Embed Size (px)
Citation preview

Antenatal hydronephrosis -
Paediatric surgeon’s perspective
❖ Dr Pavai Ganesan MS MCh
❖ Pediatric surgeon
❖ PSG Institute of Medical Sciences and Research

Why this talk
❖ We are the customer
❖ You are the salesperson

Antenatal hydronephrosis
❖ 1-5% of all pregnancy
❖ Different terminology
❖ All dilatation is not obstruction
❖ Uniformity is essential – protocol is mandatory - parental anxiety
and physician uncertainty

Basics
❖ Fetal kidneys - 12th - 13th week
❖ Fetal bladder - 14th week
❖ Amniotic fluid - reflects urine output form 16th week
❖ 380 cc at 20th week to 800 cc 28th - 40th week
❖ Polyhydraminos - > 1500 cc (AFI > 20-24)
❖ Oligohydraminos - < 500 cc (AFI < 5-6)

STORY OF ANTENATAL HYDRONEPHROSIS
INNOCENT & RESOLUTION CAKUT
UNNECESSARY WORRY AND INVESTIGATIONS
IMPORTANT THERAPEUTIC IMPLICATIONS

FATE OF GOD GIVEN NEPHRONS
Dysplasia
obstruction
infection
hyperfiltration
Nephron loss
HEALTHY NEWBORN
CAKUT
JOURNEY CALLED LIFEDR Sudipta Sen

Grading
1986
1993
2014 UTD risk stratification
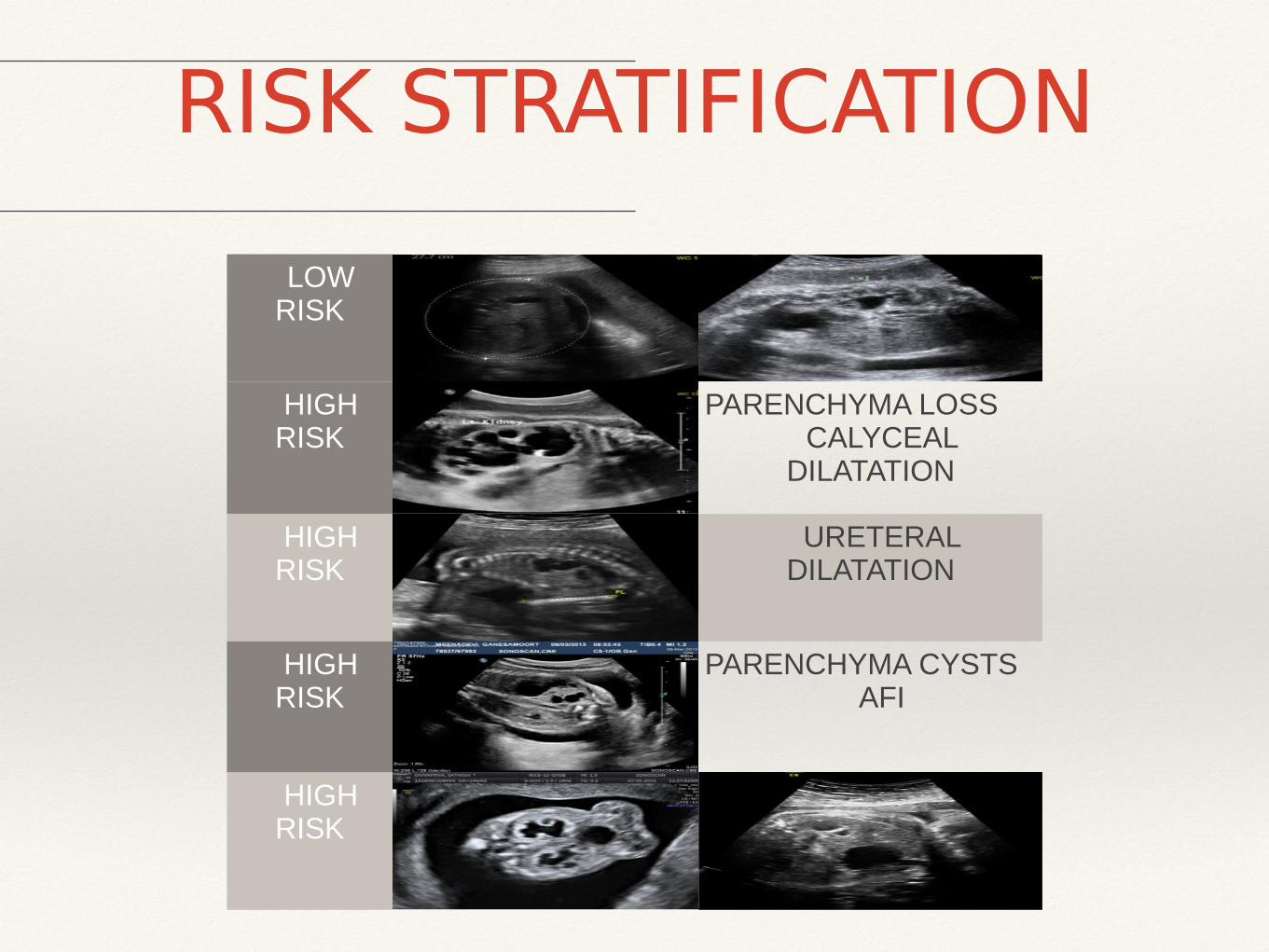
RISK STRATIFICATION
LOW RISK
HIGH RISK
PARENCHYMA LOSSCALYCEAL
DILATATION
HIGH RISK
URETERAL DILATATION
HIGH RISK
PARENCHYMA CYSTSAFI
HIGH RISK

