Embed Size (px)
DESCRIPTION
This is a PowerPoint presentation on Anxiety Disorders.
Citation preview

1
ANXIETY DISORDERS IN CHILDREN & ADULTS
THEORY
DIAGNOSIS
TREATMENT

2
Pharmacological response to medications designed to treat anxiety disorders is NOT evidence or proof of
ETIOLOGY.

3
FEAR VERSUS ANXIETY
• FEAR
• OBJECTIVE
• PAST EXPERIENCE WITH STRESSOR
• KNOWN PROBALITY OF HARM
• ANXIETY
• SUBJECTIVE
• FUTURE ORIENTED
• UNKNOWN HOW ONE WILL BE HARMED

4
NORMAL VERSUS ABNORMAL ANXIETY
• LEVEL OF ANXIETY
SOME LEVEL OF ANXIETY NECESSARY TO CREATE MOTIVATION
HIGH LEVELS OF ANXIETY RESULT IN INTERFERENCE WITH PERFORMANCE
HIGH LEVELS OF ANXIETY RESULT IN HIGH LEVEL OF COGNITIVE & PHYSIOLOGICAL AROUSAL

5
NORMAL VERSUS ABNORMAL ANXIETY
• JUSTIFICATION
ANY LEVEL OF ANXIETY WOULD BE CONSIDERED ABNORMAL IF NO RATIONAL JUSTIFICATION EXISTS FOR THE SITUATION TO TRIGGER ANXIETY.
PERCEPTION OF THE EVENT AS THREATENING TO THE INDIVIDUAL’S SAFETY IS KEY.

6
NORMAL VERSUS ABNORMAL ANXIETY
• INTERFERENCE IN FUNCTIONING
ANXIETY IS ABNORMAL IF IT CAUSES ANY
IMPAIRMENT IN FUNCTIONING IN ANY LIFE AREA:
(1) SOCIAL
(2) OCCUPATIONAL
(3) PHYSICAL
(4) RECREATIONAL

7
PREVALENCE & INCIDENCEOF ANXIETY DISORDERS
• MOST COMMON MENTAL DISORDER IN UNITED STATES.
• 15%-TO-17% OF ADULT POPULATION SUFFER FROM 1 OR MORE ANXIETY DISORDERS.
23 MILLION HAVE ONE FORM OF THE 6 ANXIETY DISORDERS
• 5% -TO-10% OF SCHOOL AGE CHILDREN HAVE AN ANXIETY RELATED DISORDER.

8
PREVALENCE & INCIDENCEOF ANXIETY DISORDERS
• 26% SUFFER FROM 2 OR MORE INDEPENDENT ANXIETY DISORDERS.
• 19% SUFFER FROM ONLY 1 ANXIETY DISORDER.
• 55% SUFFERED FROM MULTIPLE DISORDERS, ONE OF WHICH HELPED CAUSE THE OTHERS.

9
ANXIETY DISORDERS
• Generalized Anxiety Disorder
• Panic Disorder
• Obsessive-Compulsive Disorder
• Post-Traumatic Stress Disorder
• Specific Phobia
• Social Phobia
• Agoraphobia w/o Panic Attacks
• Agoraphobia with Panic Attacks

10
ANXIETY DISORDERS
• Anxiety Disorder Due to a General Medical Condition
• Substance Induced Anxiety Disorder
• Anxiety Disorder NOS
• Mixed Anxiety-Depressive Disorder

11
GENERALIZED ANXIETY DISORDER
THEORY
DIAGNOSIS
TREATMENT

12
Epidemiology of Generalized Anxiety Disorder
• One-year prevalence rate is approximately 3% of adults.
• Life-time prevalence rate approximately 5%.
• 25% of GAD patients present with comorbid condition:
Depression Panic Disorder Substance abuse Hypochondriasis Personality Disorder

13
Epidemiology of Generalized Anxiety Disorder
• Half of pts presenting for treatment report onset in childhood or adolescence.
• In children, Over-anxious Disorder of Childhood
• Gender ratio is approximately 2-to-1 females
• Course of disorder is CHRONIC but fluctuates & often WORSENS during periods of stress.
• familial association

14
PSYCHOANALYTIC EXPLANATION OF GAD & PANIC DISORDERS
• INTERNAL CONFLICTS ARE SOURCE OF BOTH DISORDERS
• UNCONSCIOUS IMPULSES THREATEN EXPRESSION
• ANXIETY IS ALARM THAT DEFENSES ARE ABOUT TO BREAK DOWN.
• SINCE NO FOCUS FOR DEFENSE, ANXIETY SYMPTOMS ARE RESULT OF UNSUCCESSFUL DEFENSE AGAINST ANXIETY PROVOKING IMPULSES.

