Embed Size (px)
Citation preview

Antimicrobial StewardshipIn-Person Safe Table
Thaddus D. Wilkerson, PharmD, BCPSDirector of Antimicrobial Stewardship ServicesCommunity and Health Systems ImprovementAlaska Native Tribal Health Consortium
November 8, 2017
Session Objectives
• Antimicrobial Stewardship Partnership for Patients• Overview of the basics• Collaborative resources
• Develop strategies for engaging stakeholders in antimicrobial stewardship• The nurses’ role in stewardship• The laboratory and microbiologist’s contribution to stewardship• Information technology – data-mining and clinical surveillance
• Provide evidence for the business case for antimicrobial stewardship• Review business plan tools for sustainability• Items to consider for program budget planning and tracking
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

AS: A Quality and Patient Safety Initiative
• Prescription of broad-based antimicrobials for too long, or when they are not indicated, can lead to an increase in complications and healthcare costs• Antibiotic resistance
• Adverse drug reactions
• Clostridium difficile infection• Antimicrobial Stewardship Programs (ASPs):
• A combination of personnel and procedures that promote the wise use of antibiotics, antifungals & antivirals.
• Right Diagnosis, Drug, Dose, Duration for the right patient at the right time
• Enhance patient outcomes and promote public health
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Resistance
• Getting an antibiotic increases a patient’s chance of becoming colonized or infected with a resistant organism.
• Antimicrobial resistance is associated with higher charges, length of stay, and death rates.
Pathogen and Antibiotic Exposure Increased Risk
Carbapenem Resistant Enterobactericeae and Carbapenems 15 fold
ESBL producing organisms and Cephalosporins 6- 29 fold
Patel G et al. Infect Control Hosp Epidemiol 2008;29:1099-1106Zaoutis TE et al. Pediatrics 2005;114:942-9
Talon D et al. Clin Microbiol Infect 2000;6:376-84Neidell M et al. CID 2012;55(6):807-15.
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

10 million people are projected to die annually from resistant infections by 2050.
317,000 deaths in North America
390,000 deathsin Europe
4.7 million deaths in Asia
4.2 million deaths in Africa
390,000 deaths in South America
22,000 deaths in Oceana
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

This translates to one person dying:
EVERYTHREE
SECONDS
Presented at WSHA/ASHNHA Partnership forPatients Safe Table – November 8, 2017

“The thoughtless person playing with penicillin
treatment is morally responsible
for the death of the man who succumbs to infection with the penicillin-resistant
organism.”Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Superbug in Alaska?
• Enterobacteriaceae = large family of GNRs found in the human gut flora• Carbapenems = broadest antibiotic class available• CREs = extremely difficult to treat; high mortality; weakened immune
systems and prolonged hospitalizations increase risk• Recurrent infections can occur• Unrecognized colonization = reservoirs for transmission for years• Carbapenemase genes can easily be transferred between bacteria!• 2015 1st Confirmed case of KPC-CRE in AK• 2016 11 cases have been reported to the State but none were
confirmed to carry the carbapenemase genePresented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Regional Variance in Resistance
2016 Alaska State and Regional Antibiogram can be found athttp://dhss.alaska.gov/dph/epi/id/siteassets/pages/hai/default/ak%202016%20antibiograms.pdf
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

The superbug issue has been called
“as big a risk as terrorism,” the BBC reports.
Think the war on terror is expensive?
Try the war on superbugs, that could easily cost
$100 trillion by 2050.
No Small Cost
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Health-care providers prescribed 842 antibiotic courses per 1,000 people
in the United States in 2011.
“About 50 percent of antibiotic use is either inappropriate or unnecessary in the U.S."
According to a report by the Centers for Disease Control
and Prevention
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Using Clinical Guidelines to Control Antibiotic Overuse
Wlodaver & Mary. Infect Dis Clin Pract 2012; 20(1):12-17 Spellberg. JAMA Intern Med 2016; 176(9).
-Antibiotic prescribing trends per care team/department-Point prevalence analysis to look for indications where antibiotics should be held-Address appropriate durations of therapy
The New Antibiotic Mantra
“Shorter is Better”
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
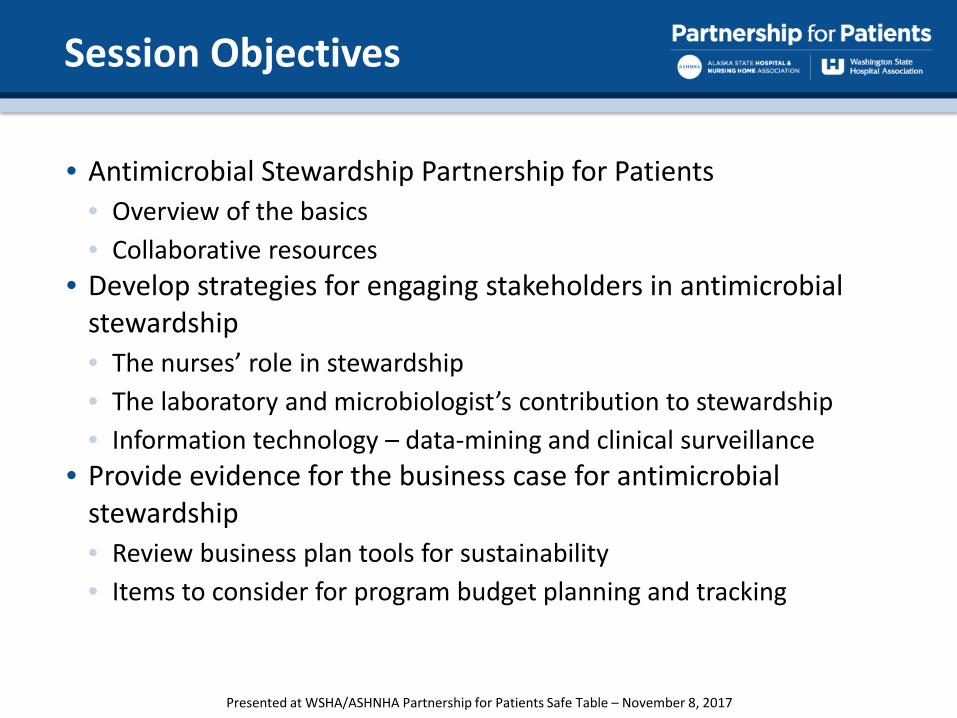
Numerator: Total days of therapy (DOT) of select antibiotics*
A Day of Therapy (DOT) will be defined as at least one dose of a selected antibiotic given on a calendar day to a patient in an inpatient unit (Med/Surg, ICU/Tele, PICU, NICU, OB). A patient on multiple antibiotics on the selected list would be counted for each separate antibiotic given each calendar day. For medications with 48-hour dosing intervals, a day of therapy will be documented only on a calendar day in which the antibiotic was administered (for e.g. levofloxacin).
Denominator: Patient days (total acute inpatient, observation and rehab days)
DATA DEFINITION: Antimicrobial Stewardship
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Overall Days of Therapy21% reduction from baseline
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

