Embed Size (px)
Citation preview

IDologist.com
Antimicrobial Use in Clinical Practice
Dr. Andrew M. MorrisMt. Sinai Hospital/University Health Network
Department of Medicine

IDologist.com
Introductory tipsdon’t learn too many individual antibiotics—no doctor should know more than about a dozen antibiotics
try to understand principles rather than specifics, and don’t bother learning dosages
Dr. Vellend covered many of the basic principles surrounding antimicrobial use ... any repetition is deliberate (to aid in recollection)

IDologist.comAn example of an antimicrobial repertoire
amoxicillin/ampicillin cloxacillin piperacillin-
tazobactamcephalexin/cefazolin cefotaxime or ceftriaxone
azithromycin or clarithromycin clindamycinmetronidazole
ciprofloxacin levofloxacin or moxifloxacintrimethoprim-sulfamethoxazole gentamicin
vancomycin

IDologist.com
Antimicrobial rules to live bytreat the patient, not the lab reportdon’t take credit for curing a self-limited disease with antibioticsdon’t use broad-spectrum, risky, expensive or new antibiotics for treating mild/minor infectionsdon’t treat a fever with antibioticsdon’t stick with a losing combinationi.v. antibiotics should be avoidedthe best antibiotics are made of steelwhen the stakes are high, don’t be a minimalist

IDologist.comCase 1
45 yo woman, previously wellworks as a pharmaceutical rep; triathleteallergic to penicillin (hives)because of genetic screening, had bilateral prophylactic mastectomies (with plan for tissue expander → breast implants)post-operatively, wound healed well: a drain was left in situ (for a seroma), and the clinic nurse sent the fluid for Gram stain and culture prior to removing the drain

IDologist.comCase 1
www.psinteractive.net

IDologist.comCase 1
Date: 2008.11.01 (14:09)
Patient: Merrick, Linda H. (10293487)
Requesting MD: Singh, P.J.
Specimen: Surgical wound (collected 2008.10.29)
Gram: No pus cells. Many gram positive cocci, few gram positive bacilli
Culture: Isolate 01 Staphylococcus aureus, heavy growth
amoxicillin Rciprofloxacin Scefazolin Sclindamycin Scloxacillin Scotrimoxazole Stetracycline Svancomycin S

IDologist.com
Case 1
What antibiotic should you start?
What class? What route? How would you monitor response to therapy?

IDologist.com
Rule #1
Treat the patient, not the lab report

IDologist.comCase 2
15m old toddler, malefirst-born child to social worker and primary school teacherpreviously healthy, appropriate achievement of ages/stages/milestoneshas had fever, irritability, and decreased food intake for >24 hoursparents say that the “only thing that helps is Tylenol”

IDologist.comCase 2
physical exam is noteworthy for a healthy-looking child who is crying, febrile (38.1℃), with a dull right tympanic membrane
Dx: acute otitis media

IDologist.com
Case 2
Should you start an antibiotic?

IDologist.comAntibiotics and acute otitis media (AOM)
whether or not to give antibiotics for AOM is controversial (meaning “we don’t yet have a clear answer”)practice guidelines around the world vary regarding antimicrobial approach to AOMin Ontario, the Guidelines Advisory Committee recommends ABx for any symptomatic episode of AOMin the Netherlands, guidelines recommend, initially, analgesics alone for symptomatic AOM in children over 6 months of age

IDologist.comEstimated antibiotic prescriptions dispensed by
month in Canadian retail pharmacy
0
400,000
800,000
1,200,000
1,600,000
2,000,000
Jan03Feb0
3Ma
r03Ap
r03
May0
3Jun03Jul03Au
g03Se
p03Oc
t03No
v03De
c03Jan04Feb0
4Ma
r04Ap
r04
May0
4Jun04Jul04Au
g04Se
p04Oc
t04No
v04De
c04Jan05
p.o. solids p.o. liquids (≃kids)
http://www.ccar-ccra.com/

IDologist.com
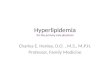
Antibiotic consumption correlates with resistance
Frequency of resistance to erythromycin among Group A Strep isolates from throat-swab and pus samples in Finland in 1990 and 1992-96
Total consumption of macrolide antibiotics by outpatients in Finland from 1976-95
NEJM 1997;337:441-6

IDologist.com
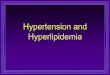
Wait-and-see prescription vs Up-front Abx for AOM
one study randomized 283 kids (age 6m-12y) to either a wait-and-see prescription (WASP) of antibiotics or a standard antibiotic prescription
0%
20%
40%
60%
80%
100%
Script filled Fever Ear pain Diarrhea
WASPStandard ABx Prescription
JAMA 2006;296:1235-1241

IDologist.com
Rule #2
Don’t take credit for curing a self-limited disease with antibiotics

IDologist.com
Other examples of diseases where utility of
ABx is questionablesinusitis
acute exacerbations of COPD
boils (following incision and drainage)
endocarditis prophylaxis prior to dental procedures

IDologist.comCase 3
57 yo F, store managerhistory of obesity, diet- and exercise-controlled DM Type 2, hyperlipidemia, hypertension and hypothyroidismpresents to family physician with fever, cough, sputum production, and some mild pleuritic chest pain for 2d

IDologist.comCase 3
physical exam noteworthy for:looks generally well (i.e. not in extremis)T 38.6℃, RR 20, BP 126/78, HR 99oropharynx clearnormal fremitus and percussion, with crackles heard over left lower lung fieldremainder of exam normal/unremarkable

IDologist.com
Case 3
Diagnosis: Community-acquired pneumonia
Should patient be managed as an outpatient or sent to ER?What antibiotic(s) should be used to treat her?

