Embed Size (px)
Citation preview

working with
Affiliated to the Royal College of Pathologists
ANNUAL SHOT REPORT2017
SE
RIO
US HAZARDS OF TRANSFU
SION
AN
NU
AL SHOT REPORT 21ST A
NNIV
ER
SA
RY
YEARS

ANNUAL SHOT REPORT 2017
Serious Hazards of Transfusion (SHOT)Steering Group Chair Professor Mark Bellamy
SHOT Medical Director Dr Paula Bolton-Maggs
Operations Manager Ms Alison Watt
Research Analyst Ms Debbi Poles
Patient Blood Management Practitioner Mrs Jayne Addison
Clinical Incidents Specialist Mr Simon Carter-Graham Mrs Ann Fogg
Laboratory Incidents Specialist Mrs Hema Mistry
National Coordinator for Mrs Rachael Morrison (Ms Dory Kovacs in 2018)Transfusion-Transmitted Infections(Public Health England)
Working Expert Group (WEG) & Writing Group, on behalf of the SHOT Steering Group
Chair: Dr Paula Bolton-Maggs
Professor Mark Bellamy, Ms Alison Watt, Ms Debbi Poles, Mrs Hema Mistry, Mr Simon Carter-Graham, Mrs Ann Fogg, Mrs Jayne Addison, Mrs Rachael Morrison, Dr Tom Latham, Mrs Diane Sydney, Dr Helen New, Dr Megan Rowley, Dr Fiona Regan, Mr Chris Robbie, Dr Peter Baker, Dr Janet Birchall, Dr Jane Keidan, Mrs Terrie Perry, Mrs Katy Cowan, Dr Sharran Grey, Mrs Clare Denison, Dr Catherine Ralph, Dr Sarah Haynes, Mrs Pamela Diamond, Dr Anicee Danaee, Ms Tracey Tomlinson, Dr Shruthi Narayan, Mrs Heather Clarke.
Steering Group (SG) during 2017Chair: Professor Mark BellamyDr Shubha Allard British Society for Haematology Guidelines National Blood Transfusion CommitteeDr Ganesh Suntharalingam Intensive Care Society, Faculty of Intensive Care MedicineDr Su Brailsford Public Health England & Faculty of Public HealthMrs Rashmi Rook UK Transfusion Laboratory CollaborativeDr Ruth Gottstein Royal College of Paediatrics and Child HealthMajor Jeremy Grindrod Defence Medical ServicesDr Ranga Mothukuri College of Emergency MedicineDr Patricia Hewitt Consultant Specialist in Transfusion Microbiology, NHSBTMs Rose Gallagher/Anna Crossley Royal College of NursingMs Mervi Jokinen Royal College of MidwivesMs Jenny Berryman Institute of Biomedical ScienceMr Chris Robbie Medicines and Healthcare Products Regulatory AgencyDr Sheila MacLennan Joint Professional Advisory CommitteeDr Gail Miflin UK ForumMr William Chaffe British Blood Transfusion SocietyDr Megan Rowley Royal College of Pathologists (also member of WEG)Dr Kieran Morris Northern Ireland Regional Transfusion CommitteeDr Krishna Ramachandran Royal College of AnaesthetistsDr Charles Percy British Society for HaematologyDr Edward Norris-Cervetto Trainee Representative for British Blood Transfusion SocietyDr Anne Morrison Scottish Clinical Transfusion Advisory CommitteeDr Rosie Hamilton Royal College of Obstetricians and GynaecologistsDr Andrew Thillainayagam British Society of Gastroenterology and Royal College of PhysiciansDr James Reid Royal College of PhysiciansMr John Thompson Royal College of SurgeonsMr Toby Richards Royal College of SurgeonsMs Nina Vinall Expertise in Patient SafetyMr Graham Donald Lay member
Honorary Steering Group MembersProfessor Hannah Cohen Founder Member and former Steering Group ChairDr Dafydd Thomas Former Steering Group ChairDr Lorna Williamson Founder MemberDr John Barbara Founder MemberProf John Lumley Founder MemberDr Brian McClelland Founder MemberDr Derek Norfolk Founder MemberDr Clare Taylor Former SHOT Medical DirectorDr Sue Knowles Former Interim Medical Director of SHOTDr Dorothy Stainsby Former National Medical Coordinator of SHOTDr Elizabeth Love Former National Medical Coordinator of SHOTNB. All members of the WEG are members of the Steering Group in their own right.

ANNUAL SHOT REPORT 2017
Requests for further information should be addressed to:
Non-infectious hazards Infectious hazards
SHOT Office Dory KovacsManchester Blood Centre Scientist (Epidemiology)Plymouth Grove Public Health England Epidemiology Unit /NHSBTManchester 61 Colindale AvenueM13 9LL London NW9 5EQ
Tel +44 (0) 161 423 4208 Tel +44 (0)20 8327 7602Website www.shotuk.org Email [email protected] Twitter @shothv1
Enquiries [email protected]
Email [email protected] [email protected] [email protected] [email protected] [email protected] [email protected]
Copyright notice
Please cite this work as:
PHB Bolton-Maggs (Ed) D Poles et al. on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. The 2017 Annual SHOT Report (2018).
This work was undertaken by SHOT. The work was funded by NHS Blood and Transplant, Northern Ireland Blood Transfusion Service, Scottish National Blood Transfusion Service and the Welsh Blood Service through the UK Forum.
This report and the individual contributions within it are protected by copyright. The report may be circulated and used for internal, non-commercial purposes within an organisation or institution.
Derivative works: Permission from SHOT is required for all derivative works including adaptations and translations.
All rights reserved. No part of this publication may be reproduced, stored or transmitted in any form or by any means, without the prior written permission of SHOT, or, in the case of reprographic reproduction, in accordance with the terms of licences issued by the Copyright Licensing Agency in the UK (www.cla.co.uk). Enquiries concerning reproduction outside the terms stated here should be sent to SHOT at the address printed on this page.
Making duplicate copies of this Report, or use of the data within, for legitimate clinical, scientific, educational or other non-commercial purposes (not including derivative data) is permitted provided that SHOT is identified as the originator of the information.
Electronic Storage or Usage:
Permission from SHOT is required to store or use electronically any material contained in this publication, including any part of a chapter.
Making alterations to any of the information contained within, or using the information in any other work or publication without prior permission, will be a direct breach of copyright. The use of registered names, trademarks etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant laws and regulation and therefore free for general use.
Copyright © Serious Hazards of Transfusion (SHOT) 2018
Published July 2018
ISBN 978-1-9995968-0-4

Contents
Chapter
1 Foreword ........................................................................................................................Mark Bellamy2 Participation in UK Haemovigilance ........................Debbi Poles, Chris Robbie and Paula Bolton-Maggs3 Headline Data: Deaths, Major Morbidity and ABO-Incompatible Transfusions ......... Paula Bolton-Maggs4 Key Messages and Recommendations ...................................... Paula Bolton-Maggs and Mark Bellamy5 Donor Haemovigilance ..................................................................................................Shruthi Narayan
ERROR REPORTS: Human Factors6 Human Factors in SHOT Error Incidents ........................................Alison Watt and Paula Bolton-Maggs7 Laboratory Errors ............................................................ Peter Baker, Heather Clarke and Hema Mistry8 Right Blood Right Patient (RBRP) ..........................................................Diane Sydney and Hema Mistry9 Handling and Storage Errors (HSE) ........................................................Diane Sydney and Hema Mistry10 Incorrect Blood Component Transfused (IBCT) ....................................................................................... .............................Jayne Addison, Peter Baker, Heather Clarke, Hema Mistry and Paula Bolton-Maggs11 Avoidable, Delayed or Under or Overtransfusion (ADU) ............... Paula Bolton-Maggs and Caroline Wall a. Delayed Transfusions b. Avoidable Transfusions c. Under or Overtransfusion d. Incidents related to Prothrombin Complex Concentrates12 Near Miss Reporting (NM) .........................................................................Alison Watt and Katy Cowan13 Errors Related to Information Technology (IT) ..................................................................Megan Rowley14 Adverse Events Related to Anti-D Immunoglobulin (Ig) .......................... Clare Denison and Katy Cowan15 Immune Anti-D in Pregnancy: Cases reported up to the end of 2017 .................................Jane Keidan
REACTIONS IN PATIENTSSerious Adverse Reactions including EU definition16 Febrile, Allergic and Hypotensive Reactions (FAHR) ...............................Janet Birchall and Fiona Regan17 Transfusion-Transmitted Infections (TTI) .......................................... Rachael Morrison and Su Brailsford18 Pulmonary Complications a. Transfusion-Related Acute Lung Injury (TRALI) ............................................................. Tom Latham b. Transfusion-Associated Circulatory Overload (TACO) ...........Sharran Grey and Paula Bolton-Maggs c. Transfusion-Associated Dyspnoea (TAD) .......................................................... Paula Bolton-Maggs19 Haemolytic Transfusion Reactions (HTR) ......................................Tracey Tomlinson and Anicee Danaee20 New or Unclassifiable Complications of Transfusion (UCT) ..................................... Paula Bolton-Maggs21 Cell Salvage (CS) .............................................................................Sarah Haynes and Catherine Ralph22 Paediatric Summary .............................................................................................................Helen New23 Haemoglobin Disorders: Update ............................................................................ Paula Bolton-MaggsAcknowledgements24 Medicines and Healthcare Products Regulatory Agency (MHRA) Report – available online only ............. ..........................................................................................................................................Chris Robbie
Page
57
101720
272834515558
818290959799
104106114
127
128134142144148154158165166170182186187

ANNUAL SHOT REPORT 2017
51. Foreword
Author: Mark Bellamy
It is now 20 years since the publication of the first Annual SHOT Report, detailing transfusion practice and the nature of error in the years 1996–97 (Love et al. 1998). That report began with two pages of summary recommendations. Reading through those now, some of them have been implemented for so long, and seem so obvious and such second nature, that is quite remarkable that, even as recently as twenty years ago, they were necessary to address major contributors in the chain of events leading to potentially fatal errors. Many such errors could be attributed to system faults and others to what we now call ‘human factors’. While it is often possible to mitigate system faults, ‘human factors’ are ever-present and likely to pose a risk to safety. It follows that we must design our practices and systems to minimise the impact of ‘human factors’.
A key recommendation of the first Annual SHOT Report is reprinted in Figure 1.1; it states that ‘the bedside check is vital in preventing transfusion error. Staff should be vigilant in checking identification details of the component against those of the patient.’ (Love et al. 1998). It is surprising that this simple but very strong recommendation has taken 20 years to be applied nationally. Last autumn, on the 9th of November 2017, the Chief Medical Officer, Professor Dame Sally Davies, together with the Chief Nursing Officer for England, Professor Jane Cummings, issued a central alerting system (CAS) alert on safe transfusion practice entitled ‘Use a Bedside Checklist’ (DH 2017). It is to be hoped that this practice becomes universal in the very near future.
Other elements of the Annual SHOT Report, and its recommendations, have changed dramatically over the 20-year period since that first report. In part, this represents the growth of the safety agenda and safety conscious practices in healthcare. In part, it reflects changes in medical practice, the technologies and blood components we use.
The key messages in Chapter 3 of this year’s Annual SHOT Report suggest that errors account for around 85% of all reported incidents. These figures are remarkably reminiscent of those in another very safety conscious industry, aviation, where around 85% of incidents are attributed to ‘pilot error’, and only 15% to technical or systems failures. These figures suggest that we can continue to learn from the parallels with aviation; and further work on minimising the impact of ‘human factors’ is key. It is also clear, from reading through the literature on aviation accidents, that incidents seldom result from a single point of failure, but rather from a chain of ‘unusual events’, none of which in themselves would be expected to lead to a problem, but which in novel and unexpected combinations may do so. The second key message in this year’s report recognises this phenomenon: ‘at each step in the transfusion process, do not assume that errors have not been made in previous steps. Verify each step, particularly patient identification’. The last of the key messages relates to the importance of accountability. In aviation safety, this is referred to as a ‘just culture’. Root-cause analysis of adverse incidents should be thorough and must identify attributable system-related as well as human factors contributions. A ‘just culture’ is crucial to this, to ensure openness and accuracy of reporting and translate safety theory into genuine improvements for patients.
When SHOT first started collecting and analysing data 20 years ago, initial improvements in safety were relatively easy to deliver by picking ‘low hanging fruit’. And those improvements in practice came about relatively quickly. The task facing us in the future is a more subtle and complex one. Progressing the process of improvement requires further education and training to reduce variability in practice. This training, however, applies not only to individuals, but also to teams. Very successful team-based training
Foreword 1

ANNUAL SHOT REPORT 2017
6 1. Foreword
in medicine, such as advanced trauma life-support (ATLS) has brought about significant improvements in patient care through the way teams function. There are opportunities to learn from this and apply team-based training in blood transfusion. (Here again, there is an aviation parallel: crew resource management). This is particularly important at the present time, as the high staffing levels we enjoyed in the past, with attendant experience and ‘systems redundancy’ is no longer the norm. There is a need to train teams to function by design, not accident. Training teams requires motivation, engagement and ‘buy in’. Moreover, good team function should be the norm, and not reserved for ‘special occasions’ such as the triggering of a massive transfusion protocol. The model works well in aviation, and medicine (e.g. ATLS), so why not in transfusion? There are further opportunities to use information technology to fill some of the gaps in human expertise, to minimise variability in practice, and to support functional teams.
Finally, SHOT continues to develop. The remit of the data collection, analysis and reporting has become considerably more comprehensive since the first report 20 years ago. This process is ongoing. As a world-leading haemovigilance programme, SHOT has a responsibility to collect data and improve safety in all areas of transfusion practice. This now includes collecting data on the donor process. But there remain domains of transfusion practice outwith the scope of our data collection, such as transfusion and administration of blood components given in the primary care setting and in general practitioner led units. We are working with key representatives of the primary care community to establish the size of such practice and whether it will be possible in the future to audit this area, where appropriate making safety recommendations.
We very much hope that the next 20 years of SHOT will be as successful, and see as much development, as the last 20.
The bedside check is vital in preventing transfusion error. Staff should be vigilant in checkingidentification details of the component against those of the patient. Every hospital should have apolicy for formally checking the identity of the patient against the blood component label at thebedside. Nursing observations during transfusion also show wide variation. National guidelines forthe administration and monitoring of transfusion are being developed by the British Committee forStandards in Haematology (BCSH) on behalf of the British Society for Haematology (BSH).
References
Department of Health (DH). Safe transfusion practice: use a bedside checklist (CAS) CEM/CMO/2017/005 (2017). https://www.cas.dh.gov.uk/ViewandAcknowledgment/ViewAlert.aspx?AlertID=102663 [accessed 27 April 2018].
Love L et al. SHOT Annual Report 1996/1997 published 1998. Summary of recommendations, p4. www.shotuk.org/shot-reports/ [accessed 27 April 2018].
Figure 1.1:
Key recommendation
from the first SHOT
Report 1996-1997

ANNUAL SHOT REPORT 2017
72. Participation in UK Haemovigilance
Authors: Debbi Poles, Chris Robbie and Paula Bolton-Maggs
Reporting in 2017
Participation in UK haemovigilance became more streamlined in March 2017 following the introduction of ‘Phase 2’ of the unified UK haemovigilance project. This development aimed to link the separate online-reporting systems of the SHOT database (Dendrite), and the Medicines and Healthcare Products Regulatory Agency (MHRA) reporting system, serious adverse blood reactions and events (SABRE).
Following successful implementation, there is now a single point of entry to the system via SABRE, and reports to SHOT are accessed by clicking a link from within the SABRE workspace which allows reporters direct access to the associated SHOT questionnaire. This has reduced the need for a separate login, and has been well received amongst regular users (https://www.shotuk.org/shot-surveys/).
Participation in UK haemovigilance remains very high, and in the calendar year 2017 there were only two registered National Health Service (NHS) Trusts/Health Boards that did not make reports to either SHOT or the MHRA.
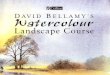
Analysis by the MHRA shows that only 31/280 SABRE accounts have not made a single report since the start of 2017 (Figure 2.1) and all, apart from three very small individual NHS hospitals in Scotland, are either private hospitals or facilities demonstrating low activity. Most reporters have reported at least once in the preceding two months. This shows that for the majority of hospitals at least, participants are actively engaging in the UK haemovigilance reporting programme.
31
3 0 1 3 1 3 7 813
35
69
106
Pre 20
17Fe
b-17
Mar-17
Apr-17
May-17
Jun-1
7Ju
l-17
Aug-17
Sep-17
Oct-17
Nov-17
Dec-17
Jan-18
Date last reported
The introduction of the new combined reporting system has meant that now all reports made on SABRE are transferred to the SHOT database automatically. This has resulted in a small increase in the number of reports received by SHOT, although any that are not reportable to SHOT are subsequently withdrawn. In addition, a new reporting mechanism for anti-D immunisations has been added to the
Figure 2.1:
The last time a
report was received
on SABRE from
an active SABRE
account
Participation in UK Haemovigilance 2

ANNUAL SHOT REPORT 2017
8 2. Participation in UK Haemovigilance
SHOT database, which was previously a paper-based system, and this has also increased the number of reports received. Both factors have contributed to reporting levels rising again following a slight dip in 2016.
2475
32003435 3545 3568 3668
3965
3634
3959
2009 2010 2011 2012 2013 2014 2015 2016 2017
SHOT reporting by UK country
In total, 3959 reports were submitted to the SHOT database in 2017 and the breakdown by country, including component issues, is shown in Figure 2.3.
Full tables containing the breakdown of data from 2017 and previous years can be found in the supplementary information on the SHOT website www.shotuk.org.
8.3%
83.5%
4.8%
3.4%
Total components issued: 200,191Number of reports: 330
Reports per 10,000 component issued: 16.5
Total components issued: 2,029,453Number of reports: 3307
Reports per 10,000 component issued: 16.3
Total components issued: 113,017Number of reports: 189
Reports per 10,000 component issued: 16.7
Total components issued: 57,072Number of reports: 133
Reports per 10,000 component issued: 23.3
Figure 2.2:
Number of reports
submitted to SHOT
2009-2017
Figure 2.3:
Percentage of
SHOT reports
submitted by UK
country

ANNUAL SHOT REPORT 2017
92. Participation in UK Haemovigilance
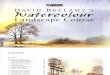
Cases included in the 2017 Annual SHOT Report n=3230
The total number of reports analysed and included in the 2017 Annual SHOT Report is 3230. This is an increase of 139 from the 3091 reports analysed in the 2016 Annual SHOT Report. This number does not include 66 reports of anti-D immunisation.
The number of reports excluding ‘near miss’ (NM) and ‘right blood right patient’ (RBRP) is 1671 (1581 in 2016).
3230total reports
Near miss 1359RBRP 200
All errors
1671 incidents
Errors 85.5%
Pathological reactions
442 (26.5%)
Others (CS & UCT)
28 (1.7%)
Error reports
1201 (71.8%)
RBRP=right blood right patient; CS=cell salvage; UCT=unclassifiable complications of transfusion
Analysis of errors by location
The trends of error reports for different locations have been updated and included again this year. Emergency departments have continued the upward trend in reporting, and account for an increasing percentage of all error reports to SHOT, from approximately 5% of all errors in 2010 to almost 10% in 2017.
3453 54 56 52
7991 95
0%
2%
4%
6%
8%
10%
12%
0102030405060708090
100
2010 2011 2012 2013 2014 2015 2016 2017
Num
ber
of
rep
ort
s
d. Adult critical carec. General wards
b. Theatres a. Emergency departments
374474
393 385 405 426 467415
0%
10%
20%
30%
40%
50%
60%
050
100150200250300350400450500
2010 2011 2012 2013 2014 2015 2016 2017
Num
ber
of
rep
ort
s
68 71 66 58 60 5573 71
43
6855 56
72 7586 81
0102030405060708090
100
2010 2011 2012 2013 2014 2015 2016 2017
% o
f to
tal e
rro
r re
po
rts
0%
2%
4%
6%
8%
10%
0102030405060708090
100
0%
2%
4%
6%
8%
10%
12%
% o
f to
tal e
rro
r re
po
rts
2010 2011 2012 2013 2014 2015 2016 2017
Figure 2.4:
Categorisation of
reports analysed in
2017 n=3230
Figure 2.5:
Trend of error
reports from
different
departments

ANNUAL SHOT REPORT 2017
10 3. Headline Data: Deaths, Major Morbidity and ABO-Incompatible Transfusions
Author: Paula Bolton-Maggs
Key SHOT messages
• Errors account for 85.5% of all reported incidents (Figure 3.1)
• At each step in the transfusion process, do not assume that errors have not been made in previous steps; verify each step, particularly patient identification
• An increasing proportion of blood components are given to older medical patients with comorbidities. Physicians need to understand and manage risks of transfusion and to know about alternative treatment approaches for anaemia
• Resource allocation is critical: inadequate staffing, lack of training and poor supervision are all likely to be associated with an increased risk of error
• Emergency transfusion saves lives. Do not delay. Do not let the patient bleed to death or die from anaemia
• A culture of accountability (as distinct from blame) is integral to prevention of mistakes. Root cause analyses of all adverse incidents should be thorough and must identify attributable system-related and human factors so that appropriate actions can be instituted
Deaths where transfusion was implicated n=21
Major morbidity n=112
Possibly preventable 137 4.2%
Not preventable 333 10.3%
Errors 2760 85.5%
Errors85.5%
Figure 3.1:
Errors account
for the majority of
reports: 2760/3230
Headline Data: Deaths, Major Morbidity and ABO-Incompatible Transfusions3

ANNUAL SHOT REPORT 2017
113. Headline Data: Deaths, Major Morbidity and ABO-Incompatible Transfusions
HTR=haemolytic transfusion reaction; TAD=transfusion-associated dyspnoea; TACO=transfusion-associated circulatory overload
2
1
4
3
1
1
1
2
5
1
0 1 2 3 4 5 6 7 8
TACO
Delays
TAD
Under andovertransfusion
HTR
Number of cases
Preventable deaths n=14/21 (66.7%)
DefiniteImputability
ProbablePossible
HTR=haemolytic transfusion reaction; TAD=transfusion-associated dyspnoea; TACO=transfusion-associated circulatory overload
Most of the deaths attributable to transfusion are associated with delays and TACO. Review of cumulative data shows that pulmonary complications are the leading cause of transfusion-related death, but it is worrying that nearly a quarter were related to delays. In this period (2010-2017) there were two deaths from ABO-incompatible transfusion.
Pulmonarycomplications
73
22.8%
11.7%
8.1%
53.7%
3.7%
TRALI5
TACO60
TAD8
Febrile/allergicreactions
HTROther
Delays 31
16
11
5
44.1%
5.9%3.7%
HTR=Haemolytic transfusion reactions; TACO=Transfusion-associated circulatory overload; TRALI=Transfusion-related acute lung injury; TAD=Transfusion-associated dyspnoea
‘Other’ includes 1 each for transfusion-transmitted infection, post-transfusion purpura, transfusion-associated graft-versus-host disease and anti-D related; there were 5 in the avoidable, over or undertransfusion category and 7 deaths related to other unclassified reactions
Errors without harm to patients n=1559 (near miss and right blood right patient reports).
Other errors with actual or potential harm n=1201 (handling and storage errors, avoidable and delayed transfusions, anti-D immunoglobulin errors and incorrect blood component transfused); Figure 2.4 in Chapter 2, Participation in UK Haemovigilance Reporting.
Figure 3.2:
Deaths related
to transfusion
(with imputability)
reported in 2017
n=21
Figure 3.3:
Transfusion-related
deaths 2010 to
2017 n=136

ANNUAL SHOT REPORT 2017
12 3. Headline Data: Deaths, Major Morbidity and ABO-Incompatible Transfusions
Missed irradiation of cellular components where indicated
Irradiation of cellular components was missed in 87 patients in 2017. In 77 (88.5%) cases the error was made in clinical areas and 10 in the laboratory. The cumulative number of reports of patients known to have missed irradiation is now 1397 since 1999. Patients were exposed to one or more components. Detailed analysis of 554 reports 2010-2016 established that the range of non-irradiated components transfused was 1 to 486 (a patient with Hodgkin lymphoma). The number of components was not reported for 61 cases (Elliot et al. 2018).
406
62
16 9
1-4 components 5-10 components 11-20 components >20 components
There have been no cases of transfusion-associated graft-versus-host disease reported since 2001 in patients who received leucodepleted red cells. Irradiation of cellular components for susceptible patients was introduced several decades ago and guidelines were published in 1996, and revised in 2010 (BSH Treleaven et al. 2010). The case reported in 2012 was caused by an intrauterine transfusion (IUT) with maternal blood (not leucodepleted, not irradiated and human leucocyte antigen (HLA)-related). None of the 13 cases reported up to 2001 occurred in patients with conditions where irradiation was recommended in the guidelines: 6 occurred in patients with B-cell diseases; 3 after cardiac surgery; 2 had no recognised risk factors. Two others were subsequently found to have immune deficiency. At least 4/13 were documented to have shared HLA haplotypes with their red cell donors and two received red cells less than 7 days old.
IUT=intrauterine transfusion
4 4 4
1 1
Leucodepletion introduced in 1999
IUT with maternal blood
Estimated risks for red cell units exceeding >5x106 leucocytes/unit is 1:1000 >1x106 leucocytes/unit is 1:200
1996
/97
1997
/98
1998
/99
1999
/00
2000
/01
2001
/02 2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
30-35 million components transfused
IUT=intrauterine transfusion.
Figure 3.4:
Number of
components received
by individual patients
who were exposed
to non-irradiated
components 2010 to
2016 n=493
Figure 3.5:
Cases of transfusion-
associated graft-
versus-host disease
reported to SHOT
since 1996

ANNUAL SHOT REPORT 2017
133. Headline Data: Deaths, Major Morbidity and ABO-Incompatible Transfusions
Summary data and risks associated with transfusion
Data collected in 2017 are shown in Figure 3.6. Near miss reporting continues to teach valuable lessons and contributed to 1359 (42.1%) of the total 3230 reports.
Cumulative data for 21 years are shown in Figure 3.7.
00
1311
172029
42
9295101
200243
284307
426
TAGvHD: Transfusion-associated graft-vs-host disease
PTP: Post-transfusion purpura
TTI: Transfusion-transmitted infection
TRALI: Transfusion-related acute lung injury
UCT: Unclassifiable complications of transfusion
CS: Cell salvage
TAD: Transfusion-associated dyspnoea
ADU: Over or undertransfusion and PCC
HTR: Haemolytic transfusion reactions
TACO: Transfusion-associated circulatory overload
ADU: Delayed transfusion
ADU: Avoidable transfusion
RBRP: Right blood right patient
HSE: Handling and storage errors
FAHR: Febrile, allergic and hypotensive reactions
IBCT: Incorrect blood component transfused
Anti-D: Anti-D immunoglobulin errors
NM: Near miss 1359
Possibly preventableNot preventableError
0 500 1000 1500 2000 2500 3000 3500 4000 4500 5000
IBCT: Incorrect blood component transfusedAnti-D: Anti-D immunoglobulin errors
HSE: Handling and storage errorsADU: Avoidable transfusion
ADU: Delayed transfusionADU: Over or undertransfusion and PCC
HTR: Haemolytic transfusion reactionsAllo: Alloimmunisation
TAGvHD: Transfusion-associated graft-vs-host diseaseTACO: Transfusion-associated circulatory overload
TRALI: Transfusion-related acute lung injuryTAD: Transfusion-associated dyspnoea
FAHR: Febrile, allergic and hypotensive reactionsCS: Cell salvage
TTI: Transfusion-transmitted infectionPTP: Post-transfusion purpura
UCT: Unclassifiable complications of transfusion
Adverse incidentsdue to mistakes
2017Cumulative to 2016
Transfusion reactions which may not be preventable
Possibly or probably preventable by improved practice and monitoring
Risks for transfusion are calculated per 100,000 components issued. This translates into a risk of death close to 1 in 114,000 and of serious harm close to 1 in 21,000. These risks are considered in relation to other risks of daily living in Figure 3.8. The risks of transfusion-transmitted infection are much lower than all other transfusion-related complications.
Figure 3.6:
Summary data for
2017 all categories
n=3230 (ranked by
number)
Figure 3.7:
Cumulative data for
SHOT categories
1996 to 2017
n=19815

ANNUAL SHOT REPORT 2017
14 3. Headline Data: Deaths, Major Morbidity and ABO-Incompatible Transfusions
Total morbidity 4.67 per 100,000 components issued 1 in 21,426
Total mortality 0.88 per 100,000 components issued 1 in 114,273
1 in 100 million
Approximate risks of transfusion complications compared with other risks, UK data
Transfusion-related deaths(by component issued)
Risk of pulmonarycomplications
Transfusion-related deathdue to error
1 in 10 million
1 in 1 million 1 in 100,000 1 in 10,000 1 in 1,000 1 in 100 1 in 10
Death from TACO (2016)
Risk of febrile/allergic/hypotensive reaction
Death from transfusion (ISTARE) Road deaths
Smoking-related deaths
Preventable hospital deaths
Death from external injury
Death from lightning strike Drowning
Alcohol-related deaths
Air traffic accident deaths
HCV HIV
HIG
HE
R R
ISK
LOW
ER
RIS
K
HBV
Sources of data: Many of these are found online in the UK office for national statistics. Red outline indicates SHOT data, blue outline indicates data from other sources. ISTARE is the International Haemovigilance Network database for the surveillance of adverse reactions and events in donor and recipients. Viral transmissions denote risk of infection, not deaths. HCV=hepatitis C virus; HIV=human immunodeficiency virus; HBV=hepatitis B virus. A full list of sources is available in supplementary information on the SHOT website www.shotuk.org.
ABO-incompatible red cell transfusions n=1
A single ABO-incompatible red cell transfusion was reported in 2017. This was a clinical administration error due to failure to complete the bedside check and is fully described in Chapter 10, Incorrect Blood Component Transfused (IBCT) (Case 10.2). The patient suffered some symptoms but recovered fully.
The trend over time towards reduced numbers of (potentially lethal) ABO-incompatible red cell transfusions is encouraging (Figure 10.2). However, review of near miss data shows that these are the tip of a much larger iceberg. Data for 2016 and 2017 show that although there were 4 ABO-incompatible red cell transfusions there were 606 near misses where an ABO-incompatible transfusion would have resulted. Most of these in 2017, 317/342, resulted from wrong blood in tube (WBIT) errors. These will not be detected unless there is a previous record in the transfusion laboratory and demonstrate the importance of the group-check policy (BSH Milkins et al. 2013). In reports of WBIT samples, the majority of institutions (77.4%) had this policy in place and 215 instances of WBIT were detected as a result of this (Chapter 12, Near Miss Reporting). These errors, which could have lethal outcomes, demonstrate the importance of correct patient identification at the time of sampling, and also the correct full completion of the final bedside check (a rule not a guideline, see Chapter 4, Key Messages and Recommendations).
Table 3.1:
Risks of death or
major morbidity from
transfusion in 2017
Figure 3.8:
Risks associated
with transfusion
compared with other
potential life events

ANNUAL SHOT REPORT 2017
153. Headline Data: Deaths, Major Morbidity and ABO-Incompatible Transfusions
4
606
ABO-incompatible red cell transfusions
ABO-incompatible near miss events
155
52
29
1996 – 2005 2006 – 2017
DeathsMajor morbidity
In addition to the single ABO-incompatible red cell transfusion in 2017, there were 4 inadvertent transfusions of ABO-incompatible fresh frozen plasma and two of platelets; no harm resulted.
These incidents and others described in previous years demonstrate that staff involved in transfusion do not check compatibility properly at the time of transfusion. Staff must not assume that the bag in their hands is necessarily safe. Compatibility check is one of the essential steps in the bedside check (BSH Robinson et al. 2018, DH 2017).
Figure 3.9:
ABO-incompatible
red cell
transfusions 2016
and 2017
Figure 3.10:
Reduction of
ABO-incompatible
transfusion of red
cells resulting in
death or major
morbidity over two
decades of SHOT
reporting

ANNUAL SHOT REPORT 2017
16 3. Headline Data: Deaths, Major Morbidity and ABO-Incompatible Transfusions
References
BSH Milkins C, Berryman J et al. Guidelines for pre-transfusion compatibility procedures in blood transfusion laboratories. Transfus Med 2013;23(1):3-35. http://onlinelibrary.wiley.com/doi/10.1111/j.1365-3148.2012.01199.x/full [accessed 21 February 2018].
BSH Robinson S, Harris A et al. The administration of blood components: a British Society for Haematology Guideline. Transfus Med 2018;28(1):3-21. http://onlinelibrary.wiley.com/doi/10.1111/tme.12481/full [accessed 26 February 2018].
BSH Treleaven J, Gennery A et al. Guidelines on the use of irradiated blood components prepared by the British Committee for Standards in Haematology blood transfusion task force. Br J Haematol 2010;152(1):35-51.
Department of Health (DH). Safe transfusion practice: use a bedside checklist (CAS) CEM/CMO/2017/005 (2017). https://www.cas.dh.gov.uk/ViewandAcknowledgment/ViewAlert.aspx?AlertID=102663 [accessed 19 February 2018].
Elliot J, Addison J et al. Outcome of failure to irradiate cellular components: a retrospective review of SHOT reports 2010-2016. Br J Haematol 2018;181 (Suppl. 1):143.

ANNUAL SHOT REPORT 2017
174. Key Messages and Recommendations
Authors: Paula Bolton-Maggs and Mark Bellamy
In every year of SHOT reporting, now 21 years, most incidents result from mistakes, often multiple, in the transfusion process. Training in basic blood group systems must not be overlooked, and continued removal of humans from the process by the use of information technology solutions can improve safety. Assumptions must not be made from one step to the next in the nine steps in the transfusion process. Verify and check.
Transfusion-associated circulatory overload (TACO) and other pulmonary complications remain the most commonly reported cause of major morbidity and death. The national comparative audit of TACO performed in 2017 included 2461 inpatient and 2119 outpatient transfusions in patients over 60 years of age (NCA 2018). Only 20.5% of inpatients were risk-assessed for TACO; fewer had assessments between units or haemoglobin checks although 89.2% of patients had at least one risk factor for TACO in addition to age. These findings indicate that more education about TACO is needed and the audit report recommends that a formal pre-transfusion risk-assessment should be included in hospital transfusion policies. We have therefore included this as our third key recommendation for 2017.
Key SHOT messages
• Guidelines or rules? Guidelines must not be translated into inflexible rules which may put patients at risk. Proportionate application of knowledge and experience may lead to a different course of action in individual circumstances. However, the final bedside check is a rule and must be completed in full
• Basic training: It is essential that all staff participating in transfusion fully understand ABO groups so that they can recognise potential ABO-incompatibility
• Information technology (IT) systems have the potential to increase transfusion safety by minimising human factors and should be considered for all transfusion steps
• Patients who develop respiratory distress during or up to 24 hours after transfusion where transfusion is suspected to be the cause must be reported to SHOT. The national comparative audit of TACO in 2017 demonstrated that risk factors are being missed
Guidelines are not rules
British Society of Haematology (BSH) and other guidelines are valuable tools to encourage safe practice but must be interpreted in the light of an individual patient’s clinical circumstances (Shah and Cifu 2018). We noted before that the guidance to avoid transfusion at night was interpreted wrongly as ‘never transfuse at night’ since for some patients with urgent clinical indications this must not be delayed (see also key message and Case 11a.3 in Chapter 11, Avoidable, Delayed or Undertransfusion (ADU)).
Patients should not die from bleeding or anaemia. Experienced clinicians can make appropriate decisions about concessionary release of alternatives (Case 11d.2). Delayed transfusion for patients with antibodies has resulted in death (Case 11a.1). In other cases, early consultation with senior colleagues may have averted serious consequences (Cases 11a.7, 11a.10). Rigid adherence to guidelines can promote wrong practice (Cases 14.2 and 14.3 in Chapter 14, Adverse Events Related to Anti-D Immunoglobulin (Ig)).
Key Messages and Recommendations 4

ANNUAL SHOT REPORT 2017
18 4. Key Messages and Recommendations
Knowledge of basic ABO and Rh blood group systems
Although the absolute number of ABO-incompatible transfusions has decreased with time, the number of near miss events that could have resulted in an ABO-incompatible transfusion (n=606 in the past 2 years) demonstrates the danger below the surface. Many incidents can be prevented by the final bedside check, as noted several times in Annual SHOT Reports and now endorsed by the Chief Medical Officer (DH 2017). There is no excuse for omission of this safety check.
An ABO-incompatible transfusion reported in the 2015 Annual SHOT Report (Case 6.1) had 12 different errors (Bolton-Maggs et al. 2016). The biomedical scientist selected incompatible units and the laboratory information management system (LIMS) permitted their electronic issue (not validated adequately after an upgrade). This incompatibility should have been detected at the bedside (group B units to a group O patient) but this was not detected on three separate occasions by at least two different nurses as the patient received all three units (across a shift change). This and other reports demonstrate that there is a lack of adequate knowledge of basic ABO and D blood group systems. A compatibility check is an essential part of the bedside process. This year we noted 4 ABO-incompatible transfusions of fresh frozen plasma (FFP), group O FFP to non-group O patients. LIMS should be set up to prevent release of group O FFP to any patients other than group O; for further details see Chapter 10, Incorrect Blood Component Transfused (IBCT). It is not sufficient for clinical staff to think it is only the responsibility of the transfusion laboratory staff. Similar facts apply to knowledge of a patient’s specific requirements, it is the responsibility of the clinician authorising the transfusion to know these, and the person administering the transfusion to check.
Key recommendation 1
• Training in ABO and D blood group principles is essential for all laboratory and clinical staff with any responsibility for the transfusion process. This should form part of the competency assessments
Action: Hospital Chief Executives and Medical Directors, National Blood Transfusion Committee, Hospital Transfusion Teams
Information technology
The summary of the Annual SHOT Report for 1999-2000 noted that ‘information technology will prevent human error’ (Love et al. 2001) and recommended that computerised identification systems which ensure safe transfusion at the bedside ‘should now be evaluated’. From 2006 the Annual SHOT Reports have included a chapter giving details about incidents where IT was implicated. These reviews have been informative and show that IT needs to be set up properly, and that human work-arounds can still result in error. IT systems are vulnerable to cyber-attack so there remains a need for manual back up. Despite these apparent disadvantages IT systems play an important role in transfusion safety, not only the essential role of LIMS but also vein-to-vein electronic blood management systems. These are of proven benefit and are recommended in the United Kingdom Transfusion Laboratory Collaborative (UKTLC) standards (Chaffe et al. 2014). Further information and justification and references are available in Chapter 12, Errors Related to Information Technology.
Key recommendation 2
• All available information technology (IT) systems to support transfusion practice should be considered and these systems implemented to their full functionality. Electronic blood management systems should be considered in all clinical settings where transfusion takes place. This is no longer an innovative approach to safe transfusion practice, it is the standard that all should aim for
Action: Hospital Chief Executives, Hospital Risk Managers and Hospital Transfusion Teams

ANNUAL SHOT REPORT 2017
194. Key Messages and Recommendations
Transfusion-associated circulatory overload
Respiratory complications remain the most common cause of major morbidity and death related to transfusion (Figures 3.2 and 3.3). Clinical staff should assess each patient prior to transfusion. Risk factors are not being recognised, and some cases of TACO are preventable.
Key recommendation 3 (repeated from last year)
• A formal pre-transfusion risk assessment for transfusion-associated circulatory overload (TACO) should be undertaken whenever possible, as TACO is the most commonly reported cause of transfusion-related mortality and major morbidity
Action: All staff authorising transfusion
References
Bolton-Maggs PHB, Poles D et al. The Annual SHOT Report 2015 (2016) www.shotuk.org [accessed 3 April 2018].
Chaffe B, Glencross H et al. UK Transfusion Laboratory Collaborative: minimum standards for staff qualifications, training, competency and the use of information technology in hospital transfusion laboratories. Transfus Med 2014;24:335–340.
Department of Health (DH). Safe transfusion practice: use a bedside checklist (CAS) CEM/CMO/2017/005 (2017). https://www.cas.dh.gov.uk/ViewandAcknowledgment/ViewAlert.aspx?AlertID=102663 [accessed 22 February 2018].
Love EM, Jones H et al. on behalf of the SHOT Steering Group. Key Observations and Recommendations Summary of Annual Report 1999–2000, 2001 www.shotuk.org [accessed 13 April 2013].
NCA. National comparative audit of blood transfusion: 2017 transfusion-associated circulatory overload audit. http://hospital.blood.co.uk/safe_use/clinical_audit/national_comparative/index.asp.
Shah SD and Cifu AS. From guideline to order set to patient harm. JAMA 2018;319:1207.

ANNUAL SHOT REPORT 2017
20 5. Donor Haemovigilance
Author: Dr. Shruthi Narayan, Consultant Donor Medicine, NHS Blood and Transplant (NHSBT)With contributions from:
Phil Carter, Senior Nurse Practitioner, Clinical Support Team; NHS Blood and Transplant (NHSBT)
Dr. Angus Wells, Clinical Director Donors and Manufacturing, and Dr. Jayne Hughes; Scottish National Blood Transfusion Service (SNBTS)
Dr. Mark Bridgham, Locum Consultant Haematologist, Northern Ireland Blood Transfusion Service (NIBTS)
Dr. Janet Birchall, Medical Director, and Joan Jones, Head of Service Development; Welsh Blood Service (WBS)
Key messages
• Whole blood and component donation is generally safe but complications do occur sometimes
• Donors need a clear understanding of what, when and how to report adverse events
• Vasovagal events resulting in donor hospitalisation or injury and nerve injuries post venepuncture continue to be the most commonly reported serious adverse events of donation (SAED)
Background
Blood donations save lives and improve health. It is only through regular voluntary contributions from blood donors that we can ensure a safe and sustainable supply of blood to patients. Blood donation is safe for most donors but a small proportion may suffer an adverse event. Even a relatively minor adverse event can impact the donor experience and retention. In more severe cases, donors may suffer an injury or disability following donation. Donor haemovigilance, the systematic monitoring and surveillance of such adverse events, helps improve donor and overall transfusion safety.
Data
The following table summarises the whole blood and apheresis donations collected in the four UK Blood Transfusion Services last year with a total of 1,913,650 donations (whole blood and component) collected.
Donor Haemovigilance5

ANNUAL SHOT REPORT 2017
215. Donor Haemovigilance
Donations from 2017 NHSBT SNBTS NIBTS WBS
Whole blood
Donations from male donors
716,366 71,045 23,699 44,942
Donations from female donors
819,707 80,997 20,029 44,062
Donations from new donors
143,148 12,800 4,208 13,362
Donations from repeat donors
1,392,925 139,242 39,520 75,642
Apheresis
Donations from male donors
68,618 9,349 3,992 2,082
Donations from female donors
7,101 794 465 402
Donations from new donors
168 0 112 71
Donations from repeat donors
75,551 10,143 4,345 2,413
Total number of donations in 2017 1,611,792 162,185 48,185 91,488
All donor adverse events are recorded according to the revised 2014 ‘Standards for Surveillance of Complications Related to Blood Donation’ (Goldman et al. 2016, ISBT 2014) which have helped harmonise reporting and permit benchmarking of the data in all the blood transfusion services.
SAED are those which either result in donor hospitalisation, interventions, significant disability/incapacity persisting for >1-year post donation or rarely death. SAED are investigated by the accountable Blood Service and reported to the Medicines and Healthcare Products Regulatory Agency (MHRA) in a timely manner. In addition, the donor SAED are classified as definitely, probably or possibly linked to donation. European legislation (European Blood Directives 2002/98/EC and 2005/61/EC) which has been subsequently transposed into UK law through the Blood Safety and Quality Regulations (BSQR) 2005 mandate submission of an annual overview of SAED and adverse events relating to the quality and/or safety of blood or components in donors and recipients.
The following caveats need to be considered in interpreting data in this report:
• All adverse events in this report are reported cases rather than confirmed cases
• We rely on donors reporting the delayed adverse events to Blood Services and these may be underreported if donors do not report and simply withdraw from future donations
• The adverse events definitions used for reporting in the four UK Blood Services has been consistent with current International Society for Blood Transfusion (ISBT) definitions only since 2016 hence data comparison prior to this must be done cautiously
• It is recognised that there is variation in the number/rate of SAED reported from each Blood Service but factors contributing to this have not been explored
The following table provides information relating to the total number of donations, number of whole blood donations, component donations and total number of SAED reported by each of the UK Blood Transfusion Services for the calendar year 2017 (January-December).
NHSBT SNBTS NIBTS WBS
Whole blood donations 1,536,073 152,042 43,728 89,004
Apheresis/component donations 75,719 10,143 4,457 2,484
Total donations 1,611,792 162,185 48,185 91,488
Total number of donor SAED in the calendar year 2017
46 3 0 1
Rate of SAED per 10,000 donations in UK
This equates to a rate of 0.26 SAED per 10,000 donations or 1 SAED per 38,273 donations in UK
Table 5.1:
Cumulative data
from the UK Blood
Services 2017
Table 5.2:
Summary of SAED
from the four UK
Blood Transfusion
Services for the
calendar year 2017
(Jan 2017–Dec 2017)

ANNUAL SHOT REPORT 2017
22 5. Donor Haemovigilance
Figure 5.1:
SAED by category
In total, there were 50 SAED reported, of which 46 were reported from NHSBT, 3 from SNBTS, 1 from WBS and none from NIBTS. The SAED reported from the four UK Blood Transfusion Services in 2017 fell into the following reporting categories:
NHSBT=National Health Service Blood & Transplant; SNBTS=Scottish National Blood Transfusion Service; WBS=Welsh Blood Service;
1
1
1
2
12
13
16
2
1
1
0 2 4 6 8 10 12 14 16 18
Other
Road traffic accident <24 hours of donation
Donor death <7/7 of donation
Acute coronary syndrome
Hospital admission within 24 hours of donation
Fracture
Arm pain >12/12 post donation
NHSBT SNBTS WBS
NHSBT=National Health Service Blood & Transplant; SNBTS=Scottish National Blood Transfusion Service; WBS=Welsh Blood Service
Trending data
There has been a steady reduction in the demand for blood in the last few years most likely resulting from effective implementation of Patient Blood Management and improved medical practices. A significant challenge to all the Blood Services is to maintain the right number and blood group mix of active donors to meet this overall decreasing demand coupled with a changing differential demand at the blood group level and to do so efficiently while retaining the goodwill of donors and maintaining high donor satisfaction.
Figure 5.2 demonstrates the steady fall in the number of donations collected in the UK.
2015 2016 2017
190,851
103,159
92,803
1,935,957
1,901,491
1,820,847
1,650,000
1,700,000
1,750,000
1,800,000
1,850,000
1,900,000
1,950,000
2,000,000
2,050,000
2,100,000
2,150,000Apheresis/component donationsWhole blood donations
Figure 5.2:
Trend in whole
blood and
apheresis
donations in the UK
from 2015-2017

ANNUAL SHOT REPORT 2017
235. Donor Haemovigilance
More SAED are being recorded which may reflect improved awareness through donor and staff education and therefore increased and more consistent reporting across the UK Blood Services. Donors are encouraged to get in touch if they experience problems post donation. Despite this the rate of SAED per 10,000 donations remains low.
2,126,808
2,004,650
1,913,650
0.200.21
0.26
0
0.05
0.1
0.15
0.2
0.25
0.3
1,800,000
1,850,000
1,900,000
1,950,000
2,000,000
2,050,000
2,100,000
2,150,000
2015 2016 2017
Total donations Rate of SAED reported per 10,000 donations
SAED=serious adverse event of donation
Case 5.1: Donor with delayed faint involved in road traffic collision within 24 hours of donation
A young female whole blood donor had an uneventful first donation. Following donation, the donor had a delayed faint whilst driving her car out of the venue car park. The donor was transferred to the local emergency department (ED) by ambulance. No injuries were sustained by the donor. The donor was found to be hypotensive and discharged from the ED following treatment with intravenous (IV) fluids. The donor has been withdrawn from blood donation. A root cause analysis confirmed that all standard procedures were followed and nothing could be identified that needed to be addressed to be able to prevent this SAED.
Adverse events relating to blood donation can occur during or after donation. Delayed complications are defined as complications which occur after the donor has left the donation venue. Delayed vasovagal reactions are a well-recognised but poorly understood complication of blood donation. They are thought to occur because of failure of the donor’s normal compensatory reflexes to respond to the volume loss associated with donation. Inadequate fluid intake post donation, prolonged standing and high environmental temperature are recognised factors increasing the risk of a delayed vasovagal reaction. Delayed reactions occur more frequently in female donors than in male donors. Off-site reactions, particularly in female donors, have been reported to be more likely to be associated with a fall, with head trauma, with other injury, and with the use of outside medical care (Kamel 2010).
Blood donation is safe, but a small proportion of donors have delayed and/or off-site reactions that have the potential to lead to serious injury. Post-donation information must be provided to all donors. This should include the risk of delayed reactions and advice on prevention, in particular, advice on maintaining post-donation fluid intake, and avoidance of known precipitating factors such as overheating, and prolonged standing. Women are more likely than men to report delayed reactions. Delayed and off-site reactions lead to potentially preventable morbidity. Understanding the physiologic basis of such delayed reactions may lead to the development of appropriate interventions to reduce their likelihood.
Figure 5.3:
Trends in donations
and reported rate
of SAED in UK
Blood Services

ANNUAL SHOT REPORT 2017
24 5. Donor Haemovigilance
Case 5.2: Venepuncture related persistent arm pain >1-year post donation
A female regular whole blood donor who had donated 11 times previously reported problems with her donation arm which had persisted for longer than 12 months post donation. The donor reported the venepuncture being painful and the donation being slow. The donation was discontinued appropriately before the full volume could be collected. The donor had local bruising for several days after donation and intermittent pain to the inner aspect of her elbow radiating down her wrist and up her upper arm. She also reported weakness in her arm when performing tasks. The donor is under the care of her general practitioner (GP) and may be referred to a specialist. The donor has been withdrawn from blood donation.
Peripheral nerve injuries have been described after venepuncture (Newman 2013). Nerves in the antecubital fossa classically lie on a plane just beneath, and in close proximity to, the veins, making them susceptible to injury during phlebotomy; also, it has been shown that there is a large range of anatomic variation, suggesting that even a non-traumatic, satisfactory venepuncture can directly damage these nerves. Needle-related complications include haematoma, arterial puncture and painful arm, which may result from nerve irritation through a haematoma or from direct injury to a nerve or other structure. It is recognised that arm symptoms from needle-related complications may take several weeks or longer to resolve, and these complications are usually over-represented among reported cases where there is long-term morbidity following a blood donation. Nerve injuries may not be completely avoidable because the nerve anatomy is variable and the nerves cannot be palpated. Most nerve injuries resolve, but in a small number of cases, it may take months, and in rare instances, there may be permanent injury. Nerve injuries are the most common cause of disability among donors. Good phlebotomy technique can minimise the incidence of painful arms. Nerve injury is usually immediately apparent with donors reporting a sharp, burning or electrical pain radiating to the lower arm or into the hand/fingers and in some cases also proximally. Donors may also experience paraesthesiae. This must be recognised by staff who insert needles and in donors reporting severe pain, the needle should be removed immediately.
References
BSQR. The Blood Safety and Quality Regulations ISBN 0110990412; 2005. http://www.legislation.gov.uk/uksi/2005/50/contents/made [accessed 13th March 2018].
EU Directives: http://ec.europa.eu/health/blood_tissues_organs/key_documents/index_en.htm#anchor0_more [accessed 13th March 2018] Then click Blood-Legislation and Guidelines to expand list and select each option below:
Directive 2002/98/EC of The European Parliament and of the Council of 27 January 2003 setting standards of quality and safety for the collection, testing, processing, storage and distribution of human blood and blood components and amending Directive 2001/83/EC [2003] OJ L33/30. Available at http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32002L0098&from=EN [accessed 13th March 2018].
Commission Directive 2005/61/EC of 30 September 2005 implementing Directive 2002/98/EC of the European Parliament and of the Council as regards traceability requirements and notification of serious adverse reactions and events [2005] OJ L 256/32. Available at http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32005L0061&from=EN [accessed on 13th March 2018].
Goldman M, Land K et al. Development of standard definitions for surveillance of complications related to blood donation. Vox Sang 2016;110:185–188.
ISBT. Standard for Surveillance of Complications Related to Blood Donation, 2014. http://www.isbtweb.org/working-parties/haemovigilance/ (click on definitions then Revised Standard 2014 Surveillance complications blood donation) [accessed 13th March 2018].
Kamel H, Tomasulo P et al. Delayed adverse reactions to blood donation. Transfusion 2010;50: 556-565.
Newman B (2013). Arm Complications After Manual Whole Blood Donation and Their Impact, Transfus Med Rev 2013;27(1):44 – 49.

