Embed Size (px)
DESCRIPTION
anti aging magazine
Citation preview

abonati
EMC
5credite


1
This year news is set to be a record-breaking year for anti-aging medicine, according to the world's leading medical society in the sector, the American Academy of Anti-Aging Medicine (A4M, www.WorldHealth.net). Fresh investment capital of US$60 million is powering the A4M expansion, as attendances at their anti-aging conferences soar, and as the society prepares its imminent entry into the Chinese market with the official backing of the Chinese government and medical authorities. One which began with a strategic US$60 million investment in Medical Conferences International Inc.(MCII) by London-based Tarsus Group PLC (www.Tarsus-Group.com). The deal saw Tarsus take an 80% stake in MCII, which was founded by Dr. Goldman and Dr. Ronald Klatz, who are respectively Chairman of the Board and President of the A4M. Now the anti-aging revolution is headed east as Tarsus/MCII prepare for upcoming major events in China; in Mumbai, India; and in Dubai, United Arab Emirates. Medical conferences and Expo's are scheduled from Bangkok to Tokyo, Lisbon, Dusseldorf, Melbourne, and Bali, Indonesia - making this is one of the fastest international growth phases of any medical group in history. There are close to 30 international co-sponsored events set for 2008. Even as the A4M/MCII takes its message to the world, Drs. Goldman and Klatz along with other pioneering anti-aging physicians have announced a global race, now spanning 100 countries, to claim a US$1Million life extension cash prize for the first scientist or team who can reliably show significant reversal or halting of aging in humans.
All my best regards,Bogdan Dimitrie NiculaePresident AMAA
Dear Members,
After the success of the Second International Anti-Aging Congress the membership number increased with 100% now our organization has over 500 paying members. Our members will receive, as we did until now, discounts at the congresses organized by our sister societies A4M, Euromedicom, SAAAM and many others. We obtained for our bilingual publication “THE ROMANIAN ANTI-AGING MAGAZINE”, 5 credits EMC from Romanian College of Medicine. The magazine will be received by all our members in our data base free of charge.After our success story many are trying to confuse the anti-aging professionals in who is representing the anti-aging medicine in Romania, by organizing old congresses with the help of the new term anti-aging included in the title of their manifestation, hopping to bring more attendees at their congress. Instead of trying to work together, to find ways of understanding each other, they are trying to demolish the hard work and good contacts that we obtained in the International anti-aging community.Our society started a new program through Romanian college of Medicine to organize two-three days courses wich are credited through The Continous Medical Education Program.Our first course was on Peelings and was held in end of June, were we tried to keep our numer of participants to maximum 20 people because we have in this way the opportunity to be an more interactive and educational course.We also announced two more courses on lasers for beginners and advanced for September – December period. Our future visit form September 6th at Harvard Medical School, were our board was invited to attend specific programs of EMC, will be a great asset for our experience in organizing such EMC events.

2
3
8
9
14
16
18
19
20
26
27
32
34
36
38
40
42
44
45
46
48
49
50
52
54
60
3
8
9
14
16
18
19
20
26
27
32
34
36
38
40
42
44
45
46
48
49
50
52
54
60
Siguranţa alimentelor şi sănătatea, radicali liberi, stresul oxidativ,antioxidanţi alimentari
Anti-Aging Program in Aesthetic Surgery Clinic
Orthomolecular Approach in Preventing and Treating Cardio - Vascular Diseases
2 International Congress of Anti-Aging Medicine
Dermography and Medical Tatooing Procedures Dermografia şi procedurile de tatuaj medical
Advanced Oxidation Protein Products and Lipid Oxidation Kinetics in ElderlyPatiens with Type 2 Diabetes Mellitus
Produşii de oxidare avansată ai proteinelor şi cinetica oxidării lipidelor la pacienţivârstnici cu diabet de tip 2
No Needle Mesotherapy An Alternative Solution for Anti Cellulite Treatmenand for Skin Rejuvenation
The Cardiovascular Diseases - Increased Risk of Death in Autoimmune Diseases
Does Liposuction Improve Results or Raise Complication Rates inAbdominoplasty
Perturbations of Calcemy in Woman in Menopause with Chronic RenalDeficiency
Perturbări ale calcemiei la femeile la menopauză cu insuficienţă renală cronică
Anti-Aging Medicine - A Faisable Medicine
Keloids
Peeling Workshop
Anti-Aging and Orthomolecular Medicine: Practical Concepts for the Preventionand Treatament of Cardiovascular Diseases
A Method to Evaluate Cerebral Senscence: P300
The Characterization of Seabuckthorn Fruits and Copses in Terms of Seroroninand Microelements Valorificarea fructelor şi lăstarilor cătinei pentru serotonină şi microlemente
Advancement in Diagnosis of Irritable Bowel Sindrome (IBS)
The Role of Lymphodynamical Disurbances in the Formation of theEndoecological Disease New Possibilities of Manual Diagnosis and Therapy of Mastopathy
Aesthetic Rhinoplasty Histopathological Changes in the Gastric Mucosa During the Ageing Process
Sarcopenia ang ageing
Newest Natural Anti HypertentationHerbal Product
Omega 3 - Ulei de peşte (capsule 400mg)
Diagnosis of Viral Hepatits
Modern Peeling Methods: Microdermabrasion (Mechanical Peeling) Metode moderne de peeling: microdermabraziunea (peeling mecanic)
Xxxxx
SUMAR
IQ MEDICAL MEDIAANUL II nr. 5, iunie 2007
EDITOR COORDONATOR CĂTĂLIN ENĂ[email protected]
DIRECTOR EXECUTIVBOGDAN DIMITRIE [email protected]
COMITET EDITORIALPREŞEDINTEROBERT GOLDMAN - SUA
RONALD KLATZ - SUAMICHAEL KLENTZE - GermaniaCATHERINE DECUYPER - FranţaCHRISTOPHE DE JAEGER - FranţaCĂLIN GIURCĂNEANU - RomâniaOTHON PAPADOPOULOS - GreciaVIRGIL FEIER - RomâniaJOHN IONESCU - GermaniaALEXANDRU TĂTARU - RomâniaRADU RĂDULESCU - RomâniaGEORGIANA OZANA TACHE - RomâniaDANIEL GRIGORE - RomâniaMARIA GEORGESCU - RomâniaAL JASHI ISAM - RomâniaMANOLE COJOCARU - RomâniaJEAN PIERRE NAIM - ElveţiaCĂLIN PETRU TĂTARU - RomâniaBOGDAN SAVU - România
ATHANASIOS CHRISTOPOULOS - CipruCRISTIAN POPA - CipruANNA MODELSKA - PoloniaIOAN ANCUŢA - RomâniaPANAGY GEORGIOU - GreciaELEONORA LUKA PILLA - Elveţia DIMITRI MIHAILOV - OlandaCRISTIAN NIŢESCU - RomâniaDRAGOŞ GEORGESCU - RomâniaDIMITRIE NANU - RomâniaECKAT HANEKE - Germânia
REDACTORLIVIA TRIŞCAŞ
CORECTURĂCIP BRAND FACTORY
DESIGNERCIP BRAND FACTORY
DIRECTOR DIFUZAREGABRIEL STOICHICI
Tipărită la LIANEDI GROUP
Articolele publicate în această ediţie sunt copyright © THE ROMANIAN ANTI-AGING
MAGAZINE
I.S.S.N. 1842 - 5666
REDACŢIA ŞI ADMINISTRAŢIADrumul Taberei 35, bl. 803, ap.4, Sector 6, BucureştiTel: (021) 725.66.08; Fax: (021) 413.02.12E-mail: [email protected]; www.amaa.ro
nd

3
Farm. Gabriela Vlăsceanu
Procesul trebuie monitorizat pe întregul parcurs, de la calitatea materiilor prime ce intră în producţie şi prelucrare, depozitarea şi transportul alimentelor, până la condiţiile de comercializare. Legea protejează sănătatea consumatorilor prin acordarea unor drepturi precum:-libertatea consumatorilor de a alege produsele,-dreptul la protecţie împotriva riscului de a achiziţiona un produs ce-i poate prejudicia sănătatea,-dreptul de a fi informat complet asupra caracteristicilor produselor,-dreptul de a fi despăgubit pentru prejudiciile cauzate de calitatea necorespunzătoare a unui produs alimentar.
Important este să cunoaştem legislaţia din acest domeniu şi să ştim cui ne adresăm când este cazul: Oficiului Judeţean pentru Protecţia Consumatorilor. Trebuie să cunoaştem care sunt aspectele unui aliment necorespunzător, ce ne poate pune sănătatea în pericol, putând prezenta:-modificări ale aspectului, culorii şi/sau consistenţei, -urme de contact cu rozătoare sau semne de infestare cu paraziţi, -miros şi gust străin de natura produsului, -pete de mucegai, -corpi străini, -aditivi alimentari neavizaţi.
Aditivii alimentari sunt substanţe care se folosesc la prepararea unor produse alimentare în scopul îmbunătăţirii calităţii acestora. Legislaţia în domeniu stabileşte care sunt aditivii admişi, precum şi cantitatea maximă permisă pentru utilizarea unui aditiv într-un anumit produs, astfel încât acesta să nu dăuneze sănătăţii.
Aditivii alimentari incluşi pe lista Uniunii Europene, preluată şi de legislaţia românească, sunt codificaţi cu litera "E" de la "Europa", urmată de un număr specific fiecărei substanţe.
Atragem atenţia că, spre deosebire de statele occidentale, România nu are o legislaţie bine pusă la punct împotriva folosirii mesajelor subliminale în materialele publicitare audio şi video.
Radicalii liberi sunt reprezentaţi de un atom, un grup de atomi sau o moleculă care au în învelişul lor electronic un electron cu spinul necompensat.
Aceşti radicali liberi ai oxigenului, denumiţi şi specii oxigen-reactive (ROS), prezintă o serie de caracteristici:-conţin unul sau mai mulţi electroni celibatari (nepereche);-din punct de vedere electrostatic, pot fi neutri sau încărcaţi pozitiv ori negativ;-posedă o foarte mare reactivitate chimică (dependenţa de concentraţie şi temperatură, pH).
Siguranþa alimentelor þisãnãtatea. Radicali liberi, stresul oxidativ, antioxidanþi alimentari
Din cauza reactivităţii radicalilor liberi ai oxigenului formaţi ca intermediari, molecula de oxigen indispensabilă vieţii poate deveni prooxidantă, toxică, agresivă pentru organism, ca urmare a activării sale în cursul proceselor biologice prin reducere univalentă, nu prin reducere cu doi electroni. Cei mai importanţi radicali liberi sunt derivaţi ai oxigenului, cunoscuţi ca specii reactive de oxigen. Acestea includ:O ·- radicalul superoxid 2
·OH radicalul hidroxil ROO· radicalul peroxilH O peroxidul de hidrogen2 21O oxigenul atomic2
NO· oxidul nitricONOO- peroxinitritulHOCl acidul hipocloros
Radicalii liberi ai oxigenului se formează la nivel mitocondrial, în cursul lanţului respirator, dar şi în urma unor reacţii enzimatice. Viteza de formare a radicalilor liberi ai oxigenului depinde de viteza de utilizare a oxigenului şi este direct proporţională cu numărul de mitocondrii din celulă.
2 International Congressof Anti-Aging Medicine
nd
4
A) Surse endogenel. AutooxidareaEste un produs secundar al mediului intern aerob. Printre moleculele care suferă autooxidare se află catecolaminele, hemoglobina, mioglobina, citocromul C redus. Principalul radical
2+format este superoxidul. În acelaşi proces, ionul feros (Fe ) poate - 3+pierde un e trecând în ion feric (Fe ).
2. Oxidarea enzimaticăUn număr mare de enzime pot genera cantităţi importante de radicali liberi, incluzând aici xantin oxidaza (activată în ischemie - reperfuzie), prostaglandin sintetază, lipo-oxigenază, aldehid-oxidază şi aminoacid-oxidază. De asemenea, enzima mieloperoxidază produsă de neutrofilele activate utilizează hidrogen peroxidul pentru a oxida ionii de clor în puternicul oxidant acid hipocloros (HOCl).3. Exploziile respiratorii (respiratory burst)Este un termen folosit pentru a descrie procesul prin care fagocitele consumă mari cantităţi de oxigen în timpul fagocitozei.Aproximativ 70 - 90% din oxigenul consumat se regăseşte în producţia de superoxid, prin activarea NADPH-oxidazei din membrana celulară la contactul cu complexe imune, bacterii învelite cu imunoglobuline, complement 5a sau leucotriene.
B) Surse exogene1. Medicamentele Un număr de medicamente stimulează producţia de radicali liberi în prezenţa hiperoxiei. Astfel de medicamente sunt: nitrofurantoinul, agenţi antineoplazici precum bleomicina, adriamicina şi metotrexatul. Alţi radicali, derivaţi de penicilamină, fenilbutazonă, acizi fenamici şi sulfasalazină pot inactiva proteazele şi diminua nivelul acidului ascorbic, accelerând peroxidarea lipidelor.2. IradiereaRadioterapia poate provoca afectări tisulare prin formarea de radicali liberi. Radiaţia electromagnetică (razele X, razele gamma) şi radiaţia corpusculară (electroni, fotoni, particule alfa şi beta) generează radicali primari prin transferul de energie către anumite componente celulare, cum ar fi apa.3. FumatulS-a dovedit faptul că oxidantii din fumul de tutun reduc dramatic nivelul intracelular de antioxidanţi printr-un mecanism legat de stresul oxidativ. S-a estimat că fiecare doză de fum conţine o cantitate impresionantă de substanţe oxidante, incluzând aldehide, epoxizi, peroxizi şi alţi radicali liberi cu o durată de viaţă suficient de lungă pentru a produce distrugeri la nivelul alveolelor, în faza gazoasă se află oxid nitric, radicali peroxil şi radicali cu carbon în centru, în timp ce gudronul conţine semichinone derivate din chinone şi hidrochinone. Microhemoragiile produse de aceşti radicali liberi duc la apariţia unor depozite de fier, care la rândul lor ajută la formarea radicalului hidroxil din peroxidul de hidrogen. S-a mai descoperit că fumătorii au niveluri ridicate de neutrofile în tractul respirator inferior, contribuind la creşterea de ROS.
În condiţii de dezechilibru redox, apar perturbări la nivelul structurilor şi funcţiilor celulare:- peroxidarea lipidelor - determină degradarea membranelor celulare şi subcelulare şi alterarea proceselor de semna-
lizare dependente de membrane;- degradarea proteinelor - oxidarea grupărilor tiol (-SH) din proteine, oxidarea centrilor catalitic activi ale enzimelor, pierderea funcţiei catalitice, alterarea structurii receptorilor membranari;- atacul asupra acizilor nucleici - cu formarea unor produşi de oxidare ai ADN, instalarea mutagenezei şi a carcinogenezei;- degradarea glucidelor - cu formarea produşilor finali de glicozilare avansată, care la rândul lor pot avea efecte toxice marcate.
Toate aceste perturbări localizate la nivel intim, celular şi molecular au drept consecinţă apariţia de leziuni celulare manifestate prin creşterea permeabilităţii capilare, perturbarea funcţiilor celulelor sangvine etc.
Consecinţele clinice ale acestor leziuni oxidative se concretizează prin apariţia fenomenelor de îmbătrânire generală a organismului, dar şi prin instalarea unor fenomene patologice localizate la nivelul anumitor aparate şi sisteme cu apariţia aterosclerozei, diabetului zaharat, fenomenelor autoimune sau inflamatorii, a bolilor canceroase etc.
În concluzie, radicalii liberi şi stresul oxidativ joacă un rol important în inducerea disfuncţiilor la nivel celular şi a diverselor maladii la nivelul organismului. Echilibrul dintre acţiunea oxidantă a radicalilor liberi şi nivelul antioxidanţilor dintr-un organism este esenţial vieţii şi caracterizează capacitatea de rezistenţă şi adaptare a unui organism viu.
Stresul este una din componentele "cvartetului" celor "4S", cu influenţe majore asupra stării de sănătate a organismului, alături de supraalimentaţie, sub- alimentaţie şi sedentarism.
În contextul social al vieţii moderne, se impune definirea conceptului de stres ce reprezintă fenomenul de încordare, forţare şi suprasolicitare a organismului uman şi include atât starea de agresiune exercitată asupra organismului, cât şi reacţiile de adaptare şi apărare la diversele solicitări din mediul intern şi/sau din mediul extern.
Stresul poate fi diferenţiat în mai multe tipuri, funcţie de nivelul la care se exercită: stresul chimic (datorat compuşilor poluanţi din aer, apă, alimente, radiaţii, polipragmaziei), senzorial (auditiv şi vizual), informaţional, decizional, legat de monotonia vieţii cotidiene, psihic etc.
Această definiţie apare ca o rezultantă a evoluţiei
2 International Congressof Anti-Aging Medicine
nd

5
istorice a unor noţiuni introduse încă din secolul al XI-lea de Avicena (care a sesizat acest fenomen atunci când, în mod experimental, a plasat un miel în apropierea unui lup, iar mielul a murit de frică...), continuând cu definirea conceptului constantei mediului intern de Claude Bernard (1858) şi a celui de homeostazie de W. Cannon (1932). În anul 1939, Hans Selye a definit propriu-zis conceptul de stres şi stadiile sale.
Termenul de stres se referă la reacţia determinată de orice stimul fizic, mental, social sau emoţional, care cere un răspuns sau determină o alterare a reacţiilor generale ale organismului la nivel psihic sau organic (somatizarea stresului).
Stresul face parte din viaţa noastră, într-o formă de intensitate mai mică sau mai mare. El poate rezulta din aproape toţi factorii cotidieni (probleme de serviciu, deziluzii în dragoste, probleme de cuplu sau financiare, trafic rutier, mediul ambiant, necesitatea adaptării organismului la temperaturi extreme sau diferenţe mari de temperatură, schimbări de fus orar etc.) În acelaşi timp, lipsa odihnei şi bolile de orice natură reprezintă un stres considerabil. Consumul excesiv de alcool şi fumatul apar şi sunt uneori crescute ca o reacţie la stres, dar care la rândul lor determină un stres şi mai mare, creând leziuni organice ireversibile.
Astfel se intră într-un cerc vicios de genul "stresul care induce stres".
Unele persoane reuşesc să surmonteze foarte bine perioadele de stres şi acestea au un impact foarte mic asupra sănătăţii lor fizice şi emoţionale, altele însă sunt mult mai vulnerabile şi reacţionează puternic chiar şi la un stres minor. Stresul poate cauza: - un sindrom de oboseală cronică,
- perturbări ale ritmului somn -veghe, - dureri de cap cronice şi iritabilitate, - dereglări ale apetitului (bulimie sau anorexie) şi probleme
digestive, - lipsa concentrării şi pierderi de memorie, - probleme circulatorii şi creşteri ale presiunii arteriale, - sindroame anxios-depresive, - dacă nu este stopat la timp, afecţiuni grave cum ar fi afecţiunile cardiace (infarctul miocardic, în principal) şi chiar cancere.
Cercetarile estimează că stresul contribuie ca şi cauzalitate la mai mult de 80% din bolile majore, incluzând bolile cardiovasculare, cancerul, bolile metabolice şi endocrine, boli ale pielii (psoriasis, vitiligo etc.), precum şi favorizarea apariţiei bolilor infecţ ioase prin scăderea semnificativă a imunităţ i i .
Deoarece stresul stă la baza majorităţii sindroamelor anxioase, atacurilor de panică, afecţiunilor obsesiv-compulsive, depresiilor, el este conştientizat la nivel general ca şi o problemă psihologică, deşi are efecte serioase organice.
Organismul răspunde la starea de stres cu o serie de modificări fiziologice care includ o secreţie crescută de adrenalină, creşterea presiunii arteriale, accelerarea bătăilor inimii, creşterea tensiunii musculare. Digestia este încetinită sau perturbată prin creşterea acidităţii gastrice, dereglarea motricităţii intestinale, încetinirea fluxului biliar; nivelul de colesterol creşte şi apar astfel dislipidemii care cresc riscul apariţiei bolilor cardiovasculare. Totodată creşte şi nivelul glicemiei (se ştie spre exemplu că stresul operator induce creşteri semnificative ale glicemiei).
Aproape toate organele reacţionează la stres. Glanda
pituitară creşte producţia de ACTH care influenţează eliberarea de cortizon şi cortizol. Astfel este inhibată funcţionarea liniei albe de apărare a organismului şi este supresat răspunsul imun creând posibilitatea apariţiei diverselor boli infecţioase. Creşterea producţiei de adrenalină este responsabilă pentru majoritatea simptomelor asociate cu stresul. Este, de asemenea, motivul pentru care stresul poate duce la deficienţe nutriţionale.
Creşterea nivelului adrenalinei face să crească metabolismul proteinelor, grăsimilor, carbohidraţilor pentru a crea rapid energia de care are nevoie. Acest răspuns determină la rândul lui creşterea excreţiei de aminoacizi, potasiu şi fosfor, depleţia de magneziu din ţesutul muscular precum şi deficienţe în stocarea calciului (apar pierderi de calciu, care duc la spasmofilii). În acelaşi timp, absorbţia de nutrienţi este deficitară într-o stare de stres. Rezultatul este că, în special în stări prelungite de stres, corpul devine deficient în mulţi nutrienţi pe care este incapabil să-i înlocuiască corespunzător. Multe din dezordinile ce apar ca urmare a stării de stres sunt rezultatul acestor deficienţe nutriţionale, printre care deficienţa în vitaminele din complexul B este una importantă şi care influenţează negativ funcţionarea normală a sistemului nervos.
Stresul poate fi acut sau prelungit. Stresul cronic este cel mai periculos putând cauza îmbolnăviri grave, unele care pot pune în pericol chiar viaţa.
Stresul oxidativ este rezultatul dezechilibrului dintre factorii pro-oxidanţi şi sistemele antioxidante protectoare. Ca urmare a unor stări prelungite de stres se produc mari cantităţi de radicali liberi, apărând astfel stresul oxidativ ce acţionează la nivelul membranelor celulare cauzând distrucţii tisulare.
La nivel molecular, noţiunea de stres oxidativ a fost introdusă de Helmut Sies ca urmare a cercetărilor efectuate între 1981 si 1993. Astfel, stresul oxidativ este definit ca situaţia rezultată din generarea intensă de radicali liberi ai oxigenului raportată la capacitatea sistemelor antioxidante existente la un moment dat în organismul viu.
Altfel spus, stresul oxidativ reprezintă agresiunea produsă la nivel molecular prin dezechilibrul balanţei prooxidant/antioxidant în favoarea primului, dezechilibru manifestat mai ales la nivelul membranelor celulare, cu repercusiuni funcţionale grave la nivelul tuturor organelor şi ţesuturilor.
Speciile reactive de oxigen (ROS - Reactive Oxygen Species) sunt produse în organismele aerobe ca produşi intermediari în condiţii fiziologice. Aceşti produşi metabolici intermediari induc modificări patologice doar când nu mai pot fi contracaraţi de antioxidanţii endogeni
De ce există radicali liberi în organism? Pentru că viaţa este un proces de oxido-reducere. Unul din paradoxurile vieţii pe planeta noastră este faptul că molecula care întreţine viaţa aerobă - oxigenul - nu este doar, în mod fundamental, esenţială pentru metabolismul energetic şi pentru respiraţie, ci este, aproape în egală măsură, implicată în etiopatogenia a numeroase boli şi stări degenerative. Dualitatea moleculei de oxigen rezultă din faptul că viaţa fără oxigen nu poate exista, oxigenul fiind, în stare fundamentală, "blând", simplu, inofesiv, dar în acelasi timp poate deveni toxic, declanşând, în anumite condiţii, formarea unor specii reactive de oxigen (ROS). Oxigenul atmosferic, în starea
.
2 International Congressof Anti-Aging Medicine
nd
6
fundamentală, este diferit de alte elemente gazoase, deoarece este un diradical sau, în alţi termeni, posedă 2 electroni nepereche (celibatari) care au spini paraleli.
Astfel, oxigenul este de obicei nereactiv faţă de majoritatea moleculelor organice care au în structura lor electroni cu spini opuşi. Acest fapt face ca oxigenul să fie un gaz paramagnetic, care participă la reacţii chimice cu molecule organice numai sub formă "activată".
Activarea moleculei de oxigen în condiţii fiziologice presupune reducerea sa cu doi electroni:
- 21/2 O2 + 2e —>O .Modificarea potenţialului redox are loc, într-o primă
etapă, în momentul în care oxigenul difuzează în sânge, după care acesta se reduce din nou la traversarea membranelor celulare.
Fiecare din aceste etape este însoţită de modificarea chimică progresivă a moleculei de oxigen şi de formarea unor specii chimice intermediare. La nivel celular, modificările chimice devin şi mai complexe, oxigenul participând la procesele metabolice globale. Mecanismele fundamentale de transformare a constituenţilor organici ai materiei vii (glucide, proteine, lipide), ciclul Krebs şi lanţul respirator implică secvenţe metabolice multiple ce decurg cu transfer de electroni şi sunt dependente de potenţialul speciilor chimice implicate. În condiţii de homeostazie redox, la nivelul organismului viu, speciile prooxidante se află în echilibru perfect cu cele antioxidante. Dacă sistemele antioxidante nu funcţionează în parametrii normali sau dacă se formează radicali liberi în cantităţi mari, se instalează stresul oxidativ ca urmare a manifestării acţiunii prooxidante a speciilor radicalice la nivel celular şi molecular.
Pentru a contracara acţiunea nocivă a speciilor prooxidante care se formează în mod fiziologic, organismul uman e echipat cu sisteme antioxidante eficiente, cu structuri şi mecanisme de acţiune diferite, ce pot acţiona sinergic. Sistemele biologice dispun de diferite sisteme antioxidante:
- sisteme enzimatice: superoxiddismutaza (SOD), glutation-peroxidaza (GPX), glutation-reductaza, glucozo-6-fosfat dehidrogenaza, glutation-S-transferaza, catalaza (CAT)etc.;
- sisteme non-enzimatice;
- macromolecule: albumina, feritina, transferina, flavonoidele;
- molecule de mici dimensiuni: hidrosolubile (tiolii, acidul uric, acidul ascorbic, acidul lipoic, glutationul), liposolubile (carotenoidele, tocoferolii, coenzima Q10);
- unii hormoni (melatonina, angiotensina etc.).
Prevenirea leziunilor oxidative constituie un obiectiv major al cercetării ştiinţifice actuale, în condiţiile în care stresul oxidativ este responsabil pentru numeroase afecţiuni inflamatorii, degenerative, neoplazice şi alte categorii ce afectează practic toate sistemele organismului.
Ce putem face pentru a ne apăra împotriva acestui atac deosebit de virulent?
Primul pas constă în eliminarea pe cât posibil a tuturor surselor de radicali liberi ca: grăsimile nesaturate, apa de la robinet, aparatele cu microunde şi fumatul.
Al doilea pas este fortificarea organismului pentru ca acesta să poată lupta în mod natural cu armele pe care le deţine. În acest sens, s-a descoperit că diverse preparate pe bază de substanţe nutritive şi plante medicinale, atunci când sunt luate în doze suficiente şi în combinaţii corecte, neutralizează radicalii liberi înainte ca aceştia să producă vătămari cuantificabile. Aceste preparate se numesc “antioxidanţi” sau "curăţători de radicali liberi".
La întrunirea anuală a Asociaţiei Americane pentru Dezvoltare Ştiinţifică din 1992, biologul Michael Ross de la Universitatea California a raportat descoperirea a ceea ce el a denumit "gena anti-îmbătrânire". Această genă este responsabilă pentru reglarea producţiei de enzime antioxidante, fără de care ţesuturile noastre ar "arde" imediat în "focul" permanent întreţinut în organism de radicalii liberi. Mulţi oameni de ştiinţă sunt de părere că procesele de îmbătrânire sunt un simplu efect secundar al scăderii producţiei de enzime antioxidante.
Glutation-peroxidaza şi superoxid-dismutaza sunt principalii distrugători de radicali liberi, iar pentru a putea să le producă pe cont propriu, organismul are nevoie de aporturi importante de minerale şi oligo-elemente ca Seleniu şi Zinc.
Fără Zinc şi Seleniu în cantităţi suficiente, sinteza acestor două enzime vitale devine imposibilă. Seleniul a dispărut aproape complet din alimentaţia omului actual, şi aceasta din cauza proceselor artificiale de cultivare şi de prelucrare. În plus, cea mai mare parte a populaţiei înregistrează un deficit cronic de zinc.
Adaosurile zilnice de zinc şi seleniu sunt de aceea esenţiale pentru a asigura cantităţile adecvate de enzime antioxidante.
Alături de producţia internă de antioxidanţi a organismului, există şi agenţi externi care manifestă activitate antioxidantă atunci când ajung în sistemul digestiv uman. Printre aceste surse externe de antioxidanţi se numără vitaminele A, C, E, B1, B5, B6, Beta-Carotenul (precursorul vitaminei A) şi aminoacizii Taurina, Cisteina, Metionina şi Glutation .
Implicarea radicalilor liberi ai oxigenului în etiopatogenia unor maladii a determinat apariţia conceptului de "terapie antioxidantă".
În acest context recomandăm suplimentele alimentare cu potenţial antistres.
În concluzie, stresul este una din cele mai grave probleme ale ultimelor decenii. Tocmai de aceea, un regim de viaţă echilibrat şi aportul de alimente şi suplimente alimentare cu potenţial antioxidant ne pot ajuta să surmontăm stările de stres fără să ajungem la consecinţe grave.
Bibliografie:
[1] Amza L., 2003,“Siguranţa alimentelor şi sănătatea”, Lumina creştinului, septembrie 2003, internet
[2] Costescu A., 2005, “Radicalii liberi”, Simpozion Hofigal, 05 noiembrie, Bucureşti
[3] Mărgineanu G.,2005, “Stressul”, Simpozion Hofigal, 05 noiembrie, Bucureşti
[4] Mitrea N., Gradinaru D., Margina D., Arsene A.,2006, “Stresul oxidativ”, Revista “Farmacist.ro”,Bucuresti, pag.34-37
[5] Calivita., 2006, “Inamicul public nr.1-radicalii liberi şi antidotul împotriva acestora: antioxidanţii naturali”, aprilie, internet
.
2 International Congressof Anti-Aging Medicine
nd

8
2 International Congressof Anti-Aging Medicine
nd
Dr. Sergey V. Nudelman, Dr. Irina A Belikova, Dr. Nikolay A. Golubkov, Dr. Elena V. Piskunova
Objectives of the presentation: 1. Present the benefits of the coordinated group activity of various specialists united by the common goal of anti-aging treatment.2. Discuss the advantages of combined surgical and therapeutic effect on age-related diseases and the grounds for simultaneous surgical procedures.
Cosmetology & Plastic Surgery Center is a private multi-disciplinary medical institution.
Its structure comprises a number of specialized departments: Arteriosclerosis and Cardiovascular Diseases, Gynecology (including Endocrinologic Gynecology and Urogynecology), Cosmetology, Plastic and Aesthetic Surgery, Laboratory Diagnosis, Physiotherapy and Rehabilitation (cosmetic, therapeutic and psychological).
These departments work as independent units developing specific approaches to particular diseases and also as components of comprehensive anti-aging program.
A comprehensive examination algorithm that meets all diagnostic requirements of different specialists reduces the risk of misdiagnosis and provides the continuity of the departments' activity.
Aesthetic surgery is the main field of the clinic's activity; hence the anti-aging program includes preoperative examination, surgery, rehabilitation and follow-up.
The diagnosis implies not only the assessment of surgery and anesthesia-related risks, but also hormone status, ultrasound examination and genetic testing (Genosense Laboratory, Austria). The purpose of the comprehensive diagnosis is to assess the patient's health status with the account of his/her hereditary predisposition factors.
The overall therapeutic efficacy and the final outcome achieved by coordinated activity of all specialists, as a group, is much higher than that of each specialist working individually.
Simultaneous surgical proceduresThe clinic offers its patients a full range of services using state-of-the-art surgical facilities and technologies that allow performing several procedures within one operative setting. This is often necessary to treat age-related diseases, i.e. genital prolapse, stress urinary incontinence, varicose veins, obesity, rectal disorders etc in aesthetic surgery patients. Simultaneous surgery provided by a gynecologist, a proctologist, a vascular surgeon or a plastic surgeon reduces the total operative and anesthesia time, and recovery period.
The rehabilitation stage is based on improving hormonal deficiency, and implies hormone replacement therapy (HRT) both in men and women. The drug dosage as well as the way of administration is chosen with the account of genetic test results. The HRT feasibility is proved by long-lasting aesthetic results achieved surgically.
Anti-Aging Program in AestheticSurgery Clinic