15
COGNITIVE THEORY OF GENERALIZED ANXIETY DISORDER
Beck (1991) - People with GAD constantly make unrealistic assumptions that they are in imminent danger:
a. ANY STRANGE SITUATION SHOULD BE REGARDED AS DANGEROUS.
b. A SITUATION OR PERSON IS UNSAFE UNTIL PROVEN SAFE.
c. IT IS ALWAYS BEST TO ASSUME THE WORST.
d. MY SECURITY & SAFETY DEPEND ON ANTICIPATING & PREPARING MYSELF AT ALL TIMES FOR ANY POSSIBLE DANGER.

16
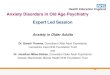
GABA & ANXIETY DISORDERS
• Research points to a problem in feedback system can cause fear or anxiety to go unchecked (Lloyd, 1992).
• GABA is released to exert inhibitory action on excitatory activity of neurons.
• A second site on GABAA receptor binds with benzodiazepines.
• People with GAD may have ongoing problems with anxiety feedback system.

17
GABA A Receptor with Binding Sites

18
GABA & GENERALIZED ANXIETY DISORDER

19
GABA & ANXIETY DISORDERS
• Brain supplies of GABA too low.
• May have too few GABAA receptors.
• GABA A receptors do not readily bind neurotransmitter.
• Brain may be releasing an excess of other
chemicals reducing GABA activity at receptor sites.

20
ASSESSMENT OF GAD
SCREENING TOOLS
Anxiety Screening Questionnaire (15 items)
Primary Care Evaluation of Mental Disorders
(PRIME-MD)
Hamilton Anxiety & Depression Scale
Beck Anxiety Scale
Center for Epidemiological Studies Depression Scale
(CESD)
Hospital Anxiety & Depression Scale

21
ASSESSMENT OF GAD
INTERVIEWING QUESTIONS:
“During the past 4 weeks, have you been bothered by feeling worried, tense, or anxious MOST of the time?”
“Are you frequently tense, irritable, and have trouble sleeping?”
If either answered YES, further investigation is warranted.

22
TREATMENT OF GAD IN PRIMARY CARE
Treatment options – Most efficaciously treated by combination of CBT & Pharmacotherapy
Cognitive-Behavior Therapy
Reframing
Cognitive Restructuring
Identifying Anxiety Triggers
Cognitive Rehearsal
Stress-Inoculation

23
TREATMENT OF GAD IN PRIMARY CARE
Pharmacotherapy
SSRI• Paroxetine (Paxil) only FDA for GAD• Fluoxetine (Prozac)• Sertraline (Zoloft)• Citalopram (Celexa)• Fluvoxamine (Luvox)
• See Table 11.4 in Kaplan & Saddock for dosing.

24
TREATMENT OF GAD IN PRIMARY CARE
Pharmacotherapy – SSRI
• Advantages of SSRI
• Few side effects• Not addictive/dependence liability• Treats co-morbid depression• Once daily dosing• Low sedation effect

25
TREATMENT OF GAD IN PRIMARY CARE
Pharmacotherapy – SSRI
• Disadvantages of SSRI
• Patient does not experience symptom attentuation with single dose
• Several weeks to full therapeutic effects
• Gastrointestinal and Sexual side-effects common

26
TREATMENT OF GAD IN PRIMARY CARE
SNRI Venaflaxine Hydrochloride (Effexor XR)
• Approved by FDA
• Reduces symptoms of: anxious mood excessive motor tension restlessness insomnia irritablility poor concentration

27
TREATMENT OF GAD IN PRIMARY CARE
SNRI Venaflaxine Hydrochloride (Effexor XR)
• Common side effects: asthenia somnolence nausea tremor constipation abnormal ejaculation/orgasm
• Patient does not experience symptom attentuation with single dose
• Several weeks to full therapeutic effects.

28
TREATMENT OF GAD IN PRIMARY CARE
Nonbenzodiazepine agent – Buspirone (Buspar)
• It is a 5-HT1A 1A receptor partial agonist.
• More effective in reducing cognitive symptoms than somatic symptoms of GAD.
• Less addictive potential associated with its use.
• Indicated if patient has co-morbid substance use disorder.