16
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
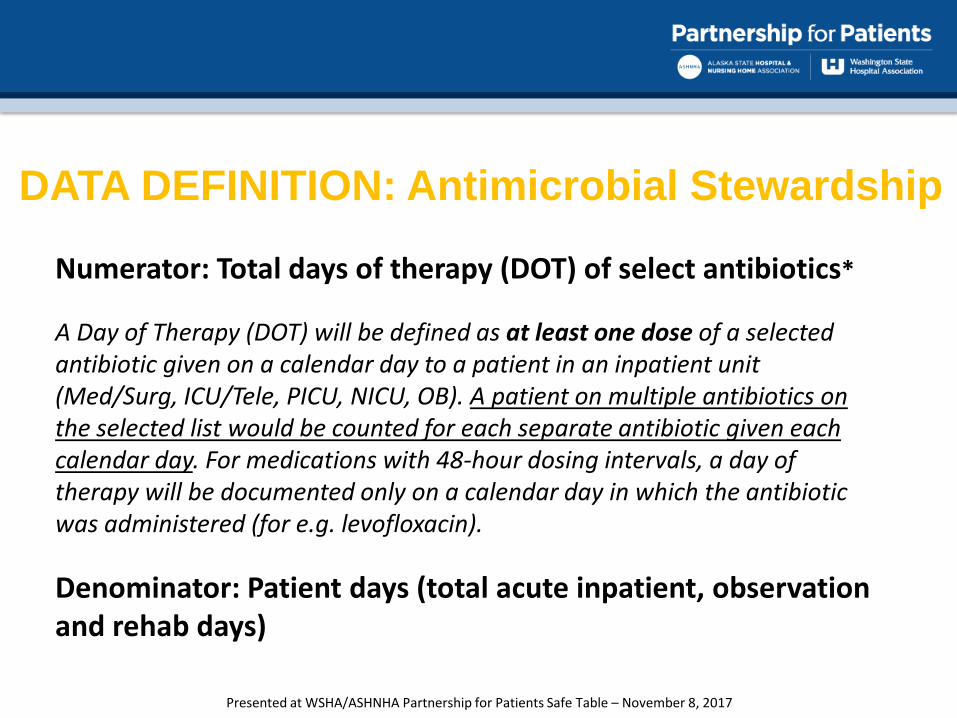
Carbapenems49% reduction from baseline
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
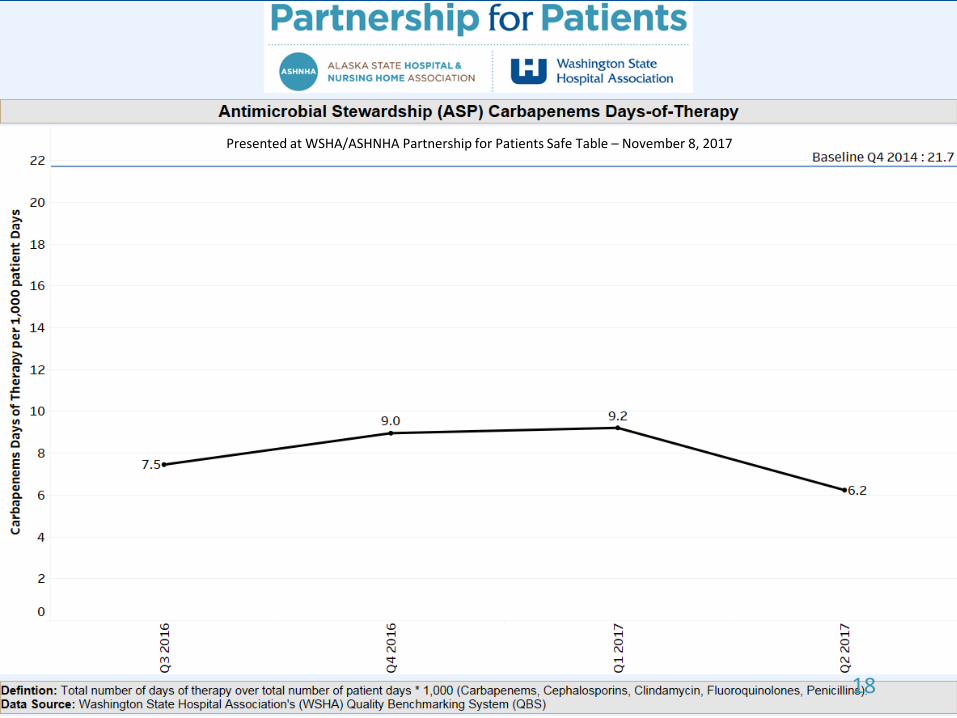
18
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Fluoroquinolones46% reduction from baseline
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
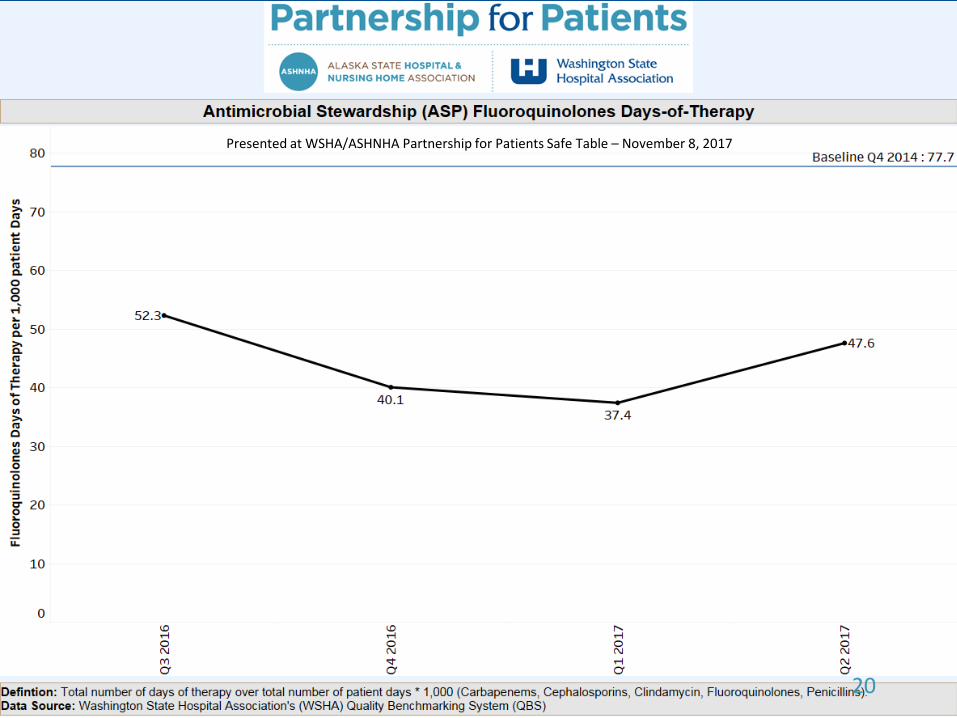
20
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Penicillins42% reduction from baseline
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

