Embed Size (px)
Citation preview

964
Chapter
83Antibiotics in the Management of Serious Hospital-Acquired InfectionsMollie Gowan, Jennifer Bushwitz, and Marin h. Kollef
IntroductIon
As antimicrobial resistance spreads and new antimicrobial agents are developed, designing an empiric antibiotic regi-men for patients in the intensive care unit (ICU) has become increasingly complex. In order to ensure that the initial anti-biotic agents chosen are appropriate, clinicians must consider a variety of risk factors for infection with resistant pathogens that are specific to the patient, hospital, and community, as well as drug-specific properties that affect efficacy at the site of infection. Although recently developed rapid diagnostic tech-niques and biomarkers may aid in optimizing antimicrobial therapy, these technologies are not currently widely available. This chapter not only reviews factors predisposing patients to infection with resistant organisms and available diagnostic tests to streamline antibiotic therapy, but also discusses strate-gies to improve antimicrobial stewardship and limit the spread of resistance.
PAtHoPHySIology
Clinical Factors That Affect Initial Antimicrobial Selection
When developing an empirical antimicrobial regimen, choice of agents should be based on multiple factors, including likely causative pathogens, local pathogen distribution, resis-tance patterns, and patient-specific risk factors for resistance. Reports from the National Nosocomial Infections Surveillance (NNIS) System describe hospital and ICU infection rates in par-ticipating acute care general hospitals throughout the United States. A 2005 publication also reported pathogen distribution by site of infection and compared data from 1975 and 2003, as shown in Table 83.1. Overall, the occurrence of hospital-acquired infections caused by potentially resistant bacteria, such as Staphylococcus aureus and Pseudomonas aeruginosa, is increasing. In hospital-acquired pneumonia, gram-negative aerobes remain the most frequently reported pathogens; how-ever, S. aureus was the most frequently reported single species (1,2). A 2013 report published by the National Healthcare Safety Network (NHSN) demonstrated that S. aureus was, overall, the pathogen isolated most frequently in hospital-acquired infections from 2009 to 2010. S aureus was also the predominant pathogen in ventilator-associated pneumonia (VAP), followed by P. aeruginosa and Klebsiella species (3).
One of the most concerning trends reported in the NNIS data is the increasing isolation of Acinetobacter species in uri-nary tract infections, pneumonia, and surgical site infections (1,2,5). Although overall numbers of isolates of Acinetobacter are still relatively small (approximately 2.0%), the percentage
increase is significant. Similarly, the NHSN report showed that Acinetobacter was the fifth most common pathogen iso-lated in VAP (3). Even more concerning is the recent report of community-acquired pneumonia (CAP) now attributed to Acinetobacter species, suggesting that this pathogen is extend-ing its area of influence outside of the health care setting (6).
Also disconcerting is the observation made by the NNIS report that for each of the antibiotic–pathogen combinations tested, there was a significant increase in resistance between study periods. Most impressive were trends in carbapenem- and cephalosporin-resistant P. aeruginosa and Acinetobacter species (1,2). The NHSN data demonstrate that over 60% of tested Acinetobacter isolates in VAP were resistant to imipenem and meropenem, and an even greater percentage met the definition of multidrug resistant (MDR) (3). Many isolates lack effective treatment options and represent a serious public health concern (2,7). Rates of carbapenem resistance, up to 30% in P. aerugi-nosa isolates and 12.8% in Klebsiella species, are concerning as these organisms are often MDR and have very limited treatment options in hospitals in the United States (3,4).
The prevalence of MDR pathogens varies by patient popu-lation, hospital, and type of floor or unit in which the patient resides, underscoring the need for local surveillance data. MDR pathogens are more commonly isolated from patients with severe, chronic underlying disease—for example, those with risk factors for health care–associated infection (Table 83.2) and patients with late-onset hospital-acquired infections. Spe-cifically, in patients with VAP, prolonged ventilation and recent antibiotic exposure have been identified as significant risk fac-tors for infection with MDR organisms (8).
Distribution of MDR pathogens has been shown to be highly variable not only between cities and countries but also among different ICUs within the same hospital (9–11). These data suggest that consensus guidelines for antimicrobial ther-apy will need to be modified at the local level (e.g., according to county, city, hospital, and ICU) to take into account local patterns of antimicrobial resistance. Additionally, it is help-ful for clinicians to appreciate local specific resistance rates of certain gram-negative pathogens such as extended- spectrum β-lactamase (ESBL)-producing Klebsiella pneumoniae or Escherichia coli, fluoroquinolone-resistant P. aeruginosa, or carbapenem-resistant Acinetobacter baumannii. When risk of these pathogens is identified, empirical therapy must be tailored accordingly.
In addition to local or regional variance, numerous patient-specific factors affect the risk of isolation of a resistant patho-gen. Therefore, the choice of empiric antibiotic agents should be based on local patterns of antimicrobial susceptibility and must also take into account patient-specific characteris-tics that may influence the risk of infection with a resistant pathogen. Patients of particular concern are those at risk for
LWBK1580_C83_p964-981.indd 964 29/07/17 11:37 AM

Tabl
e 83
.1 R
ela
tive
Pe
rce
nta
ge
by
Site
of I
nfe
ctio
n o
f Pa
tho
ge
ns a
sso
cia
ted
with
No
soc
om
ial I
nfe
ctio
n (2
,4)
Path
og
en
Pne
umo
nia
bSI
SSI
UTI
Yea
r19
7519
89–1
998
2003
2009
–201
0a19
7519
89–1
998
2003
2009
–201
0b19
7519
89–1
998
2003
2009
–201
019
7519
89–1
998
2003
2009
–201
0c
Num
be
r4,
018
65,0
564,
365
6,63
21,
054
50,0
912,
351
27,7
667,
848
22,0
432,
984
16,0
1916
,434
47,5
024,
109
19,0
58
Sta
phy
loc
oc
cu
s a
ure
us
13.4
16.8
27.8
24.1
16.5
10.7
14.3
12.3
18.5
12.6
22.5
30.4
1.9
1.6
3.6
2.1
Pse
ud
om
on
as
ae
rug
ino
sa9.
616
.118
.116
.64.
83
3.4
3.8
4.7
9.2
9.5
5.5
9.3
10.6
16.3
11.3
Ente
roc
oc
cu
s su
bsp
ec
ies
31.
91.
30.
98.
110
.314
.518
.111
.914
.513
.911
.614
.213
.817
.415
.1
Ente
rob
ac
ter
sub
spe
cie
s9.
610
.710
8.6
64.
24.
44.
54.
68.
89
44.
75.
76.
94.
2
Esc
he
rich
ia c
oli
11.8
4.4
55.
915
2.9
3.3
417
.67.
16.
59.
433
.518
.226
26.8
Kle
bsie
lla
sub
spe
cie
s8.
46.
57.
210
.14.
52.
94.
27.
92.
73.
53
44.
66.
19.
811
.2
Serra
tia
sub
spe
cie
s2.
2—
4.7
4.6
2.6
—2.
32.
50.
5—
21.
81.
4—
1.6
1
Ac
ine
tob
ac
ter
spe
cie
s1.
5—
6.9
6.6
1.8
—2.
42.
10.
5—
2.1
0.6
0.6
—1.
60.
9
aVe
ntil
ato
r-ass
oc
iate
d p
ne
um
on
iabC
ath
ete
r-ass
oc
iate
d b
loo
dst
rea
m in
fec
tion
cC
ath
ete
r-ass
oc
iate
d u
rina
ry t
rac
t in
fec
tion
Bsi,
blo
od
stre
am
infe
ctio
n; s
si, s
urg
ica
l site
infe
ctio
n; u
ti, u
rina
ry t
rac
t in
fec
tion
; —, n
ot
rep
ort
ed
.
965
LWBK1580_C83_p964-981.indd 965 29/07/17 11:37 AM

966 SeCtion 9 infeCtious Disease
hospital-acquired infections caused by S. aureus, P. aerugi-nosa, and Acinetobacter species due to the high frequency with which they cause infection, their resistance to numerous antibiotics, and their associated high mortality rates. Infec-tions with these potentially antibiotic-resistant bacteria have occurred primarily among hospitalized patients and/or among patients with an extensive hospitalization history and other predisposing risk factors like indwelling catheters, past anti-microbial use, decubitus ulcers, postoperative surgical wound infections, or treatment with enteral feedings or dialysis.
Antimicrobial Resistance: Risk Factors and Influence on Outcome
Although several factors contribute to the emergence of anti-microbial resistance, antibiotic use is the key driver for its development in both gram-positive and gram-negative bacte-ria (8,12,13). Prolonged hospitalization, invasive devices such as endotracheal tubes and intravascular catheters, residence in long-term treatment facilities, and inadequate infection control practices also promote resistance (12). Furthermore, the emer-gence of new bacterial strains in the community setting, such as community-associated methicillin-resistant S. aureus, has cre-ated additional stressors favoring the entry of resistant microor-ganisms into the hospital setting (14). However, the prolonged administration of antimicrobial therapy appears to be the most important factor associated with the emergence of resistance that is potentially amenable to intervention (8,15,16).
It is critical to maintain awareness of risk factors associated with the development of antimicrobial resistance as clinical investigations have repeatedly demonstrated that inappro-priate initial antimicrobial therapy is associated with greater in-hospital mortality (17–22). When initial therapy is inad-equate, adjusting treatment regimens once antimicrobial sensi-tivity data is available has not been shown to improve patient outcomes (23). Antimicrobial resistance is also associated with excess costs. While most of this is associated with the acquisi-tion of a nosocomial infection, the presence of antibiotic resis-tance may confer additional morbidity and further increase
cost (8,24,25). For these reasons, local antibiograms, both within individual hospitals and ICUs, should be updated fre-quently to guide clinicians in choosing appropriate therapy.
dIAgnoSIS
A thorough diagnostic assessment is essential to ensure initia-tion of appropriate antimicrobial therapy and allow for de-escalation. Data from a patient history, physical examination, and imaging are combined to create an initial antimicrobial regimen. The development of rapid molecular diagnostics has added a new element to the clinician’s arsenal that may improve the likelihood of covering all possible pathogens early in the course of therapy. Cultures from likely infectious sources enable the clinician to streamline initial antimicrobial regimens. The use of such targeted therapies minimizes the risk of medication adverse effects, decreases the risk of selecting for new, resistant pathogens, and reduces cost.
Rapid Microbiologic Diagnostics
Conventional microbiologic procedures are time consuming and often delay identification of resistant bacteria resulting in inad-vertent administration of inappropriate initial antimicrobial therapy. Recently, several molecular diagnostic platforms for the rapid identification of infectious organisms and their accom-panying resistance genes have been introduced and evaluated.
Matrix-assisted laser Desorption/Ionization Time-of-Flight Mass Spectrometry (MalDI-TOF MS)
Mass spectrometry was first utilized for bacterial identification in the 1970s (26). This technique has evolved significantly in recent years and has the potential to revolutionize the way pathogens are identified in clinical practice. Following organ-ism isolation from a clinical specimen, MALDI-TOF MS uti-lizes mass spectrometry to rapidly identify pathogens. The use of this technique has been reported to decrease time to bacte-rial identification by up to 48 hours compared to conventional techniques (27). Further, when combined with interventions from an antimicrobial stewardship team, MALDI-TOF has been shown to decrease not only time to bacterial identifi-cation but also time to effective antibiotic therapy, mortal-ity, ICU length of stay, and recurrent bacteremia compared to conventional microbiologic methods (28). While most research has focused on the identification of bacterial isolates, MALDI-TOF has also been investigated for the identification of fungi and viruses. Practical hurdles to the wide spread adap-tation of this evolving technology exist including a large up-front investment in the instrument and a current lack of clarity regarding how to best utilize MALDI-TOF when dealing with specimens other than blood (29). As this technology continues to evolve however it is likely to become a prominent feature of infectious disease management in the future.
Peptide Nucleic acid Fluorescent In Situ Hybridization (PNa-FISH)
PNA-FISH allows for rapid identification of bacteria and yeast from positive blood cultures. Compared to conventional meth-ods, PNA-FISH has been shown to decrease time to organism
Table 83.2 Definitions of Infection Categories (with Focus on bacterial Pathogens)
Infection Category Definition
Community-acquired infection
Patients with a first-positive bacterial cul-ture obtained within 48 hrs of hospital admission lacking risk factors for health care–associated infection
hospital-acquired infection
Patients with a first-positive bacterial culture >48 hrs after hospital admission
health care–asso-ciated infection
Patients with a first-positive bacterial culture within 48 hrs of admission and any of the following:
•admission source indicates a transfer from another health care facility (e.g., hospital, nursing home)
•receiving hemodialysis, wound, or infusion therapy as an outpatient
•Prior hospitalization for ≥3 days within 90 days
• immunocompromised state due to underlying disease or therapy (human immunodeficiency virus, chemotherapy)
LWBK1580_C83_p964-981.indd 966 29/07/17 11:37 AM

