Embed Size (px)
Citation preview

AR
Isccmmo
tcptpcsormp
a
b
A
2
nticancer Agents and Cardiotoxicityaymond Ng,a Nathan Better,b and Michael D. Greena
Although rare, cardiotoxicity is a significant complication of cancer treatment. The inci-dence and severity of cardiotoxicity are dependent on the type of drugs used, dose andschedule employed, and age of patients, as well as the presence of coexisting cardiacdiseases and previous mediastinal irradiation. Anthracyclines are among one of the mostactive agents in oncology, but their use is often hampered by their cumulative dose-limitingcardiotoxicity. Combination therapy with new drugs in the last decade, such as taxanes andtrastuzumab, in the treatment of metastatic breast cancer has yielded impressive resultsbut also unexpected cardiotoxicity. Existing methods of minimizing cardiotoxicity includethe use of protective agents such as dexrazoxane, different preparations of anthracyclinessuch as liposomal formulations, and alternative scheduling techniques. Assessment of leftventricular ejection fraction (LVEF) with two-dimensional (2D)-echocardiography or radio-nuclide ventriculography (RNVG) remains the most pragmatic means of monitoring forcardiotoxicity. The increasing number of long-term survivors of pediatric cancers, as well asthe use of trastuzumab, taxanes, and anthracyclines in adjuvant treatment of breast cancer,means that more than ever, cardiotoxicity will remain an important issue for clinicians.Semin Oncol 33:2-14 © 2006 Elsevier Inc. All rights reserved.
uc
ofdtchtv
itfc
ATamdagct
n 2001 the two leading causes of death in the United Stateswere diseases of the heart and malignant neoplasms, re-
pectively.1 Indeed, for those aged 65 and over, these twoontribute to more than half of the mortality. With an in-reasingly aging population, clinicians now need to be evenore cognizant of the fact that patients with cancer are everore likely to have other comorbidities, in particular diseases
f the cardiovascular system.Cardiotoxicity is a rare but serious complication of cancer
reatment and affects patients in many different ways. In theontext of this review, cardiotoxicity will be defined as im-airment of the cardiac muscles as a result of anticancerherapy. To this extent, drugs that have been previously re-orted to have electrophysiologic or vascular effects on theardiac system or drugs with low incidence of cardiotoxicity,uch as 5-fluorouracil, mitomycin, cyclophosphamide, andther alkaloids, will not be discussed in detail. Similarly, thiseview will also not deal with cardiac events related to thealignancy itself. Readers are referred to the previous re-orts2,3 in Seminars for the reviews of cardiotoxicity, partic-
Department of Medical Oncology, Royal Melbourne Hospital, Parkville,Victoria, Australia.
Department of Nuclear Medicine and Cardiology, Royal Melbourne Hospi-tal, Parkville, Victoria, Australia.
ddress correspondence to Associate Professor Michael Green, Departmentof Medical Oncology, Royal Melbourne Hospital, Grattan St, Parkville,
mVictoria 3050, Australia. E-mail: [email protected]
0093-7754/06/$-see front matter © 2006 Elsevier Inc. All rights reserved.doi:10.1053/j.seminoncol.2005.11.001
larly those dealing with other agents with lesser knownardiotoxic effects.
The incidence and severity of cardiotoxicity depend notnly on the drugs used but also on the dose, schedule, patientactors, and combination with other treatments such as ra-iotherapy. The last decade has also seen the emergence ofhe monoclonal antibody trastuzumab and the taxanes inlinical use. Together with the anthracyclines, these agentsave proven to be a highly active therapy in breast cancerreatment, but unfortunately clinical studies have also re-ealed unexpected cardiotoxicity in certain combinations.
This review will focus on chemotherapy-related cardiotox-city with particular emphasis on anthracyclines and newreatments from the last decade. Techniques in which cardiacunction is monitored and toxicity minimized are also dis-ussed with their merits in the setting of clinical practice.
nthracyclineshe anthracycline antibiotics are arguably one of the mostctive groups of chemotherapy agents in oncology. Com-only used anthracycline antibiotics include doxorubicin,aunorubicin, and epirubicin. They have proven activitygainst a spectrum of malignancies, including lymphoma,astric cancer, small cell lung cancer, sarcomas, and breastancer to name a few. Unfortunately, these agents also havehe most well-recognized cardiotoxic profile of cancer treat-
ents, which often hampers the degree of their utility.
btimci
mddpmoygtol
aacaaaMtbmdan
tcatsgd
MPrrew
RT(sv4wd
TaoaitjbDdficpTivotdet
PClcvttwdstylamwcwffa
etuptmouwNtc
Anticancer agents and cardiotoxicity 3
Although acute electrocardiograph (ECG) changes haveeen documented with the administration of anthracyclines,hese are often transient and not of any major clinical signif-cance. Daunorubicin has also been recognized to cause a
yocarditis/pericarditis phenomenon. These have been dis-ussed in greater detail in the previous reviews of cardiotox-city in this journal.2,3
The better known cardiotoxic effect of anthracyclinesanifests itself as a cardiomyopathy that is cumulative-dose–ependent. Early retrospective data suggested that the inci-ence of clinical cardiac failure is approximately 7.5% inatients receiving a cumulative doxorubicin dose of 550 mg/2, which increases linearly above 550 mg/m2.4 The majority
f patients developed the cardiomyopathy within the firstear of completion of treatment and had a mortality ratereater than 40%. More recent data, however, suggest thathe incidence of cardiomyopathy may be higher and mayccur even years after treatment and at a much lower cumu-ative dose.5-8
Part of this disparity may be explained by an increasedwareness of cardiotoxicity with improved screening as wells better long-term survival, particularly in the pediatric on-ology population. The definition of cardiomyopathy haslso been expanded from the clinical events of cardiac failures described originally by Von Hoff et al4 when cardiac im-ging was either not available or not routinely performed.ore recent data have tended to include predefined labora-
ory values such as left ventricular ejection fraction (LVEF)ased on radionuclide ventriculography (RNVG) or two-di-ensional (2D)-echocardiography in the definition of car-iomyopathy, even when patients may be asymptomatic. Asresult, the rate and cumulative dose of cardiotoxicty haveow seemingly altered with the modification of its definition.In clinical practice, most clinicians will tend to consider
he withdrawal of doxorubicin therapy at approximately aumulative dose of 450 to 500 mg/m2. This stopping of ther-py obviously becomes a dilemma if ongoing doxorubicinreatment may still otherwise be of benefit to the patient. Asuch, numerous techniques have been employed by investi-ators in an attempt to both monitor and minimize the car-iotoxicity of the anthracylines.
odifying Cardiotoxicityatient selection is obviously important in determining theate of cardiotoxicity. Groups recognized to be at increasedisk of developing doxorubicin cardiomyopathy include thelderly, those with prior cardiac disease, children, and thoseho have had previous mediastinal irradiation.4,6,8,9
adiotherapyhe Early Breast Cancer Trialists’ Collaborative GroupEBCTCG) performed a meta-analysis of 40 randomizedtudies comparing surgery alone versus surgery plus adju-ant radiotherapy in women with breast cancer treated over a0-year interval.9 A reduction in breast cancer-specific deathas seen, but overall survival remained largely unchanged
ue to an increase in non-breast cancer–related mortality. che majority of the non-breast cancer–related deaths werettributed to cardiovascular mortality secondary to the effectsf irradiation on the heart and the great vessels. This findingppears to contradict the results from the two large random-zed trials conducted by the Danish Breast Cancer Coopera-ive Group designed specifically to explore the effects of ad-uvant radiotherapy in the treatment of women with earlyreast cancer.10,11 Unlike earlier radiotherapy methods, theanish studies used modern techniques that minimized theegree of radiation exposure to the heart. Contrary to thending of the EBCTCG meta-analysis, both of these trialsonfirmed an overall survival advantage for both pre- andostmenopausal women in the radiotherapy treatment arm.he results of EBCTCG meta-analysis should therefore be
nterpreted with the understanding that although they pro-ide a more comprehensive synopsis of the available data,lder trials were included from which current radiotherapyechniques have evolved significantly. Cardiotoxicity is nooubt a genuine concern with radiotherapy treatment, but itsffects may possibly be mitigated with the current modernreatment techniques.
ediatric Considerationsommon pediatric malignancies such as acute lymphoblastic
eukemia and sarcomas are frequently treated with anthracy-lines. While there is little doubt that anthracyclines play aital role in the management of these childhood cancers,12,13
he attainment of cure comes with a significant risk of long-erm cardiac damage. As opposed to the adult population inhom the majority of clinical cardiotoxicity events appear toevelop within the first year of treatment,4 childhood cancerurvivors who have received anthracycline-based chemo-herapy remain at risk for developing cardiomyopathy evenears later. Steinherz et al6 undertook an analysis of 201ong-term survivors of pediatric malignancies 4 to 20 yearsfter completion of anthracycline treatment. Of these, abnor-al cardiac systolic function (defined by echocardiography)as detected in almost a quarter of the patients.6 Other than
umulative anthracycline dose and mediastinal irradiation,hich are recognized risks in adults, age at diagnosis and
emale gender have also been shown to be independent riskactors for the development of cardiomyopathy in the pedi-tric population.14,15
The exact incidence of long-term cardiotoxicity is, how-ver, difficult to estimate due to the considerable variation inhe literature. Recent systematic reviews in the pediatric pop-lation report the frequency of subclinical cardiotoxicity inublished data to be varying in range from zero to 57%, whilehe rate of clinical cardiac failure is zero to 16%.15,16 Theajority of these studies were noted to have serious method-
logic limitations with variations in the type of anthracyclinese, dosages, and schedule, as well as duration of follow-up,hich may partly explain the wide variance between them.ot included in the systematic review is a recent large long-
erm cohort study of 607 children treated with anthracy-lines. In this report, the cumulative risk of any anthracy-
line-induced congestive heart failure (CHF) 15 years after
sd1
iothmiee
SBpbcpsdwlbiptrwdraditRscin
EEcdmra
adsmtcu(
wcat(FsmCtrbHoiheiTFetldworacawFSb
DOiqccsiitaasplptdct0
4 R. Ng, N. Better, and M.D. Green
tart of treatment was estimated at 5% while the risk foreveloping CHF at a cumulative dose of 550 mg/m2 was0%.17
The efficacy of anticancer chemotherapy means that anncreasing percentage of adults will be cancer survivors, somef whom are likely to harbor the long-term effects of theirreatment. Indeed, in a study of long-term survivors of child-ood cancers, cardiac mortality was shown to be the secondost likely cause of death following malignancy.18 This find-
ng underscores the importance of the ongoing search forffective cardioprotectants without the sacrifice of antitumorfficacy.
