Embed Size (px)
Citation preview

Anterior Cruciate Ligament Injury
Ed Mulligan, PT, DPT, OCS, SCS, ATC
Associate ProfessorD t t f Ph i l ThDepartment of Physical TherapyDallas, TX

Lets start with the …

ACL Epidemiology
Incidence Gender Preference MOI MOI

ACL Injury Incidence
250K injuries/year in US ‐ 100K surgeries/year in US
70% of injuries are non‐contact in nature
Incidence in athletic population over 10 years = 20%
Incidence at West Point Study over 4 years– Female = 3.5%; Males = 3.2%– When comparing common sportsp g p
Incidence ratio for females = 1.5
Multiple other studies suggest females 2 6 x higher incidence2‐6 x higher incidence

ACL Mechanism of Injury
Non‐contact (70%) Approaching 90% in females Approaching 90% in females
rotational, deceleration injury poor landing mechanics
Contact (30%)• Lateral contact valgus force
• ACL, MCL, meniscus• Terrible Triad (usually lateral meniscus
acutely and medial meniscus chronically)• Anterior Contact hyperextension
• ACL, PCL

ModifiableModifiableNEUROMUSCULARNEUROMUSCULAR
NonNon--ModifiableModifiableSTRUCTURAL
NEUROMUSCULARNEUROMUSCULARTiming and Control Adaptations TechniqueTiming and Control Adaptations Technique
Risk InfluenceRisk Influence
STRUCTURALNarrow NotchSmall ACL
↑ External Tibial Torsion
NonNon--ModifiableModifiableHORMONALcollagen strength
ModifiableModifiable
↑ External Tibial TorsionGenu Valgum
Genu Recurvatum
collagen strengthjoint laxity
ModifiableModifiableBIOMECHANICALBIOMECHANICAL
Extrinsic Factors Extrinsic Factors –– Shoes/Playing SurfaceShoes/Playing Surface↑ ↓↑ ↓↑ genu valgus and hip flexion angles; ↓ knee flexion s ffness during ↑ genu valgus and hip flexion angles; ↓ knee flexion s ffness during
athletic maneuversathletic maneuvers↑ STJ prona on/navicular drop↑ STJ prona on/navicular drop
Ligament Dominance Ligament Dominance –– Quadricep Dominance Quadricep Dominance –– Dominant Extremity Dominant Extremity Imbalance Imbalance –– CORE weaknessCORE weakness

Can we prevent ACL injury?
Meta‐analysis reveals a pooled risk ratio of 0.38 which represents a 62% decrease in risk for ACL rupture for those that participate in a preventiondecrease in risk for ACL rupture for those that participate in a prevention program– Stratified by Sex: 85% decrease in risk for males and 48% for females
Sadoghi et al, J Bone Joint Surg, 2012Sadoghi et al, J Bone Joint Surg, 2012
Theoretical analysis of cost efficiency shows that cost of training is $100 less per player/season and screening was $25 less per player/season th i t tithan no intervention
Bottom line – keep training costs under $200/player/season to “save money”
Swart et al, J Bone Joint Surg, 2014
Operative vs. Non-Op Considerations
• Activity level and demands on knee “ dif k t lif t l• “modify knee to lifestyle or modify lifestyle to knee”
• Degree of instability and associated injuries• Degree of instability and associated injuries• 1% increased risk for meniscal tear for each
month post‐injury up to 2 years
• Age, status of growth plates
• Patient motivations/compliance

Non-Op or Prehab Initial Points of Emphasis
Restore Joint Mobility PASSIVE t h i t t t i PASSIVE techniques to restore extension
– ottoman stretch– prone hangs
h i / lf h– hamstring/calf stretches Heel Slides; Wall Slides, and Stationary Cycling to restore flexion ROM
Restore Muscle PerformanceRestore Muscle Performance Quad and Ham Isometrics (augmented with E. Stim prn) 4 plane Straight Leg Raises
P t t t d i t i t l t d Progress to protected arc isotonics as tolerated