29
TREATMENT OF GAD IN PRIMARY CARE
Nonbenzodiazepine agent – Buspirone (Buspar)
• Patients who had used benzodiazepines are not likely to respond to Buspirone.
• Lack or absence of anxiolytic effects (muscle relaxation & sense of well being) may be contributing factor.
• Effects take 2-to-3 weeks to become evident.

30
Treatment of GAD
• BENZODIAZEPINES ALPRAZOLAM XANAX
CHLORDIAZEPOXIDE LIBRIUM
CLONAZEPAM KLONOPIN
CLORAZAPATE TRANZENE
DIAZEPAM VALIUM
LORAZEPAM ATIVAN
OXAZEPAM SERAX
PRAZEPAM CENTREX

31
TREATMENT OF GAD IN PRIMARY CARE
Pharmacotherapy – Benzodiazepines
• Advantages
• Therapeutic effect in single dose
• Time to full therapeutic effect in days.
• Anxiolytic effect of medications helps reduce somatic symptoms of GAD

32
TREATMENT OF GAD IN PRIMARY CARE
Pharmacotherapy – Benzodiazepines
• Disddvantages
• Impaired alertness & motor performance• High addictive or dependence liability• Does not treat co-morbid depression• Requires several doses per day• High sedation effect• Memory impairment

33
TREATMENT OF GAD IN PRIMARY CARE
Pharmacotherapy – Benzodiazepines
• Most common clinical mistake is to routinely continue treatment INDEFINITELY.
• Treatment may be minimum of 6 months-to-1 year so consideration of other medications who seem warranted.
• Start treatment with benzodiazepine & buspirone & taper off benzodiazepine when buspirone reaches maximum effect ( 2-to-3 weeks).

34
PANIC DISORDER
THEORY
DIAGNOSIS
TREATMENT

35
Epidemiology of Panic Disorder
• One-year prevalence rate is approximately 1.5% of adults.
• Life-time prevalence rate approximately 3.5%.
• Panic Disorder patients present with comorbid condition:
Major Depression GAD
Substance abuse OCD
Specific Phobia Agoraphobia
Social Phobia PTSD

36
Epidemiology of Generalized Anxiety Disorder
• Typically onset between adolescence & mid-30’s.
• Females 3X more likely to have PD with agoraphobia• Males 2X more likely to have PD W/O agoraphobia
• Course of disorder is CHRONIC but waxing & waning.
• 1st degree biological relatives are 8 times more likely to develop panic disorder.
• If onset before age 20, 20 times more likely

37
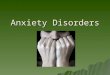
NOREPINEPHERINE & PANIC DISORDERS
• Research has focused upon abnormal norepinepherine activity in locus coeruleus.
• Function of locus coeruleus is to send messages to amygdala (limbic system) that is known to trigger emotional reactions.
• Studies have indicated that locus coerulus is involved in activating certain behaviors such as increased vigilance.

38
NOREPINEPHERINE & PANIC DISORDERS
• Over-activity in nordrenergic system has been linked to panic disorder.
• Stimulation of locus coerulus in both animal & human studies trigger panic symptoms.
• Noradrenergic over-activity may be result of fewer GABAA receptor sites and lower GABA levels in occipital cortex of panic disorder patients. (Malizia, 1998; Goddard, 2001)

39
NOREPINEPHERINE & PANIC DISORDERS
• Anti-depressant drugs act to restore appropriate norepinepherine activity in locus coerulus & helps to reduce symptoms of disorder.
• 80% will experience some significant improvement.
• 40% reach full recovery or improve markedly; 20% show NO improvement.

40
LOCUS COERULUS & PANIC DISORDER

41
ASSESSMENT OF PANIC DISORDER
SCREENING TOOLS
Anxiety Screening Questionnaire (15 items)
Primary Care Evaluation of Mental Disorders
(PRIME-MD)
Hamilton Anxiety & Depression Scale
Beck Anxiety Scale
Center for Epidemiological Studies Depression Scale
(CESD)
Hospital Anxiety & Depression Scale
Panic Disorder Self-Test (www.adaa.org)

42
TREATMENT OF GAD IN PRIMARY CARE
Cognitive Behavior Therapy
Stress-inoculation
Reframing
Cognitive Restructuring
Relaxation Training
Progressive Relaxation
Deep breathing
Positive Imagery

43
TREATMENT OF GAD IN PRIMARY CARE
Pharmacotherapy
SSRI• Paroxetine (Paxil) only FDA for GAD• Fluoxetine (Prozac)• Sertraline (Zoloft)• Citalopram (Celexa)• Fluvoxamine (Luvox)
• See Table 11.4 in Kaplan & Saddock for dosing.