ANNUAL SHOT REPORT 2017
255. Donor Haemovigilance
Serious Adverse Events following Blood Donation reported to the UK Blood Services in 2017
In 2017 the UK Blood Services collected approximately 1.9 million donations. Fifty serious adverse events of donation (SAED) have been reported last year (1 in 38,273 donations). Serious adverse events are very rare but do occur and can have a significant impact on donor health and donor retention
Breakdown of Serious Adverse Events in 2017
SAED Categories
Female donors accounted for nearly 2/3 of SAED reported
18/50 SAED were as a direct result of a
delayed vasovagal reaction
34%
36%
17/50 SAED were related to persistent arm problems more than one year post
donation
No reports of anaphylaxis, haemolysis or air embolism due to component donation reported in 2017
All 15 fractures were related to vasovagal reactions, 2 immediate and 13 delayed reactions
There was one report of a donor death <7 days of donation and two reports of acute coronary syndrome <24 hours of donation
In general 9/10 donors who suffer an SAED are withdrawn from future donations
Death , 1
Hospital admission,
13
Fracture, 15
Other, 1RTC, 1
Arm problems >12/12 …
ACS, 2
Donors need a clear understanding of what, when and how to report
adverse events
Vasovagal events resulting in donor hospitalisation or
injury and nerve injuries post venepuncture continue
to be the commonly reported SAED
Whole blood and component donation is safe
but complications do sometimes occur
Key Messages
ACS=acute coronary syndrome RTC=road traffic collision

ANNUAL SHOT REPORT 2017
26

27
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
ERROR REPORTS: Human Factors
Chapter
ERROR REPORTS: Human Factors6 Human Factors in SHOT Error Incidents ........................................Alison Watt and Paula Bolton-Maggs7 Laboratory Errors ............................................................ Peter Baker, Heather Clarke and Hema Mistry8 Right Blood Right Patient (RBRP) ..........................................................Diane Sydney and Hema Mistry9 Handling and Storage Errors (HSE) ........................................................Diane Sydney and Hema Mistry10 Incorrect Blood Component Transfused (IBCT) ....................................................................................... .............................Jayne Addison, Peter Baker, Heather Clarke, Hema Mistry and Paula Bolton-Maggs11 Avoidable, Delayed or Under or Overtransfusion (ADU) ............... Paula Bolton-Maggs and Caroline Wall a. Delayed Transfusions b. Avoidable Transfusions c. Under or Overtransfusion d. Incidents related to Prothrombin Complex Concentrates12 Near Miss Reporting (NM) .........................................................................Alison Watt and Katy Cowan13 Errors Related to Information Technology (IT) ..................................................................Megan Rowley14 Adverse Events Related to Anti-D Immunoglobulin (Ig) .......................... Clare Denison and Katy Cowan15 Immune Anti-D in Pregnancy: Cases reported up to the end of 2017 .................................Jane Keidan
Page
272834515558
818290959799104106114

28
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
6. Human Factors in SHOT Error Incidents
Authors: Alison Watt and Paula Bolton-Maggs
Key SHOT messages
• Reporters are encouraged to familiarise themselves with human factors concepts, particularly by using the SHOT human factors tuition package https://www.shotuk.org/reporting/human-factors-tuition-package/, which includes a useful video link https://t.co/qTeUoPiUlq
• Staff investigating errors in the transfusion process are advised to examine systems failures, so they can identify contributory causes beyond failure by an individual
The importance of considering human and organisational factors when reporting transfusion incidents has been highlighted by SHOT, because over the past two decades it has been established that most incidents are caused by human errors in the transfusion process. In 2016 the International Organisation for Standardisation (ISO) published a standard related to human factors (ISO 27500) which sets out high-level human-centred principles for executive board members in organisations to endorse (see below).
In order to understand how transfusion errors can be affected by human factors, a bespoke human factors investigation tool (HFIT) (Gordon et al. 2005) was created and linked to the SHOT database (Dendrite) from January 2016. Human factors questions were added in all error categories to examine which of four human factors was estimated to be implicated in each incident and it is these reports which make up the total 2760 reviewed for this summary. The reporters were asked to rate the contribution of each of the following:
• Unsafe practice by individual staff member(s)
• Unsafe conditions associated with the local environment or workspace
• Unsafe conditions associated with organisational or management issues in your Trust/Health Board (e.g. staffing levels)
• Conditions associated with the government, Department of Health or high level regulatory issues. This is not to score whether the error was reportable as a regulatory failure but to assess the impact of decisions made by regulators or conditions imposed by them
Analysis of the first year’s data from the HFIT indicated that reporters tended to attribute culpability mostly to individual staff members, 62.6% in 2016 (Bolton-Maggs et al. 2017) and scores were lower for any contribution of systems factors beyond the control of the individual. The pattern was similar in 2017, with 57.9% attributing culpability to individuals and 393/2760 (14.2%) scoring 10/10 for staff members and zero for all other factors.
Case 6.1: Total culpability attributed to individuals may fail to highlight system problems
A patient was issued and transfused platelets and red cells in separate incidents with only one group on record in the laboratory information management system (LIMS). In the morning a group and screen sample was processed and one unit of platelets was requested for the patient. The biomedical scientist (BMS) realised that there was no historic group on record for this patient and added the code to the report stating that if blood components were required, a second sample would be needed to confirm the patient’s group. In the early hours of the following day another BMS received a request for one unit of red cells and one unit of platelets. Having seen that a sample had
Human Factors in SHOT Error Incidents n=27606

29
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
6. Human Factors in SHOT Error Incidents
been received and processed earlier the day before, and that the patient had already received a unit of platelets, the BMS crossmatched red cells and issued these with a second unit of platelets, both of which were transfused although the patient had not yet had a group-check sample tested.
Case 6.1 was scored as 10 (maximum score) for individual culpability with no scores for other human factors. However, it is unlikely that two qualified, trained and competent individuals would make related mistakes if the systems were well designed to prevent errors. Other factors mentioned included workload issues, both were lone working, and in particular, the second incident occurred in the middle of the night. In addition, the second error was compounded by an assumption that the required testing had been done earlier and the important comment highlighting that it had not been done was at the bottom of the report. The corrective actions include updating the standard operating procedure (SOP) and adding a flag to the LIMS. These actions suggest there were system problems that contributed to the errors.
Studies have shown that culpability by the individual is expected to be about 10% (Reason 1997; Karl 2012) so it is likely that the higher percentages reported to SHOT are due to a lack of awareness of system failure issues among incident reporters, who would not be expected to have an in-depth knowledge of human factors. Therefore, from January 2017 a self-learning package was made available showing examples of scoring human and organisational factors. This package was published on the SHOT website http://www.shotuk.org/reporting/human-factors-tuition-package/ and includes real case studies from the first year of reporting in 2016.
It would be unrealistic to expect reporters to read the self-learning package on each occasion they report errors to SHOT, so a question was asked about if and when they have read the package. This was designed to give an indication of whether the reporters have studied how to assess the implicated human factors before recording their scores and if so, how recently did they do this (Figure 6.1).
HF=human factors
569
1296
317227
75152
3094
When making this report
On a previous occasion Not read at all No answer given
Read/not read self-learning package
Scored for HFNot scored for HF
HF=human factors
Figure 6.1 shows that 644/2760 (23.3%) reports were made by individuals who had read the self-learning package on this occasion and 1448/2760 (52.5%) by reporters who had read the package when reporting a previous error. There were 2092 reports made by individuals who had read the package either when making this report or on a previous occasion and of these, 1865/2092 (89.1%) included a score for human factors. In comparison 668/2760 (24.2%) indicated that the reporter had not read the self-learning package, either by a direct ‘no’ response to the question, or by not giving an answer, and of these 544/668 (81.4%) included a score for human factors. It is a little more likely that those who have read the self-learning package will then proceed to complete the questions about contributory human factors.
Figure 6.1:
Evaluation of uptake
of self-learning
opportunity and
whether reporters
are encouraged to
add scores to assess
the human factors

30
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
6. Human Factors in SHOT Error Incidents
Case 6.2: Failure to assign scores for human factors may reduce learning opportunities
A unit of red cells was transfused the day after the validity had expired for the sample used for crossmatch. No scores were assigned for contributory human factors and the reporter did not answer whether they had read the self-learning package, but important additional information implied system-related problems. This patient was transfusion-dependent and needed transfusing two or three times a week so samples used for crossmatching must be less than 72 hours old at transfusion. Units are crossmatched by the Blood Service (BS) due to antibody complexity and this can add delay between sampling and transfusion. To facilitate traceability, units issued via the LIMS have a default de-reservation period of 48 hours, so the date automatically prints on the compatibility label as two days later. When de-reservation is required after one day, because the sample validity would expire by then, the BMS must manually amend the label and annotate with the correct date. In this case, the BMS did not annotate the label with the correct de-reservation date and the unit was not de-reserved.
Corrective actions show there were system problems. These actions were listed as follows:
• A sample collection/testing schedule is to be created for all transfusion-dependent patients who require crossmatching by the BS
• Risk-assessment to determine whether 96 hours is more manageable for the patient’s quality of life compared to the possibility of forming new antibodies
• Problems with sample validity and changing of de-reservation dates on compatibility labels have been lodged with the provider to consider amendments to the LIMS
Analysing system problems like these identified in Case 6.2 could improve patient safety, and use of the SHOT HFIT questions could improve that analysis. The aim of adding the self-learning package was to encourage more accurate analysis of human and organisational factors contributing to errors. A comparison of reporters’ estimation of different human factors contribution to errors in both 2016 and 2017 shows a small increase in the contribution rated for organisational or environmental factors among those who had read the self-learning package (data not shown). This is a selection of comments made about the self-learning package, which were very positive:
The examples given of real incidents make it a useful tool
Very informative and useful and will make me think very differently when completing
this section
It made me think about the different factors involved
in the incident
Easy to read and undesrtand
Human Factors is an important consideration, so it is beneficial to convey this when reporting

31
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
6. Human Factors in SHOT Error Incidents
Commentary
It has been noted in several areas of SHOT reporting that the root cause analyses are not satisfactory and that the systems problems are not being recognised nor addressed. This has been noted by the MHRA and is one of the triggers for increasing the inspections in 2018 (Chapter 24, Medicines and Healthcare Products Regulatory Agency (MHRA)). If reporters start attributing incidents more to organisational factors, more could be learnt from those adverse events and this would give healthcare organisations the opportunity to resolve some of the underlying problems that are leading to errors.
This could have cost implications for the UK National Health Service (NHS), but there are also costs associated with continuing to experience serious, but preventable, incidents. These costs can be human as well as financial, such as serious harm or death caused to patients and the second victim costs related to adverse effects on staff who are being assigned sole blame for an error. Detrimental consequences for staff include losing their job, or suffering legal challenges and such outcomes for staff are likely to have a negative effect on healthcare organisations, with no improvement in patient safety.
Incorporation of a self-learning package into the process for reporting may encourage reporters to consider factors beyond the culpability of an individual. Further work will be needed to continue this improvement, so a revised self-learning package was published on the SHOT website from 01 January 2018. This has been enhanced with a link to a simple video giving more information about human factors. It is anticipated that reporting of human factors and system problems involved in transfusion incidents will improve over time as the messages about accurate examination of these aspects are disseminated. This in turn should lead to improved systems and a resultant higher level of patient safety.
ISO 27500
Other resources are available to assist learning and application of human factors, for example the ISO standard for human factors applicable to organisations (ISO 27500). Advice about application of behavioural psychology using the ‘Choices framework of behavioural drivers’ can be found at: https://www.mckinsey.com/business-functions/marketing-and-sales/our-insights/putting-behavioral-psychology-to-work-to-improve-the-customer-experience.
Lee Alford (invited by the Chair of a Pharma sub-group of the Chartered Institute of Ergonomics and Human Factors to lead a small working group to develop and raise awareness of the standard across the pharma sector) writes: In March 2016 the British Standards Institution (BSI) published BS ISO 27500: The human-centred organisation. Aimed at corporate board members, the standard explains the values and beliefs that make an organisation human-centred, the significant business and operational benefits that arise, and the policies they need to put in place to achieve this. The standard offers health and safety professionals the opportunities to raise the profile of wellbeing in their organisations. As a starting point a sub-group of the Chartered Institute of Ergonomics and Human Factors (CIEHF) has produced a survey to help organisations across the pharma and healthcare sectors to self-assess themselves against the seven principles and ways of application described in the standard. The survey is available at www.surveymonkey.co.uk/r/CF9QJRD.
Root cause analysis (RCA)
Author: Nina Vinall
When an incident or near miss occurs, it is easier and indeed quicker to come to the solution that it is a ‘human error’ as it is staff who are the ones who care for people in the NHS, yet staff do not come into work to purposefully cause harm.
So how do we find out what has gone wrong and learn from it? For organisations, teams and staff to fully understand why an incident happened and what is to blame, we must first understand the root cause(s), that is, the equipment, task, policy/protocol, the organisational situation to name a few, to truly get to the factors involved in the incident.
The National Patient Safety Agency (NPSA) website still provides a wealth of tools to support this

32
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
6. Human Factors in SHOT Error Incidents
way of investigating incidents and serious incidents. These enable the investigator to remove all subjectivity from the investigation process and allow objectivity only. This leads to truly understanding the reasons or ‘root causes’ of an incident. In identifying the root causes and realising that there are more factors involved that led to the incident, the organisation can then learn to look at their processes and policy which will inevitably reduce the risk of such an incident occurring again. This will also improve reporting of incidents or near misses, acting on the outcomes and lead overall to safer patient care. The items to support investigating using this method can be found at http://www.nrls.npsa.nhs.uk/resources/collections/root-cause-analysis/.
On this site you will find access to a presentation from NPSA’s RCA investigations (2011) and other tools such as the fishbone template (as seen below). Once familiar with these tools investigators become more confident in the outcomes and the organisation becomes more open to understanding there are other factors at play.
Team factors:
Role congruence
Leadership
Support + cultural factors
Communication factors:
Verbal
Written
Non-verbal
Management
Task factors:
Guidelines/
procedures/
protocols
Decision aids
Task design
Patient factors:
Clinical condition
Physical factors
Social factors
Psychological/
mental factors
Interpersonal
relationships
Individual (staff) factors:
Physical issues
Psychological
Social/domestic
Personality
Cognitive factors
Organisational +
strategic factors:
Organisational structure
Priorities
Externally imported risks
Safety culture
Equipment +
resources:
Displays
Integrity
Positioning
Usability
Education +
training factors:
Competence
Supervision
Availability/accessibility
Appropriateness
Working condition factors:
Administrative
Design of physical environment
Environment
Staffing
Workload and hours
Time
Problem
or issue
(CDP/SDP)
CDP=care delivery problem; SDP=service delivery problem
While root cause analysis has been part of health care and patient safety for several years, its successful application to identify and implement sustainable actions has been variable. There is a danger that health care professionals are starting to become complacent about the use of RCA and its techniques to the extent that RCA are being conducted in a more superficial manner. The fact that many RCA are conducted in and across Trusts for similar adverse events indicate that the RCA reports either did not yield sustainable solutions or were not comprehensive enough to deal with the problems and have long-lasting impact. We need to be conducting more credible RCA with tangible action plans which need to be measured to assess if they were effective in mitigating the risk. Only then will RCAs drive improvement in the process of reviewing events that cause or may cause serious harm, and in developing and implementing sustainable and measurable actions that prevent future harm to both patients and the workforce.
SHOT data have consistently shown that errors contribute to >80% of the events reported. To ensure safer transfusion practices and a consistent reduction in these errors, safe behaviours need to be identified, promoted and reinforced; safety processes that target the root cause of most incidents are vital. One such approach is a behaviour-based safety approach. This promotes interventions that are people-focused and often incorporate one-to-one or group observations of employees performing routine work tasks, setting goals carefully and giving timely feedback on safety-related behaviour, coaching and mentoring. These initiatives will have a proactive focus, encouraging individuals and their work groups to consider the potential for incident involvement and to assess their own behaviour as safe or unsafe always, no matter what. This will enhance performance and drive towards a safer culture thus promoting transfusion safety.
Figure 6.2:
Fishbone template
for analysis of root
causes

33
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
6. Human Factors in SHOT Error Incidents
References
Bolton-Maggs PHB (Ed), Poles D et al. (2017) on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. The 2016 Annual SHOT Report https://www.shotuk.org/wp-content/uploads/SHOT-Report-2016_web_11th-July.pdf [accessed 28 February 2018].
Gordon R, Flin R and Mearns K. Designing and evaluating a human factors investigation tool (HFIT) for accident analysis. Saf Sci 2005;43(3):147-171.
ISO 27500 The human-centred organisation – rationale and general principle https://www.iso.org/standard/64239.html [accessed 21 March 2018].
Karl R and Karl MC. Adverse events: root causes and latent factors. Surg Clin N Am 2012;92(1):89-100.
Reason J. Managing the risks of organizational accidents. Aldershot (UK): Ashgate; 1997.

34
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
7. Laboratory Errors
Authors: Peter Baker, Heather Clarke and Hema Mistry
Key SHOT messages for laboratory staff
Knowledge and skills:
• Laboratory staff should have an understanding of all component types, including their storage conditions, but most importantly their compatibility with the patient and specific requirements for certain patient groups e.g. gender, age, pregnancy and taking disease status into consideration (Chaffe et al. 2014)
• Laboratory staff are responsible for maintaining their own continuing professional development (CPD) including competency assessments (https://www.hcpc-uk.org/aboutregistration/standards/cpd/)
• Laboratory staff must understand warning flags, know why they have appeared and acknowledge appropriately. Warning flags should never be overridden by laboratory staff without understanding the reason for them. See information technology (IT) key message below
Shared responsibility and shared care:
• Good communication is paramount between staff in the laboratory, between the laboratory and the clinical area and vice versa
• It is important, when necessary, to look up, understand and maintain patients’ historical records and to seek out any further transfusion information that may be available for the patient from a shared care facility e.g. transplant, antibodies, adverse transfusion history. Never assume that something has been done: always double check
Information technology (IT):
• Laboratories should have a contingency procedure for IT downtime/failure and perform a simulated situation competency which renders the laboratory information management systems (LIMS) out of action in order to test that the contingency procedures are robust
• SHOT data continue to highlight many errors caused by overriding warning alerts. It is now time for LIMS suppliers to provide software that requires more than a keystroke to override the warning alert and meet the UK guidelines in transfusion (BSH Milkins et al. 2013, BSH Jones et al. 2014). Consideration could be given to allow the user to record a comment explaining the reason for the override which would certainly focus the mind of the issuing biomedical scientist (positive acknowledgment)
Summary
Laboratory errors continue to occur despite reflective best practice guidance each year in the Annual SHOT Report. Laboratory managers should not be pressurised to put partially-trained/untrained staff (contracted or locum) into positions where they undertake processes outside their competency.
Laboratory ErrorsSHOT Laboratory errors n=740
(409 errors and 331 near misses)7

35
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
7. Laboratory Errors
Failures to address long-term resource and staffing problems are being reported by laboratory managers and all the following organisations: SHOT, the UK Transfusion Laboratory Collaborative (UKTLC), the National Blood Transfusion Committee (NBTC), the UK National External Quality Assessments Scheme (UK NEQAS), and the Medicines and Healthcare Products Regulatory Agency (MHRA). It is apparent that staffing levels and numbers of qualified and knowledgeable biomedical scientist (BMS) staff are reducing and vacancies are remaining unfilled for many months (Chaffe et al. 2014, UKTLC 2017). These issues, together with increasing workloads and 24-hour routine working, are not going to be resolved in the short-term and it is imperative that laboratory managers review their processes to ensure that they are robust enough to meet these current challenges and guidelines. As new techniques, technologies and treatments emerge it is essential that robust processes and staff training are developed to mitigate potential errors within these new systems.
Processes need to be carefully planned to achieve consistent and safe outcomes for each task undertaken, and also need to consider when things do not go to plan. Procedures need to be as simple as possible, but as complex as they need to be, to ensure that staff have access to the correct instructions and information at the correct time. Training and education need to cover the situations that staff face on a daily basis. New staff need to be properly trained and supervised while they gain experience in their new working environment. Poor practice should be identified and corrected before it results in errors. The pathology services are under intense pressure in a climate where the workforce is stretched and under-staffed, therefore it is even more vital that vigilance and duty of care are upheld to ensure safe transfusion and patient safety.
A more thorough breakdown into laboratory errors is given in the remainder of the chapter.
Overview
This year there were 740 reports to SHOT where the primary error originated in the laboratory. Actual harm (where the patient was transfused, n=409) was far greater than the potential for harm (near misses where the patient was not transfused, n=331). This indicates key areas of weakness that need more care, attention and knowledge to ensure patient safety (Figures 7.1a and 7.1b). Figure 7.2 illustrates at which stage in the laboratory the error occurred and the outcome.
WCT=wrong component transfused; SRNM=specific requirements not met; HSE=handling and storage errors; RBRP=right blood right patient; Ig=immunoglobulin
47
111
7277
10
30
6259
72
8895
1
16
WCT SRNM HSE RBRP Avoidable Delayed Anti-D Ig
Laboratory errorsLaboratory near miss
WCT=wrong component transfused; SRNM=specific requirements not met; HSE=handling and storage errors; RBRP=right blood right patient; Ig=immunoglobulin
Figure 7.1a:
Laboratory
incidents and near
misses by category
of outcome n=740

36
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
7. Laboratory Errors
75
110
54
149
3
18
53 53 52
173
Sample receipt and registration
Testing Component selection
Component labelling
Collection Miscellaneous
Laboratory errorsLaboratory near miss
WCT=wrong component transfused; SRNM=specific requirements not met; HSE=handling and storage errors; RBRP=right blood right patient; Ig=immunoglobulin
3
3
24
10
7
8
1
21
63
18
72 58
1
18
8
2
2
12
1
9
6
5
6
8
19
24
0 20 40 60 80 100 120 140 160
Miscellaneous
Collection
Component labelling
Component selection
Testing
Sample receipt and registration
WCTSRNMHSERBRPAvoidableDelayedAnti-D Ig
WCT=wrong component transfused; SRNM=specific requirements not met; HSE=handling and storage errors; RBRP=right blood right patient; Ig=immunoglobulin
Sample receipt and registration errors n=75
Correct sample receipt and registration are essential to ensure that the right investigation is performed for the right patient on the right sample at the right time (dependent on the patient’s transfusion history).
Failure to act on the patient’s available historical information is the most common error at the sample receipt and registration stage (Figure 7.3).
Figure 7.1b:
SHOT laboratory
data (n=740)
showing at which
stage in the
transfusion process
the primary error
occurred
Figure 7.2:
SHOT laboratory
errors (n=409)
showing at which
stage in the
transfusion process
the primary error
occurred with
outcome

37
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
7. Laboratory Errors
WCTSRNMRBRPAvoidableDelayedAnti-D Ig
WCT=wrong component transfused; SRNM=specific requirements not met; RBRP=right blood right patient; Ig=immunoglobulin
2
5
8
10
1
17 1
1
3
1
2
1
23
0 5 10 15 20 25 30 35 40 45
Missed on request form
Demographic data entry error
Available historical information
WCT=wrong component transfused; SRNM=specific requirements not met; RBRP=right blood right patient; Ig=immunoglobulin
Learning points for sample receipt and registration errors
• Heed patient history: a patient’s historical records provide information about the patient’s transfusion requirements and should be clear and up to date. Laboratory staff must ensure that this is reviewed thoroughly at sample receipt and prior to testing and component selection. It can also indicate a patient’s specific requirement or serological history that may not be given on the clinical request form. If the transfusion history indicates a potential delay in providing a component, then the clinical area needs to be informed
• Sample acceptance: adhere to a zero-tolerance policy when accepting samples. The standard operating procedure (SOP) for sample acceptance by the laboratory must define locally agreed minimum acceptable identification criteria and the course of action to be followed when these criteria are not met. These should also comply with the British Society for Haematology (BSH) guidelines (BSH Milkins et al. 2013). Please note: If a sample is rejected, no further testing should be performed and the sample must be discarded. However, if testing is performed once a sample is to be rejected i.e. to confirm an erroneous sample, then this is reportable to SHOT. If the laboratory does not identify an incorrectly labelled sample and proceeds to test it, this is then also reportable to the Medicines and Healthcare Products Regulatory Agency (MHRA) as a failure in the quality management system (QMS) (EU 2016)
Case 7.1: Blood issued and transfused with incorrect spelling of forename
The clinical area notified the laboratory that they had removed, by remote issue, a unit of red cells from the blood refrigerator with an incorrect spelling of the patient’s forename. One unit of red cells had already been transfused to the patient with this incorrect spelling. The sample and request form used for crossmatching were labelled with the full first name but the historical record had a shortened version of the same name. This discrepancy had been checked with the electronic patient record at initial input in 2012 and again on the second sample received in 2013. In 2014 the electronic patient record was changed to the full name. When booking in this sample in 2017 the difference in the first name was not noted and it was booked in under the historical record of the short version without updating the forename to the full correct name. Two BMS failed to notice that the forename on the request form and sample were different to that on the historical record. The error was also not detected by ward staff and consequently a unit was transfused with the incorrect patient’s forename. At the time of the incident the BMS staff had up-to-date competency assessments.
Good practice: Clinical areas must always use the registered patient name when collecting and requesting pathology samples and should not use familiar or alternative names by which the patient may be known. Laboratory staff must make sure the patient record selected on the LIMS when booking in samples matches the details exactly on the request form and sample received.
Figure 7.3:
Sample receipt and
registration errors
with outcome n=75

38
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
7. Laboratory Errors
Testing n=110
Correct analyses are required to ensure the safe provision of blood components for transfusion and should be undertaken in full compliance with local and national guidelines for pre-transfusion testing (BSH Milkins et al. 2013).
Procedural errors or failures in QMS far outweigh other areas in testing (Figure 7.4). Many of the serious adverse events are due to laboratory staff failing to follow procedure:
• QMS errors i.e. inadequate processes or incorrect procedures
• Procedural errors i.e. wrong procedure performed or procedure performed incorrectly or steps omitted
For further information on these, see the 2016 Annual SHOT Report page 39 (Bolton-Maggs et al. 2017).
WCT=wrong component transfused; SRNM=specific requirements not met; RBRP=right blood right patient; Ig=immunoglobulin
1
2
4
3
5
4
6
48
1
8
1
8
5
6
8
0 10 20 30 40 50 60 70 80
Technical errors
Transcription errors
Interpretation errors
Procedural errors
WCTSRNMRBRPAvoidableDelayedAnti-D Ig
WCT=wrong component transfused; SRNM=specific requirements not met; RBRP=right blood right patient; Ig=immunoglobulin
Learning points for testing errors
• Failure to follow procedures: all policies and procedures for testing must be robust and strictly adhered to by laboratory staff without deviation. They must be validated and reviewed regularly i.e. review, improve and rewrite
• Anti-D immunoglobulin (Ig): the transfusion laboratory should have procedures in place to issue, trace and fate anti-D Ig. It is beneficial if the laboratory information management system (LIMS) can support identifying whether the patient is D-positive or is carrying or has delivered a D-negative baby. If anti-D Ig is issued from the pharmacy, the pharmacist must have access to the blood group of the patient and must understand it. This arrangement is not ideal
See Case 10.1 in Chapter 10, Incorrect Blood Component Transfused (IBCT) and case studies below.
Figure 7.4:
Testing errors with
outcome n=110

39
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
7. Laboratory Errors
Case 7.2: Preparing units for two patients with the same blood group simultaneously resulted in one patient receiving units intended for the other, 3 errors
Patient 1 received blood crossmatched for Patient 2. The incident involved two 2-unit crossmatches issued within 4 minutes of each other for two patients whose blood groups were both O D-positive with no antibodies detected. The crossmatched units were labelled and issued to the wrong patients. Patient 2’s units were labelled with Patient 1’s compatibility tag and Patient 1’s units were labelled with Patient 2’s compatibility tag.
Patient 1 was transfused both units with no adverse events reported. Patient 2 was not transfused and the units were returned.
The error was not detected either at collection or at administration because the compatibility tag was not checked against the component label it was attached to. The error was identified by the medical laboratory assistant (MLA) when fating the units as transfused in the LIMS.
Good practice: Always work with one patient at a time when crossmatching manually or electronically from start to finish, then once blood is issued and safely in the issue refrigerator ready for collection move on to preparation for the next patient.
Case 7.3: Blood issued before compatibility testing was complete
A full indirect antiglobulin test (IAT) crossmatch was set up by BMS 1 during a weekend shift for a patient with a known anti-K antibody which was not detectable at this time. Full testing was incomplete by the end of this shift as the crossmatch had not been interpreted. BMS 1 handed over the patient/testing information to BMS 2 who was starting the next shift, but they ended up working in the haematology section of the laboratory and not in transfusion. BMS 3, who also started on this shift and was covering the transfusion laboratory, assumed testing had been completed for this patient. The red cell unit was labelled, checked and moved from the holding shelf of the testing refrigerator into the issue refrigerator. K-negative red cells had been selected for this patient. The error was not detected until later in the shift when the gel card used for crossmatching was found still in the incubator. BMS 3, realising the error, checked the issue refrigerator however, the unit had been removed and transfused to the patient. The LIMS and report form indicated the units had been compatibility tested.
This incident demonstrates the importance of a robust and clear handover to the person continuing the work.
Case 7.4: Out-of-date LIMS and a manual interpretation error leads to two different blood groups being reported on a patient’s record
A new patient was grouped on two separate occasions. Manual interpretation of the results was performed by the BMS. The first result recorded was interpreted as A D-positive and the second result was interpreted as B D-positive. Group O compatible red cells were issued, and one unit was transfused before the error was noted by a second BMS. The laboratory used an out-of-date LIMS which added complication to authorising results and allowed two different blood groups to be reported on the same patient.
Good practice: Validation of a LIMS should challenge all potential areas, especially those surrounding the issue of blood components based on testing results. Systems, including LIMS, should be re-qualified as stated in the European Union (EU) Guidelines for Good Manufacturing Practice (GMP) (EU 2015).
Component selection errors n=54
The process must ensure that the correct components (together with the specific requirements) are selected to comply with the patient’s requirements and the clinical request.

40
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
7. Laboratory Errors
Learning points in component selection
• Unrecorded specific requirements: laboratory staff need to have knowledge and understanding about the requirements for key patient demographics including age-restricted requirements (pathogen-inactivated plasma components for patients born after 1 January 1996, K-negative red cells for a person of childbearing potential (BSH Milkins et al. 2013) and, in an emergency where the age is known, D-negative uncrossmatched red cells for males under 18 years of age). These requirements are not usually indicated on the clinical request form and are seldom supported by the laboratory information management system (LIMS)
• Multiple specific requirements: if a patient has several specific requirements, laboratory staff may fail to select for all of them as they may be busy focussing on one of them e.g. a pregnant person with lymphoma may get irradiated but not cytomegalovirus (CMV)-screened cellular components. A robust process should be in place to ensure that components with all the correct requirements are selected
• Compatibility of components: knowledge about the compatibility of all components is an essential requirement for laboratory staff (see SHOT Bite No. 9: Component Compatibility, www.shotuk.org/resources/current-resources/). Laboratory staff must also remember to take into consideration maternal antibodies when issuing blood components for a neonate, ensuring that the units are compatible with maternal antibodies. When only one group and screen sample has been tested for a patient for whom blood components are required, group O red cells and group AB fresh frozen plasma (FFP) (if AB not available then group A FFP) are the groups of choice until a second sample is received and analysed to confirm the patient’s blood group. In an emergency it may be acceptable to issue group-compatible red cells on a first perfectly labelled sample if locally risk-assessed
See Case 10.5 (transfusion of incompatible FFP) in Chapter 10, Incorrect Blood Component Transfused (IBCT) and case studies below.
Case 7.5: Non-irradiated platelet units issued to a <10-year-old patient despite a warning flag, 3 errors
A BMS issued two bags of platelets for a patient who required irradiated cellular components. This specific patient requirement was recorded on the LIMS. BMS 2 was covering for a break during a night shift, and receipted the platelets on arrival from the Blood Service. When BMS 1 returned from their break, they received a handover message that the platelets had been placed on the agitator but required irradiation. This message was taken verbally but not written down. It is usual practice at this hospital for all platelets to be irradiated on arrival from the Blood Service and then placed on the agitator, however in this instance that did not happen. The shift ended and day staff arrived. BMS 3 issued the platelets assuming they had been irradiated. A message flagged up that they had not been irradiated but was overridden. At administration BloodTrack® was used but it did not pick up the need for irradiated platelets, and it was not picked up by the registered nurse administering them and so the patient received the transfusion. The error was noticed during the bedside check for the second unit. The unit was returned to the laboratory and an incident form completed.
There were several assumptions that led to this error. Firstly, staff assumed that the message given verbally would be remembered; it was not written down as part of a handover. This was followed by an assumption that the platelets on the agitator had been irradiated. The clinical staff did not identify that the first unit transfused was not irradiated; this could possibly have been due to reliance on BloodTrack® to alert the staff if there were any discrepancies.
Platelets are irradiated in-house when received from the Blood Service. On this occasion, this was not done. If this laboratory received irradiated platelets direct from the Blood Service this incident would not have occurred because ‘irradiation’ is included in the product barcode. So, if the patient is flagged as needing irradiated components, the LIMS should not allow issue of non-irradiated units.

41
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
7. Laboratory Errors
Case 7.6: Multiple specific requirements for a patient where the need for K-negative units was overlooked
A telephoned request was taken for red cells for a <10-year-old girl, but full details were not entered onto the telephone request form at the time of request, therefore gender was omitted and this was not obvious from the patient’s name. The request was taken by a lone overnight worker who was interrupted by a bleep so did not complete the task by looking up the record on the LIMS. Subsequently the LIMS became unavailable due to a planned downtime. A second BMS later issued the red cells while the LIMS was still unavailable, so the patient was looked up on the in-house specific requirement back-up file which stated that the specific requirements were for CMV-screened and irradiated cellular components. This was then written on the request form. A red cell unit was crossmatched, issued and transfused. When the LIMS was back up and running it was noted that the additional requirement for K-negative units, due to patient gender and age, had been overlooked and a K-positive unit had been transfused.
It is essential to know the age and gender of a patient to determine basic requirements which should form part of the information recorded from a telephoned request. Best practice is always to receive a completed signed request form prior to component release that should have indicated the gender and all specific requirements of the patient. The incident also demonstrates reliance on the LIMS to notify the user of specific requirements. Laboratory staff can rely too much on the LIMS to inform them of component selection and specific requirements that are age- and gender-specific rather than using their knowledge achieved through training and competency assessment.
Case 7.7: Incorrect D-group red cells given following liver transplant (donor D-negative, recipient D-positive)
Following a telephone call from the transplant coordinator to the transfusion laboratory, staff became aware that D-positive blood had been issued and administered to a post-liver transplant patient outside the hospital local protocol. The blood was compatible with the recipient but not with the donor organ, which was D-negative. The error was noticed by ward staff and was quickly rectified and new blood components issued by the transfusion laboratory staff. The previous units were removed to prevent any further components being erroneously transfused. The investigation report noted that sample processing occurred outside normal working hours; this was not unusual for a liver transplant patient and workload was not excessive. The checking process and issuing of blood components had been dealt with by three members of staff and covered two handover periods. The blood sample and request also had arrived towards the end of the shift for one of the staff members.
The root cause of this incident involves both communication and educational factors. Staff failed to identify that the notes they were reading on the LIMS were from a previous transfusion. There was no telephone call from the transplant coordinator (usual practice) which would have triggered laboratory staff to look at the notes on the LIMS. Educational factors: no formal training was in place in relation to blood component transfusion for solid-organ transplantation. Staff involved were working across two different sites with two different policies in relation to living-donor transplantation. There was also wrong information on the child’s (recipient) operation record note in relation to the donor group.
Although there is a section for haemopoietic stem cell transplants in the compatibility guidelines (BSH Milkins et al. 2013) there is a lack of guidance with respect to some important aspects of transfusion management in ABO-incompatible and D-mismatched solid organ transplants. In the absence of national guidance centres will devise their own protocols (Aujayeb et al. 2014).
Component labelling, availability and handling and storage errors (HSE) n=149
The correct component needs to be labelled with the correct four (or five) key patient identifiers; first name, last name, date of birth (DOB), unique patient identifier (and first line of address in Wales) (BSH Milkins et al. 2013). Components need to be accessible and available for the time required, if this is not attainable then the clinical area need to be informed. The components need to be handled and stored in the correct way as defined in the guidelines (JPAC 2013).

42
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
7. Laboratory Errors
Learning points for labelling and availability
• Transposed labels: following component labelling laboratory staff should have a ‘stop’ moment and check that all paperwork is correct and that the right label is attached to the right unit. It is essential that only one patient’s component is labelled at a time
• Major haemorrhage protocols (MHP): one person should be nominated in the clinical area and another in the laboratory and all communication should be channelled through these identified individuals. This will avoid duplication of requests and time-consuming telephone calls during a challenging time (See SHOT Bite No. 8: Massive Haemorrhage – Delays www.shotuk.org/resources/current-resources/)
Case 7.8: Blood issued and transfused related to an incorrectly labelled sample
A patient was admitted to the emergency department (ED) and had their surname recorded on the patient administration system incorrectly with a unique patient number but no DOB was provided. Two samples labelled as above were received and processed by the transfusion laboratory. The following day the patient’s central record was updated with the name changed to a different but similar and correct surname and updated with a DOB, but the unique patient number remained unchanged. The transfusion laboratory was not informed that there had been a change to the patient’s details. Two days later the laboratory received a request for two units of red cells which was fulfilled using the original samples with the incorrect name and no DOB. A member of staff from the clinical area was sent to collect a unit of red cells for this patient and failed to undertake full patient identification checks. At the time they realised that there was no DOB recorded, that the unique patient number was the same but they did not check the patient’s name. On return to the clinical area, the staff member contacted the transfusion laboratory and enquired about the missing DOB. They were informed that the component could be transfused. However, two further samples were now needed by the transfusion laboratory. At administration a two-person check was undertaken at the bedside but no check was performed against the identification band and the unit was then transfused. On investigation the staff member said that they were concerned about the lack of a DOB however, when they telephoned the laboratory they were told that the blood was safe to use.
The DOB is an essential core identifier (BSH Robinson et al. 2018). Routine samples without this information should not be processed. In emergency situations with unknown patients the guidelines recommend ‘at least one unique patient identifier’, and a guestimate of the age which can inform about potential patient-specific requirements. Hospital transfusion policies should be clear that it is not acceptable, unless in emergency situations, to proceed with transfusion if the core identifiers are missing or incorrect.
Figure 7.5 shows the laboratory-related HSE. For additional HSE, including those in the clinical area, see Chapter 9, Handling and Storage Errors (HSE).
Learning points about handling and storage for laboratory staff
• Storage of components: adequate cold chain needs to be maintained to ensure that units out of temperature control are not transfused or returned to the storage unit
• Recovery of components beyond reservation: transfusion laboratories must have robust procedures in place for uncollected components that are beyond their reservation date and still in a storage unit to prevent them from being accessed and transfused

43
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
7. Laboratory Errors
Transport and delivery
Equipment failure
Returned to stock when should have been discarded
Failure to clear refrigerator
Incomplete cold chain
Expired unit transfused
Stored inappropriately inlaboratory area
Miscellaneous
33
8
7
13
15
4 1
Case 7.9: Transfusion of FFP which had exceeded the post-thaw expiry time
FFP was requested for an elderly patient who was bleeding during a hip replacement. The laboratory keeps stocks of different types of frozen plasmas (methylene blue-treated FFP (MB-FFP), solvent-detergent treated FFP (SD-FFP) and standard FFP) and usually keeps pre-thawed standard FFP for up to 5 days for major trauma only (JPAC 2016).
A BMS selected thawed MB-FFP, which was beyond its permitted 24-hour post-thaw storage period, and issued it for the patient. The error was detected by the transfusion practitioner while following up data collection. The BMS on duty did not notice that the pre-thawed plasma was not suitable for 5-day storage and inappropriate for non-MHP use.
Storage requirements for different types of FFP are complex. To minimise confusion, FFP types should be stored in distinct and clearly-labelled storage locations. This is also applicable for storage of pre-thawed plasma components/products. Pre-thawed FFP for major haemorrhage activations should be labelled ‘for MHP use only’. Clear training and competency assessment for BMS staff should be in place. Procedures should also be in place to remove from storage locations and discard components/products that have expired to avoid accidental issue and/or use.
Collection errors n=3
Correct procedure will ensure that the correct component is collected and that it fulfils the clinical request and meets the details on the collection slip.
There were 3 errors in collection where laboratory staff did not hand over the unit of the correct specification to the clinical staff, see Case 10.7 in Chapter 10, Incorrect Blood Component Transfused (IBCT).
Learning point about collection
• Direct handover: if laboratory staff are responsible for directly handing over components to a nurse/porter at collection, they need to ensure that all components meet the requirements of the clinical request and the collection slip. Any additional components must be confirmed with a traceable clinical request
Figure 7.5:
Laboratory-related
handling and
storage errors with
outcome n=72

44
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
7. Laboratory Errors
Miscellaneous n=18
This section includes instances where the error has occurred in areas other than the key laboratory areas in the transfusion process detailed above.
Learning point
• Blood Service errors: these are not reportable to SHOT unless they contribute to patient risk or harm. The transfusion laboratory staff should check all patient history and component selection (including components selected by a Blood Service)
Case 7.10: A patient with sickle cell disease received an incorrectly phenotyped component following an error from the Blood Service
A unit of red cells was requested from the Blood Service for a patient with sickle cell disease. The Blood Service crossmatched the unit but it was not matched for Rh and K. Specific requirements for sickle cell patients are that red cell units should be sickle-negative (HbS-), matched for both Rh and K, and <10-days old. The receiving transfusion laboratory failed to identify this omission and made the unit available for the patient. The patient subsequently developed anti-C as they should have received red cells negative for the antigens C, E and S that were also HbS-negative as recommended by the Blood Service expert laboratory report.
BMS should never take for granted that the earlier steps in the transfusion process have been undertaken correctly and should always perform their step in the transfusion process fully and with care. The bedside check is the last step in the process to identify errors made earlier in the transfusion process and staff administering blood components should have a clear understanding of the specific requirements of their patients.
Case 7.11: FFP reconnected and transfused after being disconnected
FFP was being administered to a patient when a problem arose with the cannula. The nurse stopped the transfusion and disconnected the component. The nurse took the component to the laboratory to ask how long FFP can be out the refrigerator and if it could still be given within the allowed timeframe. The BMS advised that the component could be re-connected to finish the transfusion as it was still within time. The nurse (who had received transfusion training) queried this instruction as she would not have done this with red cells but because two BMS told her the same thing she assumed this was correct. The nurse re-connected the unit and completed the transfusion. The nurse was unaware of the correct procedure to follow if a cannula becomes blocked (i.e. to discard remainder of the unit after disconnecting). It was noted that she had relied on inappropriate advice.
Staff should clearly ascertain exactly what is being asked of them and then any advice given should only be within the scope of their training. BMS staff have limited clinical knowledge and should not give clinical advice. This should be referred to a transfusion practitioner or an appropriate clinician.
Case 7.12: Pathology LIMS was down, manual back up of patient data was available but had not been updated for 3 months, so missed the patient’s specific requirements
Over time, several hard drives containing the pathology LIMS records failed and eventually the final hard drive failed. The LIMS shut down throughout pathology, which covered three teaching hospitals across two cities, including the blood transfusion department. It was not reinstated until 8 days later and was not in full use until the 9th day following validation. During this period blood requested for a patient had no indication on the request form of any specific requirements or history of alloantibodies. Some patient history was available on an out-dated spreadsheet, including specific requirements and alloantibodies, but this was not consulted before issuing blood. This was because it was time-consuming to do, and staff were very busy because of the increased workload. Education for this important step was not routinely delivered in training.
In addition, the working environment became difficult due to the amount of paper being used for each record and space became compromised due to the amount of manual work that had to be

45
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
7. Laboratory Errors
completed, all of which had to be completed with the existing number of staff. Staff morale was affected by the demands of increased concentration required, user requesting and overall stress of providing a service during this situation.
A manual backup from the LIMS to an Excel spreadsheet which records known alloantibodies was last performed three months before and was only ever done on an ad-hoc basis. Had this been done more frequently, then the potential for missing a specific requirement or alloantibody would have been reduced.
The failure of the clinical areas to inform the laboratory of any specific requirements and/or alloantibodies highlights the lack of understanding in the clinical areas of the importance of serological history and specific requirements. SHOT reports continue to indicate a national, systemic misunderstanding of the importance of this information among clinical and nursing staff. However, the laboratory staff should have sufficient robustness within their contingency planning to be able to access specific requirement data on previously-reported patients. The contingency planning should also ensure that staff are fully supported in managing changes in workload.
Medicines and Healthcare Products Regulatory Agency (MHRA)
Author: Chris Robbie
There are several differences in reporting to both haemovigilance organisations which are described in the 2016 Annual SHOT Report (Bolton-Maggs et al. 2017). Despite the variation in numbers and categorisation the MHRA can confirm that the reflective learning described throughout the SHOT laboratory chapter is similar, therefore this MHRA summary has focused on additional key areas that are only reportable to the MHRA. The full MHRA chapter, Chapter 24, is available online only on the SHOT website (www.shotuk.org).
There are several related themes in the case studies included here. Staff appear to be making assumptions, skipping steps in procedures, multitasking, using uncontrolled forms, giving advice that they are not qualified to give and showing a lack of attention to detail. All these are examples of poor laboratory practice. Collectively these can be addressed by annual GMP training which makes clear the expectations of staff to conduct themselves correctly when working in the laboratory. GMP training should make it clear to staff:
• Do not continue without having the correct information
• Do not work on two tasks at the same time
• Do not use sticky notes to document information
• Do not perform tasks or give advice you have not been trained for
• Check at all stages that the work you have done is correct before you proceed to the next stage
Simple stuff, right?
Not entirely. Analysis of SHOT and serious adverse blood reactions and events (SABRE) reports demonstrates that in many cases staff are already aware of what they should do and how to conduct themselves. MHRA inspectors having assessed compliance, as demonstrated by the blood compliance report, have shown it to be failing. Inspection findings have shown an increase in non-compliances found during inspections. SHOT, UKTLC, NBTC, laboratory managers and the MHRA are also reporting failures to address long-term resource and staffing problems.
These problems are not going to be easy or quick to solve, but a robust QMS can help to alleviate some of them. Processes need to be carefully planned to achieve consistent and safe outcomes for each task undertaken, and also need to consider when things do not go to plan. Procedures need to be as simple as possible, but as complex as they need to be, to ensure that staff have access to the correct instructions and information at the correct time. Training and education need to cover the situations that staff face on a daily basis. New staff need to be properly trained and supervised while they gain

46
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
7. Laboratory Errors
experience in their new working environment. Poor practice should be identified and corrected before this results in errors.
The QMS should not be seen as a time-consuming inconvenience, but as a tool to be used effectively to ensure safety and consistency. It should be used to gather evidence to highlight the pressures laboratory staff face. Staff should never be guilty of making basic GMP errors, but if they are not properly supported by a robust QMS then sometimes they might feel they have no choice. If this is the case, and errors are made, it is their duty to report this so the failings of their QMS can be addressed.
UK National External Quality Assessment Scheme (UK NEQAS)
Authors: Jenny White and Clare Whitham
Following last year’s report, UK NEQAS blood transfusion laboratory practice (BTLP) sent out its annual pre-transfusion testing questionnaire to laboratories in the UK and overseas. A relatively low return rate this year has, however, limited data analysis. For the first time, a question was included to collect data on the number of laboratories that use the ‘Rh shorthand’ notation, e.g. R1R1, CDe/CDe, and in what context. The responses show that 60/114 (52.6%) laboratories use the shorthand notation, mainly in conversation with blood transfusion staff, but also for blood ordering and on the LIMS. UK NEQAS (BTLP) currently send one exercise a year assessing phenotyping for Rh antigens, but intend to increase this as part of a scheme redesign. While penalty scoring for Rh phenotyping is based on the reactions recorded rather than the shorthand interpretation, during exercise 17R1, 33/532 sets of correct reactions were assigned an incorrect shorthand interpretation, with 27/33 of these due to not taking the D-type into consideration.
As reported last year, results of BTLP external quality assessment (EQA) exercises have shown some continuing issues with laboratories failing to either adhere to or understand recommendations made by the manufacturers of their chosen technology. In 2016 (exercise 16R9, D-positive cells coated with anti-D) and again in 2017, in exercise 17R5, red cells of one of the patients (D-negative) were coated with anti-c to give a 2+ positive DAT. This caused a positive reaction in the control well of BioVue grouping cassettes, invalidating the D-typing results. The majority of laboratories using BioVue either reported an interpretation of uninterpretable (UI) or undertook repeat testing with a second technique enabling them to make an interpretation of D-negative. However, eight laboratories reporting positive reactions versus anti-D reagent(s) and/or the reagent control went on to make an interpretation of D-positive or D-variant.
Ortho BioVue instructions for use for ABO-Rh/Reverse Grouping Cassette recommend that ‘all weak Rh(D) positive typing results of 2+ or less be confirmed by an alternative method’ and that ‘invalid test results due to spontaneous agglutination may occur on rare occasions with the Anti-D reagent when testing red blood cells heavily coated with antibodies.’ It is important that all users are aware of the limitations of technology that is used for any application in the blood transfusion laboratory, and that manufacturers’ instructions are understood and followed. Laboratories should have clear policies for defining and investigating anomalous ABO/D typing results, and all staff undertaking testing and reporting should have the knowledge required to recognise potential sources of error, including those specific to the technology in use.
Further issues related to lack of adherence to or misunderstanding manufacturer recommendations included one laboratory, experiencing supply problems with the panel provided for their column agglutination technology (CAT) technology, substituted this panel with one designed for a different CAT technology, causing insensitivity in the IAT. This resulted in a false negative reaction which contributed to misinterpretation of an antibody mixture. Each CAT system employs a diluent with a specific ionic strength, designed along with the volume of plasma required to give the optimal ionic strength of the final mixture of reactants.
In an exercise containing a weak anti-E, three laboratories made errors in antibody screening, despite having obtained weak positive reactions in the initial screen. One made a decision to discount a weak positive reaction with one screening cell in view of a field safety notice warning of occasional non-specific reactions with quality control (QC) samples. Two other laboratories repeated the testing on their

47
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
7. Laboratory Errors
respective analysers, obtained negative results and reported a negative screen. One of these laboratories made a decision to report the screen as negative in the context of on-going problems with occasional false positive reactions versus screening cells with clinical samples, and the other did not follow their protocol for investigation of equivocal reactions in the screen. Knowledge of current issues or problems related to different technologies or current testing environments can influence interpretation of antibody screening results. Bearing this in mind, it is important that laboratories have clear protocols for dealing with inconsistent, non-reproducible or weak reactions in antibody screening or identification panels.
In the current climate of increasing workload, loss of experienced staff due to retirement and falling staff numbers, resource and time constraints are contributory factors for errors made in EQA exercises (UKTLC 2017). A laboratory, working under such constraints, identified an anti-D in an EQA sample but misidentified a second specificity as a result of not following their own protocol for inclusion and exclusion of antibody specificities. Loss of staff knowledge and experience are further contributory factors. In an exercise with a sample containing anti-Fya+K, two laboratories identified anti-Fya, but misidentified the second specificity and did not record the potential presence of anti-K. To avoid misidentification, every antibody investigation should include a systematic process for exclusion and positive identification of antibody specificities, and all reactions should be accounted for before a conclusion is reached. In all cases, a process of exclusion/positive identification was not undertaken.
As for last year, data analysis of EQA exercises repeatedly shows transcription and transposition errors made either during testing or reporting of results. Some of these are caused or exacerbated by the fact that processing and reporting of EQA samples is not identical to that for clinical samples. However, manual testing is vulnerable to transcription and interpretation errors and must include checks at critical points. In one exercise, an error was made when manually transcribing results from an analyser, leading to misidentification of the antibody, and in another, an error occurred during interpretation of a manual ABO/D group undertaken in accordance with the laboratory’s policy for patients requiring a crossmatch, and this manual result was reported rather than the routine automated ABO/D group. Even laboratories with full automation will on occasion be required to undertake manual grouping and should have a back-up process in place that is useable 24/7.
Welsh Assessment of Serological Proficiency Scheme (WASPS)
Author: Gareth Nottage
The Welsh Assessment of Serological Proficiency scheme (WASPS) is based on a simulated compatibility test that is performed by individual members of staff using manual serological techniques. Sufficient material is provided to each laboratory so that all members of staff, including on-call and multidisciplinary staff, are able to participate. The 2012 Annual SHOT Report (published in 2013) recommended that ‘Regular practice and competency assessment of infrequently used manual techniques is important’.
Performance scores are based on the comparison of individual results to the overall modal results within technique. Laboratories are classified as persistent unsatisfactory performers (PUP) when they incur an unsatisfactory performance score in two consecutive exercises. During the period 2005-2013 no laboratories were identified as such, however, one laboratory was identified in 2014 and two identified in both 2016 and 2017.
In the first instance in 2014 five different individuals failed to detect seven weak incompatibilities over two exercises (W10/13 and W01/14).
In the first of the two laboratories identified during 2016 three individuals recorded three missed incompatibilities, in the second laboratory identified, four individuals recorded ten missed incompatibilities. In the first of the two laboratories identified during 2017 nine individuals recorded 15 missed incompatibilities, the second laboratory identified two individuals who recorded three missed incompatibilities. Where these missed incompatibilities have been recorded it has been noted that other individuals, who either tested on the same day or at a later date, completed the exercise correctly.

