Embed Size (px)
Citation preview

30/03/2015
1
Douglas H. Richie, Jr. D.P.M.Seal Beach, California
Associate Professor of Podiatric Medicine, Western University of Health Sciences
Adjunct Associate Professor of Clinical Biomechanics, California School of Podiatric Medicine, Oakland CA
Applying the “Twisted Plate Theory” of Foot Stability to Flatfoot Surgery
PAC-PFOLA SYMPOSIUM, APRIL 2015
Fig. 7. The truss is a triangular structure. Under the load (W) the struts are under
compression ( C ) and the tie-rod (AB) is under tension (T). Any joint, for example point
A, is in vectorial equilibrium as indicated in the insert diagram. C compresses the point
A and T tenses the same point.
Twisted Plate TheoryFOOT VIEWED FROM BEHIND
Rear Plate twisted clockwise (inversion)
Front Plate twisted counter clockwise
The Twisted Plate
Twisting of the lamina pedis, or skeleton of the human foot
involves Eversion or Pronation of the forefoot or… Inversion
or Supination of the rearfoot
Un-twisting of the lamina pedis involves Inversion or Supination
of the forefoot or…Eversion or Pronation of the rearfoot

30/03/2015
2
The Twisted Plate Theory of Foot Stability
Key Point: Twisting the plate will raise the medial
longitudinal arch, plantarflex the First Ray, decrease strain
on the medial central band of the plantar aponeurosis, and
decompress and improve ROM of the 1st MTP.
First described by:MACCONAILL, M. A. (1945). The postural mechanism of the human foot.
Proceedings of the Royal Irish Academy 50, 265-278.
Introduces the term “lamina pedis” to describe the footplate
Twisted Plate Model of the Human Foot
And then again by:MACCONAILL, M. A. & BASMAJIAN, J. V. (1969). Muscles and Movements. A Basis for
Kinesiology. Baltimore: Williams & Wilkins.
And Finally:SARRAFIAN S.K. (1987) Functional characteristics of the foot and plantar aponeurosis
under tibiotalar loading. Foot and Ankle Int. 8 (1): 4-18.

30/03/2015
3
The Twisted Plate
Twisting of the lamina pedis follows the lateral rotation
of the head and next of the talus, which occurs in-utero
This valgus, or eversion rotation of the neck of the talus
results in pronation positioning of the forefoot on the rearfoot…
Twisting the plate
McCarthy, 1994

30/03/2015
4
• Nine fresh frozen specimens
• Axial load in static stance 225-900N
• 6 degree wedges: Medial & Lateral, RF & FF
• Strain in plantar fascia measured with
reluctance transducer
Kogler GF, Veer FB, Solomonidis SE, Paul JP: The influence of
medial and lateral placement of orthotic wedges on loading of the
plantar aponeurosis. Journal Bone Joint Surgery 81-A:1403, 1999
In-Vitro Study
Kogler GF, Veer FB, Solomonidis SE, Paul JP: The influence of
medial and lateral placement of orthotic wedges on loading of the
plantar aponeurosis. Journal Bone Joint Surgery 81-A:1403, 1999
Wedge under lateral forefoot decreased
strain (p<0.05)
Wedge under medial forefoot increased
strain (p<0.05)
Rearfoot wedges had no significant effect
Kogler GF, Veer FB, Solomonidis SE, Paul JP: The influence of
medial and lateral placement of orthotic wedges on loading of the
plantar aponeurosis. Journal Bone Joint Surgery 81-A:1403, 1999
Plantar Fascia Strain

30/03/2015
5

30/03/2015
6
Effects of Medial & Lateral Wedges under the Foot
15 Male running subjects, asymptomatic
4 conditions w/foot inserts w/4.5 mm posting: Full Lateral, Full Medial, Half Lateral, Half Medial
COP data collected with PEDAR system
Results: Only the Full Lateral Insert caused a significant change in shift of center of pressure: this shift was towards the LATERAL SIDE
Nigg BM, Stergiou P, Cole G et al: Effect of shoe inserts on kinematics, center of pressure, and leg joint moments during running. Med Sci Sports Exerc 35(2): 314-319, 2003.
Van Gheluwe B, Dananberg HJ: Changes in Plantar Foot Pressure with In-Shoe Varus or Valgus Wedging. JAPMA 94(1) 1-11 2004
“Indeed, as displayed for forefoot wedging and for rearfoot wedging of a typical individual, the COP shifts more medially with a varus wedge and more laterally with a valgus wedge. Internal wedges behave in the opposite manner from externally applied wedges.”