9
2 International Congressof Anti-Aging Medicine
nd
Dr. Jean-Pierre Naim
A-INTRODUCTION:Cardiovascular diseases CVD are the leading cause of death in the Industrial ized countries. According to the WHO, 15 MILLION individuals died in 2005 worldwide as a result of CVD, representing 29 /100 of total mortality.
Last year, 1.4 million people died in the USA from MI,STROKE and SUDDEN DEATH.
In Europe, a difference in mortality from CVD exists between the North and the South. In Spain, Portugal and south of France, we do have a low rate of mortality related to CVD in comparison with UK, Ireland, Germany and Finland where we can find the worse mortality due to ischemic heart disease (role of Mediterranean diet, lifestyle and sun).
A-1:The Endothelial Function:The Endothelial cells- EC –are lining the interior wall of vessels, arteries and capillaries, and they are releasing NO–Nitric Oxide-which is acting as a potent vasodilator, relaxing arteries, thus increasing the blood flow. NO Synthase located in the EC, is the source of NO.
EC are releasing other chemical agents, as ENDOTHELINE which acts as a vasoconstrictor, reducing the blood flow and diameter of arteries.
Estradiol –E2-is a powerful stimulator of Nitric Oxide Synthase 3 (NOs 3) and as a result, is boosting NO production. Aromatase is converting Testosterone to E2.
EC of the coronary arteries and elsewhere (male organ, i.e) are rich in aromatase, and have important number of receptors for Testosterone, indicating that supplementation of the aging male with Testosterone will have a benefit effect on his coronaries and sexual function. Many studies and medical researchs have shown that men with chronic Angina which received low dose of Testosterone, demonstrated a significant stabilization of their symptoms and had an improvement in their physical activity .
Insulin levels and Testosterone are inversely correlated. Insulin is badly influencing the Endothelial function. Hyperinsulinimia is associated with a severe Endothelial dysfunction (metabolic syndrome).
NADH as well as L-arginine, Niacin and Magnesium boost Nos, and as a result, NO production is enhanced dramatically.
A-2: ATHEROSCLEROSISInsulin is boosting SMC-PF (Smooth Muscle Cell-Proliferating Factor).
Any high Insulin level will increase inevitably the proliferation of SMC in the endothelium of the arteries, in the lumen of the vessels, and that will lead to build the plaque.
IGF-1 has a similar effect.
Orthomolecular Approachin Preventing and TreatingCardio-vascular Diseases
The atherosclerosis process is by definition:
-invasion of the intima by SMC.-macrophages phagocyting oxidized LDL, BECOMING “foam cells”, releasing inflammatory cytokines, and cell adhesion molecules (1-CAM, V-CAM)-platelets activation and increased aggregation-deposit of collagene and fibrine-calcium accumulation, creating calcified plaque.
The plaque may rupture, this will activate the coagulation cascade and will increase platelet aggregation and as a result, a thrombus (blood clot) will create an occlusion of the artery (MI,STROKE, ETC.)
Soft plaque at distal LM and fibrocalcified plaques at proxima
A-3:CVD Risk Factors:-Hypertension -Elevated Homocysteine-Diabetes -Hyperlipemia-low HDL -Smoking-Sedentarity -Metabolic syndrome-Genetics and familial predisposition-PPHD -Elevated CRP-Elevated (lp a) -Obesity-Selenium deficiency -Male gender and age over 50
A-4:Cardiovascular polymorphism:Is utilized for CV screening purposes, and still many ongoing researchs and studies. It's a promising field.
Polymorphism of NOs can alter Endothelial Function, several possibilities of change in the gene of this NOs enzyme have been found and many of them reduce NO production.
If a heavy smoker has this kind of polymorphism, he might face a myocardial infarction at a relatively young age. In similar case, this kind of patients should be treated preventatively with NO-Donors.
On the other hand, some APOE genotypes can have a high incidence of MI.
Some studies on Angiotensin and ACE polymorphism have demonstrated that some individuals having a familial history of high blood pressure are in fact having severe polymorphism affecting Angiotensin –ACE gene expression.
Other people having increased coagulation problems as early thrombo-embolism are in reality having a polymorphism in
Fig. 1

10
2 International Congressof Anti-Aging Medicine
nd
PAI-1(Plasminogen Activator Inhibitor) leading to dysfunction in fibrinolysis and increased risk of embolism.
B-Integrative and Metabolic Cardiology:Reminder: ATP, Mitochondria and Krebbs's cycle.
ATP is composed of 3 major groups:- Adenine (purine)- A five Carbon sugar, called D-Ribose which is a pentose- 3 phosphate groups (chain of 3 phosphoric acid) with high energy bonds.
The ATPase is an enzyme breaking the last bond attaching the phosphate group to the molecule of ATP, a process releasing high energy.
The adenylate kinase is an enzyme putting together 2 molecules of ADP to form 1 mol of ATP and 1 mol of AMP, especially when the heart cells are oxygen deprived, what we call commonly a “Myokinase reaction” which can lead to a complete depletion in ATP at the end stage (complete loss pf purines and phosphore!).
The Mitochondria is the cell energy powerhouse.
Mitochondria have an outer and an inner membranes.L-carnitine acts as a shuttle to transport the fuel (fatty
acid or acyl-coA) across the inner mitochondrial membrane whereas Coenzyme Q-1 and coenzyme –Q-10 resides inside the matrix and are key constituents of the Krebbs cycle (Electron Chain Transport) FOR OXIDATIVE PHOSPHORYLATION for the ATP production.
The cell is stocking sugar in form of glycogen.
Glycolysis is the primary pathway of glucose metabolism. Each mole of glucose consumed will produce one pyruvate and 2 ATP. If no Oxygen is available (anaerobic condition), pyruvate will be converted to Lactic Acid and provide one ATP only. Accumulation of Lactic Acid in the cell will put more stress on the cell, if this happen in heart cells, it will create a pain and chest discomfort called ANGINA symptoms, and if this happen in muscle cells, it will create acute cramps and muscle-ache.
In aerobic condition with enough oxygen present in the cell, one mole of Pyruvate will enter the mitochondria, will be transformed in “fuel” by the krebbs cycle and will provide 36 Molecules of ATP, WHILE A FATTY ACID as PALMITIC acid (16 C) WILL PROVIDE THROUGH THE SAME MITOCHONDRIAL METABOLISM OF beta-OXYDATION 129 molecules of ATP !
Fig. 1 HN
o
o
o
o
o
o
o
o
o
o o
o oH
HH
HH H
H
PP
Adenine
NN C
C CN N
CH
2
P
3 - Phosphates
D - Ribose
ATP
ADP
+Pi -Pi
O2
STAGEI
STAGEII
LACTIC ACID
O2
Glycogen
Gllucose 1-P
Gllucose 6-P
Fructose 6-P
Glyceraldehyde 3-P
1,3 - Diphosphoglycerate
3 - Phosphoglycerate
2 - Phosphoglycerate
Phosphoenol Pyruvate
Pyruvate
Fig. 5
Fig. 2
Fig. 3
Outer Membrane Inner Membrane
MatrixIntermembrane Space
Fig. 4
11
2 International Congressof Anti-Aging Medicine
nd
There was a dramatic increase in CHF worldwide those last 15 years corresponding to the large use of statins without supplementing in Co-Q-10. It's a major health concern!
The recommended dosage: 100-200 mg daily in routine. Could be increased up to 600 -800 mg /day in case of severe angina, and up to 1200 mg/day in case of CHF, DILATED CARDIOMYOPATHY OR DIASTOLIC DYSFUNCTION.
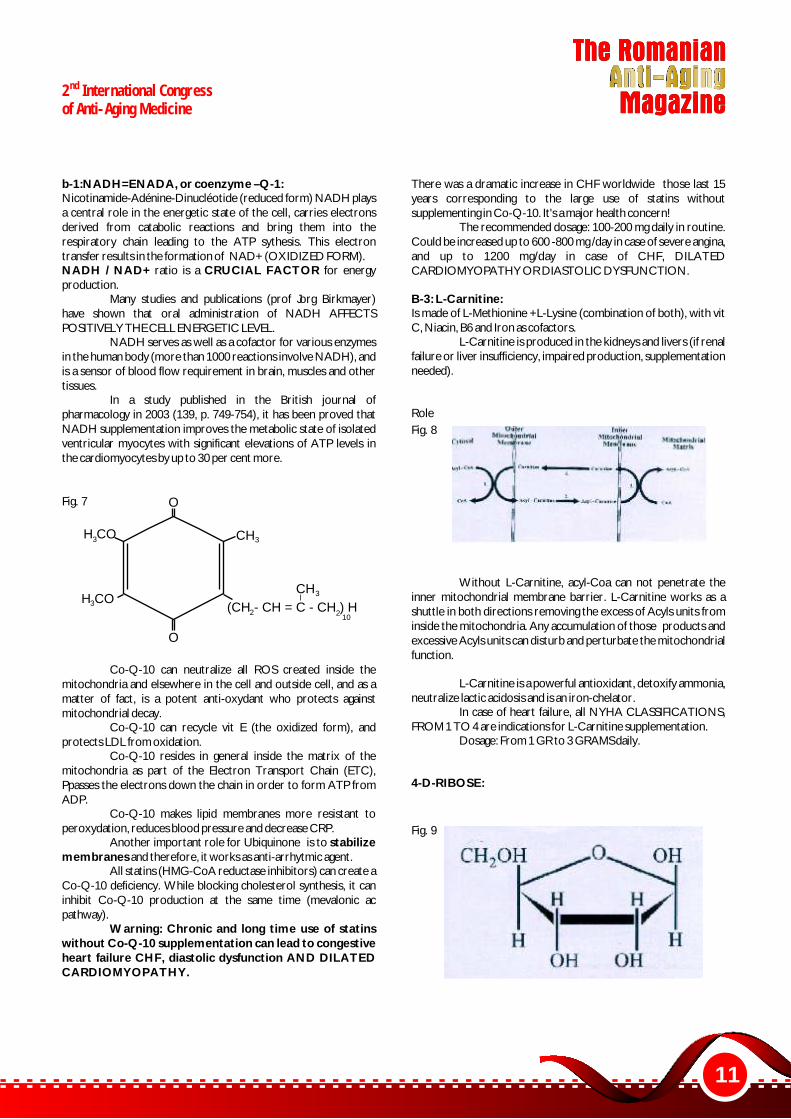
B-3: L-Carnitine:Is made of L-Methionine +L-Lysine (combination of both), with vit C, Niacin, B6 and Iron as cofactors.
L-Carnitine is produced in the kidneys and livers (if renal failure or liver insufficiency, impaired production, supplementation needed).
Role
Without L-Carnitine, acyl-Coa can not penetrate the inner mitochondrial membrane barrier. L-Carnitine works as a shuttle in both directions removing the excess of Acyls units from inside the mitochondria. Any accumulation of those products and excessive Acyls units can disturb and perturbate the mitochondrial function.
L-Carnitine is a powerful antioxidant, detoxify ammonia, neutralize lactic acidosis and is an iron-chelator.
In case of heart failure, all NYHA CLASSIFICATIONS, FROM 1 TO 4 are indications for L-Carnitine supplementation.
Dosage: From 1 GR to 3 GRAMS daily.
4-D-RIBOSE:
b-1:NADH=ENADA, or coenzyme –Q-1:Nicotinamide-Adénine-Dinucléotide (reduced form) NADH plays a central role in the energetic state of the cell, carries electrons derived from catabolic reactions and bring them into the respiratory chain leading to the ATP sythesis. This electron transfer results in the formation of NAD+ (OXIDIZED FORM).NADH / NAD+ ratio is a CRUCIAL FACTOR for energy production.
Many studies and publications (prof Jorg Birkmayer) have shown that oral administration of NADH AFFECTS POSITIVELY THE CELL ENERGETIC LEVEL.
NADH serves as well as a cofactor for various enzymes in the human body (more than 1000 reactions involve NADH), and is a sensor of blood flow requirement in brain, muscles and other tissues.
In a study published in the British journal of pharmacology in 2003 (139, p. 749-754), it has been proved that NADH supplementation improves the metabolic state of isolated ventricular myocytes with significant elevations of ATP levels in the cardiomyocytes by up to 30 per cent more.
Co-Q-10 can neutralize all ROS created inside the mitochondria and elsewhere in the cell and outside cell, and as a matter of fact, is a potent anti-oxydant who protects against mitochondrial decay.
Co-Q-10 can recycle vit E (the oxidized form), and protects LDL from oxidation.
Co-Q-10 resides in general inside the matrix of the mitochondria as part of the Electron Transport Chain (ETC), Ppasses the electrons down the chain in order to form ATP from ADP.
Co-Q-10 makes lipid membranes more resistant to peroxydation, reduces blood pressure and decrease CRP.
Another important role for Ubiquinone is to stabilize membranes and therefore, it works as anti-arrhytmic agent.
All statins (HMG-CoA reductase inhibitors) can create a Co-Q-10 deficiency. While blocking cholesterol synthesis, it can inhibit Co-Q-10 production at the same time (mevalonic ac pathway).
Warning: Chronic and long time use of statins without Co-Q-10 supplementation can lead to congestive heart failure CHF, diastolic dysfunction AND DILATED CARDIOMYOPATHY.
O
H CO
H CO
O
(CH - CH = C - CH ) H
CH
CH3
210
33
32
Fig. 7
Fig. 8
Fig. 9

12
2 International Congressof Anti-Aging Medicine
nd
Dosage: 5-7 grams/daily In case of MI and CHF: 7-10 gr/daily
5-Magnesium:Is a crucial cofactor for all biochemical reactions involving ATP.
Involved in many as 300 enzyme-reactions in the body.Is essential for the transport of ATP in the cytosol, helps to relax the muscle walls of the arteries, acts as an “calcium channel blocker”, as a result, decreases blood pressure.
Magnesium is used for arryhtmias and mitral valve prolapsus.
IV administration is used in a variety of cardiac emergencies, improve NOs activity, and as result, increase coronary blood flow.
Works very well against migraine (orally, 400 mg bid daily) and IV in case of acute crisis.
C-Clinical cardiology:C-1: Hidden source of CVD risk: The PostPrandial Hyperlipidemia Disorder -PPHD-This disorder is characterized by abnormally persistent lipid remnants that persist in the bloodstream for up to 18-24 hours after meal. Those lipoproteins after a lipid-rich dinner f. ex, can inflict serious damage to the arteries. Those fat particles are among the most potent causes of heart attacks and strokes.
Normally, in healthy adults, those particles should be cleared from the blood within 4 to 6 hours.
Many clinical studies have indicated that those postprandial lipoproteins are powerful instigators of coronary plaque, carotid plaque and plaque in the aorta.
In reality, they block NO production, increase releasing of Endothelin by EC, causing Endothelial dysfunction, increase cell adhesion molecules CAM allowing white blood cells to adhere and enter the arterial wall, leading to plaque formation, and activate blood clotting factors while inhibiting clot breakdown.
Last, they trigger the production of small LDL particles.
High levels of fasting TG strongly suggest the presence of PPHD.
For example, in a patient having metabolic syndrome, we can find that the level of TG 6 hours after a meal will be >260 mg/dl, indicating clearly a PPHD.
No IDL (Intermediate) density lipoprotein should be present in blood draw fasting. If present, it means that PPHD exist in a given patient, and that he will experience more serious CVD RISKS.How to lower PPHD?a) replace saturated fats by Monounsaturated and PUFA n-3) stimulation of the lipoprotein lipase activity)b) weight lossc) low glycemic index dietd) green tea, soy protein e) vigorous physical exercisef) statins, fibrates, red rice yeast, policosanol and roseglitazone
D-Ribose is a 5 carbons sugar (pentose), and is not a part of glycolysis (6C).
Synthethized from glucose through an independent mechanism called “the Pentose Phosphate Pathway” which is:- Time consuming- Rate-limited by 2 enzymes:G-6-P-D (glucose-6-phosphate dehydrogenase) 6-P-G-D (6phosphogluconate dehydrogenase)
Supplementing with D-Ribose bypasses this slow and rate limited pathway, will inevitably accelerate ATP synthesis.
This pentose is quickly absorbed orally, 95 per cent of it will be used by different tissues while only 5 per cent will be excreted in the urine.
In case of heart attack or acute coronary syndrome, the heart will loose more than 50 /100 of his ATP pool, any administration of D-Ribose will help to a quick recovery and diastolic function within 24-48 hours.
13
2 International Congressof Anti-Aging Medicine
nd
- Curcumin in turmeric inhibits COX-2 AND 5-LOX- Green tea inhibits 5-lox- Ginger inhibits COX-2- Ginkgo biloba reduces excess fibrinogen- Vit K: MENAQUINONE -4 AND 7 (Vit K2) inhibits the production of inflammatory cytokines and has been shown to reserve the hardening of the vessels walls in regulating osteocalcin and shifting calcium out of the arteies.- Pomegranate: Inhibits inflammation, has a direct effect on IL-1 Béta (suppressing effect), moreover, is a potent anti-oxidant of LDL and some promising studies have shown that a regular intake of this fruit (one full fruit daily) can reverse atherosclerosis.- DHEA: Suppresses inflammatory cytokines, lower dramatically CRP and fibrinogen.
Vit D: Down regulate gene expression of NF-Kappa Béta (key role in inflammation and cancer) and has a powerful immuno-modulator activity.
Anti-Inflammatory diet:Rich in nuts, cereals, MU fats, fish, Colza oil, low
glycemic index, low in arachidonic acid and rich in fibers.
Homocystein, the silent killer:Homocysteine is a byproduct of the metabolism of Methionine.
High plasma level of homocysteine is a powerful risk factor for MI,stroke, Alzheimer, depression osteoporosis, etc…and is an independent risk factor for CVD.
You can reduce your homocysteine by enhancing methylation, by transferring a methyl group-CH3 from one molecule to another. Methylation takes place in every cell several times daily.
When Methionine donates her methyl group, it becomes Homocysteine.
Other Methyl donors: TMG, SAMe, MSM. They can facilitate the recycling of homocysteine back to Methionine. This is what we call a “Methylation process”. This reaction does need the help of methylating factors as, Vit B6, Vit B12, folic ac and zinc.
Homocystein is causing the initial damage to the lining of the blood vessels, opening the door to oxidized LDL to penetrate the intima and build up inside the walls with macrophages, increasing free radical activity, blood clotting mechanisms and impairing fibrinolysis. The plasma level of homocysteine should be kept below 10 mc mol/l.
References:“The new science of growing older without aging” BY Dr Philip Lee Miller, life extension foundation edition
“The Sinatra solution”by Dr Stephen Sinatra
“The british journal of pharmacology “2003-139,749-754
“Magnesium intake and risk of coronary heart disease among men” j Amer coll Nutri 2004,23(63-70)By Al –Delaimy et all
Zimmer HG, Hibel: ”the oxidative pentose phosphate pathway in the heart: regulation, physiological significance and implications”Basic res cardio 1992-87 :3003-3016.
Suzuki y, Masuma et all : »Myocardial carnitine deficiency in chronic heart failure »Lancet 1982Rundek t, A Naini, R Sacco et all:”Atorvastatin decreases theCO-Q-10 level in patient's blood at risk for CV disease and stroke”Arch Neuro 2004-61.889-92
“Polymorphism diagnostics” Dr Huber, antiaging for professionals journal, num 2,2005 .57-58
C-2:How to prevent and treat CVD? a) NIACIN When taken at a dose of 500 -1500 mg a day, Niacin benefits are: - Increase in HDL by 20-35 per cent - Decrease in lp(a) - Decrease in LDL by 10-20 per cent - Decrease in small LDL particles - Action on NOs
Combination with n-3 fatty acids is a powerful treatment in combating heart disease.b) Tocotrienols and tocopherols –Vit E famil
Alpha and gamma tocopherols and all tocotrienols are fat soluble antioxidants that protect LDL and lipid membranes from peroxidation, natural vit E (GAMMA –TOCOPHEROL) is a COX-2 inhibitor, improve blood viscosity and rheology and act as a free radical scavenger, particularly against peroxynitrite.
Tocotrienols can decrease LDL at a dosage of 75 mg a day.
Total daily intake of tocopherols and tocotrienols should not exceed 500 mg/daily.c) n3-PUFA fish oilsEPA and DHA at a daily dose of 2 gr can:- lower total cholesterol, decrease TG and reduce LDL- diminish fibrinogen and CRP- reduce coagulation's factors- reduce COX-2 gene expression and decrease inflammatory cytokines.d) Aspirin- very recent publication of the “Nurses health study”carried out by Harvard medical school and general Mass. hospital (Boston) who monitored 80000 women for over 20 years.
During this study, 30000 took low to moderate doses of Aspirin.
The conclusion was very clear:- Women who reported taking low to moderate doses of aspirin had a 25 per cent lower risk of death from any cause.- Aspirin users had a 38 per cent lower risk of death from CV disease, and 12 per cent lower risk of death from cancer.
It speaks for itself.
e) Fight against inflammation:Inflammation is an important contributor to atherosclerosis and development of heard disease.-5-lipoxygenase (5-lox) is an important enzyme producing mainly Leucotriene-B4 “fueling” inflammation and attacking arterial walls (and joints) creating atherosclerosis (pro-inflammatory agent).
Inflammation causes arterial plaques to breakoff and plays a deadly role in destabilizing arterial plaques. Meanwhile, it can cause excessive free radical damage, therefore it can deplete the body's reserves in antioxidants.
New strategy to cool inflammation -protocol- :- Use of Boswellia extract to inhibit 5-lox (5-loxin).- Lipid lowering medications, as n-3 PUFA fish oils, statins

14
nd

15
La Al Doilea Congres International de Medicina Anti-Aging desfasurat la Palatul Parlamentului sub Inaltul Patronaj al Comisiei pentru Sanatate si Familie Camera Deputatilor condusa de Academician Profesor Doctor Mircea IFRIM am avut onoarea de a ne fi oaspete Catheryne DECUIPER Presedinte EUROMEDICOM, Chr i s thophe LOUINO Genera l Manager EUROMEDICOM, Chistope de JAEGER Pesedinte Comitet Stiintific EUROMEDICOM , Michael KLENTZE Secretar General al Societatii Europene de Medicina Anti-Aging , Samuel BERGMAN Presedintele Asociatei Canadiene de Medicina Anti-Aging, Jean Pierre NAIM Presedinte Comitet Stiintific al Academiei Elvetiene de Medicina Anti-Aging , Irina BELIKOVA Vicepresedinte al Societatii Ruse de Medicina Anti-Aging.Multumim oaspetilor nostri, participantilor cat si companiilor prezente la acest eveniment si ai anuntam pe aceasta cale ca in data de 2-4 mai 2008 se va organiza Al Treilea Congres International de Medicina Anti-Aging si Primul Congres International din Romania de Lasere in Medicina si Chirurgie.Cele doua congrese vor avea loc in acelasi timp, sub patronajul Asociatiei de Medicina Anti-Aging, in Bucuresti organizandu-se numeroase workshop-uri atat de medicina anti-aging cat si de estetica si lasere .Toate manifestarile stiintifice vor fi acreditate de Colegiul Medicilor iar participantii vor primi credite EMC. De asemenea datorita bunelor relatii cu Academia Americana de Medicina Anti-Aging avem bucuria de a va anunta ca initiatorul conceptului de medicina anti-aging Dr. Robert GOLDMAN a confirmat participare ca Invitat de Onoare al acestor manifestari stiintifice.Reamintim membrilor AMAA ca beneficiaza de reduceri considerabile la inscrierea in evenimentele internationale organizate de EUROMEDICOM si ACADEMIA AMERICANA DE MEDICINA ANTI-AGING A4M.
16
2 International Congressof Anti-Aging Medicine
nd
Dr. Gabriela Najjar & Dr. Ahmad Najjar
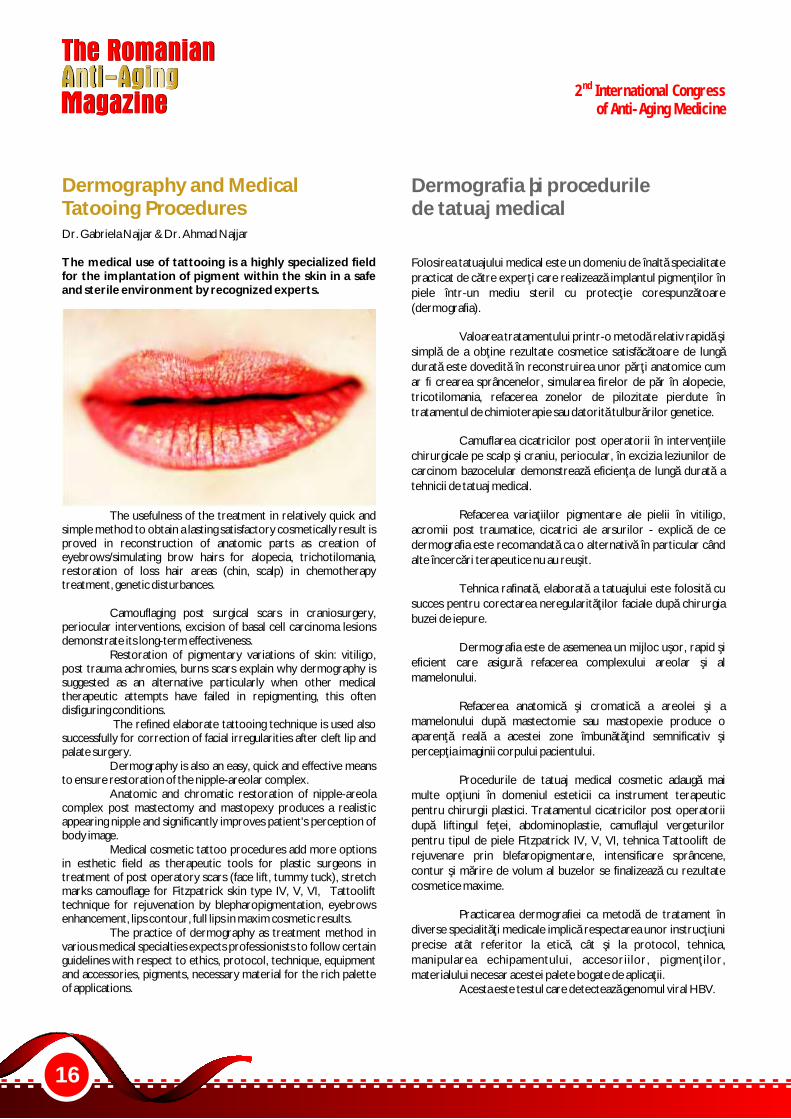
The medical use of tattooing is a highly specialized field for the implantation of pigment within the skin in a safe and sterile environment by recognized experts.
The usefulness of the treatment in relatively quick and simple method to obtain a lasting satisfactory cosmetically result is proved in reconstruction of anatomic parts as creation of eyebrows/simulating brow hairs for alopecia, trichotilomania, restoration of loss hair areas (chin, scalp) in chemotherapy treatment, genetic disturbances.
Camouflaging post surgical scars in craniosurgery, periocular interventions, excision of basal cell carcinoma lesions demonstrate its long-term effectiveness.
Restoration of pigmentary variations of skin: vitiligo, post trauma achromies, burns scars explain why dermography is suggested as an alternative particularly when other medical therapeutic attempts have failed in repigmenting, this often disfiguring conditions.
The refined elaborate tattooing technique is used also successfully for correction of facial irregularities after cleft lip and palate surgery.
Dermography is also an easy, quick and effective means to ensure restoration of the nipple-areolar complex.
Anatomic and chromatic restoration of nipple-areola complex post mastectomy and mastopexy produces a realistic appearing nipple and significantly improves patient's perception of body image.
Medical cosmetic tattoo procedures add more options in esthetic field as therapeutic tools for plastic surgeons in treatment of post operatory scars (face lift, tummy tuck), stretch marks camouflage for Fitzpatrick skin type IV, V, VI, Tattoolift technique for rejuvenation by blepharopigmentation, eyebrows enhancement, lips contour, full lips in maxim cosmetic results.
The practice of dermography as treatment method in various medical specialties expects professionists to follow certain guidelines with respect to ethics, protocol, technique, equipment and accessories, pigments, necessary material for the rich palette of applications.
Dermography and Medical Tatooing Procedures
Folosirea tatuajului medical este un domeniu de înaltă specialitate practicat de către experţi care realizează implantul pigmenţilor în piele într-un mediu steril cu protecţie corespunzătoare (dermografia).
Valoarea tratamentului printr-o metodă relativ rapidă şi simplă de a obţine rezultate cosmetice satisfăcătoare de lungă durată este dovedită în reconstruirea unor părţi anatomice cum ar fi crearea sprâncenelor, simularea firelor de păr în alopecie, tricotilomania, refacerea zonelor de pilozitate pierdute în tratamentul de chimioterapie sau datorită tulburărilor genetice.
Camuflarea cicatricilor post operatorii în intervenţiile chirurgicale pe scalp şi craniu, periocular, în excizia leziunilor de carcinom bazocelular demonstrează eficienţa de lungă durată a tehnicii de tatuaj medical.
Refacerea variaţiilor pigmentare ale pielii în vitiligo, acromii post traumatice, cicatrici ale arsurilor - explică de ce dermografia este recomandată ca o alternativă în particular când alte încercări terapeutice nu au reuşit.
Tehnica rafinată, elaborată a tatuajului este folosită cu succes pentru corectarea neregularităţilor faciale după chirurgia buzei de iepure.
Dermografia este de asemenea un mijloc uşor, rapid şi eficient care asigură refacerea complexului areolar şi al mamelonului.
Refacerea anatomică şi cromatică a areolei şi a mamelonului după mastectomie sau mastopexie produce o aparenţă reală a acestei zone îmbunătăţind semnificativ şi percepţia imaginii corpului pacientului.
Procedurile de tatuaj medical cosmetic adaugă mai multe opţiuni în domeniul esteticii ca instrument terapeutic pentru chirurgii plastici. Tratamentul cicatricilor post operatorii după liftingul feţei, abdominoplastie, camuflajul vergeturilor pentru tipul de piele Fitzpatrick IV, V, VI, tehnica Tattoolift de rejuvenare prin blefaropigmentare, intensificare sprâncene, contur şi mărire de volum al buzelor se finalizează cu rezultate cosmetice maxime.
Practicarea dermografiei ca metodă de tratament în diverse specialităţi medicale implică respectarea unor instrucţiuni precise atât referitor la etică, cât şi la protocol, tehnica, manipularea echipamentului, accesoriilor, pigmenţilor, materialului necesar acestei palete bogate de aplicaţii.
Acesta este testul care detectează genomul viral HBV.
Dermografia þi procedurile de tatuaj medical

