Embed Size (px)
DESCRIPTION
An approach to vertigo from a medical point of view
Citation preview

Approach to vertigoAmina TighiltAsma MohammadLubna AhmadMariam Waleed

Introduction • Vertigo is a symptom, not a diagnosis.
• It arises because of asymmetry in the vestibular system due to damage to or dysfunction of the labyrinth, vestibular nerve, or central vestibular structures in the brainstem.
• In most cases history and examination distinguish between central and peripheral etiologies identifying those patients that require urgent diagnostic evaluation.

History taking A. Chief complain:• Vertigo
Description: • Patient can interpret it as self motion or motion of the environment. • It can be spinning , swaying , or tilting.• Not all patients are able to describe their vertigo in such concrete terms. • Vague dizziness, imbalance, or disorientation may eventually prove to be due to
a vestibular problem.
Time duration• (seconds – minutes – hours – days )• Central adapts within days to weeks , constant dizziness up to months is not
vestibular.

Attacks are they single or recurrent Aggravating and provoking factors
• All causes are worse with head movements , if not then it’s a different type of dizziness.
• BPPV is provoked with certain movements and posture .(ex , rolling over bed, neck extension).
• Vertigo aggravated with coughing , sneezing , exertion , loud noises should rise a suspicion of perilyphmatic fistula.
Associated symptoms• Nausea and vomiting : typical with acute attacks unless its mild and brief like in
BPPV.• Postural instability: vertigo of central origin impairs gait and posture to a greater
degree than does vertigo of peripheral origin.• Auditory symptoms : hearing loss , tinnitus.• Ask about recent viral symptoms
ROSDiplopia , dysarthria , dysphasia, numbness stroke Neurological symptoms MSHeadaches , photopia migrainoiues vertigo
B. Past Medical and Surgical History:• Migraine • Stroke risk factors • DM , HTN , Hx of vascular disease
• History of trauma • Previous ear surgery
C. Drug history :• Cisplatin , aminoglycosides vestibular toxicity• Phenytoin cerebellar toxicity
D. Family history • A family history of vertigo may suggest a rare hereditary channelopathy.
E. Social History
Physical examination Differentiate between central and peripheral vertigo:
• Nystagmus:o Freznel lenseso Dix Hallpikeo Head thrusto Head shakingo Caloric testing
• Gait instability• Rinne and Webber tests• Other neurologic signs
Diagnostic testing The need for diagnostic testing in vertigo is a clinical decision
made based on certain patient characteristics. Examples of indications for neuroimaging:
Findings in history and examination suggestive of a central cause(new onset headache, focal neurological signs and symptoms, vertical nystagmus) Unilateral vertigo of gradual progression to rule out a vestibular shwanommaMultiple risk factors of stroke or co-morbiditiesLack of response to conservative treatment

