Embed Size (px)
Citation preview

O
ArA
Ord
Stt
Rwp
Ca
AgpnFcF
Ftagwssto
FaR
R2
R
TNB
0©d
Research www.AJOG.org
BSTETRICS
ntepartum high-frequency fetal heart rate sinusoidalhythm: computerized detection and fetal anemiaparna Reddy, MB, MSc; Mary Moulden; Christopher W. G. Redman, MB, BChir
Tm
Cclmp
K
BJECTIVE: Our aim was to identify antepartum fetal heart rate (FHR)ecords of high-frequency (HF) sinusoidal rhythms from an electronicatabase (1983-2003) and determine clinical outcomes.
TUDY DESIGN: At the John Radcliffe Hospital (Oxford, UK), 72,297races from 19,506 women were analyzed using an algorithm that iden-ifies HF sinusoidal rhythms. The case records were reviewed.
ESULTS: There were 15 (0.21/1000) traces from 8 (0.41/1000)omen with an HF sinusoidal rhythm. In 5 of 8 women (62.5%), this
nv
mmssmtlTrm6
ptcnta
(tmmp(idibrain.5-9
oi: 10.1016/j.ajog.2008.10.026
heir FHR patterns were distinguished from those of the other nonane-ic fetuses by significantly lower long-term variability.
ONCLUSION: An antepartum HF sinusoidal rhythm is rare but asso-iated with fetal anemia, particularly if it is combined with reducedong-term variability without episodes of high FHR variability within 60
inutes. The automated system can alert inexperienced staff, who su-ervise FHR monitoring, by an online warning.
ey words: antepartum fetal anemia, computerized fetal heart rate
attern was associated with fetal anemia (hemoglobin � 10.0 g/dL). patterns, high-frequency sinusoidal rhythm, sinusoidal rhythmite this article as: Reddy A, Moulden M, and Redman CWG. Antepartum high-frequency fetal heart rate sinusoidal rhythm: computerized detection and fetalnemia. Am J Obstet Gynecol 2009;200:407.e1-407.e6.
tawAwracc
ctqawhrt
MThwvros
Sl
sinusoidal rhythm is a rare fetalheart rate (FHR) pattern and is re-
arded by most as indicative of a com-romised fetus. This pattern was origi-ally described by Modanlou andreeman,1 who developed diagnosticriteria based on visual assessment ofHR readings.Computerized analysis of antepartum
HR records gives objective and quanti-ative assessment of fetal condition thatugments clinical visual assessment.2 Itives consistency of interpretation,hereas visual assessment suffers from
ubstantial interobserver and intraob-erver variability,2 probably in relationo inexperienced staff. We have previ-usly described the Oxford system for
rom the Nuffield Department of Obstetricsnd Gynecology, University of Oxford, Johnadcliffe Hospital, Oxford, UK.
eceived March 21, 2008; revised Aug. 8,008; accepted Oct. 7, 2008.
eprints not available from the authors.
his study was supported in part by Oxfordational Institute of Health Researchiomedical Research Centre Programme.
002-9378/$36.002009 Mosby, Inc. All rights reserved.
umerical analysis,2,3 which has beenalidated for use in the antenatal period.Short- and long-term variability iseasured. Short term variability (STV)easures heart rate variability between
uccessive ‘epochs’ averaged over 3.75econds. Long term variability (LTV) is
easured as the average excursion of fe-al heart from below to above the base-ine over successive minute windows.he average of consecutive minute
anges is the mean minute range. Botheasures are valid only if derived from
0 minutes of recording.Fetal heart rate monitors measure
ulse intervals in milliseconds ratherhan heart rates, which are derived byalculation. Although pulse intervals areon-intuitive, they are used by the sys-
em for all analyses because they are whatre measured.
A low-frequency sinusoidal rhythm1/2-5 min), on an otherwise flat FHRracing, usually signifies fetal compro-
ise and poor outcome, associated withetabolic acidemia. Its incidence is 1.6
er 1000 records.4 A high-frequencyHF) sinusoidal rhythm (2-4/min) mayndicate fetal anemia caused by rhesusisease, fetal-maternal hemorrhage, or
nternal fetal bleeding, for example in the
nAPRIL 2009 Americ
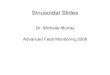
The incidence of sinusoidal FHR pat-erns identified solely by computerizednalysis is not known, nor is the extent tohich it is associated with fetal anemia.n example is shown in Figure 1. Hence,e analyzed our database for sinusoidal
ecords applying our current criteria andlgorithms.3 We reviewed the fetal out-omes to determine how often they indi-ate fetal anemia.