General Rehab Progression
Initiate Weight BearingPWB progressing to FWB as patient demonstrates a• PWB progressing to FWB as patient demonstrates a normal gait pattern
Mimic Function• Mini‐Squats• Heel Raises• Lateral Step UpsLateral Step Ups
Build muscular and cardiovascular endurance with ACL safe weight‐bearing activities
Initial Goals
Full ROMC ll bl b ff i Controllable or absent effusion
Good quad control 60 80% of uninvolved– 60‐80% of uninvolved
No extensor lag; normal gait Address kinesiophobia tendencies p
that are magnified in “non‐copers”Hartigan et al, J Orthop Sports Phys Ther, 2013
“quiet joint” quiet joint

Decision Making
Traditionally, we know that 20‐40% of appropriate patients40% of appropriate patients are successful with a non‐
operative approach
With the use of specific selection criteria, this success may , yincrease to as high as 80%

Non-Operative Candidate Evaluation
4 criteria that have been shown to correlate with a successful non operative (potential coper) approach are:successful non‐operative (potential coper) approach are:
1. > 80% on 20’ unilateral timed hop test2 > 80% score on KOS ADL Scale2. > 80% score on KOS ADL Scale3. > 60% on Global Rating Scale 4. No more than one “giving way” episode g g y p
since the original traumatic event
Fitzgerald GK, Axe MJ, Snyder‐Mackler L.JOSPT 30(4):194 203 2000
JOSPT 30(4):194‐203, 2000

ACL deficient copers, adapters, and non-copers have distinct differences in their pattern of gait recovery by 40 days post injury
Button K, et al, Brit J Sports Med, 2006

Critical Element of Rehabilitation
Perturbation Training
• Stork Standd• BAPS Board
• Bi/Multiaxial Boards• Roller Board Translations• Roller Board Translations• Tilt Board• Roller Board Stabilization

Critical Element of Rehabilitation
Perturbation Training
Re‐establishes neuromuscular control and d i t bilit th h d li f fdynamic stability through delivery of forces to the lower extremity in various directions when the patient is on an unstable or punpredictable surface
R i i iReaction training to unexpected forces

Delaware Perturbation Training Protocol
Roller Board Rocker Board Roller Board-Platform
detailed handout in your Article Resources folder

Extensive, Activity-Specific Agility/Running Program
– Bounds/Hops/Jumps– Walk – Jog – Run Progression– Figure 8s– Backpedaling– Sidestepping– Cariocas– Open and Crossover Cutsp– Starts and Stops

C it i B d P g i f Criteria-Based Progression for Return to Sport Phase Example Myer GD, J Orthop Sports Phys Ther, 2006
Structured, measurable objective criteria to guide terminal phasescriteria to guide terminal phases and return to athletic activities

Suggestions on Return to Sport JOSPT Theme Issue 42:4 – April 2012
Soccer – Skiing – Football – Basketball

Non-Operative Prognosis
Systematic Review– Good short to mid‐term outcomes in terms of knee function (87/100 Lysholm) andfunction (87/100 Lysholm) and performance (symmetrical hop tests), however, activity levels decreased on average by 21%
Muaidi QI, et al, Sports Med, 2007

Rehab + Early Reconstruction vs. Rehab Alone
RCT of 121 young, active adults62 surgical subjects
• 39 i t i t KOOS
59 non‐operative subjects (23 underwent delayed reconstruction)
39 i t i t KOOS
No significant between groups difference on SF‐36 or Tegner Activity Scale
• 39 point improvement on KOOS • 39 point improvement on KOOS
Tegner Activity Scale
Frobell RB, et al, N Engl J Med, 2010

P t O ti M tPost‐Operative ManagementACL Reconstruction

Surgical Variables
Graft– Tensile Strength
Surgeon variables– Preferencesg
– Single/Double Bundle– Auto vs. Allograft– Donor Source
– Protocols– Timing of Surgery
Patient goals/expectations Surgical considerations
– Surgical Approach– Graft Placement/Isometricity
Co‐morbidities present– Other ligament involvement– Meniscal health
– Intra‐operative graft tension– Method of fixation– Ligament augmentation– PRP
– Osteoarthritis– Osteochondral bruising
Rare to have an “isolated” injuryPRP– Physeal Status
j y