22
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Clindamycin32% reduction from baseline
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

24
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
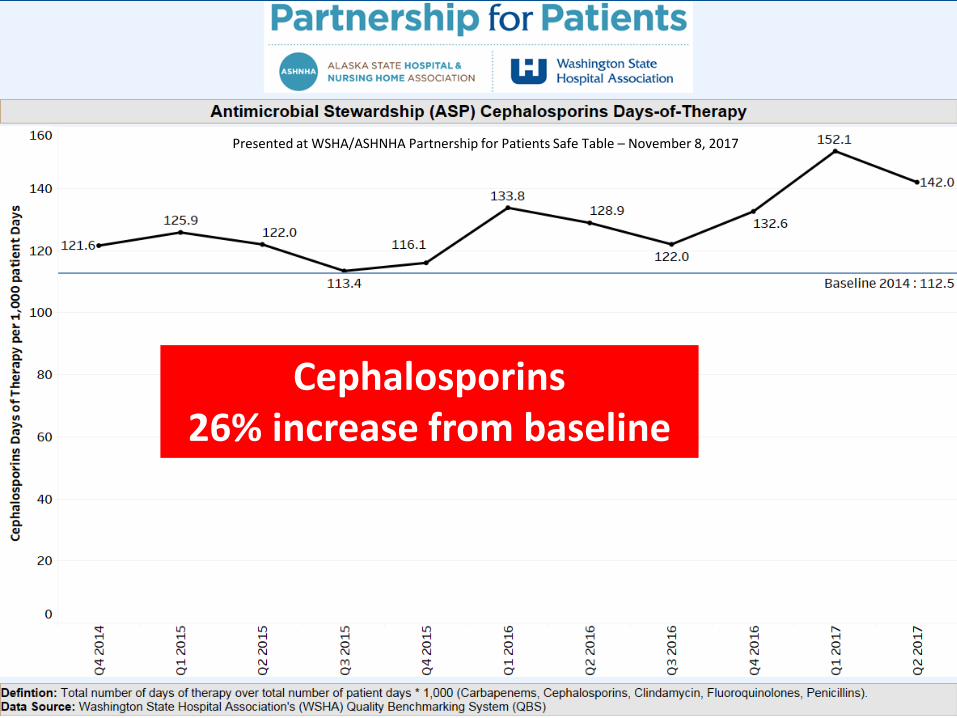
Cephalosporins26% increase from baseline
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

26
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
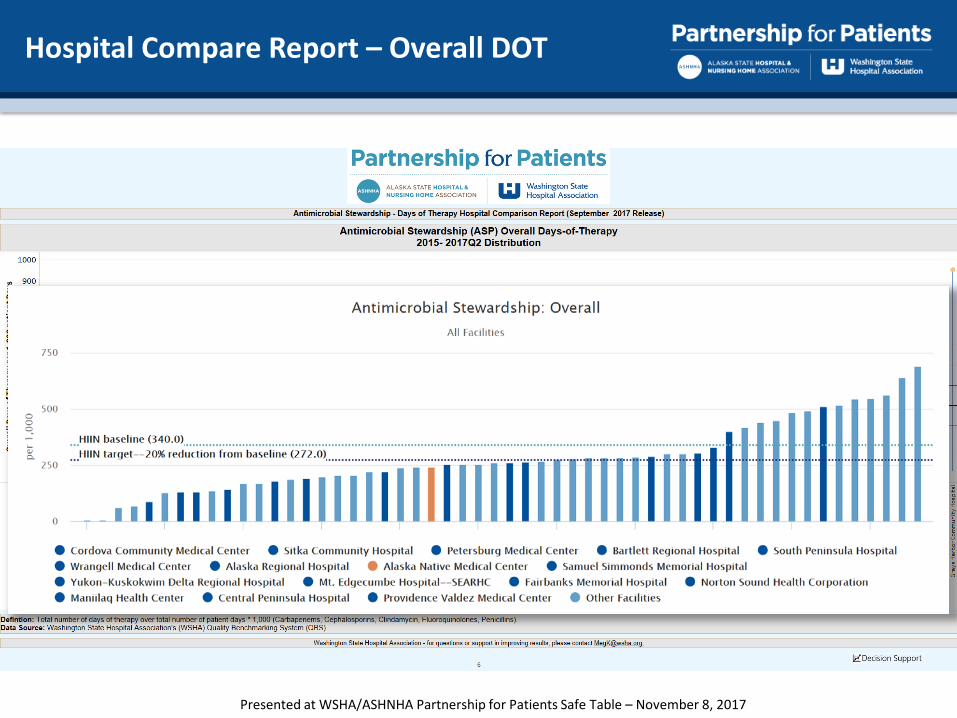
Hospital Compare Report – Overall DOT
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Q & A
This Photo by Unknown Author is licensed under CC BY-SA
WSHA Medication Safety Homepage: http://www.wsha.org/quality-safety/projects/medication/
Contact: [email protected]
Questions? Not submitting data?
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