Our aim was first, to determine the in-idence of sinusoidal patterns in our da-abase and second, to determine how fre-uently they were associated with fetalnemia. We sought also to determinehether computerized detection of aigh-frequency FHR pattern provided aeliable first clinical alert to the operatoro seek more expert assessment.
ATERIALS AND METHODShe derivation of the FHR parametersas been previously described,2 togetherith identification of episodes of highariability and fetal movements. Heartate is averaged over consecutive epochsf 3.75 seconds with allowance made forpurious or missing data.2
The Oxford system (now available asonicaid Teamcare or Fetalcare; Hunt-eigh Health Care, Cardiff, UK) recog-
izes and measures STV and LTV sepa-an Journal of Obstetrics & Gynecology 407.e1

rSqsaraotdeccrq
itdtSftt2ro
ri
cstpmt
rmswdmrqom
amratss
pSd
mShloog
dswmi
ocRmonfn
cyawu2bti
s(fcChtc
PMme.eaa
RTt
TcdbpR
Research Obstetrics www.AJOG.org
4
ately. The relation between LTV andTV can be used to identify high-fre-uency sinusoidal patterns. The timepan over which variability is assessedcts as a filter: a short period (STV) caneflect only high frequency oscillations,nd a longer period (LTV) detects slowerscillations. Hence, LTV is increased inhe presence of a low-frequency sinusoi-al rhythm but unaffected by the pres-nce of a high-frequency rhythm. Theonverse applies to the STV, which is in-reased by a high-frequency sinusoidalhythm but unaffected by the low-fre-uency pattern.Random variability of normal FHRs
ncreases both measures to a similar ex-ent so that they are highly correlated un-er normal conditions.2 Deviation fromhis correlation is assessed by the ratio ofTV/LTV. An unusually large ratio isound in high-frequency sinusoidal pat-erns. An HF sinusoidal rhythm is iden-ified if its frequency is predominantly-4 cycles per minute and the STV/LTVatio is higher than the empirical thresh-ld of 1 SD.2
From 1983 to 2003, a total of 72,297ecords from 19,506 patients were stored
FIGURE 1An example of a sinusoidal trace s
he display is a simplified version of the screenase notes, on 1 page. Episodes of low variationecelerations are identified by the vertical arrowsy a handheld button, are marked by the lower versists for the duration of the 60 minute recoreddy. Computerized antepartum high-frequency fetal heart
n the Oxford database. The major indi- a
07.e2 American Journal of Obstetrics & Gynecolo
ations for monitoring were current ob-tetric problems, a poor obstetric his-ory, medical disorders complicatingregnancy, or a history of decreased fetalovements. None of the records were
aken during labor.Regular oscillations of the fetal heart
ate, cycling between 2 and 4 times perinute were sought as previously de-
cribed.2,3 The system first interactivelyarns the operator of a possible sinusoi-al pattern in records that are at least 20inutes long and continuation of the
ecord is requested. A true high-fre-uency sinusoidal rhythm was defined asne that persisted throughout a 60inute recording.During the time of data collection, the
nalytical algorithm underwent severalodifications, although only the most
ecent version was used in the presentnalysis. In some of the older records, theraces were considered normal andtopped early, whereas they would be toohort by the current criteria.
In the group with definite sinusoidalatterns, clinical details were noted.ome patients had more than 1 sinusoi-al trace and each trace was assessed sep-
ected to computerized analysis
play, which can be printed out to be filed in theidentified by the arrows on the upper bar. Smallder the FHR display. Four movements, recordedcal lines. The high frequency sinusoidal patterng.sinusoidal rhythm. Am J Obstet Gynecol 2009.
rately. Neonatal outcome was deter- t
gy APRIL 2009
ined from the neonatal notes.ignificant fetal anemia was defined as aemoglobin value in the first 24 hours of
ife without prior extra uterine blood lossf less than 10.0 g/dL. The normal rangef hemoglobin in a neonate is 14-18/dL.An unconfirmed sinusoidal pattern was
efined as one in which the trace wastopped prematurely before 60 minuteshen criteria of normality had not beenet. If a sinusoidal pattern did not persist,
t was considered to be pseudosinusoidal.For those who delivered after 1990,
utcome details were available from theomputerized clinical database at Johnadcliffe Hospital. If the baby was ad-itted to the special care baby unit, its
utcome was assessed from the neonatalotes. For details of cases delivered be-
ore 1991, individual maternal and neo-atal notes were reviewed.To determine whether there were
ases of fetal anemia that the FHR anal-sis missed, we identified all babies withdischarge diagnosis of anemia, whoere admitted to the special care babynit, from January 1995 to December003. This time period was consideredecause the hospital’s computerized da-abase could not provide diagnostic cod-ng before 1995.
