-
8/8/2019 Antibacterial Poly(D,L-Lactic Acid) Coating of Medical
Implants
1/8
Journal of Antimicrobial Chemotherapy (2003) 51, 585591
DOI: 10.1093/jac/dkg105
Advance Access publication 28 January 2003
585
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . .
2003 The British Society for Antimicrobial Chemotherapy
Antibacterial poly(D,L-lactic acid) coating of medical implants
using a
biodegradable drug delivery technology
Hans Gollwitzer1,2*, Karim Ibrahim1, Henriette Meyer1, Wolfram
Mittelmeier2, Raymonde Busch3
and Axel Stemberger1
1Institut fr Experimentelle Onkologie und Therapieforschung;
2Klinik und Poliklinik fr Orthopdie und
Sportorthopdie; 3Institut fr Medizinische Statistik und
Epidemiologie, der Technischen Universitt Mnchen,
Ismaninger Strasse 22, 81675 Munich, Germany
Received 4 September 2002; returned 16 October 2002; revised 26
November 2002; accepted 26 November 2002
Objectives: Biomaterial-associated bacterial infections present
common and challenging com-plications with medical implants. The
purpose of this study was to determine the antibacterialproperties
of a low molecular weight biodegradable poly(D,L-lactic acid)
coating with integratedantibiotics gentamicin and teicoplanin.
Methods: Coating of Kirschner-wires was carried out by a solvent
casting technique underaseptic conditions with and without
incorporated antibiotics. Release kinetics of gentamicin
andteicoplanin were studied in phosphate-buffered saline. Initial
bacterial adhesion of Staphylo-coccus epidermidison coated and bare
implants was determined by radiolabelling and countsof detached
viable organisms.
Results: The incorporated antibiotics showed a continuous
release over a period of at least 96 hwith an initial peak of
release in the first 6 h. Attachment of non-viable microorganisms,
detectedby radiolabelled bacteria, was increased significantly by
the polymer coatings (P< 0.05). Incontrast, the number of viable
bacteria was reduced by the pure polymer (P< 0.01) and further
bythe polymerantibiotic combinations (P< 0.05).
Conclusions: Poly(D,L-lactic acid) coating of implants could
offer new perspectives in preventingbiomaterial-associated
infections. Combinations with other drugs to formulate
custom-tailoredimplant surfaces are feasible.
Keywords: polylactide, PDLLA, drug release, Staphylococcus,
biomaterial
Introduction
Since the first applications of biomaterials in medicine,
infections and deficient tissue-integration represent the
most
important complications, which still limit the unrestricted
use
of biomaterials in humans. Implant-associated infections
account for nearly 50% of the estimated 2 million nosocomial
infections in the United States per year,1 and infection rates
up
to 100% are reported for certain implants, like external
fix-
ation pins.24 Treatment of these infections is associated
with
high complication rates and places an enormous burden on
both the patient and healthcare providers; prolonged
hospital
stay, increased morbidity and mortality, and serious
economic
sequelae being common consequences.5
It is possible that the risk of infection can be reduced by
an
antiseptic surface coating for medical implants. The purpose
of this study was therefore to determine the anti-infective
properties of a new biodegradable coating for medical
implants with regard to Staphylococcus epidermidis, one of
the
most important pathogens in biomaterial-associated infec-
tions.6,7 This coating is based on a polymer of low
molecular
weight poly(D,L-lactic acid) (PDLLA) and can be combined
with drugs like antibiotics or growth factors to establish a
locally acting drug-delivery system.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . .
*Corresponding author. Tel/Fax: +49-89-4140-7242; E-mail:
[email protected]
-
8/8/2019 Antibacterial Poly(D,L-Lactic Acid) Coating of Medical
Implants
2/8
H. Gollwitzer et al.
586
Materials and methods
The polymer coating
The commercially available Resomer R203 is a polymer of
PDLLA with a molecular weight of 29 000 Da and was pur-
chased from Boehringer Ingelheim (Ingelheim, Germany).The
polymer is a racemic mixture of the D- and L-enantiomers
of lactic acid and serves as a biodegradable coating for
med-
ical implants.
Implants were coated with PDLLA by a solvent casting
technique. In brief, the drug-carrier was dissolved in
ethyl-
acetate (SigmaAldrich AG, Deisenhofen, Germany) at a
concentration of 133.3 mg/mL. The coating solution was main-
tained on dry ice to prevent evaporation of the organic
solvent
and a subsequent increase in the polymer concentration.
