Embed Size (px)
Citation preview

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Robert Timmerman, MDRobert Timmerman, MDUT Southwestern Medical Ctr. UT Southwestern Medical Ctr. Dallas, TexasDallas, Texas
Application of Application of HypofractionationHypofractionationin the Lungin the Lung

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Evolution of Radiation DeliveryEvolution of Radiation Delivery•• BrachyBrachy to to orthoortho to cobalt to to cobalt to linaclinac, 1, 1--D to 2D to 2--D to 3D to 3--D to D to
IMRTIMRT
•• All used to deliver low dose rate treatment (40 All used to deliver low dose rate treatment (40 radrad per per hour or 2 hour or 2 GyGy per day)per day)
•• Why?Why?-- We think it is has biological advantages (4 RWe think it is has biological advantages (4 R’’s)s)-- We are good at itWe are good at it-- We have long term outcome data that we can quoteWe have long term outcome data that we can quote-- Our clinics are set up specifically to deliver itOur clinics are set up specifically to deliver it-- We get reimbursed for itWe get reimbursed for it

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Indications for Conventional Indications for Conventional RadiotherapyRadiotherapy
•• Adjuvant treatment: treating for suspected occult Adjuvant treatment: treating for suspected occult microscopic tumormicroscopic tumor-- Involves treating large volumes of Involves treating large volumes of ““normalnormal”” tissuetissue
•• Primary treatment: treating gross deposits of Primary treatment: treating gross deposits of tumortumor-- Often done in conjunction with an adjuvant treatmentOften done in conjunction with an adjuvant treatment-- So, involves treating large volumes of So, involves treating large volumes of ““normalnormal”” tissuetissue

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
My Observations about My Observations about Conventional RadiotherapyConventional Radiotherapy
•• By its nature and historical use, it treats By its nature and historical use, it treats considerably more normal tissue than tumor to a considerably more normal tissue than tumor to a high dose (50+ high dose (50+ GyGy))
•• Works well as regional adjuvant therapy (e.g., Works well as regional adjuvant therapy (e.g., breast, rectum, sarcoma)breast, rectum, sarcoma)
•• However, conventional radiotherapy is However, conventional radiotherapy is patheticallypathetically ineffective for gross disease, ineffective for gross disease, especially for common carcinogenespecially for common carcinogen--induced induced carcinomas (ask your patients)carcinomas (ask your patients)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
How do radiation oncologistsHow do radiation oncologistsbear this?bear this?
•• They focus on the better tolerance of They focus on the better tolerance of radiotherapy compared to surgery (we can treat radiotherapy compared to surgery (we can treat frail patients)frail patients)
•• They fiercely maintain the They fiercely maintain the ““first do no harmfirst do no harm””dictum (reasonable considering the therapy dictum (reasonable considering the therapy doesndoesn’’t work)t work)
•• BUT, they donBUT, they don’’t consider tumor recurrence to be t consider tumor recurrence to be a toxicity or their fault (the patient failed a toxicity or their fault (the patient failed radiotherapy, not radiotherapy failed the patient)radiotherapy, not radiotherapy failed the patient)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Spreading out Entrance DoseSpreading out Entrance Dose

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Lesion Produced by Lesion Produced by the Gamma Knifethe Gamma Knife
•• Dose per fraction > 8Dose per fraction > 8--10 10 GyGy
Steep dose gradientsSteep dose gradients

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Imitation is FlatteringImitation is Flattering

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Why is radiosurgery so successful?Why is radiosurgery so successful?
•• Advanced technology to avoid entrance damage Advanced technology to avoid entrance damage and normal tissue exposure and normal tissue exposure
•• Advanced imaging to insure accurate targetingAdvanced imaging to insure accurate targeting
•• Very large dose per treatment to Very large dose per treatment to ablateablate the targetthe target

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Iodine Scavenging Iodine Scavenging by Thyroid Tissueby Thyroid Tissue
IV administration of RadioactiveIV administration of RadioactiveIodine 131 (beta emitter)Iodine 131 (beta emitter)
••Well differentiated thyroid cancer Well differentiated thyroid cancer frequently metastaticfrequently metastatic
••Prior to 1942 often lethalPrior to 1942 often lethal
••II--131 first and still most successful 131 first and still most successful targeted therapytargeted therapy