ACL Injury Pathoanatomy
“Isolated ACL tear” is misnomer– ACL only < 10%– Meniscus injuries ‐ 60‐75%“B b i ” MRI 80%– “Bone bruises” on MRI ‐ 80%
– Collateral ligament tears MCL & LCL: 5‐24%
– Articular cartilage injuries up to 46%

ACL R i ACL Reconstruction Time Frames for Healing
Process of ligamentization takes 12‐18 months
Between post‐op weeks 1‐6, avascular necrosis and revascularization occur simultaneously
l f l Complete graft revascularization takes 8‐20 weeks
One year post op until the graft One year post‐op until the graft resembles the vascular, histologic al, and structural properties of the native ACLthe native ACL

ACL R i ACL Reconstruction Criteria Based Progression
individualized decisions based on the patient’s function symptoms stability strength and motionfunction, symptoms, stability, strength, and motion …
rather than solely on therather than solely on the passage of time

Rehabilitation Pearls
Perfect surgery can be nullified by inappropriate rehabilitation ‐ perfect rehabilitation can not overcome inadequate surgery
All patients need to be challenged athletically
No specific protocol other than to PREVENT COMPLICATIONS
Improve overall conditioning without placing unnecessary stress on the healing graft
Slow down for allografts, hamstring grafts, concurrent g , g g ,meniscal repairs or articular cartilage procedures
Functional, activity specific rehab to retrain neuromuscular systems for anticipated demandsy p

ACL Rehab Points of Emphasis
Avoid flexion contractures and/or h fib iarthrofibrosis
the three most common complications of knee ligament surgery are:of knee ligament surgery are:
1. flexion contractures2. quadriceps weakness3. patellofemoral irritabilitythese complications are strongly interrelated
RA Sachs, DM Daniel, ML Stone, RF GarfeinAm. J. Sports Med., Nov 1989; 17: 760 - 765

How soon should you get full extension?
Early, aggressive passive extension training without any restriction does not affect post‐op knee laxity – Isberg, et al. Knee Surg Sports Traumatol Arthrosc. 2006
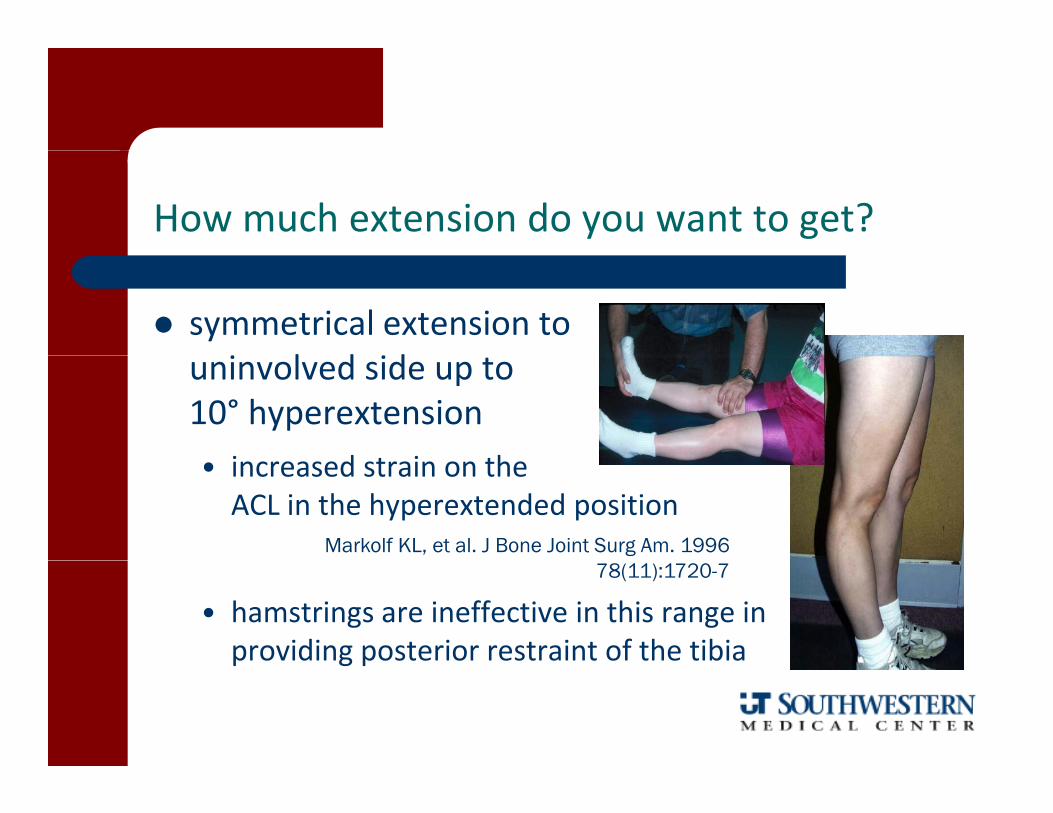
How much extension do you want to get?
symmetrical extension to i l d iduninvolved side up to 5‐
10° hyperextensioni d t i th• increased strain on the ACL in the hyperextended position
Markolf KL, et al. J Bone Joint Surg Am. 1996
• hamstrings are ineffective in this range in providing posterior restraint of the tibia
78(11):1720-7
p g p