Chapter 83 antibiotics in the Management of serious hospital-acquired infections 967
identification by nearly 72 hours and has been associated with decreased mortality and antibiotic use (30,31). Compared with other rapid diagnostics, PNA-FISH has the advantage of a relatively small investment in equipment up front and comparative ease of use. A major limitation of this technol-ogy currently is the lack of probes for some clinically relevant organisms. However, this technology has evolved rapidly in recent years and will likely continue to grow and expand its place in therapy.
Microarrays
Compared to the previously discussed rapid diagnostic tech-niques, DNA-probe–based assays, or microarrays, have the comparative advantage of being able to simultaneously iden-tify organisms and resistance markers from positive blood cultures. Probes for commonly encountered resistance mech-anisms, such as mecA, vanA/vanB, and a number of genes responsible for production of extended-spectrum β-lactamases and carbapenemases exist (32–34). To date, microarrays have been predominantly studied clinically in gram-positive blood-stream infections. In this setting, time to organism and resis-tance identification has been shown to be decreased by up to 48 hours compared to conventional techniques (32). As the role of microarrays for the treatment of gram-positive infec-tions becomes more established, it is likely that its role will continue to expand to gram-negative infections as well.
Quantitative Cultures and Assessment of Infection Risk
Pneumonia is the most common hospital-acquired infection among mechanically ventilated patients. A meta-analysis of four randomized trials demonstrated that the use of quanti-tative bacterial cultures obtained from the lower respiratory tract may, in theory, facilitate de-escalation of empiric broad-spectrum antibiotics and reduce drug-specific antibiotic days of treatment (35). Another study found that patients with a clinical suspicion for VAP and culture-negative bronchoalveo-lar lavage (BAL) results for a major pathogen could have anti-microbial therapy safely discontinued within 72 hours (36). Interestingly, the mean modified clinical pulmonary infection scores (CPISs) of these patients was approximately six, sug-gesting that this quantitative clinical assessment of the risk for VAP could have been used to discontinue antibiotics as previously suggested (37). Regardless of whether quantitative culture methods are used, the results of microbiologic testing should be used to routinely modify or discontinue antibiotic treatment in the appropriate clinical setting.
treAtMent
Antibiotics, Their Mode of Action, Clinical Indications for Use, and Associated Toxicities
Most antimicrobial agents used for the treatment of infections may be categorized according to their principal mechanism of action. For antibacterial agents, the major modes of action are the following (38):• Interference with cell wall synthesis• Disruption of the bacterial cell membrane
• Inhibition of protein synthesis• Interference with nucleic acid synthesis• Inhibition of a metabolic pathway
Tables 83.3 to 83.5 review the major pathogens, the anti-microbials of choice by pathogen, and the major toxicities of specific agents, respectively.
Cell Wall active antibiotics
Antibacterial drugs that work by inhibiting bacterial cell wall synthesis include the β-lactams—such as the penicillins, ceph-alosporins, carbapenems, and monobactams—and the gly-copeptides, including vancomycin and teicoplanin. β-Lactam agents inhibit the synthesis of the bacterial cell wall by inter-fering with the enzymes required for the synthesis of the pep-tidoglycan layer. Vancomycin and teicoplanin also interfere with cell wall synthesis by preventing the cross-linking steps required for stable cell wall synthesis.
Disruption of bacterial Cell Membrane
Disruption of the bacterial membrane is a less well charac-terized mechanism of action. Polymyxin antibiotics appear to exert their inhibitory effects by increasing bacterial membrane permeability, causing leakage of bacterial contents. The cyclic lipopeptide, daptomycin, appears to insert its lipid tail into the bacterial cell membrane, causing membrane depolarization and eventual death of the bacterium.
Inhibition of bacterial Protein Synthesis
Macrolides, aminoglycosides, tetracyclines, chloramphenicol, streptogramins, and oxazolidinones produce their antibacte-rial effects by inhibiting protein synthesis. Bacterial ribosomes differ in structure from their counterparts in eukaryotic cells. Antibacterial agents take advantage of these differences to selectively inhibit bacterial growth. Macrolides, aminoglyco-sides, and tetracyclines bind to the 30S subunit of the ribo-some, whereas chloramphenicol binds to the 50S subunit. Linezolid is a gram-positive antibacterial oxazolidinone that binds to the 50S subunit of the ribosome on a site that has not been shown to interact with other classes of antibiotics.
Inhibition of Nucleic acid Synthesis
Fluoroquinolones exert their antibacterial effects by disrupt-ing DNA synthesis and causing lethal double-strand DNA breaks during DNA replication.
Inhibition of a Metabolic Pathway
Sulfonamides and trimethoprim block the pathway for folic acid synthesis, which ultimately inhibits DNA synthesis. The common antibacterial drug combination of trimethoprim, a folic acid analogue, plus sulfamethoxazole (a sulfonamide) inhibits two steps in the enzymatic pathway for bacterial folate synthesis.
Mechanisms of Resistance to Antibacterial Agents
Most antimicrobial agents exert their effect by influencing a single step in bacterial reproduction or bacterial cell function. Therefore, resistance can emerge with a single point mutation aimed at bypassing or eliminating the action of the antibiotic. Some species of bacteria are innately resistant to at least one class of antimicrobial agents, with resulting resistance to all
LWBK1580_C83_p964-981.indd 967 29/07/17 11:37 AM

968 SeCtion 9 infeCtious Disease
Table 83.3 Most Common Pathogens associated with Sites of Serious Infection Commonly Seen in the adult Intensive Care Unit Setting
Infection Site Pathogens
Pneumonia1. Community-acquired pneumonia (nonimmunocompromised
host)Streptococcus pneumoniaeHaemophilus influenzae
Moraxella catarrhalis
Mycoplasma pneumoniaeLegionella pneumophilaChlamydia pneumoniaeMethicillin-resistant Staphylococcus aureus (MRSA)influenza virus
2. health care–associated pneumonia Mrsa
Pseudomonas aeruginosa
Klebsiella pneumoniae
Acinetobacter species
Stenotrophomonas species
Legionella pneumophila
3. Pneumonia (immunocompromised host)
a. neutropenia any pathogen listed above
Aspergillus species
Candida species
b. hiV any pathogen listed above
Pneumocystis jirovecii
Mycobacterium tuberculosis
Histoplasma capsulatum
other fungi
Cytomegalovirus
c. solid organ transplant or bone marrow transplant any pathogen listed above(Can vary depending on timing of infection to transplant)
d. Cystic fibrosis Haemophilus influenzae (early)
Staphylococcus aureus
Pseudomonas aeruginosa
Burkholderia cepacia
4. lung abscess Bacteroides species
Peptostreptococcus species
Fusobacterium species
Nocardia (in immunocompromised patients)
Amebic (when suggestive by exposure)
5. empyema Staphylococcus aureusStreptococcus pneumoniaeGroup a StreptococciHaemophilus influenzae
usually acute
anaerobic bacteriaEnterobacteriaceaeMycobacterium tuberculosis
usually subacute or chronic
Meningitis Streptococcus pneumoniae
Neisseria meningitidis
Listeria monocytogenes
Haemophilus influenzae
Escherichia coliGroup B streptococci
neonates
Staphylococcus aureusEnterobacteriaceaePseudomonas aeruginosa
Postsurgical or posttrauma
brain abscess streptococci
Bacteroides species
EnterobacteriaceaeStaphylococcus aureus
Postsurgical or posttrauma
NocardiaToxoplasma gondii
immunocompromised or hiV infected
LWBK1580_C83_p964-981.indd 968 29/07/17 11:37 AM

Chapter 83 antibiotics in the Management of serious hospital-acquired infections 969
Infection Site Pathogens
encephalitis west nile virus
herpes simplex
arbovirus
rabies
Cat-scratch disease
endocarditis Streptococcus viridans
Enterococcus species
Staphylococcus aureus
Streptococcus bovis
Mrsa intravenous drug user, prosthetic valve
Candida species Prosthetic valve
Catheter-associated bacteremia Candida species
Staphylococcus aureus
Enterococcus species
Enterobacteriaceae
Pseudomonas aeruginosa
Pyelonephritis Enterobacteriaceae
Escherichia coli
Enterococcus species
Pseudomonas aeruginosaAcinetobacter species
Catheter-associated, postsurgical
Peritonitis1. Primary or spontaneous Enterobacteriaceae
Streptococcus pneumoniae
Enterococcus species
anaerobic bacteria (rare)
2. secondary (bowel perforation) Enterobacteriaceae
Bacteroides species
Enterococcus species
Pseudomonas aeruginosa (uncommon)
3. tertiary (bowel surgery, hospitalized on antibiotics) Pseudomonas aeruginosaMrsa
Acinetobacter species
Candida species
Skin structure infections1. Cellulitis Group a streptococci
Staphylococcus aureus
Enterobacteriaceae Diabetics
2. Decubitus ulcer Polymicrobial
Streptococcus pyogenes
Enterococcus species
Enterobacteriaceae
anaerobic streptococci
Pseudomonas aeruginosa
Staphylococcus aureus
Bacteroides species
3. necrotizing fasciitis Streptococcus species
Clostridia species
Mixed aerobic/anaerobic bacteria
Muscle infection1. Myonecrosis (gas gangrene) Clostridium perfringens
Other Clostridium species
2. Pyomyositis Staphylococcus aureus
Group a streptococci
anaerobic bacteria
Gram-negative bacteria (rare)
Table 83.3 Most Common Pathogens associated with Sites of Serious Infection Commonly Seen in the adult Intensive Care Unit Setting (Continued )
(Continued )
LWBK1580_C83_p964-981.indd 969 29/07/17 11:37 AM