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Why Ablate?Why Ablate?
•• Cancer vs. Conventional Cancer Cancer vs. Conventional Cancer Therapy:Therapy: Cancer usually winsCancer usually wins
•• Cancer vs. Ablative Therapy:Cancer vs. Ablative Therapy:Therapy usually winsTherapy usually wins

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Fractionation OptionsFractionation Options•• Conventionally fractionated radiotherapyConventionally fractionated radiotherapy
-- small daily dosessmall daily doses-- go to very high cumulative dosesgo to very high cumulative doses-- strategy for IMRT implementationstrategy for IMRT implementation
•• HypofractionatedHypofractionated radiotherapyradiotherapy-- larger daily doses (3larger daily doses (3--6 Gy)6 Gy)-- used for palliationused for palliation
•• Ablative radiotherapyAblative radiotherapy-- very high daily doses (8very high daily doses (8--20 Gy)20 Gy)-- overwhelm tumor repairoverwhelm tumor repair-- causes causes ““latelate”” effects that may be intolerableeffects that may be intolerable

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Ablative Treatments Must Avoid Ablative Treatments Must Avoid VolumeVolume
•• Requirements for ablative Requirements for ablative hypofractionationhypofractionation::-- Abandon prophylactic treatmentAbandon prophylactic treatment
-- Account for organ motionAccount for organ motion
-- Achieve sharper dose fallAchieve sharper dose fall--off gradients to normal off gradients to normal tissue (mimic tissue (mimic radiosurgeryradiosurgery))
•• These requirements need advanced technologyThese requirements need advanced technology

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Conformal high doseConformal high dose
--This constitutes the tumor control (place it well)This constitutes the tumor control (place it well)-- Being conformal is easy Being conformal is easy –– especially with many beams or arcsespecially with many beams or arcs

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Compact intermediate doseCompact intermediate dose
-- This accounts for toxicity. All of this dose is in normal tissThis accounts for toxicity. All of this dose is in normal tissuesues-- Infinite possibilities Infinite possibilities –– some much more toxic than otherssome much more toxic than others
This is the hardest This is the hardest part of the SBRT part of the SBRT process and process and distinguishes a distinguishes a good plan from a good plan from a poor plan!poor plan!

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Respect Normal Tissue ConstraintsRespect Normal Tissue Constraints
-- Scant data for 5 or fewer fractionsScant data for 5 or fewer fractions-- Particularly more difficult for serial tissues compared to paraParticularly more difficult for serial tissues compared to parallelllel
Pulmonary VeinPulmonary VeinBronchusBronchus
EsophagusEsophagus
CordCord SkinSkin
ChestwallChestwall
LungLung

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Very large low dose volumeVery large low dose volume
-- SBRT (and radiosurgery) Assumption: A little dose to a lot ofSBRT (and radiosurgery) Assumption: A little dose to a lot ofnormal tissue is better than a lot of dose to a little normal tinormal tissue is better than a lot of dose to a little normal tissuessue

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
33--5 Year Outcome in5 Year Outcome inEarly Stage Lung CancerEarly Stage Lung Cancer
Rx ModalityRx Modality % alive% alive•• Stage IStage I SurgerySurgery 6060--80%80%
Stage I*Stage I* Radiotherapy (RT)Radiotherapy (RT) 1515--45%45%
Rx ModalityRx Modality % LC% LC•• Stage IStage I SurgerySurgery 6060--80%80%
Stage IStage I Radiotherapy (RT)Radiotherapy (RT) 1515--45% 45%
*clinically staged and mostly medically inoperable*clinically staged and mostly medically inoperable
RT generally 60RT generally 60--66 Gy delivered in 666 Gy delivered in 6--7 weeks7 weeks

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Typical Patient Scenario with Typical Patient Scenario with Conventional RadiotherapyConventional Radiotherapy
•• T2,N0,M0 lung cancer in a 65 year old smoker T2,N0,M0 lung cancer in a 65 year old smoker with poor with poor PFTsPFTs and heart disease and heart disease -- not a surgical not a surgical candidatecandidate
•• Nice person, wants to liveNice person, wants to live
•• We get to know and like the patient during 6We get to know and like the patient during 6--7 7 week course of radiationweek course of radiation
•• Most likely tumor recurs, metastasizes, causes Most likely tumor recurs, metastasizes, causes morbidity and ultimate death within 3 years.morbidity and ultimate death within 3 years.