ACL Rehab Points of Emphasis
• Prevent Osteoarthritis • a successful outcome is not how fast you get back to activity• a successful outcome is not how fast you get back to activity but what your knee looks like in 5‐15 years
• small deficits in terminal extension range increased presence of OA at 10 yearsincreased presence of OA at 10 years particularly if concurrent meniscal or articular cartilage damageShelbourne KD et al Am J Sports Med 2008Shelbourne KD, et al, Am J Sports Med, 2008
At 15 years the incidence of TKR is 1.4% ‐ this is 7 times higher than those who have not had an ACL reconstructionthan those who have not had an ACL reconstructionLeroux et al, J Bone Joint Surg, 2014
ACL Rehab Points of Emphasis
Monitor for Graft Stretch Outh ll h f l k f• theoretically, the graft progressively weakens from its original strength at implantation to its weakest point between 6‐12 weeks after surgery, and then begins to strengthen again
• this process continues for 12‐18 months

Theoretical Graft Strength Curve of a Patellar Tendon Autograft JOSPT, June 1992
16014 mm graft
120140
100ngth
14 mm graft
100
6080
40% s
tren 10 mm graft
02040%
12 24 36 52Weeks
820

Impact of Osteochondral Bone Bruise
80% of traumatic ACL injuries sustain osteochondral lesionsosteochondral lesions– more common with non‐contact MOI ‐
Viskontis, et al, AJSM, 2008– most common on lateral tibial plateau and
LFC (bruising on medial side associated with more severe injuries)Bisson, et al, AJSM, 2013
h k l These patients take a longer time to reach normal homeostasis (pain, swelling, ROM, NM control) and may have to delay reconstruction
MRI image of knee with a small geographic bone bruise in the weight-bearing lateral femoral condyle and an extensive bruise of the lateral tibial plateau in association with have to delay reconstruction
Johnson, et al. AJSM 28(2):152‐155, 2000
an ACL rupture

OOther Factors Associated with Poor Outcomes
In addition to severe osteochondrosis,
– Obesity (BMI > 30) had 0.35 times the odds of success
– Smoking had 0.36 times the odds of success
Kowalchuk DA, et al, Arthroscopy, 2009

ACL R h b P i f E h iACL Rehab Points of Emphasis
restoration of function through training of the neuromuscular recognitionthe neuromuscular recognitionof the “position of stability”
unilateral stance with kneeunilateral stance with knee flexed 20‐30°
t ti t l d i l idmust ensure patient loads surgical side as research indicates patients avoid symmetrical weight bearing for up to 6 months despite their
lack of perception of the asymmetrylack of perception of the asymmetry