30/03/2015
7
In the weight bearing foot:
Increase ground reaction forces under
metatarsals 4 and 5
Twisting the plate
Increase ground reaction forces under
metatarsals 1 and 2
Untwisting the plate
In the weight bearing foot:
(During loading phase of gait):
Congruent motion is communicated to the subtalar joint and the talus is
effectively screwed home into the acetabulum pedis, about the comparatively
upright subtalar axis, and the leg bones reflect this movement by showing
medial rotation.
As the full weight is thus applied to the- foot the lamina pedis becomes flattened
or untwisted and this plays its part in causing the centre of gravity to veer back
towards the other side. The major part of this untwisting movement occurs at the
calcaneocuboid joint - effectively the calcaneus is exorotated. The lamina pedis is
now in a close-packed position with the plantar calcaneocuboid (short plantar)
ligament, plantar calcaneonavicular (spring) ligament and bifurcated ligament all
tensed.
Other descriptions of the “Twisted Plate”
LEWIS, 0. J. (1980a). The joints of the evolving foot. I. The ankle joint. Journal of
Anatomy. 130, 527-543.
The Twisted Plate The lamina pedis becomes twisted upon itself as we compare primates
and humans:
In primates, the lamina pedis is a flat plat resting on the ground. The
calcaneus is lateral to the talus, on the same flat plane as the metatarsals.
The subtalar joint is oriented vertical, separating the horizontal
arrangement of the talus and the calcaneus
In humans, the lamina pedis is “twisted” i.e the calcaneus has become
“twisted” to move under or beneath the talus. This change occurs in-utero.
The subtalar joint complex is now horizontal, separating the vertically
oriented talus and calcaneu

30/03/2015
8
The Twisted Plate
Un-twisting the lamina pedis allows the human foot to assume
the appearance of the adult acquired flatfoot: Lowering of the
medial longitudinal arch, eversion of the calcaneus, widening of
the Talo-Calcaneal angle, supinatus deformity of the forefoot.

