Embed Size (px)
Citation preview
Antibiotics:Only Part of the Story
Gina Suh, MD/ Mayo clinic
May 10 20182019 California Orthopaedic Association Annual Meeting
May 16-19, 2019

I have no disclosures

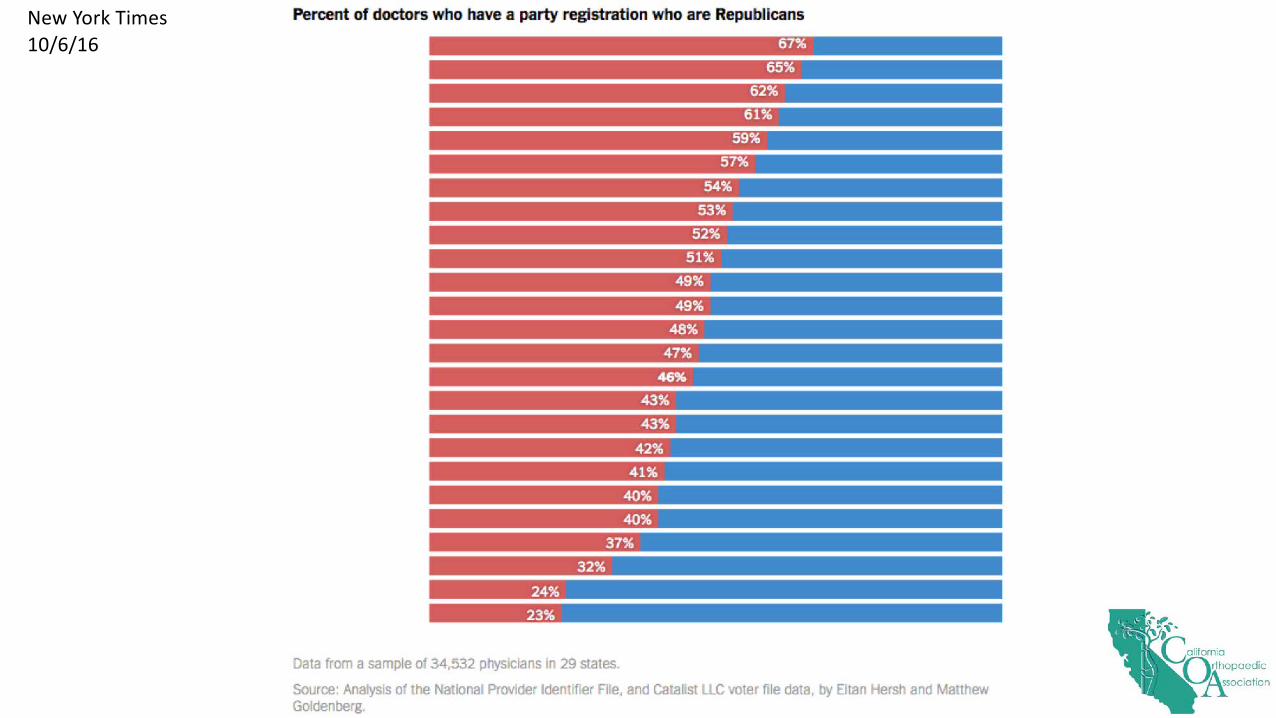
New York Times10/6/16
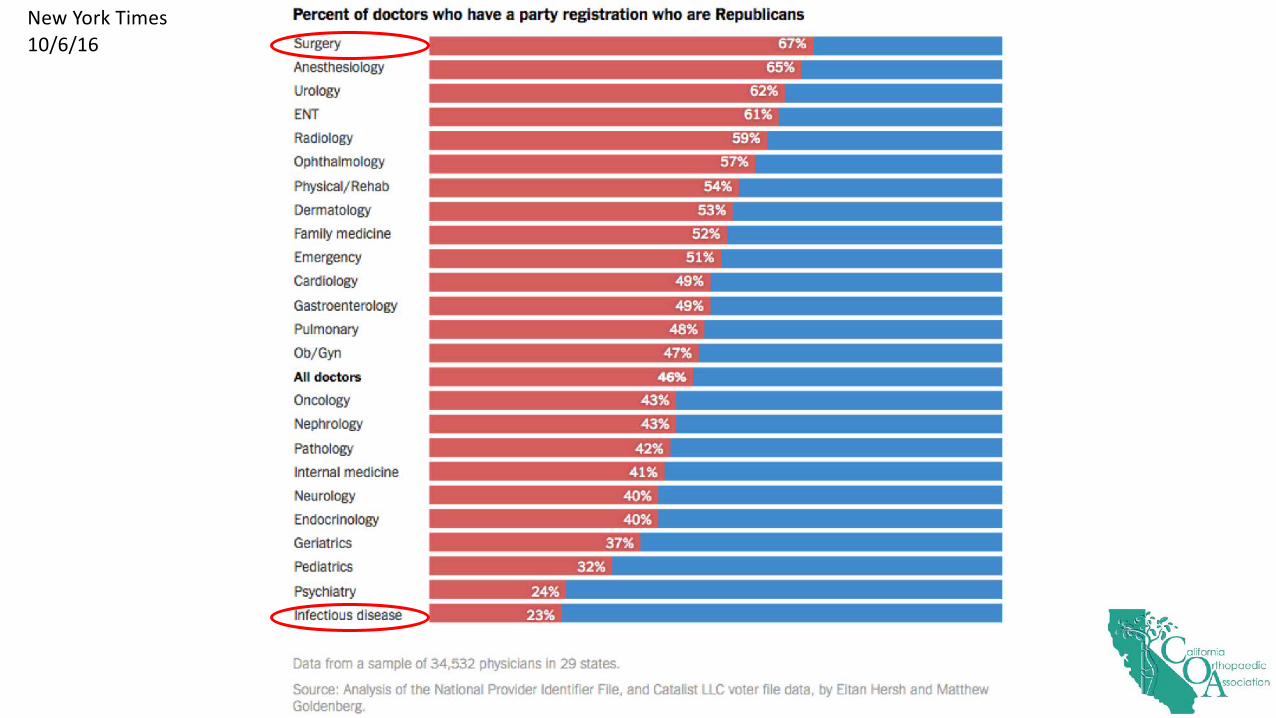
New York Times10/6/16
Hatfields vs. McCoys
Hatfields vs. McCoys
Just take out the hardware!
How hard could it be?
Just suppress for life! How hard could it
be?

