP group were excluded from the study and directed to psychiatry clinics back, because of worsening of the symptoms to the extent that the diagnosis differed to severe MDD and they were supposed to be on psychiatric medication. Two patients in CBT group, two in ExP group and four in SUP group left the study from second to seventh of weekly sessions. Two patients in CBT group, one in ExP group and two in SUP group completed the weekly sessions, however, did not come for booster sessions.
Prior to the therapy sessions, patients received Sociodemographic Data Form prepared for the study, SCID-I, 20 item Toronto Alexithymia Scale (TAS-20) and Hamilton Depression Rating Scale (HDRS). The control group received Sociodemographic Data Form, SCID-I and TAS-20. Each patient received TAS-20 and HDRS twice more, former after weekly sessions and the latter after booster sessions.
The Structured Clinical Interview for DSM-IV Axis 1 Disorders (SCID-I): It is a form for psychiatric interview for axis-1 disorders identified in DSM-IV, structured by First et al.31. Adaptation to Turkish and reliability analysis of Turkish form were performed by Özkürkçügil et al.32.
Hamilton Depression Rating Scale (HDRS): Developed originally by Hamilton for measurement of severity of depressive symptoms33, the structured form was developed by Williams34. The validity and reliability study of Turkish form was performed by Akdemir et al.35.
20-Item Toronto Alexithymia Scale (TAS-20): It is a Likert type self report scale. Each item is scored between 1 and 5. Some items are scored in reverse order. There are three subscales as follows: Difficulty in Identifying Feelings (TAS-1), Difficulty in Describing Feelings (TAS-2) and Externally Oriented Thinking (TAS-3). It is considered that, as the scale total score gets higher, level of alexithymia gets higher. The scale was developed by Bagby et al.36. Turkish adaptation study was performed by Güleç et al.37. Scale total scores are categorized according to the cutoff points such that, a total score of ≥ 61 points indicates alexithymia, and ≤ 51 points indicates no alexithymia.
Therapists and sessions
Before study beginned, flowcharts for CBT and ExP were prepared (Figures 1 and 2). As it should be, there was no flowchart for SUP. First booster sessions were performed four weeks after weekly sessions have been completed. Second booster sessions were performed four weeks after the first booster.
Two therapists performed traditional CBT, two therapists performed ExP and one clinical psychologist, performed SUP. One of our CBT therapists, aged 63, was certified by Turkish Association for Cognitive and Behavioral Therapy (Istanbul, Turkey) and by Academy of Cognitive Therapy (Philadelphia, United States). Other CBT therapist, aged 25, was certified by Turkish Association of Psychiatry (Ankara, Turkey). ExP therapists, aged 40 and 31, were both certified by Existential Academy of Istanbul, which is affiliated to Viktor Franl Institute of Logotherapy (Dallas, Texas). Our SUP therapist, while SUP is not entirely considered to be a professional psychotherapeutic approach, was not specified on any psychotherapy echoles, however, she was a clinical psychologist. The durations of experience as psychotherapists and the number of patients with whom they performed and completed therapy sessions were as follows: 2 years (10 patients) and 6 years (12 patients) for CBT therapists, 2 years (9 patients) and 5 years (13 patients) for ExP therapists and 5 years (22 patients all) for SUP therapist. In this way, we intended to minimize the possible inequality regarding the therapy offered to patients and provide the utmost uniformity.

158 Yilmaz O et al. / Arch Clin Psychiatry. 2019;46(6):156-64
Figure 1. Flowchart for CBT sessions
Session number
Content of session in brief
W1 Noting current complaints,Getting brief knowledge about patient’s history of disorder, pharmacotherapy and psychotherapy (if any),Showing some cognitive contradictions, Setting appropriate and available targets,Proposing treatment rationale for the agenda.
W2 Discussing available cognitive contradictions and showing some more,Mentioning the term “automatic thoughts” and deriving them from existing contradictions,Demonstrating possible initiating, triggering and maintaininig factors,Setting homework(s).
W3 Evaluation of homework(s),Exploring more automatic thoughts and evaluating alternative thoughts against them,Elaborating triggering and maintaining factors,Setting new homework(s).
W4 Evaluation of homework(s),Testing certain automatic thoughts and elaborating more,Evaluating alternative thoughts,Retracing triggering and maintaining factors, Setting new homework(s).
W5 Evaluation of homework(s),Testing and evaluating more (new, if explored any) automatic thoughts,Elaborating and retracing initiating factors,Mentioning the term “intermediary beliefs” and deriving some of them from outcomes until then,Setting new homework(s).
W6 Evaluation of homework(s),Elaborating and testing intermediary beliefs,Evaluating original and current targets,Setting new homework(s).
W7 Evaluation of homework(s),Testing more (new, if explored any) intermediary beliefs,Retracing initiating factors,Setting new homework(s).
W8 Evaluation of homework(s),Overall assessment of alternative automatic thoughts and intermediary beliefs,Overall assessment of original and current targets,Setting new (monthly) homework(s).
B1 Evaluation of homework(s),Overall assessment of alternative automatic thoughts and intermediary beliefs,*Mentioning the term “core beliefs” and deriving some from intermediary beliefs (if needed),Overall assessment of original and current targets,Setting new (monthly) homework(s).
B2 Overall assessment of alternative automatic thoughts and intermediary beliefs (and core beliefs if needed),Overall assessment of original and current targets,Evaluating how to use new skills in case of relapse and recurrence.
Notes: Despite following this flowchart, sessions were flexible to some extent, according to patients’ needs and circumstances. Hamilton Depression Rating Scale and 20-item Toronto Alexithymia Scale were repeated after W8 and B2. *Core beliefs are not usually needed to be explored for mild and moderate depression. Abbreviations: CBT: cognitive behavioral therapy; W: weekly session; B: booster session.
Figure 2. Flowchart for ExP sessions
Session number
Content of session in brief
W1 Noting current complaints,Getting brief knowledge about patient’s history of disorder, pharmacotherapy and psychotherapy (if any),Introducing basic route for ExP and assessing suitability of patient.
W2 Letting the patient give more details of complaints,Trying to cover how authentic is patient’s life and which obstacles are working against authenticity,Trying to cover which aspects of patient’s life are already close to authenticity.
W3 Structuring the therapeutic dialogue on phenomenologic basis, Exploring intangible statements and directing the patient to embody his/her speech,Demonstrating how apart the patient is from or how close to authenticity in certain fields.
W4 Improving the phenomenologic dialogue,Improving embodiment of patient’s statements,Assessment for patient’s stance toward self-relatedness,Directing the patient to express him/herself including physical, relational and spiritual fields of living.
W5 Improving the phenomenologic dialogue,Exploring curbs resulting from avoiding embodiment,Exploring the patient’s stance toward responsibility and choices of life.
W6 Improving the phenomenologic dialogue Trying to receive feedbacks concerning patient’s certain patterns interfering with functionality,Exploring curbs resulting from avoiding responsibility,Directing the patient to negotiate about taking the responsibility of his/her choices.
W7 Improving the phenomenologic dialogue, Inviting the patient to give feedbacks about his/her patterns interfering with functionality,Exploring curbs resulting from avoiding responsibility and freedom,Directing the patient to negotiate about taking the responsibility of predictible and unpredictible outcomes of his/her choices.
W8 Improving the phenomenologic dialogue, Inviting the patient to give feedbacks about his/her feelings about the sessions and the therapist,Exploring strengths of the patients that might have been gained through enhanced sense of responsibility,Inviting the patient to negotiate about his/her fears concerning freedom.
B1 Evaluation of experiences until session date,Overall assessment of the patient’s stance toward responsibility, authenticity and freedom,Overall assessment of patient’s stance toward desirable and undesirable experiences,Directing the patient to talk about his/her experiences with minimized labels and habitual attitudes.
B2 Evaluation of experiences until session date,Overall assessment of the patient’s stance toward responsibility, authenticity and freedom,Overall assessment of patient’s stance toward his/her will to look for living a meaningful life,Assessment of patient’s approach about habitual reactions and labeling his/her experiences,Evaluating how to use new skills in case of relapse and recurrence.
Notes: Despite following this flowchart, sessions were flexible to some extent, according to patients’ needs and circumstances. Hamilton Depression Rating Scale and 20-item Toronto Alexithymia Scale were repeated after W8 and B2. Abbreviations: ExP: existential psychotherapy; W: weekly session; B: booster session.

159Yilmaz O et al. / Arch Clin Psychiatry. 2019;46(6):156-64
Statistics
While response to the therapy was measured via changes in HDRS and TAS-20 scores, when power analysis was assessed with power value of 0,80 and significance level of 0,05, a minimum of 16 patients were required for each of three groups. We eventually decided for 22 subjects in each group.
Statistical evaluation of data was done with IBM SPSS Statistics 24 package program. All numerical variables were expressed as either mean ranks or mean ± standard deviation, while categorical variables were expressed with frequency and possibility tables.
Given more than two independent groups and relatively limited number of subjects (<30) in each group, Kruskal-Wallis was used for comparison of numerical and Chi-Square was used for categorical variables. When a significant difference between groups was detected with Kruskal-Wallis, each group were paired with another and compared with Mann-Whitney U test. Comparisons of groups in themselves were made by Wilcoxon Signed Rank Test. Probability value (p) was taken as <0.05 for statistical significance in all statistical analyses.
Results
All three patient groups and control group were matched in terms of age, gender, marital status and education (Table 1). At the end of the study, mean rank of HDRS scores demonstrated significant differences between patient groups (p < 0,05) (Table 2). When the groups were compared in pairs, there was a significant difference between ExP-SUP and CBT-SUP. Thus, HDRS scores were significantly lower than SUP group both in CBT and ExP groups. However, the difference between ExP and CBT groups was not significant (Table 3). When each group is compared in itself with Wilcoxon Signed Rank Test, all patient groups had lower mean scores of HDRS at the end of booster
sessions than mean scores at the beginning, while none of the groups’ mean HDRS scores changed significantly between the end of weekly sessions and booster sessions (Table 4). Changes in HDRS scores did not differ significantly between therapists in ExP and CBT groups.