30/03/2015
9
Orangutan
ChimpAssembled Bonobo
Assembled

30/03/2015
10
Removing FF SuppinatusSuppinatus Uncorrected
Twisted Plate Theory:
How Can We Raise the Arch?
Evert the Forefoot:
Increase Ground Reaction Forces under Lateral Metatarsals
Invert the Rearfoot:
Increase Ground Reaction Forces under Medial Calcaneus
► Is there any other evidence that increasing pressure
under the lateral forefoot will raise the medial arch
and/or decrease strain in the plantar aponeurosis?
Answer: Look at studies of lateral column lengthening
for flatfoot correction
Twisted Plate Theory:
Lateral Forefoot wedging
Lengthen Lateral Column
Twisted Plate Theory:
How do we increase GRF under lateral metatarsals?
Otis JC, Deland JT, Kenneally S et al: Medial arch strain after lateral column lengthening: An in vitro study. Foot Ankle Int 20: 797-802. 1999
30/03/2015
11
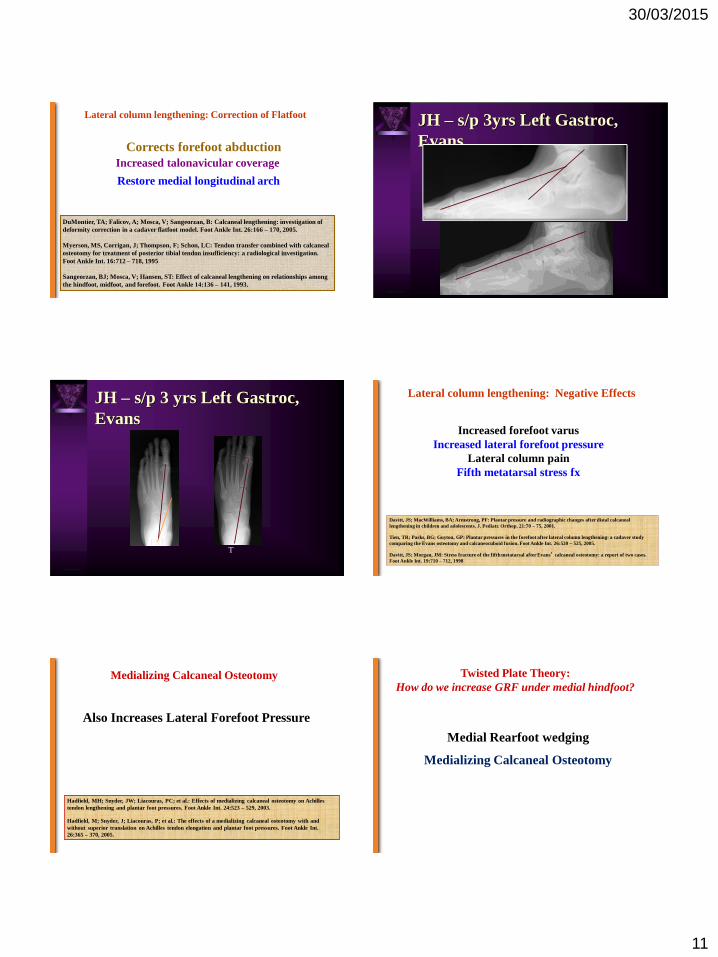
Lateral column lengthening: Correction of Flatfoot
Corrects forefoot abduction
DuMontier, TA; Falicov, A; Mosca, V; Sangeorzan, B: Calcaneal lengthening: investigation of
deformity correction in a cadaver flatfoot model. Foot Ankle Int. 26:166 – 170, 2005.
Myerson, MS, Corrigan, J; Thompson, F; Schon, LC: Tendon transfer combined with calcaneal
osteotomy for treatment of posterior tibial tendon insufficiency: a radiological investigation.
Foot Ankle Int. 16:712 – 718, 1995
Sangeorzan, BJ; Mosca, V; Hansen, ST: Effect of calcaneal lengthening on relationships among
the hindfoot, midfoot, and forefoot. Foot Ankle 14:136 – 141, 1993.
Restore medial longitudinal arch
Increased talonavicular coverage
JH – s/p 3yrs Left Gastroc,
Evans
JH – s/p 3 yrs Left Gastroc,
Evans
PRE POS
T
Lateral column lengthening: Negative Effects
Increased forefoot varus
Increased lateral forefoot pressure
Lateral column pain
Fifth metatarsal stress fx
Davitt, JS; MacWilliams, BA; Armstrong, PF: Plantar pressure and radiographic changes after distal calcaneal
lengthening in children and adolescents. J. Pediatr. Orthop. 21:70 – 75, 2001.
Tien, TR; Parks, BG; Guyton, GP: Plantar pressures in the forefoot after lateral column lengthening: a cadaver study
comparing the Evans osteotomy and calcaneocuboid fusion. Foot Ankle Int. 26:520 – 525, 2005.
Davitt, JS; Morgan, JM: Stress fracture of the fifth metatarsal after Evans’ calcaneal osteotomy: a report of two cases.
Foot Ankle Int. 19:710 – 712, 1998
Medializing Calcaneal Osteotomy
Also Increases Lateral Forefoot Pressure
Hadfield, MH; Snyder, JW; Liacouras, PC; et al.: Effects of medializing calcaneal osteotomy on Achilles
tendon lengthening and plantar foot pressures. Foot Ankle Int. 24:523 – 529, 2003.
Hadfield, M; Snyder, J; Liacouras, P; et al.: The effects of a medializing calcaneal osteotomy with and
without superior translation on Achilles tendon elongation and plantar foot pressures. Foot Ankle Int.
26:365 – 370, 2005.
Twisted Plate Theory:
How do we increase GRF under medial hindfoot?
Medial Rearfoot wedging
Medializing Calcaneal Osteotomy

30/03/2015
12
Medial Calcaneal Displacement
Myerson MS, Badekas A, Schon LC: Treatment of stage II posterior tibial tendon deficiency with flexor digitorum longus tendon transfer and calcaneal osteotomy. Foot & Ankle Int, 25: 445-450
• 129 Patients.
• Mean follow up, 5.2 years post op
• 118 Patients entirely satisfied, 7 patients partially satisfied, 4 patients dissatisfied.
• 125 Patients (97%) experienced pain relief.
• 121 Patients (94%) showed improvement of function.
Resnick RB, Jahss MH, Choveka J et al: Deltoid ligament forces after tibialis posterior tendon rupture: effects of triple arthrodesis and calcaneal displacement osteotomies. Foot Ankle Int 16: 14-20, 1995
• After medial displacement calcaneal osteotomy, strain decreased at the attachment point of the deltoid ligament

