Embed Size (px)
Citation preview

Indian .l ou rn ~iI of Exper illlental B iology Vol. 41. 'ovclllber 2003, pp. 1226- 1232
Review Article
Antituberculosis drug-induced hepatiti s: Risk factors , prevention and management
Z HlI ssa in l .~, P Kar l & S A HlIsain2.*
'Departillent of M edici ne, Maulana Azad Medical College. New Delhi 11 0002, India
2Dcparllllent of Biosc ience, l alllia Millia Islaillia. New Delhi 11 0025, India
A part frolll in fec ti ous or v iral hepatiti s. other IllO, t comillon non-infecti ous causes of hepa titi s arc alcohol, cho leslat ie. drugs and tox ic malcrials. The mos t common Illode lhal leads lo li ver injuri es is an l i luherculosis drug- induced h pa ti li s. The severity of drug- induced li ve r injury va ries frolll l1Iinor nonspec ifi c changes in hepalic Sl ruClllre lO fulminanl hepal ie fa ilure, cirrhos is and li ver cancer. Pali enlS receiving anlilubercul ar drug frequen ll y deve lop acule or chronic hepalil i<;. The li llle requin;d ror the mctaholil es to reach hepa lolOx ic level s is much ea rl ier w ilh isoni az id plus rifampicin lrea lmenl th an i so ni ~lI. id alonc and lhi s has been shown lO he sy nergistic ralher lhan addilive. An liluberculosis drug (Arr')- indueible cY lochromc P-4502E I (CYP2E I ) is constitut ive ly expressed in the li ve r. Recent studi es show lhat polYlllorphism of the Nacetyl transkrasc 2 (NAT2) genes and glutathione-S-t ran srCl'a se (GST ) arc the Illajor suscept ibility ri sk factors for ATTinduced hepatiti s. Thc hepa tic NAT and GST arc in vo lwd in the melabo li sl1l o f several carci nogenic ary laill ines and drugs. The NAT2 enzy llle has a gc ncti c polymorphi sm in hUlllan . - accty l tra nsferase 2 genes ( AT2) have been ident i ri ed to be responsihle for genetic pol ymorphi slll or slow and I'ap id accty lation in humans. Slow accty lators of NAT2 pro ve to dcvelop Illore scvere hepatolox icity than rapid acety lators making it a signi ficant r isk factor. Deficiency of GST ac ti vilY. hecau se of homozygous nul l mutat ions at GSTM I and GSTT I loc i, Illay modulate susceptibi l i ty to drug and xenobiotic -lndueed hepatotox icit y. PolYlllorphi sms at GSTM I . GS'IT I ;1I1d AT2 loci had been linked to va ri ous rorms of li ve r injury. includ ing hepatocellular carci noma.
Keywurds : Antituberculos is drug. Drug-induced hepati t is, Hcpatic drug metabol ism, Idiosyncrat ic hepalOtoxim .. Isoniazid. Rifampicin. Vi ral hepatiti s
V iral hepatiti s is a systemic in fecti on affec ting primari ly the li ver t. A t leas t 8 different types of viruses direc tl y assoc iated w ith vi ral hepa titi s have been identified. The causes of hepatiti s can be broadl y class ified into infecti ous and non-infectious2
. The infec t ious causes inc I ude bacteri a and more cOlllmonl y vi ruses.The non-i n fectious causes are alcohol (alcoholi c hepatiti s), cholcs tati c, drugs and tox ic material s3A
Apart from in l'cctious or v iral hepatiti s,oth er most common non- i n fcctious causes th at lead to I i ve l' inj uri es are antituberculos is drug-induced hepatiti sl.2 Tubercu losis continues to be a major health prob lem in both deve loping and developed cou ntri es because of its resurgence in immunosuppressed pati ents"' Epidem iolog ica l data suggest that antituberculos is drug- induced hepatiti s is due to its metabolic id iosyncrasy rat her th an direct tox icit/ . Some host
*Correspondcnt aut hor: [ -m;l i l: ak htarhusain2000 @yah(lo.eoIrl akh ll·_b i@jllli .erncl.i n Phone : 9 1-0 11-26<)8 16 11 (R) F;lx: 9 1-0 11 -26830337
factors that increase the hepatotoxici ty o f ATT are o ld age), pregnanc/ , mal nutriti onS, and concurrent administrati on of other drugs such as rifamp i c in ~, alco h o l ~, etc. T he great suscepti bi I ity o f l iver damage to chemica l agen ts (such as A dru gs) is a consequence of its primary role in the metaboli sm of fo reign subst a nces~.5. Liver injury is present when abnormaliti es of li ver tes ts inc lude an increase to more th an tw ice the upper limit or se rum alan ine amino-transferase (A LT)()·7, serum alka linephosphatase (ALP/·7 or biliru bin6
.7 .The severit y or
drug-induced li ver Injury van es from III 111 0 1'
nonspec ifi c changes in hepati c structu re to fulminant hepati c fai lure, ci rrhos is and I i vel' cancers .The term drug- induced li ver disease shou ld be confined to cases in which the nature of li ver injury has been confirmed hi stolog ica ll /. Short course chemotherapy con taining isoniazid and ri fampicin in comb i nati on has proved to be highly effec ti ve in the treatment of tuberculos is, but one of its adverse effec ts is hepatoloxicit / ·13
.