MSK infections
• By nature a multi-disciplinary problem• Eradication of infection may not be
best for preserving structure, function, and stability
• Preserving structure, function, and stability may not be best for eradicating the infection
• Not a lot of data – but this is getting better
The Role of the Ortho-ID Physician
TOLD FROM THE PERSPECTIVE OF AN ORTHO-ID DOC
• To give a nuanced recommendation• To understand the surgical perspective• To understand the surgical procedure• More than just bug and drug
Today’s Talk
• But first I will start with “The Bug and the Drug”
• Local delivery - doses• DAIR• Duration of antibiotics• Chronic suppression
• Empiric antibiotics• While cultures are cooking• Culture-negative PJI
• Prophylaxis• Role of oral antibiotics• Some lessons• Novel therapeutics
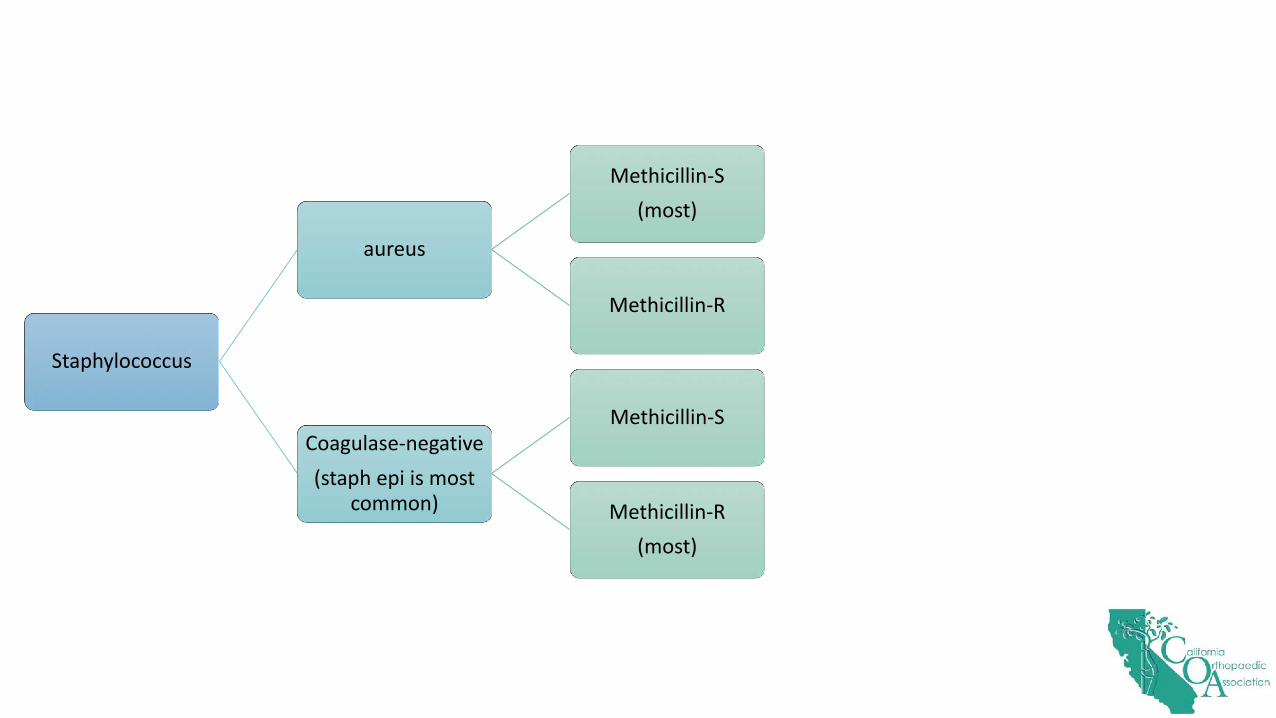
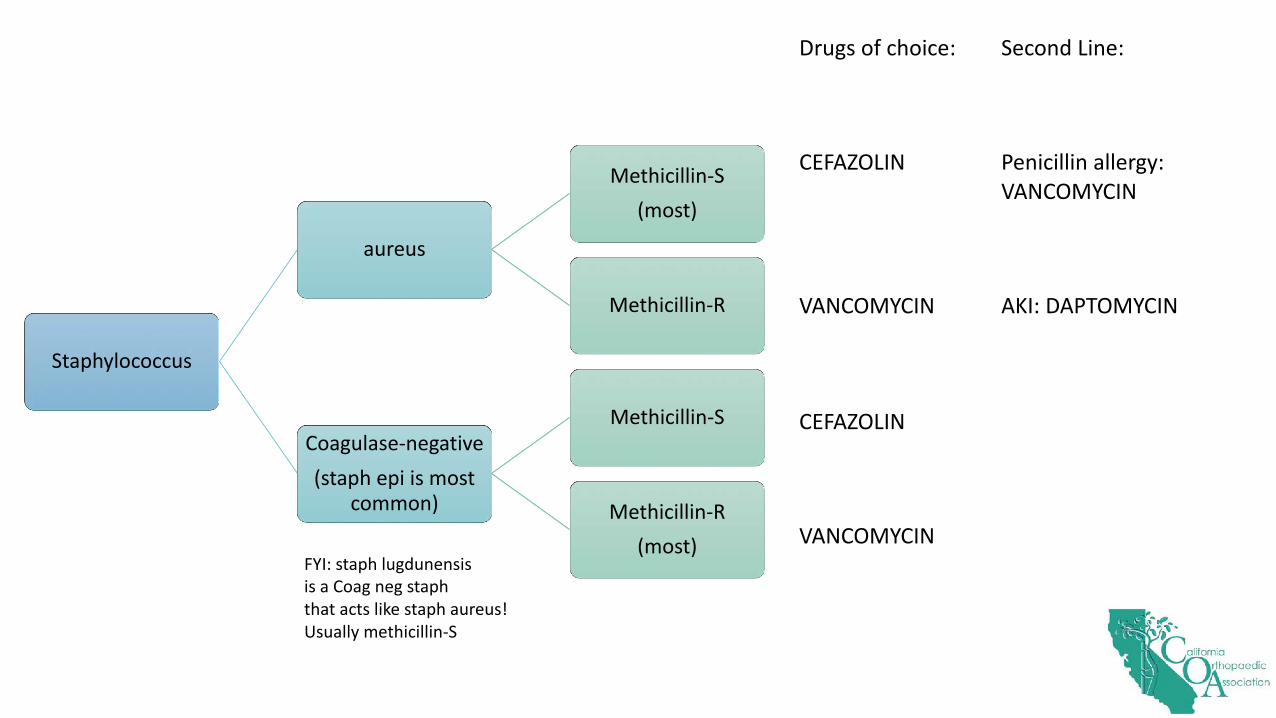
Staphylococcus
aureus
Methicillin-S(most)
Methicillin-R
Coagulase-negative(staph epi is most
common)
Methicillin-S
Methicillin-R(most)
Staphylococcus
aureus
Methicillin-S(most)
Methicillin-R
Coagulase-negative(staph epi is most
common)
Methicillin-S
Methicillin-R(most)
Drugs of choice:
CEFAZOLIN
VANCOMYCIN
CEFAZOLIN
VANCOMYCIN
Second Line:
Penicillin allergy:VANCOMYCIN
AKI: DAPTOMYCIN
FYI: staph lugdunensisis a Coag neg staphthat acts like staph aureus!Usually methicillin-S
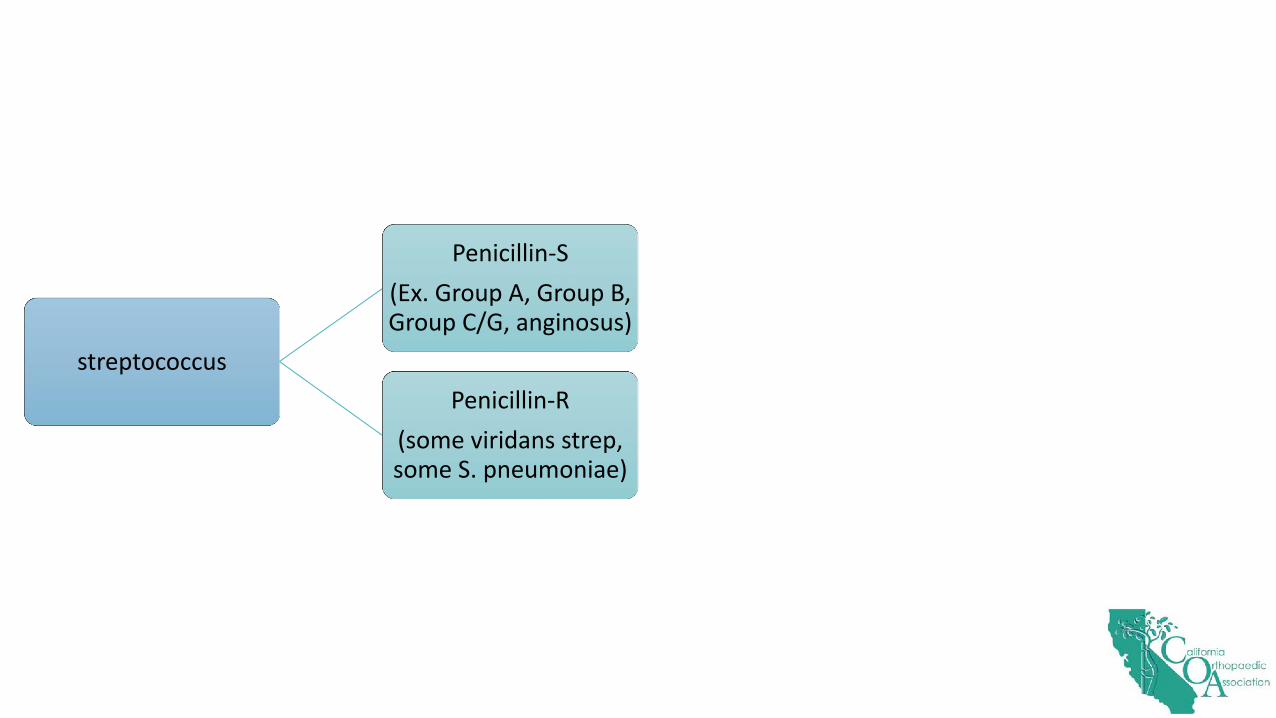
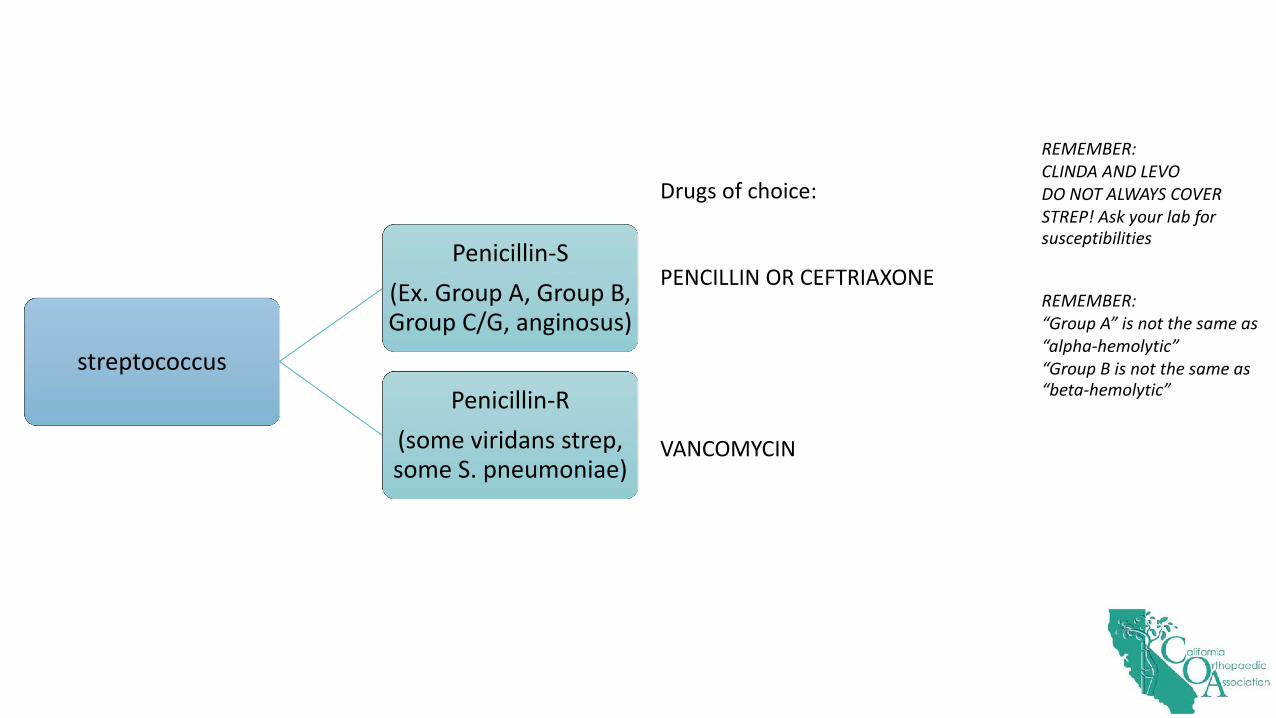
streptococcus
Penicillin-S(Ex. Group A, Group B, Group C/G, anginosus)