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Clinical Model: Medically Inoperable Clinical Model: Medically Inoperable Stage I Lung Cancer using SBRTStage I Lung Cancer using SBRT
•• Indiana University (IU) phase I toxicity study:Indiana University (IU) phase I toxicity study:Doses as high as 22 Gy X 3 fractions Doses as high as 22 Gy X 3 fractions tolerable (47 patients)tolerable (47 patients)11
•• IU phase II efficacy study:IU phase II efficacy study:Doses of 20Doses of 20--22 Gy X 3 fractions yields 22 Gy X 3 fractions yields extremely high levels of local control (70 extremely high levels of local control (70 patients)patients)22
11 Timmerman, et. al., Chest, 2003Timmerman, et. al., Chest, 200322 Timmerman, et. al., JCO, 2006Timmerman, et. al., JCO, 2006

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Phase I Dose Escalation StudyPhase I Dose Escalation StudyChest 124:1946Chest 124:1946--55, 200355, 2003
•• 47 patient Phase I study using 3 fractions47 patient Phase I study using 3 fractions
•• Starting dose 24 Starting dose 24 GyGy total (8 total (8 Gy/fxGy/fx))
•• 3 separate dose escalation groups:3 separate dose escalation groups:-- T1 tumors: 60 Gy total (20 T1 tumors: 60 Gy total (20 Gy/fxGy/fx) without DLT) without DLT-- Small T2 tumors: 66 Gy total (22 Small T2 tumors: 66 Gy total (22 Gy/fxGy/fx) without DLT) without DLT-- Big T2 tumors (5Big T2 tumors (5--7 cm): 2/5 patients with DLT at 72 7 cm): 2/5 patients with DLT at 72
Gy total (24 Gy per fraction)Gy total (24 Gy per fraction)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
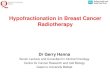
T2 Tumor, 36 GyT2 Tumor, 36 Gy
PrePre--TreatmentTreatment 22 mo. Post22 mo. Post--TreatmentTreatment

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
PrePre--RxRx
3 mo.3 mo.
9 mo.9 mo.
18 mo.18 mo.
T2 Tumor, 72 GyT2 Tumor, 72 Gy

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
PrePre--RxRx 18 mo.18 mo.
T2 Tumor, 72 GyT2 Tumor, 72 Gy

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
T1 tumor, 60 GyT1 tumor, 60 GyT1 tumor, 60 Gy
PrePre--treatmenttreatment One year post treatmentOne year post treatment
WedgeWedge--like collapselike collapseof segmental bronchusof segmental bronchus
No evidence of tumorNo evidence of tumorrecurrence on PETrecurrence on PET
No tumor cells on bronchialNo tumor cells on bronchialbiopsy or brushingsbiopsy or brushings
Post treatment bronchoscopyPost treatment bronchoscopy
Treatment planningTreatment planning

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Pulmonary Function TestsPulmonary Function Tests
-20
-10
0
10
20
1.5 3 6 9 12 15 18
FEV1
-20
-10
0
10
20
1.5 3 6 9 12 15 18
FVC
-20
-10
0
10
20
1.5 3 6 9 12 15 18
DLCO
-20
-10
0
10
20
1.5 3 6 9 12 15 18
pO2
Perc
ent C
hang
ePe
rcen
t Cha
nge
Perc
ent C
hang
ePe
rcen
t Cha
nge
Months from Therapy Months from Therapy
Months from Therapy Months from Therapy

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
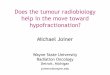
Phase I Dose Response for Phase I Dose Response for Local ControlLocal Control
0
20
40
60
80
100
0 20 40 60 80
Total Dose (Gy) in 3 Fractions
17 M
onth
Lo
cal C
ontro
l (%
)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Indiana Phase II StudyIndiana Phase II Study•• NIH RNIH R--21 grant funded prospective study21 grant funded prospective study
•• Phase I dose:Phase I dose: T1 = 20 Gy X 3 fractions = 60 GyT1 = 20 Gy X 3 fractions = 60 GyT2 = 22 Gy X 3 fractions = 66 GyT2 = 22 Gy X 3 fractions = 66 Gy
•• Control and toxicity monitored by independent Control and toxicity monitored by independent Data Safety Monitoring CommitteeData Safety Monitoring Committee
•• 70 patients (35 T1, 35T2)70 patients (35 T1, 35T2)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
IU Phase II Local ControlIU Phase II Local ControlLocal Tumor Control
0 12 24 36 48
Months from Therapy
100
80
60
40
20
0
Per
cent
Loc
ally
Con
trolle
d
n=5
n=60 n=32n=70
Preliminary Preliminary ResultsResults
•• Median Median followfollow--up = up = 18 months18 months
•• One year One year local control local control = 98%= 98%
•• Two year Two year local control local control = 95%= 95%