While a total score of ≥ 61 indicates the presence of alexithymia, the number of alexithymic subjects before the sessions start were 2 (9.1%), 1 (4.5%) and 3 (13.6%) for ExP, CBT and SUP respectively. Thus, the total number of alexithymic individuals among patient group was 6 (9.1%). On the other side, two control subjects (3.0%) were alexithymic. Despite the clear difference between percentages of alexithymic individuals between patient and control groups, the numbers were not adequate to perform statistical analysis for comparement. For this reason, we decided to compare the groups with regard to TAS-20 total and subscale scores. Patients’ mean TAS-20 total, TAS-1 and TAS-3 scores were greater than of controls at the beginning (p < 0,05), while the difference in mean TAS-2 score was not significant (Table 5). TAS-20 scores of any patient groups did not differ significantly after weekly or booster sessions. Subsequently, comparement of all patient groups in pairs demonstrated that, significant difference of TAS-20 total or subscale scores were neither present at the end of weekly, nor at the end of booster sessions (Table 6). Besides, each group were assessed in terms of alteration of mean TAS-20 scores from the beginning of study to the end. Mean TAS-20 scores of SUP and CBT groups were shown to remain unchanged at the end of weekly and booster sessions. ExP group also did not have significant alteration of TAS-total and subscales, except for TAS-3 (Table 7). Mean TAS-3 scores among ExP group did not show any significant change after weekly sessions, though, change was visible between weekly and booster sessions (Table 7).
We performed Pearson Correlation Test for detection of possible correlation of alexithymia and the response to treatment (Table 8).
Table 1. Comparison of sociodemographic data of patient and control groupsExP (N = 22) CBT (N = 22) SUP (N = 22) Controls (N = 66) p
Age 32.2 ± 12.5 31.6 ± 10.5 32.2 ± 11.5 36.2 ± 10.9 0.164GenderFemale 18 (81.8%) 9 (86,4%) 18 (81.8%) 54 (81.8%) 0.967Marital statusMarriedSingleDivorced, widow, seperated
8 (36,4%)12 (54,5%)2 (9,1%)
6 (27,3%)14 (63,6%)2 (9,1%)
10 (45.5%)11 (50.0%)1 (4.5%)
18 (27.3%)41 (62.1%)7(10.6%)
0.779
EducationLiterateElementaryHigh schoolAssociate licence, licencePost-graduate, doctorate
1 (4.5%)3 (13,6%)6 (27.3%)10 (45.5%)2 (9.1%)
1 (4,5%)3 (13,6%)5 (22,7%)11 (50,0%)2 (9,1%)
1 (4.5%)3 (13.6%)7 (31.8%)9 (40.9%)2 (9.1%)
2 (3.0%)16 (24.2%)17 (25.8%)21 (31.8%)10 (15.2%)
0.945
Notes: Kruskal-Wallis was used for comparison of numerical data and chi-square test was used for comparison of categorical variables. Ages of groups are expressed as mean ± standard deviation. Other values are expressed as percentiles. Abbreviations: N: number of subjects; p: probability value; ExP: existential psychotherapy group; CBT: cognitive behavioral therapy group; SUP: supportive counselling group.
Table 2. Comparison of mean HDRS ranks between patient groupsExP (N = 22) CBT (N = 22) SUP (N = 22) p
Bgn 34.36 35.59 30.55 0.659Awk 29.41 28.95 42.14 0.035*ABst 29.89 26.11 44.50 < 0.01*
Notes: Kruskal-Wallis was used for comparison of numerical data; *Significant difference between groups. Abbreviations: N: number of subjects; p: probability value; ExP: existential psychotherapy group; CBT: cognitive behavioral therapy group; SUP: supportive counselling group; Bgn: mean rank for HDRS scores before the start of sessions; Awk: mean rank for HDRS scores after weekly sessions; ABst: mean rank for HDRS scores after booster sessions.

160 Yilmaz O et al. / Arch Clin Psychiatry. 2019;46(6):156-64
Table 3. Paired comparisons of mean HDRS ranks of each patient groupExP vs SUP CBT vs SUP ExP vs CBT
m p m p m pBgn 23.82 vs 21.18 0.494 24.14 vs 20.86 0.396 22.05 vs 22.95 0.813Awk 18.25 vs 26.75 0.028* 18.11 vs 26.89 < 0.023* 22.66 vs 22.34 0.934ABst 17.43 vs 27.57 < 0.01* 16.57 vs 28.43 < 0.01* 23.95 vs 21.05 0.450
Notes: Mann-Whitney U was used for comparison of numerical data. *Significant difference between groups. Abbreviations: p: probability value; ExP: existential psychotherapy group; CBT: cognitive behavioral therapy group; SUP: supportive counselling group; vs: versus; Bgn: mean values before the start of sessions; Awk: mean values after weekly sessions; ABst: mean values after booster sessions; m: mean rank.
Table 4. Comparisons of mean HDRS scores for all treatment groups in themselvesExP (N = 22) CBT (N = 22) SUP (N = 22)
mean p mean p mean pBgn vs ABst (18.1 ± 3.6) vs (10.1 ± 3.4) < 0.01* (18.4 ± 3.2) vs (9.2 ± 3.9) < 0.01* (17.3 ± 4.0) vs (13.1 ± 3.7) < 0.01*Bgn vs Awk (18.1 ± 3.6) vs (10.9 ± 4.6) < 0.01* (18.4 ± 3.2) vs (10.9 ± 5.0) 0.01* (17.3 ± 4.0) vs (14.3 ± 4.9) < 0.01*Awk vs ABst (10.9 ± 4.6) vs (10.1 ± 3.4) 0.526 (10.9 ± 5.0) vs (9.2 ± 3.9) 0.232 (14.3 ± 4.9) vs (13.1 ± 3.7) 0.253
Notes: Wilcoxon Signed Rank Test was used for comparison of numerical data. HDRS scores are expressed as mean ± standard deviation. *Significant difference. Abbreviations: N: number of subjects; p: probability value; ExP: existential psychotherapy group; CBT: cognitive behavioral therapy group; SUP: supportive counselling group; vs: versus; Bgn: mean values before the start of sessions; Awk: mean values after weekly sessions; ABst: mean values after booster sessions.
Table 5. Comparison of mean ranks of TAS-20 total and subscale scores between all groupsExP (N = 22) CBT (N = 22) SUP (N = 22) Control (N = 66) p
TAS-20 totalBgn 84.73 80.91 83.84 49.84 < 0.01*Awk 32.36 31.41 36.73 0.618ABst 30.95 31.57 37.98 0.404TAS-1Bgn 88.59 75.89 86.98 49.18 < 0.01*Awk 34.80 28.75 36.95 0.336ABst 35.23 28.66 36.61 0.336TAS-2Bgn 76.59 79.20 69.18 58.01 0.060Awk 32.55 35.68 32.27 0.803ABst 32.52 34.77 33.20 0.922TAS-3Bgn 78.23 77.30 78.80 54.89 < 0.01*Awk 31.36 32.95 36.18 0.696ABst 29.57 33.80 37.14 0.421
Notes: Kruskal-Wallis was used for comparison of numerical data. *Significant difference between groups. Abbreviations: N: number of subjects; p: probability value; ExP: existential psychotherapy group; CBT: cognitive behavioral therapy group; SUP: supportive counselling group; TAS-20: 20-item Toronto Alexithymia Scale; TAS-1: Difficulty in Identifying Feelings subscale; TAS-2: Difficulty in Describing Feelings subscale; TAS-3: Externally Oriented Thinking subscale; Bgn: mean ranks before sessions start; Awk: mean ranks after weekly sessions; ABst: mean ranks after booster sessions.
Table 6. Paired comparisons of mean ranks of TAS-20 total and subscale scores after weekly and booster sessions between patient groupsExP vs SUP CBT vs SUP ExP vs CBT
m p m p m pTAS-20 totalAwk 20.77 vs 24.23 0.371 21.00 vs 24.00 0.438 23.09 vs 21.91 0.760ABst 19.95 vs 25.05 0.188 20.57 vs 24.43 0.318 22.50 vs 22.50 1.000TAS-1Awk 21.80 vs 23.20 0.714 19.75 vs 25.25 0.153 24.50 vs 20.50 0.299ABst 21.86 vs 23.14 0.741 20.02 vs 24.98 0.198 24.86 vs 20.14 0.218TAS-2Awk 22.59 vs 22.41 0.962 23.64 vs 21.36 0.553 21.45 vs 23.55 0.585ABst 22.14 vs 22.86 0.850 23.16 vs 21.84 0.731 21.89 vs 23.11 0.749TAS-3Awk 21.07 vs 23.93 0.459 21.25 vs 23.75 0.517 21.80 vs 23.20 0.744Abst 20.30 vs 24.70 0.254 21.07 vs 23.93 0.457 20.77 vs 24.23 0.370
Notes: Mann-Whitney U was used for comparison of numerical data. *Significant difference between groups. Abbreviations: p: probability value; m: mean rank; ExP: existential psychotherapy group; CBT: cognitive behavioral therapy group; SUP: supportive counselling group; TAS-20: 20-item Toronto Alexithymia Scale; TAS-1: Difficulty in Identifying Feelings subscale; TAS-2: Difficulty in Describing Feelings subscale; TAS-3: Externally Oriented Thinking subscale; Bgn: mean ranks before sessions start; Awk: mean ranks after weekly sessions; ABst: mean ranks after booster sessions.