48
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
7. Laboratory Errors
UK Transfusion Laboratory Collaborative Update
Author: Rashmi Rook
Capacity planning – safer staffing
The UKTLC standards (Chaffe et al. 2014) are regarded as industry standards, and laboratories should strive towards meeting these requirements. The standards were devised based on historical knowledge of transfusion processes and years of analysing laboratory error data by the SHOT and MHRA teams, which identified the factors that contributed to these errors.
Transfusion teams are strongly advised to plan their staffing levels and skill mix to ensure that all aspects of service provision are met and continually assessed through their local governance structures. A simple template for capacity planning and review was released on the MHRA blood forum and can also be located at the foot of the SHOT current resources web page (under UK transfusion laboratory collaborative resources, https://www.shotuk.org/resources/current-resources/); the sole aim for this process is to have:
• Right staffing levels
• Right skill mix
• Right knowledge
• Right supervision
• Right equipment
• Right procedures
• Right resources
Considerations when capacity planning:
• The senior and lead BMS should be excluded from the shift rotas if this impacts on core-hours availability
• If it is necessary to use the senior team for out-of-hours provision, then additional staffing resource must be built into the plan, i.e. if a senior member of staff is on a full shift and their core-hour availability (09:00-17:00) is 0.7 whole time equivalent (WTE), then additional 0.3 WTE staffing resource is needed
• There must be staff available to support the transfusion laboratory manager with the following service aspects:
– Supervision
– Training
– Equipment management
– Error management, audit, improvements, validation and changes
– Traceability
– Haemovigilance
• Consider using permanent MLA staff to support the functions of traceability and some training functions such as stock entry, sample, and stock management
• Ensure that time is built in to enable staff to be released to meet training commitments
• Allow staff opportunities to attend courses and external transfusion meetings to build on their interest and knowledge
• To allow for continued stability of the department it is essential that any changes to working patterns

49
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
7. Laboratory Errors
of shared rotational staff are assessed through a formal change-management process to review the impact on the transfusion department, and the potential to undermine adherence to the regulations
• Any deviations from the required staffing levels should be managed via the hospital risk governance procedures (risk register), for full visibility and planning improvements
• A simple way to work out what staffing is needed is to look at the tasks not achieved both in the laboratory and QMS activities, and to identify what the service needs are to meet the standards, and thereby comply with the Blood Safety and Quality Regulations (BSQR) (BSQR 2005):
– Documents past review dates
– Training delays
– Delays with annual competencies
– Overdue audits
– Overdue equipment cleaning/planned preventative maintenance (PPM)/or reviews not performed to schedules
– Overdue error investigations
– Processes/equipment/tests not re-qualified within timescales
– Pre-acceptance testing not performed
– Staff not reading/signing standard operating procedure (SOP)
– Staff unable to be released to attend professional meetings
The transfusion team must ensure that the QMS is embedded as part of their normal working practice, and not considered to be the sole responsibility of quality personnel, as the knowledge of errors, and the improvements needed reside with the expertise of the transfusion team.
As previously mentioned, we all come to work intending to do a good job. It is faulty systems and processes that let us down and place our staff in situations where they are more likely make an error that may result in patient harm, as well as affecting their own confidence. It is time to build a resilient workforce and give staff the right tools and capabilities to succeed via the capacity planning process, so that errors of the past are not repeated. The workforce can then be developed and encouraged, and we can bring back the pleasure and pride in our working environment.
Updating current standards
The UKTLC standards (Chaffe et al. 2014) are under review. There will be some guidance on demonstrating equivalence to the qualification requirements.
Conclusions relating to laboratory errors
Cases in this Annual SHOT Report have demonstrated that staff are stepping beyond their capability or knowledge and giving out information they are not qualified to give or incorrectly modifying laboratory practice to try and achieve a safe conclusion. There should be robust SOP that indicate what staff should do when events fall outside their understanding or the detail of the SOP. It should be made clear that these events need to be referred to either a more senior/experienced BMS or a clinician with a knowledge of transfusion to advise on the appropriate course of action to be taken. Where additional laboratory procedures may cause delay in provision of suitable components the clinical staff should be informed as soon as practicably possible.
The BSH administration guidelines have been updated and highlight that clinical staff are required to perform the critical bedside checks including knowledge of compatibility prior to administering the component (BSH Robinson et al. 2018). However, the laboratory staff must perform essential checks in the transfusion laboratory to ensure that the component is correct for the patient prior to it leaving the laboratory. The transfusion process requires all staff working in blood transfusion to work as a

50
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
7. Laboratory Errors
team, and not only within their key areas, to ensure patient safety. This requires communication and effective handovers between staff. The key laboratory messages and learning points above need to be considered for both routine and out-of-hours service. Laboratory staff must be responsible for keeping their competencies up to date (https://www.hcpc-uk.org/aboutregistration/standards/cpd/). The pathology services are under intense pressures and demands in a climate where workforce is stretched and under-staffed, therefore it is even more vital that vigilance and duty of care is upheld to ensure safe transfusion and patient safety.
References
Aujayeb A, Lordan J et al. The passenger lymphocyte syndrome – experience from a cardiothoracic transplant unit. Transfus Med 2014;24:423–425.
Bolton-Maggs PHB (Ed), D Poles et al. on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. The 2016 Annual SHOT Report (2017) www.shotuk.org [accessed 4 April 2018].
BSH Jones J, Ashford P et al. Guidelines for the specification, implementation and management of information technology (IT) systems in hospital transfusion laboratories. 2014. https://b-s-h.org.uk/guidelines/guidelines/specification-implementation-and-management-of-information-technology-it-systems-in-hospital-transfusion-laboratories/ [accessed 22 April 2018].
BSH Milkins C, Berryman J et al. Guidelines for pre-transfusion compatibility procedures in blood transfusion laboratories. Transfus Med 2013;23(1):3-35.
BSH Robinson S, Harris A et al. The administration of blood components: a British Society for Haematology Guideline. Transfus Med 2018;28(1):3-21. http://onlinelibrary.wiley.com/doi/10.1111/tme.12481/pdf [accessed 23 March 2018].
BSQR blood safety and quality regulation, (SI 2005/50, as amended) (2005). http://www.legislation.gov.uk/uksi/2005/50/contents/made [accessed 26 February 2018].
Chaffe B, Glencross H et al. UK Transfusion Laboratory Collaborative: minimum standards for staff qualifications, training, competency and the use of information technology in hospital transfusion laboratories. Transfus Med 2014;24(6):335-340.
European Union: Good practice guidelines for standards and specifications for implementing the quality system in blood establishments. https://www.edqm.eu/sites/default/files/goodpracticeguidelines-standards_specifications_for_implementing_quality_system_in_blood_establishments-december2016.docx [accessed 14 February 2018].
European Union: Guidelines for Good Manufacturing Practice (GMP) for Medicinal Products for Human and Veterinary Use. https://ec.europa.eu/health/sites/health/files/files/eudralex/vol-4/2015-10_annex15.pdf). [accessed 28 January 2018].
HCPC: Standards of continuing professional development. https://www.hcpc-uk.org/aboutregistration/standards/cpd/ [accessed 14 February 2018].
JPAC 2013 Guidelines for the blood transfusion services in the UK, 8th edition. https://www.transfusionguidelines.org/red-book [accessed 14 February 2018].
JPAC 2016 Position statement: Review of the shelf life of fresh frozen plasma components following thawing. www.transfusionguidelines.org/document-library/documents/position-statement-review-of-the-shelf-life-of-fresh-frozen-plasma-components-following-thawing [accessed 13 April 2018].
SHOT Bite No. 8: Massive Haemorrhage – Delays. https://www.shotuk.org/wp-content/uploads/SHOT-Bites-No8-Massive-Haemorrhage-Delays-1.pdf [accessed 14 February 2018].
SHOT Bite No. 9: Component Compatibility. https://www.shotuk.org/wp-content/uploads/SHOT-Bite-No-9-Component-Selection.pdf [accessed 10 April 2018].
UKTLC Staffing capacity planning template. https://www.shotuk.org/resources/current-resources/ [accessed 26 February 2018].
UKTLC survey key findings 2017. https://www.shotuk.org/wp-content/uploads/UKTLC-Report-Final-Report-Findings-2017_V2.pdf [accessed 26 February 2018].

51
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
8. Right Blood Right Patient (RBRP)
Authors: Diane Sydney and Hema Mistry
Definition:
Incidents where a patient was transfused correctly despite one or more serious errors that in other circumstances might have led to an incorrect blood component transfused (IBCT).
Key SHOT messages
• Staff must perform patient identification steps thoroughly and with attention to detail during all stages of the transfusion process. The four main key identifiers must be checked i.e. first name, last name, date of birth, unique identifier (and first line of address in Wales) (BSH Robinson et al. 2018)
• All National Health Service (NHS) Trusts/Health Boards must ensure that a bedside checklist is introduced in accordance with the SHOT recommendation (Bolton-Maggs et al. 2017 and DH 2017). All staff must use a bedside checklist. Further information can be found in Chapter 10, Incorrect Blood Component Transfused (IBCT)
In 2017, 200 cases were reported compared to 227 cases in 2016 (Bolton-Maggs et al. 2017). Clinical errors accounted for 123/200 (61.5%) and laboratory errors for 77/200 (38.5%), Figure 8.1. Patient identification (ID) errors accounted for 115/200 (57.5%).
Right blood right patient n=200
77
Patient identification errors n=115
Labelling errorsn=48
Laboratory
Clinical 123
48
Prescription errorsn=37
37
29
86
Patient ID n=115
Errors in patient ID occur in both the clinical area and in the laboratory, but 86/115 (74.8%) of these occurred in the clinical area, Table 8.1.
Figure 8.1:
Breakdown of
2017 RBRP reports
n=200
Right Blood Right Patient (RBRP) n=200 8

52
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
8. Right Blood Right Patient (RBRP)
Area/location Patient ID error Number of reports
Clinical
Incorrect ID in relation to four key identification datasets i.e. first name, last name, date of birth (DOB), unique identifier
71
No identification band 12
Bedside check not performed 3
LaboratoryDemographic data entry errors in relation to four key identification datasets i.e. first name, last name, DOB, unique identifier
29
Total 115
Case 8.1: Doctor uses their own name by mistake when completing the transfusion record sheet
A unit of red cells had been collected according to hospital policy by using the collection slip. However, when the transfusion record sheet (TRS) was returned to the laboratory for traceability purposes, the name on the TRS did not correspond with the expected patient’s name. On investigation the doctor had filled in their own name when completing the TRS with the patient’s hospital number and DOB. This was not identified when two clinical staff (one reading the tag and one reading the TRS) were undertaking the final bedside check and subsequently signing the TRS. The tag attached to the unit had the correct details for the patient.
Case 8.2: Final bedside check not undertaken correctly
A unit of red cells was administered without the final bedside check being undertaken correctly. Another member of staff had the electronic hand-held personal digital assistant (PDA) which is used in the checking process to verify the patient details. The nurse proceeded to administer the transfusion, stating it was to save time rather than waiting for the PDA. Furthermore, the correct checks could have been carried out by using the tag attached to the unit which has a checklist. This can also be used for the correct procedure to administer the unit to the patient. The error was identified by another staff member who brought the PDA over for the staff member to use. The staff member knew the correct hospital procedure but thought that a short cut would save time and permit the transfusion to proceed more rapidly.
Each of the errors reviewed including the two cases outlined above, and Case 7.1 in Chapter 7, Laboratory Errors, highlight that staff must always remain vigilant when identifying patients, particularly at the final bedside check. They must use information technology (IT) devices correctly including when entering patient ID onto the laboratory information management systems (LIMS).
Learning points
• When available, staff should always use electronic devices correctly to enhance patient safety
• All staff working in transfusion should follow standard operating procedures (SOP), especially during busy or stressful periods when errors are more likely to occur
Near miss RBRP cases n=138
The near miss incidents related to RBRP cases show similar learning points to the full incidents that led to transfusion of components.
Table 8.1:
Patient ID errors in
2017 n=115

53
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
8. Right Blood Right Patient (RBRP)
Sample taking
39, 28.3%
Sample receipt
23, 16.7%
Component labelling
72, 52.2%
Prescription2, 1.4%
Collection2, 1.4%
IT-related RBRP cases n=24
Discrepancy between LIMS and patient administration system (PAS) or wrong record selected on LIMS or PAS n=8
In 3 cases there was some discrepancy between LIMS and the PAS or hospital information system (HIS), one of which was due to use of the American configuration of the date of birth (MM/DD/YYYY instead of DD/MM/YYYY). A further 5 cases were reported where the wrong record was selected on either LIMS or PAS/HIS. This manual step is prone to human error.
Blood issued against wrong ID n=1
This case related to collection of blood from an electronically tracked refrigerator and the details were not checked correctly between the blood compatibility label and the screen.
Incorrect result or data entered or accessed manually n=9
Manual steps are error-prone and there were 9 cases in this category.
IT systems and equipment failure n=3
During a cyber-attack, a sample was processed manually and when retrospectively entering the sample onto the LIMS an incorrect spelling was noted. In another case there was a mismatch between the number of characters permitted in LIMS and PAS so that a shortened last name was printed on the compatibility label and this did not match the identification band.
Case 8.3: Inadequate validation of new LIMS results in potential for inappropriate electronic issue (EI)
Following implementation of a new LIMS it was noted that the default to 72-hour sample validity was not present on all patients to whom red cells had been issued. Further investigation revealed that the product codes for some red cells had been put into the LIMS directory incorrectly so that the EI algorithm indicated that ‘crossmatch was not necessary’. Nine patients were given the right blood but should not have been eligible for electronic issue. A full validation of the EI programme would have identified this problem but was not carried out.
Figure 8.2:
Near misses that
could have led to
RBRP n=138

54
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
8. Right Blood Right Patient (RBRP)
Incorrect use of an electronic blood management system n=3
There were 3 cases in this category. In one the system worked as intended because bedside tracking prevented transfusion of a unit with an incorrect spelling of the name.
Case 8.4: Bedside alarm not heeded
A patient with gastrointestinal (GI) bleeding was admitted to the emergency department (ED) where he was registered with a misspelling of his first name (by one letter). The doctor used these details to generate request forms and labelled the samples from details on the identification band. After the samples had been dispatched the error was noted and the first name changed so a new identification band was printed. When the blood was issued it did not match the identification band so the bedside PDA highlighted the discrepancy. The doctor checked this with the laboratory who advised that the blood should not be given but the doctor said he knew it was the right patient and that it was an emergency. The transfusion of three units went ahead.
Commentary
SHOT continues to highlight that all staff participating in the transfusion process must adhere to correct patient identification procedures with attention to detail in all steps in the transfusion process.
For further laboratory-related errors and key messages and learning points for laboratory staff please see Chapter 7, Laboratory Errors.
References
BSH Robinson S, Harris A et al. The administration of blood components: a British Society for Haematology Guideline. Transfus Med 2018;28(1):3-21. http://onlinelibrary.wiley.com/doi/10.1111/tme.12481/pdf [accessed 22 February 2018].
Bolton-Maggs PHB (Ed), Poles D et al. on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. 2016 Annual SHOT Report (published 2017). https://www.shotuk.org/wp-content/uploads/SHOT-Report-2016_web_11th-July.pdf [accessed 8 January 2018].
Department of Health (DH). Safe transfusion practice: use a bedside checklist (CAS) CEM/CMO/2017/005 (2017). https://www.cas.dh.gov.uk/ViewandAcknowledgment/ViewAlert.aspx?AlertID=102663 [accessed 22 February 2018].

55
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
9. Handling and Storage Errors (HSE)
Authors: Diane Sydney and Hema Mistry
Definition:
All reported episodes in which a patient was transfused with a blood component or plasma product intended for the patient, but in which, during the transfusion process, the handling and storage may have rendered the component less safe for transfusion.
Key SHOT messages
• Communication is important at all stages in the transfusion process i.e. during handover, between laboratory and clinical areas, between departments, and with the patient. Unambiguous communication is pivotal in every aspect of the transfusion process
• Do Not Assume: Verify! Many cases demonstrated a lack of communication which directly led to the error or was a contributing factor
In 2017 there were 243 cases reported compared to 192 in 2016. Clinical errors accounted for 169/243 (69.6%) and laboratory errors for 72/243 (29.6%). The other 2/243 (0.8%) errors were neither in a clinical or laboratory category as they occurred in non-transfusion service vehicles, for example taxis.
There has been an increase in cold chain errors (CCE) from 61 in 2016 to 90 in 2017 (Figure 9.1). There were 74 reports where the duration of transfusion of a unit exceeded 5 hours.
Handling and storage errors n=243
72
Cold chain errorsn=90
Expired unit transfused n=15
Laboratory
Clinical 169
5
Excessive time totransfuse n=74
7466
22
2Neither
Technical administration
error n=59
59
Transfusion of a damaged
component n=3
3
Miscellaneousn=2
1
2
10
1
Case 9.1: Communication error leads to excessive time to transfuse
Nurse 1 asked if she could help her colleague (Nurse 2) by administering the transfusion for a haematology patient to allow Nurse 2 to have her break. Nurse 2 went for her break while the blood was being collected but left the instruction that the blood had to ‘run slow’ as the patient was breathless. The transfusion was commenced by Nurse 1 at 11:10 with observations being completed according to hospital policy, prior to, and 15 minutes into the transfusion. On completion of these observations Nurse 1 returned to her allocated clinical area and assumed that her responsibility for the transfusion was over and that Nurse 2 would resume responsibility on return from their break.
Figure 9.1:
Breakdown of 2017
HSE reports n=243
Handling and Storage Errors (HSE) n=243 9

56
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
9. Handling and Storage Errors (HSE)
However, at 16:45 an agency nurse taking over from Nurse 2 reported that the transfusion was still running (more than 5 hours). On this occasion the patient did not come to any harm.
The patient was put at additional risk by lack of communication during the handover and a lack of clarity about where responsibility starts and ends, especially when staff are covering breaks. Each nurse assumed that the other was responsible for the management of the transfusion. Good communication between clinical teams could have prevented this error.
Case 9.2: Staff multitasking and being distracted during a suspected transfusion reaction led to miscommunication
Following a suspected transfusion reaction, the nurse, who had limited experience of administering transfusions, contacted the laboratory for advice and was asked to return the unit ‘to the refrigerator’. The nurse then proceeded to return the blood to the ward refrigerator and not to the temperature-monitored transfusion laboratory refrigerator. The inexperienced nurse was distracted by the suspected transfusion reaction in the patient and did not understand the instruction from the laboratory staff leading to a miscommunication between the laboratory and the nurse.
This account suggests that the transfusion training for this nurse was inadequate.
Case 9.3: Incorrect transport and delivery of red cells by clinical staff
A porter was asked to collect blood urgently by theatre staff in a ‘cool box’. When the porter arrived at the laboratory there was no biomedical scientist (BMS) there to assist. After speaking to a BMS from another discipline who stated that they did not know where the cool packs were, the porter took a ‘cool box’ and signed the blood out of the refrigerator. On arrival in theatres ice was added from the theatre ice machine before delivering to the theatre. It was not established if this was by the porter or theatre staff. The first unit was transfused and the second unit was returned to the laboratory and discarded. Theatre staff were aware of the correct procedure which was to page the BMS to request blood to be delivered in a special box.
All staff (clinical and laboratory) should ensure that components are packaged appropriately in a validated transport box and that the correct documentation accompanies the components. Clinical staff should contact their local transfusion laboratory to seek advice and refer to local policy for collection of components.
Learning point
• Staff should have knowledge and understanding about handling and storage of all components to ensure that they are safe for transfusion
Near miss HSE cases n=154
The near miss incidents related to HSE show similar learning points to the full incidents that led to transfusion of components.

57
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
9. Handling and Storage Errors (HSE)
Administration
Component selection
Collection
Incorrect storage in the laboratory
Outside sample suitability45, 29.2%
65, 42.2%
13, 8.4%
28, 18.2%
3, 2.0%
Information technology (IT)-related HSE cases n=27
Refrigerator failure. Blood that had been out of temperature control was transfused n=25
Following a refrigerator failure, a retrospective audit showed that 21 units were transfused that had been out of temperature control. The refrigerator was taken out of use after the third temperature excursion and replaced by the manufacturer. In another refrigerator failure where the temperature dropped below zero one unit was transfused and 70 were wasted. In a third event a refrigerator temperature was >6oC for 3 hours. Four units were transfused to three patients and a further five units discarded.
Transfusion of expired units n=2
One unit of platelets was transfused 2 hours after expiry because the correct expiry date was not set when booking into the laboratory information management system (LIMS). A unit of red cells was transfused although the validity of the sample used to crossmatch had expired following recent transfusion and the allocated units had not been removed from the refrigerator.
Commentary
As in previous years there has been very little alteration in the overall findings. SHOT continues to highlight that all staff participating in the collection and administration of components should be adequately trained and adhere to the correct procedures. All staff need to be aware of infusion times and use the correct administration giving sets (BSH Robinson et al. 2018).
All laboratory related HSE including key messages and learning points are discussed in further detail in Chapter 7, Laboratory Errors.
References
Bolton-Maggs PHB (Ed), Poles D et al. on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. 2016 Annual SHOT Report (published 2017). https://www.shotuk.org/wp-content/uploads/SHOT-Report-2016_web_11th-July.pdf [accessed 8 January 2018].
BSH Robinson S, Harris A et al. The administration of blood components: a British Society for Haematology Guideline. Transfus Med 2018;28(1):3-21. http://onlinelibrary.wiley.com/doi/10.1111/tme.12481/pdf [accessed 22 February 2018].
Figure 9.2:
Near misses that
could have led to
HSE n=154

58
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
Authors: Jayne Addison, Peter Baker, Heather Clarke, Hema Mistry and Paula Bolton-Maggs
Definitions:
Wrong component transfused (WCT)
Where a patient was transfused with a blood component of an incorrect blood group, or which was intended for another patient and was incompatible with the recipient, which was intended for another recipient but happened to be compatible with the recipient, or which was other than that prescribed e.g. platelets instead of red cells.
Specific requirements not met (SRNM)
Where a patient was transfused with a blood component that did not meet their specific requirements, for example irradiated components, human leucocyte antigen (HLA)-matched platelets when indicated, antigen-negative red cell units for a patient with known antibodies, red cells of extended phenotype for a patient with a specific clinical condition (e.g. haemoglobinopathy), or a component with a neonatal specification where indicated. (This does not include cases where a clinical decision was taken to knowingly transfuse components not meeting the specification in view of clinical urgency).
Key SHOT messages
• Hospital transfusion teams should review their procedures for the collection of blood components to ensure that the necessary checks are always completed even when there is direct handover of components from laboratory to clinical staff
• Transfusion practitioners should ensure that knowledge of blood group compatibility is included and emphasised in training and competency assessments
Please see Chapter 7, Laboratory Errors for key messages related to laboratory staff
Deaths n=0
There were 19 deaths reported under IBCT (8 incidents due to clinical errors and 11 resulting from primarily laboratory errors), however none of the deaths were attributable to the transfusion.
Imputability 0: excluded or unlikely.
Major morbidity n=3 (3 laboratory errors)
Two women of childbearing potential developed anti-K following transfusion with K-positive red cells, as a result of component selection errors.
In the third case a D-negative 1-month old baby was transfused with a unit of D-positive red cells. In this case an interpretation error was made by four different biomedical scientists (BMS) who grouped the baby manually incorrectly on several occasions. The baby required exchange transfusion and anti-D immunoglobulin (Ig).
Incorrect Blood Component Transfused (IBCT) n=30710

59
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
10. Incorrect Blood Components Transfused (IBCT)
Case 10.1: A newborn baby (AB D-negative) was transfused with O D-positive red cells due to a manual interpretation error that went undetected on several occasions
Day 1 - a newborn baby was admitted with cardiac and respiratory compromise due to tetralogy of Fallot. A group and screen (G&S) sample was received with an electronic tracking number as no unique number was yet assigned. The sample was labelled ‘Baby’ plus the last name containing one ‘L’. BMS 1 processed the sample on the analyser. The analyser was unable to interpret the result. BMS 1 manually interpreted the result incorrectly as AB D-positive and entered this on to the laboratory information management system (LIMS). Patient identification (ID) check was carried out by BMS 2 and results authorised.
Day 17 - another sample was received with a unique number and labelled with a forename and the same last name as above but spelt with two ‘L’s. BMS 3 assumed that it was the same patient as detailed above because blood group AB D-positive was stated on the request form. The sample was processed on the analyser which was unable to interpret the result. BMS 4 incorrectly manually interpreted this again as AB D-positive. BMS 5 carried out the patient ID check and the results were authorised.
Day 34 - the baby eventually required extracorporeal membrane oxygenation (ECMO) following sudden deterioration. A further sample was received labelled the same as the one from day 1. The request was for a G&S, four red cell units and two units of platelets according to the ECMO protocol. BMS 6 selected four O D-positive red cell units (no suitable AB D-positive available) for crossmatching. As the baby had a previous G&S on file an uncrossmatched O D-positive unit was prepared to prime the ECMO system because of low blood volume in newborn children. BMS 7 carried out the patient ID check and the unit was released. Once analysis of the sample was complete, BMS 7 identified a difference in blood group (AB D-negative) from that on file (AB D-positive). The clinical area was contacted who advised that the ECMO system had already been primed with the O D-positive unit. BMS 7 returned all other blood components and suitable O D-negative components were ordered (no suitable AB D-negative available).
The baby had received 200mL of O D-positive red cells. The haematology consultant recommended exchange transfusion to avoid alloimmunisation to the D-antigen by removing the bulk of the D-positive red cells, followed up with measurement of residual D-positive red cells and administration of an appropriate dose of anti-D Ig. The baby was unstable for other reasons and was not fit enough for exchange until day 4 post D-incompatible transfusion. A 1.5 x blood volume exchange transfusion took place which reduced D-positive red cells to 2.8mL and a suitable dose of anti-D Ig was given. There were no side effects, however, the baby’s underlying clinical condition deteriorated and the decision was made to withdraw organ support and the baby died.
This was an avoidable incident caused by human error by four different BMS staff.
This case demonstrates multiple opportunities to validate results including second checks that only verified patient demographics and not results of manual interpretations. Following the initial misinterpretation, the same error occurred in two further G&S samples involving manual interpretations. Historical SHOT data definitively indicate that human errors associated with manual techniques involving ABO/D grouping may result in a potentially lethal outcome (Mistry et al. 2013).

60
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
Incorrect blood component transfused n=307 (100%)
158 (51.5%)
Wrong component transfused n=82
Laboratory
Clinical 149 (48.5%)
Specific requirementsnot met n=225
47 (57.3%)
35 (42.7%)
111 (49.3%)
114 (50.7%)
ABO-incompatible blood component transfusions n=7 (2 clinical and 5 laboratory errors)
Unintentional transfusion of ABO-incompatible blood components is a National Health Service (NHS) ‘Never Event’, (NHS England 2018). In Scotland these would be reported as ‘red incidents’ through the Scottish National Blood Transfusion Service clinical governance system and/or those of the Health Board.
Good news - the number of ABO-incompatible red cell transfusions has reduced further this year to one reported case, Figure 10.2.
9
10
7
3
1
2013 2014 2015 2016 2017
The risk of haemolysis and serious harm is more likely with ABO-incompatible red cells than with other components, but there were 6 additional cases of unintentional ABO-incompatible transfusions, 4 of fresh frozen plasma (FFP), all laboratory errors, and 2 of platelets (one clinical and one laboratory error). These provide important lessons for both clinical and laboratory staff. These cases are also reportable as NHS England never events.
The use of a bedside checklist at the final step (administration) of the transfusion process has been recommended in three previous Annual SHOT Reports and in November 2017 the NHS England Chief Medical and Nursing Officer endorsed this by issue of a central alerting system (CAS) alert to Medical Directors of all NHS organisations in England for immediate action, (DH 2017). The actions required are shown below. This alert has also been issued by Chief Medical Officers in the devolved countries.
Figure 10.1:
Overview of reports
where an incorrect
blood component
was transfused in
2017 n=307
Figure 10.2:
Reduction in the
number of ABO-
incompatible red
cell transfusions
2013-2017

61
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
10. Incorrect Blood Components Transfused (IBCT)
‘Safe blood transfusion. Use a bedside checklist.’
• Organisations should assess their bedside systems (including electronic systems) to ensure a confirmatory step is in place where the individual performing the checks must sign to say all steps have been followed
• This alert (and supporting information) should be circulated to all relevant staff, including to community nursing staff and midwives who may be involved in the transfusion of blood products in the community
This is the final opportunity to identify an error before the component is transfused. It is important to note that a bedside checklist will not detect a wrong component due to a wrong blood in tube (WBIT). That may be detected by a difference in blood group from a previous sample and is the reason for the recommendation for two independent samples to be taken prior to a first transfusion of red cells (BSH Milkins et al. 2013).
SHOT conducted a survey of progress with implementation of the bedside checklist 6 months following the recommendation published in July 2017. This survey also asked if the publication of the CAS alert in November 2017 made a difference to the implementation of this recommendation.
The results of the survey showed 91/222 (41.0%) Trusts/Health Boards have implemented a bedside checklist and in a further 65/222 (29.3%) implementation is in progress or plan to implement one. The results can be viewed at https://www.shotuk.org/wp-content/uploads/2016-SHOT-Recommendations-Survey-report-FINAL-1.pdf.
Patient group O+Donor group A+
Administration
Case 10.2
Case 10.2: Failure to complete the administration check at the bedside correctly leads to an ABO-incompatible red cell transfusion
Two units of red cells were issued for Patient 1. A healthcare assistant collected the correct unit and took this to the correct ward and handed it to the nurse looking after Patient 1. Two nurses then checked the component against the prescription in the clinical utility room and not next to the patient. The nurse who was to administer the blood then went to the wrong side room and administered the blood (donation group A D-positive) to Patient 2 (group O D-positive).
Within 5-10 minutes the patient complained of lumbar pain, a general feeling of being unwell, a hot sensation on his back, and had developed tachycardia. Transfusion was stopped and the clinical team informed. The patient stabilised and recovered with minimal medical intervention. No further information was provided.
Figure 10.3:
ABO-incompatible
red cell transfusion
n=1 (clinical error)

62
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
Learning points
• It is essential to identify the patient and complete all the final checks next to the patient immediately prior to administration
• If local policy states a two-person check, then both nurses must carry out the process next to the patient and independently of each other
• Completion of all necessary checks, including compatibility of the blood group of the component and the patient will prevent ABO-incompatible transfusions
Patient group B+ Donor group A-
WBIT
Case 10.3
Patient group A Donor group O
Componentselection
Case 10.4
WBIT=wrong blood in tube
Case 10.3: Duplicate samples lead to unintentional ABO-incompatible platelet transfusion because of a wrong blood in tube error
A male patient post chemotherapy for a brain tumour was admitted via the emergency department with a fever but no obvious focus for infection. Two samples were obtained from the patient in the medical admissions unit and received in the transfusion laboratory from the same person but different times documented, both grouped as A D-negative. Platelets were issued based on these two results.
Seven weeks later a new request form and sample were received for this patient, which grouped as B D-positive. Due to the discrepancy in the group history a full blood count sample taken 3 days earlier was tested which grouped as B D-positive.
The duplicate samples from the original admission were from a different patient, i.e. WBIT, and led to the issue and subsequent transfusion of incompatible platelets; group A D-negative to a group B D-positive patient. The patient had no adverse outcome.
Learning points
• A wrong blood in tube error cannot be detected at the bedside. Clarity of the process and reasons for obtaining a second sample as confirmation for the patient’s blood group should be emphasised with clinical staff at a local level
• Use of platelets across blood groups may be appropriate and is advocated in certain situations. These components should be tested and found negative for high-titre haemagglutinins (NHSBT 2017)
Figure 10.4:
Unintentional ABO-
incompatible platelet
transfusions n=2
(1 clinical,
1 laboratory error)

63
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
10. Incorrect Blood Components Transfused (IBCT)
Case 10.4: ABO-incompatible platelets selected incorrectly by a BMS who was not paying attention to the task
A unit of platelets was requested for a patient with non-Hodgkin lymphoma and critical site bleeding. The laboratory staff issued group O platelets by mistake for a group A patient. The ward staff completed the pre-transfusion checks and transfused the unit. When the error was identified by the laboratory staff they contacted the ward staff and advised them not to transfuse the platelets but were informed that the transfusion had been completed.
The BMS issuing the platelets was experienced and had regularly worked in transfusion but was new to this laboratory. The BMS assumed that they were to take the platelets from the top shelf of the stock incubator. The LIMS flagged that group O platelets were being selected for a group A patient but the BMS overrode the warning. The BMS could not explain why they issued mismatched platelets but it was discovered that although the BMS had most competencies up to date they did not have competency for issue. The patient did not suffer any untoward harm.
In addition to the primary laboratory error, the bedside administration check was not performed correctly or was performed by staff with insufficient knowledge. The bedside check includes confirmation of compatibility.
Learning point
• Staff should be reminded that they should never perform any tasks for which they have not been competency-assessed
Patient group A+Donor group O+
Componentselection
Patient group A+Donor group O+
Sample receiptand registration
Case 10.8
Patient group A+Donor group O+
Testing
Patient group B+Donor group O+
Componentselection
Case 10.5
Case 10.5: A patient whose blood group was B was transfused with group O FFP resulting from poor communication during handover
A patient received multiple transfusions of red cells, FFP and platelets for recurring gastrointestinal (GI) bleeding in the presence of liver disease. The patient had been grouped as O due to the presence of donor red cells in the test samples (the patient’s actual blood group was B).
Several messages had been hand written on a single sticky note by a junior member of laboratory staff undergoing transfusion training. During handover these messages were misinterpreted and in addition, no formal request form for FFP had been received from the clinical area. Unused, pre-thawed group O FFP prepared for an earlier patient was issued knowingly against national guidelines (BSH O’Shaughnessy et al. 2004) as the BMS thought that concessionary release had been approved.
The LIMS allowed major ABO mismatches for plasma components although it did display a warning flag that was overridden. The laboratory staff did not seek formal confirmation before handing the FFP to a porter. The patient was transfused the incompatible FFP. There was no reported clinical adverse outcome.
Figure 10.5:
ABO-incompatible
FFP transfusions
n=4 (laboratory
errors)

64
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
The incident was caused by poor communication at handover by an untrained/inexperienced member of staff and was further exacerbated by an experienced member of staff who made assumptions from the written note including approval of concessionary release (although they should know this incompatibility). The validation process had not been completed fully as a recent upgrade to the LIMS had not had ABO-incompatible prevention activated in the live system; the test worked in test mode but did not work in the live mode.
Clear documentation must always be available to the issuing BMS (i.e. request form, clearly documented telephone request and concessionary release form). This case clearly demonstrates the requirement for robust processes and communication during validation and handover, especially when junior/inexperienced members of staff are involved. It is also essential to ensure that the LIMS is fully validated in the live mode as well as the test mode when changes or software updates are made. The ABO-incompatibility should have been detected both by the BMS and at the bedside check.
See also Case 10.8.
Critical steps in the transfusion process
Errors occur at each of the nine steps in the transfusion process. Each step incorporates independent checks at every point that should, if carried out correctly and in full, be able to identify any errors made earlier.
Figure 10.6 illustrates the nine steps including both clinical and laboratory areas and the two critical points where positive patient identification is essential. The clinical cases in this chapter demonstrate where the incident initially occurred, the category of error and helps to understand why they happen and identify any learning points for clinical and laboratory staff.
Note: Errors associated with laboratory steps are discussed in more detail in Chapter 7, Laboratory Errors.
1 REQUEST
Critical points wherepositive patientidentification isessential
Critical points in the laboratory
2 SAMPLE TAKING
3 SAMPLE RECEIPT
4 TESTING
5 COMPONENT SELECTION
6 COMPONENT LABELLING
7 COMPONENT COLLECTION
8 PRESCRIPTION
9 ADMINISTRATION
Note: Once a decision to transfuse is made, the authorisation or prescription may be written at variable times during this sequence, but must be checked during the final stage
Figure 10.6:
Transfusion
process
(nine steps)

65
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
10. Incorrect Blood Components Transfused (IBCT)
WCT=wrong component transfused; SRNM=specific requirements not met
5
5
26
24
10
7
2
3
10
1
2
1
21
63
18
109
0 20 40 60 80 100 120
Miscellaneous
Administration
Prescription
Collection
Component labelling
Component selection
Testing
Sample receipt
Sample taking
Request
SRNMWCT
WCT=wrong component transfused; SRNM=specific requirements not met
2
1
2
4
19
3
1
1
2
0 5 10 15 20 25
Wrong patient
Wrong component
D-mismatch
Wrong blood in tube
ABO-incompatible red cells
RequestSample takingCollectionAdministrationMiscellaneous
Figure 10.7:
Points in the
process where
the first mistake
occurred (clinical
and laboratory)
leading to wrong
component
transfusion
or specific
requirements not
being met n=307
Figure 10.8a:
Clinical errors
resulting in wrong
component
transfused n=35

66
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
HEV=hepatitis E virus; CMV=cytomegalovirus
72
9
18
5
5
2
1
1
1
0 10 20 30 40 50 60 70 80
Irradiated
CMV-screened
HEV-screened
Incorrect phenotype
Mutliple missed requirementse.g irradiated & HEV-screened
Blood warmer
RequestPrescriptionAdministrationMiscellaneous
HEV=hepatitis E virus; CMV=cytomegalovirus
FFP=fresh frozen plasma; HSCT=haemopoietic stem cell transplant
5
1
1
1
5
1
1
2
4
6
2
11
1
3
1
2
0 2 4 6 8 10 12 14 16
Wrong ABO/D to HSCT patient
D-mismatch
ABO-incompatible FFP
Wrong component
Wrong patient
ABO non-identical
ABO-incompatible platelets
Sample receipt and registrationTestingComponent selectionCollectionMiscellaneous
FFP=fresh frozen plasma; HSCT=haemopoietic stem cell transplant
Figure 10.8b:
Clinical errors
leading to specific
requirements not
being met n=114
Figure 10.8c:
Laboratory errors
resulting in wrong
component
transfused n=47

67
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
10. Incorrect Blood Components Transfused (IBCT)
HEV=hepatitis E virus; HLA=human leucocyte antigen; CMV=cytomegalovirus
2
1
1
2
6
1
5
6
57
1
1
1
3
5
5
1
4
1
1
1
5
1
0 10 20 30 40 50 60 70 80
Sampling errors
Apheresis platelets
CMV-screened
HLA-matched
Irradiated
Methylene-blue treated
Incorrect phenotype
HEV-screened
K-negative
Washed platelets
Blood warmer Sample receipt and registrationTestingComponent selectionComponent labellingMiscellaneous
HEV=hepatitis E virus; HLA=human leucocyte antigen; CMV=cytomegalovirus
Step 1: Request errors n=112 (109 SRNM and 3 WCT)
The request is the first of the nine steps in the transfusion process following the decision to transfuse. The request for the selection and release of components must include patient core identifiers and should also include gender, reason for request and any relevant factors which influence transfusion, e.g. current diagnosis, any comorbidities, pregnancy status and any clinical requirements (BSH Robinson et al. 2018).
Specific requirements not met account for 109/112 (97.3%) of primary request errors and this is similar to previous years. The introduction of universal screening of all components for HEV by UK Blood Services in late spring 2017 is reflected in the lower number of reported missed specific requirements compared to 2016. There were 128 primary request errors in 2016 of which 123 (96.1%) were SRNM.
The common themes resulting in request errors are similar to those in previous years:
• Failure of communication between clinical and laboratory areas
• Failure of communication between shared care hospitals
• Failure to identify a historical diagnosis of Hodgkin lymphoma
• A lack of knowledge and awareness of specific requirements
• Failure to provide full clinical details on request forms e.g. pregnancy as a requirement for CMV-screened components
There is an opportunity to detect omission of irradiation at other steps in the transfusion process if staff complete their part of the process correctly and in full. Haematology and oncology nursing staff should be very knowledgeable about specific requirements for their patients and before commencing administration of blood components should always check that any additional clinical requirements have been met particularly irradiated (BSH Robinson et al. 2018).
Figure 10.8d:
Laboratory errors
leading to specific
requirements not
being met n=111

68
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
Learning points
• Hospital transfusion teams should review their procedures for identification of specific requirements to ensure these reduce the possibility for error locally
• Hospital transfusion teams should explore ways to improve communication between themselves and with other hospitals with which patient care may be shared
Step 2: Taking the blood sample n=2
Taking a blood sample for pre-transfusion compatibility testing is one of two critical positive patient identification steps in the transfusion process. The collection of the blood sample from the patient and subsequent completion of details on the sample must be performed as one continuous, uninterrupted procedure, involving one patient and one trained, competent and authorised member of staff. The minimum sample tube information requirements are patient core identifiers, date and time sample taken and identification of member of staff taking the sample. Sample tubes must be immediately labelled at the patient’s (bed)side by the individual who took the sample (BSH Robinson et al. 2018).
In both cases there was a failure to follow the correct procedure for obtaining two samples for pre-transfusion compatibility testing resulting in WBIT and consequently the wrong component transfused.
• ABO-incompatible transfusion of platelets, Case 10.3
• ABO-non identical transfusion of red cells to a neonate
Step 3: Sample receipt and registration n=25
Correct procedures for sample receipt and registration are essential to ensure that the right investigation is performed for the right patient on the right sample at the right time (dependent on the patient’s transfusion history).
• Missed information on request form n=8 (6 specified irradiated, 1 CMV-screened and 1 recorded that this was a patient with sickle cell disease)
• Demographic data entry error n=2
• Available historical information not heeded n=15
Learning point
• Laboratory staff must heed patient history and adhere to a zero-tolerance policy during sample receipt and registration, see Chapter 7, Laboratory Errors for further information
Step 4: Testing n=73
The correct tests/analyses are required to ensure the safe provision of blood components and should be undertaken in full compliance with local and national guidelines for pre-transfusion testing (BSH Milkins et al. 2013).
• Technical error n=6
• Transcription error n=6
• Interpretation error n=10
• Procedural error n=51

69
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
10. Incorrect Blood Components Transfused (IBCT)
Learning point
• All policies and procedures must be robust and strictly adhered to by laboratory staff without deviation. They must be validated and reviewed regularly (review, improve and rewrite if changes are needed); Chapter 7, Laboratory Errors, provides further information
Step 5: Component selection n=45
This step ensures that the correct components (together with the specific requirements) are selected to comply with the patient’s requirements and the clinical request.
Learning point
• Care needs to be taken when selecting components to ensure they are compatible and meet the specific requirements of the patient; Chapter 7, Laboratory Errors provides further information
Step 6: Labelling, availability and handling and storage errors n=1
The correct component needs to be labelled with the correct four (or five) key patient identifiers; first name, last name, date of birth (DOB), unique patient identifier (and first line of address in Wales) (BSH Milkins et al. 2013). Components need to be accessible and available for the time required, if this is not attainable then the clinical staff need to be informed. The components need to be handled and stored correctly as defined in national guidelines (JPAC 2013).
Step 7: Collection n=26 (23 clinical, 3 laboratory errors) 19/26 (73.1%) were urgent/emergency transfusions
This step ensures that the correct component is collected from the storage site and delivered to the correct clinical area. The blood component must only be collected and received by trained, competent and authorised members of staff. Authorised collection documentation must contain the patient’s verified core identifiers and details of the component to be collected. These details must be checked against the details on the laboratory-generated label attached to the blood component pack (BSH Robinson et al. 2018).
Further checks must include the correct component type, expiry date and on receipt in the clinical area a check that the correct blood component has been delivered.
Collection as the primary error accounted for 23/35 (65.7%) clinical WCT. This year there were a further 3 collection errors where laboratory staff handed over components to clinical staff that were incorrect or intended for a different patient (Case 10.7). Collection of blood components may be carried out by several different healthcare workers as shown below for these 26 cases:
• Healthcare assistant n=5
• Porter n=4
• Nurse n=5
• Midwife n=2
• Unknown n=10
In 16/26 (61.5%) staff were trained and competency-assessed to carry out this step in the transfusion process but it was unknown for the remaining 10/26 (38.5%). Several cases demonstrated lack of knowledge about different blood components both in cases that involved unregulated healthcare workers and also (surprisingly) registered staff also lacked sufficient knowledge in this area.
It should be noted that 11/26 (42.3%) cases were categorised as emergency transfusions and 8/26 (30.8%) as urgent (together 19/26, 73.1%). These were required for high stress/busy clinical areas including intensive therapy units, theatres, obstetrics and emergency departments.

