Embed Size (px)
Citation preview

“A VIEW FROM THE TRENCHES”
PRECONCEPTION CARE: A RADICAL PARADIGM SHIFT FOR IMPROVING PERINATAL OUTCOMEJordan H. Perlow MDPartner: Phoenix Perinatal AssociatesMFM;; Banner University Med [email protected] high risk pregnancy
OBJECTIVES:¢ Review our current approach to achieving optimal pregnancy outcomes
¢ Present rationale for suggesting alternative approach
¢ Present specific case examples¢ Provide recommendations for achieving further improvement in perinatal outcomes
NO:DISCLOSURES
CONFLICTS OF INTEREST

Improving Perinatal Outcome“Building the Case
For A Radical Change”“marked by
a considerable departure from the usual or traditional”PRECONCEPTION / INTERCONCEPTION CARE
Interventions that aim to identify and modify BIOMEDICAL, BEHAVIORAL, and SOCIAL RISKS to a woman's health and pregnancy outcome
through prevention and management
What Is Our Mission As Providers Of Obstetrical Care?
¢“To achieve the very best perinatal outcomes possible, given the clinical circumstances presented” HOW DO WE ACCOMPLISH THIS?
¢Extensive Education and Training ¢Implementation / Application of a “Fund of Knowledge”
¢Utilization of Available Technology and Therapy
¢Evidence-Based / Outcomes-Driven Practice
With Passion, Commitment, and Empathy
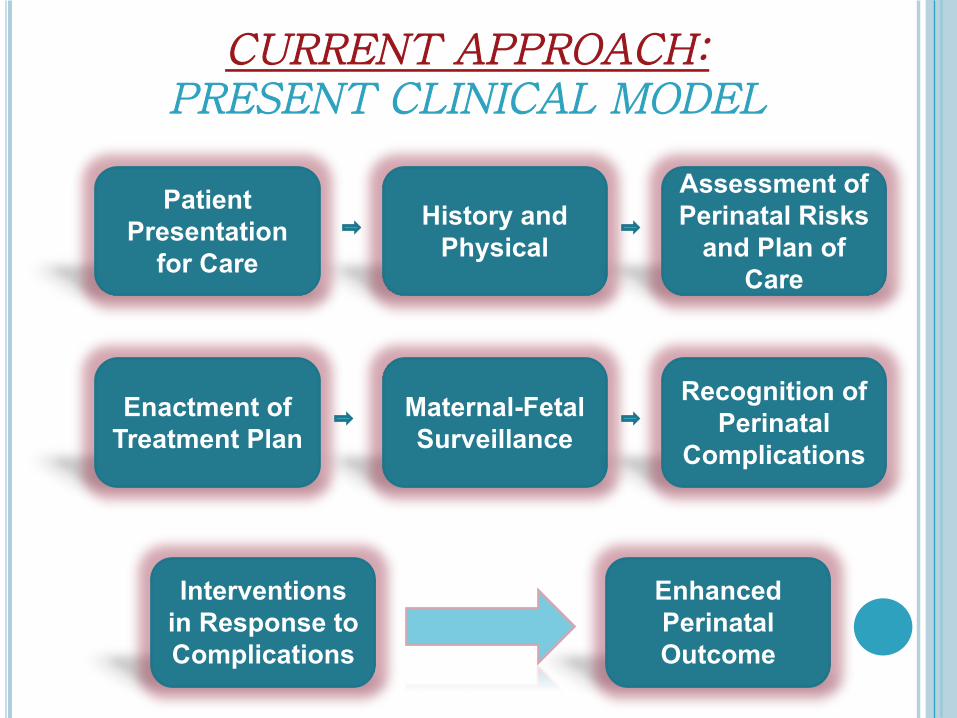
CURRENT APPROACH:PRESENT CLINICAL MODEL
Patient Presentation for Care
History and Physical
Assessment of Perinatal Risks and Plan of
Care
Enactment of Treatment Plan
Maternal-Fetal Surveillance
Recognition of Perinatal
Complications
Interventions in Response to Complications
Enhanced Perinatal Outcome
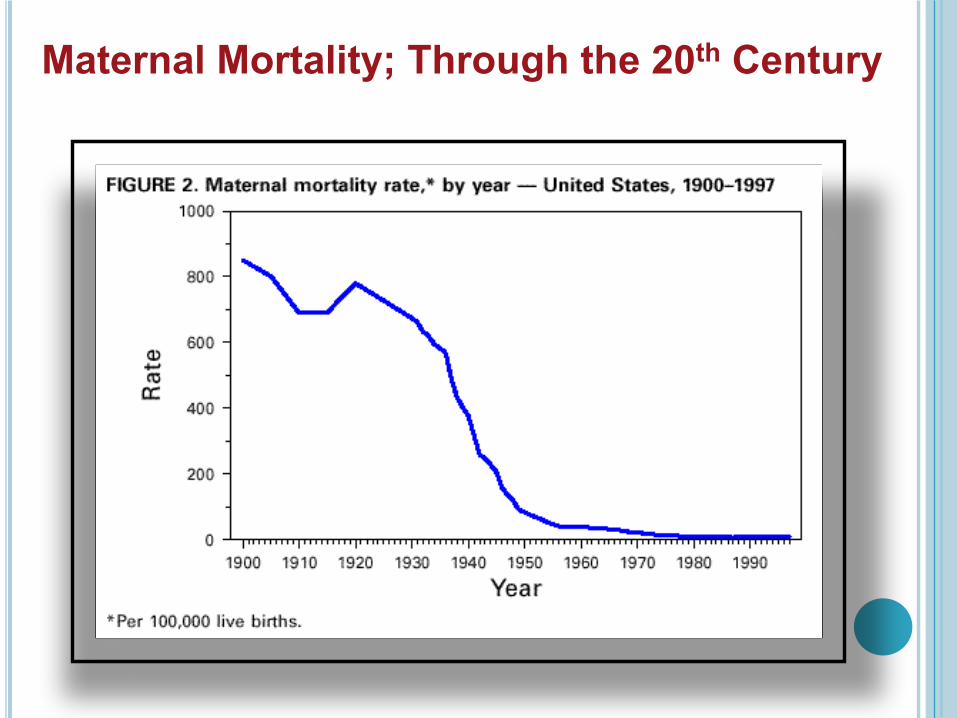
Maternal Mortality;; Through the 20th Century
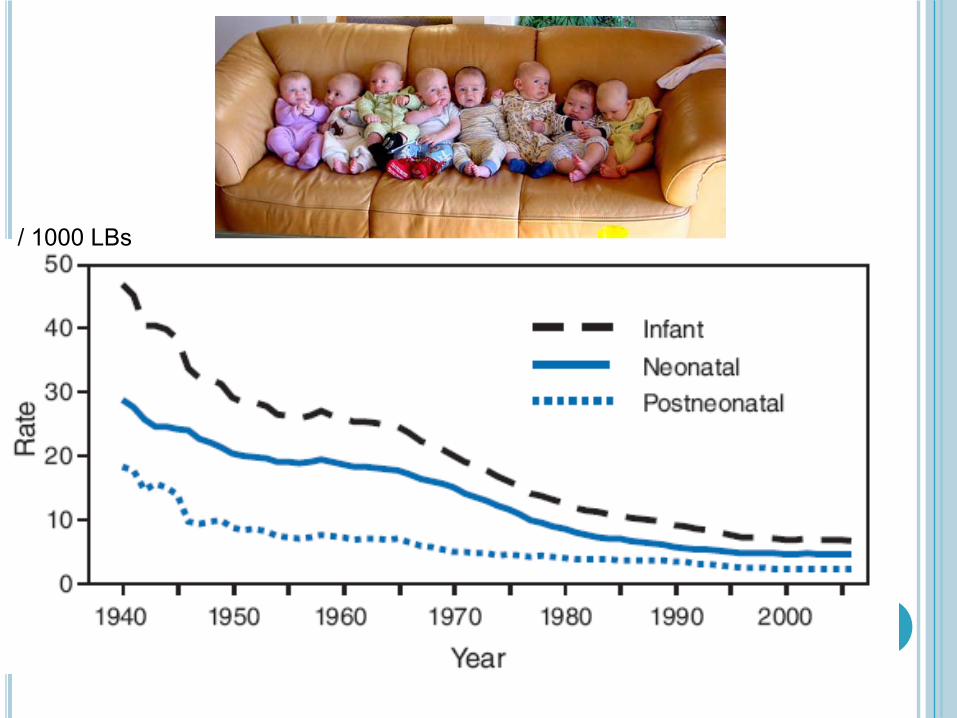
/ 1000 LBs
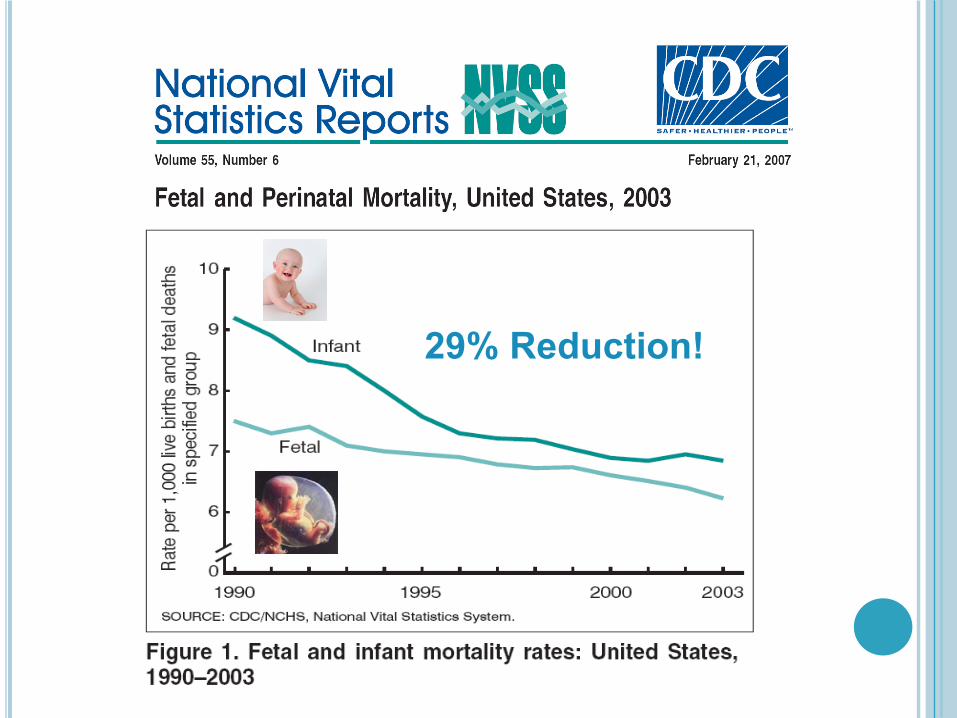
29% Reduction!
NOT TOO SHABBY!!!