Athletic Ready Position

Co-activation Exercise Activities
Begalle RL, J Athl Train, 2012

Appreciation for Quad Function
Quad inhibition/avoidance is common following ACL injuryI d k i 9 h Inadequate knee extension moments present 9 months post‐op
Ernst, et al Phys Ther 2000
Non‐copers adopt immature co‐contraction tendencies, altered hip/ankle movement strategies and function in more upright positionsmovement strategies and function in more upright positions
Chmielewski, et al Phys Ther 2005
Pre‐op quad strength is a significant predictor (better than demographic or other impairments) of self‐report outcomes at 6 monthsp ) p
Logerstedt D, Knee, 2013
Need to emphasize and progress quad function after patellar t d bidit ltendon morbidity resolves

Contrast of OKC and CKC Knee Extension JOSPT J 1992JOSPT, June 1992
20 Knee Extension with 25% BW
ant.tibial translation with leg extension at angles above 64 Yack, AJSM, 1993.
men
t (m
m) 16
12Squat with 25% BW
Knee Extension with 25% BW
Knee Extension
al Di
splac
e
8
4Squat
Tibi
0
4
Zone of SafetyZone of Safety
Knee Flexion Angle (°)
Anterior tibial displacement during active knee extension ( ith d ith t i t ) d t t ( ith
90° 60° 30° 0°
(with and without resistance) compared to a squat (with and without resistance) in chronic ACL deficient knees

Common Problems to Overcome:
1. Reflexive inhibition of the quadriceps
2 Tendency to hold the knee in2. Tendency to hold the knee in resting position 20‐30° flexion to accommodate swellingaccommodate swelling
3. Flexed knee gait
ACL Rehab Points of Emphasis
Used to prevent the onset of infrapatellar fat pad syndromeinfrapatellar fat pad syndrome(Paulos, 1987) that cause loss of sagittal plane motion and isg pcharacterized by exaggeratedpathological fibrous hyperplasiaf th t i ft tiof the anterior soft tissues
beyond that which is associatedwith normal healingwith normal healing

ACL Exercise Points of Emphasis
1. Dynamic control of valgus moment – avoid medical collapse2. Train hip and trunk control ‐ “avoid the corkscrew” (hip IR/add in landing)2. Train hip and trunk control avoid the corkscrew (hip IR/add in landing)3. Train the hip muscles to assist in stabilization
• Hams/Quads generally control the sagittal plane; need hip muscles to control frontal/transverse plane/ p
4. Train to control knee extension (knee stability)• Land and function in greater knee flexion
5. Enhance NM control and protective pattern reflexes ‐ keep foot under5. Enhance NM control and protective pattern reflexes keep foot under the center of mass
6. Train muscular endurance7. Include weight‐bearing exercise to enhance and proprioception and g g p p p
replicate functional synergistic movement patterns

ACL Exercise Considerations
• “0‐40° Range Safe” in early rehab Henning 1985 Voight 1991 Ohkoshi 1991 Lutz 1993 Escamilla 2012 Henning, 1985, Voight, 1991, Ohkoshi, 1991, Lutz, 1993, Escamilla, 2012
• Technique• Dynamic frontal plane control• Dynamic frontal plane control• Vertical Squat (feet under hips)• Slight forward trunk incline (increases gluteal
and hamstring activity)and hamstring activity)• Push through heels (keep knees behind toes)• As resistance increases later in rehab may
t t li it t i l t i b twant to limit terminal extension range but monitor for patellofemoral irritation

Hamstring Dominant Exercise
Non Weight Bearing• Ham Curls• Ham Curls• Reverse Leg Lifts• Roller Stool Forward
W i ht B iWeight Bearing• Bridging
uni/bilateral; stable‐unstableN di L• Nordic Leans
• Roman Chair Hip Extension• Deadlifts (bi/unilateral• Retrograde Stair Climbing