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
PrePre--RxRx
3 mo.3 mo.
9 mo.9 mo.
15 mo.15 mo.
15 mo.15 mo.
T1 Patient, 60 GyT1 Patient, 60 Gy
•• Ongoing heavy smokingOngoing heavy smoking•• Local recurrence at 15 mo.Local recurrence at 15 mo.•• Fatal hemoptysis at 19 months Fatal hemoptysis at 19 months
postpost--RxRx•• Death scored related to RxDeath scored related to Rx

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Grade 3Grade 3--5 Toxicity: Location5 Toxicity: Location
p = 0.003

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
T2 tumor, 42 GyT2 tumor, 42 Gy
PrePre--TreatmentTreatment
10 wks. Post10 wks. Post--TreatmentTreatment
6 wks. Post6 wks. Post--TreatmentTreatment((radiation pneumonitisradiation pneumonitis))
Grade 3 Radiation PneumonitisGrade 3 Radiation Pneumonitis

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Skin/Chest Wall ToxicitySkin/Chest Wall Toxicity
Solution: Spread out entrance dose (more beams)Solution: Spread out entrance dose (more beams)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Malignant Obstruction Malignant Obstruction ––Recurrent NSCLCRecurrent NSCLC
CTCT--PET FusionPET Fusion
EsophagusEsophagusTargetTarget
SBRT treatmentSBRT treatment

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Malignant Obstruction Malignant Obstruction ––Recurrent NSCLCRecurrent NSCLC
4 Months Post4 Months Post--Rx Upper Endoscopy Rx Upper Endoscopy –– Severe Esophagus DamageSevere Esophagus Damage

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
RTOG 0236 Dose ConstraintsRTOG 0236 Dose Constraints

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
TolerancesTolerances•• Based on some experience, some derivation, and Based on some experience, some derivation, and
considerable speculation for 3 fraction treatments considerable speculation for 3 fraction treatments –– not validated with long term datanot validated with long term data
•• Total dose limits over 3 fractions:Total dose limits over 3 fractions:Spinal cordSpinal cord any pointany point 18 Gy 18 Gy EsophagusEsophagus any pointany point 27 Gy 27 Gy Trachea/BronchusTrachea/Bronchus any pointany point 30 Gy 30 Gy Heart/Great VesselsHeart/Great Vessels any pointany point 30 Gy 30 Gy Brachial plexusBrachial plexus any pointany point 24 Gy 24 Gy SkinSkin any pointany point 1818--24* Gy24* Gy
*15 Gy if in a skin fold*15 Gy if in a skin fold

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
RTOG 0236 StatusRTOG 0236 Status•• RTOG 0236 Phase II: SBRT using 54 Gy in 3 RTOG 0236 Phase II: SBRT using 54 Gy in 3
fractions for patients with early stage medically fractions for patients with early stage medically inoperable lung cancerinoperable lung cancer
•• ExcludedExcluded patients with central tumorspatients with central tumors
•• Closed October 2006 after enrolling 56 patientsClosed October 2006 after enrolling 56 patients
•• Median Median f/uf/u 9 months, one patient with local failure 9 months, one patient with local failure (toxicity analysis at ASTRO annual meeting)(toxicity analysis at ASTRO annual meeting)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
RTOG Stage I Lung CancerRTOG Stage I Lung CancerStage I PatientStage I Patient
OperableOperable MedicallyMedicallyInoperableInoperable
CentralCentral PeripheralPeripheral CentralCentral PeripheralPeripheral
AwaitAwait06330633
0618 0618 ––Phase IIPhase IIbasedbased
on 0236on 0236
0633 0633 ––Phase IPhase I
0236 0236 ––Phase IIPhase II
0624 0624 ––Phase IIPhase IIĉĉSystemicSystemic

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
RTOGRTOG--0618: Stereotactic Body 0618: Stereotactic Body Radiation Therapy (SBRT) in Radiation Therapy (SBRT) in
Operable Early Stage NonOperable Early Stage Non--small small Cell Lung CancerCell Lung Cancer
PI: Robert Timmerman, M.D.PI: Robert Timmerman, M.D.Surgery CoSurgery Co--PI: Harvey Pass, M.D.PI: Harvey Pass, M.D.Med Med OncOnc CoCo--PI: Marty Edelman, M.D.PI: Marty Edelman, M.D.Pathology CoPathology Co--PI: William PI: William GeddieGeddie, M.D., M.D.ComorbidityComorbidity CoCo--PI: Beth Gore, M.D.PI: Beth Gore, M.D.Physics CoPhysics Co--PI: Jim Galvin, Ph.D.PI: Jim Galvin, Ph.D.

