Embed Size (px)
Citation preview
Antimicrobial Surgical Prophylaxis: A Pharmacology ReviewPaul Staffieri, PharmD
PGY2 Critical Care Pharmacy Resident
University of Illinois at Chicago
41st Annual ASPSN Convention
October 19th 2015
Objectives
• Discuss antimicrobial coverage for the major classes of antibiotics utilized for surgical prophylaxis
• Evaluate the appropriateness of antimicrobial regimens to individualize therapy
2
We’ve Come a Long Way…
• Prior to the mid-19th century, limb amputation was associated with an alarming 50% postoperative mortality from sepsis.
• Father of surgical aseptic technique: Joseph Lister
Newsom BD. Int J Infect Control. 2008
3

Surgical Site Infections
• 16 million surgeries performed in 2010
• 30 surgeries per minute!
• Reported ~157,000 surgical site infections (SSI)
• ~1/3 of health-care associated infections (HAI)
Magill SS et al. Infection Control Hospital Epidemiology. 2012http://www.cdc.gov/nchs/data/nhds/4procedures/2010pro_numberpercentage.pdf. Accessed Aug 1st 2015
4

Magill SS et al. NEJM. 2014
Most Frequent Types of HAI
Type of InfectionPatients with Type
of Infection (%)Estimated Infections in the
United States
Pneumonia 24.3 157,500
Surgical-site 24.3 157,500
Gastrointestinal 19.0 123,100
Urinary Tract 14.4 93,300
Primary Bloodstream 11.1 71, 900
Ears, nose, throat or mouth 6.2 40,200
Lower Respiratory Tract 4.4 28,500 5

Impact of SSI
SSI
Increased Morbidity Mortality
Increased Length of
Stay
Financial Implications
Anderson AE et al. ICHE. 2008
6
Defining SSI
• Timeframe: within 30 days post-procedure
• Extended to a year if implant involved
• At least one of the following:
• Purulent drainage from the incision
• Organisms isolated from an aseptic culture of incisional fluid or tissue
• Incision deliberately opened by the surgeon when the patient has signs or symptoms of infection such as pain, erythema, or edema
Horan TC, Andrus M, Dudeck MA. Am J Infect Control. 2008
7

Horan TC et al. Infect Control Hosp Epidemiol. 1992
8

Clinical Signs of SSI
Subjective
• Erythema
• Localized swelling
• Pain + tenderness
• Pus/purulent drainage
• Abscess
Objective
• Fever (>38 °C)
• WBC (> 12x10^3 cell/µL)
• Tachycardia (>90 BPM)
• Inflammatory markers
• Erythrocyte sedimentation rate (ESR)
• C-reactive protein (CRP)
Cheadle WG. Surg Infect. 2006
9

SSI Risk Factors
General Surgery
• Duration
• Distal infections
• Age
• Poor hemostasis
• Obesity
• Immunosupression
Plastic Surgery
• Implants
• Skin irradiation prior to procedure
• Procedures below the waist
Cheadle WG. Surg Infect. 2006
10

SSI in Plastic SurgeryHead and Neck: <5%
Oral Pharynx/Larynx: 5-10%
Dermatological: ~5%
Medicalanatomy.net. Accessed Aug 1st 2015Dale WB et al. Am J Health-Syst Pharm. 2013
11
Wound Infection Classification:
Clean: < 5%Clean-Contaminated: 5-10%Contaminated: >10%

http://www.who.int/patientsafety/safesurgery/tools_resources/SSSL_Checklist_finalJun08.pdf. Accessed Aug 1st 2015
12