44
Pharmacotherapy of Panic Disorder
SSRI
Paroxetine (Paxil)
Fluvoxamine (Luvox)
Sertraline (Zoloft)
DOSE
5-10 mg start
20-60 mg maintenance
12.5 mg start
50-125 mg maintenance
12.5 – 25 mg start
100-150 mg maintenance

45
Pharmacotherapy of Panic Disorder
TCA
Clomipramine (Anafrinil)
Imipramine (Tofranil)
DOSE
5-12.5 mg start
50-125 mg maintenance
10-12.5 mg start
150-500 mg maintenance

46
Pharmacotherapy of Panic Disorder
Benzodiazepines
Alprazolam (Xanax)
Clonazepine (Klonopin)
Lorazepam (Ativan)
DOSE
.25-.5 mg tid start
.5-2 mg tid maintenance
.25 -.5 mg bid start
.5-2 mg bid maintenance
25 -.5 mg bid start
.5-2 mg bid maintenance

47
OBESSIVE-COMPULSIVE DISORDER
THEORY
DIAGNOSIS
TREATMENT

48
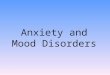
OBSESSIONS
• INTRUSIVE THOUGHTS WISHES THAT CANNOT BE IGNORED, DISMISSED OR RESISTED.
• COMMON THEMES:
CONTAMINATION ORDERLINESS
VIOLENCE SEXUALITY

49
COMPULSIONS COMMON FORMS
These behaviors or mental acts either are not connected in a realistic way with what they are designed to neutralize or prevent or are clearly excessive:
cleaning hand washing
ordering checking
touching counting
repeating words silently praying

50
COMMOM OBSESSIONS & COMPULSIONS

51

52
ASSESSMENT OF OCD
SCREENING TOOLS Yale-Brown Obsessive Compulsive Scale (YBOCS) Anxiety Screening Questionnaire (15 items) Primary Care Evaluation of Mental Disorders (PRIME-MD) Hamilton Anxiety & Depression Scale Beck Anxiety Scale Center for Epidemiological Studies Depression Scale (CESD) Hospital Anxiety & Depression Scale

53
PSYCHOANALYTIC VIEW OF OBSESSIVE-COMPULSIVE DISORDER
OCD develops when child comes to fear his own ID impulses & uses EDMs as counter-thoughts or compulsive actions to lessen resulting anxiety.
Three ego-defenses are common in OCD:
isolation- isolates & disowns undesirable/unwanted thoughts & experiences them as intrusions
undoing - Individual engages in acts that implicitly cancel out their undesirable impulses.
reaction formation - Takes on lifestyle that directly opposes their unacceptable impulses.

54
SEROTONIN & OBSESSIVE-CONPULSIVE DISORDER
• Serotonin plays role in operation of orbital region & caudate nuclei.
• Low levels of serotonin disrupts functioning. • Research has found:Reducing serotonin activity results in an
increase of OCD symptoms.Low levels of serotonin are related to high levels
of OCD symptoms.Increasing serotonin levels reduces symptoms.

55

56

57

58
PHOBIC DISORDERS:SPECIFIC PHOBIASOCIAL PHOBIAAGORAPHOBIA
THEORY
DIAGNOSIS
TREATMENT

59
SPECIFIC PHOBIASPECIFIC PHOBIA
A. Marked & persistent fear that is excessive or unreasonable, cued by presence or anticipation of a specific object or situation.
B. Exposure to phobic stimulus almost invariably provokes an immediate anxiety response
C. Person recognizes that the fear is excessive or unreasonable.

60
SPECIFIC PHOBIASPECIFIC PHOBIA
.
Animal Type
Natural Environment Type (heights, storms, water)
Blood Injection Injury type
Situational Type (airplanes, elevators, enclosed places)

61
AGE OF ONSET OF PHOBIA

62
PSYCHOANALYTIC MODEL OF PHOBIC PSYCHOANALYTIC MODEL OF PHOBIC REACTIONSREACTIONS
• PHOBIAS ARE EXPRESSIONS WISHES/ FEARS WHICH ARE UNACCEPTABLE TO EGO
• UNCONSCIOUS CONFLICT IS DISPLACED TO EXTERNAL OBJECT OR SITUATION
• PHOBIA IS LESS THREATENING TO PERSON THAN THE RECOGNITION OF THE UNCONSCIOUS IMPULSE

63
PSYCHOANALYTIC MODEL OF PHOBIC PSYCHOANALYTIC MODEL OF PHOBIC REACTIONSREACTIONS
PHOBIA IS ONLY A SYMPTOM OF UNDERLYING CONFLICT.
LEVEL OF PHOBIC FEAR INDICATES STRENGTH OF CONFLICT.
ONCE UNDERLYING CONFLICT IS DISPLACED ONTO EXTERNAL SITUATION, CONFLICT CAN BE CONTROLLED SIMPLY THROUGH AVOIDANCE.