CDC’s Core Elements on Implementing Antimicrobial Stewardship in Small and Critical Access Hospitals
The CDC has provided a framework for implementation strategies for the CDC Core Elements, specific to small hospitals. The strategies provide suggestions and examples for implementing the following elements of AMS:
1. Leadership Commitment2. Accountability3. Drug Expertise4. Action5. Tracking 6. Reporting7. Education
https://www.cdc.gov/getsmart/healthcare/implementation/core-elements-small-critical.htmlPresented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Elements of Performance:• Leaders establish antimicrobial stewardship as an organizational
priority.– Accountability documents – Budget plans – Infection prevention plans – Performance improvement plans – Strategic plans – Using the electronic health record to collect antimicrobial stewardship data
• Educate staff & licensed independent practitioners upon hire or granting of initial privileges & periodically thereafter
• Educate patients & families
https://www.jointcommission.org/assets/1/6/New_Antimicrobial_Stewardship_Standard.pdf
Joint Commission Medication Management Standard (MM.09.01.01)
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
• Antimicrobial Stewardship Team in place– Infectious disease physician– Infection preventionist– Pharmacist(s)– Practitioner– Part-time/consultant staff and/or telehealth staff are acceptable
members• Stewardship program implements CDC Core Elements• Program uses organization-approved protocols• Assessment of Appropriateness of Antibiotics• Collect, analyze & report data• Must take action on improvement opportunities identified
https://www.jointcommission.org/assets/1/6/New_Antimicrobial_Stewardship_Standard.pdf
Joint Commission Medication Management Standard (MM.09.01.01)
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Pres
ente
d at
WSH
A/AS
HNHA
Par
tner
ship
for P
atie
nts S
afe
Tabl
e –
Nov
embe
r 8, 2
017

WSHA Antimicrobial Stewardship Homepage
http://www.wsha.org/quality-safety/projects/medication/antimicrobial-stewardship/
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

• Success depends on
• Defined leadership• Coordinated multi-disciplinary approach
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Session Objectives
• Antimicrobial Stewardship Partnership for Patients• Overview of the basics• Collaborative resources
• Develop strategies for engaging stakeholders in antimicrobial stewardship• The nurses role in stewardship• The laboratory and microbiologist’s contribution to stewardship• Information technology – data-mining and clinical surveillance
• Provide evidence for the business case for antimicrobial stewardship• Review business plan tools for sustainability• Items to consider for program budget planning and tracking
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Stakeholders in AS
• Providers• Pharmacy• Infection
Prevention• Information
Technology• Laboratory• Nursing• Quality• Compliance• Administration• Community
JAM
A Pe
diat
r. 20
13;1
67(9
):859
-866
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Nurse Role in Antimicrobial Stewardship
ANA/CDC White Paper 2017 www.nursingworld.org

Nurse Role in Antimicrobial Stewardship
Recognize & Utilize Established Nursing Functions to Synergize with Optimal ASP
Goals & Outcomes
• Practical Education topics to Cover:• Antibiotic management by protocol vs. individual patient
choices• The role of clinical practice guidelines• The difference between infection versus colonization• The distinction between positive test results (eg, urine culture
& chest X-ray reports) and active disease• The difference between antibiotic adverse events and true
antibiotic allergies
Olans RN, Olans RD & A Demaria. CID 2016;62(1):84-9
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Nurse Role in Antimicrobial Stewardship
Recognize & Utilize Established Nursing Functions to Synergize with Optimal ASP
Goals & Outcomes
• Hoped-for results of such information:• Improved timing, collection & quality of microbiology
specimens• Prioritization of laboratory result communication• Enhanced antibiotic de-escalation linked to patient response• Improved patient and family education about antibiotics
Olans RN, Olans RD & A Demaria. CID 2016;62(1):84-9
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Nurse Role in Antimicrobial Stewardship
ANA White Paper: Redefining the AS Team
• Engage nursing on the Hospital level:• Provide AS education for bedside nurses• Include nurses in stewardship rounds• Participate in journal clubs• Develop specific content and messages for nurses as part of any
hospital effort to raise awareness about abx use & resistance• Encourage nurse antibiotic stewardship champions at the unit
level• Some facilities have added C.difficile infection to Magnet
Recognition Program criteria as a measure related to abx use.• Engage nursing in diagnostic stewardship
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Diagnostic Stewardship
• Definition in the GLASS Manual:• “coordinated guidance and interventions to improve
appropriate use of microbiological diagnostics to guide therapeutic decisions. It should promote appropriate, timely diagnostic testing, including specimen collection, and pathogen identification and accurate, timely reporting of results to guide patient treatment.”
• Main objective of microbiological diagnostic stewardship is to deliver:• Patient management guided by timely microbiological data to
deliver safer and more effective and efficient patient care• Accurate and representative AMR surveillance data to inform
treatment guidelines, and AMR control strategies
Used with permission from the WHO http://apps.who.int/iris/handle/10665/251553
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Diagnostic Stewardship
Used with permission from the WHO http://apps.who.int/iris/handle/10665/251553
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