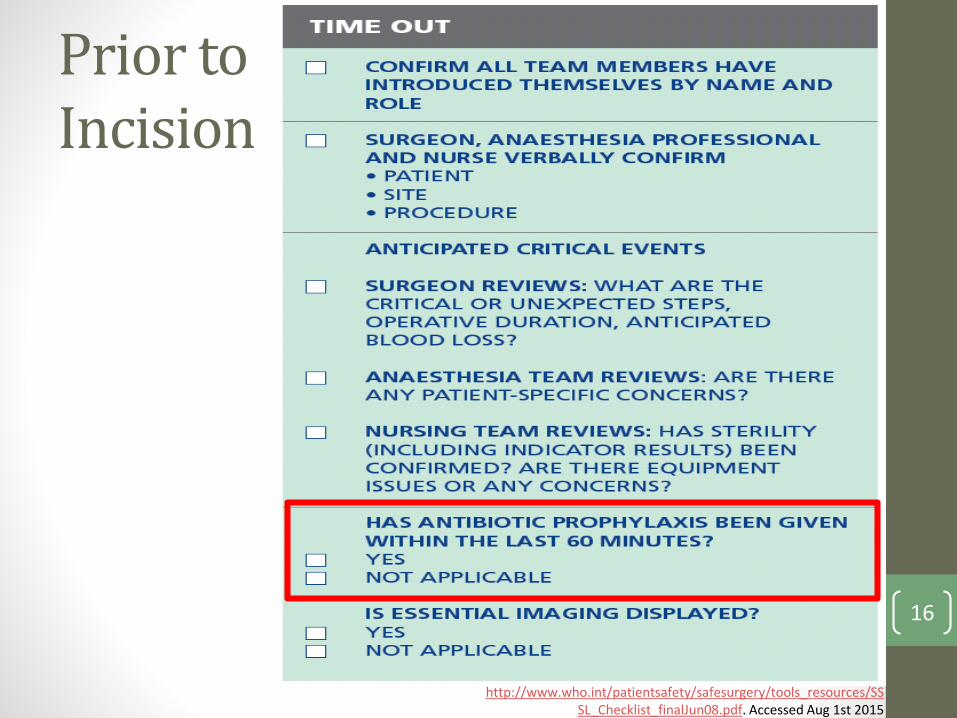
Prior to Incision
http://www.who.int/patientsafety/safesurgery/tools_resources/SSSL_Checklist_finalJun08.pdf. Accessed Aug 1st 2015
13

General Preventative Measures
Hemani ML, Lepor H. Reviews in Urology. 2009
14

Skin Preparation
Proportion of Patients With Surgical Site Infections, According to Type of Infection
Type of InfectionChlorhexidine-
Alcohol (n = 409)Povidone-Iodine
(n = 440)Relative Risk
(95% CI)P Value
Any surgical site infection
39 (9.5) 71 (16.1)0.59 (0.41 –
0.85)0.004
Superficial incisional infection
17 (4.2) 38 (8.6)0.48 (0.28 –
0.84)0.008
Deep incisional infection
4 (1.0) 13 (3.0)0.33 (0.11 –
1.01)0.05
Organ space infection
11 (4.4) 20 (4.5)0.97 (0.52 –
1.80)0.99
Sepsis from SSI 18 (2.7) 19 (4.3)0.62 (0.3 –
1.29)0.26
Rabih OD et al. NEJM. 2010
15
Prior to Incision
http://www.who.int/patientsafety/safesurgery/tools_resources/SSSL_Checklist_finalJun08.pdf. Accessed Aug 1st 2015
16