64
SOCIAL PHOBIASOCIAL PHOBIA
LIFE TIME PREVALENCE 11% MALES
15% FEMALESONSET IN ADOLESCENCE
COMMON IN FAMILIES WHO :
USE SHAME AS CONTROL TECHNIQUE
STRESS IMPORTANCE OF OPINIONS OF OTHERS

65
SOCIAL PHOBIASOCIAL PHOBIA
CAN BE DIVIDED INTO 3 TYPES:
PERFORMANCE
LIMITED INTERACTIONAL
GENERALIZED

66
SOCIAL PHOBIASOCIAL PHOBIA
PERFORMANCE
EXCESSIVE ANXIETY OVER ACTIVITIES
PLAYING INSTRUMENT
SPEAKING IN PUBLIC
EATING IN RESTAURANT
USING PUBLIC RESTROOM

67
LIMITED INTERACTIONAL
EXCESSIVE FEAR ONLY IN SPECIFIC SOCIAL or VOCATIONAL SITUATIONS
ex. INTERACTING WITH AUTHORITY FIGURE
GOING OUT ON A DATE
SOCIAL PHOBIA

68
SOCIAL PHOBIA
GENERALIZED
EXTREME ANXIETY DISPLAYED IN MOST SOCIAL SITUATIONS
MAY RESULT IN AVOIDANCE OF ALL SOCIAL INTERACTION

69
AGORAPHOBIAAGORAPHOBIA
Anxiety about being in places or situations from which:
escape might be difficult (or embarrassing) OR help may not be available in the event of having an
unexpected or situationally predisposed Panic Attack or panic like symptoms.

70
AGORAPHOBIAAGORAPHOBIA
Agoraphobic fears typically involve characteristic clusters of situations that include:
being outside home alone
being in a crowd or standing in line
being on bridge
traveling in bus, train, or automobile.

71
AGORAPHOBIAAGORAPHOBIA
• LIFE TIME PREVALENCE 5% OF MALES & 12% OF FEMALES.
• DEVELOPS IN 50% OF PANIC DISORDERS
• FAMILY & TWIN STUDIES INDICATE 3-TO-5 TIMES GREATER RISK FOR PANIC DISORDER/ AGORAPHOBIA THAN IN GENERAL POPULATION

72
• AFFECTS 1/2 OF VICTIMS BY AGE 8
• SOME MAY HAVE BEEN BORN WITH TENDENCY TOWARDS EXTREME SHYNESS
• 1-IN-5 DEMONSTRATED CONSISTENT FEAR & DISTRESS IN NOVEL SITUATIONS AS EARLY AS 8 WEEKS OF AGE.
• DISORDER THOUGHT TO OCCUR MORE OFTEN IN FEMALES BUT MALES
POST-TRAUMATIC STRESS DISORDER IN CHILDREN

73
POST-TRAUMATIC STRESS DISORDERPOST-TRAUMATIC STRESS DISORDER
• MUST EXPERIENCE TRAUMATIC EVENT
• INTRUSIVE RE-EXPERIENCING OF EVENT
(DREAMS, FLASHBACKS, IMAGES, THOUHGTS, RECOLLECTIONS)
• AVOIDANCE OF STIMULI ASSOCIATED WITH EVENT

74
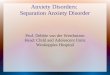
PERCENTAGE OF INDIVIDUALS DX WITH PTSD

75
POST-TRAUMATIC STRESS DISORDERPOST-TRAUMATIC STRESS DISORDER
• NUMBING OF RESPONSIVENESS TO THE WORLD & RESTRICTION OF AFFECT
• SYMPTOMS OF INCREASED AROUSAL
EXAGGERATED STARTLE REACTION
HYPERVIGILANCE
DIFFICULTY CONCENTRATING
INSOMINIA
NIGHTMARES

76
POST-TRAUMATIC STRESS DISORDERPOST-TRAUMATIC STRESS DISORDER
• PTSD can occur at any age even childhood.
• In young people, the response may be expressed as agitated behavior.
• Most young people with PTSD avoid things that remind them of what happened.
• Many have physical symptoms as well, such as startling easily.