70
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
Case 10.6: Staff under pressure to collect and administer platelets before surgery results in WCT
A woman in her 50s was admitted for planned dental surgery and required platelets. Platelets were prescribed but the healthcare assistant thought she had been asked to collect red cells and was unaware there were other types of components. The staff nurse administered the red cells following the correct identity checks but failed to notice it was the wrong component according to the prescription.
The patient was an unexpected admission to the ward and was due in theatre after the platelet transfusion; there was pressure and distraction from several calls from theatre asking if the patient was ready.
Case 10.7: Laboratory staff removed blood from a satellite refrigerator and handed over incorrect blood components to clinical staff
A male patient in his 20s required red cell transfusion in theatre following major trauma. Ten units were crossmatched and available in the remote issue theatre refrigerator. Clinical staff were unable to gain access to the refrigerator; it was ‘thinking’ so they asked the attending laboratory staff for help. The laboratory staff managed to open the refrigerator and removed two O D-negative units (that were designated for remote allocation) rather than the available crossmatched components.
The correct procedure for removal of units from the kiosk did not take place. The units were given directly into the hands of the clinical staff instead of being scanned. Completing the correct step of scanning the units following their removal from the kiosk would have alerted both the clinical and laboratory staff that the incorrect components had been removed.
Learning point for the laboratory
• Direct handover: if laboratory staff are responsible for directly handing components to a collecting nurse/porter, they need to ensure that the component(s) meets the requirements of the clinical request and the collection slip. Any additional units must be confirmed with a traceable clinical request
Learning points for clinical staff
• If laboratory staff hand blood components over directly to clinical/portering staff, then the correct checks should still take place before leaving the storage site, for both electronic and manual collection systems
• When components are required for urgent or emergency transfusions it is essential that time and care is taken to carry out checks correctly and in full
• Ensure that blood component type and specification is emphasised in collection training
Step 8: Prescription (written authorisation) n=2
This step is identified in Figure 10.6 as step 8, but although the prescription may be written at different points in the transfusion process it should be completed and checked prior to the final administration step.
Blood components should only be authorised by an appropriately trained, competent and locally designated registered regulated health care professional (HCP). Blood component authorisation must include the patient’s core identifiers, the component to be transfused, date of transfusion, the volume/number of units, the rate of transfusion, any other clinical requirements or instructions required and must be signed by the authoriser (BSH Robinson et al. 2018).

71
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
10. Incorrect Blood Components Transfused (IBCT)
Two primary errors occurred at this step; in both the specific requirement for a blood warmer was not documented on the written authorisation. However, this was evident on the transfusion laboratory documentation and could have been identified at the administration step.
Learning point for clinical staff
• The prescription is not the only place where specific instructions for administration may be documented. If there is any discrepancy between laboratory and clinical instructions, check before commencing the transfusion
Step 9: Administration n=6 (5 WCT, 1 SRNM)
Administration is the final opportunity to prevent patients receiving the incorrect component or missing their specific requirements due to errors earlier in the transfusion process. It is essential that the final administration check is conducted by trained, competent and authorised, registered regulated HCP.
This final administration check must be performed next to the patient. The donation number, blood group and expiry date on the component pack label must match the laboratory-generated label attached to the component and the component blood group must be appropriate for the patient. Check that any additional clinical requirements have been met e.g. irradiated or CMV-screened components (BSH Robinson et al. 2018).
Transfusion to the wrong patient in 4/6 cases was attributable to a failure to follow policy for correct patient identification. In these 4 cases two registered HCP were involved in the checking procedure.
The blood group of the recipient and blood component of all clinical WCT collection and administration errors show the outcome as:
• 13/28 (46.4%) ABO-identical (3 FFP, 2 platelets, 7 red cells, 1 combination)
• 7/28 (25.0%) ABO-non-identical (6 red cells, 1 platelets)
• 1/28 (3.6%) ABO-incompatible (red cells)
• 7/28 (25.0%) unknown (5 red cells, 2 unknown)
The blood group check at the final step is essential to prevent transfusion of components with the wrong ABO or D-group. If this had been noticed and challenged, 8/28 (28.6%) wrong transfusions may have been prevented (7 red cells and 1 platelets).
26 of the primary errors in collection progressed to the bedside and the number of people who were involved in this final administration step is shown below:
• Two registered HCP n=12 cases
• One registered HCP n=5 cases
• Unknown n=9 cases
The participation of two registered HCP at the administration step seems common practice however, there is no confirmation this is carried out properly by double independent checking as recommended in guidelines (BSH Robinson et al. 2018).
The 2016 Annual SHOT Report included a learning point to explore a two-person dependent check by use of a verification checklist. A pilot is currently in progress.

72
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
Version 1.2 February 2018 Review Date: May 2018
PRE-TRANSFUSION ADMINISTRATION ABO D BLOOD GROUP CHECK Group O FFP/ Octaplas / Cryoprecipitate
MUST only be administered to Group O Patients Compatibility of plasma components differs from red cells
When performing the pre-transfusion bedside check, you must check the blood component (Red Cells, Fresh Frozen Plasma, Octaplas, Cryoprecipitate, or Platelets) is compatible. If the blood component blood group is not the same as the blood group of the patient, you must check the compatibility table below or contact the transfusion laboratory if unsure (STH ext 84774, Guy’s ext 82766, bleep 0201).
This check is only one part of the full bedside pre-transfusion checks – see overleaf
Patient ABO D blood group
Compatible RED CELLS
Compatible FRESH FROZEN PLASMA
/ OCTAPLAS / CRYOPRECIPITATE
Compatible PLATELETS
Unknown O AB, A*, B* AB, A*, B*, O*
O O O, A, B, AB O, A, B, AB
A A, O A, AB, B* A, AB, B*, O*
B B, O B, AB, A* B, AB, A*, O*
AB AB, A, B, O AB, A*, B* AB, A*, B*, O*
Pos Pos or Neg Not applicable Pos or
Neg
Neg# Neg# Not applicable Neg#
Compatible blood groups are listed in order of preference
*Issued when permitted due to component availability
# D positive red cells & platelets may be issued for D negative women over the age of 50yrs and D negative males of any age according to availability and urgency of transfusion
Miscellaneous n=15 (4 clinical and 11 laboratory errors)
In some cases, the error was not related to the defined nine steps in the transfusion process, Figure 10.6.
Laboratory n=11
In 3 cases the patient received the wrong component. Two patients received D-mismatched components. In 1 case the BMS did not activate a flag for a patient with a variant D group to highlight that they required D-negative components. The patient history was not available in the 2nd case due to a cyber-attack where information technology (IT) systems were down. In the 3rd, the wrong ABO group was given to a haemopoietic stem cell transplant (HSCT) patient because the patient record had not been updated.
In 8 cases the patients’ specific requirements were not met. In 6 cases IT was a contributing factor: 2 were due to a cyber-attack, other causes were LIMS failure, and the BMS having no access to the reference laboratory antibody database, ordering the wrong component and not maintaining the patient record.
Figure 10.9:
Example of blood
group compatibility
chart for use at
the bedside, Guys
and St Thomas’
hospital NHS
Foundation Trust

73
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
10. Incorrect Blood Components Transfused (IBCT)
The Blood Service supplied wrong components in 2 cases that were not detected by the transfusion laboratory staff prior to issue. Case 7.10 in Chapter 7, Laboratory Errors.
Clinical errors n=4
In 2 cases specific requirements were not met when blood was required in an emergency (HEV-screened in 1 because the Blood Centre was unable to meet the request, and irradiated in the other case when emergency O D-negative units were transfused).
In 2 cases wrong components were transfused where blood was required in an emergency:
• Incorrect unit number used to access the electronic collection system
• Configuration of software of the blood refrigerator resulted in the kiosk not asking for the patient’s age when accessing for emergency blood
Working as a team
The following incidents demonstrate that in cases with multiple errors there were missed opportunities to detect an earlier error that could prevent IBCT.
• 19/158 (12.0%) errors that originated in the laboratory could have been detected in the clinical area
• 132/307 (43.0%) errors could have been detected in the clinical area at the administration step and in 12/132 (9.1%) the errors could have been detected in the laboratory before reaching the clinical area
• There was a total of 1020 near miss IBCT cases (899 WCT and 121 SRNM) of which 839 (82.3%) resulted from clinical errors early in the process at request or sampling. Most of these near miss errors (684/839, 81.5%) were detected by laboratory (n=653) or clinical procedures (n=31) later in the process, although 155/839 (18.5%) were only discovered accidentally, e.g. by an individual realising their earlier error or someone else involved in the process noticing something unusual. See also Chapter 12, Near Miss Reporting (NM)
Multiple errors:
Case 10.8: A demographic data entry at sample receipt results in a patient receiving ABO-incompatible FFP
Five units of FFP were ordered by telephone for Patient 1. During the laboratory IT process, the copy and paste function was used to populate the sample identification number field. However, the sample ID number pasted into the sample ID field belonged to the previous patient (Patient 2).
At collection, the porter noted the discrepancy between patient details of the person he was sent to collect for and those on the FFP that was given to him by the BMS.
The FFP was then re-labelled for Patient 2, but the BMS failed to note that the FFP was incompatible. The nurse administering the FFP noted the group was different to the patient but believed that group O components were compatible for all patients. This resulted in group O (Patient 2) FFP being administered to Patient 1 (group A).
Sample receipt and registration: a telephone request was taken, and the BMS selected the wrong patient.
Component selection: the BMS did not identify that the wrong patient had been selected.
Component labelling: the BMS did not check the label against the request. When the porter noticed the discrepancy the BMS took the FFP and re-labelled it for Patient 2 however the BMS failed to note that the FFP was incompatible.
Collection: at collection, the porter noted the discrepancy between patient details of the person he was sent to collect for and those on the FFP that was given to him by the BMS.

74
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
Administration: the nurse administering the FFP noted the group was different to the patient but believed that group O components were compatible for all patients.
To maintain the integrity of the request, the sample barcode should always be used to request components; copy and paste should not be used. When labelling components, especially re-labelling, the patient request should be reviewed against the demographic and blood group data. This case again demonstrates the lack of knowledge in the clinical area which is the last opportunity to stop the transfusion.
Learning point
• Staff involved in the transfusion process need to understand all component types including their storage conditions but most importantly their blood group compatibility with the patient and restrictions for specific patient groups e.g. gender, age, pregnancy and taking disease status into consideration
Case 10.9: Failure at multiple points in the transfusion process both in clinical and laboratory steps leads to a patient receiving CMV-unscreened red cells
A request form was received in the transfusion laboratory for red cells, diagnosis stated as ‘at risk of PPH’ (postpartum haemorrhage) and was marked as ‘urgent’. There was no indication that the red cells were required for antenatal anaemia and the laboratory staff assumed the red cells were required during or at delivery. A new request form was completed, but the transfusion laboratory was not contacted by telephone to inform them of the change. The pneumatic tube system was not working so the original form was printed by the BMS and used to issue CMV-unscreened red cells. At both collection and administration staff failed to notice the requirement for CMV-screened blood despite this being evident on the prescription.
Request: initial failure to understand the indication for CMV-screened components by the requesting clinician and provision of misleading information to the laboratory. Failure to contact the laboratory to confirm the second request and explain the transfusion was required prior to delivery.
Sample receipt and registration: no revision received and assumption from the given diagnosis that the transfusion was required post delivery.
Component selection: the BMS printed the original request and selected unscreened red cells unaware the transfusion was required pre delivery.
Collection: specific requirements should be checked at this step as identified on the blood collection slip.
Prescription: CMV-screened blood was indicated on the prescription.
Administration: the midwife failed to complete the full checks at the bedside which should include the specific requirements on the blood component against the prescription.
Learning points
• Clear instructions communicated to the transfusion laboratory are essential to ensure the correct components are selected and issued
• Clinical staff must ensure that the bedside check is completed in full and includes specific requirements
Near miss IBCT-WCT cases n=899
As in previous years, most near miss cases that could have led to IBCT were WBIT incidents n=789/899 (87.8%).

75
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
10. Incorrect Blood Components Transfused (IBCT)
Collection
Request errors
AdministrationWrong blood in tube (WBIT)
Laboratory errors
789
3118
592
WBIT87.8%
WBIT potentially leading to IBCT n=789
Definition of WBIT incidents:
• Blood is taken from the wrong patient and is labelled with the intended patient’s details
• Blood is taken from the intended patient, but labelled with another patient’s details
386
469505
643686
780 776
0
100
200
300
400
500
600
700
800
900
2010 2011 2012 2013 2014 2015 2016 2017Year
Nea
r m
iss
WB
IT
0
10
20
30
40
50
60
70
Num
ber
of
WB
IT le
adin
g t
o IB
CT
3 3
789
5 6
0 02 2
Near miss WBITWBIT leading to IBCT
Figure 10.10:
Most near miss
IBCT were WBIT
Figure 10.11:
Cumulative
comparison of near
miss WBIT and
those leading to
IBCT

76
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
Detection of WBIT incidents
Most WBIT incidents, 688/789 (87.2%), are detected during laboratory procedures, although sometimes the detection is fortunate, such as the sample taker realising their error while the sample is being processed. Patient safety relies on vigilance or quality management by all staff involved in the transfusion process. However, these detection measures should ideally be unnecessary if sample taking is always carried out accurately with positive patient identification.
Testing87.2%
974
688
Other
Sample receiptTesting
4
97
688
Near miss IBCT-SRNM cases n=121
The near miss incidents related to patients’ specific requirements show similar learning points to the full incidents that led to transfusion of components where specific requirements were not met.
Administration(outside sample validity)
1, 0.8%
Failure to request
46, 38.0%
Sample receipt
22, 18.2%
Testing
26, 21.5%
Componentselection
24, 19.8%
Sample-taking error2, 1.7%
Figure 10.12:
Point in the
process where
a wrong blood
in tube (WBIT)
incident was
detected
Figure 10.13:
Near misses that
could have led to
IBCT-SRNM n=121

77
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
10. Incorrect Blood Components Transfused (IBCT)
IT-related IBCT-WCT cases n=21
Laboratory n=17 and clinical n=4
There were 10/21 (47.6%) ‘wrong blood’ incidents that were in HSCT or solid organ transplant patients.
Use of warning flags or alerts n=7
There were 5 cases where a warning flag was in place but not heeded and 2 cases where the flag was not updated.
Failure to consult the historical record n=7
In 7 cases there was a failure to consult the historical record; 2 cases because the wrong record was selected on the LIMS or patient administration system (PAS); 4 cases where the historical record was not consulted; 1 case occurred as a result of a failure to link or merge records.
Incorrect result entered manually n=3
Wrong blood was transfused from three manual entry errors. In one a manual group was performed following anomalous ABO/D testing on the analyser but the incorrect D group was assigned at data entry and O D-positive red cells were administered instead of O D-negative in a male patient in his 60s. In another case group AB solvent detergent-treated FFP for plasma exchange was issued to the wrong patient following a verbal request where only the last name was given. This hospital commented that they were exploring electronic ordering of components as a future development. Incorrect entry of the blood groups required for a HSCT patient led to the wrong red cells being transfused, although there was no harm to the patient.
Electronic blood management systems n=3
Two errors in this category related to removing emergency blood for critically ill neonates from a remote issue refrigerator. In 1 case, instead of using the emergency procedure, the midwife used the mother’s hospital number to obtain an adult unit of blood and in the 2nd case the emergency programme was used but a recent software upgrade meant that the age of the recipient was not required to remove emergency blood so adult (not neonatal) blood was collected.
Case 10.10: Wrong blood transfused despite having a full electronic blood management system
Incorrect but compatible blood was transfused to a day-case patient in a hospital with a full electronic blood management system including both refrigerator collection and bedside safety checks. The same nurses were caring for two patients. The health care assistant was asked to collect blood for Patient 1 (B D-positive). She was given the compatibility tag from the first unit to collect the second unit for Patient 1 (incorrect practice). At the same time, she was given the compatibility tag from Patient 2 (O D-positive) to return to the laboratory for traceability purposes. She used the blood audit and release system (BARS) to collect blood from the refrigerator but used Patient 2’s details on the compatibility tag in error. Back on the day-case unit, the BARS system was available but was not used. The error was not detected at the beside with manual checking so the O D-positive blood labelled for Patient 2 was transfused, fortunately without adverse event. The error was detected when someone went to collect the next unit of blood for Patient 2, and it was found to be missing.

78
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
Learning points
• Failure to use electronic transfusion systems when available at critical points in the transfusion process, increases risk of error. Staff must retain the skills to perform the necessary checks manually and not rely on the checks performed earlier in the process
• If the blood group compatibility has been checked as recommended at the bedside, and the blood group of the component does not match with the recipient this should trigger the question ‘is this compatible?’ The practitioner should then establish whether this is the correct unit for the patient about to be transfused
Computer downtime n=1
Despite the high-profile cyber-attacks against NHS computers in the last year there was only 1 wrong blood event in this category. D-positive platelets were inadvertently issued to a D-negative patient but this was a male over 70 years of age.
IT-related IBCT-SRNM cases n=112
Laboratory n=53 and clinical n=59
Use of warning flags or alerts n=83
Not in place n=42, not heeded n=12, not updated n=29
The information was most frequently not provided to the laboratory to activate a warning flag on the LIMS. Even when provided, the updating of the LIMS warning flag in response to clinical information was not always timely. The mode of presentation of warnings is inconsistent between different specific requirements and also varies between different LIMS which can lead to flags being ignored or misinterpreted. Some systems will prevent issue of the wrong component specification whereas others will provide the information in a field that can be ignored or overridden. As a result of failure of the warning flags as described above, in 41 cases irradiated components were not provided and in 22 cases phenotyped/antigen-negative blood was not provided.
Failure to consult the historical record n=17
Use of the historical computer record n=6 and failure to link, merge or reconcile computer records n=11
In many of these cases, the relevant information about specific requirements was not available on the current LIMS because the data had not been migrated from a legacy system and a manual process was in place to look up each patient prior to issuing blood or blood components. Manual look-up processes are time consuming and subject to errors of omission as well as transcription.
Incorrect result entered manually n=1
There was 1 case where incorrect manual transcription of data in the laboratory led to the wrong phenotype being issued to a patient.
Other computer system failures n=10
During this reporting year there were some notable cyber-security incidents and healthcare IT systems were affected. A number of errors related to specific requirements were reported because of IT failure; 1 where a woman was not known to be pregnant and was provided with CMV-unscreened blood, 1 failure to provide irradiated components and 8 where the exact red cell phenotype required was not issued.
The following two examples are of incorrectly configured or validated systems.

79
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
10. Incorrect Blood Components Transfused (IBCT)
Case 10.11: LIMS not correctly configured for sample validity
The transfusion laboratory identified that the incorrect sample validity had been set up in the LIMS. This was correct at the time of configuration but had not been changed when new British Society for Haematology guidelines were issued in 2012 (BSH Milkins et al. 2013). In a look-back over 2 months it was identified that 30 units of red cells were transfused to 12 previously transfused individuals using 7-day rather than 3-day sample validity.
Case 10.12: Specific requirements message does not transmit from the hospital information system (HIS) to LIMS
A patient for solid organ transplant required irradiated blood components. Although there was no specific requirements form provided to the laboratory, the request for blood was made electronically and the requirement for irradiated blood components was indicated in that request. Unfortunately, this message did not auto-populate the specific requirement field on the LIMS. Investigation showed that a recent update to the specific requirement wording on HIS had not fully been tested to see if it still auto-populated.
Online blood ordering system (OBOS) n=1
There was 1 case where the laboratory selected the wrong component on OBOS.
Electronic issue n=13
Electronic issue should be entirely dependent on the LIMS algorithm and there were 13 cases in 2017 where blood was issued electronically where the patient was not eligible. Most of these resulted in blood of the wrong phenotype being issued to patients with current or historical antibodies. One case should not have been eligible for remote electronic issue and another case should have been ineligible because of a recent solid organ transplant. These cases have already been included within the numbers in the subheadings above.
Commentary
There are many opportunities to prevent incorrect blood components being transfused. Analysis of both clinical and laboratory cases demonstrates gaps in blood component knowledge that are contributing to the errors.
Although hospitals deliver blood transfusion training and complete competency assessments to a high standard both in clinical and laboratory settings there is a need to place greater emphasis in training about the different component types, their specific indications, importance of specific requirements especially those related to age and gender, and training must include an understanding of blood group compatibility.
The importance of the bedside check must also be emphasised in training as the final opportunity to ensure the patient receives the correct component and as one of two critical steps in the process that must be completed correctly and in full every time. It is especially important during emergency and urgent situations when additional pressure and distractions are evident.
References
BSH Milkins C, Berryman J et al. Guidelines for pre-transfusion compatibility procedures in blood transfusion laboratories: Transfus Med 2013;23(1):3-35. http://onlinelibrary.wiley.com/doi/10.1111/j.1365-3148.2012.01199.x/full [accessed 21 February 2018].
BSH O’Shaughnessy DF, Atterbury C et al. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol 2004;126(1):11-28. (Note that new FFP/cryo guidelines have been published as below)
BSH Green L, Bolton-Maggs P et al. BSH Guidelines on the spectrum of fresh frozen plasma and cryoprecipitate products: their handling and use in various patient groups in the absence of major bleeding. Br J Haematol 2018;181(1):54-67.

80
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
10. Incorrect Blood Components Transfused (IBCT)
BSH Robinson S, Harris A et al. The administration of blood components: a British Society for Haematology Guideline: Transfus Med 2018;28(1):3-21. http://onlinelibrary.wiley.com/doi/10.1111/tme.12481/pdf [accessed 26 February 2018].
Department of Health (DH). Safe transfusion practice: use a bedside checklist (CAS) CEM/CMO/2017/005 (2017). https://www.cas.dh.gov.uk/ViewandAcknowledgment/ViewAlert.aspx?AlertID=102663 [accessed 19 February 2018].
JPAC. Guidelines for the Blood Transfusion Services in the UK: 8th Edition Red Book 2013. http://www.transfusionguidelines.org.uk/red-book [accessed 21 February 2018].
Mistry H, Asher D et al. Human error associated with manual techniques with or without automation in ABO/RhD grouping are associated with potentially lethal outcomes: Vox Sang 2013;105:23.
NHS England. Never Events list 2018 https://improvement.nhs.uk/resources/never-events-policy-and-framework/#h2-revised-never-events-policy-and-framework-and-never-events-list-2018 [accessed 19 February 2018].
NHSBT. Appropriate use of platelets across blood groups. 2017. http://hospital.blood.co.uk/media/28910/appropriate-use-of-platelets-across-blood-groups-final-_1_-_2_.pdf [accessed 22 March 2018].

81
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
11. Avoidable, Delayed and Under or Overtransfusion (ADU)
Authors: Paula Bolton-Maggs and Caroline Wall
Overview
• Avoidable transfusion n=101 (near miss n=10)
• Delayed transfusion n=95 (near miss n=1)
• Under or overtransfusion n=24 (near miss n=1)
• Cases related to prothrombin complex concentrate (PCC) n=5
Avoidable, Delayed and Under or Overtransfusion (ADU) n=225(n=246 in 2016) 11

82
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
11a. Delayed Transfusion
Definition:
Where a transfusion of blood/blood component was clinically indicated but was not undertaken or non-availability of blood components led to a delay with impact on patient care (not restricted to emergency transfusion).
Delays in transfusion of patients with antibodies
One death (Case 11a.1) and 2 other cases of delay (Cases 11a.7 and 11a.9 below) were caused by the presence of antibodies.
Key SHOT messages
• Guidelines must not be oversimplified and made into rules. While it may be safer not to transfuse at night, the patient’s clinical need for transfusion must override this (Bolton-Maggs et al. 2014). However, transfusion should not be undertaken without adequate trained staff on duty to monitor the patient and react appropriately to any complications, and this would be particularly important at night
• Desire to follow good transfusion practice in some areas, if taken out of context, may risk patient death or morbidity due to delays in transfusion in major haemorrhage scenarios. This includes withholding any blood when the patient’s antibody screen is positive, but antibody identification is not yet completed:
– There are safety concerns regarding a possible delayed haemolytic transfusion reaction (DHTR) due to an antibody (with poor haemoglobin (Hb) increment, jaundice and renal failure) but if clinical harm to patients from withholding blood outweighs these, then emergency blood is essential and should be offered. Patients should not die from lack of blood
– If antibody investigations have not been completed, or the patient has known antibodies for which compatible blood is not readily available:
• ABO-, full Rh- and K-matched blood may be given, with intravenous (IV) methylprednisolone 1g and/or IV immunoglobulin (Ig) cover if required
• Discuss with a clinical haematologist regarding the need for IV methylprednisolone and/or IVIg and monitoring for DHTR (including urine output), in light of any alloantibodies subsequently identified, and if any incompatible blood has been transfused
• If full Rh and K phenotypes are not known, give ABO- and D-matched blood, with cover as above; if ABO and D groups not known, give O D-negative blood (or O D-positive blood may be given to males and post-menopausal women) with cover as above
For further key messages on delays in massive haemorrhage, see SHOT Bite No. 8 www.shotuk.org/resources/current-resources/.
Delays are often additive since there are several points in the transfusion pathway where there may be hold-ups. These are illustrated in Figure 11a.4.
Delayed Transfusion n=9511a

83
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
11a. Delayed Transfusion
Overview
Delayed transfusion was reported for 95 patients, age range newborn to 100 years (median age 30 years); 49 were female and 45 male (1 not specified). There was 1 near miss delay related to laboratory testing.
2
12
21
34
50
94101
95
2010 2011 2012 2013 2014 2015 2016 2017
Figure11a.2: Figure 11a.3: Location of emergency and
Urgency of delayed transfusions n=95 urgent transfusions n=56
16
23
56
Unknown
Routine
Urgent or emergency
2
4
11
11
28
Unknown
Obstetrics
ED/MAU
Ward
Theatres and ITU
ED=emergency department; MAU=medical admissions unit; ITU=intensive therapy unit (all types)
Figure 11a.1:
Delayed transfusion
reports by year
2010-2017

84
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
11a. Delayed Transfusion
Haemorrhage call
Blood samples to laboratory Transport of components to patient
Recognition of bleeding
Communication between clinical area and laboratory
Laboratory – grouping, antibody screen,
prepares and issues components
Components received and
transfused – poor venous access
Logistics:Porter availability
Distance
Logistics:Porter availability
Distance
Deaths n=6
Overall 14 deaths were reported. One death was directly attributable to the delay. Three deaths probably resulted from delayed transfusion and in 2 there was a possible relationship. Eight deaths were not thought to be related to the delay in transfusion.
Imputability
Transfusion priority Definite Probable Possible Unrelated Total
Emergency 0 2 1 4 7
Urgent 1 0 1 2 4
Routine 0 1 0 0 1
Unknown 0 0 0 2 2
Total 1 3 2 8 14
Death definitely related to delay n=1
Case 11a.1: Death as a result of delayed transfusion for autoimmune haemolytic anaemia
A man in his 60s presented with Hb 38g/L secondary to autoimmune haemolytic anaemia (AIHA). The hospital laboratory referred the sample to an external reference laboratory (2 hours away) for further analysis due to the presence of a strong pan-reactive autoantibody. The patient died before the results were issued and without receiving any red cells. There had been an opportunity for a group and screen (G&S) sample to be sent a day earlier when the patient first presented. It was noted that there was no haematology consultant on site overseeing the patient’s care out-of-hours due to centralisation of specialist services.
A G&S sample should have been sent at the earliest opportunity in anticipation of difficulties that would be encountered with full serological compatibility testing in a patient with AIHA. AIHA is caused by an autoantibody which reacts against non-specific red cell antigens. The presence of a pan-reactive autoantibody can mask additional alloimmune antibodies and therefore extended (and time-consuming) testing is required to exclude or identify these.
The mainstay of treatment for AIHA is immune suppression avoiding transfusion unless absolutely necessary. In cases with life-threatening anaemia blood transfusion is necessary and may be lifesaving. The primary risk of transfusing a patient without the results of an alloantibody panel would be the potential for a haemolytic transfusion reaction if a clinically significant alloantibody is present. When
Figure 11a.4:
Potential hold-
up points in
the transfusion
pathway
Table 11a.1:
Relationship
of transfusion
priority to deaths
in delayed
transfusions

85
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
11a. Delayed Transfusion
anaemia is life-threatening, transfusion with ABO-, full Rh- and K-matched blood is more appropriate than delaying until full serological investigations have been completed (BSH Hill et al. 2017). Incompatible red cells may be transfused where the anaemia is life-threatening. Alert the transfusion laboratory staff early when transfusion may be required for patients with irregular antibodies. Where incompatible red cells are transfused, monitor the patient carefully, including renal function and urine output, and consider use of IVIg (see also Chapter 19, Haemolytic Transfusion Reactions (HTR), 3 cases).
Deaths probably related to delay n=3
Case 11a.2: Delayed transfusion contributes to death from haematemesis
A non-English-speaking man in his 40s with a history of alcohol dependence, hepatitis C and substance misuse (on a methadone programme) attended the ED with haematemesis after a 999 call by his friends at 03:20. The patient was not triaged appropriately (ambulance records of vomiting blood, pulse 130 beats per minute (bpm), blood pressure (BP) 94/60mm Hg) and his clinical state was not monitored adequately in accordance with hospital guidelines (no hourly observations and no early warning score monitoring). He should have been seen within 10 minutes but was seen after 1.5 hours. At 04:28 the Hb was 56g/L. The laboratory contacted the ED to report this result and later at 05:45 to offer emergency O D-negative blood. This advice was declined and fully crossmatched red cells were requested at 05:09 with ‘routine’ priority. The patient’s clinical deterioration was not detected by nursing or clinical staff. The major haemorrhage protocol (MHP) was not activated.
The patient died at 08:06 following cardiac arrest with further large haematemesis and melaena prior to receiving any blood components.
Poor clinical judgement by both nursing and medical staff was noted with failure to recognise the severity of the patient’s clinical state and failure to activate the MHP. These contributed to the death of the patient. Hospital procedures were not followed and it was noted on review that both the doctor and nurse involved in the case were agency staff (3/7 nurses were agency staff) and therefore not required to attend mandatory training. The medical and nursing shifts changed over at 07:00 so that the patient was seen by a succession of different staff. The case review resulted in improved arrangements for orientation for agency staff to ensure that the correct triage procedures are followed.
Case 11a.3: Delayed transfusion for severe anaemia related to gastrointestinal (GI) haemorrhage contributes to death
A man in his 70s presented with a 2-day history of bilateral leg pain and was found to have a Hb of 49g/L at 08:00. He had multiple comorbidities including a history of angiodysplasia and ischaemic heart disease with multiple stents with atrial fibrillation for which he was on aspirin and rivaroxaban. Blood was requested (although the first sample was rejected due to incorrect date of birth) and available for collection at 11:49. The plan (at 13:54) was to transfuse to Hb >90g/L cautiously given a high risk of transfusion-associated circulatory overload (TACO).
However, the patient was not transfused until the following day, when found unresponsive with an unrecordable BP, metabolic acidosis and Hb 34g/L. He was transfused four units of red cells (post-transfusion Hb 73g/L) and three units of fresh frozen plasma (FFP) (international normalised ratio (INR) >2.5) and admitted to the ITU. The patient died 24 hours after admission from cardiogenic shock related to profound anaemia in the context of cardiomyopathy.
There was a delay of more than 18 hours from the decision to transfuse. The incident report noted that there were concerns about transfusing the patient while in transit between wards and transfusing overnight but there was also evidence of poor handover at several points and excessive workload for junior doctors leading to lack of clinical review and documentation overnight. Concerns regarding TACO were valid but should have been overcome with close monitoring and use of diuretics if required. It was also noted in the case review that pressures to meet waiting targets in the ED may have led to an initial delay. It may have been appropriate for the patient to have received part of the planned transfusion prior to moving to the medical ward, regardless of targets. There were several recommendations for change in practice as a result including transfer checklist from ED to ward, teaching on transfusion to medical and nursing staff, a review of overnight medical cover and the importance of good handover.

86
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
11a. Delayed Transfusion
Learning point
• A patient should not die from anaemia. The guidance to not transfuse at night has been translated into a rule which it is not. Patients may need urgent transfusion at any time in 24 hours and this should not be delayed
Case 11a.4: Access to the laboratory refrigerator contributed to delay in provision of emergency blood
A man in his 60s, managed on ITU for ongoing variceal bleeding, deteriorated acutely with a further massive haemorrhage. Two units were issued at 02:56, the first was collected at 03:31. He became unstable with resistance to fluids and two units of red cells. The MHP was activated at 03:38; units were available by 03:47 but it took 36 minutes for further red cell units to reach the ward. The patient was profoundly hypotensive throughout this period and was not suitable for resuscitation by the time the blood components arrived.
Several problems contributed to the delay: a reduced number of porters, distance and problems with the issue refrigerator. The main issue refrigerator was awaiting repair and the blood was stored in another refrigerator in the laboratory requiring additional steps to access blood that would not have occurred if the main issue refrigerator was in operation. The procedural review recommended an increase in porters and giving them access codes for the laboratory. A designated cool box was made available for immediate collection. The review also noted that there was delay in implementation of barcoded identification bands due to funding issues.
Death possibly related to delay n=2
Case 11a.5: Failure to follow MHP correctly contributes to delay and death
A man in his 80s was admitted to the ED with massive haemorrhage (no further details). The MHP was activated. Emergency O D-negative units and pre-thawed FFP were available and issued for use by the laboratory in a timely manner. The blood components were available to collect but the clinical staff were not aware of this and another doctor contacted the laboratory 20 minutes after the components had been issued. The patient was then transferred to the radiology department but the components were delivered to the ED. The patient died the same day.
Poor communication and lack of understanding of the MHP led to delays in transfusion that possibly contributed to this patient’s death. MHP drills and retraining have been implemented in the ED as a result of this incident. In a second case suboptimal communication between laboratory and clinical staff led to a 2-hour delay in transfusion after activation of the MHP in association with the laboratory information management system being down for a long period.
Major morbidity n=1
In 1 case delayed transfusion was a contributory factor to major morbidity.
Case 11a.6: Delayed transfusion in a patient with cardiac ischaemia contributes to major morbidity
A man in his 50s was admitted from the endoscopy unit with chest pain confirmed due to non-ST-elevation myocardial infarction (NSTEMI). The Hb was 43g/L at 10:45 (he had a previous history of GI bleeding). At 13:37 red cells were available for collection but were not transfused until 16:25. The reason for the delay is unclear, although there was likely inadequate communication as a contributory factor. The patient was admitted to ITU and made a full recovery.
It is uncertain whether failure to recognise the severity of the patient’s condition, or lack of clarity as to the urgency of transfusion, caused the delay in this case. Patients with cardiac chest pain should have their anaemia managed as a matter of urgency.

87
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
11a. Delayed Transfusion
In the following case a patient was put at risk of serious harm due to delay.
Case 11a.7: Delayed transfusion in a patient with chest pain due to lack of knowledge about how to manage critical anaemia in the presence of pan-reactive antibodies
A woman in her 50s with chronic significant gynaecological haemorrhage was admitted from clinic with Hb 56g/L at 16:00. She was clinically stable. A G&S sample was not sent until 08:58 the following morning. She was found to have a pan-reactive antibody which required further testing and the sample was sent to the local external reference laboratory. At 14:00 the patient became acutely unwell with crushing central chest pain and a respiratory rate >40 breaths per minute (/min), thought to be secondary to cardiac ischaemia. A repeat blood count showed Hb 46g/L. Blood was not available until 17:00, 3 hours after the development of cardiac symptoms.
This case demonstrates several areas for improvement. There should not have been a lengthy delay sending transfusion samples, particularly in a patient considered high enough risk to warrant inpatient admission. There was failure to communicate the change in the patient’s clinical status, and urgency of blood requirement, to the laboratory. The sample had been sent to the reference laboratory as a ‘routine’ case as had the delivery of blood components ‘when available’. This is another instance where the patient could have received ABO group-specific, full Rh- and K-matched red cells when it became apparent there was going to be delay. The risk of leaving a severely anaemic patient with cardiac chest pain is likely higher than the risk of transfusing blood with a potential alloantibody.
Delays involving the management of MHP n=19
Poor communication was a common cause of delays. There were logistical issues in notifying laboratories of activation of the MHP in 5 cases and 4 further cases in which porters were not alerted. It is essential that there are dedicated lines of communication to the transfusion laboratory and that porters are included in the alert and updated as to any changes in patient location (Case 11a.5 above: death possibly related to delay).
Case 11a.8: Wrong patient details supplied to laboratory in a major obstetric haemorrhage
A woman in her 20s had a postpartum haemorrhage leading to MHP activation. The midwife gave the wrong patient details to the laboratory staff which was not recognised until the red cells (incompatible ABO group) arrived in the maternity unit. They were returned and correct details applied but this resulted in a 25-minute delay to provision for the group O patient.
The review noted that this was an unusually busy evening with complicated cases causing demands of the staff and service. The error was detected because of correct checking processes prior to transfusion.
Case 11a.9: Lack of knowledge about emergency blood provision in patients with alloantibodies leads to delayed transfusion
A man in his 50s with variceal haemorrhage related to alcoholic liver disease was admitted to the ED. A MHP call was instigated at 01:40. The patient had alloantibodies, anti-K and anti-Cw. The biomedical scientist (BMS) was reluctant to issue the shock pack (four units of red cells and four of FFP) and informed the ED not to use the emergency O D-negative blood in the local refrigerator. A consultant haematologist was contacted 25 minutes after the MHP call and authorised the transfusion. Blood was collected at 02:16. The patient was admitted to ITU and eventually made a full recovery.
An unnecessary delay in issuing emergency blood components resulted from a lack of knowledge by the BMS, who was working alone at night, and failure to follow the standard operating procedure (SOP) for patients with known irregular antibodies (to issue group O K-negative units and immediately contact the haematologist on call).

88
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
11a. Delayed Transfusion
Case 11a.10: Change in status of the patient and poor communication compound the delay
A young man was admitted with trauma from a road traffic accident with closing speed of 70 miles per hour. He was initially stable; four units of blood were requested urgently to be available at 18:55. The BMS acknowledged that these would be available in 10 minutes. However, the blood sample was not taken until 19:00, was booked into the laboratory at 19:20 but had to be reprocessed at 19:47 as the antibody screen had not been done. During computerised tomography (CT) scanning the patient started to deteriorate with an increase in pulse rate to 135 beats/min such that the internal bleeding was now thought to be greater than it seemed at first.
A porter was sent to collect the blood and a telephone request was made for platelets and plasma as indicated by thromboelastogram (TEG) testing. Although there was an agreed TEG protocol in place for a 1:1 red cells to plasma ratio the BMS noted that this request would require authorisation by the haematology registrar (as this had not triggered the MHP). The BMS did not inform the ED staff that there had been a problem with the antibody screen. The MHP was called at 20:37 when blood and plasma were issued and collected. Plasma was infused at 21:15 and platelets at 22:15. The ED staff could have used the emergency O D-negative units.
This case demonstrates that it may be difficult to determine the severity of bleeding in closed injuries. If there is a change in urgency for blood component delivery this should be clearly communicated to the transfusion laboratory staff; the BMS is likely to have had several actions in progress and will need to know if the priority has changed. It would be normal practice to require haematology authorisation for platelets requests but not once the MHP has been activated. The outcome of the case was to ensure that communication between the ED and transfusion laboratory is clear and concise.
Case 11a.11: Telephone check prior to high risk surgery detects failure of process
A woman was scheduled for elective caesarean section for placenta praevia; blood samples were sent for group and crossmatch four units of red cells 2 days prior to the procedure. At the time of surgery, after the spinal anaesthetic had been placed, a telephone call to the laboratory established that no units were available due to a laboratory error in processing the request. The request form had been put in the wrong location for crossmatch requests at the time of a shift changeover. The four units were made available within 40 minutes. The start of surgery was delayed but the red cells were not used.
Preparation for surgery where blood loss is high risk requires red cells to be available at the time of surgery. It was fortunate that the staff chose to check prior to starting the surgery in this case.
Information technology (IT)-related delayed transfusions n=11
Equipment failure n=2
In one case the printers failed and then blood components issued manually were returned due to a transcription error. In another the MHP was not correctly activated because the bleeps do not work throughout the hospital.
Electronic blood management systems (EBMS) n=7
In all 7 cases blood could not be accessed from a satellite refrigerator under the control of an electronic blood management system and this caused delay in 6 emergencies and 1 urgent clinical situation.
Case 11a.12: Refrigerator incorrectly stocked for remote electronic issue (EI)
Two high-risk cases, both blood group A, were anticipated to require significant amounts of blood during surgery. The group A drawer of a remote electronic issue refrigerator was full so additional units were put in the ‘crossmatched blood’ drawer. As expected the group A blood was rapidly depleted and the clinicians were warned by the EBMS that the supplies were low. However, the BMS viewing the stocks remotely could see that there were plenty of group A units remaining. These were not available for remote electronic issue and had to be issued from the laboratory.

89
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
11a. Delayed Transfusion
In two critical situations where blood was required immediately, the clinical staff removing blood from the satellite refrigerator did so incorrectly. In one case all the units were scanned out at the same time and became ‘invalid’ for use so had to be reissued from the laboratory causing delay. On the other occasion neonatal emergency blood was required. The first collector used the wrong programme so a second trained operator removed the blood correctly but left the refrigerator drawer and door open. The process was therefore incomplete and no further blood could be safely removed without intervention from the laboratory.
In two other cases blood was not available because the refrigerator locked closed. This was as a result of a motherboard failure in one and because the screen froze on the kiosk in another. Downtime procedures were available, but were not always followed immediately.
Training is essential for all EBMS operation and training against routine and emergency procedures could have prevented all the cases mentioned above. Training is particularly important during implementation of a new system and when new staff join the organisation. There was one delay because porters did not have the necessary barcodes to collect blood and another because there were both new and old systems in place during a transition to an EBMS and the completion of two collection processes caused unacceptable delay.
Others n=2
In one case a laboratory information management system (LIMS) flag stating the need for a serological crossmatch was not heeded.
In another case there was a delay to transfusion, and to transfer to a specialist unit, because methylene-blue-treated FFP could not be issued to a neonate. The component choice (and component code) had not been set up on the LIMS so this had to be issued manually.
References
Bolton-Maggs PHB, Poles D et al. on behalf of the SHOT Steering Group. The 2014 Annual SHOT Report (2015) www.shotuk.org pages 26-27.
BSH Hill Q A, Stamps R et al. Guidelines on the management of drug-induced immune and secondary autoimmune, haemolytic anaemia. Br J Haematol 2017;177(2): 208-220.

90
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
11b. Avoidable Transfusion
Definition:
Where the intended transfusion is carried out, the blood/blood component is suitable for transfusion and compatible with the patient, but where the decision leading to the transfusion is flawed. This includes transfusions based on poor knowledge, communication failures, incorrect decisions or poor prescribing.
In addition to the total above, 2 delayed transfusions resulted in inappropriate use of O D-negative units and 1 case of undertransfusion was a result of transfusion of a low volume of FFP that was also inappropriate (not indicated for reversal of rivaroxaban). These are counted in their own sections (giving an overall total of 104). Two avoidable infusions of PCC are included in the PCC section.
Overview
No serious harm was known to have occurred as a result of avoidable transfusion, although there was one episode of probable transfusion-associated circulatory overload (TACO) reported in association with an avoidable transfusion and additionally reported in TACO. Four deaths occurred in this group, none of which were related to the transfusion.
Sample errors n=29
Blood component prescriptions based on the wrong blood results accounted for a third of avoidable transfusions.
Error Number of cases
Result from another patient used 8
Dilute sample (drip arm) 5
Clotted sample 2
Transcription error 2
Historical results reviewed 3
Erroneous near-patient-testing results 1
Other 6
Laboratory error: platelet clumps 1
Erroneous platelet count from WBIT 1
Total 29
WBIT=wrong blood in tube
Case 11b.1: WBIT with failure to verify unexpected results
A nursing home resident in her 70s was reviewed in the community. A blood sample taken by the general practitioner (GP) showed a platelet count of 6x109/L with a white cell count of 1.98x109/L. She was admitted to hospital later that day for a platelet transfusion. Blood sampling was repeated on arrival to hospital prior to transfusion; the platelet count was 186x109/L and white blood count was 11.7x109/L. These results were not reviewed by the admitting doctor and a unit of platelets was prescribed and administered. The error was detected by laboratory staff.
Table 11b.1:
Causes of wrong
blood results n=29
Avoidable Transfusion n=10111b

91
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
11b. Avoidable Transfusion
This primary error in blood sampling caused unnecessary admission to hospital for an elderly patient and exposure to a blood component that was not indicated. However, a series of events contributed to this outcome. Firstly, the report noted that the sample was taken from another patient in the nursing home. Initial patient identification, if performed correctly, would have prevented this. The results should then have been reviewed by the GP and admitting doctors. If these results were unexpected, based on the patient’s symptoms and previous trends (if available), then investigation into the abnormal results is required. This should include consideration of an erroneous result and thorough clinical investigation. This should occur prior to transfusion unless the patient is at high risk due to significant active bleeding. In this case a repeat sample was requested and a normal platelet count demonstrated. There was failure to review the most contemporaneous results prior to authorising a transfusion. There were at least four errors in procedure.
Case 11b.2: Poor management leads to excessive transfusion
An elderly man required a revision hip replacement (40-year-old prosthesis). At preoperative assessment a week before surgery his Hb was 127g/L. He bled during the technically difficult and long procedure (about 5 hours) and received six units of red cells before the Hb was checked and found to be 170g/L.
The review noted reliance on estimated blood loss as an indicator for transfusion, an ‘I know best’ attitude and a loss of situational awareness. Preoperative preparation was suboptimal. The patient did not have an arterial line nor central venous access and was lying on his side for the surgery which meant that only one arm was accessible for blood sampling.
Inappropriate management of haematinic deficiency n=10
There were 8 cases where patients with iron deficiency anaemia were treated inappropriately with blood transfusion. A further case was identified in the overtransfusion category (Case 11c.4). One patient was transfused for folate deficiency and 1 for B12 deficiency.
Case 11b.3: Inappropriate transfusion in a patient with iron deficiency and failure to check response to transfusion
A woman in her 50s with iron deficiency anaemia and Hb of 57g/L presented with fatigue as her only symptom. She weighed 54kg and was prescribed a five-unit red cell transfusion by a junior doctor. All five units were transfused with a repeat full blood count (FBC) only checked after the fifth unit had been given. The post-transfusion Hb was 131g/L.
This patient was exposed to risks of transfusion, and in particular TACO, due to an unnecessary transfusion that was also inadequately monitored. Given that this patient was relatively asymptomatic with no cardiovascular risk factors, a more considered approach may have been to transfuse one unit of red cells at most, with repeat clinical assessment afterwards. A course of oral or intravenous iron would be appropriate management.
Investigation into to the underlying cause of iron deficiency is also required.
Case 11b.4: Perioperative transfusion of red cells due to failure to manage iron deficiency anaemia preoperatively
A man in his 70s was found to be iron deficient 6 months prior to an elective abdominal aortic aneurysm repair (AAA). The iron deficiency was not managed adequately. Preoperatively, the Hb was 106g/L but it was felt that surgery could not be deferred. The Hb fell to 83g/L following the procedure and four units of red cells were transfused.
Preoperative anaemia is associated with increased postoperative morbidity and mortality, and increased transfusion needs. National Institute for Health and Care Excellence (NICE) guidelines on blood transfusion recommend treating iron deficiency with iron supplements (NICE 2015). Hospitals should design pathways to manage these patients effectively.