30/03/2015
13
“The medial displacement calcaneal osteotomy resulted in decreased length and, likely, less tension in the spring ligament.”
Otis JC, Deland JT, Kenneally S et al: Medial arch strain after medial displacement calcaneal osteotomy: An in vitro study. Foot Ankle Int 20:222-226, 1999
“From these results, we concluded that reconstruction LCL provides more
correction of the longitudinal arch at the midfoot and overall realignment of the
medial column of the foot than a reconstruction with MTO.”
“This result establishes that the final correction achieved in the LCL group was
significantly greater than the one achieved in the MTO group.”
“In summary, reconstructions performed with LCL produced a greater change
in the realignment of a flexible flatfoot, maintained more of their initial
correction over time, and were associated with a lower incidence of additional
surgery than reconstructions with a MTO of the calcaneus.”
MDCO vs Evans Osteotomy: Comparison of Correction
Patrick M. Bolt, M.D.; Samuel Coy, M.D.; Brian C. Toolan, M.D. A Comparison of
Lateral Column Lengthening and Medial Translational Osteotomy of the Calcaneus
for the Reconstruction of Adult Acquired Flatfoot. Foot & Ankle International/Vol.
28, No. 11/November 2007
Answer: It has to do with ligament strain and motion of the
foot at joints other than the subtalar joint
Twisted Plate Theory:
► Why would lateral forefoot wedging and lateral column
lengthening not cause pronation of the foot at the subtalar joint?
Mosca, V.S. Calcaneal lengthening for valgus deformity of the hindfoot. Results in children
who had severe, symptomatic flatfoot and skewfoot. J. Bone Joint Surg. 77A:500-512, 1995.
Lateral Column Lengthening: Facilitate the Windlass??
Mosca has suggested that the effects of lengthening
of the lateral column results in elevation of the
longitudinal arch and correction of the valgus
deformity due to the windlass effect of the plantar
fascia.
In fact, the opposite:
“The original hypothesis was that these manipulations would result in increased
tension on the plantar fascia with elevation of the medial longitudinal arch
secondary to an increase in the windlass mechanism. The results obtained reveal
that tightening of the plantar fascia does not occur with either medial calcaneal
displacement or lateral column lengthening. Medial translation resulted in an
average of 1.1 mm of loosening of the plantar fascia. Lateral column lengthening
through the calcaneocuboid joint resulted in even more loosening of the plantar
fascia (average, 1.9 mm). Lateral column lengthening was shown to produce
statistically significantly looser plantar fascia than medial displacement.
MDCO and Evans: No increased tension on the plantar fascia!
Horton GA, Myerson MS, Parks BG, Park YW. Effect of calcaneal osteotomy and lateral
column lengthening on the plantar fascia: a biomechanical investigation. Foot Ankle Int.
1998 Jun;19(6):370-3.

30/03/2015
14
Calcaneal Lengthening Osteotomy
The navicular center of rotation is within the head of the talus. The
shape of the talar head is therefore important to the degree of deformity
correction.
The effective center of rotation of the cuboid is within the calcaneus and
is compatible with rotation about the long plantar ligament.
The bony architecture and the plantar soft tissues, including the long
plantar ligament and possibly the plantar talonavicular capsule and the
lateral portion of the calcaneonavicular ligament, appear to contribute to
the mechanism of deformity correction.
Timothy A. DuMontier, Alexis Falicov, Vincent Mosca, Bruce Sangeorzan. Calcaneal
Lengthening: Investigation of Deformity Correction in a Cadaver Flatfoot Model. Foot & Ankle
International/Vol. 26, No. 2/February 2005.
It has been suggested that the long plantar ligament is
important in the success of the calcaneal neck osteotomy
for correction of flatfoot.
Long Plantar Ligament
Sangeorzan, B.J., Mosca, V., and Hansen, S.T. Effect of calcaneal lengthening on
relationships among the hindfoot, midfoot, and forefoot. Foot Ankle, 14:136-141, 1993.