970 SeCtion 9 infeCtious Disease
Infection Site Pathogens
Septic shock1. Community-acquired Streptococcus pneumoniae
Neisseria meningitidis
Haemophilus influenzae
Escherichia coli
Capnocytophaga (Df-2 with splenectomy)
2. health care—associated Mrsa
Pseudomonas aeruginosa
Acinetobacter species
Candida species
3. toxic shock syndrome Staphylococcus aureus
streptococci species
4. regional illness or special circumstances rickettsial species
ehrlichiosis
Babesiosis
Cat-scratch disease (immunocompromised hosts)
Yersinia pestis
Francisella tularensis
Leptospira
Salmonella enteritidis
Salmonella typhi
hiV, human immune deficiency virus.
Table 83.3 Most Common Pathogens associated with Sites of Serious Infection Commonly Seen in the adult Intensive Care Unit Setting (Continued )
the members of those antibacterial classes. However, the emer-gence and spread of acquired resistance due to the selective pressure to use specific antimicrobial agents is of greater con-cern due to the spread of such resistance. Several mechanisms of antimicrobial resistance are readily transferred to various bacteria.
First, the organism may acquire genes encoding enzymes, such as β-lactamases, that destroy the antibacterial agent before it can have an effect. Second, bacteria may acquire efflux pumps that extrude the antibacterial agent from the cell before it can reach its target site and exert its effect. Third, bacteria may acquire several genes for a metabolic pathway that ultimately produces altered bacterial cell walls that no longer contain the binding site of the antimicrobial agent, or bacteria may acquire mutations that limit access of antimicro-bial agents to the intracellular target site via downregulation of porin genes. Susceptible bacteria can also acquire resistance to an antimicrobial agent via new mutations such as are noted above.
New Antimicrobial Agents
Most new antibiotics have been developed for the treatment of gram-positive bacteria. Until recently, the glycopeptides, vancomycin and teicoplanin, were the only antibacterial com-pounds available to which MRSA strains remained uniformly susceptible. In 1996, the first clinical isolate of S. aureus with reduced susceptibility to vancomycin (vancomycin-intermedi-ate S. aureus, or VISA) was reported in Japan and, since then, similar cases have been reported around the world. Only a few years later, clinical isolates of S. aureus that were fully resistant to vancomycin were reported in South Africa and Michigan. The emergence of MRSA strains with reduced vancomycin susceptibility has limited the treatment options and increased the incidence of treatment failure (39); infection with one of
these strains may be an independent predictor of mortality (40). More concerning are the observations that upward drift in the minimum inhibitory concentrations (MICs) for vanco-mycin in MRSA are associated with an increased risk of clini-cal treatment failures (41). As a result of this upsurge in MRSA resistance, most of the recent advances in the development of new antibiotic agents have predominantly occurred for gram-positive bacteria.
Unfortunately, gram-negative antibiotic development has lagged behind. In an effort to encourage development and mar-keting of new antimicrobials against resistant bacteria, the FDA began offering a Qualified Infections Disease Product (QIDP) designation as a part of the Generating Antibiotic Incentives Now (GAIN) act in 2012. This designation allows priority review and an extended period of market exclusivity for quali-fying products (42). All of the following antimicrobials mar-keted after 2012 were granted QIDP status.
Dalbavancin (Dalvance)
Approved by the FDA in 2014, dalbavancin is a lipoglycopep-tide antimicrobial that has been studied in the treatment of com-plicated skin and skin structure infections and catheter-related bloodstream infection. Dalbavancin is a bactericidal agent whose long-terminal plasma half-life (8.5 days) allows for the unique dosing of 1,000 mg given on day 1 and 500 mg given on day 8. The long half-life may turn out to be the strength of the drug, allowing for more convenient treatment options in patients requiring prolonged antibiotic therapy (e.g., right-sided infective endocarditis or osteomyelitis). However, the impact of this prolonged half-life on adverse reactions also needs further evaluation.
Oritavancin (Orbactiv)
Oritavancin is a lipoglycopeptide antibacterial that gained FDA approval in 2014. It has demonstrated in vitro bactericidal
LWBK1580_C83_p964-981.indd 970 29/07/17 11:37 AM

Chapter 83 antibiotics in the Management of serious hospital-acquired infections 971
Table 83.4 Drugs of Choice in Serious Infectionsa
Organism Drug of Choice alternative Drugs
GRaM-POSITIVe COCCIStaphylococcus aureusb or
Staphylococcus epidermidis
Penicillin-sensitive Penicillin G Cephalosporin, vancomycin, or clindamycinc
Penicillinase-producingd oxacillin or nafcillin Cephalosporin, vancomycin, or clindamycin
Methicillin-resistante Vancomycin (linezolid for pneumonia) Quinolone, tMP/sMX, minocycline, clindamycin, line-zolid, ceftaroline, daptomycin (unless pneumonia)
nonenterococcal streptococci Penicillin G Cephalosporin, vancomycin, or clindamycin
Enterococcus Penicillin or ampicillin + gentamicin Vancomycin + gentamicin
Streptococcus pneumoniaef Penicillin G Cephalosporin, vancomycin, macrolide, or clindamycin
GRaM-POSITIVe baCIllIActinomyces israelii Penicillin G tetracycline
Bacillus anthracis Penicillin G tetracycline, macrolide
Clostridium difficile Metronidazole oral vancomycin
Clostridium perfringens Penicilling Clindamycin, metronidazole, tetracycline, imipenem
Clostridium tetani Penicillinh tetracycline
Corynebacterium diphtheriae Macrolideg Penicillin
Corynebacterium JK Vancomycin Penicillin G + gentamicin, erythromycin
Listeria monocytogenes ampicillin gentamicin tMP/sMX
Nocardia asteroides tMP/sMX carbapenem + amikacin
Propionibacterium sp. Penicillin Clindamycin, erythromycin
GRaM-NeGaTIVe COCCIMoraxella catarrhalis tMP/sMX amoxicillin/clavulanic acid, ceftriaxone, macrolide,
tetracycline
Neisseria gonorrhoeae Ceftriaxone Penicillin G, quinolone
Neisseria meningitidis Penicillin G Ceftriaxone
eNTeRIC GRaM-NeGaTIVe baCIllIBacteroides
oral source Penicillin Clindamycin, cefoxitin, metronidazole, cefotetan
Bowel source Metronidazole Cefoxitin, cefotetan, imipenem, ampicillin/sulbactam ticarcillin/clavulanate, piperacillin/tazobactam, clindamycin
Citrobacter Cefepime or imipenem/meropenem aminoglycoside, quinolone, piperacillin, aztreonam
Enterobacter sp.i Cefepime or imipenem/meropenem Ciprofloxacin, aminoglycoside, aztreonam
Escherichia coli j 3rd-generation cephalosporin aminoglycoside, carbapenem, cefepime, ß-lactam/ß-lactamase inhibitor, ciprofloxacin, tMP/sMX
Klebsiella j 3rd-generation cephalosporin as for E. coli
Proteus mirabilis ampicillin aminoglycoside, quinolone, cephalosporin, piperacillin, ticarcillin, tMP/sMX
Proteus, nonmirabilis 3rd-generation cephalosporin aminoglycoside, quinolone, piperacillin, aztreonam, imipenem
Providencia 2nd- or 3rd-generation cephalosporin Gentamicin, amikacin, piperacillin, aztreonam, imipenem, ticarcillin, mezlocillin, tMP/sMX
salmonella typhi Ceftriaxone or quinolone ampicillin, tMP/sMX
Salmonella, nontyphik Cefotaxime, ceftriaxone, or quinolone ampicillin, tMP/sMX
Serratia Cefepime or imipenem/meropenem aminoglycoside, aztreonam piperacillin, tMP/sMX, quinolone
Shigella Quinolone ampicillin, tMP/sMX, ceftriaxone, cefixime
Yersinia enterocolitica tMP/sMX aminoglycoside, tetracycline, 3rd-generation cephalosporin, quinolone
OTHeR GRaM-NeGaTIVe baCIllI
Acinetobacter imipenem Cefepime, aminoglycoside, tMP/sMX, colistin, sulbactam
Eikenella corrodens ampicillin Penicillin G, erythromycin, tetracycline, ceftriaxone
Francisella tularensis streptomycin, gentamicin tetracycline
Fusobacterium Penicillin Clindamycin, metronidazole, cefoxitin
Haemophilus influenzae 3rd-generation cephalosporin ampicillin, imipenem, quinolone, cefuroximel, quinolone, macrolide, tMP/sMX
(Continued )
LWBK1580_C83_p964-981.indd 971 29/07/17 11:37 AM

972 SeCtion 9 infeCtious Disease
Organism Drug of Choice alternative Drugs
Legionella erythromycin (1 g q6h) + rifampin
Pasteurella multocida Penicillin G tetracycline, cephalosporin, ampicillin/sulbactam
Pseudomonas aeruginosa antipseudomonal penicillinm + aminoglycoside
aztreonam, cefepime, imipenem, quinolone
Pseudomonas cepacia tMP/sMX Ceftazidime
Spirillum minus Penicillin G tetracycline, streptomycin
Streptobacillus moniliformis Penicillin G tetracycline, streptomycin
Vibrio choleraen tetracycline tMP/sMX, quinolone
Vibrio vulnificus tetracycline Cefotaxime
Xanthomonas maltophilia tMP/sMX Quinolone, minocycline, ceftazidime
Yersinia pestis streptomycin tetracycline, gentamicin
CHlaMYDIaeChlamydia pneumoniae (twar) Macrolide tetracycline
Chlamydia psittaci tetracycline Chloramphenicol
Chlamydia trachomatis Macrolide sulfonamide, tetracycline
MYCOPLASMA sp. Macrolide tetracycline
tetracycline Quinolone
SPIROCHeTeSBorrelia burgdorferi Doxycycline, amoxicillin Penicillin G, macrolide, cefuroxime, ceftriaxone,
cefotaxime
Borrelia sp. tetracycline Penicillin G
Treponema pallidum Penicillin tetracycline, ceftriaxone
VIRUSeSCytomegalovirus Gancicloviro foscarnet, cidofovir
herpes simplex acyclovir foscarnet, ganciclovir
hiV see Centers for Disease Control web site
influenza amantadine rimantadine, oseltamivir, zanamivir
respiratory syncytial ribavirin
Varicella zoster acyclovir famciclovirp
FUNGIAspergillus Voriconazole amphotericin B, echinocandin, itraconazoler
Blastomyces amphotericin B or itraconazole Ketoconazole
Candidaq
Mucosal fluconazole, echinocandins Ketoconazole, itraconazole
systemic fluconazole, echinocandin amphotericin B
Coccidioides amphotericin B or fluconazole itraconazole, ketoconazole
Cryptococcus amphotericin fluconazole, itraconazole
Histoplasma itraconazole or amphotericin B
Pseudallescheria Ketoconazole or itraconazole
zygomycosis (“mucor”) amphotericin B Posaconazole
athis table does not consider minor infections that may be treated with oral agents, single-agent therapy, or less toxic drugs. sensitivity testing must be done on bacterial isolates to confirm the sensitivity pattern.
bsome authorities recommend clindamycin as the first choice for susceptible toxin-producing staphylococci, streptococci, or clostridia.cfirst-generation cephalosporins are most active. if endocarditis is suspected, do not use clindamycin. some authorities recommend the addition of gentamicin for
endocarditis caused by nonenterococcal streptococci or tolerant staphylococci.dPenicillinase-producing staphylococci are also resistant to ampicillin, amoxicillin, carbenicillin, ticarcillin, mezlocillin, and piperacillin.eMethicillin-resistant staphylococci should be assumed to be resistant to all cephalosporins and penicillins, even if disk testing suggests sensitivity. Dalbavancin and
oritavancin may be alternatives for specific types of methicillin-resistant infection pending future studies and indications.fsome strains show intermediate- or high-level penicillin resistance. highly resistant strains are treated with vancomycin, or rifampin, or both. in regions with high prevalence of
resistant pneumococcus, ceftriaxone or vancomycin should be considered until sensitivity is known.guse as an adjunct to debridement of infected tissues.huse as an adjunct to active and passive immunization.iBecause of rapid development of resistance, cephalosporins not recommended even if initial tests indicate susceptibility.jKlebsiella sp. and E. coli producing extended-spectrum β-lactamase (esBl) should be preferentially managed with a carbapenem.kuncomplicated Salmonella enteritis should not be treated with antibiotics.lshould not be used in meningitis because of poor Cns penetration.mantipseudomonal penicillins include ticarcillin, mezlocillin, and piperacillin.nPrimary therapy is fluid and electrolyte repletion.ooral form should be used only in maintenance therapy of retinal cytomegalovirus.papproved only for mild herpes zoster in immunocompetent hosts.qCandida krusei and Torulopsis glabrata may be resistant to azole therapy, Candida parapsilosis may be resistant to echinocandins.rin multidrug combinations.sechinocandins include caspofungin, micafungin, and anidulafungin.
Table 83.4 Drugs of Choice in Serious Infectionsa (Continued )
LWBK1580_C83_p964-981.indd 972 29/07/17 11:37 AM