H d H t i PTG How does Hamstring vs. PTG graft rehab differ?
Delayed hamstring strengthening– Submax isometrics begin at 4‐6 wks– Light isotonics at 6‐8 weeksStandard progression after two months– Standard progression after two months
Delayed functional progressionN i il l 3 h– No running until at least 3 months
– No jumping/plyometrics for at least 4 months– No unrestricted return to activity for at least 6 months
Quadriceps Dominant Exercise
NWB• Leg Extension (90‐45°)Leg Extension (90 45 )
− Early initiation is effective and safe – Fukada TY, Am J Sports Med, 2013• Roller Stool Backward
Weight Bearingg g• Leg Press 45‐100°• Wall Squat or Sit• Lateral Step Ups
PF Protection• weight back on heels• Move hands forward to maintain COG• 90‐45° in OKC and 45‐0° in CKC

Stationary Cycle
• cycling produced 7% elongation of an 80 lb. Lachman’s test and produced 1/5 of the ACLLachman s test and produced 1/5 of the ACL strain as walking on level ground
Henning CE, et al. .Am J Sports Med. 13:22–26,1985
• ACL stresses during cycling was 1/20 of unprotected isokinetic knee extension
Ericson MO Nisell R et al: Scand J Rehabil Med 18:165–172 1986Ericson MO, Nisell R, et al: Scand J Rehabil Med, 18:165 172,1986
• Insignificant strain on the ACL during stationary cycling
Fleming BC, Beynnon BD, et al. Am J Sports Med. 26:109‐18, 1998

What is the need for regular, supervised physical therapy visits …
Can you get the same benefitwith a comprehensive HEP and periodic check ups?and periodic check ups?

7 visits (HEP based visits) vs. 20 (structured PT visits) had similar out‐comes in regards to ROM, isokinetic strength, and subjective ratingD C l M l J O h S Ph Th 1997DeCarlo M, et al, J Orthop Sports Phys Ther, 1997
Supervised exercise, in addition to a HEP, had minimal extra benefit for patients who had undergone ACL reconstruction in regards tofor patients who had undergone ACL reconstruction in regards to function, activity level, muscle strength, and anterior tibial translationBeard DJ, et al, J Orthop Sports Phys Ther, 1998Beard DJ, et al, J Orthop Sports Phys Ther, 1998
Recreational athletes undergoing ACL reconstruction had a higher % of subjects have a successful ROM outcome at
f3 months post‐op with a HEP consisting of 4 visits than a group who attended therapy twice/week (ave. 17 visits)Grant JA, et al, Am J Sports Med, 2005

but, that Grant study just looked at short term impairment outcomes …
Follow‐up on 70% of those subjects at 2‐4 years showed2 4 years showed– ACL QoL score significantly higher
for home exercise cohortNo significant difference in– No significant difference in Knee ROM Knee laxity Quad/Ham strength Quad/Ham strength IKDC score
So, do we need to change our paradigm?

Current Best Evidence of Selected Interventions based on Systematic Reviews
Intervention Value
CPM d t i li ht f tCPM no advantage in light of cost
Early weight‐bearingand ROM
no adverse effect(given good quad control and no concurrent surgery that necessitates limiting weight‐bearing for healing)necessitates limiting weight bearing for healing)
Post‐op/Functionalbracing
Neither necessary or beneficial(Additionally, preponderance of the data indicates that the current brace designs cannot prevent injury)
Home‐based PT Effective in motivated patients
OKC vs. CKC exercise Safe to start OKC at 6 wks (or earlier)
“Accelerated” protocol Safe, but needs additional verificationAccelerated protocol Safe, but needs additional verification

ACL Clinical GuidelinesKnee Stability and Movement Coordination Impairments - Knee Ligament SprainOrthopedic Section of the APTA
U /Intervention Implement
Unnecessary/ Not as
Beneficial
Level of EvidenceSupporting
Recommendation
Recommendation Grade
CPM for Post‐Op Pain II
CPM for Post‐Op ROM
Cryotherapy for Post‐Op Pain
Early Weight‐Bearing
II
II
IIEarly Weight‐Bearing
Mobilization Early Delayed
Post‐Op Bracing
II
I ‐ II
I ‐ III
Functional Bracing
ACL Deficient Bracing
Home Program Supplementation
I ‐ II
II ‐ III
I ‐ IIg pp
NMES (re‐education/strengthening)
I ‐ II
I ‐ II
I ‐ II
Therapeutic Exercise (OKC an CKC)
Eccentric Strengthening
“Accelerated” Rehab Safety
I ‐ II
II