Several reports suggest that hepatiti s is more Frequen t and severe with chemotherapeuti c regimens con taining both isoniaz id and rifampicin th an those

HUSSAIN et at.: ANTITUBERCULOSIS DRUG-IND UCED HEPATITIS 1227
isoniazid alone with other antitubercular drugs6-IO. Lesobre el ai . II also described 12 cases (24%) of jaundice with 4 deaths among 50 patients receiving isoniazid and rifampicin , although many of these patients had pre-ex isting liver di sease with high doses of isoni az id and rifampicin.
Lees et al.14 observed 4 cases (8%) of hepatiti s among 50 patients without known liver di sease. The hepatotoxicity of isoniazid plus rifampicin is
.. h h dd" 7 12 13 Th ' . d h synergistic rat er t an a It I ve ' ' . IS IS ue to t e remarkably potent inducing effect of rifampicin on the hepatic P-4S0 mixed ox idase enzyme pathways leading to the increased formation of tox ic intermediate from monoacetylhydrazine I5-19. The time required for the toxic metabolites (hepatotoxicity) to reach is much earlier on isoniazid plus rifampicin treatment than isoniazid alone2o. In addition, rifampicin can induce isoni azid hydrol ase resulting in an increase in the formation of hydrazine from isoni az id through the direct pathway, with consequent manifestati on of hepatic injur/ I-27
. Today , we are speaking much more of an " INH hepatotoxicity" which is aggravated by the mi crosomal enzy meinducing effect of rifampicin6.23.25.2R3o. Many questions in the pathogenesis of liver cell necros is caused by noxae still remain open, it seems to be certain that the damage to the membrane is the dec isive incident triggering the pat!iology . The preparati on of Essentiale Forte besides vitamins mainly contains "essential " phospholipids can positively influence thi s damage, because phospholipids are an integral component of the cellular membrane systems and sub-cellular particles25 . Their importance in the liver therapy becomes obvious by their role'as structural elements, mediators between the intracellul ar and intercellular space, activators of different enzy me systems and III . I' I 1'; Immuno oglca processes-· .
Hepatic drug metabolism and toxic mechanisms of liver injury
Biotransformation reactions in liver have traditionally been considered protective as detox ifers of potentially toxic foreign compounds8
. Such reactions can also convert nontoxic agents to potentially toxic products3A.5. Jt has become clear that the formation of reactive, and therefore toxic, metabolic intermediates within the hepatocyte accounts for injury that the liver sustains from many of the known toxic chemicals and drugs4
.6
. Most drugs and other xenobiotics that react with body tissues are
nonpolar, lipid-soluble compounds, since absorpti on from the intestine requires lipid solubilitl ·9 .
Accordingly, biotransformation of lipid solubility to water so lubility is necessary to prevent intolerable accumulation of foreign and endogenous moleculesx.16. The enzyme systems responsible fo r the biotran sformation are integral parts of smooth endoplasmi c
. 8 16 f d b I' retlclilum ' . The pathway 0 rug meta 0 Ism divides into phases I and II. Phase J reactions are largely oxidative, yielding active transient metabolites. Their reactivity serve to permit to produce hepatic injurl·8
.9
. Phase 1 reactions may be regarded as tox ificati on reactions6
.8
.'J . The enzyme y tem responsible for phase 1 reaction is ca ll ed mixed function oxidase or monooxygenase4
. Cytochrome P-4S0 is a key enzyme of phase I metaboli sm, a haemoprotein located in SER4
•X
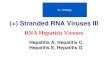
.'J. The haem-moiety binds O2 which is then reduced by accepting an electron from flavoprotein reductase, the resultan t activated O2 is incorporated into lipophili c substance·s I6. Such activation results in the form ation of chemically reactive intermedi ates such as N-acetylP-ben7.0quinoneimine (NA PQ I) as shown in Fig. I. It causes ce ll damage by per-ox idati ve damage of lipid moiety of biological membrane, form s direct covalent binding with protein or DNA I.I6. Co-valent binding of reacti ve metabolite with macromolecule may produce injury by inactivating key enzymes or forming protein drug adducts that are potenti al target f·· d' d " ~ 16 PI II . or Immune-me \ate IIlJury · . lase reactions may be regarded as detox ification react ions. Conjugation with glutathione (GSH) serves to detoxify an active intermediate as shown in Fig. 2.