Chapter 83 antibiotics in the Management of serious hospital-acquired infections 973
Table 83.5 Toxicities associated with antimicrobials
antimicrobial Serious Toxicities, Uncommon Common Toxicitiesa
PenicillinsampicillinPenicillin
anaphylaxis, seizures, hemolytic anemia, neutrope-nia, thrombocytopenia, drug fever
Diarrhea, nausea, vomiting
antistaphylococcal penicillinsnafcillinoxacillin
anaphylaxis, neutropenia, thrombocytopenia, acute interstitial nephritis, hepatotoxicity
Diarrhea, nausea, vomiting
a-lactam/a-lactamase inhibitors anaphylaxis, seizures, hemolytic anemia, neutrope-nia, thrombocytopenia
Clostridium difficile colitis, cholestatic jaundice, drug fever
Diarrhea, nausea, vomiting
amoxicillin/clavulanate
ampicillin/sulbactam
Piperacillin/tazobactam
ticarcillin/clavulanate
Cephalosporins anaphylaxis, seizures, neutropenia, thrombocytopenia, drug fever
Diarrhea, nausea, vomiting
Carbapenemsimipenem
anaphylaxis, seizures (imipenem > meropenem, ertapenem, doripenem)
Diarrhea, nausea, vomiting
Meropenem C. difficile colitis, drug fever
ertapenem
Doripenem
GlycopeptidesVancomycin
ototoxicity, nephrotoxicity (unlikely without concomitant nephrotoxins), thrombocytopenia
red-man syndrome
Oxazolidinoneslinezolid
More common with long-term use: Peripheral and optic neuropathy, myelosuppression
Diarrhea
Possible with short-term use:
lactic acidosis, myopathy anemia
lipopeptidesDaptomycin Diarrhea, constipation, vomiting
Streptogramin arthralgia, myalgia, inflammation, pain, edema at infusion site, hyperbilirubinemiaQuinupristin/dalfopristin
aminoglycosides nephrotoxicity, ototoxicity
amikacin
Gentamicin
tobramycin
Fluoroquinolones2nd generation
anaphylaxis, dysglycemia Qtc prolongation, joint toxicity in children
nausea, vomiting, diarrhea, photosensitiv-ity, rash
Ciprofloxacin Cns stimulation, dizziness, somnolence
3rd generation
levofloxacin
4th generation
Gatifloxacin
Moxifloxacin
Gemifloxacin
MacrolideserythromycinazithromycinClarithromycin
Qtc prolongation (erythromycin > clarithromycin > azithromycin), cholestasis
nausea, vomiting, diarrhea, abnormal taste
Ketolides acute hepatic failure nausea, vomiting, diarrhea
telithromycin Qtc prolongation
Clindamycin C. difficile colitis nausea, vomiting, diarrhea, abdominal pain, rash
TetracyclinestetracyclineDoxycyclineMinocycline pseudotumor
cerebri
tooth discoloration and retardation of bone growth (in children), renal tubular necrosis, dizziness, vertigo
Photosensitivity, diarrhea
Glycylcyclines nausea, vomiting, diarrhea
tigecycline
Trimethoprim/sulfamethoxazole Myelosuppression rash, nausea, vomiting, diarrhea
stevens–Johnson syndrome, hyperkalemia, aseptic meningitis, hepatic necrosis
Metronidazole seizures, peripheral neuropathy nausea, vomiting, metallic taste, disulfiram-like reaction
(Continued )
LWBK1580_C83_p964-981.indd 973 29/07/17 11:37 AM

974 SeCtion 9 infeCtious Disease
antimicrobial Serious Toxicities, Uncommon Common Toxicitiesa
Nitrofurantoin Pulmonary toxicity, peripheral neuropathy urine discoloration, photosensitivity
aNTIFUNGal aGeNTSazoles
fluconazoleitraconazoleVoriconazolePosaconazole
hepatic failure, increased ast/alt, cardiovascular toxicity, hypertension, edema
nausea, vomiting, diarrhea, rash, visual disturbances, phototoxicity
amphotericin b productsamphotericin B deoxycholateaBlCaBCDliposomal amphotericin B
acute liver failure, myelosuppression nephrotoxicity (less common with lipid formulations), acute infusion-related reactions, hypokalemia, hypomagnesemia
echinocandinsCaspofunginMicafunginanidulafungin
hepatotoxicity, infusion-related rash, flushing, itching
Flucytosine Myelosuppression, hepatotoxicity, confusion, hallucinations, sedation
nausea, vomiting, diarrhea, rash
aNTIVIRal aGeNTSNucleoside analogues
acyclovirValaciclovirGanciclovirValganciclovir
nephrotoxicity, rash, encephalopathy, inflammation at injection site, phlebitis
Bone marrow suppression, headache, nau-sea, vomiting, diarrhea (with oral forms)
amantadine Cns disturbances (amantadine > rimantadine) nausea, vomiting, anorexia, xerostomia
RimantadineNeuraminidase inhibitors
oseltamivir anaphylaxis, bronchospasm nausea, vomiting, cough, local discomfort
zanamivir
Cidofovir anemia, neutropenia, fever, rash nephrotoxicity, uveitis/iritis, nausea, vomiting
Foscarnet seizures, anemia, fever nephrotoxicity, electrolyte abnormalities (hypocalcemia, hypomagnesemia, hypo-kalemia, hypophosphatemia), nausea, vomiting, diarrhea, headache
atoxicities were classified as “common” relative to the other toxicities that agent is known to cause. Because toxicities are classified as “common” does not imply they are not serious.
Table 83.5 Toxicities associated with antimicrobials (Continued )
activity against a variety of gram-positive organisms includ-ing methicillin-resistant, vancomycin-intermediate, and vanco-mycin-resistant, S. aureus and vancomycin-resistant VanA and VanE strains of Enterococcus faecalis and Enterococcus faecium (43,44). Oritavancin has been investigated chiefly for the treat-ment of skin and skin structure infections. It has been observed to have a terminal half-life of approximately 10 days allowing for single-dose administration to treat most infections (45).
Tedizolid (Sivextro)
Tedizolid is an oxazolidinone antibacterial that gained FDA approval in 2014. Tedizolid has a similar spectrum of activ-ity to linezolid with the added advantage of having activity against linezolid-resistant strains of MRSA (46). Tedizolid has a similar side effect profile to linezolid and is available in both oral and IV dosage forms (47).
Ceftaroline (Teflaro)
Ceftaroline is an intravenous, broad-spectrum, cephalosporin antibiotic that gained FDA approval in 2010. Ceftaroline has activity against gram-positive organisms, oral anaerobes, and a variety of Enterobacteriaceae. It is the only antibiotic in the cephalosporin class with activity against methicillin-resistant,
vancomycin-intermediate, and vancomycin-resistant S. aureus. Its activity against Enterobacteriaceae, though, is limited to organisms that do not produce Amp-C β-lactamase. Addition-ally, most nonfermenting gram-negative bacilli, such as P. aeru-ginosa, are inherently resistant to ceftaroline (48). The adverse effects of ceftaroline are similar to those observed with other cephalosporins (49). Originally approved for the treatment of skin and skin structure infections and community-acquired pneumonia, clinical experience with ceftaroline has expanded to a variety of infectious processes and is likely to continue to expand based on its spectrum of activity and favorable side effect profile.
Ceftolozane/Tazobactam (Zerbaxa)
This intravenous combination product was approved by the FDA in 2014 and contains ceftolozane, a new cephalosporin antibiotic, and tazobactam, a β-lactamase inhibitor. Ceftolo-zane alone is a broad-spectrum, bactericidal antibiotic that closely resembles ceftazidime. Ceftolozane has activity against a variety of resistant gram-negative bacilli including some ESBL producing strains. The addition of tazobactam extends this spectrum of activity to include many ESBL organisms, MDR strains of P. aeruginosa, and some anaerobes (50,51).
LWBK1580_C83_p964-981.indd 974 29/07/17 11:37 AM