Pathogens in Plastic Surgery
Dermatological pathogens
• Gram positive cocci
• Pairs and chains
• Clusters
Oropharyngeal pathogens
• Gram positive cocci (pairs and chains)
• Oral anaerobes
Wet/moist environments (pannus, axilla, genitalia)
• Enterobacteriaceae
17
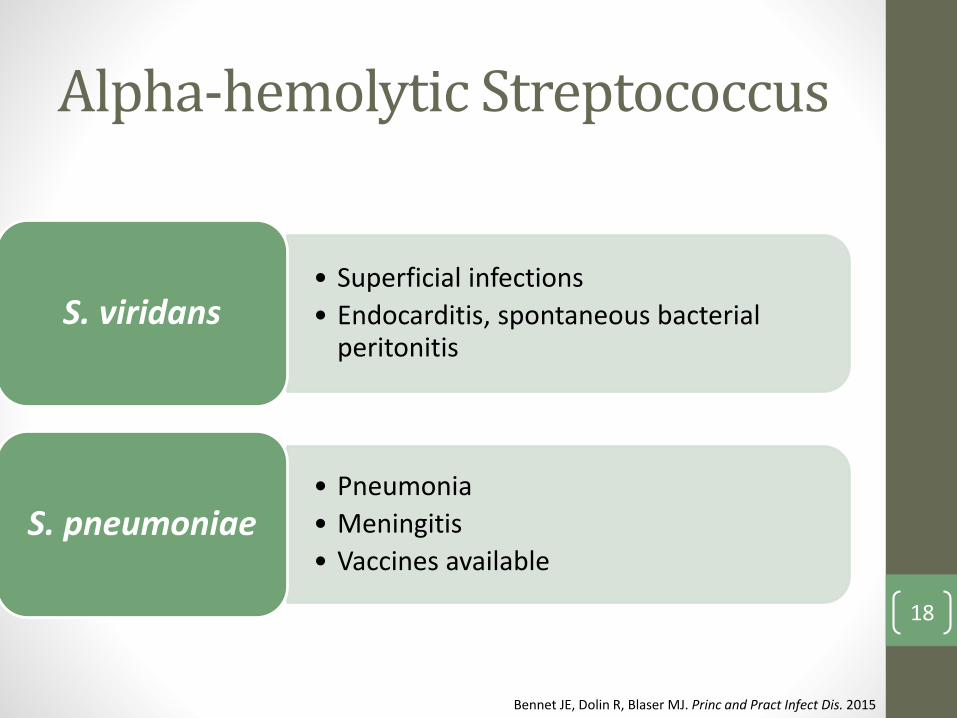
Alpha-hemolytic Streptococcus
• Superficial infections
• Endocarditis, spontaneous bacterial peritonitis
S. viridans
• Pneumonia
• Meningitis
• Vaccines availableS. pneumoniae
Bennet JE, Dolin R, Blaser MJ. Princ and Pract Infect Dis. 2015
18
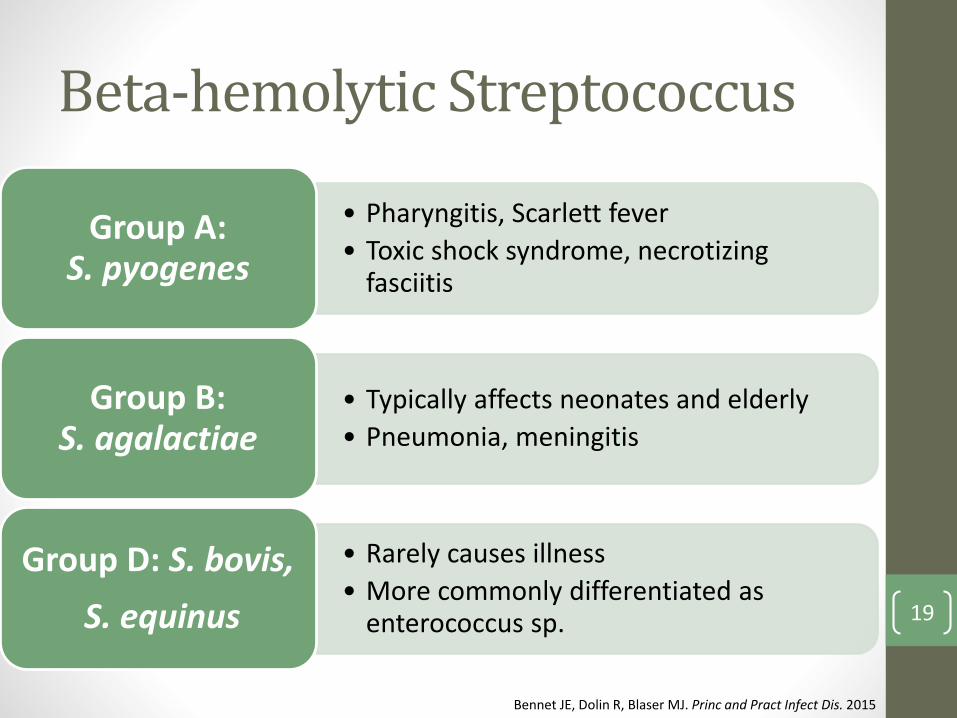
Beta-hemolytic Streptococcus
• Pharyngitis, Scarlett fever
• Toxic shock syndrome, necrotizing fasciitis
Group A: S. pyogenes
• Typically affects neonates and elderly
• Pneumonia, meningitis
Group B: S. agalactiae
• Rarely causes illness
• More commonly differentiated as enterococcus sp.
Group D: S. bovis,
S. equinus
Bennet JE, Dolin R, Blaser MJ. Princ and Pract Infect Dis. 2015
19