To create a local drug delivery system, 5% (w/w) of the
antibiotics gentamicin sulphate (COM Pharma, Hamburg,
Germany) and/or teicoplanin (Aventis, Frankfurt, Germany)
were added to the polymer solution. The implants were coated
by two dip-coating procedures to achieve a dense and regular
polymer coating. All coating steps were carried out under
aseptic conditions in a laminar air-flow.
Medical implants
Commercially available Kirschner-wires (K-wires) of stain-
less steel (ISO 5832-1; Synthes GmbH & Co. KG, Umkirch,
Germany) and titanium alloy (TiAl6V4, ISO 5832-11 and ISO
5832-3; Synthes GmbH & Co. KG) were studied. The wireswere
cut into lengths, cleaned and sterilized by autoclaving.
The wires used for microbiological and antibiotic release
studies and their abbreviations are shown in Table 1.
Bacterial strains
A clinical isolate of a biofilm-forming strain
ofS.epidermidis
(strain SE 183) was used for the in vitro studies. The test
strain
was susceptible to both gentamicin and teicoplanin (genta-
micin MIC 2 mg/L, teicoplanin MIC 0.5 mg/L). Biofilm for-
mation was demonstrated by qualitative assessment with the
tube assay previously described by Christensen et al.8 Stock
cultures of the isolate were lyophilized or stored at 70C.
Preparation of bacteria
S. epidermidis (SE 183) was cultured to late logarithmic
growth phase on blood agar plates at 37C for 18 h before
test-ing. Bacterial cells were then resuspended in normal
saline
and adjusted to 5 107 cfu/mL by visual comparison with a0.5
McFarland standard. This suspension was diluted with
normal saline to an inoculum of 2.5 105 cfu/mL.
Antibiotic release
Drug release from antibiotic- and polymer-coated K-wires
(n = 4; size 1.5, length 150 mm; stainless steel) was studied
in
10 mL of phosphate-buffered saline (PBS) at 37C (pH 7.4).Samples
were coated with the PDLLA polymer (133.3 mg/mL
ethylacetate) including gentamicin or teicoplanin (5% w/w).
PDLLA-coated samples without antibiotics served as a con-
trol. To assess antibiotic stability during the test period,
PBS
of the control groups was supplemented with the gentamicin
and teicoplanin. Aliquots of 500 L were taken at the timepoints
10 min, 1, 6, 24 and 96 h from the PBS and assayed for
gentamicin and teicoplanin. Antibiotic concentrations were
determined by the fluorescence polarization immunoassays
TDx/TDxFLx Gentamicin assay (Abbott Laboratories, Abbott
Park, IL, USA) and Innofluor Teicoplanin assay system
(Opus Diagnostics, Fort Lee, NJ, USA).
Total bacterial adhesion
The total amount of live and dead adhering bacteria was
studied in a radiolabelling experiment, as described by
Chris-
tensen et al.9S. epidermidis was grown in MuellerHinton
broth (Oxoid GmbH, Wesel, Germany) substituted with
[3H]thymidine. After 24 h of incubation on a rotary shaker
(100 rpm), inoculum suspensions were prepared as described
earlier. Coated and bare K-wires of stainless steel and
titanium alloy (n = 9; size 1.8, length 12 mm) were
incubated
with the radiolabelled bacterial cell suspension for 2 h at
37Cunder static conditions. Individual wires were removed with
sterile forceps, washed three times with sterile normal
saline
Table 1. Sample groups and surface coating of stainless steel
(S) and titanium alloy (T) for the
in vitro tests
Surface coating Stainless steel Titanium alloy
Bare K-wires without coating (control group) S1 T1
K-wires coated with PDLLA S2 T2K-wires coated with PDLLA and
gentamicin (5.0% w/w) S3 T3K-wires coated with PDLLA and
teicoplanin (5.0% w/w) S4 T4
K-wires coated with PDLLA and gentamicin (1.7% w/w)
and teicoplanin (3.3% w/w)
S5 T5
-
8/8/2019 Antibacterial Poly(D,L-Lactic Acid) Coating of Medical
Implants
3/8
Antibacterial poly(D,L-lactic acid) coating
587
for 15 s and air-dried. After transfer to scintillation vials
con-
taining scintillation fluid, counts per minute were measured
in
a-counter (1219 Rackbeta; LKB Wallac, Bromma, Sweden).