Chapter 83 antibiotics in the Management of serious hospital-acquired infections 975
Ceftazidime/avibactam (avycaz)
This intravenous combination product was approved by the FDA in 2015 and contains the cephalosporin ceftazidime with a new synthetic β-lactamase inhibitor, avibactam. The addi-tion of avibactam expands the gram-negative spectrum of ceftazidime to include activity against a variety of otherwise resistant organisms. Notably ceftazidime/avibactam has dem-onstrated activity against a variety of carbapenemase produc-ing Enterobacteriaceae and MDR P. aeruginosa. The addition of avibactam does not appear however to enhance the activity of ceftazidime against Acinetobacter spp or enhance its gram-positive spectrum (52,53).
Initial Antimicrobial Therapy
An initial appropriate antibiotic regimen should be pre-scribed with adequate activity against all pathogens likely to be responsible for the infection. Inappropriate initial anti-biotic therapy has been associated with a very high risk of mortality in patients with septic shock attributable to a vari-ety of bacterial and fungal pathogens from numerous sources (17,19,21,54–58). Patient history, including drug intolerances, recent receipt of antibiotics, underlying disease, the clinical syndrome, and susceptibility patterns of pathogens in the com-munity and hospital should be utilized when making decisions regarding initial antimicrobial regimen selection. However, given the severity of illness for patients with severe sepsis and septic shock, erring on the side of initial overtreatment may be preferable to the administration of an inappropriately narrow initial antibiotic regimen. Balancing these competing interests is at the core of antimicrobial stewardship in the ICU; methods for refining this balance are described below.
StrAtegIeS tHAt oPtIMIze tHe effIcAcy of AntIbIotIcS WHIle MInIMIzIng AntIbIotIc reSIStAnce
Hospital and System Level Interventions
Formal Protocols and Guidelines
Antibiotic practice guidelines or protocols have emerged as a means of both avoiding unnecessary antibiotic administration and increasing the effectiveness of prescribed antibiotics. Auto-mated antimicrobial utilization guidelines have been success-fully used to identify and minimize the occurrence of adverse drug effects and improve antibiotic selection (12). Their use has also been associated with stable antibiotic susceptibility patterns for both gram-positive and gram-negative bacteria, possibly as a result of promoting antimicrobial heterogeneity and specific end points for antibiotic discontinuation. Auto-mated and nonautomated guidelines have also been employed to reduce overall antibiotic use and limit inappropriate antimi-crobial exposure, both of which could affect the development of antibiotic resistance (59). One way these guidelines limit the unnecessary use of antimicrobial agents is by recommending that therapy be modified when initial empiric broad-spectrum antibiotics are prescribed and the culture results reveal that narrow-spectrum antibiotics can be used.
Hospital Formulary Restrictions
Restricted use of specific antibiotics or antibiotic classes from the hospital formulary has been used to reduce resistance, min-imize adverse drug reactions, and reduce cost. However, not all experiences have been uniformly successful, and the homo-geneous use of a single or limited number of drug classes may actually promote the emergence of resistance (12). Restricted use of specific antibiotics has generally been applied to those drugs with a broad spectrum of action (e.g., carbapenems), rapid emergence of antibiotic resistance (e.g., cephalosporins), and readily identified toxicity (e.g., aminoglycosides). To date, it has been difficult to demonstrate that restricted hospital formularies are effective in curbing the overall emergence of antibiotic resistance. While this may be due in large part to methodologic problems, their use has been successful in spe-cific outbreaks of infection with antibiotic-resistant bacteria, particularly in conjunction with infection control practices and antibiotic educational activities.
Formalized Antimicrobial Stewardship Programs
Formally implemented antimicrobial stewardship programs (ASPs) have been associated not only with reduced infection rates but also significant cost savings associated with reduc-tions in the defined daily doses of the antimicrobials targeted by the ASP (60,61). ASPs have been shown to increase the appropriateness of therapy and increase the number of infec-tious diseases consultations, which may improve patient outcomes including mortality, hospital lengths of stay, and readmission rates by providing more precise antibiotic pre-scription (60,62–65). These attributes of ASPs account for why they are now recognized as mandatory components of hospital quality improvement efforts. Formalized ASPs not only restrict the use of unnecessary antibiotics but also insure that antimicrobials are employed in an effective manner to optimize patient outcomes.
Antimicrobial Exposure
Use of Narrow-Spectrum antibiotics
Another proposed strategy to curtail the development of anti-microbial resistance, in addition to the judicious overall use of antibiotics, is to use drugs with a narrow antimicrobial spectrum. Several investigations have suggested that infections such as CAP can usually be successfully treated with narrow-spectrum antibiotic agents, especially if the infections are not life threatening. Similarly, the avoidance of broad-spectrum antibiotics, especially those associated with rapid emergence of resistance (cephalosporins, quinolones), and the reintro-duction of narrow-spectrum agents (penicillin, trimethoprim, gentamicin), along with infection control practices have been successful in reducing the occurrence of specific infections in the hospital setting (12). Unfortunately, ICU patients often have already received prior antimicrobial treatment, making it more likely that they will be infected with an antibiotic-resistant pathogen (8). Therefore, initial empiric treatment with broad-spectrum agents is often initially necessary for hospitalized patients to avoid inappropriate treatment until culture results become available and de-escalation can occur (Fig. 83.1) (18).
LWBK1580_C83_p964-981.indd 975 29/07/17 11:37 AM

976 SeCtion 9 infeCtious Disease
Combination antibiotic Therapy
Several meta-analyses recommend the use of monotherapy with a β-lactam antibiotic, as opposed to combination ther-apy including an aminoglycoside, for the definitive treatment of severe sepsis once antimicrobial susceptibilities are known (66,67). Additionally, there is no definitive evidence that the emergence of antibiotic resistance is reduced by the use of com-bination antimicrobial therapy. However, empiric combination therapy directed against high-risk pathogens such as P. aeru-ginosa should be encouraged until the results of antimicrobial susceptibility become available. Such an approach to empiric treatment can increase the likelihood of providing appropriate initial antimicrobial therapy with improved outcomes (19).
Shorter Courses of antibiotic Treatment
Prolonged administration of antibiotics to hospitalized patients has been shown to be an important risk factor for the emer-gence of colonization and infection with antibiotic-resistant bacteria (8,16). Therefore, attempts have been made to reduce the duration of antibiotic treatment for specific bacterial infec-tions. Several clinical trials have found that 7 to 8 days of anti-biotic treatment is acceptable for most nonbacteremic patients with VAP (15,37). Similarly, shorter courses of antibiotic treat-ment have been successfully used in patients at low risk for VAP (36,37,59), with pyelonephritis (68), and for CAP (69). In general, the shorter-course treatment regimens have been associated with a significantly lower risk for the emergence of antimicrobial resistance and several guidelines for the antibi-otic management of nosocomial pneumonia and severe sepsis currently recommend the discontinuation of empiric antibiotic therapy after 48 to 72 hours if cultures are negative or the signs of infection have resolved (70,71). There are clinical scenarios in which shorter durations of therapy may not be appropriate, including fungemia, endocarditis, osteomyelitis, meningitis, and VAP caused by P. aeruginosa or other nonfermenters. In ICU patients, all antimicrobials should be reviewed on a daily basis to ensure they are needed (59).
De-escalation approach for the antibiotic Treatment of Serious Infection in the Hospitalized Patient
After an initial, appropriately broad-spectrum, antibiotic regi-men is prescribed, modification of the regimen using a de-esca-lation strategy should occur based on the results of the patient’s clinical response and microbiologic testing (Fig. 83.2). Based on the de-escalation strategy, modification of the initial anti-biotic regimen should include decreasing the number and/or spectrum of antibiotics, if possible based on culture and sen-sitivity results, shortening the duration of therapy in patients with uncomplicated infections who are demonstrating signs of clinical improvement, or discontinuing antibiotics altogether in patients who have a noninfectious cause identified accounting for the patient’s signs and symptoms. A number of strategies have been used to promote de-escalation including the use of computer decision support systems, protocol-guided therapies, and clinical pharmacist–supported guidelines (60,72–74).
PHArMAcokInetIc conSIderAtIonS
Optimizing Pharmacokinetic/Pharmacodynamic (Pk/Pd) Principles
Antibiotic concentrations that are sublethal can promote the emergence of resistant pathogens. Optimization of antibiotic regimens on the basis of pharmacokinetic/pharmacodynamic principles could play a role in the reduction of antibiotic resistance (13). The duration of time the serum drug concen-tration remains above the MIC of the antibiotic (T > MIC) enhances bacterial eradication with β-lactams, carbapenems, monobactams, glycopeptides, and oxazolidinones (Fig. 83.3). Frequent dosing, prolonged infusion times, or continuous infu-sions can increase the T greater than MIC and improve clini-cal and microbiologic cure rates. To maximize the bactericidal
Step 1: Initial suspicion of serious infection in critically ill patient:
Step 2: Subsequent evaluation of clinical and microbiologic date:
ClinicalImprovement
Lack ofClinical
Improvement
Evaluate patient’s clinicalresponse at 48–72 hours
(temperature, white blood cellcount, organ function)
• Narrow antimicrobial spectrum based on microbiologic data (Figure 2)
• Reassess antimicrobial need beyond 7 days (unless bactermia is present)
Reassess patient for the following:
Obtain appropriatespecimens for culture and
special stains
Begin initial antimicrobial based onrisk factors for antibiotic-resistant pathogens
(resistant hospitalization or antibiotictherapy, admission from nursing home,
late-onset infection)
• Pathogen(s) resistant to inital therapy• Unidentifield source of infection• Complication of infection (abscess)• Noninfectious cause (drug fever)
Consider a change in antimicrobial therapy(Tables 3 and 4)
fIgure 83.1 Clinical algorithm for the de-escalation approach to antibiotic treatment of serious infections in patients with risk factors for multidrug-resistant pathogens. optimally, de-escalation of antimicrobial treatment would always occur once the pathogen causing infection and its antimicrobial suscepti-bility are known.
LWBK1580_C83_p964-981.indd 976 29/07/17 11:37 AM

Chapter 83 antibiotics in the Management of serious hospital-acquired infections 977
effects of aminoglycosides, clinicians must optimize the maxi-mum drug concentration (Cmax)-to-MIC ratio. A Cmax:MIC ratio of at least 10:1 using once-daily aminoglycoside dosing (5–7 mg/kg) has been associated with preventing the emer-gence of resistant organisms, improving clinical response to treatment, and avoiding toxicity. The 24-hour area under the antibiotic concentration curve-to-MIC ratio (AUIC) is corre-lated with fluoroquinolone efficacy and prevention of resis-tance development. An AUIC value higher than 100 has been associated with a significant reduction in the risk of resistance development while on therapy. As a general rule, clinicians should use the maximum approved dose of an antibiotic for a potentially life-threatening infection to optimize tissue concen-trations of the drug and killing of pathogens.
Augmented Renal Clearance
Augmented renal clearance (ARC) is defined as an 8-hour creati-nine clearance more than or equal to 130 mL/min/1.73 m2 (39). It has been suggested that a large proportion of ICU patients experience at least one occasion of ARC during the first 7 days of their critical illness (75). ARC has been linked with subtherapeu-tic β-lactam (76) and glycopeptide concentrations (77), as well
as increased therapeutic failures in patients receiving antimicro-bial therapy resulting in adverse patient outcomes (78,79). Addi-tionally, data suggest that shorter durations of therapy among patients with ARC, and thus lower circulating antibiotic levels, may contribute to excess mortality (80).
A scoring system to identify patients at high risk for ARC has been developed (81) and validated with a 100% sensitiv-ity and 71.4% specificity (82). The following factors were included: age of 50 years or younger (6 points), trauma (3 points), and SOFA score of 4 or less (1 point). Monte Carlo pharmacokinetic simulations demonstrated increased time at therapeutic antibiotic levels with the use of extended infusion dosing in the setting of ARC at a drug cost savings of up to 66.7% over multiple intermittent dosing regimens. In addi-tion to ARC, the use of renal replacement therapies can also result in under exposure of antibiotics at the site of infection requiring careful dosing adjustments (83).
Therapeutic Drug Monitoring
The use of therapeutic drug monitoring (TDM) for antibiot-ics other than vancomycin, aminoglycosides, and voriconazole has not become a routine or standard practice in most ICUs. TDM for β-lactams and carbapenems can be accomplished by several methodologies (84,85). Unfortunately, at the present time, large variations exist in the type of β-lactams tested, the patients selected for TDM, drug assay methodologies, Pk/Pd targets, and dose-adjustment strategies employed in the criti-cally ill (86). Further studies are needed to determine which patients should receive TDM and how best to perform it, to include robustly defining Pk/Pd targets and dosing adjustments for optimizing β-lactam and carbapenem delivery.
controverSIeS
Antibiotic Cycling and Scheduled Antibiotic Changes
The concept of antibiotic class cycling, in which a class of anti-biotics or a specific drug is withdrawn from use for a defined period of time and later reintroduced, has been suggested as
Escalation/De-escalation
Increasing
Decreasing
Narrow BroadN
umbe
r of
Ant
imic
robi
als
De-escalation
De-escalation De-escalation
Antibiotic Spectrum of Activity
Initial AntimicrobialRegimen
Escalation Escalation
Escalation
Escalation
fIgure 83.2 antimicrobial de-escalation promotes initial administration of broad-spectrum antibiotics to patients at risk for infection with multidrug-resistant patho-gens, followed by the reduction of the number of antimicrobials used and/or their spectrum of activity based on subsequent pathogen identification and antimicrobial susceptibility testing.
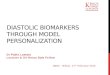
Pharmacodynamic Parameters
Cmax (Peak Concentration)
AUC
Dru
g C
once
ntra
tion
Time
fIgure 83.3 Pharmacodynamic parameters found to be important for the efficacy of antimicrobial agents. auC, area under the concentra-tion–time curve; Cmax, maximum concentration; MiC, minimum inhibitory concentration; t, time.
LWBK1580_C83_p964-981.indd 977 29/07/17 11:37 AM