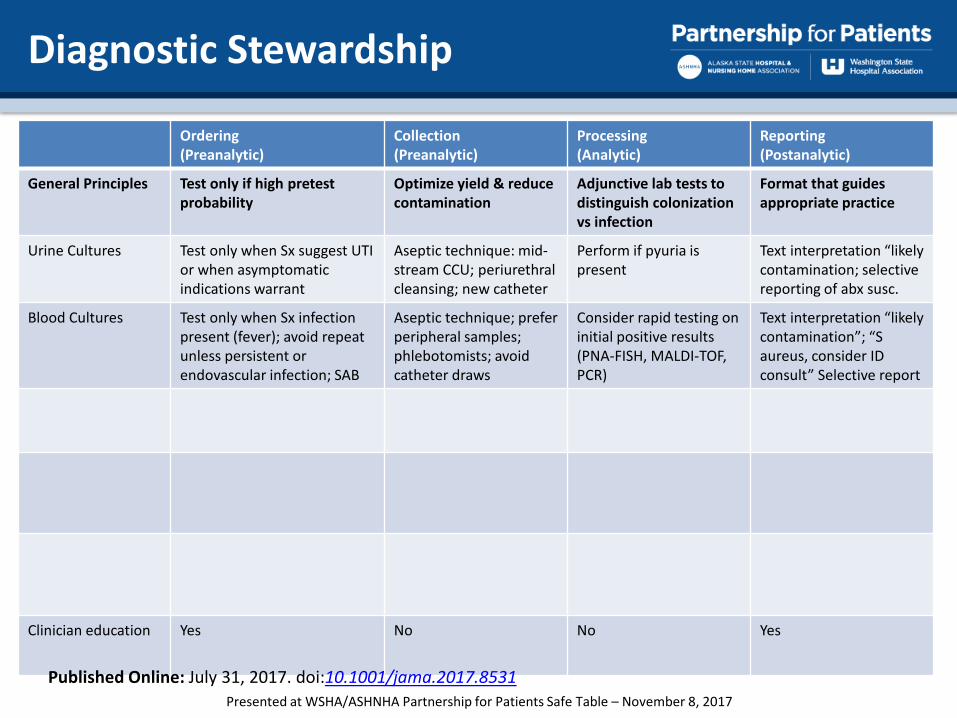
Diagnostic Stewardship
Ordering(Preanalytic)
Collection(Preanalytic)
Processing(Analytic)
Reporting(Postanalytic)
General Principles Test only if high pretest probability
Optimize yield & reduce contamination
Adjunctive lab tests to distinguish colonization vs infection
Format that guides appropriate practice
Clinician education Yes No No Yes
Published Online: July 31, 2017. doi:10.1001/jama.2017.8531Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Diagnostic Stewardship
Ordering(Preanalytic)
Collection(Preanalytic)
Processing(Analytic)
Reporting(Postanalytic)
General Principles Test only if high pretest probability
Optimize yield & reduce contamination
Adjunctive lab tests to distinguish colonization vs infection
Format that guides appropriate practice
Urine Cultures Test only when Sx suggest UTI or when asymptomatic indications warrant
Aseptic technique: mid-stream CCU; periurethralcleansing; new catheter
Perform if pyuria is present
Text interpretation “likely contamination; selective reporting of abx susc.
Clinician education Yes No No Yes
Published Online: July 31, 2017. doi:10.1001/jama.2017.8531Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
Diagnostic Stewardship
Ordering(Preanalytic)
Collection(Preanalytic)
Processing(Analytic)
Reporting(Postanalytic)
General Principles Test only if high pretest probability
Optimize yield & reduce contamination
Adjunctive lab tests to distinguish colonization vs infection
Format that guides appropriate practice
Urine Cultures Test only when Sx suggest UTI or when asymptomatic indications warrant
Aseptic technique: mid-stream CCU; periurethralcleansing; new catheter
Perform if pyuria is present
Text interpretation “likely contamination; selective reporting of abx susc.
Blood Cultures Test only when Sx infection present (fever); avoid repeat unless persistent or endovascular infection; SAB
Aseptic technique; prefer peripheral samples; phlebotomists; avoid catheter draws
Consider rapid testing on initial positive results(PNA-FISH, MALDI-TOF, PCR)
Text interpretation “likely contamination”; “Saureus, consider ID consult” Selective report
Clinician education Yes No No Yes
Published Online: July 31, 2017. doi:10.1001/jama.2017.8531Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Diagnostic Stewardship
Ordering(Preanalytic)
Collection(Preanalytic)
Processing(Analytic)
Reporting(Postanalytic)
General Principles Test only if high pretest probability
Optimize yield & reduce contamination
Adjunctive lab tests to distinguish colonization vs infection
Format that guides appropriate practice
Urine Cultures Test only when Sx suggest UTI or when asymptomatic indications warrant
Aseptic technique: mid-stream CCU; periurethralcleansing; new catheter
Perform if pyuria is present
Text interpretation “likely contamination; selective reporting of abx susc.
Blood Cultures Test only when Sx infection present (fever); avoid repeat unless persistent or endovascular infection; SAB
Aseptic technique; prefer peripheral samples; phlebotomists; avoid catheter draws
Consider rapid testing on initial positive results(PNA-FISH, MALDI-TOF, PCR)
Text interpretation “likely contamination”; “Saureus, consider ID consult” Selective report
C.difficile testing Test only when dx likely (>3loose stools/d, duration> 24h, no recent laxatives); no TOC
Only collect & send loose stool (conforms to the container)
Consider use of test algorithm that includes toxin immunoassay
Text interpretation “toxin-/PCR+ indicating possible colonization”
Clinician education Yes No No Yes
Published Online: July 31, 2017. doi:10.1001/jama.2017.8531Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Diagnostic Stewardship
Ordering(Preanalytic)
Collection(Preanalytic)
Processing(Analytic)
Reporting(Postanalytic)
General Principles Test only if high pretest probability
Optimize yield & reduce contamination
Adjunctive lab tests to distinguish colonization vs infection
Format that guides appropriate practice
Urine Cultures Test only when Sx suggest UTI or when asymptomatic indications warrant
Aseptic technique: mid-stream CCU; periurethralcleansing; new catheter
Perform if pyuria is present
Text interpretation “likely contamination; selective reporting of abx susc.
Blood Cultures Test only when Sx infection present (fever); avoid repeat unless persistent or endovascular infection; SAB
Aseptic technique; prefer peripheral samples; phlebotomists; avoid catheter draws
Consider rapid testing on initial positive results(PNA-FISH, MALDI-TOF, PCR)
Text interpretation “likely contamination”; “Saureus, consider ID consult” Selective report
C.difficile testing Test only when dx likely (>3loose stools/d, duration> 24h, no recent laxatives); no TOC
Only collect & send loose stool (conforms to the container)
Consider use of test algorithm that includes toxin immunoassay
Text interpretation “toxin-/PCR+ indicating possible colonization”
Molecular detection panels
Test only when pretest probability moderate to high & when results will influence management
Use recommended collection & transport conditions to reduce contamination
Stringent contamination prevention guidance in lab to avoid false +
Text interpretation results discussing colonization
Clinician education Yes No No Yes
Published Online: July 31, 2017. doi:10.1001/jama.2017.8531Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Diagnostic Stewardship
Ordering(Preanalytic)
Collection(Preanalytic)
Processing(Analytic)
Reporting(Postanalytic)
General Principles Test only if high pretest probability
Optimize yield & reduce contamination
Adjunctive lab tests to distinguish colonization vs infection
Format that guides appropriate practice
Urine Cultures Test only when Sx suggest UTI or when asymptomatic indications warrant
Aseptic technique: mid-stream CCU; periurethralcleansing; new catheter
Perform if pyuria is present
Text interpretation “likely contamination; selective reporting of abx susc.
Blood Cultures Test only when Sx infection present (fever); avoid repeat unless persistent or endovascular infection; SAB
Aseptic technique; prefer peripheral samples; phlebotomists; avoid catheter draws
Consider rapid testing on initial positive results(PNA-FISH, MALDI-TOF, PCR)
Text interpretation “likely contamination”; “Saureus, consider ID consult” Selective report
C.difficile testing Test only when dx likely (>3loose stools/d, duration> 24h, no recent laxatives); no TOC
Only collect & send loose stool (conforms to the container)
Consider use of test algorithm that includes toxin immunoassay
Text interpretation “toxin-/PCR+ indicating possible colonization”
Molecular detection panels
Test only when pretest probability moderate to high & when results will influence management
Use recommended collection & transport conditions to reduce contamination
Stringent contamination prevention guidance in lab to avoid false +
Text interpretation results discussing colonization
Forms of automation
Clinical decision support requiring documentation of Sx; hard stops for contraindications
Recording site & method of collection; orders requiring supp. Tests (ex, UA before culture)
Lab support systems performing cascade of tests
Prepopulated reports that can be reviewed & modified by lab personnel
Clinician education Yes No No Yes
Published Online: July 31, 2017. doi:10.1001/jama.2017.8531Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Diagnostic Stewardship
Appropriate Total Percent InapproriateCulture 187 288 65% 35%Abx 82 119 69% 31%
INDICATIONS FOR URINE CULTURE 1) Febrile children <2 years of age without another source 2) Fever PLUS symptoms referable to the urinary tract (flank pain, dysuria, hesitancy, and/or bladder pain) 3) Symptoms referable to the urinary tract PLUS presence of an indwelling urethral catheter, stent, nephrostomy tube or urinary diversion 4) Cystitis, if:
a) Failing 1st-line therapy b) Patient with recent antibiotic use c) Inability to use Keflex or nitrofurantoin first-line
5) Suspected prostatitis or epididymitis 6) Screening for asymptomatic bacteriuria in pregnant patients 7) Screening for asymptomatic bacteriuria prior to urological procedures with anticipated bleeding Please note, in the ABSENCE of UTI symptoms, urine cultures are NOT needed for the following groups:
• Diabetes • Advanced age • Presence of urinary catheters • Hospital admission • Prior to non-urological surgery • Turbid or malodorous urine • Fever due to non-urinary cause
Recommended reading: Avdic & Carroll. The Role of the Microbiology Laboratory in Antimicrobial Stewardship Programs. Infect Dis Clin N Am 28 (2014) 215-235.
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