Metabolism of isoniazid Isoniaz id is the major drug incriminated in anti
tuberculosis drug-induced hepatotoxicitiA.6-IO.lc. IJ. The frequency that causes 6-12% mortality if the drugs are continued after the onset of sy mptoms is typicall y between I and 36%3 1. Isoni azid (INH ) gets acetylated to acetyl isoniazid (AdNH) by N-acetyltransferase (NAT) enzy me which IS
h '() 16 A I' . 'd . non epatotoxlc · . cety IsonlHZI In turn gets hydrolyzed to monoacetylhydrazine (MAH ) and isonicotini c ac id (lNA)32 P-4S0-dependent hepatic microsomal enzy mes lJ .27-JO.33-37to a potent acylating agent that binds covalently to apparently vital hepatic
O2 Acetam inophen • CYP2El
Fig.1 - Formati on of chemicall y reaclive inlermedi ate, N-acely lP- benzoquillolleiminc (N APQ I)

1228 I DI AN J EXP 1310L, OVEMBER 2003
AIT-drug, like Isoniazid (fNH)
N- Acetyltransferase (NAT) & other CYPs ------------_~ Acetyl isoniazid (AclNH)
1 Hydrazine (Hepatotoxic)
Phase I (Toxification) 1 MonoacetYltrlferase (MAH)
Microsomal Enzyme CYP-4502 E I
_---;.-P.:..::ha=::se::..,;..:I1'--:---- Covalent binding Conj~gation 4 detoxification Toxic Metabolite_ Hepatic
• GSH in presence of GST Necros is
Removal of toxic metabolites
Fig . 2 - Digralllillalic repn:SC ll lal ioll or ill l~ rplay belwce ll drugs alld ellzYllles lhal causes aillilubercu los is drug- indllc~d hepatoloxicily
macromolecules and causes hepati c necros is can M H616 1J . I convert A ' " -. A lternatI ve y MAH can be
acety lated to diacety lhydrazine (non-hepatotox ic) as shown in Fig. 2. I A on the other hand is conjugated w ith glyc ine to form ison ico tin glyc ine ( INAG). It has been direc tl y hyd rolyzed by isoni az id hydrolase to I A and hydraz ine that is hepatotox ico.l(d2
Role (~l rifampicin
When rifampicin IS used in combination w ith isoniazid the inter va l bctween th e commencement o f therapy and onset o r hepatiti s is much shorter
l5. This
is due to the fac t thar rirampi cin is a known microsomal enzyme (P-450:?E I ) inducer35
-:1X
and increases th e concen trati on or tox ic mctabo lites or iSlln iazid. Ran el al. ~o reported that the average inlerval I'm the onse t or jaund ice was 15.5 days in patien ts treated w ith isoni azid and rirampi cin Cl)mbi nat iun. while it was 7 1 days in the pati ents treated w ith ison iazid and other companion drugs. In the study conducted by Lees el al. l.J it was round that jaundice occurred w ithin 7 weeks w ith a mode and 3 weeks in-pati ents rece i ving isoniazid and rirampi cin . Gupta el (11 ,-'.1 also reported simil ar results wi th nearl y all or their patient s (26 out o r 29) deve loping hepatiti s wi th in 2 weeks of sta rting therapy.
Rela/ionship of ace/yla/or sta/lis /0 hepatotoxicity of isouiazid and rifampicin combillatio/l
In the sllldy or isoniazid- induced hepatiti s observed that out o f 2 1 patients w ith probab le isoniazid li ver injury 18(86%) WilS rap id acety lator\ although the expectcd rreq uency was 4S IJ( .\.5 Hence, they
suggesteu th at isoniazid may be more hepatotox ic for rarid acety lator th an for slow acety lato rs. The rapid
acety lators might be ex pected to fo rm monoacety lhydrazine (M A H) from isoniaziu more rapidly than slow acety lator and MAH can be converted by hepatic
. I 2S?X-1lJ"J7 . m lcrosoma enzymes " - . .. to a potent hepatotox Ic
agent. Thi s hypothes is was qucsti oned on the ground that rapid acety lator acely lates M A H more rapidl y than do slow acety lators to the non-tox ic diacety lhydrazine DA H·w-45
. Therefore slow acety lators instead or rapid acety lator have been determined to cause antitube rculos is drug-i nduced hepatitis.J(,-.J, .
Ev idence abounds from clinical studies that the ri sk of hepat ic reacti ons during treatment wi th ison iazid w ith or w ithout rirampicin is no greater 1'0 1' rap id acety lator th an slow acety lator I1
. .JlJ-5, . A subsequent study has
shown that hepat iti s in pati ents rece i ving isonia/.id and rirall1picin occurred morc orten in slow than in rap id acety lators. The proporti ons among those whuse acety lator phenotype was determ ined were II Ik or ] 17 slow and I % o f 244 rapid acet y latol·s. Recent study shows that po ly morph ism or th N-acety ltransfe rase 2 ( AT2) genes are the maj or susceptibility ri sk ractors·
q N-acety ltransrerase ( AT) is one or the
major li ver enzy mes in volved in bio transformation of drugs and other exogenous substances·w . .Jo.H.J5 . .J6 . AT
cata lyzes the transfer of acety l group I'rom acety l coenzy me A to the primary am ino group of the acceptor molecule, which results in the format ion of
-acety l de ri va ti ves5~.55 The hepati c (NAT) I S
in vo lved in the metabol ism or sever,t1 ca rci no!!enic ary lamines and drugs55 Th is enzyme has a gC~l e ti c pol y morphism in human, N-acety ltransf'erase 2 genes (NAT2) have been located on chromosome 8p22.J,· 5 1 5657 . d . t" lb " . ... ,I entl ICC to e responSible fo r genet ic pol y morphi sm of slow and rapid acety iati on5S NAT2 is composed o f one intronless open reading f rame

I '1
HUSSAI el al .. · ANTITUBERCULOSIS DRUG-INDUCED HEPATITIS l 229
(ORF) of-870-bp fragments contallling the protein coding region of the gene59
. Polymorphi sms in NAT2 are also associated with higher incidence of cancer and drug tox i c it i9.52.5~. Classification of humans as rapid and slow acetylators is based on hereditary differences in rates of N-acetylation of therapeutic
d . . 57
an carcll10genlc agents .