WE HAVE MADE A DIFFERENCE!
Why do we need a “RADICAL PARADIGM SHIFT” for improving outcomes???

Experts: U.S. Childbirth Deaths on RiseAugust 24th, 2007
11
“U.S. women are dying from childbirth at the highest rate in decades, new government
figures show.”
U.S. ranks 41st in maternal mortalityNew report will be discussed at London meetingBy ASHLEY GOSIKCOX NEWS SERVICEWASHINGTON -- The United States ranks 41st in the world for maternal mortality, with 1 in 4,800 women dying from pregnancy complications, several major international organizations reported Friday.The U.S. was tied with the eastern European country of Belarus and just above Serbia and Montenegro. Ireland led the world with one death in 47,600, followed by Bosnia and Herzegovina and Italy. Niger had the most deaths per pregnancy at 1 in 7.
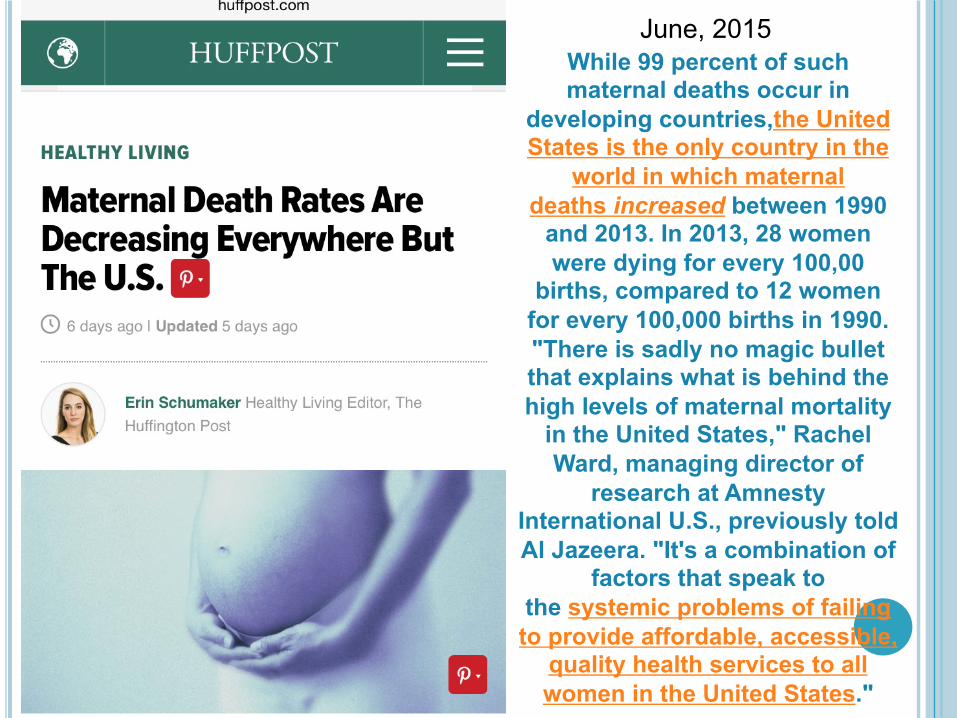
While 99 percent of such maternal deaths occur in
developing countries,the United States is the only country in the
world in which maternal deaths increased between 1990 and 2013. In 2013, 28 women were dying for every 100,00 births, compared to 12 women for every 100,000 births in 1990."There is sadly no magic bullet that explains what is behind the high levels of maternal mortality in the United States," Rachel Ward, managing director of
research at Amnesty International U.S., previously told Al Jazeera. "It's a combination of
factors that speak to the systemic problems of failing to provide affordable, accessible, quality health services to all women in the United States."
June, 2015

PREGNANCY-RELATED MORTALITY IN THEUNITED STATES;;
Pregnancy Related Mortality Ratio
16 / 100,000 Live Births
Highest Mortality compared to the past 20 years
15
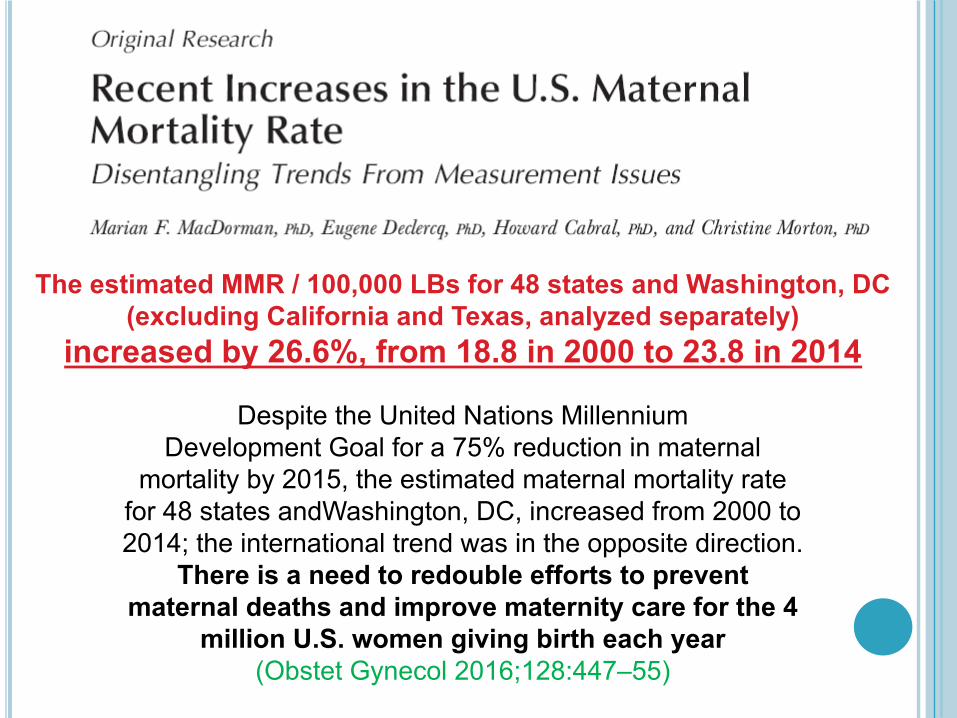
Despite the United Nations MillenniumDevelopment Goal for a 75% reduction in maternal
mortality by 2015, the estimated maternal mortality ratefor 48 states andWashington, DC, increased from 2000 to2014;; the international trend was in the opposite direction.
There is a need to redouble efforts to preventmaternal deaths and improve maternity care for the 4
million U.S. women giving birth each year(Obstet Gynecol 2016;;128:447–55)
The estimated MMR / 100,000 LBs for 48 states and Washington, DC(excluding California and Texas, analyzed separately)
increased by 26.6%, from 18.8 in 2000 to 23.8 in 2014
WHY ARE WE NOT DOING BETTER?
¢Hospitals are full of patients¢Providing “state of the art” treatments¢We are committed, dedicated professionals….
¢We update our knowledge and “give our best” to our patients
¢We have drugs, equipment, skilled providers at all levels, and consultants available
Hypothesis:SIGNIFICANT FURTHER REDUCTIONS IN ADVERSE
OUTCOME WILL COME FROM ELSEWHERE
“Reduce the risk of adverse health effects for the woman, fetus or neonate by optimizing the woman’s health and knowledge before planning and conceiving a pregnancy”
Reaffirmed 2015
Committee Opinion Number 313, September 2005The Importance of Preconception Care in the Continuum of Women's Health Care
¢Core Preconception Care Considerations: Undiagnosed, untreated or poorly controlled medical conditions
Immunization history Medication exposure Nutritional issues / BMI Family history and genetic risk / spec pops Substance use and high-risk behaviors Social issues / Intimate Partner Violence Mental health issues
Prior cesareans, avoidance of mult gest, maternal age, pre-existing “controlled” disease???
GUIDELINES FOR PERINATAL CAREACOG / AAP;; 5th ed.
¢“Preconceptional care consists of the identification of those conditions that could affect a future pregnancy or fetus and that may be amenable to intervention”
¢“ALL HEALTH CARE ENCOUNTERS during a woman’s reproductive years….should include counseling on appropriate medical care and behavior to optimize pregnancy outcomes¢KEY!

¢
Preconception Care Can Improve Perinatal Outcomes;;
TODAY
PRECONCEPTION CARE:A View From The Trenches: CASE EXAMPLES
¢Several Specific Examples: Specific Risks / Adverse outcomes Demonstrate EVIDENCED BASED Benefit of Preconception Counseling
Provide motivation and passion for incorporation into clinical management of our patients
ROADBLOCKS TO FURTHER IMPROVEMENTS INPERINATAL OUTCOMES
“VIEW FROM THE TRENCHES”
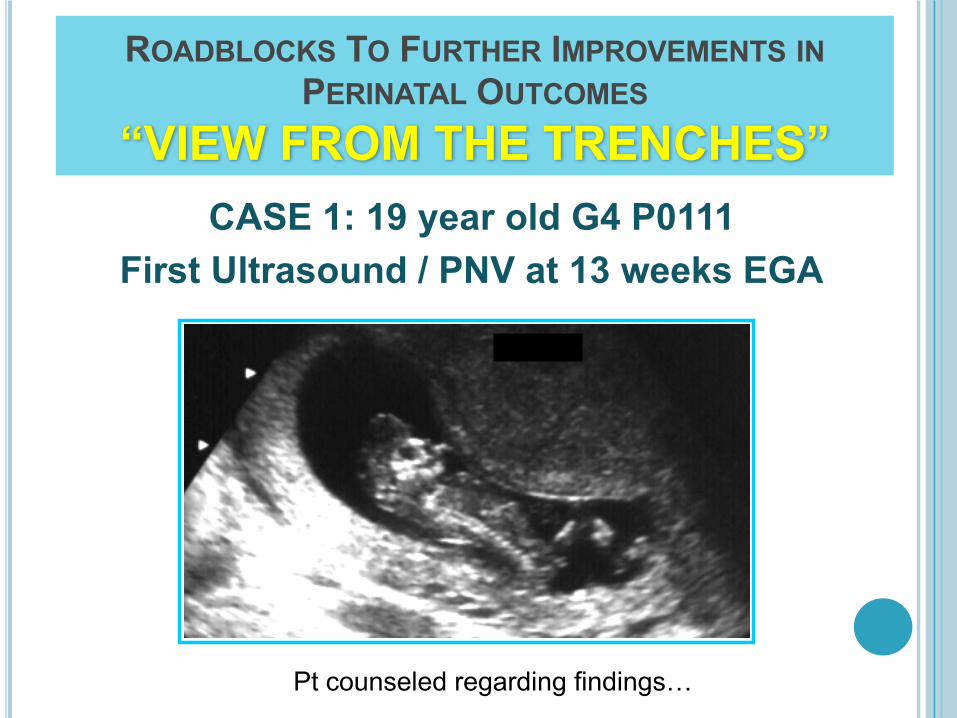
¢CASE 1: 19 year old G4 P0111 1 Spont Ab: 1 Preterm Birth at 27 weeks:
¢ 10 week NICU stay: IVH / RDS / SEPSIS
2010: presents for u/s 12 weeks;; 1st visit
Preconception Counseling: WHY?CASE 1: 19 year old G4 P0111
¢Prior Hx of PRETERM BIRTH More on that in a moment
¢Teen Opportunities for birth control, pregnancy / reproductive life-plan, other priorities above childbearing / Provision of effective contraception
¢Need to evaluate preparedness for pregnancy Normal Pap, BMI, Folic Acid intake, other health issues, etc….
