Embed Size (px)
Citation preview
Approach to HeadacheDR. AMAL ALKHOTANI
FRCPC NEUROLOGY, EPILEPSY
Headache
Headache is one of the 10 most common reasons for health care visits in USA.
It also account for 4.5% of ER visits.

Types of headache
Primary :-benign headache syndromes in which there are no structural cause for the headache e.g. migraine, tension, cluster.
Secondary :-headache is a symptom of underlying disease e.g. tumor.
Careful evaluation is required to recognize secondary causes of headache.
Secondary Headache
Headache attributed to head or neck trauma
Headache attributed to cranial or cervical vascular disorder
Headache attributed to nonvascular, noninfectious intracranial disorder
Headache attributed to a substance or its withdrawal
Headache attributed to infection
Headache attributed to disturbance of homeostasis
Headache or facial pain attributed to disorder of cranium, neck, eyes, ears, nose, sinuses, teeth, mouth, or other facial or cranial structures
Headache attributed to psychiatric disorder
Cranial neuralgias and central causes of facial pain
Other headache, cranial neuralgia, central or primary facial pain
History
Types of headaches.
Onset of headaches.
Frequency & periodicity of episodic headaches.
Temporal profile.
Time of day & precipitating factors.
Location.
Quality & severity.
Aura & accompanying symptoms.
Aggravating factors.
Family history of headaches.
Other medical or neurological problems.

68 year old female present to ER with headache.
What historical points will let you worry about this headache?
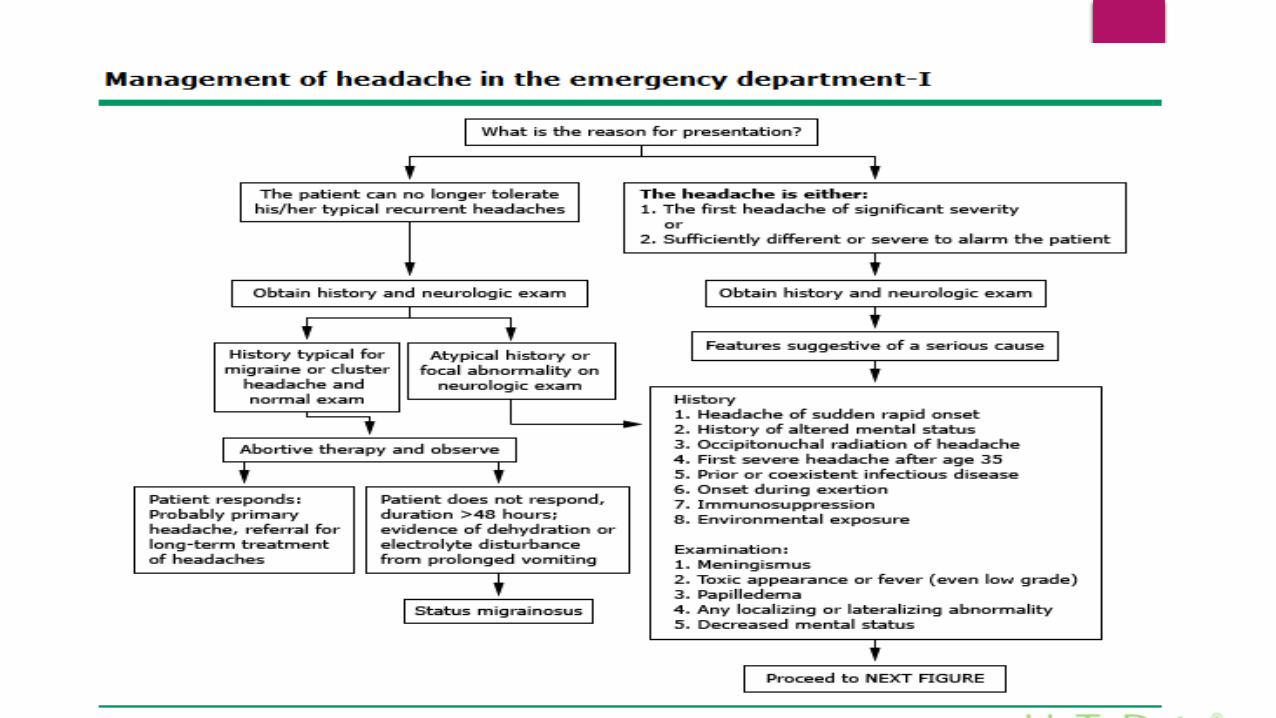
Red Flags For Worrisome Headaches
New onset headache or onset of new type of headache or change of preexisting headache.