March-May 2017
0
50
100
150
200
250
300
350
AFB PCR MTB CMPLX (DIRECT) BLOOD CULTURE ID-MULTIPLEX PCR
C. DIFFICILE DNA AMPLIFICATION INFLUENZA PCR (RAPID)
MENINGITIS/ENCEPHALITIS-MULTIPLEX PCR PCR RESPIRATORY PANEL
Rapid Diagnostics
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Rapid Diagnostics
• 89 Unique Patients
0
5
10
15
20
25
30
BCID Result Distribution
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
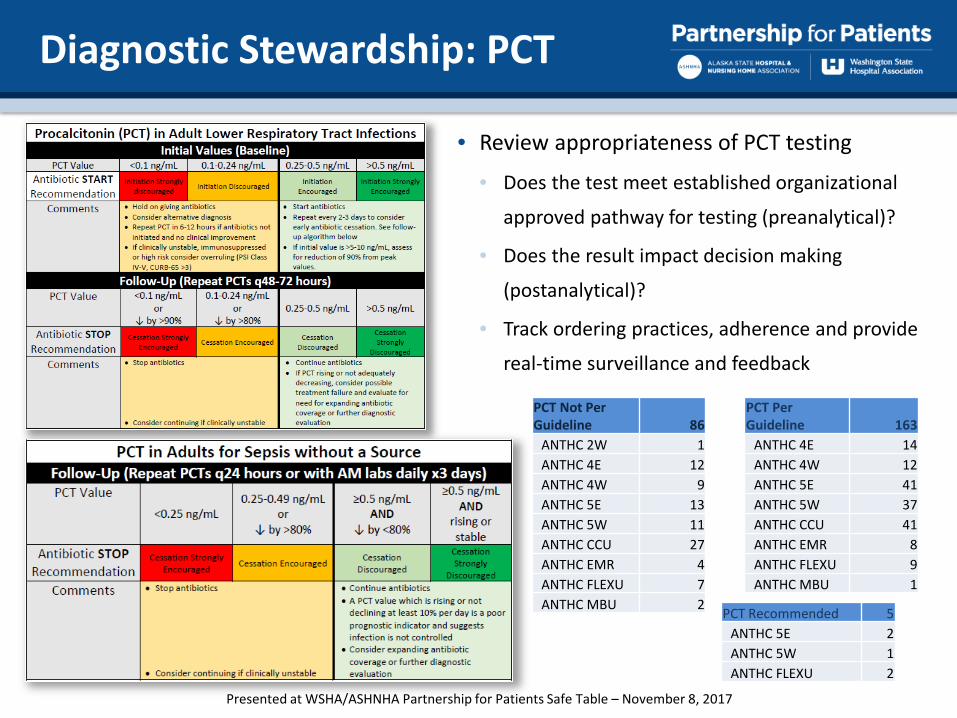
Diagnostic Stewardship: PCT
• Review appropriateness of PCT testing
• Does the test meet established organizational
approved pathway for testing (preanalytical)?
• Does the result impact decision making
(postanalytical)?
• Track ordering practices, adherence and provide
real-time surveillance and feedback
PCT Not Per Guideline 86
ANTHC 2W 1ANTHC 4E 12ANTHC 4W 9ANTHC 5E 13ANTHC 5W 11ANTHC CCU 27ANTHC EMR 4ANTHC FLEXU 7ANTHC MBU 2
PCT Per Guideline 163
ANTHC 4E 14ANTHC 4W 12ANTHC 5E 41ANTHC 5W 37ANTHC CCU 41ANTHC EMR 8ANTHC FLEXU 9ANTHC MBU 1
PCT Recommended 5ANTHC 5E 2ANTHC 5W 1ANTHC FLEXU 2
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Data-mining Clinical Surveillance
• Clinical surveillance systems can improve post analytical diagnostic stewardship by decreasing turnaround time to therapeutic decision making
• Data-mining can provide antibiotic utilization and micro/lab data for unit-based feedback, trending or highlighting areas for targeted intervention
Forrest et al. Use of EHR & CDSS for ASP. CID 2014:59(Suppl3)
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Session Objectives
• Antimicrobial Stewardship Partnership for Patients• Overview of the basics• Collaborative resources
• Develop strategies for engaging stakeholders in antimicrobial stewardship• The nurses role in stewardship• The laboratory and microbiologist’s contribution to stewardship• Information technology – data-mining and clinical surveillance
• Provide evidence for the business case for antimicrobial stewardship• Review business plan tools for sustainability• Items to consider for program budget planning and tracking
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