cheduling of Anthracyclinesesides cumulative dose of anthracyclines, it has also beenostulated that exposure to peak levels of anthracylines maye an important factor in the pathogenesis of anthracyclineardiomyopathy. Several studies in the 1980s and 1990s ex-lored the use of weekly and protracted anthracycline infu-ions in an attempt to search for an alternative scheduling ofoxorubicin to the standard 3-week bolus therapy. Theeekly doxorubicin regimen appeared to be correlated with a
esser degree of histologic damage seen on endomyocardialiopsies when compared to standard 3-week bolus treatment
n several randomized clinical studies of approximately 100atients,19-21 as well as in a historical comparison.22 Pro-racted doxorubicin infusion was similarly associated with aeduced rate of histologic damage as well as cardiac failurehen compared to standard treatment.23-25 However, theata are not consistent and have not been replicated in aandomized study of a pediatric population with high-riskcute lymphoblastic leukemia that received 360 mg/m2 ofoxorubicin.26,27 Whether this finding is secondary to an
nherent biology of cardiac damage in the pediatric popula-ion different from that of the adult cohort remains unknown.egardless, both weekly and protracted anthracycline infu-ion regimens have not been widely adopted into currentlinical practice due in large part to the lack of large random-zed data in both and probably the perceived cumbersomeature of protracted infusions.
pirubicinpirubicin is a stereoisomer of doxorubicin introduced intolinical practice in the 1980s. Whereas cumulative dosages ofoxorubicin are limited to approximately 450 mg/m2 to 500g/m2, the similar degree of clinical cardiotoxicity with epi-
ubicin tends to occur much later at cumulative doses ofpproximately 900 to 1,000 mg/m2.28-30
Several studies have demonstrated that whether usedlone or in combination with other agents, epirubicin pro-uces antitumor responses similar to doxorubicin, whilehowing a trend in reducing the cardiotoxicity rate in treat-ent of women with advanced breast cancer.31,32 The inves-
igators in the Italian Multicentre Breast Study with Epirubi-in performed a randomized phase III study comparing these of 5-fluorouracil, cyclophosphamide, and doxorubicin
FAC) with the same regimen but substituting doxorubicin iith epirubicin (FEC) for women with advanced breast can-er. The mean reduction in LVEF was 6.6% in the epirubicinrm compared to 17.6% in the doxorubicin arm, while arend in reduction of the incidence of CHF was also seenFAC, 1.6%; FEC, 0.4%). These findings mirror those of therench Epirubicin study, which had an equivalent trial de-ign comparing epirubicin to doxorubicin in a similar regi-en for women with metastatic breast cancer. No cases ofHF occurred in the epirubicin arm, compared to 3.2% in
he doxorubicin arm. On balance, it appears that while epi-ubicin is equimolar with doxorubicin in the treatment ofreast cancer, the rate of cardiotoxicity is probably reduced.owever, the potential advantage that epirubicin may havever doxorubicin in cardiotoxicity has been offset somewhatn the adjuvant treatment setting of breast cancer where trialsave demonstrated that six cycles of FEC with 100 mg/m2 ofpirubicin (FEC100) to be the most effective epirubicin reg-men for women with node-positive primary disease.33,34
his means that a woman who undergoes six cycles ofEC100 chemotherapy would have received a cumulativepirubicin dose of 600 mg/m2. Considering that the cumula-ive epirubicin dose of 1,000 mg/m2 approximates the cumu-ative 450-500 mg/m2 dose of doxorubicin in terms of car-iotoxic events, the adjuvant epirubicin dose with FEC100ill be almost equivalent to the cumulative doxorubicin dosef 240-360 mg/m2 (for four or six cycles of 60 mg/m2 doxo-ubicin, respectively) in terms of cardiotoxicity risk. Hence,t the time of disease relapse, both regimens will essentiallyonfer similar cardiotoxic risks when the further need fornthracycline therapy arises. At present, epirubicin has beenidely used in Europe for the past two decades and receivedood and Drug Administration (FDA) approval in the Unitedtates in 1999 for the adjuvant treatment of node-positivereast cancer.
exrazoxanene of the proposed mechanisms of doxorubicin cardiotox-
city involves the formation of a ferrous complex with subse-uent generation of free radicals that cause progressive myo-yte damage.35 Dexrazoxane is a bis-diooxopiperazineompound that hydrolyzes to an open ring form, similar intructure to EDTA. This open-ring form, in turn, chelatesntracellular iron generated by doxorubicin, thereby inhibit-ng the subsequent production of free radicals responsible forhe cardiac damage. Dexrazoxane was initially formulated asn antineoplastic agent due to its topoisomerase II inhibitorctivity,36,37 but appreciation of its iron-chelating effect sub-equently led to its investigation as an anthracycline cardio-rotectant. Several studies with dexrazoxane in different ma-
ignancies treated with anthracyclines, both in adult andediatric populations, revealed its activity as a cardiopro-ectant.38-42 A meta-analysis of seven randomized studies ofexrazoxane use with anthracyclines confirmed that its useonfers a significant reduction in the risk of clinical cardio-oxicity (risk ratio, 0.24; 95% confidence interval, 0.11 to.52; P � .00031).43 However, questions were raised regard-
ng its efficacy with the finding of a reduced response rate in

oscacirb
rrCtcctct
iaianhd
LTitjtpdasMa
tompwdRmoWtpmsMob
waasttwlctgU
fwscliosaagc1dvwctaas
onwfrru
CMDficcacti
Anticancer agents and cardiotoxicity 5
ne of the larger randomized placebo-controlled trials.44 De-pite this, time-to-progression and survival were not signifi-antly different, and meta-analysis of objective responsecross five other trials of 818 breast cancer patients did notonfirm this reduced efficacy.43 Moreover, when the admin-stration of dexrazoxane is delayed until a cumulative doxo-ubicin dose of more than 300 mg/m2 has been reached, theenefit of cardioprotection is still evident.45
However, because of concern related to the reduction inesponse rate in this one, albeit largest, placebo-controlledandomized controlled trial, the current American Society oflinical Oncology (ASCO) Guideline recommends against
he routine use of dexrazoxane at the initiation of doxorubi-in-based chemotherapy in patients with metastatic breastancer.46 However, it may still be considered for those pa-ients who have received more than 300 mg/m2 of doxorubi-in and may still benefit from continued doxorubicin-con-aining therapy.
There are limited data at present on the use of dexrazoxanen the adjuvant setting or its long-term effects. The Cancernd Leukemia Group B (CALGB) recently completed enroll-ng women into a 2 � 2 � 2 factorial randomized studyssessing the use of dexrazoxane and trastuzumab in theeoadjuvant setting for women with breast cancer. It isoped the result of this study will help clarify the role thatexrazoxane plays as a cardioprotective agent.
iposomal Doxorubicin Formulationshe rationale of encapsulating doxorubicin within liposomes
s to allow the sequestration of the drug from organs such ashe heart and gastrointestinal tract that have tight capillaryunctions, while enhancing delivery of the cytotoxic agent toumor sites lined by compromised vasculature.47 Indeed,reclinical studies confirmed that liposomal packaging ofoxorubicin results in prolongation of plasma half-lives andlteration in its tissue distribution.48 The two forms of lipo-omal doxorubicin currently commercially available areyocet (The Liposome Company, Elan Corp, Princeton, NJ)
nd Doxil/Caelyx (Alza Pharmaceuticals, San Bruno, CA).Three studies have been performed with Myocet in the
reatment of women with metastatic breast cancer. In anpen-label, randomized study of the Myocet form of liposo-al doxorubicin with cyclophosphamide versus cyclophos-hamide and doxorubicin (AC) chemotherapy in 297omen,47 Myocet was found to produce a significantly re-uced cardiotoxicity rate (defined both clinically and onNVG scan) at 6% compared to the AC arm of 21%, whileaintaining comparable tumor response. Five cases of CHF
ccurred on the study, all of which were in the AC arm.hen compared to epirubicin and cyclophosphamide in a
rial with smaller patient numbers,49 the Myocet form of li-osomal doxorubicin in combination with cyclophospha-ide was found to have a similar cardiotoxicity rate but a
uperior progression-free survival. The third study comparedyocet as a single agent against doxorubicin alone in an
pen-label randomized trial of 244 women with metastatic
reast cancer.50 Cardiotoxicity occurring in the Myocet arm mas again reduced at 2% compared to 8% in the doxorubicinrm. The study was not powered sufficiently to show equiv-lence in response rate; an apparent trend towards inferiorurvival in the Myocet arm was seen despite an equivalentime-to-progression and time-to-treatment-failure betweenhe two arms. Based on results from the first study, Myocetas approved by the European Commission in 2000 as first-
ine therapy for metastatic breast cancer in combination withyclophosphamide. Because of concern with results from thehird study, FDA marketing approval has not yet beenranted for the Myocet form of liposomal doxorubicin in thenited States.51
Another variant of liposomal doxorubicin, Caelyx/Doxil, isormulated as liposomal doxorubicin additionally pegylatedith a polyethylene glycol coat. This process enhances eva-
ion of the pegylated liposomal doxorubicin (PLD) fromlearance by the mononuclear phagocyte system,52 henceeading to significant prolongation of its half-life, as well asncreased delivery to tumor tissue.53 In a recent phase III trialf 509 women with metastatic breast cancer designed tohow non-inferiority, PLD was demonstrated to have equiv-lent efficacy to single-agent doxorubicin, while maintainingreduced rate of cardiotoxicity.54 At a cumulative dose of
reater than 500 to 550 mg/m2, the risk for developing aardiac event (defined on RNVG and/or clinical grounds) was1% with PLD, compared with 40% in the conventionaloxorubicin group. Of the 10 patients treated PLD who de-eloped protocol-defined cardiotoxicity, none had CHFhile 10 of the 48 doxorubicin-treated patients who had
ardiotoxicity by LVEF criteria developed signs and symp-oms of CHF. At present, there are no randomized data avail-ble comparing liposomal doxorubicin to the pegylated vari-nt, nor are there data available on their use in the adjuvantetting.