Adhesion of viable bacteria
Adhesion of viable bacteria was evaluated in a bacterialadhesion
assay. Coated and bare K-wires of stainless steel and
titanium alloy (n = 10; size 1.8, length 12 mm) were
immersed
in 2 mL of the bacterial suspension (2.5 105 cfu/mL
normalsaline) and incubated for 2 h at 37C under static
conditions.After washing in normal saline, the K-wires were placed
in
vials containing 2 mL of trypsin solution (1% w/w) and
sonicated (Sonorex RK255H, 50 kHz; Bandelin Electronic,
Berlin, Germany) for 15 min to remove the adhering micro-
organisms. Serial dilutions of each trypsin solution were
plated on blood agar plates for quantification of viable
organ-
isms. Blood agar plates were incubated for 48 h at 37C, and
the cfu were counted visually.Complete detachment of the
adhering microorganisms by
sonication was verified through scanning electron micro-
scopy (SEM).
Morphological analysisSEM
Representative K-wire specimens from the in vitro studies
were prepared for SEM as follows. Specimens were fixed
in an aqueous solution of 1% (v/v) glutaraldehyde (Serva,
Heidelberg, Germany) in a buffer of sodium phosphate
(dibasic) monohydrate (Merck KGaA, Darmstadt, Germany)
and sodium hydroxide (Merck KGaA) for a minimum of 16 h.The
buffer contained 18.8 g/L sodium phosphate (dibasic)
monohydrate and 4.3 g/L sodium hydroxide. Dehydration
was carried out in an ascending ethanol series (50708090
100%) and samples were dried in a critical point dryer (CPD
030; BAL-TEC AG, Balzers, Liechtenstein) with carbon di-
oxide. Once coated with gold palladium (Polaron Autocoating
Unit SEM 5200; Quorum Technologies, Newhaven, UK)
each specimen was examined through a low vacuum SEM
(JEOL 5900; JEOL Germany GmbH, Eching, Germany).
Calculations and statistical methods
Data from bacterial adherence studies were compared for
statistical significance using non-parametric methods and
the
method of closed testing procedure,10 with P < 0.05
consid-
ered significant (KruskalWallis and MannWhitney tests).
Results
Morphological analysis
After the dip-coating procedure, a stable and regular PDLLA
coating could be observed through SEM. Complete detach-
ment of adhering bacteria was observed after sonication.
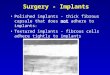
Antibiotic release
The concentrations of the released antibiotics gentamicin
and
teicoplanin in the elution buffer are shown in Figure 1.
Acontinuous drug release could be demonstrated for at least
96 h for both antibiotics. After an initial peak of release in
the
first few hours, a slow and continuous drug release could be
observed for the rest of the testing interval. Gentamicin
showed a pronounced initial peak of release in the first
hour.
Teicoplanin release, in contrast, was delayed compared with
gentamicin, the initial peak of release lasted 6 h and
theremaining teicoplanin was released to the PBS with kinetics
similar to that of gentamicin. Both gentamicin and
teicoplanin
showed a marked variation of initial release between indi-
vidual wires (between 3.87 and 10.58 mg/L for gentamicin
and between 2.71 and 15.11 mg/L for teicoplanin after 6 h).
Antibiotic concentrations of the control groups remained
constant throughout the entire study interval and gentamicin
and teicoplanin were stable in PBS in control experiments
for
at least 96 h.
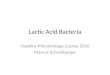
Total bacterial adhesion
The total biomass of bacteria adhering to the wires was
measured using the radioactively labelled bacteria method.
In
Figure 1. Elution profiles of gentamicin (left-hand panel) and
teicoplanin (right-hand panel) into PBS from individual stainless
steel K-wires with
PDLLA coatings containing either gentamicin or teicoplanin. In
each panel the different lines show the release kinetics of the
four samples tested.
-
8/8/2019 Antibacterial Poly(D,L-Lactic Acid) Coating of Medical
Implants
4/8
H. Gollwitzer et al.
588
this method, the number of counts per minute is directly
pro-
portional to the number of implant-adhering microorganisms,
and independent of their viability (data not shown). The
median counts and inter-quartile ranges (along with
outliers)
obtained for the different wires are shown in Figure 2. The
titanium alloy used showed a slightly lower biomass ofS.
epi-
dermidis adhering to the wire than stainless steel alloys,
although the results are not significantly different (P >
0.05).
