Embed Size (px)
Citation preview

Anxiety disordersFEB 25 TH 2020, WAVA MCH COR

Agenda TODAY
1. Updates on CME
2. Poll question
3. Didactics and case presentation on Anxiety disorders in children/youth
4. NEXT SESSION is on 3/10/20 ; Managing Trauma in Pediatric Primary care.

Launched: VMAP CME & MOC-4 Project
http://depts.washington.edu/lend/pmh-cor/2019/index.html

POLLING QUESTION
How often are your diagnosing anxiety in your patient population?
1. 10%, 2. 20%, 3. 30%, 4. 50%
What screeners do you use?
1.SCARED
2.SPENCE
3. GAD 7
4. Clinical only

Didactics – anxiety disordersBETH ELLEN DAVIS MD, Professor, Developmental Pediatrics
CECILIA MARGRET MD, Assistant professor, Child and Adol. Psychiatry

Objectives At the end of the session providers will be able to list and discuss the following about childhood and adolescent anxiety disorders
1. Prevalence and presentation
2. Clinical course and subtypes
3. Screening tools
4. Behavioral approaches
5. Medications

Prevalence • 20% of children and youth in primary care will screen positive for anxiety on brief screen
• Presents as PSYCHOSOMATIC condition
• 1 in 8 will have a diagnoses
• Specific disorders like social anxiety, GAD and specific phobias (range 0.5 – 10 %) are common ; Female preponderance
•Only 20-30% with diagnoses have a treatment plan
•

Presentation and course
RISK FACTORS :Neurodevelopmental, parental pathology, behavioral inhibition, adverse events (ACE), traumatic, abnormal arousal state
Comorbidities : Depression 5%, externalizing disorder like ADHD 20%, other anxiety 15 – 50 %
50% of the cohort have comorbidities
Early treatment modifies illness course - Cognitive Behavioral therapy and SSRI /SNRI
Pure anxiety reduces with age, with persistence and increased comorbidities natural progression is into adulthood
Safety CHECKS in children : ABUSE, Bullying, Parental impairment, Psychosis, Medical and Substance abuse
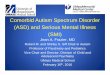
Anxiety is Excess FEAR,AVOIDANCE, NEGATIVE EMOTION and PHYSIOLOGICAL AROUSAL ( Fright, Flight, Fight

Normative and pathological evolution of anxiety disorder – a framework, Beesdo-Baum and Knappe 2012,Clin, NA

SCREENERS SPENCE Children’s anxiety scale ( www.scaswebsite.com)
• Free, has both child and parent and teacher scales, Ages 3- 17 years , screens for anxiety and subtypes
SCARED
• Free, Ages 9 – 17 years, has both child and Parent scales, screens broad and specific types, can be a tracking tool

SCREENERSGAD – 7
• Brief, has only 7 Items, Valid for 14 years and up, greater than 10 triggers evaluation and can be a tracking tool
SCARED for TRAUMA
• Brief, initial scale with 4 items, greater than 6 points to treatment

Screeners links SCARED ( Age 4 – 18)
SCARED traumatic stress disorder scale ( Age 7 – 19)
http://www.seattlechildrens.org/healthcare-professionals/access-services/partnership-access-line/resources/
Spence anxiety scale for children www.scaswebsite.com
CYBOCS ( Age 6 – 17) http://www.cappcny.org/home/media/CYBOCS.pdf
GAD 7 ( Age 11 - 17 )
file:///C:/Users/drcec/Downloads/APA_DSM5_Severity-Measure-For-Generalized-Anxiety-Disorder-Child-Age-11-to-17.pdf
Child PTSD symptom scale (age 8 -1 8) https://www.aacap.org/App_Themes/AACAP/docs/resource_centers/resources/misc/child_ptsd_symptom_scale.pdf

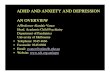
Anxiety subtypes and its comorbidities
(A) Age of onset of anxiety, depression and Substance use disorders
(B) Cumulative incidence of anxiety subtypes into adulthood. (Wehry et al 2015 )

Management

Cognitive Behavioral and Exposure therapies
1. Psychoeducation
2. Relaxation techniques
3. Exposure and response prevention, COPING
4. Externalizing the worry tendencies
5. Reframing the worry/maladaptive thoughts

Effective treatment for anxiety has long lasting benefit
3 arm intervention◦ Sertraline
◦ CBT
◦ Combination or placebo
Randomized control study N > 400
Consistently 24-80% showed improvement to one of three treatment arms, greatest impact for combined treatment (80%)
Piacentini CAMS ( 2014 JAACAP)

When to consider medication ?
WHEN
A. Therapy is LIMITED
B. Moderate to severe impairment
C. Rapid intervention needed
D. Comorbidities needing attention ( Depression or ADHD)
E. Barriers to therapy

Evidences for medications for child and adolescent anxiety disorders, Strawn et al 2012, Clin of N America

Medications : clinical pearls Start LOW and SLOW ( prepubertal age consider 1/3 of recommended dose)
Allow 4 weeks for titration to next dose
Monitor side effects in 2 – 3 weeks ( SI, activation, apathy, GI and weight changes etc. )
Continue successful plan for 6 – 12months which is MAINTENANCE phase
Consider stopping if symptoms are stable – gradual weaning plan, across 3- 6 months and plan for summer
CHOICES other than SSRI when co-morbid conditions or severity of illness are present consider Atomoxetine, alpha agonists, atypical antipsychotics


Overview of subtypes DISORDERS SCREENS THERAPY Primary MEDICATIONS
ANXIETY DISORDERS SCARED, SPENCE, GAD 7
CBT - relaxation, psychoeducation to parents to avoid accommodations, exposure, regulation
SSRI/ SNRI
OCD Children’s Yale-Brown OC scale
CBT SSRI and augmentation with atypical antipsychotic agent
PTSD SCARED traumatic stress scaleChildhood PTSD symptom scale
Trauma focused CBT/ Play therapy
None established * SSRI, alpha agonists
TRICHOTILLOMANIA Clinical Habit reversal therapy SSRI?
EXCORIATION DISORDER
Clinical Habit reversal therapy SSRI?