Several recent phase I and II studies have explored the usef pegylated and standard liposomal doxorubicin in combi-ation with other agents, including taxanes and trastuzumab,ith no significant rate of cardiotoxicity demonstrated thus
ar.55-57 Although these are small, early-phase studies, the lowate of cardiotoxicity in these studies is noteworthy given theecognized high cardiotoxicity rate of an anthracycline whensed in combination with trastuzumab.58
ardiotoxicityonitoring During Treatment
espite the introduction of cardioprotectants and liposomalormulations, the incidence of cardiotoxicity remains a realssue in anthracycline therapy. Monitoring for the early sub-linical onset of cardiomyopathy is therefore a paramountomponent in prevention of subsequent overt cardiac dam-ge. The cumulative dose-dependent nature of doxorubicinardiotoxicity lends itself to appropriate monitoring and in-ervention when the need arises. The significant heterogene-ty of anthracycline tolerance also allows one to titrate the
aximum dose of doxorubicin for an individual, instead of

ua
EE“digamtstcaeoTw4ittcmpi
LIhatvrtcttptdttcisccs
amcts
tpd
mTwlLt
tgwTctwievt�aLar
Freotepd
6 R. Ng, N. Better, and M.D. Green
sing the empiric ceiling dose of 450 to 500 mg/m2 whenppropriate monitoring is in place.
ndomyocardial Biopsyndomyocardial biopsy has traditionally been viewed as thegold standard” test for the evaluation of anthracycline car-iomyopathy. Billingham et al59 developed a histologic scor-
ng system based on endomyocardial biopsy that has shownood correlation with the cumulative dose of anthracyclinesnd displays higher sensitivity for early cardiac damage thanethods based on evaluation of LVEF alone.60-62 However,
he lack of data in correlating these histologic changes toubsequent risk of CHF makes the interpretation of such aest difficult, especially when damage can often be seen atumulative doxorubicin levels as low as 180 mg/m2.61 Whilen endomyocardial biopsy provides a sensitive measure ofarly myocardial injury, it nevertheless does not provide datan myocardial function and the clinical state of the patient.his point is demonstrated in a necropsy series of 64 patientsho had received previous anthracycline treatment. Of the4 patients who had no documentation of clinical cardiotox-
city, almost 50% of them nevertheless displayed some his-ological changes of anthracycline cardiomyopathy.63 Fur-hermore, the requirement for appropriately trainedlinicians and the invasive nature of the test with its attendantorbidity means that cardiac biopsies remain largely an im-ractical means of monitoring for anthracycline cardiotoxic-
ty.
VEF Assessmentn contrast to endomyocardial biopsy, evaluation of the LVEFas been widely adopted as the preferred option of assessingnthracycline cardiotoxicity. Schwartz et al,64 in a retrospec-ive series, reviewed 1,487 doxorubicin-treated patients in-estigated over a 7-year interval using RNVG. Patients at highisk for developing doxorubicin cardiomyopathy were iden-ified as: (1) those with a decline of 10 ejection fraction per-entage points from normal baseline to a final value of lesshan 50%; (2) total doxorubicin dose of 450 mg/m2; or (3)hose with a baseline ejection fraction of less than 50%. Aroposal from the authors64 suggests that concordance withheir guidelines will lead to a fourfold reduction in the inci-ence of clinical cardiac failure. Indeed, a recent retrospec-ive analysis of the experience at a single institute followinghis guideline suggests that serial RNVG is an appropriate andost-effective approach for the prediction and prevention ofmpending congestive heart failure.65 In practice, LVEF as-essment is now an integral part of investigations for anthra-ycline cardiomyopathy, and, in fact, the majority of recentlinical trials44,47,50 include cardiotoxicity monitoring criteriaimilar to those proposed by Schwartz et al.64
Other than the calculation of LVEF, RNVG scans can nowlso routinely incorporate the assessment of regional wallotion and diastolic function as part of the screening of
ardiac function as there are now data that diastolic dysfunc-ion may be a more accurate predictor of cardiotoxicity than
ystolic function assessment alone.66,67 This diastolic func- tion assessment may include isovolumetric relaxation time oreak filling rate, both of which are assessable by 2D-echocar-iography, while the latter can be monitored by RNVG.2D-echocardiography is another means of LVEF assess-ent that is widely available for use in the clinical setting.his availability is especially true in the pediatric settinghere it holds a potential advantage over RNVG by not uti-
izing ionizing radiation. Other than providing assessment ofVEF, 2D-echocardiography also gives additional informa-ion pertaining to valve anatomy as well as diastolic function.
The presence of cardiotoxicity is assessed both quantita-ively and qualitatively. In addition to a fall in LVEF withlobal hypokinesis, early cardiotoxicity may be associatedith an apical wall motion abnormality, such as apical lag.he acquisition on both RNVG and echocardiography areompared to previous studies performed on the same patient,o ensure that acquisition details, such as patient positioning,hich can slightly alter the LVEF, are the same. The RNVG
ncorporates the radiolabeling of the patient’s red blood cellsither in vitro or by a modified in vivo method. Ventricularolumes at end-systole and end-diastole are proportional tohe amount of radioactivity. (LVEF � end-diastolic volume
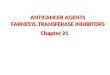
end systolic volume/end-diastolic volume). This methodllows an accurate and highly reproducible calculation ofVEF in a single patient at two points in time (Fig 1). Thebsolute amount of ionizing radiation the patient receives iselatively low. Echocardiography is radiation-free and similar
igure 1 The radionuclide ventriculogram uses autologous-labeleded blood cells with technetium-99m in an acquisition gated to thelectrocardiograph and is analyzed in a left anterior oblique positionn a standard gamma camera. Regions of interest are placed aroundhe left ventricle to obtain counts at end-diastole on the left andnd-systole on the right, to calculate LVEF. Panel A shows a normalatient, while Panel B represents a patient with cardiotoxicity due tooxorubicin.
o RNVG both qualitatively and in cost. However, calculation

ohcemt
AAiiibmsLlamorarc5fr
TTdaoi
taimtaltcamow9ca
pgtoo
ld
mgecfidte
CTsvbibtLi
TStcttcprgcccdsabidwaii
pwmrbdp
Anticancer agents and cardiotoxicity 7
f the LVEF is area dependent using 2D assumptions, andence reproducibility may be slightly more difficult. It isommonly recommended to use the technique done best inach individual institution. Complete details regarding theethods of performing these tests are beyond the scope of
his review.
ntimyosin Antibody Scintigraphyntimyosin antibody scintigraphy has previously been stud-
ed for the monitoring of anthracycline cardiotoxicity. In an-mals treated with doxorubicin, the severity of myocardialnjury was correlated with the intensity of antimyosin anti-ody uptake.68 Clinical studies confirmed radiolabeled anti-yosin antibody scintigraphy to be a significantly more sen-
itive marker of early cardiac damage than measurements ofVEF alone. In fact, myosin uptake becomes apparent at
evels as low as a cumulative doxorubicin dose of 120 mg/m2,nd almost all patients will exhibit a positive result at a cu-ulative dose of 240 to 300 mg/m2.69,70 This high sensitivity
bviously somewhat limits its clinical utility given that mostegimens of adult doxorubicin-based chemotherapy [such asdjuvant breast chemotherapy with four cycles of AC (doxo-ubicin 60 mg/m2, cyclophosphamide 600 mg/m2) or six cy-les of CHOP (cyclophosphamide 750 mg/m2, doxorubicin0 mg/m2, vincristine 1.4 mg/m2, and prednisone 40 mg/m2)or lymphoma routinely exceed these cumulative doses. As aesult, this technique has not been routinely used worldwide.
roponinsroponins (I and T) are highly sensitive markers of myocyteamage that predict both short- and long-term prognosis incute coronary syndrome.71-73 The availability and ease of usef this test presents itself as an attractive alternative for mon-toring of anthracycline cardiotoxicity.