Gram Positive Cocci
• Staphylococcus aureus
• Staphylococcus epidermidis
• AKA coagulase-negative staphylococcus epidermidis (CoNS)
https://www.cdph.ca.gov/programs/hai/Pages/MRSAresistancePage.aspx. Accessed Aug 1st 2015
20

Oral Pathogens
• Oral anaerobes• Actinomyces spec.
• Fusobacterium spec.
• Prevotella spec.
• Peptostreptococcus spec.
• S. viridans
• E. coli
Aas JA et al. JCM. 2005
21
Gram Negative Organisms
Wet/moist environments (pannus, axilla, genitalia)
• Enterobacteriaceae
• Eschericia coli
• Klebsiella pneumoniae
• Proteus mirabilis
• Serratia marcesens
• Associated with increased morbidity and mortality
• Decreasing in incidence
Gaynes R, Edwards JR. Clin Infect Dis. 2005
22

Gram Negative Resistance
http://www.cdc.gov/drugresistance/biggest_threats.html. Accessed Aug 1st 2015
23

Antibiotics in Preventing SSI
Guidelines (2)
• Surgical Care Improvement Project (SCIP)
• SCIP INF-1 Antibiotic timing
• SCIP INF-2 Antibiotic selection
• SCIP INF-3 Antibiotics discontinued within 24 hours
• American Society of Health-System Pharmacists (ASHP)
24
SCIP Guidelines (Jan 2015)
SCIP INF-1 – Antibiotic Timing
• Start one hour prior to surgery
• Will vary based on antibiotic infusion time
SCIP INF-2 – Antibiotic Selection
• Safe
• Cost-effective
• Appropriate coverage
SCIP INF-3 – Antibiotic discontinuation (within 24 hours)
Fry DE. Surg Infect. 2008
25

ASHP 2013 Guidelines
Collaboration of the following:
• American Society of Health-System Pharmacists (ASHP)
• Infectious Disease Society of America (IDSA)
• Surgical Infection Society (SIS)
• Society of Healthcare Epidemiology of America (SHEA)
Mirror SCIP recommendations
• Antibiotics 60 minutes prior to incision*
• Discontinuation of antibiotics within 24 hours
*Depending on infusion time of antibiotic
Dale WB et al. Am J Health-Syst Pharm. 2013
26

ASHP 2013 GuidelinesRecommendations for Surgical Antimicrobial Prophylaxis
Type of Procedure Recommended AgentsAlternative Agents in B-lactam Allergy
Strength of Evidence
Plastic Surgery• Clean + risk factors • Clean-contaminated
Cefazolin, ampicillin-sulbactam
Clindamycin,vancomycin
C
Head and Neck (Clean) None None B
Head and Neck• Clean + placement of
prosthesisCefazolin, cefuroxime Clindamycin C
Head and Neck• Clean-contaminated +
cancer
Cefazolin or cefuroxime + metronidazole,
ampicillin-sulbactamClindamycin A
Dale WB et al. Am J Health-Syst Pharm. 2013
27

Principles of Treatment
Choose the antimicrobial agent that should:
1) Prevent SSI
2) Prevent SSI related morbidity and mortality
3) Reduce the duration and cost of health care
4) Minimize adverse effects
5) Have minimal impact on microbiome
28

Antibiotics!
• Beta-lactams
• Penicillins
• Cephalosporins
• Vancomycin
• Clindamycin
• Metronidazole
29