Penicillin-R(some viridans strep, some S. pneumoniae)
streptococcus
Penicillin-S(Ex. Group A, Group B, Group C/G, anginosus)
Penicillin-R(some viridans strep, some S. pneumoniae)
Drugs of choice:
PENCILLIN OR CEFTRIAXONE
VANCOMYCIN
REMEMBER:CLINDA AND LEVODO NOT ALWAYS COVERSTREP! Ask your lab forsusceptibilities
REMEMBER:“Group A” is not the same as“alpha-hemolytic”“Group B is not the same as“beta-hemolytic”
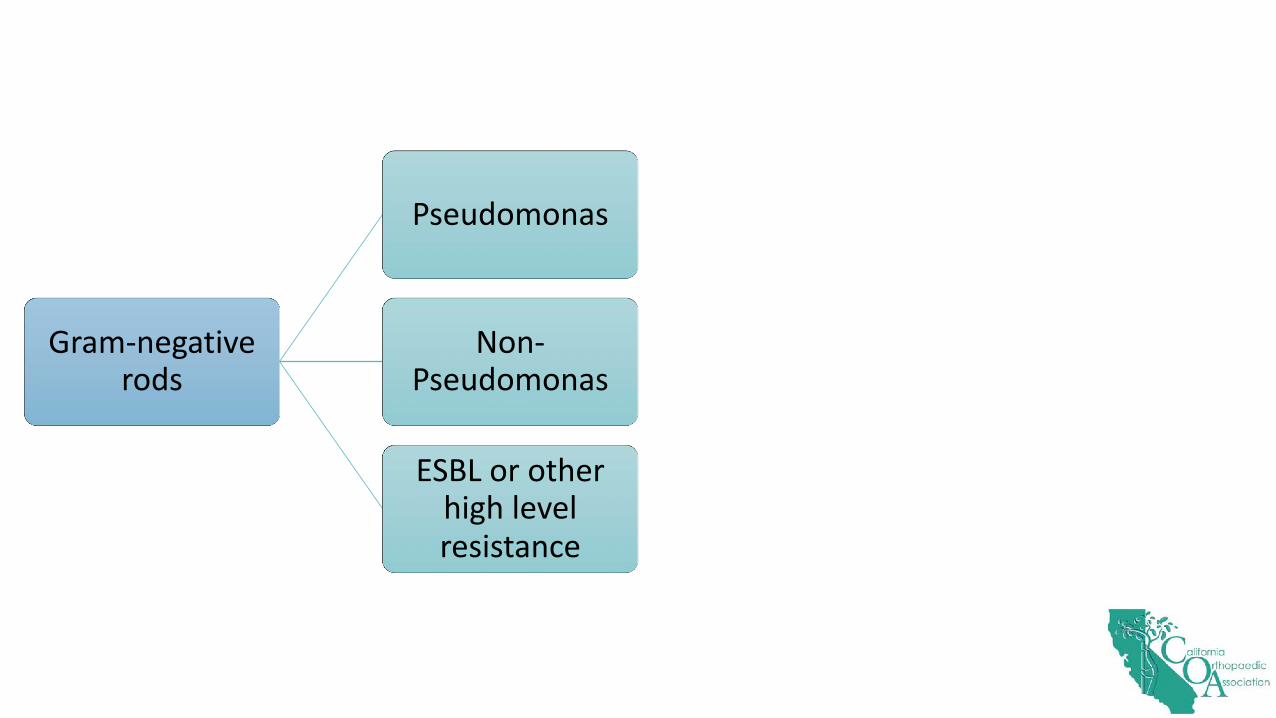
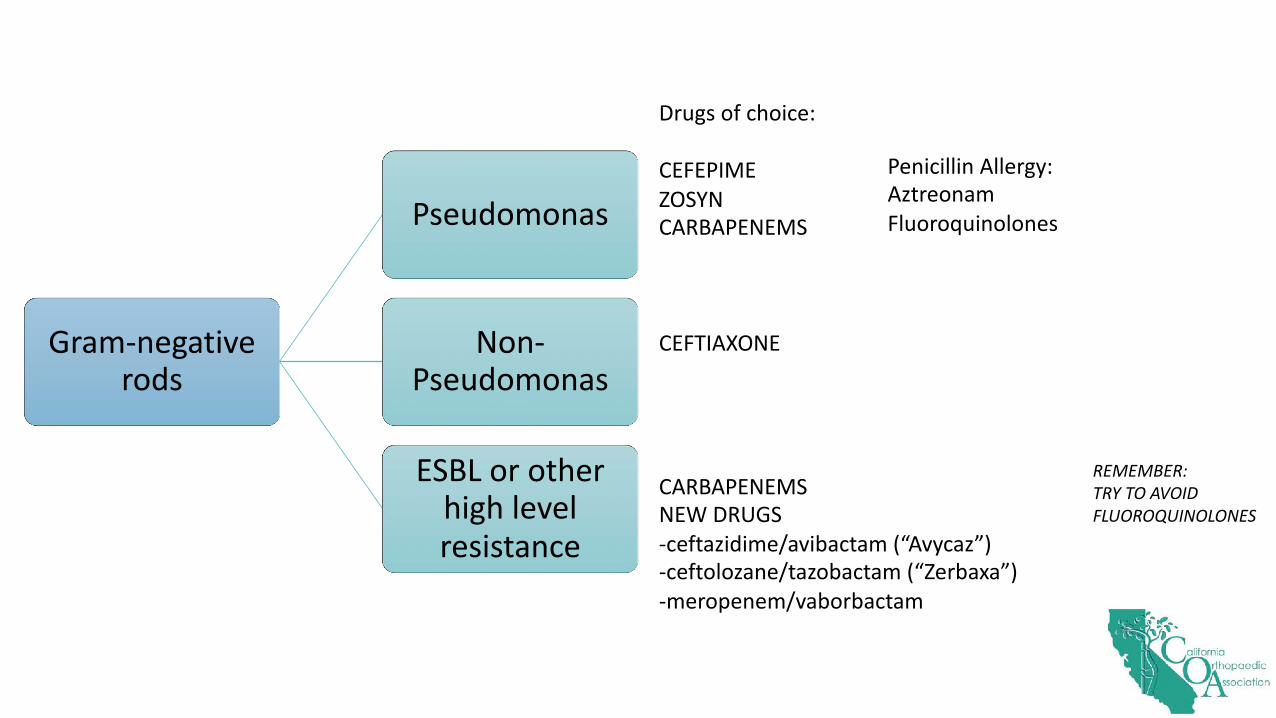
Gram-negative rods
Pseudomonas
Non-Pseudomonas
ESBL or other high level resistance
Gram-negative rods
Pseudomonas
Non-Pseudomonas
ESBL or other high level resistance
Drugs of choice:
CEFEPIME ZOSYNCARBAPENEMS
CEFTIAXONE
CARBAPENEMSNEW DRUGS -ceftazidime/avibactam (“Avycaz”)-ceftolozane/tazobactam (“Zerbaxa”)-meropenem/vaborbactam