Progressive worsening headache.
Worst ever pain.
Age > 50.
Abrupt onset headache.
Headache initiated by exertion or valsalva.
Head trauma.
Neurological symptoms & signs.
Systemic symptoms & signs.
Secondary risk factors.
Examination
Vital signs
General appearance
Meningeal signs
Full neurological examination
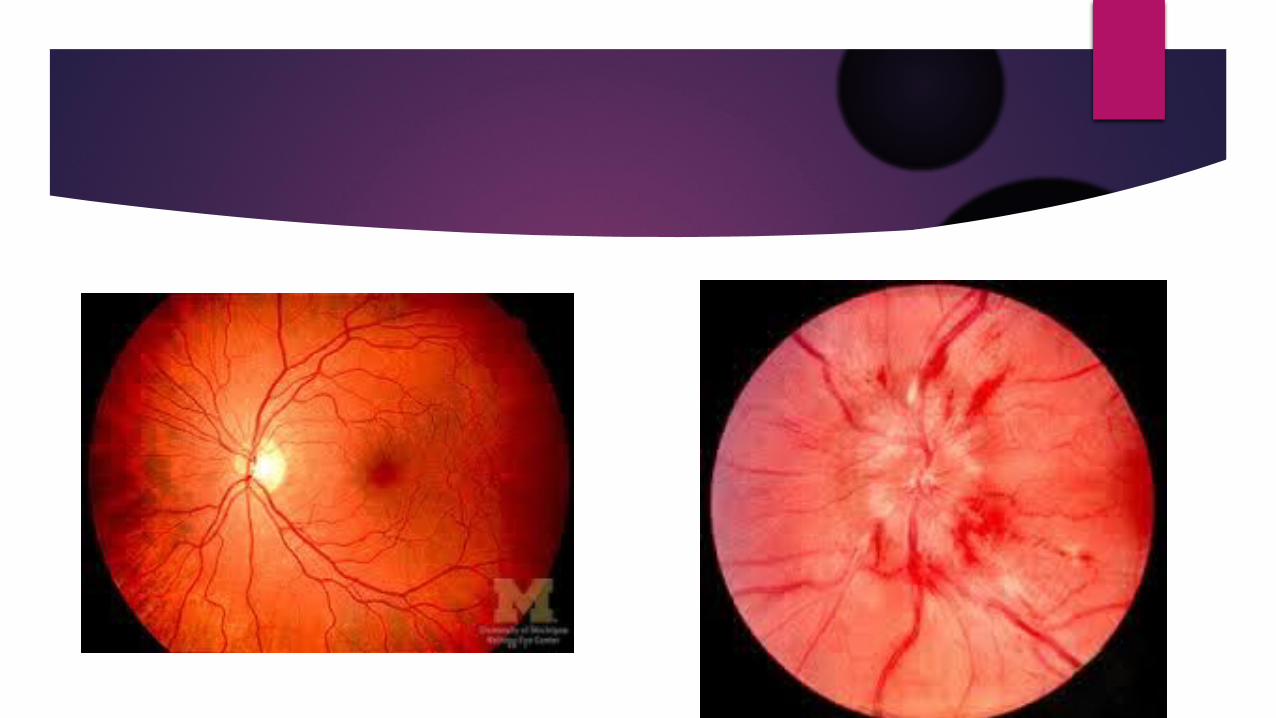
DO NOT FORGET THE FUNDUS EXAMINATION
Skull and c spine examination
Palpate the paranasal sinuses
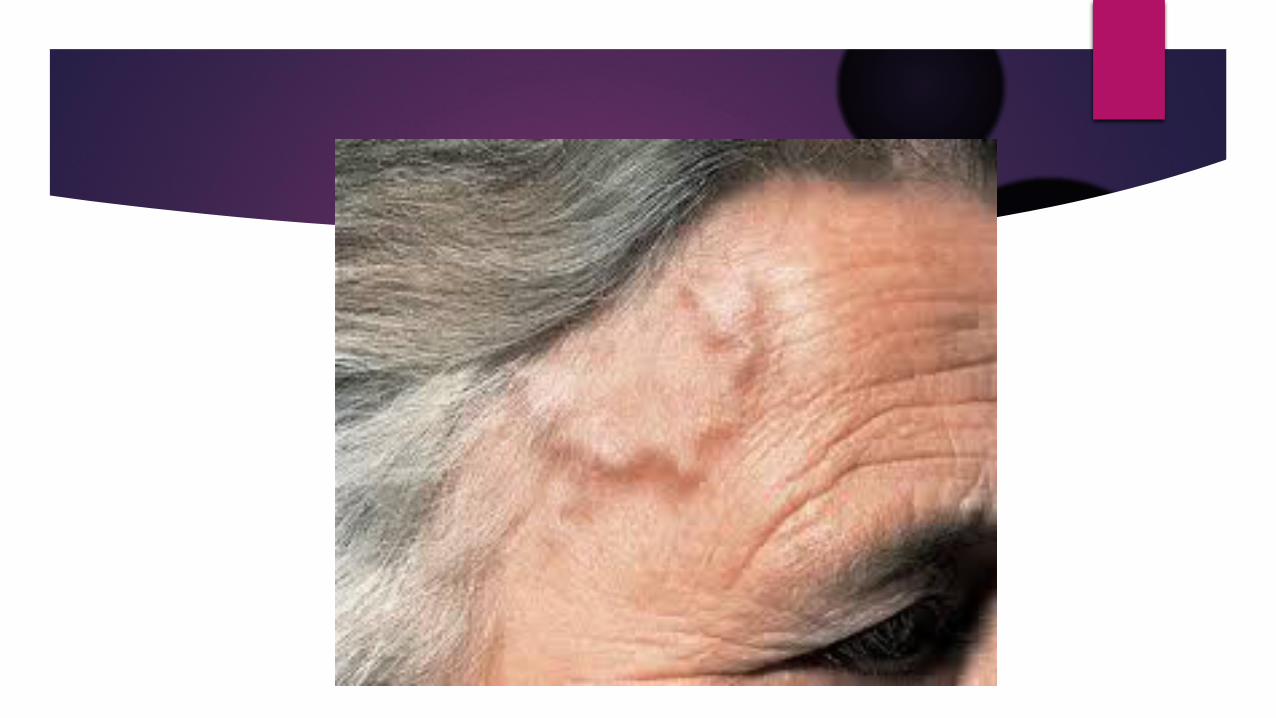
Temporal artery
High risk examination finding
Abnormal vital signs:-fever, severe hypertension
Toxic appearance
Localizing neurological finding