18
2 International Congressof Anti-Aging Medicine
nd
Dr. C. Borşa, Dr. C. Rusu, Dr. M. Borşa
Diabetes mellitus is associated with oxidative and carbonyl stress and accelerated non-enzymatic glycation.
These processes impairs endothelial function and may play an important role in the pathogenesis of cardiovascular events.
We investigated the in vitro serum lipid oxidation kinetics and the advanced oxidation protein products in elderly patients with type 2 diabetes mellitus for assessing oxidative status and its relationships with other metabolic parameters.
Material and Methods: The kinetics of in vitro copper ions induced lipid oxidation in unfractionated serum was assessed by continuous recording of the time-dependence of the oxidation products accumulation at 245 nm during five hours and after 24 hours of the oxidation induction.
Advanced oxidation protein products (AOPP) were determined spectrophotometrically at 340 nm.
Results: The studies concerning the in vitro lipid oxidation kinetics were pointed out markant and significant increased values of recorded kinetic parameters in the elderly patients with type 2 diabetes mellitus (N=24), compared with control (N=20). Thus, the maximal absorbance of oxidation products accumulation at 245 nm (OD ; 0.493+0.142 vs. 0.346+0.07; p<0.05), and the maximal max
oxidation rate (V ; 2.86+0.71 vs. 1.83+0.49; p<0.05) were max
significant higher in diabetes group; whereas the lag time was markant lower.
The oxidation products accumulation at 24 hours after its inducement with copper ions, as well as the rate of their accumulation at 5 hours have been recorded markant increases in study group, compared with control.
The levels of serum advanced oxidation protein products were significant higher in elderly patients with type 2 diabetes mellitus versus control group (78.8+13.1 vs. 71.3+9.7; p<0.05). For diabetic patients a significant positive correlation of AOPP with serum triglycerides (r=0.665; p<0.05) was pointed out.
Conclusions: Our results reveal the incresed oxidative status and the acceleration of oxidative processes in elderly patients with type 2 diabetes, which may contribute to extenssive formation of advanced oxidation protein products, which acts as inflammatory mediators and lead to progression of atherogenic injuries.
Advanced Oxidation ProteinProducts and Lipid OxidationKinetics in Elderly Patiens withType 2 Diabetes Mellitus
Diabetul este asociat cu stresul oxidativ şi carbonil, precum şi cu intensificarea proceselor de glicare neenzimatică.
Aceste procese afectează funcţia endotelială şi pot juca un rol important în patogeneza evenimentelor cardiovasculare.
Scopul acestui studiu constă în investigarea cineticii de oxidare "in vitro" a lipidelor serice şi a acumulării produşilor de oxidare avansată ai proteinelor la pacienţi vârstnici cu diabet de tip 2, în vederea determinării statusului oxidativ şi a relaţiilor lui cu alţi parametri metabolici.
Material şi metode: Cinetica de oxidare a lipidelor în ser total, nefracţionat, indusă "in vitro" cu ioni de cupru (II), a fost urmărită prin înregistrarea continuă, în funcţie de timp a acumulării produşilor de oxidare la lungimea de undă de 245 nm, timp de 5 ore; precum şi după 24 de ore de la inducerea ei.
Produşii de oxidare avansată ai proteinelor (AOPP) au fost determinaţi spectrofotometric la 340 nm.
Rezultate:Studiile privind cinetica oxidării "in vitro" a lipidelor serice au relevat valori marcant sau semnificativ crescute ale parametrilor cinetici urmăriţi la grupul de pacienţi vârstnici cu diabet de tip 2 (N=24), comparativ cu grupul de control (N=20).
Astfel, absorbanţa maximă la 245 nm, a acumulării produşilor de oxidare (OD ; 0.493+0.142 vs. 0.346+0.07; max
p<0.05), şi viteza maximă de oxidare (V ;2.86+0.71 vs. 1.83+0.49; max
p<0.05) au fost semnificativ crescute la grupul cu diabet, în timp ce timpul de "lag" a fost mult diminuat.
Acumularea produşilor de oxidare la 24 de ore de la inducerea ei cu ioni de cupru, ca şi viteza acumulării lor după 5 ore au înregistrat creşteri marcante la lotul de studiu, comparativ cu cel de control.
Nivelele serice ale produşilor de oxidare avansată ai proteinelor au fost semnificativ crescute la pacienţi vârstnici cu diabet de tip 2, faţă de grupul de control (78.8+13.1 vs. 71.3+9.7; p<0.05). La pacienţii diabetici s-a semnalat o corelaţie pozitivă semnificativă a AOPP cu trigliceridele serice (r=0.665; p<0.05).
Concluzii: Rezultatele obţinute relevă statusul oxidativ crescut precum şi accelerarea proceselor oxidative, la pacienţii vârstnici cu diabet de tip 2, care ar putea contribui la extensiva formare a produşilor de oxidare avansată ai proteinelor, care, acţionând ca mediatori ai inflamaţiei, pot conduce la progresia leziunilor aterogene.
Produþii de oxidare avansatã ai proteinelor þi cinetica oxidãriilipidelor la pacienþii vârstnici cudiabet de tip 2

19
2 International Congressof Anti-Aging Medicine
nd
Dr. Cătălin Enăchescu
No Needle Mesotehrapy represents a new alternative for micro injection treatment, a solution for anti rejuvenation treatment to the face and body.
The new treatment, called Derma Wave No Needle Mesotherapy™, use electrical shocks and has biostimulative effects on tissue.
Derma Wave treatment is based on a new technique named Aquaphoresis™, and use special electrical waveforms H for reactivity of physiological processes from tissue for washing out the cellulite.
No Needle Mesotherapy™ is a sure method and represents an alternative and a treatment for face rejuvenation, but also an anti - cellulite treatment.
No Needle MesotherapyAn Alternative Solution for AntiCellulite Treatment and for SkinRejuvenation
This technique is characterized by a comfortable position of clients
during therapy, does not require bandages, time for post operator
return, it is pain free and does not require anesthesia. After the end of the therapy the accommodation of
clients in society is more easily because of a new natural look
results to the face and body. No Needle Mesotherapy™ results
are semnificative. After the end of a complete therapy session,
generally after maximum 1 month the clients are pleased and they
can observe a high quality of face skin, an increase of face tonus and
body tonus. The treatment represents a combination between the
photodynamic therapy based on wavelength non invasive laser
beam and non invasive mesotherapy. No Needle Mesotherapy™ use special technique
named Aquaphoresis™ based on different special current forms
which permit the transport of active substances - in mezo layer
without use needle. This treatment contributes meaningful to the
microcirculation improvement, to the sanguine circulation
improvement of treated zones, and on the lymphatic drainage.

20
2 International Congressof Anti-Aging Medicine
nd
Dr. Ciomaga Georgeta
The high risk for cardiovascular diseases at young ages in autoimmune affections is well known. The mechanism of producing these diseases remains unknown and incites to studies. It is demonstrated that in this process much more mechanisms intervene which determine alterations of coagulation, perturbations in the equilibrium and structure of vascular endothelium functions. Ox LDL is promoter of atherosclerosis together with inflammatory and immunological mechanisms which are related to deregulation of lipids and formation of spumous cells. Recent studies demonstrate the presence of complexes formed by ox LDL with glycoprotein-1 and/or C reactive protein in the intima of atherosclerotic cells. The atherosclerotic cells contain immunogobulins which recognize ox LDL. Ox LDL stimulates production of auto antibodies of B cells while antibodies dependant of T cell have a protective role. The auto antibodies against ox LDL are present at patients with cardiovascular diseases and have an increased level in carotid atherosclerosis, vascular peripheral diseases and myocardial infarction. The high prevalence was observed in patients treated with corticosteroids, which indicates also an immune response. The increase of ant-ox LDL antibodies levels is observed at patients with autoimmune diseases in rheumatoid arthritis, diabetes mellitus, uremia, psoriasis, systemic lupus erythematosus, antiphospholipid antibodies syndrome, chronic periaortitis, hepatocellular carcinoma, ß-thalassemia, preeclampsia or eclampsia. The native antibodies and anti-idiotype antibodies with IGIV have a stimulating effect of atherosclerosis and proeression of cardiovascular diseases. The administration of IGIV at deficiency of apoE modulates the development of fats and progression of fibro-fats in the atherosclerotic plaque and results the reduction of atherosclerosis. The treatment with IV immunoglobulins associated with active T cells reduces the titer of anti-ox LDL IgM antibodies. Human IGIV represents a protection for anti-ox LDL antibodies.
Atherosclerosis, even known from very long time, still remains an enigma. The specific diseases caused by atherosclerosis includes diseases of the coronary artery, the cerebral vascular diseases, thromboembotic strokes, transient ischemic strokes and vascular complications from diabetes mellitus.
The thrombocytes are directly involved in the atherosclerotic process. These contain trigger substances of platelet growth factor and of prostaglandins which stimulate the smooth muscles cells from the wall of the arteries. (1).
Fibrinogen, thrombocytes and other coagulation factors aggregate with LDL cholesterol, triglycerides and calcium on the arterial wall, this being the starting point for the development of the atherosclerotic plaque. The abnormal aggregation will
The Cardiovascular Diseases -Increased Risk of Death inAutoimmune Diseases
Riscul crescut al bolilor cardiovasculare la vârste tinere în bolile autoimune este bine cunoscut. Mecanismul producerii acestora rămâne încă necunoscut şi incită la studiu. Este demonstrat că în producerea acestora intervin mai multe mecanisme care determină perturbări ale coagulării, perturbări ale echilibrului structurii şi funcţiei endoteliului vascular. Ox LDL este promotor al aterosclerozei împreună cu mecanismele inflamatorii şi imunologice ce ţin de dereglarea lipidelor şi formarea de celule spumoase. Studii recente demonstrează prezenţa complexelor formate din ox LDL cu glicoproteină -1 şi/sau proteină C reactivă, în intima leziunilor aterosclerotice. Leziunile aterosclerotice conţin imunoglobuline care recunosc oxLDL. Ox LDL stimulează producţia de autoanticorpi ale celulei B în timp ce anticorpii dependenţi de celula T au rol protectiv. Autoanticorpii împotriva ox LDL sunt prezenţi la pacienţii cu boli cardiovasculare şi au nivel crescut în ateroscleroza carotidiană, bolile periferice vasculare şi infarctul de miocard. Înalta prevelanţă s-a observat la pacienţii trataţi cu corticosteroizi şi indică de asemeni răspuns imun. Creşterea nivelului anticorpilor anti ox-LDL este evidenţiată la pacienţii cu boli autoimune în artrita reumatoidă, diabet zaharat, uremie, psoriasis, lupus eritematos sistemic, sindrom anticorpi antifosfolipid, periaortită cronică, carcinomul hepatocelular, beta talasemia şi preeclampsia sau eclampsia. Anticorpii nativi şi anticorpii anti-idiotip cu IGIV au efect de stimulare a aterosclerozei şi progresie a bolilor cardiovasculare. Administrarea de IGIV la deficienţa de apoE modulează dezvoltarea grăsimilor şi progresia fibrogrăsimi în placa aterosclerotică şi rezultă reducerea aterosclerozei. Tratamentul cu imunglobuline IV asociat cu celule T anergice reduc titrul anticorpilor IgM anti ox LDL . IGIV umani conţin protecţie pentru anticorpii anti-ox LDL şi anticorpii anti ox LDL.
Ateroscleroza, deşi cunoscută de foarte mult timp, rămâne încă o enigmă. Bolile specifice cauzate de ateroscleroză includ bolile arterei coronare, bolile cerebrale vasculare, atacuri trombotice, atacuri tranzitorii ischemice şi complicaţii vasculare din diabetul zaharat.
Trombocitele sunt implicate direct în procesul aterosclerotic. Acestea conţin substanţe trigger ale factorului de creştere plachetar şi ale prostaglandinelor care stimulează celulele muşchilor netezi din pereţii arterelor.
Fibrinogenul, trombocitele şi alţi factori de coagulare agregă cu LDL colesterol, trigliceride şi calciu pe peretele arterial, fiind punctul de plecare pentru dezvoltarea plăcii aterosclerotice. Agregarea anormală va determina apariţia trombusului cu producerea ischemiei şi/sau infarctul.
La procesul trombotic intervin factorii intrinseci, mai ales genele, factorii de creştere, celulele peretelui vaselor şi alte componente sanguine. Toate acestea interacţionează contribuind la procesul trombotic.
Agregarea trombocitelor este normală în homeostazie, unde trigger este expunerea plachetelor la matricea subendotelială după injuria peretelui vaselor.
Bolile Cardiovasculare - risccrescut de deces în boli autoimune
21
2 International Congressof Anti-Aging Medicine
nd
determine the appearance of the clot with the production of ischemia and/or infarction.
At the thrombotic process intrinsic factors, especially genes, growing factors, cells of the vessels arteries and other blood components intervene. All these interact, contributing to the thrombotic process.
The aggregation of thrombocytes is normal in homeostasis, where trigger is the exposure of platelets to the sub-endothelial matrix after injury of vessels wall. The formation of thrombus is initiated by membrane receptor and the complex glycoprotein I-IX-V which interact with von Willebrand factor. The signal is transmitted to the plasmatic membrane of the thrombocytes, which once activated determine the secretion of agonist ADP with the increase of citosolic Ca++ and of Ca++ dependant of the activation of áIIbâ integrine. Through that, the aggregation of thrombocytes and the adherence of von Wilebrand factor are mediated. (2)
GPIbá connects subsequently to thrombin, P-selectin, and Mac-1 integrin.
The glycoprotein Ib (or apolipoprotein H) is directly involved into the development of human atherosclerosis through the activation of complement complexes and the reduction of oxLDL activity.
The genetic involvement of unleashing the atherosclerosis is demonstrated through the alteration of pro-thrombin gene G20210A.
The lipoprotein a is a major and independent to atherosclerosis and cardiovascular diseases risk factor. It represents a special class of lipoproteins which is composed of a molecule of LDL connected to a glycoprotein. The lipoprotein a has the capacity to connect fibrin to the membrane proteins of endothelial cells and monocytes, inhibiting the adherence of plasminogen and the generation of plasmin. The inhibition of plasmin generation and the accumulation of lipoprotein a favor this way the deposit of fibrin and cholesterol on the vascular sites. (3,4,5).
The interleukin 18 plays a role in unleashing of the inflammatory cascade from atherosclerosis through the induction of gamma interpheron and T lymphocytes. The increased level of these constitutes an independent factor predictor of death in cardiovascular diseases. (6,7).
The matrix metalloproteinases (MMP-9), or B gelatinases secreted by macrophages or other cells of inflammation are increases at patients with instable angina, constituting, after Blakenberg, a somber predictor in the cardiovascular disease. (8)
The proinflammatory cytokines like: C reactive protein, cytokines (interleukin 18, interleukin 6), E selectin, intercellular molecules of adherence-1 constitute procoagulant factors. (9, 10, 11, 12, 13, 14, 15)
Although there still are different opinions, the hypercoagulant status constitute an increased risk for unleashing the atherosclerosis.
The endothelium remains a great enigma, it is hidden and unknown. Both platelets and endothelium have the same origin, the bone marrow, which give them resembling phisiopathological properties (16,17).
The immune disease which is characterized by arterial
Formarea trombusului este iniţiată de receptorul de membrană şi complexul glicoproteina I -IX-V care interacţionează cu factorul von Willebrand. Semnalul este transmis la membrana plasmatică a trombocitelor, care odată activate determină secreţia de agonist ADP cu creşterea Ca++citosolic şi al Ca++dependent de activarea integrinei aIIbß.
Prin aceasta se mediază agregarea trombocitelor şi adeziunea factorului von Willebrand sau al fibrinogenului.
GPIb alfa se leagă consecutiv la trombină, P-selectină şi integrină Mac-1.
Glicoproteina Ib (sau apolipoproteina H) este direct implicată în dezvoltarea aterosclerozei umane prin activarea complexelor complement şi reducerea activităţii oxLDL.
Implicarea genetică a declanşării aterosclerozei este demonstrată prin modificările genei protrombinei G20210A.
Lipoproteina a este un factor de risc genetic major şi independent pentru ateroscleroză şi boli cardiovasculare.
Reprezintă o clasă specială de lipoproteine ce se compune dintr-o moleculă de LDL legată la o glicoproteină.
Lipoproteina are capacitatea de a lega fibrina la proteinele de membrană ale celulelor endoteliale şi monocitelor inhibând aderarea plasminogenului şi generarea de plasmină. Inhibarea generării de plasmină şi acumularea lipoproteinei favorizează depozitarea de fibrină şi colesterol pe situsurile vasculare. (3 ,4, 5)
Interleukina 18 joacă rol în declanşarea cascadei inflamaţiei din ateroscleroză prin inducerea producţiei de interferon gama şi limfocite T. Nivelul crescut al acestora constituie un factor independent predictor al morţii în bolile cardiovasculare. (6, 7)
Mteloproteinazele de matrice (MMP-9), sau gelatinaza B secretată de macrofage sau alte celule de inflamaţie sunt crecute la pacienţii cu angină instabilă, constituind după Blankenberg un predictor sumbru în bolile cardiovasculare. (8)
Citokinele proinflamatorii ca: proteina C reactivă, citokinele (interleukina 18, si 6 ) selectina E, moleculele de adeziune intercelulare -1 constituie factori procoagulanţi. (9, 10, 11, 12, 13, 14, 15)
Deşi sunt încă păreri diferite, statusul hipercoagulabil constituie un risc crescut de declanşare a aterosclerozei.
Endoteliul rămâne o mare enigmă, este ascuns şi . necunoscut. Atât plachetele cât şi endoteliul au aceeaşi origine,
măduva osoasă, ceea ce le conferă proprietăţi fiziologice asemănătoare. (16, 17)
Afecţiunea imună care se caracterizează prin tromboze arteriale şi/sau venoase este sindromul anticorpi antifosfolipidic. Pacienţii cu această afecţiune au în 10% cazuri ateroscleroză prematură în absenţa altor factori. (18)
Fosfatidiletanolamina împreună cu molecule de kininogen cu greutate moleculară joasă şi anticorpii anti –fosfatidilinositol sunt cofactori în declanşarea proceselor
aterogenetice. (Steven J. Kittner, Personal Communication, April 1998).
Prezenţa unor titruri înalte ale anticorpilor antifosfatidilinositol la pacienţii tineri cu atacuri ischemice tranzitorii sugerează implicarea acestora în declanşarea modificărilor aterosclerozice.
Implicarea imunologică a anticorpilor antifosfolipidici în declanşarea proceselor aterogenetice şi implicit în declanşarea
22
2 International Congressof Anti-Aging Medicine
nd
and/or venous thrombosis is the antiphospholipid antibodies syndrome. The patients with this disease have in 10% of the cases premature atherosclerosis in the absence of other factors. (18)
The phosphatidilatanolamine together with molecules of kininogen with low molecular weight and the anti-phosphatidilinositol antibodies are cofactors in the unleashing of
the atherogenetic processes. (Steven J. Kittner, personalcommunication, April 1998).
The presence of high titers of anti- phosphatidilinositol antibodies at young patients with transient strokes suggests their involvement in the unleashing of the atherosclerotic changes.
The immunological involvement of the antiphospholipid antibodies in the unleashing of the atherogenetic processes and subsequently in the unleashing of the cardiovascular diseases is proven in multiple studies. Patients with antiphospholipid antibodies syndrome have and increased level of antibodies of oxLDL. This is associated with the progression of atherosclerosis and risk of thrombo-occlusive events. OxLDL seems to be an immunogenetic molecule which stimulates the induction of anti-oxLDL antibodies.
In antiphospholipid antibodies syndrome an interaction between IgG antibodies anti-beta2 glycoprotein I and the complex beta 2 glycoprotein I takes place, which determines the change of ox LDL at the level of macrophages. Ox LDL aggravates the clinical manifestation of antiphospholipid antibodies syndrome through the acceleration of atherosclerosis in this syndrome. (19, 20, 21).
The accumulation of ox LDL in the wall of the vessels simulates the endothelial cells to produce numerous proinflammatory molecules, which include molecules of adherence, especially intercellular molecules of adherence-1, molecules of vascular cellular adherence-1 and endothelial selectin (E-selectin). These constitute some stimulating factors for colonies of macrophages and seem to contribute to the stimulation of leucocytes. A vast number of T cells, present in the
+ +memory of CD4 CD45RO cells, (a large proportion of HDL-DR% expression and the important activation of the antigen -+1) are significant for atherosclerotic lesions. The presence of these cells in the atherosclerotic plaque is the result of the direct answer to the accumulation of oxLDL in the artery wall. The high concentration of oxLDL in the wall of the vessel is recognized and phagocytated by macrophages and contributes to the cascade of events characterized through immune-inflammatory reactions of atherosclerosis.
OxLDL stimulates the production of auto-antibodies of B cells. The titers of anti oxLDL antibodies are individual. In order for the antibodies to protect or neutralize pathogens and immunogens, the humoral immunity of oxLDL can reduce the incidence of atherosclerosis. The protective role of antibodies dependant on T cell is demonstrated by immunization with oxLDL. The transfer of B cell for apolipoprotein E seems to be protective for the development of this disease. The interleukin-10 plays a crucial role in the anti-ox LDL pathogeny, because the deficit of IL-10 determines the progression of the disease. The intravenous therapy with IGIV induces the adjustment of IL-10 and the protection for atherosclerosis.
The monoclonal antibodies IgM anti oxLDL derived from apo-E blocks in macrophages the CD36 and SR-B1
proceselor aterogenetice şi implicit în declanşarea bolilor cardio-vasculare este demonstrat prin multiple studii. Pacienţii cu sindrom anticorpi antifosfolipidic au nivel crescut de anticorpi al oxLDL.
Acesta este asociat cu progresia aterosclerozei şi risc de evenimente trombo-ocluzive. OxiLDL pare a fi o moleculă imunogenetică care stimulează inducerea de anticorpi anti-oxLDL.
În sindrom, anticorpii cu antifosfolipid se produc ca interacţiune dintre anticorpii IgG anti beta2 glicoproteina I şi complexul beta 2 glicoproteina I care determină schimbarea ox LDL la nivelul macrofagelor. Ox LDL agravează manifestările clinice ale sindromului anticorpi antifosfolipid prin accelerarea aterosclerozei în acest sindrom. (19, 20, 21)
Acumularea ox LDL în peretele vaselor stimulează celulele endoteliale la producerea a numeroase molecule proinflamatorii, ce includ moleculele de adeziune, îndeosebi moleculele de adeziune intercelulare –1, moleculele de adeziune celulare vasculare-1 şi selectina endotelială (E-selectina). Aceştia constituie factori stimulatori ai coloniilor de macrofage şi par a contribui la stimularea leucocitelor. Un vast număr de celule T,
+ +prezente în memoria celulelor CD4 CD45RO , (o largă proporţie a expresiei a HDL-DR şi activarea importantă a antigenului -+1) sunt semnificative pentru leziunile aterosclerotice. Prezenţa acestor celule în placa aterosclerotică este rezultatul raspunsului direct la acumularea oxLDL în peretele arterial. Înalta concentrare a oxLDL în peretele vasului este recunoscută şi fagocitată de macrofage , contribuie la cascada evenimentelor caracterizate prin reacţii imunoinflamatorii a aterosclerozei.
OxLDL stimulează producţia de autoanticorpi ai celulelor B. Titrurile anticorpilor anti oxLDL sunt individuale.
Pentru că anticorpii pot proteja sau neutraliza patogene şi imunogene, imunitatea umorală a oxLDL poate reduce incidenţa aterosclerozei. Rolul protectiv al anticorpilor dependent de celula T este demonstrat prin imunizare cu oxLDL. Reducerea aterosclerozei este corelată cu nivelul IgG anticorpi anti oxLDL.
Transferul celulei B pentru apolipoproteina E pare a fi protectoare pentru dezvoltarea acestei boli. Interleukina –10 joacă rol crucial în patogenia anti-ox LDL, pentru că deficitul de IL-10 determină progresia bolii. Terapia intravenoasă cu IGIV induce reglarea IL-10 şi protecţia pentru ateroscleroză.
Anticorpii monoclonali IgM anti oxLDL derivaţi din apo-E blochează în macrofage receptorii CD36 si SR-B1 pentru legarea oxLDL determinând raspuns imun cu rol protectiv via macrofage.
Anticorpii anti-oxLDL joacă rol important în reglarea nivelului oxLDL. Aceşti anticorpi circulanţi ce recunosc ox LDL, au titrul semnificativ înalt la copii, modulează antigenul şi protejează instalarea bolilor cardio-vasculare.
Leziunile aterosclerotice conţin imunoglobuline care recunosc oxLDL. Nivelul concentraţiei anticorpilor anti-oxLDL poate fi un predictor pentru dezvoltarea aterosclerozei şi mai ales, constituie un predictor pentru ateroscleroza coronariană. Nivelul crescut al anticorpilor anti-ox LDL sunt relataţi în hipertensiunea arterială, vasculită sistemică, bolile periferice arteriale, disfuncţia de endoteliu, ateroscleroză şi bolile cardio-vasculare.
Titruri crescute ale anticorpilor antifosfolipid, ale oxLDL, ale beta 2 glicoproteina I, constituie spectrul autoanticorpilor, din sindromul anticorpi antifosfolipid, asociaţi aterosclerozei. (18)
23
2 International Congressof Anti-Aging Medicine
nd
receptors for connection of oxLDL determining an immune response with a protective role via macrophages.
The anti-oxLDL antibodies play an important role in the regulation of oxLDL level. These circulant antibodies whichrecognize ox LDL, have a high significant titer in children, modulate the antigen and protect from the installation of cardio-vascular diseases.
The atherosclerotic lesions contain immunoglobulin, which recognize oxLDL. The level of concentration of anti-oxLDL antibodies can be a predictor for the development of atherosclerosis and especially for the coronarian atherosclerosis. The increased level of anti-ox LDL antibodies is related in arterial hypertension, systemic vasculitis, disfunction of endothelium, atherosclerosis and the cardio-vascular diseases.
Increased titers of antiphospholipid antibodies, of OxLDL, of Beta 2 glycoprotein I, constitute the spectrum of autoantibodies, from the antiphospholipid antibodies syndrome, associated to atherosclerosis (18).
The increase of the level of anti ox-LDL antibodies is demonstrated in patients with auto-immune diseases such as: rheumatoid arthritis, diabetes mellitus, uremia, psoriasis, systemic lupus erythematosus, antiphospholipid antibodies syndrome, chronic periaortitis, hepatocellular carcinoma, thalassemia, preeclampsia or eclampsia.
The antibodies against cardiolipin and oxLDL are predictive for the cardiovascular diseases. These antibodies are partially recognized y some epitops and have a representative specificity. The auto-antibodies anti-cardiolipin are considered severe risk factors for the thrombotic events. (22)
The risk of the cardiovascular diseases is associated with a high substantial rate of IgG isotype of antiphospholipid antibodies.
The protein C represents an important endogen antithrombotic mechanism with direct participation to the adherecce of thrombomodulin to thrombin at the level of the endothelial cells. This adherence substantially changes the specific substrate of thrombin. Subsequently, the enzyme losses the procoagulant capacity and breaks the protein C, situated together with its receptor on the surface of the cell. Through this last mechanism, the protein C is activated. The complex formed of protein C, Protein S and the associated enzyme coagulates the Va and VIIIa factors. (19, 23-32)
The mechanisms through which the antiphospholipid antibodies interfere with protein C are:1. They inhibit the formation of thrombin2. They decrease the activation of protein C and the thrombomodulin-thrombin complex3. They inhibit the formation of protein C complex4. They inhibit the activation of protein C, directly or via cofactor protein S5. They connect to the Va and VIIIa factors protected for proteolysis by protein C
Interesting is the fact that the oxidization of phosphatidiletanolamine determines the coagulant activity through the activation of protein C. The inhibition of this process by antiphospholipid antibodies determines the stimulation of thrombin generation. Frequently, patients with antiphospholipid antibodies syndrome have a deficiency of protein S.
Creşterea nivelului anticorpilor anti ox-LDL este evidenţiată la pacienţii cu boli autoimune ca: artrita reumatoidă, diabet zaharat, uremie, psoriasis, lupus eritematos sistemic, sindrom anticorpi antifosfolipid, periaortită cronică, carcinomul hepatocelular, beta talasemia şi preeclampsia sau eclampsia.
Anticorpii împotriva cardiolipinei şi oxLDL includ malondialdehyde-modified LDL(MDA-LDL) sunt predictivi pentru
bolile cardiovasculare. Aceşti anticorpi sunt recunoscuţi parţial de unii epitopi şi au specificitate reprezentativă. Autoanticorpii anti cardiolipina sunt consideraţi factori de risc sever pentru evenimente trombotice. (22)
Riscul bolilor cardiovasculare este asociat cu rata substanţială înaltă a isotipului IgG al anticorpilor antifosfolipidici.
Proteina C reprezintă un important mecanism endogen antitrombotic prin participarea directă la aderarea trombomodulinei la trombină la nivelul celulelor endoteliale.
Această aderare modifică substratul specific al trombinei. Ulterior enzima pierde capacitatea procuagulantă, clivează proteina C care este situată împreună cu receptorul ei pe suprafaţa celulei. Prin acest ultim mecanism se activează proteina C . Complexul format din proteina C, proteina S şi enzima asociată coagulează factorul Va şi VIIIa. (19, 23-32)Mecanisme prin care anticorpii antifosfolipidici interferă cu proteina C sunt: (33)1. Inhibă formarea de trombină2. Descreşte activarea proteinei C şi complexul trombomodulină –trombină3. Inhibă ansamblarea complexului proteina C4. Inhibă activarea proteinei C, direct sau via cofactor proteina S5. Leagă la factorul Va şi VIIIa protejat pentru proteoliza de proteina C.
Interesant este că oxidarea fosfatidiletanolaminei determină activitatea coagulantă prin activarea proteinei C.
Inhibarea acestui proces de anticorpii antifosfolipidici determină stimularea generării de trombină. Frecvent pacienţii cu sindrom anticorpi antifosfolipidici au deficienţă de proteina S.
Mecanisme prin care se declanşează trombozele din sindromul anticorpi antifosfolipid sunt:- perturbări ale reglării proceselor endoteliale- perturbarea fibrinolizei- creşterea activităţii plachetare şi/sau- adeziunea trombocitelor - inhibarea activităţii antiprotrombinei- inhibarea activităţii anticoagulante ale beta 2 glicoproteinei I şi ale anexin V.
Studiile relevă rolul beta 2 glicoproteina I ca anticoagulantnatural şi efectele procoagulante ale anticorpilor antifosfolipidici, prin interacţiunea privind acţiunea proteinei C şi generarea de trombină şi creşterea activităţii factorului tisular.
Alte mecanisme propuse pentru hipercoagulabilitate, prin care anticorpii antifosfolipidici intervin fără a fi dependente de beta 2 glicoproteină I sunt: - activarea trombocitelor la aderare la endoteliu- activarea endoteliului vascular care facilitează aderarea trombocitelor şi monocitelor- producerea de anticorpi împotriva factorilor de coagulare, inclusiv protrombina, proteina C, proteina S.
Reacţia anticorpilor LDL , (aceasta este predispoziţia individuală la ateroscleroză şi infarct miocardic)
24
2 International Congressof Anti-Aging Medicine
nd
The mechanisms through which thromboses from the antiphospholipid syndrome unleashes are: - perturbations of adjustment for endothelial processes - perturbation of fibrinolysis - the increase of the platelets activity and/or - the adherence of thrombocytes - the inhibition of antiprothrombin activity- the inhibition of the anticoagulant activity of beta 2 glycoprotein I and of annexin V
The studies show the role of beta 2 glycoprotein I as natural anticoagulant and the procoagulant effects of the antiphospholipid antibodies, through the interaction regarding the action of protein C and the generation of thrombin and the increase of the tissue factor activity.
Other proposed mechanisms for hypercoagulation, through which the antiphospholipid antibodies intervene without being dependant on beta 2 glycoprotein I are:- the activation of thrombocytes to adhere to the epithelium- the activation of the vascular endothelium which facilitates the adherence of thrombocytes and monocytes- the production of antibodies against the coagulation factors, inclusively prothrombine, protein C, protein S- the reaction of LDL antibodies, (this is the individual predisposition to atherosclerosis and myocardial infarction) - the activation of the complement
The events of hypecoagulation and recurrent thrombosis can affect the extremities and virtually any systemic organ. (34)
The administration of corticosteroids is long time known in the treatment of the auto-immune diseases.
The glucocorticoids are immune-suppressors which act on lukocytes, on the gamma interferon, but also on other cytokines or of the adherence cells, inhibiting their synthesis.
The glucocorticoids produce the depletion in circulation of T cells, inhibit the growing factor of T cells.
They also produce deregulations of the lipid metabolism, with the increase of the cholesterol level and of the triglycerides. It is also produced an increase of LDL/HDL rate, with the appearance of the vascular changes.
After the administration of glucocorticoids a down regulation of the genes for glucocorticoids produces, which determines their reduction of the antiproliferative effect.
Therefore, in the last years more and more frequently is evoked the atherogenic role of the glucocorticoids. (34)
References: 1-Barger AP, Hurley R. Evaluation of the hypercoagulable state: whom to screen, how to test and treat. Postgrad Med 2000;108(4):59-66 2-Hoffmann, R., Valencia, A. A gene network for navigating the literature. Nature Genetics 36, 664 (2004) . Originally published on June 26, 2002
§ 3--Sarah Uff, Jeannine M. Clemetson , Tim Harrison, Kenneth J. Clemetson, and Jonas EmsleyJ. Biol. Chem., Vol. 277, Issue 38, 35657-35663, September 20, 2002Thromb J. 2003; 1: 4. 4-Raul Altman Published online 2003 July 17. doi: 10.1186/1477-9560-1-4. 5-Angles-Cano ; Structural basis for the pathophysiology of lipoprotein(a) in the athero-thrombotic process. Braz J Med Biol Res 1997 Nov;30(11):1271-80.6-Sasu S, LaVerda D, Qureshi N, et al. Chlamydia pneumoniae and chlamydial heat shock protein 60 stimulate proliferation of human vascular smooth muscle cells via toll-like receptor 4 and p44/p42 mitogen activated protein kinase activation. Circ Res. 2001;89:244–250. [PubMed] [Free Full Text]7-Blankenberg S, Tiret L, Bickel Ch, et al. Interleukin-18 is a strong predictor of cardiovascular death in stable and unstable angina. Circulation. 2002;106:24–30. [PubMed]8-Blankenberg S, Rupprecht HJ, Odette Poirier O, et al. Plasma Concentrations and Genetic Variation of Matrix Metalloproteinase 9 and Prognosis of Patients With Cardiovascular Disease. Circulation. 2003;107:1579–1585. [PubMed] [Free Full Text]
Activarea complementului Aceste evenimente de hipercoagulabilitate şi tromboze recurente pot afecta extremităţile şi virtual orice organ sistemic . (34)
Administrarea corticosteroizilor este de mult cunoscută în tratamentul bolilor autoimune.
Glucocorticoizii sunt imunosupresoare ce acţionează asupra leukinelor, asupra interferonului gama, dar şi asupra altor citokine sau ale celulelor de adeziune, inhibând sinteza acestora.
Glucocorticoizii produc depleţia în circulaţie a celulelor T, inhibă factorul de creştere al celulelor T. Produc de asemeni dereglări ale metabolismului lipidic, cu creşterea nivelului colesterolului şi al trigliceridelor. Se evidenţiază creşterea ratei LDL/HDL cu apariţia modificărilor vasculare. După administrarea de corticosteroizi se produce o down regulation a genelor de glucocorticoizi ceea ce determină reducerea efectului antiproliferativ pe care îl au. De aceea, în ultimii ani se evocă tot mai des rolul aterogenic al corticoizilor. (34)
9-Altman R, Rouvier J, Scazziota A, Gonzalez C. No causal association between inflammation and Chlamydia Pneumoniae in patients with chronic ischemic arterial disease. Inflammation. 2002;26:25–30. [PubMed] [Full Text] 10-Liuzzo G, Biasucci LM, Gallimore JL, et al. The pronostic value of C-reactive protein and serum amyloid A protein in severe unstable angina. N Engl J Med. 1994;331:417–424. [PubMed] [Free Full Text] 11-Biasucci LM, Vitelli A, Liuzzo G, et al. Elevated level of interleukin-6 in ustable angina. Circulation. 1996;94:874–877. [PubMed] [Free Full Text] 12-Blake GJ, Ridker PM. Novel clinical markers of vascular wall inflammation. Circulation Res. 2001;89:763–771. [PubMed] [Free Full Text] 13-Libby P, Ridker PM, Maseri A. Inflammation and Atherosclerosis. Circulation. 2002;105:1135–1143. [PubMed] [Free Full Text] 14-Wu KK, Aleksic N, Ballantyne Ch M, Ahn Ch, Juneja H, Boerwinkle E. Interaction between soluble thrombomodulin and Intercellular Adhesion Molecule-1 in predicting risk of coronary heart disease. Circulation. 2003;107:1729–1732. [PubMed] [Free Full Text] 15-Blankenberg S, Tiret L, Bickel Ch, et al. Interleukin-18 is a strong predictor of cardiovascular death in stable and unstable angina. Circulation. 2002;106:24–30. [PubMed] [Free Full Text16-Bonetti PO, Lerman LO, Lerman A. Endothelial dysfunction. A marker of atherosclerotic risk. Arterioscler Thromb Vasc Biol. 2003;23:168–175. [PubMed] [Free Full Text]17-Sela S, Shurtz-Swirski R, Awad J, Shapiro G, Nasser L, Shasha SM, Kristal B. The involvement of peripheral polymorphonuclear leukocytes in the oxidative stress and inflammation among cigarette snokers. Israel Med Ass J. 2002;4:1015–1019. [PubMed] 18-Vlachoyiannopoulos PG, Samarkos M. Peripheral vascular disease in antiphospholipid syndrome. Thromb Res. 2004;114(5-6):509-19.19-Galve-de Rochemonteix B, Kobayashi T, Rosnoblet C, et al. Interaction of anti-phospholipid antibodies with late endosomes of human endothelial cells. Arterioscler Thromb Vasc Biol. 2000;20:563–574. , [PubMed] [Free Full Text]20-Del Papa N, Guidali L, Spatola L, et al. Relationship between anti-phospholipid and anti-endothelial cell antibodies III: beta 2 glycoprotein I mediates the antibody binding to endothelial membranes and induces the expression of adhesion molecules. Clin Exp Rheumatol. 1995;13:179–185. [PubMed] 21-Rand JH. Molecular pathogenesis of the antiphospholipid syndrome. Circulation Research. 2002;90:29–37. [PubMed] [Free Full Text] 22-Georgios N Dalekos MD, , Kalliopi Zachou MD, and Christos Liaskos MD, Larisa Medical School, 22 Papakiriazi str, University of Thessaly, Larisa, 412 22, Greece. Anticardiolipin antibodies in patients with multiple sclerosis do not represent a subgroup of patients according to clinical, familial, and biological characteristics Current Rheumatology Reports 2001 3: 277-28523-VanCott EM, Laposata M. Laboratory evaluations of hypercoagulable states. Hematology/Oncology Clinics of North America. 1998 12:1141-1166.24-Huisman M, Rosendaal F. Thrombophilia. Current Opinion in Hematology. 1999;6: 291-297.25-DeStefano V, et al. Prothrombin G20210A mutant genotype is a risk factor for cerebrovascular ischemic disease in young patients. Blood. 1998;91:3562-356526-Reuner KH, et al. Prothrombin gene G20210 A transition is a risk factor for cerebral venous thrombosis. Stroke. 1998;29:1765-1769.27-Martinelli I, et al. High risk of cerebral vein thrombosis in carriers of a prothrombin gene mutation and in users of oral contraceptives. NEJM. 1998; 25: 1793-1797.28-Sakata T, et al. Analysis of 45 episodes of arterial occlusive disease in Japanese patients with congenital protein C deficiency. Thromb Research. 1999; 94: 69-78.29-Potti A, et al. Thrombophilia in ischemic stroke. West J Med. 1998;169:385-386, 1998. 30-Arkel YS, Ku DH, Gibson D, Lam X. Ischemic stroke in a young patient with protein C deficiency and prothrombin gene mutation G20210A. Blood Coagulation and Fibrinolysis. 1998; 9:757-760.31-Chaturvedi S, Dzieczkowski JS. Protein S deficiency, activated protein C resistance and sticky platelet syndrome in a young woman with bilateral strokes. Cerebrovasc Dis. 1999;9:127-130.32-Epstein FH. Homocysteine and atherothrombosis. NEJM. 1998; 338: 1042-1050.33-Hanly 1676 JAMC 24 JUIN 2003; 16834 -A Sa to , KE Sheppard , M J Fu l l e r ton , DD Sv i r i dov and JW Funder Baker Medical Research Institute, Melbourne, Australia. Annals of the New York Academy of Sciences
a936:261-275 (2001) EDUARDO ANGLÉS-CANO ,(Received for publication, July 31, 1995; and in revised form, August 11, 1995)