However, for both types of wire a marked increase in
bacterial
adhesion can be observed for all PDLLA-coated samples
compared with the bare specimens. For all of the titanium
alloy wires this increase was significant at the P < 0.05
level,
whereas for the stainless steel wires the increases were
statistically significant (P < 0.05) for all except the
PDLLA/
gentamicin-coated (S3) wire.
With regard to the effect of antibiotic integration, genta-
micin showed a tendency (P = 0.050.1) to reduce bacterial
biomass after 2 h compared with pure PDLLA. Integration of
teicoplanin on the other hand significantly increased thebiomass
of S. epidermidis compared with implants coated
with pure PDLLA and the PDLLA/gentamicin combination
(P < 0.05).
Adhesion of viable bacteria
The number of viable bacteria adhering to the stainless
steel
and titanium alloy implants was evaluated in a quantitative
adhesion assay. Results are expressed in colony forming
units
per agar dilution plate (Figure 3), this measurement being a
direct indicator of the number of viable counts adhering to
the
implants.
Figure 2. Total biomass (median and inter-quartile ranges) ofS.
epidermidis adhering to either stainless steel and PDLLA-coated
K-wires (n = 9;
left-hand panel) or titanium alloy and PDLLA-coated K-wires (n =
9; right-hand panel), as assessed by the binding of radiolabelled
bacteria.
*, extremes (cases with values more than 3 box lengths from the
upper or lower edge of the box); H, outliers (cases with values
between 1.5 and 3 box
lengths from the upper or lower edge of the box).
Figure 3. Median viable counts ofS. epidermidis adhering to
either stainless steel and PDLLA-coated K-wires (n = 10; groups
S1S5 according to
Table 1; left-hand panel) or titanium alloy and PDLLA-coated
K-wires (n = 10; groups T1T5 according to Table 1; right-hand
panel). *, extremes
(cases with values more than 3 box lengths from the upper or
lower edge of the box);H, outliers (cases with values between 1.5
and 3 box lengths from
the upper or lower edge of the box).
-
8/8/2019 Antibacterial Poly(D,L-Lactic Acid) Coating of Medical
Implants
5/8
Antibacterial poly(D,L-lactic acid) coating
589
The PDLLA-coated implants significantly reduced adhe-
sion of viable staphylococci compared with bare K-wires
made from either titanium or stainless steel alloy (P <
0.01).
Combination of PDLLA with either gentamicin or teico-
planin or both antibiotics on the implant together reduced
viable counts to almost undetectable levels (P < 0.05).
Although there were no significant differences between
gentamicin and teicoplanin (P > 0.05), there was a slight
tendency towards less bacterial growth with gentamicin-
containing coatings, and also between the titanium alloy and
stainless steel (Figure 3).
Discussion
Bacterial adhesion to biomaterials and the capability of
many
microorganisms to form biofilms on foreign bodies are well-
established steps in the pathogenesis of
implant-associatedinfections.1113 In a biofilm, bacteria are
protected from the
host immune defence11,14 and exhibit a marked but reversible
increase in antibiotic resistance.11,15,16 Even high local
drug
concentrations beyond the MBC for planktonic microorganisms
do not completely eradicate bacteria located in
biofilms.15,17
As a result, prevention of bacterial colonization and bio-
film formation is an important consideration and may be sup-
ported by the use of antiseptic surface coatings. In the
present
work, a new antibacterial surface coating using a biodegrad-
able drug-delivery system was studied.
The chosen PDLLA coating enables the possibility of
covering medical implants with a biodegradable and
biocom-patible surface coating. This polymer is applied to implants
by
a solvent casting technique that allows coating of alloys
and
plastics with polished, irregular or porous surface
materials.
Breakdown of the polylactic acids is based on hydrolytic
splitting of the polymer backbone over several months to
oligomers, and release of lactic acid, which is metabolized
in
the citric acid cycle of the organism.1820
Incorporation of antibacterials into this coating to give a
local drug-delivery system ensures high concentrations
around
the implant for long periods of time and the risks and side-
effects for the host organism are minimized compared with
systemic drug application.21
In this study, elution fluids were not changed, and an elu-
tion model that is broadly applied in the literature,
especially
with antibiotic loaded bone cement, was used.22,23 Powdered
teicoplanin and gentamicin do not dissolve very well in the
volatile organic solvents used, and the final coating on the
implants consisted of antibiotic particles in the polymer.