30/03/2015
15
Lateral Plantar Ligament (LPL)
“Thus after an Evans procedure, the lateral one-third of the LPL is
under maximum strain, the spring ligament is extremely lax, and the
medial band of the plantar fascia is also lax.”
“In addition, when shortening bony procedures to the medial column
are performed in addition to the Evans procedure, the rippling effect
may be compounded: even more laxity in the PF and spring ligament
could be created.”
DiNucci, KR, Christensen, JC, Christensen, Kris A: Biomechanical Consequences of
Lateral Column Lengthening of the Calcaneus: Part I. Long Plantar Ligament Strain.
Journal of Foot Ankle Surg 43: 10-15 2004
DiNucci, KR, Christensen, JC, Christensen, Kris A: Biomechanical Consequences of Lateral Column Lengthening of the Calcaneus: Part I. Long Plantar Ligament Strain. Journal of Foot Ankle Surg 43: 10-15 2004
Before Evans Graft After Evans 8mm Wedge
The Twisted Plate Theory of Foot Stability
Key Point: With the foot resting on the ground, inverting the hindfoot will
increase ground reaction forces (plantar pressure) against the 4th and 5th
metatarsal heads.
Applying a 6 degree lateral (valgus) wedge across the forefoot
will increase ground reaction forces (plantar pressure) against the 4th and
5th metatarsal heads.
A calcaneal lengthening osteotomy will increase ground
reaction forces (=plantar pressure) against the 4th and 5th metatarsal
heads.
The Twisted Plate Theory of Foot Stability
Key Point: Increasing plantar pressure against the
4th and 5th metatarsal heads will:
- Increase tension in the long plantar ligament
- Close-pack or “lock” the Calcaneal-Cuboid Joint
The Twisted Plate Theory of Foot Stability
Key Point: With the foot resting on the ground, everting the hindfoot will
increase ground reaction forces (plantar pressure) against the First
metatarsal head.
Applying a 6 degree medial (varus) wedge across the forefoot will increase
ground reaction forces (plantar pressure) against the First metatarsal head.
A Cotton osteotomy or plantar flexion osteotomy anywhere along the First
Ray will increase ground reaction forces (plantar pressure) against the First
metatarsal head.
Solution to Increased Lateral Forefoot Pressure:
Plantarflexion, opening wedge osteotomy
(Cotton) of the medial cuneiform
Hirose, CB; Johnson, JE: Plantarflexion opening wedge medial cuneiform osteotomy for correction of fixed
forefoot varus associated with flatfoot deformity. Foot Ankle Int. 25:568 – 574, 2004.
Johnson, JE: Plantarflexion opening wedge cuneiform-1 osteotomy for correction of fixed forefoot varus.
Tech. Foot Ankle Surg. 3:2 – 8, 2004.

30/03/2015
16
Aaron T. Scott, M.D.; Travis M. Hendry, M.D.; Joseph M. Iaquinto, M.S.; Plantar Pressure Analysis in
Cadaver Feet After Bony Procedures Commonly Used in the Treatment of Stage II Posterior Tibial
Tendon Insufficiency. Foot and Ankle Int. 28: 1143-1153, 2007.
Methods: Eight matched pairs of cadaver lower extremities were
axially loaded onto a TekScan HR Mat. (TekScan, Inc., South Boston,
MA) After intact testing, each specimen had a lateral column
lengthening (either a calcaneocuboid distraction arthrodesis [CCDA]
or Evans procedure), a medializing calcaneal osteotomy (MCO), and
a plantarflexion (Cotton) osteotomy of the medial cuneiform. The
measured plantar pressures were divided into three forefoot regions,
two midfoot regions, and two hindfoot regions. For each region,
average pressure, peak pressure, and contact area data were collected.
Aaron T. Scott, M.D.; Travis M. Hendry, M.D.; Joseph M. Iaquinto, M.S.;
Plantar Pressure Analysis in Cadaver Feet After Bony Procedures Commonly
Used in the Treatment of Stage II Posterior Tibial Tendon Insufficiency. Foot
and Ankle Int. 28: 1143-1153, 2007.
Conclusions: The present study demonstrated increased lateral forefoot
pressures after a combined lateral column lengthening and MCO and does not
support the idea that a Cotton osteotomy significantly reduces loading of the
lateral forefoot.
Clinical Relevance: The incidence of lateral forefoot pain and fifth metatarsal
stress fractures subsequent to either lateral column lengthening procedure
may not significantly decline after a Cotton osteotomy.
Cotton Osteotomy: Improved Alignment?
Radiographic and Pedobarographic Comparison of Femoral Head Allograft Versus
Block Plate with Dorsal Opening Wedge Medial Cuneiform Osteotomy: A
Biomechanical Study
Alan C. League, MD; Brent G. Parks, MSc; Lew C. Schon, MD Foot & Ankle
International/Vol. 29, No. 9/September 2008
“Radiographic change in this model was inconclusive.
The small radiographic differences noted in this study
fall within the 2- to 3-degree variation in angle
measurements taken by different examiners.”
STUDIES SHOW NO IMPROVEMENT OF
METATARSUS PRIMUS ELEVATUS OR HALLUX
EQUINUS MEASUREMENTS AFTER DISTAL FIRST
METATARSAL HEAD OSTEOTOMIES
Laakmann G, Green RM, Green DR: “The modified Waterman procedure: A
preliminary Retrospective Study” in Reconstructive Surgery of the Foot and
Leg: Update ’95, ed by CA Camasta, p 128, The Podiatry Institute, Tucker, BA,
1995.
Dickerson JB, Green R, Gren DR: Long-term follow-up of the Green-
Waterman osteotomy for hallux limitus. JAPMA 92: 543, 2002.
Roukis TS, Jacobs PM, Dawson DM, ET AL: A prospective comparison of
clinical, radiographic, and intraoperative features of hallux rigidus: short-term
follow-up and analysis. J Foot Ankle Surg 41: 158, 2002.
The Twisted Plate
When the rearfoot inverts, ground reaction force increases under mets 4 & 5:
Forefoot pronates, tension increases in long and short plantar ligaments,
medial arch raises, first ray passively plantarflexes: Twisting the Plate
When the rearfoot everts, ground reaction force increases under 1st Met:
First ray dorsiflexes, forefoot supinates : Un-twisting the plate

