Embed Size (px)
Citation preview

The Saudi Journal for Dental Research (2016) 7, 69–72
King Saud University
The Saudi Journal for Dental Research
www.ksu.edu.sawww.sciencedirect.com
CASE REPORT
Aplastic anemia presenting as bleeding of gingiva:
Case report and dental considerations
* Corresponding author. Tel.: +91 8802536376.
E-mail addresses: [email protected] (A. Rai), drvnmasur@
gmail.com (V.G. Naikmasur), [email protected] (A. Kumar).1 Fax: +91 8362467612.
Peer review under responsibility of King Saud University.
Production and hosting by Elsevier
http://dx.doi.org/10.1016/j.sjdr.2015.04.0042352-0035 ª 2015 The Authors. Production and hosting by Elsevier B.V. on behalf of King Saud University.This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Arpita Rai a,*, Vanita Vaishali b, Venkatesh G. Naikmasur c,1, Ansul Kumar d,
Atul Sattur c
a Department of Oral Medicine and Radiology, Faculty of Dentistry, Jamia Millia Islamia, New Delhi 110025, Indiab College of Dental Sciences and Hospital, Indore, Indiac Department of Oral Medicine and Radiology, S.D.M. College of Dental Sciences & Hospital, Dharwad, Karnataka 580 009, Indiad Dr. RML PGIMER Hospital, New Delhi, India
Received 10 April 2015; accepted 18 April 2015
Available online 27 April 2015
KEYWORDS
Aplastic anemia;
Pallor;
Petechiae;
Hematoma;
Gum bleeding
Abstract The article describes a case of aplastic anemia in a 44-year-old male patient which pre-
sented as spontaneous bleeding of gums. Though bleeding of gums is a very common complaint
encountered in a dental clinic, bleeding of gums due to systemic causes is an infrequent finding.
Patient from blood dyscrasias may present in a dental office with bleeding of gums as sole or the
first complaint. The acknowledgment of the patients underlying condition is the responsibility of
the dentist for pertinent referral and further management.ª 2015 The Authors. Production and hosting by Elsevier B.V. on behalf of King Saud University. This is
an open access article under the CCBY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Aplastic anemia is a serious and often fatal hematologic disor-der characterized by hypoplastic bone marrow and peripheralpancytopenia. Aplastic anemia is a rare, non contagious and
potentially life threatening disorder caused by destruction ofpluripotent stem cells in the bone marrow with an annual
incidence of 2 to 6/1,000,000.1 In contrast to the term ‘aplastic
anemia’, suggesting suppression of erythropoietic cell lines, allcell lines may be affected in this disorder.2 Depending onaffected cell lines, aplastic anemia is associated with not only
fatigue, but also bleeding due to thrombocytopenia and recur-rent infections due to neutropenia.3 The diagnosis ‘aplasticanemia’ is confirmed by hypocellularity of the bone marrow.
The remaining cells are morphologically unaffected withoutmalignant infiltration.
Aplastic anemia is classified as acquired or congenital. Thecongenital type is rare and usually associated with Fanconi’s
anemia and dyskeratosis congenita.4 In more than 50% ofthe acquired cases of aplastic anemia, the cause is unknown.Potential triggers for the onset of aplastic anemia include
T-cell mediated auto-immune disease, iatrogenic agents, viralinfection and pregnancy.1 This notion is supported by thesimilar incidence of aplastic anemia in men and women.1 It

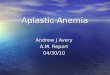
Figure 1 Clinical photograph of the patient showing extreme
pallor of lower palpebral conjunctiva.
70 A. Rai et al.
is more common in Asian countries than in the United Statesand Europe with about 6000–7000 new diagnosis reportedannually worldwide. It can appear at any age but is most com-
monly diagnosed in children aged 2–5 years, young adultsbetween 20 and 25 years and adults aged 55–60 years.5
A wide array of disorders of red cells and hemostasis
encountered in internal medicine has manifestations in the oralcavity and the facial region. These manifestations must beproperly recognized if the patient must receive appropriate
diagnosis and referral for treatment. Though bleeding of gumsis a very common complaint encountered in a dental clinic,bleeding of gums due to systemic causes is an infrequent find-ing. Patients from blood dyscrasias may present in a dental
office with bleeding of gums as the sole or the first complaint.Acknowledgment of the patients underlying condition is theresponsibility of the dentist for pertinent referral and further
management.
Figure 2 Clinical photograph of the patient showing pallor of
nail beds.
Figure 3 Intra-oral photograph showing oral hematoma on the
right buccal mucosa in relation to the line of occlusion in the
molar region which is approximately 2 mm in size.