Host factors: Genetic poLymorphism of humall cytochrome P-4502El
Antituberculos is drug (ATT)-induc ible cy tochrome P-4502E I (CY P2E I ) is constitutively expressed in the I· '7·1035·17 TI b ' f'" b d d Iver- . . ' . l e su strate speci IClty IS roa an includes at present at least 80 different characteri zed substrates.19 The enzy me is induced by a vari ety of chemicals , mainly substrates, and induction in these cases IS to a major ex tent med iated at the posttran slational level4x . It is ev ident that CYP2EL plays an important toxico log ica l role3').55 . It acti vates precarcinogens, and drugs to cy totox ic or carcinogenic products that might be harmful and of importance fo r the sy nergisti c effect of ATT on many
f I· d' "1941475557 Th ' .. types olver Iseases· · ·····. IS reactI on IS impli cated as being of imporrance in the eti ology of A TT-induced li ver di sease. Becau se of the imporrant tox ico log ica l role of CYP2E I , a lot o f research has been conducted aimed at elucidat ing a genetic polymorphism of the human CYP2E I gene and the linkage of vari ous allelic rorms to ditlerent types o f ATT-induced li ver di seases61J Restriction fragment length polymorphi sm (RFLP) analys is of the human CYP2E I gene revea led polymorphi sm detectable with I . . I I 6(J Th I I " t l e res trI cti on enc onuc ease. e po y morp llC Sit s
are all present in the non-coding reg ions or the genc('O The open reading frame (ORF) of the human CY P2E I gene has been found to be we ll conserved, and f . I ' 60 l ' . uncti ona mutations are very rare . wo major polymorph ic sites have been studied in relation to thi s disease. The first is located in the 5' -flanking reg ion at about 1020 bp upstream59 and in intron 66
0. T hi s allele has been seq uenced and r ou nd to carry mutations near the promoter and in the 3' -flanking region, but not in the open reading frame (ORF)(>I.
Host Jactors: Glutathione - S - trallsferase Drug hepatotox icity in general, is the outcome of
dynamic processes in vo l ving tox ic metabol ite generation and its detox ifi ca tion in the li ver 0. 10 .
Gl utathione (GSH) plays an important protecti ve ro le as an intrace llular free radi ca l scavenger by conjugatin g with tox ic reacti ve metabo lites th at are
generated from biotransformati on of drugs and xenobiotics62
. Su lphydryl (SH) conjugation of the metabolites facilitates their elimination from the body,
d d I . If ' . (;? 63 65 l 'h . an so re uces t l e potentIa or toxICity -. '. us, It pl ays an important role in preventing acetaminophen and ATT-induced hepatotoxi city. Glutathi one-Stransferase (GST ) cata lyze these conjugation reactions and they ex ist in several iso forms with varying ti ssuespec i fic express ion6J
. Defi ciency in GST act i vity, because of homozygous null mutations at GSTM I and GSTTI loc i, may modulate susceptibility to drug and xenobioti c-i nduced hepatotox iCit/ 5
. Some geneti c loc i of these isoenzymes, notably GSTM I and GSTT I are pol ymorphic6465 Polymorph isms at GSTM I , GSTTI and NAT2 loci had been linked to vari ous forms of li ver Injury, including hepatocellu lar carci noma65
.66
.
J ndi viduaL risk factors M any factors influence the ri sk of drug-induced
li ver di sease: dose6.66
, blood l eve l ~ ·6 , and duration of intake for dose dependent hepatotox i n s ~a nd occas ionall y some idi osyncrati c reactions. For these drugs, however, other host determinants are more . I ~ t I 8.26 X.26 t ' f' t 10.2(, I e evan, examp es: age , sex , gene IC ac ors . Most hepati c drug reactions are more common in adults than in children l8.19 Women are parti cularly pred isposed to drug- induced hepatiti sJ
".
Concomitant exposllre to other agents One drug can increase the hepatotox icity of another
drug when adm ini stered concurrently , by inducing the cytochrome P-450 (C YP) mediated metabo li sm to
.. d' . I <1 I )7'x67 tOX IC Interme lates e.g. acetumllloplen , a cohol - ._ C . ,
. . . d4 94 1 I . . 14 . 4 Isonl azl .. , va prolC aCl e an ti cancer drugs and nutriti onal status2(, . Chronic excess i ve alcohol ingesti on decreases the dose threshold and enhances the severity of acetaminophen induced hepatotoxicit/,l, increases the ri sk and severit y of isoniazid hepatiti s. Many ex trahepati c mani festation s may be seen in conjugation with certain lIledicinal agents as part of clini ca l spectrum6
.. I. Hallmarks of hypersensi ti vity
reactions such as fever, rash, anthralgias and eos inophili a, point to an immunoa llergic basis of Injur/1.64
Diagnosis of drug-induced liver disease Drug-i nduced liver di sease is discovered by fi ndi ng
abnormalities in hepatic assoc iated enzymes" or, in some cases, by the deve lopment of hepatiti s-like
r · d' JH·11 4' Th d' . f sy mptoms 0 jaun Ice .. -. e lagnoSlS are 0 ten

1230 INDIA J EXP BIOL, 'OVEM I:l ER 2003
based on a high index o f clini ca l suspIcion and whether the implicated drugs fit the known description has similarl y reported cases. A temporal relati onship is usuall y ev ident w ith an impli ca ted drug, vvith most cases o f acute drug- induced li ver disease occurring w ithin I week to 3 months of exposure. A positi ve response to discontinuing the agent ( Ie-challenge) cnhances the suspIcion espec iall y when the biochem ica l and clinical manifestations of the injury subside rapidl y . The general rul e is a 50% reduction in hepatic associated cnzymes after 2 weeks, w ith a return to normal by 4 weeks in cases of acute hepatocellular injury. Drugs causing cholestati c inj ury may have a more prolonged
. (,·1 . . I II recovery Ii III . A POS l tl ve re-c 1a engc to a suspected drug may be a definiti ve means of confirming drug-induced li ve r di sease but thi s is generall y not done, especiall y when dea ling w ith agcnts ca using hepatoce llular necros is, because a more severe react ion may prec ipitate hepatic failure.
