-
8/10/2019 Anticoagulants and HIT
1/27
Anticoagulants and HIT
-
8/10/2019 Anticoagulants and HIT
2/27
Heparin-induced thrombocytopenia
Type II or delayed type (HIT): occurs in 0.3-3% of patients
exposed to heparin for more than 4
days. It is an immune-mediated disorder It is associated with
thrombosis
This is a serious disorder.Type I or early type: occurs in
10-20% of patients within the first 2 days after heparin
initiation It is non-immune disorder due to a direct effect of
heparin on
platelet activation. Lesser fall in platelet count that often
returns to normal with
continued heparin administration.This type is of no clinical
significance.
-
8/10/2019 Anticoagulants and HIT
3/27
Platelets aggregation
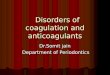
Pathophysiology of HIT
IgG
PF4
HeparinHeparin-PF4-IgG
complexHeparin-PF4complex
Fc -RIIAreceptors
Platelet activationand release
-
8/10/2019 Anticoagulants and HIT
4/27
Clinical picture
Onset:
Typical:4-10 days after the initiation of therapy
Unusual:after two weeks
Earlier:as early as 10 hoursHeparin in the previous 3-4 months
(persistent
antibodies in 30%)
Delayed:after heparin has been withdrawn
High antibodies titer that exhibit heparin-independentplatelet
activation
-
8/10/2019 Anticoagulants and HIT
5/27
Amount & route of heparin administration:
Most:IV or SC prophylactic dose
Occasionally:very small amount e.g.
after exposure to 250 U from a heparin flush after the use of
heparin-coated catheters
-
8/10/2019 Anticoagulants and HIT
6/27
Manifestations:
Thrombocytopenia:
Rarely severe (pl count > 20,000/L)
Spontaneous bleeding is unusual
50% subsequent 30-day risk of thrombosis
-
8/10/2019 Anticoagulants and HIT
7/27
Thrombosis:
50% of patients present with a thrombotic event
Most common (80%): venous thrombosis
75% DVT
25% pulmonary embolism
Less common (20%): arterial thrombosis
Stroke
MI
Limb ischemia
Warfarin-induced venous limb gangrene
-
8/10/2019 Anticoagulants and HIT
8/27
Thrombosis:
Skin lesions associated with HIT antibodies, even in theabsence
of thrombocytopenia
Cerebral sinus thrombosis: Fever, chills, flushing, ortransient
global amnesia beginning 5 to 30 minutesafter an IV heparin
bolus
Adrenal hemorrhage (caused by adrenal veinthrombosis)
HIT-associated mortality is high (about 18%)
-
8/10/2019 Anticoagulants and HIT
9/27
Diagnostic testing:
1. The diagnosis is initially made on clinicalgrounds
The assays with the highest sensitivity & specificitymay not
be readily available and have a slowturnaround time.
2. The most specific diagnostic tests:
1. Serotonin release assays.2. Heparin-induced platelet
aggregation assays.
3. Solid phase immunoassays.
-
8/10/2019 Anticoagulants and HIT
10/27
Prevention
Judicious use of UFH: limiting duration to < 5 days &
early warfarin starting
substitution with LMH
Recognize that:
LMH should not be substituted for UFH after HIT develops:Igs
once synthesized can cross react with LMH. In addition LMH
may induce heparin-dependent IgG antibody formation
Warfarin should not be given to patients who have HIT untilthe
thrombocytopenia resolves
Warfarin -without other anticoagulants- increases the risk
ofvenous limb gangrene
-
8/10/2019 Anticoagulants and HIT
11/27
Treatment
Immediate cessation of all exposure to heparins
However, heparin cessation is often not sufficient,since these
patients remain at risk for thrombosis.
Give an alternative anticoagulant: Direct thrombin inhibitor
Lepirudin (recombinant hirudin) & Bivalirudin
Argatroban Selective factor X inhibitors
Danaparoid
Fondaparinux
-
8/10/2019 Anticoagulants and HIT
12/27
How a thrombus is formed?