26
2 International Congressof Anti-Aging Medicine
nd
Dr. Panagis N. Georgiou
The ideal candidate for an abdominoplasty is a fairly young thin woman, who has had her children and has skin and abdominal wall laxity. When abdominal wall thickness is small, complication rate in abdominoplasties is low, and aesthetic results are satisfactory for the patients.
Some abdominoplasty candidates have severe lipodystrophy of the flanks (love handles), which will not be corrected surgically unless extended lateral dermolipectomies are employed, resulting in extensive scars. These patients can benefit from liposuction of the flanks together with abdominoplasty, having a contour reshaping with a standard abdominoplasty scar.
Ideally an obese patient should first have diet control or bariatric surgery for weight loss, and go on with dermolipectomies after achieving ideal body weight. This is not always possible because some obese patients are not able to lose weight with various diets, others do not want to undergo bariatric surgery or they may have undergone some (mild) form of bariatric surgery without significant results. The above patients would benefit from adding liposuction treatment in abdominoplasty. Usually the upper abdominal flap and the flanks should have fat aspiration resulting in significant contour reshaping.Purpose: The purpose of our study was to investigate the usefullness of liposuction as an adjuvant treatment in abdominoplasty, and to compare complication rates in standard abdominoplasties and those performed together with liposuction. Material and Method: During the last 7 years, 149 patients with abdominal skin and wall laxity were treated with abdominoplasty in our Dpt. Most of these patients (114) were treated with standard abdominoplasty which included abdominal flap undermining to the level of the xiphoid and ribs with umbilical preservation, rectus sheath plication, dermolipectomy of the excess part of the dissected flap and umbilical transposition. In six (6) cases with extreme obesity a dermolipectomy without undermining and rectus sheath plication was employed. Finally, during the last 4 years 29 patients were treated with liposuction together with abdominoplasty. A postoperative corset was used in all patients for 4 – 6 weeks.
Patient's wish was taken into account for ading liposuction in abdominoplasty. If abdominal wall thickness was more than 3 cm (pinch test more than 6 cm) the doctor could also advise the adjuvant procedure. Fat aspirate was 300 – 1100cc (av 600cc) for the abdomen. Wet technique was used, and liposuction of the lateral thighs, medial thighs, medial kness or breasts in male gynecomastia couls be performed simultaneously, according to patients' wishes. Liposuction did not extend the period of corset application for abdominoplasty.Results: Photographs were taken pre and postoperatively at 6 weeks in most of the cases. Abdominal wall perimeter was
Does Liposuction Improve Results or Raise ComplicationRates in Abdominoplasty
measured usually 10 cm below the umbilicus, at the point of maximal flank projection. Abdominal wall diameter was decreased in all cases. In standard abdominoplasty, dicrease was from 1 to 8 cm (av 3,5 cm), while this was significantly smaller when liposuction was added (5 to 12 cm, av 6,5 cm). Would dehissence with discharge and delayed would healing was noted in two cased of liposuction patients, and in 4 patients with standard abdominoplasty and in 1 patient with dermolipectomy of the lower abdomen without abdominal flap elevation. Drains were kept in place in average for 2,5 days for abdominoplasty patients, and this was delayed significantly when liposuction was added (5,7 days).
Contour reshaping in obese patients was significantly better in liposuction patients, as judged by both doctors and patients.Conclusion: Liposuction is a usefull tool in contour reshaping with abdominoplasty, when used cousiously. It does not add significantly in complication rate, although it needs prolonged wound drainage.

27
2 International Congressof Anti-Aging Medicine
nd
Dr. Ciomaga Georgeta
The metabolic syndrome at women after menopause include: increase of weight, changes concerning the metabolism of lipids, resistance at insulin, endothelial dysfunction, the increase of homocystein, lipoprotein-a levels, alterations of coagulation factors, the increase of triglycerides, the increase of reactive C protein.
The hyperparatiroidism is frequent at old ages. It includes manifestations like: osteoporosis, the increase of arterial function, peptic ulcer, the increase of urinary excretion. In renal insufficiency, the osteodistrophy is installing even from the beginnings, having several physiopathological mechanisms. The secondary hyperparatiroidism manifests itself through fibro-cystic osteodistrophy, osteomalacy (through perturbations of active compounds of vitamin D synthesis). In advanced phases of renal insufficiency it is produced an amplification of factors that lead to secondary hyperparatiroidism, (it exacerbates the deficiency of vitamin D andof calcium, concomitant with increase of phosphates). During dialysis there is a tendency of calcium increase at serum level. Phosphatemy at dialyzed patients remain increased, which subsequently determines hypocalcemy. The sedentary life, common at the third age amplifies even more the risk of fracture. A series of endocrine factors contributes to the gonadal dysfunction on uremy (the increase of prolactin level the increase of FSH, LH, and PTH). All these electrolytic changes in female patients of the third age, which also have renal insufficiency determine an increase of the fracture risk level.
Once with the installation of the menopause, the metabolic climax syndrome also installs, syndrome through which metabolic perturbations take place with a powerful predisposition to atherosclerosis. Defined as the X syndrome or central syndrome of obesity, it comprise: resistance to insulin, central obesity, hyperinsulism, dyslipidemy, arterial hypertension, hyperuricemia, gout and fat liver. The lack of protection from estrogens determines the appearance in time of osseous dystrophies. (1)
The osteoporosis represents the reduction of osseous tissue determining a fragile bone predisposed to fractures. The osteoporosis is considered a pediatric disease with geriatric results. The changes of the osseous mass are genetically dependant, but they also depend on hormonal changes, calcium deficiency and deficiency of vitamin D. (2, 3, 4)
Osteoporosis is most known in Caucasian women from post menopause because of the negative balance of the calcium. The concentration of the calcium is bi-dimensional adjusted.
The transport of calcium is produced in and from the plasmatic membrane of cells and intracellular organits, especially from endoplasmic reticulum, sarcoplasmic reticulum of muscular cells and mitochondria. The cytosolic ionized calcium is maintained in micromolecular concentrations. (5, 6)
Perturbations of Calcemy inWoman in Menopause with Chronic Renal Deficiency
Menopauza implică instalarea sindromului metabolic de climax, ce include: creşterea în greutate, schimbări privind metabolismul lipidelor, rezistenţa la insulină, disfuncţia endotelială, creşterea nivelului homocisteinei, a lipiproteinei a, tulburări ale factorilor de coagulare, creşterea trigliceridelor, creşterea proteinei C reactive. Hiperparatiroidismul este frecvent la vârste înaintate.
Acesta include manifestări ca: osteoporoză, creşterea tensiunii arteriale, ulcer peptic, creşterea excreţiei urinare. În insuficienţa renală se instalează, încă de la debut, osteodistrofia care are mai multe mecanisme fiziopatologice. Hiperparatiroidismul secundar se manifestă prin osteodistrofia fibrochistică, osteomalacia (prin perturbări ale sintezei compuşilor activi ai vitaminei D). În fazele avansate ale insuficienţei renale se produce o amplificare a factorilor ce conduc la hiperparatiroidism secundar, (se exacerbează deficitul de vitamina D , dar şi de calciu, concomitent cu creşterea fosfaţilor).
În timpul dializei există o tendinţă de creştere a nivelului calciului seric. Fosfatemia la bolnavii dializaţi rămâne crescută, ceea ce antrenează ulterior hipocalcemia. Viaţa sedentară, obişnuită la vârsta a treia, amplifică şi mai mult riscul de fracturi. O serie de factori endocrini contribuie la disfuncţia gonadală în uremii (creşterea nivelului prolactinei, creşterea FSH, a LH si PTH). Toate aceste modificări electrolitice la pacientele de vârsta a treia, care au şi insuficienţă renală determină o creşterea a riscului de fractură.
Odată cu instalarea menopauzei se instalează sindromul metabolic de climax prin care se produc perturbări metabolice cu predispoziţie puternică spre ateroscleroză. Definit ca sindrom X sau sindrom central de obezitate, acesta cuprinde: rezistenţa la insulină, obezitatea centrală, hiperinsulinism, dislipidemie, hipertensiunea arterială, hiperuricemie, guta şi ficatul gras. Lipsa protecţiei estrogenilor determină apariţia în timp a distrofiilor osoase.
Osteoporoza reprezintă reducerea ţesutului osos determinând os fragil predispus la fracturi. Osteoporoza este considerată boală pediatrică cu rezultate geriatrice. Modificările masei osoase sunt dependente genetic, dar şi de schimbările hormonale, deficienţa de calciu şi de vitamina D. (2, 3, 4)
Osteoporoza este mai cunoscută la femeile caucaziene din post menopauză din cauza balanţei negative a calciului
Concentaţia calciului este reglată bidirecţional. Se produce transportul calciului în şi din membrana plasmatică a celulelor şi organitelor intracelulare, mai ales în reticulul endoplasmatic, reticulul sarcoplasmic a celulelor musculare şi mitocondrie. Calciu citosolic ionizat este menţinut în concentraţii micromoleculare. (5, 6)
Reglarea metabolismului calciului şi al PO este 4
influenţată de nivelul hormonului paratiroidian, vitamina D şi calcitonina. (1, 2)
Parathormonul creşte nivelul plasmatic, creşte absorbţia calciului şi metabolizează rapid absorbţia calciului şi mobilizează
Perturbãri ale calcemiei lafemeile la menopauzã cuinsuficienþã renalã cronicã

28
2 International Congressof Anti-Aging Medicine
nd
The adjustment of the calcium metabolism and of PO4 is influenced by the level of para-thyroidian hormone, vitamin D and calcitonine. (1, 2)
The parathormone increase the plasmatic level and the absorption of calcium and metabolize rapidly the calcium absorption and mobilize calcium and PO4 for bone (resorption).
The excretion of renal calcium is correlated with the excretion of sodium and it is influenced by some factors which transport sodium in the proximal tube. Or, the parathormone changes the tubular reabsorption of calcium independent on sodium. The parathormone decreases reabsorption of PO4 and increase the loss of PO4. The parathormone increases the plasmatic level by stimulating the conversion of vitamin D. The increase of calcium absorption after long time of increase for the secretion of parathormone determines bone resorption, inhibiting the function of osteoclasts. The level of calcium and phosphor are directly influenced by the circulant level of the parathyroidian hormone and of vitamin D and extended to calcitonine. (1, 2)
The parathormone is a polypeptide hormone synthesized in prepoparathyroidian hormone. The hormone is stocked in cellular vesicles and activate via protein-like receptors on the surface of the cells. These receptors, which use cAMP, are secondary messengers at the adjustment of phosphorilation of intracellular proteins and of calcium. At the renal level, it increases the resorption of ionic calcium stimulating the activity in the distal tube. The parathormone acts on osteoblasts by adjusting the activity of regulatory osteoclast cells via prostaglandins. The parathormone determines erosions of the bone producing ionic calcium and phosphor. (1, 2)
It acts through: - direct inhibition of collagen synthesis in osteoblast- indirect stimulation of osseous osteoclast erosion- increases the syntheses of colagenases in bone erosion - increases the hydrogen ion determining an acid environment which favor the erosion of bone (1)
The kidney plays a crucial role in the balance of calcium and phosphor. The phosphor regulates the level of calcium in the bone. The postmenopause and the age determine a great risk for loss of bone substance (8)
The vitamin E, which is intestinally absorbed, synthesized with the help of ultraviolet rays, maintains the level of calcium and phosphates through action in intestines. It is transported by specific protein or chilomicrons, being soluble in fat. It acts through specific receptors and has some locations on parathormone receptors. It is implicated in the regulation of calcium.
At renal level, vitamin D determines:- increase of calcium reabsorption in the proximal and distal tube- increase of phosphate reabsorption in the proximal tube- inhibition of 1 alpha hydroxilazes, this being the negative feedback- direct stimulation of osteoblasts activity and increase of the osseous mass and calcification.
Disorders of its absorption determine osteodistrophy in renal insufficiency. (1, 9)
At the level of intestines (duodena and jejun), the
calciu şi PO4 pentru os (resorbţie). Excreţia calciului renal este corelată cu excreţia de sodiu şi influenţată de unii factori ce transportă sodiu în tubul proximal. Or, parathormonul schimbă reabsorbţia tubulară a calciului independent de sodiu.
Parathormonul descreşte reabsorbţia PO şi creşte 4
pierderea PO Parathormonul creşte nivelul plasmatic stimulând 4.
conversia vitaminei D. Creşterea absorbţiei de calciu după lung timp de creştere a secreţiei de parathormon determină resorbţia osoasă, inhibând funcţia osteoclastelor. Nivelul calciului şi fosforului sunt direct influenţate de nivelul circulant al hormonului paratiroidian şi de vitamina D, şi extins la calcitonină. (1,2)
Parathormonul este un hormon polipeptid sintetizat în hormonul prepoparatiroidian. Hormonul este stocat în vezicule celulare şi activează via protein-like receptori pe suprafaţa celulelor. Aceşti receptori ce utilizează cAMP, sunt mesageri secundari la reglarea fosforilării a proteinelor intracelulare şi al calciului. La nivel renal creşte resorbţia calciului ionic stimulând activitatea în tubul distal. Parathormonul acţionează pe osteoblaste, reglează activitatea celulelor reglatoare de osteoclaste via prostaglandine. Parathormonul determină eroziuni ale osului realizând calciu şi fosfor ionic. (1,2)
Acţionează prin:- inhibarea directă a sintezei colagenului în osteoblast - indirect stimulează eroziunea osteoclastului osos- creşte sinteza colagenazei în erodarea osului- creşte ionul hidrogen determinând mediul acid ce favorizează eroziunea osului. (1,2)
Rinichiul joacă rol crucial în balanţa calciului şi fosforului. Fosforul reglează nivelul calciului în os. Postmenopauza
şi vârsta detemină un mare risc de pierdere a substanţei osoase. (8)Vitamina E ce este absorbită intestinal, sintetizată cu
ajutorul razelor ultraviolete, menţine nivelul calciului şi fosfonaţi prin acţiune pe intestine. Este transportată pe proteine specifice sau chilomicroni, fiind solubilă în grasime. Acţionează prin receptori specifici şi are unele locaţii pe receptorii parathormonului. Este implicată în reglarea calciului.
La nivel renal, vitamina D determină:- creşterea reabsorbţiei calciului în tubul proximal şi distal - creşterea reabsorbţiei de fosfaţi în tubul proximal - inhibă activitatea 1 alfa hidroxilazei, aceasta fiind feedbackul negativ. - stimulează direct activitatea osteoblastelor şi creşte masa osoasă şi calcificarea.
Dezordini ale absorbţiei ei determină în insuficienţa reanală osteodistrofia. (1,9)
La nivelul instinelor (duoden şi jejun) meţinerea acţiunii vitaminei D este stimulată de absorbţia de calciu şi fosfaţi. Nu se cunoaşte mecanismul, dar determină creşterea sintezei de calciu legat de proteine în celulele intestinale.
Calcitonina este secretată de celulele parafoliculare din glanda tiroidă, ca răspuns la nivelul calciului sanguin. Calcitonina este un hormon polipeptid, este stocat în veziculele secretorii şi acţionează pe G proteina cuplând receptorii care eliberează cAMP favorizând efectul celular. (9)

29
2 International Congressof Anti-Aging Medicine
nd
maintenance of vitamin D actions is stimulated by the absorption of calcium and phosphates. The mechanism is not known, but it determines the increase of calcium synthesis bounded by proteins in intestinal cells.
The calcitonine is secreted by parafolicular cells from the thyroid gland, as a response to the level of sanguine calcium.
The calcitonine is a polypeptide hormone, it is stocked in the secretor vesicles and it acts o G protein cy coupling the receptors which release cAMP, favoring the cellular effect. (9)
At the renal level, it inhibits the resorption of calcium and of phosphate.
The calcitonine acts mainly on the osteoclasts from the bone.its inhibition determines all stages of cellular destruction. But, it is not necessary for regulating calcium and there are no consequences for the deficiency of calcitonine.
The parathormone remains the most important in calcium homeostasis.
In chronic renal insufficiency, hypocalcaemia is secondary to hyperparatiroidism. (10)
In prolonged hypocalcaemia the stimulation of parathormone secretion produces through parathyroid gland hyperplasia.
In renal insufficiency a deficit of calcium reabsorption produces. It results renal osteodistrophy which can determine deficit of I alpha hidroxylazes activity. (10, 11)
The symptoms are those of muscular constrictions, demineralization of bone with fractures.
The tubular renal diseases, inclusive renal proximal tubular acidosis determine nephrotoxicity through which severe hypocalcaemia produces which leads to the abnormal renal losses (1, 12)
People with chronic moderate renal insufficiency can have reduction of bone density as a result of acido-basic abnormalities and those of vitamin D-parathormone homeostasis.
In the final stages of the chronic renal diseases, the dialysis reduce the osseous mineral density which determines an increased risk for development of osteopenia with a relatively high risk for fractures.
The chronic mineral acidosis determines the dissolution of the osseous structure.
The osteopenia is directly correlated with the degree of renal insufficiency, sex and age, and at women in menopause the predisposing factors sums each other. (13)In the final stage of renal insufficiency with dialysis the risk factors for development of the mineral metabolism disorders and renal osteo-dystrophia are recognized.
The disorders are determined by the increased secretion of parathyroid and the decrease of calcitriole synthesis.
The osteopenia is an increased risk factor and a great complication in renal disease.
Factors that influence the bone density and the mineral metabolism in insufficiency are: steroids, the duration of dialysis, age, hyperparathyroidism. The rate of bone turnover is directly correlated with the increased secretion of parathormone.
The bone mineral density at the transplanted kidney is reduced (reshaping, forming and resorbtion). The increase of the calcitonine level is produced. There is a correlation between
La nivel renal inhibă resorbţia calciului şi fosfatului. Calcitonina acţionează în principal pe osteoclastele din
os. Inhibarea acesteia determină toate stadiile de distrugere celulară.
Dar, nu este necesară pentru reglarea calciului şi nu sunt consecinţe pentru deficienţa calcitoninei.
Parathormonul rămâne cel mai important în homeostazia calciului.
În insuficienţa renală cronică hipocalcemia este secundară hiperparatiroidismului. (10)
În hipocalcemia prelungită se produce stimularea secreţiei parathormonului prin hiperplazia glandei paratiroide.
În insuficienţa renală se produce deficit de reabsorbţie de calciu. Rezultă osteodistrofie renală care poate detemina deficit de activitate a1 alfa hidroxilazei. (10,11)
Simptomele sunt de senzaţie de constricţii musculare, demineralizarea osului cu fracturi.
Bolile tubulare renale, inclusiv acidoza tubulară renală proximală, determină nefrotoxicitate prin care se produce hipocalcemia severă ce duce la pierderi renale anormale. (1, 12)
Persoane cu insuficenţă renală cronică moderată pot avea reducerea densităţii osoase ca rezultat al anomaliilor acido-bazice şi al homeostaziei vitaminei D-parathormon.
În stadiile finale ale bolii renale cronice, dializa reduce densitatea minerală osoasă care determină un risc crescut de dezvoltare a osteopeniei cu risc relativ crescut de fracturi.
Acidoza minerală cronică detemină disoluţia structurii osoase. Osteopenia este direct corelată cu gradul de insuficienţă
30
2 International Congressof Anti-Aging Medicine
nd
parathormone and biochemical markers of the bone formation and resorption. (14)
The administration of bicarbonate, inpatients at menopause, ameliorates the calcium deficit and corrects the calcium-phosphor balance, reduce the bone resorption. Patienst with moderate insufficiency have a decreased level of 1,25 (OH)2 vitamin D and an increased level of parathormone. (15, 16, 17)
The decreased level of 1,25(OH)2 is a risk factor independant on the risk for fractures. (18)
The reduction of the renal function is an independent factor for the reduction of bone density. (19)
Although it is suggested that the renal insufficiency is an independent risk factor, studies shows that their installing in women from menopause determines the acceleration of bone density diminution. (1, 20, 21, 22)
The reduction of parathormone glamds in adapting the changes of ionized calcium is pronounced in haemo-dialysed patients. The cause is the result of parathyroid gland sensitivity reduction at ionized calcium correlated with the fact that the reduction of calcium receptors from the parothydian surface cells is noticed in uremia. (23, 24)
The calciphylaxy is a phenomena whose etiology is unknown, but it is observed in patients in the final stages of renal insufficiency as a result of hyperparathyroidism associated with changes of calcium metabolism. (25)
The calciphylaxy is the disorder determined by systemic and cutaneous calcifications and fibrosis in the lumen of small and medium vessels, as a result of hyperparathyroidism. (26) It is estimated that 1% of the patients with renal insufficiency. The micrivascular calcifications, the occlusion and the thrombosis determine violaceous lesions with progression of ulcers and sepsis. Patients have abnormalities of calcium/phosphate axis, the increase of parathomone level, but the mechanisms of calciphylaxy are not yet known. (27) The important complication determined by calciphylaxy n chronic renal insufficiency is the cutaneous necrosis with microvascular calcifications. (28)
Patients with renal transplant have a low bone density associated with the increase of parathormone, osteocalcine and procolagene. It is an inverse, negative relationship, between the duration of dialysis, osteopenia and osteoporosis at transplanted patients. The reduction of bone density is associated with bone reshaping mediated by hypersecretion of parathormone. (29)
The administration of estrogens in the advanced stage of renal insufficiency is not indicated because it determines the increase of thrombosis in dialysis and increase the risk of cardiovascular diseases. In postmenopausal and steroid induced osteoporosis associated with chronic renal insufficiency the treatment with biphophates, calcitonine, calcium, vitamin D are recommended.
Conclusions:Perturbations of equilibrium and metabolism of calcium are frequent both in postmenopause and in chronic renal insufficiency.
The installation of the climax syndrome through deficit of estrogens determines the installation of perturbations of absorption and metabolism of calcium but also of bone
renală, sex şi vârstă, iar la femeile în menopauză, factorii predispozanţi se însumează. (13)
În stadiul final al insuficienţei renale cu dializă sunt recunoscuţi factorii de risc ai dezvoltării dezordinelor metabolismului mineral şi osteodistrofia renală.
Dezordinile sunt determinate de secreţia crescută a paratiroidei şi descreşterea sintezei de calcitriol. Osteopenia este un factor de risc crescut şi o mare complicaţie în boala renală.
Factorii ce influenţează densitatea osoasă şi metabolismul mineral în insuficienţă sunt: steroizii, durata dializei, vârsta, hiperparatiroidismul. Rata turnoverului osos este direct corelată cu secreţia crescută de parathormon. Densitatea minerală osoasă la rinichiul transplantat este redusă (remodelarea, formarea şi resorbţia). Se produce creşterea nivelului osteocalcinei. Este corelaţie dintre parathormon şi markerii biochimici ai formării osului şi resorbţie. (14)
Administrarea de bicarbonat, la pacientele la menopauză, ameliorează deficitul de calciu şi corectează balanţa calciu–fosfor, reduce resorbţia osului. Pacientele cu insuficienţă renală moderată au nivelul scăzut al 1,25 (OH) vitamina D şi 2
nivelul crescut al parathormonului. (15, 16, 17 )Nivelul scăzut al vitaminei D 1,25(OH) este un factor de 2
risc independent pentru riscul de fracturi. (18)Reducerea funcţiei renale este un factor independent
pentru reducerea densităţii osoase. (19)Deşi se sugera că insuficienţa renală este un factor de
risc independent, studiile arată că instalarea acesteia la femeile din menopauză determină accelerarea diminuării densităţii osoase 1. (20,21, 22)
Reducerea capacităţii glandelor parathormonului în adaptarea schimbărilor calciului ionizat este pronunţată la pacienţii hemodializaţi.
Cauza este rezultatul reducerii sensitivităţii glandelor paratiroide la calciu ionizat corelat cu faptul că se observă reducerea densităţii receptorilor de calciu a celulelor de suprafaţă paratiroidiene în uremia. ( 23, 24)
Calcifilaxia este un fenomen a cărei etiologie este necunoscută, dar este observată la pacienţii în stadiile finale ale insuficienţei renale ca rezultat al hiperparatiroidsmului asociată cu modificări ale metabolismului calciului. (25)
Calcifilaxia este dezordinea determinată de calcificări şi fibroze în lumenul vaselor mici şi medii, sistemice şi cutanate ca rezultat al hiperparatiroidismului. (26). Este estimată la 1% dintre pacienţii cu insuficienţă renală. Calcificările microvasculare, ocluzia şi tromboza determină leziuni violacee, cu progresia ulcerelor şi sepsisului.
Pacienţii au anomalii ale axei calciului/fosfat, creşterea nivelului parathormonului, dar mecanismele calcifilaxiei nu sunt încă cunoscute. (27)
Complicaţia importantă determinată de calcifilaxie în insuficienţa renală cronică este necroza cutanată cu calcificări microvasculare. (28)
Pacienţii cu transplant renal au densitatea osoasă redusă asociată cu creşterea parathormon, osteocalcin şi procolagen.
Este o relaţie inversă, negativă, între durata dializei,
31
2 International Congressof Anti-Aging Medicine
nd
density destruction. The association at climax of chronic renal insufficiency
determines even more severe perturbations of bone density with increased risk for fractures.
The dialysis accentuates this calcium deficit. It is noticed, in a small proportion, the presence of calciphylaxy, perturbation which consist in calcium deposition not at osseous level, but at the level of small, systemic and cutaneous vessels. The administration of estrogens for the correcting of the calcium balance is contraindicated because it increase the risk of cardiovascular diseases through the increase of thrombosis risk.
Bibliography:1 Disorders of Calcium Regulation 95 Clinical Nephrology – Epidemiology – Clinical Trials Kidney International (2002) 61, 1814–1820 doi:10.1046/j.1523-1755.2002.00306.x
2 Scientific Review 3rd Edition, Apr 03, 9-19 Scientific Review 3rd Edition, Apr 03, 9-19
3 Bendich A et al, Supplemental calcium for the prevention of hip fracture: potential health-economic benefits, Clin Ther 1999;21(6):1058-72
4 Reid IR et al, The roles of calcium and vitamin D in the prevention of osteoporosis, Endocrinol Metab Clin North Am 1998;27(2):389-98
5 Riggs BL et al, Long-term effects of calcium supplementation on serum parathyroid hormone level, bone turnover, and bone loss in elderly women, J Bone Miner Res 1998;13(2):168-74
6 Cumming RG et al, Calcium for prevention of osteoporotic fractures in postmenopausal women, J Bone Miner Res 1997;12(9):1321-9
7 Devine A et al, A 4-year follow-up study of the effects of calcium supplementation on bone density in elderly postmenopausal women, Osteoporos Int 1997;7(1):23-8
8 Claus P. Schmitt and Franz Schaefer Calcium sensitivity of the parathyroid in renal failure: another look with new methodology Nephrol Dial Transplant (1999) 14: 2815-2818
9 Last full review/revision November 2005 Disorders of Calcium Concentration
10 Hsu CY & Chertow GM. Chronic renal confusion: Insufficiency, failure, dysfunction, or disease. Am J Kidney Dis 2000; 36: 415–418. | PubMed | ISI | ChemPort |
11 Alem AM, Sherrard DJ & Gillen DL et al. Increased risk of hip fracture among patients with end-stage renal disease. Kidney Int 2000; 58: 396–399. | Article | PubMed | ISI | ChemPort
12 Chi-Yuan Hsu, Steven R Cummings, Charles E Mcculloch and Glenn M ChertowBone mineral density is not diminished by mild to moderate chronic renal insufficiency Received 26 September 2001; Revised 4 December 2001; Accepted 5 December 2001. Bone mineral density is not diminished by mild to moderate chronic renal insufficiency
13 Claus P. Schmitt and Franz Schaefer Calcium sensitivity of the parathyroid in renal failure: another look with new methodology
14 Kušec et al: Bone Metabolism after Kidney Transplantation Croat Med J 2000;41:396-400
15 Frassetto LA, Morris RC, Jr & Sebastian A. Effect of age on blood acid-base composition in adult humans: Role of age-related renal functional decline. Am J Physiol 1996; 271: F1114–F1122. | PubMed | ISI | ChemPort
16 Lemann J, Jr, Litzow JR & Lennon EJ. The effects of chronic acid loads in normal man: Further evidence for the participation of bone mineral in the defense against chronic metabolic acidosis. J Clin Invest 1966; 45: 1608–1614. | PubMed | ISI | ChemPort
17 Sebastian A, Harris ST & Ottaway JH et al. Improved mineral balance and skeletal metabolism in postmenopausal women treated with potassium bicarbonate. N Engl J Med 1994; 330: 1776–1781. | Article | PubMed | ISI | ChemPort |
18 Cummings SR, Browner WS & Bauer D et al. Endogenous hormones and the risk of hip and vertebral fractures among older women. N Engl J Med 1998; 339: 733–738. | Article | PubMed | ISI | ChemPort |
19 Jones CA, McQuillan GM & Kusek JW et al. Serum creatinine levels in the US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis 1998; 32:
osteopenia şi osteoporoza la pacienţi transplantaţi. Reducerea densităţii osoase este asociată cu remodelarea osoasă mediată de hipersecreţia de parathormon. (29 )
Administrarea de estrogeni în stadiul avansat al insuficienţei renale cu dializă nu este indicată pentru că determină creşterea trombozelor în dializă şi creşte riscul de boli cardiovasculare.
În osteoporoză, postmenopauză şi steroid indusă asociată cu insuficienţă renală cronică se recomandă tratament cu bifosfonaţi, calcitonină calciu, vitamia D.
Concluzii:
Perturbări ale echilibrului şi metabolismului calciului sunt frecvente atât în postmenopauză cât şi insuficienţă renală cronică.
Instalarea sindromului de climax prin deficit de estrogeni determină instalarea unor perturbări ale absorbţiei, metabolizării calciului dar şi al distrugerii densităţii osoase.
Asocierea la climax a insuficienţei renale cronice determină perturbări şi mai severe ale densităţii osoase, cu risc crescut de fracturi.
Dializa accentuează acest deficit de calciu. Se constată, într-o proporţie mică a calcifilaxiei, perturbare ce constă în depozitarea calciului nu la nivel osos ci la nivelul vaselor mici, sistemice şi cutanate.
Administrarea de estrogeni pentru corectarea balanţei calciului este contraindicată deoarece creşte riscul de boli cardiovasculare prin creşterea riscului de tromboză.
20 Hsu CY, Bates DW, Kuperman GJ & Curhan GC. Relationship between hematocrit and renal function in men and women. Kidney Int 2001; 59: 725–731. | Article | PubMed | ISI | ChemPort |
21 Hsu CY, McCulloch CE & Curhan GC. Epidemiology of anemia associated with chronic renal insufficiency among adults in the Unites States: Results from NHANES III.J Am Soc Nephrol 2002; 13: 504–510. | PubMed | ISI |
22 Chi-Yuan Hsu, Steven R Cummings, Charles E Mcculloch and Glenn M ChertowBone mineral density is not diminished by mild to moderate chronic renal insufficiencyReceived 26 September 2001; Revised 4 December 2001; Accepted 5 December 2001
23 Gogusev J, Duchambon P, Hory B et al. Depressed expression of calcium receptor in parathyroid gland tissue of patients with hyperparathyroidism. Kidney Int 1997; 51: 328–336[ISI][Medline]
24 Snyder RJ, Beylin M, Weiss SD. J Nephrol 2002 May-Jun;15(3):324-9Painful cutaneous lesions, renal failure and urgent parathyroidectomy
25 Younis N, Sells RA, Desmond A, Helliwell T, Guerin D, Jibani M, Vora J Q J Med 1991 May;79(289):443-50Proximal cutaneous necrosis associated with small vessel calcification in renal failure.
26 Budisavljevic MN, Cheek D, Ploth DW. Ostomy Wound Manage 2000 Oct; 46(10):40-7Calciphylaxis and its relation to end-stage renal disease: a literature review and case presentation.
27 Ross CN, Cassidy MJ, Thompson M, Russell Jones R, Rees AJ Nephrol Nurs J 2002 Oct;29(5):433-8, 443-4; quiz 445-6Calciphylaxis: what nurses need to know
28 Bliss DE Clin Nephrol 1998 Oct;50(4):258-61Uremic small artery disease: calciphylaxis with penis involvement.
29 Mattix H Singh AK Curr Opin Nephrol Hypertens. 2000 May;9(3):207-14