Tests to rule out central causes: MRI or MRA CT scan
Tests to assess vestibular function and ocular motility: Electronystagmography video nystagmography
Vestibular evoked myogenic potentials (VEMPs) are a new means of assessing otolith function
Audiometry Pure tone audiometry Speech audiometry( SRT and speech discrimination test) Impedance audiometry( tympanogram)
Brainstem auditory evoked potentials (BAEPs) have a 90 to 95 percent sensitivity for detecting acoustic neuromas.
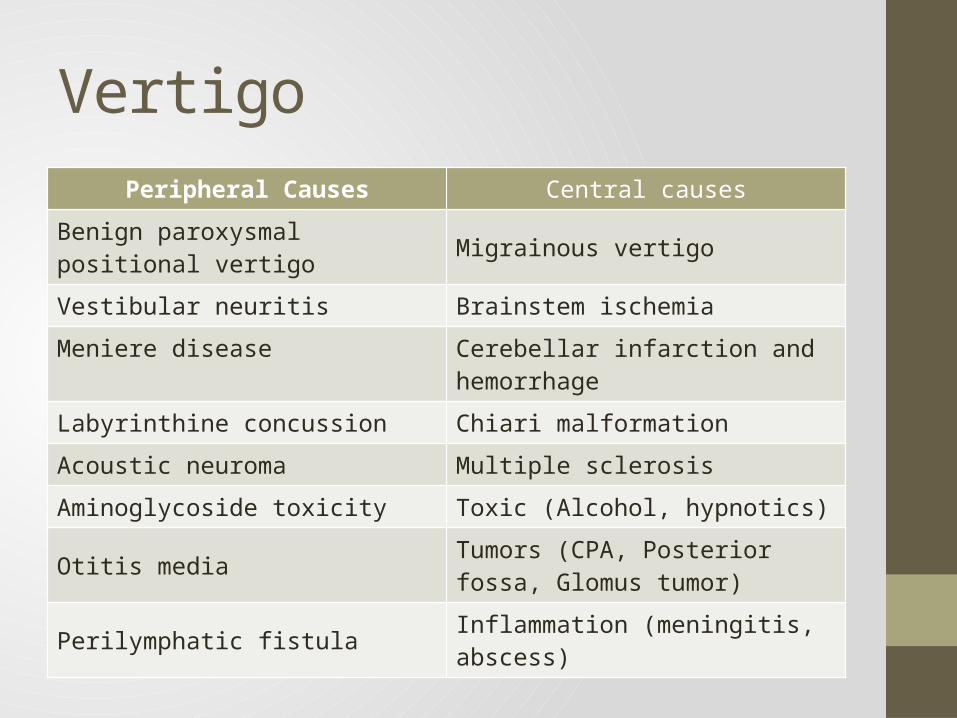
VertigoPeripheral Causes Central causes
Benign paroxysmal positional vertigo Migrainous vertigoVestibular neuritis Brainstem ischemiaMeniere disease Cerebellar infarction and hemorrhageLabyrinthine concussion Chiari malformation
Acoustic neuroma Multiple sclerosis
Aminoglycoside toxicity Toxic (Alcohol, hypnotics)
Otitis media Tumors (CPA, Posterior fossa, Glomus tumor)
Perilymphatic fistula Inflammation (meningitis, abscess)
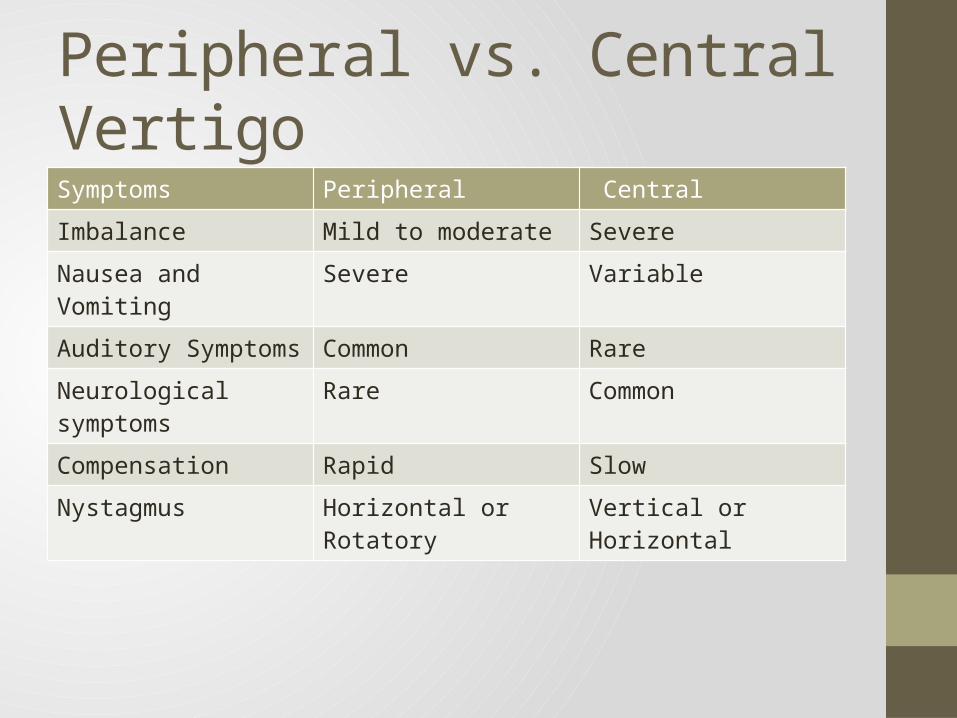
Peripheral vs. Central Vertigo Symptoms Peripheral Central
Imbalance Mild to moderate Severe
Nausea and Vomiting Severe Variable
Auditory Symptoms Common Rare
Neurological symptoms Rare Common
Compensation Rapid Slow
Nystagmus Horizontal or Rotatory Vertical or Horizontal
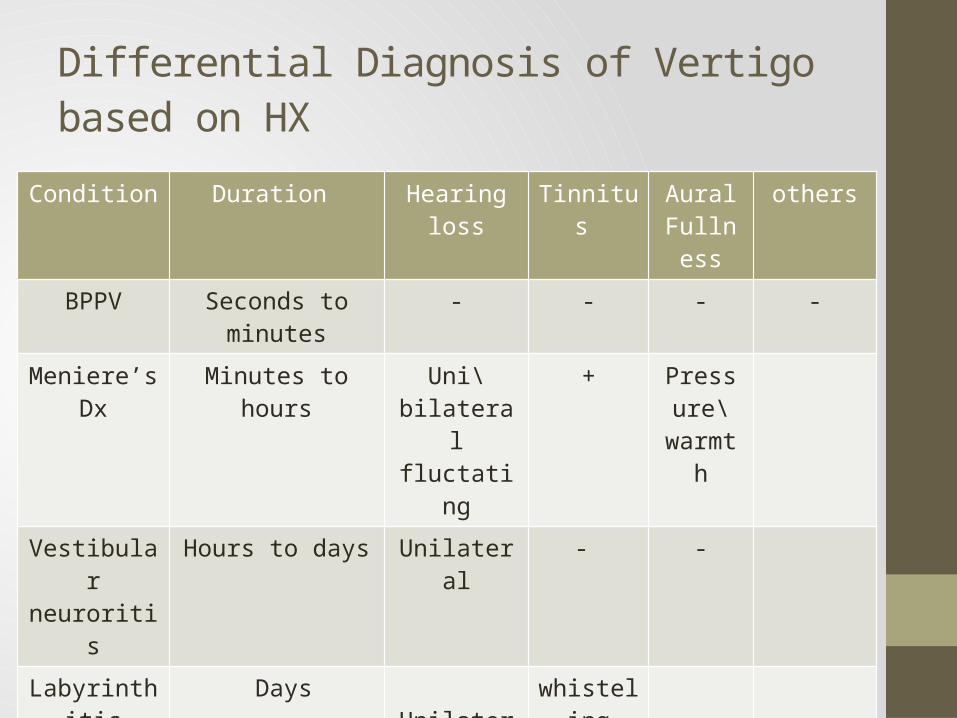
Differential Diagnosis of Vertigo based on HX
Condition Duration Hearing loss Tinnitus Aural Fullness
others
BPPV Seconds to minutes - - - -
Meniere’s Dx Minutes to hours Uni\bilateral fluctating
+ Pressure\
warmthVestibular neuroritis
Hours to days Unilateral - -
Labyrinthitis Days Unilateral whisteling