Platelet
TF
VIIa
X Xa
Proth
Th
1. Initiation(Thrombin is generated)
-
8/10/2019 Anticoagulants and HIT
13/27
2. Amplification(Further thrombin is generated)
XIXIa XXa
Th Proth
IXIXa
VVa
VIIIVIIIa
Prothrombinase
-
8/10/2019 Anticoagulants and HIT
14/27
3. Propagation(Fibrin is deposited)
Fibrinogen
Fibrin
Th
THROMBIN is the key enzyme in the clotting cascade
Factor X comes next
-
8/10/2019 Anticoagulants and HIT
15/27
ThrombinAntithrombin
Active site
Reactive center
ThrombinAntithrombin
Anticoagulants targeting thrombin(Thrombin inhibitors)
XaAntithrombin
-
8/10/2019 Anticoagulants and HIT
16/27
a. Indirect thrombin inhibitorsUnfractionated Heparin UFH
Thrombin
Exosite II
Antithrombin
Heparin binding site
The amino
terminus
Heparin
Exosite I
-
8/10/2019 Anticoagulants and HIT
17/27
b. Direct thrombin inhibitors
Thrombin
Exosite I
Exosite II
Bivalent:Hirudin, Lepirudin, BivalirudinUnivalent:Argatroban
& Ximelagatran
-
8/10/2019 Anticoagulants and HIT
18/27
Lepirudin (Refludan)65 amino acids peptide
([Leu1, Thr2]-63-desulfohirudin )
Antihirudin antibodiesin 45% of cases daily monitoring ofAPTT
and dose should be reduced accordingly.
Cautious in patients with renal insufficiency
-
8/10/2019 Anticoagulants and HIT
19/27
Bivalrudin (Angiomax)Hemodialyzable hirudin analog; 20 amino
acid peptide
-
8/10/2019 Anticoagulants and HIT
20/27
Argatroban (Argatroban)
Lower starting dosage in patients with hepatic dysfunction.
-
8/10/2019 Anticoagulants and HIT
21/27
Ximelagatran (Exanta)
-
8/10/2019 Anticoagulants and HIT
22/27
Anticoagulants targeting active factor X(Selective Factor Xa
inhibitors)
Thrombin
Exosite II
Exosite I
Antithrombin
LMH
XaAntithrombin
LMH
Antifactor Xa to antithrombin activity ratio is 3:1
1. Low molecular weight heparins LMH
-
8/10/2019 Anticoagulants and HIT
23/27
Low Molecular Weight HeparinsGenericname
Tradename
Manufacturer
Enoxaparin LovenoxClexane
Rhone
Poulenc Rorer, Collegeville, PAAventis
Dalteparin Fragmin PharmaciaUpjohn, Kalamazoo, MI
Ardeparin Normiflo WyethAyerst, Philadelphia, PA
Tinzaparin Innohep Novo Nordisk, Princeton, NJ
Nadroparin Fraxiparine SanofiWinthrop, New York, NY
Certoparin Sandoparin Sandoz Pharmaceuticals, East Hanover,
NJ
Reviparin Clivarin Knoll, Parsippany, NJ
Parnaparin Fluxum Opocrin, Italy
-
8/10/2019 Anticoagulants and HIT
24/27
2. Heparinoid 3. Synthetic heparinpentasaccharides
XaAntithrombin
Fondaparinux
No antithrombin activityAntifactor Xa to antithrombin
activity ratio is 28:1
Danaparoid It is derived from porcine
intestinal mucosa (MWt: 1,000-10,000 daltons):
The inactivation of factor Xa ismediated by ATwhile inactivation
of thrombin ismediated by both AT and HC II.
-
8/10/2019 Anticoagulants and HIT
25/27
Danaparoid (Danaparoid)
84% heparin sulfate
12% dermatan sulfate
4% chondroitin sulfate
Although it is not FDA-approved for HIT, there is extensive
experience using thisagent in patients with HIT
10 % cross-reactivity between danaparoid and the HIT antibody
(in vitro)
Persistence or recurrence of thrombocytopenia without thrombosis
in 6.5% of
HIT patients switched to danaparoid
-
8/10/2019 Anticoagulants and HIT
26/27
Fondaparinux (Arixtra)
Blood, 1 January 2005, Vol. 105, No. 1, pp. 139-144.Effect of
fondaparinux on platelet activation in the presence of heparin-
dependent antibodies: a blinded comparative multicenter study
withunfractionated heparin
Fondaparinux is nonreactive to HIT sera which raises the
possibility that thedrug may be used for prophylaxis and treatment
of thrombosis in patients
with a history of HIT
-
8/10/2019 Anticoagulants and HIT
27/27
Re-exposure to heparin
Three facts make re-exposure to heparin possible:
1. Disappearance of the antibodies usually occurs 50-85days
after cessation of heparin treatment.
2. Secondary immune response should not occur until at
least 3 days after exposure.3. Heparin is rapidly cleared (even
if antibodies appeared,
they would not be thrombogenic in the absence ofheparin).
Short-term re-exposure to heparin (e.g. cardiopulmonarybypass)
may be safe if:
HIT antibodies are no longer detectable
Heparin is restricted to the operative procedure