While animal studies suggest a good correlation betweenroponin levels and histologic changes of early cardiac dam-ge,74,75 the evidence for its clinical utility has been conflict-ng in human studies. A study in adults with hematologic
alignancies showed that levels of troponin I are elevated inhose patients who received anthracycline-based chemother-py, as well as those that are chemotherapy-naive, albeit at aower level.76 Another study in 10 adults receiving their ini-ial cycle of anthracycline therapy showed no significanthanges in the troponin T measurements.77 In children withcute lymphoblastic leukemia undergoing doxorubicin treat-ent, elevated troponin I was present following the first cycle
f chemotherapy, and the magnitude of elevation correlatedith the degree of wall thinning and left ventricular dilatationmonths later.78 This finding is contrary to other studies in
hildren, which showed no association between troponin Tnd echocardiographic changes.79,80
The utility of troponins in high-dose chemotherapy ap-ears to be more promising. In a study of 204 adults under-oing high-dose anthracycline-based chemotherapy, 65 pa-ients had a raised troponin I level of whom 29% had a LVEFf less than 50%, and three developed clinical CHF. In the
ther 139 patients who never had an elevated troponin I revel, all maintained a LVEF greater than 50%, and noneeveloped CHF.81
It therefore appears that at least in the high-dose setting,easurement of troponin levels allows one to identify the
roup at risk developing significant cardiomyopathy. How-ver, for the majority of patients undergoing standard anthra-ycline treatment, the role of troponins remains to be de-ned. It should be also noted that troponins mayemonstrate problems with specificity, being elevated in po-entially coexisting conditions such as ischemic heart dis-ase,82 pulmonary embolus,83 and sepsis.84
onclusionshere is little doubt that even at low doses of anthracyclines,ome degree of myocardial damage already takes place. Theery nature of the sensitivity of tests such as endomyocardialiopsies, antimyosin scintigraphy and to an extent, troponins
nvariably limits their utility in the clinical setting. Until it cane shown that a particular test can provide significant sensi-ivity without the sacrifice of specificity, measurements ofVEF will continue to be the most pragmatic means of mon-
toring for anthracycline cardiotoxicity.
axanestudies in 1990s showed the taxanes docetaxel and paclitaxelo be among the most active drugs in the treatment of breastancer. As a single agent, the taxanes have negligible cardio-oxicity when compared to anthracyclines.85,86 Several trialsherefore explored its use in combination with anthracy-lines. Early phase II studies confirmed that a combination ofaclitaxel and anthracyclines resulted in impressive responseates but also an unacceptably high incidence of CHF inreater than one fifth of patients.87,88 Subsequently, pharma-okinetic studies showed that interaction between doxorubi-in and paclitaxel to be the likely cause for this increase inardiotoxicity, which is both schedule- and sequence-depen-ent. The total doxorubicin plasma exposure was demon-trated to be 30% greater when paclitaxel infusion immedi-tely follows doxorubicin, compared to a delay of 24 hoursetween the two infusions. Similarly, doxorubicin clearance
s also reduced by a third when paclitaxel infusion precedesoxorubicin, compared to the reverse order in this schedulehen doxorubicin is administered first.89,90 A retrospective
nalysis indicated that the rate of cardiotoxicity can be min-mized to less than 5% if the cumulative dose of doxorubicins limited to 360 mg/m2.91
The latter hypothesis was tested in an EORTC study com-aring the combination of doxorubicin and paclitaxel (AT)ith doxorubicin and cyclophosphamide (AC) in the treat-ent of women with metastatic breast cancer. This phase III
andomized study restricted the cumulative dose of doxoru-icin to 360 mg/m2 in both arms and allowed a 30-minuteelay between the administration of doxorubicin prior toaclitaxel. This study demonstrated that although the AT arm
esulted in a higher rate of LVEF fall, it was not predictive of
Cl
pcoatli
tsahad
ddld
ooicdwcgdcppbi
epmmfsc
TTbtmtswotw
iutoatIcoIfrvztc7tlpst
pitsistHmiw
ompTot
TTTcEhnCa(mtth
8 R. Ng, N. Better, and M.D. Green
HF development. The incidence of CHF in both arms wasow and not statistically different.92
Similarly, another phase III eastern European study com-ared AT chemotherapy with the combination of fluoroura-il, doxorubicin, and cyclophosphamide (FAC). The infusionf paclitaxel was delayed for 24 hours after doxorubicin tovoid the pharmacokinetic interaction. At a median cumula-ive doxorubicin dose of 400 mg/m2, the rate of LVEF fall wasow and similar in both groups with no statistical differencen the rates of CHF.93
The Intergroup E1193 study tested whether the combina-ion of paclitaxel and doxorubicin might prove superior toequential single-agent therapy. In this trial the combinationrm consists of doxorubicin followed 3 hours later by a 24-our paclitaxel infusion. Cardiac complications were equiv-lent in the combination arm compared to the single-agentoxorubicin arm.86
It therefore appears that combination use of paclitaxel andoxorubicin is relatively non-cardiotoxic provided thatoxorubicin is administered first and there is a delay of at
east 30 minutes between the infusions or that the cumulativeose of doxorubicin is restricted to 360 mg/m2.The combination of docetaxel with doxorubicin, on the
ther hand, does not appear to produce any significant effectn doxorubicin in pharmacokinetic studies94,95 nor on thencidence of cardiac failure in clinical trials. Nabholtz et al96
ompared the use of AC chemotherapy with doxorubicin andocetaxel in a randomized phase III study. The rate of CHFas low and comparable in both groups with a higher per-
entage of patients in the AC arm more likely to experience areater than 20 percentage-point fall in LVEF, although theose of doxorubicin was 20% greater in the AC arm.96 Theombination of docetaxel with doxorubicin and cyclophos-hamide (TAC) also resulted in a low incidence of CHF com-arable to FAC chemotherapy in the treatment of women inoth adjuvant and metastatic breast cancer randomized stud-
es.97,98
Epirubicin in combination with taxanes has similarly beenxplored, mainly in European studies. A German study com-aring epirubicin and cyclophosphamide (60 mg/m2, 600g/m2) with epirubicin and paclitaxel (60 mg/m2, 175 mg/2) confirmed a low rate of cardiotoxicity,99 and experience
rom the International Breast Cancer Study Group (IBCSG)imilarly showed that the combination of epirubicin and do-etaxel to be a safe and relatively noncardiotoxic regimen.100
rastuzumabrastuzumab is a recombinant, humanised monoclonal anti-ody targeted against human epidermal growth factor recep-or-2 protein (HER2), which is overexpressed in approxi-ately 30% of breast cancer.101 As a monotherapy,
rastuzumab use in women with metastatic breast cancer re-ults in responses either as first-line treatment or in patientsho have progressed through chemotherapy.102-104 The piv-tal trial by Slamon et al58 in 2001 showed that use of tras-uzumab in combination with chemotherapy for patients
ith HER2�, metastatic breast cancer led to a significant ancrease in response rate as well as survival. However, annexpected disproportionate percentage of patients (27%) inhe combination anthracycline and trastuzumab arm devel-ped cardiotoxicity, including 16% New York Heart Associ-tion (NYHA) class III or IV heart failure: compared to 8% inhe single-agent anthracycline arm with only 3% NYHA classII/IV heart failure. Cardiotoxicity also occurred in 13% of theombination paclitaxel and trastuzumab arm compared tonly 1% in the single-agent paclitaxel arm with NYHA III orV heart failure rate of 2% and 1%, respectively. Cardiacunction subsequently improved in 75% of the patients whoeceived standard medical therapy. Further retrospective re-iew of seven phase II/III trials involving the use of trastu-umab confirmed this cardiotoxic combination between tras-uzumab and anthracyclines.105 As a single agent, theardiotoxicity rate of trastuzumab varies between 3% and%,105 and unlike anthracyclines, the cardiotoxicity of tras-uzumab does not appear to be dependent on either cumu-ative dose or treatment duration. An extension study to theivotal study by Slamon et al,58 designed to obtain additionalafety data, confirmed that the prolonged use of trastuzumabo be both safe and well tolerated.106
Several hypotheses have been proposed regarding theathogenesis of trastuzumab cardiotoxicity. They include
mmune-mediated toxicity, drug-drug interaction, and directoxicity. The available evidence supports the latter hypothe-is.107 Murine models have shown that the HER2 protein ismportant in the growth and repair of cardiac muscles,108 andcintigraphic evidence of myocardial uptake of radiolabeledrastuzumab has also been demonstrated in women withER2� metastatic breast cancer.109 It is postulated that theechanism necessary for the reparation of cardiac damage
nduced by anthracyclines may be impaired by trastuzumabhen these two agents are administered concomitantly.Recent phase II studies have also reported the combination
f trastuzumab with other agents such as docetaxel, liposo-al doxorubicin, vinorelbine, and platinum com-ounds55,110-114 in the treatment of metastatic breast cancer.hese data have been sufficiently encouraging with low ratesf cardiotoxicity to form the impetus for their further inves-igations in phase III studies.
rastuzumab in Adjuvantreatment of Breast Cancerhe efficacy of trastuzumab therapy in metastatic breast can-er led to the exploration of its use in the adjuvant setting.arly data from several of the trials of adjuvant trastuzumabave recently been published. Results from the Breast Inter-ational Group Herceptin Adjuvant (HERA) study, the Northentral Cancer Treatment Group (NCCTG) Study N9831,nd the National Surgical Adjuvant Breast and Bowel ProjectNSABP) Study B-31 all showed a highly significant improve-ent in disease-free survival in women treated with adjuvant
rastuzumab, compared to chemotherapy alone.115,116 De-ailed prospective cardiac monitoring in these trials has alsoelped shed some light on the early incidence of cardiac
dverse events given in the adjuvant setting (Table 1).