Resistant to first line care1. Reassess for COMORBIDITIES, SELF- MEDICATION, Sleep Problems
2. Augment with THERAPY ( Family, Substance use, Dialectical Behavioral or IEP at school)
3. Trial another SSRI ( Cross- over or cross titrate across q 1-2 weeks as per tolerance )
4. Self care and sleep hygiene practices, SYSTEMIC supports

QUESTIONS

Case discussion
Patient: 16 yo female with mixed anxiety and depression
Consult ?: Increase SSRI? Suggestions on sleep health?
Symptoms of concern:
At age 14, presented for WCC for entry into HS sports. Based upon patient interactions, SCARED completed:
Parent form Total=34 (high) GAD=17 Social anxiety=9 Patient form Total=27 (high) GAD=13 Social anxiety=9
Referred to counseling and started on escitalopram 10mg. Compliant with Rx, but noncompliant with counseling follow up. Provider declined refill of Rx until follow up in office and resumption of counseling, which induced follow up in office (1/2020)PHQ-9 completed (16) c/w “moderately severe depression”. Patient reports long naps after school/sports, then awakening to complete school work and staying up late at night. Lengthy discussion with family re: sleep hygiene & health: power nap only, strict bedtime.
Screen? See above
Med/dev hx:Patient of practice since birth. First diagnosed with anxiety at 10yo (2013) after Mom reported picking at sites, anxious in situations and worried about events. Referred to counseling. Fell from follow up for three years (no visits).
Meds: Escitalopram (Lexapro)10mg Qday
Family hx/ dynamics:
Lives with mother. Parents divorced. Alternate weekends and holidays with father. FHxpaternal anxiety. Stable finances.
School/social:
Patient high achieving student attending local Governor’s School (STEM magnet school beginning sophomore year) and athlete (field hockey & soccer). Stopped playing sports in middle school due to conflict with peer groups, but returned to play after starting Rx above. Denies SU, sexual maltreatment. No significant other.

FOLLOW UP Case report 2/20
Is now on Lexapro 20 mg
PHQ-9 is 9. Self report of anxiety is still 20-24.
Asked to see counselor – has had one session
Has had friends over.
Sleeping better

Separation anxiety
➢Excess fear of separation from those strongly attached
➢Prevalence : 3-5% ; more in childhood than teen years
➢Etiology – parental psychopathology, attachment, fear dysregulation, behavioral inhibition trait, environmental precipitants ( divorce, moving)
➢Normal phenomenon between 6 – 30month, stabilizes with age and most recover
➢Treatment – CBT, school accommodations, predictable calm routine, support for family and SSRI
Dulcan 2018

Selective mutism➢ Mutism in 1 or more settings despite having the ability to comprehend spoken language and
speak in other settings ( ATLEAST 1 month)
➢ 0.3 – 1%
➢ Common among immigrant families, social anxiety disorder , heritable (70%)
➢ Evaluation includes psychiatric evaluation, speech and language eval., medical or
neurological assessment for delays
➢ Treatment : Self limiting, therapy including family therapy to reinforce efforts to speak, SSRI
Dulcan 2018

Social anxiety and phobias
➢Fear out of proportion to actual danger present for 6months
➢Normal fears and phobia differentiated by persistence, irrationality, and functional impairment
➢5 – 15%
➢Course : self – limiting, predict other disorders ( mood, eating, pain) , persist into adulthood
➢Treatment – exposure response prevention, CBT, SSRI

Generalized anxiety ➢UNCONTROLLABLE pervasive WORRY for atleast 6 mo with one accompanying symptom – restlessness, fatigue, inattention, irritable mood, muscle tension, sleep disturbance.
➢1- 3% ; more females
➢Behavioral inhibition, environmental ( parental control, adverse events, modeling), inheritable
➢Chronic, waxing and waning course with overlapping somatic symptoms, depression, other anxiety disorders
➢TREATMENT : CBT and SSRI (FDA approved Sertraline, Fluoxetine, Duloxetine)

Panic disorder➢a sudden unexpected and spontaneous onset of fear or discomfort, typically reaching a peak within 10 minutes/ association with physical symptoms followed by fear of the panic attack
➢1 – 4 % in children and teens
➢Agoraphobia less common than adults
➢Heritable and somatic sensitivity increased ( interoception)
➢Chronic course
➢Comorbid – anxiety and mood disorders, ADHD,
➢TREATMENT: CBT and if persistent then SSRI

School Avoidance Poor attendance to school
2- 5 %
Associated with physical symptoms that tend to prompt leaving school early or not going
Progresses into defiance, aggression, separation anxiety and avoidance
TRIGGERS - bullying, new school, lack of perceived or actual support at school, stressful life events
Behavioral is primary – getting back to school with support, home not rewarding and may be consider SSRI

Post-Session EvaluationAs a result of attending the session, to what extent did your Confidence in the learning objectives change?
Anxiety disorders Much more confident
Somewhat more confident
Confidence unchanged
Less confident
Define and discuss Prevalence
Define and discussCourse, types and progression
Define and discussScreeners
Define and discuss Behavioral approaches
Define and discussMedications