32
2 International Congressof Anti-Aging Medicine
nd
Dr. Olga Djamo
Recent scientific evidence shows that nearly every biological marker of aging is profoundly influenced by excess insulin and its effect on other hormonal systems. Therefore reducing excess insulin becomes a critical factor in any anti-aging program. In fact, all of the markers of aging may be thought of as a growing degree of hormonal miscommunication, facilitated by excess insulin as we age.
Slowing the aging process stems from improved hormonal control. Improved hormonal control is itself primarily determined by the dietary choices we make. We can expect a twenty-year difference between our actual age and our true biological age. Reversing aging is not about living forever but about 'living better longer'. In addition to eating correctly, moderate exercise, detoxifying the body and stress reduction all effect the overall hormonal control. Certain longevity treatments when added to the basic wellness program can have a powerful synergistic effect on health and well-being.
Aging is the general deterioration of the body over time. Age is inevitable, but aging is not. Ninety percent of all adult illness is due to the degenerative process of aging. With early detection and appropriate intervention, most of these diseases can be prevented, cured, or have their downward course reversed.
Procaine ( GH3 and KH3 ) is the first drug suggested for use in reversing aging in modern times.
Romanian physician Dr. Anna Aslan suggested in 1956 that procaine could be used to combat arthritis, arteriosclerosis, senile skin changes and baldness. Procaine containing benzoic acid has been shown to markedly improve the absorption of procaine by fats, thus quickening its absorption by the human body. Procaine also increases the speed with which the nerves conduct impulses, and decreases the rate of excretion of the 17 kerosteroids, which usually increases with age.
Age-related changes do not occur uniformly in individuals; rather, they are controlled by genetic and environmental factors.
Several lifestyle practices have been linked to disease processes that curtail longevity. Smoking, excessive alcohol consumption, illegal drug use, reckless driving, exposure to environmental and occupational pollutants hasten the demise of many people who would otherwise reach an advanced age. Proper diet and nutrition are fundamental to living a long and healthy life. Processed foods containing transfatty acids, refined sugars, and saturated fat are to be avoided, while unprocessed foods such as fruits, vegetables, and lean meat are important in providing essential nutrients and antioxidants.
Excess body fat, commonly determined by the body mass index (BMI), is associated with greater mortality and morbidity. The incidence of obesity (BMI greater than 30) has
Anti-Aging Medicine - A FaisableMedicine
rapidly increased in the last 10 years, while diseases such as diabetes, stroke and cardiac disease have grown as well. Anti-aging physicians stress the need to maintain a body weight close to the ideal.
A similar concept that interests anti-aging physicians is the practice of calorie restriction. Long advocated by UCLA School of Medicine professor Roy Walford, M.D., one of the world's foremost experts on aging, this concept suggests that by reducing calories by 10% or more human life span can be substantially increased. Various groups practice this concept called CRAN (Calorie Restriction with Adequate Nutrition). CRAN has been shown to dramatically extend the lives of laboratory animals. Rats, mice and hamsters experience significant life span extension from a diet containing 35% of the calories, but all of the required nutrients.
Mean life span was increased 65% and maximum life span was increased by 50% when CRAN is begun just before puberty. The exact mechanism by which caloric restriction has such dramatic effects is still unknown. Probably the most controversial anti-aging therapy is called multi-hormone optimization. This practice is based on the Neuroendocrine theory of aging. Developed by Valdimir Dilman, Ph.D., this theory notes that when we are young hormone levels tend to be high and decline as we mature, usually after age thirty. Hormones are vital for repairing and regulating our bodily functions. This age-related decrease in the production of key hormones such as DHEA, melatonin, testosterone, thyroid and human growth hormone (HGH) is associated with a decline in the body's ability to repair and regulate itself. In addition, catabolic hormones such as cortisol, insulin and estrogen (in men) increase as we age.
Overall, these multiple hormonal changes result in fat gain, loss of muscle mass (sarcopenia), fatigue, insulin resistance, cardiovascular disease, mental decline, poor immune response, and sense of poor health.
With the advent of anti-aging medicine, hormone replacement therapy now becomes a choice to being made jointly by the informed patient and the knowledgeable physician, one in which the potential for unknown health consequences are weighed against the known benefits. Exercise is also extremely important. It not only increases muscle mass and endurance, but exercise has also been shown to reduce serious falls in the elderly. While most traditional physicians stress the need for aerobic exercise such as walking, swimming and jogging, anti-aging physicians are more aggressive and typically recommend a combination of aerobic exercise and resistance training. Numerous studies have confirmed that resistance training increases or maintains muscle mass. At a minimum, resistance training helps to slow the rate of decline in strength and muscle mass.
Twenty to thirty minutes three or four times a week of aerobic exercise plus a couple sessions a week of weight training is adequate.
Many of the effects of aging are believed to be due to damage caused by free radicals. Although pollutants make the problem worse, free radicals are always present in the body-they

33
2 International Congressof Anti-Aging Medicine
nd
are an unavoidable result of the chemical reactions that sustain life. Our body uses antioxidants to defend itself against their depredations. There is still controversy in the scientific community as to whether a balanced diet provides all the antioxidants and other nutrients essential to optimal health.
Not every scientist believes that supplementation is necessary. In my opinion we should all be taking a good vitamin and mineral supplement. Not only do most people not eat the recommended five servings of fruit and vegetables daily, but the produce we do eat usually has been picked green, possibly grown on mineral-depleted soils, and may be contaminated with pesticides or other pollutants.
The various formulas contain optimal amounts of vitamins, trace minerals, antioxidants and phytonutrients, as well as sufficient calcium and other nutrients necessary to promote bone health.
Conclusion:The attitudes are gradually changing as evidence accumulates strongly suggesting that significant anti-aging medicine is indeed
feasible, and that the most important effect of such medicine would be improvement in our ability to treat age-related diseases.
References: 1. Blackman MR, Sorkin JD, Munzer T, et al. Growth hormone and sex steroid administration in healthy aged women and men: a randomized controlled trial. JAMA 2002;288:2282-2292.
2. Goldsmith, T. The Evolution of Aging, ISBN 0-595-28069-2, 2003
3. Goldsmith, Theodore. C. Aging as an Evolved Characteristic – Weismann's Theory Reconsidered Medical Hypotheses 2004 62-2 304:308 DOI: 10.1016 S0306-9877(03) 00337-2.
4. Kimura KK, Tissenbaum HA, Liu Y, Ruvkun G. daf-2, an insulin receptor-like gene that regulates longevity and diapause in Caenorhabditis elegans. Science 1997; 277: 942.
5. Lane, M. A. The Serious Search for an Anti-Aging Pill, Scientific American Aug 2002
6. Mitteldorf, Joshua. Chaotic population dynamics and the evolution of aging, Evolutionary Ecology Research, 2006, 8: 561–5
7. Rudman D, Feller AG, Nagraj HS, et al. Effects of human growth hormone in men over 60 years old. N Engl J Med 1990;323:1-6. Vance ML. Growth hormone for the elderly? N Engl J Med 1990;323:52-54.

34
2 International Congressof Anti-Aging Medicine
nd
Prof. Eckart Haneke
A scar is the repair of tissue loss by the body with own tissue components, mainly connective tissue. Skin scars develop from defects reaching into the reticular dermis. They usually lack elastic fibres. All scars tend to shrink with time. The end stage of scars is reached after approximately two to four years. Keloids are defined as excessive scars that overgrow the site of original damage. They have to be differentiated from hypertrophic scars, which are exuberant wound repair processes; however, they remain confined to the site of the original skin defect.
Sometimes, a clear-cut differentiation between a hypertrophic scar and a keloid is not unequivocally possible and remains somewhat arbitrary.
Keloids and hypertrophic scars are produced by uncontrolled collagen synthesis of dermal collagen, most commonly after injury, rarely spontaneously. A scarless wound healing in mammals is only observed during the first two trimesters of pregnancy, all wounds incurred later and reaching into the reticular dermis heal with a scar.
Scars may be classified according to their aetiology and mechanism of skin wounding, by their growth characteristics, by depth or elevation, and certainly by their localisation, size and shape. Although a clinical examination is almost always sufficient, there are some more means to determine the size and consistency of a scar, such as ultrasound, (xero)radiography, histopathology and biochemistry.
A hypertrophic scar is rarely spontaneous, but usually due to a surgical wound, a burn wound, an infected wound and prolonged healing is one of the most important pathogenetic factors. For deep burns, which quite often healing with hypertrophic scars, a particular mechanism of development is evident: The hair follicles and other cutaneous appendages are completely destroyed and epidermisation of the granulation tissue cannot take place from them, but only from the surrounding skin. Until the central parts of the burn become epidermised considerable amounts of granulation tissue may have formed that later appear as a hypertrophic or even keloidal scar. The same factors that may lead to hypertrophic scars are also responsible for keloid formation. However, a strong racial and genetic influence is evident in keloids. The differential diagnosis is very varied with benign and malignant fibrohistiocytic and smooth muscle tumours, myofibroblastic neoplasms and desmoplastic melanoma being the most important. Some infections are also characteristically associated with keloidal scars such as lobomycosis or infected chronic foreign body granulomas such as in acne keloidalis.
Keloid fibroblasts were found to be less sensitive to TNF-a inhibition, to be less inhibited by corticosteroids, to contain more insulin-like growth factor 1 (IGF1) and TGF-b mRNA, to respond less to apoptotic factors and to have only a 50% rate of apoptotic cells as compared to normal skin. Fibroblasts from the centre proliferate at about double the rate.
Keloids occur in all races but are considerably more frequent in dark-skinned subjects. They have never been observed in albinos. Areas that are particularly prone to develop
Keloids keloids are the lateral face regions, ear lobes, mandibular arch, occipital regions, nape of the neck, shoulder, upper back and the presternal area (décolleté). In a person at risk, wounds under tension are more likely to become keloidal, but also dermatoses with an infectious component such as erysipelas, inflamed cysts, foreign body reactions have a much higher risk to develop a keloid.
Hormones also appear to play a role, as keloids before puberty and after menopause are quite rare.
A huge number of hypotheses exist concerning the treatment of this problematic lesion. Up to now there is no single therapy that is effective in all cases. This is reflected by the enormous variability in treatment modalities reaching from physical measures to various topical and systemic drug regimes.
Many reports are only anecdotal and most studies have not been well controlled or biased. Many physicians treat according to their “own experience”, which, scientifically spoken, is usually mere self-deception. The management of keloids and hypertrophic scars is always a protracted and staged process. It involves preparation of the skin b hygienic measures, scar softening with corticosteroids, both topical and intralesional, application of silicon gel sheets, pressure garments, and many more. In case a surgical intervention is considered a treatment plan has to be established and discussed with the patient who has to do the most important part of the treatment. Prolonged postoperative care is essential. The patient has to know that the final result will be a compromise.
For hypertrophic scars, localised pressure, silicone gel or gel sheets, liquid nitrogen, surgical planing or even excision, intralesional steroid injections, and vascular lasers have been used with variable success. However, a single measure is rarely effective and a combination of several of these procedures will certainly give better results.
Hypertrophic burn scars are often treatment with pressure garments, silicon gel and silicon gel sheets, intrascar excisions, often multiple V-Y and Z-plasties to release contractions, local, regional and microvascular flaps as well as expanded flaps, flattening of the elevated scar portions by dermabrasion of laser ablation plus keratinocyte suspensions.
Pseudohypertrophic scars develop when the skin was cut very obliquely and the acutely angled superficial portion of the skin shrinks giving rise to a rim. This may be excised and meticulously sutured or planed by dermabrasion or laser ablation.
All these measures are also recommended for true keloids. However, treatment has to be even more consistent and the patients usually require psychological support by their family and physician in order to not give up in despair.
Corticosteroids are probably the drugs the most frequently used. They have to be very potent, usually class 3 or 4, but their risk is epidermal atrophy, redness, hypopigmentation, telangiectasiae and even Cushing's syndrome upon long-term use and Hoigné's syndrome when injected near the angular vein. Used with care and experience they may help to considerably flatten the keloids.
Silicone gel sheets, but also plain silicone gel was shown to exert a marked prophylactic effect in high-risk individuals, but had no considerable effect on size, induration, colour and symptoms in another study.
Cryotherapy is one of the most traditional keloid1(one)

35
2 International Congressof Anti-Aging Medicine
nd
treatments. Though fibroblasts are relatively resistant to cold collagen I synthesis was reduced after cryotherapy. Intralesional cryotherapy offers some advantages over the spray or cryo probe method.
Radiotherapy is an “old” treatment modality for keloids. Through the last 80 years, radiation modalities have changed considerably, but radiotherapists insist on achieving good to excellent results assumedly not matched by other non-surgical methods. The most reasonable approach is the excision of the keloid and intraoperative, immediate or near-immediate
192irradiation with orthovolt or Ir brachytherapy. However, the long-term risk for cancer development is not yet fully clear.
Postoperative interferon-a2b injections reduced the recurrence rate of keloids from 51% to only 19% (p <0.025); the mechanism of action may be the increase in keloidal collagenase activity, reduction in collagen neosynthesis by keloidal fibroblasts, reduction of glycosaminoglycan synthesis and induction of fibroblast apoptosis.
Imiquimod, well known to dermatologists as a topical immune response modifier and effective for the treatment of condylomata acuminata and superficial cancerous lesions, also has an antiangiogenic action, which may be – in addition to the induction of natural interferons and interleukins – responsible for its favourable effect on keloids, both therapeutically as well as prophylactically.
Bleomycin injections have been used as an alternative to intralesional steroid injections. A few studies report favourable results, which may be due to bleomycin's induction myofibroblast apoptosis by activating caspase-3. However, in our hands the effects were not as pronounced and most patients complained of severe pain.
Another cytotoxic drug, 5-fluorouracil, was also successfully used for the treatment or prevention of keloids after excision.
Verapamil in association with silicone sheeting, topical tacrolimus, tamoxifen and bacterial collagenase were also used.
Topical mitomycin C, a cytotoxic drug developed for the topical treatment of skin metastases of mammary carcinoma, was successfully applied on the wound base after shaving keloids. It significantly inhibits fibroblast proliferation.
Surgery has for a long time been the mainstay of keloid treatment, however, in most cases, the keloid grew larger after the surgery than it was before. Various different surgical methods have therefore been developed. Intrascar keloid excision war advocated as was shelling out of certain keloids, particularly the round and hard acne keloids on the shoulders. Nevertheless, it must be stressed that surgery alone is not an option and has to be combined with other methods.
Lasers have been recommended for keloid treatment and uncritical use of various types of lasers by unskilled physician have discredited its use. No laser alone is better than any other surgical approach, and the inexperienced may make it a powerful and harmful weapon. For old keloids, an ablative laser may be used to plane it for further topical treatment whereas vascular lasers may improve red scars and keloids. It is of utmost importance to explain to the patient that no laser can make a scar disappear – it may be able to improve it when used by a skilled laser therapist. Furthermore, the results described vary very much between different groups and particularly according to the sponsor of a study.
In conclusion, keloid treatment still remains an art requiring patience from the side of the patient and guidance by the physician. The combination of cryotherapy, surgical planing, intralesional corticosteroids and long-term silicone sheeting probably gives the best results whereas most monotherapies fail.
36

37
Lecturers: Dr. Daniela Taher –Lebanon, Dr. Bogdan Dimitrie Niculae, Dr. Cătălin Enăchescu
First day09.00 – 09.30 Cofee 09.30 – 10.00 History of chemical peels 10.00 – 11.00 Histologic effects of photoaging and resurfacing11.00 – 11.10 Questions and Answers 11.10 – 11.30 Pause 11.30 – 12.30 Clasiffication of chemical peels, Wound healing12.30 – 14.00 Lunch 14.00 – 15.00 Patient evaluation, Indications for chemical peeling15.00 – 16.00 Skin conditioning, before and after peeling16.00 16.10 Questions and Answers
Second day09.00 – 10.00 Superficial peels10.00 – 11.00 Medium and Deep peels11.00 – 13.00 Live presentation superficial and medium peels 13.00 – 13.30 Cofee break13.30 – 14.30 Complications after chemical peels 14.30 – 14.50 Questions and Answers15.00 – 16.00 Handling the dissatisfied pations, combining peels with other cosmetic procedures
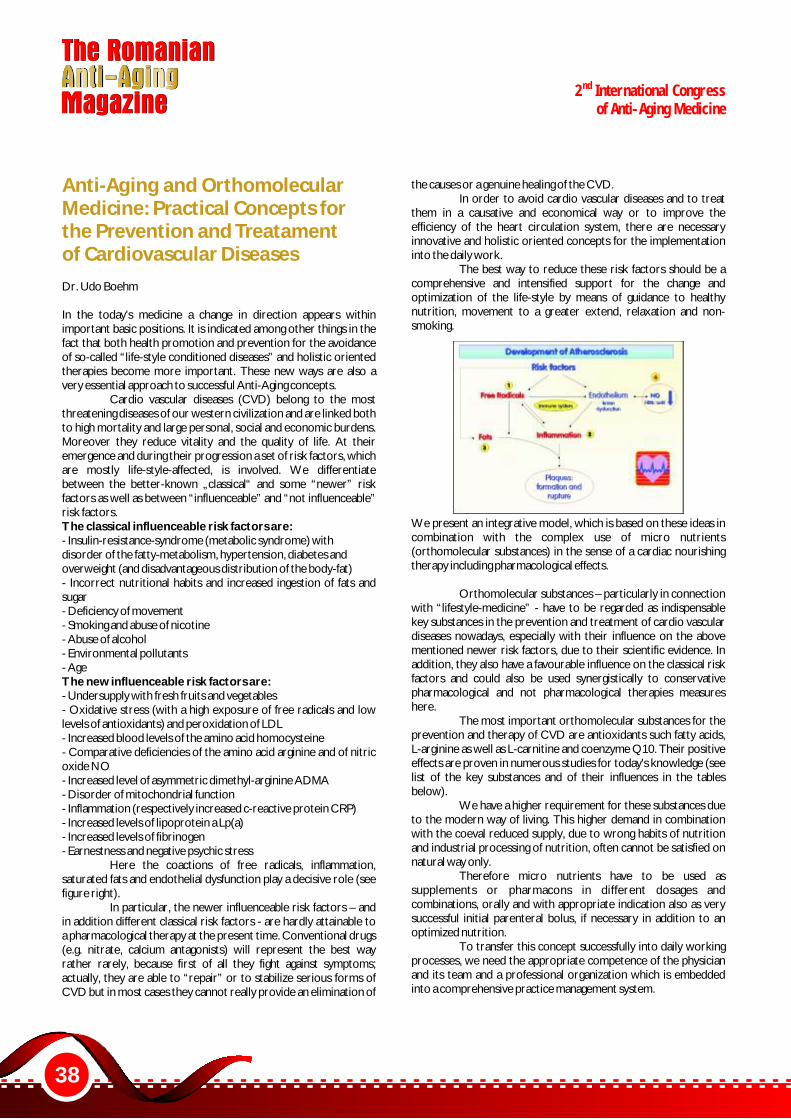
38
2 International Congressof Anti-Aging Medicine
nd
Dr. Udo Boehm
In the today's medicine a change in direction appears within important basic positions. It is indicated among other things in the fact that both health promotion and prevention for the avoidance of so-called “life-style conditioned diseases” and holistic oriented therapies become more important. These new ways are also a very essential approach to successful Anti-Aging concepts.
Cardio vascular diseases (CVD) belong to the most threatening diseases of our western civilization and are linked both to high mortality and large personal, social and economic burdens. Moreover they reduce vitality and the quality of life. At their emergence and during their progression a set of risk factors, which are mostly life-style-affected, is involved. We differentiate between the better-known „classical“ and some “newer” risk factors as well as between “influenceable” and “not influenceable” risk factors. The classical influenceable risk factors are:- Insulin-resistance-syndrome (metabolic syndrome) withdisorder of the fatty-metabolism, hypertension, diabetes andoverweight (and disadvantageous distribution of the body-fat)- Incorrect nutritional habits and increased ingestion of fats and sugar- Deficiency of movement- Smoking and abuse of nicotine- Abuse of alcohol- Environmental pollutants- AgeThe new influenceable risk factors are:- Undersupply with fresh fruits and vegetables- Oxidative stress (with a high exposure of free radicals and low levels of antioxidants) and peroxidation of LDL- Increased blood levels of the amino acid homocysteine- Comparative deficiencies of the amino acid arginine and of nitric oxide NO- Increased level of asymmetric dimethyl-arginine ADMA- Disorder of mitochondrial function- Inflammation (respectively increased c-reactive protein CRP)- Increased levels of lipoprotein a Lp(a)- Increased levels of fibrinogen- Earnestness and negative psychic stress
Here the coactions of free radicals, inflammation, saturated fats and endothelial dysfunction play a decisive role (see figure right).
In particular, the newer influenceable risk factors – and in addition different classical risk factors - are hardly attainable toa pharmacological therapy at the present time. Conventional drugs (e.g. nitrate, calcium antagonists) will represent the best way rather rarely, because first of all they fight against symptoms; actually, they are able to “repair” or to stabilize serious forms of CVD but in most cases they cannot really provide an elimination of
Anti-Aging and Orthomolecular Medicine: Practical Concepts for the Prevention and Treatament of Cardiovascular Diseases
the causes or a genuine healing of the CVD. In order to avoid cardio vascular diseases and to treat
them in a causative and economical way or to improve the efficiency of the heart circulation system, there are necessary innovative and holistic oriented concepts for the implementation into the daily work.
The best way to reduce these risk factors should be a comprehensive and intensified support for the change and optimization of the life-style by means of guidance to healthy nutrition, movement to a greater extend, relaxation and non-smoking.
We present an integrative model, which is based on these ideas in combination with the complex use of micro nutrients (orthomolecular substances) in the sense of a cardiac nourishing therapy including pharmacological effects.
Orthomolecular substances – particularly in connection with “lifestyle-medicine” - have to be regarded as indispensable key substances in the prevention and treatment of cardio vascular diseases nowadays, especially with their influence on the above mentioned newer risk factors, due to their scientific evidence. In addition, they also have a favourable influence on the classical risk factors and could also be used synergistically to conservative pharmacological and not pharmacological therapies measures here.
The most important orthomolecular substances for the prevention and therapy of CVD are antioxidants such fatty acids, L-arginine as well as L-carnitine and coenzyme Q10. Their positive effects are proven in numerous studies for today's knowledge (see list of the key substances and of their influences in the tables below).
We have a higher requirement for these substances due to the modern way of living. This higher demand in combination with the coeval reduced supply, due to wrong habits of nutrition and industrial processing of nutrition, often cannot be satisfied on natural way only.
Therefore micro nutrients have to be used as supplements or pharmacons in different dosages and combinations, orally and with appropriate indication also as very successful initial parenteral bolus, if necessary in addition to an optimized nutrition.
To transfer this concept successfully into daily working processes, we need the appropriate competence of the physician and its team and a professional organization which is embedded into a comprehensive practice management system.