The Hospitalist Blog, AAP News
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Cost of Adverse Events
In 2008, there were 142,000 visits to emergency departments for adverse events attributed to antibiotics.
• Drug-drug interactions• Cardiac toxicity• Altered mental status• Acute renal failure• Acute hepatic failure• Superinfection
Incomplete recovery of the gut microbiome
Shehab N et al. Clinical Infectious Diseases 2008; 15:735-43Fouhy F et al. Antimicrob Agents Chemother 2012;56:5811.
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

57
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Dubberke & Olsen. Burden of Clostridium difficile on the Healthcare System. CID 2012;55(Suppl2)
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Cost Savings of Interventions & Activities
Clinical Category Intervention/Activity Cost Savings ($)Adverse Drug Event Major ADE prevention 6000
Minor ADE prevention 191-471Allergy prevention/clarification 396-1090Drug-drug interaction avoided 153-910Discontinued of contraindicated medication 785
General Practice Medication monitoring recommendation 0-228Drug therapy recommendation/change 62-153Discontinue of medication 50-98IV compatibility recommendation 153PK/PD consult 78Therapeutic dose adjustment 62-79IV to PO 21-516Medication reconciliation 153-398Discharge medication counseling 75-96Medical staff education 0-26Drug Information Consult 0-383Chart review 42Height/weight added to CPOE 153
ASP Abx consult 153Abx therapy adjustment 200Tx drug monitoring - AMG 200Tx drug monitoring - Vanc 153
Hamblin et al. J Trauma Acute Care Surg: 2012;73(6)Shepler. Am J Pharm Ed 2014;78(4)Wooley et al. Am J Pharm Ed: 2013;77(8)Campbell et al. Am J Pharm Ed 2011;75(1)
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Cost of Drugs
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

ASP Budget
• MD/PharmD FTE: $180,000 - $225,000
• Tertiary ID Consult Service: $12,000 - $24,000
• Nurse job expansion: $42,000
• Assistant job expansion: $20,000
• IT Professional support services: $20,000 - $75,000
• Training/Conference: $4550
• Certification: $750
• Dues/Subscriptions: $375
• Software/Licensing CDSS: $70,000 - $130,000
• Advertising: $500
• Food: $280
• Copy Center: $500
• Equipment: $3000
• Small critical access hospital: $88,590
• Large Hospital with 3rd Party CDSS: $353,585
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
Annual Report
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
Next Steps for ANMC ASP
• Investigate cost savings/avoided with interventions• Train and deploy liaison pharmacists, nurses and unit provider champions• Participate in the NHSN AUR submission for resistance tracking and
benchmarking unit-level abx’s• Formalize ambulatory and emergency department goals and strategic plan• Incorporate stewardship into job descriptions and performance reviews• Integrate data management systems• Engage nurse leadership in addressing antibiotic allergies• Provide direction for diagnostic stewardship• Collaborate with state, regional and national efforts
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

AHRQ: Recruitment of Acute Care Hospitals Interested in AHRQ Antibiotic Stewardship Project
• Recruiting acute care hospitals, or individual units within hospitals, for participation in a 12-month project beginning December 2017.
• Free program that incorporates both technical and behavioral components to improve antibiotic prescribing. Will support hospitals’ efforts to improve antibiotic use and reduce associated harms while safeguarding antibiotics’ effectiveness for future generations and help participating organizations meet The Joint Commission’s new AMS Standard.
• Hospitals taking part in this effort will receive antibiotic-use guidelines for several infectious disease syndromes, expert coaching, online education, improvement tools, patient education materials, and other resources to help run an effective antibiotic stewardship program.
• For details, email [email protected].
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
This presentation is intended for educational use only, and does not in any way constitute medical consultation or advice related to any specific patient.
Tele-Antimicrobial Stewardship: The ECHO Model
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

“The baseline assessment looks like a lot of work.”
“We just lost our only ICP. There is no PharmD. We have no one.”
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Vision Support WA hospitals with ASP
implementation or refinement High-quality ID fellow training Financially self-sustaining Partnerships with WSHA & WA-DOH
Marisa D’Angeli, MD, MPH
Inception Summer 2016
UW ApprovalFall 2016
“Go Live”Jan 2017
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Hospital Stewardship Program Teams
Infection Prevention Pharmacy
Physicians Microbiology
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Project ECHO: How it works
69
10-15 min didactic De-identified cases sent
in advance Rural clinicians present
cases to specialist panel Multi-specialty
co-management “Learning Loops”
Pres
ente
d at
WSH
A/AS
HNHA
Par
tner
ship
for P
atie
nts S
afe
Tabl
e –
Nov
embe
r 8, 2
017

Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Week 1 Making Tele-Stewardship Work for Your HospitalWeek 2 Metrics - Processes and OutcomesWeek 3 The Big Goal of Stewardship - Changing Behaviors Week 4 The Key Actions and Activities of the AS Pharmacist Week 5 Low Hanging Fruit in Antimicrobial Stewardship Week 6 The Clinical Microbiology Lab in AS Week 7 Double-Coverage for Anaerobes: Where's the Data? Week 8 Markers of Infection: ESR, CRP and Procalcitonin Week 9 Empiric Antimicrobial Therapy Week 10 Sepsis, Part 1Week 11 Sepsis, Part 2Week 12 P&T : Good, Bad, Ugly?
CURRICULUM
Goals Actionable Adaptable Snappy
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

www.uwtasp.orgPresented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

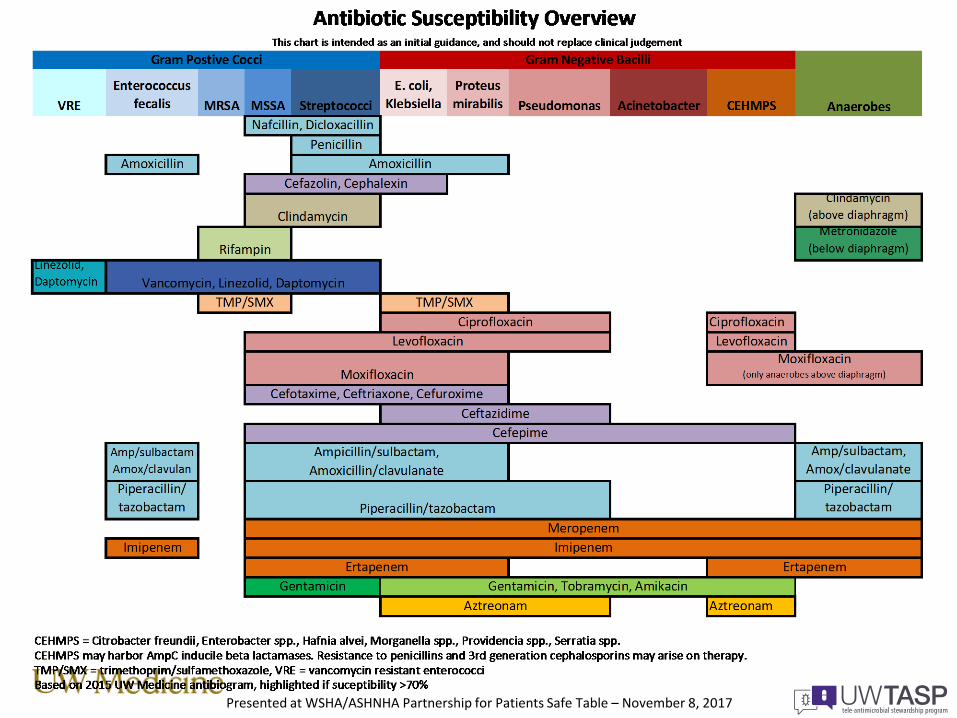
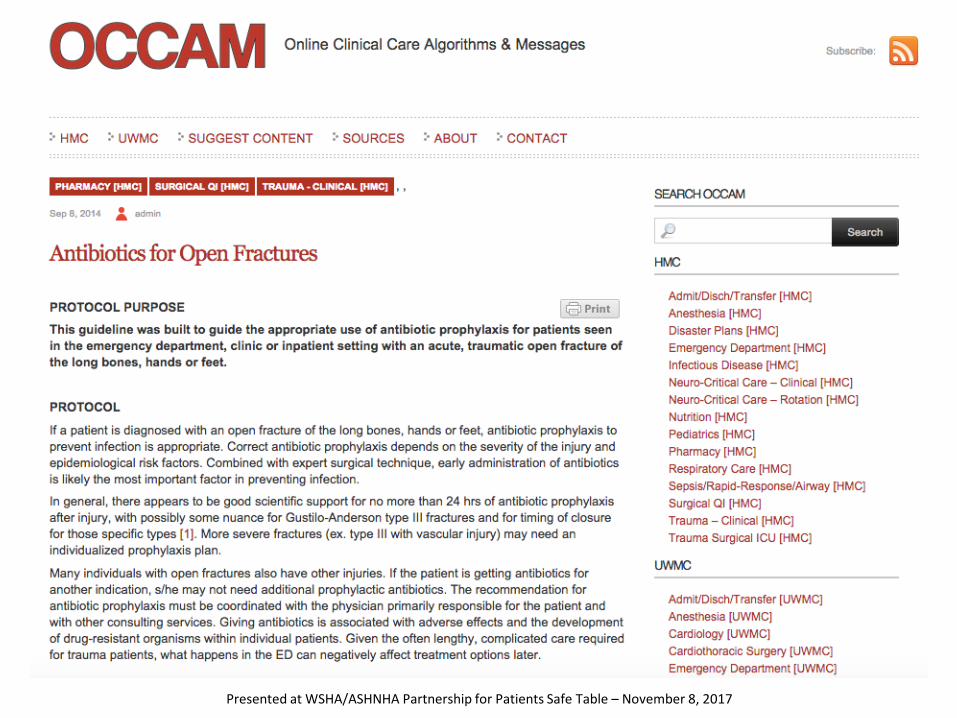
Resource Sharing: Empiric Abx Guidelines
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017
UW TASP – Shared Expertise
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Challenges
• “We have no pharmacist. At all.”
• “If we have to pay for this, what will we give up?”
• Silence….
Opportunities
• “We can advocate for change.”
• “UW, CDC and WA-DOH want to help.”
• Patience, empathy, outreach (peer-to-peer)
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Vision: Coming Year
• Expand to include all critical access hospitals• Work with non-CAH ACHs in WA• Work with other WWAMI states (Alaska!)• Partner with skilled nursing & long term care
facilities
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

Natalia Martínez Paz, MA, MPATASP ECHO Program Manager
John Lynch, MD, MPHMedical Director
Paul Pottinger, MDCo-Founder
Zahra Escobar, PharmD
Rupali Jain, PharmD
Marisa D’Angeli, MD, MPHWashington DOH
John Scott, MD, MScDirector of Telehealth
Rob Cybulski, PhDMicro Fellow
Laura Quilter, MDID Fellow
Erica Stohs, MD, MPHID Fellow
Chloe Bryson-Cahn, MDID Fellow
Ted Wright, MDID Fellow
Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

WHAT CAN YOU DO?
• Ask your doctor if you REALLY need antibiotics the next time you are prescribed them…
• If so, please take them as directed…
• Ask us how you can support UW-TASP
Reminder! U.S. Antibiotic Awareness Week is November 13-19, 2017
https://www.cdc.gov/antibiotic-use/week/index.html
THANK YOU!Presented at WSHA/ASHNHA Partnership for Patients Safe Table – November 8, 2017

"The analyses upon which this publication is based were performed under Contract Number HHSM-500-2016-00077C entitled, "Hospital Improvement
Innovation Network," sponsored by the Centers for Medicare & Medicaid Services, Department of Health and Human Services."