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Should Surgery be Challenged?Should Surgery be Challenged?•• Surgery is not a perfect treatmentSurgery is not a perfect treatment
•• Local failures, death from cancer (even controlling Local failures, death from cancer (even controlling for pathological staging)for pathological staging)
•• Toxicity, pain and sufferingToxicity, pain and suffering
•• ExpenseExpense-- hospitalization, recovery, lost work/income, hospitalization, recovery, lost work/income, etc.etc.

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Legitimate Alternative to Legitimate Alternative to Lobectomy for Stage I NSCLCLobectomy for Stage I NSCLC
•• Requirements:Requirements:-- Local control Local control 90%90% or more at or more at 5 years5 years (actuarial)(actuarial)-- Survival Survival 6060--80%80% at at 5 years5 years (actuarial)(actuarial)-- Grade III or higher toxicity Grade III or higher toxicity <15<15--20%20%-- Ideally less invasive than thoracotomyIdeally less invasive than thoracotomy-- Ideally more convenientIdeally more convenient-- Ideally less costlyIdeally less costly-- All proven by prospective testingAll proven by prospective testing

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
RTOG 0618RTOG 0618•• Build on experience, guidelines, and QA program Build on experience, guidelines, and QA program
from RTOG 0236 using 18 Gy X 3 fractions (54 from RTOG 0236 using 18 Gy X 3 fractions (54 Gy) given in about one weekGy) given in about one week
•• Primary objective = 2 year local control, Primary objective = 2 year local control, secondary objectives survival and toxicitysecondary objectives survival and toxicity
•• Target local control = 90% (similar to lobectomy) Target local control = 90% (similar to lobectomy) justifying treatment dosejustifying treatment dose

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
94% (3 years)94% (3 years)12 12 GyGy X 4X 4Nagata, 2005Nagata, 2005
70% (3 years)70% (3 years)6 6 GyGy X 8X 8OnimaruOnimaru, 2003, 2003
100% (3 years)100% (3 years)7.5 7.5 GyGy X 8X 8OnimaruOnimaru, 2003, 2003
80% (3 years)80% (3 years)3030--34 34 GyGy X 1X 1Hara, 2006Hara, 2006
95% (3 years)95% (3 years)5 5 GyGy X 10X 10XiaXia, 2006, 2006
AsiaAsia
90% (2 years)90% (2 years)1818--24 24 GyGy X 3X 3Timmerman, 2003Timmerman, 2003
87% (3 years)87% (3 years)12.5 12.5 GyGy X 3X 3Zimmerman, 2005Zimmerman, 2005
80% (crude)80% (crude)15 15 GyGy X 3X 3Nyman, 2006Nyman, 2006
80% (3 years)80% (3 years)30 30 GyGy X 1X 1Fritz, 2006Fritz, 2006
80% (3 years)80% (3 years)15 15 GyGy X 3X 3Bauman, 2006Bauman, 2006
95% (2+ years)95% (2+ years)2020--22 22 GyGy X 3X 3Timmerman, 2006Timmerman, 2006
NorthNorth AmericaAmerica//EuropeEurope
Local ControlLocal ControlTreatmentTreatmentAuthorAuthor
Local Control LungLocal Control Lung
••In all series, tumor recurrence is late (median about 18 months)In all series, tumor recurrence is late (median about 18 months)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
WhatWhat’’s the Right Dose?s the Right Dose?•• Many institutional experiences (some called phase Many institutional experiences (some called phase
II) using a variety of prescriptions dosesII) using a variety of prescriptions doses
•• Most often, dose was chosen by institutional Most often, dose was chosen by institutional leader(sleader(s) using educated guessing or conversions) using educated guessing or conversions
•• Only two classic phase I dose finding studies Only two classic phase I dose finding studies published (Indiana and Cleveland)published (Indiana and Cleveland)
•• Editorial: Retrospective pooling of multiple Editorial: Retrospective pooling of multiple institution data using different dose prescriptions is institution data using different dose prescriptions is NOT a legitimate dose finding studyNOT a legitimate dose finding study