Early detection It is :1 criti cal point to warn patient s to rcport an)'
untoward sy mptoms, part icula rl y unexp lained nausea, malai se. ri ght upper quadrant abdomina l pain , leth argy or !'e ve/'·x. These non-speci fic fea tures may rcpresent the prodrome of drug-induced hepatitis. They are th c indic:llions to perform li ve r tes ts and if the results suggest li ver injury, to stop trea tment. A more difficult issue is protoco l screeni ng \-vith li ver te;. ts. A lthough o ften recom mended by authors and drug m:lIlufact urers. it s efficacy and cost effectiveness arc unknown. It has been shown thalthc onset o f li ver injury is o ften rapid , rendering monthl y or even second sc reening fu ti !e6 I f li ver tes ts are monitored. the Ieve! uf abnormal ity at which drugs shou ld be discontinucd is often uncert ain. A class ic::! example is isoniaz id , which causes some li ver test abnormality in 30% of exposed subj "cts9 Generall y. it is rccolll mended th al the drug be stopped if ulanine tran sferase (A LT) va lues exceed 250 l UlL or more than 5 times the upper limit of the normal, but th e prc;.ence of :Ibnormal iti es in serum bilirubin 0 :'
albu min concentrations or pro thrombin time provides a clearer indicati on to stop therap / . Conversely, a ri se in GPT or minor elevati on of SAP does not usually ind icate li ver injury. Protocol screening is not rou tinely reeommended, but could be use ful for agen ts such as isoniazid (INI-I) because the onset o f li ver injury may be delayed and gradual in some cases to underscore the hepatotoxi c potential of particular
drugs in the minds of pati ents and ph ys ician '. Acti ve management might include removal of the drug and the administrati on o f ant idotes and anti-inflammatory
d . 1·?5
an cy toprotec tl ve agents' - .
Preventioll am/managemellt With the excepti on of acetami nophcn hepato
tox icity there is little effecti ve treatment for drug -induced li ver di sease. Thi s puts a spec ial onus on preven ti on and earl y detec ti on of li ver injury as we ll as on prompt w ithdrawa l of the o ffending agent. The majority o f drugs associated w ith drug - induced li ver di sease are idiosyncratic hepatotox insfl
.x.4. Thu s, li ver
injury occurs rarel y . The overa ll incidence of adverse hepati c react ions can be minimi zed on ly th rough avo idance of ove ruse of thcse drugs6 Sim ilarly, polypharmacy should be avoided where pDssible7
The rarity of adverse drug react ions also means that the hepatotox ic potcntial of new agents may not be recogn ized until after their induct ion. Thus, all phys icians share th e responsibi l i ty to rt:po rt sllspeclcd advcrse crfects to mon itoring agenc ics during postmarketing surveillance Df new drugs. For those dependent hepatotox ins, prevcn ti on i" dependent on adherence to dosage guidelines or use o f blood leve ls. Thi s approach has virtuall y abo li shed so me forms o f drug-induced li ver injury. In cases w i th specific ri sk fac tors. strateg ies 10 avo id tox icit y are essen tial.
References I Wong W M . Wu p c. Yucn M F, Cheng C C, Yew W W.
WOllg I> C. TallO C ~ 1'1 al ., A nt i tubcrc ulosis e1rug-n:lalcd li ve r dys functi on In chron ic hcpalit i , B i llkclilJn. I " 'fI(lIologv, 3 1 (2000) 20 I.
2 Wu J C. Lee S O. Yell P F, Chall C Y. W,II1g Y J, Il u;lIlg Y S, T sa i Y T el 01 .. lson i;I /.id-rifalllpici n illduccd hcpalili s III
hepat iti s B carrier, G(/VIl'Ol' llI mlogv, 9R ( 1990) 502. :; Mitehcll J R. Thorgc irss(l ll P. Black M. Timbrel J .A.
SilO Igrass W R. POller W Z, Joll ow 0 J 1'1 al .. Increascd incidcncc or isoni aLiel hcpatiti s in rapid aCC!y l:ilOr: Possibk relalion 10 hyelrazinc Il1ctabolites. Clill Pll({mlUcol Tiler . I X ( 1975) 70.
-l Z immcrman II J. I kpaloloxicily: Th \.: ad verse erkcts or drugs and mher chemicals on lil\.: l iVl' r (A pplc({)Il -CellILII') ' Cru rIs. Ncw York) t97H.
5 Ce lltrc ror e1i sease eO l1l rol. National conscniU, conk rcncc on tubercu losis pn;ventivc Ireatmcnt o r tubLTeuloi is. CI,t'SI. H7 (suppI2) ( 19H5) 128.