2. Case report
A 44-year-old patient reported to the Department of OralMedicine and Radiology with complaints of bleeding of gumsfor the duration of 1 month. Bleeding of gums was sponta-
neous and continuous. Greater frequency of bleeding wasnoticed in the early mornings. Bleeding occurred from allquadrants of the mouth and the patient reported that about
one cup of blood per day was oozing from the gums. Thepatient reported a negative history of rectal bleeding, hemopt-ysis or hematemesis. The patient had visited a local physician20 days back and had been prescribed antibiotics (metronida-
zole, albendazole), vitamin C supplement and a multivitamin.He also gave a history of acid peptic disease for the past25 years. Patient reported a history of easy bruising and
reported ecchymosis and petechiae on arms, legs and buttocks.On examination, extreme pallor of lower palpebral conjunctiva(Fig. 1), nail beds (Fig. 2) and palms was evident. Ecchymotic
patches were present on the left lower limb, right arm and dor-sogluteal region bilaterally. Intra oral examination revealedgeneralized pallor of the oral mucosa. There was presence of
multiple hematomas on the oral mucosa, one on the right buc-cal mucosa (Fig. 3), two on the left buccal mucosa and two onthe upper labial mucosa (Fig. 4). The hematomas were bluishred, approximately 2–3 mm in size and non-tender. The tongue
showed pallor and three hematomas were present on the dorsalsurface (Fig. 5). Pallor of hard and soft palate was marked.Generalized gingival recession was evident with oozing of
blood from the gingiva which was more evident in the loweranterior region (Fig. 6). There was collection of blood in thelower vestibule. On manipulation, there was accentuated
bleeding of gingiva (Fig. 7).Panoromic radiograph revealed generalized extensive alve-
olar bone loss. Hemogram of the patient revealed pancytope-nia with RBC count of 1.92 millions/mm3 and hemoglobin
was 6.6 gm%. Total leukocyte count was 1100 cells/mm3
(P–40%, L–60%, M–0%, E–0%, B–0%). ESR was raised to92 mm in the 1st hour. Bleeding time was more than 15 min,
though the Clotting time was 4.30 min. Platelet count hadreduced to 19,000 cells/mm3. The peripheral smears revealedanisopoikilocytosis in relation to red blood cells. There was
reduction in the number of white blood cells with a shift tothe left. There was also a reduction in the number of platelets.

Figure 4 Intra-oral photograph showing two hematomas on the
upper labial mucosa. The lesion on the right side is formed by
coalescing of multiple small lesions.
Aplastic anemia presenting as bleeding of gingiva 71
Bone marrow aspiration cytology was advised to the patientwhich revealed bone marrow aplasia (Fig. 8). The diagnosisof aplastic anemia was established and the patient was referred
to a higher center for further investigation and management.Oral hygiene instructions were given to the patient. The
patient was also advised to use tranexamic acid mouthwash
to control spontaneous gingival bleeding. Further manage-ment of chronic periodontitis was synchronized with platelettransfusions received by the patient.
3. Discussion
Aplastic anemia is a rare hematologic disease characterized bya hypoplastic bone marrow and peripheral pancytopenia. A
pancytopenia is diagnosed when two of three criteria aremet: a neutrophil count of less than 0.5 · 109 cells/L, a plateletcount less than 20 · 109 cells/L and a reticulocyte count less
than 1%. When the neutrophil count is less than 0.2 · 109,the disease is then characterized as severe.1
Oral manifestations are common in patients with aplastic
anemia and are directly associated with pancytopenia. These
Figure 5 Intra-oral photograph showing three hematomas on
the dorsum of the tongue.
manifestations include petechial hemorrhages, gingival swel-ling and spontaneous bleeding, ulceration, pallor and severeperiodontal disease.4,6–8 Gingivitis and periodontitis have been
reported in 36.36% of the patients with Fanconi’s anemiawhich is not associated with the lower platelet count but isattributed to poor oral hygiene.9 Cases of advanced or rapidly
progressive periodontitis have been reported to occur with pro-longed neutropenia and may be due to several qualitative andquantitative neutrophil defects, including neutropenia, agranu-
locytosis and leukocyte adhesion deficiency.6 In addition,thrombocytopenia can induce compromised clotting, so surgi-cal intervention should be delayed until the patient is con-trolled with platelet administration.4 Gingival bleeding is
another common manifestation associated with decreased pla-telet level seen in aplastic anemia patients.7 Oral traumatic andpetechial hemorrhagic lesions have been associated with the
decreased platelet level.8 Brennan6 describes the risk factorsassociated with oral manifestations of aplastic anemia and sug-gests that the level of thrombocytopenia is not necessarily
indicative of the degree of petechial hemorrhaging. Theselesions most likely result from the thrombocytopenia-inducedclotting disorder, which causes excessive bleeding after minor
trauma associated with normal oral functioning.In patients first choice therapy for aplastic anemia is
allogenic stem cell transplantation with a 5-year survival of70–80%.10 Graft rejection and graft-versus host disease remain
serious risks, but can be contained by careful patient manage-ment. A supportive therapy with erythrocyte and platelettransfusions is a widely used, reasonable alternative. The ben-
efit of transfusions to prevent bleeding should be weighedagainst the likelihood of developing HLA antibodies andhemochromatosis.11 In case the patient responds insufficiently
to supportive therapy, immune-modulating treatment basedon a short course of anti-thymocyte globulin or anti-lympho-cyte globulin and several months of cyclosporin to modulate
the patient’s immune response may be tried. The prognosisof the immune-modulating treatment is relatively high, with5-year survival rates of up to 75%.12
Little research has been published about gingival bleeding
in aplastic anemia. In fact, only case reports and series withsmall sample sizes are available. The present case exemplifiesthe role of the oral physician in diagnosing one of the critical
Figure 6 Intra-oral photograph showing gingival recession with
oozing of blood from the gingival sulcus.