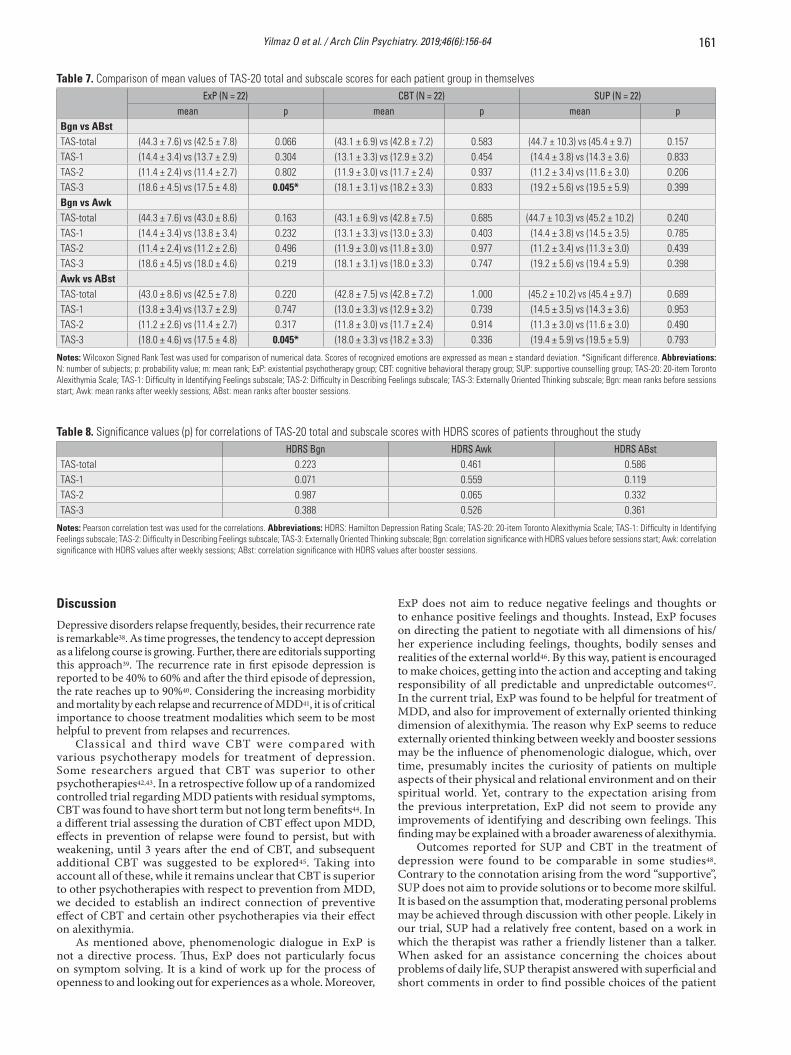
161Yilmaz O et al. / Arch Clin Psychiatry. 2019;46(6):156-64
Table 7. Comparison of mean values of TAS-20 total and subscale scores for each patient group in themselvesExP (N = 22) CBT (N = 22) SUP (N = 22)
mean p mean p mean pBgn vs ABstTAS-total (44.3 ± 7.6) vs (42.5 ± 7.8) 0.066 (43.1 ± 6.9) vs (42.8 ± 7.2) 0.583 (44.7 ± 10.3) vs (45.4 ± 9.7) 0.157TAS-1 (14.4 ± 3.4) vs (13.7 ± 2.9) 0.304 (13.1 ± 3.3) vs (12.9 ± 3.2) 0.454 (14.4 ± 3.8) vs (14.3 ± 3.6) 0.833TAS-2 (11.4 ± 2.4) vs (11.4 ± 2.7) 0.802 (11.9 ± 3.0) vs (11.7 ± 2.4) 0.937 (11.2 ± 3.4) vs (11.6 ± 3.0) 0.206TAS-3 (18.6 ± 4.5) vs (17.5 ± 4.8) 0.045* (18.1 ± 3.1) vs (18.2 ± 3.3) 0.833 (19.2 ± 5.6) vs (19.5 ± 5.9) 0.399Bgn vs AwkTAS-total (44.3 ± 7.6) vs (43.0 ± 8.6) 0.163 (43.1 ± 6.9) vs (42.8 ± 7.5) 0.685 (44.7 ± 10.3) vs (45.2 ± 10.2) 0.240TAS-1 (14.4 ± 3.4) vs (13.8 ± 3.4) 0.232 (13.1 ± 3.3) vs (13.0 ± 3.3) 0.403 (14.4 ± 3.8) vs (14.5 ± 3.5) 0.785TAS-2 (11.4 ± 2.4) vs (11.2 ± 2.6) 0.496 (11.9 ± 3.0) vs (11.8 ± 3.0) 0.977 (11.2 ± 3.4) vs (11.3 ± 3.0) 0.439TAS-3 (18.6 ± 4.5) vs (18.0 ± 4.6) 0.219 (18.1 ± 3.1) vs (18.0 ± 3.3) 0.747 (19.2 ± 5.6) vs (19.4 ± 5.9) 0.398Awk vs ABstTAS-total (43.0 ± 8.6) vs (42.5 ± 7.8) 0.220 (42.8 ± 7.5) vs (42.8 ± 7.2) 1.000 (45.2 ± 10.2) vs (45.4 ± 9.7) 0.689TAS-1 (13.8 ± 3.4) vs (13.7 ± 2.9) 0.747 (13.0 ± 3.3) vs (12.9 ± 3.2) 0.739 (14.5 ± 3.5) vs (14.3 ± 3.6) 0.953TAS-2 (11.2 ± 2.6) vs (11.4 ± 2.7) 0.317 (11.8 ± 3.0) vs (11.7 ± 2.4) 0.914 (11.3 ± 3.0) vs (11.6 ± 3.0) 0.490TAS-3 (18.0 ± 4.6) vs (17.5 ± 4.8) 0.045* (18.0 ± 3.3) vs (18.2 ± 3.3) 0.336 (19.4 ± 5.9) vs (19.5 ± 5.9) 0.793
Notes: Wilcoxon Signed Rank Test was used for comparison of numerical data. Scores of recognized emotions are expressed as mean ± standard deviation. *Significant difference. Abbreviations: N: number of subjects; p: probability value; m: mean rank; ExP: existential psychotherapy group; CBT: cognitive behavioral therapy group; SUP: supportive counselling group; TAS-20: 20-item Toronto Alexithymia Scale; TAS-1: Difficulty in Identifying Feelings subscale; TAS-2: Difficulty in Describing Feelings subscale; TAS-3: Externally Oriented Thinking subscale; Bgn: mean ranks before sessions start; Awk: mean ranks after weekly sessions; ABst: mean ranks after booster sessions.
Table 8. Significance values (p) for correlations of TAS-20 total and subscale scores with HDRS scores of patients throughout the studyHDRS Bgn HDRS Awk HDRS ABst
TAS-total 0.223 0.461 0.586TAS-1 0.071 0.559 0.119TAS-2 0.987 0.065 0.332TAS-3 0.388 0.526 0.361
Notes: Pearson correlation test was used for the correlations. Abbreviations: HDRS: Hamilton Depression Rating Scale; TAS-20: 20-item Toronto Alexithymia Scale; TAS-1: Difficulty in Identifying Feelings subscale; TAS-2: Difficulty in Describing Feelings subscale; TAS-3: Externally Oriented Thinking subscale; Bgn: correlation significance with HDRS values before sessions start; Awk: correlation significance with HDRS values after weekly sessions; ABst: correlation significance with HDRS values after booster sessions.
Discussion
Depressive disorders relapse frequently, besides, their recurrence rate is remarkable38. As time progresses, the tendency to accept depression as a lifelong course is growing. Further, there are editorials supporting this approach39. The recurrence rate in first episode depression is reported to be 40% to 60% and after the third episode of depression, the rate reaches up to 90%40. Considering the increasing morbidity and mortality by each relapse and recurrence of MDD41, it is of critical importance to choose treatment modalities which seem to be most helpful to prevent from relapses and recurrences.
Classical and third wave CBT were compared with various psychotherapy models for treatment of depression. Some researchers argued that CBT was superior to other psychotherapies42,43. In a retrospective follow up of a randomized controlled trial regarding MDD patients with residual symptoms, CBT was found to have short term but not long term benefits44. In a different trial assessing the duration of CBT effect upon MDD, effects in prevention of relapse were found to persist, but with weakening, until 3 years after the end of CBT, and subsequent additional CBT was suggested to be explored45. Taking into account all of these, while it remains unclear that CBT is superior to other psychotherapies with respect to prevention from MDD, we decided to establish an indirect connection of preventive effect of CBT and certain other psychotherapies via their effect on alexithymia.
As mentioned above, phenomenologic dialogue in ExP is not a directive process. Thus, ExP does not particularly focus on symptom solving. It is a kind of work up for the process of openness to and looking out for experiences as a whole. Moreover,
ExP does not aim to reduce negative feelings and thoughts or to enhance positive feelings and thoughts. Instead, ExP focuses on directing the patient to negotiate with all dimensions of his/her experience including feelings, thoughts, bodily senses and realities of the external world46. By this way, patient is encouraged to make choices, getting into the action and accepting and taking responsibility of all predictable and unpredictable outcomes47. In the current trial, ExP was found to be helpful for treatment of MDD, and also for improvement of externally oriented thinking dimension of alexithymia. The reason why ExP seems to reduce externally oriented thinking between weekly and booster sessions may be the influence of phenomenologic dialogue, which, over time, presumably incites the curiosity of patients on multiple aspects of their physical and relational environment and on their spiritual world. Yet, contrary to the expectation arising from the previous interpretation, ExP did not seem to provide any improvements of identifying and describing own feelings. This finding may be explained with a broader awareness of alexithymia.
Outcomes reported for SUP and CBT in the treatment of depression were found to be comparable in some studies48. Contrary to the connotation arising from the word “supportive”, SUP does not aim to provide solutions or to become more skilful. It is based on the assumption that, moderating personal problems may be achieved through discussion with other people. Likely in our trial, SUP had a relatively free content, based on a work in which the therapist was rather a friendly listener than a talker. When asked for an assistance concerning the choices about problems of daily life, SUP therapist answered with superficial and short comments in order to find possible choices of the patient

162 Yilmaz O et al. / Arch Clin Psychiatry. 2019;46(6):156-64
together. SUP, though less effective than ExP and CBT, was found to be helpful for treatment of MDD. However, at the end of the trial, levels of alexithymia remained unchanged in SUP group.
The etiology of alexithymia is controversial. Some researchers put forward that, alexithymia is more likely to be a personality trait than a pathological condition49. Childhood traumas are relatively common among alexithymic individuals, thus, trauma may be the key factor for alexithymia50. Genetic factors are also pronounced to have an important role in development of alexithymia51. Thus, personality organisation, which is mostly the conclusion of genetics and early life experiences, seems to have a bigger role than recent psychosocial stress in development of alexithymia. This statement partly explains our findings that none of the psychotherapies improved alexithymia significantly.
Alexithymic individuals have difficulty in expressing their psychosocial stress, which leads to a limited chance to get help from other people. Thus, they are prone to feel like lonely and dismissed over time52. The term “emotional intelligence (EI)” was originally conceptualised as the ability to perceive accurately, apraise and express emotion; the ability to access and/or generate feelings when they facilitate thought; the ability to understand emotion and emotional knowledge; and the ability to regulate emotions to promote emotional and intellectual growth53. This definition seems to include the components of individual intelligence expressed by Gardner, mostly known of which are social intelligence and intrapersonal intelligence54. While social intelligence can be conceptualised as the ability to perceive emotions, intentions and desires of others, intrapersonal intelligence can be described as the ability to reach own emotional world. Despite the lack of implication about the ability to perceive other people’s emotions and feelings in the definition of alexithymia, experimental studies demonstrated that, alexithymic individuals are having difficulty in recognizing facial emotions of others55,56. As it is seen, the term alexithymia may be accepted to have a close conceptual relationship with EI57. Moreover, alexithymic individuals are reported to have difficulty to distinguish different emotional expressions58 and to have limited abilities to think functionally and use emotions in the way to cope with stressful situations59. Taking into account all of these and our findings, we suggest that, alexithymia might be a constitution in which the individual tends to get depressed more than the general population.