Penicillins
• Mechanism of action: Inhibit bacterial cell wall synthesis
• Resistance increasing exponentially since discovery
• Penicillinase
• Beta-lactamase
• Penicillin-binding proteins (PBPs)
• Beta-lactamase inhibitors (BLI)
• Clavulanate
• Sulbactam
• Tazobactam
• Avibactam30
Classification of PenicillinsSingle Agents
• Natural• Penicillin G
(intravenous)• Penicillin V (oral)
• Aminopenicillins• Ampicillin• Amoxicillin
• Anti-staphylococcal• Dicloxacillin• Nafcillin• Oxacillin• Piperacillin
Combination Products
• Amoxicillin/clavulanate(Augmentin)
• Ampicillin/sulbactam(Unasyn)
• Piperacillin/tazobactam(Zosyn)
31

Spectrum of Activity
• Ampicillin
• Gram positive
• S. pneumoniae
• Group A, B streptococcus
• Poor coverage:
• Gram negatives
• Majority of anaerobes
• S. aureus
• Ampicillin/sulbactam
• Covers gram negatives, anaerobes, and methicillin-susceptible S.aureus (MSSA)
32
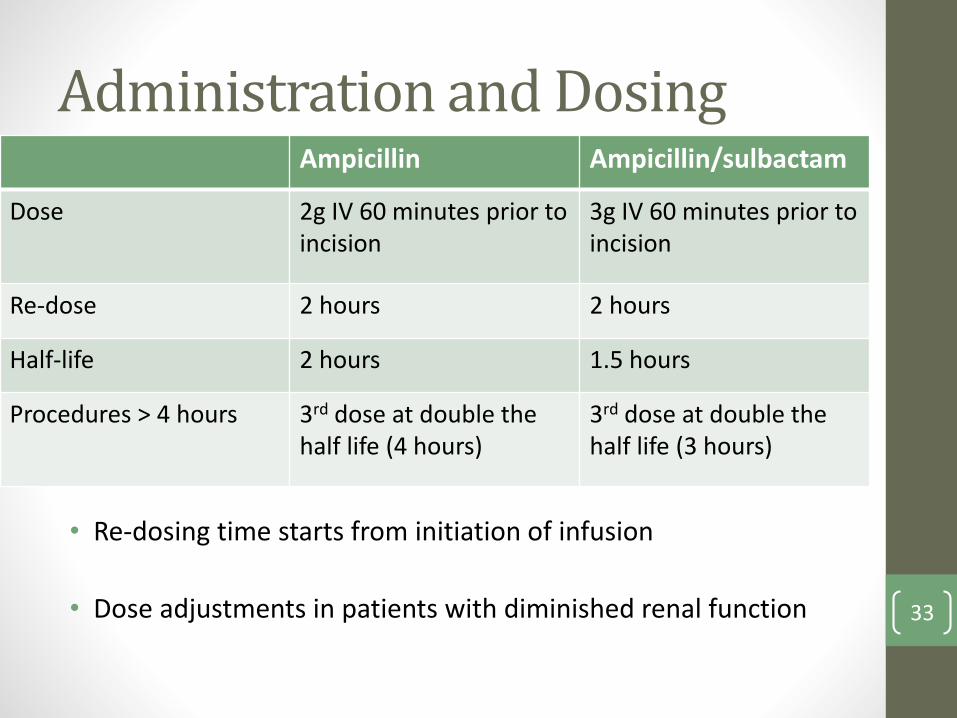
Administration and Dosing
• Re-dosing time starts from initiation of infusion
• Dose adjustments in patients with diminished renal function
Ampicillin Ampicillin/sulbactam
Dose 2g IV 60 minutes prior to incision
3g IV 60 minutes prior to incision
Re-dose 2 hours 2 hours
Half-life 2 hours 1.5 hours
Procedures > 4 hours 3rd dose at double the half life (4 hours)
3rd dose at double the half life (3 hours)
33

Adverse Reactions
• Rash: 4-8%
• Abdominal cramping/diarrhea: 2-5%
• Ampicillin > amoxicillin
• C. difficile infection
• Anaphylaxis ~0.01%
• Seizures: Limited to case reports
Campagna JD et al. J Emerg Med. 2012
34

Cephalosporins
• A few modifications to the penicillin structure = cephalosporin
• Categorized into “generations”
• As you go travel through the generations
• Gram positive activity decreases
• Gram negative activity increases
• *Certain restrictions apply*
35