ROADBLOCKS TO FURTHER IMPROVEMENTS INPERINATAL OUTCOMES
“VIEW FROM THE TRENCHES”CASE 1: 19 year old G4 P0111
First Ultrasound / PNV at 13 weeks EGA
Pt counseled regarding findings…
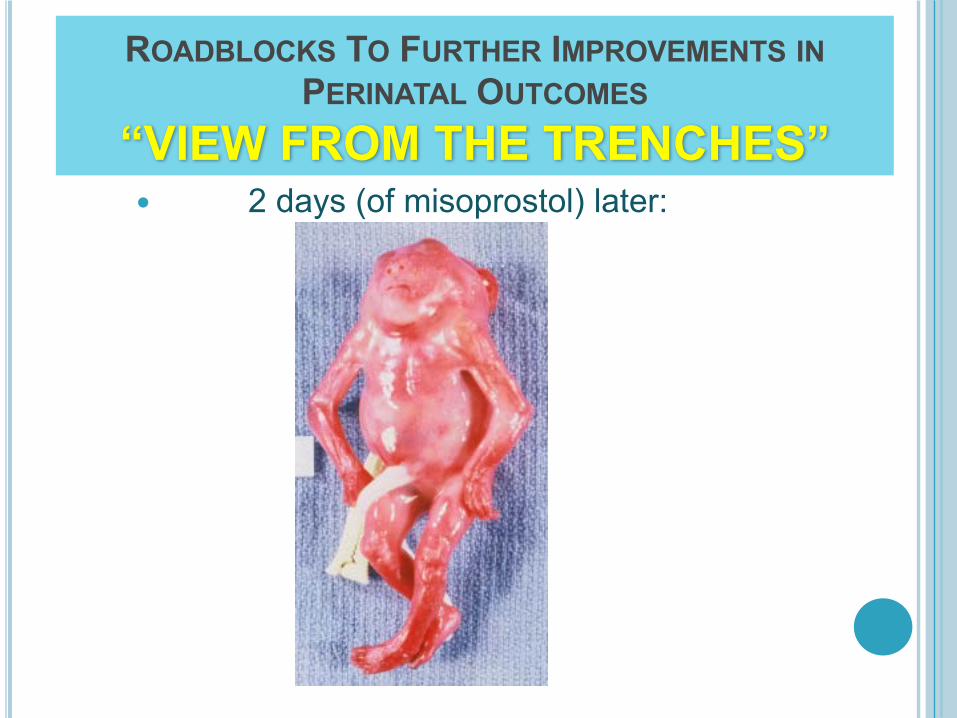
ROADBLOCKS TO FURTHER IMPROVEMENTS INPERINATAL OUTCOMES
“VIEW FROM THE TRENCHES” 2 days (of misoprostol) later:
ONE OF THE GREATEST PUBLIC HEALTH OPPORTUNITIES OF OUR TIME,
DEPENDENT UPON PRECONCEPTION CARE AND COUNSELING!
¢
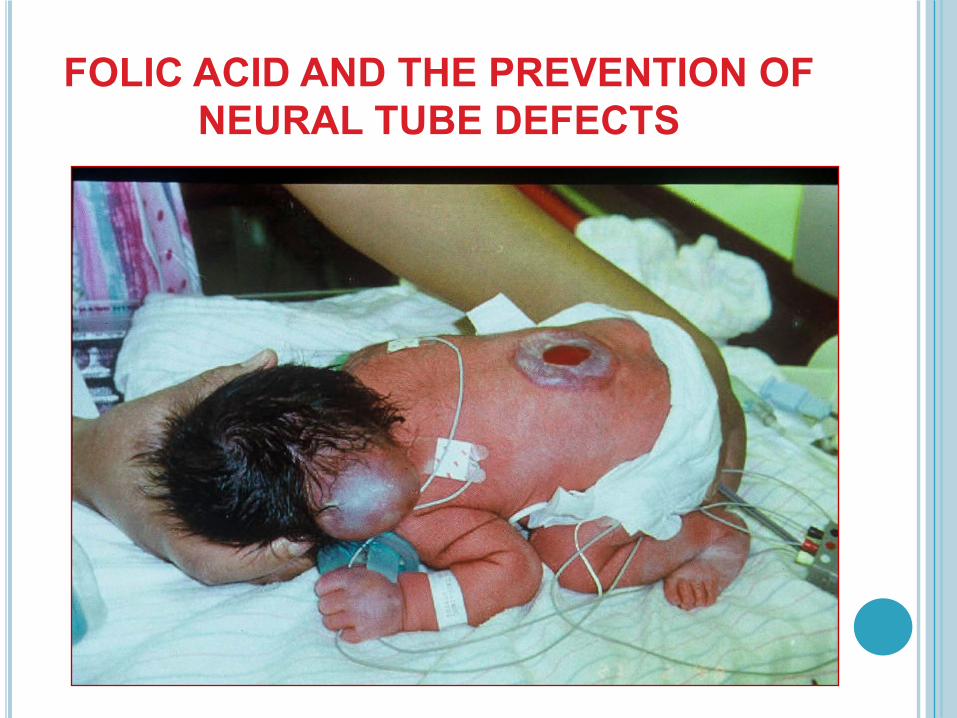
FOLIC ACID AND THE PREVENTION OF NEURAL TUBE DEFECTS
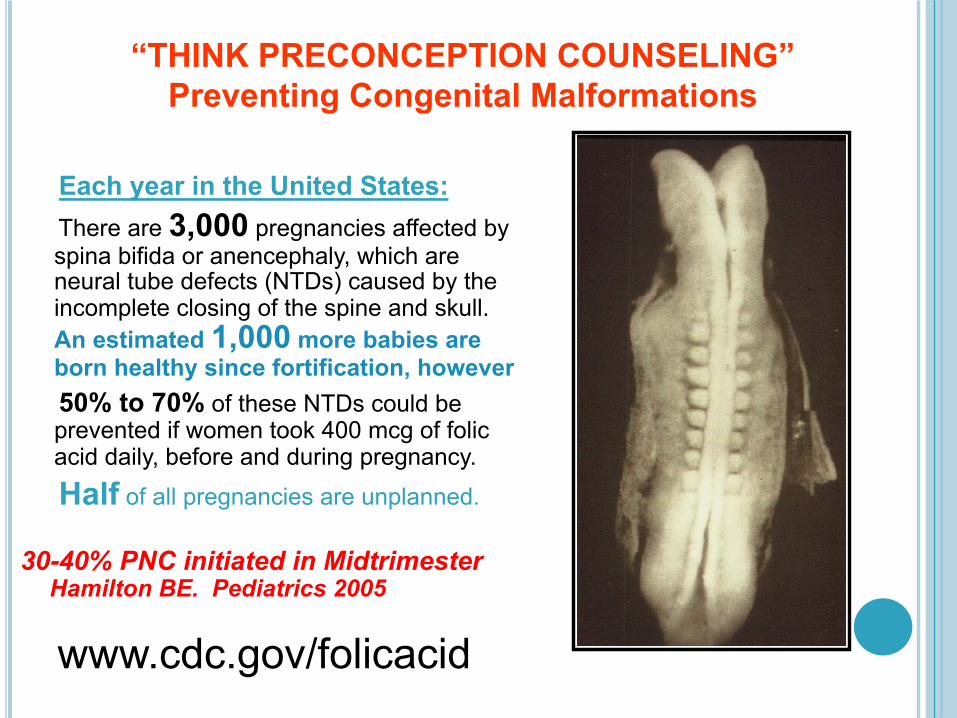
“THINK PRECONCEPTION COUNSELING”Preventing Congenital Malformations
Each year in the United States:There are 3,000 pregnancies affected by spina bifida or anencephaly, which are neural tube defects (NTDs) caused by the incomplete closing of the spine and skull. An estimated 1,000 more babies are born healthy since fortification, however50% to 70% of these NTDs could be prevented if women took 400 mcg of folic acid daily, before and during pregnancy. Half of all pregnancies are unplanned.