trpttccttToedwcUrabdcLpapm
r
NNsw6dt31abp
cgottctiarvCoti
T
M
A
A
*†‡§
¶ iteria)
Anticancer agents and cardiotoxicity 9
The NCCTG N9831 study compared three regimens: (1)he control arm of group A consisted of four cycles of doxo-ubicin and cyclophosphamide (AC) followed by weeklyaclitaxel for 12 weeks; (2) group B consisted of the samereatment as group A but with the addition of 52 weeks ofrastuzumab given upon completion of the AC and paclitaxelhemotherapy (sequential trastuzumab); (3) group C re-eived the same chemotherapy (AC and paclitaxel), but therastuzumab was administered from the first day of paclitaxelreatment and given for 52 weeks (concurrent trastuzumab).he NSABP B-31 study compared two regimens: four cyclesf AC followed by four cycles of 3-weekly paclitaxel givenither with or without 52 weeks of trastuzumab starting onay 1 of the paclitaxel administration. In both trials, the LVEFas assessed before trial entry, after completion of the AC
hemotherapy, and 6, 9, and 18 months after randomization.pon completion of the AC chemotherapy, participants were
equired to have an LVEF above the institutional normal limitnd a reduction of less than 16 percentage points from theaseline value. Cardiac criteria for trastuzumab cessationuring the 6- and 9-month LVEF assessment periods in-luded any symptomatic cardiac deterioration, reduction ofVEF below the normal limit or a decline of less than 15ercentage points from baseline. In the latter two situations,repeat LVEF assessment was undertaken after 4 weeks withermanent discontinuation of the drug if no further improve-ent had occurred by then.Combined data from the B-31 and N9831 studies were
able 1 Rates of Cardiotoxicity in Randomized Phase III Trial
ChemotherapyRegimen
SymptomaticCHF
SevereCHF*
etastaticSlamon et al
AC 8% 3%AC�H 27% 16%P 1% 1%P�H 13% 2%
djuvantNCCTG N9831
AC¡ — —AC¡P¡ — 0%AC¡P¡H — 2.2%AC¡P�H¡H — 2.9%
NSABP B-31AC¡P 1.6%¶ 0.8%AC¡P�H¡H 8.7%¶ 4.1%
HERAObservation 0.06%¶ 0.06%Trastuzumab, 1 yr 1.73%¶ 0.54%
bbreviations: AC, doxorubucin � cyclophosphamide; P, paclitaxel;National Surgical Adjuvant Breast and Bowel Project; HERA, He
Protocol defined severe CHF (NYHA class III/IV cardiac dysfunctioProtocol defined LVEF reduction on at least one assessment (whePersistent LVEF reduction resulting in trastuzumab withdrawal/noPercentage in the N9831 and B31 study who were withdrawn from
to protocol-defined cardiotoxicity.Includes both non–protocol-defined CHF (ie, did not meet LVEF cr
ecently presented in a joint analysis approved by both the a
ational Cancer Institute and the US FDA.116 Group B of the9831 study was excluded from this joint analysis due to its
equential trastuzumab administration. Of the 3,947 patientsho had an LVEF evaluation after the AC chemotherapy,.7% were excluded from starting trastuzumab treatmentue to protocol-defined cardiotoxicity as described above. Inhe cohort of participants who received trastuzumab therapy,1.4% discontinued treatment before 52 weeks. A total of4.2% were due to asymptomatic LVEF reduction and 4.7%s a result of symptomatic cardiac events. Thus, the com-ined rate of treatment withdrawal as a result of cardiac com-lications from trastuzumab was 18.9%.In the N9831 study the cumulative incidence of NYHA
lass III/IV CHF or cardiac deaths was zero in the controlroup, 2.9% in the concurrent trastuzumab arm (20 CHF,ne cardiomyopathy death), and 2.2%117 in the sequentialrastuzumab arm (12 CHF, one cardiac death). In the B-31rial, the cumulative incidence of NYHA class III/IV CHF orardiac deaths was 0.8% in the control group and 4.1% in therastuzumab arm, giving a difference in cumulative 3-yearncidence of 3.3%. Multivariate analysis confirmed that agend LVEF at baseline or following the AC chemotherapyemained the most significant predictive factors for the de-elopment of subsequent CHF.118 In the 31 patients withHF, 27 had been followed for at least 6 months after devel-pment of cardiac dysfunction, and only 1 reported persis-ent CHF symptoms, although 18 remained on cardiac med-cations. Twenty-four of the 27 patients underwent LVEF
g Trastuzumab
ardiaceaths
>12LVEFEpisode†
Withdrawal Due toAsymptomatic 2LVEF‡
0% — —0% — —0% — —0% — —
— — 6.7%§0% 8% —
(0.17%) 18% —(0.16%) 21% 14.4%
(0.1%) 17% —0% 34% 14%
(0.06%) 2.2% —0% 7.1% —
tuzumab; NCCTG, North Central Cancer Treatment Group; NSABP,Adjuvant.
or cardiac death).rsistent or not).
ion.to trastuzumab component of study following four cycles of AC due
and severe CHF.
s Usin
CD
11
1
1
H, trasrceptinn and/ther peninitiatentry in
ssessments again more than 6 months following their CHF,

al
wltwotrC3csloLmt
ctwgastzdc0
brca1cwaosalsjfiwmapv
PATe
mgatmnpPpdttrssestdgstIaeersbf
CCtpattroavt
zizusmc
AT
10 R. Ng, N. Better, and M.D. Green
nd 17 of them still had decreased LVEF compared to theirast LVEF assessment.
The HERA study was an international trial that requiredomen with HER2� breast cancer who had completed at
east four cycles of adjuvant chemotherapy to be randomizedo one of three groups: observation alone, trastuzumab giveneekly for 1 year, or trastuzumab for 2 years. A total of 94%f the participants received an anthracycline-based chemo-herapy and 26%, a taxane-based regimen. Participants wereequired to have an LVEF of at least 55% for study entry.ardiac LVEF assessment was repeated at 3, 6, 12, 18, 24, 30,6, and 60 months after randomization. Cardiac criteria foressation of trastuzumab were similar to the N9871 and B-31tudies and included symptomatic CHF, LVEF of 45% oress, or a LVEF less than 50% with a reduction from baselinef 10 percentage points. In asymptomatic patients, a repeatVEF assessment was undertaken after 3 weeks, and treat-ent was allowed to recommence if the LVEF had returned
o a level above the criteria for withdrawal.Results of the interim analysis were recently published
omparing the observation arm with the 1-year trastuzumabreatment cohort.115 One hundred thirteen patients treatedith trastuzumab (7%) and 34 (2.2%) in the observationroup had a protocol-defined LVEF reduction on at least onessessment. There was one cardiac death (0.06%) in the ob-ervation arm, while none occurred in the trastuzumab-reated group. Twenty-nine patients (1.7%) in the trastu-umab group and one patient (0.06%) in the observation armeveloped symptomatic CHF. Severe CHF/cardiac deaths oc-urred in 0.54% of the patients treated with trastuzumab and.06% in the control group.These results of adjuvant trastuzumab use in early-stage
reast cancer have demonstrated a substantial benefit ineducing the rate of breast cancer relapse. Although small,ardiotoxicity remains a tangible risk in these women whore potentially cured of their breast cancer. Approximately4% of patients who received trastuzumab starting con-urrently with paclitaxel following AC chemotherapyithdrew before the completion of 1 year of trastuzumab
s a result of asymptomatic cardiac dysfunction. The ratef significant cardiotoxicity (NYHA class III/IV) was reas-uringly lower at around 4% in the N9831/B-31 studiesnd 0.54% in the HERA study. Whether these rates areikely to increase with longer follow-up remains to beeen. In patients who developed symptomatic CHF, a ma-ority recovered following the cessation of therapy. Thisnding is in keeping with data in the metastatic setting,hich suggest that the cardiotoxic effects of trastuzumabay be potentially reversible upon cessation of therapy
nd, indeed, re-treatment with trastuzumab may even beossible without causing further significant damage, pro-iding appropriate cardiac therapy is administered.119
rognosis and Treatment ofnthracycline Cardiotoxicity
he prognosis of anthracycline-induced cardiotoxicity in
arly retrospective studies was generally poor with a high nortality rate of greater than 40%.4 More recent studies sug-est that treatment of anthracycline cardiotoxicity is manage-ble with better clinical recovery in a majority of pa-ients.58,120 One reason for this improvement in prognosisay be that in the early studies, many patients were diag-osed late with cardiac failure while current practice is torevent as well as treat cardiac failure with better screening.rogress in treatment of cardiac failure may also partly ex-lain the improved prognosis, in particular the availability ofrugs such as angiotensin-converting enzyme (ACE) inhibi-ors, spironolactone, and beta blockers that have been proveno improve morbidity and mortality in non–anthracycline-elated cardiovascular disease.121-127 However, a recent retro-pective review of doxorubicin-exposed childhood cancerurvivors treated with ACE inhibitors suggests that the ben-ficial effects in the pediatric population may only be tran-ient.128 An initial improvement in cardiac function seen inhe first six to 10 years nevertheless resulted in subsequenteterioration both on clinical and echocardiographicrounds. The results of a double-blind, placebo-controlledtudy of enalapril in long-term survivors of doxorubicin-reated pediatric cancer have also been reported recently.129
n this study of patients aged 8 to 20 years who developedsymptomatic evidence of cardiac dysfunction based onchocardiography, RNVG, or ECG, the prophylactic use ofnalapril resulted in the reduction of cardiac function dete-ioration (as measured by an increase in left ventricular end-ystolic wall stress). Whether this improvement would haveeen sustained in the long term is unknown given the medianollow-up of only 3 years in this trial.
onclusionsardiotoxicity is a rare but serious complication of cancer
reatment. The class with the most recognized cardiotoxicrofile, the anthracyclines, contains some of the most activegents in oncology. Combination therapy with new drugs inhe last decade, such as the taxanes and trastuzumab, in thereatment of metastatic breast cancer has yielded impressiveesults but also unexpected cardiotoxicity. The increasing usef these drugs now in the adjuvant breast cancer clinical trialsnd growing population of long-term pediatric cancer survi-ors means that more than ever, cardiotoxicity will continueo remain an important issue for oncology.
Proven methods of minimizing cardiotoxicity with dexra-oxane and liposomal anthracycline formulations need to bencorporated into clinical use with the taxanes and trastu-umab. One such trial, the CALGB study that explores these of dexrazoxane and trastuzumab, points towards the pos-ible future of breast cancer treatment, which aims to mini-ize cardiotoxicity without the sacrifice of antitumor effi-
acy.
cknowledgmenthe authors thank James Westcott for supplying the radio-
uclide ventriculography images.
