Embed Size (px)
Citation preview

Antithyroid Drugs
PHRM 412

Thyroid gland
• Thyroid: Meaning Shield shaped (the word introduced by Wharton)
• In mammals only this gland has capacity to incorporate iodine into organic substances: invented by Baumann

Thyroid gland
• The gland is highly vascular and flat structure• The thyroid gland has a blood flow about five
times the weight of the gland each minute• Located at the upper portion of the trachea
and just below the larynx

Thyroid gland
• Large gland, bi-lobed, connected by a central isthmus

Thyroid gland
Two class of hormones are secreted:• Iodide containing hormones of two types
T3 – triiodothyronineT4 – thyroxine
• Thyrocalcitonin
• Both of these hormones profoundly increase the metabolic rate of the body. • A hormone, also called
calcitonin, produced by the thyroid gland that lowers the levels of calcium and phosphate in the blood and promotes the formation of bone.

Thyroid gland
• Complete lack of thyroid secretion usually causes the basal metabolic rate to fall 40 to 50 percent below normal
• Extreme excesses of thyroid secretion can increase the basal metabolic rate to 60 to 100 percent above normal

Regulation of thyroid secretion
• Increased thyroid hormone in the body fluids decreases secretion of TSH by the anterior pituitary.
• When the rate of thyroid hormone secretion rises to about 1.75 times normal, the rate of TSH secretion falls essentially to zero.

Regulation of thyroid secretion
Thyrotropin-releasing hormone
Thyroid-stimulating hormone
TSH, also known as thyrotropin

Regulation of thyroid secretion
Thyrotropin-releasing hormone
Thyroid-stimulating hormone

Thyroid gland
• Thyroid gland: functional units is follicles.• Follicle consists of a luminal cavity surrounded
by a one-cell-deep layer of cells called follicular or acinar cells.
• The center of the follicles is filled with a gelatinous colloid, the main component of which is a glycoprotein called thyroglobulin.

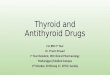
Follicular cell
Thyroglobulin

Fig: Microscopic appearance of the thyroid gland

Functions of follicular cells
• Produces thyroglobulin that is delivered to the follicle lumen
• Delivers hormones at the basolateral cell membrane
• Parafollicular cells: Thyrocalcitonin- hormone involved in calcium homeostasis

Requirement of iodine
• To form normal quantities of thyroxine, about 50 milligrams of ingested iodine in the form of iodides are required each year, or about 1 mg/week.
• To prevent iodine deficiency, common table salt is iodized with about 1 part sodium iodide to every 100,000 parts sodium chloride.

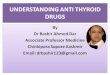
Fig: Biosynthesis and secretion of the thyroid hormones
Thyroperoxidase

Thyroid hormones synthesis
• When TSH binds to the TSH receptor at the basal membrane of the follicular cell , the biosynthesis of thyroglobulin (TG), thyroperoxidase (TPO) and hydrogen peroxide stimulated.
• Iodide enters the follicular cell by the iodide pump and is then transported into the follicular lumen.

Thyroid hormones synthesis
• In the lumen, the iodide is oxidized to hypoiodate anion (OI-) by thyroperoxidase (TPO) and hydrogen peroxide
• Then aromatic iodination of selected tyrosyl residues on TG to form diiodotyrosyl (DIT) and monoiodotyrosyl (MIT) residues.

Thyroid hormones synthesis
• The tyrosyl ring of DIT couples with adjacent DIT and MIT residues with an ether linkage to form of thyroxine (T4) and triiodothyronine (T3), both of which remain attached to TG.
• Low plasma levels for T4 cause the iodinated TG to be resorbed into the follicular cell, here complete proteolysis occurs by lysosomal protease to T4, T3, DIT, MIT, and noniodinated amino acids.

Thyroid hormones synthesis
• Both T4 and T3 are secreted by the cell into the blood; T4 is deiodinated to active T3.
• Both DIT and MIT are recycled by a dehalogenase (or deiodinase) to free tyrosine and iodide, both of which are recycled back into iodinated thyroglobulin.