REMEMBER:TRY TO AVOID FLUOROQUINOLONES
Penicillin Allergy:AztreonamFluoroquinolones

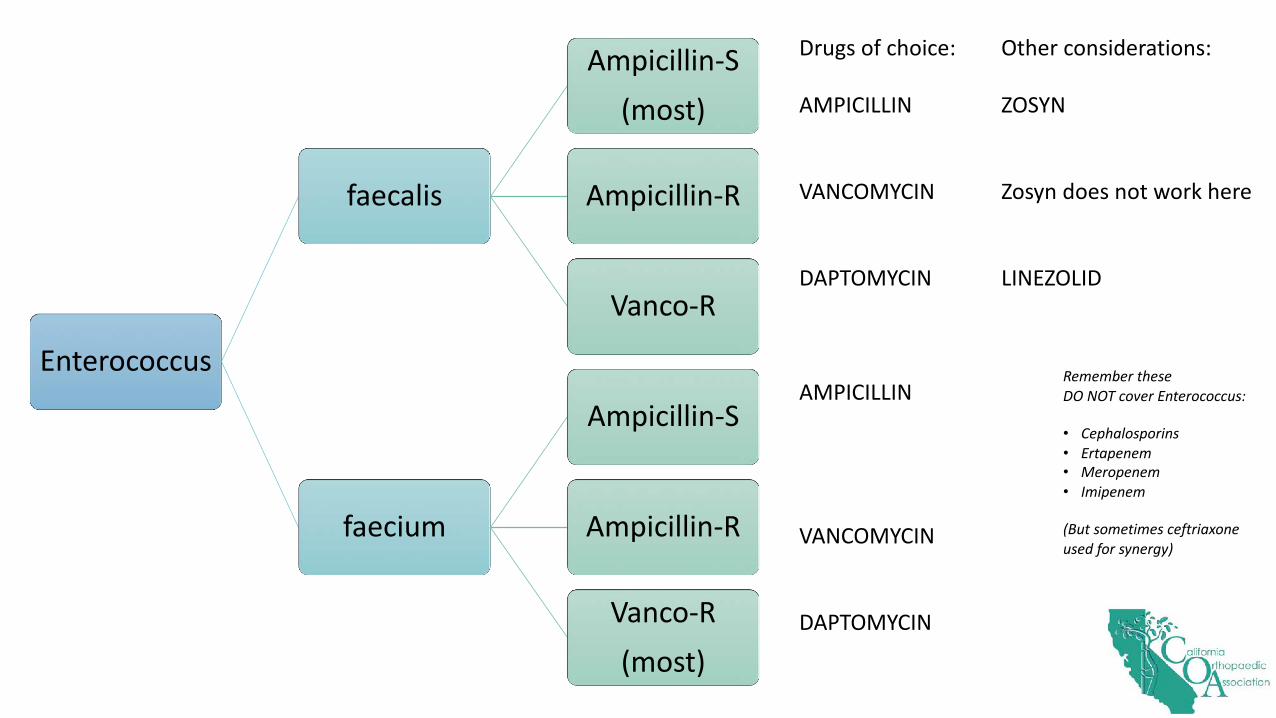
Enterococcus
faecalis
Ampicillin-S(most)
Ampicillin-R
Vanco-R
faecium
Ampicillin-S
Ampicillin-R
Vanco-R(most)
Enterococcus
faecalis
Ampicillin-S
(most)
Ampicillin-R
Vanco-R
faecium
Ampicillin-S
Ampicillin-R
Vanco-R
(most)
Drugs of choice:
AMPICILLIN
VANCOMYCIN
DAPTOMYCIN
AMPICILLIN
VANCOMYCIN
DAPTOMYCIN
Other considerations:
ZOSYN
Zosyn does not work here
LINEZOLID
Remember theseDO NOT cover Enterococcus:
• Cephalosporins• Ertapenem• Meropenem • Imipenem
(But sometimes ceftriaxone used for synergy)
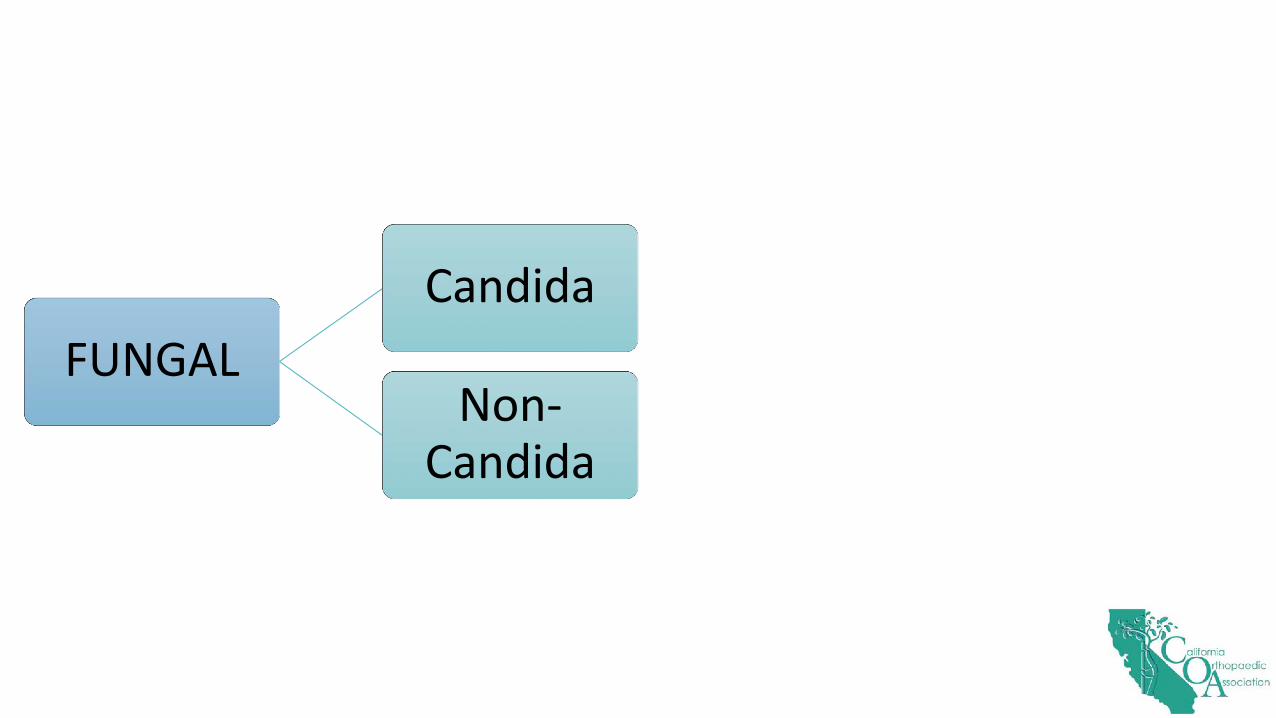
FUNGALCandida
Non-Candida

FUNGALCandida
Non-Candida