Figure 7 Intra-oral photograph showing accentuated bleeding
o gingiva on manipulation.
Figure 8 Photomicrograph showing the hypocellular bone
marrow.
72 A. Rai et al.
conditions like aplastic anemia through its oral manifestation.Any signs of excessive bleeding, or a poor response to the stan-
dard treatment of infections and oral ulcerations, should beinvestigated to rule out a possibility of pancytopenia.Correlation of the oral presentation of spontaneous and
remarkable gingival bleeding with intra-oral hematomas,ecchymotic patches elsewhere in the body and severe pallorled to the suspicion of pancytopenia. Further investigations
in the form of hemogram and bone marrow aspiration cytol-ogy confirmed the diagnosis of aplastic anemia. Early referralof the patient for specialized care will undoubtedly be of con-siderable value to the patient in the management of this poten-
tially fatal disease.Dental management of patients of aplastic anemia requires
interdisciplinary care with the consultation of the treating den-
tist with hematologist. It is advisable to perform dental
treatment on the day of platelet transfusion.13 To reduce therisk of uncontrolled bleeding during major dental treatments,the patients should take antifibrinolytics. These agents may
decrease bleeding, particularly oral mucosal bleeding, inpatients with thrombocytopenia by stabilization of thrombi.4
Jones et al have reported a case of idiopathic aplastic anemia
which was treated with a combination of modalities includinginitial platelet transfusion, oral hygiene instruction, dental pro-phylaxis and systemic aminocaproic acid.14 Patients with
aplastic anemia are more susceptible to infection; therefore,dental treatment should be postponed until the patient’s whiteblood cell count rises to a normal level.15 Dentists should con-sider prescribing antibacterial mouthwash and oral antibiotics
before dental procedures. Since chronic periodontitis is a focusof infection and considered a potential risk for systemic infec-tion in patients with aplastic anemia, it would be prudent to
treat this condition in consultation with a hematologist.
Conflict of interest
None.
References
1. Young NS. Acquired aplastic anemia. Ann Intern Med
2002;136:534–46.
2. Tichelli A, Socie G, Marsh J, Barge R, Frickhofen N, McCann S,
et al. Outcome of pregnancy and disease course among women
with aplastic anemia treated with immunosuppression. Ann Intern
Med 2002;137:164–72.
3. Snyder TE, Lee LP, Lynch S. Pregnancy-associated hypoplastic
anemia: a review. Obstet Gynecol Surv 1991;46:264–9.
4. Oyaizu K, Mineshiba F, Mineshiba J, et al. Periodontal treatment
in severe aplastic anemia. J Periodont 2005;76:1211–6.
5. Young NS, Kaufman DW. The epidemiology of acquired aplastic
anemia. Haematologica 2008;93:489–92.
6. Brennan MT, Sankar V, Baccaglini L, et al. Oral manifestations
in patients with aplastic anemia. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod 2001;92:503–8.
7. Schofield IDF, Worth AT. Malignant mucosal change in
Fanconi’s anemia. J Oral Surg 1980;38:619–22.
8. Schofield IDF, Abbot WG. Review of aplastic anaemia and report
of a rare case (Fanconi type). JCDA 1978;3:106–8.
9. de Araujo MR, de Oliveira Ribas M, Koubik ACGA, Mattioli T,
de Lima AAS, Franc BHS. Fanconi’s anemia: clinical and
radiographic oral manifestations. Oral Dis 2006. http://
dx.doi.org/10.1111/j.1601-0825.2006.01282.x.
10. Young NS. Current concepts in the pathophysiology and treat-
ment of aplastic anemia. ASH Educ Book 2013. http://dx.doi.org/
10.1182/ asheducation-2013.1.76.
11. Ascarelli MH, Emerson ES, Bigelow CL, Martin Jr JN. Aplastic
anemia and immune-mediated thrombocytopenia: concurrent
complications encountered in the third trimester of pregnancy.
Obstet Gynecol 1998;91(803):806.
12. Brodsky RA, Jones RJ. Aplastic anaemia. Lancet
2005;365:1647–56.
13. Padayachee S, Holmes H, Dreyer WP. Oral medicine case book
56: oral manifestations of aplastic anaemia. SADJ
2014;69(1):26–7.
14. Jones JE, Thomas MS, Coates D, Poland C. Dental management
of idiopathic aplastic anemia: report of a case. Pediatr Dent
1981;3(3):267–70.
15. Sepulveda E, Brethauer U, Rojas J, et al. Oral manifestation of
aplastic anemia in children. J Am Dent Assoc 2006;137(4):474–8.