39
2 International Congressof Anti-Aging Medicine
nd
Micro nutrients as key substances against CVD
Substance Dose Effect
Vit E (fat soluble) Vit C (water soluble)
200-600 mg 500-1500 mg
Antioxidant, decreasing aggregation and adhesion of thrombocytes, decreasing lipid peroxidation, protecting unsaturated adipose acids of oxidation; decreased growing of smooth muscle cells; anti-inflammatory Antioxidant, reducing oxidized Vit E, decreasing Lp(a) / fibrinogen / blood pressure, stabilizing blood vessels, normalising fat metabolism, regulating clot and aggregation of thrombocytes, increasing HDL and dilation of arteries
Vit B6 Vit.B12 Folic acid Vit B3
4-25 mg 10 µg 0,4-2 mg 40 mg
Decreasing homocysteine Optimizing cell-functions Decreasing homocysteine, important for division and forming of cells Decreasing LDL and inflammation, increasing HDL and endothelial function
Vit A (fat soluble)
0,6-1,5 mg Antioxidant, stabilizing membranes, reduces radical-forming in leukocytes
Coenzyme Q 10 (Ubichinon) L-Carnitine
10-50 mg 0,2–0,6 g
Antioxidant (reducing LDL-oxidation), key-substance for enzymatic reactions in heart-energy-metabolism (cofactor of the respiratory chain in mitochondria), decreasing blood pressure, improving NYHA-stages of cardiac insufficiency and arrhythmia (reduced in cardiac insufficiency), increasing tolerance for stress decreased by statins ((HMC-CoA-Reductase-Inhibitor) Increase of fat burning (b-oxidation in mitochondria) and energy supply in the heart, improving tolerance for stress
Selenium Zinc Magnesium
50-100 µg 10-60 mg 150-250 mg
Antioxidant (component of glutathione-peroxidase: catalyzing hydrogen peroxide reduction, decreasing lipid peroxidation, repairing cell damages, antiphlogistic (transcription factor NF-Kappa B) Antioxidant (component of superoxide-dismutase, improving therapy of diabetes Cofactor for enzymes energy supply, physiological Ca-antagonist, improving rhythm and tolerance for ischemia, decreasing of blood pressure
Omega-3- fatty acids
0,5-3 g decreasing aggregation of thrombocytes, insulin resistance, dysrhythmia, blood pressure, lp (a), fibrinogen, trigylcerides, VLDL, production of antiphlogistic substances and cell membrane growth factor PDCF, increasing NO formation
Carotenoids Flavonoids Resveratrol
4-20 mg 4-20 mg 4-20 mg (10 mg per red wine)
Antioxidants (quenchers of singulet oxygen), decreasing LDL oxidation
β-carotene: reduction of Angina pectoris (50% in the Physician‘s Health Study) Antioxidants, decreasing inflammation, cholesterol, LDL, hypertension, inhibitors of platelets aggregation Scavenging oxygen free radicals, increasing HDL, nitrite oxide synthesis, decreasing LDL, Lp (a), lipid oxidation
Argenine Lysine Cysteine (N-acetyl-cysteine) Tryptophane and Tyrosine Taurine
1,5-6 g 0,5-4 g 0,5-1,5 g 0,5-3 g 1-4 g 0,5-4 g
Influence on the arterial vessel system, precursor of nitric oxide NO -> forming of NO in the vascular endothelium, vasodilatative, promoting circulation, decreasing LDL, aggregation of thrombocytes, lipid peroxidation, blood pressure Component of vascular collagen, decreasing proatherogenic potential of Lp (a), increasing synthesis of carnitine Important for NO imparted processes, increasing activity of ACE-Inhibitors, decreasing nitrate tolerance and Lp (a), normalizing fat metabolism Decreases blood pressure , forming antihypertensive tryptophan metabolites (in combination with vitamin B6) positiv-inotropic, antiarrhythmic, decreasing blood pressure, stabilizing membranes (similar magnesium, saving magnesium)
40
2 International Congressof Anti-Aging Medicine
nd
Dr. Christophe de Jaeger, Dr. Elena Voronska
As adults age, central nervous system function slows appreciably. This phenomenon has been assessed with a wide variety of behavioral paradigms and originates from neurobiological factors related to aging.
Given the growth of the elderly population and the concomitant increase in the proportion of cognitively impaired individuals, accurate measurement of the mental changes stemming from aging is an important scientific and social problem.
Moreover, because neuroelectric measures have provided some of the most direct evidence for the relationship between central nervous system function and age-related cognitive changes, they have played an increasingly important role in the quantification and understanding of these effects.
A particularly successful application of electro- physiological techniques has employed event-related brain potentials (ERPs).
More specifically, the P300 component of the ERP has demonstrated considerable utility in the study of aging because it is thought to result from neural activity associated with attentional and memory processes.
For example, P300 amplitude age-variation indexes changes in neural activity across the scalp, the timing of its peak provides a measure of mental processing speed that is independent of behavioral responding, and characterization of its normative values has yielded baseline measures against which cognitive illness can be evaluated.
Even though much progress has been made in the 30 years since the P300 potential was discovered, the primary question remains: What cognitive events does the P300 component reflect?
The answer is still uncertain, with the interpretation of the P300 based on neurophysiological investigations of the brain mechanisms that underlie its generation, evidence from experimental studies that manipulate psychological variables, and results obtained from neuropsychological reports that examine the correlational relationships between P300 values and responses from behavioral tests.
The P300 component is often elicited with a simple discrimination task.
This procedure has been dubbed the "oddball" paradigm because two stimuli are presented in a random series such that one of them occurs relatively infrequently, that is, the oddball.
The auditory version of this task uses two different tones, interstimulus intervals of 1-3 s, and a target stimulus occurring less frequently than the nontarget or standard stimulus (e.g., probabilities of .20 and .80, respectively).
The subject is required to distinguish between the two tones by responding to the target (e.g., mentally counting, pressing a button, etc.) and not responding to the standard.
This task has been used to study a wide variety of
A Method to Evaluate CerebralSenscence: P300
information processing issues and has been the paradigm most often employed when normative aging data are acquired.
The P300 is measured by quantifying its amplitude (size) and latency (timing). Amplitude (ItV) is defined as the voltage difference between a prestimulus baseline and the largest positivegoing peak of the ERP waveform within a latency range (e.g., 250-400 ms, although the range can vary depending on subject characteristics, stimulus modality, task conditions, etc.). Latency (ms) is defined as the time from stimulus onset to the point of maximum positive amplitude within the latency window (with 300 ms being the modal latency when the component is elicited by using auditory stimuli in young adults - hence the name).


42
2 International Congressof Anti-Aging Medicine
nd
Farm. Vlăsceanu Gabriela, Prof. Ion Brad
The content of micro- and infra-micro elements from seabuckthorn fruits and copses was determined by the activation of neutrons. We also analysed the content of Zn, Cu. Mn, Fe, Ba, Mo, determined by fotometric of atomic absorbtion in 11 seabuckthorn bio-types. (Brad et al.1976).
The content in the dry matter has been analysed macro, micro, semimicro- and inframicro-elements from the ashes of the seabuckthorn, depending of the time of harvesting. There has been analysed the variation in content of serotonin depending, on the origin of the fruits (three geografic regions) (Cojocaru and Brad, 1984; Brad et al.1997). Estimations were made regarding: - some ways of processing different plant organs; - the biological effects of seabuckthorn; - the perspective for serotonin as an imunoinductor in different diseases.
The effects of seabuckthorn are the results of a large number of active physiologic substances, like hydro- and lypo-soluble vitamins, hormones and phytohormones, organic acids with an important role in metabolism, aminoacids (including the essentials), flavonoides, pro-vitaminsA, carotenoides, serotonin, melatonin (Mathiev and Azizov, 1981; Uluitu and Brad, 1984).
The use of seabuckthorn products (single or in association), act as immune-inductor and have other benefits, due to the fact that they act simultaneous, synergic and harmonic, determines effects of the many active ingredients from seabuckthorn fruits, leaves and copses (Brad and Medesan, 1987).
Most of our research done together with research centers: industrials, hospitals and production units. (Uluitu et al. 1997; Brad et al. 2002)
Today, micro-ements are considered to be ”mineral vitamins” because they meet all the requirements of what vitamins are. The vitamins are not synthesized by the human organism; they are co-enzymes or co-factors of numerous enzymes that act in all the human chains, tracks and metabolic cycles. Macro-, micro- and inframicro-elements have the same characteristics, they play dîfferent roles in the metabolic chain. Being at the same time stimulants and inhibitors, synergic or antagonists, being found in the structure of some substances, with different physiologic roles than vitamins. These „mineral-vitamins” are function inducers and structure stabilizers or play a role in catalyst processes or regulate the enzymatic activities. For some micro-elements the intimate, subtle process is unknown, but their inexistence is often harmful but their presence has exceptional effects, even in small amounts.(ppm).(Bazarova, 1978; Talichova, 1998; Puhalskaia, 2000; Brad et al., 2007)
Materials and methods As biologic materials we used seabuckthorn fruits, leaves, offshoots and offshoot bark. Micro and inframicro-elements were determined by the activation of neutrons from the Atomic Physics
Institute and through atomic absorbtion spectro-
The Characterization of Seabuckthorn Fruits and Copses inTerms of Serotonin and Microelements
Conţinutul în microelemente şi inframicroelemente din lăstarii şi fructele de cătina a fost determinat prin activare cu neutroni. De asemenea, a fost analizat conţinutul de Zn, Cu, Mn, Fe, Ba, Mo, din frunze şi fructe, determinat prin fotometrie, la 11 biotipuri de cătina (Brad et al.1976).
Analiza conţinutului în substanţa uscată, în macro-, micro-, semimicro- şi inframicroelemene s-a realizat din cenuşa fructelor de cătină, urmărindu-se şi variaţia funcţie de momentul recoltării. A fost determinată variaţia concentraţiei în serotonina funcţie de provenienţa fructelor, în 3 zone geografice (Cojocaru and Brad, 1984; Brad et al.1997). S-au făcut aprecieri asupra: - diverselor forme de prelucrare a diferitelor organe de plantă; - efectelor biologice deosebite ale cătinei; - perspectivei utilizării serotoninei ca factor imunomodulator îndiverse maladii.
Efectele extraordinare ale cătinei se datorează unui număr mare de substanţe fiziologic active, precum vitamine hidro- şi liposolubile, hormoni şi fitohormoni, acizi organici cu rol important în metabolism, aminoacizi (inclusiv esentiali), terpene, flavonoide, provitamine A, carotenoizi, serotonină, melatonină (Mathiev and Azizov, 1981; Uluitu and Brad, 1984) .
Utilizarea preparatelor din cătină (simplă sau în diferite asocieri), au demonstrat un efect imunomodulator datorită acţiunii simultane, sinergice şi armonice a numeroaselor principii active din frunze şi tulpini (lăstari). (Brad and Medesan, 1987).Majoritatea cercetărilor au fost realizate în colaborare cu unităti de cercetare: industriale, medicale şi de producţie (Uluitu et al. 1997; Brad et al. 2002)
Microelementele sunt astăzi considerate drept „vitamine” minerale deoarece întrunesc toate condiţiile cerute de definiţia termenului de "vitamină". Vitaminele nu sunt sintetizate de organismul uman; sunt co-enzime sau co-factori a numeroase enzime care acţionează în toate lanţurile, căile şi ciclurile metabolice. Macro-, micro- şi inframicroelementele au acţiuni asemănătoare, fiind implicate în întregul lanţ metabolic. În acelaşi timp stimulatori sau inhibitori, sinergici sau antagonici, intră şi în structura unor substanţe cu alt rol fiziologic decât vitaminele.
Aceste „vitamine” minerale sunt inductori de sarcină, stabilizatori de structuri şi au rol în procesele de cataliză şi reglare a activităţii enzimatice. Cu alte cuvinte, rolul lor este mai extins chiar decât al vitaminelor. Pentru unele microelemente nu se cunosc încă procesele biochimice intime la care participă, dar s-au putut evidenţia efectele grave generate de carenţa lor; prin studii clinice s-a dovedit rolul lor chiar la cantităti extrem de mici (ppm).(Bazarova, 1978; Talichova, 1998; Puhalskaia, 2000; Brad et al., 2007)
Materiale şi metode Ca material biologic s-au folosit fructe, frunze, lăstari şi scoarţa lăstarilor de cătină. Micro- şi inframicroelementele au fostdeterminate prin activare cu neutroni, la Institutul de Fizică Atomică şi prin spectofotometrie de absorbţie atomică la Institutul de Pedologie al ASAS. S-a determinat conţinutul în zinc, cupru, mangan, fier, bor şi molibden la 11 biotipuri. Serotonina a
Valorificarea fructelor şi lăstarilorcătinei pentru serotoninã şimicroelemente

43
2 International Congressof Anti-Aging Medicine
nd
photometry were determined at the Pedologic Institute at ASAS. It was determined the content in Zn, Cu, Mn, Fe, Br, Mo in 11 biotypes.
The serotonin was determined with a fluorescent method at the Normal and Pathologic Physiology Institute. We are presenting the results regarding the content in dry substance, ashes and micro-elements in white seabuchthorn fruits.
Determinations were made on micro-elments: Zn, Cu, Mn, Fe, Mo where there could be seen impressive quantities that vary by breed and soil/ weather conditions. In the dry fruits and ashes are found elements enumerated by us in alphabetical order: Al, As, Au, Ba, Ca, Ce, Co, Cr, Cs, Fe, Hf, K, La, Rb, Mg, Mn, Mo, Na, Sb, Se, Se, Sm, Sr, Th, U, V, Zn, Yb. Being found in the metabolism in different chains and cycles (according to the nowadays knowledge în regard with the micro-elements) it was revealed that they participate or constrain in more than 80-100 metabolic sequences. The serotonin was analyzed from seabuckthorn fruits obtained from different sources (Bucharest, Buzăau and Craiova). It could be seen a slightly smaller difference expressed in micrograms/gram of serotonin, the quantity was necessary and sufficient to have some effects from 8-10 g of dry substance daily, that corresponds to 40-50g of fruits.
Results and discusionsIt was also determined the serotonin in leaves, offshoots, offshoot bark; we can see big differences between the content in serotonin from dry leaves and fruits (the offshoots contain almost the same quantity of serotonin as the dry fruits and the offshoot's bark contain 6-7 times more serotonin than the offshoot and 4 times more than the leaves, the values being between 30-100 micro-grams/day).
For the serotonin there can be used as extraction methods the concentrated acid solutions through reverse osmosis or there can be extracted plain serotonin or associated with a precipitation element or co-precipitation, knowing the chemical proprieties of serotonin. Serotonin's effects are well known: immune-inductor, energizing, anti-depressive, chemical mediator, with implications in disabilities like insufficiency in transmitting the information through the nervous system to the organs. The serotonin with the other substances from seabuckthorn is recommended for sickness or discomfort, too. Mostly concerning the severe conditions that affect the XXI century: cancer, HIV, depression, anxiety, suicide tendencies, insomnia, alcohol abuse, schizophrenia, any disease generate by a phisical, chemical or biological agent. (Koslowski, 1970; Morichi, 1977; Takasahi, 1983; Muster, 1984).
References:1. Koslowski I. (1970) „The Phisiopathology and the general treatment of the grave burn”, Surgery, p. 9, 385-390, 410 pag.2. Brad I.L., Silva F., Cojocariu O., Jokl E., Marcu Z., Martinovski G., Voicu E. (1976) „The dinamic's of some active principles from the fruits of Hippophae rhamnoides”, Analele ICCPT vol.XII; p.1-9, 65 pag.3. Morichi A.(1977) „The vitel prognostic of burns”, Anesthesia, Analgesia, Reanimation, nr. 34, p.1293-1302, 1560 pag.4. Bazarova A. (1978) „The seabuckthorn – a drug remedium into the tibethan medicine”, Rastit. Resursi, XIV5. Mathiev N.K.,Azizov F.S.(1981)„Biological active agents of the fruct of the sea buckthorn”, Izv. Akad.Nauk, 6, p.118-123, 280 pag.6. Takasahi A. (1983), „The local treatment for burns”, Asian Medical Journal, 26(3), p.189-198, 250 pag.7. Munster A.(1984) „The immunological answer to traumas and burns”, American Journal of Medicine, nr.76 ;3 A; p.142-145, 251 pag.8. Cojocaru V., Brad L.(1984), "Establishing the content of micro-elements in the white seabuckthorn through neutron activation”, Symposium "Oltenia medicala", June 2-3, Craiova9. Uluitu M., Brad L.(1984) "Establishing the content of serotonin in the organs of white seabuckthorn", Symposium "Oltenia medicala", June 2-3, Craiova
fost determinată prin metoda fluorimetrică, la Institutul de Fiziologie Normală şi Patologica. S-au obţinut rezultatele privind conţinutul în substanţa uscată, cenuşa şi microelemente în fructele de cătină albă. Cantităţile de microelemente (Zn, Cu, Mn, F, Mo) obţinute au fost apreciabile, ele variind în funcţie de soi şi condiţiile pedoclimatice. În fructele uscate şi cenuşă au fost identificate următoarele elementele, enumerate în ordine alfabetică: Al, As, Au, Ba, Ca, Ce, Co, Cr, Cs, Fe, Hf, K, La, Rb, Mg, Mn, Mo, Na, Rb, Sb, Se, Se, Sm, Sr, Th, U, V, Zn, Yb. Plasate în metabolism în diferite lanţuri şi cicluri (raportat la cunoştinţele actuale), participă sau condiţionează 80-100 secvenţe metabolice. Serotonina a fost determinată iniţial din fructe, obţinute din surse diferite (Bucureşti, Buzău, Craiova). A rezultat o foarte mică diferenţă, exprimată în µg/g de serotonină, cantitate necesară şi suficientă pentru a avea efecte dacă se consumă 8-10g substanţa uscată zilnic, ceea ce corespunde la aproximativ 40-50 g fructe integrale.
Rezultate şi discuţiiS-a determinat serotonina din frunze, lăstari, scoarţă de lăstari, observându-se diferenţe mari ale concentraţiei de serotonină, funcţie de partea de plantă analizată (lăstarii conţin aproximativ aceeaşi cantitate de serotonină ca şi fructele uscate, iar scoarţa conţine de 6-7 ori mai multă serotonină decât lăstarii ca atare şi de 4 ori mai multă decât frunzele, valorile fiind cuprinse între 30-100 µg/g. Pentru micro şi inframicroelemente rentabilitatea este mică în ceea ce priveşte obţinerea de concentrate tip complex anorganic. De aceea trebuiesc consumate produsele din fructe, frunze, tulpini şi scoarţă ca atare, uscate, pulverizate sau în capsule şi sub formă de ceaiuri (în cantităţi cuprinse între 5-10 g /zi).
Pentru obţinerea serotoninei se pot utiliza metode de extragere în soluţii acide concentrate prin osmoza inversă sau asociată cu un element de precipitare sau co-precipitare, cunoscând proprietăţile chimice ale serotoninei. Serotonina are un bine cunoscut efectul imunomodulator, energizant, antidepresiv, mediator chimic, cu implicaţii legate de bolile în care se constată o insuficientă transmitere a informaţiei prin sistemul nervos către toate organele, în special către muşchi. A s o c i a t ă c u t o a t e microelementele din cătină este indicată atât în stări de disconfort cât şi în patologiile severe care afectează mileniul nostru: cancerul, HIV-SIDA, stări depresive, stări anxioase cu tendinţe suicidare, epuizări fizice şi nervoase, insomnii, stări comitiale, enurezis, abuz de alcool, schizofrenie şi orice boală provocată de un agent fizic, chimic sau biologic (Koslowski, 1970; Morichi, 1977; Takasahi, 1983; Muster, 1984).
10. Brad L, Medesan C. (1987), „Research regarding the immune-inductor effect of some white seabuckthorn breeds”, Symposium "Oltenia medicala", May 30-31, Craiova11. Brad I., Iganus V., Brad I.L., Rati L., Rati V., Acatrinei F.(1997), „A comparative research of the ash content (total mineralization) and micro-elements at 11 white seabuckthorn breeds, selected at S.C. FRUCTEX S.A. Bacau”, Symposium "50 years since the Inauguration of The Agronomic Institute Timisoara", June 1-2, Timisoara12. Uluitu M., Brad L, Chis R., Brad I.L., Rati I.V., Rati L., Acatrinei F.(1997), "Variation in seabuckthorn population (Hippophae rhamnoides) selected at S.C. Fructex S.A. Bacau”. Symposium „50 years since the inauguration of The Agronomic Institute Timisosoara", June 1-3, Timisosoara13. Talichova L.(1998) „Morphological change in the rat liver under sea buckthorn oil administration against a background of alcohol poisoning”, Experimental Pathology Pehm, 3, p.177-184, 784 pag.14. Puhalskaia E., (2000) „The seabhckthorn extracts effect on the thumoral transplants at the animals”,. Bull.Exlt. Biol.Med., 45, p.363-364, 470 pag.15. Brad I., Brad I.L., Radu F.(2002), "White Seabuckthom - a pharmacy into a plant" , Bucharest, Editura Tehnica, p. 114,115,116; 178 pag.16. Brad I., Brad I.L., Vlasceanu G.A., Manea St., Tamas V., (2007), „Usage of lipidic extract from dried sea buckthorn fruit (Hippophae rhamnoides L.) in burns and wounds of the members", ISA 2007, Quebec, Canada.

44
2 International Congressof Anti-Aging Medicine
nd
Dr. Claus Muss
Irritable bowel syndrome (IBS), also referred to as spastic colon, intestinal neurosis, and mucous colitis, is characterized by abnormal muscle contractions of the small and large intestines. In this condition, the gastrointestinal tract is sensitive to many stimuli including stress, diet, and drugs.
This sensitivity results in irregular muscle contractionsthat interfere with the normal transit of food and waste matter.
The food and fecal matter pass through the intestines quickly, generally leading to diarrhea.
The strong contraction result in cramps (often severe) in the lower abdominal region. (1)Definition: The current definition of IBS was reached by consensus at an international working party of experts in Rome in 1989. The Rome criteria for IBS are:
At least 3 months continuous or recurrent symptoms of abdominal pain which is:• relieved by defaecation or• associated with change in stool consistency or• associated with change in stool frequency,with two of:• altered stool frequency (>3 times per day or <3 times per week) altered stool form• altered stool passage (straining, urgency, incomplete evacuation) passage of mucus• abdominal bloating (2)
IBS is a chronic relapsing condition, and some suggest it occurs in most adults at some point in their lives. (2) Studies indicate that 10-20% of all adults have symptoms (abdominal pain, flatulence, irregular bowel movements), corresponding to about 25-50% of all patients who visit a gastro-enterologist’s clinic. (3)Epidemiology: Symptoms begin before age of 35 in 50% of patients, and 40% of patients are aged 35-50. IBS is recognized in children, and many patients can trace the onset of their symptoms back to childhood. Onset in old age is rare. (2)Pathogenesis: The cause of IBS has confounded physicians for almost two centuries. (2 )
Many factors are likely to give rise to the symptoms of IBS, like e.g. food intake, endocrine imbalance, disturbances in the intestinal bacterial flora, malabsorption, postoperative changes, and psychosomatic influences. (3)
Despite much research no convincing pathgogenesis has been revealed by studies and clinical expierence so far.
Diet problems and motility disorders due to altered perception, as well as psychological disorders have been claimed to be serious pathogenic factors. (4)
The only proven causal factor was severe gastroenteritis, exacerbated by high anxiety.
Also inflammatory cells were considered to be of a central role in the patho-physiology of IBS.
This thesis was based on the fact that Stress-related hormones, (such as epinephrine) which are more abundant in
Advancement in Diagnosis ofIrritable Bowel Sindrome (IBS)
states of anxiety, result in the release of certain inflammatory cytokines, including Interleukines (1 and 6). Such a release could prime the gut and lead to an exaggerated inflammatory reaction to normally harmless stimuli, such as foods or minor infections.
Evidence exists to link primary gut inflammation to changes in motility and mast-cell degranulation is known to result in changes in muscle contraction and in the excitability of enteric nerves. (2)Diagnostics: For many troubled IBS patients seen by specialists, cure or even acceptance of the diagnosis has been proven to be an unrealistic goal.
No drug has been proven globally effective in IBS so far. Therefore, Physicians had to discourage the chronic use
of costlysystemic drugs whose unwanted consequences were more troublesome than some IBS itself. (4)Advancement in lab diagnosis techniques have altered the prognosis and regime of treatment in IBS however recently.
Practical methods to detect abnormalities in the gut flora and the adjacent bowel mucosa have been established now in modern lab diagnosis recently to discern serious cause. Both experimental work and field studies have proven such parameters valuable in the diagnosis of inflamative intestinal disorders.
For instance impaired induction of beta defensins in human fecal samples suggests a deficient mucosal barrier function.
Beta Defensin expression was recognized after stimmualtion with efficacious probiotic treatment. A Field trail with 69 patients from a medical practice showed alpha antitrypsin excretions in feces to serve as critical lab parameter in determination of leaky gut diagnosis by feces controll aswell.
Also Calprotectin proofed to be a very sensitive marker of leaky gut entailing inflamatory reactions in the submucous system of the gut. Detection of an increased gut permeability by means of this parameter may be linked to a certain probability of food sensitivity. Actually food sensitivity plays a dominant role in the differentiation of IBS. Field trails have shown genuine food sensitivity to be more often associated to IgG4 reactions in our study group (Muss et al. 2004). However only a small subgroup of IBS patients had genuine food sensitivity associated to IGE reactions.
Further evidence was given by studies that also lysozyme can be used in the diagnosis of gut mucosa inflammation associated with neutrophil granulozytosis and monozytosis.
The use of such biological markers in fecal samples has opened a new age of clinical differential diagnosis in IBS.
One possible factor involved in the pathogenesis was discribed as an inflammatory reaction by extending the diagnosis program in this population to newly discribed parameters in feces and IgG4-Serology. In our studies over 70 (71%) of our patients classified as IBS priorily, suffered from food intolerance due to type III immunological disorders (IgG4-Antibody possitive reactions). A significant elevation was proven in is this group regarding alpha-1-Antitrypsin in feces and histamine extinction in urine samples.
When our patients showed positive samples of alpha-1-Antitrypsin in feces and histamine extinction in urine the majority of them had also an positive rast IgG4.
We consider IgG4-Diagnosis which is now even available as bed side diagnosis by Fast Check Kit to be a very important tool in distingushing our IBS patients.

45
2 International Congressof Anti-Aging Medicine
nd
Dr. Olga Safonicheva
Frank Chapman, Dr. of ostheopaty described the lymph circulation loss and possibilities of correction of those disturbance in 1930 for the first time. He revealed neurolymphatic points and zones (NL), that appear automatically at the level of skin in the projection of definite organs and glands when the lymphatic system is overloaded. Frank Chapman correlate "so called NL reflexes" with different stages of pathological processes and health problems. The subcutaneous tissue becomes denser at the early stage of illness and it changers in chronic stages. NL points are located primarily along the anterior intercostals spaces, on the abdomen down to the pubis, and posteriorly along the spinal column. There are some NL zones located on the legs and arms.
At present time the problem of the endoecological crisis and immune deficiency are being discussed by leading specialists of different branches of medicine. More specifically this problem is formulated by Academic V.P. Kaznacheev: "If the majority of the population safer from toxication of the body, we can
Dr. Olga Safonicheva
Stress is known to be the reason of psychsomatic diseases, such as infarct, hypertension and others. We suppose the post-stress reactions to become the non-specific base of mastopathy in women.
Materials: 78 patients with combination of musculoskeletal pain in the cervical part of the vertebral column and mastopathy were examined.
All of them had en emotional stress in anamnesis. The main complains were: rigidity in the shoulder girdle,
syndrome of chronic tiredness, pain and breast engorgement of mammary glans.Discussion: Clinical examination revealed pathobiomechanical disturbances: shorten muscles of the anterior part of the chest and neck, kyphosis of the chest, subluxations in the spine, and lymphodynamical disturbances - edematosity of the axillary and subclavicular zones.
The Role of LymphodynamicalDisurbances in the Formationof the Endoecological Disease.
establish the new specific epidemic of endoecological disease, different clinical forms of which are realizing in numerous nosologic variants".
The basic disciplines of the "Endoecological medicine" are - clinical lymphology and interstitiology.
The lymphatic system is the basis for the functional immune system that consists of: lymphoepithelian organs (thymus, spleen, marrow) - immune organs, lymphatic vessels (3%) - transport sector, and interstitial liquid (27%) - metabolic sector.
The function of the lymphatic (immune) system depends on free motion of the lymphatic liquid (30%) toward the subclavicular angles and optimal body statics (vertical axis).
Conclusion:1. Manual diagnosis allows to reveal changes in soft tissues at the early stages of pathological process and special soft tissue techniques enable to prevent the development of advanced visceral diseases and complications.2. Soft - tissue manual therapy promotes balanced functioning of systems, providing circulation rate autoregulation for optimal work of the brain, visceral organs, musces and all tissues.
This technique we recommend to use not only with the purpuse to cure, but also to prevent illnesses.
Clinical observation allows us to offer some statements: emotional stress lead to muscle spasms and mechanical obstacles lead to retrograde lymph flow in its movement to subclavicular veins.
The scheme of correction of poor lymph outflow and pathobiomechanical disturbances is worked out in Moscow medical academy.
The aims of the treatment are: releasing of the spasmodic muscles and restoring the lymph outflow.
The therapeutic scheme includes the soft - tissue manual techniques and it contains several stages.
Duration of the course is 7-9 procedures. Positive results were received in 87% and confirmed by
objectively instrumental methods.
Conclusion:1. Biomechanical and lymphatic disturbances suppose to be the main non-specific base and reason of the musculoskeletal pain syndromes and mastopathy.2. The manual therapy is specific diagnostical and therapeutical method which has possibilities to reveal biomechanical and lymphatical disturbances and remove them using soft -tissue non - traumatic techniques.
New Possibilities of Manual Diagnosis and Therapy ofMastopathy

46
2 International Congressof Anti-Aging Medicine
nd
Aesthetic RhinoplastyDr. Dimitrios Karypidis
The concept of improving the appearance of an aesthetically distinct facial landmark such as the nose, contributes to the enhancement of the overall facial aesthetics. Many features of aging represent a variable differentiation from the aesthetically ideal proportions and anatomic relationships.
The rejuvenation effect that results from a prospective restoration of these proportions and the establishment of an aesthetically acceptable nasal-facial balance is therefore obvious.Patients and Methods: This presentation refers to a series consisting of 292 patients, 90 (30%) males and 202 (70%) females. 141 (48%) aesthetic primary rhinoplasties took place, 109 (77%) in female and 32 (23%) in male patients. 151 (52%) combined rhinoplasties, comprising of both an aesthetic and a functional component, were performed, 93 (61%) in female and 58 (39%) in male patients.
The mean age in male patients was 51-years-old and in female patients 44-years-old.
The method of choice was the closed rhinoplasty procedure due to its superior aesthetic potential (lack of the stair step columella incision, less time for recovery, lower rate of complications).
The open procedure was performed in 14 (9%) cases of combined rhinoplasty (functional and aesthetic), were better anatomical exposure and the use of autologous cartilage grafts were needed. Results:The aesthetic outcome can be categorized as excellent, good, fair and poor depending on the ideal aesthetic analysis and proportions as well as the extend of patients' satisfaction concerning a rejuvenating and restoring effect. 231 (79%) results were excellent, 29 (10%) good, 24 (8%) fair and 8 (3%) poor.
No major complications were observed. Mild edema and perinasal ecchymosis were observed or slightly prolonged in 3 (1%) cases.
Dr. Carazanu Crina Amalia
Our approach was a post-mortem study made on a group of seven pacients who died in the clinic of our institute and having no active gastric pathology. Their age was between 78 and 87 years old and there were four men and three women . The gastric tissue samples were taken from the gastric body and from the antral part , fixed in formalin 10 % and then , processed by histopathological technique
Conclusion:The nose is a prominent aesthetic hallmark of the face. Aesthetic rhinoplasty is a considerable aid towards effectively restoring ageing related or resembling deformities.
of paraffin embedding and cut in sections of 5 microns. These sections were coloured by hematoxilin-eosin routine staining and Van Gieson special staining for connective tissue. By light microscopic examination we noticed resemblant histopathological changes in all examined cases like: inflammatory lympho-plasmocytic infiltrate, more abundant in the antral part, tending to form lymphoid follicles, some mitotic figures at basis of the foveolae, reflecting the specific turn-over, the expansion of lamina propria, tending to dissociate glands, sign of atrophy and the phenomenum of pyloric metaplasia which by replacement of body type of glands by mucous antral type, could explain the acid production decline during ageing process.
Histopathological Changes in the Gastric Mucosa during the Ageing Process
48
2 International Congressof Anti-Aging Medicine
nd
Dr. Christophe de Jaeger
The term sarcopenia refers to the loss of muscle mass that occurs with age and is derived from the Greek meaning 'poverty of flesh'.
Sarcopenia results in a loss of strength and is a major contributing factor to frailty, falls and loss of independence. As a part of normal ageing, muscle mass is reduced by approximately one-third between the ages of 50 and 80. Although there is also a decline in specific force (force per cross-sectional area), reduced muscle mass accounts for most of the loss of strength that occurs with ageing.
Sarcopenia differs from acute difuse atrophy in several ways: with difuse atrophy, muscle mass is reduced, but fibre number and specific force are maintained and there is a shift toward expression of fast fibre types; with sarcopenia, muscle mass, fibre number and specific force are all reduced and there is a shift toward expression of slow fibre types.
Many factors contribute to sarcopenia, including the loss of motoneurons, nutrition, physical inactivity, reduction in levels of sex steroids and impairments in the growth hormone (GH)/ insulin-like growth factor (IGF-I) pathway.
Age is accompanied by losses in motoneurons in the anterior horn and ventral root of the spinal column, and by losses in the number of functioning motor units in large muscles, such as vastus lateralis. In elderly people, there is a decrease in food intake, despite the increase in adiposity.
Reduced food intake has a number of causes, including reduced activity and resting metabolic rate, impaired taste and smell, and rapid satiation due to an impairment of cholecystokinin mediated dilation of the stomach during a meal.
A substantial number of elderly men are hypogonadal.Circulating testosterone is highly bound to sex
hormone-binding globulin (SHBG), and because serum SHBG increases with age, bioavailable testosterone (free plus albumin-bound testosterone) declines more markedly with age than does total testosterone. Loss of testosterone is associated with loss of muscle mass and strength, decreased bone mineral density, lowered libido, lowered haematocrit and increased risk of fracture following falls.
Menopause is associated with the well-documented loss of bone mass, but also with loss of strength.
Muscle weakness develops earlier in women than in men and muscle strength can be preserved with hormone replacement therapy.
The latter finding is especially important because elderly women have greater functional impairment and longer life expectancy than do men. GH is required for maintenance of muscle and bone in adulthood.
GH exerts most of its anabolic actions through IGF-I, by stimulating the liver to secrete IGF-I into the circulation and by stimulating tissues, including muscle and bone, to produce IGF-I for local paracrine action. In addition, an important component of exercise-induced muscle hypertrophy is an increase in muscle IGF-I that occurs independently of GH.
Sarcopenia and Ageing
Secretion of GH is impaired in elderly men and women, with the amplitude of night-time GH pulses declining by between 30% and 70%.
Resistance training remains the most effective intervention for increasing muscle mass and strength. People have reduced food intake and increased protein requirements. As a result, adequate nutrition is sometimes a barrier to obtain full benefits from resistance training in this population. Growth hormone replacement in subjects produces a high incidence of side-effects, does not increase strength and does not augment strength gains resulting from resistance training.