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Classic Methodology for Classic Methodology for Prospectively Determining Optimal Prospectively Determining Optimal Therapy Dose for Lethal CancersTherapy Dose for Lethal Cancers
•• Want to find a balanced between benefit and harm Want to find a balanced between benefit and harm from the new therapyfrom the new therapy
•• Start with phase I dose escalation toxicity study Start with phase I dose escalation toxicity study ––ONLY variable effecting outcome is doseONLY variable effecting outcome is dose
•• Escalate until exceeding predetermined level of Escalate until exceeding predetermined level of severe toxicity (usually 15severe toxicity (usually 15--20%)20%)
•• Determine highest (maximum) tolerable dose (MTD)Determine highest (maximum) tolerable dose (MTD)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Further TestingFurther Testing•• Phase II study:Phase II study:
-- Use the MTD from the phase I study (cancer is a tough Use the MTD from the phase I study (cancer is a tough competitor)competitor)
-- Treat more patients at this dose than in the phase I Treat more patients at this dose than in the phase I study (e.g., 50 patients rather than 10)study (e.g., 50 patients rather than 10)
-- Confirm toxicity with larger sample (<15Confirm toxicity with larger sample (<15--20% severe)20% severe)-- Look for glimmer of benefit (inconclusive)Look for glimmer of benefit (inconclusive)
•• Phase III study:Phase III study:-- Randomized Randomized –– controls for selection bias (not true for controls for selection bias (not true for
phase II)phase II)-- Compares the most potent form of the new therapy vs. Compares the most potent form of the new therapy vs.
standardstandard

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Why Use the MTD in a Phase III Trial?Why Use the MTD in a Phase III Trial?•• Assume cancer recurrence is potentially deadlyAssume cancer recurrence is potentially deadly
•• You usually get only one chance at a phase III trial:You usually get only one chance at a phase III trial:-- Phase III trials are very expensive (around $6000 per patient)Phase III trials are very expensive (around $6000 per patient)-- Phase III trials are big (usually over 100 patients)Phase III trials are big (usually over 100 patients)-- Phase III trials take a long time (therapies change)Phase III trials take a long time (therapies change)-- Colleagues consider treatment a black box (perturbations donColleagues consider treatment a black box (perturbations don’’t t
matter)matter)
•• Example of moving the wrong form of a therapy to phase Example of moving the wrong form of a therapy to phase III:III:-- Radiation vs. surgery for inguinal lymph node therapy in Radiation vs. surgery for inguinal lymph node therapy in vulvarvulvar
CACA

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Further Testing IIFurther Testing II•• Assume new therapy wins in the phase III trialAssume new therapy wins in the phase III trial
•• Now do refinement studies (phase II or III)Now do refinement studies (phase II or III)-- Change schedule (e.g., number of fractions)Change schedule (e.g., number of fractions)-- Change dose (deChange dose (de--escalate)escalate)-- Change technique (e.g., shrink margins)Change technique (e.g., shrink margins)-- Add combination therapyAdd combination therapy-- etc.etc.

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Question?Question?•• Since the only formal prospective phase I study Since the only formal prospective phase I study
completed for lung cancer using SBRT was the completed for lung cancer using SBRT was the Indiana University trial (MTD = 54Indiana University trial (MTD = 54--60 60 GyGy in 3 in 3 fractions),fractions),
Why doesnWhy doesn’’t everyone use this dose for further t everyone use this dose for further study rather than the multitude of dose study rather than the multitude of dose prescriptions seen in institutional published prescriptions seen in institutional published reports?reports?

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Answer(sAnswer(s))•• Several trials were already ongoing and reporting Several trials were already ongoing and reporting
good preliminary results (e.g., from Germany and good preliminary results (e.g., from Germany and Japan) prior to completing and publishing the Japan) prior to completing and publishing the Indiana trialIndiana trial
•• 5454--60 60 GyGy in 3 fractions sounds kind of frighteningin 3 fractions sounds kind of frightening
•• Editorial: The starting dose for the Indiana trial Editorial: The starting dose for the Indiana trial was 24 was 24 GyGy in 3 fractions, the in 3 fractions, the whimpiestwhimpiest dose dose ever used in a SBRT trial!ever used in a SBRT trial!

