Embed Size (px)
Citation preview

Anticoagulation and Antiplatelets in Coronary Angioplasty
Patients with High Hemorrhagic Risk- Indications and evidence for a tailored
treatment
Alexandra Lansky, MD
Yale University School of Medicine
University College of London

• Antiplatelet drugs
• Cox-1 inhibitors
• P2Y12 inhibitors
• Glycoprotein Inhibitors
• Oral Anticoagulants
• Vit K Antagonists
• Factor Xa inhibitors
• Antithrombins
• Indirect thrombin Inhibitors (Heparin, LMWH)
• Direct Thrombin Inhibitors (Bivalirudin)
Anticoagulation and Antiplatelets in
Coronary Angioplasty

High Hemorrhagic Risk
Clinical Senarios to Discuss
The Patient requiring anticoagulation
The Patient who bleeds
The Patient who needs surgery
What Stent?
What Drug?
How Long?

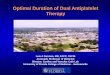
Impact of BARC type 3-5 Bleeding
on 1 Year Mortality
Prognosis of Bleeding after Stent
Implantation
P<0.001
Ndrepepa G et al. Circulation 2012

High Hemorrhagic Risk
Clinical Senarios to Discuss
Procedural anticoagulation Consideration

Bivalirudin vs Heparin + GPI in ACS
STEMI
AHA/ACC 2012 GPG
In Patients with STEMI Bivalirudin is the preferred
IV anticoagulant agent
NSTEMI
AHA/ACC 2012 GPG
In Patients with NSTEMI Bivalirudin OR Heparin
* GPI with high risk features not adequately treated with
P2Y12 (Class I a); adequately pretreated (Class IIb)
B

EUROMAX BRIGHT HEAT PPCI
N Center 65 82 1
N patients 2,198 2,194 1,812
- Bivalirudin 1,089 735 905
- Heparin 460 729 907
- Heparin + GPI 649 730 --
- Heparin bolus 60 IU/kg 100 IU/kg 70 IU/kg
- Bival Infusion 4.5 hrs 4.0 hrs No
- GPI Bail out 7.9% vs 25% 4.4% vs 5.6% 13.5% vs 15.5%
- New P2Y12 59% 0 89%
- Radial 47% 79% 81%
Current Controversies
Bivalirudin vs Heparin in STEMI
Recent Studies (6,200 pts)

Sabatine M. The Lancet 2014
Metananalysis:Bivalirudin vs Heparin
MACE

Sabatine M. The Lancet 2014
Metananalysis:Bivalirudin vs Heparin
Ischemic Events

GPI mainly in Heparin Arm
Provisional GPI in both Arm
Planned GPI in both Arm
Metananalysis:Bivalirudin vs Heparin
Bleeding and GPI Utilization

Increasing Bleeding According to
GPI Utilization L
og
od
ds
ra
tio
Favors
Heparin
Favors
Bivalirudin P:0.02
Presented at TCT September 2014

ESC 2014 Guidelines

High Hemorrhagic Risk
Clinical Senarios to Discuss
The Patient requiring anticoagulation

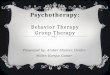
Incidence of Bleeding in Relation to Antithrombotic Therapy
Sørensen R et al. Lancet 2009;374:1967-74
40,812 patients with MI between 2005-2008
Yearl
y i
ncid
en
ce (
%)
Single
Therapy
Dual
Therapy
Triple
Therapy

0.0
0.0
20
.04
0.0
60
.08
0.1
0
0.0 0.5 1.0 1.5
OAC
Clopidogrel+ASA
ACTIVE W: OAC vs ASA+ Clopidogrel
6706 Pts with Afib at risk of Stroke C
um
ula
tive H
aza
rd R
ate
s
Years
3.93 %/year
5.64 %/year RR = 1.45
P = 0.0002
Lancet 2006 Jun 10;367(9526):1903-12.
Stroke, Non-CNS Systemic Embolism, MI & Vascular Death

Is OAC needed? Stroke Risk in Afib: CHADS-VASc Score > 2

Predicting Bleeding after Stent Implantation
HAS-BLED Score > 2

Management of Antithrombotic Therapy in Afib Patients
with ACS or Undergoing PCI: ESC
ESC WG Thrombosis Consensus Document: Lip G et al. Eur Heart J 2010;31:1311-18
Hemorrhagic
Risk Clinical Setting Stent Type Recommendation
Low
or
Intermediate
Elective BMS 1 month: ASA, Clop, OAC
Lifelong: OAC alone
Elective DES
3 months: ASA, Clop, OAC
3-12 months: Clop, OAC
Lifelong: OAC alone
ACS BMS/DES
6 months: ASA, Clop, OAC
6-12 months: OAC, ASA or Clop
Lifelong: OAC alone
High
Elective BMS 2-4 weeks: ASA, Clop, OAC
Lifelong: OAC alone
ACS BMS
4 weeks: ASA, Clop, OAC
1-12 months: OAC, ASA or Clop
Lifelong: OAC alone