Decrease level of consciousness
Meningeal signs

High risk examination finding
Abnormal vital signs:-fever, severe hypertension
Toxic appearance
Localizing neurological finding
Decrease level of consciousness
Meningeal signs
Ophthalmic finding
Traumatic finding
Abnormalities of the temporal artery

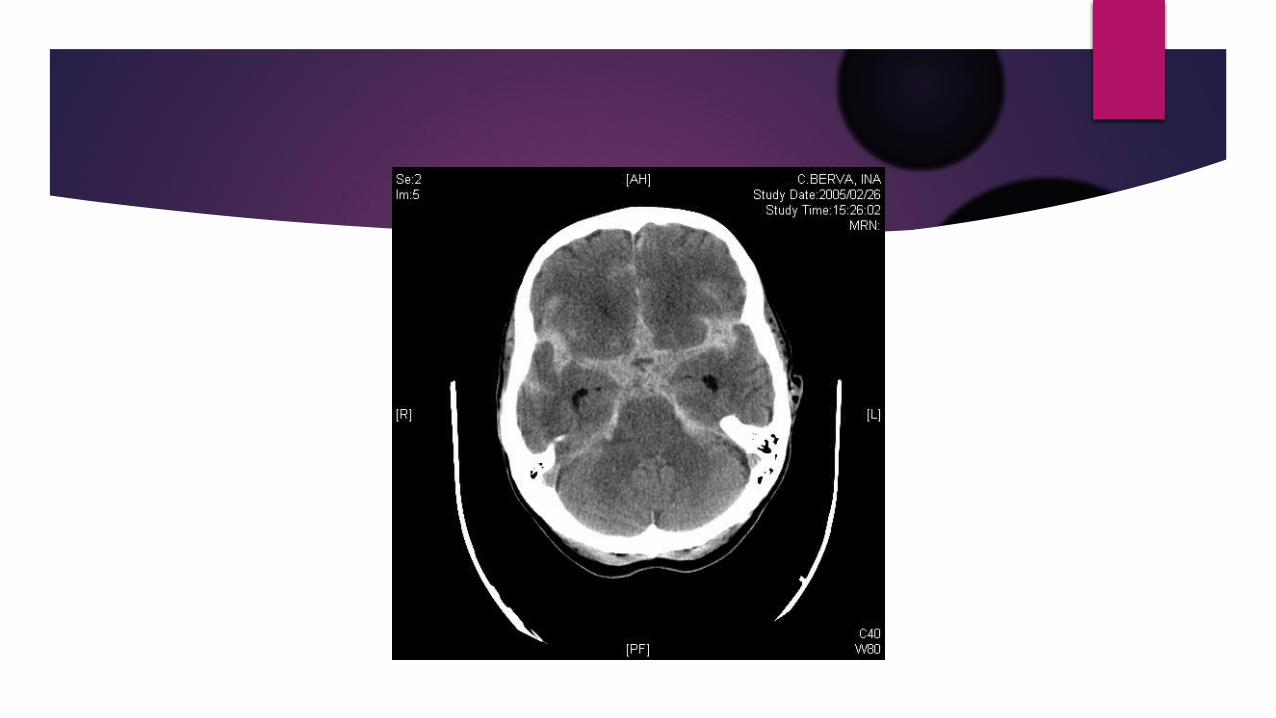
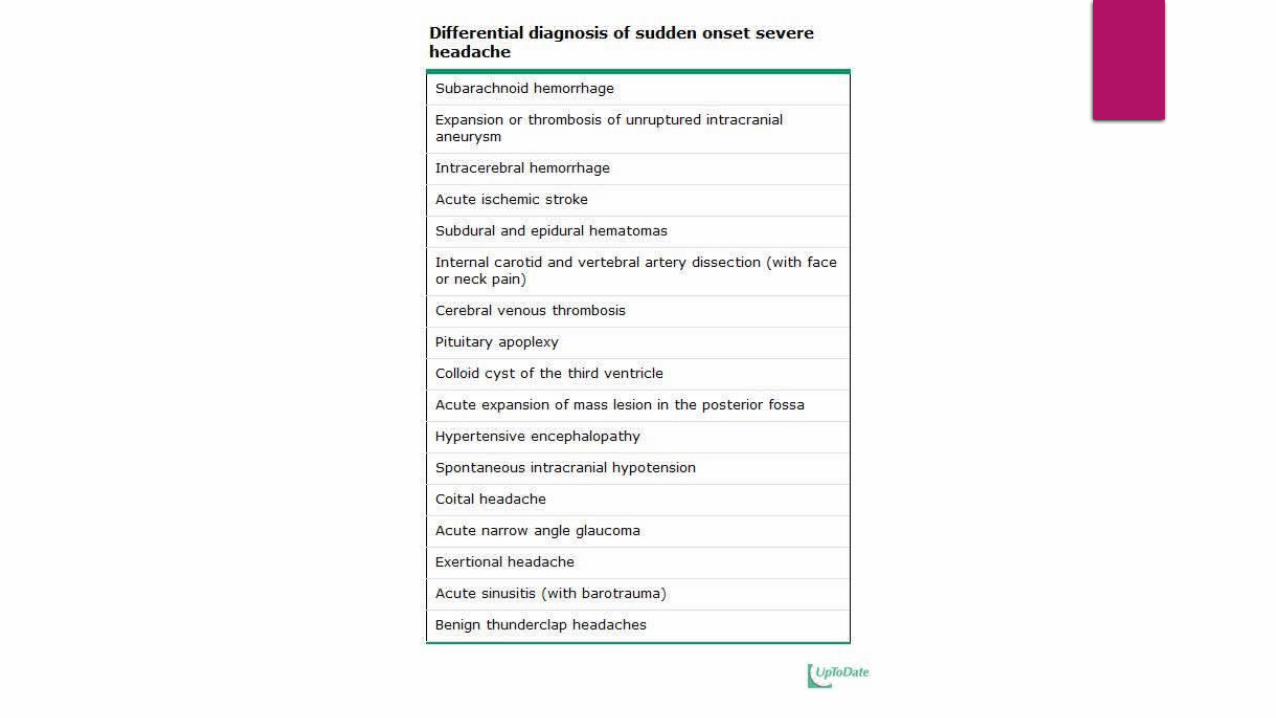
Sudden severe headache
Non contrast CT brain
Normal Abnormal
Lumbar Puncture for xnthochromia
Neurosurgery
Yes NO
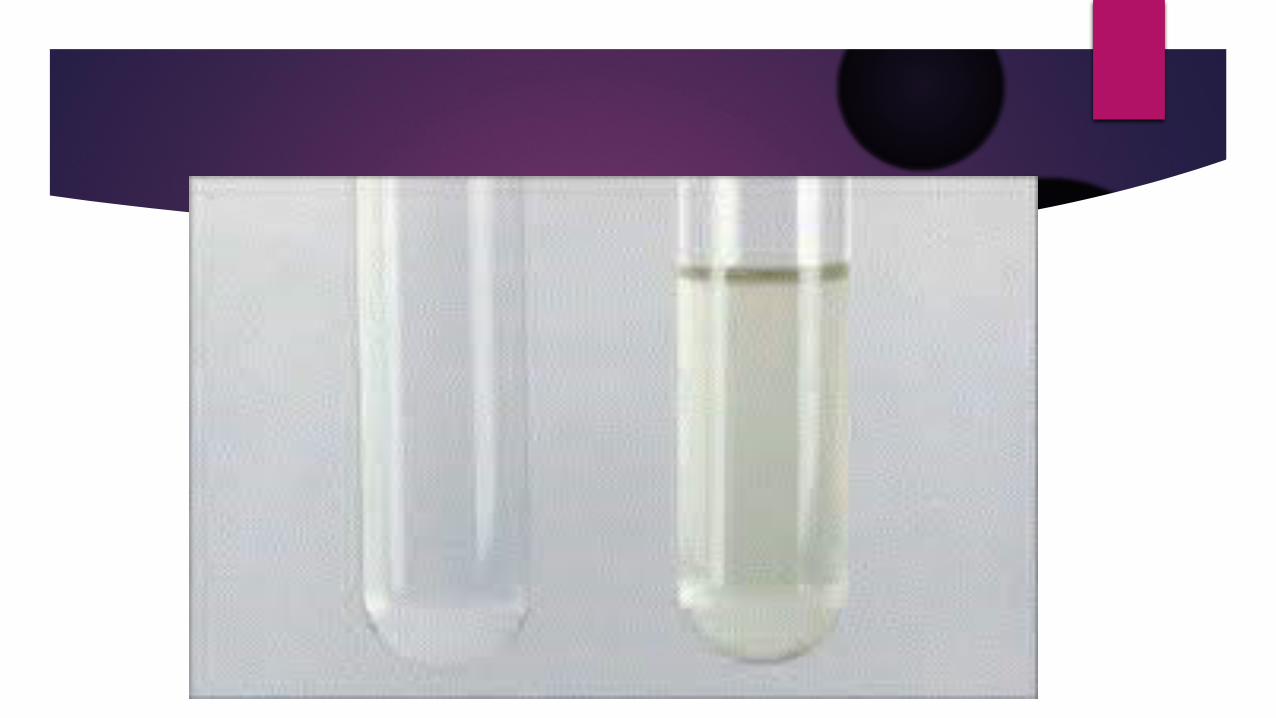
What is Xanthochromia?
Xanthochromia ( yellow or pink discoloration) represent Hg degradation.