www.cdc.gov/folicacid
30-40% PNC initiated in MidtrimesterHamilton BE. Pediatrics 2005
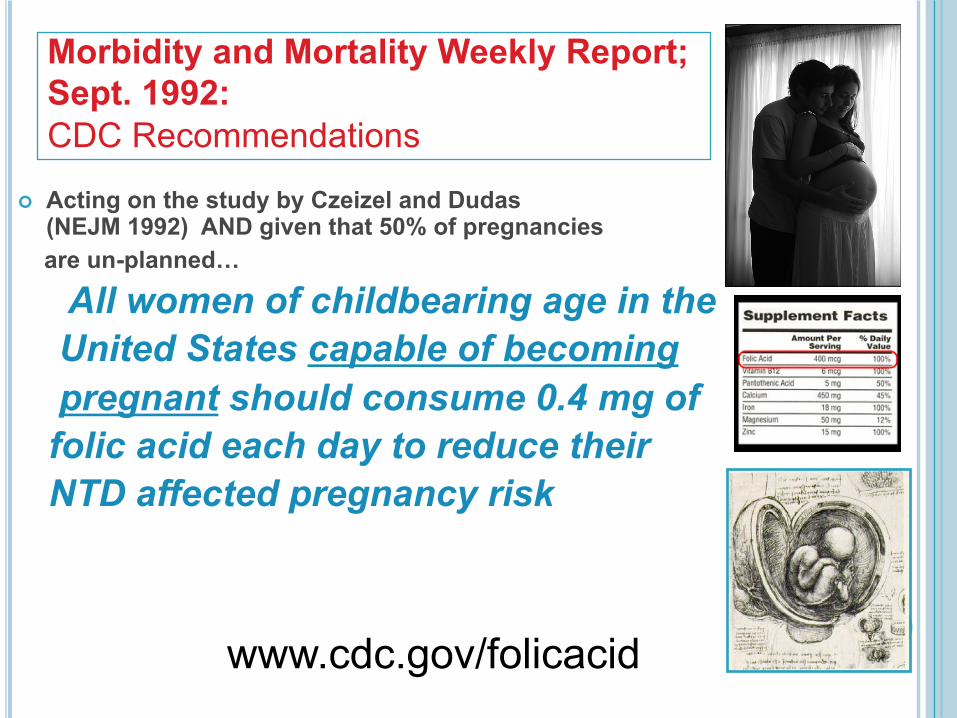
Morbidity and Mortality Weekly Report;; Sept. 1992:CDC Recommendations
¢ Acting on the study by Czeizel and Dudas (NEJM 1992) AND given that 50% of pregnancies are un-planned…
All women of childbearing age in the United States capable of becoming pregnant should consume 0.4 mg of folic acid each day to reduce their NTD affected pregnancy risk
www.cdc.gov/folicacid
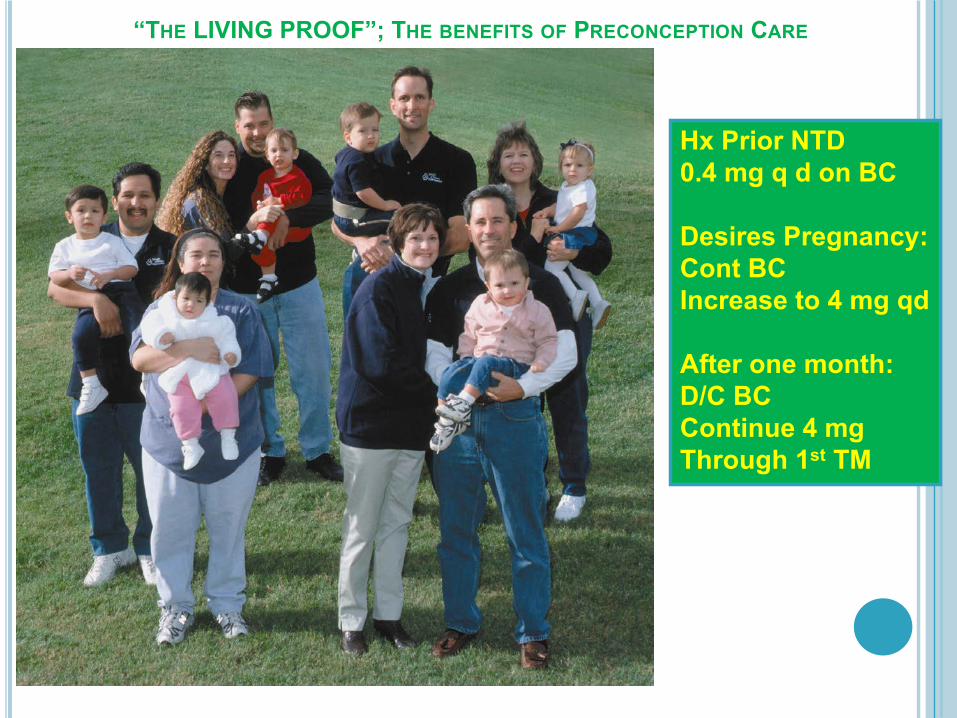
“THE LIVING PROOF”;; THE BENEFITS OF PRECONCEPTION CARE
Hx Prior NTD0.4 mg q d on BC
Desires Pregnancy:Cont BC Increase to 4 mg qd
After one month:D/C BCContinue 4 mg Through 1st TM
The Impact of Multiple Gestation
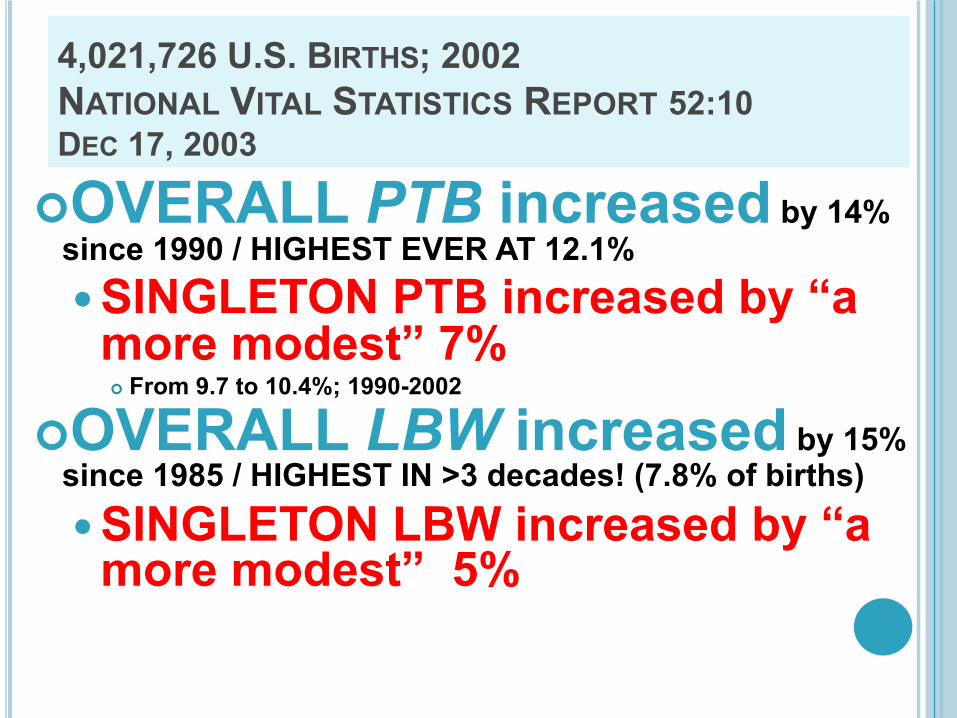
4,021,726 U.S. BIRTHS;; 2002NATIONAL VITAL STATISTICS REPORT 52:10 DEC 17, 2003
¢OVERALL PTB increased by 14% since 1990 / HIGHEST EVER AT 12.1%SINGLETON PTB increased by “a more modest” 7%¢ From 9.7 to 10.4%;; 1990-2002
¢OVERALL LBW increased by 15% since 1985 / HIGHEST IN >3 decades! (7.8% of births)SINGLETON LBW increased by “a more modest” 5%
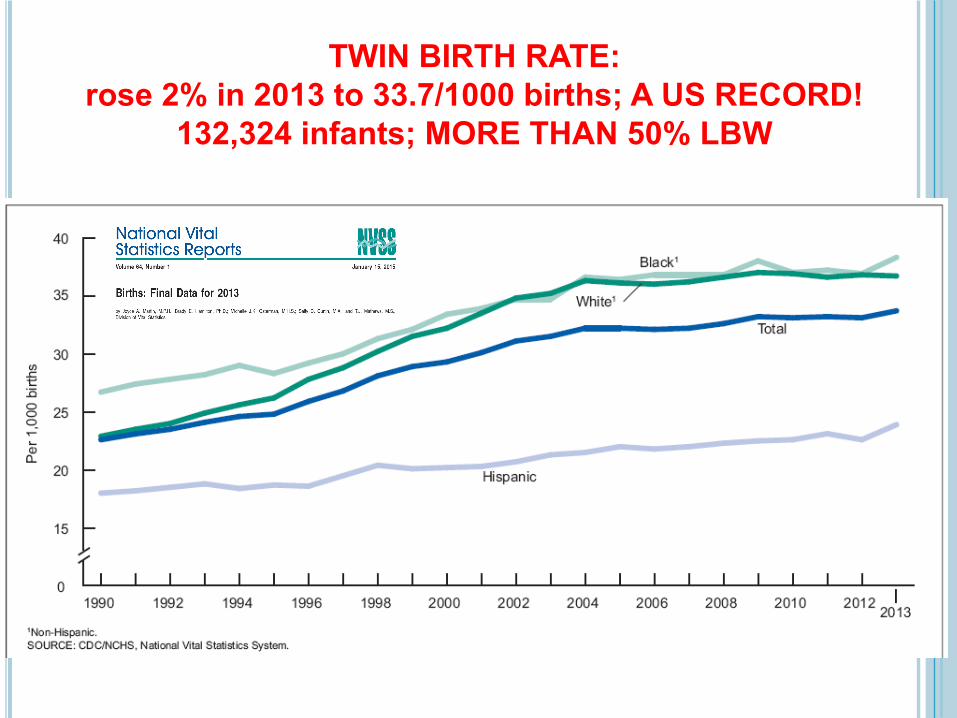
TWIN BIRTH RATE:rose 2% in 2013 to 33.7/1000 births;; A US RECORD!
132,324 infants;; MORE THAN 50% LBW
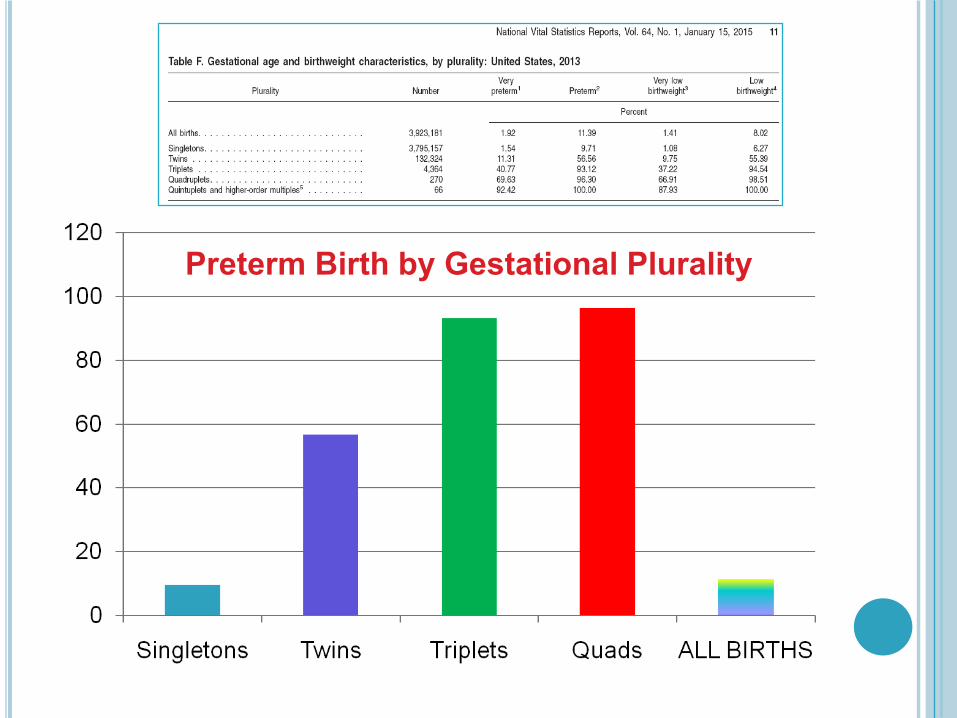
Preterm Birth by Gestational Plurality
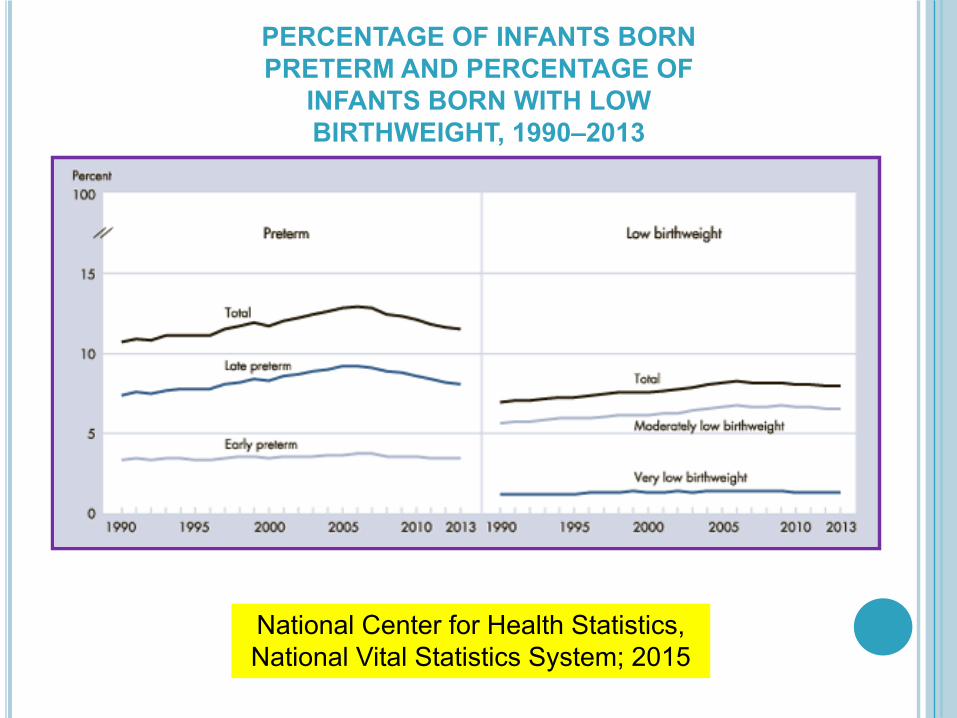
PERCENTAGE OF INFANTS BORN PRETERM AND PERCENTAGE OF
INFANTS BORN WITH LOW BIRTHWEIGHT, 1990–2013
National Center for Health Statistics, National Vital Statistics System;; 2015
THE NEED FOR PRE-PRENATAL CAREAGE MATTERS!