92
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
11b. Avoidable Transfusion
Potentially avoidable use of emergency O D-negative units n=17
Seventeen cases have been identified when emergency O D-negative units were issued inappropriately. Five emergency or urgent transfusions were in the ED, 2 in the delivery ward, and 2 in theatre. Other locations included the medical admissions unit and wards. Two additional cases are included where delays resulted in inappropriate use; in both instances there was delayed provision of crossmatched red cells due to an earlier error with pre-transfusion compatibility testing. This is a waste of a precious resource and moreover, O D-negative red cells are unsuitable and potentially unsafe for certain patients, e.g. those with anti-c antibodies.
Avoidable use of emergency O D-negative units Number of cases
O D-negative used when crossmatched available 4*
O D-negative used when group-specific available 1
Delayed provision of correct components due to earlier error 9
O D-negative blood used in non-emergency scenario 3
Total 17
*In 1 case EI could have been used to issue crossmatched units if historical records had been checked
In 9 cases, emergency O D-negative red cells were issued because of earlier errors. These included: labelling errors (n=2), failure to notify the laboratory to convert group and screen to a crossmatch request (n=1), samples misplaced in laboratory (n=2), delays sending samples to the laboratory (n=3), failure of laboratory staff to check if EI was appropriate (n=2) resulting in delays due to unnecessary requests for repeat sample testing, and delays in processing samples that were not required. In some cases, more than one error occurred.
Case 11b.5: Delayed provision of red cells for postpartum haemorrhage caused by miscommunication by the clinical team and failure to check sample validity in the laboratory
A young woman had an estimated 3.6L blood loss from a vascular tear following vacuum-assisted vaginal delivery at 07:45. A valid sample was available for EI from the previous day. Two litres of fluid were infused and another transfusion sample was sent to the laboratory at 08:00 with a request for two units of red cells to be crossmatched. The urgency of the request was not conveyed to the laboratory. The laboratory staff then failed to check for sample availability and therefore unnecessarily processed the new sample. This caused additional delay, preventing EI from the existing sample. Crossmatched blood was issued at 09:22 after one unit of emergency O D-negative blood had been transfused at 08:30.
Clear communication is vital. It is essential to inform the laboratory when blood is required urgently. The laboratory should check for availability of a valid sample. In this case group-specific blood could have been issued.
Inappropriate transfusion of FFP n=6; given to reverse anticoagulant effect n=3
FFP was given inappropriately to three patients to reverse anticoagulant effect. One woman in her 70s on warfarin with INR 3.7 developed a rectus sheath haematoma. PCC should be used in emergencies to reverse warfarin together with vitamin K. There is no role for FFP. Two patients were anticoagulated with rivaroxaban, and while there is as yet no licensed reversal agent current guidelines recommend the use of PCC in emergency situations. In one of these cases, the dose of FFP was also inadequate (counted in the undertransfusion category) and would have had little therapeutic benefit even in an appropriate situation.
Case 11b.6: Unexpected severely abnormal results should be checked prior to release by the laboratory
A man with alcoholic liver disease undergoing surgery was reported to have INR >11 with an abnormal fibrinogen result and was transfused FFP and cryoprecipitate on the basis of this result which should have been repeated by the laboratory.
Table 11b.2:
Reasons for use
of emergency O
D-negative units

93
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
11b. Avoidable Transfusion
Learning point
• Laboratory staff should not issue results which they know or suspect to be unreliable or incorrect
Case 11b.7: Avoidable transfusion of FFP associated with poor communication and the distance of surgical treatment centre from transfusion laboratory
A patient at a local treatment centre (TC) (12 miles away) was bleeding following emergency evacuation of a haematoma two weeks following a hip replacement. This emergency surgery took place at a weekend. The patient required four units of group O D-negative red cells. There was no group and screen sample at the main hospital as the procedure was considered low risk for bleeding (the TC keeps O D-negative red cells as stock).
At 12:00 a request for FFP was referred to the on-call consultant haematologist who advised that due to the clinical situation and distance two units of plasma should be thawed and sent. He also requested that FBC and clotting samples were taken as soon as possible, but there was a significant delay in taking these samples. At 14:00 the consultant haematologist was contacted by the anaesthetist to inform him that the patient was in recovery, and was now ‘haemodynamically stable’ although hypotensive with a tachycardia. Four units of red cells had been transfused. The haematologist advised that given this information and in the absence of the clotting results that the previously authorised FFP be transfused. At 15:30 the clotting results (all parameters within normal limits) were telephoned to the haematologist but not conveyed to the TC. Although no further red cells were transfused two units of FFP were transfused, at 17:30 and 18:00, despite the patient being stable and 2 hours after clotting results were available showing normal parameters.
This was the first occasion that staff at the TC had to manage a major bleed (pathology services supplied offsite since 2012) and resulted in review and revision of their major haemorrhage protocols to include management of major haemorrhage at a site which is 12 miles away from the supplying transfusion laboratory. There may be more issues similar to this with the proposed centralisation of pathology services in an expanded number of hub and spoke models.
Inappropriate transfusion of platelets n=15: make a diagnosis before ordering platelets
Platelets were issued on the basis of erroneous results n=6: 2/6 as result of WBIT, 3/6 due to platelet clumping, 1/6 cause unknown.
One patient received platelets for a low platelet count that was later diagnosed to be due to thrombotic thrombocytopenic purpura (TTP). This is a thrombotic condition in which platelet transfusions are contraindicated except for life-threatening bleeding as they may increase the risk of thrombosis. This illustrates the importance of establishing the cause of thrombocytopenia prior to transfusion. Early review of a blood film is essential for assessment of unexpected thrombocytopenia and may have established this diagnosis (fragmented red cells are characteristic) and prevented potentially dangerous transfusion. The diagnosis of TTP is urgent, and patients should be started on plasma exchange as soon as possible, and platelet transfusion avoided.
Platelets were transfused inappropriately when not indicated prior to procedures, in excess quantity for the procedures undertaken, and prior to procedures that were subsequently cancelled.
There were 2 cases in which patients were transfused platelets inappropriately in order to achieve a count of >50x109/L prior to insertion of a nasogastric tube. This is not in accordance with British Society for Haematology (BSH) guidelines on the use of platelet transfusions (BSH Estcourt et al. 2017).
Case 11b.8: Excessive platelets requested to cover a procedure that was subsequently cancelled
A patient with myelofibrosis and a chronically low platelet count was due to undergo a liver biopsy. The platelet count was stable at around 40x109/L. Six units of platelets were requested to cover the procedure by a consultant haematologist. Two units were transfused prior to the procedure,

94
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
11b. Avoidable Transfusion
which was subsequently cancelled, following concerns raised by a junior doctor and interventional radiologist who had not been consulted in advance and considered the procedure too risky. The laboratory staff had also raised concerns regarding this request. There was a comment made in relation to this event, that due to the culture at the hospital, laboratory staff did not feel empowered to act further.
Platelets are a valuable resource that should be used judiciously and in accordance with national guidelines. It is important that hospitals have policies to guide the use of platelets and that all members of staff, including the laboratory team, are empowered to raise concerns in a culture of openness. An adult treatment dose is a single bag of platelets.
Learning point
• Thrombocytopenia has several causes, many of which are not best managed by platelet transfusions. It is important to make a diagnosis as platelet transfusion may be contraindicated. Unexpected thrombocytopenia should always prompt film examination and, if necessary, confirmation on a repeat sample
IT-related avoidable transfusions n=5
Transfused on the wrong result n=5
Two patients were transfused because of an incorrect Hemocue™ result and one following a series of incorrect Hb levels on a blood gas analyser. In another patient a WBIT led to a platelet transfusion but the previous FBC result could not be checked because of computer downtime. The wrong (old) Hb result was used to initiate transfusion rather than the current (higher) Hb because the electronic patient record (EPR) results screen did not default to the current result.
Commentary
All the examples reported here are similar to previous years. It is important that clinical staff understand the rationale and indications for any blood component transfusion and ensure that there is no alternative. A novel approach has been taken in one district general hospital. The transfusion prescription is a comprehensive folded document which includes prescribing codes for red cells, platelets, FFP and cryoprecipitate. This was introduced in May 2017; nursing staff were trained not to proceed without a code, and if none was applicable to contact a haematologist. Audit demonstrated a 16.2% reduction in red cell use (McGrann 2018).
References
BSH Estcourt L J, Birchall J et al. Guidelines for the use of platelet transfusions. Br J Haematol 2017;176(3):365-394.
McGrann A. Reducing red cell use by 16% by mandating an indication code derived from NICE guidance and the NBTC’s transfusion audit codes on every blood prescription in a large District General Hospital. Br J Haematol 2018;181 Suppl 1:34.
NICE. Guideline NG24 Blood transfusion 2015 https://www.nice.org.uk/guidance/ng24/chapter/Recommendations#alternatives-to-blood-transfusion-for-patients-having-surgery-2 [accessed 18 March 2018].

95
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
11c. Under or Overtransfusion
A similar number of errors of transfusion volume were reported as in 2016 (n=21). There were 2 deaths where these errors were contributory, and several mistakes were made for transfusions in children. These cases are reported in Chapter 22, Paediatric Summary.
Undertransfusion n=5
Death probably related to undertransfusion n=1
Case 11c.1: Undertransfusion in a patient with GI bleeding probably contributes to death
A man in his 50s presented with postural hypotension. It was not initially recognised to be secondary to GI bleeding as initially he was physiologically well-compensated. On decompensation it came apparent that he had had a significant GI bleed. Two units of red cells were transfused but the patient died and was probably under filled.
Prompt recognition of bleeding is essential but this can sometimes be difficult due to the large volume of blood that can be concealed intra abdominally. Regular clinical monitoring is required when there is a suspicion of GI bleeding. Once confirmed, activation of the MHP with use of adjuncts such as tranexamic acid may help stabilise patients while the underlying cause is detected and treated.
Overtransfusion n=19
Death possibly related to overtransfusion n=1
Case 11c.2: Failure to check response to transfusion led to overtransfusion and possibly contributed to a poor outcome
A man in his 70s had a cardiac arrest, while in a CT scanner, following an endovascular aneurysm repair (EVAR). The arrest was thought to be secondary to major haemorrhage and the MHP was initiated. Four units of red cells and two units of FFP were transfused. The pre-transfusion Hb was 154g/L. No repeat FBC was taken before transfusing a further four units of red cells. The post-transfusion Hb was 269g/L. The patient required venesection but subsequently died.
This was a complex case and it was noted in the procedural review that the patient had to be moved several times during the course of resuscitation. This may have contributed to the failure to reassess transfusion requirements with repeat blood tests. Nonetheless, it is crucial to monitor response and the need for ongoing blood components.
There were several other cases reported including Case 11c.4 below, in which overtransfusion occurred as a result of inadequate clinical evaluation prior to giving further blood components.
Major morbidity n=1
Case 11c.3: Inadequate clinical monitoring leads to overtransfusion and contributes to intensive care admission
A woman in her 70s was admitted with a chest infection and Hb 66g/L due to suspected myelodysplastic syndrome (MDS). She also had a history of chronic obstructive pulmonary disease and ischaemic heart disease. A chest X-ray (CXR) on admission suggested a left lower respiratory infection. Four units of red cells were given over a 9-hour period; unit one was given over 60 minutes, units two and three over 90 minutes and unit four over 120 minutes. There was no recorded clinical
Under or Overtransfusion n=24 11c

96
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
11c. Under or Overtransfusion
review or repeat Hb between the units. The patient deteriorated and required admission to intensive care for ventilator support. Case review by respiratory and ITU consultants with the post-transfusion CXR concluded this was primarily left lobar pneumonia and not TACO.
Failure to adequately monitor clinical response to transfusion is a recurring issue. Particular care should be taken in patients at high risk of overload including patients with ischaemic heart disease. The TACO checklist is a useful prompt (Chapter 18b, Transfusion-Associated Circulatory Overload (TACO)).
Case 11c.4: Inadequate monitoring and overtransfusion for iron deficiency in a patient with low body weight
A woman in her 40s was admitted with severe iron deficiency and Hb 28g/L. She weighed 33.4kg and was haemodynamically stable. Over the course of 3 days she received nine units of blood. A FBC was not repeated until all units had been given at which point the Hb was 171g/L.
Several errors were made in this case which led to unnecessary inpatient stay and exposure to blood components:
• Failure to check response of Hb level following each unit
• Overtransfusion in respect of underlying cause. Given the severity of anaemia in this case, initial transfusion of one to two units was reasonable but the mainstay of treatment should have been iron supplementation
• Low body weight not taken into account when considering volume requirement
Case 11c.5: Miscommunication and failure to challenge an unusual order leads to massive overtransfusion of cryoprecipitate
A man in his 70s was admitted with a stroke requiring thrombolysis. He later deteriorated with suspected (intracranial?) haemorrhage. The on-call haematology registrar advised cryoprecipitate if the fibrinogen level was less than 1.5g/L. Ten units of cryoprecipitate were requested and transfused.
There was either miscommunication or misunderstanding between the on-call haematologist and the medical middle grade doctor. Two units of cryoprecipitate, each made of five donor pools, is the correct dose. The patient was given five times this. There were missed opportunities for this dose to be questioned, by the BMS particularly, but also the nursing staff.
Over and undertransfusion in paediatric patients n=14/24 (58.3%)
Thirteen of 19 cases of overtransfusion and 1/5 cases of undertransfusion occurred in paediatric patients. These are described in Chapter 22, Paediatric Summary.
Learning point
• Junior staff working in paediatrics require training in blood component prescribing to avoid potentially dangerous errors. Components should be prescribed in mL. This is particularly important for trainees who rotate from adult medicine. These errors are reported every year. Paediatric guidelines for transfusion should be readily available in all paediatric areas as recommended in recent guidelines (BSH New et al. 2016)
Errors related to transfusion pumps n=4
There were 4 errors related to improper transfusion pump setup. Incorrect setting of the rate led to overtransfusion in 3 cases, all of which occurred in paediatric patients. A case of undertransfusion in an adult occurred due to pump failure and was only noticed after 4 hours. Vigilance is needed, particularly in respect to checking rates and volumes administered to paediatric patients where inaccuracies can have significant consequences due to small circulating volumes.
ReferenceBSH New HV, Berryman J et al. Guidelines on transfusion for fetuses, neonates and older children. Br J Haematol 2016;175(5):784-828.

97
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
11d. Incidents Related to Prothrombin Complex Concentrate (PCC)
A small number of errors in relation to PCC were reported as shown below. These resulted from poor knowledge, inappropriate ‘rules’ and careless errors.
Learning point
• Guidelines relating to anticoagulant reversal can be followed but must take into account the precise clinical circumstances (Case 11d.2, prothrombin complex concentrate)
Case 11d.1: PCC algorithms should state maximum dosage
A woman in her 40s, weight 138kg, with a retroperitoneal haematoma was prescribed (by a foundation year 2 doctor) and given a PCC dose in the ED based on her weight (4140 units) which exceeded the maximum recommended dose of 3000 units for that particular PCC. This resulted in revision of the PCC algorithm to add the maximum dose and a notice was added to the refrigerator in transfusion to ensure more than the maximum dose could not be issued.
Case 11d.2: Guidelines are not rules
A woman in her 70s who was very unwell with INR 1.3 required an urgent laparotomy for bowel resection. She was on warfarin for atrial fibrillation and had a previous pulmonary embolism. She had initial surgery some days earlier and had been restarted on warfarin. The consultant anaesthetist refused to take her to theatre without PCC; 500 units were authorised by a consultant haematologist. This was against hospital and anaesthetic policy for the management of INR results.
The anaesthetist reported that the plan was to use epidural anaesthesia, which has a higher risk of vertebral canal haematoma, and that since she had recently restarted warfarin the INR was likely to be rising. The operation could not be delayed. The Association of Anaesthetists of Great Britain and Ireland (AAGBI) guidelines (AAGBI 2013) for neuraxial blockade recommend that an INR of <1.5 should be considered safe in a patient with normal risk but notes also that guidelines need to be interpreted for a given clinical situation, so he felt the decision to use PCC was justified.
Learning point
• Guidelines are not rules and should not be oversimplified. Clinical circumstances may overrule the guidance due to other factors which need to be taken into account, and recorded in the case notes. This is resilience
Case 11d.3: FFP should not be used to reverse warfarin
A woman in her 70s who was on warfarin for atrial fibrillation (INR 3.7) developed a rectus sheath haematoma. FFP (two units) was given for warfarin reversal instead of PCC. These were prescribed by a surgical registrar. The patient had a mild allergic reaction. As a result of this case, the PCC pathway was made more accessible to clinical staff.
Case 11d.4: Read the results carefully
A man in his 80s on warfarin for bilateral pulmonary emboli, was admitted with abdominal pain and distension. He was treated with PCC (3000 units) based on an erroneous blood result reported from a point-of-care test where the doctor misread the result (reporting that the Hb had fallen from 145g/L
Incidents Related to Prothrombin Complex Concentrate (PCC) n=5 11d

98
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
11d. Incidents Related to Prothrombin Complex Concentrate (PCC)
to 45, but this was the %; actual Hb was 90-102g/L). The patient had already received vitamin K.
Case 11d.5: Consider the timing carefully
A man in his 60s on warfarin received PCC in advance of a renal transplant, but the interval between admission and transplant was sufficient that the INR was corrected to 1.2 by vitamin K and stopping the warfarin so the PCC was unnecessary.
Reference
AAGBI. Regional Anaesthesia and Patients with Abnormalities of Coagulation. 2013 https://www.aagbi.org/sites/default/files/rapac_2013_web.pdf [accessed 18 March 2018].

99
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
12. Near Miss Reporting (NM)
Authors: Alison Watt and Katy Cowan
Definition:
A ‘near miss’ event refers to any error which if undetected, could result in the determination of a wrong blood group or transfusion of an incorrect component, but was recognised before the transfusion took place.
An increase in near miss reports is noted, n=1359 in 2017, compared to n=1283 in 2016. Continued reporting is important to support learning from near miss cases, which do not cause patient harm. The long-term aim of an incident reporting system, such as SHOT, is to help reduce incidents that result in harm while moving towards increased reporting of near miss events for future learning.
Key SHOT messages
• Near miss errors often result from underlying poor practices, many of which are triggered by inadequate systems. Root cause analyses of near miss events should be designed to highlight and resolve these system failures, i.e. the human factors and ergonomics aspects
• In addition, all staff should have personal accountability for their own actions, fully completing their specific role in the transfusion process. Staff should also be empowered to refuse requests from colleagues which may be outside the standards of safe practice
• Constant vigilance and education are needed to encourage sample-takers to understand the importance of a group-check sample and to discourage poor practice, including attempts to circumvent the process
• Group-check policies should consider the criteria for a valid historical record in that institution, taking account of the addendum to the British Society for Haematology (BSH) guidelines (BSH addendum 2015) for pre-transfusion compatibility procedures in blood transfusion laboratories
Discussion of near miss errors in other categories
Near miss cases are detailed in each relevant chapter and Table 12.1 shows the chapters that include near miss incidents according to SHOT definitions.
Categorisation of all near misses according to SHOT definitions
Discussed in chapter
Number of cases
Percentage of cases
Incorrect blood component transfused (IBCT)
Wrong component transfused (WCT) Chapter 10 899 66.1%
Specific requirements not met (SRNM) Chapter 10 121 8.9%
Handling and storage errors (HSE) Chapter 9 154 11.3%
Right blood right patient (RBRP) Chapter 8 138 10.2%
Adverse events related to anti-D immunoglobulin (Anti-D Ig) Chapter 14 35 2.6%
Avoidable, delayed or undertransfusion (ADU) Chapter 11 12 0.9%
Total 1359 100%
Table 12.1:
Possible outcomes
from near miss
incidents if not
detected
Near Miss Reporting (NM) n=1359 12

100
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
12. Near Miss Reporting (NM)
Near miss wrong blood in tube (WBIT) n=789
WBIT errors continue to make up a disproportionately large proportion of the total near miss incidents 789/1359 (58.1%). Further discussion of these errors can be found in Chapter 10, Incorrect Blood Component Transfused (IBCT). It appears the efforts to reduce this potentially dangerous error are not proving successful. Alternatively, the ongoing increase may be due to improved reporting and/or a higher rate of detection, e.g. because of the group-check sample. Approximately 220 organisations are registered to report to SHOT, so the rate of reported near miss WBIT is 3-4 per organisation per year (789/220). The actual rate may be higher as a regional study showed WBIT errors may be underreported (Varey et al. 2013). These are serious errors and further efforts are required to reduce the problem.
Group-check samples
The recommended group-check policy prior to a first-time transfusion should prevent potentially lethal errors. In reports of WBIT incidents 611/789 (77.4%) indicated that their institution required two separate samples before issuing group-specific blood and 215/789 (27.2%) reported that the error was detected as a result of their group-check policy (Cases 12.3 and 12.4 below).
Case 12.1: Routine non-application of an identification band contributes to a WBIT incident
Patient 1 was due to attend for an outpatient assessment, but nursing staff had used Patient 2’s details to admit Patient 1 to the hospital system, because Patient 2 had the same last name, forename and year of birth, although a different day and month of birth. There was then failure to check that the patient identity and records matched on admission, because day case attenders are not issued with an identification band. The blood request form was generated with Patient 2 details and the doctor took a group and save sample from the intended Patient 1 having verbally confirmed the name only, without checking the date of birth. Ward staff realised the identification error when other pathology results were not available for the expected patient. A contributory factor was that the ward clerk was on long-term sick leave and had not been replaced, so there was no one to check if correct documentation had been supplied for the patient. An additional factor was the lack of procedure to check if new doctors have completed a phlebotomy assessment on appointment.
Case 12.2: WBIT incident after failure to put correct equipment in place
A sample and form were both correctly labelled with Patient 2 demographics, but the sample-taker later realised the sample was actually taken from Patient 1. A doctor, who was already under extreme pressure due to workload, was called to an outpatient area to take a transfusion sample and a nurse provided verbal details of Patient 1 identity. The doctor could not print the request form due to the lack of an enabled printer and there were no paper forms available. Therefore, the doctor took the unlabelled sample back to the ward and mistakenly printed a form for Patient 2, then used Patient 2 demographics to label the sample. This task is undertaken infrequently in the outpatient department and the process for obtaining transfusion samples is different from other pathology samples because transfusion is not part of the electronic requesting system. The department manager was aware of a previous incident caused by having no printer for transfusion requests, but the correct equipment had not been installed due to lack of space. An interim supply of paper request forms has been provided.
Cases 12.1 and 12.2 clearly describe system failures that contributed to poor practices. One means of reducing WBIT incidents would be to review the human factors that make it difficult to follow standard procedures. Further information can be found in Chapter 6, Human Factors in SHOT Error Incidents.
Learning point
• Wrong blood in tube (WBIT) errors often result from underlying poor practices, many of which are triggered by inadequate systems. Root-cause analyses of WBIT events should be designed to highlight and resolve these system failures, i.e. the human factors and ergonomics aspects

101
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
12. Near Miss Reporting (NM)
ABO-incompatibility prevented by detection of near miss incidents n=342
A total of 899 near miss errors were reported that could have resulted in IBCT and 342/899 (38.0%) could have resulted in an ABO-incompatible red cell transfusion. Most, 226/342 (66.1%), would have resulted in transfusions of group A, B or AB units to patients of group O which is particularly dangerous because group O individuals have three ABO antibodies, anti-A, -B and -A,B which may react more strongly than anti-A and anti-B produced by individuals who are group A or group B (Klein and Anstee 2005). This is an unacceptable risk and these errors should be investigated as fully as those that actually led to transfusion of ABO-incompatible red cells, n=1 (Chapter 10, Incorrect Blood Component Transfused (IBCT)). Most potential ABO-incompatible transfusions, 317/342 (92.7%) resulted from WBIT errors, which means 317/789 (40.2%) of all WBIT could have resulted in an ABO-incompatible transfusion. In a further 38/789 (4.8%) the groups were unknown, so may also have been ABO-incompatible risks. There are excellent procedures in transfusion laboratories designed to detect WBIT, including comparing patient history, supplemented by a group-check policy in many organisations (BSH Milkins et al. 2013). Therefore, it is uncommon for WBIT errors to result in a wrong component transfused. However, sample-takers and those involved in designing the processes for safe phlebotomy must not underestimate the potential danger of these errors and staff cannot assume these errors will always be detected in the laboratory. All except 9 of the total 342 ABO-incompatible near misses resulted from clinical errors.
Cause of potential ABO-incompatible transfusions
Number of casesPercentage of
cases
Wrong blood in tube (WBIT) 317 92.7% Clinical errorn=333Component collection/administration error 16 4.7%
Sample receipt error, wrong patient's record 2 0.6%Laboratory error n=9
Wrong group component selected 3 0.9%
Grouping/testing error 4 1.1%
Total 342 100%
Quality management systems (QMS)
Good quality processes in both the laboratory and clinical areas often detect errors in near miss incidents and are therefore shown to prevent unsafe transfusions. However, 312/1359 (23.0%) near misses were detected accidentally and 658/1359 (48.4%) were only detected by a level of good fortune, because the ABO/D or other laboratory test result differed.
QMS=quality management system
100
658
289
312
Laboratory QMS
Laboratory QMS, but good fortunethat ABO/D or other test result differed
Clinical QMS
Accidental detection, QMS wouldnot have detected the error
QMS=quality management system
Table 12.2:
Cause of potential
ABO-incompatible
transfusions
Figure 12.1:
Near miss
detected by quality
management system
or good fortune

102
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
12. Near Miss Reporting (NM)
Case 12.3: Group-check policy detects WBIT incident
A patient was bled twice prior to surgery. One sample was taken by a phlebotomist in the early morning and the other sample was taken by a member of the ward staff approximately 2 hours later. One of the samples grouped as A D-negative and the other was group A D-positive. The group of a further sample showed the original sample taken by the phlebotomist contained the wrong patient’s blood.
Case 12.4: WBIT incident uncovers department-wide circumvention of group-check policy
Two WBIT samples were detected from the same department. The investigation identified that a member of staff took two samples at the same time for two different patients. The second samples of each were given to another member of staff to label and these were mislabelled. These two patients required two samples under the group-check policy for patients who do not have a historical blood group on the system. On further investigation it was established that this practice was common within a selected group of staff from this department. The staff were taking two samples at the same time and asking another member of staff to complete the details on the second sample. Although the staff had been trained they felt that this process was kinder to the patient as they did not have to be bled twice and did not need to stay for the second sample to be taken. All staff involved were prevented from taking samples until retrained with further emphasis on the reason for the group-check rule included in the training.
Case 12.3 demonstrates the value of a group-check policy to prevent a potentially dangerous error, whereas Case 12.4 shows that processes can become distorted over time, often with good intentions, because staff either forget or do not understand the importance of such checks. A culture of sidestepping a standard process can become prevalent, but this incident shows individuals placing unwarranted trust in the actions of their colleagues.
Learning points
• All staff should take personal responsibility for their own actions, fully completing their specific role in the transfusion process and should be empowered to refuse requests from colleagues which may be outside the standards of safe practice
• Constant vigilance and education is needed to encourage sample-takers to understand the importance of a group-check sample and to discourage poor practice, including attempts to circumvent the process
Value of historical samples
The WBIT incidents include 68/789 (8.6%) reports of historical errors, some of which date from as far back as the 1990s, although many occur within the same patient episode.
Case 12.5: Results from neonatal samples may not provide a valid historical group
A sample received from the antenatal clinic correctly grouped as AB D-negative, but the historical group was recorded as B D-negative. However, this historical sample was taken many years ago, when the patient would have been a neonate. It was not possible to determine whether the historically incorrect group was due to a clinical sampling error or a laboratory processing error. The criteria for acceptance of a historical group as the first sample are being reviewed.
A WBIT at birth is the most likely explanation in Case 12.5, including that it may have been maternal instead of cord blood, because a common reason for this patient to have been grouped at birth would be a cord blood taken for the anti-D immunisation prevention scheme. In 2017 there were 36 ‘near miss’ incidents associated with maternal and cord/baby samples of which 35 were WBIT. Testing of fetal/neonatal and cord blood samples can be difficult because ABO red cell antigens may be poorly expressed at birth (BSH New et al. 2016); in the case above the sample could group as B if the A antigen was poorly expressed. Depending upon technique it is possible that maternal blood rather than baby

103
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
12. Near Miss Reporting (NM)
blood is sampled from the placenta. The placenta contains maternal blood in the intervillous spaces and fetal blood in the placental villi and umbilical cord. To ensure that the newborn blood sample is not contaminated with maternal blood it is best to sample only from the umbilical cord (Duerbeck et al. 1992).
Learning point
• Group-check policies should consider the criteria for a valid historical record in that institution, taking account of the addendum to the British Society for Haematology (BSH) guidelines (BSH addendum 2015) for pre-transfusion compatibility procedures in blood transfusion laboratories
Commentary
Near miss incidents provide an excellent opportunity to learn valuable lessons before a patient is harmed. Incident investigations should focus on how to ensure the implicated processes are safe and that the systems are designed to reduce the likelihood of error. Incident investigators are encouraged to use the questions in the SHOT human factors investigation tool (HFIT) to understand failures in the transfusion process that have been identified by these incidents with no patient harm. Further information can be found in Chapter 6, Human Factors in SHOT Error Incidents.
References
BSH Addendum to guidelines for pre-transfusion compatibility procedures in blood transfusion laboratories 2015. http://www.b-s-h.org.uk/media/5149/pre-transfusion-historical-samples-scenarios-version-_-final290115.doc [accessed 28 February 2018].
BSH Milkins C, Berryman J et al. Guidelines for pre-transfusion compatibility procedures in blood transfusion laboratories. Transfus Med 2013;23:3-35 http://onlinelibrary.wiley.com/doi/10.1111/j.1365-3148.2012.01199.x/pdf [accessed 28 February 2018].
BSH New HV, Berryman J et al. Guidelines on transfusion for fetuses, neonates and older children. Br J Haematol 2016; 175:784-828 http://onlinelibrary.wiley.com/doi/10.1111/bjh.14233/full [accessed 28 February 2018].
Duerbeck NB, Chaffin DG, Seeds JW. A practical approach to umbilical artery pH and blood gas determination. Obstet Gynaecol 1992;79:959-962.
Fisher B and Hackney JH. Modifications in the alkali denaturation test for fetal hemoglobin. Am J Clin Path 1957;27(1):48-51.
Flanagan CJ and Mitoma TF. Clumping (false agglutination) of blood from the umbilical cord. Am J Clin Path 1958;29(4):337-339.
Klein HG and Anstee DJ. Mollison’s blood transfusion in clinical medicine; 11th edition. Blackwell publishing 2005:122
Varey A, Tinegate H et al. Factors predisposing to wrong blood in tube incidents: a year’s experience in the North East of England. Transfus Med 2013;23(5):321-325.

104
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
13. Errors Related to Information Technology (IT)
Author: Megan Rowley
Definition:
This chapter covers transfusion adverse events that relate to laboratory information management systems (LIMS) as well as other information technology (IT) systems and related equipment used in the delivery of hospital transfusion services.
Cases selected include events where IT systems may have caused or contributed to the errors reported, where IT systems have been used incorrectly and also includes cases where IT systems could have prevented errors but were not used. Where the corrective and preventive action suggested by hospitals in response to errors included IT solutions, these have been included.
Overview
This report highlights the small number of situations where IT systems have not been used correctly or have not performed as expected. By understanding what can go wrong, users of IT systems that support transfusion practice can be aware of potential problems so that the specification, configuration, implementation and testing of IT systems is optimised, thereby improving patient safety. A summary of these errors can be found in the supplementary information on the SHOT website (www.shotuk.org) and the detail and some examples can be found in the individual chapters.
While electronic and automated systems should be easy to use, and have the general aim of simplifying transfusion practice, the importance of adequate and timely training of all staff in their correct use is of paramount importance. As has been stated before, IT systems support clinical and laboratory transfusion practice, but do not replace the knowledge of safe transfusion practice.
The importance of IT systems in supporting safe transfusion practice should not be underestimated. It is no longer possible to operate a transfusion laboratory without a LIMS. Full automation with a bidirectional interface and electronic issue of blood are standards expected by the UK Transfusion Laboratory Collaborative (UKTLC) (Chaffe et al. 2014).
Likewise, vein-to-vein electronic blood management systems (EBMS) have successfully delivered safer and more efficient transfusion practice across a variety of clinical settings. EBMS are of proven value and should be considered in all settings where transfusion takes place. The UKTLC standards also recommend ‘It is expected that where remote issue of components is being considered as part of service delivery, consideration will also be given to installing complete blood tracking (vein-to-vein) as an integral feature of this development’ (Chaffe et al. 2014).
The 2015 National Institute for Health and Care Excellence (NICE) guidelines on blood transfusion addressed the clinical and cost effectiveness of electronic identification systems (EIS) and clinical decision support systems using computerised physician order entry (CPOE) in the blood transfusion setting. EIS at the point of blood sampling, blood collection and blood administration promote safety by reducing human error and one of the recommendations was that ‘Hospitals should consider using electronic patient identification systems to improve the safety and efficiency of the blood transfusion process’ (NICE 2015). In respect of CPOE the evidence was not strong enough to make a recommendation and further research was advised on this topic.
Some UK hospitals, notably the Oxford University Hospitals National Health Service (NHS) Trust, have successfully implemented vein-to-vein EBMS and have benefited from improved safety and efficiency
Errors Related to Information Technology (IT) n=20013

105
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
13. Errors Related to Information Technology (IT)
(Staves et al. 2008, Hibbs et al. 2014, Murphy et al. 2012). Both EIS and CPOE are used in the wider clinical setting and where they are implemented, transfusion functionality should be considered in scope. In a British Medical Journal (BMJ) article summarising the NICE guidelines the authors comment that the implementation of electronic patient identification systems to improve the safety and efficiency of routine transfusion practice will cost money but bring substantial savings in nursing and laboratory staff time and reduced red blood cell unit wastage. They recommend that ‘Organisations should identify local barriers to implementation and develop action plans for overcoming them’ (Padhi et al. 2015).
Recommendation
• All available information technology (IT) systems to support transfusion practice should be considered and these systems implemented to their full functionality. Electronic blood management systems should be considered in all clinical settings where transfusion takes place. This is no longer an innovative approach to safe transfusion practice, it is the standard that all should aim for
Action: Hospital Chief Executives, Hospital Risk Managers and Hospital Transfusion Teams
References
Chaffe B, Glencross H et al. UK Transfusion Laboratory Collaborative: minimum standards for staff qualifications, training, competency and the use of information technology in hospital transfusion laboratories. Transfus Med 2014;24:335–340.
Hibbs SP, Noel S et al. The impact of electronic decision support and electronic remote blood issue on transfusion practice. Transfus Med 2014;24(5):274-9.
Murphy MF, Fraser E et al. How do we monitor hospital transfusion practice using an end-to-end electronic transfusion management system? Transfusion 2012;52:2502-2512.
National Institute for Health and Care Excellence. Blood transfusion. (NICE guideline 24) 2015. www.nice.org.uk/guidance/NG24 [accessed 3 April 2018].
Padhi S, Kemmis-Betty S et al. on behalf of the Guideline Development Group. Blood transfusion: summary of NICE guidance. BMJ 2015;351:h5832.
Staves J, Davies A et al. Electronic remote blood issue: a combination of remote blood issue with a system for end-to-end electronic control of transfusion to provide a ‘total solution’ for a safe and timely hospital blood transfusion service. Transfusion 2008;48(3):415-24.

106
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
14. Adverse Events Related to Anti-D Immunoglobulin (Ig)
Authors: Clare Denison and Katy Cowan
Definition:
An adverse event related to anti-D immunoglobulin (Ig) is defined as related to the prescription, requesting, administration or omission of anti-D Ig which has the potential to cause harm to the mother or fetus immediately or in the future.
Key SHOT messages
• A total of 426 reports related to errors involving anti-D immunoglobulin (Ig) were reviewed in 2017, of which 327/426 (76.8%) related to omission or late administration of anti-D Ig. This is a continuing and worrying trend that is resulting in many women being put at risk of sensitisation to the D antigen
• This year, in addition to poor knowledge about indications and delivery of anti-D Ig, there is also evidence of a lack of knowledge of basic blood group theory. This was demonstrated by the interpretation of cell-free fetal deoxyribonucleic acid (cffDNA) results and the requirements for anti-D Ig based on these results
• It is important that D-negative women understand the importance of reporting potentially sensitising events (PSE) to their midwife or maternity provider, so that they receive appropriate anti-D Ig cover in a timely manner
Recommendations
• All staff involved in the requesting, issuing or administration of anti-D immunoglobulin (Ig) should have received appropriate training and education in relation to anti-D Ig, such as completion of the anti-D Ig module in the Learn Blood Transfusion (LBT) e-learning package (www.learnbloodtransfusion.org.uk)
Action: Hospital Transfusion Laboratories, Hospital Transfusion Committees, Trust/Health Board Chief Executive Officers (CEO), Obstetric Departments, Community Midwifery Teams
• Maternity services should have systems in place to ensure that women who are D-negative are made aware of their results and the importance of attending their midwife for anti-D Ig prophylaxis in the event of having a potentially sensitising event (PSE) from 12/40 onwards
• D-negative women should be educated about what constitutes a PSE so that they are aware of when anti-D Ig may be required
Action: Royal College of Obstetricians and Gynaecologists, Royal College of Midwives
Adverse Events Related to Anti-D Immunoglobulin (Ig) n=42614

107
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
14. Adverse Events Related to Anti-D Immunoglobulin (Ig)
• All healthcare professionals, including laboratory staff, are responsible for ensuring that women who are found to have become sensitised to the D antigen in pregnancy are reported to SHOT with an accurate and complete dataset
Action: Hospital Transfusion Laboratories, Hospital Transfusion Committees, Trust/Health Board Chief Executive Officers (CEOs), Obstetric Departments, Community Midwifery Teams
Good practice point
• Hospital blood transfusion laboratories should have systems in place to identify any anti-D Ig that has been issued for a woman but not collected from the laboratory. The system should include a mechanism to escalate the urgency of the anti-D Ig administration to ensure that it is administered before the 72-hour time limit has elapsed. Although this is a suggested time limit, there is some evidence* that giving anti-D Ig after these limits may offer some protection
*Note: Experimental evidence is quoted (in Klein and Anstee 2005) ‘there is evidence that in a proportion of subjects the response to D can be suppressed by giving antibody [anti-D Ig] as late as 2 weeks’. The experimental evidence was from a study by Samson and Mollison following development of anti-D in volunteer male blood donors injected intravenously with 1mL D-positive red cells (Samson and Mollison 1975)
Learning points
• Hospitals should ensure that there are robust systems in place for the administration of anti-D immunoglobulin (Ig) in a timely manner in response to a potentially sensitising event (PSE). This is particularly important when other departments may be involved in the care of the woman but not directly administer the anti-D Ig (i.e. emergency departments)
• Hospitals should have clear processes developed for the checking of historical blood group records prior to the requesting of anti-D Ig by clinical staff or issue of anti-D Ig by laboratory staff to prevent inappropriate requests and administration
• Where cell-free fetal deoxyribonucleic acid (cffDNA) testing is performed there should be robust systems in place for checking of the results to prevent inappropriate requesting and administration of anti-D Ig when the fetus is predicted to be D-negative
In 2017 two new categories have been introduced to the report for errors related to anti-D Ig
• Right product right patient; where women have received anti-D Ig prophylaxis appropriately, with the correct dose at the correct time but where an error related to the issue of anti-D Ig from the blood transfusion laboratory has been noted subsequently, e.g. the transfusion sample tested in the laboratory was inadequately labelled but this error was only noticed following testing of the sample and release of the product
• Unnecessary administration of anti-D Ig; where a woman has received a dose of anti-D Ig that was not clinically required as they have not experienced a PSE
Commentary
The 2017 Annual SHOT Report highlights some recurring issues about provision of anti-D Ig. A lack of knowledge and understanding particularly among clinical staff continue to result in women being put at risk of sensitisation.
The many reports of late administration of anti-D Ig illustrate the lack of awareness of the importance of administering anti-D Ig within 72 hours of a PSE by both D-negative women and the clinical staff that manage their care. This requirement should be emphasised to all staff involved in the care of pregnant women and the women identified as being D-negative. There have been cases reported this year where a woman has presented with a PSE and a subsequent appointment for her to receive anti-D Ig has been made for more than 72 hours later.

108
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
14. Adverse Events Related to Anti-D Immunoglobulin (Ig)
2
2
7
12
14
16
23
23
327
Right product right patient
Unnecessary administration of anti-D Ig
Anti-D Ig handling and storage errors
Anti-D Ig given to the wrong woman
Anti-D Ig given to a D-positive woman
Anti-D Ig given to the mother of a D-negative infant
Anti-D Ig given to a woman with immune anti-D
Wrong dose of anti-D Ig given
Omission or late administration of anti-D Ig
77.4%
18.8%5
11
80
330
MultipleOther
Community
Hospital 2.6%
1.2%
Deaths n=0
No deaths were reported related to errors associated with anti-D Ig in 2017.
Major morbidity n=2
Two women developed immune anti-D. The first resulted from an error in clinical management. This woman delivered at 32/40, no post-delivery blood samples from mother or baby were received in the laboratory and post-delivery anti-D Ig was not issued by the laboratory. Mother and baby were both transferred to another hospital. Immune anti-D was detected in this woman’s booking sample for a subsequent pregnancy in 2017.
The second case was not fully investigated in a timely manner therefore putting the baby at an increased risk of developing haemolytic disease of the fetus and newborn (HDFN). This woman had anti-D detected in her sample at 20/40, however this was not investigated by the transfusion laboratory at the time and there was no record of anti-D Ig having been administered to account for it. The woman’s 28/40 sample was also found to contain anti-D which was then investigated. The quantification result was 17.1IU/mL, however routine antenatal anti-D prophylaxis (RAADP) had already been administered unnecessarily before this result was available.
Figure 14.1:
Distribution of
anti-D Ig-related
error reports
Figure 14.2:
Location of errors
associated with
anti-D Ig
n=426

109
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
14. Adverse Events Related to Anti-D Immunoglobulin (Ig)
Potential for major morbidity n=326
Altogether a total of 327/426 (76.8%) case reports related to the omission or late administration of anti-D Ig. In one of these cases a woman developed an immune anti-D (counted in major morbidity above), but the remainder of the omission or late administration incidents (326) have the potential for the woman to develop an immune anti-D. This is a worrying situation, putting a significant number of women at risk of potential sensitisation to the D antigen.
Overview of cases
Most errors 385/426 (90.4%) occurred during normal working hours. Clinical staff were responsible for 331/426 (77.7%) of the errors reported across all categories with 47/426 (11.0%) involving doctors, including consultants.
284
240
62
16
47
38
33
33
0 50 100 150 200 250 300 350 400 450
Total
Omission/late administration of anti-D Ig
Anti-D Ig given to a D-positive woman
Anti-D Ig given to a woman with immune anti-D
Anti-D Ig given to mother of a D-negative infant
Anti-D Ig given to wrong woman
Wrong dose of anti-D Ig given
Anti-D Ig handling and storage errors
Right product right patient
Unnecessary administration of anti-D IgNurse/midwifeLaboratory
Doctor
Other/unknown
Omission or late administration of anti-D Ig n=327 (76.8%)
Most errors associated with the omission or late administration of anti-D Ig occurred in the hospital environment (237/327, 72.5%). However, there were still many errors occurring in the community including at general practitioner (GP) surgeries.
Common themes identified in this category include:
• Failure to administer anti-D Ig within 72 hours following a PSE
• Failure to follow up or check blood group results to determine the need for anti-D Ig
• Failure in the timely collection of anti-D Ig from the laboratory, in particular when women are discharged quickly post delivery
• Communication failures when women have shared care between hospital and community midwifery teams
• Failure to understand the results of cffDNA testing and the requirements for anti-D Ig
Additional case reports illustrating these themes are available in supplementary material on the SHOT website, www.shotuk.org.
Case 14.1: RAADP not given due to erroneous cffDNA testing result
The cffDNA testing predicted a fetus to be D-negative but at delivery the cord sample was shown to be D-positive. RAADP had not been administered during the pregnancy because of the cffDNA result. Further testing revealed that the likely cause of the discrepancy was very low levels of fetal DNA in the maternal plasma, below the limit of detection.
Figure 14.3:
Staff group
responsible for
primary error
associated with
anti-D Ig by
category

110
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
14. Adverse Events Related to Anti-D Immunoglobulin (Ig)
Handling and storage errors related to anti-D Ig n=7 (1.6%)
There were 3 clinical and 4 laboratory errors, all occurred in a hospital environment.
Doses of anti-D Ig should not be split in order to provide 250IU. It is safe to give a larger dose.
Case 14.2: Decanting of anti-D Ig to give a smaller dose than the one in the vial
A woman was due 250IU anti-D Ig, however no 250IU or 500IU vials were available in the laboratory, therefore 1500IU was issued. Clinical staff decanted the pre-filled syringe into a graduated syringe, and gave a third of the amount. This is against the manufacturer’s recommendations.
Case 14.3: Decanting of half a vial of anti-D Ig to achieve the recommended dose
250IU anti-D Ig was prescribed following an ectopic pregnancy at less than 20/40 for a D-negative woman. The 250IU dose is no longer supplied by the manufacturer therefore the smallest dose available in the organisation was 500IU. The doctor overseeing the care of the woman noted that 250IU was the correct dose according to the departmental guidelines and the nurse was instructed to draw up half of a 500IU vial issued by the laboratory and administer it to the woman. The nurse did this despite objecting and informing the doctor of the smallest dose of anti-D Ig available.
Anti-D Ig given to D-positive women n=14 (3.3%)
There were 7 clinical staff and 7 laboratory staff errors; 10 in hospital and 4 in the community.
The main theme identified in this category was failure to check the woman’s blood group on historical records prior to ordering or issuing anti-D Ig.
There were also 3 reports where the woman’s blood group had been confirmed as ‘Weak D-positive’ however anti-D Ig was still issued by the laboratory.
Anti-D Ig given to a woman with a known immune anti-D n=23 (5.4%)
There were 10 clinical staff and 13 laboratory staff errors; 22 were in hospital and 1 in the community.
The main theme identified in this category was a failure to check historical records by both clinical and laboratory staff.
Case 14.4: Anti-D Ig issued from pharmacy for a woman with immune anti-D
RAADP was administered to a woman at 28/40. However, she was already alloimmunised with an anti-D level of 4.9IU/mL. In this organisation anti-D Ig is currently issued by pharmacy not the blood transfusion laboratory but plans are in place for the blood transfusion laboratory to take over the issue and distribution of anti-D Ig prophylaxis in the near future.
Case 14.5: Historical records not available results in inappropriate administration of anti-D Ig
Anti-D Ig was administered to a patient at 28/40 without checking the historical record of her blood group as her notes were not available at the time. The midwife did not look for the notes, or access them via the electronic report browser. The woman had been provided with an appointment in the 28-week RAADP clinic for blood sampling to determine her known immune anti-D level at 28/40. The woman confirmed that her blood group was D-negative verbally with the midwife and anti-D Ig was given. When the midwife was placing the administration record in the woman’s notes once they became available, they realised that the patient had immune anti-D (reported levels between 0.1IU/mL and 0.8IU/mL) and anti-D Ig was not indicated.
Case 14.6: Biomedical scientist (BMS) did not understand notes on the laboratory information management system (LIMS) related to the antibody result
An inexperienced BMS did not understand the significance of the notes against the woman’s records on the LIMS. The woman had a complex antenatal history with anti-G being detected as well as anti-D. As a result, anti-D Ig was issued without the BMS seeking advice from a senior member of staff.

111
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
14. Adverse Events Related to Anti-D Immunoglobulin (Ig)
Anti-D Ig given to the mother of a D-negative infant n=16 (3.8%)
The majority, 10/16, resulted from BMS errors, 4 from midwife errors and 2 from doctor errors.
The laboratory errors resulted from issue of postnatal anti-D Ig before the infant blood group had been confirmed as D-positive or where the infant’s blood group had been incorrectly recorded as D-positive.
For the first time this year there are also reports related to the misinterpretation of or failure to check cffDNA results by clinical staff.
Case 14.7: RAADP given at 29/40 because the midwife failed to check results of cffDNA
A D-negative woman with a predicted D-negative fetus based on cffDNA results was administered 1500IU RAADP anti-D Ig at 29/40 weeks gestation because the midwife failed to check the results of the cffDNA testing.
Case 14.8: Consultant administered anti-D Ig to a D-negative woman despite cffDNA results predicting fetus to be D-negative
Following external cephalic version (ECV) the midwife noted that the woman was D-negative and the fetus was predicted to be D-negative. The midwife informed the consultant obstetrician that there had been a previous case on the postnatal ward where the cffDNA results predicted a D-negative fetus but once born the baby typed as D-positive. Following this information, the consultant telephoned the haematology consultant and discussed the case and was advised ‘to do what you think is clinically appropriate’. The consultant decided to give the anti-D Ig.
Anti-D Ig given to the wrong woman n=12 (2.8%)
There were 10 midwife/nurse errors and 2 doctor errors. 11 occurred in hospital and 1 in the community.
The themes identified in this category of reports were:
• Insufficient identification checks of the woman prior to administration of anti-D Ig
• Anti-D Ig administered that was labelled with the details of another woman
Wrong dose of anti-D Ig given n=23 (5.4%)
There were 14 errors by clinical staff, and 9 by laboratory staff.
In 10/23 cases women received less than the recommended dose of anti-D Ig which left them potentially susceptible to sensitisation.
Right product right patient n=2 (0.5%)
Both errors occurred in the laboratory. Anti-D Ig was issued and administered appropriately to women that needed it, however an error was subsequently identified related to inadequate labelling of the blood sample received in the laboratory. In one case the woman’s date of birth (DOB) on the sample was incorrect and in the other case the sample had been labelled with the incorrect first name. Had these labelling errors been identified prior to testing, the samples would have been rejected and no blood products would have been issued until further samples had been received.
Unnecessary administration of anti-D Ig n=2 (0.5%)
This category has been introduced to include administration of anti-D Ig where the administration has not been deemed clinically necessary.
Case 14.9: Request, issue and administration of anti-D Ig unnecessarily
A woman was undergoing an appendectomy at 22/40. The clinical staff on the ward requested a Kleihauer test and the laboratory issued the anti-D Ig as the BMS incorrectly thought that an appendectomy was a PSE. The anti-D Ig was administered to the woman without there being a clinical need for it.

112
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
14. Adverse Events Related to Anti-D Immunoglobulin (Ig)
Near miss anti-D Ig cases n=35
The near miss incidents related to anti-D Ig errors show similar learning points to the full incidents.
31.4%
2.9%
2.9%
22.8%
14.3%
5.7%
20.0%
7
2
5
8
1
1
11
AdministrationComponent labelling
Component selection
TestingSample receiptSample taking
Request
It is important not to confuse fetal and maternal samples, either because they are wrongly labelled or because maternal blood has been obtained from the placenta. In 2017 there were 35 wrong blood in tube cases associated with maternal and cord/baby samples. The sample should be taken from the cord vessels (fetal blood) and not from the placenta which has maternal blood in the intervillous spaces.
Information technology (IT)-related anti-D Ig cases n=10
There are several examples where the use of IT systems failed to prevent women getting anti-D Ig unnecessarily and perhaps caused omissions or delays in anti-D Ig prophylaxis.
On 2 occasions anti-D Ig was given unnecessarily to a D-positive woman because the LIMS or analyser was not working, and back-up processes were not sufficiently robust.
There were 2 incorrect anti-D Ig administrations: 1 because the wrong DOB was input to the LIMS but not detected at the bedside and the other because a cord blood group report was interpreted incorrectly, manually authorised and transmitted.
There were 4 cases where a woman had an anomalous D group and there was some confusion in how to record the interim D group and then final D group on the LIMS, and to communicate this to the clinical team.
Case 14.10: A string of errors lead to a D-positive (variant) woman getting anti-D Ig
A pregnant woman with an anomalous D group was assigned a D-negative blood group pending reference testing. The reference report confirmed a D-variant and recommended that she should be managed as D-positive. This report was uploaded to her hospital LIMS record, which was in her maiden name. Subsequent tests were performed under her married name and the records were not merged or linked. A midwife used the report of the initial D-negative blood group in the maternity record and allocated the woman to an anti-D Ig prophylaxis regime as well as issuing the patient a D-negative card. Anti-D Ig was given without accessing the updated original record or the correct record in her married name.
Figure 14.4:
Near misses that
could have led to
anti-D Ig errors n=35

113
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
14. Adverse Events Related to Anti-D Immunoglobulin (Ig)
Case 14.11: Delayed administration of anti-D Ig to a woman with an anomalous D group
A woman had a surgical termination of pregnancy and the D group was anomalous and referred for further testing. Although she was assigned a D-negative blood group, the laboratory staff were unable to issue anti-D Ig through the LIMS because the initial reference laboratory report stated that she was D-variant and should be treated as D-positive. Subsequently, after genotyping, she was found to have a D-variant associated with some D-sensitisations so the advice was to treat as D-negative for the purposes of anti-D Ig prophylaxis. Anti-D Ig was given but she had to return to hospital following discharge and administration was outside the 72-hour window.
Two women were given anti-D Ig despite having immune anti-D although the information was available on the LIMS and, if consulted, this unnecessary administration would have been prevented. On one occasion the LIMS was down but on the other occasion, the complex presentation of data on the screen was thought to have led to the BMS missing this important information.
References
BSH Austin E, Bates S et al. Guidelines for the estimation of fetomaternal haemorrhage. 2009 http://www.bcshguidelines.com/documents/BCSH_FMH_bcsh_sept2009.pdf [accessed 2 February 2018].
BSH Qureshi H, Massey E et al. Guideline for the use of anti-D immunoglobulin for the prevention of haemolytic disease of the fetus and newborn. Transfus Med 2014;24:8–20.
BSH White J, Qureshi H et al. Guideline for blood grouping and red cell antibody testing in pregnancy. Transfus Med 2016;26:246-263.
Klein HG and Anstee DJ. Immunology of red cells in Mollison’s Blood Transfusion in Clinical Medicine 11th Edition 2005, Blackwell Publishing, page 83.
Learn Blood Transfusion e-learning programme http://www.learnbloodtransfusion.org.uk/ [accessed 2 February 2018].
NICE Guidance on management of ectopic pregnancy and early miscarriage. 2012 https://www.nice.org.uk/guidance/cg154 [accessed 2 February 2018].
NICE Guidance on High throughput non-invasive prenatal testing for foetal RHD genotype. 2016 https://www.nice.org.uk/guidance/dg25 [accessed 2 February 2018].
Samson D and Mollison PL. Effect on primary Rh immunisation of delayed administration of anti-Rh. Immunology 1975;28:349–357.