Neonates with the International Clas-ification of Diseases, 10th revisionICD10) codes P61.3 (congenital anemiarom fetal blood loss) or P61.4 (otherongenital anemias) were identified.ases with FHR analysis less than 48ours before birth were identified fromhe patient database and the neonatalase notes were reviewed.
The data were analyzed with Graph-ad Prism software (San Diego, CA).ann Whitney test was used to compareedian values. Differences were consid-
red to be statistically significant at P �05. This retrospective study was ex-mpted from institutional review boardpproval because it involved databasenalysis only.
ESULTShere were 8 fetuses with 15 traces with
rue high-frequency sinusoidal FHR pat-
ubj
disareunertidinrate
erns. The maternal and neonatal details

airh0(mfari(
wwttcpa
wsjfi5ttnaItcaba
wwgaoMtvfhmwTfqdfHg
terstebuFf
t1sbf6nbgnf
art r
www.AJOG.org Obstetrics Research
re shown in Table 1, respectively. Thencidence of high-frequency sinusoidalhythm in this series of predominantlyigh-risk pregnancies was 8 of 19,506 or.41 of 1000 pregnancies. Five of 862.5%) were associated with fetal ane-ia, the causes being Rhesus disease,
etal-maternal hemorrhage, and fetalnemia because of intracerebral hemor-hage. The interval to delivery was longern the 3 cases not associated with anemiaon average by 24 days).
The mean gestational age was 29 weekshen it is not our practice to interveneithout confirming the unfavorable pat-
erns. But they were not confirmed, jus-ifying the delays in intervention. In all 8ases, the first detection of a sinusoidalattern was by the computerizednalysis.
The neonatal morbidity, as expected,as high. All cases were admitted to the
pecial neonatal care. Of the 5 neonatesudged to be anemic (hemoglobin in therst 24 hours less than 10.0 g/dL [mean,.5 � 1.2 g/dL]), all required bloodransfusions, including an exchangeransfusion for hemolytic disease of theewborn. Developmental milestones atge 1 year for 6 of 8 babies were normal.n the case of the baby who suffered in-racranial hemorrhage, milestones wereonsistently delayed after 4 months ofge. For 1 baby, no follow-up was possi-le because the mother moved out of therea.
The cases were analyzed in 2 groups,ith or without anemia, to determinehether the pathology could be distin-uished by other attributes of the FHRnalysis (Table 2). Median values of eachf the criteria were compared using theann-Whitney test. In the anemic fe-
uses, the duration of episodes of highariability was shorter than nonanemicetuses and associated with a higher basaleart rate. Both the LTV and STV of ane-ic fetuses were lower. All these changesere statistically significant (Table 2).his combination of features indicated
etuses with major problems that re-uired prompt investigation and earlyelivery. In the course of this analysis, we
ound 2 further categories with possibleF sinusoidal patterns. In the first cate-
ory, a sinusoidal pattern was detected at c
he end of the record, which was, how-ver, too short (� 60 minutes) for accu-ate analysis. In the second category, ainusoidal pattern was detected at someime during the record but not when itnded (pseudosinusoidal). We reviewedoth these patterns, which were denotednconfirmed and pseudosinusoidalHR. The fetal outcome and incidence ofetal anemia was determined.
There were 39 FHR records from 38
TABLE 1Maternal and neonatal detailsMaternal details
..........................................................................................................
Cases identified..........................................................................................................
Nulliparae..........................................................................................................
Maternal age (y)..........................................................................................................
Indications for monitoring.................................................................................................
Decreased fetal movements.................................................................................................
Preterm premature rupture of membra.................................................................................................
Threatened preterm labor.................................................................................................
MCDA twin with discordant growth.................................................................................................
Assessment after intrauterine transfus.................................................................................................