¢CASE 2: 47 year old G3P0101¢Hx Myomectomy x 2;; “EXTENSIVE”¢Prior PTD;; 28 weeks: Severe Preeclampsia
Classical Cesarean Delivery¢ IVF / ICSI / BLASTOCYST TRANSFER¢EARLY PRENATAL CARE VISIT
Initial BP: 159/96 Ultrasound Findings
¢Quadruplet Pregnancy¢Monochorionic Diamniotic Twin Pair
¢BMI 41
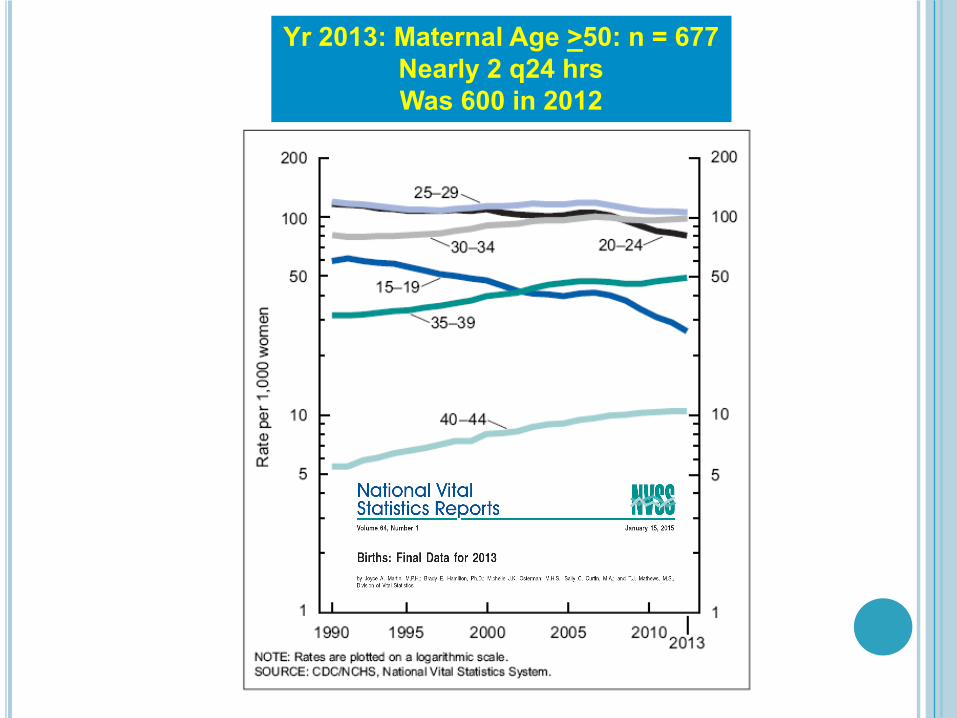
Yr 2013: Maternal Age >50: n = 677Nearly 2 q24 hrsWas 600 in 2012

Pregnancy-Related Mortality in the US: 1998 to 2005Berg CJ et al. Obstet Gynecol Dec. 2010
41
All RacesWhite
AAOther
Maternal Age
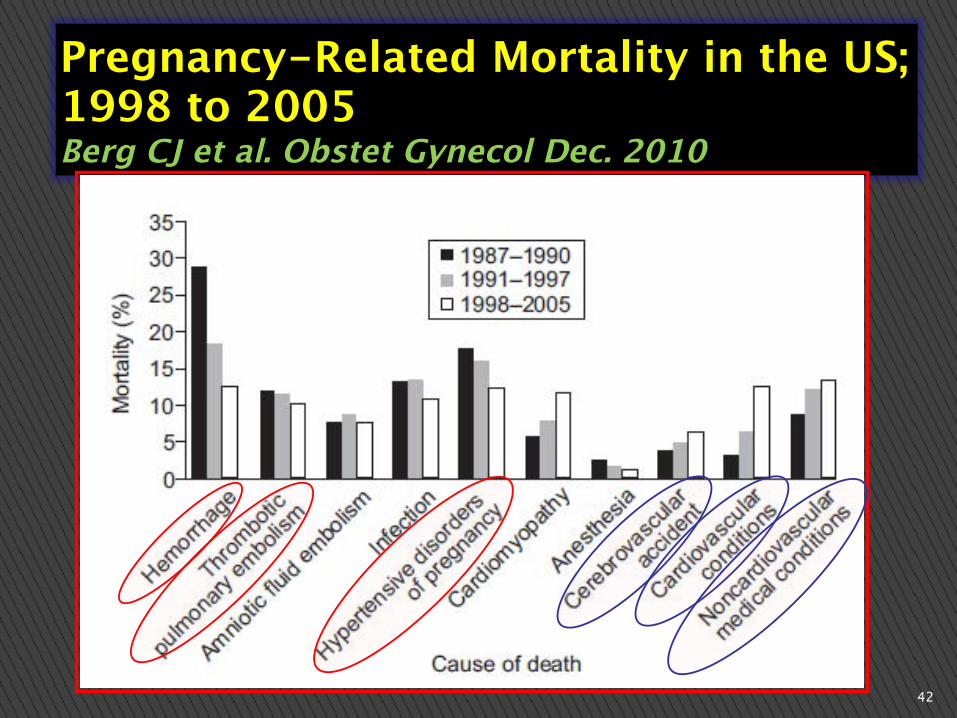
Pregnancy-Related Mortality in the US; 1998 to 2005Berg CJ et al. Obstet Gynecol Dec. 2010
42
Preconception Opportunities to Improve Perinatal Outcomes
“VIEW FROM THE TRENCHES”
¢WHY PRECONCEPTION CARE?¢ OPPORTUNITIES FOR IMPROVED OUTCOME
Review issues of AMA / Aneuploidy Review AMA Perinatal Risk Issues
¢ Preeclampsia, DM, Severe Maternal Morbidity/Mortality, Prematurity Sequelae
¢ Compounded risks of multiple gestation, anomalies w/ ART¢ Options for declining multiple embryo transfer, risks of blastocyst transfer, surrogacy/adoption options
Review risks of OBESITY / CHTN Risks of Prior Hx Preeclampsia / PTD Risks of prior uterine surgery / accreta risk
CASE 2: 47 year old G3P0101
¢ Developed TTTS (Quads A/B) at 23 weeks¢ Loss of FHTs on Quad A ¢ Hydrocephalus develops on Quad B c/w neurological injury
¢ Develops HELLP syndrome at 29 weeks¢ Mg / Steroids / Worsening Labs and BP¢ Delivery at 29 5/7 weeks¢ Neo Death of Quad B¢ Quads C/D lengthy NICU stay;; last update “doing well” with “mild CP”.
¢ Persistent maternal hypertension postpartum
CASE 2: 47 year old G3P0101
Preconception Opportunities to Improve Perinatal Outcomes
“VIEW FROM THE TRENCHES”

How can something so beautiful be “a problem”?
PRAETER NATURAM“OUTSIDE NATURE’S COURSE”
Aristotle;; On multiple gestationAristotle. De Generationes
Animalium, 4th Century BC
PRECONCEPTION COUNSELING FOR
ALL ART PATIENTS
“A Captured Audience”
¢CASE HISTORY: 28 y/o G3P1011 Class B IDDM / BMI 35 / CHTN Non-compliant with DM care Sexually active / No birth control Presents EARLY for prenatal care Complete Evaluation
¢Hgb A1C = 12 %¢ACE inhibitor
Why PRECONCEPTION CARE?¢She’s in the office at 10 weeks!¢Half the OB population is OBESE!