R
Anticancer agents and cardiotoxicity 11
eferences1. Anderson R, Smith B: National Vital Statistics Reports 52 (9). Atlanta,
GA: Centers for Disease Control and Prevention/National Center forHealth Statistics, November 2003
2. Von Hoff D, Rozencweig M, Piccart M: The cardiotoxicity of antican-cer agents. Semin Oncol 9:23-33, 1982
3. Allen A: The cardiotoxicity of chemotherapeutic drugs. Semin Oncol19:529-542, 1992
4. Von Hoff D, Lajard M, Basa P, et al: Risk factors for doxorubicin-induced congestive heart failure. Ann Intern Med 91:710-717, 1979
5. Swain S, Whaley F, Ewer M: Congestive heart failure in patientstreated with doxorubicin: A retrospective analysis of three trials. Can-cer 97:2869-2879, 2003
6. Steinherz L, Steinherz P, Tan C, et al: Cardiac toxicity 4 to 20 yearsafter completing anthracycline therapy. JAMA 266:1672-1677, 1991
7. Lipshultz S, Colan S, Gelber R: Late cardiac effects of doxorubicintherapy for acute lymphoblastic leukemia in childhood. N Engl J Med324:808-815, 1991
8. Hequet O, Le QH, Moullet I, et al: Subclinical late cardiomyopathyafter doxorubicin therapy for lymphoma in adults. J Clin Oncol 22:1864-1871, 2004
9. Early Breast Cancer Trialists’ Collaborative Group: Favourable andunfavourable effects on long-term survival of radiotherapy for earlybreast cancer: An overview of the randomised trials. Lancet 355:1757-1770, 2000
10. Overgaard M, Jensen M-B, Overgaard J, et al: Postoperative radiother-apy in high-risk postmenopausal breast-cancer patients given adju-vant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82crandomised trial. Lancet 353:1641-1648, 1999
11. Overgaard M, Hansen P, Overgaard J et al: Postoperative radiotherapyin high-risk premenopausal women with breast cancer who receiveadjuvant chemotherapy. N Engl J Med 337:949-955, 1997
12. Hitchcock-Bryan S, Gelber R, Cassady J: The impact of inductionanthracycline on long-term failure-free survival in childhood acutelymphoblastic leukemia. Med Pediatr Oncol 14:211-215, 1986
13. Smith M, Ungerleider R, Horowitz M, et al: Influence of doxorubicindose intensity on response and outcome for patients with osteogenicsarcoma and Ewing’s sarcoma. J Natl Cancer Inst 83:1460-1470, 1991
14. Lipshultz S, Lipsitz S, Mone S, et al: Female sex and drug dose as riskfactors for late cardiotoxic effects of doxorubicin therapy for child-hood cancer. N Engl J Med 332:1738-1743, 1995
15. Kremer L, van der Pal H, Offringa M, et al: Frequency and risk factorsof subclinical cardiotoxicity after anthracycline therapy in children: Asystematic review. Ann Oncol 13:819-829, 2002
16. Kremer L, van Dalen E, Offringa M, et al: Frequency and risk factors ofanthracycline-induced clinical heart failure in children: A systematicreview. Ann Oncol 13:503-512, 2002
17. Kremer L, van Dalen E, Offringa M, et al: Anthracycline-inducedclinical heart failure in a cohort of 607 children: Long-term follow-upstudy. J Clin Oncol 19:191-196, 2001
18. Green D, Hyland A, Chung C, et al: Cancer and cardiac mortalityamong 15-year survivors of cancer diagnosed during childhood oradolescence. J Clin Oncol 17:3207-3215, 1999
19. Valdivieso M, Burgess M, Ewer M, et al: Increased therapeutic index ofweekly doxorubicin in the therapy of non-small cell lung cancer: Aprospective, randomized study. J Clin Oncol 2: 207-214, 1984
20. Torti F, Bristow M, Howes A, et al: Reduced cardiotoxicity of doxo-rubicin delivered on a weekly schedule. Assessment by endomyocar-dial biopsy. Ann Intern Med 6: 745-749, 1983
21. Umsawasdi T, Valdivieso M, Booser D, et al: Weekly doxorubicinversus doxorubicin every 3 weeks in cyclophosphamide, doxorubi-cin, and cisplatin chemotherapy for non-small cell lung cancer. Can-cer 64:1995-2000, 1989
22. Weiss A, Metter G, Fletcher W, et al: Studies on adriamycin using aweekly regimen demonstrating its clinical effectiveness and lack ofcardiac toxicity. Cancer Treat Rep 60:813-822, 1976
23. Legha S, Benjamin R, Mackay B et al: Reduction of doxorubicin car-diotoxicity by prolonged continuous intravenous infusion. Ann Intern
Med 96:133-139, 198224. Hortobagyi G, Frye D, Buzdar A, et al: Decreased cardiac toxicity ofdoxorubicin administered by continuous intravenous infusion incombination chemotherapy for metastatic breast carcinoma. Cancer63:37-45, 1989
25. Shapira J, Gotfried M, Lishner M, et al: Reduced cardiotoxicity ofdoxorubicin by a 6-hour infusion regimen. A prospective randomizedevaluation. Cancer 65:870-873, 1990
26. Speyer J, Green M, Dubin N, et al: Prospective evaluation of cardio-toxicity during a six-hour doxorubicin infusion regimen in womenwith adenocarcinoma of the breast. Am J Med 78:555-563, 1985
27. Lipshultz S, Giantris A, Lipsitz S, et al: Doxorubicin administration bycontinuous infusion is not cardioprotective: The Dana-Farber 91-01Acute Lymphoblastic Leukemia protocol. J Clin Oncol 20:1677-1682,2002
28. Jain K, Casper E, Geller N, et al: A prospective randomized compari-son of epirubicin and doxorubicin in patients with advanced breastcancer. J Clin Oncol 3:818-826, 1985
29. Jensen B, Skovsgaard T, Nielsen S, et al: Functional monitoring ofanthracycline cardiotoxicity: A prospective, blinded, long-term obser-vational study of outcome in 120 patients. Ann Oncol 13:699-709,2002
30. Ryberg M, Nielsen D, Skovsgaard T, et al: Epirubicin cardiotoxicity:An analysis of 469 patients with metastatic breast cancer. J Clin Oncol16:3502-3508, 1998
31. The Italian Multicentre Breast Study With Epirubicin: Phase III ran-domized study of fluorouracil, epirubicin, and cyclophosphamide vfluorouracil, doxorubicin, and cyclophosphamide in advanced breastcancer: An Italian multicentre trial. J Clin Oncol 6:976-982, 1988
32. The French Epirubicin Study Group: A prospective randomized phaseIII trial comparing combination chemotherapy with cyclophospha-mide, fluorouracil, and either doxorubicin or epirubicin. J Clin Oncol6:679-688, 1988
33. The French Adjuvant Study Group: Benefit of a high-dose epirubicinregimen in adjuvant chemotherapy for node-positive breast cancerpatients with poor prognosis factors: 5-year follow-up results ofFrench Adjuvant Study Group 05 randomized trial. J Clin Oncol19:602-611, 2001
34. Fumoleau P, Kerbrat P, Romestaing P, et al: Randomized trial com-paring six versus three cycles of epirubicin-based adjuvant chemo-therapy in premenopausal, node-positive breast cancerpatients: 10-year follow-up results of the French Adjuvant Study Group 01 trial.J Clin Oncol l21:298-305, 2003
35. Myers C, Gianni L, Zweier J, et al: Role of iron in Adriamycin bio-chemistry. Fed Proc 45:2792-2797, 1986
36. Creighton A, Hellmann K, Whitecross S: Antitumour activity in aseries of bisdiketopiperazines. Nature 222:384-385, 1969
37. Von Hoff D, Howser D, Lewis B: Phase I study of ICRF-187 using adaily for 3 days schedule. Cancer Treat Rep 65:249-252, 1981
38. Wexler L, Andrich M, Venzon D, et al: Randomized trial of the car-dioprotective agent ICRF-187 in pediatric sarcoma patients treatedwith doxorubicin. J Clin Oncol 14:362-372. 1996
39. Venturini M, Michelotti A, Del Mastro L, et al: Multicenter random-ized controlled clinical trial to evaluate cardioprotection of dexrazox-ane versus no cardioprotection in women receiving epirubicin che-motherapy for advanced breast cancer. J Clin Oncol 14:3112-3120,1996
40. Lopez M, Vici P, Di Lauro K, et al: Randomized prospective clinicaltrial of high-dose epirubicin and dexrazoxane in patients with ad-vanced breast cancer and soft tissue sarcomas. J Clin Oncol 16:86-92,1998
41. Feldmann J, Jones S, Weisberg S, et al: Advanced small cell lungcancer treated with CAV (cyclophosphamide, Adriamycin � vincris-tine) chemotherapy and the cardioprotective agent dexrazoxane(ADR529, ICRF-187. Zinecard). Proc Am Soc Clin Oncol 11:296,1992 (abstr 993)
42. Speyer J, Green M, Zeleniuch-Jacquotte A, et al: ICRF-187 permitslonger treatment with doxorubicin in women with breast cancer.J Clin Oncol 10:117-127, 1992
43. Seymour L, Bramwell V, Moran L: Use of dexrazoxane as a cardiopro-

12 R. Ng, N. Better, and M.D. Green
tectant in patients receiving doxorubicin or epirubicin chemotherapyfor the treatment of cancer. The Provincial Systemic TreatmentDisease Site Group. Cancer Prev Control 3:145-149, 1999
44. Swain S, Whaley F, Gerber M, et al: Cardioprotection with dexrazox-ane for doxorubicin-containing therapy in advanced breast cancer.J Clin Oncol 15:1318-1332, 1997
45. Swain S, Whaley F, Gerber M, et al: Delayed administration of dexra-zoxane provides cardioprotection for patients with advanced breastcancer treated with doxorubicin-containing therapy. J Clin Oncol15:1333-1340, 1997
46. Schuchter L, Hensley M, Neal J, et al: 2002 update of recommenda-tions for the use of chemotherapy and radiotherapy protectants: Clin-ical practice guidelines of the American Society of Clinical Oncology.J Clin Oncol 20:2895-2903, 2002