This
leads to an initial peak of release and high variability
between
experiments, caused by fine drug particles located at, and
washed out of the polymer coating surface, a process that is
not well-defined. On the other hand, after the initial peak,
subsequent release is very predictable and comparable for
all
samples, being primarily the result of diffusion of
incorpor-
ated antibiotics from deeper levels of the coating.
In this study, we observed significant differences between
the results of adhesion studies depending on whether total
or
viable bacteria were assessed. The coating increased the
total
amount of attached microorganisms but at the same time
significantly reduced the number of viable bacteria even
with-
out antibiotics, suggesting that the bare PDLLA coating has
bactericidal action against adhering S. epidermidis SE 183.
Since most of the bacterial adhesion studies only employ one
type of test, either counting the total number of attached
microorganisms2426 or counting only viable bacteria,2729
results from these studies may be misleading. Since genta-
micin and teicoplanin are integrated into the polymer as
fine
particles, drugs located at the surface can be washed out to
leave small irregularities in the polymer. As one of the
most
important features in primary bacterial adherence is the
topography texture,30,31 this may promote the bacterial
adhe-
sion seen in this study. Apart from morphological features
of the polymer, physiochemical characteristics like surface
charge influence bacterial adhesion as well. In the present
study, teicoplanin increased the total number of adhering
micro-
organisms compared with gentamicin. Gallardo-Moreno et al.32
and Wilcox et al.33,34 have previously described promotion
of
bacterial adhesion to implant surfaces by subinhibitory
concen-
trations of glycopeptide antibiotics.3234 Our results would
sug-
gest that this effect may also occur at inhibitory
concentrations
and highlight the importance of undertaking total as well as
viable bacterial counts.
PDLLA has excellent features with respect to implant coat-ing,
with high mechanical stability,35 good osteoinductive
potential36 and excellent biocompatibility in vivo.36 The
material also shows good anti-thrombogenic characteris-
tics.37 In this study we have been able to demonstrate that
the
antibacterials gentamicin and teicoplanin can be
incorporated
into the polymer to give local drug-delivery systems that
reduce bacterial adhesion in vitro. We conclude that a com-
bination of the antibioticpolymer coating with other drugs
to
create a multifunctional and custom-tailored surface is
there-
fore possible and could offer new opportunities in the use
of
established biomaterials.
Acknowledgements
We gratefully acknowledge the contributions of I. Kappstein
(Associate Professor of the Department of Hospital Epidemi-
ology, University Hospital, Technical University Munich,
Germany) for inspiring discussions, constructive micro-
biological advice and for reading the manuscript. We would
also like to thank V. Vatou and M. Chihaja for their
assistance
in microbiological testing. Furthermore, we acknowledge the
contributions of D. Hall of the 1st Medical Clinic of the
Tech-
nical University Munich for assistance in preparing the
manu-
-
8/8/2019 Antibacterial Poly(D,L-Lactic Acid) Coating of Medical
Implants
6/8
H. Gollwitzer et al.
590
script. This study was supported by a grant from the
Bavarian
Research Cooperation for Biomaterials (FORBIOMAT).
The authors did not receive any payments or benefits from
any
other research fund, foundation, educational institution or
other non-profit organization. No benefits in any form have
been received or will be received from a commercial party
related directly or indirectly to the subject of this
article.
References
1. Schierholz, J. M. & Beuth, J. (2001). Implant infections:
a haven
for opportunistic bacteria. Journal of Hospital Infection49,
8793.
2. Green, S. A. (1983). Complications of external skeletal
fixation.
Clinical Orthopaedics and Related Research180, 10916.
3. Ahlborg, H. G. & Josefsson, P. O. (1999). Pin-tract
compli-
cations in external fixation of fractures of the distal radius.
Acta
Orthopaedica Scandinavica70, 1168.
4. Garberina, M. J., Fitch, R. D., Hoffmann, E. D., Hardaker, W.
T.,Vail, T. P. & Scully, S. P. (2001). Knee arthrodesis with
circular
external fixation. Clinical Orthopaedics and Related
Research382,
16878.