In a study with 33 outpatients who were positive responders to psychotherapy, the TAS-1 subscale was found to predict the severity of residual symptoms, over and above the effect of initial levels of depression and anxiety, form of psychotherapy, and use of antidepressant medication60. In another trail, designed as a follow up study, short term psychodynamic psychotherapy (STTP) with mentalization-based techniques was used in MDD patients. A baseline evaluation of reflective functioning, alexithymia and depression was conducted before treatment started. Patients were tested after forty weeks and in a follow up after one year at the end of the treatment. Results demonstrated an improvement of both depression and alexithymia61. Our findings did not demonstrate any improvement on alexithymia in CBT and SUP groups, however, a significant improvement was detected for TAS-3 in ExP group. This may partly be a conclusion of relatively short follow up period in our study, because, the improvement of TAS-3 in ExP group was detected in the final part of the study.
An article which summarizes findings from a series of studies that examined the effect of alexithymia on various aspects of psychotherapeutic approaches, reported some tendency for alexithymic patients to prefer group therapy. However, both in individual and group therapies, alexithymia was associated with poor outcome in both traditional psychodynamic psychotherapy and SUP. Moreover, the negative reaction that therapists had toward patients with high levels of alexithymia appeared to be in response to the lack of positive emotions expressed by these patients62. In our study, findings did not demonstrate any
significant correlation between levels of alexithymia and severity of depression, neither at the beginning, nor after weekly or booster sessions. Thus, alexithymia did not seem to be a predictor of response to the treatment. This interpretation is valid for relatively short period of our study, that is to say, a longer follow up period might have revealed different outcomes.
Current habitudes of daily living directs most of the community to live in urban centers. This in turn provides a culture of hurry, performance, massification, and superficiality in interpersonal relationships. Not surprisingly, this ends up with many types of suffering contained largely in anxiety disorders. On the other hand, psychotherapy, which optimally promises a deeper exploration of problems and finding the causative ground behind the scenes, every so often seems to force itself to meet expectations of the consumption society and ultimately falls into the trap of instantaneous and/or transient healing. Nevertheless, psychotherapy is one of the most effective ways to create greater openness to the expression of patients from a wide range of experience. This proposal directs us to the phenomenological particularity of each individual and it seems to best fit with ExP while phenomenologic dialogue can be defined as a kind of invitation to the individual to let happenings and things to demonstrate themselves just like what actually they are24.
Besides, a scientific doubt may be focused on psychotherapeutic approaches which target relatively short psychotherapy durations and relatively quick healing of symptoms, while symptomatic improvement often does not seem to make room for real emotional world of patients as a whole. In view of our findings which are in favor of ExP particularly in the late phase of the current study, we put forward that longer period of time may be needed for necessary deepening of the topics to be worked on the process and eventually to resolve the suffering brought as complaints to be worked in psychotherapy. Additionally, the psychotherapeutic approach of choice to respect for individuality seems to be phenomenology.
Our study has several limitations. At the onset, number of male patients were much less than female patients in all groups. So, we could not be able to compare therapeutic outcomes between genders. Alexithymic subjects (TAS-20 total score ≥ 61) were few in number, thus, we could not be able to compare the therapeutic outcomes of them with patients who do not have alexithymia (TAS-20 total score ≤ 51). We did not measure whether reactions of therapists toward patients worsened as the alexithymic level increases or not. Well organized further follow up studies in psychotherapy, preferably with large samples, focusing on therapist reactions is needed. We could compare the therapeutic outcomes of two therapists for ExP and CBT in themselves and did not find any significant difference. However, while there was one therapist for SUP, we did not have the chance to a likely comparison in SUP group. Sample size and number of sessions were relatively small.
Conclusions
Depressive patients were more alexithymic than healthy controls. CBT and SUP did not promote a reduction in alexithymia. ExP lead to a significant improvement in externally oriented thinking. The improvement observed in patients with alexithymia undergoing ExP was probably due to the greater appreciation of the phenomenological peculiar expressions and the longer period of therapeutic process. Alexithymia might be a personality trait which poses a remarkable risk for the individuals to get depressed. For further lightening of this issue, long term follow up studies with larger samples are needed.
ExP, CBT and SUP all led to a reduction in MDD. ExP and CBT had comparable effects, but both were more effective than SUP. Further studies, preferably with larger samples and long term follow up should be conducted to investigate all these differentials in other psychiatric disorders as well.

163Yilmaz O et al. / Arch Clin Psychiatry. 2019;46(6):156-64
Disclosure
The authors report no conflicts of interest.
Acknowledgements
Tezer Kiliçarslan, MD, Irem Gökgöz, MD, Fatma Büşra Parlakkaya, MD, Residents of Psychiatry, Bezmialem Foundation University Medical Faculty, Department of Psychiatry, İstanbul, Turkey (helped for acquisition of data, performed TAS-20).
References1. Sifneos PE. The prevalence of ‘alexithymic’ characteristics in
psychosomatic patients. Psychother Psychosom. 1973;22(2):255-62. 2. Kojima M, Senda Y, Nagaya T, Tokudome S, Furukawa TA. Alexithymia,
depression and social support among Japanese workers. Psychother Psychosom. 2003;72(6):307-14.
3. Suslow T, Rufer M, Kersting A, Guenther V. Predicting symptoms in major depression after inpatient treatment: The role of alexithymia. Eur Psychiatry. 2016;33(Suppl):s524.
4. Nakao M, Takeuchi T. Alexithymia and somatosensory amplification link perceived psychosocial stress and somatic symptoms in outpatients with psychosomatic illness. J Clin Med. 2018;7(5):112.
5. Di Trani M, Mariani R, Renzi A, Greenman PS, Solano L. Alexithymia according to Bucci’s multiple code theory: A preliminary investigation with healthy and hypertensive individuals. Psychol Psychother. 2018;91(2):232-47.
6. Sasioglu M, Gulol C, Tosun A. Aleksitimi Kavramı [The Concept of Alexithymia]. Current Approaches in Psychiatry. 2003;5(4):507-27.
7. Joukamaa M, Taanila A, Miettunen J, Karvonen JT, Koskinen M, Veijola J. Epidemiology of alexithymia among adolescents. J Psychosom Res. 2007;63(4):373-6.
8. Mason O, Tyson M, Jones C, Potts S. Alexithymia: its prevalence and correlates in a British undergraduate sample. Psychol Psychother. 2005;78(Pt 1):113-25.
9. Salminen JK, Saarijärvi S, Aärelä E, Toikka T, Kauhanen J. Prevalence of alexithymia and its association with sociodemographic variables in the general population of Finland. J Psychosom Res. 1999;46(1):75-82.
10. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990-2020: Global Burden of Disease Study. Lancet. 1997;349(9064):1498-504.
11. Walker ER, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiatry. 2015;72(4):334-41.
12. Beck A, Rush A, Shaw B, Emery G. Cognitive Therapy of Depression. New York, NY: The Guilford Press; 1979.
13. Beck AT. The current state of cognitive therapy: a 40-year retrospective. Arch Gen Psychiatry. 2005;62(9):953-9.
14. Beck J. Cognitive Behavior Therapy: Basics and Beyond. New York, NY: The Guilford Press; 2011.
15. Cuijpers P, Hollon SD, van Straten A, Bockting C, Berking M, Andersson G. Does cognitive behaviour therapy have an enduring effect that is superior to keeping patients on continuation pharmacotherapy? A meta-analysis. BMJ Open. 2013;3(4):e002542.
16. Kahl KG, Winter L, Schweiger U. The third wave of cognitive behavioural therapies. Curr Opin Psychiatry. 2012;25(6):522-8.
17. Podina IR, David D. Acceptance and Commitment Therapy. In: Vernon A, Doyle KA, eds. Cognitive Behavior Therapies: A Guidebook for Practitioners. Alexandria, VA: Wiley- American Counseling Association; 2018. p. 177-208.
18. Greenberg J, Shapero BG, Mischoulon D, Lazar SW. Mindfulness-based cognitive therapy for depressed individuals improves suppression of irrelevant mental-sets. Eur Arch Psychiatry Clin Neurosci. 2017;267(3):277-282.
19. Steiner CJ, Reisinger Y. Understanding existential authenticity. Ann Tourism Res. 2006;33(2):299-318.
20. Schnell T. Existential ındifference: another quality of meaning in life. J Hum Psychol. 2010;50(3):351-73.
21. Rae G. Sartre, Group Formations, and Practical Freedom. In: Realizing Freedom: Hegel, Sartre, and the Alienation of Human Being. London: Palgrave Macmillan; 2011. p. 91-109.
22. Danner H. Existential Responsibility – The Civic Virtue. Studies in Philosophy and Education. 1998;17(4):261-70.
23. Dearborn Nill J, Halling S. A Brief History of Existential – Phenomenological Psychiatry and Psychotherapy. Journal of Phenomenological Psychology. 1995;26(1):1-45.
24. Arnett RC. Toward a phenomenological dialogue. West J Comm. 1981;45(3):201-12.
25. Frankl VE. Logotherapy and existential analysis – a review. Am J Psychother. 1966;20(2):252-60.
26. DiPetta G. Addictions and depression: the paradise lost. Eur Psychiatry. 2015;30(1):114.
27. Ventegodt S, Clausen B, Langhorn M, Kromann M, Andersen NJ, Merrick J. Quality of life as medicine III. A qualitative analysis of the effect of a five-day intervention with existential holistic group therapy or a quality of life course as a modern rite of passage. ScientificWorldJournal. 2004;4:124-33.
28. Reiter MD, Chenail RJ, eds. Behavioral, humanistic-existential, and psychodynamic approaches to couples counseling. New York, NY: Taylor & Francis; 2017.
29. Cuijpers P, Driessen E, Hollon SD, van Oppen P, Barth J, Andersson G. The efficacy of non-directive supportive therapy for adult depression: a meta-analysis. Clin Psychol Rev. 2012;32(4):280-91.
30. Barth J, Munder T, Gerger H, Nüesch E, Trelle S, Znoj H, et al. Comparative efficacy of seven psychotherapeutic ınterventions for patients with depression: a network meta-analysis. PLoS Med. 2013;10(5):e1001454.
31. First MB, Spitzer R, Giboobn M, Williams J. Structed Clinical Interview for DSM IV Axis Disorders (SCID-1 SCID-I) Clinical Version. Washington DC, WA: American Psychiatric Press; 1997.
32. Özkürkçügil A, Aydemir O, Yıldız M, Esen-Danaci A, Köroğlu E. DSM-IV Eksen I bozuklukları için yapılandırılmış klinik görüşmenin Türkçeye uyarlanması ve güvenilirlik çalışması. İlaç ve Tedavi Dergisi. 1999;12(4):233-6.
33. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23:56-62.
34. Williams JB. A Structured Interview Guide for the Hamilton Depression Rating Scale. Arch Gen Psychiatry. 1988;45(8):742-7.