Antenatal hydronephrosis - progress
❖ Spontaneous resolution - 60%
❖ PUJO - 20% - do all of them progress
❖ VUR
❖ PUV
❖ Other - duplex, prune belly, ureterocele
❖ Associated with ARM

❖ Antenatal diagnosis of right PUJO – APD – 15 mm – 34
weeks
❖ PN scan – Dilated PCS – APD 24 mm
❖ Palpable kidney
❖ DTPA – 15%
❖ Clear cut - pyeloplasty
❖ Post op
Baby of R

❖ AN diagnosis of left PUJO
❖ PN - APD 23 mm
❖ Reported after 3 months
❖ Urosepsis
❖ Ultrasound – left infected hydronephrosis
❖ Nephrostomy
❖ Pyeloplasty
Master M

Mast A❖ Antenatal hydronephrosis
❖ APD - 15 mm
❖ DTPA - 48:52
❖ Partial obstruction
❖ Two years - APD - 17
❖ DTPA - 45% ???
❖ MRU

Indication for pyeloplasty
❖ Palpable kidney
❖ Function less than 40%
❖ Decrease in (10%) function on follow up
❖ Increasing dilation of APD
❖ Pain

PUV
❖ Antenatal diagnosis of bilateral UHN
❖ Post natal - bladder palpable
❖ BUN - raised
❖ Catheterisation
❖ MCUG
❖ DMSA

Cystoscopy

Master P
❖ Newborn
❖ AN diagnosis of bilateral UHN
❖ Bladder not palpable
❖ MCUG
❖ DMSA

Hydronephrosis
❖ ? Hydronephrosis
❖ Multiple cysts in the parenchyma
❖ DTPA
❖ MRU
❖ Hydronephrotic type of MCDS

MCDK
❖ Multiple cysts - Non communicating
❖ Ultrasound
❖ DMSA
❖ Nephrectomy

MCDK
Total no. of patients
11
R: L 4:7
M:F 5:6
PN scan size All > 3 cm but < 5 cm
Hydronephrotic type
3
MCDK
ATRETIC VESSELS CLIPPED

Double moiety
❖ Upper pole UHN with ureterocele
❖ PN - scan - double moiety with ureterocele
❖ DTPA scan - 6 weeks
❖ Scopy and incision
❖ Eight months - ultrasound
❖ DTPA

One year study - PSG - 108 patients❖ CAKUT - 4.2% - antenatal
❖ 79% - normalized and 21 % follow up
❖ 6 - pyeloplasty, 2 - PUV, 4 - MCDK
❖ Red signals - Parenchymal thinning, distended bladder and bilaterality

Has AN diagnosis made a difference
❖ PUJO - Pyeloplasty - loss of nephron prevented
❖ VUR - ????


End - Questions to be answered❖ Nuclear imaging - obstruction - definite signs
❖ Decreased function - is it dysplasia / scarring
THANK YOU





