6 Lcc W M. Ol'ug-induccd hcpalOlOxicity, N t:lIg l ) Mer!, 333 ( 1995) 111 8.
7 H W<l ll g S J, Wu J C, Lee C N, YCIl F S. Lu C J, l. in T P & Lcc S D. A Pl'Ospccti vl' cli nical slUdy or isonia/.idrirampi cin·pyrazinamide- ineluccd l ivcr injury in an area cndcmic 1'0 1' hcpatitis, Br) GaSll'Oelllerol /-felli/wi. 12 ( 1997 ) 87.

HUSSAIN el 01.: ANTITUBERCULOS IS DRUG-I DUCED HEPATITIS 123 1
8 DeLeve L D & KaplowilZ M <.:c hanism of drug- induced li ver di sease, Casi melll l'mi Clill Nonh Alii , 24 ( 1995) 787 .
9 Dickinson D S. Bai ley W C. HirchowilZ B I. Soong S J, Eidus L & Hidgkin M M , Ri sk faeLOrs for isoniazid (INH)induced li ve r dys funclion. J Clill CaslroellIerol . 3 ( 1981) 27.
10 Fontana R J & Warkins P B, Genelic predispositi on to druginduced l iver di sease. Ca.\"Imelllerol Clill Nonh Alii . 24 ( 1995) 8 11 .
II Lesobre R, Ru ffino J el 01 .. Les iclerus au cou rs du lraitmenl par la refumpicine, ReVile Tllberculose Pllewllolog ie. 33 ( 1969) 393.
12 Parrh asan hy R. Sarm G R, Janardhan B. Ramchandran P. Santha T. Sivasubramanians, Somasundram P R 1'1 al., Hepati c tox icilY in soulh Indian palieills during lrealmenl of llI be rcu lo,is with shon -course regimcns conlaining isoniazid,rifampicin and pyraz inamide. Tllbercle . 67 ( 1986) 502.
13 Sarma G R. Immanuel C, Narayana A S & Venkatesan P. Rifampicin -induced release of hydrazine from isoniazid .A possiblc causc of hepatili s during lrealment of tu berculosis with regimens containing isoniaz id and rifampicin , 11 111 Re\' Re,lpir Oil', 133 ( 1986) 1072.
14 Lees A W. Asgher B. Hashein M A & Si nha B N. Jau ndice afte r rifampicin. Br J Dis Chesl , 64 ( 1970) 90.
15 Steele M A. Burk R F & DesPrez R M. Tox ic hepal iti s with isoniazid and ri famp icin. A metaanalysis. Cllesl , 99 ( 199 1) -U:'5.
16 Aw T Y CI 01 .. Hepati c dl'ug mctaboli sm and drug- induced li ver injury. Cllrr t-IefJ {l/o l . 5 ( 1985) 11 3.
17 Bi ssell D M. Gores G J. Laskin D L & Hoo fnagle J H, Druginduced li ve r injury : Mechanisms and test syslem. t-Iepillologr. 33 (200 I ) 1009.
18 Black M . Mitchel l JR. Z imillerm an H J, Ishak KG & Epler G R. Isoniazid assoc i:ilcd hcpatiti s In 11 4 pali ents. Casiroell irolo!!.\', 69 ( 1975) 28.
19 Byrd C R B. Horn B R, So loillon D A & Griggs G A . Toxic cffects of isoniazid in llIberculosis chcmoprophy lax is: Role of biochemica l mon itor ing in 1,000 pati cnts. JAMII , 2-11 ( 1979) 1:239.
:20 Rao N K. Wad ia R S, Karvc S R & Gran t K B, Hcpatotox icity of antituberculosis drugs . .1111'1, 30 ( 198:2) 295.
2 1 Kamat S R. Mahashur A A. Dubcy G R & Gormade MY, Hcpatotoxicity in shon coursc chemolherapy. LIIIII( I lldia. I ( 1 9~3) 257
:22 Guru munhy P, Krishnaillurthy M S. Nazan:th O. Panhasanhy R. Sarma G R. Somaasundram P R. Tri pathy S P 1'1 al ., L~lC l-. of relationship between hcpal ic toxic ity and accty lator phenolypc in threc thousand south Indian pati ents du ri llg treatlllc'nt \\ ith i,unia /.id during tu berculus is. Alii Re\' Respi r Dis. 129 ( 19R4) SR.
23 Kopannll D C. Snider D E & Caras G J. Isolli azid-relat ed hepati tis a U publi c he:.ll th ,crvice cooperati ve surve ill ance sludy. Alii NI' I' R<'Spir iJ is, 11 7 ( 1978) 99 1.
2-1 Lauterburg B H. Smith C V, Todd E L & Mitchell J R. Pharmacok inet ics of the tox ic hydrazinc Illetabo lites formed from isoniazid in human s. J Phamwcol Exp Tile r. 235 ( 1985) 5(\6.
25 Mcilleron H. Wash P, Burgcr A . Folb P & Smith P. Widespread distribut ion of a singlc drug ri fampici n formul ation of in I'c ri or bioavailabi lilY in Soulh Afri ca. 111/ J Tll berc I_Illig Dis, 6 (2002) 3S(i.
26 Pande J ,S ingh S P N, Khilnani S & Tandon R K. Ri , k factors ror hepaloLOx ieit y from anlitubcrcu los is drug: A casc control study. Thorax, 5 1 ( 19%) 132.
27 Johannson I & Ingelman-Sundberg M , Carbon tet rachloride induced lipid pcrox idalion depcndent on an elhanol-inducib le form of rabbil li ver microsomal PASO. FEBS Lell. I R3 ( 1985) 265.