Interval between index trace and deliv.................................................................................................
Anemic fetuses (h).................................................................................................
Nonanemic fetuses (d)...................................................................................................................
Neonatal details..........................................................................................................
Live born..........................................................................................................
Neonatal deaths..........................................................................................................
Gestational age at the time of delivery (wk..........................................................................................................
Admissions for special or intensive care..........................................................................................................
Mean duration of stay in neonatal special..........................................................................................................
Associated pathology.................................................................................................
Fetal-maternal hemorrhage.................................................................................................
Rhesus disease.................................................................................................
Intracranial hemorrhage.................................................................................................
No cause identified..........................................................................................................
Neonatal Hb within 24 h of birth (g/dL).................................................................................................
Anemic fetuses (Hb � 10 g/dL) (n � 5.................................................................................................
Nonanemic fetuses (n � 3)..........................................................................................................
Other outcomes..........................................................................................................
Neonatal transfusion..........................................................................................................
Born � 37 wks...................................................................................................................
Hb, hemoglobin; MCDA, monochorionic diamniotic twin ges...................................................................................................................
Reddy. Computerized antepartum high-frequency fetal he
ases with other sinusoidal FHR pat- g
APRIL 2009 Americ
erns. There were 10 FHR records from0 fetuses (Table 3 and Figure 2), whichhowed consistent sinusoidal patternsut in incomplete traces terminated be-ore the criteria of normality were met or0 minutes had elapsed.2 One of the neo-atal case notes could not be traced. Oneaby was anemic (hemoglobin of 6.6/dL) owing to hemolytic disease of theewborn. Some of the antepartum traces
or this index case were in the definite
..................................................................................................................
8..................................................................................................................
12.5%..................................................................................................................
29.8 � 2.9..................................................................................................................
..................................................................................................................
4..................................................................................................................
1..................................................................................................................
1..................................................................................................................
1..................................................................................................................
1..................................................................................................................
..................................................................................................................
29.3 � 3..................................................................................................................
25.6 � 19.1..................................................................................................................
..................................................................................................................
8..................................................................................................................
0..................................................................................................................
31.5 � 3..................................................................................................................
8..................................................................................................................
(d) 21.4 � 13.6..................................................................................................................
..................................................................................................................
2..................................................................................................................
2..................................................................................................................
1..................................................................................................................
3..................................................................................................................
..................................................................................................................
5.5 � 1.2..................................................................................................................
16.4 � 3.9..................................................................................................................
..................................................................................................................
6/8 (75%)..................................................................................................................
7/8 (88%)..................................................................................................................
...................................................................................................................
ate sinusoidal rhythm. Am J Obstet Gynecol 2009.
.........
.........
.........
.........
.........
.........
nes.........
.........
.........
ion.........
ery.........
.........
.........
.........
.........
.........
s).........
.........
care.........
.........
.........
.........
.........
.........
.........
).........
.........
.........
.........
.........
tation.........
roup 48 hours after the short trace. Be-
an Journal of Obstetrics & Gynecology 407.e3

ccfwu
tfcwihp
mwslcvtodb
wn
mtnc1bctacdOmno
wdimiFwwew
hllbtqmtbnn
CAaccfsmIbwupl
art r
Research Obstetrics www.AJOG.org
4
ause this case has been included in theonfirmed group, it has been excludedrom this group. Of the remaining 8, 3ere admitted to the special care babynit and were not anemic at birth.In those with pseudosinusoidal pat-
erns (Table 3), there were 29 recordsrom 28 fetuses. One set of case notesould not be located. Six of 27 babiesere admitted for special care. One baby
n this group was mildly anemic with aemoglobin level of 11.1 g/dL. Two ante-artum records from this case were inter-
TABLE 2High-frequency sinusoidal FHR trac
CriteriaAnemia(Hb < 10 g/dL)
Cases 5...................................................................................................................
FHR records (n) 12...................................................................................................................
Episodes of highFHR variation (min)
0 (0-23)
...................................................................................................................
Basal heart rate(beats/min)
149 (141-163)
...................................................................................................................
Long-term variation(milliseconds)
24 (9.9-37.4)
...................................................................................................................
Short-termvariation(milliseconds)
5.6 (2.1-8.8)
...................................................................................................................
Accelerations 0 (0-7)...................................................................................................................
Decelerations 1 (0-3)...................................................................................................................