30/03/2015
17
Untwisting the Plate
Increasing GRF under the First
Metatarsal will not raise the arch of the foot
Untwisting the Plate: Theory
Medial column procedures intending to increase GRF under
the First Metatarsal will not change alignment of the arch
because the joints of the twisted plate will react with a
reciprocal lowering of the arch. Only when arthrodesis is
performed will the twisted plate mechanism be nullified.
Raising the Medial Longitudinal ArchRole of the Ligaments
Spring Ligament does not increase tension after calcaneal lengthening
Otis, JC; Deland, JT; Kenneally, S: Medial arch strain after lateral column lengthening: An in vitro
study. Foot Ankle Int. 20:12,797 –802, 1999.
Plantar Fascia reduces tension after calcaneal lengthening
Horton GA, Myerson MS, Parks BG, Park YW. Effect of calcaneal osteotomy and lateral column
lengthening on the plantar fascia: a biomechanical investigation.Foot Ankle Int. 1998 Jun;19(6):370-3.
Increased tension in the long plantar ligament is the key to
deformity correction with lateral column lengthening
Timothy A. DuMontier, Alexis Falicov, Vincent Mosca, Bruce Sangeorzan. Calcaneal Lengthening:
Investigation of Deformity Correction in a Cadaver Flatfoot Model. Foot & Ankle International/Vol.
26, No. 2/February 2005.
Conclusion: Interventions which INCREASE STRAIN on the Long Plantar ligament
will raise the arch of the human foot.
Answer: Yes. Numerous studies have verified.
Twisted Plate Theory:
Do Lateral Column Lengthening Procedures improve alignment by:
► Change forefoot alignment to increase supination moment at the STJ?
► Increase pressure (GRF) under the lateral metatarsals?
Answer: No. At least no evidence thus far
Essential Key Point!
Any measure which increases plantar pressure at the 1st metatarsal will
deliver dorsiflexion moment, resulting in dorsiflexion motion across the key
joints of the First Ray. As long as there is motion available in the N-C and
Med Cun-1st Met joints, any surgical procedure which increases pressure
against the plantar surface of the first metatarsal will cause an immediate
dorsiflexion of the first ray back to its original state of equilibrium.
In the lateral column, increased plantar pressure under 4th and 5th
metatarsals does not cause dorsiflexion motion of the Calc-Cuboid or
Cuboid-4th and 5th mets because these joints are inherently stable.
The Twisted Plate Theory of Foot Stability
Key Point: Increasing pressure under the plantar surface of the 4th and
5th metatarsal heads will decrease pressure under the 1st metatarsal head
due to:
-Direct mechanical offloading (the more pressure you put
under one side of the foot, the less pressure on the other side)
-Tensioning of the long plantar ligament, which raises the
Calcaneal inclination angle, inverts the hindfoot, raises the medial
longitudinal arch
….in other words, this increased pressure
under mets 4 and 5 “Twists the Plate”!!
The Twisted Plate Theory of Foot Stability

30/03/2015
18
- There is decreased tension in the medial slip of the central band
of the plantar aponeurosis.
- Improved dorsiflexion range of motion of the 1st MTP
- The medial longitudinal arch will elevate
Key Point: Decreasing plantar pressure under the 1st metatarsal
head will allow the First Ray to passively plantarflex.
When the First Ray plantarflexes:
The Twisted Plate Theory of Foot Stability




