Some important points:About 93% of the hormones secreted by the thyroid gland is thyroxine, and 7% triiodothyronine.
However, almost all the thyroxine is eventually converted to triiodothyronine in the tissues.The functions of these two hormones are qualitatively the same, but they differ in rapidity and intensity of action.
Triiodothyronine is about four times as potent as thyroxine, but it is present in the blood in much smaller quantities and persists for a much shorter time than does thyroxine.

Effects of thyroid hormones
• For normal growth and development of the nervous, skeletal, and reproductive systems
• Controls the metabolism of fats, carbohydrates, proteins and vitamins


Hyperthyroidism
• Two types:• Diffuse toxic goiter or Grave’s disease • Toxic nodular goiter or Toxic multinodular
goiter or Plummer's disease

Hyperthyroidism
• Also called Graves’ disease, Basedow’s disease, thyrotoxicosis, or exophthalmic goiter.
• Thyroid gland: increase two to three times of normal size (tremendous hyperplasia and in folding of the follicular cell lining into the follicles, so that the number of cells is increased greatly)
• Each cell increases its rate of secretion several fold (at rates 5 to 15 times normal)


Graves' disease
• Graves' disease is an autoimmune disease where the thyroid gland is overactive, producing an excessive amount of thyroid hormones (a serious metabolic imbalance known as hyperthyroidism and thyrotoxicosis).

Graves' disease
• This is caused by autoantibodies to the TSH-receptor (TSHR-Ab) that activate that TSH-receptor (TSHR), thereby stimulating thyroid hormone synthesis and secretion, and thyroid growth (causing a diffusely enlarged goiter).
*Plasma TSH concentrations are less than normal rather than enhanced in almost all patients and often are essentially zero

Hyperthyroidism: Symptoms
• Symptoms are from mild to severe• Restless despite feeling fatigued and weak,
highly excitable, and constantly agitated• Fine tremors of the hands occur, resulting in
unusual clumsiness


Antithyroid drugs
The best known antithyroid substances are:• Thiocyanate ion, thioamides, and high
concentrations of inorganic iodides.

Antithyroid drug: Thiocyanate ion
• Thiocyanate Ions Decrease Iodide Trapping• Competitive inhibition of the iodide pump in
high enough concentration• The same active pump that transports iodide
ions into the thyroid cells can also pump thiocyanate ions (SCN-)

Antithyroid drug: Thiocyanate ion• The decreased availability of iodide in the
glandular cells does not stop the formation of thyroglobulin, it prevents hormone synthesis only.
• This deficiency of the thyroid hormones in turn leads to increased secretion of TSH by the anterior pituitary gland, which causes overgrowth of the thyroid gland even though the gland still does not form adequate quantities of thyroid hormones.

Antithyroid drug: Thiocyanate ion
• The use of thiocyanates can lead to development of a greatly enlarged thyroid gland, which is called a goiter.
• Ions follow the similar mechanism: perchlorate ions, and nitrate ions

Antithyroid drugs: Thioamides
• Thioamides Decreases Thyroid Hormone Formation
• Thioamides (Propylthiouracil, methimazole and carbimazole) prevents formation of thyroid hormone from iodide and tyrosine.

Structure of thioamides
6-propyl-2-thiouracil 1-methylimidazole-2-thiol

The thiouracils is a tautomeric compound and can be represented as follows:

Antithyroid drugs: Thioamides
• These agents are actively concentrated by the thyroid gland against a concentration gradient.
• Their primary effect is to inhibit thyroid hormone synthesis by interfering with thyroperoxidase (TPO)– mediated iodination of tyrosine residues in thyroglobulin.

Antithyroid drugs: Thioamides
• Partly block the coupling of two iodinated tyrosines (DIT and MIT) to form thyroxine (T4) or triiodothyronine (T3).
• Induce the formation of goiter.

Antithyroid drugs: Thioamides
• Thioamide (rarely, thionamide) are the most important class of antithyroid compounds in clinical practice used in nondestructive therapy of hyperthyroidism.
• These agents are potent inhibitors of TPO, which is responsible for the iodination of tyrosine residues of thyroglobulin and the coupling of iodotyrosine residues to form iodothyronines.

Antithyroid drugs: Thioamides
• These drugs have no effect on the iodide pump or on thyroid hormone release.