Values are medians (ranges).Hb, hemoglobin.a Mann-Whitney test....................................................................................................................
Reddy. Computerized antepartum high-frequency fetal he
TABLE 3Outcomes with unconfirmed high f
Cases...................................................................................................................
Traces...................................................................................................................
Excludeda
...................................................................................................................
Notes reviewed...................................................................................................................
Neonatal admissions to special care unit...................................................................................................................
Fetal anemia (Hb � 10 g/dL)...................................................................................................................
Neonatal death...................................................................................................................
Hb, hemoglobin.a Later developed a true sinusoidal pattern and is analyzed s...................................................................................................................
Reddy. Computerized antepartum high-frequency fetal heart r
07.e4 American Journal of Obstetrics & Gynecolo
ittently sinusoidal. Subsequent tracesere abnormal as judged by visual as-
essment with baseline tachycardia andate decelerations. After an emergencyesarean section, the baby suffered intra-entricular hemorrhages, required mul-iple transfusions, and died on day 6. Thether babies admitted for high-depen-ency neonatal care were not anemic atirth.To determine how many other fetusesere born with anemia but with nonsi-usoidal FHR patterns, a sample of ad-
with or without fetal anemia
No anemiaProbability ofno differencea
3..................................................................................................................
3..................................................................................................................
53 (45-56) .01
..................................................................................................................
136 (134-138) .01
..................................................................................................................
52 (50-52) .01
..................................................................................................................
11 (10.8-11.6) .01
..................................................................................................................
3 (3-10) .03..................................................................................................................
0 (0-1) .27..................................................................................................................
..................................................................................................................
ate sinusoidal rhythm. Am J Obstet Gynecol 2009.
uency sinusoidal patternsUnconfirmed(< 60 min) Pseudosinusoidal
10 28..................................................................................................................
10 29..................................................................................................................
1 0..................................................................................................................
8 27..................................................................................................................
3 6..................................................................................................................
0 0..................................................................................................................
0 1b
..................................................................................................................
tely (Table 2). b Intraventricular hemorrhage...................................................................................................................
fate sinusoidal rhythm. Am J Obstet Gynecol 2009.
gy APRIL 2009
issions for special neonatal care wasaken. Satisfactory diagnostic coding wasot available before 1995, so the sampleovered the 9 years between January995 and December 2003. Exactly 100abies were discharged with the ICD10odes P61.3 (congenital anemia from fe-al blood loss) or P61.4 (other congenitalnemias) (Table 4). Four of the indexases (Table 2) with confirmed sinusoi-al traces delivered before January 1995.f the other 4, 2 were born without ane-ia and were not included in the diag-
ostic listing. This left 2 of the index ne-nates in this analysis.In the same period, 12 of 100 babiesere transferred from other units, whichid not have the facility for computer-
zed antepartum FHR records. Of the re-aining 88 women who were delivered
n our unit, 29 had 1 or more antepartumHR records at any time (150 traces), ofhich 18 (35 traces) were monitoredithin 48 hours of delivery. Unless oth-
rwise stated, the diagnosis of anemiaas made after birth.In this group, 5 of 29 (17.2%) had a
emoglobin within 24 hours of birth ofess than 10 g/dL. The antepartum eventseading to fetal anemia are shown in Ta-le 4. Two of these 5 cases (40%) werehe index cases with a definite high fre-uency sinusoidal FHR pattern. Theirean hemoglobin was 5.5 � 1.2 g/dL. Of
he remaining 3 cases (mean hemoglo-in 8.7 � 3.3 g/dL), the FHR records didot display sinusoidal patterns and wereormal to analysis.
OMMENT
n HF sinusoidal FHR has been associ-ted with severe fetal anemia of diverseauses, effects of drugs, especially nar-otics, fetal asphyxia/hypoxia, fetal in-ection, fetal cardiac anomalies, fetalleep cycles, and fetal sucking move-
ents.9 It is a rare pattern before labor.ts true incidence is unknown but muste less than the 0.41 per 1000 cases thate measured in a selected high-risk pop-lation. Although it is rare, it mayresent in a routine clinic for women at
ow risk as, for example, with reduced
es
.........
.........
.........
.........
.........
.........
.........
.........
.........
req
.........
.........
.........
.........
.........
.........
.........
epara.........
etal movements.