978 SeCtion 9 infeCtious Disease
a potential strategy for reducing the emergence of antimicro-bial resistance (12). Early mathematical modeling suggested that the use of antibiotic cycling would be inferior to mixing empiric antibiotics as a strategy to reduce the emergence of antimicrobial resistance (87). Subsequent studies of antimicro-bial cycling have found beneficial effects on antibiotic resis-tance, including a 2014 meta-analysis of 11 clinical studies demonstrating that antibiotic cycling reduced the number of resistant infections (88,89). Although antimicrobial heteroge-neity or mixing seems to be a logical policy, simple cycling of antibiotics combined with prolonged treatment exposures seems to be a strategy that will only promote further antibiotic resistance.
Antimicrobial Decolonization Strategies
The prophylactic administration of parenteral antibiotics has been shown to reduce the occurrence of nosocomial infections in specific high-risk patient populations requiring intensive care (90). Similarly, selective digestive decontamination with topical antibiotics, with or without concomitant parenteral antibiotics, has also been shown to be effective at reducing nosocomial infections caused by the targeted organism(s) (91,92). However, the routine use of selective digestive decon-tamination has also been linked to the emergence of antimi-crobial resistance (93). Similarly, selective oropharyngeal decontamination has also produced mixed results (93–96). Based on these studies, antimicrobial and non-antimicrobial agents should be considered for oral decontamination only in appropriate high-risk ICU patients or to assist in the contain-ment of outbreaks of MDR bacterial infections in conjunction with established infection control practices.
Use of Antibiotic Resistance Prediction Tools
Knowledge of patient risk factors for the presence of infection with antibiotic-resistant pathogens should be a routine part of antibiotic decision making and can be used in a de-escalation algorithm. For example, antibiotic-resistant pathogens are more commonly found in patients with CAP who have health care–associated risk factors (recent hospitalization, admission from a nursing home, recent antibiotic treatment). Shorr et al. examined patients admitted with pneumonia and found four variables predictive of antibiotic-resistant pneumonia: recent hospitalization, nursing home residence, hemodialysis, and ICU admission (97). A scoring system assigning 4, 3, 2, and 1 points, respectively, for each variable had moderate predic-tive power for segregating those with and without resistant bacteria. Among patients with fewer than 3 points, the preva-lence of resistant pathogens was less than 20% compared with 55% and more than 75% in persons with scores ranging from 3 to 5 and more than 5 points, respectively (p < 0.001). In an independent population, this score better identified patients infected with resistant bacteria than the definition of HCAP (98). Similarly, a 2014 meta-analysis also found that the cur-rent definition of HCAP did not accurately identify infections caused by antibiotic-resistant pathogens, further underscoring the need for more objective criteria to determine patients’ risk for resistant infections (99).
Independent risk factors for antibiotic-resistant bacteria have been demonstrated in both patients diagnosed with CAP and HCAP including prior hospitalization, immunosuppression,
previous antibiotic use, use of gastric acid–suppressive therapy, tube feeding, and nonambulatory status (100). In another pro-spective study of CAP and HCAP patients, MDR pathogens were more common in patients with HCAP (101). Basing empiric antibiotic therapy on disease severity and the presence of multiple risk factors for MDR pathogens may be a poten-tially useful approach that achieves good outcomes without excessive use of broad-spectrum antibiotic therapy. However, it is not clear that clinicians can effectively apply such prediction tools prospectively in order to target broad-spectrum antibiotics to patients at greatest risk for infection with antibiotic-resistant infections.
Clinical decision support systems represent one way of automating informatics data, to include potential risk fac-tors for infection with antibiotic-resistant bacteria, for bed-side decision making (74,102). Other specific examples of benefits derived from the use of computerized systems include improvements in the efficiency and costs of existing steward-ship programs, improvements in clinicians’ knowledge regard-ing the treatment of infectious diseases, and improvements in pathogen prediction (102–108). These data suggest that an opportunity exists to employ hospital informatics systems to improve the identification of patients infected with antibiotic-resistant bacteria in order to prescribe more appropriate initial therapy.
Biomarker Guidance of Antibiotic Therapy
When prescribing antimicrobial therapy, clinicians frequently look for objective indicators that antibiotic treatment is appropriate and to determine duration of treatment. Procalci-tonin (PCT), a precursor of calcitonin that is rapidly released into the bloodstream in the presence of an infection, has dem-onstrated utility in guiding decisions regarding antimicrobial therapy (109–111). However, not all experiences with PCT-guided decision making have shown reductions in duration of antibiotic exposure (112,113). A recent comprehensive lit-erature review of PCT-guided antibiotic management in criti-cally ill patients found that the diagnostic value of serum PCT concentrations to discriminate among systemic inflammatory response syndrome (SIRS), sepsis, severe sepsis, and septic shock was unestablished (114). Moreover, although higher PCT concentrations suggest the presence of a systemic bacte-rial infection as opposed to a viral, fungal, or inflammatory etiology of sepsis, serum PCT concentrations did not corre-late with the severity of sepsis or with mortality and therefore should not be employed to dictate the timing and appropriate-ness of escalation of antimicrobial therapy in septic patients (114). On the other hand, at least two meta-analyses suggest that PCT guidance can be used to shorten the duration of anti-microbial therapy in the ICU setting (115,116). The routine use of PCT as an aid in antibiotic decision making should depend on whether or not a particular ICU has an already established culture of successful antimicrobial de-escalation and stewardship (59).• The serum markers, (1,3)-β-D-glucan and galactomannan,
have been used in identifying pathogens associated with invasive fungal infections to assist clinicians in guiding anti-fungal therapy. Fungal infections often present a consider-able diagnostic challenge to clinicians, and mere suspicion of these infections often leads to liberal and prolonged antimicrobial use. Based on their high negative predictive
LWBK1580_C83_p964-981.indd 978 29/07/17 11:37 AM

Chapter 83 antibiotics in the Management of serious hospital-acquired infections 979
value in the appropriate clinical setting, the most suitable use of these markers seems to be in excluding the pres-ence of invasive fungal infections (117,118). However, one study suggests that (1,3)-β-D-glucan may be the most rapid method for the identification of intra-abdominal candidiasis in order to provide timely therapy in such patients (119). In addition, an investigation that measured galactomannan levels in BAL fluid obtained from ICU patients lends sup-port to its use in pathogen identification and early treatment of pulmonary infection (120). Nonetheless, a more recent study only showed modest agreement between galactoman-nan in BAL fluid and validated clinical diagnostic criteria for invasive fungal disease (121). These markers of infec-tion certainly have the potential to enhance stewardship—primarily through de-escalation once a fungal infection has been excluded—and future clinical experience with these markers will determine if this potential can be fully realized.
summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect Con-trol Hosp Epidemiol. 2013;34:1–14.
5. Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomial infections in combined medical-surgical intensive care units in the United States, 1. Infect Control Hosp Epidemiol. 2000;21:510–515.
6. Leung WS, Chu CM, Tsang KY, et al. Fulminant community-acquired Aci-netobacter baumannii pneumonia as a distinct clinical syndrome. Chest. 2006;129:102–109.
7. Paterson DL, Bonomo RA. Extended-spectrum beta-lactamases: a clinical update. Clin Micro Rev. 2005;18:657–686.
8. Trouillet JL, Chastre J, Vuagnat A, et al. Ventilator-associated pneumonia caused by potentially drug-resistant bacteria. Am J Respir Crit Care Med. 1998;157:531–539.
9. Rello J, Sa-Borges M, Correa H, et al. Variations in etiology of ventilator-associated pneumonia across four treatment sites: implications for antimicro-bial prescribing practices. Am J Respir Crit Care Med. 1999;160:608–613.
10. Masterton RG, Kuti JL, Turner PJ, et al. The OPTIMA programme: utiliz-ing MYSTIC (2002) to predict critical pharmacodynamic target attain-ment against nosocomial pathogens in Europe. J Antimicrob Chemother. 2005;55:71–77.
11. Namias N, Samiian L, Nino D, et al. Incidence and susceptibility of patho-genic bacteria vary between intensive care units within a single hospital: implications for empiric antibiotic strategies. J Trauma. 2000;49:638–645.
12. Kollef MH, Fraser VJ. Antibiotic resistance in the intensive care unit. Ann Intern Med. 2001;134:298–314.
13. Kollef MH, Micek ST. Strategies to prevent antimicrobial resistance in the intensive care unit. Crit Care Med. 2005;33:1845–1853.
14. Kollef MH, Micek ST. Methicillin-resistant Staphylococcus aureus: a new community-acquired pathogen. Curr Opin Infect Dis. 2006;19:161–168.
15. Chastre J, Wolff M, Fagon JY, et al; PneumA Trial Group. Comparison of 15 vs. 8 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA. 2003;290:2588–2598.
16. Dennesen PJ, van der Ven AJ, Kessels AG, et al. Resolution of infectious parameters after antimicrobial therapy in patients with ventilator-associ-ated pneumonia. Am J Respir Crit Care Med. 2001;163:1371–1375.
17. Ibrahim EH, Sherman G, Ward S, et al. The influence of inadequate anti-microbial treatment of bloodstream infections on patient outcomes in the ICU setting. Chest. 2000;118:146–155.
18. Kollef MH. Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000;31:S131–S138.
19. Micek ST, Lloyd AE, Ritchie DJ, et al. Pseudomonas aeruginosa blood-stream infection: importance of appropriate initial antimicrobial treat-ment. Antimicrob Agents Chemother. 2005;49:1306–1311.
20. Dhainaut JF, Laterre PF, LaRosa S, et al. The clinical evaluation commit-tee in a large multicenter phase 3 trial of drotrecogin alfa (activated) in patients with severe sepsis (PROWESS): role, methodology, and results. Crit Care Med. 2003;31:2291–2301.
21. Harbarth S, Garbino JK, Pugin J, et al. Inappropriate initial antimicrobial therapy and its effects on survival in a clinical trial of immunomodulating therapy for severe sepsis. Am J Med. 2003;115:529–535.
22. Garnacho-Montero J, Garcia-Garmendia JL, Barrero-Almodovar A, et al. Impact of adequate empirical antibiotic therapy on the outcome of patients admitted to the intensive care unit with sepsis. Crit Care Med. 2003;31: 2742–2751.
23. Kollef MH, Ward S. The influence of mini-BAL cultures on patient out-comes: implications for the antibiotic management of ventilator-associated pneumonia. Chest. 1998;113:412–420.
24. Rello J, Ollendorf DA, Oster G, et al. Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest. 2002;122:2115–2121.
25. Shorr AF, Combes A, Kollef MH, Chastre J. Methicillin-resistant Staphy-lococcus aureus prolongs intensive care unit length of stay in ventilator-associated pneumonia—despite initially appropriate antibiotic therapy. Crit Care Med. 2006;34:700–706.
26. Anhalt JP, Fenselau C. Identification of bacteria using mass spectrometry. Anal Chem. 1975;47(2):219–225.
27. La Scola B, Raoult D. Direct identification of bacteria in positive blood culture bottles by matrix-assisted laser desorption ionization time-of-flight mass spectrometry. PLoS One. 2009;4(11):e8041.
28. Huang A, Newton D, Kunapuli A, et al. Impact of rapid organism identi-fication via matrix-assisted laser desorption/ionization time-of-flight com-bined with antimicrobial stewardship team intervention in adult patients with bacteremia and candidemia. Clin Infect Dis. 2013;57(9):1237–1245.
29. Croxatto A, Prod’hom G, Greub G. Application of MALDI-TOF mass spectrometry in clinical diagnostic microbiology. FEMS Mircrobiol Rev. 2012;36:380–407.
• Initial treatment with an appropriate antibiotic regi-men is one of the most important factors influencing the outcome of critically ill patients with infection.• Infection with antibiotic-resistant microorganisms
increases the likelihood that inappropriate initial antibiotic therapy will be prescribed to critically ill patients.
• The prevalence of antibiotic resistance varies locally and regionally.
• Host factors influence the likelihood that a patient will be infected with antibiotic-resistant pathogens (e.g., prior hospitalization or antibiotic treatment, admission from a nursing home or other high-risk environment).
• Efforts should be made to rapidly identify the source and site of infection and to obtain specimens for cul-ture, antimicrobial susceptibility testing, and rapid diagnostic tests. Obtaining these specimens should not delay initial empiric therapy in a critically ill patient.
• Avoidance of unnecessary antibiotic exposure in the ICU setting is important to reduce the emergence of and subsequent infection with antibiotic-resistant microorganisms.
• Optimization of antibiotic regimens using pharmaco-kinetic and pharmacodynamic principles to minimize organism exposure to sublethal antimicrobial concen-trations could play a role in the reduction of antibiotic resistance.
key Points
References 1. National Nosocomial Infections Surveillance (NNIS) system report, data
summary from January 1992-April 2000, issued June 2000. Am J Infect Control. 2000;28:429–448.
2. Gaynes R, Edwards JR. National Nosocomial Infections Surveillance Sys-tem. Overview of nosocomial infections caused by gram-negative bacilli. Clin Infect Dis. 2005;41:848–854.
3. Dudeck MA, Weiner LM, Allen-Bridson K, et al. National Healthcare Safety Network (NHSN) report, data summary for 2012: device-associ-ated module. Am J Infect Control. 2013;41:1148–1166.
4. Sievert DM, Ricks P, Edwards JR, et al. National Healthcare Safety Net-work (NHSN) Team and Participating NHSN Facilities. Antimicrobial-resistant pathogens associated with healthcare-associated infections:
LWBK1580_C83_p964-981.indd 979 29/07/17 11:37 AM