35. Akdemir A, Türkçapar MH, Orsel SD, Demirergi N, Dag I, Ozbay MH. Reliability and validity of the Turkish version of the Hamilton Depression Rating Scale. Compr Psychiatry. 2001;42(2):161-5.
36. Bagby RM, Parker JD, Taylor GJ. The twenty-item Toronto Alexithymia Scale – I. Item selection and cross-validation of the factor structure. J Psychosom Res. 1994;38(1):23-32.
37. Güleç H, Köse S, Güleç M, Çitak S, Evren C, Borckardt J, Sayar K. Reliability and factorial validity of the Turkish version of the 20-item Toronto alexithymia scale (TAS-20). Klinik Psikofarmakoloji Bülteni. 2009;19(3):214-20.
38. Monroe SM1, Harkness KL. Recurrence in major depression: a conceptual analysis. Psychol Rev. 2011;118(4):655-74.
39. Scott J. Depression should be managed like a chronic disease. Br Med J. 2006;332(7548):985-6.
40. Moffitt TE, Caspi A, Taylor A, Kokaua J, Milne BJ, Polanczyk G, et al. How common are common mental disorders? Evidence that lifetime prevalence rates are doubled by prospective versus retrospective ascertainment. Psychol Med. 2010;40(6):899-909.
41. Keller MB, Boland RJ. Implications of failing to achieve successful long-term maintenance treatment of recurrent unipolar major depression. Biol Psychiatry. 1998;44(5):348-60.
42. Eysenck HJ. The outcome problem in psychotherapy: what have we learned? Behav Res Ther. 1994;32(5):477-95.
43. Shapiro DA, Shapiro D. Meta-analysis of comparative therapy outcome studies: A replication and refinement. Psychol Bull. 1982;92(3):581-604.
44. Perlis RH. Cognitive behavioural therapy has short term but not long term benefits in people with residual symptoms of depression. Evid Based Ment Health. 2005;8(3):75.
45. Paykel ES, Scott J, Cornwall PL, Abbott R, Crane C, Pope M, et al. Duration of relapse prevention after cognitive therapy in residual depression: follow-up of controlled trial. Psychol Med. 2005;35(1):59-68.
46. Reker GT. Personal meaning, optimism, and choice: existential predictors of depression in community and ınstitutional elderly. Gerontologist. 1997;37(6):709-16.

164 Yilmaz O et al. / Arch Clin Psychiatry. 2019;46(6):156-64
47. Kuhl J, Koole S. Workings of the will: a functional approach. In: Greenberg J, Koole S, Pyszczynski T, eds. Handbook of experimental existential psychology. New York, NY: The Guilford Press; 2004. p. 411-30.
48. Pybis J, Saxon D, Hill A, Barkham M. The comparative effectiveness and efficiency of cognitive behaviour therapy and generic counselling in the treatment of depression: evidence from the 2nd UK National Audit of psychological therapies. BMC Psychiatry. 2017;17(1):215.
49. Salminen JK, Saarijärvi S, Toikka T, Kauhanen J, Aärelä E. Alexithymia behaves as a personality trait over a 5-year period in Finnish general population. J Psychosom Res. 2006;61(2):275-8.
50. Berenbaum H. Childhood abuse, alexithymia and personality disorder. J Psychosom Res. 1996;41(6):585-95.
51. Jørgensen MM, Zachariae R, Skytthe A, Kyvik K. Genetic and environmental factors in alexithymia: a population-based study of 8,785 Danish twin pairs. Psychother Psychosom. 2007;76(6):369-75.
52. Taylor GJ. Recent developments in alexithymia theory and research. Can J Psychiatry. 2000;45(2):134-42.
53. Salovey P, Mayer JD. Emotional Intelligence. Imag Cogn Pers. 1990;9(3):185-211.
54. Gardner H. Multiple ıntelligences: prelude, theory and aftermath. In: Sternberg R, Fiske S, Foss D, eds. Scientists making a difference. New York, NY: Cambridge University Press; 2016. p. 167-70.
55. Lane RD, Sechrest L, Reidel R, Weldon V, Kaszniak A, Schwartz GE. Impaired verbal and nonverbal emotion recognition in alexithymia. Psychosom Med. 1996;58(3):203-10.
56. Parker JD, Taylor GJ, Bagby RM. Alexithymia and the recognition of facial expressions of emotion. Psychother Psychosom. 1993;59(3-4):197-202.
57. Parker JD, Taylor GJ, Bagby RM. The relationship between emotional intelligence and alexithymia. Pers Individ Dif. 2001;30(1):107-15.
58. Bagby RM, Parker JDA, Taylor GJ, Acklin MW. Alexithymia and the ability to distinguish different emotional states. Psychother Psychosom. 1993;55:122.
59. Parker JD, Taylor GJ, Bagby RM. Alexithymia: relationship with ego defense and coping styles. Compr Psychiatry. 1998;39(2):91-8.
60. Ogrodniczuk JS, Piper WE, Joyce AS. Alexithymia as a predictor of residual symptoms in depressed patients who respond to short-term psychotherapy. Am J Psychother. 2004;58(2):150-61.
61. Bressi C, Fronza S, Minacapelli E, Nocito EP, Dipasquale E, Magri L, et al. Short‐Term Psychodynamic Psychotherapy with Mentalization‐Based Techniques in Major Depressive Disorder patients: Relationship among alexithymia, reflective functioning, and outcome variables – A Pilot study. Psychol Psychother. 2017;90(3):299-313.
62. Ogrodniczuk JS, Piper WE, Joyce AS. Effect of alexithymia on the process and outcome of psychotherapy: a programmatic review. Psychiatry Res. 2011;190(1):43-8.

Review article
Address for correspondence: Bruno Terra Junho. Instituto Raul Soares. Avenida do Contorno, 3017, Santa Efigênia – 30110-080 – Belo Horizonte, MG, Brazil. Telephone: +55 (31) 99201-1332/Fax: +55 (31) 3239-9900. E-mail: [email protected]
The role of NMDA receptor antagonists, amantadine and memantine, in schizophrenia treatment: a systematic review BRuNo teRRa juNHo1https://orcid.org/0000-0003-3677-7383
victoR FeRNaNdes de oliveiRa2https://orcid.org/0000-0003-3156-0249
1 Department of Mental Health, Faculty of Medical Sciences of Minas Gerais, Belo Horizonte, MG, Brazil.2 Department of Clinical and Toxicological Analyses, School of Pharmaceutical Sciences, University of São Paulo, São Paulo, SP, Brazil.
Received: 12/27/2018 – Accepted: 09/17/2019DOI: 10.1590/0101-60830000000218
AbstractObjective: Schizophrenia is a complex and chronic psychiatric disorder. In recent years, studies have found glutamatergic system participation in its etiopathogenesis, especially through aberrant NMDA receptors functioning. Thus, drugs that modulate this activity, as amantadine and memantine, could theoretically be used in its treatment. To perform a systematic literature review about memantine and amantadine use as adjunct in schizophrenia treatment. Methods: A systematic review of papers published in English indexed in the electronic database PubMed® using the terms “memantine”, “amantadine” and “schizophrenia” published until October 2016. Results: We found 144 studies, 8 selected for analysis due to meet the objectives of this review. Some of these have shown benefits from such drug use, especially in symptoms measured by PANSS and its subdivisions, while others do not. Discussion: The data in the literature about these drugs use for schizophrenia treatment is still limited and have great heterogeneity. Thus, assay with greater robustness are needed to assess real benefits of these drugs as adjuvant therapy.
Junho BT et al. / Arch Clin Psychiatry. 2019;46(6):165-8
Keywords: Schizophrenia, memantine, amantadine.
Introduction
Schizophrenia is a complex and heterogeneous psychiatric disorder characterized by an intriguing constellation of symptoms that are classically grouped into three main categories, positive (delusions and hallucinations), negative (apathy, social withdrawal and emotional blunting, for example) and cognitive symptoms (wide range of constituent elements, such as attention and memory impairments)1. This condition has a chronic course and important impact on this patients’ lives and currently is among the ten most disabling diseases2.
Despite the extensive efforts that have been made in therapeutic approaches, treatment still faces events that have not been overcome yet. The broad side effects profile of drugs available, the absence of well-established treatments for some disease dimensions, such as cognitive symptoms, and the modest response in the control of positive symptoms in refractory cases are some of these examples1. It is estimated that one-fifth to one-third of patients do not respond adequately to drug treatment3. Therefore, new drugs research is a pressing need and a deeper understanding of its pathophysiology is essential for this achievement.
Neurobiological processes comprehension underlying the schizophrenia has advanced immensely in the last decades with the new methodological approaches’ development. Initially, only the dopaminergic hyperactivity in the mesolimbic pathway had been described. However, recent evidence points to the involvement of glutamatergic pathways and glutamate receptors, especially the N-methyl-D-aspartate glutamatergic receptors (NMDAr), in its pathogenesis4.
As a main excitatory neurotransmitter, glutamate performs several functions in human brain such as attention5, memory and cognition processes6,7. Nevertheless, high glutamate levels overactive their receptors inducing neuronal damage, a process known as excitotoxicity, due to high calcium influx8. Glutamate receptors were divided basically in two different types: metabotropic and ionotropic receptors. The glutamate metabotropic receptors are members of a
receptor group coupled to G-protein. When this receptor is activated, a signal transduction cascade starts resulting various changes inside the neuron. Others receptors, such as a-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPAr), kainate and NMDAr, are classified as ionotropic receptors, i.e., a receptor linked to an ionic channel6,9.
There are various glutamatergic pathways in human brain. Among them, it is important to highlight the cortico-cortical pathways. In prefrontal cortex, glutamatergic neurons establish synapses with parvoalbumin-containing gamma-aminobutyric acid (GABA) interneuron. Then, this interneuron connects with another glutamatergic neuron that directs to the nucleus accumbens in the brainstem. This last neuron forms a synapsis with a dopaminergic neuron of mesolimbic pathway. These intricate connections are the link between glutamatergic and dopaminergic pathways. Therefore, the decrease in GABAergic activity in this pathway consequently increases the activity on the mesolimbic pathway as observed in schizophrenia10. In fact, the administration of phencyclidine and ketamine, dissociative anesthetics and NMDAr antagonists, causes psychotic, negative7 and cognitive symptoms8,9 development in healthy subjects and in animal models. Moreover, evidence supports the NMDAr autoantibodies involvement on lupus psychosis development10.
Hence drugs that modulate this pathway hypothetically could mitigate the symptoms observed in patients with schizophrenia. Amantadine and its derivate, memantine, show this ability. These drugs are NMDAr antagonists with moderate affinity and rapid receptor dissociation property leading to a sustained trait to block pathological hyperactivity, but not compromising physiological activity11.