5. Hebert, C. K., Williams, R. E., Levy, R. S. & Barrack, R.
L.
(1996). Cost of treating an infected total knee replacement.
Clinical
Orthopaedics and Related Research331, 1405.
6. Peters, G., Locci, R. & Pulverer, G. (1982). Adherence
and
growth of coagulase-negative staphylococci on surfaces of
intra-
venous catheters. Journal of Infectious Diseases146, 47982.
7. von Eiff, C., Heilmann, C. & Peters, G. (1998). New
aspects on
staphylococcal infections associated with orthopaedic implants.
Hip
International8, 19.
8. Christensen, G. D., Simpson, W. A., Younger, J. J.,
Baddour,
L. M., Barrett, F. F., Melton, D. M. et al. (1985). Adherence
of
slime-producing strains of Staphylococcus epidermidis to
smooth
surfaces. Infection and Immunity37, 31826.
9. Christensen, G. D., Baldassarri, L. & Simpson, W. A.
(1995).
Methods for studying microbial colonization of plastics. Methods
in
Enzymology253, 477500.
10. Marcus, R., Peritz, E. & Gabriel, K. R. (1976). On
closed testing
procedures with special reference to ordered analysis of
variance.
Biometrika63, 65560.
11. Gristina, A. G. (1994). Implant failure and the immuno-
incompetent fibro-inflammatory zone. Clinical Orthopaedics
and
Related Research298, 10618.
12. Habash, M. & Reid, G. (1999). Microbial biofilms: their
develop-
ment and significance for medical device-related infections.
Journal
of Clinical Pharmacology39, 88798.
13. Gristina, A. G. (1987). Biomaterial-centered infection:
microbial
adhesion versus tissue integration. Science237, 158895.
14. Peters, G., Gray, E. D. & Johnson, G. M. (1989).
Immuno-
modulating properties of extracellular slime substance. In
Infections
Associated with Indwelling Medical Devices (Bisno, A. L. &
Wald-
vogel, F. A., Eds), pp. 6174. American Society for
Microbiology,
Washington, DC, USA.
15. Darouiche, R. O., Dhir, A., Miller, A. J., Landon, G. C.,
Raad, I.
I. & Musher, D. M. (1994). Vancomycin penetration into
biofilm
covering infected prostheses and effect on bacteria. Journal
of
Infectious Diseases170, 7203.
16. von Eiff, C., Heilmann, C. & Peters, G. (1999). New
aspects in
the molecular basis of polymer-associated infections due to
staphylococci. European Journal of Clinical Microbiology and
Infectious Diseases18, 8436.
17. Dunne, W. M., Jr, Mason, E. O., Jr & Kaplan, S. L.
(1993).
Diffusion of rifampin and vancomycin through a
Staphylococcus
epidermidisbiofilm. Antimicrobial Agents and Chemotherapy
37,
25226.
18. Pitt, C. G., Gratzl, M. M., Kimmel, G. L., Surles, J. &
Schindler,
A. (1981). Aliphatic polyesters II. The degradation of
poly(DL-
lactide), poly(epsilon-caprolactone) and their copolymers in
vivo.
Biomaterials2, 21520.
19. Cutright, D. E., Perez, B., Beasley, J. D., III, Larson, W.
J. &
Posey, W. R. (1974). Degradation rates of polymers and
copolymers of polylactic and polyglycolic acids. Oral Surgery,
Oral
Medicine, Oral Pathology37, 14252.
20. Kohn, J. & Langer, R. (1996). Bioresorbable and
bioerodiblematerials. In Biomaterials Science (Ratner, B. D.,
Hoffman, A. S.,
Schoen, F. J. & Lemons, J. E., Eds), pp. 6473. Academic
Press,
San Diego, CA, USA.
21. Cowsar, D. R. (1974). Introduction to controlled
release.
Advances in Experimental Medicine and Biology47, 113.
22. Diez-Pena, E., Frutos, G., Frutos, P. & Barrales-Rienda,
J. M.
(2002). Gentamicin sulphate release from a modified
commercial
acrylic surgical radiopaque bone cement. I. Influence of the
genta-
micin concentration on the release process mechanism.
Chemical
and Pharmaceutical Bulletin50, 12018.
23. Zhang, Y. & Zhang, M. (2002). Calcium
phosphate/chitosan
composite scaffolds for controlled in vitro antibiotic drug
release.Journal of Biomedical Materials Research62, 37886.