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Typical Slide Shown at MeetingsTypical Slide Shown at Meetings
10010072722 2 GyGy X 30 = 60 X 30 = 60 GyGy
460 460 (192%)(192%)180 (170%)180 (170%)20 20 GyGy X 3 = 60 X 3 = 60 GyGy300 300 (125%)(125%)132 (125%)132 (125%)12 12 GyGy X 5 = 60 X 5 = 60 GyGy330 330 (138%)(138%)120 (113%)120 (113%)30 30 GyGy X 1 = 30 X 1 = 30 GyGy270 (113%)270 (113%)113 (107%)113 (107%)15 15 GyGy X 3 = 45 X 3 = 45 GyGy240 (100%)240 (100%)106 (100%)106 (100%)12 12 GyGy X 4 = 48 X 4 = 48 GyGy
BEDBED--3 (3 (GyGy))LateLate
BEDBED--10 (10 (GyGy))Early (tumor)Early (tumor)
Prescription DosePrescription Dose

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Models in Radiation OncologyModels in Radiation Oncology•• Models are NOT real!Models are NOT real!
-- ““All models are wrong. Some models All models are wrong. Some models are useful". are useful". -- George BoxGeorge Box
•• Results from models do NOT trump Results from models do NOT trump measured datameasured data..
•• If there is a discrepancy between If there is a discrepancy between the model and data, believe the data.the model and data, believe the data.

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
The Actual DataThe Actual Data

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Linear Quadratic ModelLinear Quadratic Model•• Originally called the Originally called the ““theory of dual radiation theory of dual radiation
actionaction”” by by KellererKellerer and Rossi in describing high vs. and Rossi in describing high vs. low LET radiation (1972)low LET radiation (1972)
•• Truncated power series (two terms) Truncated power series (two terms) -- Fits the Fits the shoulder very wellshoulder very well
•• Cell kill contributions from linear and quadratic Cell kill contributions from linear and quadratic termsterms
•• DNA double strand breaks DNA double strand breaks incorporated incorporated as as mechanism of cell inactivationmechanism of cell inactivation

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
LQ ModelLQ Model
βd2
αd Dose
Ln( SF)
)( 2DDeSF ⋅+⋅−= βα

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Survival CurveSurvival Curve from from ExperimentsExperiments
•• The first known mammalian cell survival curveThe first known mammalian cell survival curve
Puck and Marcus, J Exp Med, 1956;103:653

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
OverOver--Prediction by LQ and BEDPrediction by LQ and BED
LQ curve Curve from experiments
DoseO
A
B
Ln(SF)
actual effect
LQ-predicted effect
Dose (Gy)
C
D
E
slope = - α
F G
actual BED BEDLQ
over-estimation

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
•• GuerreroGuerrero--Li Modified LQ model and Curtis LethalLi Modified LQ model and Curtis Lethal--PotentiallyPotentially--Lethal ModelLethal Model-- Mathematically soundMathematically sound-- Too complicated for everyday clinical use.Too complicated for everyday clinical use.-- Modification factors not well characterized.Modification factors not well characterized.
•• Using extremely large Using extremely large αα//ββ ratio (~ 20 Gy)ratio (~ 20 Gy)-- Valid?Valid?-- The curve straightens, but the lowThe curve straightens, but the low--dose fit suffersdose fit suffers..
Models for SBRTModels for SBRT
Guerrero, Phys Med Biol, 2004, 49:4825Curtis, Radiat Res, 1986, 106:252Fowler, Personal Communications

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
H460 Survival CurveH460 Survival Curve

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
H460 Fitted with LQH460 Fitted with LQ(applied only to low dose range)(applied only to low dose range)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
H460 Fitted with LQH460 Fitted with LQ(entire dose range)(entire dose range)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
H460 Hybrid Curve Fit H460 Hybrid Curve Fit (entire dose range)(entire dose range)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
The MultiThe Multi--target modelstarget models•• Originally proposed by Originally proposed by
Puck and Markus (1956)Puck and Markus (1956)
•• Each cell contains a Each cell contains a defined number of critical defined number of critical sites (targets) each of sites (targets) each of which are essential for which are essential for survivalsurvival
•• Terminal portion is Terminal portion is exponential (linear on log exponential (linear on log scale) consistent with datascale) consistent with data

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Single Fraction Equivalent DoseSingle Fraction Equivalent Dose•• Definition: Definition: ““The dose of radiation, if The dose of radiation, if delivered in a delivered in a
single fractionsingle fraction,, that that would achievewould achieve the same the same effecteffectas the doseas the dose--fractionation scheme in question.fractionation scheme in question.””
•• Can be used just like how BED is being used for Can be used just like how BED is being used for CFRT. CFRT. -- To compare potency and toxicity.To compare potency and toxicity.-- To design rational dose escalation schemeTo design rational dose escalation scheme
•• More intuitive than BED.More intuitive than BED.