47. Batist G, Ramakrishnan G, Rao C, et al: Reduced cardiotoxicity andpreserved antitumour efficacy of liposome-encapsulated doxorubicinand cyclophosphamide compared with conventional doxorubicin andcyclophosphamide in a randomized, multicenter trial of metastaticbreast cancer. J Clin Oncol 19:1444-1454, 2001
48. Swenson C, Bolcsak L, Batist G, et al: Pharmacokinetics of doxorubi-cin administered i.v. as Myocet (TLC D-99; liposome-encapsulateddoxorubicin citrate) compared with conventional doxorubicin whengiven in combination with cyclophosphamide in patients with meta-static breast cancer. Anticancer Drugs 14:239-246, 2003
49. Chan S, Davidson N, Juozaityte E, et al: Phase III study of liposome-encapsulated doxorubicin (TLC D-99) and cyclophosphamide (CPA)vs. epirubicin (EPI) and CPA in first-line treatment of metastatic breastcancer (MBC). Abstracts and Proceedings from ECCO 1999 (Abstract:1263). Eur J Cancer 35:315, 1999
50. Harris L, Batist G, Belt R, et al: Liposome-encapsulated doxorubicincompared with conventional doxorubicin in a randomized multi-center trial as first-line therapy of metastatic breast carcinoma. Cancer94:25-36, 2002
51. Williams G, Cortazar P, Pazdur R: Developing drugs to decrease thetoxicity of chemotherapy. J Clin Oncol 19:3439-3441, 2001
52. Storm G, Kate M, Working P, et al: Doxorubicin entrapped in steri-cally stabilized liposomes: Effects on bacterial blood clearance capac-ity of the mononuclear phagocyte system. Clin Cancer Res 4:111-115,1998
53. Symon Z, Peyser A, Tzemach D, et al: Selective delivery of doxorubicinto patients with breast carcinoma metastases by stealth liposomes.Cancer 86:72-78, 1999
54. O’Brien M, Wigler ??, Inbar N, et al. Reduced cardiotoxicity and com-parable efficacy in a phase III trial of pegylated liposomal doxorubicinHCl (CAELYX/Doxil) versus conventional doxorubicin for first-linetreatment of metastatic breast cancer. Ann Oncol 15:440-449, 2004
55. Theodoulou M, Campos S, Batist G, et al: TLC D99 (D, Myocet) andHerceptin (H) is safe in advanced breast cancer (ABC): Final cardiacsafety and efficacy analysis. Proc Am Soc Clin Oncol 21:55a, 2002(abstr 216)
56. Jones V, Finucane D, Rodriguez R, et al: Phase II study of weeklypaclitaxel (Taxol) and liposomal doxorubicin (Doxil) in patients withlocally advanced and metastatic breast cancer. Proc Am Soc Clin On-col 19:116a, 2000 (abstr 451)
57. Gogas H, Papadimitriou C, Kalofonos H, et al: Neoadjuvant chemo-therapy with a combination of pegylated liposomal doxorubicin (Cae-lyx) and paclitaxel in locally advanced breast cancer: A phase II studyby the Hellenic Cooperative Oncology Group. Ann Oncol 13:1737-1742, 2002
58. Slamon D, Leyland-Jones B, Shak S, et al: Use of chemotherapy plus amonoclonal antibody against HER2 for metastatic breast cancer thatoverexpresses HER2. N Engl J Med 344:783-792, 2001
59. Billingham M, Bristow M: Evaluation of endomyocardial cardiotoxic-ity: predictive ability and functional correlation of endomyocardialbiopsy. Cancer Treat Symp 3:71-76, 1984
60. Bristow M, Mason J, Billingham M, et al: Doxorubicin cardiomyopa-thy: Evaluation by phonocardiography, endomyocardial biopsy, andcardiac catheterization. Ann Intern Med 88:168-175, 1978
61. Friedman M, Bozdech M, Billingham M, et al: Doxorubicin cardiotox-
icity. Serial endomyocardial biopsies and systolic time intervals. JAMA240:1603-1606, 1978
62. Ewer M, Ali M, Mackay B. A comparison of cardiac biopsy grades andejection fraction estimation in patients receiving adriamycin. J ClinOncol 2:112-117, 1984
63. Isner J, Ferrans V, Cohen S, et al: Clinical and morphologic cardiacfindings after anthracycline chemotherapy. Analysis of 64 patientsstudied at necropsy. Am J Cardiol 51:1167-1174, 1983
64. Schwartz R, McKenzie W, Alexander J, et al: Congestive heart failureand left ventricular dysfunction complicating doxorubicin therapy.Seven-year experience using serial radionuclide angiocardiography.Am J Med 82:1109-1118, 1987
65. Mitani I, Jain D, Joska T, et al: Doxorubicin cardiotoxicity: Preventionof congestive heart failure with serial cardiac function monitoring withequilibrium radionuclide angiocardiography in the current era. J NuclCardiol 10:132-139, 2003
66. Ganz W, Sridhar K, Forness T: Detection of early anthracycline car-diotoxicity by monitoring the peak filling rate. Am J Clin Oncol 16:109-112, 1993
67. Stoddard M, Seeger J, Liddell N, et al: Prolongation of isovolumetricrelaxation time as assessed by Doppler echocardiography predictsdoxorubicin-induced systolic dysfunction in humans. J Am Coll Car-diol 20:62-69, 1992
68. Hiroe M, Ohta Y, Fujita N, et al: Myocardial uptake of 111In monoclo-nal antimyosin Fab in detecting doxorubicin cardiotoxicity in rats.Morphological and hemodynamic findings. Circulation 86:1965-1972, 1992
69. Valdes Olmos R, Carrio I, Hoefnagel C, et al: High sensitivity of ra-diolabelled antimyosin scintigraphy in assessing anthracycline relatedearly myocyte damage preceding cardiac dysfunction. Nucl MedCommun 23:871-877, 2002
70. Carrio I, Lopez-Pousa A, Estorch M, et al: Detection of doxorubicincardiotoxicity in patients with sarcomas by indium-111-antimyosinmonoclonal antibody studies. J Nucl Med 34:1503-1507, 1993
71. Ohman E, Armstrong P, Christenson R, et al: Cardiac troponin Tlevels for risk stratification in acute myocardial ischemia. N Engl J Med335:1333-1341, 1996
72. Antman E, Tanasijevic M, Thompson B, et al. Cardiac-specific tropo-nin I levels to predict the risk of mortality in patients with acutecoronary syndromes. N Engl J Med 335:1342-1349, 1996
73. Lindahl B, Venge P, Wallentin L: Relation between troponin T and therisk of subsequent cardiac events in unstable coronary artery disease.Circulation 93:1651-1657, 1996
74. Herman E, Zhang J, Lipshultz S, et al: Correlation between serumlevels of cardiac troponin-T and the severity of the chronic cardiomy-opathy induced by doxorubicin. J Clin Oncol 17:2237-2243, 1999
75. Herman E, Zhang J, Rifai N, et al: The use of serum levels of cardiactroponin T to compare the protective activity of dexrazoxane againstdoxorubicin- and mitoxantrone-induced cardiotoxicity. Cancer Che-mother Pharmacol 48:297-304, 2001
76. Missov E, Calzolari C, Davy J, et al: Cardiac troponin I in patients withhematologic malignancies. Coron Artery Dis 8:537-541, 1997
77. Raderer M, Gabriela K, Weinlander G, et al: Serum troponin levels inadults undergoing anthracycline therapy. J Natl Cancer Inst 89:171,1997 (letter)
78. Lipshultz S, Rifai N, Sallan S, et al: Predictive value of cardiac troponinT in pediatric patients at risk for myocardial injury. Circulation 96:2641-2648, 1997
79. Kismet E, Varan A, Ayabakan C, et al: Serum troponin T levels andechocardiographic evaluation in children treated with doxorubicin.Pediatr Blood Cancer 42:220-224, 2004
80. Kremer L, Bastiaansen B, Offringa M, et al: Troponin T in the first 24hours after the administration of chemotherapy and the detection ofmyocardial damage in children. Eur J Cancer 38:686-689, 2002
81. Cardinale D, Sandri MT, Martinoni A, et al: Left ventricular dysfunc-tion predicted by early troponin I release after high-dose chemother-apy. J Am Coll Cardiol 36:517-522, 2000
82. Newby L, Goldmann B, Ohman E: Troponin: an important prognostic

1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Anticancer agents and cardiotoxicity 13
marker and risk-stratification tool in non-ST-segment elevation acutecoronary syndromes. J Am Coll Cardiol 41:31S-36S, 2003 (suppl S)
83. Yalamanchili K, Sukhija R, Aronow W, et al: Prevalence of increasedcardiac troponin I levels in patients with and without acute pulmo-nary embolism and relation of increased cardiac troponin I levels within-hospital mortality in patients with acute pulmonary embolism.Am J Cardiol 93:263-264, 2004
84. Ammann P, Maggiorini M, Bertel O, et al: Troponin as a risk factor formortality in critically ill patients without acute coronary syndromes.J Am Coll Cardiol 4:2004-2009, 2003
85. Chan S, Friedrichs K, Noel D, et al: Prospective randomized trial ofdocetaxel versus doxorubicin in patients with metastatic breast can-cer. J Clin Oncol 17:2341-2354, 1999
86. Sledge G, Neuberg D, Bernardo P, et al: Phase III trial of doxorubicin,paclitaxel, and the combination of doxorubicin and paclitaxel asfront-line chemotherapy for metastatic breast cancer: An Intergrouptrial (E1193). J Clin Oncol 21:588-592, 2003
87. Gianni L, Munzone E, Capri G, et al: Paclitaxel by 3-hour infusion incombination with bolus doxorubicin in women with untreated met-astatic breast cancer: High antitumor efficacy and cardiac effects in adose-finding and sequence-finding study. J Clin Oncol 13:2688-2699, 1995