Thus, memantine and amantadine, NMDAr antagonists, are possible agents to be evaluated for schizophrenia treatment by their ability to modulate glutamatergic system12, besides possessing neuroprotective activity13 and improve cognitive deficits and memory14. This paper aims to conduct a systematic review of the
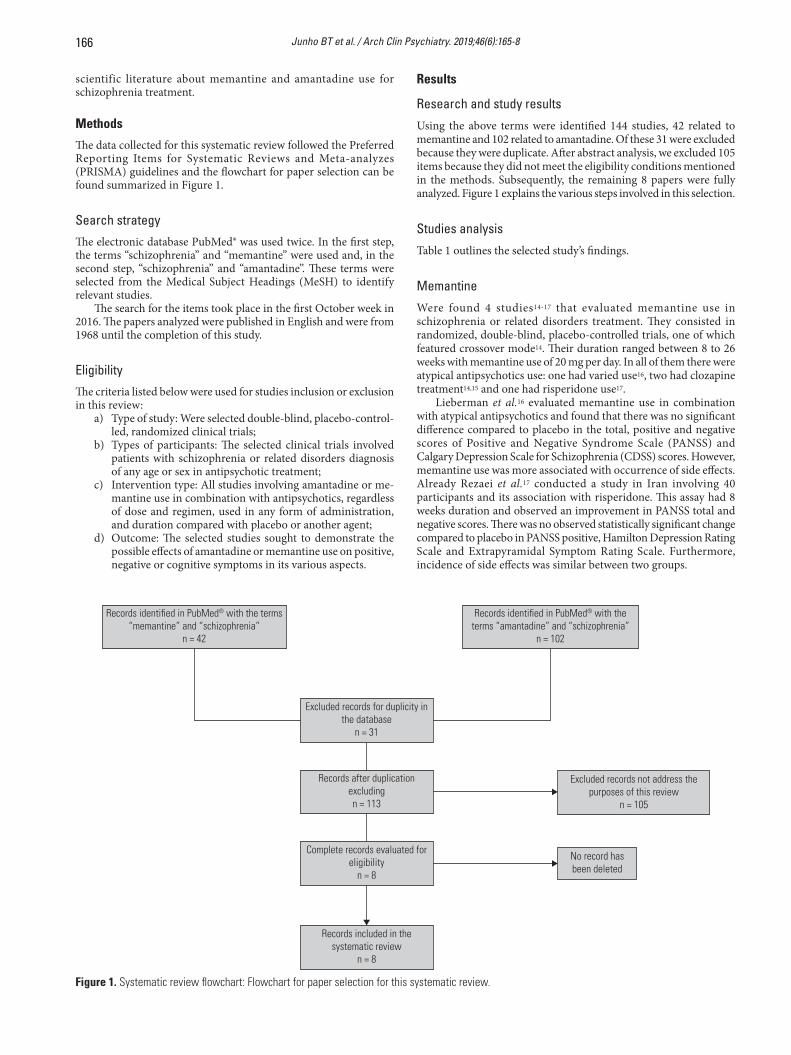
166 Junho BT et al. / Arch Clin Psychiatry. 2019;46(6):165-8
scientific literature about memantine and amantadine use for schizophrenia treatment.
Methods
The data collected for this systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyzes (PRISMA) guidelines and the flowchart for paper selection can be found summarized in Figure 1.
Search strategy
The electronic database PubMed® was used twice. In the first step, the terms “schizophrenia” and “memantine” were used and, in the second step, “schizophrenia” and “amantadine”. These terms were selected from the Medical Subject Headings (MeSH) to identify relevant studies.
The search for the items took place in the first October week in 2016. The papers analyzed were published in English and were from 1968 until the completion of this study.
Eligibility
The criteria listed below were used for studies inclusion or exclusion in this review:
a) Type of study: Were selected double-blind, placebo-control-led, randomized clinical trials;
b) Types of participants: The selected clinical trials involved patients with schizophrenia or related disorders diagnosis of any age or sex in antipsychotic treatment;
c) Intervention type: All studies involving amantadine or me-mantine use in combination with antipsychotics, regardless of dose and regimen, used in any form of administration, and duration compared with placebo or another agent;
d) Outcome: The selected studies sought to demonstrate the possible effects of amantadine or memantine use on positive, negative or cognitive symptoms in its various aspects.
Results
Research and study results
Using the above terms were identified 144 studies, 42 related to memantine and 102 related to amantadine. Of these 31 were excluded because they were duplicate. After abstract analysis, we excluded 105 items because they did not meet the eligibility conditions mentioned in the methods. Subsequently, the remaining 8 papers were fully analyzed. Figure 1 explains the various steps involved in this selection.
Studies analysis
Table 1 outlines the selected study’s findings.
Memantine
Were found 4 studies14-17 that evaluated memantine use in schizophrenia or related disorders treatment. They consisted in randomized, double-blind, placebo-controlled trials, one of which featured crossover mode14. Their duration ranged between 8 to 26 weeks with memantine use of 20 mg per day. In all of them there were atypical antipsychotics use: one had varied use16, two had clozapine treatment14,15 and one had risperidone use17.
Lieberman et al.16 evaluated memantine use in combination with atypical antipsychotics and found that there was no significant difference compared to placebo in the total, positive and negative scores of Positive and Negative Syndrome Scale (PANSS) and Calgary Depression Scale for Schizophrenia (CDSS) scores. However, memantine use was more associated with occurrence of side effects. Already Rezaei et al.17 conducted a study in Iran involving 40 participants and its association with risperidone. This assay had 8 weeks duration and observed an improvement in PANSS total and negative scores. There was no observed statistically significant change compared to placebo in PANSS positive, Hamilton Depression Rating Scale and Extrapyramidal Symptom Rating Scale. Furthermore, incidence of side effects was similar between two groups.
Figure 1. Systematic review flowchart: Flowchart for paper selection for this systematic review.
Records identi�ed in PubMed® with the terms “memantine” and “schizophrenia”
n = 42
Excluded records for duplicity in the database
n = 31
Records after duplication excludingn = 113
Complete records evaluated for eligibility
n = 8
Records included in the systematic review
n = 8
No record has been deleted
Excluded records not address the purposes of this review
n = 105
Records identi�ed in PubMed® with the terms “amantadine” and “schizophrenia”
n = 102

167Junho BT et al. / Arch Clin Psychiatry. 2019;46(6):165-8
A study conducted in Netherlands14 with 26 weeks duration and participation of 52 schizophrenic patients taking clozapine found that memantine use was associated with negative symptoms reduction, as assessed by PANSS Negative, compared to placebo. There was no statistically significant difference in PANSS total, positive and side effects occurrence between them.
Finally, Lucena et al.15, in a study conducted in Brazil, evaluating 21 patients with refractory schizophrenia, who were taking clozapine, verified that memantine addition to treatment regimen is associated with improvement in all aspects evaluated in Brief Psychiatry Rating Scale (BPRS). However, side effects incidence, Clinical Global Impressions and Mini-Mental State Examination (MMSE) score did not differ from that observed in placebo.
Amantadine
Were found 4 studies18-21 evaluated the amantadine use in association with various antipsychotics in patients with schizophrenia and schizoaffective disorder.
In the study conducted by Czepielewski et al.18 in Brazil, involving 20 patients and amantadine administration of 400 mg per day, was verified better scores in Hopkins Verbal Learning Test-Revised in treated group with this drug compared to placebo. Moreover, Silver et al.21 found no improvement in clinical parameters of PANSS total and AIMS subdivisions with amantadine use.
Two Israeli studies19,20 evaluating biperiden or amantadine response in combination with antipsychotics in crossover noted that there were no significant changes between the groups with respect to PANSS negative and positive, BPRS scores and incidence of extrapyramidal symptoms with amantadine use in relation to biperiden, but there was a better score on Benton Visual Retention Test in amantadine treated group. The extrapyramidal symptoms incidence was higher in placebo group. The values found in MMSE and Weschler Memory Scale total score were not statistically significant between amantadine and biperiden use.
Discussion
In the last years the understanding of glutamatergic pathways involvement in schizophrenia etiopathogenesis has advanced dramatically, especially after the implication that aberrant NMDAr functioning plays in this condition4,19. Therefore, the search for drugs that modulate these receptors activity could hypothetically bring benefits, especially with regard to cognitive symptoms1,5-7,10. Although their mechanisms are not yet completely understood, amantadine and memantine are very interesting drugs because their ability to antagonize NMDAr and promoting a regulation in this pathological receptor activity without compromising the physiological action22. This property is already explored in Alzheimer disease treatment23,24, nevertheless, its use in schizophrenia is an initial objective of interest.
Table 1. Memantine and amantadine studies in schizophrenia: studies characteristics summary involving memantine and amantadine use in patients with schizophreniaStudy Study
designDiagnosis Diagnosis
criterian (case/placebo)
Duration (week)
Age (years ± SD)
Men (%) Drug Dose (mg/day)
Outcomes
MemantineLieberman et al., USA16
DBPCT Schizophrenia or schizoaffective
disorder
DSM-IV 69/67 8 MEM: 40,9 ± 9,8
PLA:40,1 ± 11,3
MEM: 59.4PLA: 79.1
Memantine + atypical
antipsychotics
20 PANSS Total, Positive, Negative and CDSS: MEM = PLA
SE: MEM > PLA
Rezaei et al., Iran17
DBPCT Schizophrenia DSM-IV-TR
20/20 8 MEM:33,5 ± 6,9
PLA:33,0 ± 6,9
MEM: 60PLA: 55
Memantine + risperidone
20 PANSS Total and Negative: MEM > PLA
PANSS Positive, HDRS, ESRS and SE: MEM = PLA
Veerman et al., Netherlands14
DBPCT(crossover)
Schizophrenia DSM-IV 52 26 42,35 ± 9,55 75 Memantine + clozapine
20 PANSS Total, Positive and SE: MEM = PLA
PANSS Negative: MEM > PLA
De Lucena et al., Brazil15
DBPCT Schizophrenia DSM-IV 10/11 12 MEM:34,67 ± 9,04
PLA: -
MEM: 90,5PLA: -
Memantine + clozapine
20 BPRS Total, Positive and Negative: MEM > PLA
SE, GCI e MMSE: MEM = PLAAmantadineCzepielewski et al., Brazil18
DBPCT Schizophrenia DSM-IV 9/11 12 27,80 ± 5,05 75 Amantadine + variable
antipsychotic
400 HVLT-R: AMA > PLA
Silver et al., Israel21
DBPCT(crossover)
Schizophrenia or schizoaffective
disorder
DSM-IV 29 6 36,86 ± 10,77
75,86 Amantadine + variable
antipsychotic
200 Cognitive tests, PANSS Total, Positive and Negative and
AIMS: AMA = PLASilver and Geraisy, Israel19
DBPCT(crossover)
Schizophrenia DSM-III-R 26 6 36,65 ± 8,89 69,23 Amantadine or biperiden + variable
antipsychotic
- PANSS Negative, Positive, BPRS and ES: AMA = BIPES: PLA > AMA and BIP
Silver and Geraisy, Israel20
DBPCT(crossover)
Schizophrenia DSM-III-R 26 6 36,65 ± 8,89 69,23 Amantadine or biperiden + variable
antipsychotic
AMA: 200
BIP: 4
BVRT: AMA > BIPMMSE and WMS Total: AMA
= BIPWMS Subtest (Visual
reproduction): AMA > BIP
SD: standard deviation; DBPCT: double-blind placebo-controlled trials; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; DSM-III-R: Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised; MEM: memantine; AMA: amantadine; BIP: biperiden; PLA: placebo; PANSS: Positive and Negative Syndrome Scale; CDSS: Calgary Depression Scale for Schizophrenia; SE: side effects; HDRS: Hamilton Depression Rating Scale; ESRS: Extrapyramidal Symptom Rating Scale; BPRS: Brief Psychiatry Rating Scale; ES: extrapyramidal symptoms; MMSE: Mini-Mental State Examination; CGI: Clinical Global Impressions; HVLT-R: Hopkins Verbal Learning Test-Revised; AIMS: Abnormal Involuntary Movement Scale; WMS: Wechsler Memory Scale.