980 SeCtion 9 infeCtious Disease
30. Harris DM, Hata DJ. Rapid identification of bacteria and Candida using PNA-FISH from blood and peritoneal fluid cultures: a retrospective clini-cal study. Ann Clin Microbiol Antimicrob. 2013;22:2–9.
31. Ly T, Gulia J, Pyrgos V, et al. Impact upon clinical outcomes of translation of PNA FISH-generated laboratory data from the clinical microbiology bench to bedside in real time. Ther Clin Risk Manag. 2008;4(3):637–640.
32. Samuel LP, Tibbetts RJ, Agotesku A, et al. Evaluation of a microarray-based assay for rapid identification of positive organisms and resistance markers in positive blood cultures. J Clin Microbiol. 2013;51(4):1188–1192.
33. Fishbain JT, Sinyavskiy O, Riederer K, et al. Detection of extended-spec-trum beta-lactamase and Klebsiella pneumoniae carbapenemase genes directly from blood cultures by use of a nucleic acid microarray. J Clin Microbiol. 2012;50(9):2901–2904
34. Cleven BE, Palka-Santini M, Gielen J, et al. Identification and character-ization of bacterial pathogens causing bloodstream infections by DNA microarray. J Clin Microbiol. 2006;44(7):2389–2397.
35. Shorr AF, Sherner JH, Jackson WL, et al. Invasive approaches to the diag-nosis of ventilator-associated pneumonia: a meta-analysis. Crit Care Med. 2005;33:46–53.
36. Kollef MH, Kollef KE. Antibiotic utilization and outcomes for patients with clinically suspected ventilator-associated pneumonia and negative quantitative BAL culture results. Chest. 2005;128:2706–2713.
37. Singh N, Rogers P, Atwood CW, et al. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit: a proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 2000;162:505–511.
38. Tenover FC. Mechanisms of antimicrobial resistance in bacteria. Am J Med. 2006;119:s3–s10.
39. Howden BP, Ward PB, Charles PG, et al. Treatment outcomes for seri-ous infections caused by methicillin-resistant Staphylococcus aureus with reduced vancomycin susceptibility. Clin Infect Dis. 2004;38:521–528.
40. Fridkin SK, Hageman J, McDougal LK, et al. Epidemiological and micro-biological characterization of infections caused by Staphylococcus aureus with reduced susceptibility to vancomycin, United States, 1997–2001. Clin Infect Dis. 2003;36:429–439.
41. Sakoulas G, Moellering RC, Eliopoulos GM. Adaptation of methicillin-resistant Staphylococcus aureus in the face of vancomycin therapy. Clin Infect Dis. 2006;42:S40–S50.
42. H.R. 2182—112th Congress: Generating Antibiotic Incentives Now Act of 2011. Available at: https://www.govtrack.us/congress/bills/112/hr2182. Accessed March 19, 2015.
43. Arhin FF, Draghi DC, Pillar CM, et al. Comparative in vitro activity profile of oritavancin against recent gram-positive clinical isolates. Antimicrob Agents Chemother. 2009;53(11):4762–4771.
44. Mendes RE, Farrell DJ, Sader HS, Jones RN. Oritavancin microbiologic features and activity results from the surveillance program in the United States. Clin Infect Dis. 2012;54(Suppl 3):S203–S213.
45. Orbactiv® [package insert]. Parsippany, NJ: The Medicines Company; 2014.
46. Shaw KJ, Poppe S, Schaadt R, et al. In vitro activity of TR-700, the anti-bacterial moiety of the prodrug TR-701, against linezolid-resistant strains. Antimicrob Agents Chemother. 2008;52(12):4442–4447.
47. Prokocimer P, De Anda C, Fang E, et al. Tedizolid phosphate vs linezolid for treatment of acute bacterial skin and skin structure infections: the ESTABLISH-1 randomized trial. JAMA. 2013;309(6):559–569.
48. Saravolatz LD, Stein GE, Johnson LB. Ceftaroline: a novel cephalospo-rin with activity against methicillin-resistant Staphylococcus aureus. Clin Infect Dis. 2011;52(9):1156–1163.
49. Lim L, Sutton E, Brown J. Ceftaroline: a new broad-spectrum cephalospo-rin. Am J Health Syst Pharm. 2011;68(6):491–498.
50. Craig WA, Andes DR. In vivo activities of ceftolozane, a new cephalo-sporin, with and without tazobactam against Pseudomonas aerugi-nosa and Enterobacteriaceae, including strains with extended-spectrum β-lactamases, in the thighs of neutropenic mice. Antimicrob Agents Che-mother. 2013;57(4):1577–1582.
51. Zhanel GG, Chung P, Adam H, et al. Ceftolozane/tazobactam: a novel cephalosporin/β-lactamase inhibitor combination with activity against multidrug-resistant gram-negative bacilli. Drugs. 2014;74(1):31–51.
52. Sader HS, Castanheira M, Flamm RK, et al. Antimicrobial activity of ceftazidime-avibactam against gram-negative organisms collected from U.S. medical centers in 2012. Antimicrob Agents Chemother. 2014;58(3): 1684–1692.
53. Keepers TR, Gomez M, Celeri C, et al. Bactericidal activity, absence of serum effect, and time-kill kinetics of ceftazidime-avibactam against β-lactamase–producing Enterobacteriaceae and Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2014;58(9):5297–5305.
54. Vardakas KZ, Rafailidis PI, Konstantelias AA, Falagas ME. Predictors of mortality in patients with infections due to multi-drug resistant gram nega-tive bacteria: the study, the patient, the bug or the drug? J Infect. 2013;66(5): 401–414.
55. Kollef MH, Sherman G, Ward S, et al. Inadequate antimicrobial treat-ment of infections: a risk factor for hospital mortality among critically ill patients. Chest. 1999;115(2):462–474.
56. Labelle AJ, Micek ST, Roubinian N, Kollef MH. Treatment-related risk factors for hospital mortality in Candida bloodstream infections. Crit Care Med. 2008;36(11):2967–2972.
57. Kollef M, Micek S, Hampton N, et al. Septic shock attributed to Candida infection: importance of empiric therapy and source control. Clin Infect Dis. 2012;54(12):1739–1746.
58. Bassetti M, Righi E, Ansaldi F, et al. A multicenter study of septic shock due to candidemia: outcomes and predictors of mortality. Intensive Care Med. 2014;40(6):839–845.
59. Micek ST, Ward S, Fraser VJ, et al. A randomized controlled trial of an antibiotic discontinuation policy for clinically suspected ventilator-associ-ated pneumonia. Chest. 2004;125:1791–1799.
60. Jenkins TC, Knepper BC, Sabel AL, et al. Decreased antibiotic utilization after implementation of a guideline for inpatient cellulitis and cutaneous abscess. Arch Intern Med. 2011;171(12):1072–1079.
61. Malani AN, Richards PG, Kapila S, et al. Clinical and economic outcomes from a community hospital’s antimicrobial stewardship program. Am J Infect Control. 2013;41(2):145–148.
62. Ambroggio L, Thomson J, Murtagh Kurowski E, et al. Quality improve-ment methods increase appropriate antibiotic prescribing for childhood pneumonia. Pediatrics. 2013;131(5):e1623–e1631.
63. Morrill HJ, Gaitanis MM, LaPlante KL. Antimicrobial stewardship pro-gram prompts increased and earlier infectious diseases consultation. Anti-microb Resist Infect Control. 2014;3:12.
64. Pasquale TR, Trienski TL, Olexia DE, et al. Impact of an antimicrobial stewardship program on patients with acute bacterial skin and skin struc-ture infections. Am J Health Syst Pharm. 2014;71(13):1136–1139.
65. Wenisch JM, Equiluz-Bruck S, Fudel M, et al. Decreasing Clostrid-ium difficile infections by an antimicrobial stewardship program that reduces moxifloxacin use. Antimicrob Agents Chemother. 2014;58(9): 5079–5083.
66. Paul M, Benuri-Silbiger I, Soares-Weiser K, Leibovici L. Beta-lactam monotherapy versus beta-lactam-aminoglycoside combination therapy for sepsis in immunocompetent patients: systematic review and meta-analysis of randomized trials. BMJ. 2004;328:668.
67. Safdar N, Handelsman J, Maki DG. Does combination antimicrobial therapy reduce mortality in gram-negative bacteraemia? A meta-analysis. Lancet Infect Dis. 2004;4:519–527.
68. Talan DA, Stamm WE, Hooton TM, et al. Comparison of ciprofloxacin (7 days) and trimethoprim-sulfamethoxazole (14 days) for acute uncom-plicated pyelonephritis in women: a randomized trial. JAMA. 2000; 283:1583–1590.
69. Dunbar LM, Wunderink RG, Habib MP, et al. High-dose, short-course levofloxacin for community-acquired pneumonia: a new treatment para-digm. Clin Infect Dis. 2003;37:752–760.
70. Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis Campaign Management Guidelines Committee. Surviving Sepsis Campaign guide-lines for management of severe sepsis and septic shock. Crit Care Med. 2004;32:858–873.
71. American Thoracic Society, Infectious Diseases Society of America. Guide-lines for the management of adults with hospital-acquired, ventilator-asso-ciated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388–416.
72. Rello J, Vidaur L, Sandiumenge A, et al. De-escalation therapy in ventila-tor-associated pneumonia. Crit Care Med. 2004;32(11):2183–2190.
73. Ibrahim EH, Ward S, Sherman G, et al. Experience with a clinical guide-line for the treatment of ventilator-associated pneumonia. Crit Care Med. 2001;29(6):1109–1115.
74. Thursky KA, Buising KL, Bak N, et al. Reduction of broad-spectrum anti-biotic use with computerized decision support in an intensive care unit. Int J Qual Health Care. 2006;18(3):224–231.
75. Udy AA, Baptista JP, Lim NL, et al. Augmented renal clearance in the ICU: results of a multicenter observational study of renal function in critically ill patients with normal plasma creatinine concentrations. Crit Care Med. 2014;42(3):520–527.
76. Carlier M, Carrette S, Roberts JA, et al. Meropenem and piperacillin/tazo-bactam prescribing in critically ill patients: Does augmented renal clear-ance affect pharmacokinetic/ pharmacodynamic target attainment when extended infusions are used? Crit Care. 2013;17(3):R84.
LWBK1580_C83_p964-981.indd 980 29/07/17 11:37 AM