114
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
Author: Jane Keidan
Royal College of Obstetrics and Gynaecology adviser: Rosie Hamilton
New questions arising from these data:
• Now that the majority of women receive routine antenatal anti-D prophylaxis (RAADP) in the form of one injection of 1500 international units (IU) of anti-D immunoglobulin (Ig) between 28 and 30 weeks gestation, if the pregnancy extends beyond 40 weeks, especially beyond late term (41-42 weeks), is an additional dose of prophylactic anti-D Ig required, particularly in obese women?
• Does obesity pose an increased risk of sensitisation, especially in the presence of other risk factors?
• Do placenta accreta and other pathological placentae pose an increased risk of fetomaternal haemorrhage (FMH) in the absence of overt antepartum bleeding?
Recommendations
• Clearer advice for healthcare professionals and women on the use of anti-D immunoglobulin (Ig) in early pregnancy
– United Kingdom (UK) guidance of the use of anti-D Ig prophylaxis (BSH Qureshi et al. 2014) should be reviewed to avoid conflicting and thus confusing advice, especially in early pregnancy. The definition of ‘early pregnancy’ should be harmonised (National Institute for Health and Care excellence (NICE) defines this as <13 weeks, and British Society for Haematology (BSH) as <12 weeks
Action: BSH Transfusion Task Force and NICE
• Informing and empowering women
– All primiparous women and multiparous women with unknown D status who are identified as D-negative from booking bloods, should be informed of the results as soon as possible so that prophylaxis for early potentially sensitising events is not overlooked. This should include, as a minimum, discussion with a healthcare professional about the implications of D-negative status, explanation of potentially sensitising events and how to seek appropriate and timely advice and prophylaxis. It should include written patient information
Action: Royal College of Obstetricians and Gynaecologists, Royal College of Midwives
• Errors resulting from cell free fetal deoxyribonucleic acid (cffDNA) testing should be reported to SHOT
– The introduction of cffDNA analysis to identify pregnancies with D-negative babies (where the mother does not require prophylaxis with anti-D Ig), while reducing unnecessary exposure of these women to blood products, has the potential to result in new types of error. SHOT has worked in collaboration with National Health Service Blood and Transplant (NHSBT) to add additional questions to the alloimmunisation questionnaire specifically related to cffDNA testing. The initial data will be reported next year
Action: All healthcare professionals involved in the management of D-negative women in pregnancy
Immune Anti-D in Pregnancy: Cases reported up to the end of 201715

115
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
• Accurate and complete datasets on women who become alloimmunised.
– All healthcare professionals, including laboratory staff, are responsible for ensuring that women who become immunised to the D antigen in pregnancy are reported to SHOT with an accurate and complete dataset
Action: All healthcare professionals involved in the management of women in pregnancy
Introduction
To improve understanding of the causes of continuing anti-D immunisations, SHOT is conducting a prospective study of women who have produced immune anti-D detected for the first time in the current (index) pregnancy. The reporters are requested to provide data on booking weight, management of sensitising events during pregnancy and the administration of routine anti-D prophylaxis, both in the index pregnancy and the pregnancy immediately before the index pregnancy (if applicable).
Results
In 2017 a total of 68 cases were reported, 16 cases occurred in women with no previous pregnancies (NPP) and 52 in women with previous pregnancies (PP), 1 case was excluded as immunisation had occurred several years ago and 1 case was excluded as there was insufficient information available for the case to be informative. Cumulatively SHOT now has data on 58 women with NPP and 165 women with PP.
4
14
3234
31
50
2
95
17
9
16
2012 2013 2014 2015 2016 2017
Previous pregnancyNo previous pregnancy
No previous pregnancy (NPP) n=16 in 2017, cumulative n=58
When was the alloimmune anti-D detected?
Number of new cases 2017
Number of cases cumulative to 2017
Before 28 weeks 2 6
At or after 28 weeks, before delivery 4 15
At delivery 10 35
Other 0 1*
No information 0 1
Total 16 58
*Alloimmune anti-D was detected 6 months postpartum after large FMH of 12.7mL at delivery managed correctly
Figure 15.1:
Number of
reports of anti-D
immunisation in
pregnancy by year,
2012-2017
Table 15.1:
Time of detection
of alloimmune
anti-D NPP

116
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
What was the booking weight?
Weight at booking in kgNumber of new
cases 2017Number of cases
cumulative to 2017
<68 8 29
68-80 1 5
>80 (obese) 0 7
No information 7 17
Total 16 58
Did the women receive appropriate RAADP?
RAADP regimenNumber of new
cases 2017Number of cases cumulative 2017
Single dose 1500IU at 28-30 weeks 11 44
Two dose regimen 500IU 0 1
Not given 4* 9
Total 15 54 (eligible cases)*1 late booking, 1 refused, 1 already in labour, 1 case no reason given
One case already had alloimmune anti-D present before RAADP was due to be given.
The route was specified in 4 cases from 2017 as intramuscular (IM) into deltoid, 1 case into gluteal region and the rest were not specified.
Details of potentially sensitising events (PSE)
Number of cases PSE Management
14 None
1 Fall at 22 weeks Kleihauer negative, 1500IU anti-D Ig given
One case had no information on PSE supplied.
PSE Number of cases
None 44
7 antepartum haemorrhage (APH)2 interventions (chorionic villous sample, amniocentesis)2 falls1 large FMH at delivery1 twin pregnancy
Some women had more than one PSE
Pregnancy outcomes
In 2017 all 16 pregnancies resulted in live births of which 8 women were delivered at or before 40 weeks and 6 at more than 40 weeks. In 2 cases the gestation at delivery was not supplied. In 6/10 pregnancies where alloimmune anti-D was detected only at delivery the gestation was >40 weeks.
One baby was D-negative, but septic so did require medical intervention at birth. Ten babies had no complications, 2 required phototherapy, 2 cases required both phototherapy and exchange transfusion. In 1 case no information was submitted.
Cumulatively, all 58 pregnancies resulted in 59 live births, of which 37 had no complications, 13 babies required phototherapy and 6 cases required exchange transfusion. No details in 2 cases.
Table 15.2:
Booking weight
NPP
Table 15.3:
Details of RAADP
for eligible NPP
cases n=15 (2017)
n=54 cumulative
Table 15.4a:
Details of potentially
sensitising events
NPP n=15
Table 15.4b:
Details for all NPP
cases reported
since 2012

117
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
Case studies
Case 15.1: Ideal care and delivered at term
Primipara (primip) in her 30s. Booking weight 59kg. Received RAADP (single dose of 1500IU anti-D Ig at 28 weeks). There were no PSE. Alloimmune anti-D detected at term delivery (2.7IU/mL). The baby required no interventions for haemolytic disease of the fetus and newborn (HDFN).
Case 15.2: Gestation >40 weeks
Primip in her 30s. Booking weight 61kg, body mass index (BMI) 24. Received RAADP (single dose of 1500IU anti-D Ig at 28 weeks). Delivered at 42 weeks. Alloimmune anti-D detected at delivery (2.4IU/mL). There were no PSE. The baby required no interventions for HDFN.
Case 15.3: Gestation >40 weeks
Primip in her 20s. Booking weight 64kg, BMI 22. Received RAADP (single dose of 1500IU anti-D Ig at 28 weeks). There were no PSE. Delivered at 42 weeks. Alloimmune anti-D detected at delivery (7.4IU/mL). The baby required no interventions for HDFN.
Summary of 2017 NPP data update
The majority of women (10/16) were found to be immunised at delivery, and 6/10 of these cases were delivered beyond 40 weeks, all received apparently ‘ideal’ care, with timely RAADP and no identifiable sensitising episodes. One case was obese, and in 1 the weight was not reported.
Review of all previous years shows that there have been 26 NPP cases where alloimmune anti-D was detected only at full term delivery and 13 of these (50.0%) were delivered at >40 weeks.
Question:
Now that the majority of women receive RAADP in the form of one injection of 1500IU between 28 and 30 weeks gestation, if the pregnancy extends beyond 40 weeks, is an additional dose of prophylactic anti-D Ig required and if so, when should this be given?
Previous pregnancies (PP) n=50 in 2017, cumulative n=165 cases
The index pregnancy in these cases refers to the current pregnancy i.e. the pregnancy in which alloimmune anti-D was first detected.
When was alloimmune anti-D detected in index (current) pregnancy?
Time of anti-D detectionNumber of new
cases 2017Number of cases cumulative total
At booking (if first trimester) 18 68 (41.2%)
After booking to 28 weeks (includes late booking) 11 15 (8.9%)
At or after 28 weeks 11 50 (30.3%)
At delivery 8 24 (14.5%)
Other 2* 8** (4.8%)
Total 50 165 (100%)
*1 postpartum follow up, 1 unknown
** 2 preoperative assessment following pregnancy, 3 at planned follow up of large FMH at delivery where correct dose of anti-D Ig had been given, 2 unknown
Where alloimmune anti-D was detected at booking in the index (current) pregnancy, only the events in the preceding pregnancy are relevant to the sensitisation (assuming no other exposure to the D antigen occurred e.g. transfusion, an unlikely event in healthy fertile women). Where anti-D is detected later in the index pregnancy, the relative contribution of events in the previous and index pregnancy is less certain. In the 8 women who had alloimmune anti-D detected for the first time at delivery, 3 had gestation >40 weeks.
Table 15.5:
When alloimmune
anti-D was
detected PP

118
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
Alloimmune anti-D was first detected at delivery in the index pregnancy in 24 pregnancies: 9 of these cases (37.5%) were delivered after 40 weeks gestation, suggesting that gestation beyond term may be a risk factor for alloimmunisation.
Information about the pregnancy immediately preceding index (current) pregnancy
One woman underwent surgical termination of her early pregnancy, 1 woman had medical termination at 6 weeks gestation (no anti-D Ig required), 3 women had miscarriages at <12 weeks, 1 woman had a stillbirth at 34 weeks, and 1 woman had an intrauterine death with large FMH at 40 weeks. Forty women had live births of which 3 resulted in D-negative babies. Twelve of these 40 live births were delivered >40 weeks gestation. In 3 cases no information was available.
Did the women receive appropriate anti-D Ig prophylaxis for pregnancy loss in preceding pregnancy?
One case received an appropriate dose (250IU) of anti-D Ig after early surgical termination at 9 weeks. Four cases required no anti-D Ig after early (<12 weeks) miscarriages (3) or medical termination (1). After the stillbirth at 34 weeks, the Kleihauer test was negative and 1500IU anti-D Ig was given. The woman whose pregnancy was complicated by an intrauterine death had a large FMH of 165mL and received a correct dose of anti-D Ig and follow up at 72 hours showed full clearance of fetal cells.
What was the booking weight of preceding pregnancy? (Cases where previous pregnancy resulted in live birth)
Weight at booking in kgNumber of new
cases 2017Number of cases cumulative total
<68 12 48
68-80 1 12
>80 (obese) 12 26
No information 18 59
Total 43 145
Cumulatively, 26 out of 145 total women reported were clinically obese in the preceding pregnancy, and, of the 86 women where booking weight was provided, 26/86 (30.2%) were obese.
Did the women who carried to term receive RAADP in preceding pregnancy?
RAADPNumber of new
cases 2017Number of cases cumulative total
Single dose 25 85
Two doses 3 10
Not given 5* 21**
No information 12 31
Total 45 147
*1 case typed incorrectly as D-positive, 1 case omitted in error, 3 cases refused
** Learning difficulties, concealed pregnancy, needle phobic, prior to RAADP introduction (3), delivered abroad (3), no reason given (5), declined (5), typed incorrectly (1), midwife error (1)
Note: these numbers are different from Table 15.6 as mothers with early fetal loss will not receive RAADP
In 10 cases the route was specified as deltoid, in 3 cases intravenous, in the other cases it was not specified/known.
Where no RAADP was given in preceding pregnancy (5 cases), in 2 cases alloimmune anti-D was detected at booking and in 2 further cases alloimmune anti-D was detected before RAADP had been given in the current pregnancy. Where no information on RAADP in preceding pregnancy was provided (12 cases) in 8 cases alloimmune anti-D was detected before 28 weeks (before RAADP) in the current pregnancy, and in 4 cases at booking.
Table 15.6:
Booking weight PP
Table 15.7:
Details of RAADP
in preceding
pregnancy

119
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
Details of potentially sensitising events in preceding pregnancy for cases reported in 2017
Sixteen PSE were reported, 18 cases had no PSE and 16 had no information about PSE.
For the 16 PSE, 4 occurred at <12 weeks so no anti-D Ig was indicated or given. Eight cases were correctly managed, and 4 cases were not correctly managed. The details are given below.
• 4 cases occurred <12 weeks, no anti-D Ig indicated or given:1 medical termination of pregnancy (MTOP)3 miscarriages
• 8 cases correctly managed:1 surgical TOP, 250IU anti-D Ig3 APH at 14 weeks, given 250IU anti-D Ig1 abdominal trauma at 19 weeks, 250IU anti-D Ig1 APH at 36 weeks, Kleihauer indicated 2.2mL FMH, 500IU anti-D Ig1 intrauterine death in third trimester, Kleihauer indicated 165mL FMH, 20,000IU anti-D Ig given intravenously, no fetal cells detectable at 72 hours
• 4 cases incorrectly managed:1 APH at 13 weeks, no anti-D Ig given1 APH at 20 weeks, unknown if anti-D Ig given but not recorded1 large FMH (176mL) at 33 weeks, given correct dose of anti-D Ig but not followed up to check for clearance of fetal cells1 external cephalic version at 38 weeks, 500IU anti-D Ig given, no test for FMH performed
Since reporting began in 2013, 44 PSE have been reported in the preceding pregnancies of which 27 (61.4%) were correctly managed.
Method of delivery of preceding pregnancy
TypeNumber of new
cases 2017Number of cases cumulative total
No information 4 44
Vaginal 23 60
Instrumental 1 7
Elective caesarean section (El CS) 5 13
Emergency CS (Em CS) 10 21
Total 43 145
Gestation more than 40 weeks at delivery of preceding pregnancy
Gestation at delivery (weeks) Number of new cases 2017
40 weeks or less 30
More than 40 weeks 12 cases in total, of which 7 cases >41 weeks
No information 1
Total 43
Cumulatively (data collected from 2015 onwards), 21 out of 101 previous pregnancies (20.8%) lasted longer than 40 weeks. National Health Service (NHS) maternity statistics 2014-2015 indicate 17.5% pregnancies extended beyond 40 weeks. http://content.digital.nhs.uk/catalogue/PUB19127.
Table 15.8:
Details of 16
potentially
sensitising events
in the preceding
pregnancy
Table 15.9:
Mode of delivery
for PP cases
Table 15.10:
Gestation >40
weeks PP

120
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
Postpartum prophylaxis (PPP) in preceding pregnancy
What happened?Number of new
cases 2017Number of cases cumulative total
Kleihauer test and appropriate dose of anti-D Ig 25 87
No prophylaxis 4* 10**
Incorrect dose/timing of anti-D Ig 1 3***
No information 9 36
D-negative baby 4 9
Total 43 145
*I case typed in error as D-positive, 1 case refused, 2 cases missed anti-D Ig in error
**2 from overseas, 1 learning difficulties, 1 needle phobic, 2 declined, 1 case typed in error as D-positive, 2 cases missed anti-D Ig in error
*** 1 dose 250IU, 2 doses given late
Anti-D detected at first trimester booking of index pregnancy n=18
The details of the preceding pregnancy may provide information on the cause of immunisation in these cases.
Casenumber
Obese (booking
weight >80kg)RAADP PSE
Delivery gestation
Delivery route
PPP ‘Risk factors’ identified
1 Yes (81) Yes No ? Vaginal Yes Obesity
2 Yes (102) Yes No 39+6 Vaginal Yes Obesity
3in Poland
? ? ? 38 Em CS ? Em CS
4 ? ? Yes 40 ? ? 176 mL FMH at 33 weeks given anti-D Ig, not followed up for clearance of fetal cells
5 No Yes No 39+6 Vaginal Yes Ideal care
6 No Refused ? 37 Em CS Refused No anti-D Ig-refused
7 ? Yes No 32 Em CS No PPP omitted afterEm CS due to midwife error
8 Yes (119) Yes (2 dose)
Yes 40 El CS Yes ECV at 38 weeks, given anti-D Ig but no test for FMH
9 Yes (86) Yes ? 41+6 Em CS Yes Obesity, gestation >40 weeks, Em CS
10 Yes (89.4) Yes Yes 38 El CS Yes APH at 13 weeks, no anti-D Ig given
11 ? ? Yes - - - IUD (?gestation) with large FMH, given correct dose of anti-D Ig, full clearance of
fetal cells at 72 hours
12 No Yes ?no 40 Vaginal Yes ideal, no record of PSE. Immunised at 11 weeks in
index (next) pregnancy
13 No Yes ?no 41 Vaginal No Gestation >40 weeks, PPP omitted in error
14 ? ? ? ? ? ? No information
15 Yes (102) Yes No 39+6 Vaginal Yes Obesity
16 - - - - - - Miscarriage at <12 weeks
17 No Yes ?no 41 Vaginal Yes Gestation >40 weeks
18 ? No ? - ? No Typed in error asD-positive and managed
accordingly
Totals of those cases with
sufficient data
6 obese5 not obese
11 yes2 no
(1 refused, 1 error)
4 yes,5 no,
7 no/?no
3 delivered
>40 weeks
2 ElCS,4 EmCS
9 yes,3 no
(1 refused, 2 errors)
Table 15.11:
Details of
postpartum
anti-D Ig
prophylaxis PP
Table 15.12:
Details of
management in
previous pregnancy

121
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
Missing data in these cases make analysis difficult, but as in NPP reports, there are cases where apparently ‘ideal’ management with no risk factors still resulted in immunisation, including cases where management of PSE was correct.
Alloimmune anti-D detected after first trimester in index (current) pregnancy n=30
Further information is requested on the index pregnancy when alloimmune anti-D is detected after the booking (first trimester) sample, as it may be that the sensitisation occurred in the index pregnancy rather than in the preceding pregnancy.
What was the booking weight of index pregnancy?
Weight at booking in kgNumber of new
cases 2017Number of cases cumulative total
<68 11 38
68-80 8 18
>80 7 14
No information 4 19
Total 30 89
7/30 cases were clinically obese.
RAADP in index pregnancy
RAADP given or not Number
Single dose 1500IU 27
Not given Late booker: alloimmune anti-D present at 28-week visit Refused
21
Total 30
Details of potentially sensitising events in index pregnancy
Number of women Details
7 cases where PSE reported before alloimmune anti-D detected
• APH at 6 weeks, no anti-D Ig• APH at 16 weeks, 1500IU anti-D Ig• APH at 17 weeks, 1500IU anti-D Ig• Twin pregnancy, obese, APH at 21 and 23 weeks, given anti-D Ig• APH at 24 weeks, Kleihauer negative, 1500IU anti-D Ig given• Abdominal trauma (abusive relationship) at 17 weeks, 1500IU anti-D Ig• Frequent epileptic fits, not reported, no anti-D Ig
22 cases no PSE reported Includes one case of placenta accreta with no reported PSE
1 case no information on PSE
In a number of cases PSE were reported but occurred after alloimmune anti-D had been found, with no reported PSE before alloimmune anti-D detection.
In 3 cases, where alloimmune anti-D was detected at delivery, antenatal care was ideal but delivery was >40 weeks.
Table 15.13:
Booking weight in
index pregnancy
Table 15.14:
Details of RAADP in
index pregnancy
Table 15.15:
Details of potentially
sensitising events in
index pregnancy PP

122
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
Outcomes of pregnancies reported in 2017:
Number of cases Outcome
4529121111
Live birthsNo treatment (4 D-negative babies)Required phototherapyRequired intrauterine transfusion and phototherapyRequired exchange transfusionRequired phototherapy and exchange transfusionRequired intrauterine transfusion and exchange transfusion after delivery
2 No information
1 Anti-D detected at 6-month follow up of previous pregnancy with large FMH
2 Early pregnancy loss (1 ectopic, 1 TOP)
Case studies
Case 15.4: Ideal care in previous pregnancy, alloimmune anti-D present at booking (11 weeks) in index pregnancy
Multiparous (multip) in her 40s. Booking weight in previous pregnancy 50kg. RAADP (1500IU anti-D Ig) given into deltoid at 28 weeks. No PSE. Delivered vaginally at 40 weeks with no complications. Postpartum prophylaxis (500IU anti-D Ig) given. Found to have all immune anti-D at 11-week booking appointment in index (next) pregnancy. Fetus required intrauterine transfusion and exchange transfusion was given after birth at 36 weeks gestation.
Comment: This woman appeared to be managed ideally in her previous pregnancy and yet was immunised at early booking in her index pregnancy.
Case 15.5: Ideal care with no complications
Multip woman in her 20s. Booking weight 72kg, BMI 26.1. Four previous pregnancies. In index pregnancy, no alloantibodies detected in booking or 28-week samples. Received RAADP (single dose of 1500IU anti-D Ig at 28 weeks IM into deltoid). No PSE. Delivered healthy baby at 39 weeks and found to have alloimmune anti-D. The baby required no interventions for HDFN.
Comment: This woman was managed in line with current guidance but became immunised.
Case 15.6: Stillbirth at 34 weeks gestation given correct dose of anti-D Ig
Multip in her 40s. Booking weight 67kg, BMI 27. Seven previous pregnancies. In the pregnancy immediately prior to index pregnancy she received RAADP (single dose of 1500IU anti-D Ig at 28 weeks). No PSE until stillbirth at 34 weeks gestation, cause unknown – not HDFN. Kleihauer negative. Given single dose of 1500IU anti-D Ig. Antibody screen at booking of index pregnancy negative, alloimmune anti-D detected at 28 weeks. There were no PSE. The baby required no interventions for HDFN.
Comment: This woman was managed in line with current guidance but became immunised.
Case 15.7: Large FMH
Multip in her 20s. Previous pregnancy ended as intrauterine death at 40+6 weeks following placental abruption. Kleihauer showed large FMH and the Blood Centre confirmed bleed of 165mL. The Blood Service recommended the woman should receive anti-D Ig 15000IU intravenous (IV) and 2000IU IM. She was given 20,000IU IV in total. Follow up Kleihauer at 72 hours showed full clearance of fetal cells. Alloimmune anti-D was detected at 9 weeks in the booking sample of the index pregnancy, which was terminated as woman required chemotherapy.
Comment: This woman was managed in line with current guidance but became immunised. It may be that her bleeding was acute on chronic making up 165mL total FMH, so that earlier bleeds would not have been covered by anti-D Ig in time.
Table 15.16:
Outcome of
pregnancies
reported in 2017

123
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
Case 15.8: Obese
Multip in her 20s. Booking weight in previous pregnancy 100kg. Received RAADP (single dose of 1500IU anti-D Ig IM at 28 weeks). No known PSE. Delivered spontaneously at 42 weeks. Kleihauer negative. 500IU anti-D Ig as PPP. Booking weight of index pregnancy 98kg. APH at 17 weeks for which she received 1500IU anti-D Ig IM. Alloimmune anti-D detected at 27 weeks gestation. The baby required no interventions for HDFN.
Comment: This woman was managed in line with current guidance but became immunised.
Case 15.9: Variant D typed as D-positive in previous pregnancies
Multip in her 20s. In her first pregnancy she was typed as D-positive (strong reaction) so received no anti-D Ig as RAADP or PPP. She received transfusion with D-positive blood for PPH. In her next pregnancy at booking she was again typed as D-positive with no antibodies so received no anti-D Ig as RAADP or PPP. In her index pregnancy alloimmune anti-D was detected at 6 weeks in the booking sample and she was subsequently investigated by the International Blood Group Reference Laboratory which showed her to have a D-variant (weak D type 1 and 2 alleles were not detected by deoxyribonucleic acid (DNA) amplification).
Comment: D-variants can be erroneously typed as D-positive and this should be considered if the reaction in D-typing is weak, as such cases should be referred for further investigation to exclude D-variants. In this case the reaction in D-typing was strong and the true D-type was only identified when alloimmune anti-D developed.
Case 15.10: Early miscarriage of a non-viable pregnancy with repeated bleeding
Multip in her 30s. First pregnancy, D-negative baby. Second pregnancy resulted in an early miscarriage of a non-viable pregnancy. She then bled for 5 weeks but received no anti-D Ig. Review of BSH guidance (BSH Qureshi et al. 2014) shows that there is potential for confusion in such cases as the key recommendations section states:
‘In pregnancies <12 weeks gestation, anti-D Ig prophylaxis is only indicated following ectopic pregnancy, molar pregnancy, therapeutic termination of pregnancy and in cases of uterine bleeding where this is repeated, heavy or associated with abdominal pain. The minimum dose should be 250IU. A test for fetomaternal haemorrhage (FMH) is not required’.
This would suggest that as the bleeding was repeated in this case anti-D Ig may have been indicated, although the pregnancy was very early and non-viable. By contrast, in the same guideline, the relevant section of PSE <12 weeks gestation states:
‘In cases of spontaneous complete miscarriage confirmed by scan where the uterus is not instrumented, or where mild painless vaginal (PV) bleeding occurs before 12 weeks, prophylactic anti-D immunoglobulin is not necessary because the risk of FMH and hence maternal exposure to the D antigen is negligible’.
Comment: This woman was managed in line with current guidance (if interpreted in one way) but became immunised.
Case 15.11: APH at 6 weeks, developed alloimmune anti-D in third trimester
Multip in her 30s, obese. APH at 6 weeks in index pregnancy. No anti-D Ig indicated or given. Received RAADP at 29 weeks. Alloimmune anti-D found at 34 weeks gestation. The baby required no interventions for HDFN.
Comment: This woman was managed in line with current guidance but became immunised.
Case 15.12: External cephalic version (ECV)
Multip in her 30s, obese 119kg, BMI 39.9. RAADP 500IU anti-D Ig x 2 (at 29 and 36 weeks gestation). ECV at 38 weeks gestation. Given 500IU anti-D Ig IM but no test for FMH performed. Baby delivered by elective CS at 40 weeks, Kleihauer negative, 500IU anti-D Ig given. Alloimmune anti-D found at booking in her subsequent pregnancy. The baby required intrauterine transfusion and exchange transfusion after delivery at 36 weeks gestation.

124
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
Comment: Following ECV, no sample was taken to measure size of FMH, and although a dose of prophylactic anti-D Ig was given, the woman became immunised.
Case 15.13: Alloimmunisation after correctly managed FMH
Multip in her 20s. Obese 96kg. Received RAADP (1500IU anti-D Ig at 30 weeks IM). Delivered by emergency CS in index pregnancy and had 4mL FMH and received postpartum prophylaxis (1500IU anti-D Ig IM). FMH volume was checked by flow cytometry and clearance of fetal cells was checked at 72 hours and was complete (as per guidelines). Follow up at 6 months showed woman had developed alloimmune anti-C, anti-D and anti-G.
Comment: Immunised after FMH at delivery.
Case 15.14: Placenta accreta
Multip in her 30s. Previous pregnancy managed correctly with no PSE, and anti-D Ig given as RAADP and PPP following emergency CS at 36 weeks. In index pregnancy anti-D was detected at 28 weeks but mistakenly assumed to be due to anti-D Ig given for RAADP (in fact the blood sample had been taken before anti-D Ig was given). Placenta accreta was diagnosed at 36 weeks and the woman was found to have a significant titre of anti-D (21.7IU/mL). The baby required phototherapy.
Comment: Do placenta accreta and other pathological placentae pose an increased risk of FMH in the absence of overt antepartum bleeding?
Case 15.15: Multiple risk factors: twin pregnancy, APH, obesity
Multip in her 30s. Weight 95kg, BMI 34. Index pregnancy complicated by twins, APH at 21 and 22 weeks for which she received anti-D Ig 500IU. RAADP given IM at 29 weeks (1500IU anti-D Ig). Alloimmune anti-D was first detected at 36+5 when the babies were delivered. The babies required phototherapy.
Comment: (as in 2016) Do twin pregnancies pose a higher risk of alloimmunisation during pregnancy as well as the recognised risk of increased FMH at delivery?
Case 15.16: Failed prophylaxis after TOP 10 years ago
Multip in her 20s. Weight 74.2kg, BMI 25.4. Surgical TOP 10 years previously, given anti-D Ig 250IU. Index pregnancy managed correctly with no PSE, and anti-D Ig given as RAADP (1500IU at 28+6 into deltoid muscle). No alloantibodies detected in booking or 28-week samples. Alloimmune anti-D was detected at delivery at 40+4. The baby required no interventions for HDFN.
Summary of 2017 PP data
• Eighteen women were found to be immunised at first trimester booking indicating that sensitisation had probably occurred in the preceding pregnancy. In 30 cases alloimmune anti-D was detected later in the index pregnancy so that the relative contribution of previous pregnancies is less clear
• Although the data has gaps, we continue to see cases where despite apparently ‘ideal’ care in preceding or index pregnancy, sensitisation to anti-D occurs and alloimmune anti-D develops
• Twelve of 43 of the previous pregnancies to term lasted longer than 40 weeks and cumulatively (data collected from 2015 onwards), 21 out of 101 previous pregnancies (20.8%) lasted longer than 40 weeks. NHS maternity statistics 2014-2015 indicate 17.5% pregnancies extended beyond 40 weeks http://content.digital.nhs.uk/catalogue/PUB19127
• Twelve of 25 PP cases where booking weight was known were obese and cumulatively of the 86 PP cases where booking weight was known 26/86 (30.2%) were obese

125
ERROR REPORTS: Human Factors ANNUAL SHOT REPORT 2017
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
Conclusion
The dataset continues to grow and 2017 had the largest annual number of immunisation cases reported to SHOT. Some cases can clearly be attributed to omission of anti-D Ig prophylaxis or testing for FMH. In other cases, the management appeared ideal but immunisation still occurred and it is these cases that require careful scrutiny to ensure current guidelines provide adequate prophylaxis.
Obesity was not seen in any NPP cases this year, but cumulatively since 2012, 7 of 41 (17.1%) NPP cases where the booking weight was known were obese. By contrast in this year’s reports, 12 of 25 PP cases where booking weight was known were obese and cumulatively of the 86 PP cases where booking weight was known 26/86 (30.2%) were obese. The important question as to whether obese women should receive anti-D Ig intravenously cannot yet be answered by the SHOT dataset.
The cumulative data both in NPP and PP begin to raise questions about pregnancies delivered beyond 40 weeks. There have been 26 NPP cases where alloimmune anti-D was detected only at delivery and 13 of these (50.0%) were delivered at >40 weeks. For PP cases, from 2015 onwards, 21 of the 101 previous pregnancies (20.8%) lasted longer than 40 weeks, and of 24 women where alloimmune anti-D was first detected at delivery in the index pregnancy, 9 cases (37.5%) were delivered after 40 weeks gestation. Cases where alloimmune anti-D was first detected at term will now be analysed in more detail by dividing the cases into four groups: early term (37-38+6 weeks), full term (39-40+6 weeks), late term (41-42 weeks) and post term (>42 weeks) and adding booking weight and age. This more detailed analysis may enable us to identify women who are at increased risk of developing alloimmune anti-D and who would benefit from an additional dose of anti-D Ig prophylaxis near term.
Several cases were reported this year where despite apparently adequate anti-D Ig prophylaxis women became immunised after a PSE, raising concerns that the current recommendations for prophylaxis may be inadequate, for example in medical termination where prophylaxis is not currently recommended. In addition, several cases highlight the continuing confusion around the correct management of PSE in early pregnancy. There is also a group of NPP women who may experience PSE in early pregnancy before they have been informed of their D-negative status and thus will not seek appropriate advice. There may be a case for informing all NPP (primips) of their D-negative status as soon as the result is available rather than waiting for their booking clinic visit at 16 weeks.
This year a case of placenta accreta was reported where, despite apparently ideal management, sensitisation occurred raising the possibility that placenta accreta, and possibly other pathological placentae, may increase the risk of occult FMH. Further work should be considered to clarify this risk.
The introduction of cffDNA analysis (NICE 2016) to identify pregnancies with D-negative babies (where the mother does not require prophylaxis with anti-D Ig), while reducing the unnecessary exposure of these women to blood products, has the potential to result in new types of error. SHOT has worked in collaboration with NHSBT to add additional questions to the alloimmunisation questionnaire specifically related to cffDNA testing. We hope to present the initial data in next year’s report.
All healthcare professionals, including laboratory staff, involved in the care of pregnant women must be encouraged to provide fully completed datasets on newly identified cases of anti-D immunisation in pregnancy, as the SHOT anti-D immunisation database may be the only way the important questions posed at the beginning of this chapter will be answered, particularly why women with apparently ideally managed pregnancies are still becoming immunised.
References
BSH Austin E, Bates S et al. Guidelines for the estimation of fetomaternal haemorrhage. 2009 http://www.b-s-h.org.uk/media/15705/transfusion-austin-the-estimation-of-fetomaternal-haemorrhage.pdf [accessed 25 January 2018].
BSH Qureshi H, Massey E et al. BSH guideline for the use of anti-D immunoglobulin for the prevention of haemolytic disease of the fetus and newborn. Transfus Med 2014;24(1):8-20. http://onlinelibrary.wiley.com/doi/10.1111/tme.12091/full [accessed 25 January 2018] Note: Royal College of Obstetricians and Gynaecologists green top guideline on use of anti-D has been archived and replaced by BSH guideline.

126
ANNUAL SHOT REPORT 2017 ERROR REPORTS: Human Factors
15. Immune Anti-D in Pregnancy: Cases reported up to the end of 2017
National Institute for Health and Care Excellence (NICE). Routine antenatal anti-D prophylaxis for women who are rhesus D negative. Technology Appraisal Guidance No. 156. 2008 https://www.nice.org.uk/Guidance/TA156 [accessed 21 March 2018].
National Institute for Health and Care Excellence (NICE). Ectopic pregnancy and miscarriage: diagnosis and initial management. Clinical guideline [CG154] 2012 https://www.nice.org.uk/guidance/cg154?unlid=971536770201642184428 [accessed 21 March 2018].
National Institute for Health and Care Excellence (NICE). High-throughput non-invasive prenatal testing for fetal RHD genotype. Diagnostic guideline (DG25) 2016 https://www.nice.org.uk/guidance/dg25/chapter/3-The-diagnostic-tests#.Wmn-lZGy-8E.email [accessed 21 March 2018].

127
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
REACTIONS IN PATIENTS
Serious adverse reactions (SAR) are defined for European Union (EU) reporting as follows:
Definition: an unintended response in a donor or in a patient that is associated with the collection, or transfusion of blood or blood components that is fatal, life-threatening, disabling or incapacitating, or which results in or prolongs hospitalisation or morbidity…blood establishments and the person responsible for the management of a hospital blood bank shall notify the Secretary of State (Competent Authority) of any serious adverse reactions observed during or after transfusion which may be attributable to the quality or safety of blood or blood components:
(i) Collected, tested, processed, stored or distributed by the blood establishment, or
(ii) Issued for transfusion by the hospital blood bank
These must be reported to the Medicines and Healthcare Products Regulatory Agency (MHRA). This is a legal requirement.
These are described under the following headings:
REACTIONS IN PATIENTS16 Febrile, Allergic and Hypotensive Reactions (FAHR) ...............................Janet Birchall and Fiona Regan17 Transfusion-Transmitted Infections (TTI) .......................................... Rachael Morrison and Su Brailsford18 Pulmonary Complications a. Transfusion-Related Acute Lung Injury (TRALI) ............................................................. Tom Latham b. Transfusion-Associated Circulatory Overload (TACO) ...........Sharran Grey and Paula Bolton-Maggs c. Transfusion-Associated Dyspnoea (TAD) .......................................................... Paula Bolton-Maggs19 Haemolytic Transfusion Reactions (HTR) ......................................Tracey Tomlinson and Anicee Danaee20 New or Unclassifiable Complications of Transfusion (UCT) ..................................... Paula Bolton-Maggs21 Cell Salvage (CS) .............................................................................Sarah Haynes and Catherine Ralph22 Paediatric Summary .............................................................................................................Helen New23 Haemoglobin Disorders: Update ............................................................................ Paula Bolton-MaggsAcknowledgements24 Medicines and Healthcare Products Regulatory Agency (MHRA) Report – available online only ............. ..........................................................................................................................................Chris Robbie
128134142144148154158165166170182186187

128 16. Febrile, Allergic and Hypotensive Reactions (FAHR)
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
Table 16.1:
Targeted treatment
for febrile and
allergic transfusion
reactions
Authors: Janet Birchall and Fiona Regan
Definition:
To reduce confusion, the title of this chapter has been changed to reflect the reactions assessed i.e. isolated febrile type (not associated with other specific reaction categories), allergic and hypotensive reactions occurring up to 24 hours following a transfusion of blood or components, for which no other obvious cause is evident.
Introduction
These reactions are classified according to the International Haemovigilance Network/International Society for Blood Transfusion (IHN/ISBT) definitions, which are summarised below in Table 16.2 (ISBT/IHN 2011), and have been adopted by the British Society for Haematology (BSH) (BSH Tinegate et al. 2012).
Key SHOT messages
• For febrile reactions alone, give paracetamol
• For allergic reactions give an antihistamine as first line; give adrenaline if anaphylaxis is suspected. The effect of steroids is delayed by several hours, will have no immediate effect, and should only be used to prevent a late recurrence. The use of steroids may further immunosuppress already immunocompromised patients and increase the risk of side effects such as infection
Key recommendations from previous years
• Platelets suspended in platelet additive solution (PAS) are associated with a reduction in allergic response (BSH Estcourt et al. 2017). Hospitals should consider preferential use of readily available pooled platelets suspended in PAS in patients with a history of allergic reactions. This should include paediatric patients where apheresis platelets are usually the platelet component of choice. If reactions continue, despite antihistamine cover, then platelets re-suspended in 100% PAS can be supplied
• Give appropriate targeted treatment and if needed, preventative cover for future transfusion (BSH Tinegate et al. 2012), as indicated in Table 16.1:
Reaction Treatment Prevention of recurrent reactions
Febrile Paracetamol Paracetamol 60 minutes before anticipated time of reaction
Allergic Antihistamine (steroid should not be used routinely)If anaphylaxis, adrenaline is essential
If previous reaction with apheresis platelets try pooled platelets in PASIf reactions continue, give pre-transfusion antihistamineIf reactions continue, consider washed platelets/red cells; for fresh frozen plasma (FFP) try a pooled component e.g. solvent-detergent treated plasma
Febrile, Allergic and Hypotensive Reactions (FAHR) n=28416

12916. Febrile, Allergic and Hypotensive Reactions (FAHR)
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
• Outpatient departments and day care units, including those in the community, should ensure patients have information about what to do if they experience a reaction after leaving the unit
• The treatment of reactions and management of subsequent transfusions should be directed by recognised guidelines e.g. BSH guidelines on the investigation and management of acute transfusion reactions (BSH Tinegate et al. 2012)
Action: Hospital Transfusion Teams (HTT)
• Reporters should report cases fully, including clinical data such as temperature and blood pressure prior to, and during, a reaction, especially if fever or hypotension are features. The International Haemovigilance Network/International Society for Blood Transfusion (IHN/ISBT) classification should be used to grade severity (Table 16.2)
• SHOT has a role in identifying trends in reactions and events, including the monitoring of new components. It is therefore important to identify the implicated component e.g. standard/washed red cells; pooled/apheresis and/or washed or human leucocyte antigen (HLA)-matched platelets; standard/virally inactivated (including type) plasma
Action: SHOT reporters
• Patients who have experienced transfusion reactions should only be tested for platelet or granulocyte antibodies within guidelines such as those set out in England by the National Health Service Blood and Transplant (NHSBT) in their Histocompatibility and Immunogenetics user guide (NHSBT 2015/16). The main indication, other than platelet refractoriness, is persistence of severe reactions despite the use of platelets where the plasma has been removed and replaced by suspension medium
Action: HTT, Histocompatibility and Immunogenetics laboratories
• Transfusions should only be performed where there are facilities to recognise and treat anaphylaxis, according to UK Resuscitation Council (UKRC) guidelines (Resuscitation Council 2008). This recommendation is also relevant for other transfusion-related emergencies such as respiratory distress caused by transfusion-associated circulatory overload (TACO) or transfusion-related acute lung injury (TRALI). When supplying to community hospitals or for home transfusions, providers must ensure that staff caring for patients have the competency and facilities to deal with reactions. This is particularly relevant in the light of proposals to increase patient treatment outside secondary care
Action: HTT, Royal College of General Practitioners

130 16. Febrile, Allergic and Hypotensive Reactions (FAHR)
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
1 = Mild 2 = Moderate 3 = Severe
Febrile-type reaction
A temperature ≥38°C and a rise between 1 and 2°C from pre-transfusion values, but no other symptoms/signs
A rise in temperature of 2°C or more, or fever 39°C or over and/or rigors, chills, other inflammatory symptoms/signs such as myalgia or nausea which precipitate stopping the transfusion
A rise in temperature of 2°C or more, and/or rigors, chills, or fever 39°C or over, or other inflammatory symptoms/signs such as myalgia or nausea which precipitate stopping the transfusion, prompt medical review AND/OR directly results in, or prolongs hospital stay
Allergic type reaction
Transient flushing, urticaria or rash
Wheeze or angioedema with or without flushing/urticaria/rash but without respiratory compromise or hypotension
Bronchospasm, stridor, angioedema or circulatory problems which require urgent medical intervention AND/OR, directly result in or prolong hospital stay, or anaphylaxis (severe, life-threatening, generalised or systemic hypersensitivity reaction with rapidly developing airway and/or breathing and/or circulation problems, usually associated with skin and mucosal changes)
Reaction with both allergic and febrile features
Features of mild febrile and mild allergic reactions
Features of both allergic and febrile reactions, at least one of which is in the moderate category
Features of both allergic and febrile reactions, at least one of which is in the severe category
Hypotensive reaction
Isolated fall in systolic blood pressure of 30 mmHg or more occurring during or within one hour of completing transfusion and a systolic blood pressure 80 mmHg or less in the absence of allergic or anaphylactic symptoms. No/minor intervention required
Hypotension, as previously defined, leading to shock (e.g. acidaemia, impairment of vital organ function) without allergic or inflammatory symptoms. Urgent medical intervention required
Number of reactions and reaction rates n=284
Deaths n=0
There were no deaths related to the transfusion reaction.
Major morbidity n=71
Reactions have been classified as shown in Table 16.3. Severe reactions, as classified above, are used to define major morbidity.
Moderate Severe Total
Febrile 119 21 140
Allergic 55 44 99
Mixed allergic/febrile 30 5 35
Hypotensive 9 1 10
Total 213 71 284
NB: in 25 of the 71 reactions classified as severe this was primarily because the patient was admitted
The percentage of severe reactions remains similar to previous years, 71/284 (25.0%) of all reactions. Many reactions, largely of febrile type, continue to be difficult to classify because of insufficient information, the IHN/ISBT grade of reaction not being used and because of the difficulty distinguishing true transfusion reactions from symptoms and signs associated with the patient’s underlying condition.
Table 16.4 identifies the total number of cases submitted for review into the category of FAHR over the last 4 years and demonstrates that the percentage of cases excluded is consistent. The number of cases included in the report is therefore correlated to the total number of cases reported.
Table 16.2:
Classification of
reactions
Table 16.3:
Classification of
FAHR in 2017

13116. Febrile, Allergic and Hypotensive Reactions (FAHR)
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
Cases reported 2014 2015 2016 2017
Total reported 434 407 357 390
Included 312 296 253 284
Excluded (withdrawn or unclassifiable) 122 111 104 106
% Excluded 28.1% 27.3% 29.1% 27.2%
The incidence of allergic reactions linked to pooled platelets (suspended in PAS) continues to be lower than the incidence of allergic reactions linked to apheresis platelets and this is likely associated with the reduction in plasma content (Cohn et al. 2014, Tobian et al. 2014). The incidence of febrile reactions continues to be higher with pooled platelets compared to apheresis. Overall pooled platelets are associated with fewer reactions than apheresis platelets as the incidence of febrile reactions to platelets is lower than allergic reactions (Figures 16.1a and b). Reactions to platelets are at least in part caused by release of substances from the platelets themselves and therefore cannot be completely eliminated (Garraud et al. 2016, Maurer-Spurej et al. 2016).
a: Febrile type reactions b: Allergic reactions
0.0182 0.01850.0169
0.0245
0.0321
0.0163
0.0129
0.0069
2014 2015 2016 2017
Rea
ctio
ns a
s a
% o
f un
its is
sued
ApheresisPooled
0.0039
0.0058
0.0024
0.0046
0.01170.0133
0.0065
0.0100
2014 2015 2016 2017
Rea
ctio
ns a
s a
% o
f un
its is
sued
ApheresisPooled
Type of reaction by component
These remain similar to previous Annual SHOT Reports; Figure 16.2. Red cells are usually associated with febrile type reactions (~70%) whereas plasma and platelets more commonly cause allergic reactions (~80% and ~60% respectively). Three reactions were associated with solvent detergent (SD)-FFP and there were no reactions associated with methylene-blue treatment.
HLA=human leucocyte antigen; cryo=cryoprecipitate
Per
cent
age
of
reac
tions
Component type
119
21
12
33
73
11
22
74
17 12 4
1
18 2
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Red cells (167)
Platelets (90)
Plasma/cryo (18)
Granulocytes (1)
Multilple components
(8)
HypotensiveMixed allergic/febrileAnaphylactic/severe allergicModerate allergicFebrile
Each star represents a case of:HLA-matched plateletsWashed red cellsSolvent-detergent plasma
HLA=human leucocyte antigen; cryo=cryoprecipitate
Table 16.4:
Total FAHR cases
reviewed over a
4-year period
Figures 16.1:
Percentage of
reactions to
apheresis and
pooled platelets
2014 to 2017
Figure 16.2:
Reactions by
component type

132 16. Febrile, Allergic and Hypotensive Reactions (FAHR)
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
Analysis of the characteristics of reactions remains comparable to those in previous years.
Characteristic Occurrence
Age distribution About 90% of patients were aged 18 years or over
Gender 45% male and 55% female cases
Urgency of transfusion 66% were given routinely
Timing of transfusion 46% occurred within standard hours
Location 59% were on wards and 14% in outpatient/day-case units
Treatment of reactions
An antihistamine with or without steroid continues to be used to treat reactions with only febrile/inflammatory type symptoms and/or signs however this practice may be reducing; Table 16.6. In addition to no evidence of benefit, the use of steroids may further immunosuppress already immunocompromised patients and increase the risk of side effects such as infection.
Number Medication stated Antihistamine +/- steroid
Febrile
2017 140 121/140 (86.4%) 46/121 (38.0%)
2016 124 102/124 (82.3%) 51/102 (50.0%)
2015 142 101/142 (71.1%) 57/101 (56.4%)
2014 144 97/144 (67.4%) 42/97 (43.3%)
Number Medication stated Paracetamol
Allergic
2017 99 97/99 (98.0%) 10/97 (10.3%)
2016 107 101/107 (94.4%) 11/101 (10.9%)
2015 122 106/122 (86.9%) 10/106 (9.4%)
2014 139 112/139 (80.6%) 14/112 (12.5%)
Following a purely febrile reaction, in cases where information about subsequent plans for management were provided, a lower percentage (22.7%) than in previous years (42.9% in 2016) planned to use an antihistamine with or without steroids. However, the numbers of reporters providing these data were small. It is notable that future treatment with pooled platelets was much more commonly stated to avoid allergic reactions than in previous years.
Illustrative cases
This year cases have been selected to demonstrate good practice.
Case 16.1: A febrile reaction appropriately treated with paracetamol
A patient in their 80s received a red blood cell transfusion to treat ongoing non-severe bleeding associated with a haemoglobin (Hb) of about 80g/L. After 100mL had been transfused (30–60 minutes) the patient experienced rigors, an increase in respiratory rate and the temperature was noted to have risen from a baseline of 36.6°C to 38.3°C. There were no other symptoms or signs. The transfusion was initially slowed and then discontinued. Paracetamol was prescribed and the patient’s observations returned to baseline. Bacterial cultures from the patient at the time of the reaction were negative. No change in management was planned for any subsequent blood transfusion.
Case 16.2: A febrile reaction to red cells. To receive iron as future management of iron deficiency anaemia
A patient with menorrhagia and Hb of 50g/L was transfused with red cells. After the first unit her post-transfusion observations identified a pyrexia of 39.6°C (an increase of more than 2°C from baseline) and tachycardia of 120 beats/minute. She was given treatment which included paracetamol and
Table 16.5:
Characteristics of
FAHR
Table 16.6:
Treatment of
reported reaction

13316. Febrile, Allergic and Hypotensive Reactions (FAHR)
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
made a complete recovery with observations returning to baseline over 1-4 hours. Repeat serology was negative and future management was planned with intravenous iron and avoidance of blood transfusion.
Case 16.3: Allergic reaction to apheresis platelets with planned transfusion of pooled platelets suspended in PAS for future management
A child with reversible bone marrow failure and thrombocytopenia received apheresis platelets prior to an operation. Within 10 minutes of the start of the transfusion, periorbital oedema, wheezing and a fall in oxygen saturations to 92% on air occurred. Oxygen therapy, hydrocortisone, chlorphenamine and salbutamol nebuliser were given with complete recovery within 1-4 hours. Investigation did not identify IgA deficiency and mast cell tryptase remained within the normal range. The patient had experienced previous mild reactions to apheresis platelets and so it was agreed that in future platelets suspended in PAS would be used to reduce the risk of a further allergic reaction.
References
BSH Estcourt LJ, Birchall J et al on behalf of the British Committee for Standards in Haematology. Guidelines for the use of platelet transfusions. Br J Haematol 2017;176(3):365-394.
BSH Tinegate H, Birchall J et al. Guideline on the investigation and management of acute transfusion reactions. Prepared by the BCSH Blood Transfusion Task Force. Br J Haematol 2012;159(2):143-153.
Cohn CS, Stubbs J et al. A comparison of adverse reaction rates for PAS C versus plasma platelet units. Transfusion 2014;54(8):1927-34, doi/10.1111/trf.12597.
Garraud O, Tariket S et al. Transfusion as an inflammation hit: knowns and unknowns. Front Immunol 2016;7:534. eCollection 2016.
ISBT/IHN Haemovigilance Working Party of the ISBT: Proposed standard definitions for surveillance of non-infectious adverse transfusion reactions. 2011 http://www.ihn-org.com/wp-content/uploads/2011/06/ISBT-definitions-for-non-infectious-transfusion-reactions.pdf. [accessed 31 March 2018].
Maurer-Spurej E, Larsen R et al. Microparticle content of platelet concentrates is predicted by donor microparticles and is altered by production methods and stress. Transfus Apher Sci 2016;55(1):35-43, doi/10.1016/j.transci.2016.07.010.
NHSBT Histocompatibility and Immunogenetics diagnostic services user guide.2015/16 http://hospital.blood.co.uk/diagnostic-services/diagnostic-user-guides/ [accessed 31 March 2018].
Resuscitation Council. Emergency treatment of anaphylactic reactions 2008. http://www.resus.org.uk/pages/reaction.pdf [accessed 31 March 2018].
Tobian AA, Fuller AK et al. The impact of platelet additive solution apheresis platelets on allergic transfusion reactions and corrected count increment (CME). Transfusion 2014;54(6):1523-9; quiz 1522 doi/10.1111/trf.12498.