Cephalosporin Classification
Generation 1 Generation 2 Generation 3 Generation 4 Generation 5
IV Cefazolin CefoxitinCefotetan
Cefuroxime
CefotaximeCeftriaxoneCeftazidime
Cefepime Cefotetan
PO Cephalexin Cefuroxime
Cefprozil Cefdinir - -
36

Cephalosporin Spectrum
Generation 1: Cefazolin
• Active against
• MSSA (variable CoNS)
• S. pneumoniae
• Gram negatives: E.coli, K. pneumoniae, P. mirabilis
• Not active against
• Enterococcus spec.
• H. influenzae
• Enterobacter spec, Citrobacter spec, P.aeruginosa
• Bacteroides fragilis37

Cephalosporin Spectrum
Generation 2: Cefuroxime
• Compared to cefazolin…
• Greater activity against S. pnuemoniae
• Less active against MSSA, CoNS
• Greater activity against gram negatives
• Covers oral anaerobes
• Same pitfalls as cefazolin (enterococcus, MRSA, B. fragilis)
38

Administration and Dosing
• Re-dosing time starts from initiation of infusion
• Dose adjustments in patients with diminished renal function
Edmiston CE et al. Surgery. 2004;136:738-744
Cefazolin Cefuroxime
Dose 2g IV 60 minutes prior to incision3g IV if weight > 120kg
1.5g IV 60 minutes prior to incision
Re-dose 4 hours 4 hours
Half-life 2 hours 2 hours
Procedures > 4 hours 3rd dose at double the half life
3rd dose at double the half life
39
Penicillin Allergies?
• Often over-reported
• Historically, cross-reactivity with cephalosporins ~10%
• Most recent data: ~1%, even less with 3rd generationcephalosporins
• General rule of thumb: If documented anaphylaxis, would judiciously avoid other B-lactams (cephalosporins)
Campagna JD et al. J Emerg Med. 2012
40

Vancomycin
Large glycopeptide molecule
Mandell GL, Bennet JE, Dolin R et al. Princ and Pract of Infect Diseas. 2010
41

Vancomycin Spectrum
• Easy to remember: Gram + only!
• All streptococcus species
• MSSA, MRSA, CoNS
• E. faecium, E. faecalis
• High rates of resistance in E. faecium
• AKA Vancomycin resistant enterococcus (VRE)
42
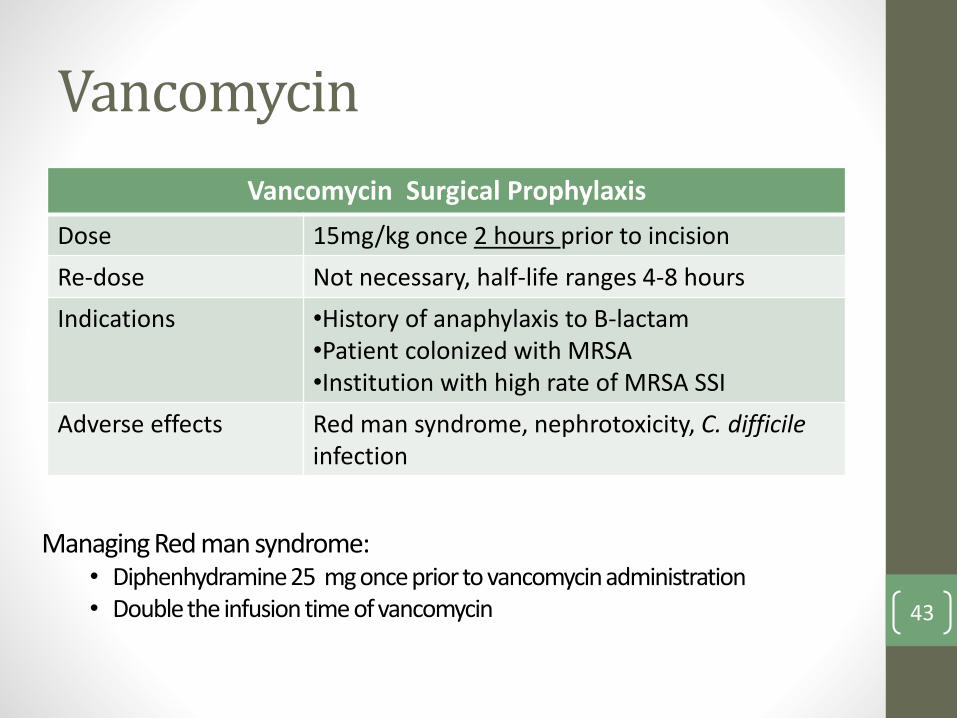
Vancomycin
Vancomycin Surgical Prophylaxis
Dose 15mg/kg once 2 hours prior to incision
Re-dose Not necessary, half-life ranges 4-8 hours
Indications •History of anaphylaxis to B-lactam•Patient colonized with MRSA•Institution with high rate of MRSA SSI
Adverse effects Red man syndrome, nephrotoxicity, C. difficileinfection
Managing Red man syndrome:• Diphenhydramine25 mg once prior to vancomycin administration• Double the infusion time of vancomycin 43