49
2 International Congressof Anti-Aging Medicine
nd
Dr. Eleonora Luka Pilla
One of the major pathologies of our modern world is a cardiovascular disease with a leading problem which is HYPERTENTION. It's known more than 25% of the world's population is HYPERTENSIVE.
As a complication and target organ damages, CEREBRAL IMFARCTION, STROKE, ISCHEMIC DISEASE, RENAL DISFUNCTION and FAILURE are rather frequent.
Classical antihypertensive drugs, like DIURETICS, DIRECT VASODILATATORS, Ca2+ channel blockers are widely used and their mechanisms and sites of action are known. However their SIDE EFFECTS like: FATIGUE, LETHAGY, DIZZENESS, SEXUAL DISFUNCTION or KIDNEY FAILURE are important and not NEGLECTABLE.
Newest Natural AntiHypertentation Herbal Product
This study proposes a NEW, NATURAL solution, derivated from the ROOTH and LEAVES of PIPER CANINUM (wild pepper) family PIPERACEAE, origin from MALAYSIA. By an innovative technological process of FREESE DRYING, active princip from a rooth was obtained. AFTER, an alchoholic solution was prepared.
An animal study took place, during the last six months 2006 with a WKY (wistar Kyoto rats) and SHS (spontaneous hypertensive rats) who were administrated alchoholic solution of Piper CANINUM. Another study by oral gavage of Piper caninum was also done for 18 days. These two measurements gave all the necessary results concerning behavioural changes with dose dependent quantities as well as the degree of toxicity and the LD50.
A monitoring of the BP (blood preassure), the indirect and the conscious one was done after by the Tail'S Cuff methode. Some of the animals were also vagotomized and a comparative study with the Proranolol and Phenntolamine took place in order to understand the mechanism of action.
50
2 International Congressof Anti-Aging Medicine
nd
Dr. Sorin Marinaş
Produs realizat din peşte tip sardină şi cod, cu un conţinut ridicat de acizi graşi esenţiali (
). Supliment nutritiv uşor resorbabil, cu un conţinut bogat în acizi graşi esenţiali şi vitamine.
Peştele şi sunt o sursă directă de aport al cu lanţ lung de carbon .
Aceşti acizi sunt lipide esenţiale care se găsesc din abundenţă în creier în proporţie de 60% şi fac parte integrantă din membranele celulare şi neuronale. Acizii sunt transformaţi în eicosanoizi (molecule semnalizatoare puternice pentru sistemul imun, dintre care unele cu efecte inflamatorii şi cu rol crucial în transmiterea eficientă a impulsurilor nervoase).
fluidifică membranele celulare (dublu strat lipoproteic), restabilesc mobilitatea şi funcţionalitatea receptorilor de membrană şi a canalelor ionice.
sunt obţinuţi exclusiv prin aport alimentar, iar într-un regim alimentar ideal, între cele două tipuri de acizi graşi există un echilibru optim (raport de 4/1). În alimentaţia umană sunt frecvente dietele dezechilibrate, ceea ce creează stări patologice din cele mai diverse, cum ar fi boli cardiovasculare, neuropsihice, neoplazii.
Statisticile OMS au demonstrat o creştere alarmantă a morbidităţii şi mortalităţii datorate vieţii cotidiene şi a dietelor dezechilibrate. Ministerul Sănătăţii din Singapore a publicat un studiu oficial referitor la rata mortalităţii (Singapore 2002, după ROYAL OMEGA INSTITUTE).
Studiul se referă la o largă patologie; evident este faptul că patologia cardiovasculară, neurologică şi neoplazică sunt în top (rata mortalităţii: 15 persoane/zi; 1 persoană la 2 ore).
Morbiditatea este la fel de critică.
omega 3_acid eicosapentanoic_ EPA si omega 6_acid docosahexanoic_DHA
uleiul de peşteacizilor graşi omega 3 EPA si DHA
EPA şi DHA
EPA şi DHA
Acizii graşi esenţiali: linolenic (omega 3) şi linoleic (omega 6)
Omega 3 - Ulei de peþte(capsule 400 mg)
Conform studiului ROYAL OMEGA INSTITUTE, rata spitalizărilor per zi este de 93 persoane; 4 internări/oră. Factorii de risc şi speranţa de viaţă s-ar putea îmbunătăţi prin administrare de
Interesul deosebit al lumii medicale pentru acest produs a rezultat în urma cercetărilor laborioase din clinici de referinţă cum ar fi Mayo Clinic USA şi National Institutes of Health of US Gov. precum şi ale clinicilor din Europa, Canada, Japonia etc.
Studii clinice ale acţiunii terapeutice
Studiu realizat timp de 11 ani (SUA) pe 20.557 subiecţi (bărbaţi) a demonstrat că administrarea de , 2g/zi a dus la o scădere cu 52% a deceselor datorate patologiei cardiovasculare.
Prof. Durrington (2001) a monitorizat 59 de pacienţi cu patologie cardiovasculară administrând 2g/zi observând o scădere a trigliceridelor serice cu 20-30% şi a lipoproteinelor colesterolului cu 30-40%.
Prin consumul regulat de se ameliorează automat şi aritmiile, prin redobândirea elasticităţii membranei celulare cardiace. Suprasaturarea acestei membrane cu acizi graşi duce la aritmii majore prin deteriorarea celulelor musculare contractile cardiace. Dr. Harper si Dr. Jacobsen (2001) au raportat o scădere semnificativă a riscului ocluziv în cazul by-pass-ului arterei coronare folosind autogrefa venoasă.
Dr. Moham şi Dr.Das (1999) au demonstrat că administrarea de şi a dus la o scădere majoră a fosfolipidelor
plasmatice, având ca urmare o remisie a manifestărilor clinice fără efecte secundare în cazul LED.
Administrarea de a validat prin tehnica de osteodensitometrie o diminuare a demineralizării osoase (cunoscut fiind faptul că acidul eicosapentanoic este implicat în depunerile de Ca).
Colectivul de cercetători nefrologi de la Clinica Mayo (2001) a arătat că terapia cu a dus la o scădere a ratei de progresie a imunoglobulinei A la pacienţii cu risc nefropatogen.
Consumul de a dus la o scădere semnificativă a nivelului calciuriei, diminuind rata de apariţie de calculi renali.
Pacienţii hemodializaţi sub tratament cu , 3g/zi au necesitat cu 16% mai puţină eritropoetină, scăzând şi riscul tulburărilor de coagulare.
Un studiu pe 6.272 subiecţi (Suedia 2002) a evidenţiat o scădere de 72% a neoplasmului de prostată la un consum de 2g/zi de . Prof. Augustsson (2003, Swidish Cancer Institute) a elaborat o temă de cercetare la nivel naţional pe 47.882 de subiecţi, arătând o scădere de 24% a metastazelor în cazul administrării a 2g/zi, timp de un an, a Omega 3.
OMEGA 3-6 (EPA-DHA).
Omega 3-Omega 6 (4/1)
Omega 3
Omega 3,
ulei de peşte
Omega 3 Omega 6
Omega 3-Omega 6 (raport 4/1)
ulei de peşte
Omega 3
Omega 3
Omega 3
1. Boli cardiovasculare, HTA, Ateroscleroza
2. Lupus eritematos difuz
3. Osteoporoza
4. Tulburări renale
5. Cancerul de prostată
Cancer
Total nr. decese
Cauze (în %)
Cardiovascular Respirator Cerebrovascular Diabet Nefropatii
15.693 2000
27.0 25.1 11.4 10.4 2.3 1.3
2001 15.367
28.2 26.3 10.0 9.2 3.3 1.7
200215.820
28.024.213.18.82.71.6
Total nr. spitalizări
Cauze (în %) CancerCardiovascular Respirator Cerebrovascular Diabet Nefropatii
2000 387.100
5.4 6.1 2.7 2.7 2.0 1.5
2001 381.900
5.6 6.2 2.7 2.7 1.6 1.7
2002386.200
5.76.22.42.61.81.6

51
2 International Congressof Anti-Aging Medicine
nd
6. Cancerul de sân
7. Cancerul de colon
8. Cancerul de piele
9. Astm
10. Obstrucţii cronice pulmonare
11. Dismenoreea
12. Scleroza multiplă
13. Suport prenatal şi postpartum
Singapore (2001): după 5 ani de studii prospective pe 35.298 de paciente (vârste 45-74 ani) s-a concluzionat că dieta
a dus la o scădere cu 26% a neoplasmului mamar.
Collett (2000 Belgia) a arătat că administrarea de favorizează o diminuare a riscului de neoplasm de colon.
Dr. Rhodes şi colaboratorii (2002 Israel) au arătat că arsurile solare (42 subiecţi) duc la o scădere majoră a din organism, facilitând riscul apariţiei cancerului de piele. Astfel, suplimentând cu 2g-3g/zi raţia de Omega 3, se anihilează acest proces.
Dr. Nagakura (2000 Tokio) a studiat un lot de 29 de subiecţi (copii între 5-14 ani) cu astm bronhic sever. La administrarea a 5.4g/zi
timp de 10 luni, s-a observat o remisie semnificativă a manifestarilor clinice.
Romieu şi Trenga (2001, Paris) au observat pe 8.960 de subiecţi (fumători) că administrarea a 4g/zi are efect protectiv asupra hiperactivităţii căilor respiratorii şi asupra activităţii pulmonare.
Un studiu efectuat în Danemarca a relevat că administrarea de în perioada premenstruală duce la o creştere
a concentraţiei de prostaglandine care acţionează ca şi hormonii ce controlează contractilitatea uterină şi sindromul algic.
Cunnance şi colaboratorii (1992, Paris) au observat că pacienţii cu SM au o concentraţie scazută de în plasmă. Gallal (1999, Paris) a observat că suplimentarea raţiei de în cazul SM duce la modelarea activităţii imunologice în cazul acestei patologii.
Administrarea de între a 24-a şi a 28-a lună de sarcină s-a arătat a fi benefică în evoluţia fătului (greutate, lungime, circumferinţă craniană). Institutul de neonatologie norvegian a comunicat o scădere semnificativă a riscului apariţiei diabetului tip 1 la copii după administrarea de în timpul sarcinii. Malcom şi Uauy (2003, Mayo Clinic) au studiat un lot de 100 de gravide sub administrare .
La nivelul membranelor celulare, neurostimulatorilor, modulatorilor de gene, cu referire în special la nivelul retinei, creierului şi ţesutului neuronal. Datele oferite de Dunstan şi colaboratorii (2003, Mayo Clinic) au arătat că implicarea la nou născuţi duce la diminuarea riscului de boli alergice. Prof. Williams (1995, Mayo Clinic) a demonstrat că preeclampsia are la bază printre altele şi hiperlipidemia.
Administrarea scade cu 46% rata preeclampsiei.
EPA-DHA (4/1)
Omega 3
EPA
Omega 3-Omega 6,
ulei de peşte
Omega 3 şi Omega 6
EPAOmega 3
ulei de peşte
EPA-DHA
Omega 3-Omega 6
EPA
Omega 3-Omega 6
S-a demonstrat că nou-născuţii au beneficiat de creşterea activităţii. Dr. Grimminger (1993, Germania) a afirmat că administrarea de
are efect antiinflamator asupra leziunilor tegumentare în cazul a 20 de pacienţi spitalizati şi diagnosticaţi cu psoriazis.
Maes şi colaboratorii (1999, Paris) a observat un deficit major de , fosfolipide cu afectarea membranei hematiei la pacienţii
cu depresii majore. În atare situaţie, aportul de ca adjuvant al terapei antidepresive este de un real folos. Hibbein şi Salem (2001, Israel) au arătat că scăderea concentraţiei de acizi graşi suprasaturaţi creşte incidenţa la depresii, alcoolism, suicid şi depresii post-partum. Administrarea de , 9.6 g/zi în schizofrenie a avut rezultate semnificative în reducerea episoadelor maniacale, pe scala de rating a depresiei Hamilton, fapt demonstrat în 28 de studii clinice.
În 2003, Dr. Zanarini şi Dr. Frankenburg (2002, Israel) au studiat efectul administrării a 1g/zi şi au constatat o scădere a agresivităţii. Tulburările de atenţie şi hiperreactivitate beneficiază de aportul a 3g/zi obsevându-se o ameliorare semnificativă: Puri, Kidd si Richardson (2000, Mayo Clinic).
Prof. Delarue (2004, Mayo clinic) a efectuat un studiu pe 7 voluntari în 2 faze. Faza 1. 3 săptămâni, cei 7 subiecţi au fost supuşi la un stres mental major, prin bombardare cu informaţii în progresie aritmetică. La 30 de minute după şedinţa de stres au fost monitorizate constantele somatoadrenalitice (cortizolul plasmatic, cate- colaminele, cantitatea de energie celulară pierdută, lipoliza) observându-se o creştere semnificativă a lor.Faza 2. S-au introdus în raţia alimentară 7.2 g/zi pentru următoarele 3 săptămâni, după care s-au monitorizat aceleaşi constante, observându-se o scădere marcantă a lor.
În concluzie, s-a demonstrat că reprezintă o barieră de protecţie majoră a SNC la factorii de stres.
Studiile şi cercetarile referitoare la complexul pot fi subiectul unor lucrări laborioase. Acţiunea acestor
2 acizi graşi esenţiali asupra organismului uman a fost cu prisosinţă demonstrată; nu vom sublinia în încheiere decât câteva din avantajele acestei diete:• scade colesterolul şi trigliceridele, scade riscul avansării aterosclerozei;• stimulează metabolismul şi funcţionabilitatea sistemului nervos central şi periferic;• acţionează favorabil în tulburările bipolare;• acţiune benefică în evoluţia sarcinii şi asupra produsului de concepţie;• stimulează regenerarea ţesuturilor;• hipotensor şi cardioreglator;• imunostimulator;• antiinflamantorie;• adaptogenă;• antiasmatiformă.
14. Psoriazis
15. Tulburările psihice
16. Stres
EPA
Omega 3 EPA
Omega 3
EPA
Omega 3,
Omega 3
Omega 3
Omega 3 - Omega 6
EPA şi DHA

52
Dr. med. Manole Cojocaru
Viral hepatitis continues to be a major cause of morbidity and mortality. Hepatitis is largely a nondiscriminatory disease. Acute hepatitis is highly common disease, affects in particular many people in lower socio-economic regions.
Viral causes of hepatitis are clinically indistinguishable from one another. It is known that this disease usually does not require hospitalisation and medication nor any other intervention. However, mismanagement of this acute and mostly self-limiting disease, often occurs.
This can be a problem because appropriate management often depends on the specific virus involved. Fortunately, advances in serologic and molecular testing now allow accurate identification of the viral causes of both acute and chronic hepatitis.
Although illness is often subclinical, viral hepatitis has a substantial impact on society in terms of days lost from work and school, the need for hospitalization, and even loss of life.
Seven known pathogens can bring about the clinical picture of acute viral hepatitis.
Hepatotropic viruses also have the potential to cause chronic disease and can be associated with development of liver cirrhosis, hepatocellular carcinoma, and liver failure.
Hepatitis B infection and chronic hepatitis C are both premalignant diseases. Consequently, accurate diagnosis of the specific cause of hepatitis is important for appropriate management.
Vaccination has been proven to reduce infection rates and the incidence of hepatocellular carcinoma. In the case of hepatitis C, vaccination is not a possibility, and a reliable vaccine is not on the horizon.
In conclusion, diagnosing the specific agent responsible for viral hepatitis is difficult because the signs and symptoms of each type are similar.
Furthermore, many individuals who contact the disease have few or no symptoms. It would therfore appear that both hepatitis B- and C-induced liver damage are conditions that will account for significantly more morbidity and mortality in the European Union in the future.
Diagnosis of Viral Hepatits1) Anticorpii anti-HAV (valoarea normală Negativ)Sunt anticorpi împotriva virusului hepatitei A (HAV). După infecţie anti-HAV IgM devin pozitivi (diagnosticul de hepatită acută); după aproximativ 2 luni, aceştia se schimbă cu cei din clasa IgG (infecţia este depaşită). Anti-HAV IgG persistă ani şi protejează organismul de reinfecţie. 2) Antigenul HBs (HBsAg), (valoarea normală Negativ)Este un grup de glicoproteine la nivelul învelişului virusului hepatitei B (HBV). Antigenul HBs (HBsAg) apare în circulaţia sanguină după infecţia cu virusul hepatitei B, apar cu aproximativ 4 săptămâni înaintea simptomelor clinice. Testul pozitiv pentru HBsAg indică infecţia curentă cu virusul hepatitei B. Acest marker este în general prezent 1-2 luni după apariţia simptomelor, apoi dispare iar anticorpii împotriva acestuia (HBsAb) încep să crească. Dacă HBsAg persistă peste 6 luni, este probabil infecţie cronică.
3) Anticorpul HBs (HBsAb), (valoarea normală Negativ)Sunt anticorpi împotriva antigenului HBs. Sunt ultimii anticorpi care apar după infecţie şi sunt un indicator că infecţia este depaşită. Aceştia neutralizează HBV şi protejează organismul. HBsAb sunt induşi prin vaccinare.
4) Anticorpul HBc (HBcAb), (valoarea normală Negativ)Sunt anticorpi împotriva antigenului HBc (HBcAg) ce apare după aproximativ 8 săptămâni de la infecţie (aceştia sunt primii anticorpi detectabili). Când HBcAb apar în circulaţie nivelul transaminazelor (AST si ALT) începe să crească. Iniţial răspunsul în anticorpi este din clasa IgM, apoi, după aproximativ 2 luni, este schimbat cu cei din clasa IgG.
Prin urmare, HBcAb din clasa IgM sunt detectaţi când este o infecţie recentă (faza acută) şi HBcAb din clasa IgG când infecţia este rezolvată. În infecţia cronică HBcAb IgM este persistent pozitiv.
Aceşti anticorpi nu neutralizează HBV, aceştia indică dacă există o infecţie (nu apar după vaccinare)
5) Antigenul HBe (HBeAg), (valoarea normală Negativ)Este un peptid care este produs şi devine detectabil în ser în timpul replicării HBV, ca HBV DNA şi DNA polimerază. În infecţia acută HBeAg este tranzitor, acesta este în general detectabil în acelaşi timp cu HBsAg şi dispare înaintea acestuia. Clearance-ul HBeAg indică un pronostic favorabil (virusul nu se mai replică şi se întrerupe lezarea ficatului). În infecţia cronică acesta este pozitiv în timpul reactivării virale. Există mutanţi virali ai HBV care nu produc HBeAg. Aceşti mutanţi par să fie mult mai agresivi. Pacienţii HBeAg pozitivi sunt foarte infecţioşi.
6) Anticorpul HBe (HBeAb), (valoarea normală Negativ)În infecţia acută, după câteva săptămâni, clearance-ul HBeAg, anticorpii împotriva HBeAg (HbeAb) devin detectabili, iar transaminazele încep să scadă. În infecţia cronică infecţia devine pozitivă când reactivarea virală se opreşte.
Diagnosticul hepatitei virale

53
detectarea genomului viral în sânge (PCR şi bDNA). Încărcarea virală este un important factor de predicţie
care determină răspunsul la terapie (interferon). Se stabileşte cu bDNA sau cu PCR (mai sensibil).
11) GenotipurileCu PCR se poate determina genotipul HCV. Există 6 genotipuri majore HCV cu diferite trăsături clinice şi răspuns la terapie (genotipul 1b pare să fie asociat cu forma mai agresivă şi cu răspuns mai slab la terapie).
12) Anticorpii anti-HDV (HDV Ab), (valoarea normală Negativ)Sunt anticorpii produşi de sistemul imun împotriva HDV. Acesta este pozitiv în hepatita D acută (din clasa IgM) şi în cronică (dacă persistă peste 6 luni). Acest test se efectuează numai la pacienţii HbsAg pozitivi (HDV este un virus defectiv care necesită prezenţa HbsAg).
Hepatita virală este mai periculoasă la adult decât la copil, mai ales după 40 de ani. Hepatita acută poate sa fie cauzată de un virus, toxină sau poate să fie prima manifestare a unei boli cronice de ficat. Alanin aminotransferază crescută în ser este cel mai bun indicator al injuriei hepatice acute, dar nu reflectă severitatea bolii: se recomandă bilirubina şi INR (International Normalized Ratios).
În HCV acută este important să testăm pentru HCV RNA şi anti-HCV. Dacă ambele sunt pozitive, posibil să apară HCV cronică. Dacă numai HCV RNA este pozitivă, este probabil HCV acută, se urmăreşte dezvoltarea anti-HCV.
Virusul hepatitei D (HDV) este un virus RNA monocatenar defectiv din tipul Deltaviridae. Acesta este un virus RNA incomplet, are nevoie de antigenul de suprafaţă al hepatitei B pentru a transmite genomul său de la celulă la celulă. Prin urmare se întâlneşte numai la pacienţii care sunt HB sAg pozitivi. Replicarea HBV este supresată la pacienţii infectaţi cu HDV. Trăsăturile caracteristice ale pacienţilor cu infecţie HBV cronică care sunt suprainfectaţi cu HDV sunt: 1) titrul HBsAg scade în timpul apariţiei HDVAg în ser, 2) HDVAg şi HDV RNA rămân detectabile în ser, 3) sunt detectabile titruri crescute ale anti-HDV atât din clasa IgM cât şi IgG. Frecvent replicarea HBV este supresată.
Virusul hepatitei E (HEV) este un virus din tipul Caliciviridae care conţine RNA. Hepatita este autolimitată. Se decelează HEVAg şi se testează anticorpi anti-HEV din clasa IgM/IgG (nu se lucrează de rutină).
Bibliografie:
Maddrey W. C. Hepatitis B: an important public health issue. J Med Virol 2000; 61(3): 362-6.
Torberson M., Thomas D. L. Occult hepatitis B. Lancet Infect Dis. 2002; 479-86.
EASL HBV Consensus paper (http://www.easl.ch/hbv2002/01630170.pdf)
NIH Consensus paper HCV (http://consensus.nih.gov/cons/116/116cdc_intro.htm)
BMJ 2001; 322: 151. Acute hepatitis (http://bmj.bmjjournals.com/cgi/content/full/322/7279/151)
D Lavanchy; Journal of Gastroenterology and Hepatology. 2002; 17: 5452-9.
7) HBV DNA (PCR), (valoarea normală Negativ)Acesta este testul care detectează genomul viral HBV (DNA) în sânge.
Devine pozitiv în timpul replicării virale, după infecţie (hepatită acută) şi în timpul reactivării virale (hepatită cronică). 8) Anti-HCV (HCV Ab), (valoarea normală Negativ)Acest test detectează anticorpii produşi de sistemul imun împotriva HCV (core şi proteine virale nestructurale).
Anti-HCV pozitivi indică expunerea anterioară, nu infecţia curentă. La pacienţii imunocompromişi, testul negativ cu hepatită acută sau recent după expunere nu exclude infecţia HCV din cauză că există o perioadă liberă “window period” de câteva săptămâni înaintea prezenţei seroconversiei (apariţia anti- corpului).
Testul se poate efectua cu:1. EIA (Enzime Immune Assay) sau ELISA (Enzime linked Immuno Sorbent Assay) sunt folosite pentru screening-ul donatorilor de sânge si ca test iniţial pentru pacienţii cu patologie hepatică.2. RIBA (Recombinant Blot Assay or Western blots) prezintă acurateţe mai crescută, dar este mai costisitor decât EIA, prin urmare este folosit pentru confirmare.
Testele pentru anticorpii HCV sunt de trei generaţii:1. Generaţia I (1989), a fost primul test comercial la îndemâna laboratoarelor. Acesta detectează anticorpi împotriva antigenului C100-3 derivat din regiunea nestructurală de HCV (NS3 si NS4). Rezultatele fals pozitive au fost între 5-25%, iar perioada liberă (perioada între infecţie şi seropozitivitate) până la 6 luni.2. Generaţia II (1991) detectează anticorpi împotriva altor antigene: C22 (regiunea core), C33c (regiunea NS3) şi C200 (NS3 si NS4). Testul prezintă sensibilitatea şi specificitatea crescute şi reduce perioada liberă. 3. Generaţia III (1995) conţine un epitop adiţional nestructural (Ns5)Reacţiile fals pozitive pot fi datorate:
- prezenţei factorului reumatoid- concentraţiei crescute de imunoglobuline
9) HCV RNA (PCR and bDNA), (valoarea normală Negativ)Acesta este cel mai sensibil test care determină prezenţa HCV. Genomul viral este prezent în sânge în cantităţi mici şi trebuie amplificat pentru a fi detectabil (PCR poate să amplifice de milioane de ori).
După infecţie, HCV RNA este cel mai timpuriu test care devine pozitiv, fiind detectabil la 2 săptămâni după expunerea virală (diagnosticul de hepatită C acută). Acest test confirmă diagnosticul în cazul: - pacienţilor anti-HCV pozitivi, dar cu transaminaze normale;- pacienţilor imunocompromişi (AIDS, transplant, insuficienţă renală cronică); nu produc anticorpi.
10) Încărcarea viralăEste cantitatea de virusuri prezentă în circulaţie. Acesta este un test cantitativ, efectuat cu aceleaşi tehnici folosite pentru

54
Dr. Mariana Tent
In the last 10 years, microdermabrasion (MDA) has risen impressively in popularity, both among professionals and the public (Lloyd, 2001). MDA is a process using aluminium oxide crystals (ceramic, inert) or other abrasive materials, most of the time combined with negative pressure (vacuum), for the partial ablation of the epidermis (Spencer, 2005). The 3rd generation of the MDA equipment has already been developed. It features a completely closed circuit for the crystals, disposable crystals containers, electronic controls for the vacuum power and for the crystal consumption. To suggest the level of the MDA' popularity it should be noted that, in 2002, the American Society for Aesthetic Plastic Surgery has reported MDA to rank No. 2 in nonsurgical procedures, after Botulinum toxin injections.
In this article, the authors review the studies published in academic journals (1995-2007), dealing with practical and theoretical aspects of the procedure. After shortly exploring the mechanism of action, the MDA' efficacy is analyzed (as it is proven by the changes it produces). The authors present the skin's both structural changes (histopathology and clinical effects) and functional changes (the effects on the barrier function and the permeation of topicals). Some of the clinical indications are then presented and, finally, the complications, the advantages, and the disadvantages of the method are discussed.
1. The mecanism of actionAlthough MDA is widely used in practice, the mechanism by wich the strucural and functional changes are promoted is poorly understood. Spencer (2005) emphasizes that, during a regular MDA treatment, the ablation of the epidermis is only superficial and no real wound is produced. Nevertheless, important changes have been found in the dermis. Tan et al (2001) performed histology studies and noted dramatic vascular changes in the reticular dermis. They have atributed these changes to the effects of vacuum. On the other hand, Karimipour et al (2006) have proven that, although the vacuum alone produces molecular changes in the dermis, both the vacuum and the abrasion are needed to activate all the genes involved in the dermal remodeling.
2. EfficacyClinical trials verifying the efficacy and the safety of MDA are scarce, they are conducted in academic settings, on small samples (usually without the industry interference). The lack of scientific data to support the wide popularity of the method is probably due to the fact that FDA has approved the use of MDA without claiming such clinical trials (Spencer, 2006). Most of these trials' protocols are based on series of 4-8 MDA sessions at 7 or 10-day intervals, but no definite guidelines regarding the treatment's technique have been adopted. This could be a disadvantage, as it is believed the MDA' effects are technique dependent and, finding the right treatment protocol could increase the benefits
Modern Peeling Methods: Microdermabrasion (Mechanical Peeling)
Metode moderne de peeling: microdermabraziunea(peeling mecanic)În ultimii 10 ani, microdermabraziunea (MDA) a crescut mult în popularitate, atât în rândul medicilor, cât şi al pacienţilor (Lloyd, 2001). MDA este un proces care utilizează cristalele de oxid de aluminiu (material ceramic, inert) sau alte substanţe abrazive, de cele mai multe ori în asociere cu presiunea negativă (vacuum), pentru a produce peeling mecanic la nivelul epidermului (Spencer, 2005). Cristalele sunt puse în mişcare prin acţiunea presiunii negative, lovesc epidermul prin intermediul piesei manuale aplicate pe tegument (de obicei oblic, la 45º) şi realizează o ablaţie parţială. Aparatele de MDA au ajuns deja la a treia generaţie. Circuitul prin care sunt circulate cristalele abrazive spre piesa manuală este complet închis, iar puterea vacuumului sau cantitatea de cristale care realizează abraziunea sunt controlate electronic. Pentru a sugera dimensiunea popularităţii metodei, este de remarcat că, în 2002, Societatea Americană de Chirurgie Plastică a raportat că MDA ocupă locul 2 în topul celor mai utilizate proceduri nechirurgicale, dupa injecţiile cu toxină botulinică.
În acest articol, autorii trec în revistă studiile publicate în jurnalele academice având ca subiect diverse aspecte practice sau toretice ale procedurii. După scurte consideraţii privind mecanismul prin care acţionează, este studiată eficacitatea MDA, aşa cum este tradusă prin modificările pe care le promovează. Sunt raportate atât modificările structurale (histopatologice şi clinice), cât şi modificările funcţionale (cu accent pe efectul asupra funcţiei de barieră a pielii şi asupra absorbţiei substanţelor administrate topic). Sunt dezbătute apoi câteva dintre aplicaţiile clinice ale metodei. În final, sunt prezentate complicaţiile, avantajele, cât şi dezavantajele metodei.
1. Mecanism de acţiuneDeşi MDA este o procedură larg folosită, mecanismul prin care se produc modificările structurale şi funcţionale la nivelul pielii este puţin cunoscut. Spencer (2005) remarca faptul că, în timpul unui tratament obişnuit cu MDA, ablaţia epidermului este superficială şi nu se produce o rană adevarată. Totuşi, deşi se lucrează superficial, apar modificări importante în derm. Tan et al (2001) au demonstrat prin studii de histologie, că la nivelul dermului reticular se produc modificări vasculare dramatice şi au atribuit aceste modificări acţiunii vacuumului. Pe de altă parte, Karimipour et al (2006) au descoperit că, deşi vacuumul aplicat în monoterapie produce modificări moleculare la nivelul dermului, este nevoie şi de componenta abrazivă a MDA pentru a activa toate genele implicate în remodelarea dermului. Se pare, deci, că este nevoie de ambele componente, vacuum şi ablaţia parţială a epidermului, pentru a obţine efectul optim.
2. Eficacitate Studiile clinice având ca scop stabilirea profilului de eficacitate şi siguranţă al MDA nu sunt numeroase, includ loturi mici de pacienţi şi au fost efectuate în medii academice, fără intervenţie din partea industriei producătoare de aparatură. Probabil că situaţia se datorează faptului că FDA a aprobat utilizarea MDA fără a cere


