Embed Size (px)
Citation preview

Pediatr Surg Int (1994) 9:429-430 © Springer-Verlag 1994
C A S E R E P O R T
Appendix vermiformis duplex - a lesson for the unwary
Javed Akhtar, Tallat Ejaz, and Edward J. Guiney
Department of Paediatric Surgery, Our Lady's Hospital for Sick Children, Crumlin, Dublin 2 Ireland
Accepted 4 May 1993
Abstract. Appendix vermiformis du- plex is a rare phenomenon. A case of a double appendix with one caecum and inf lammation of one of the appendices is presented. The unusual presentations of the anomaly can cause diagnostic di lemmas. Awareness of a duplicat ion is important, as failure to recognise the condit ion may lead to cl inical pro- blems and possible litigation.
Key words: Vermiform appendix - Duplex - Duplicat ion - Inf lammation
Introduction
Duplicat ion occurs in about 1 in 12,500 human appendices [2]. In- f lammation of the two appendices se- parately can cause diagnostic difficulty at an initial operat ion or subsequent explorat ion [3]. The anomaly can mimic other condit ions such as colonic carcinoma in adults [1]. Awareness of this anomaly can prevent errors in clinical management and possible liti- gation.
Case report Discussion
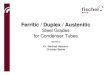
A 9-year-old Caucasian boy was admitted with a clinical diagnosis of suspected acute appen- dicitis. Examination under anaesthesia re- vealed a small mass, thought to be of appen- dicular origin, in the right iliac fossa. On opening the abdomen through a Lanz incision, a normal appendix was found in the anterior position. There was no evidence of mesenteric adenitis or a Meckel's diverticulum. After appendicectomy, the mass could still be pal- pated in relation to the posterior caecal wall. Following retrocaecal dissection, an inflamed, cystic lesion with a lumen communicating with the caecum was identified and excised (Fig. 1). Postoperative recovery was unevent- ful. Histopathological examination of the specimens confirmed a normal anterior and an inflamed retrocaecal appendix.
The first description of duplication of the vermiform appendix was made by Picoli in 1892 [4]. Collins found four cases of appendix duplex in a study of 50,000 human appendices [2], an in- cidence of 1 in 12,500. However, fewer than 100 cases have been reported in the world literature [3]. One case of triple appendix has been recorded [5].
The accepted Wallbr idge classifi- cation [6] describes three types of the anomaly, namely: A: a single caecum with partial duplicat ion of a normal ly sited appendix; B: a single caecum with two separate appendices; sub- types, B l : two appendices arising on
Correspondence to: J. Akhtar, Department of Paediatric Surgery, The Royal Hospital for Sick Children, Yorkhill, Glasgow G3 8SJ, Scotland
Fig. 1. The second (duplicated) appendix presenting as an inflamed cystic lesion, excised with mesoappendix from posterior aspect of caecum

430
either side of the ileocaecal valve [avian type], B2: a normally sited appendix with an additional appendix arising from the caecum along the line of a taenia [taenia coli type]; and C: a double caecum, each bearing its own appendix. The case reported here was of the B2 variety. There was no evi- dence of associated congenital ab- normalities, which are more common with types B1 and C [1].
Different theories have been pre- sented to explain the aetiology of ap- pendix duplex. These include: (1) persistence of a transient appendix appearing in the 10-mm embryo, which normally atrophies, leading to type A or B2 duplication [1, 4, 6]; (2) failure of proper differentiation of the cloaca, giving rise to type B1 [1]; (3) partial twinning of hindgut struc- tures, resulting in type C duplication [1]; (4) failure of obliteration of one of the two caeca in greater specialisation of mammals [4]; and (5) phylogenetic reversion to the paired caecal arrange- ment found in birds [4, 6[. The phy- logenetic theory is supported neither by the evolutionary development of man [6] nor by the case of triple ap- pendix, which can probably be ex- plained by a genetically determined disordered tissue-organizer action [5].
The majority of cases of duplication of the appendix are found at lapar- otomy for reasons other than acute appendicitis or at post-mortem ex- amination. It may present as acute ap- pendicitis in which one or both ap- pendices are inflamed [4], however, it poses a diagnostic dilemma when the patient presents with inflammation of the second appendix after a previous appendicectomy [3]. In this situation, other conditions such as a solitary caecal diverticulum, carcinoid tumour, endometriosis, colonic polyp, lipoma, Crohn's disease, pseudoduplication, and adenocarcinoma have to be con- sidered. If clinical findings and radio- logical imaging suggest malignant disease, an unnecessarily extensive bowel resection [5], with the asso- ciated clinical and emotional problems, may follow.
The diagnosis of appendix duplex is confirmed when mucosa normally found in the appendix, lymphoid fol- licles in the lamina propria, and two muscular layers are seen on histologi- cal examination of an excised caecal appendage. Moreover, it is necessary to confirm the presence of a complete tip from each appendix to exclude the possibility of a residual stump after previous subtotal appendicectomy. In
our case, the anomalous lesion was found at operation because of the pre- sence of a persisting mass following removal of a normal appendix. How- ever, failure to recognise the anomaly can result in a difficult clinical di- lemma. As the majority of emergency appendicectomies are performed by surgeons in training with varying de- grees of experience, they should be aware of the anomaly. Each patient must be assessed clinically regarding the need for surgical intervention; an appendicectomy scar does not always exclude acute appendicitis!
References
1. Bluett MK, Halter SA, Salhany KE, O'Leary JP (1987) Duplication of the ap- pendix mimicking adenocarcinoma of the colon. Arch Surg 122:817-820
2. Collins DC (1955) A study of 50,000 spe- cimens of the human vermiform appendix. Surg Gynaecol Obstet 101:437-446
3. Harman J, Schroeder D (1986) Double appendix. NZ Med J 99:469
4. Khanna AK (1983) Appendix vermiformis duplex. Postgrad Med J 59:69-70
5. Tinckler LF (1968) Triple appendix ver- miformis - a unique case. Br J Surg 55: 79-81
6. Wallbridge PH (1963) Double appendix. Br J Surg 50:346-347





















![Duplex and Super Duplex [Fittings and Flanges] final](https://img.dokumen.tips/doc/110x75/61a6ddf752ba2a16af77519c/duplex-and-super-duplex-fittings-and-flanges-final.jpg)