Medial Knee Injuries
Grade Presentation
I T d i t bilitI Tenderness, no instability
II Broad tenderness, partial tear, laxity to stress
III End point absent with valgus stress in RPCC OO
Supported by posterior oblique ligament and superficial and deep tibial collateral ligaments
sMCLsMCL -- POLPOL
dMCLdMCL
Evaluated by valgus stress tests at 0/30° and anterior drawer test in external rotation

Medial Knee Rehabilitation
Hinged knee brace and protected arc of motion 20 90° for first 2 6 wks dependentmotion 20‐90 for first 2‐6 wks dependent upon grade severity
Emphasis on frontal and transverse plane p p(internal rotators) dynamic stabilizers
Protocol provided in appendix of Clinical C t ti l i filCommentary article in your resource file
LaPrade RF, et al, J Orthop Sports Phys Ther, 2012
Posterior Cruciate Ligament
Vertical orientationP 94% f Prevents 94% of posterior translation of tibia on femur
Prevents hyperextension

Posterior Cruciate Ligament Injury
Isolated PCLIsolated PCL Combine PCL InjuryCombine PCL Injury
Grade IGrade I Grade IIGrade II Grade IIIGrade IIIPCL/LCLPCL/LCL PCL/MCLPCL/MCL PCL/ACLPCL/ACL
NonNon‐‐op rehab op rehab with quadwith quad
NonNon‐‐op rehab op rehab unless pain &unless pain &
PCL/LCLPCL/LCL
Surgery within 2 weeks Surgery within 2 weeks –– PCL PCL reconstruction and acute repair ofreconstruction and acute repair of
PCL/MCLPCL/MCL PCL/ACLPCL/ACL
with quad with quad emphasis and emphasis and activity activity modsmods
unless pain & unless pain & instability instability continuescontinues
reconstruction and acute repair of reconstruction and acute repair of collateral ligaments and/or ACL collateral ligaments and/or ACL
reconstructionreconstruction

I
Posterior InstabilityII
III
Grade III immobilized in full extension for 2‐4 weeks with FWB to toleranceFWB to tolerance
Quad emphasis for dynamic stability
A id f i l d h i i i Avoidance of isolated hamstring activity
“Mirror” perspective to ACL rehabilitation philosophyrehabilitation philosophy

Multi-Ligamentous Knee Injuries
• Pathoanatomy ‐ “dislocation” with significant soft tissue disruption with at leastsignificant soft tissue disruption with at least 3 of 4 ligaments involved
• 60% chance of tibial or femoral fracture • 50% chance of vascular injury with A/P• 50% chance of vascular injury with A/P dislocation
• 25% chance for common peroneal nerve injuryinjury
• Prognosis: poor− complications frequent and rarely does knee return to pre‐injury statereturn to pre‐injury state
MLKI Management
Initial Treatment– Immediate reduction and evaluation of vascular status confirmed by– Immediate reduction and evaluation of vascular status confirmed by
arterial duplex ultrasound or CT angiography– Limited indication for non‐operative care
Operative Intervention Operative Intervention– emergent surgical intervention indicated if:
• vascular injury repair (takes precedence)f d di l ti• open fx and open dislocation
• irreducible dislocation• compartment syndrome
d l d li i / i– delayed ligamentous reconstruction/repair

MLKI Management continued -
Delayed Surgical Reconstruction/Repair ‐– 1 or 2 staged intervention with PCL + medial and lateral structures repaired– 1 or 2 staged intervention with PCL + medial and lateral structures repaired acutely and ACL reconstructed at a later time as needed
– improved outcomes with early treatment (within 3 weeks)
Post‐Operative TherapyPost Operative Therapy – early mobilization with functional bracing
ComplicationsStiffness (arthrofibrosis) is the most common complication (particularly with– Stiffness (arthrofibrosis) is the most common complication (particularly with delayed mobilization)
– Laxity and instability (37%)– Peroneal nerve injury (25%) (particularly with posterolateral dislocations)Peroneal nerve injury (25%) (particularly with posterolateral dislocations)