168 Junho BT et al. / Arch Clin Psychiatry. 2019;46(6):165-8
Various studies have evaluated the clinical impact that amantadine and memantine use in schizophrenia treatment14-21. It is important to note that Lieberman et al.16 and Silver et al.21 studies included patients with schizoaffective disorder in memantine and amantadine clinical trials in their analysis, respectively.
Memantine studies showed in this review are double-blind placebo-controlled trials (DBPCT)15-17, but only one was conducted in a crossover design14. All trials used Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) diagnosis criteria, except an Iranian research that used the revised version17. In all studies, memantine was associated with atypical antipsychotics, two of them used clozapine14,15.
Memantine showed to improve negative symptoms of schizophrenia assessed by PANSS14,17, but not positive symptoms14,16. De Lucena et al.15 found an improvement in all three BPRS subscales. The data related to the incidence of side effects are divergent among the studies. Lieberman et al.16 found that they are more frequent in subjects taking memantine than placebo, while two other studies did not find this association14,17.
The studies involving amantadine were mostly DBPCT crossover18-21, one of which also included patients with schizoaffective disorder21 and two compared the efficacy of this drug with biperiden19,20. According to a Brazilian study18, patients with schizophrenia using amantadine showed better verbal learning and memory than the placebo group. In addition, the visual reproduction capacity was greater in patients using amantadine than biperiden21.
Both clinical trials have important limitations such as small number of patients and sparse follow-up period. The variety of antipsychotics and the scales used, especially in the studies involving the use of amantadine, make it difficult to compare them.
Thus, it would be essential to develop researches involving a larger number of patients with a longer follow-up and standardization of the used scales to evaluate the various symptomatic dimensions. Therefore, a more emphatic approach is necessary in this direction to elucidate the true role of these drugs as adjuncts to antipsychotic treatment since the data currently available in the scientific literature do not recommend its widespread use in clinical practice22.
Ackowledgment
We are grateful for the support of the Neurosciences program team of the Universidade Federal de Minas Gerais and the psychiatric residency program staffs of the Instituto Raul Soares.
References
1. Owen MJ, Sawa A, Mortensen PB. Schizophrenia. Lancet. 2016;388(10039):86-97.
2. Lopez AD, Murray CCJL. The global burden of disease, 1990-2020. Nat Med. 1998;4(11):1241-3.
3. Conley RR, Buchanan RW. Evaluation of treatment-resistant schizophre-nia. Schizophr Bull. 1997;23(4):663-74.
4. Moghaddam B, Javitt D. From revolution to evolution: the glutamate hypothesis of schizophrenia and its implication for treatment. Neurop-sychopharmacology. 2012;37(1):4-15.
5. Thiele A, Bellgrove MA. Neuromodulation of attention. Neuron. 2018;97(4):769-85.
6. Dauvermann MR, Lee G, Dawson N. Glutamatergic regulation of cog-nition and functional brain connectivity: insights from pharmacologi-
cal, genetic and translational schizophrenia research. Br J Pharmacol. 2017;174(19):3136-60.
7. Gécz J. Glutamate receptors and learning and memory. Nat Genet. 2010;42(11):925-6.
8. Arundine M, Tymianski M. Molecular mechanisms of calcium-de-pendent neurodegeneration in excitotoxicity. Cell Calcium. 2003;34(4-5):325-37.
9. Traynelis SF, Wollmuth LP, McBain CJ, Menniti FS, Vance KM, Ogden KK, et al. Glutamate Receptor Ion Channels: Structure, Regulation, and Function. Pharmacol Rev. 2010;62(3):405-96.
10. Schwartz T, Sachdeva S, Stahl S. Glutamate neurocircuitry: theoretical underpinnings in schizophrenia. Front Pharmacol. 2012;3:195.
11. Javitt DC. Glutamate as a therapeutic target in psychiatric disorders. Mol Psychiatry. 2004;9(11):984-97, 979.
12. John JP, Lukose A, Manjunath S. Off-label use of memantine as adjunctive treatment in schizophrenia: a retrospective case series study. Pharma-copsychiatry. 2014;47(6):202-9.
13. Lipton SA. Paradigm shift in neuroprotection by NMDA receptor blockade: memantine and beyond. Nat Rev Drug Discov. 2006;5(2): 160-70.
14. Veerman SR, Schulte PF, Smith JD, de Haan L. Memantine aug-mentation in clozapine-refractory schizophrenia: a randomized, double-blind, placebo-controlled crossover study. Psychol Med. 2016;46(9):1909-21.
15. de Lucena D, Fernandes BS, Berk M, Dodd S, Medeiros DW, Pedrini M, et al. Improvement of negative and positive symptoms in treatment-re-fractory schizophrenia: a double-blind, randomized, placebo-controlled trial with memantine as add-on therapy to clozapine. J Clin Psychiatry. 2009;70(10):1416-23.
16. Lieberman JA, Papadakis K, Csernansky J, Litman R, Volavka J, Jia XD, et al.; MEM-MD-29 Study Group. A randomized, placebo-controlled study of memantine as adjunctive treatment in patients with schizophrenia. Neuropsychopharmacology. 2009;34(5):1322-9.
17. Rezaei F, Mohammad-Karimi M, Seddighi S, Modabbernia A, Ashrafi M, Salehi B, et al. Memantine add-on to risperidone for treatment of negative symptoms in patients with stable schizophrenia: randomi-zed, double-blind, placebo-controlled study. J Clin Psychopharmacol. 2013;33(3):336-42.
18. Czepielewski LS, Sodre L, Souza AC, Bucker J, Burke KP, Cereser KM, et al. Changes in verbal learning of patients with schizophrenia: results from a randomized, double-blind, placebo-controlled trial of amantadine adjunctive to antipsychotics. Schizophr Res. 2015;168(1-2):571-2.
19. Silver H, Geraisy N. No difference in the effect of biperiden and amanta-dine on negative symptoms in medicated chronic schizophrenic patients. Biol Psychiatry. 1995;38(6):413-5.
20. Silver H, Geraisy N. Effects of biperiden and amantadine on memory in medicated chronic schizophrenic patients. a double-blind cross-over study. Br J Psychiatry. 1995;166(2):241-3.
21. Silver H, Goodman C, Isakov V, Knoll G, Modai I. A double-blind, cross--over comparison of the effects of amantadine or placebo on visuomotor and cognitive function in medicated schizophrenia patients. Int Clin Psychopharmacol. 2005;20(6):319-26.
22. Kishi T, Iwata N. NMDA receptor antagonists interventions in schi-zophrenia: Meta-analysis of randomized, placebo-controlled trials. J Psychiatr Res. 2013;47(9):1143-9.
23. Kishi T, Matsunaga S, Oya K, Nomura I, Ikuta T, Iwata N. Memantine for Alzheimer’s Disease: An Updated Systematic Review and Meta-analysis. J Alzheimers Dis. 2017;60(2):401-25.
24. McShane R, Westby MJ, Roberts E, Minakaran N, Schneider L, Farri-mond LE, et al. Memantine for dementia. Cochrane Database Syst Rev. 2019;3:CD003154.
Letter to the editor
Primary hyperparathyroidism presenting as major depression with psychotic featuresjosepH kuo1
yoNe-HaN MaH2,3https://orcid.org/0000-0002-5439-176X
jui-teNg wu4
cHiH-cHuNg sHiao5,6https://orcid.org/0000-0003-2220-7574
1 Department of Psychiatry, Camillians Saint Mary's Hospital Luodong, Yilan, Taiwan. 2 Division of Gastroenterology, Department of Internal Medicine, Camillians Saint Mary's Hospital Luodong, Yilan, Taiwan.3 Division of Gastroenterology, Department of Internal Medicine, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwan.4 Division of General Surgery, Department of Surgery, Camillians Saint Mary's Hospital Luodong, Yilan, Taiwan. 5 Division of Nephrology, Department of Internal Medicine, Camillians Saint Mary's Hospital Luodong, Yilan, Taiwan.6 Saint Mary’s Junior College of Medicine, Nursing and Management, Yilan, Taiwan.
Received: 3/5/2019 – Accepted: 5/21/2019DOI: 10.1590/0101-60830000000219
Kuo J et al. / Arch Clin Psychiatry. 2019;46(6):169-70
Address for correspondence: Chih-Chung Shiao. Division of Nephrology, Department of Internal Medicine, Camillians Saint Mary's Hospital Luodong. 160 Chong-Cheng South Road, Loudong 265, Yilan, Taiwan. Telephone: +886-3-9544106#7951. E-mail: [email protected]
Dear Editor,
Primary hyperparathyroidism (PHPT) might associate with multiple neuropsychiatric symptoms, but it is often overlooked by physicians when making differential diagnosis for patients with psychiatric disorders. We report a case of PHPT presenting as major depression with psychotic features.