134
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
17. Transfusion-Transmitted Infections (TTI)
Authors: Rachael Morrison and Su Brailsford
Definition of a TTI:
A report was classified as a transfusion-transmitted infection if, following investigation:
• The recipient had evidence of infection following transfusion with blood components, and there was no evidence of infection prior to transfusion, and no evidence of an alternative source of infection
and either:
• At least one component received by the infected recipient was donated by a donor who had evidence of the same transmissible infection
or:
• At least one component received by the infected recipient was shown to contain the agent of infection
Note that for the purposes of the European Union (EU) legislation, serious adverse reactions (SAR) are defined as any reactions in patients that are ‘life-threatening, disabling or incapacitating, or which result in or prolong hospitalisation or morbidity.’
These must be reported to the Medicines and Healthcare Products Regulatory Agency (MHRA) (a legal requirement). This includes all confirmed transfusion-transmitted infections.
Introduction
This chapter describes the possible TTI incidents investigated by the United Kingdom (UK) Blood Services and reported to the National Health Service Blood and Transplant (NHSBT)/Public Health England (PHE) Epidemiology Unit in 2017.
Summary of reports made to the NHSBT/PHE Epidemiology Unit in 2017
During 2017, UK Blood Services investigated 106 suspected bacterial cases and 8 suspected viral incidents (Figure 17.1). From these suspected cases, there has been:
• One confirmed transfusion-transmitted hepatitis A virus (HAV) incident reported by the Scottish National Blood Transfusion Service (SNBTS)
• One confirmed transfusion-transmitted hepatitis E virus (HEV) incident from NHSBT
• One probable transfusion-transmitted HEV incident from NHSBT
• One possible Staphylococcus capitis bacterial transfusion-transmitted incident from SNBTS
Further information about how and what to report can be found in ‘SHOT Bite No. 7 Transfusion-transmitted infections’ at www.shotuk.org/resources/current-resources/.
Transfusion-Transmitted Infections (TTI) n=117

135
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
17. Transfusion-Transmitted Infections (TTI)
114reports for investigation
106suspected bacterial
incidents investigated
89concluded post
transfusionreactions with no
evidence of bacteriaon investigation
5concluded
NOT viral TTI(2 CMV, 3 HCV)
1concluded
PROBABLE viralTTI (1 HEV)
2concluded
viral TTI(1 HAV, 1 HEV)
9concluded
NOTbacterial TTI
7concluded
indeterminatebacterial
incidents**
1concludedPOSSIBLE
bacterial TTI
suspected viral incidentsreported and investigated
*Hepatitis C virus (HCV) investigations where the transfusion was prior to screening are not included in the above figure (1 HCV incidentreported in 2017, transfusion pre-1991)
**No packs to test but investigation based on information received indicates unlikely to reflect a TTI
TTI=transfusion-transmitted infection; CMV=cytomegalovirus; HEV=hepatitis E virus; HAV=hepatitis A virus
Major morbidity n=1
A patient with a confirmed case of transfusion-transmitted HAV suffered a serious reaction (Case 17.4) after being transfused in 2017.
Bacterial TTI reports 2017
In 2017, no reported suspected bacterial TTI were confirmed, but 1 incident reported by the SNBTS is assigned as possible. The four UK Blood Services all use the BacTALERT system for bacterial screening which has had an impact on the number of confirmed bacterial TTI (McDonald et al. 2017). Each country uses slightly different sampling methods which are described in Table 17.1.
Case 17.1: Possible case: (Morbidity: Major; Imputability: 1-possible)
A 3-day old pooled platelet unit was transfused to a female patient in her 50s who was receiving a second cycle of chemotherapy for relapsed acute myeloid leukaemia (AML). She had a history of a perianal abscess and neutropenic fever, was reported as pyrexial prior to transfusion, and had been given antibiotic prophylaxis. Four hours post transfusion her condition worsened, she was found collapsed, confused, septic with a temperature of 40°C, hypoxic, and hypotensive with a tachycardia. She remained pyrexial over the following week and was treated with broad spectrum antibiotics; she continued to improve and recovered well. Bacterial screening signalled a reactive result after the pack had been transfused, and Staphylococcus capitis was isolated from the initial pouch sample and the anaerobic culture bottle, but the transfused unit was unavailable for culture. Blood cultures were taken from the patient but these results were not available to the Blood Service. The significant symptoms and persistent fever post transfusion resulted in the case being reported as a bacterial TTI although the symptoms may have been related to the patient’s underlying condition. On the basis of these results this incident is reported as a possible TTI.
Figure 17.1:
Outcome of reports
of suspected
TTI made to the
NHSBT/PHE
Epidemiology Unit
in 2017*

136
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
17. Transfusion-Transmitted Infections (TTI)
Bacterial TTI 1996–2017
Screening of platelet components cannot guarantee freedom from bacterial contamination. Packs are released for issue as ‘negative-to-date’, which may be before bacteria have multiplied sufficiently to trigger an initial screening reaction. There have been 8 bacterial near misses, all but 1 in platelet components, reported to the PHE Epidemiology Unit between 2011 and 2017. Overall, out of a total of 44 bacterial transfusion-transmissions to individual recipients, 37 (34 incidents) have been caused by the transfusion of platelets, and 7 by red cells (Table 17.3) since reporting began.
Haemovigilance systems for bacterial TTI are passive and as such rely on clinical colleagues to report suspected TTI. Following the introduction of bacterial screening of platelets, colleagues were reminded that there was still the possibility of TTI occurring from both platelet and red cell transfusion and the number of reported suspected TTI has remained almost constant. Current British Society for Haematology (BSH) guidance recommends that patients are advised to report any symptoms that occur within 24 hours of transfusion (BSH Tinegate et al. 2012) although our experience suggests that patients with confirmed TTI become unwell very rapidly.
Time of sampling (hour)
Volume sampled (mL)
Apheresis sample
Time at release (hour)
Length of screening
NHSBT 36 2 x 8 Post-split 6 Day 7
NIBTS 48 2 x 8 Pre-split 6 Day 9
SNBTS 18 2 x 7 Pre-split 6 Day 7
WBS 16 2 x10 Pre-splitFrom start of
screeningDay 7*
*Additional 10mL sample taken at day 4 to extend shelf-life from 5 to 7 days
NIBTS=Northern Ireland Blood Transfusion Service; WBS=Welsh Blood Service
Time of sampling: time samples are taken from the pack for screening in hours after donation is made
Apheresis sample: two or three packs may be manufactured from one donation, NHSBT sample each pack i.e. 2 or 3 packs
Time at release: time bottles remain on the machine before packs are released as negative
Viral TTI reports 2017
In 2017, there was 1 probable transfusion-transmitted HEV incident, 1 confirmed transfusion-transmitted HEV incident and 1 confirmed transfusion-transmitted HAV incident.
Case 17.2: Probable viral HEV TTI case 1: (Morbidity: Major; Imputability: 2-probable)
A male patient in his 60s received a transfusion of one platelet pool and one apheresis platelet in mid-2015 prior to a prostate biopsy. Platelets were given due to the patient’s low platelet count ascribed to significant alcohol intake. The patient developed acute hepatitis 2 months later and was found to have chronic liver disease with portal hypertension. Further investigations revealed hepatocellular carcinoma. The patient deteriorated due to liver failure and died 2 months after the transfusion. A blood sample which was taken a day prior to the patient’s demise was confirmed to be anti-HEV IgM positive and IgG positive, indicating recent HEV infection.
Archive samples of the five donations (four donors from the platelet pool donation and one from the apheresis pool donation) were retrieved and tested for HEV ribonucleic acid (RNA). The four platelet pool donation samples were confirmed as HEV RNA-negative, but the apheresis platelet donation was HEV RNA-positive, with a viral load of 2044IU/mL. The associated platelet split had been transfused and the clinical team looking after this patient were informed of the potential risk of HEV transmission.
Since there was no remaining blood sample from the patient to refer for HEV RNA testing, it was not possible to prove conclusively that the recipient virus was identical to the donor virus. Therefore, it has been concluded that the infection was probably acquired through transfusion.
Table 17.1:
Bacterial screening
methods used
by the UK Blood
Services

137
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
17. Transfusion-Transmitted Infections (TTI)
Case 17.3: Confirmed viral HEV TTI case 2: (Morbidity: Major; Imputability: 3-confirmed)
A male patient in his 60s received multiple plasma exchanges with fresh frozen plasma (FFP) as treatment for focal segmental glomerulosclerosis (FSGS) which he developed after renal transplant in November 2014. Between January and July 2015, he received 238 units of FFP. He was discharged to his home country.
In March 2017 the patient was noted to have developed ascites over 6 months and portal hypertension was diagnosed. On further investigation the patient was found to be HEV RNA-positive. A sample was referred to the Virus Reference Department at Public Health England which confirmed the HEV RNA result with a viral load of 1,500,000IU/mL, and a genotype 3 virus. The patient was also found to be HEV IgM positive and IgG positive. Testing of stored patient samples confirmed that the HEV infection was present at completion of, but not prior to, the plasma exchange therapy. The patient had therefore developed chronic HEV infection, dating from at least August 2015, on a background of immunosuppression following a renal transplant. The patient subsequently developed multi-organ failure and died.
Patient samples predating each cycle of plasma exchange were tested for HEV RNA; it was found that all samples up to mid-March were HEV RNA-negative, whereas those from May 2015 were HEV RNA-positive. An investigation was therefore carried out into the 59 units of FFP transfused in late March. Archive samples were retrieved and tested: 57 were HEV RNA-negative, one sample was insufficient for testing and one was identified as HEV RNA-positive, IgM- and IgG-negative, indicating early acute HEV infection in the donor at the time of donation. Sequence analysis indicated that the viruses in the donor and recipient samples (both genotype 3c) were likely to be linked and therefore this case is confirmed as a TTI.
An associated red cell pack from the same donation did not result in transmission, probably due to low levels of virus in the pack.
This case has been added to the number of confirmed TTI for 2015 in Table 17.3.
Case 17.4: Confirmed viral HAV TTI case 3: (Morbidity: Major; Imputability: 3-confirmed)
Hepatitis A is usually transmitted by contaminated food and water, although other routes have been identified including sexual transmission and blood transfusion. Outbreaks of hepatitis A were identified during 2017 in adults across the UK, including one associated with a bakery in Scotland. The last confirmed report of hepatitis A transfusion transmission was in 2005.
An apheresis platelet donor felt unwell 2 days prior to donation but recovered and attended to donate. The following day the donor again felt unwell and developed dark urine but no jaundice. A week after donation the donor was hospitalised with acute hepatitis A infection. On investigation, it was found that the donor had visited the bakery linked to a hepatitis A outbreak.
Investigation of the issued platelet doses was carried out. One recipient, a female in her 50s with renal cancer, neutropenic sepsis and a low platelet count, was transfused with one apheresis platelet unit. Post transfusion, the patient had evidence of hepatitis A immunity (HAV IgG, but no HAV IgM detected), with transient HAV RNA positivity. Sequence analysis indicated that the viruses in the donor and recipient samples were likely to be linked and therefore this TTI is confirmed. Sadly, the patient died of her underlying disease.
Health Protection Scotland and SNBTS worked together to ensure that no other donors potentially affected by the outbreak donated for a 6-month period, and sessions were cancelled in the areas affected by the HAV outbreak. The Public Health services in England and Scotland have modified their hepatitis A questionnaire for patients and contacts to ask an additional question about recent blood donation. Public health teams will notify their Blood Service if patients answer ‘yes’ to this question to allow appropriate actions to be taken.

138
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
17. Transfusion-Transmitted Infections (TTI)
Update on viral TTI reports investigated in 2016
Of the 2 pending HEV cases in 2016, 1 case was found to be probable viral HEV TTI and 1 was a confirmed viral HEV TTI.
Case 17.5: Probable HEV viral TTI 2016 case 1: (Morbidity: Major; Imputability: 2-probable)
A male patient in his late teens received blood transfusions between December 2013 and January 2014 in association with a liver transplant. He received four units of red cells, 12 units of FFP, two units of apheresis platelets and two platelet pool donations, equivalent to 26 donor exposures. In 2015, the patient developed persistent transaminitis and tested HEV RNA-positive in October 2015.
Records of all donors were examined; all except two had donated at least once since the donation transfused to the patient. An archive sample of a follow-up donation from each of the 24 returning donors was retrieved: 18 tested HEV IgG-negative and six were HEV IgG-positive, indicating prior HEV infection. For two of these donors the index archive was available and tested HEV RNA-negative. Given the time elapsed since the transfused donations there was no index archive sample available for the other four donors whose follow-up sample was HEV IgG positive, nor for the two donors who did not re-attend. Therefore, it was possible to eliminate 20 of the 26 donors as a source of HEV infection. Five of the six remaining donors contributed FFP and the final one contributed platelets as part of a platelet pool. Due to lack of archive samples for these six donors it was not possible to assess when the four donors known to have become HEV IgG-positive may have acquired their hepatitis E infection, nor confirm if they were the source of the hepatitis E infection in the patient, however it was assessed that this was likely to be a probable transfusion-transmitted infection.
Case 17.6: Confirmed HEV viral TTI 2016 case 2: (Morbidity: Major; Imputability: 3-confirmed)
A male in his 60s diagnosed with myelodysplastic syndrome (MDS), had an allogeneic stem cell transplant, and received blood transfusions from late 2014 to mid-2015. A deterioration in liver function test results in early 2016 led to HEV testing; the patient was HEV IgM-positive, IgG not detected. The patient received 66 units of red cells, 33 units of apheresis platelets and 14 platelet pools during this time, with 155 donor exposures. Archive samples of all the donations were retrieved and tested for HEV RNA. One donation was identified as HEV RNA-positive with a viral load of 2,000,000IU/mL. The platelets and plasma from this donation were used in preparation of a platelet pool which was transfused to the patient. Sequence analysis indicated that the viruses in the donor and recipient samples were likely to be linked and therefore this TTI is confirmed. The associated red cell unit was transfused to an immunocompetent patient; the clinical team looking after this patient was informed of the HEV status of the donation.
This case has been added to the number of confirmed TTI for 2015 in Table 17.3.
Viral TTI 1996–2017
The year of transfusion may be many years prior to the year in which the case is investigated and reported to SHOT because of the chronic nature, and therefore late recognition, of some viral infections. Since 1996, 33 confirmed incidents of transfusion-transmitted viral infections have been documented, involving 40 recipients. Hepatitis B virus (HBV) is the most commonly reported proven viral TTI in the UK. This is partly because the ‘window period’ where an infectious donation from a recently infected donor cannot be detected by the screening tests is longer than for HCV or human immunodeficiency virus (HIV), despite nucleic acid (NAT) screening of blood donations.
Residual risk of HBV, HCV or HIV
The risks of a potentially infectious HBV, HCV or HIV window period donation not being detected on testing in the UK are very low at less than 1 per million donations tested (Table 17.2) (PHE 2016).

139
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
17. Transfusion-Transmitted Infections (TTI)
HBV HCV HIV
Number per million donations 0.47 0.010 0.06
95% confidence interval 0.08-1.06 0.00-0.05 0.02-0.12
At 2.3 million donations per year testing will miss a potentially infectious window period donation every:
1.02 years 46 years 7 years
*The window period is the time at the start of an infection before the tests can detect it
Far fewer TTI are observed in practice than the estimated risks in Table 17.2 indicate, partly because the estimates have wide uncertainty and the model used to calculate risk is based on the risk in all donations tested. The model does not incorporate pack non-use, recipient susceptibility to infection, or under-ascertainment/under-reporting, for example due to recipients dying from an underlying medical condition before a chronic asymptomatic viral condition is identified, or, in the case of HBV, an asymptomatic acute infection.
Testing update: 2017
SNBTS began 100% HEV screening of donations from 1 March 2017. NHSBT implemented 100% screening of blood donations from 10 April 2017, followed by the other Blood Services. HEV screening for non-blood donors (stem cell, tissues and organs) went live in NHSBT on 2 October 2017.
NHSBT changed human T-cell lymphotropic virus (HTLV) screening from universal to selective (new donors and donations that will be used for non-leucodepleted blood components) in January 2017.
Parasitic TTI
There were no reported parasitic infections for investigation in 2017. There have been two proven malaria TTI reported to SHOT, the last in 2003 (Table 17.3). Malaria antibody testing according to information supplied at donation was not applicable at the time, and the donor selection guidelines were updated after these incidents to minimise the risk of further malaria TTI (Kitchen et al. 2005). The current selection guidelines on deferral and additional testing for malaria can be accessed at the UK transfusion guidelines web pages at http://www.transfusionguidelines.org.uk/red-book.
Variant Creutzfeld-Jakob Disease (vCJD) 2016
There were no vCJD investigations in 2016.
vCJD 1996-2017
Three vCJD incidents (Table 17.3) took place prior to the introduction of leucodepletion and other measures taken by the UK Blood Services to reduce the risk of vCJD transmission by blood, plasma and tissue products. All these measures have been reviewed and endorsed by the Advisory Committee on the Safety of Blood, Tissues and Organs (SABTO) (SABTO 2013). Risk assessment and research into vCJD continues. Currently there is no suitable blood test available for screening blood donations for vCJD. More information can be found here: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/407681/measures-vcjd.pdf.
Table 17.2:
The estimated risk
of a potentially
infectious HBV,
HCV or HIV window
period* blood
donation not
detected on testing,
UK 2014-2016

140
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
17. Transfusion-Transmitted Infections (TTI)
Year of transfusion**
Number of incidents (recipients) by infection Implicated component
Bac
teri
a
HA
V
HB
V
HC
V**
*
HE
V
HIV
HT
LV I
Par
vovi
rus
(B19
)
Mal
aria
vCJD
/ p
rio
n
Tota
l
RB
C
Po
ole
d
pla
tele
t
Ap
here
sis
pla
tele
t
FFP
Cry
o
Pre 1996 - - 1 (1) - - - 2 (2) - - - 3 (3) 3 - - - -
1996 - 1(1) 1 (1) 1 (1) - 1 (3) - - - 1 (1) 5 (7) 5 1 - 1 -
1997 3 (3) - 1 (1) 1 (1) - - - - 1 (1) 2 (2) 8 (8) 6 1 1 - -
1998 4 (4) - 1 (1) - - - - - - - 5 (5) 2 1 2 - -
1999 4 (4) - 2 (3) - - - - - - ‡ (1) 6 (8) 5 3 - - -
2000 7 (7) 1 (1) 1 (1) - - - - - - - 9 (9) 1 5 3 - -
2001 5 (5) - - - - - - - - - 5 (5) 4 1 - -
2002 1 (1) - 1 (1) - - 1 (1)† - - - - 3 (3) 2 1 - - -
2003 3 (3) - 1 (1) - - - - - 1 (1) - 5 (5) 1 1 3 - -
2004 †† - - - 1 (1) - - - - - 1 (1) 1 - - - -
2005 2 (2) 1 (1) 1 (1) - - - - - - - 4 (4) 1 3 - - -
2006 2 (2) - - - - - - - - - 2 (2) - 1 1 - -
2007 3 (3) - - - - - - - - - 3 (3) 2 1 - - -
2008 4 (6) - - - - - - - - - 4 (6) - 2 4 - -
2009 2 (3) - - - - - - - - - 2 (3) 1 - 2 - -
2010 - - - - - - - - - - - - - - - -
2011 - - 1 (2) - 1 (2) - - - - - 2 (4) 2 - - 2 -
2012 - - 1 (1) - 1 (1) - - 1(1) - - 3 (3) 2 - - 1 -
2013 - - - - - - - - - - - - - - - -
2014 - - - - 2 (3) - - - - - 2 (3) 1 - - 2 -
2015 1(1) - - - 4 (5) - - - - - 5 (6) - 3 1 1 1
2016 - - - - 1 (1) - - - - - 1 (1) 1 - - - -
2017 - 1(1) - - - - - - - - 1 (1) - - 1 - -
Number of incidents
41 4 12 2 10 2 2 1 2 3 79
Number of infected recipients
44 4 14 2 13 4 2 1 2 4 90 36 27 19 7 1
Death due to, or contributed to, by TTI
11 0 0 0 1 0 0 0 1 3 16
Major morbidity 29 3 14 2 8 4 2 1 1 1§ 65
Minor morbidity 4 1 0 0 4 0 0 0 0 0 9
Implicated component
RBC 7 1 11 2 4 2 2 1 2 4 36
Pooled platelet 21 2 1 - 2 1 - - - - 27
Apheresis platelet 16 1 1 - 1 - - - - - 19
FFP - - 1 - 5 1 - - - - 7
Cryoprecipitate - - - - 1 - - - - - 1
Note: Numbers in brackets refer to recipients, and probable incidents are excluded.
* No screening was in place for vCJD, HTLV, HAV, HEV or parvovirus B19 at the time of the documented transmissions. In both malaria transmissions, malaria antibody testing was not applicable at the time according to information supplied at donation
** Year of transfusion may be prior to year of report to SHOT due to delay in recognition of chronic infection
*** HCV investigations where the transfusion was prior to screening are not included in the above figure.
† The two HIV incidents were associated with window period donations (anti-HIV negative/HIV RNA-positive) before HIV NAT screening was in place. A third window period donation in 2002 was transfused to an elderly patient, who died soon after surgery. The recipient’s HIV status was therefore not determined and not included
†† In 2004 there was an incident involving contamination of a pooled platelet pack with Staphylococcus epidermidis, which did not meet the TTI definition because transmission to the recipient was not confirmed, but it would seem likely. This case was classified as ‘not transfusion-transmitted’
‡ Same blood donor as one of the 1997 transmissions so counted as the same incident; note: counted as two separate incidents in previous reports
Table 17.3:
Number of confirmed
TTI incidents*, by
year of transfusion**
with total infected
recipients and
outcomes (death,
major morbidity, minor
morbidity) in the UK
between October 1996
and December 2017
(Scotland included
from October 1998)

141
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
17. Transfusion-Transmitted Infections (TTI)
§ A further prion case died but transfusion was not implicated as the cause of death. The outcome was assigned to major morbidity instead because although there was post-mortem evidence of abnormal prion proteins in the spleen the patient had died of a condition unrelated to vCJD and had shown no symptoms of vCJD prior to death
For further information or alternative breakdown of data please contact the National Coordinator for Transfusion Transmitted Infections via the NHSBT/PHE Epidemiology Unit at [email protected].
References
BSH Tinegate H, Birchall J et al. Guideline on the investigation and management of acute transfusion reactions. Prepared by the BSH Blood Transfusion Task Force. Br J Haematol 2012;159(2):143-153.
Kitchen AD, Barbara JA, et al. Documented cases of post-transfusion malaria occurring in England: a review in relation to current and proposed donor-selection guidelines. Vox Sang 2005;89:77-80.
McDonald C, Allen J et al. Bacterial screening of platelet components by National Health Service Blood and Transplant, an effective risk reduction measure. Transfusion 2017;57:1122–1131; doi/10.1111/trf.14085.
PHE. NHSBT/PHE Epidemiology Unit: Safe Supplies: A baseline for change. Annual Review from the NHS Blood and Transplant/Public Health England Epidemiology Unit, 2016. https://www.gov.uk/government/publications/safe-supplies-annual-review [accessed 18 January 2018].
SABTO. Measures currently in place in the UK to reduce the potential risk of transmitting variant Creutzfeldt-Jakob disease via blood. 2013. https://www.gov.uk/government/publications/current-measures-to-reduce-the-risk-of-vcjd-transmission-by-blood [accessed 18 January 2018].

142
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
18. Pulmonary Complications
Author: Paula Bolton-Maggs
Pulmonary complications remain a serious outcome of transfusion, particularly for elderly patients with comorbidity. The distinction between the three categories, transfusion-related acute lung injury (TRALI), transfusion-associated circulatory overload (TACO) and transfusion-associated dyspnoea (TAD) remains fluid, as demonstrated by the number of reports that were moved between these categories. Ten cases were moved from TACO to TAD, 4 from TRALI to TAD, 2 from TAD to TACO and 1 from TRALI to TACO. An international group, including representatives from SHOT, the International Society of Blood Transfusion (ISBT), the International Haemovigilance Network (IHN) and the American Association of Blood Banks (AABB), has continued to review reporting criteria for TACO. A revised definition of these has progressed with validation studies, and these were reviewed at a 1-day meeting in November 2017. The pathophysiology of the pulmonary complications of transfusion is not well understood. In parallel with this, another group is reviewing the definition of TRALI. A workshop is planned for autumn 2018 to review the state of knowledge of TRALI, TACO and TAD accepting that there are gaps in knowledge and overlap between these three entities. There is great interest in the role of the glycocalyx (Brettner et al. 2017). Other relevant references: (Force et al. 2012, Juffermans and Vlaar 2017, Morsing et al. 2018, Toy et al. 2016).
The refined SHOT definitions for TRALI and TACO have resulted in an increase of cases moved to TAD. Reporters are strongly encouraged to keep notifying cases of respiratory distress even when it is not clear to which category these belong, but also to record as much detail as possible. Reporting of dyspnoea in the febrile, allergic and hypotensive reactions (FAHR) category triggers additional questions which request information about fluids, whether there is a history of lung, renal or cardiac disease together with other factors which may help to understand the pathology of this particular reaction. Advice is given in the British Society for Haematology (BSH) guidelines on action to take in the event of acute transfusion reactions (BSH Tinegate et al. 2012). These are not only allergic/febrile reactions but incorporate any adverse reactions that occur in the first 24 hours.
A national comparative audit of TACO was undertaken in the UK in 2017 with collection of data from more than 4000 patients over 60 years of age. More than 80% of these patients had additional risk factors for TACO (other than their age) but less than 1% were identified as such (Morton et al. 2017). Awareness needs to be improved and the use of the TACO checklist is encouraged.
If a patient develops a reaction, or becomes breathless, stop the transfusion, maintain venous access with saline, undertake rapid clinical assessment and call for assistance if necessary. For patients at risk of TACO careful clinical assessment of cardiac status and fluid balance should be documented before the transfusion is started. The respiratory rate should be monitored throughout transfusion (NICE 2015, BSH Robinson et al. 2018). The oxygen saturations should also be measured in patients identified at risk of TACO. Patients with renal dysfunction and those with positive fluid balance prior to transfusion are also at risk of TACO. Measurement of B-natriuretic peptide (BNP) before and after a transfusion reaction may be helpful in establishing a diagnosis of TACO (Zhou et al. 2005) and has been considered as one of the diagnostic criteria for TACO but this is not widely performed or available in the UK.
Pulmonary Complications18

143
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
18. Pulmonary Complications
TRALI=transfusion-related acute lung injury; TACO=transfusion-associated circulatory overload; TAD=transfusion-associated dyspnoea
59
41
7 5 4 30
3
18
3440
71
82
9691 89
8692
14
35 35
19
6 73
10
20
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
TADTACOTRALI
TRALI=transfusion-related acute lung injury; TACO=transfusion-associated circulatory overload; TAD=transfusion-associated dyspnoea
References
Brettner F, von Dossow V and Chappel D. The endothelial glycocalyx and perioperative lung injury. Curr Opin Anaesthesiol 2017;30:36-41.
BSH Robinson S, Harris A et al. The administration of blood components: a British Society for Haematology Guideline. Transfus Med 2018;28(1):3-21. http://onlinelibrary.wiley.com/doi/10.1111/tme.12481/pdf [accessed 23 March 2018].
BSH Tinegate H, Birchall J et al. Guideline on the investigation and management of acute transfusion reactions Prepared by the BCSH Blood Transfusion Task Force. Br J Haematol 2012;159:143-153.
Force ADT, Ranieri VM et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA 2012;307:2526-2533.
Juffermans NP and Vlaar AP. Possible TRALI is a real entity. Transfusion 2017;57:2539-2541.
Morsing KSH, Peters AL et al. The role of endothelium in the onset of antibody-mediated TRALI. Blood Rev 2018;32:1-7.
Morton S, Grant-Casey J et al. Skating on thin ice: national audit of TACO demonstrates poor recognition of risk factors. Blood 2017;130 Suppl 1:2406.
NICE Guideline NG24 Blood transfusion 2015 https://www.nice.org.uk/guidance/ng24/chapter/Recommendations#alternatives-to-blood-transfusion-for-patients-having-surgery-2 [accessed 19 March 2018].
Toy P, Kleinman SH and Looney MR. Reply to concerns regarding dropping the term ‘possible TRALI’. Transfusion 2016;56:2394-2395.
Zhou L, Giacherio D et al. Use of B-natriuretic peptide as a diagnostic marker in the differential diagnosis of transfusion-associated circulatory overload. Transfusion 2005;45:1056-1063.
Figure 18.1:
Reports of
pulmonary
complications by
year 2010-2017

144
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
18a. Transfusion-Related Acute Lung Injury (TRALI)
Author: Tom Latham
Definition:
Transfusion-related acute lung injury (TRALI) is defined as acute dyspnoea with hypoxia and bilateral pulmonary infiltrates during or within 6 hours of transfusion, in the absence of circulatory overload or other likely causes, or in the presence of human leucocyte antigen (HLA) or human neutrophil antigen (HNA) antibodies cognate with the recipient.
There were 3 confirmed cases of TRALI this year. Eleven cases were reported as suspected TRALI, 4 cases were transferred to transfusion-associated dyspnoea (TAD), 1 case to transfusion-associated circulatory overload (TACO) and 3 cases were withdrawn.
TRALI=transfusion-related acute lung injury
5
21 1 1
0
2
0 0 01 1
3
0 0
24
14
7
3
11
5
9
4
1
7
54
3
0
3
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Number of deathsConfirmed TRALI cases
TRALI=transfusion-related acute lung injury
Figure 18a.1 shows TRALI cases from 2003 to 2017, reclassified using the criteria introduced in the 2016 Annual SHOT Report. The use of male donors only for fresh frozen plasma (FFP) was implemented in 2003. Cases are recorded as deaths if death was at least ‘possibly’ related to transfusion (imputability 1 or greater).
Assessment of TRALI
The classification criteria are outlined in Table 18a.1 below. A mapping of how the revised criteria compare to the widely used Canadian Consensus definitions for TRALI is given in Table 18a.3, in order to help international comparison.
Figure 18a.1:
Number of
suspected TRALI
cases and deaths
at least possibly
related to TRALI by
year of report
Transfusion-Related Acute Lung Injury (TRALI) n=318a

145
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
18a. Transfusion-Related Acute Lung Injury (TRALI)
Classification DefinitionMapping to Canadian Consensus definition
Highly likelyCases with a convincing clinical picture and positive serology
TRALI + positive serology
ProbableCases with positive serology but other coexisting morbidity which could independently cause acute lung injury or fluid overload
Possible TRALI (pTRALI) + positive serology
EquivocalCases with positive serology in the clear presence of lung injury due to other causes or fluid overload
not TRALI [excluded because of other morbidity but meets positive criteria] + positive serology
Antibody-negative TRALI
Cases with a convincing clinical picture where serology is not available or negative
TRALI + absent or negative serology
Unlikely- reclassify as TAD
Cases where the picture and serology was not supportive of the diagnosis. These cases are transferred to TAD
pTRALI or not TRALI + negative or absent serology
Probability Number of cases
Highly likely 0
Probable 1
Equivocal 1
Antibody-negative 1
Unlikely (transferred to TAD/TACO) 5
Table 18a.2 includes notified cases which have been transferred to other categories but not cases which have been withdrawn.
Canadian Consensus classification Number of cases
TRALI 1
Possible TRALI 1
Not TRALI 1
Table 18a.3 includes only cases classified as TRALI - withdrawn or transferred cases would by definition be classified as ‘Not TRALI’.
Case histories
Case 18a.1: Antibody-negative TRALI - a possible role for HLA cross-reactivity?
A <10-year-old girl with acute lymphocytic leukaemia (ALL) attended as an outpatient for a prophylactic platelet transfusion. Thirty minutes after transfusion of a unit of pooled platelets, the patient suffered acute vomiting, abdominal pain, acute tachypnoea, and desaturated to 70% on air. The chest X-ray showed a complete white-out. The patient required intubation and ventilation but subsequently made a complete recovery. The patient had previously been well and there were no clinical features of fluid overload or additional fluids.
One male donor had HLA antibodies against HLA-A25, -A34, -A66, -A68; the recipient typed as HLA-A2;A26.
This case has been classified as ‘antibody-negative TRALI’ based on a classical history and absence of alternative explanations. However, although the antibodies are not cognate with the recipient it is noted that they are in the same ‘cross-reactive group’. Cross-reactive groups (CREG) denote operationally monospecific HLA antisera that react with two or more HLA antigens due to public epitopes that are differentially shared among HLA class I gene products (Focosi 2014). In this case, A2 (recipient) and A68 (donor antibody) are in the same CREG group and A26 (recipient) is in the same group as A25, A34 and A66 (donor).
Table 18a.1:
Revised SHOT criteria
for assessment of
TRALI cases
Table 18a.2:
TRALI case
probability (SHOT
criteria) 2017 cases
Table 18a.3:
Classification using
Canadian Consensus
definitions

146
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
18a. Transfusion-Related Acute Lung Injury (TRALI)
HLA cross-reactivity has not been reported as having an association with TRALI but has a moderate effect on platelet refractoriness. It is therefore feasible that there could be a causative relationship for TRALI.
Case 18a.2: Probable TRALI
A female teenager developed acute respiratory deterioration, hypoxia and bilateral patchy air space shadowing 4 hours after transfusion of red cells. The transfusion was given for anaemia 2 days after a liver transplant for Alagille syndrome. She had a positive fluid balance and impaired renal and cardiac function secondary to the underlying syndrome although these had not caused functional compromise. She required ventilation but made a complete recovery.
The red cell donor had HNA-1a antibodies which were cognate with the recipient.
The case was classified as ‘probable TRALI’ in view of the positive serology and the treating clinician’s impression that fluid overload was unlikely, however the patient also had coexisting risk factors for fluid overload which therefore cannot be ruled out.
Case 18a.3: Equivocal TRALI
A female patient in her 60s was already under prolonged ventilation following oesophageal surgery complicated by a perforated oesophagus and splenic rupture and she was also recovering from postoperative sepsis. She developed increased oxygen requirements and deterioration in the chest X-ray (CXR) following a transfusion of two units of red cells. There was pre-existing pulmonary oedema on a CXR prior to the transfusion, but this was worse after transfusion and a computerised tomography (CT) scan showed patchy ground-glass shadowing within the lung fields in keeping with acute respiratory distress syndrome (ARDS).
Investigation of the donors showed that both red cell donors had HLA class 1-specific antibodies, in particular to HLA-A2. The patient also had the cognate HLA-A2 antigen.
This case has been classified as ‘equivocal TRALI’ - it is practically impossible to assign causation retrospectively in the presence of pre-existing lung injury, infection and fluid overload but the presence of cognate antibodies in both donors raises the possibility of TRALI as a causative or contributory factor.
Cumulative serological data
Since 1996, 207/327 (63.3%) reported cases have had full laboratory investigation for TRALI. Concordant antibodies were identified in 118/207 (57.0%) of these. The most frequently identified antibody specificities (either alone or in combination with other concordant antibodies) have been HLA-DR4 (22/118 cases, 18.6%), HLA-DR52 (17/118, 14.4%) and HLA-A2 (19/118, 16.1%). All other HLA antibody specificities have been identified in less than 10% of cases. Concordant HNA specific antibodies, alone or in combination, have been found as follows: HNA-1a (10/118 cases, 8.5%); HNA-2 (2/118, 1.7%); HNA-3a (2/118, 1.7%).
Analysis of reports of 187 complete TRALI investigations between 2001 and 2017 inclusive has shown that the specificities of concordant antibodies were as follows:
Concordant donor antibodies 2001 to 2017 inclusive
HLA class I alone HLA class II alone Both HLA class I and HLA class II
Granulocyte-specific antibody (+/- HLA antibodies)
None identified
21/187 (11.2%) 36/187 (19.3%) 27/187 (14.4%) 19/187 (10.2%) 84/187 (44.9%)
Table 18a.4:
Concordant donor
antibodies 2001 to
2017 inclusive

147
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
18a. Transfusion-Related Acute Lung Injury (TRALI)
Commentary
Three confirmed cases of TRALI were reported this year, including 1 delayed report of a case from 2016. This number is comparable to the annual incidence over the last decade. The revised classification, as intended, gives a better proportion of cases where TRALI is thought to be at least a possible explanation for the clinical picture.
Part of the motivation for including the presence of leucocyte antibodies in the definition used by SHOT is to be able to monitor the effectiveness of TRALI prevention measures. In the 3 confirmed cases, all components transfused were consistent with TRALI-reduction measures (male donor FFP and screening of parous female platelet donors). Case 18a.1 is a reminder that male donors can have HLA antibodies and that it is worthwhile testing male donors for antibodies if there is a high clinical suspicion of TRALI.
The question raised by Case 18a.1 of whether HLA cross-reactivity could cause TRALI needs further investigation. The most direct way of demonstrating that antibodies in the donor are reactive with the recipient would be to perform a lymphocyte crossmatch. While this is logistically difficult to arrange, it is suggested that this would be a useful addition to the investigation of suspected TRALI cases. For the moment, it is proposed to continue classifying cases with cross-reactive but not matching antibodies in the ‘antibody-negative TRALI’ category so that they can receive additional scrutiny.
Blood Centres should consider performing a lymphocyte crossmatch in suspected transfusion-related acute lung injury (TRALI) cases where donors are found to have human leucocyte antigen (HLA) antibodies in the same cross-reactive group as the recipient.
References
Focosi D. HLA nomenclature 2014. http://www.ufrgs.br/imunovet/molecular_immunology/hla.html#CREG [accessed 15 April 2018].

148
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
18b. Transfusion-Associated Circulatory Overload (TACO)
Authors: Sharran Grey and Paula Bolton-Maggs
The reporting criteria for TACO have been revised by a joint working group from the International Society of Blood Transfusion (ISBT) haemovigilance working party, the International Haemovigilance Network (IHN) and American Association of Blood Banks (AABB) with wide international consultation. SHOT has continued to be a key contributor and collaborator in this work. Validation of the revised criteria took place throughout 2017.
An international consensus conference was the ultimate objective of the working party following validation of the reporting criteria. The working party recognised that the revised reporting criteria are an important improvement and will likely be further revised as research advances. The revision group is planning to finalise the validation and publish the criteria to make them available for use in due course. The validation process and expert discussions highlighted significant gaps in knowledge of TACO pathogenesis and diagnosis, and for this reason a consensus conference will be deferred until these issues can be more satisfactorily addressed. However, it was recognised that a workshop to appraise current and ongoing research would be valuable for future planning.
Experts agreed that delineating the current categories of pulmonary complications is problematic and there is likely considerable overlap. It is important this does not act as a barrier in reporting to SHOT. Transfusion-associated dyspnoea (TAD) is an essential category for capturing these cases.
Key SHOT message
• Patients who develop respiratory distress during or up to 24 hours after transfusion where transfusion is suspected to be the cause must be reported to SHOT. The transfusion-associated circulatory overload (TACO) definition criteria can be used as guidance but this should not be restrictive. SHOT experts can transfer cases between categories
Recommendation
• A formal pre-transfusion risk assessment for transfusion-associated circulatory overload (TACO) should be undertaken whenever possible, as TACO is the most commonly reported cause of transfusion-related mortality and major morbidity
Action: All staff authorising transfusion
Transfusion-Associated Circulatory Overload (TACO) n=9218b

149
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
18b. Transfusion-Associated Circulatory Overload (TACO)
If ‘yes’ to any of these questions
• Review the need for transfusion (do the benefits outweigh the risks)?
• Can the transfusion be safely deferred until the issue can be investigated, treated or resolved?
• Consider body weight dosing for red cells (especially if low body weight)
• Transfuse one unit (red cells) and review symptoms of anaemia
• Measure the fluid balance• Consider giving a prophylactic
diuretic• Monitor the vital signs closely,
including oxygen saturation
TACO Checklist Red cell transfusion for non-bleeding patients
Does the patient have a diagnosis of ‘heart failure’ congestive cardiac failure (CCF), severe aortic stenosis, or moderate to severe left ventricular dysfunction?
Is the patient on a regular diuretic?
Is the patient known to have pulmonary oedema?
Does the patient have respiratory symptoms of undiagnosed cause?
Is the fluid balance clinically significantly positive?Is the patient on concomitant fluids (or has been in the past 24 hours)?Is there any peripheral oedema?Does the patient have hypoalbuminaemia?Does the patient have significant renal impairment?
Due to the differences in adult and neonatal physiology, babies may have a different risk for TACO. Calculate the dose by weight and observe the notes above.
Recommendation
• Use weight-adjusted red cell dosing to guide the appropriate number of units required for all non-bleeding adult patients, ideally using tools which also highlight inappropriate transfusion (Grey et al. 2018)
Action: All staff authorising transfusion
Deaths n=7
Two of the 7 deaths were clearly related to transfusion. One of these cases had major gastrointestinal haemorrhage while anticoagulated. Serial full blood counts showed the patient was overtransfused/over-resuscitated with red cells and died following development of pulmonary oedema. The patient in the other case had a history of left ventricular failure and received two units of red cells for symptomatic relief of anaemia. The patient developed pulmonary oedema during the second unit and died within an hour of transfusion. The remaining deaths were in patients who all had pre-existing comorbidities that are known risks for circulatory overload.
Major morbidity n=20
Sixteen of the 20 cases of major morbidity had evidence of pre-existing fluid overload, pulmonary oedema, comorbidities predisposing to circulatory overload and/or were also receiving significant volumes of non-blood fluids and were therefore at risk of TACO. Two cases had no apparent risk factors for TACO but had received large volumes of blood components, and in 1 case there was evidence of over-estimation of haemorrhage. There were only 2 cases where TACO developed with no apparent risk factors reported.
Figure 18b.1:
TACO pre-
transfusion
checklist

150
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
18b. Transfusion-Associated Circulatory Overload (TACO)
Demographic overview of cases
Demographic Number of reports
Deaths (imputability 3) 2
Deaths (imputability 2) 4
Deaths (imputability 1) 1
Major morbidity (serious sequelae) 0
Major morbidity (minor sequelae) 3
Major morbidity (signs and symptoms with risk to life with full resolution/unknown outcome)
17
AgeRange 3-97 years Median 77 years
Specialties
Haematology=18Acute medicine=17Intensive therapy unit (ITU)/anaesthetics=6Adult surgical specialties=13Other adult medical specialties=31Paediatrics=1Obstetrics=1Other specialties/unknown=5
Bleeding patients (indication code R1 or ‘massive bleeding’ indicated)
15
Non-bleeding patients (other indication codes or not stated) 77
In agreement with previous years, the demographic analysis shows that TACO is more commonly reported in the older population and where transfusion is given for anaemia rather than bleeding. Haematology and adult medical specialties are again the most common specialties where TACO is reported.
Analysis by definition criteria
This year’s data have been analysed using the draft TACO reporting criteria developed by the joint working group described in the introduction (ISBT 2017). These criteria are summarised below:
Patients classified as having TACO (surveillance diagnosis) should have acute or worsening respiratory compromise during or up to 12 hours after transfusion (SHOT accepts cases up to 24 hours after transfusion) and should exhibit two or more of the criteria below:
• Evidence of acute or worsening pulmonary oedema based on clinical physical examination and/or radiographic chest imaging and/or other non-invasive assessment of cardiac function e.g. echocardiogram
• Evidence of cardiovascular system changes not explained by the patient’s underlying medical condition, including development of tachycardia, hypertension, jugular venous distension, enlarged cardiac silhouette and/or peripheral oedema
• Evidence of fluid overload including any of the following: a positive fluid balance; response to diuretic therapy combined with clinical improvement; and change in the patient’s weight in the peri-transfusion period
• Elevation in B-type natriuretic peptide (BNP) levels (e.g. BNP or N-terminal (NT)-pro BNP) to greater than 1.5 times the pre-transfusion value. A normal post-transfusion BNP level is not consistent with a diagnosis of TACO; serial testing of BNP levels in the peri-transfusion period may be helpful in identifying TACO
These criteria establish a surveillance definition based on a complete description of an event, including information that becomes available well after onset. This is for reporting and tracking purposes and the criteria do not constitute clinical diagnosis for the purpose of real-time clinical interventions.
Table 18b.1:
Demographics of
reported TACO
cases

151
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
18b. Transfusion-Associated Circulatory Overload (TACO)
TACO=transfusion-associated circulatory overload
2
4346
1
1 2 3 3 (late onset)
Number of TACO criteria met
TACO=transfusion-associated circulatory overload
Ninety-two reports were accepted into the TACO category. Eighty-nine (96.7%) met the revised surveillance criteria for TACO (89/92). In 1 of the 3 cases that did not strictly meet the criteria the timing of onset of symptoms was reported as 12-24 hours after transfusion. On review of the case the patient had received a large volume transfusion over a long period of time, which highlights the need for standardisation of the timing of symptom onset in relation to transfusion and is discussed further below. The 2 other cases scored only one criterion. One patient had pulmonary oedema following a large volume transfusion for haemorrhage, however due to lack of unanticipated cardiovascular parameter changes, no fluid balance record, no record of diuretic therapy and BNP not tested, only one criterion was met in an otherwise clinically compelling scenario. The other patient had received only a single unit of red cells and developed pulmonary oedema. In the absence of fluid balance measurement, lack of unanticipated cardiovascular parameter changes, failure to improve with diuretic therapy and BNP not tested, this case did not fully meet the new criteria. Although the patient had chronic underlying pulmonary pathology, the clinical scenario suggested that on balance the pulmonary oedema was probably precipitated by transfusion in this patient with risk factors for circulatory overload (renal impairment and requirement for regular diuretic medication).
The new criteria focus on the pathophysiology of circulatory overload based on the effects on cardiovascular and pulmonary systems. Pro-inflammatory features are being increasingly recognised in cases of pulmonary complications of transfusion. Whether these are purely circulatory overload, an overlapping syndrome or another unidentified entity is not understood. The two previous years’ data have been analysed in the context of fever to explore this further.
Fever in cases reported and categorised as TACO
Author: Harriet Lucero
There is a recognised association between TACO and fever. The incidence was reported as 45/107 (42.1%) cases of TACO in a retrospective review (Parmar et al. 2017). Fever was defined as a temperature rise >1oC to reach >38oC and/or rigors or chills. Another study reported febrile or inflammatory symptoms in 65/97 (67.0%) cases of TACO (Andrzejewski et al. 2012).
A review of cases reported to SHOT in 2015 and 2016 showed that fever was a symptom in 34/164 (20.7%) cases reported as TACO. ‘Fever’ is not defined in the TACO questionnaire; it is a yes/no answer. In 15/34 (44.1%) cases with fever no alternative explanation for the fever was provided. In the cases where potential alternative explanations existed the patients were already on antibiotics or were being treated for infection prior to the transfusion.
Figure 18b.2:
Analysis of reports
by the revised
surveillance
diagnosis criteria

152
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
18b. Transfusion-Associated Circulatory Overload (TACO)
If there are respiratory signs or symptoms suggestive of TACO, then the presence of fever does not exclude the diagnosis. This is reflected in the revised TACO surveillance diagnosis criteria (ISBT 2017). Research continues into the potential inflammatory processes involved in pulmonary oedema associated with transfusion.
Timing of TACO symptoms
Author: Harriet Lucero
TACO is generally considered to occur within 6 hours of transfusion, but SHOT has accepted cases within 24 hours of transfusion. Part of the revision work on the international surveillance criteria for TACO includes the timing of the reaction. The revised ISBT surveillance definition (ISBT 2017) is ‘during or up to 12 hours after transfusion’.
All cases reported to SHOT between 2010 and 2016 where the timing of reaction was reported to be greater than 6 hours have been reviewed (Table 18b.2). A total of 83/555 (15.0%) of TACO cases were reported as being 6 hours or more after transfusion by the reporting organisation. Review of these shows that the ‘time of transfusion’ is often recorded as the time the first unit was started.
Certainly, in the case of multiple red cell transfusions, the total transfusion time will be more than 6 hours. Many of the cases analysed experienced a reaction during the transfusion or shortly after completion. Cases categorised as ‘unclear’ are where the data submitted were insufficient to reach a firm conclusion.
Time given for symptom onset by reporting hospital
Time of symptom onset from end of transfusion following review of the full data set
<6 hours 6-12 hours 12-24 hours unclear >24 hours
6-12 hours 53 31 16 6
12-24 hours 30 10 4 8 5 3
A small number of patients experienced delayed reactions beyond 12 hours and 3 cases occurred beyond 24 hours, 2 of which were following outpatient transfusions and the timing of symptom onset was therefore potentially prior to the time of presentation to hospital.
The analysis demonstrates the need for an internationally agreed standard for the timing of the onset of TACO in relation to the transfusion episode.
Illustrative cases
Case 18b.1: An inappropriate transfusion leading to TACO and cancelled elective surgery
A patient in their 90s was admitted for an elective total knee replacement. The patient’s haemoglobin (Hb) was 95g/L and weight was 73kg. Two units of red cells were prescribed for preoperative Hb optimisation. A Hb check was not performed between units and a fluid balance chart was not in place. At the end of the second unit the patient had dyspnoea and was hypoxic, with hypertension and tachycardia. The chest X-ray was suggestive of pulmonary oedema and the post-transfusion Hb was 128g/L. The patient responded to diuretic therapy. The patient’s surgery was cancelled due to TACO.
Preoperative Hb optimisation should take place prior to admission where anaemia is identified, investigated and treated following surgical pre-assessment. Red cell transfusion is rarely appropriate except in occasional circumstances, for example where a patient has chronic bleeding or marrow impairment leading to anaemia that cannot be controlled medically.
Notwithstanding this, the patient in this case had a pre-transfusion Hb level that exceeded the trigger for transfusion and transfusion resulted in an excessive Hb level. The development of TACO then unfortunately led to the patient being discharged following recovery without having their surgery.
Table 18b.2:
Timing of reported
TACO cases

153
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
18b. Transfusion-Associated Circulatory Overload (TACO)
Case 18b.2: Lack of attention to appropriate red cell dose leads to TACO
A patient in their 90s weighing 75kg with a newly diagnosed haematological condition was admitted with sepsis and a Hb level of 79g/L. The patient was known to have heart failure, renal impairment and peripheral oedema and therefore had risk factors for circulatory overload. Two units of red cells were prescribed with prophylactic diuretics. During transfusion of the second unit the patient became breathless, began coughing up frothy sputum, developed bilateral crackles, tachycardia and hypertension. The chest X-ray was consistent with pulmonary oedema.
The root-cause analysis and preventive actions decided by the reporting hospital focused on future slow-rate transfusion, prophylactic diuretics and improved fluid balance measurement. Although these are important factors, the rate of transfusion in this case was not excessive (2-4 hours per unit) and diuretics were administered, suggesting TACO would not have been avoided in this scenario. However, the dose of red cells prescribed was not questioned as part of the root-cause analysis. Based upon a calculation of 0.4mL/kg raising the Hb level by 1g/L, this patient required less than a single unit of red cells to meet their target Hb. A weight-adjusted dose may have avoided TACO in this patient which developed during transfusion of the second unit.
Case 18b.3: Inappropriate and excessive transfusion causing TACO in a patient without risk factors for circulatory overload
A patient in their 50s weighing 67kg was prescribed six units of red cells for iron deficiency anaemia after being admitted with Hb 37g/L. The patient had no risk factors for TACO except for profound anaemia. During the fifth unit the patient became dyspnoeic, hypoxic and hypertensive. The patient recovered after diuretic therapy and had a post-transfusion Hb level of 100g/L.
Blood transfusion in iron deficiency anaemia is only appropriate as initial treatment if the patient is symptomatic. This patient was likely to be symptomatic with profound anaemia however the dose should have been limited to one or two units to resolve symptoms. The decision-making for this case appears to be aimed at a ‘back to normal’ Hb level with no attempt to treat the iron deficiency. Although a root-cause analysis was undertaken by the reporting hospital, much of the preventive action was focused on national education for junior medical staff and local implementation of the TACO checklist. Although these are important measures this case of TACO could have been avoided by a local policy of single unit or weight-adjusted red cell dosing. The transfusion laboratory has an important role in identifying and avoiding excessive and/or inappropriate transfusion.
References
Andrzejewski C Jr, Popovsky M et al. Hemotherapy bedside biovigilance involving vital sign values and characteristics of patients with suspected transfusion reactions associated with fluid challenges: can some cases of transfusion-associated circulatory overload have pro-inflammatory aspects? Transfusion 2012;52(11):2310-20.
Grey S, Farrar K et al. A web-App for weight-adjusted red cell dosing: post-development implementation and clinical effectiveness. Br J Haematol 2018;181 Suppl 1:146.
ISBT (2017). TACO reporting criteria (April 2017) draft for validation. http://www.isbtweb.org/fileadmin/user_upload/TACO_reporting_criteria_April_2017_draft_for_validation.docx [accessed 4 January 2018].
Parmar N, Pendergrast J et al. The association of fever with transfusion-associated circulatory overload. Vox Sang 2017;112(1):70-78.