Drugs of choice:
Fluconazole – usually susceptibleCaspofungin – use until you have sensi’s if sick
Voriconazole – if AspergillusFluconazole or itraconazole – if coccidioidesFluconazole or itraconazole – if histoplasmosisFluconazole or itraconazole – if blastomycosis
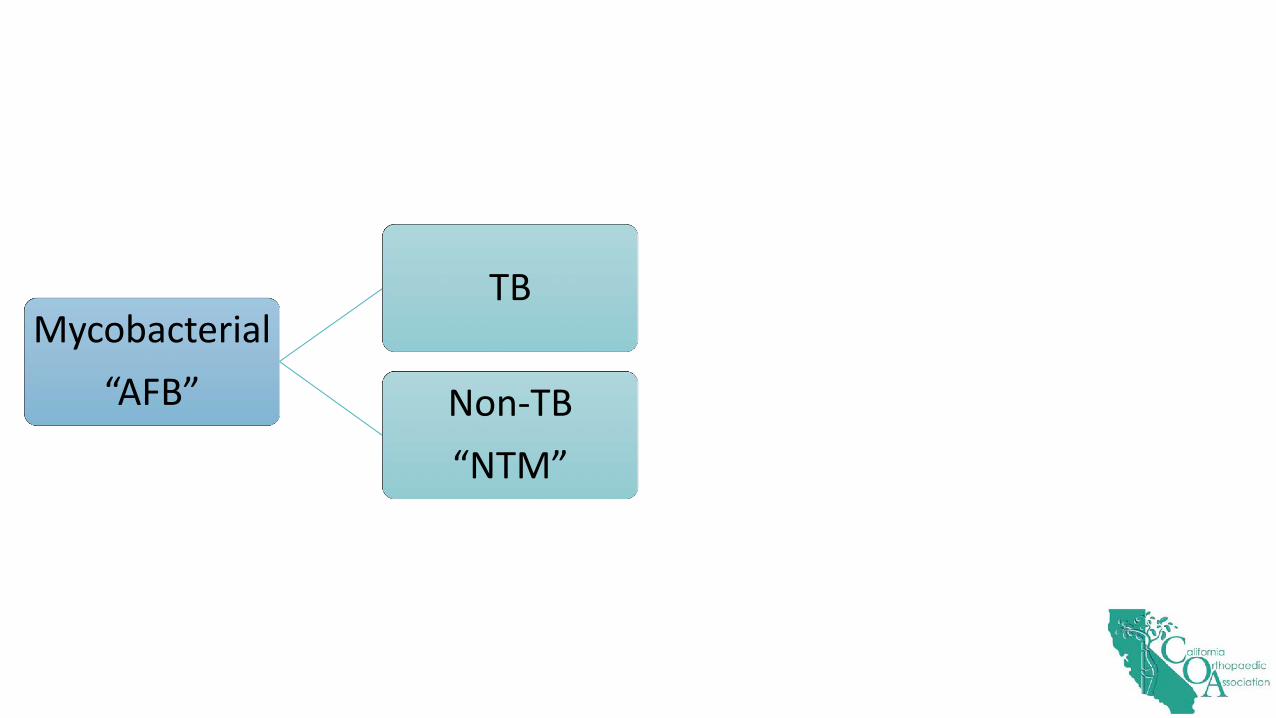
Mycobacterial“AFB”
TB
Non-TB“NTM”

Mycobacterial“AFB”
TB
Non-TB“NTM”
Drugs of choice:
Too complicated for this slide-MUST be multi-drug regimen
Too complicated for this slide-Hundreds of different species (ex. MAC, Mycobacterium abscessus, Mycobacterium chelonae, etc”)
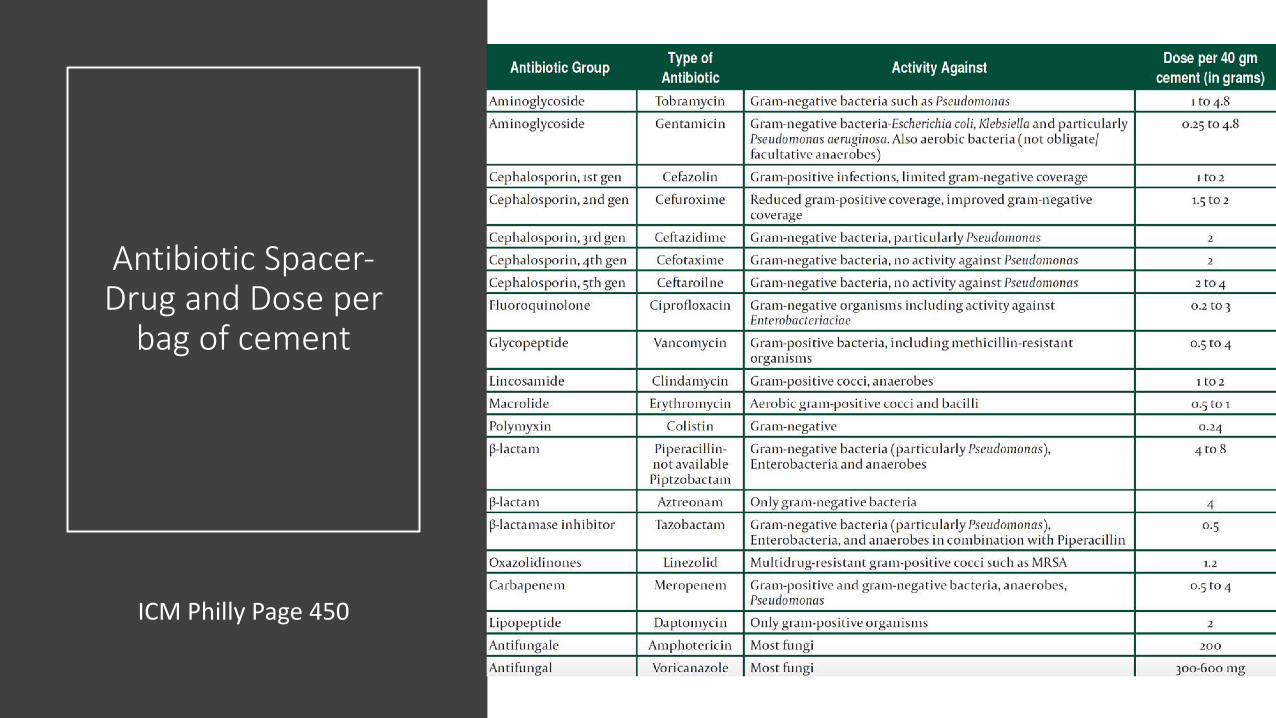
Antibiotic Spacer-Drug and Dose per
bag of cement
ICM Philly Page 450
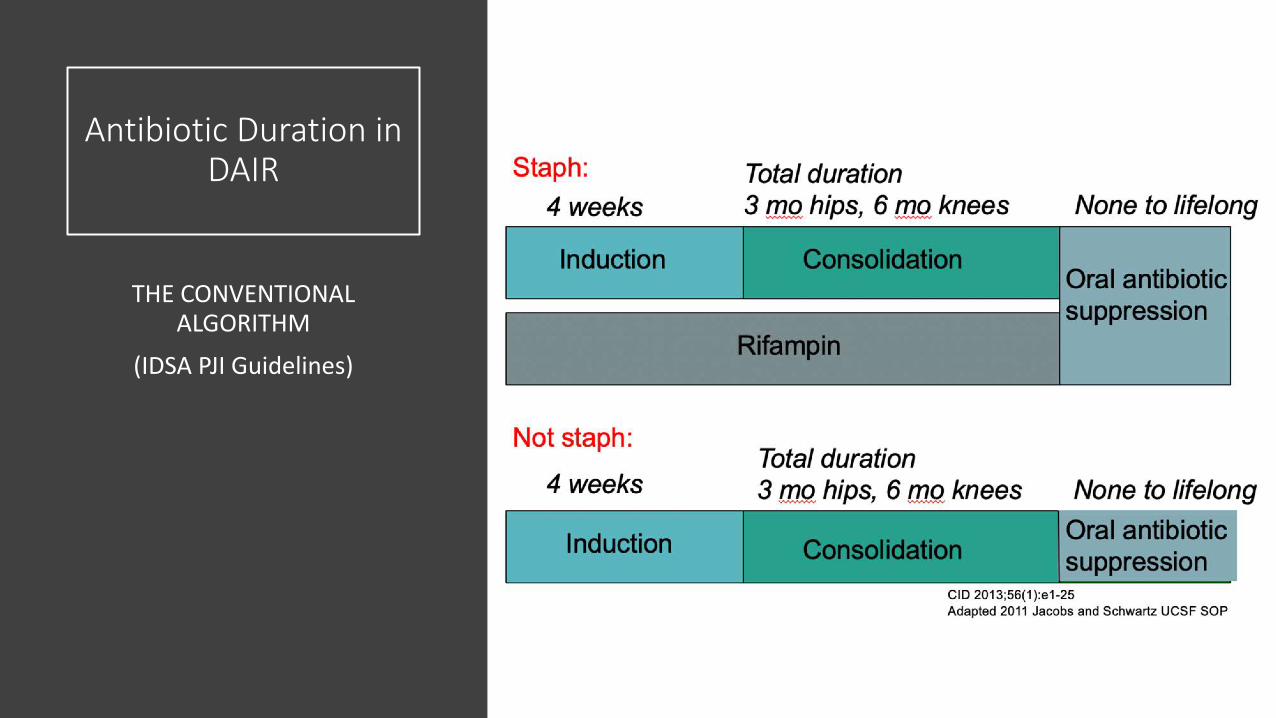
Antibiotic Duration in DAIR