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
SFED for SBRTSFED for SBRT
Dose = f · d
A
SFEDSBRT
Dq
Dq
Dq Dq
Dq
BCD
Ln(SF)
O Dose (Gy)
A’
qSBRT D1)(fDSFED ⋅−−=

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Updated ComparisonsUpdated Comparisons
56 56 (133%)(133%)180 (170%)180 (170%)20 20 GyGy X 3 = 60 X 3 = 60 GyGy52 52 (124%)(124%)132 (125%)132 (125%)12 12 GyGy X 5 = 60 X 5 = 60 GyGy30 30 (71%)(71%)120 (113%)120 (113%)30 30 GyGy X 1 = 30 X 1 = 30 GyGy41 (98%)41 (98%)113 (107%)113 (107%)15 15 GyGy X 3 = 45 X 3 = 45 GyGy42 (100%)42 (100%)106 (100%)106 (100%)12 12 GyGy X 4 = 48 X 4 = 48 GyGy
SFEDSFED--2 (2 (GyGy))BEDBED--10 (10 (GyGy))Early (tumor)Early (tumor)
Prescription DosePrescription Dose

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
SBRT + SBRT + ErlotinibErlotinib for 2for 2ndnd Line Line Therapy in NSCLC (PI, Therapy in NSCLC (PI, KavanaghKavanagh))
•• NSCLC failed 1NSCLC failed 1stst line chemotherapyline chemotherapy
•• ≤≤ 6 discrete lesions (any site except brain)6 discrete lesions (any site except brain)
•• Week 1 Week 1 ErlotinibErlotinib, Week 2, Week 2--4 4 SBRT+ErlotinibSBRT+Erlotinib, Week , Week 5+ 5+ ErlotinibErlotinib until progressionuntil progression
•• Endpoint = progression free survivalEndpoint = progression free survival
•• Test of NortonTest of Norton--Simon hypothesisSimon hypothesis

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Extreme or Ablative Extreme or Ablative HypofractionationHypofractionation•• One option to increase dose potency (others One option to increase dose potency (others
include sensitizers, etc) and control tumorsinclude sensitizers, etc) and control tumors
•• Obviously will cause late effects (desirable in Obviously will cause late effects (desirable in tumor, not in normal tissues)tumor, not in normal tissues)
•• Must follow patients carefully for long periodsMust follow patients carefully for long periods
•• More SBRT prospective trials than any other More SBRT prospective trials than any other radiotherapy related innovation in history of field radiotherapy related innovation in history of field (doesn(doesn’’t mean itt mean it’’s not used inappropriately)s not used inappropriately)

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Obvious SBRT ShortcomingsObvious SBRT Shortcomings•• SBRT enabled by technological innovation. BUT, SBRT enabled by technological innovation. BUT,
wonwon’’t be enough to allow broad implementationt be enough to allow broad implementation
•• We donWe don’’t understand mechanisms of actiont understand mechanisms of actionVascular injury?Vascular injury?Mucosal injury?Mucosal injury?Supporting Supporting stromalstromal injury?injury?
•• Can this injury be modulated?Can this injury be modulated?
•• Frontier of basic/translational science researchFrontier of basic/translational science research

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
ConclusionsConclusions•• Technology facilitates, but does not always allow, Technology facilitates, but does not always allow,
ablative dose SBRTablative dose SBRT•• SBRT requires different strategy formulation (e.g., SBRT requires different strategy formulation (e.g.,
abandon adjuvant Rx)abandon adjuvant Rx)•• Medically inoperable early stage lung cancer has Medically inoperable early stage lung cancer has
been an important clinical model to test SBRTbeen an important clinical model to test SBRT•• Toxicity is late and mostly related to serial organsToxicity is late and mostly related to serial organs•• Put LQ to BEDPut LQ to BED•• Investigation is continuing in multiple organ modelsInvestigation is continuing in multiple organ models•• SBRT may realistically challenge surgerySBRT may realistically challenge surgery

DEPT OF RADIATION ONCOLOGYDEPT OF RADIATION ONCOLOGY
Happy Trials!Happy Trials!