The presence of xanthochromia is indicative that the blood has been present in CSF for at least 2hours prior to the tape.
Highly suggestive of SAH
What causes of xanthochromia other than SAH?

68 ear old female with one month history of headache and jaw pain while eating.
What other historical points will you consider?
What specific examination and investigation you will consider?
Constitutional symptoms
Visual symptoms
Shoulder and hip aching and stiffness

Examination of temporal artery
ESR
Temporal artery biopsy
In presence of high clinical suspicion and high ESR start steroid awaiting temporal artery biopsy
Temporal Arteritis
Chronic vasculitis of large and medium sized vessels.
Prevalence 1 in 500 individual.
Classification criteria:-- Age above or equal to 50 year of age- Localized headache of new onset- Tenderness or decrease pulse of the temporal artery- ESR >50- Biopsy revealing a necrotizing vasculitis
Why temporal arteritis should be treated promptly?
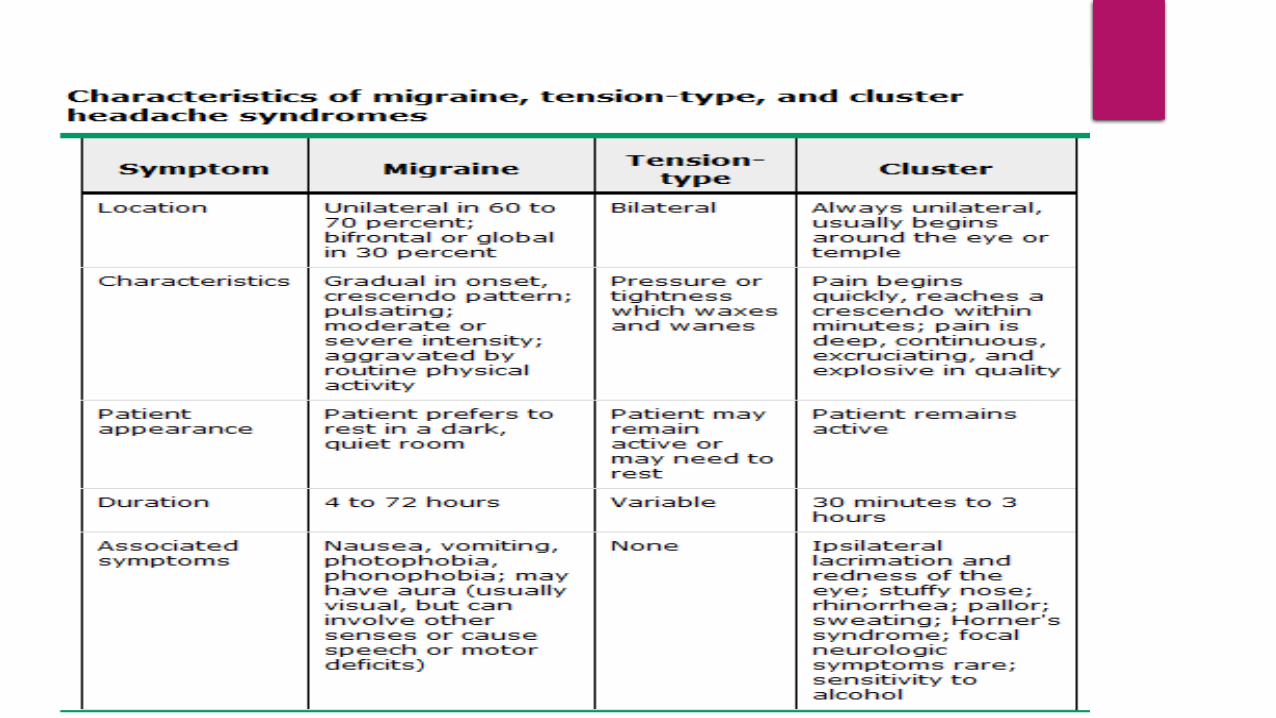
Primary Headache
Migraine
Tension headache
Cluster headache
Other primary headache
Take home messages
Carful evaluation is necessary when evaluating a patient with headache.
Be alert about headache red flags.





