THE CONVENTIONAL ALGORITHM
(IDSA PJI Guidelines)
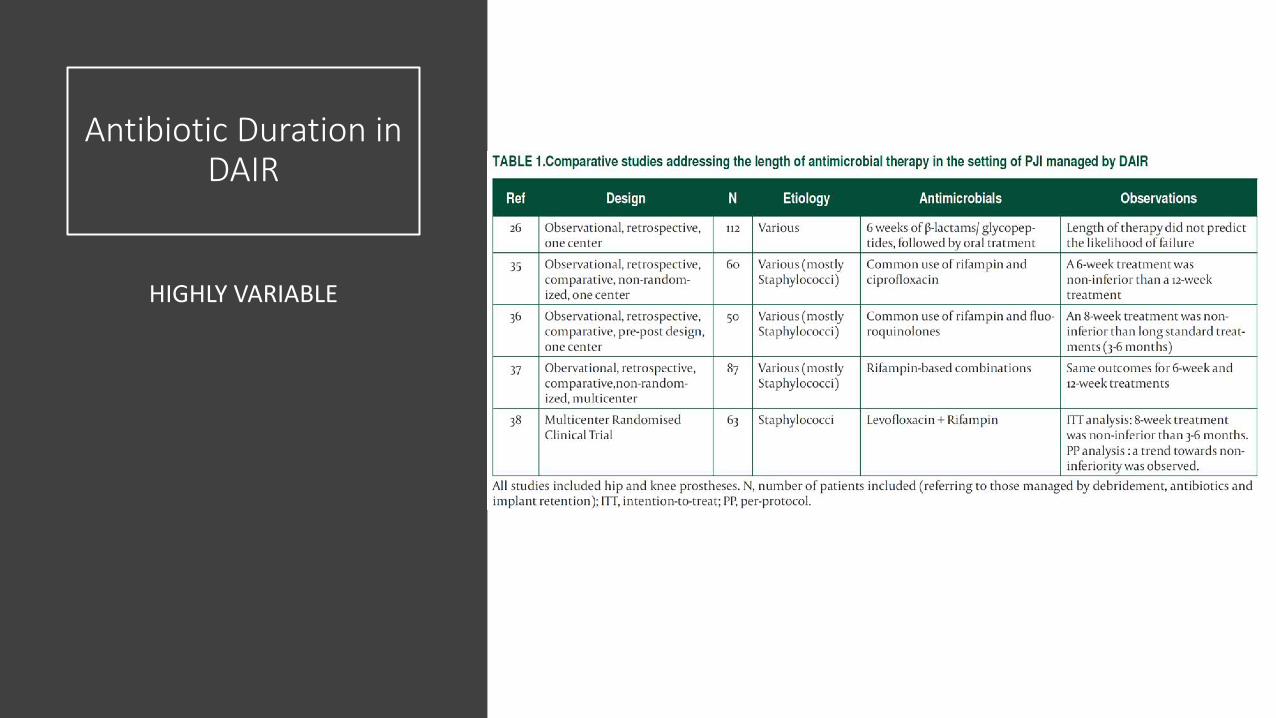
Antibiotic Duration in DAIR
HIGHLY VARIABLE
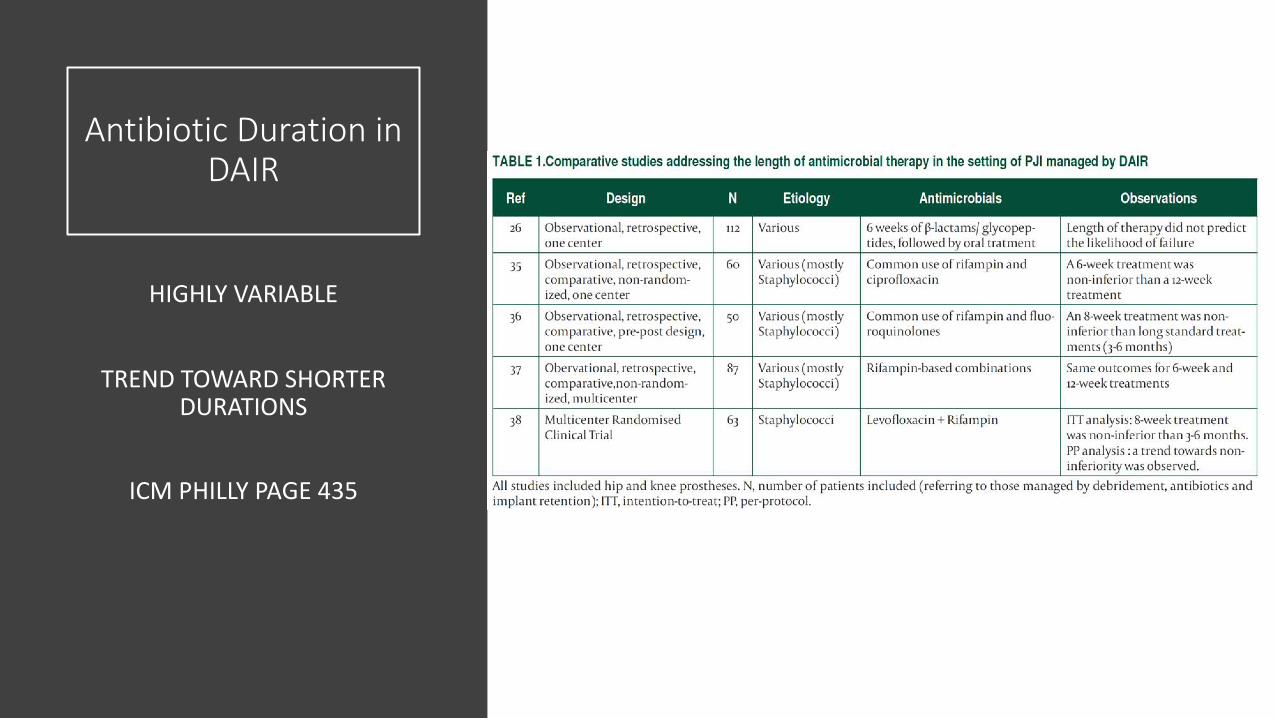
Antibiotic Duration in DAIR
HIGHLY VARIABLE
TREND TOWARD SHORTER DURATIONS
ICM PHILLY PAGE 435

Antibiotics for DAIR
GRAM NEG RODS
FUNGALAFB
• GNR: Beta-lactams or oral quinolones, durations generally shorter than GPC except Pseudomonas
• Fungal: Avoid DAIR• AFB: Avoid DAIR
Chronic Suppression
INDICATION
DURATION
PITFALLS
• Who gets chronic suppression?• Immunosuppressed• Inadequate debridement• Markers don’t normalize• Surgeon’s level of confidence• Consequences of failure
• How long?• VERY variable• My practice has been
• Staph 12-24 months• Strep 6 months• GNR 3-6 months• Candida Indefinite?