Chapter 83 antibiotics in the Management of serious hospital-acquired infections 981
77. Baptista JP, Sousa E, Martins PJ, Pimentel JM. Augmented renal clear-ance in septic patients and implications for vancomycin optimisation. Int J Antimicrob Agents. 2012;39(5):420–423.
78. Roberts JA, Paul SK, Akova M, et al. DALI: defining antibiotic levels in intensive care unit patients: Are current β-lactam antibiotic doses sufficient for critically ill patients? Clin Infect Dis. 2014;58(8):1072–1083.
79. Claus BO, Hoste EA, Colpaert K, et al. Augmented renal clearance is a common finding with worse clinical outcome in critically ill patients receiving antimicrobial therapy. J Crit Care. 2013;28(5):695–700.
80. Kollef MH, Chastre J, Clavel M, et al. A randomized trial of 7-day doripe-nem versus 10-day imipenem-cilastatin for ventilator-associated pneumo-nia. Crit Care. 2012;16(6):R218.
81. Udy AA, Roberts JA, Shorr AF, et al. Augmented renal clearance in septic and traumatized patients with normal plasma creatinine concentrations: identifying at-risk patients. Crit Care. 2013;17(1):R35.
82. Akers KS, Niece KL, Chung KK, et al. Modified Augmented Renal Clear-ance score predicts rapid piperacillin and tazobactam clearance in criti-cally ill surgery and trauma patients. J Trauma Acute Care Surg. 2014;77 (3 Suppl 2):S163–S170.
83. De Waele JJ, Carlier M. Beta-lactam antibiotic dosing during continu-ous renal replacement therapy: How can we optimize therapy? Crit Care. 2014;18(3):158.
84. Barco S, Bandettini R, Maffia A, et al. Quantification of piperacillin, tazobac-tam, meropenem, ceftazidime, and linezolid in human plasma by liquid chro-matography/tandem mass spectrometry. J Chemother. 2015;27(6):343–347.
85. Zander J, Maier B, Suhr A, et al. Quantification of piperacillin, tazobac-tam, cefepime, meropenem, ciprofloxacin and linezolid in serum using an isotope dilution UHPLC-MS/MS method with semi-automated sample preparation. Clin Chem Lab Med. 2015;53(5):781–791.
86. Wong G, Brinkman A, Benefield RJ, et al. An international, multicentre survey of β-lactam antibiotic therapeutic drug monitoring practice in intensive care units. J Antimicrob Chemother. 2014;69(5):1416–1423.
87. Bergstrom CT, Lo M, Lipsitch M. Ecological theory suggests that antimi-crobial cycling will not reduce antimicrobial resistance in hospitals. Proc Natl Acad Sci USA. 2004;101:13285–13290.
88. Sarraf-Yazdi S, Sharpe M, Bennett KM, et al. A 9-year retrospective review of antibiotic cycling in a surgical intensive care unit. J Surg Res. 2012; 176(2)e73–e78.
89. Abel zur Wiesch P, Kouyos R, Abel S, et al. Cycling empirical antibi-otic therapy in hospitals: meta-analysis and models. PLoS Pathogens. 2014;10(6):e1004225.
90. Sirvent JM, Torres A, El-Ebiary M, et al. A protective effect of intrave-nously administered cefuroxime against nosocomial pneumonia in patients with structural coma. Am J Respir Crit Care Med. 1997;155:1729–1734.
91. Krueger WA, Lenhart FP, Neeser G, et al. Influence of combined intra-venous and topical antibiotic prophylaxis on the incidence of infections, organ dysfunctions, and mortality in critically ill surgical patients: a pro-spective, stratified, randomized, double-blind, placebo-controlled clinical trial. Am J Respir Crit Care Med. 2002;166:1029–1037.
92. de Smet AM, Kluytmans JA, Cooper BS, et al. Decontamination of the digestive tract and oropharynx in ICU patients. N Engl J Med. 2009; 360:20–31.
93. Oostdijk EA, Kesecioglu J, Schultz MJ, et al. Effects of decontamination of the oropharynx and intestinal tract on antibiotic resistance in ICUs. JAMA. 2014;312(14):1429–1437.
94. Kollef MH, Pittet D, Sánchez García M, et al. A randomized, double-blind, placebo-controlled, multinational phase III trial of iseganan in pre-vention of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2006;173:91–97.
95. Fourrier F, Dubois D, Pronnier P, et al. Effect of gingival and dental plaque antiseptic decontamination on nosocomial infections acquired in the inten-sive care unit: a double-blind placebo-controlled multicenter study. Crit Care Med. 2005;33:1728–1735.
96. Koeman M, van der Van A, Hak E, et al. Oral decontamination with chlorhexidine reduces the incidence of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2006;173:1348–1355.
97. Shorr AF, Zilberberg MD, Micek ST, Kollef MH. Prediction of infection due to antibiotic-resistant bacteria by select risk factors for health care-associated pneumonia. Arch Intern Med. 2008;168(20):2205–2210.
98. Shorr AF, Zilberberg MD, Reichley R, et al. Validation of a clini-cal score for assessing the risk of resistant pathogens in patients with pneumonia presenting to the emergency department. Clin Infect Dis. 2012;54(2):193–198.
99. Chalmers JD, Rother C, Salih W, Ewig S. Healthcare-associated pneumo-nia does not accurately identify potentially resistant pathogens: a system-atic review and meta-analysis. Clin Infect Dis. 2014;58(3):330–339.
100. Shindo Y, Ito R, Kobayashi D, et al. Risk factors for drug-resistant patho-gens in community-acquired and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2013;188(8):985–995.
101. Maruyama T, Fujisawa T, Okuno M, et al. A new strategy for healthcare-associated pneumonia: a 2-year prospective multicenter cohort study using risk factors for multidrug-resistant pathogens to select initial empiric ther-apy. Clin Infect Dis. 2013;57(10):1373–1383.
102. Micek ST, Heard KM, Gowan M, Kollef MH. Identifying critically ill patients at risk for inappropriate antibiotic therapy: a pilot study of a point-of-care decision support alert. Crit Care Med. 2014;42(8): 1832–1838.
103. Evans RS, Pestotnik SL, Classen DC, et al. A computer-assisted manage-ment program for antibiotics and other anti-infective agents. N Engl J Med. 1998;338(4):232–238.
104. Pestotnik SL, Classen DC, Evans RS, Burke JP. Implementing antibiotic practice guidelines through computer-assisted decision support: clinical and financial outcomes. Ann Intern Med. 1996;124(10):884–890.
105. Paul M, Nielsen AD, Goldberg E, et al. Prediction of specific pathogens in patients with sepsis: evaluation of TREAT, a computerized decision sup-port system. J Antimicrob Chemother. 2007;59(6):1204–1207.
106. McGregor JC, Weekes E, Forrest GN, et al. Impact of a computerized clinical decision support system on reducing inappropriate antimicro-bial use: a randomized controlled trial. J Am Med Inform Assoc. 2006; 13(4):378–384.
107. Bochicchio GV, Smit PA, Moore R, et al. Pilot study of a web-based antibiotic decision management guide. J Am Coll Surg. 2006;202(3): 459–467.
108. Thiel SW, Asghar MF, Micek ST, et al. Hospital-wide impact of a standard-ized order set for the management of bacteremic severe sepsis. Crit Care Med. 2009;37(3):819–824.
109. Stolz D, Smyrnios N, Eggimann P, et al. Procalcitonin for reduced antibi-otic exposure in ventilator-associated pneumonia: a randomised study. Eur Respir J. 2009;34(6):1364–1375.
110. Bouadma L, Luyt CE, Tubach F, et al; PRORATA Trial Group. Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial. Lancet. 2010;375(9713):463–474.
111. Hochreiter M, Köhler T, Schweiger AM, et al. Procalcitonin to guide dura-tion of antibiotic therapy in intensive care patients: a randomized prospec-tive controlled trial. Crit Care. 2009;13(3):R83.
112. Jensen JU, Hein L, Lundgren B, et al. Procalcitonin and Survival Study (PASS) Group. Procalcitonin-guided interventions against infections to increase early appropriate antibiotics and improve survival in the intensive care unit: a randomized trial. Crit Care Med. 2011;39(9):2048–2058.
113. Shehabi Y, Sterba M, Garrett PM, et al. Procalcitonin algorithm in critically ill adults with undifferentiated infection or suspected sepsis: a randomized controlled trial. Am J Respir Crit Care Med. 2014;190(10):1102–1110.
114. Sridharan P, Chamberlain RS. The efficacy of procalcitonin as a biomarker in the management of sepsis: slaying dragons or tilting at windmills? Surg Infect (Larchmt). 2013;14(6):489–511.
115. Prkno A, Wacker C, Brunkhorst FM, Schlattmann P. Procalcitonin-guided therapy in intensive care unit patients with severe sepsis and septic shock: a systematic review and meta-analysis. Crit Care. 2013;17(6):R291.
116. Soni NJ, Samson DJ, Galaydick JL, et al. Procalcitonin-guided antibi-otic therapy: a systematic review and meta-analysis. J Hosp Med. 2013; 8(9):530–540.
117. Maertens J, Deeren D, Dierickx D, Theunissen K. Preemptive antifungal therapy: still a way to go. Curr Opin Infect Dis. 2006;19(6):551–556.
118. Pfeiffer CD, Fine JP, Safdar N. Diagnosis of invasive aspergillosis using a galactomannan assay: a meta-analysis. Clin Infect Dis. 2006;42(10): 1417–1427.
119. Tissot F, Lamoth F, Hauser PM, et al. β-Glucan antigenemia anticipates diagnosis of blood culture-negative intraabdominal candidiasis. Am J Respir Crit Care Med. 2013;188(9):1100–1109.
120. Meersseman W, Lagrou K, Maertens J, et al. Galactomannan in bron-choalveolar lavage fluid: a tool for diagnosing aspergillosis in intensive care unit patients. Am J Respir Crit Care Med. 2008;177(1):27–34.
121. Affolter K, Tamm M, Jahn K, et al. Galactomannan in bronchoalveolar lavage for diagnosing invasive fungal disease. Am J Respir Crit Care Med. 2014;190(3):309–317.
LWBK1580_C83_p964-981.indd 981 29/07/17 11:37 AM