56
of the method (Alam et al, 2002). Nevertheless, a body of scientific evidence has emerged to objectively support the MDA efficacy (Hernandez-Perez and Ibiett, 2001).
2.1 Structural changes a. HistopathologyKarimipour et al (2005) found that, despite minimal injury to the epidermis, MDA produces epidermal and dermal remodeling similar with wound healing. The authors propose to study further the timing of the molecular cascades triggered by MDA, in order to improve the MDA' outcomes by adopting the optimal number of treatments and the optimal interval between the sessions. Coimbra et al (2004) studied the MDA' effect on the thickness of the epidermis and found an increase from 103 +/- 23 [mu]M - before the treatment to 148 +/- 41 [mu]M – after MDA. The authors also reported an increase of the organized collagen in the treated area. The 2001 studies conducted independently by Freedman et al and by Tan et al, confirm that MDA produces clinical improvements via a mechanism of action similar to the dermal and epidermal healing of the wounds. The authors have described the thickening of the epidermis and the dermis, the flattenting of rete ridges, vascular ectasia, perivascular mononuclear cell infiltrate and the hialinization of the papilar dermis, with new collagen and elastin fibers.
The changes have been found 1 week after a series of MDA treatments. Shim et al (2001) note among the MDA' chronic effects, the hyperplasia of the epidermis, the increase of the elastin and the decrease of the melanization. They also describe the acute effect, the homogenized and compacted stratum corneum. Bark-Lynn et al (2006) certify changes in the epidermis ceramide level (lipids barrier), that is, the level increases after the first 2 sessions and, subsequently, returns to the normal level.
b. Clinical changesSpencer and Kurtz (2006) note that the parameters they have measured (superficial lines, pigmentation, enlarged pores, general appearance) have shown significant improvement after the first 3 treatments and continued to improve throughout the study (6 MDA sessions for the treatment of photodamage) The colorimetry has shown the continuing increase in the brightness of the skin and the descrease of the dulness. The patients have confirmed the improvements. In another study, Coimbra et al (2004) confirm that patients are very pleased with the results and the investigators note significant improvements of the discromia characteristic to photoaged skin. Additionaly, Hernandez-Perez and Ibiett (2001) report clinical and histopathology improvements in all their patients treated for photoaging and for all the parameters they tested (sebum, the thickness of the epidermis and dermis, dilated pores, general appearance). Another study (Shim et al, 2001) has reported significant improvement in the skin texture, pigmentation and general appearance, but more modest results for deeper wrinkles. Post-acne scars have been improved in some cases and needed deeper ablation. Tan et al (2001) discovered that, immediately after the treatment, the skin temperature increases, the sebum quantity decreases and a temporary increase in firmness and elasticity, as well as a slight reduction of the wrinkles, appear.
producătorilor să efectueze astfel de studii (Spencer, 2006). Majoritatea studiilor au adoptat ca protocol terapeutic efectuarea unor serii de 4-8 şedinţe spaţiate la 7-10 zile, dar nu există scheme unitare privind tehnica de tratament. Este o carenţă, deoarece se bănuieşte că efectele MDA sunt în mare măsură dependente de protocolul terapeutic şi de tehnica de operare (Alam et al, 2002). Chiar şi aşa, s-au acumulat deja dovezi obiective privind eficacitatea MDA (Hernandez-Perez şi Ibiett, 2001).
2.1 Modificări structurale a. HistopatologiceKarimipour et al (2005) au demonstrat că MDA activează cascade moleculare care produc remodelarea dermică similar cu vindecarea rănilor, cu toate că injuria adusă epidermului este minimă şi nu se provoacă o rană (exceptând unele indicaţii ale MDA unde ablaţia se face mai profund). Autorii văd o consecinţă practică în această descoperire, care poate furniza un ghid în elaborarea unor protocoale terapeutice care să prevadă numărul şi spaţierea sesiunilor de MDA pentru obţinerea rezultatelor optime. Coimbra et al (2004) au urmărit evoluţia grosimii epidermului, care a fost 103 +/- 23 [mu]M înainte de tratament, ajungând la 148 +/- 41 [mu]M după MDA. Autorii au descoperit şi o creştere a cantităţii de colagen organizat în ariile tratate, comparativ cu cele netratate. Studiile din 2001 efectuate independent de Freedman et al şi de Tan et al confirmă că MDA produce ameliorări clinice prin mecanisme asemănătoare proceselor reparatorii atât la nivel epidermic cât şi dermic. Ei au descris îngroşarea epidermului şi a dermului, aplatizarea crestelor interpapilare, ectazie vasculară, infiltrat inflamator perivascular şi hialinizarea dermului papilar, cu depunere de fibre noi de colagen şi elastină. Efectele au fost demonstrate la o săptămână după încheierea unei serii de MDA. Shim et al (2001) constată că, printre efectele cronice ale MDA, se numără hiperplazia epidermului, creşterea cantităţii de elastină şi scăderea melanizării. Ca efect imediat, autorii citează omogenizarea şi compactarea stratului cornos. Bark-Lynn et al (2006) certifică modificări ale nivelului ceramidelor (barierei lipidice) la nivelul epidermului (cantitatea creşte după primele două şedinţe, apoi revine la normal).
b. CliniceSpencer şi Kurtz (2006) au constatat că variabilele clinice măsurate în studiul lor (riduri superficiale, pigmentare, pori lărgiţi, aspect general) s-au ameliorat semnificativ după primele 3 tratamente şi au continuat să se amelioreze până la sfârşitul studiului (6 şedinte pentru tratarea semnelor de foto-îmbătrânire). Colorimetria a demonstrat creşterea continuă a luminozităţii şi reducerea aspectului tern al pielii. Pacienţii au confirmat ameliorările. Într-un alt studiu, Coimbra et al (2004) confirmă că pacienţii au fost foarte satisfăcuţi de rezultate, iar investigatorii au notat ameliorări semnificative în ceea ce priveşte discromiile pielii foto-îmbătrânite. La rândul lor, Hernandez-Perez şi Ibiett (2001) au raportat ameliorare clinică şi histopatologică la toţi subiecţii trataţi pentru foto-îmbătrânire şi pentru toţi parametrii testaţi (sebum, grosimea dermului şi epidermului, pori dilataţi, aspect general). Într-un studiu din 2001, Shim et al au obţinut ameliorări semnificative statistic în ceea ce priveşte textura, pigmentarea şi aspectul general al pielii, dar rezultate modeste în cazul ridurilor mai profunde. Cicatricile postacneice au fost ameliorate în unele

57
2.2 Functional changesSome authors have been preoccupied by the effects MDA could have on the functions of the epidermis, especially the barrier function. While some have proposed MDA to be a new method for enhancing the delivery of topicals through the epidermis (Woan-Ruoh et al, 2006), others have sought to quantify the effects of the barrier function disruption after MDA (Song et al, 2004).
Rajan and Grimes (2002) find that MDA significantly increases the TEWL 24 hours after the treatment and this could spell out acute damage to the barrier function. On the contrary, they note, 7 days after MDA, the TEWL level drops beneath the baseline level. This means that the acute damage is subsequently replaced by the actual strengthening of the barrier function. Additionaly, the epidermis moisture binding capacity is increased. Song et al (2004) compare MDA' and glycolic acid peel's effects on the barrier function. Both methods produce significant damage acutely, but the damage is less severe after MDA. For both methods, the barrier function is completely recovered 24 hours later. In practice, the temporary disruption of the barrier warrants additional care for the skin during the first 24 hours after the procedure. If erythema occurs, it is more severe after glycolic acid and it dissapears after 1 day, for MDA and 4 days, for glycolic acid.
As regards MDA' proposed enhancement of the epidermal permeation of topicals, Fang et al (2004) have studied this effect for ALA (hydrophilic substance, precursor for protoporphirin IX - used in photodynamic therapy). The authors reported 5-15 fold higher epidermal permeation of ALA in the treated area. Woan-Ruoh et al (2006) confirmed the increase of the epidermal permeation of hydrophilic substances. The authors used 5-FU and the permeation was 8-24 fold higher. It has also been noted that the increase is technique dependent (vacuum power, number of passes over one area). Fujimoto et al (2005) have tried to quantify the treatment's parameters to better control the fraction of the epidermis that is removed. The authors postulate that the key parameters are the duration of the handpiece contact with the skin (L) and the vacuum power (V). According to their theory, the epidermal permeation is a direct function of the multiplication of the parameters (L×V), that is, the barrier decreases and the permeation increases with the length of the treatment and the vacuum strength (permeation increases with the depth of the ablation).
3. IndicationsSpencer notes in 2005 that the clinical use of the method has grown rapidly. Relatively superficial skin problems are treated: photo- and chronodamage, hyperpigmented lesions (melasma, lentigines), acne, scars, stretch marks (Hernandez-Perez, 2001).
Some authors have reported good results after employing MDA (in series of treatments) for photodamage (Freedman et al, 2001; Coimbra et al, 2004; Spencer si Kurtz, 2006). Others recommend combination therapies, that is, MDA with chemical peels: TCA 15% (Cotellessa et al, 2003), retinoic acid 5% (Hexsel, 2005), glycolic acid (Briden et al, 2007), or MDA with laser 1064 nm Nd:YAG (Guttman, 2002).
The acne severity classes that are suited for MDA treatment are still being investigated. Seborrhea (with dilated pores) and comedone acne are widely accepted indications
cazuri, acestea necesitând ablaţie mai profundă. Tan et al (2001) au descoperit că, imediat după tratament, temperatura tegumentului creşte, cantitatea de sebum scade şi se constată o creştere temporară a fermităţii şi elasticităţii pielii şi o uşoară aplatizare a ridurilor.
2.2 Modificări funcţionale O serie de autori au fost preocupaţi de efectul pe care MDA l-ar putea avea asupra funcţiilor epidermului, cu precădere funcţia de barieră. În vreme ce unii au emis ipoteza că MDA ar putea fi o nouă metodă de facilitare a penetrării substanţelor active în tegument (Woan-Ruoh et al, 2006), alţii au căutat să cuantifice eventualele efecte negative ale alterării funcţiei de barieră (Song et al, 2004).
Rajan şi Grimes (2002) au constatat că MDA este urmată de o creştere semnificativă statistic a pierderii transcutanate de apă (TEWL) la 24 de ore după procedură, ceea ce s-ar putea traduce ca afectare acută a funcţiei de barieră. Dimpotrivă, după 7 zile, nivelul pierderii transcutanate de apă scade sub cel dinainte de tratament, deci scăderea acută este înlocuită ulterior de o îmbunătăţire a funcţiei de barieră. În plus, la 24 de ore după MDA s-a constatat şi o creştere a hidratării stratului cornos. Song et al (2004) au comparat efectele MDA şi ale peelingului chimic cu acid glycolic asupra funcţiei de barieră. Ambele metode produc daune semnificative asupra funcţiei de barieră imediat după procedură, dar daunele sunt mai puţin severe după MDA. Pentru ambele proceduri, funcţia de barieră a fost recuperată după 24 de ore. Concluzia practică ar fi că în primele 24 de ore după MDA, pielea necesită îngrijiri suplimentare, pentru a compensa afectarea temporară a barierei epidermice. În ce priveşte eritemul, acesta a fost mai sever după acid glycolic. Eventualul eritem dispare după o zi în cazul MDA şi după 4 zile în cazul acidului glycolic.
În ceea ce priveşte efectul benefic de creştere a absorbţiei topicelor aplicate după MDA, Fang et al (2004) au studiat efectul microdermabraziunii asupra permeabilităţii epidermului pentru ALA (substanţa hidrofilă, precursor de protoporfirină IX - folosită în terapia fotodinamică). S-a constatat că absorbţia cutanată a ALA este de 5-15 ori mai mare în zonele tratate prin MDA comparativ cu zonele intacte. Woan-Ruoh et al (2006) au confirmat creşterea absorbţiei transcutanate a substanţelor hidrofile. Autorii au folosit 5-FU şi creşterea a fost de 8-24 de ori faţă de normal. S-a constatat, de asemenea, că efectul de facilitare a absorbţiei depinde de tehnica şi parametrii de tratament (intensitatea vacuumului şi numărul de pase efectuate peste o suprafaţă). Fujimoto et al (2005) au încercat să cuantifice parametrii de tratament pentru a controla mai exact fracţiunea din stratul cornos îndepartată prin MDA. Autorii au postulat că parametrii determinanţi sunt durata de contact a piesei manuale cu pielea (L) şi puterea vacuumului (V). Astfel, susţin autorii, rata de absorbţie a substanţelor topice se corelează direct proporţional cu L×V (bariera scade şi absorbţia creşte dacă se folosesc valori mai mari pentru vacuum şi dacă tratamentul este mai îndelungat, ceea ce face ca ablaţia să fie mai profundă).
3. Indicaţii Spencer remarca în 2005 că utilizarea acestei metode s-a extins foarte rapid. Sunt tratate o serie de afecţiuni relativ superficiale, de la semnele foto-şi crono-îmbătrânirii la leziuni hiperpigmentate

58
(Freeman, 2001; Spencer, 2005). Papulo-pustular acne is accepted by some (widely used in practice) and rejected by some (widely used in practice) and rejected by others, but clearly there is not enough scientific evidence (clinical trials) to support either sides. Lloyd (2001) has conducted a pilot study, investigating the usefulness of MDA in treating grade II-III acne. The protocol was based on 8 MDA sessions with 7 to 10-day intervals and the results were promising. 71% of the patients achieved more than 50% improvement and the most prominent results were seen with postinflammatory acne changes and the overall skin quality. Typical of MDA, the questionnaires showed the positive perceptions among patients, as 92% of them noticed the improvement in their skin and 96% were pleased with their peel results and would recommend the method to others.
Freeman (2001), Mala and Gurvinder (2006), Spencer (2006) recommend MDA in the treatment of scars, post-acne scars and melasma. The results are better with combination therapy (MDA and topical treatment). Cotellessa et al (2003) demonstrate in their trial that MDA, both alone and in combination with TCA 15%, is effective and well tolerated in the treatment of melasma. Tsai (1995) studied MDA' efficacy in treating the facial scars. Of 41 patients, all achieved good/excellent results after an average of 9 MDA sessions.
4. Complications. Advantages of MDAMDA is a mechanical peeling method and produces only minimal injury to the skin (Tope and Kageyama, 2001). Lloyd (2001) emphasizes that MDA' advantage over other forms of peeling is the ability to offer a non-surgical, non-chemical, minimal invasive procedure, easy to control and free of the manipulation of any form of energy to the skin. Additionaly, no anesthesia is required (Tsai, 1995). Koch and Hanason (2001) add to the advantages the fast results, the safety and the lack of downtime for the patient. Indeed, claim Tope and Kageyama (2001), the less invasive a method is, the shorter the recovery time. Tsai (1995) and Lloyd (2001) have found that MDA is very well tolerated and yields a high satisfaction rate among patients, increasing patients' compliance and adherence to the treatment. Most probably, MDA' safety profile and the lack of complications are among its bigest strenghts. Coimbra et al (2004) claim in their study they have not registered infections, scars or discromia and Lloyd (2001) mentions erythema being the sole inconvenient of the method (it fades away in 24 hours). And, finally, the cost of the equipment and the training necessites are relatively modest (Koch and Hanason, 2001).
5. DisadvantagesTope and Kageyama (2001) mention the big disadvantage being the less impressive results, compared to more aggresive/destructive methods. Additionaly, the results could be temporary, warranting for maintenance sessions. The authors postulate the efficacy and lastingness of a resurfacing method is directly linked to the depth of the wound, the length of the recovery time, or both. On the other hand, there is a growing demand from the public for effective and minimal invasive methods, with minimal interference with everyday life.
6. ConclusionsMDA has become one of the most performed peeling methods -superficial resurfacing (Grimes, 2005). Already there is a
(melasma, lentigine), acnee, cicatrici, vergeturi (Hernandez-Perez, 2001).
Mai mulţi autori au demonstrat că utilizarea MDA (în tratamente multiple) pentru ameliorarea semnelor asociate cu fotoîmbătrânirea determină rezultate bune (Freedman et al, 2001; Coimbra et al, 2004; Spencer şi Kurtz, 2006). Alţii au recomandat utilizarea MDA în terapii combinate cu peeling chimic, de exemplu TCA 15% (Cotellessa et al, 2003), acid retinoic 5% (Hexsel, 2005), acid glycolic (Briden et al, 2007) sau cu laser 1064 nm Nd:YAG (Guttman, 2002).
Formele clinice de acnee care se pretează la tratament prin MDA sunt încă în curs de investigare. Seboreea (şi porii dilataţi) şi acneea comedoniană sunt indicaţii unanim acceptate deja (Freeman, 2001; Spencer, 2005). Acneea papulo-pustuloasă este o indicaţie acceptată în unele ţări şi contestată în altele. Este subiectul mai multor studii în curs de desfăşurare (Karimipour et al – la Universitatea din Michigan, Diaconeasa et al – studiu multicentric în România). Lloyd (2001) a efectuat un studiu pilot având ca subiect tratamentul acneei de grad II-III prin MDA. Protocolul terapeutic a prevăzut 8 şedinţe spaţiate la 7-10 zile, iar rezultatele au fost mai mult decât promiţătoare. 71% dintre pacienţi au obţinut o ameliorare mai mare de 50%. Cele mai importante ameliorări au fost legate de leziunile post-inflamatorii şi de calitatea generală a pielii. Caracteristic pentru MDA, chestionarele adresate pacienţilor demonstrează percepţia pozitivă pe care MDA o determină în rândul pacienţilor. 92% dintre subiecţii acestui studiu au remarcat o îmbunătăţire a aspectului pielii, iar 96% dintre pacienţi au fost plăcut impresionaţi de rezultate şi au declarat că vor recomanda metoda şi altor pacienţi.
Freeman (2001), Mala şi Gurvinder (2006), Spencer (2006) recomandă MDA în tratamentul cicatricilor post-acneice şi al melasmei. Rezultate superioare se obţin când se asociază şi tratament topic. Cotellessa et al (2003) demonstrează într-un studiu clinic că microdermabraziunea, atât în monoterapie cât şi în terapie combinată cu TCA 15%, este o metodă eficientă şi bine tolerată pentru tratamentul melasmei. Tsai (1995) a studiat eficacitatea MDA în tratamentul cicatricilor faciale. Din totalul de 41de pacienţi trataţi, toţi au avut ameliorări clinice bune/excelente, având nevoie în medie de aproximativ 9 sedinţe de tratament.
4. Complicaţii. Avantajele MDMDA se bazează pe peeling mecanic şi determină o injurie minimă asupra pielii (Tope si Kageyama, 2001). Lloyd (2001) subliniază că avantajul MDA faţă de alte metode de peeling este abilitatea de a oferi o procedură non-chirurgicală, non-chimică, neinvazivă, uşor de controlat şi fără manipularea unor surse de energie luminoasă sau de altă natură la nivelul pielii. În plus, nu necesită anestezie (Tsai, 1995). Koch şi Hanason (2001) adaugă la avantaje rezultatele rapide, siguranţa şi timpul de recuperare foarte scurt. Într-adevăr, remarcau Tope şi Kageyama (2001), cu cât o metodă este mai puţin invazivă, cu atât este mai scurtă perioada neplăcută de recuperare. Tsai (1995) şi Lloyd (2001) constată că MDA este foarte bine tolerată şi determină un grad foarte mare de satisfacţie în rândul pacienţilor, ceea ce creşte mult complianţa şi aderenţa la tratament. Probabil că siguranţa metodei şi absenţa complicaţiilor este unul dintre punctele forte ale MDA. Coimbra et al (2004) menţionează în studiul lor că nu au înregistrat infecţii sau cicatrici,

59
scientific and practical body of evidence proving MDA' effectiveness. It is likely that the effects are produced by the combination between abrasion and negative pressure. The histology and clinical changes have been certified by monitoring objective parameters in clinical trials. As regards the functions of the skin, the most promising consequence of MDA could be the increase of the epidermis permeation of topicals. The indications are numerous and include relatively superficial problems of the skin. The simplicity, suitability for combination treatments, lack of complications, good tolerability and patients' acceptance and the lack of downtime are among the arguments imposing the method.At the same time, Grimes (2005) notices the discrepancy between MDA' popularity and the relatively small number of clinical trials supporting scientifically the results and the observations from practice. More clinical trials would allow the substatiation of treatment guidelines for improving the results, as it is believed the results are technique dependent. Conducting well designed clinical trials, using objective criteria, as well as studies attesting MDA results on the long run, represent an opportunity and challenge for the researchers in dermatology (Mala and Garvinder, 2006).
References:Bark-Lynn, L., Yunhi, C. and Mu-Hyoung, L. (2006) Effect of Serial Microdermabrasion on the Ceramide Level in the Stratum Corneum. Dermatological Surgery. 32(3), p. 376
Briden, E., Jacobsen, E. and Johnson, C. (2007) Combining superficial glycolic acid (alpha-hydroxy acid) peels with microdermabrasion to maximize treatment results and patient satisfaction. Cutis. 79(1), p. 13-16
Coimbra, M., Rohrich, R.J., Chao, J., Brown, S.A. (2004) A prospective controlled assessment of microdermabrasion for damaged skin and fine rhytides. .Plast Reconstr Surg. 113(5), p. 1438-1443
Cotellessa, C., Peris, K., Fargnoli, M.C., Mordenti, C., Rita Sparacio Giacomello, R.S. and Chimenti, S. (2003) Microabrasion Versus Microabrasion Followed by 15% Trichloroacetic Acid for Treatment of Cutaneous Hyperpigmentations in Adult Females. Dermatologic Surgery. 29(4), p. 352
Fields, K.A. (2000) Skin breakthroughs in the year 2000. Int J Fertil Women Med, 45(2), p. 175-181
Freedman, B.M., Rueda-Pedraza, E., Waddell, S.P. (2001) The epidermal and dermal changes associated with microdermabrasion. Dermatol Surg. 27(12), p. 1031-1033.
Fujimoto, T., Shirakami, K. and Tojo, K. (2005) Effect of microdermabrasion on barrier capacity of stratum corneum. Chem Pharm Bull (Tokyo), 53(8), p. 1014-1016
Hernandez-Perez, E., Ibiett, E.V. (2001) Gross and microscopic findings in patients undergoing microdermabrasion for facial rejuvenation. . Dermatol Surg. 27(7), p. 637-640
Hexsel, D., Mazzuco, R., Dal'forno, T. And Zechmeister, D. (2005) Microd ermabrasion followed by a 5% retinoid acid chemical peel vs. a 5% retinoid acid chemical peel for the treatment of photoaging - a pilot study. Journal of Cosmetic Dermatology. 4(2), p. 111-116
Karimipour DJ; Kang S; Johnson TM; Orringer JS; Hamilton T; Hammerberg C; Voorhees JJ; Fisher G (2005) Microdermabrasion: a molecular analysis following a single treatment. J. Am. Acad. Dermatol. 52(2), p. 215-223
Karimipour, D.J., Kang, S., Johnson, T.M., Orringer, J.S., Hamilton, T., Hammerberg, C., Voorhees, J.J., Fisher, G. (2006) Microdermabrasion with and without aluminum oxide crystal abrasion: a comparative molecular analysis of dermal remodeling. J. Am. Acad. Dermatol. 54(3), p. 405-410.
Koch, R.J., Hanasono, M.M. (2001) Microdermabrasion. Facial. Plast. Surg. Clin. North. Am. 9(3), p. 377-382
Lloyd, J.R. (2001) The Use of Microdermabrasion for Acne: A Pilot Study. Dermatologic Surgery. 27 (4), 329–331.
Mala, B. and Gurvinder, P.T. (2006) Microdermabrasion: Reappraisal and Brief Review of Literature. Dermatologic Surgery. 32 (6), 809–814.
Rajan, P. and Grimes, P.E. (2002) Skin Barrier Changes Induced by Aluminum Oxide and Sodium Chloride Microdermabrasion. Dermatologic Surgery. 28 (5), p. 390–393.
Shim, E.K., Barnette, D., Hughes, K., Greenway, H.T. (2001) Microdermabrasion: a clinical and histopathologic study. Dermatol. Surg. 27(6), p. 524-530
Shpall R, Beddingfield FC, Watson D, Lask GP: Microdermabrasion: a review. . Facial Plast Surg 2004; 20(1): 47-50
iar Lloyd (2001) citează ca unic inconvenient posibilitatea apariţiei eritemului, care însă dispare în maxim 24 de ore. Nu în ultimul rând, costul echipamentului pentru MDA şi necesităţile de training sunt modeste (Koch şi Hanason, 2001).
5. DezavantajeTope si Kageyama (2001) remarcă faptul că marele dezavantaj al MDA este acela că rezultatele sunt mai puţin impresionante ca rezultatele obţinute prin tehnici agresive. De asemenea, rezultatele pot fi temporare, pacienţii necesită tratament de întreţinere. Ei concluzionează că eficacitatea şi durabilitatea ameliorărilor clinice par a fi direct proporţionale cu adâncimea rănii provocate, cu lungimea perioadei de recuperare, sau cu ambele variabile. Pe de altă parte, există o cerere din partea pacienţilor pentru metode eficiente şi puţin invazive, care să nu interfereze cu viaţa de zi cu zi.
6. ConcluziiMicrodermabraziunea a devenit una dintre cele mai des folosite metode de peeling - superficial resurfacing (Grimes, 2005). Există deja o bază ştiinţifică şi una practică ce atestă eficacitatea MDA. Este probabil că efectele MDA sunt determinate de combinaţia dintre abraziune şi vacuum. Modificările histopatologice şi clinice au fost confirmate folosind monitorizarea unor parametri obiectivi. Din punct de vedere funcţional, poate cea mai promiţătoare consecinţă a MDA este creşterea absorbţiei unor substanţe active administrate topic. Aplicaţiile MDA sunt multiple şi se referă mai ales la afecţiuni cantonate în zonele relativ superficiale ale pielii. Simplitatea, posibilitatea de a combina MDA cu alte metode, absenţa complicaţiilor, buna tolerabilitate şi acceptare din partea pacienţilor, ca şi recuperarea extrem de rapidă sunt câteva argumente care au impus această metodă.
În acelaşi timp, Grimes (2005), remarcă faptul că există o discrepanţă între popularitatea MDA în practica de zi cu zi şi numărul relativ mic de studii clinice care să suplimenteze cu date ştiinţifice aprofundate observaţiile din practică şi să permită propunerea unor protocoale terapeutice optime. Se bănuieşte că rezultatele sunt dependente de tehnica de tratament. Realizarea unor trialuri clinice cu protocoale bine construite, folosind criterii obiective de monitorizare, ca şi a unor studii care să ateste efectele MDA pe termen lung, reprezintă o cerinţă pentru viitor şi o oportunitate pentru investigatorii din dermatologie (Mala şi Garvinder, 2006).
Spencer, J.M. (2005) Microdermabrasion. Am. J. Clin. Dermatol. 6(2), p. 89-92
Spencer, J.M. and Kurtz, E. S. (2006) Approaches to document the efficacy and safety of microdermabrasion procedure. Dermatologic surgery. 32(11):1353-7.Tan, M.H., Spencer, J.M., Pires, L.M., Ajmeri, J., Skover, G. (2001) The evaluation of aluminum oxide crystal microdermabrasion for photodamage. Dermatol. Surg. 27(11): 943-949.
Tsai, R.Y., Wang, C.N., Chan, H.L. (1995) Aluminum oxide crystal microdermabrasion. A new technique for treating facial scarring. Dermatol. Surg. 21(6), p. 539-542 Tope, W.D. and Kageyama, N. (2001) New methods in cutaneous resurfacing. Adv Dermatol. Vol. 17, p. 301-323.
Woan-Ruoh, L. et al (2006) Microdermabrasion as a Novel Tool to Enhance Drug Delivery via the Skin: An Animal Study. Dermatologic Surgery. 32(8), p. 1013–1022

60
ca terapie, propriile celule stem. De aceea recoltarea sângelui din cordonul ombilical, imediat dupa naştere, reprezinta o decizie înţeleaptã.În prezent, celulele stem sunt folosite în tratamente specifice unor afecţiuni cum sunt leucemia, cancerul si afectiuni autoimune. Oamenii de stiinţa apreciazã cã aceste celule stem vor avea un rol determinant in tratamentele viitoare şi vor fi aplicate multor alte afecţiuni.
De ce Cryo-Save?
? Suntem cea mai mare companie din domeniu din Europa având peste 100.000 de clienţi.? Personalul beneficiaza de îndrumare şi suport ştiintific permanent.? Livrãm kitul de recoltare în cel mai scurt timp de la formularea cererii.? Recuperãm kitul imediat dupa recoltarea sângelui din cordonul ombilical.? Avem experientã in prelevarea si stocarea celulelor stem.? Prelevarea celulelor stem este facutã conform standardelor internaţionale.? Beneficiem de participare si suport financiar in cadrul ITERA-Life Science Forum (International Tissue Engineering Research Association).? Suntem asiguraţi împotriva falimentului.? Avem metode corecte de depozitare? Oferim maxim de siguranţã.? Clienţii nostri pot conta pe confidenţialitate.? Laboratorul are acreditare NBN EN ISO 17025.? Depozitarea se face în douã tuburi criogenice speciale, de ultimã generaţie.? Depozitarea tuburilor criogenice se face in douã locaţii diferite din Belgia si Olanda - nici o altã bancã nu oferã aceastã variantã.
Life RenaissanceCal.Plevnei 137ATel/Fax 021.310.72.89Mob.0731.685.328www.celulestem.comwww.cryo-save.com
Cryo Save este liderul European al bancilor private de stocare a celulelor stem in urma procesului de recoltare a sangelui placentar la nasterea cop i lu lu i , cu pes t e 100 .000 de p robe de j a depozitate.Compania a fost infiintata in anul 2000 avand laboratorul central in Belgia,mai precis la Mechelen.Este prezenta in 36 de tari cu participare activa si oferind suport financiar forumului stiintific numit ITERA(International Tissue Eingeenering Research Association)localizat in ITERTAL Hospital -Germany,Bad-Achen avand in componenta sa 19 Universitati,19 Spitale Universitare,4 Spitale private.Din luna Iulie 2007 este reprezentata in Romania de catre societatea Life Renaissance oferind astfel posibilitatea parintilor din Romania de a beneficia de serviciile de stocare a celulelor stem in locatiile Cryo Save din Belgia si Olanda.Cu ajutorul serviciului Cryo-Cord, oferit de Cryo-Save, la naşterea copilului sunt prelevate un numar însemnat de celule stem. Recoltarea se face prin utilizarea unei proceduri simple, care nu implica nici mama, nici noul nascut.
Dupã ce mostra de sânge provenit din cordonul ombilical este procesatã în laboratorul nostru din Belgia, celulele stem recoltate sunt depozitate în douã recipiente speciale, de ultimã generaţie şi sunt stocate în douã locaţii diferite din Belgia si Olanda. Acestea sunt în permanenţã disponibile pentru un eventual tratament al copilului in cauza.Cea mai mare cantitate de celule stem care poate fi recoltata se aflã în cordonul ombilical,de aceea nasterea este momentul optim pentru recoltare. Celulele stem pot fi prelevate şimai tarziu, dar din pacate atât calitatea, cât şi cantitatea lor sunt semnificativ reduse.Prelevarea si stocarea celulelor stem din cordonul ombilical prezintã o serie de avantaje:? celulele pot fi stocate pe o perioada îndelungatã? în cazul unui eventual transplant nu apare riscul de rejectare? nu exista riscul infecţiei prin virusi sau alţi agenţi infectioşiCercetarile medicale indicã faptul cã în cazul unei afecţiuni majore se pot administra,
Depozitarea Celulelor STEM la CRYO SAVE LABS