Consensus Document: Antithrombotic Therapy In Patients With Atrial Fibrillation Undergoing Coronary Stenting
A North-American Perspective
Faxon D et al. Thromb Haemost 2011; 106: 571–584
High risk ST and low bleeding risk
Low risk ST and low bleeding risk
Any risk ST and high bleeding risk
BMS - Triple Rx for at least 1 mo then OAC+ single
AP for 12 mo
DES - Triple Rx for at least 6 mo then OAC+ single
AP for 12 mo
After 12 mo OAC indefinitely
BMS - Triple Rx for at least 1 mo then OAC+ single
AP for 12 mo
DES - not recommended
BMS - Triple Rx for at least 6 mo then OAC+ single
AP for 12 mo
DES - Triple Rx for 12 mo
Atrial fibrillation and a coronary stent with moderate/high stroke risk (CHADS2>1)

High Hemorrhagic Risk
Clinical Scenarios to Discuss
The Patient who bleeds

A 67-year-old Woman Admitted with melanotic stool
Risk factors: hypertension, dyslipidemia, chronic atrial fibrillation, and smoking, prior TIA
No history of bleeding diathesis
HPI:
- 4 weeks ago was hospitalized for STEMI, was treated with primary PCI to Prox LAD using drug-eluting stent, LVEF 40%
- Meds at discharge: ASA 325 mg/d qd, coumadin 5.0 mg alter with 2.5 mg /day, Clopidogrel 75 mg/d qd, Carvedilol 12.5 mg bid, Lisinopril 40 mg qd, rosuvastatin 20 mg qd
CHADsVAS= 4

Physical Findings
• BP 96/68 mm Hg;
• HR 110/min, irregular;
• RR 18/min, Sat – 96%
• Cardiac exam: normal S1, S2,
no murmurs or rubs
• Clear lungs
• Abdomen: soft, mild
tenderness in epigastrium,
normal bowel sounds
• Labs: Hgb – 9.2 g/dL (12.8
g/dL 1 months ago), Hct –
26%
Management
• 0.9% Sodium Chloride IV
• Blood type was defined
• Omeprazole IV was
started: 80 mg bolus
followed by 8 mg/hr
infusion
• Gastroenterologist was
called, and urgent
endoscopy was
performed

Endoscopy: a bleeding duodenal ulcer with
adherent clot
• Endoscopic treatment: epinephrine injection plus thermocoagulation to the point of vessel obliteration
• Campylobacter pylori (+)

Rockall Scoring System for Predicting Re-bleeding and Mortality Based on Endoscopic and Clinical Variables
Score
Age
<60 0
60-79 1
>79 2
Shock
None 0
tachycardia 1
Hypotension 2
Comorbidity
None 0
CAD, CHF, other major comorbidity 1
Renal failure, liver failure, malignancy 2
Diagnosis
Mallory Weiss tear or no lesion observed 0
All other diagnosis 1
Malignant lesion 2
Stigmas of recent hemorrhage
None or spot in ulcer base 0
Blood in the GI tract, clot, visible vessel in ulcer base
2
Rockhall TA et al: Lancet 1996:347: 1138-1140

Rockall Scoring and Prognosis after Upper GIB
Score Re-bleeding % Mortality %
1 3% 0%
2 5% 0%
3 12% 2%
4 13% 4%
5 17% 8%
6 30% 15%
7 40% 20%
8 48% 39%
Rockhall TA et al: Lancet 1996:347: 1138-1140

Post Endoscopy
Omeprazole infusion 8 mg/hr for 72 hrs, followed
by Omeprazole 20 mg qd
ASA discontinued, coumadin held
Clopidogrel 75 mg qd continued
Clarithromycin 500 mg bid and amoxicillin 1 g bid
for 2 weeks
No signs of continuing GIB for 2 weeks
Repeated EGDS: healing duodenal ulcer
coumadin restarted 2.5 mg/day
F/U: uneventful at 1 year

High Hemorrhagic Risk
Clinical Scenarios to Discuss
The Patient who needs surgery

Bleeding Risk in Various Surgeries
Bleeding Risk Clinical Severity Type of Surgery
Low • Transfusions
rare
• Peripheral: plastic/general, biopsies
• Minor orthopedic, ENT general
• Endoscopy
• Eye: anterior chamber
• Dental
Intermediate
• Transfusions may be frequent
• More re-op, LOS
• Visceral
• Cardiovascular surgery
• Major orthopedic, ENT
• Urologic reconstructive
High • Bleeding into a
closed space
• Intracranial
• Spinal
• Eye: posterior chamber
Adapted from Abualsaud and Eisenberg, JACC: CV Intv 2010

Late Surgery Group
(Beyond 3 months)
Early Surgery Group
(3 months)
3/34 8.9%
2 Deaths 1 MI
1/159 0.6% 1 MI
SENS Registry
p<0.001
Patients treated with ZES Undergoing Surgery and Discontinuing DAPT within 1 Year
Kim JW et al, ACC 2009

Patients undergoing PCI:
Treatment interruption

Strategies for Upcoming Surgery
• If at all possible, delay surgery!
Ideally 6 weeks for BMS*
• Less only if necessary
Ideally 6 months to 1 yr for DES*
• Likely 3-6 months with 2nd gen DES
• If surgery is needed and bleeding risk
low, continue DAPT through surgery