Clindamycin
• Mechanism of action: Inhibition of protein synthesis by binding to the 50S subunit of the bacterial ribosome
• Spectrum of Activity• Gram-positives: Streptococci, Staphylococci (including some
MRSA), Enterococcus (+/-)
• Most anaerobes
• Minimal activity against Gram-negatives and atypicals
• Clindamycin 900mg IV 60 minutes prior to surgery• Can re-dose in 6 hours
• T ½ 3 hours
• For longer procedures, can redose @ 2x half-life 44
Metronidazole
Spectrum: Only covers anaerobes (gram +/-)
• Great tissue penetration (gut, CNS, etc.)
• PO to IV = 1:1
Dose: 500mg IV one hour prior to incision
• Half-life ~6-8 hours
• Guidelines do not recommend re-dosing
Adverse drug effects
• Dilsulfiram-like reaction avoid alcohol!
• Taste perversion (metallic taste)
• C. difficile infection 45

Antimicrobial Resistance
• Lack of data regarding plastic surgery prophylaxis and antimicrobial resistance
• Data does exist regarding both resistance-targeted antibiotics and specific microorganism
• Expert opinion suggests assessing the following:
• Surgical site
• Area of colonization (lungs, GI tract, nares, etc.)
• Penetration of drug to site of infection
46

Antimicrobial ResistancePotential Antimicrobial Resistance Treatment Options
Resistant BacteriaTypical Sites of
InfectionPotential Antimicrobial
Methacillin-resistantS. aureus (MRSA)
SkinNaresLungs
VancomycinLinezolid
Daptomycin
Vancomycin-resistant enterococcus (VRE)
GI tractUrinary tract
LinezolidDaptomycin
Extended spectrum beta-lactamse inhibitors (ESBL)
LungsGI tract
Urinary tract
CarbapenemFluoroquinolones
TigecyclineAminoglycosides
Carbapenem-resistantenterobacteriaceae (CRE)
LungsGI tract
Urinary tract
ColistinTigecycline
47

ASHP 2013 Guidelines RecapRecommendations for Surgical Antimicrobial Prophylaxis
Type of Procedure Recommended AgentsAlternative Agents in B-lactam Allergy
Strength of Evidence
Plastic Surgery• Clean + risk factors • Clean-contaminated
Cefazolin, ampicillin-sulbactam
Clindamycin,vancomycin
C
Head and Neck(Clean)
None None B
Head and Neck• Clean + placement
of prosthesisCefazolin, cefuroxime Clindamycin C
Head and Neck• Clean-contaminated
+ cancer
Cefazolin or cefuroxime + metronidazole,
ampicillin-sulbactamClindamycin A
Dale WB et al. Am J Health-Syst Pharm. 2013
48

Summary
• SSI are preventable adverse events that span throughout the spectrum of surgical procedures
• Recognizing patients and procedures at risk of developing SSI is imperative in stratifying preventative measures
• Understanding the pharmacology of agents which have proven to reduce the risk of infection will ultimately enhance patient outcomes
• A multi-disciplinary, team focused approach will be successful in preventing SSI 49

Antimicrobial Surgical Prophylaxis: A Pharmacology ReviewPaul Staffieri, PharmD
PGY2 Critical Care Pharmacy Resident
University of Illinois at Chicago
41st Annual ASPSN Convention
October 19th 2015