wnwceuTteTct
eantp
nf(uimItmopbv
r(wbfbgacet
thws(ast
r
cspet
tc
ccn
hfaF
R
www.AJOG.org Obstetrics Research
The characteristics of the FHR patternill be unusual and may not be recog-ized as sinister by less experienced staff,ho are delegated to supervise the re-
ording. It is in this context that comput-rized identification and warning can beseful in avoiding delay in treatment.hat all 8 cases of true sinusoidal pat-
erns were detected first by the comput-rized system indicates its effectiveness.his does not imply that an expert clini-ian would not have immediately comeo the same conclusion.
The system does not supplant such anxpert but makes some of the skills avail-ble to nursing and auxiliary staff. Theumbers are too small to give robust es-
imates of the specificity and negativeredictive value of the system.Flat or unreactive records are recog-
ized by a low STV, which may identifyetuses that are hypoxemic or acidemicSTV � 3.0 milliseconds).2 Sinusoidalndulations, associated with intrauter-
ne anemia, increase the STV, which thenay give false reassurance of fetal health.
f this is the only numerical variable usedo consider fetal well-being, then abnor-
ality will be missed. But we have dem-nstrated that the analysis system canick out the sinister pattern against thisackground of numerically satisfactoryariability and give appropriate warning.Not all sustained HF sinusoidal
hythms are associated with fetal anemia62.5% in this small series). But thoseith fetal anemia can be discriminatedy reduced LTV (� 40 milliseconds)rom those without anemia. It has thuseen possible to amend the analytical al-orithm to highlight this by an appropri-te warning at the bedside. This modifi-ation requires prospective testing tonsure that it distinguished reliably be-ween anemic and nonanemic fetuses.
Another important feature of the pat-ern is its consistency, sustained over 1our. In traces of short duration or inhich a sinusoidal pattern was noted at
ome time during the trace, 1 new case1/10) of fetal anemia was noted (Table 3nd Figure 2). The same case laterhowed a consistent HF sinusoidal pat-ern over 60 minutes.
These observations do not imply that all
ecords need to be 60 minutes long. Mostan be terminated much earlier if no HFinusoidal pattern has been detected. If aossible HF sinusoidal pattern is detectedarlier, then the requirement to continuehe recording is clearly signaled.
The causes of pseudosinusoidal pat-erns are obscure. In the majority of ourases, the pattern was transient, nonre-
FIGURE 2The sources of the cases and tracereviewed in each section of this stu
All
Confirmed Sinusoidal pattern 8 cases (15 records)
Unconfirmed (< 6010 cases (10 reco
Excluded (2 cases) 1. Case notes missing
2. Later confirmed sinusoidal pattern
8 cases (8 records)
eddy. Computerized antepartum high-frequency fetal heart
TABLE 4Neonates admitted with diagnosisanemia (January 1995-December 2Total
..........................................................................................................
In-born babies..........................................................................................................
With antepartum computerized FHR record..........................................................................................................
Hb � 10 g/dL and FHR analysis � 48 h b..........................................................................................................
High frequency sinusoidal FHR patterns.................................................................................................
Causes of anemia.................................................................................................
Intraventricular hemorrhage.................................................................................................
Fetomaternal hemorrhage.................................................................................................
Maternal parvovirus infection.................................................................................................
Sepsis...................................................................................................................
Sinusoidal antepartum traces and anemia...................................................................................................................
Mean Hb with sinusoidal FHR (g/dL)...................................................................................................................
Mean Hb with nonsinusoidal FHR (g/dL)...................................................................................................................
Hb, hemoglobin....................................................................................................................
Reddy. Computerized antepartum high-frequency fetal heart r
APRIL 2009 Americ
urrent, not associated with other clini-al abnormalities, and associated with aormal outcome (Table 3).In 1995-2003, 29 babies admitted for
igh-dependency neonatal care wereound to be anemic shortly after birthnd had antepartum FHR recordings.ive neonates had anemia relating to an
es
Other Sinusoidal pattern 38 cases (39 records)
n) Pseudo-sinusoidal pattern 28 cases (29 records) )
Excluded (1 case) Case notes missing
27 cases (28 records)
sinusoidal rhythm. Am J Obstet Gynecol 2009.
congenital3)
100..................................................................................................................
88..................................................................................................................
50 records) 29..................................................................................................................
re birth 5..................................................................................................................
2..................................................................................................................
..................................................................................................................
2..................................................................................................................
1..................................................................................................................
1..................................................................................................................
1..................................................................................................................