Preconception Opportunities to Improve Perinatal Outcomes
“VIEW FROM THE TRENCHES”

RISK OF FETAL MALFORMATIONS IN DIABETICS WITH HIGHHAEMOGLOBIN A1C VALUES IN EARLY PREGNANCYYLINEN K, ET AL. BR MED J 1984
N = 142 IDDMA1C measured before 15 wks EGAMEAN A1C 9.5%: + MalformationsMEAN A1C 8.0%: - MalformationsP < 0.001
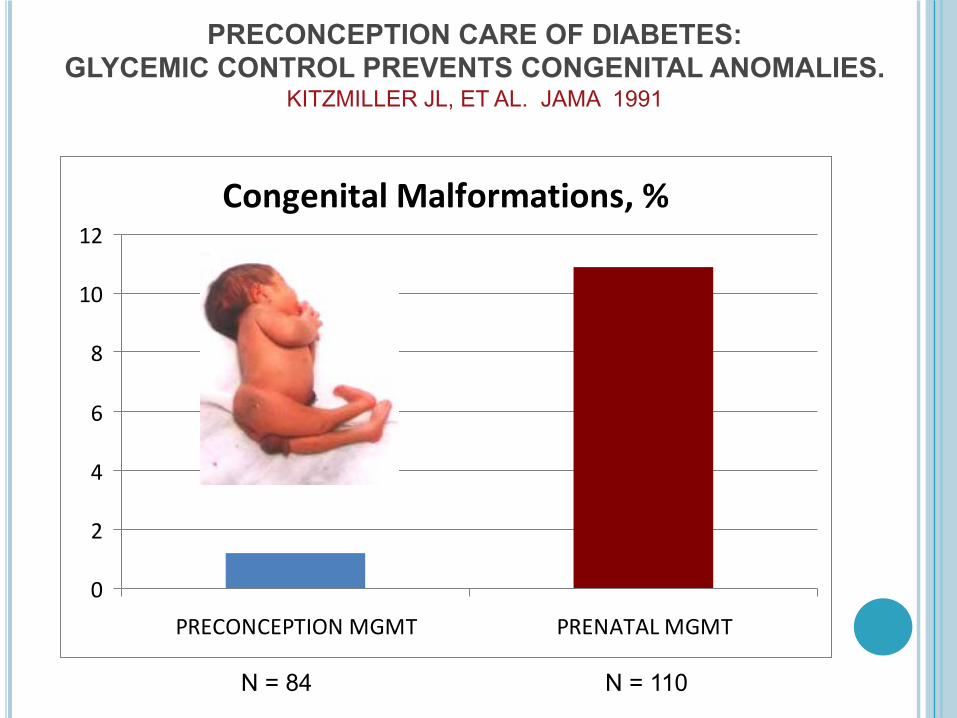
PRECONCEPTION CARE OF DIABETES: GLYCEMIC CONTROL PREVENTS CONGENITAL ANOMALIES.
KITZMILLER JL, ET AL. JAMA 1991
Congenital Malformations, %
0
2
4
6
8
10
12
PRECONCEPTION MGMT PRENATAL MGMT
N = 84 N = 110
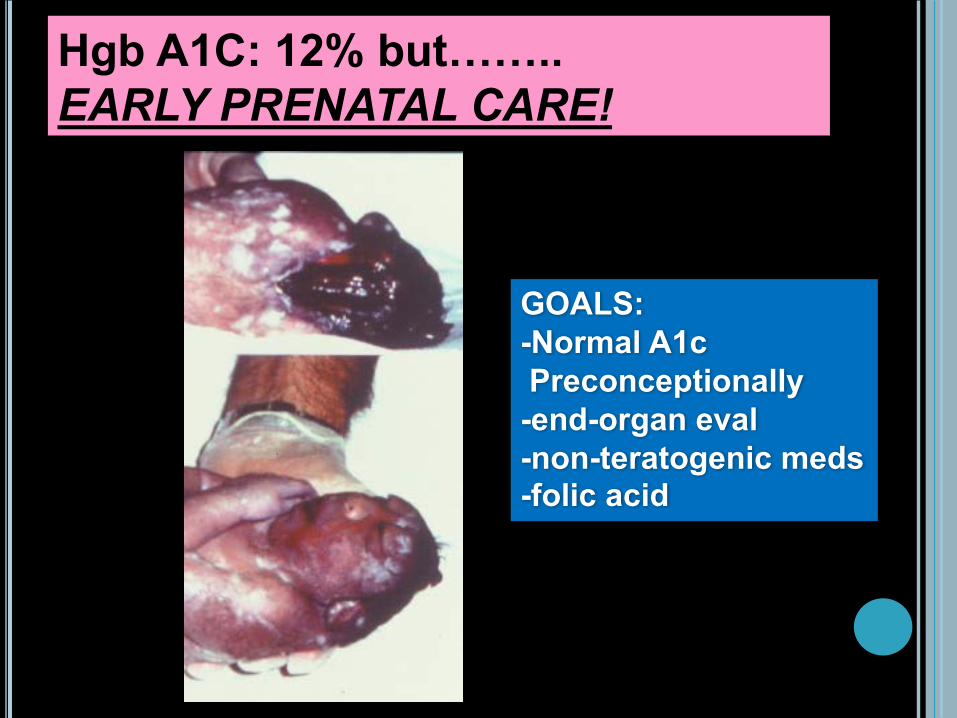
Hgb A1C: 12% but…….. EARLY PRENATAL CARE!
GOALS: -Normal A1c Preconceptionally-end-organ eval-non-teratogenic meds-folic acid
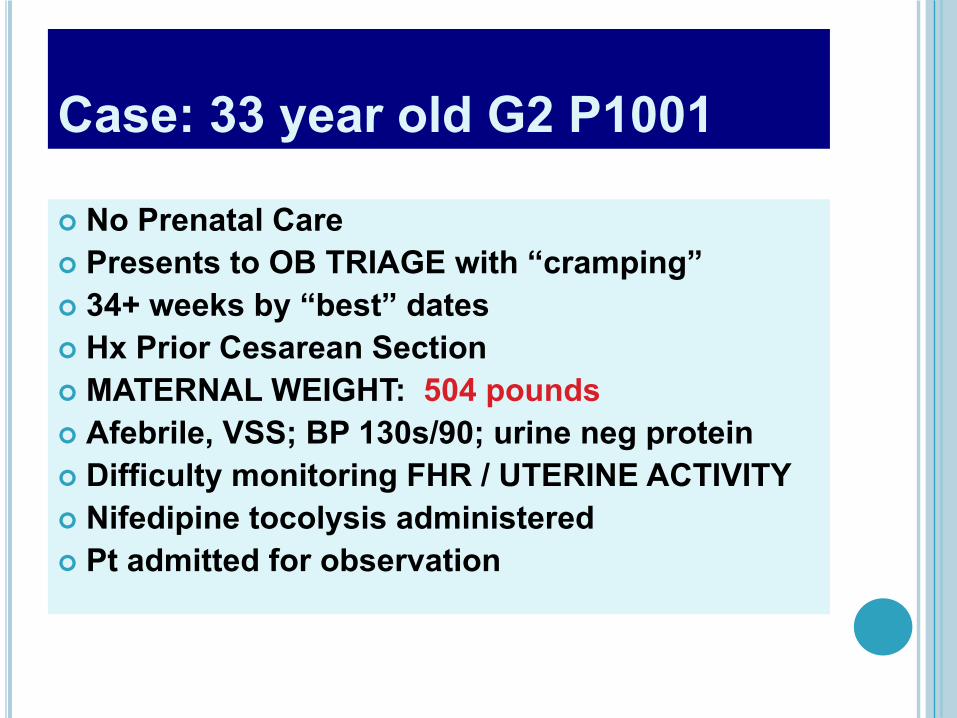
Case: 33 year old G2 P1001
¢ No Prenatal Care¢ Presents to OB TRIAGE with “cramping”¢ 34+ weeks by “best” dates¢ Hx Prior Cesarean Section¢ MATERNAL WEIGHT: 504 pounds¢ Afebrile, VSS;; BP 130s/90;; urine neg protein¢ Difficulty monitoring FHR / UTERINE ACTIVITY¢ Nifedipine tocolysis administered¢ Pt admitted for observation

Case: 33 year old G2 P1001¢ Pt admitted for observation¢ Bedside ultrasound confirms FHTs¢ Difficulty obtaining ctx tracing¢ Sudden onset HYPOTENSION: 80/47¢ Develops Maternal TACHYCARDIA;; 130s-150s and increased respiratory rate
¢ Rapid response code team called¢ Unable to get FHTs¢ Maternal Cardiac Arrest¢ CRASH PERIMORTEM SECTION CALLED
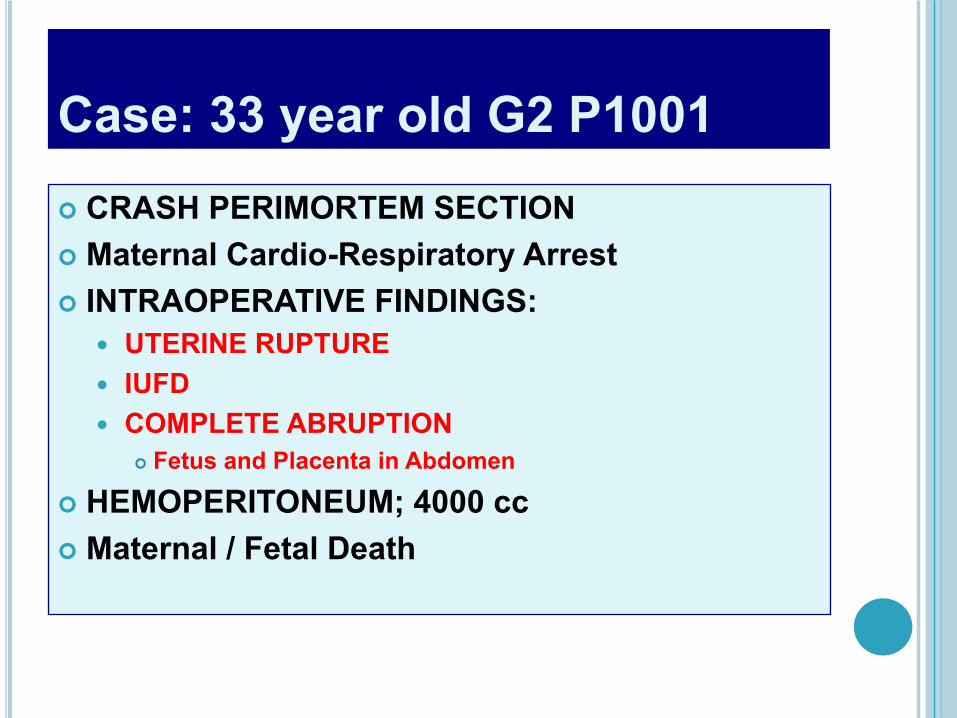
Case: 33 year old G2 P1001¢ CRASH PERIMORTEM SECTION¢ Maternal Cardio-Respiratory Arrest¢ INTRAOPERATIVE FINDINGS:
UTERINE RUPTURE IUFD COMPLETE ABRUPTION
¢ Fetus and Placenta in Abdomen
¢ HEMOPERITONEUM;; 4000 cc¢ Maternal / Fetal Death
1980 1999
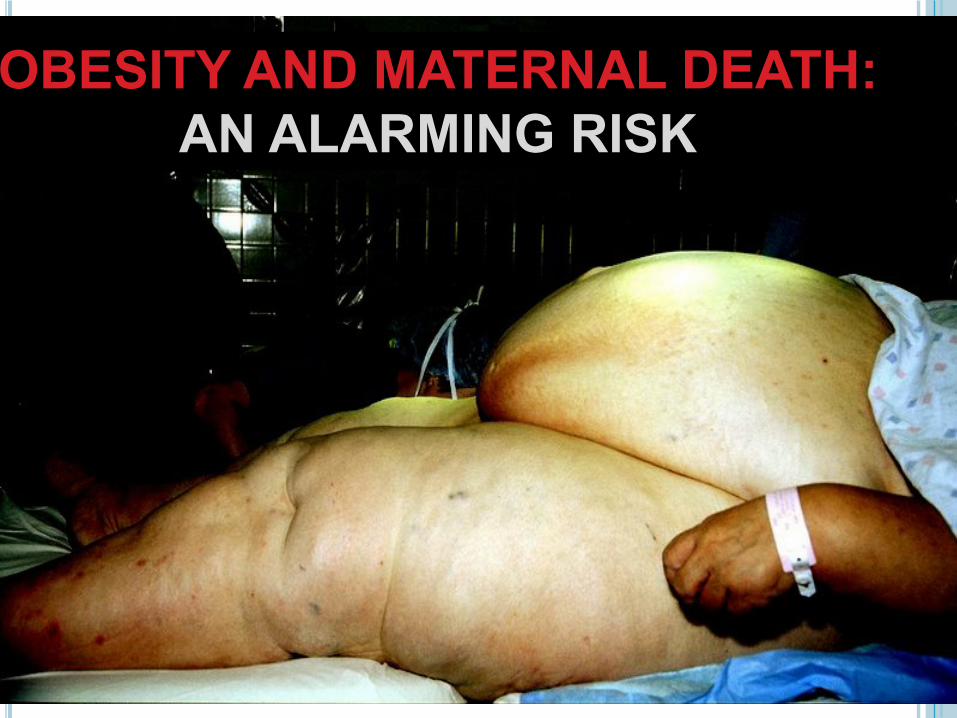
OBESITY AND MATERNAL DEATH:AN ALARMING RISK
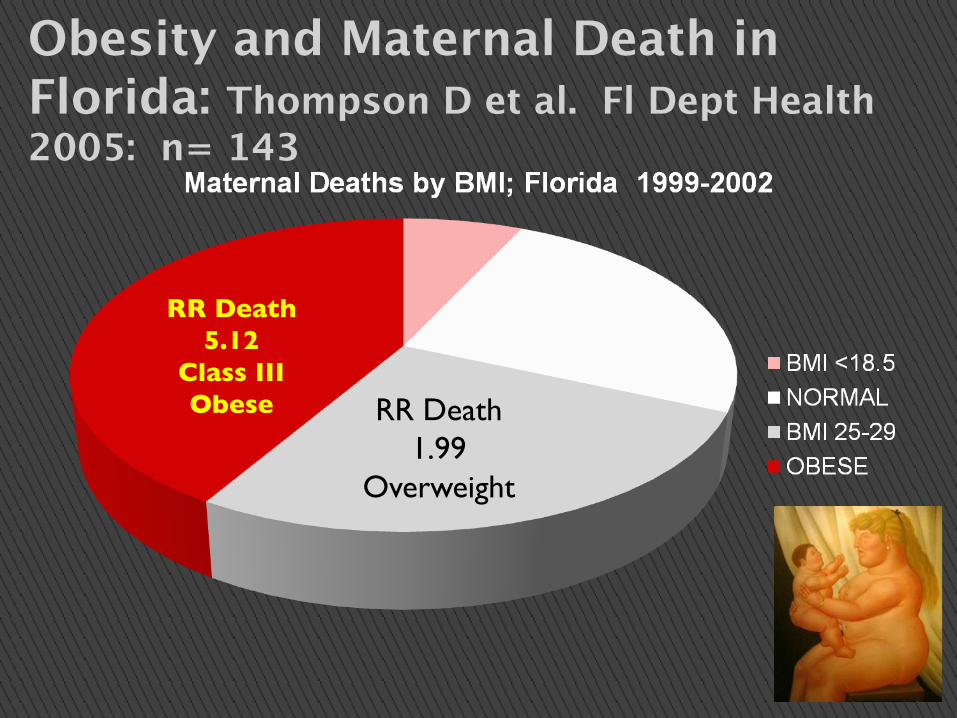
Obesity and Maternal Death in Florida: Thompson D et al. Fl Dept Health 2005: n= 143
56
RR Death 5.12
Class III Obese RR Death