Antithyroid drugs: Thioamides
• The most clinically useful thioamides are thioureylenes (=N-CS-N=), which are five- or six- membered structures.
• Six membered thioamides are:

Antithyroid drugs: Thioamides
• Five membered thioamides are:

Antithyroid drugs: Thioamides• Thioureylene structure may exist in either the
thioketo or thioenol tautomeric forms.

Six membered thioamides
• The study of 6-alkylthiouracil showed maximal antithyroid activity with 6-propylthiouracil.
• 6-Methylthiouracil has less than one-tenth the activity of PTU.

Six membered thioamides
• The ability of PTU to inhibit the enzyme 5 -D-I ′(thyroxine 5'-deiodinase)( i.e., the peripheral deiodination of T4 to T3) in addition to its intrathyroidal inhibition of thyroid hormone formation has made PTU the drug of choice in the emergency treatment of thyroid storm.

Structure-activity relationships
• The C2 thioketo/ thioenol group and an unsubstituted N1 position are essential for activity of six membered thioamides.

Structure-activity relationships
• The enolic hydroxyl group at C4 in PTU and the presence of alkyl group at C5 and C6 enhance the inhibitory potency.

Structure-activity relationships
• Methimazole has more TPO inhibitory activity and is longer -acting than PTU but , in contrast to PTU, is not able to inhibit the peripheral deiodination of T4, presumably because of the presence of the methyl group at N1 position.
1

Structure-activity relationships
• Efforts to improve the taste and decrease the rate of release of methimazole led to the development of carbimazole.
• Carbimazole, the pro-drug derivative of methimazole, gives rise to methimazole in vivo and is used in the same dosage.

Antithyroid drugs: Iodide ion
• Iodides in High Concentrations Decrease Thyroid Activity and Thyroid Gland Size.
• When iodides are present in the blood in high concentration (100 times the normal plasma level: 0.6 to 0.8 µg/lit), most activities of the thyroid gland are decreased.

Antithyroid drugs: Iodide ion
• Reduce the rate of iodide trapping • Decrease its blood supply• It also lowers the elevated BMR.• Net effect is the reduction of size of thyroid
gland

Antithyroid drugs: Iodide ion
• It also has been suggested that excess iodide might change the conformation of thyroglobulin, making the protein less susceptible to thyroidal proteolysis.

Antithyroid drugs: Iodide ion
• Iodide, as Lugol's solution (Strong Iodine Solution USP) or as saturated potassium iodide solution, is administered for approximately 2 weeks to ensure decreased vascularity and firming of the gland.
Lugol’s solution contains 5% iodine (5 grams in 100 mL) and 10% potassium iodide (10 grams in 100 mL).

Radioiodine therapy
• Definitive treatment: given primarily to destroy the hyperfunctioning thyroid tissue.
• Available as Sodium iodide I 131 (Na131I)

Radioiodine therapy
• Radioiodine is an oral medication and given as single dose.
• Patients taking radioiodine therapy, few required more than one dose.
• Usual dose: 100 to 200 µCi per gram of weight of thyroid gland.

Radioiodine therapy
• Radioiodine is taken by the follicular cell in the same way as iodine and beta emission of radioiodine causes necrosis and decrease the activity of thyroid tissue.

Radioiodine therapy
• The cell necrosis induced by radioiodine occurs gradually.
• May elapse hyperthyroidism (after 6-18 weeks or later of the treatment) before a hypothyroid or euthyroid state is achieved.
If previously used: • Antithyroid drugs: 3-7 days• beta-adrenergic blocking agents: continued

Radioiodine therapy
• Pregnancy: Sodium iodide I 131 has been shown to cause harm to a developing fetus. Use in pregnant women should be avoided.
• Nursing mother: Iodine is excreted in breast milk. Therefore, formula feedings for infants are strongly recommended for nursing women requiring sodium iodide I 131 treatment.

Radioiodine therapy
• The side effects commonly seen with sodium iodide I 131 treatment are mild with the smaller doses given for hyperthyroidism but may be more severe with the larger doses given for thyroid cancer.

Radioiodine therapy
• Sodium iodide I 131 may cause suppression of the bone marrow, resulting in anemia, and reductions in white blood cells and platelets.
• Increased risk of death from cardiovascular disease.