2/5..................................................................................................................
4.2 � 1.5..................................................................................................................
8.4 � 0.5..................................................................................................................
..................................................................................................................
sdy
cas
mirds
rate
of00
.........
.........
s (1.........
efo.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
.........
ate sinusoidal rhythm. Am J Obstet Gynecol 2009.
an Journal of Obstetrics & Gynecology 407.e5

anp
tcitibtnptttacc
fwrFwtawr
ccTcitpwe
utdtsfd
R1hn12cnG3pa
4ri25o16Mowr17th18H19crG1eF1Pgn1st
Research Obstetrics www.AJOG.org
4
ntepartum event. A high-frequency si-usoidal rhythm was noted in 2 of theseatients.Despite the limitations of a retrospec-
ive study, a thorough review has beenompleted. The large database used todentify this rare pattern adds strength tohis study. This is the first study thatdentifies the incidence of this patternased on algorithms that avoid subjec-ive bias. The incidence of confirmed si-usoidal patterns was 0.41 per 1000regnancies. Identification of a sus-ained high-frequency sinusoidal pat-ern identified fetal anemia in 62.5% ofhe cases. By consideration of the vari-bility of the record, all nonanemic casesould be distinguished from the anemicases.
This report differs in important waysrom that of Maeda and Nagasawa,10
ho analyzed power spectrums ofecords digitized from the paper record.irst, in our report, the electronic signalsere directly stored and analyzed, with
he analysis given online to the operator,nd not derived retrospectively. Second,e related the records to the total expe-
ience of antepartum fetal heart rate re- 1
07.e6 American Journal of Obstetrics & Gynecolo
ording in a major teaching hospital toonfirm the rarity of such presentations.hird, we retrospectively reviewed allases of neonatal anemia that could bedentified over a period limited by his-orical records and related their clinicalresentation to determine how manyere identified by antepartum comput-
rized FHR analysis.The system is clinically useful when
sed in routine screening of the antepar-um FHR. An immediate alert enableseployment of other investigations (ma-ernal Kleihauer count, Doppler ultra-ound of the fetal middle cerebral artery,etal blood sampling)11,12 and a quickecision about the need for delivery. f
EFERENCES. Modanlou HD, Freeman RK. Sinusoidal fetaleart rate pattern: its definition and clinical sig-ificance. Am J Obstet Gynecol 1982;142:033-8.. Pardey J, Moulden M, Redman CWG. Aomputer system for the numerical analysis ofon stress tests. Review. Am J Obstetynecol.2002;186:1095-103.. Dawes GS, Moulden M, Redman CWG. Im-rovements in computerized fetal heart ratenalysis antepartum. Review. J Perinat Med
996;24:25-36. ogy APRIL 2009
. Modanlou HD, Murata Y. Sinusoidal heartate pattern: reappraisal of its definition and clin-cal significance. J Obstet Gynecol Res004;30:169-80.. Giacoia GP. Severe fetomaternal hem-rrhage—a review. Obstet Gynecol Surv997;52:372-80.. Catanzarite VA, Schrimmer DB, Maida C,endoza A. Prenatal sonographic diagnosisf intracranial hemorrhage: report of a caseith a sinusoidal fetal heart rate tracing, and
eview of the literature. Prenat Diagn 1995;5:229-35.. Burch D. Computerised measurement of fe-al heart rate variability in a case of fetomaternalemorrhage. Br J Obstet Gynecol 1994;101:089-90.. Sadovsky G, Visser GH, Nicolaides KH.eart rate patterns in fetal anemia. Fetal Ther988;3:216-23.. Olah KS, Gee H, Taylor EW. The etiology andlinical significance of the sinusoidal fetal heart-ate pattern: two case reports. Eur J Obstetynecol Reprod Biol 1989;31:189-93.0. Maeda K, Nagasawa T. Automatic comput-rized diagnosis of fetal sinusoidal heart rate.etal Diagn Ther 2005;20:328-34.1. Mari G, Detti L, Oz U, Zimmerman R, Duerig, Stefos T. Accurate prediction of fetal hemo-lobin by Doppler ultrasonography. Obstet Gy-ecol 2002;99:589-93.2. Eichbaum M, Gast AS, Sohn C. Doppleronography of the fetal middle cerebral artery inhe management of massive fetomaternal hem-
rrhage. Fetal Diagn Ther 2006;21:334-8.