1.99Overweight
A PLEA TO PROVIDERS CARING FOR OBESE WOMEN OF REPRODUCTIVE AGE
THINK PRECONCEPTION COUNSELINGRECOGNIZE PERINATAL RISKS
PROVIDE PRECONCEPTION RECs AND ASSISTANCE:ACHIEVE NORMAL BMI BEFORE PREGNANCY
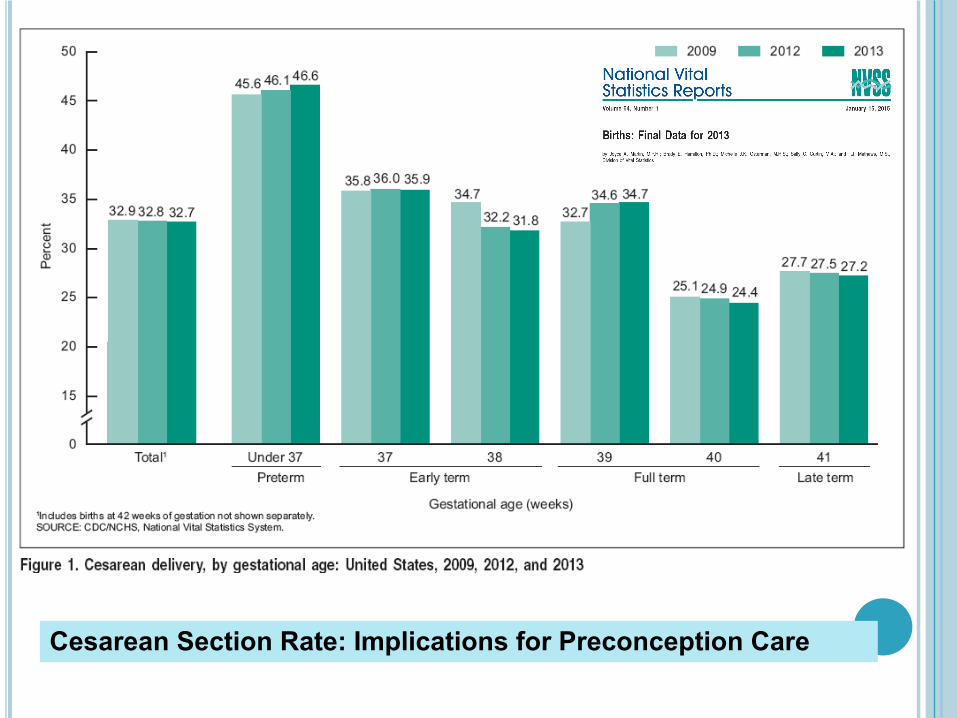
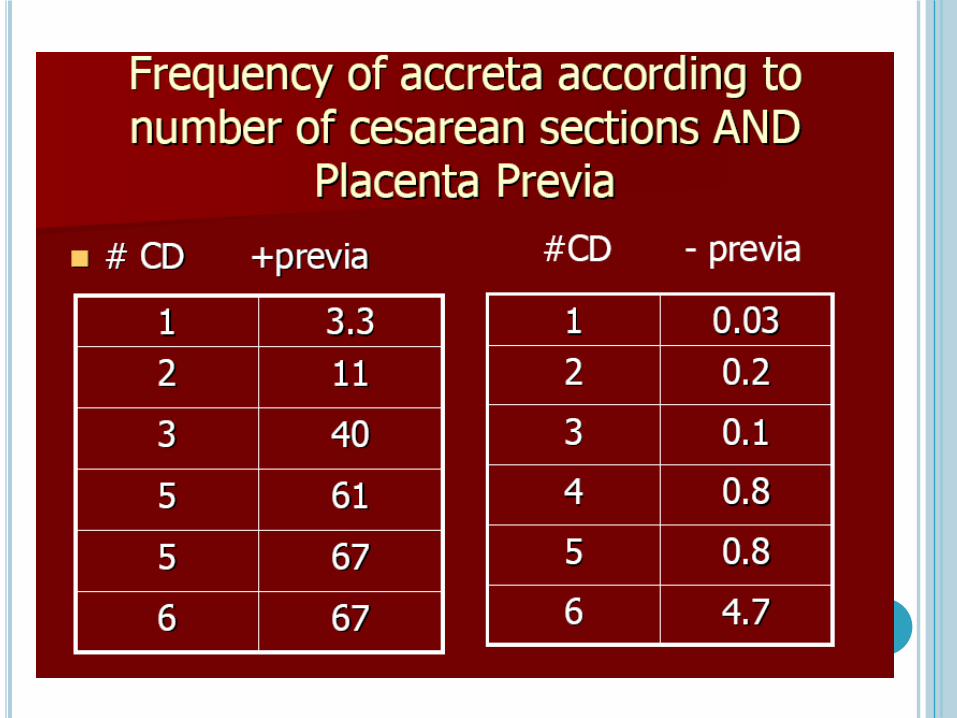
Cesarean Section Rate: Implications for Preconception Care
A PLEA TO PROVIDERS CARING FOR WOMEN OF
REPRODUCTIVE AGE: PROVIDE PRECONCEPTION
COUNSELING REGARDING RISKS OF PRIOR CESAREAN SECTION
AND PREVIA / ACCRETA

Any Woman With Placental Previa and One or More Cesarean Deliveries Should Be Evaluated and Delivered in a Tertiary Care Medical Center
Obstetrics and Gynecology;; February 2012
Obstetrics and Gynecology
Case: 29 year old G3 P0202¢ Past Obstetrical Hx:
PTD x 2 Preterm labor 1st pregnancy;; PTD 31 4/7 weeks
¢ Infant Alive and Well PROM 2nd pregnancy at 25 weeks;; PTD 28 weeks
¢ Chorio¢ CP
Current Pregnancy¢ Presents for first prenatal visit at 24 weeks EGA¢ Counseled regarding risks of recurrent PTD
¢Beyond generally recommended EGA for initiation of preventative measures………
Ultrasound performed

Case: 29 year old G3 P0202¢ Sadly
Cx length noted at first visit at 1.2 cm w/ funneling
Admittted to labor and delivery Received first course betamethasone PROM 4 hours later Fever, contractions, uterine tenderness FHR decelerations Cesarean Section 660 gm / apgars 3/6 / Grade 3 IVH
Case: 29 year old G3 P0202¢ PRECONCEPTION CARE OPPORTUNITIES¢ HX Spontaneous Preterm Birth:
Impress upon the patient the significant perinatal risks of recurrent SPTB
Review the availability of evidenced based interventions to reduce recurrent SPTB likelihood
Emphasize need for early prenatal care for timely implementation of such interventions
Evidenced Based Efficacy
Let’s Conclude on a Happier Note!Case: 25 y/o G1 P0100
¢Pt presents for consultation¢NOT PREGNANT!¢Hx of prior IUFD at 23 weeks¢No Autopsy Performed¢No Chromosomes¢At Her Postpartum Visit…....