A 47-year-old previously healthy woman presented with a 2-weeks history of depressed mood, loss of interest, insomnia, poor concentration, fatigue and poor appetite with prominent body weight loss. Besides, blunted affect, prominent psychomotor retardation, occasional irrelevant speech, the delusion of guilt, persecution, and negation were also noted. Under the impression of major depressive disorder, she was treated with escitalopram
20 mg and aripiprazole 10 mg per day. After drug treatment for four weeks, the score of the 17-item Hamilton Depression Rating Scale (HAMD-17) was decreased from the initial 46 to 35, which didn’t reach obvious response (defined by a decrease of scores for 50% or more). The following laboratory tests revealed severe hypercalcaemia of 16.8 (reference, 8.6-10.0) mg/dl, hypokalemia of 2.4 (3.5-5.1) mg/dl, borderline thyroid function with free-T4 of 1.74 (0.93-1.7) ng/dl and thyroid-stimulating hormone of 1.18 (0.27-4.2) μIU/ml, along with blood urea nitrogen of 26.2 (6-20) mg/dl and creatinine of 1.4 (0.5-0.9) mg/dl.
The diagnosis of PHPT was established by the extraordinarily high level of PTH [911.8 (17-65) pg/ml], and one huge mass at left lower parathyroid gland was subsequently found by echography and Tc-99m scan (Figure 1). The parathyroidectomy was undergone soon,
Figure 1. Parathyroid scan with intravenous Technetium-99m methoxyisobutylisonitrile injection revealed a huge parathyroid adenoma in the left lower thyroid region.

170 Kuo J et al. / Arch Clin Psychiatry. 2019;46(6):169-70
and the pathological report disclosed one 5 x 3 x 1.5 cm parathyroid gland with oncocytic and chief cell hyperplasia. Both serum calcium (9.9 mg/dl) and PTH levels (52.57 pg/ml) dramatically decreased to the normal range in one day following the parathyroidectomy. The score of HAMD-17 decreased to 23 in seven days and to 4 in 14 days after the surgery, indicative of complete remission of the depression. Her somatic symptom remitted and her body weight returned back to the same before this episode.
Psychiatric symptoms were reported in 4.2%-10% patients with PHPT1,2, whereas higher prevalence rates of neuropsychiatric disturbances were observed in patients with more severe PHPT necessitating parathyroidectomy3. These prevalence rates include 43.1%-53% for anxiety, 33.0%-62.1% for depression, 22% for thoughts of death or suicide, 51.9% for anger and irritability, 5-20% for hallucination and delusions, and 37.3%-46.6% for impaired cognition3. The occurrence and severity of psychiatric symptoms are associated with increased levels of serum calcium and PTH4. The mechanism is presumably related to the low levels of monoamine metabolites and increased calcium levels found in the cerebrospinal fluid1.
A primary psychiatric disorder is a diagnosis of exclusion. PHPT should be considered as a differential diagnosis for a patient with a psychiatric disorder. To establish the diagnosis of PHPT, some biochemical tests including serum total calcium, PTH, creatinine, 25-hydroxy vitamin D and 24-hour urinary calcium and creatinine are recommended, and certain disorders causing secondary
hyperparathyroidism must be excluded4. Parathyroidectomy is the only curative therapy for PHPT, which significantly leads to a reduction of depressive symptoms and an improvement of patients’ quality of lives2.
Acknowledgment
The authors declare no potential conflicts of interest in writing this report.
Funding
None declared.
References1. Chiba Y, Satoh K, Ueda S, Kanazawa N, Tamara Y, Horiuchi T. Marked
improvement of psychiatric symptoms after parathyroidectomy in elderly primary hyperparathyroidism. Endocr J. 2007;54(3):379-83.
2. Wilhelm SM, Lee J, Printz RA. Major depression due to primary hyperparathyroidism: a frequent and correctable disorder. Am Surg. 2004;70(2):175-9.
3. Parks KA, Parks CG, Onwuameze OE, Shrestha S. Psychiatric complica-tions of primary hyperparathyroidism and mild hypercalcaemia. Am J Psychiatry. 2017;174(7): 620-2.
4. Parnell KE, Oltmann SC. The surgical management of primary hyper-parathyroidism: an updated review. Int J Endo Oncol. 2018;5(1):IJE07.

Letter to the editor
Address for correspondence: Yu-Chih Shen. Department of Psychiatry, Tzu-Chi General Hospital, 707, Sec. 3, Chung Yang Rd, Hualien 970, Taiwan. Telephone: 886-3-8561825 ext. 15041. Fax: 886-3-8466863. E-mail: [email protected]
Complex drug interaction of carbamazepine, fluvoxamine and clozapine in a patient with bipolar depressionwei-yuaN cHeN1https://orcid.org/0000-0002-0507-8187
yu-cHiH sHeN1,2https://orcid.org/0000-0002-3503-5778
1 Department of Psychiatry, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Hualien, Taiwan.2 School of Medicine, Tzu Chi University, Hualien, Taiwan.
Received: 04/26/2019 – Accepted: 05/21/2019DOI: 10.1590/0101-60830000000220
Chen WY et al. / Arch Clin Psychiatry. 2019;46(6):171
Dear Editor,
In the treatment of bipolar depression, classes of commonly used drugs include lithium, anticonvulsants and antipsychotics. Sometimes antidepressants can also be considered a choice1. Some of them may induce or inhibit cytochrome P450 isoenzymes and, when combined in clinical use, may not accurately predict the effects of drug interactions. For example, previous studies have shown that carbamazepine (CBZ) can reduce plasma levels of clozapine (CLZ), while fluvoxamine (FVX) can increase plasma levels of CLZ2. Additionally, the combined administration of FVX and CBZ may increase plasma concentrations of CBZ3. Here, we report the drug interaction in a patient with bipolar depression with the concomitant use of CBZ, CLZ and FVX.
A 46-year-old man with bipolar II disorder treated with 800 mg quetiapine and 400 mg CBZ controlled release daily. He was admitted to an acute psychiatric ward because of his depressed mood, insomnia, and suicidal thoughts. He maintained a blood CBZ level of 8.86 μg/mL on admission (normal range: 4 to 12 μg/mL). Initially, we added 50 mg of agomelatine for depression and insomnia, but to no avail. Therefore, we administered 100 mg FVX plus 100 mg CLZ in place of quetiapine and agomelatine. The result was wonderful in improving his depressive symptoms and insomnia, with the exception of dizziness that complained of the patient during the day. The blood level of CBZ increased to 13.83 μg/mL after re-verification. We adjusted the dose of CLZ from 100 mg to 50 mg and used fast-acting CBZ instead of controlled release without dose modification. After adjustment, her dizziiness improved and also remained effective in cases of depression and insomnia with a CBZ blood level of 10.82 μg/mL.
To our knowledge, this is the first case describing the concomitant use of CBZ, FVX and CLZ. Previous studies had suggested that FVX increased plasma levels of CLZ and CBZ as an inhibitor of
CYP1A2 and 3A4, respectively2,3. In contrast, CBZ decreased the plasma level of CLZ by being a CYP3A4 inducer2. The increase in blood levels of CBZ in this patient could be explained mainly by the effect of FVX. Although FVX and CBZ have an opposite effect on CLZ, we have suggested that the effect of FVX on CLZ was much greater than that of CBZ on CLZ, which would reduce the dose of CLZ required in this patient. Formal pharmacokinetic studies examining the potential interaction between these three drugs are needed to confirm this finding. In summary, this case highlights the importance of monitoring plasma concentrations or clinical status when multiple drugs that inhibit or inhibit CYP450 are combined.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Disclosure
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.
References
1. Shen YC. Treatment of acute bipolar depression. Ci Ji Yi Xue Za Zhi. 2018;30(3):141-7.
2. Jerling M, Lindstrom L, Bondesson U, Bertilsson L. Fluvoxamine inhi-bition and carbamazepine induction of the metabolism of clozapine: evidence from a therapeutic drug monitoring service. Ther Drug Monit. 1994;16(4):368-74.
3. Cottencin O, Regnaut N, Thevenon-Gignac C, Thomas P, Goudemand M, Debruille C, et al. Carbamazepine-fluvoxamine interaction. Consequen-ces for the carbamazepine plasma level. Encephale. 1995;21(2):141-5.

Index
Searches for research keywords can be done at the Journal homepage: http://www.archivespsy.com/
Adherence 85Adolescent 40Alcohol use 44, 50Alexithymia 156Alzheimer’s disease 120Amantadine 165Anxiety 14, 40Anxiety and depressive disorders 107Aripiprazole 33Assessment 89Attention deficit/hyperactivity disorder (ADHD) 40Biomarkers 120Bipolar disorder 66, 125Bisexuality 97Blunted affect 132Body composition 66BSPS 27Bullying 97Caregiver 145Cathelicidin 66Cerebral palsy 145Children 145China 107Clinically significant depressive symptoms 14Cognition 61Cognitive behavioral therapy 156Community 72Coping style 145Cross-cultural adaptation 132Current health perception 53Depression 9, 14, 40, 145, 156Depressive symptoms 137Drug attitude 85Egypt 27Elderly 14, 151Epidemiology 72Executive functions 89Existential psychotherapy 156Frailty 151Ganglion cell layer volume 125General hospitals 107Glucose and lipid 33Health outlook perception 53Health perception 53Health personnel 115Health promotion 115Homosexuality 97Illness impact 85Illness self-management 1Inflammation 9, 137Internet 97Internet addiction 40Intracellular cytokines 137Lipopolysaccharide 137
Ll-37 66Mean platelet volume 9Memantine 165Mental health 151Mental health resources 107Mental illness 85Mild cognitive impairment 72, 120Mobile applications 1Monoamine oxidase B 21 Negative symptoms 132Neurodegeneration 125Neutrophil to lymphocyte ratio 9Nicotine dependence 21 Olanzapine 33Older adults 137Optic coherence tomography 125Parental attitudes 103Parental bonding 40Persistent developmental stuttering 103Personality beliefs 61Physical activity 14Plasma 120Polyamines 120Positive symptoms 5Prevalence 72Primary health care 115Prior health perception 53Psychological well-being 53Psychopathology 5Quality of life 115Rating scale 5Reliability 89Retinal nerve fiber layer thickness 125Risk factors 44Risk factors 50Schizophrenia 1, 5, 21, 33, 132, 165Self-regulation 89Severity 103Sex difference 33Smart phone addiction 61Smartphone 97Social anxiety disorder 27Social norms 44, 50Social phobia 27Students 27Supportive counselling 156Technology 1Treatment 9University 27University students 44, 50, 61Validation studies 132Validity 89Variant 21







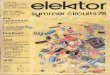




















![SSC - prepadda.comprepadda.com/wp-content/uploads/english/ARTICLE IMPORTANT NOTES[].pdf Means to say ( ) Vowel Consonant Consonant Vowel Vowel = Vowel Consonant = Consonant ... I had](https://img.dokumen.tips/doc/110x75/5e4437036ae6ba6d743ded6b/ssc-prepaddacomprepaddacomwp-contentuploadsenglisharticle-important-notes.jpg)