• This decision is made with YOU• Pitfalls
• They fail anyway• They fail anyway with a different and more resistant bug• C difficile – recurrent, never-ending, colostomy• Side effects: Renal failure, liver failure, lactic acidosis,
hyperkalemia and torsades, tendon rupture, tendonitis, decreased appetite, feeling lousy
Doxycycline
MY FAVORITE ANTIBIOTIC
• MSSA – highly likely (check sensi’s)
• MRSA – likely (check sensi’s)
• Strep – no
• Enterococcus – maybe (check sensi’s)
• E coli – maybe (check sensi’s)
• Pseudomonas – no
• Relatively non-toxic
• Lower rates of Clostridium difficile• Ok in renal failure
• Downsides:
• Photosensitivity
• GI upset and nausea

Empiric antibiotics after DAIR or stage-one of two stages
IMMEDIATELY POST-OP WHILE CULTURES ARE COOKING
• If they grew something in the past• Cover it!
• Broad-spectrum coverage• Vanco + Ceftriaxone• Vanco + Cefepime• Vanco + Ceftazidime• Empiric anaerobic coverage usually not needed• Avoid Vanco/Zosyn combination
• My approach: risk stratify• Start with vanco• Add Gram-negative coverage if they have risk
factors• Elderly• GI/GU issues (prostate, recurrent UTI)
Culture-negativePJI
COMMON REGIMENS
SOMETIMES IT’S SOMETHING WEIRD
• Vancomycin + ceftriaxone
• Vancomycin + cefepime
• Vancomycin + cipro
• Vancomycin + ertapenem/meropenem if high levels of MDR
• Avoid vanco/zosyn due to risk of AKI and difficulty with administration
• Unusual organisms not detectable by culture• Coxiella, Bartonella, Brucella, Mycoplasma
Extended Oral Prophylaxis Post
Re-implant
S/P RE-IMPLANT
INTRA-OP CULTURES NEG
• 2 retrospective studies and 1 RTC• Lower rates of failure in group treated with
oral prophylaxis for 3 months post-op• The failures were usually with a different
bug• There is further work to be done• Longer duration of follow up• Risk stratify
• Multiple previous failures• Retained osteomyelitis suspected• Host factors
Clin Orthop Relat Res. 2017 Jan;475(1):56-61.
OVIVA Trial
“Oral versus IV antibiotics”
A randomized control trial
• Multi-center out of UK
• 1,054 Bone and joint infections
• Randomly assigned to oral or IV 7 days
post-op or 7 days after start of abx if no
surgery indicated
• Primary endpoint: failure within 1 year
• Results: Failure 14.6% IV group 13.2% oral
group
• PO non-inferior to oral
• 1% adverse events PO group 9.3% oral
group
N Engl J Med 2019; 380:425-436
OVIVA Trial
CAVEATS
• Not a lot of staph infections
• Many streptococcal and gram-neg rods
• Not much beta-lactam use
• High levels fluoroquinolone use
• Fluoroquinolones (cipro/levo/moxi) have
been issued a black box warning for cardiac
adverse events, QT prolongation
• Clostridium difficile and tendon rupture are
major side effects
• Recommend avoidance of quinolones
N Engl J Med 2019; 380:425-436

SOME LESSONS
• Durations getting shorter and shorter• Antibiotics matter less than we like to think?• When you lift the antibiotic, the infection can recur, no matter the
duration• The debridement matters the most• But debridements are un-quantifiable• The reason why the guidelines are so conservative? They have to
“cover” all the debridements• Are debridement techniques becoming more refined?
The Real Game Changer
NEW THERAPIES
Slide modified from Paul Bollyky, with permission
Phage&biology&
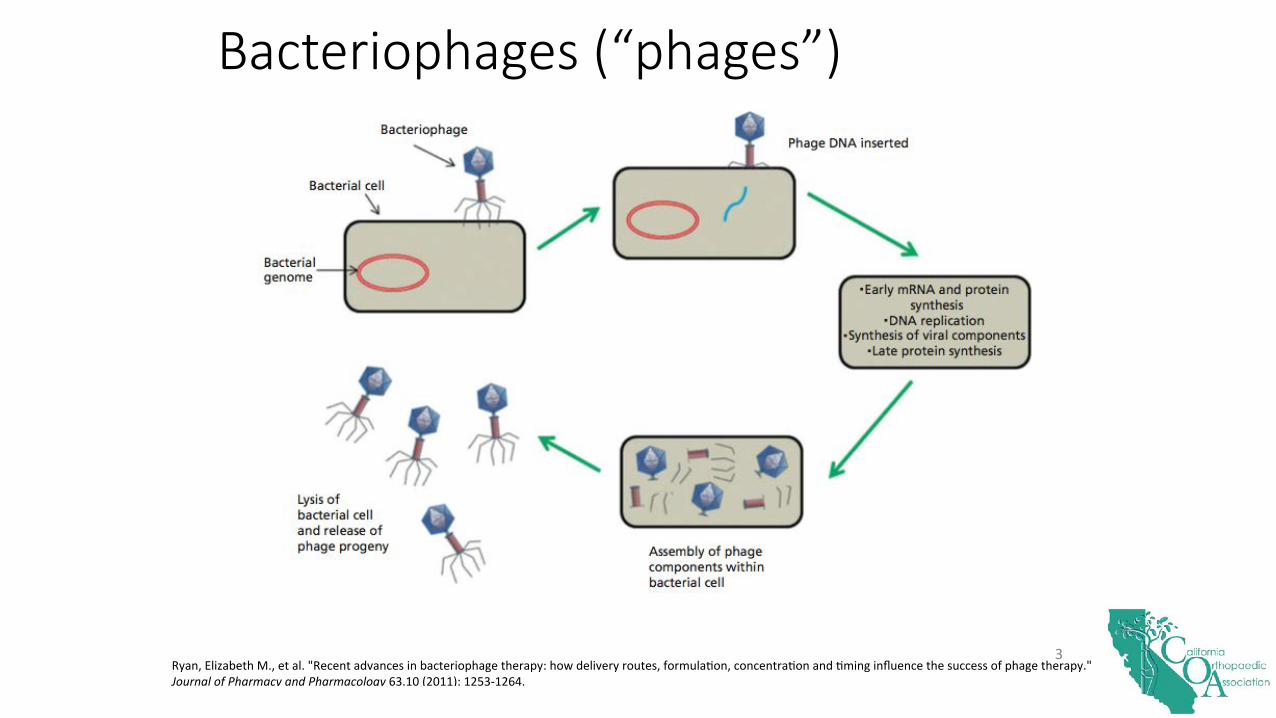
Ryan,&Elizabeth&M.,&et&al.&"Recent&advances&in&bacteriophage&therapy:&how&delivery&routes,&formulaMon,&concentraMon&and&Mming&influence&the&success&of&phage&therapy."&Journal(of(Pharmacy(and(Pharmacology&63.10&(2011):&1253R1264.&&
3&
Bacteriophages (“phages”)
A Potential Solution: Bacteriophage Therapy
• Viruses that target bacteria• Highly specific• Low systemic dose• Low toxicity
Slide courtesy Paul Bollyky

Thanks for your attention!!!

























![A Gearbox Story r6c1 [Read-Only]](https://img.dokumen.tips/doc/110x75/5695cf961a28ab9b028eb414/a-gearbox-story-r6c1-read-only.jpg)