PT: Why did this happen??? MD: “These things just happen”
Case: 25 y/o G1 P0100¢ Pt gets on Internet¢ Presents for Preconception / Post IUFD Consultation IUFD 20 wk size fetus at 23+ weeks First Trimester Dating Family Hx Thrombosis Pt with hx of ? DVT;; resolved untreated Physical Exam Unremarkable;; Normotensive
¢ LABORATORY EVALUATION Normal CBC, TSH, Chemistries, A1C Thrombophilia Assessment Evaluation for APLAb Syndrome
Case: 25 y/o G1 P0100¢Thrombophilia Assessment
Factor V Leiden Mutation¢Heterozygous
Positive Lupus Anticoagulant Positive Anticardiolipin Antibodies
¢ IgG: 60¢ IgM: 80
¢Preconception Counseling followup to review labs / implications of APLAbS AND FVL mutation
Case: 25 y/o G1 P0100¢Plan of care;; await early pregnancy and provide anticoagulation;; LMWH + LDA
¢Perinatal Course:Normal Fetal GrowthNo Preeclampsia Term Delivery
- 7 lbs, Apgars 8/9
Case: 25 y/o G2 P1101

NOT SO DARN FAST
!!!
A “PROCEDURAL PAUSE”
THAT MAKES A DIFFERENCE
ACTION PLAN¢Get PRECONCEPTION COUNSELING “on the radar”!
¢Become familiar with related literature¢Use the recognition of current pregnancy complications to discuss implications for the FUTURE….”captured audience”
¢Use the postpartum visit as an INTERCONCEPTION VISIT
¢Engage other medical colleagues in this important endeavor
¢A CHANGE in approach could be just what we need!
Obstetrics & Gynecology. April, 2015.

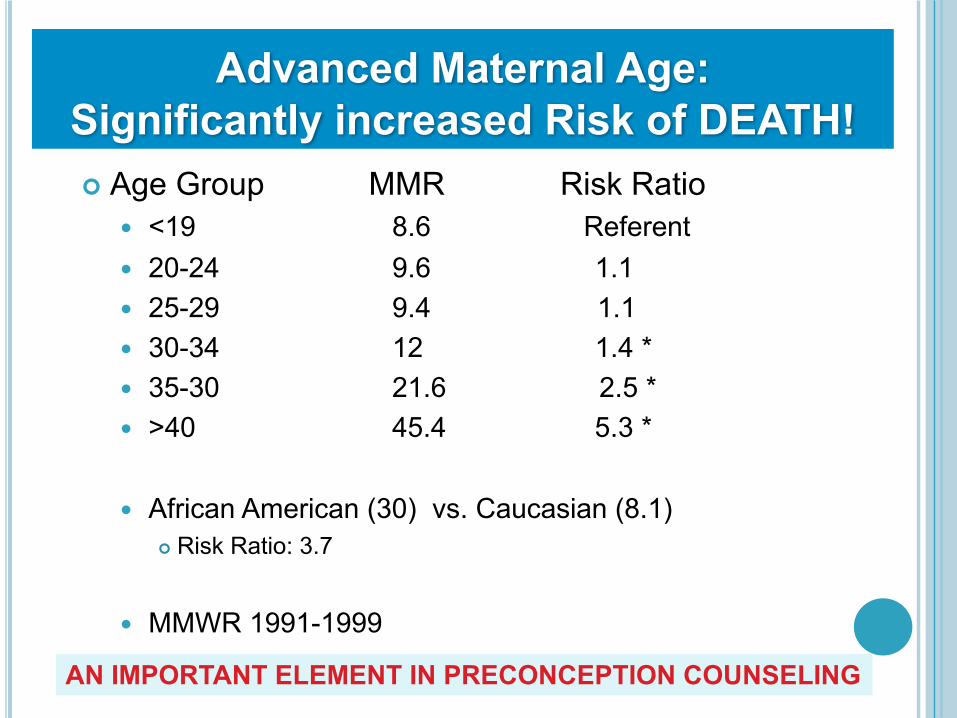
Advanced Maternal Age: Significantly increased Risk of DEATH!¢ Age Group MMR Risk Ratio
<19 8.6 Referent 20-24 9.6 1.1 25-29 9.4 1.1 30-34 12 1.4 * 35-30 21.6 2.5 * >40 45.4 5.3 *
African American (30) vs. Caucasian (8.1)¢ Risk Ratio: 3.7
MMWR 1991-1999
AN IMPORTANT ELEMENT IN PRECONCEPTION COUNSELING

Congenital Cardiac Disease• 24 y/o– Born with complex CHD– Repair at age 6 mos– NYHA I – Followed for mitral regurgitation: Mod/Severe– Asymptomatic– Never advised avoid pregnancy– Regular GYN care, paps, endometriosis treatment, LSO, laser
• Followup ECHO: Severe MR, Ejection fxn 50% (from 60%)
• Referred to cardiac surgeon for repair/replacement
Congenital Cardiac Disease• Schedules surgery and cardiac cath….• Ooops; menses late; off to the pharmacy• 6+ wk IUP• Notifies Cardiologist and CV surgeon• Goes to ob; “possible options”• Cardiologist tasks RN via email with telling pt “unfortunately
our recommendation is to terminate ASAP” • RN refuses J• Cardiologist calls pt:– Ob knows nothing of your heart– You must terminate
• Pt terminates pregnancy
Congenital Cardiac Disease• Pt gets call from CV Surgeon 2 da prior to surgery• “your too complicated for me”; surgery is cancelled….I’m
sending you to……• Pt goes to referral
– No meds? No Feeling fine? Like I always have– Hmmmmm; lets get an ECHO
• Echo with EF 60% and mod/severe MR• Cardiology team to pt:
– “you don’t need surgery”
• 8 mos later– Robotic hysterecotmy for stage IV endometriosis with intractable
pain
• Sadly, a lost childbearing opportunity• Never provided with a multidisciplinary approach to discuss
pregnancy issues, despite life-‐long “care”
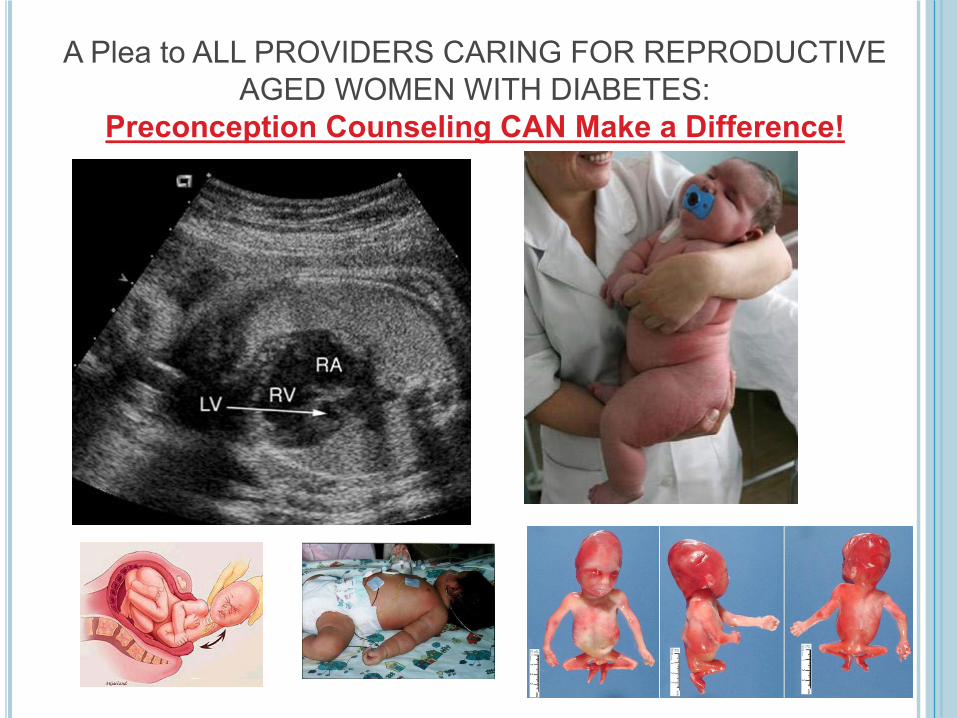
A Plea to ALL PROVIDERS CARING FOR REPRODUCTIVE AGED WOMEN WITH DIABETES:
Preconception Counseling CAN Make a Difference!
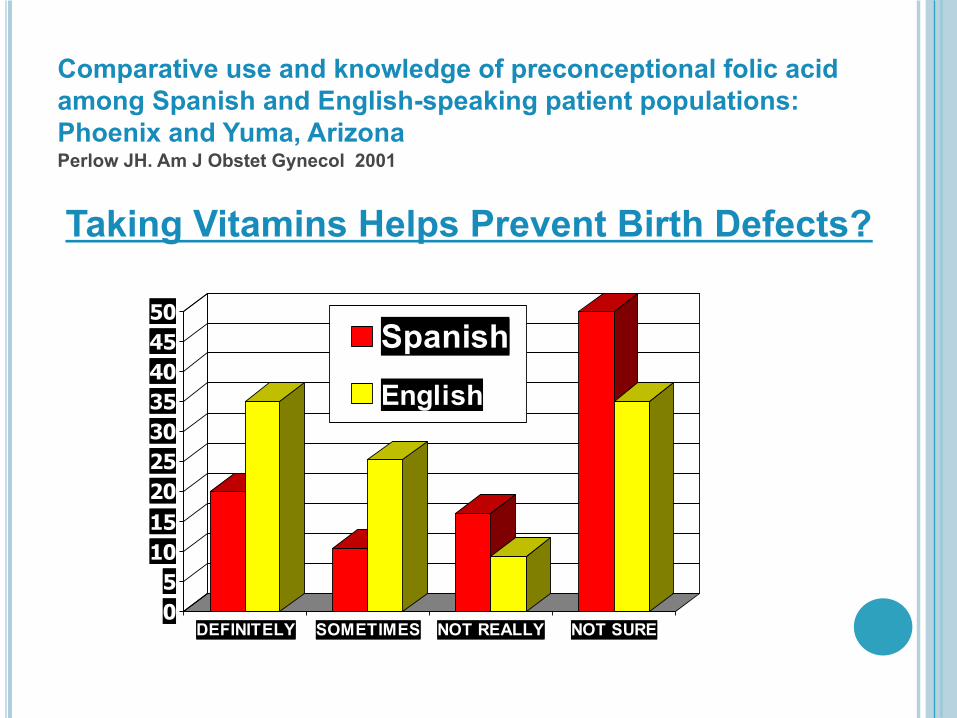
Comparative use and knowledge of preconceptional folic acid among Spanish and English-speaking patient populations: Phoenix and Yuma, ArizonaPerlow JH. Am J Obstet Gynecol 2001
05101520253035404550
DEFINITELY SOMETIMES NOT REALLY NOT SURE
SpanishEnglish
Taking Vitamins Helps Prevent Birth Defects?