77
PTSD IN CHILDRENPTSD IN CHILDRENETIOLOGICAL FACTORSETIOLOGICAL FACTORS
• Certain PREMORBID personality profiles & attitudes are more likely to develop PTSD.
• Pre-morbid personality or psychological difficulties are associated with increase risk & more severe ASD & PTSD symptoms:
poor interpersonal relationships external locus of control pessimism

78
ETIOLOGICAL FACTORS
• NATURE & QUALITY OF SOCIAL SUPPORT SYSTEM
• Person with a strong social support system after a traumatic event less likely to develop an extended disorder.
• If feels loved/accepted/valued, will be more likely to recover.
• Societal support for appears to be important in lessening severity & duration of symptoms.

79
ETIOLOGICAL FACTORS ETIOLOGICAL FACTORS
• DEGREE OF EXPOSURE & SUBJECTIVE EXPERIENCE OF THREAT PLAYS CRITICAL ROLE IN DEVELOPMENT OF PTSD & ASD.
• DURATION OF THE EXPOSURE
• LEVEL OF INVOLVEMENT
• SALIENCE
• DEGREE OF HARM EXPERIENCED

80
MIXED ANXIETY & DEPRESSIONMIXED ANXIETY & DEPRESSION
• SHARED SYMPTOMS
• EXCESSIVE WORRY
• MOTOR TENSION
• EASY FATIGABILITY
• DIFFICULTY CONCENTRATING
• SOMATIC COMPLAINTS

81
MIXED ANXIETY & DEPRESSION
• ANXIETY
• SHORTNESS OF BREATH
• CHEST PAIN• NERVOUSNESS• IRRITABILITY• BURNING STOMACH• DIFFICULTY FALLING
ASLEEP
• DEPRESSION
• DEPRESSED MOOD• ANHEDONIA• WEIGHT LOSS OR
GAIN• SUICIDAL
THOUGHTS• EARLY MORNING
AWAKENING

82
MEDICATIONS THAT REDUCE ANXIETYMEDICATIONS THAT REDUCE ANXIETY
• AZASPIRONES
BUSPRIONE BUSPAR
• BETA BLOCKERS
PROPANOLOL INDERAL
ATENOLOL TENORMIN

83
ANXIETY DISORDERS IN PRIMARY CARE: ANXIETY DISORDERS IN PRIMARY CARE: GUIDELINESGUIDELINES
• RECOGNIZE ANXIETY AS CAUSE OF PT’s PRESENTING SYMPTOMS:
LOOK FOR MULTIPLE SYMPTOMS
GREATER # OF PHYSICAL SYMPTOMS, MORE LIKELY ANXIETY D/O PRESENT
GREATER # OF SOMATOFORM SYMPTOMS, MORE LIKELY ANXIETY D/O PRESENT

84
ANXIETY DISORDERS IN PRIMARY CARE: GUIDELINESANXIETY DISORDERS IN PRIMARY CARE: GUIDELINES
RECOGNIZE ONLY A SMALL NUMBER OF PT’S WITH ANXIETY SYMPTOMS ARE A RESULT OF GENERAL MEDICAL CONDITION.
LOOK FOR ANXIETY IN OTHER LIFE AREAS
LOOK FOR TRIGGERS OR AVOIDANCE (TIME/PLACE/SETTING/CONTEXT)
LOOK FOR MULTIPLE SYMPTOMS
LOOK FOR SOMATOFORM SYMPTOMS
EPIDEMIOLOGY = APPEARS IN YOUNGER PT--> LESS RISK FOR ILLNESS

85
ANXIETY DISORDERS IN PRIMARY CARE: ANXIETY DISORDERS IN PRIMARY CARE: GUIDELINESGUIDELINES
• A SIGNIFICANT # OF PT’S WITH ANXIETY SYMPTOMS HAVE CO-MORBID PSYCHIATRIC DISORDERS.
• 26% SUFFER FROM 2 OR MORE INDEPENDENT ANXIETY DISORDERS. 55% SUFFERED FROM MULTIPLE DISORDERS, ONE OF WHICH HELPED CAUSE THE OTHERS.
• MAJOR DEPRESSION
• SUBSTANCE DEPENDENCE/ ABUSE