28 Morgan E T el al ., CatalYlie activ it y of cy tochromc P-450 isoenzy me 3a.i solaled from li ver microsomcs of ethanol lrealed rabbi ls. J Bioi Chelll , 26 ( 1982) 1395 1.
29 Potenza C L , Pendunhi U R, Slorm D K & Tukey R H, Regulati on of the rabbil Cy tochrome PASO 3c gene, J Bioi Chell/ , 264 ( 1989) 16222.
30 Ryan D E, Ramanathan L , Li da S, T homas P E. Haniu M . Shi ve ly J E, Lieber C S el al. , Characleri zation of a major form of rat hepatic microsomal cy tochrome P-450 induced by isoni azid, .1 Bioi Chelll , 260 ( 1985) 6385.
3 1 Fare II G C, Drug- induced acule hep:.llili s. (Churchi l l Li vi ngstone. Ed inburgh) 1994,247.
32 FOl1lana R J & Warkins P B, Genclic predi sposi l ion to druginduced li ver disease, Casiroellierol Clill Nonh Am. 24 ( 1995)8 11.
33 Gupla P R, Purohit S D, Sharma T N, Sharma M L 1'1 al., Hcp:.llo tox ic of isoni az id-ri rampici n-pyrazi nam ide thcrapy, Lllllg Illdia, I ( 1983) 2-15.
34 Scheur P J el al .. Rifampic in hepat i tis: A clinical and hi sto logical study, Lall cel , I ( 1974) 42 1.
35 Schwab G E. Raucy J L & Johnson E F, Modulati on of rabbit and human hepa ti c' cy tochrome PASO catalyzcd steri od hydroxy lation by al fa Napthonavonc. Mol Plw /'I llacol. 33 ( 1988) 493.
36 Theodcre A, Hoeven V & Coon M J, Preparati on and propenics of pania ll y purified cy tochromc PASO and reduced nicot inamide adcnine dinucleotide phosphatecy tochrome P-450 reductase from rabbit l iver microsome., J Bioi Chelll. 2-19 ( 1974) 6302.
37 'vVatkins P B, Role of cy tochromc PASO in drug metaboli sm and hepatotoxicit y, Seill i ll Live r Dis, 10 ( 1990) 235.
38 Yamamoto T. Suou T & Hiryama C. Elevaled se rum :lIninol ransferase induced by isoni az id in rclati on to ison iazid ace ty lator phenotypc. Hepl l/olog.l', 6 ( 1986) :295.
39 Blum M , Dcmierr. A, Grant D M. Heim M & Meyer A. Molecu lar mechanism of slow acety lal ion or drugs and ca rcinogens humans. Proc Nml Acad Sci USA. 88 ( 199 1) 5237.
40 Dcguchi T. Mashimo M & Suzuk i T. Corrclati on between acciy lator phenolypcs and gcnotypes or polymorphic ary lamine I-acc tyll ransrcrase in human li ve r. J Biul Chell/. 265 ( 1990) 12757.
4 1 Gari baldi R A el ai., I so niaz id ~ a ssoc i ated hepatitis : rcport of an outbreak , Alii Ne\' Nespir D is. 106 ( 1972) 357.
42 Gronhagen-Ri ska C, Hell strom P E & Fro,eth 13 , Pred ispos ing fac tors ill hepati ti s induced by isoniuzidrifampicin trca tment of tuberculos is. Alii Nel' i?e.I'I'ir Dis. 11 8 ( 1978)-16 1.
43 Bell D A, Taylor J A. Butl cr M A , Stephens E A. Wicst J. Brubaker L H. Kad lu bar F F 1'1 af., Gcnotype I phcnotypc discordancc for human arylum ine N-ace ly ltransfe rasc (NAT2) rcvea ls :1 new slow aeely lalor al lcle common in African-A merican, Carcill ogl' lIesis, 14 ( 1993) 1689.
44 Blum M , Granl D M. I-kim H, Mcyer U A el al ., Human ary lamines N-acetyllransferase genes: isolation, chromosomal

1232 INDIAN J EXP BIOl, NOVEMBER 2003
loca li za ti on and functi onal ex press ion, DN!I Cell Bioi. 9 ( 1990) 193.
45 Cascorbi , Drakouli s N, I3rockmo llcr J, Maurer A , Spcr l ing K & Roots I. Ary lamines -acety llransfcrasc (NAT2) mu tations and their all cli c linkage in unrclatcd Caucasian individuals: correlation w ith phenotypic activity, Alii J 111/111
Gent'/. 57( 1995) 5, I. 46 Doll M A , I'ret land A J. Dei tz A C & I-Icin D W.
Determination or Human NAT2 accty laLOr gcnotype by rcstri ction rragmcnt Icngth polymorph ism and allek- spcc ifi c amplification,. Allal Biocitelll . 23 1 ( 1995) 41 3.
-t7 Ebisawa T & Deguchi T . Struc ture and restri cti on fragment length polymorph ism of gencs ror human li ver ary laminc acc ty ltransfcrase. Biocit t'11i iliopitvs Nt's COIiIl IIUIi. 177 ( 1991 ) 1252.
-t il Ferguson R J. Doll M A. Rustan T D. Gray K & Hein D W, Cloning, express ion and runcti onal charactcri zat ion of tlVO mutant (NAT2- 19 1 and AT2- 34 1/i1(3) and wild type human polymorph ic N-accty ltransrcrasc (NAT2) all cles. Drtlt: M ew/Jol D is/los, 22 ( 1994) 37 1.