IDologist.com
Community-acquired pneumonia
there are 2 algorithms that are recommended to predict severity of CAP: CURB-65 and Pneumonia Severity Index (PSI)using either of these algorithms, this patient is “low risk”

IDologist.com
CURB-65
CURB-65 (Confusion, Urea > 7, RR > 30, BP < 90mmHg systolic or 60mmHg diastolic, age > 65)
easy, fast
relies on mostly clinical factors ... but is unreliable to guide site of care
Am J Med 2005;118:384-392Eur Respir J 2006;27:151-157

IDologist.com
CURB-65
CURB-65 30-day mortality:0 0.7%1 2.1%2 9.2%3 14.5%4 40.0%5 57.0%

IDologist.com
PSIstratifies patients into 5 groupsa collection of 20 variables, predominantly historicalderived from 1 cohort and validated with another cohortuptake has been rather low, but PSI calculators are readily available (e.g. http://pda.ahrq.gov/clinic/psi/psicalc.asp)
NEJM 1997;336:243-50

IDologist.comWhat antibiotics to use
for outpatient CAPthe Brits recommend penicillinsthe Aussies recommend penicillins or doxycycline for low-riskin N. America, macrolide or doxycycline are recommended for very low risk, but with underlying co-morbidities (e.g. heart, lung or renal disease, DM, alcoholism, etc.) a respiratory fluoroquinolone OR a β-lactam + macrolide are recommended

IDologist.comOutpatient CAP
controversy exists over what is the best choice because:
microbiology would suggest covering “atypical bacteria” (e.g. Legionella, Mycoplasma, and Chlamydophila) is necessaryresistance patterns suggest that macrolides are not a great choicecost considerations are a matter of perspective

IDologist.com
Covering “atypical bacteria” doesn’t seem to matter
Number of patients failing to achieve clinical cure or improvement with β lactam antibiotics compared with antibiotics active against atypical pathogens in all cause non-severe community acquired pneumonia
BMJ 2005;330:456-62

IDologist.com
Newer antibiotics are usually more expensive
Approximate cost for 5 days’ treatment:amoxicillin 1g q8h = $10 (generic)doxycycline 100mg bid = $12 (generic)cefuroxime 500mg bid = $20 (generic)azithromycin 500 mg then 250 daily = $22 (generic)clarithromycin 500mg bid = $26levofloxacin 500mg daily = $28moxifloxacin 400mg daily = $34amoxicillin-Clav 2g bid = $44

IDologist.com
New antibiotics might carry a safety risk
grepafloxacin removed in 1999 due to safety concerns regarding fatal cardiac arrhythmiassparfloxacin removed in 2001 due to phototoxicitytrovafloxacin removed in 2001 due to hepatotoxicitygatifloxacin removed in 2006 due to dysglycaemiagemifloxacin causes rash in 32% of women <40 yrstelithromycin carries a black box warning regarding hepatotoxicity

IDologist.com
Case 3Dx: outpatient community-acquired pneumoniaamoxicillin or another oral β-lactam (e.g. cephalosporin) seems reasonableguidelines would also support broader coverage (e.g. doxycycline, macrolides + β-lactam, or respiratory fluoroquinolones) but does the patient’s CAP risk justify broader/newer coverage?

IDologist.com
Rule #3
Don’t use broad-spectrum, dangerous, expensive or new antibiotics for treating mild/minor infections

IDologist.comCase 450 yo M, truck driver currently on disability benefitshistory of hypertension, hyperlipidemia, smoking (50 pack-years), obesity, asthma and osteoarthritispresents to ER with fever, cough, retrosternal chest pain and SOB x 4 daysphysical exam largely unremarkable, although looks unwell, has ↑RR/↑HR, 38.1℃ and requires supplemental oxygen

IDologist.comCase 4
chest x-ray unremarkable (apart from some evidence of emphysema)CBC: Hb 125 g/L (slightly low), WBC 19.7 x 106/L (high) with neutrophilia, platelets 510 x 109/L (slightly high)chemistry normalurinalysis normalECG: sinus tachycardia

IDologist.comCase 4
Dx: community-acquired pneumoniastarted on levofloxacin 750mg dailygiven enoxaparin for DVT prophylaxisafter 24hrs afebrile, albeit remains tachycardic and tachypneic--doesn’t feel betterrepeat CXR reported as normaldischarged home on levofloxacin 750mg daily, but returns to ER within 8hrs with worsening SOB