Impact of Pain and Fear
Pain is consistently associated with function across the time span of the rehabilitation processspan of the rehabilitation process
Fear of movement and re‐injury gradually decrease as function is restored and is a factor in the return to activityy
Do we need a FABQ modified for the knee?
Ch i l ki TL Ph Th 2008Chmielewski TL, Phys Ther, 2008

Functional Testing ResearchTesting Reliability has been Established
5-6”.3 sec
Test (Uninjured Patients) ICC SEMSingle Hop for Distance .96 4.56 cm (2”)
Reid A, et al. Phys Ther, 2007
( )6 m Hop for Time .66 .13 secondsTriple Hop for Distance .95 15.44 cm (6”)Crossover Hop for Distance .95 15.95 cm (6”)p .95 15.95 cm (6 )Bolgla, et al. J Orthop Sports Phys Ther. 26:138‐143, 1997

Hop Test Examples
• Single Leg Hop for Distance
• Single Leg Triple Hop for Distance
• Single Leg 20’ (6m) Hop for Timeg g ( ) p
• Single Leg Crossover Hop for Time or Distance
• Single Leg Vertical Jump

Hop Testing Research
• 50% have asymmetrical scores on distance hop 62% have asymmetry on distance or time hop• 62% have asymmetry on distance or time hop Noyes F, et al, Amer J Sports Med, 1991
Gustavsson A, et al. Knee Surg Sports Traumatol Arthrosc, 2006

Strength Test Examples
• PSLC Single Leg Squats
• Lateral or Front Step Downs
• Single Leg Wall SitSingle Leg Wall Sit
• Squat Depth Excursion
d l• Sport Cord Single Leg Squats

Dynamic Postural Control Tests
Balance Tests– Maintain COG over a base of support that is unpredictable
M i t i COG fi d b f t– Maintain COG over a fixed base of support while body segments move (reach tests)
Time to Stabilization Tests Time to Stabilization Tests– Vertical Hop or Dynamic Movement

functional tests
T run Box run Carioca test Carioca test Shuttle runS i t T t Sprint Test
Landing Stability
Resource Folder on your CD-ROM
Logerstedt DS, Snyder‐Mackler L, Ritter RC, Axe MJ. Knee Stability and Movement Coordination Impairments: Knee Ligament Sprain. J Orthop S t Ph Th 2010 40(6) A1 A35Sports Phys Ther. 2010:40(6):A1‐A35
Wilk KE, Macrina LC, Cain EL, Dugas JR, Andrews JR. Recent advances in the rehabilitation of anterior cruciate ligament injuries. J Orthop Sports Phys Ther. 2012 Mar;42(3):153‐71.y ; ( )
van Grinsven S, van Cingel RE, Holla CJ, van Loon CJ. Evidence‐based rehabilitation following anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2010 Aug;18(8):1128‐44.
Logerstedt DS, Snyder‐Mackler L, Ritter RC, Axe MJ; Orthopedic Section of the American Physical Therapy Association. Knee pain and mobility impairments: meniscal and articular cartilage lesions. J Orthop Sports Phys Ther. 2010 Jun;40(6):A1‐A35.

Resource Folder on your CD-ROM
Laprade RF, Wijdicks CA. The management of injuries to the medial side of the knee. J Orthop Sports Phys Ther. 2012 Mar;42(3):221‐33.
Howells NR, Burnton LR, Robinson J, Porteus AJ, Eldridge JD, Murray JR. Acute knee dislocation: An evidence based approach to the management of the multiligament injured knee. Injury. 2011. 42(11):1198‐1204
Rosenthal MD, Rainey CE, Tognoni A, Worms R. Evaluation and management of posterior cruciate ligament injuries. Phys Ther Sport. Epub May 18, 2012
h ff bl d l ll ll Mithoeffer K, Hambly K, Logerstedet D, Ricci M, Silvers H, Della Villa S. Current concepts for rehabilitation and retun to sport after knee articular cartilage repair in the athlete. J Orthop Sports Phys Ther 2012;42(3):254‐273
Questions - Discussion





