24. Franson, T. R., Sheth, N. K., Rose, H. D. & Sohnle, P.
G.
(1984). Scanning electron microscopy of bacteria adherent to
intra-
vascular catheters. Journal of Clinical Microbiology20,
5005.
25. Barnes, L. M., Lo, M. F., Adams, M. R. & Chamberlain, A.
H.
(1999). Effect of milk proteins on adhesion of bacteria to
stainless
steel surfaces. Applied and Environmental Microbiology65,
45438.
26. Bellon, J. M., G-Honduvilla, N., Jurado, F., Carranza, A.
&
Bujan, J. (2001). In vitrointeraction of bacteria with
polypropylene/
ePTFE prostheses. Biomaterials22, 20214.
27. Carballo, J. C., Ferreiros, M. & Criado, M. T. (1991).
Importance
of experimental design in the evaluation of the influence of
proteinsin bacterial adherence to polymers. Medical Microbiology
and
Immunology180, 14955.
28. Kramer, S. J., Spadaro, J. A. & Webster, D. A. (1981).
Anti-
bacterial and osteoinductive properties of demineralized
bone
matrix treated with silver. Clinical Orthopaedics and
Related
Research161, 15462.
29. Schierholz, J. M., Fleck, C., Beuth, J. & Pulverer, G.
(2000). The
antimicrobial efficacy of a new central venous catheter with
long-
term broad-spectrum activity. Journal of Antimicrobial
Chemo-
therapy46, 4550.
30. Quirynen, M. (1994). The clinical meaning of the surface
rough-
ness and the surface free energy of intra-oral hard substrata on
the
-
8/8/2019 Antibacterial Poly(D,L-Lactic Acid) Coating of Medical
Implants
7/8
Antibacterial poly(D,L-lactic acid) coating
591
microbiology of the supra- and subgingival plaque: results of in
vitro
and in vivoexperiments. Journal of Dentistry22, Suppl. 1,
S136.
31. Bollen, C. M., Lambrechts, P. & Quirynen, M. (1997).
Com-
parison of surface roughness of oral hard materials to the
threshold
surface roughness for bacterial plaque retention: a review of
the
literature. Dental Materials13, 25869.
32. Gallardo-Moreno, A. M., van der Mei, H. C., Busscher, H.
J.,Gonzalez-Martin, M. L., Bruque, J. M. & Perez-Giraldo, C.
(2001).
Adhesion of Enterococcus faecalis1131 grown under
subinhibitory
concentrations of ampicillin and vancomycin to a hydrophilic and
a
hydrophobic substratum. FEMS Microbiology Letters203, 759.
33. Wilcox, M. H., Winstanley, T. G. & Spencer, R. C.
(1994).
Binding of teicoplanin and vancomycin to polymer surfaces.
Journal
of Antimicrobial Chemotherapy33, 43141.
34. Wilcox, M. H., Finch, R. G., Smith, D. G., Williams, P.
& Denyer,
S. P. (1991). Effects of carbon dioxide and sub-lethal levels of
anti-
biotics on adherence of coagulase-negative staphylococci to
poly-
styrene and silicone rubber. Journal of Antimicrobial
Chemotherapy
27, 57787.
35. Schmidmaier, G., Wildemann, B., Stemberger, A., Haas, N.
P.
& Raschke, M. (2001). Biodegradable poly(D,L-lactide)
coating of
implants for continuous release of growth factors. Journal of
Bio-
medical Materials Research (Applied Biomaterials)58, 44955.
36. Schmidmaier, G., Wildemann, B., Bail, H., Lucke, M., Fuchs,
T.,
Stemberger, A. et al. (2001). Local application of growth
factors
(insulin-like growth factor-1 and transforming growth
factor-beta 1)
from a biodegradable poly(D,L-lactide) coating of
osteosynthetic
implants accelerates fracture healing in rats. Bone28,
34150.
37. Herrmann, R., Schmidmaier, G., Markl, B., Resch, A.,
Hhnel,
I., Stemberger, A. et al. (1999). Antithrombogenic coatings of
stents
using a biodegradable drug delivery technology. Thrombosis
and
Haemostasis82, 517.
-
8/8/2019 Antibacterial Poly(D,L-Lactic Acid) Coating of Medical
Implants
8/8