88. Gehl J, Boesgaard M, Paaske T, et al: Combined doxorubicin andpaclitaxel in advanced breast cancer: Effective and cardiotoxic. AnnOncol 7:687-693, 1996
89. Gianni L, Vigano L, Locatelli A, et al: Human pharmacokinetic char-acterization and in vitro study of the interaction between doxorubicinand paclitaxel in patients with breast cancer. J Clin Oncol 15:1906-1915, 1997
90. Holmes F, Madden T, Newman R, et al: Sequence-dependent alter-ation of doxorubicin pharmacokinetics by paclitaxel in a phase I studyof paclitaxel and doxorubicin in patients with metastatic breast can-cer. J Clin Oncol 14:2713-2721, 1996
91. Gianni L, Capri G: Experience at the Instituto Nazionale Tumori withpaclitaxel in combination with doxorubicin in women with untreatedbreast cancer. Semin Oncol 24:S3-1-S3-3, 1997
92. Biganzoli L, Cufer T, Bruning P, et al: Doxorubicin-paclitaxel. A saferegimen in terms of cardiac toxicity in metastatic breast carcinomapatients. Results from a European Organization for Research andTreatment of Cancer multicenter trial. Cancer 97:40-45, 2003
93. Jassem J, Pienkowski T, Pluzanska A, et al: Doxorubicin and paclitaxelversus fluorouracil, doxorubicin, and cyclophosphamide as first-linetherapy for women with metastatic breast cancer: Final results of arandomized phase III multicenter trial. J Clin Oncol 19:1707-1715,2001
94. Bellot R, Robert J, Dieras V, et al: Taxotere does not change the phar-macokinetic profile of doxorubicin and doxorubincinol. Proc Am SocClin Oncol 12:221a, 1998 (abstr 853)
95. Schuller J, Czejka M, Kletzl H, et al: Doxorubicin and Taxotere: Apharmacokinetic study of the combination in advanced breast cancer.Proc Am Soc Clin Oncol 17:205a, 1998 (abstr 790)
96. Nabholtz J-M, Falkson C, Campos D, et al: Docetaxel and doxorubicincompared with doxorubicin and cyclophosphamide as first-line che-motherapy for metastatic breast cancer: Results of a randomized, mul-ticenter, phase III trial. J Clin Oncol 21:968-975, 2003
97. Mackey J, Paterson A, Dirix L, et al: Final results of the phase IIIrandomized trial comparing docetaxel (T), doxorubicin (A) and cy-clophosphamide (C) to FAC as first-line chemotherapy (CT) for pa-tients (pts) with metastatic breast cancer (MBC). Proc Am Soc ClinOncol 21:137, 2002 (abstr 137)
98. Martin M, Pienkowski T, Mackey J, et al: Adjuvant docetaxel fornode-positive breast cancer. N Engl J Med 352:2302-2313, 2005
99. Luck H, Thomssen C, Untch M, et al: Multicentric phase III study infirst line treatment of advanced metastatic breast cancer (ABC): epi-rubicin/paclitaxel (ET) vs epirubicin/cyclophosphamide (EC). Astudy of the AGO Breast Cancer Group. Proc Am Soc Clin Oncol19:73, 2000 (abstr 280)
00. Sessa C, Pagani O: Docetaxel and epirubicin in advanced breast can-
cer. Oncologist 6: 13-16, 2001 101. Slamon D, Clark G, Wong S, et al: Human breast cancer: Correlationof relapse and survival with amplification of the HER-2/neu oncogene.Science 235:177-182, 1987
02. Cobleigh M, Vogel C, Tripathy D, et al: Multinational study of theefficacy and safety of humanized anti-HER2 monoclonal antibody inwomen who have HER2-overexpressing metastatic breast cancer thathas progressed after chemotherapy for metastatic disease. J Clin Oncol17:2639-2648, 1999
03. Vogel C, Cobleigh M, Tripathy D, et al: Efficacy and safety of trastu-zumab as a single agent in first-line treatment of HER2-overexpressingmetastatic breast cancer. J Clin Oncol 20:719-726, 2002
04. Baselga J, Tripathy D, Mendelsohn J, et al: Phase II study of weeklyintravenous recombinant humanized anti-p185HER2 monoclonalantibody in patients with HER2/neu-overexpressing metastatic breastcancer. J Clin Oncol 14:737-744, 1996
05. Seidman A, Hudis C, Pierri MK, et al: Cardiac dysfunction in thetrastuzumab clinical trials experience. J Clin Oncol 20:1215-1221,2002
06. Tripathy D, Slamon D, Cobleigh M et al: Safety of treatment of meta-static breast cancer with trastuzumab beyond disease progression.J Clin Oncol 22:1063-1070, 2004
07. Schneider JW, Chang AY, Garratt A: Trastuzumab cardiotoxicity:Speculations regarding pathophysiology and targets for further study.Semin Oncol 3:22-28, 2002 (suppl 11)
08. Crone SA, Zhao YY, Fan L, et al: ErbB2 is essential in the prevention ofdilated cardiomyopathy. Nat Med 8:459-465, 2002
09. Behr T, Behe M, Wormann B, et al: Trastuzumab and breast cancer.N Engl J Med 345:995-998, 2001
10. Burstein H, Harris L, Marcom P, et al: Trastuzumab and vinorelbine asfirst-line therapy for HER2-overexpressing metastatic breast cancer:Multicenter phase II trial with clinical outcomes, analysis of serumtumor markers as predictive factors, and cardiac surveillance algo-rithm. J Clin Oncol 21:2889-2895, 2003
11. Pegram M, Pienkowski T, Northfelt D, et al: Results of two open-label,multicenter phase II studies of docetaxel, platinum salts, and trastu-zumab in HER2-positive advanced breast cancer. J Natl Cancer Inst96:759-769, 2004
12. Montemurro F, Choa G, Faggiuolo R, et al: A phase II study of three-weekly docetaxel and weekly trastuzumab in HER2-overexpressingadvanced breast cancer. Oncology 66:38-45, 2004
13. Esteva F, Valero V, Booser D, et al: Phase II study of weekly docetaxeland trastuzumab for patients with HER-2-overexpressing metastaticbreast cancer. J Clin Oncol 20:1800-1808, 2002
14. Tedesco K, Thor A, Johnson D, et al: Docetaxel combined with tras-tuzumab is an active regimen in HER-2 3� overexpressing and fluo-rescent in situ hybridization-positive metastatic breast cancer: Amulti-institutional phase II trial. J Clin Oncol 22:1071-1077, 2004
15. Piccart-Gebhart M, Procter M, Leyland-Jones B, et al: Trastuzumabafter adjuvant chemotherapy in HER2-positive breast cancer. N EnglJ Med 353:1659-1672, 2005
16. Romond E, Perez E, Bryant J, et al: Trastuzumab plus adjuvant che-motherapy for operable HER2-positive breast cancer. N Engl J Med353:1673-1684, 2005
17. Perez E, Suman V, Davidson N, et al: Interim cardiac safety analysis ofNCCTG N9831 Intergroup adjuvant trastuzumab trial. Proc Am SocClin Oncol 23:16S, 2005 (abstr 556)
18. Tan-Chiu E, Yothers G, Romond E, et al: Assessment of cardiac dys-function in a randomized trial comparing doxorubicin and cyclophos-phamide followed by paclitaxel, with or without trastuzumab as ad-juvant therapy in node-positive, human epidermal growth factorreceptor 2-overexpressing breast cancer: NSABP B-31. J Clin Oncol23:7811-7819, 2005
19. Ewer M, Vooletich M, Durand J, et al: Reversibility of trastuzumab-related cardiotoxicity: New insights based on clinical course and re-sponse to medical treatment. J Clin Oncol 23:7820-7826, 2005
20. Jensen BV, Skovsgaard T, Nielsen SL: Functional monitoring of an-thracycline cardiotoxicity: A prospective, blinded, long-term observa-tional study of outcome in 120 patients. Ann Oncol 13:699-709, 2002
21. The SOLVD Investigators: Effect of enalapril on mortality and the

1
1
1
1
1
1
1
1
14 R. Ng, N. Better, and M.D. Green
development of heart failure in asymptomatic patients with reducedleft ventricular ejection fractions. N Engl J Med 327:685-689, 1992
22. Yusuf S, Sleight P, Pogue J, et al: Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk pa-tients. The Heart Outcomes Prevention Evaluation Study Investiga-tors. N Engl J Med 342:145-153, 2000
23. Hjalmarson A, Goldstein S, Fagerberg B, et al: Effects of controlled-release metoprolol on total mortality, hospitalizations, and well-beingin patients with heart failure: The Metoprolol CR/XL RandomizedIntervention Trial in congestive heart failure (MERIT-HF). MERIT-HFStudy Group. JAMA 283:1295-1302, 2000
24. Packer M, Fowler M, Roecker E, et al: Effect of carvedilol on themorbidity of patients with severe chronic heart failure: Results ofthe Carvedilol Prospective Randomized Cumulative Survival (CO-PERNICUS) study. Circulation 106:2194-2199, 2002
25. CIBIS-II Investigators and Committees: The Cardiac Insufficiency
Bisoprolol Study II (CIBIS-II): A randomised trial. Lancet 353:9-13,1999
26. Remme W, Riegger G, Hildebrandt P, et al: The benefits of earlycombination treatment of carvedilol and an ACE-inhibitor in mildheart failure and left ventricular systolic dysfunction. The Carvediloland ACE-Inhibitor Remodelling Mild Heart Failure Evaluation Trial(CARMEN). Cardiovasc Drugs Ther 18:57-66, 2004
27. Pitt B, Zannad F, Remme W, et al: The effect of spironolactone onmorbidity and mortality in patients with sever heart failure: Random-ized Aldactone Evaluation Study Investigators. N Engl J Med 341:709-717, 1999
28. Lipshultz S, Lipsitz S, Sallan S, et al: Long-term enalapril therapy forleft ventricular dysfunction in doxorubicin-treated survivors of child-hood cancer. J Clin Oncol 20:4517-4522, 2002
29. Silber J, Cnaan A, Clark B, et al: Enalapril to prevent cardiac functiondecline in long-term survivors of pediatric cancer exposed to anthra-
cyclines. J Clin Oncol 22:820-828, 2004