-t9 Dicki nson D S. Bailey W C & Hirschowitz B I, The effcc t or acetylati on sta tus of isoni az id (IN H) hepatiti s. Alii Rev Nt's/lir D is, 115 ( 1977) 395.
50 Kostas P. Vat sis. Karen J. M ancil & Webcr W W. Di vcrsc point mutations in thc hUlIlan gene 1'0 1' po lymorph ic :Icctyl tran srcrasc, Proc N([/I !lead Se USA. 8~ ( 199 1) 6333.
5 1 l in II J. Han C Y. lin B K & Hardy S. Ethni c distrlbu!ion or slow acc ty lator mutati ons In the polymorphi c N acety llransrerasc ( IAT2) genc, PllOrlllilcogt'llesis. -t ( 199-t ) 12-t .
52 L in I I J. Han C Y. Lin K 13 & I lardy S. Slow accty lator mutat ions in th t: human polymorphic N-acct y llransk rasc 2 gene in ni6 As ians, Blacks. I l ispanics. Whit t:s:A ppli cat ion to mctabol i-: epidcmiology, , \ 111 J !-IU/Il Cellel. 52 ( 1993) 817.
53 Mala~ M . Th ygescn P. Stacey M. Ri sch A & Sim A, M apping ACC I . ACC2. and AACP. thc gencs for ary lalllincs I-acety ltransfcrases. carcinogcn metaboli zing cnzymcs on
human chromosomc 8p22,a region frcquentl y delctcd in tumors. C.I'IfJgt'II(' 1 Cdl Ct' lIel , 77 ( 1997) 290.
54 Huang (' I al ., Polymorphi sm of N-accty ltransfcrase 2 Gcne as a susccpt ibili ty ri sk ractor for antituberculos is drug-induced hepatit is, !-Iepawlugy, 35 (2002) 883.
55 Bluill M. Dcnlierc A , Grant D M . Heim M & M eyer U A ,. M olecular mechanism or slow acety lation of drugs and
carcinogcns humans, Proc N([{ I Acad Sei USA . 8i1 ( 199 1) 5237.
56 Franke S, Kl awitz I, Schnakenberg E, SChOOl W el 01 .. Isolation and mapping or a cos illid clone containi ng the human NAT2 genc. ll i()chell/ ll iopit.l's Ne.' C(/IIlIlIlIIl. 199 ( 1994) 52.
57 Schnakenberg E. Ehc lrs C, Feyerband W, Werdin R. Hubotter R, Dreikorn K & SChOOl W. Genotyping of thc polymorphi c N-acety lt ra nsfcrasc 2(NAT2) and loss or hctt: rozygosity in bladder cancer pati cllls, Cfill C t'Ilt'I, 53 ( 1998) 396.
58 Vatsis K P, Weber W W. Bell D A . Dupret J 1vI . Evans D A. Grant D A er 01., olllenclaturc: for -ae ' ty ltransl'c rase. Geneti c polYlllorphism of cy tochrome P450~E I in a Swedish popUlati on. Relati onship to incidence of lung cancer, PllIlnllacogeliesis, 5 ( 1995) I .
59 Pe l'sson I, Johansson I, l3 crglingn H. Dahl M L , Scidegcrd R. Ry lander R. Rannug A, Hogberg J & Ingell1lan-Sundberg M. FEllS Le{{. ( 1993) 3 19.
60 M eister A , Selecti vc modificati on of glutat hione mctabo li sm, Sciell ce, 220 ( 1983) 547.
6 1 Boycr T D, The glutathionc-S -transk ra se: A n updatc. !-Iepawlogy, 20 ( 1989) 585 .
62 M eycr D T. Co les 13 , Pcmble S E el 01 .. Theta a ncw class or glutathion..:-S-transfcras..:, pu ri fi cd rrom rat and man. ll iociJ elll J, 27-t ( 199 1) -t09.
63 Davies M H. Elias E, Acharaya S el al .. GSTM I null polymorphi sm at the glutathionc-S-transl'crase M I locus: Phenotypc and gcnotype studit:s in patients with primary bi li ary cirrhosis, CUI, 34 ( 1993) - -t9.
64 Lieb..: r C S. Biochcmi cal and mol..:cular basis or al coholinduccd inj ury to li ver and otht:r ti ss ue, . N D ig/. J Med. 319 ( 198R) 1639.
65 Roy B, Chowdhury . Kundu S. Santra A. Dcy 13. Chakraborty M & Maj llllldar P P. Tuberculosis and Li ve r di sease. Increased ri sk of ,1I1l ituberculo, is dru g-induccd hcpatotox icit y in indi viduals with glutathi onc-S -trilnsrerasc M I ' null ' mutat ion. J Caslrol !-Ieparol, 16 (200 1) 1033.
66 Maddrcy W C. Isoniazid- induccd li ver diseasc. Sell/ ill Liver Disease, I ( 198 1) 129.
67 Watanabc J, Yang J P, Eguchi II , Hayashi S, I Ill:.li K. Nakaachi K & Kawaji ri K , A Rsa l polymorphism in the Cy P2EI gene does not alTect lung cancer r isk in a Japancse popUlat ion, }pII} COil Res. 86 ( 1995) 245.