Benign Paroxysmal Positional Vertigo (BPPV)• Definition: acute attacks of transient vertigo lasting seconds to
minutes initiated by certain head positions.• Etiology: due to canalithiasis or cupulolithiasis• Hx, Examination, Dix-Hallpike Positional Testing• Management: • Reassure patient that process resolves spontaneously• Particle repositioning maneuvers• Epley maneuver • Brandt-daroff exercises (performed by patient)• Anti-emetics for nausea/vomiting• Drugs to suppress the vestibular system delay eventual recovery
and are therefore not used

Meniere's Disease• Definition: episodic attacks of tinnitus, hearing loss, aural fullness, and vertigo lasting
minutes to hours• Proposed Etiology: inadequate absorption of endolymph leads to endolymphatic hydrops
(over accumulation) that distorts the membranous labyrinth• Treatment
• Acute management may consist of bed rest, antiemetics, antivertiginous drugs [e.G. Betahistine and low molecular weight dextrans (not commonly used)
• Long term management may include:Medical:• Low salt diet, diuretics (e.G. Hydrochlorothiazide, triamterene, amiloride)• Sere'" prophylactically to decrease intensity of attacks• Local application of gentamicin to destroy vestibular end-organ, results in complete
SNHLSurgical:• Selective vestibular neurectomy or transtympanic labyrinthectomy• Vestibular implants have recently been introduced, experimentally• Must monitor opposite ear as bilaterality occurs in 35% of cases

Vestibular Neuronitis• Acute onset of disabling vertigo often accompanied by nausea,
vomiting and imbalance withouthearing loss that resolves over days leaving a residual imbalance that lasts days to weeks.
• Treatment:• Treatment• , and Acute phase:• Bed rest, vestibular sedatives (gravole), diazepam• Convalescent phase:• Progressive ambulation especially in the elderly• Vestibular exercises: involve eye and head movements, sitting,
standing and walking
Labyrinthitis
• Acute infection of the inner ear resulting in vertigo and hearing loss• Causes
• May be serous (viral) or purulent (bacterial)• Occurs as a complication of acute and chronic otitis media, bacterial meningitis,
cholesteatoma,• And temporal bone fractures• Bacterial: S. Pneumoniae, H, influenzae, M. Catarrhalis, P. Aeruginosa, P. Mirabilis• Viral: rubella, CMV, measles, mumps, varicella zoster
• Clinical features• Sudden onset of vertigo, nausea, vomiting, tinnitus, and unilateral hearing loss, with
no• Associated fever or pain• Meningitis is a serious complication
• Investigations• Cthead• If meningitis is suspected: lumbar puncture, blood cultures
• Treatment• Treat with IV antibiotics, drainage of middle ear ± mastoidectomy
Reference:• Furman, JM. . Approach to the patient with vertigo. In:
UpToDate, Aminoff, MJ (Ed), UpToDate, Waltham, MA, 2013. Retrieved from: http://www.uptodate.com/contents/approach-to-the-patient-with-vertigo





![Vertigo and Imbalance - Dergisijns.dergisi.org/pdf/pdf_JNS_32.pdf · J.Neurol Sci [Turk] WHAT IS VERTIGO ? a. Vertigo is an illusion of rotation. It is due to unequal neural activity](https://img.dokumen.tips/doc/110x75/5a856d7e7f8b9a001c8c5181/vertigo-and-imbalance-sci-turk-what-is-vertigo-a-vertigo-is-an-illusion-of.jpg)