IDologist.comCase 4
patient was seen by ER doc, who prescribed amoxicillin-clavulanic acid, and was discharged from ERpatient went to pharmacy to fill prescription, but suffered a cardiac arrest and died at the pharmacycoroner notified, who ordered an autopsy

IDologist.comCase 4
Diagnosis at autopsy: massive pulmonary embolism

IDologist.com
Rule #4
Don’t treat a fever with antibiotics

IDologist.comCase 5
66-year-old woman admitted for CAPhistory of COPD, penicillin allergy and chronic lymphocytic leukemia (not currently requiring Rx)had received a 10d course of ciprofloxacin 6 months earlier and a 10d course of levofloxacin 1 month previously, both for the treatment of an acute exacerbation of COPD

IDologist.comCase 5
2 wks before admission, URTI developed. 8d before admission, ciprofloxacin was begun because of respiratory symptomsat admission, her clinical condition had deteriorated, and she was found to have a RLL/RML infiltrate and a small right-sided pleural effusionblood cultures grew S. pneumoniaeRx was switched oral levofloxacin daily

IDologist.comCase 5pleural fluid cultures on the fourth hospital day grew S. pneumoniae.on 5th hospital day, septic shock developed and patient died the following dayeventually, testing was performed which demonstrated fluoroquinolone-resistant S. pneumoniae
NEJM 2002;346:747-50

IDologist.comCase 5
post-mortem testing was performed on the blood and pleural fluid isolates which demonstrated fluoroquinolone-resistant S. pneumoniae
NEJM 2002;346:747-50

IDologist.com
Rule #5
Don’t stick with a losing combination

IDologist.comCase 6
12 year-old F, at camp, with insect bite to armsubsequent erythema, swelling, warmth and pain surrounding insect bite over course of hoursafebrile, stable, feels otherwise welladvised by camp MD to go to ER

IDologist.comCase 6
WBC 13.5 x 106/Lremainder of bloodwork normalstarted on i.v. cefazolin for 14d for cellulitis ... and camp fun was ruined

IDologist.comCellulitis
~ 80% of cellulitis is caused by Group A Streptococcus (most of remainder caused by methicillin-sensitive S. aureus)there is no penicillin-resistant Group A Streppatients rarely get very sick with cellulitis5 days levofloxacin is as good as 10 days

IDologist.comCellulitis
“e disease is self-limited and a large majority of the cases get well without any internal medication. I can speak definitely on this point, having, at the Philadelphia Hospital, treated many cases in this way.”
William Osler, M.D.e Principles and Practice of Medicine: Designed for
the use of practitioners and students of medicine.New York, Appleton and Company. 1893

IDologist.com
Rule #6i.v. antibiotics should be avoided ...
... and remember Rule #2: don’t take credit for curing a self-limited disease with antibiotics (although almost all MDs would treat cellulitis with antibiotics)

IDologist.comCase 739 yo M undergoing radiation therapy for intra-abdominal lymphomacurrently on prednisone 20mg dailyno prior antimicrobial therapypresented to ER in septic shock, with BP 65/pulse, HR 140, RR 40, T 38.7℃oxygen saturation on 100% O2 by non-invasive positive-pressure ventilationchest x-ray: diffuse white outabdomen rigid ... CT abdomen pending

IDologist.comCase 7
www.surgical-tutor.org.uk

IDologist.comCase 7
Dx: Peritonitisantibiotics? Which ones?what else?

IDologist.comCase 7
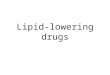
http://radiographics.rsnajnls.org/cgi/content-nw/full/24/3/703/F24
Perforated appendix with peritonitis. Axial contrast-enhanced CT scan shows enhancement and disruption (arrow) of the appendiceal wall. Inflamed bowel wall and severe fat stranding are also present (arrowheads).

IDologist.comPeritonitis in an antibiotic-naive patient
patient needs surgery +/- drains

IDologist.comPeritonitis in an antibiotic-naive patient
need to treat gut organisms (gram-negative aerobes and anaerobes, predominantly)many MDs will also want to cover Gram-positives, although probably unnecessarymany regimens available

IDologist.comPeritonitis in an antibiotic-naive patient
amp&gent OR cefotaxime/ceftriaxone OR ciprofloxacin/levofloxacin
+metronidazole (OR clindamycin)
pip-tazo OR meropenem OR moxifloxacin

IDologist.com
Rule #7The best antibiotics are made of steel
Rule #8When the stakes are high, don’t be a minimalist

IDologist.com
Antimicrobial rules to live bytreat the patient, not the lab reportdon’t take credit for curing a self-limited disease with antibioticsdon’t use broad-spectrum, risky, expensive or new antibiotics for treating mild/minor infectionsdon’t treat a fever with antibioticsdon’t stick with a losing combinationi.v. antibiotics should be avoidedthe best antibiotics are made of steelwhen the stakes are high, don’t be a minimalist