154
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
18c. Transfusion-Associated Dyspnoea (TAD)
Author: Paula Bolton-Maggs
Definition:
TAD is characterised by respiratory distress within 24 hours of transfusion that does not meet the criteria for transfusion-related acute lung injury (TRALI) or transfusion-associated circulatory overload (TACO) or allergic reaction. Respiratory distress in such cases should not be adequately explained by the patient’s underlying condition (International Society of Blood Transfusion (ISBT) definition).
Twenty cases are included, 8 males and 12 females. Five were reported as TAD, 10 transferred from TACO, 1 from febrile, allergic and hypotensive reactions (FAHR) and 4 from TRALI. Two cases were transferred from TAD to TACO. Four patients suffered major morbidity defined by admission to intensive therapy units (ITU). Seven patients died, and in 5 cases the reaction was considered contributory. The age range was 15 to 93 years with a median age of 71 years. In 6 cases (30.0%) ‘sepsis’ was flagged and it is likely that this contributed to the reaction. Most reactions occurred in relation to red cells either alone, n=15, or with other components n=2. One reaction each was reported for platelets, granulocytes and plasma.
Key SHOT messages
• Pulmonary reactions to transfusion are difficult to classify, often because these occur in elderly patients with significant comorbidity. They may have features to suggest transfusion-associated circulatory overload (TACO) but cannot be classified as TACO if the data are incomplete (particularly missing information about fluid balance, and post-reaction chest X-ray (CXR) to confirm presence or absence of pulmonary oedema)
• TRALI is considered within 6 hours of transfusion in the absence of circulatory overload or other likely causes, or in the presence of human leucocyte antigen (HLA) or human neutrophil antigen (HNA) antibodies cognate with the recipient. Some cases of acute lung injury will therefore be reported as, or transferred to TAD
TACO and TAD have been included in SHOT reporting from 2008 together with a pulmonary questionnaire intended to capture as much information as possible about the event. This followed the introduction of TAD as a category by ISBT.
There is no clear international agreement on what TAD is, and the definitions of both TACO and TRALI are currently under international review. The use of more stringent criteria for both TACO and TRALI, and the absence of data in many fields contributes to the increase in number accepted as TAD compared to previous years.
The cases of TAD resulting in death and major morbidity are summarised below. The other 11 cases are available in the supplementary information provided for this Annual Report (by chapter) on the SHOT website www.shotuk.org.
Transfusion-Associated Dyspnoea (TAD) n=2018c

155
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
18c. Transfusion-Associated Dyspnoea (TAD)
Deaths n=5
Case 18c.1: Acute severe reaction to transfusion
A lady in her 80s was transfused for anaemia after a fall and minor head injury resulting in bleeding from the scalp (on a background of iron deficiency anaemia). The plan was to give a single unit of red cells then follow this with an iron infusion the next day. She was being treated for an infective exacerbation of chronic obstructive pulmonary disease. She had renal impairment and a low albumin. Within 5 minutes of transfusion starting she developed a worsening wheeze and became agitated, had an increase in respiratory rate from 24 to 44 breaths per minute (/min), and was immediately treated for anaphylaxis with adrenaline, hydrocortisone and chlorphenamine, and intravenous (IV) fluids with some improvement, and later given furosemide with further improvement. She died 2 days later.
The clinicians were unable to decide if this was an allergic reaction or circulatory overload but in view of the clinical history she was more likely to have overload, but there was not enough evidence to classify this as TACO. The patient was already acutely unwell before the transfusion started (history of deterioration since starting treatment for a chest infection at home with increased confusion culminating in a fall). They considered that transfusion may have contributed to her death.
Case 18c.2: A frail elderly woman developed pulmonary symptoms related to transfusion
A woman in her 90s received regular red cell transfusions for myeloproliferative disease. She had community-acquired pneumonia with acute kidney injury. She was already very frail, and was drowsy on admission with Hb 59g/L. The respiratory rate was 25-26/min, oxygen saturation was 94-95% on 2L of oxygen. Blood pressure (BP) was 110/60mmHg and she had tachycardia 100-105/min. At the end of the second unit the respiratory rate increased to 30/min with a fall in oxygen saturation to 76% but no significant change in BP or pulse. She was reviewed by the doctor who reported peripheral oedema and raised jugular venous pressure. Furosemide treatment did not give any benefit. She died the following day and transfusion was considered as a possible contributing factor.
Case 18c.3: A man with leukaemia and fungal chest infection died after transfusion
An elderly man with acute myeloid leukaemia (AML) received a unit of red cells and a unit of platelets as part of a regular transfusion regime. He had received six cycles of chemotherapy. He also had interstitial lung disease was very unwell with pulmonary aspergillosis with a progressive cavity, new consolidation, poor left ventricular function (ejection fraction 22%) with a pericardial effusion and cardiac failure. He went home after the transfusion, and 9 hours after the end of the transfusion (01:25) the patient became breathless and was coughing. He arrested and was pronounced dead in hospital at 03:09.
The case was reported to the coroner who decided that the death was from ‘natural causes and rare complications from necessary treatment’.
Case 18c.4: A man with liver disease reacted to cryoprecipitate (transfer from TRALI)
A man in his 40s with a known history of alcohol abuse and liver cirrhosis was admitted to the intensive therapy unit with a variceal bleed. His Hb was 71g/L and platelet count was 43x109/L with coagulopathy. He received several blood components (three units of red cells, two units of platelets, four units of fresh frozen plasma (FFP)) prior to two units of cryoprecipitate (cryo). Before he received the cryo he was self-ventilating on room air, respiratory rate was 25/min and oxygen saturation was >94%. After starting the cryo there was an abrupt deterioration in his gas exchange resulting in emergency intubation and ventilation. His post-intubation CXR showed marked (new) bilateral interstitial infiltrates. Prior to the transfusion of cryo the central venous pressure (CVP) was 13mmHg and his fluid balance was 3L positive over 36 hours. He had received a total of 1.4L of crystalloid in the 24 hours prior to his intubation. The remainder of his positive fluid balance represented blood component support. An echocardiogram performed later in his admission showed a normal left ventricle with an estimated ejection fraction of 60% and normal right ventricular function. He received a total of 300mg of furosemide in bolus doses over the 24 hours after intubation. This had

156
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
18c. Transfusion-Associated Dyspnoea (TAD)
no appreciable effect on his gas exchange and he continued to require very high levels of ventilatory support with FiO2 consistently greater than 60% with mean airway pressures around 20cm of water.
Advice was sought from the TRALI panel with the following response: ‘There is very significant liver impairment and big bleed with massive transfusion (and almost certainly a lot of crystalloid infusion as well). These patients are notoriously volume- and sodium ion-intolerant and this is TACO with extremely low possibility of TRALI’. It appears that no antibody investigations were performed. The clinical team remained of the view that this was TRALI. He remained on the ventilator and died 8 days after this event. The reporters concluded that death was ‘possibly related’ to the transfusion of cryoprecipitate.
Case 18c.5: A complex case with sudden deterioration in relation to transfusion requiring admission to ITU and ventilation
A man in his 60s with peripheral vascular disease received a postoperative (debridement of necrotic foot) transfusion for anaemia (Hb 76g/L). He was already on antibiotics and was a known diabetic. Transfusion of the first unit was uneventful. Three hours after starting the second unit his heart rate rose from 125 to 142/min, blood pressure increased from 120/65 to 154/83 and oxygen saturation fell from 98% to 95% with increase in respiratory rate from 20 to 29/min. His temperature increased from 36.5 to 37.5oC. A doctor found him to be breathless, with audible wheeze, no crepitations on auscultation but pulse irregularly irregular and vomiting. Electrocardiogram (ECG) confirmed fast atrial fibrillation. Critical care outreach review took place and blood tests including cultures were taken. Portable CXR: consolidation of right middle lobe. He had a metabolic acidosis. IV fluids were given, 1000mL over 4 hours, together with IV chlorphenamine, IV paracetamol, and salbutamol nebuliser. He was transferred to the high dependency unit (HDU) for haemofiltration and noradrenaline infusion and was put onto nasal high flow the following day. He was treated for diabetic ketoacidosis. He was noted to be struggling with breathing. At 07:30 he was started on continuous positive airway pressure (CPAP). At 11:20 he needed intubation; during this his cardiac output stopped and he could not be resuscitated. He died 3 days after the transfusion reaction which was considered contributory.
The CXR was normal preoperatively. After the reaction ‘there are florid ground-glass changes affecting both lungs with upper zone predominance. There is relative sparing of the lung bases. No pleural effusion or obstructing endobronchial lesion. Conclusion: Florid pulmonary abnormalities are visible. These could represent infection, adult respiratory distress syndrome, or possibly other entities such as drug reaction or other rarer causes of interstitial lung disease. These may well be contributing to the patient’s metabolic instability’.
This was initially escalated as a potential TRALI. Staff contacted the Blood Service and information was submitted to the expert panel. The expert panel believed the pulmonary symptoms were due to TACO. The report was reviewed by the TACO expert who noted: ‘difficult to attribute TACO as although pulmonary oedema is mentioned, the post-transfusion CXR report does not confirm this. There is no fluid balance record, the heart rate at time of reaction is lower than baseline and the mean arterial pressure (MAP) is normal. Given the inflammatory symptoms, suggest consider transferring to TAD or withdraw’.
Local case review: the doctors now think this was possibly pneumonia alongside a diabetic ketoacidosis episode and septic shock with the transfusion being a contributory factor. Note that the blood culture taken at the time of reaction was negative.
Major morbidity n=4
Case 18c.6: Transfusion reaction on a background of autoimmune disease
A woman in her 70s underwent insertion of a permanent pacemaker for heart block. She had a background of autoimmune disease (systemic lupus erythematosus, immune thrombocytopenia and autoimmune haemolytic anaemia). She developed a transfusion reaction resulting in admission to the ITU. She became clammy with increasing shortness of breath (respiratory rate increased from 18 to 32/min), wheeze and tachycardia of 129/min. She improved with diuretic treatment.
There was not enough information to classify this as TACO.

157
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
18c. Transfusion-Associated Dyspnoea (TAD)
Case 18c.7: Acute hypoxia follows transfusion (transfer from TRALI)
A woman in her 60s received a blood transfusion without complications following coronary artery bypass surgery and observations were stable during transfusion. She had diabetes and known ischaemic heart disease. She developed rigors (but no measurable increase in temperature) after blood transfusion with a tachycardia of 199/min, BP 175/77 and decreased oxygen saturation. The CXR showed bilateral alveolar infiltration, and she was readmitted to intensive care shivering and shaking uncontrollably. IV fluid and antibiotics were started. This was thought to be TRALI because of acute hypoxia and bilateral infiltrates seen on CXR after one unit of blood with normal echocardiogram and no suggestion of fluid overload. A Blood Centre was informed but no TRALI investigations were suggested.
Case 18c.8: Breathlessness after transfusion (transfer from TRALI)
A woman in her 50s was receiving a course of chemotherapy for myelodysplasia in leukaemic transformation and was also on IV antibiotics for infection (but she was not neutropenic). These had been started earlier on the same day as her transfusion when she had fever 38.3oC associated with a fall in oxygen saturation to 86% requiring oxygen. She recovered from this. Later the same day she started feeling breathless following the end of the red cell transfusion and this increased over the following 6 hours with worsening hypoxia and increasing oxygen requirement. She required admission to the ITU. Her antibiotics and other drugs were given in a total infusion volume of about 1600mL plus blood components to 700mL during the same day. The CXR showed clear evidence of opacification which was not present before transfusion. She did not improve after treatment with diuretics. The TRALI panel considered TACO more likely but this reaction did not meet the TACO criteria.
Case 18c.9: Bronchospasm under anaesthetic (transfer from TRALI)
A young woman underwent emergency caesarean section at around 03:30 for placental abruption under general anaesthesia. She was difficult to ventilate and she developed respiratory failure with profound bronchospasm. It was not clear what the cause was and she was initially treated for possible acute exacerbation of asthma, but an acute reaction to blood transfusion was possible (she had received four units of red cells, two units of FFP and one unit of platelets) or an allergic reaction. Postoperatively she was transferred to ITU and remained intubated and ventilated. She improved after a few hours and was extubated. Overnight she was stable and was discharged to the labour ward at 07:00 for removal of uterine packs and tamponade balloon. Following removal of the balloon she started to complain of difficulty breathing. She was coughing and her saturation dropped to 88%. Her oxygen requirement continued to increase and she required transfer back to the critical care unit for nasal high flow oxygen therapy and CPAP. Acute respiratory distress syndrome (ARDS) was noted, but the clinicians were unsure whether this was from treatment or the smoking history that predisposes to this, or this might be TRALI or TACO (her mast cell tryptase was normal). She made a full recovery.
Additional cases are available in the supplementary information for this Annual Report by chapter on the SHOT website www.shotuk.org.
Commentary
As can be seen from the cases above, some might have been classified as TACO had there been more information, particularly evidence of pulmonary oedema or details of fluid balance. Others might be classified as TRALI if non-antibody cases of acute lung injury (ALI) were included in that category. The international consensus on both these categories will help to clarify how the pulmonary complications are reported. A review of transfusion reactions classified as TAD 2011-2013 was published from the New Zealand haemovigilance scheme (Badami et al. 2015). The authors examined 37 reactions that had been reported as TAD. With additional information from the case notes 34 initially classified as TAD by reviewer 1 were reduced to 16, and from 33 to 15 by the second reviewer. Several were reclassified as TACO, from initial 1 to 8 by the first reviewer, and 0 to 6 by the second reviewer. None were reclassified as TRALI. These authors ‘renew the call’ for better diagnosis and reporting of TACO.
ReferenceBadami KG, Joliffe E and Stephens M. Transfusion-associated dyspnoea – shadow or substance? Vox Sang 2015;109:197-200.

158
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
19. Haemolytic Transfusion Reactions (HTR)
Authors: Tracey Tomlinson and Anicee Danaee
Definition:
Acute haemolytic transfusion reactions (AHTR) are defined as fever and other symptoms/signs of haemolysis within 24 hours of transfusion, confirmed by one or more of the following: a fall in haemoglobin (Hb), rise in lactate dehydrogenase (LDH), positive direct antiglobulin test (DAT), positive crossmatch.
Delayed haemolytic transfusion reactions (DHTR) are defined as fever and other symptoms/signs of haemolysis more than 24 hours after transfusion; confirmed by one or more of the following: a fall in Hb or failure to increment, rise in bilirubin, incompatible crossmatch not detectable pre transfusion.
Simple serological reactions (development of antibody with or without a positive DAT but without clinical or laboratory evidence of haemolysis) are defined as alloimmunisation: these data are no longer collected by SHOT.
Key SHOT messages
• Anti-Jka and anti-Jkb remain the most commonly implicated antibodies in haemolytic transfusion reactions (HTR)
• Hospital transfusion laboratories should ensure that red cell antibodies are managed in the same way as other specific blood requirements. The antibody history must be clearly documented against the patient’s record. A national database such as the Specialist Services Electronic Reporting using Sunquest ICE (Sp-ICE) should be used to make this information available in the event of the patient moving between hospitals or other areas of shared care
• Incentives to share the antibody history of the patient need to be supported by patient education to inform the patient of their specific red cell requirements and encourage them to take ownership and alert the clinicians. Clinicians must take responsibility for listening to patients and to act on any information regarding specific blood requirements and take note of any antibody history
Number of cases n=42
A total of 42 cases have been included, 13 acute and 29 delayed reactions (including 6 cases of hyperhaemolysis). The number of delayed reactions reported has increased compared to the previous year (18 delayed transfusion reactions reported in 2016 out of 35 HTR) but is comparable to previous years. Three cases related to emergency transfusions in which antigen-positive blood was transfused due to the clinical urgency with the knowledge that the patient had the antibody.
Age range and median
There was only 1 paediatric case reported (age less than 10 years). The overall age range was <10 to 87, with a median age of 52 years.
Haemolytic Transfusion Reactions (HTR) n=4219

159
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
19. Haemolytic Transfusion Reactions (HTR)
Deaths n=1
There was only one patient death attributed to the transfusion. A further two patient deaths were reported but post mortem examinations confirmed that death was due to the underlying conditions and not the transfusion. One death occurred in an acutely unwell patient who was admitted in cardiac failure and post mortem examination confirmed this was the cause of death. The other death was related to complications of sickle cell disease (SCD) and is described under the hyperhaemolysis and major morbidity section.
Major morbidity n=7
There were 7 cases of major morbidity, 6 of which involved hyperhaemolysis syndrome in patients with SCD. In 5/6 cases the symptoms improved following treatment with intravenous immunoglobulin (IVIg) and methylprednisolone.
Hyperhaemolysis and major morbidity
The diagnosis of hyperhaemolysis remains a challenge. Hyperhaemolysis is characterised by more severe haemolysis than DHTR, with haemolysis affecting the transfused red cells and also the patient’s own red cells; there is a decrease in Hb to below pre-transfusion levels, which is often associated with a reticulocytopenia. It may be triggered by a new red cell alloantibody, but frequently no new red cell antibody is identified. Therefore, for the purpose of analysing the SHOT data any case reported as hyperhaemolysis by the reporter but in which the serology supports a conclusion of antibody-mediated haemolysis without additional features, the case has been classified as a haemolytic transfusion reaction.
Case 19.1: Death following emergency transfusion of a patient in sickle crisis
A pregnant patient in her 40s with SCD in sickle crisis and symptoms of acute chest syndrome received an urgent red cell exchange transfusion prior to emergency caesarean section. During the transfusion the patient developed symptoms of a transfusion reaction and the transfusion was stopped. The patient had a history of anti-U and possible anti-Jka, however due to the emergency nature of the transfusion and the rarity of U-negative, Jka-negative red cells, Jka-negative units were not selected and units negative to the U antigen only were transfused. The justification given for this was that the presence of anti-Jka had not been positively confirmed. The patient developed disseminated intravascular coagulation (DIC) and possible hyperhaemolysis syndrome. At post mortem the death was attributed to acute chest syndrome related to SCD.
SHOT considers that all reported cases of probable hyperhaemolysis where there is a significant fall in Hb should be considered as major morbidity. Following application of this criterion 3 cases of hyperhaemolysis reported with ‘minor morbidity’ were upgraded. Case 19.2 was further complicated by the presence of pre-existing alloantibodies and the patient having a confirmed variant Rh phenotype.
Case 19.2: Hyperhaemolysis in patient with variant Rh phenotype and known alloantibodies
A patient with SCD received an elective ten-unit exchange transfusion prior to surgery. The patient was known to have allo anti-Ce, anti-s, anti-K and anti-Jkb. The patient also had a previously-reported auto anti-e. The patient was genotyped as part of the Blood Service genotyping project for haemoglobinopathy patients and found to have a variant D- and e-genotype. The previously reported auto anti-e was therefore recharacterised as allo anti-e. Due to the unavailability of D- C- E+ c+ e- s- K-Jkb- red cells the decision was made not to provide e-negative units. The rationale for excluding the anti-e for the purposes of blood selection was that the patient had been transfused e-positive units prior to the identification of the variant e-genotype without symptoms of haemolysis and also that data collected by National Health Service Blood and Transplant (NHSBT) for transfusion of antigen-positive units to patients with variant phenotypes had no reports of haemolysis in e-variant patients with anti-e.
Five days post transfusion the patient developed haemoglobinuria and was readmitted to hospital and required ventilation. The Hb fell from 83g/L to 48g/L and the bilirubin and LDH were raised.

160
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
19. Haemolytic Transfusion Reactions (HTR)
The patient was transfused three units of D+ C- E+ c+ e- s- K- Jkb- red cells. However, monitoring of HbS levels demonstrated that these transfused cells were also haemolysed. No new antibodies were detected on serological investigation and the DAT was positive pre and post transfusion with no change seen in the reaction strength.
Learning point
• Patients with haemoglobinopathies should be monitored for signs and symptoms of haemolysis following transfusion and diagnosis of hyperhaemolysis considered early. It is important that patients are educated when discharged home about signs and symptoms they might develop so they can present early should any of these occur, including signs of haemoglobinuria
Clinical and laboratory signs and symptoms
Acute haemolytic transfusion reactions (AHTR) n=13
There appears to be no typical set of clinical symptoms associated with an acute haemolytic reaction. In 10/13 (76.9%) of cases the reaction was identified by the patient becoming unwell during transfusion, with the most common symptoms being fever and rigors. Other symptoms included dyspnoea, rash and red/brown urine due to haemoglobinuria.
All reports provided laboratory evidence of haemolysis, with 12/13 patients experiencing an acute transfusion reaction with a raised bilirubin and a fall in Hb.
Delayed haemolytic transfusion reactions (DHTR) n=23 (excluding potential cases of hyperhaemolysis)
The most commonly reported clinical indications of a DHTR were haemoglobinuria (9 cases) and jaundice (7 cases) with fever and back pain also being reported. However, in 10 cases (43.5%) there were no obvious clinical signs or symptoms associated with the DHTR and the reaction diagnosed by laboratory signs of haemolysis only. The main indicators are shown in Figure 19.1.
Laboratory indicationsof DHTR
Hb
bilirubin
LDHDAT positive
New anitbodyin plasma
and/or eluate
DHTR=delayed haemolytic transfusion reaction; Hb=haemoglobin; DAT=direct antiglobulin test; LDH=lactate dehydrogenase
Figure 19.1:
Laboratory
indications of
DHTR

161
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
19. Haemolytic Transfusion Reactions (HTR)
Antibodies implicated in haemolytic transfusion reactions
Mixture including Jka or Jkb
c
Mixture
M
Fya
Jkb 1
Jka
1
1
2
2
4
10
Antibodies to low frequency antigens where red cells were issued electronically
Antibodies to low frequency antigens were identified in 2 cases of AHTR (anti-Wra and anti-Cob) and 1 DHTR (anti-Wra). In all cases the pre-transfusion antibody screen was negative and blood was issued by electronic crossmatch. Pre- and post-transfusion samples were referred to the Blood Service reference laboratory where the antibody was identified in both patient samples and the implicated units confirmed as positive to the corresponding antibody.
The specification for red cell screening cells used for pre-transfusion testing in the UK does not require the inclusion of cells positive for the Kpa, Wra and Cob antigens. It is therefore not possible to detect these antibodies in a standard antibody screen. The lack of a serological crossmatch step in electronic issue means that the potential to miss low frequency antigens prior to transfusion is a known risk for electronic issue of blood components. However due to the low frequency of these antigens in the donor population the risk of transfusion with an antigen-positive unit remains low.
Reactions associated with antibodies to the Kidd blood group system
In 16/42 cases (38.1%) anti-Jka or anti-Jkb, either in isolation or combination with other antibodies, was detected in the post-transfusion sample only. Antibodies to the Kidd system were implicated in another 3 cases. In 2 cases antigen-negative blood could not be provided despite the antibody being present due to the emergency nature of the transfusion, and in the 3rd case anti-Jka had not been fully excluded during an out-of-hours investigation and crossmatch.
Learning point
• Robust methods of recording antibody history against patient’s records should be developed and antibody warning cards issued to patients. This should be supported with patient education to empower them to take ownership and inform clinicians that they have specific red cell requirements and clinician education to ensure that they have the understanding to act on this information
Figure 19.2:
Antibodies
implicated in DHTR

162
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
19. Haemolytic Transfusion Reactions (HTR)
Classic delayed HTR
Twenty-three of 29 cases reported as DHTR followed the classic pattern of a negative antibody screen on the pre-transfusion sample and the identification of an alloantibody in the post-transfusion sample.
In all reported cases of DHTR the period between transfusion and identification of the reaction meant that it was not possible to repeat testing on the pre-transfusion sample or repeat compatibility testing against the implicated units. It can therefore be difficult to confirm imputability. However, in 5 cases it was possible to confirm from Blood Service records that the transfused unit was antigen-positive for the implicated antigen.
Case 19.3: DHTR due to anti-c
A patient receiving chemotherapy was transfused two units of red cells issued by electronic crossmatch following a negative antibody screen using a fully automated system. The following week the patient returned to hospital with discoloured urine and anaemia. The patient’s bilirubin had risen from 10 to 40micromol/L and her Hb had dropped from 102g/L to 88g/L. The antibody screen on the new samples was positive and anti-c was identified. The transfused units were confirmed as c-antigen positive.
Case 19.4: DHTR due to anti-Fya
A renal patient with history of a negative antibody screen was transfused two units of red cells. Eleven days later the patient returned for their next routine appointment. Investigation of the samples taken during this admission found that anti-Fya was now detectable in the plasma. Anti-Fya was also eluted from the patient’s red cells. The patient had reported no clinical symptoms but laboratory tests indicated the Hb had not incremented following the transfusion and she had now developed a positive DAT.
Delayed HTR is the main cause of HTR and many are only detected by careful analysis of laboratory results.
Review of antibodies implicated in DHTR
Figure 19.3 summarises the antibodies implicated in DHTR reports over the last 5 years. No data on antibody mixtures were available for 2013 and 2014.
Anti-Jka and anti-Jkb remain the antibodies most commonly implicated in haemolytic transfusion reactions. This is probably due to the known tendency for the levels of these antibodies to fall to undetectable levels after the initial immunisation event. It is therefore important that when detected, the presence of the antibody is recorded against the patient’s antibody record and a blood group warning card issued to patient.
1
1
1
2
2
3
4
5
5
8
8
9
10
32
s
A
U
Fyb
S
C
M
E
Fya
Jkb
Mixture
c
Mixture inc Jka or Jkb
Jka
Figure 19.3:
Antibodies
implicated in DHTR
2013-2017

163
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
19. Haemolytic Transfusion Reactions (HTR)
Shared care
Case 19.5: Failure to identify previous antibody history available in a patient treated across multiple hospitals
Anti-C and anti-S were confirmed in a patient in 2000 by the Blood Service and a report and antibody warning card for the patient issued to the referring hospital (Hospital 1). In 2015 the same patient was seen in Hospital 2 and samples referred to the International Blood Group Reference Laboratory (IBGRL) for red cell genotyping. In February 2017 the patient was seen in Hospital 3 and another sample was sent to the IBGRL for genotyping. At this time both the report from 2000 and the genotype report from 2015 were available on Sp-ICE.
In May 2017 the patient was seen at a 4th hospital (Hospital 4). Samples were again referred to the Blood Service reference laboratory and this time anti-Lua and anti-Fya were detected. A report was issued to Hospital 4 stating the new antibodies and also the previously detected anti-C and anti-S. A new antibody card for the patient, listing all four antibody specificities was sent with the report. This new report was also uploaded to Sp-ICE.
In July 2017 the patient presented again to Hospital 1. An antibody screen was performed and found negative and ABO, Rh and K group-matched blood was issued. Approximately 5 days later, the patient was admitted to a 5th hospital (Hospital 5) with symptoms of a HTR including an acute drop in Hb and positive DAT.
Learning points
• It is important that resources such as Specialist Services Electronic Reporting using Sunquest ICE (Sp-ICE) are used to identify previously detected antibodies prior to transfusion, especially when patient care is being provided by multiple hospitals
• Patients should also be informed of the risks associated with changing their care provider and empowered to inform clinicians of their red cell requirements
Emergency transfusion
Three cases of HTR were reported following transfusion of antigen-positive red cells in an emergency.
Emergency transfusion to treat major haemorrhage is vital to avoid hypovolaemic shock and its consequences allowing the patient to survive long enough for clinicians to treat the cause of the blood loss (NPSA 2010). It is therefore important to remember that it is often lifesaving. In these cases, the risk of an adverse reaction is outweighed by the need to support the patient over the initial phase allowing treatment to take place.
Case 19.6: Transfusion of emergency O D-negative red cells
A patient suffered a major gastrointestinal arterial bleed and required immediate transfusion. The two emergency O D-negative units were taken from the hospital transfusion laboratory refrigerator and a further three uncrossmatched group O units were provided. Subsequent testing of the pre-transfusion sample identified anti-Jkb in the patient’s plasma. Three of the units issued were confirmed to be positive for the Jkb antigen. The patient developed fever and jaundice and laboratory tests confirmed haemoglobinuria, raised bilirubin, raised LDH, a rapid drop in Hb and positive DAT. The patient recovered and survived.
Case 19.7: Issue of ‘best match’ in major haemorrhage
A major haemorrhage alert was called on a bleeding patient with cholecystitis and the emergency O D-negative units were collected. Part of the first unit was transfused before the transfusion laboratory staff were able to inform the clinical area that the patient had a history of anti-E, anti-Fya and anti-Jka. On discussion with the consultant haematologist it was agreed to crossmatch two E-negative Fya-negative, Jka-untyped units as no suitable Jka-negative units were available in the hospital transfusion

164
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
19. Haemolytic Transfusion Reactions (HTR)
laboratory. These units were subsequently confirmed as Jka-positive. The patient did not suffer any clinical symptoms of a HTR but laboratory tests showed a positive DAT and rapid fall in Hb. The patient recovered and survived.
The third case has been described above (Case 19.1).
Learning points
• It is important that lifesaving transfusion is not withheld due to a history of alloantibodies. However, in such cases the patient should be carefully monitored, both during and after transfusion for signs of a haemolytic transfusion reaction
• The Blood Service recommends that where the antibody screen is positive or the patient has known antibodies for which compatible blood is not readily available, ABO, full Rh and K-matched blood may be given, with intravenous (IV) methylprednisolone 1g and/or IV immunoglobulin (IVIg) cover if required. 80% of patient antibodies are within the Rh and K systems (Win et al. 2018)
• Discuss with a clinical haematologist regarding the need for methylprednisolone and/or IVIg and monitoring (including urine output) for delayed haemolytic transfusion reactions (Win et al. 2008, Win et al. 2018, Woodcock et al. 1993)
Reactions probably not associated with red cell alloantibodies (low imputability)
Similar to last year there were 2 cases that were likely to have been exacerbation of autoimmune haemolysis, 1 case where the clinical and serological symptoms could be associated with the patient’s underlying condition and another 3 where no cause was found.
References
Kohan AI, Niborski RC et al. High-dose intravenous immunoglobulin in non-ABO transfusion incompatibility. Vox Sang 1994;67:195-198.
NPSA, Rapid Response report NPSA/2010/RRR017, 2010 http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=83689 [accessed 26 February 2018].
Patel A. Management of sickle cell disease. Beware of transfusions and hyperhaemolysis. BMJ 2008;337:1397.
Petz LD, Garratty G. Blood Transfusion in AIHAs. In Immune Haemolytic Anaemias, 2nd edition, 2004:375-400, Churchill Livingstone, New York.
SHOT Bite No. 8: Massive Haemorrhage – Delays, 2016 https://www.shotuk.org/wp-content/uploads/SHOT-Bites-No8-Massive-Haemorrhage-Delays-1.pdf [accessed 26 February 2018].
Win N, Needs M et al. Transfusions of least-incompatible blood with intravenous immunoglobulin plus steroids cover in two patients with rare antibody. Transfusion 2018 May 6. doi: 10.1111/trf.14648.
Win N et al. Hyperhaemolysis syndrome in sickle cell disease: case report and literature review. Transfusion 2008;48:1231-1237.
Woodcock BE, Walker S and Adams K. Haemolytic transfusion-successful attenuation with methylprednisolone and high dose immunoglobulin. Clin Lab Haematol 1993;15:59-61.
Young P, Uzieblo A et al. Autoantibody formation after alloimmunisation: are blood transfusions a risk factor for autoimmune haemolytic anaemia? Transfusion 2004;44:67-72.

165
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
20. New or Unclassifiable Complications of Transfusion (UCT)
Author: Paula Bolton-Maggs
Definition:
Occurrence of an adverse effect or reaction temporally related to transfusion, which cannot be classified according to an already defined transfusion event and with no risk factor other than the transfusion, and no other explanation.
Seven cases were reported in this category and 4 others were transferred from the febrile, allergic, and hypotensive reaction category (FAHR, formerly acute transfusion reactions (ATR)). Three of these were cases of suspected transfusion-associated necrotising enterocolitis (TANEC) in premature infants, one of which was associated with major morbidity but the baby recovered and was discharged.
Major morbidity n=1
Case 20.1: TANEC 1
A red cell transfusion was given to a fully fed 25-week twin for anaemia (haemoglobin (Hb) 88g/L). During transfusion the baby became unsettled but no change in observations. Within a short time, the baby’s abdomen became distended and she had features of NEC and required ventilation. The baby was treated conservatively and made a full recovery.
The remaining 10 cases are described in the supplementary information for this Annual SHOT Report on the SHOT website www.shotuk.org.
New or Unclassifiable Complications of Transfusion (UCT) n=11 20

166
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
21. Cell Salvage (CS)
Authors: Sarah Haynes and Catherine Ralph
Definition:
Any adverse events or reactions associated with autologous transfusion methods, including intraoperative and postoperative cell salvage (washed or unwashed), acute normovolaemic haemodilution or preoperative autologous donation (PAD).
Death n=0
Major morbidity n=0
Seventeen cases were reported (12 female; 4 male; 1 not specified); on review none were withdrawn, nor transferred to or from other categories. All cases reported were related to the use of intraoperative cell salvage (ICS), possibly reflecting the reduced usage of postoperative devices in orthopaedic procedures.
The number of reported cases (n=17) is likely to represent only a small fraction of the number of incidents and under-reporting of cell-salvage incidents remains a concern. There is currently no national reporting scheme capturing denominator data, although the introduction of the office of population censuses and surveys (OPCS) clinical codes for cell salvage, available since 2014, and recommended by the UK Cell Salvage Action Group (UKCSAG), can provide data so long as this coding has been consistently used.
Obstetrics reports predominate. Of the 8 obstetrics incidents only 3 cases used a leucocyte depletion filter, and all 3 reported incidents related to its use; 2 resulted in hypotension and 1 slowed re-infusion and led to time-expiry.
Machine failures and human factors related to managing ICS emphasise the importance of competency-based training and the need to provide learning opportunities.
Cell salvage cases by speciality
Speciality Elective Emergency
Obstetrics 6 2
Orthopaedic 1
*Other 3 1
Trauma 2
Urology 1
Vascular 1
Total 12 5
*Other comprised 3 spinal surgeries and an emergency laparotomy
Types of cell salvage
All cases involved the use of washed ICS techniques. No reports were received for postoperative cell salvage (PCS).
Table 21.1:
Specialty for cell
salvage reports
Cell Salvage (CS) n=1721

167
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
21. Cell Salvage (CS)
Cell salvage adverse events and reactions
There were 14 adverse events comprising 7 machine failures, 5 operator errors and 2 others.
Within the category of machine failure all devices were under service contracts, however it was also of note that some of these devices were approaching expiry and were due to be replaced. It was reported in one instance of machine failure that a patient received an avoidable allogeneic blood transfusion. In 5 other incidents patients were put at risk of receiving allogeneic blood as autologous blood was discarded. Reporters stated that only 2 of the 7 machine failures were reported to the Medicines and Healthcare Products Regulatory Agency (MHRA) under the Yellow Card Scheme.
Information received from the MHRA Devices Division revealed 7 reported incidents related to cell salvage devices in 2017. It is not clear whether this represents a further 5 cases not reported to SHOT. It should however be noted that cell-salvage machines are classified as medical devices and an adverse incident that caused, or almost caused, injury to a patient or wrong or delayed treatment of a patient is reportable under the Yellow Card Scheme (England & Wales) or regulatory equivalent (Scotland and Northern Ireland).
Of the adverse events attributed to operator error, 2 involved incorrect assembly of equipment, 1 related to the use of non-intravenous (IV)-grade saline for swab washing, in another the suction line was dropped, and finally a failure to address slow administration of the cell-saved blood resulted in time-expiry. No adverse consequences were reported, although in the case of the dropped suction line the reporter stated that the patient received two units of blood intraoperatively which may have been avoided if autologous red cells had been available. All operators involved in these incidents had been trained and competency-assessed.
In the further 2 adverse events, both in obstetrics, unforeseeable factors resulted in patients not receiving their own blood back. In 1 case a patient underwent a caesarean section with hysterectomy and experienced an intraoperative haemorrhage of approximately 3L. Salvaged red cells were reinfused under pressure and an extravasation injury occurred resulting in approximately 300-400mL of red cells being infused into the subcutaneous tissue of the patient’s forearm. Although cannula extravasation is not exclusive to blood transfusion, infusing cell salvaged blood under pressure is not recommended.
In a second obstetric case, a patient’s unusual lipid profile caused technical difficulties with the cell-salvage process. During an elective caesarean section for twins, cell salvage was used and the operating department practitioner noted that the blood in the collection chamber of the cell-salvage machine was clotting, despite adequate titration of heparinised saline. The collection volume was estimated to be large enough to process and this was commenced intraoperatively in the usual way. Drawing the blood from the collection chamber into the bowl required additional heparinised saline and it was noted the waste bag was pink and milky looking in appearance. The final product for re-infusion looked dilute and had small clots of blood within. A sample taken from the processed autologous blood could not be analysed due to clotting. A decision was made to discard the autologous blood and not re-infuse.
On dismantling the cell-salvage processing equipment, a large fatty substance was found occluding the outflow tubing. Analysis of this substance of light brown tissue 55x10x5mm, showed under microscopy, eosinophils, debris, red cells, mixed inflammatory cells, and was nondescript.
Samples for full blood count (FBC), clotting, urea and electrolytes, and amylase from the mother in recovery were all normal, however the samples were all lipaemic and showed very high triglycerides and cholesterol levels. Consequently, a diagnosis of hyperlipidaemia was made and the cell-salvage blood discarded.
Comment: The lipaemic maternal blood appeared to affect the cell-salvage machine-processing mechanism producing a series of unusual events recognised by the clinical team and ultimately providing an opportunity to diagnose maternal hyperlipidaemia. An awareness of cell-salvage blood quality is important for both operators and clinicians, with decisions to re-infuse cell-salvaged blood taken in the context of each individual case.

168
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
21. Cell Salvage (CS)
Minor or moderate morbidity n=3
There were 3 clinical reactions, all in obstetric patients. All were classed as having minor or moderate morbidity at the time of the reaction and all recovered.
Case 21.1: Possible allergic reaction to salvaged red cells
A patient undergoing emergency caesarean section developed anaphylactic-like symptoms within a few minutes of commencement of reinfusion of salvaged red cells. The patient reported difficulty in breathing and tongue swelling and the infusion was stopped with a prompt resolution of symptoms. When reviewed the following day the patient revealed that the effects of a high epidural had caused numbness in her face and hands, she panicked and this affected her breathing. She also stated this reaction started before the infusion of the salvaged red cells commenced.
Comment: Whilst it may be unlikely, an allergic reaction to the autologous transfusion cannot be entirely ruled out. It is difficult to speculate as to the possible allergen responsible, but the final salvaged red cell product can contain trace amounts of any substrate entering the system including citrate anticoagulant.
Case 21.2: Hypotension on reinfusion of salvaged red cells
A patient with placenta praevia underwent elective caesarean section with cell salvage. Intraoperative blood loss was approximately 800mL and a reinfusion of 200mL of salvaged red cells was commenced using a leucocyte-depletion filter. The patient experienced a sudden and profound hypotension and the infusion was stopped. The patient’s blood pressure was normalised with vasoconstrictors and other obvious causes of hypotension ruled out. The leucocyte-depletion filter was removed and the remainder of the autologous red cells reinfused without further incident.
Comment: Since 2010, when SHOT started to report on cell-salvage incidents, there have been 27 ICS hypotensive incidents; 20 occurred with the use of a leucocyte-depletion filter with citrate anticoagulant on 18 occasions (Haynes et al. 2017). This is a further reported case where a leucocyte-depletion filter was used and citrate was the anticoagulant. In this scenario a pragmatic decision was taken to abandon the filter and continue with the reinfusion with no further incident. National Institute for Health and Care Excellence (NICE) guidance on cell salvage in obstetrics published in 2005 states that ‘A leucocyte-depletion filter is nearly always used in this process to reduce the amount of amniotic fluid contaminants in transfused blood to levels approaching those found in maternal blood.’ However, a pragmatic cell-salvage study in obstetrics, the SALVO (Cell SALVage in Obstetrics) trial (Khan et al. 2017) reported that in 26 UK obstetric units leucocyte-reduction filters were used in only 54.9% of cases randomised to receive cell salvage. This data illustrates current practices in obstetric cell salvage and a move away from the use of leucocyte-depletion filters in this setting, presumably as a result of concerns over hypotensive reactions.
Case 21.3: Hypotension resulting from reinfusion of salvaged red cells confirmed by a secondary challenge
A patient with a grade IV placenta praevia underwent elective caesarean section. As the patient was being transferred from theatre, reinfusion of 361mL of autologous red cells via a leucocyte-depletion filter commenced. The patient then complained of nausea and vomiting, looked unwell and became slightly less responsive. Monitoring revealed sinus tachycardia with a heart rate of 165 beats per minute (bpm) with systolic blood pressure (BP) of 78mmHg. The red cell infusion was stopped and the symptoms resolved with a bolus infusion of 60 micrograms of phenylephrine. Having stabilised the patient in the recovery area (heart rate 78bpm, systolic BP 98mmHg), the autologous red cell transfusion was recommenced. This resulted in rapid rise in heart rate to 150bpm with concomitant hypotension. The infusion was stopped immediately with rapid resolution of symptoms. The remaining 150mL of autologous red cells was then discarded. The reporter noted that cell salvage was carried out following standard protocols, however, at the end of the case a partial bowl was washed without using the ‘concentrate’ function and the saline wash volume was not increased to compensate for this.
Comment: This is a further confirmed case of hypotension associated with reinfusion of salvaged red

169
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
21. Cell Salvage (CS)
cells through a leucocyte-depletion filter where citrate was used in the collection of the salvaged blood. The second challenge with the red cell infusion provides compelling evidence. It is not clear whether the use of a partially full bowl and single wash added to this reaction. The use of partial bowls is discouraged as it is thought to result in inadequate clearance of contaminants as washing processes in bowl based cell salvage systems are thought to be aided by red cell packing and exclusion of fluid. Limited work in this field, however, suggests that a good quality product can be produced from a partially full bowl when the wash volume is doubled (Serrick et al. 2005).
Recommendations
• Cell-salvage devices are medical devices and as such any failures should be additionally reported to the appropriate regulatory authority responsible for monitoring medical device safety
• Cell-salvage operators should be trained and have documented evidence of competency assessment. Organisations should review ongoing competence and institute re-training or update training as necessary to ensure patient safety
• Cell salvage should be performed to standard protocols identified by the organisation to reflect best practice. Variations in practice to suit an individual patient’s circumstances should be discussed prior to intervention and risks and benefits considered
• Cell-salvage operators and clinicians must be alert to unusual unpredictable events related to patient factors. Monitoring of the process in relation to quality of the reinfused product is just as important as monitoring the reinfusion itself
• Organisations should consider whether a failure in provision of cell salvage, as a result of adverse event or logistics, puts a patient at risk of an avoidable allogeneic transfusion and report to SHOT accordingly
• Organisations should ensure that clinical coding for cell salvage is used consistently (office of population censuses and surveys (OPCS) codes X36.4 and X33.7) to assist with establishing national denominator data
Action: Cell salvage teams
References
UKCSAG. https://www.transfusionguidelines.org/transfusion-practice/uk-cell-salvage-action-group/framework-for-service-provision [accessed 27 March 2018].
Haynes SL, Ralph C and Thomas D. Cell salvage incident reporting - The UK experience. Vox Sang 2017;112 Suppl 1:278.
Khan KS, Moore PAS et al. Cell salvage and donor blood transfusion during caesarean section: A pragmatic, multicentre randomised controlled trial (SALVO). PLoS Med 2017;14(12):e1002471. https://doi.org/10.1371/journal.pmed.1002471 [accessed 28 March 2018].
National Institute for Health and Care Excellence (NICE): Intraoperative blood cell salvage in obstetrics. Interventional procedure guidance, published 23 November 2005. https://www.nice.org.uk/guidance/ipg144/chapter/2-The-procedure Section 2.2.3 [accessed 29 March 2018].
Serrick CJ, Scholz M. Partial bowls using the Haemonetics Cell Saver 5: does it produce a quality product? J Extra Corpor Technol 2005;37(2):161-164.

170
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
22. Paediatric Summary
Author: Helen New
Definition:
Paediatric cases comprise all reports for patients under 18 years of age, including all paediatric cases from the other chapters in this report. Paediatric reports have been subdivided by recipient age group: neonates ≤28 days; infants >28 days and <1 year; children ≥1 year to <16 years and young people aged 16 to <18 years.
Key SHOT messages
• Over and undertransfusion, largely due to mistakes in prescribing on a weight-basis, was a significant problem, with 13/19 (68.4%) of overtransfusion cases in paediatrics; this reflects the complexity of paediatric prescribing
• In 6 cases adult emergency O D-negative units were given to neonates, an area for hospital focus in developing strategies to help staff correctly identify the age-specific emergency units
• Most handling and storage errors (HSE) resulted from technical administration problems (12/16), including using incorrect pump settings; vigilance is required in the paediatric setting where pumps are so often used
• There were 2 confirmed paediatric reports of transfusion-related acute lung injury (TRALI) and 1 of transfusion-associated circulatory overload (TACO); it is important for these pulmonary complications to be considered in neonates and paediatrics as in older patients
Recommendation
• Clinical staff who prescribe blood for paediatric patients should not do so unless they have been given training in weight-based prescribing of blood components. Additional resources that can support best practice include the ‘Bookmarks’ and ‘Blood Component App’ with key information from the British Society for Haematology (BSH) paediatric transfusion guidelines (New et al, 2016; see SHOT website https://www.shotuk.org/resources/current-resources/)
Action: Hospital Transfusion Teams, Hospital Paediatricians, Royal College of Paediatrics and Child Health
Introduction and commentary
The paediatric chapter brings together the cases related to the <18-year age group in a ‘mini-SHOT Report’ in order to identify areas that have particularly relevant findings for professionals involved in the care of neonates and older children.
The number of paediatric cases in 2017 was similar to 2016 at 139/1671 (8.3%) total reports, 255/3230 (7.9%) if near miss (NM) and right blood right patient (RBRP) are included. As can be seen from Figure 22.1, paediatric cases are disproportionately represented in three of the error categories:
• 18/82 (22.0%) incorrect blood component transfused-wrong component transfused (IBCT-WCT)
Paediatric Summary22

171
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
22. Paediatric Summary
• 23/225 (10.2%) IBCT-specific requirements not met (IBCT-SRNM)
• 31/225 (13.8%) avoidable, delayed or undertransfusion (ADU)
This pattern is similar to previous years and reflects the complexity of paediatric transfusion. As before, neonatal and infant reports were almost all in the error categories, (Figure 22.2), where they constituted a particularly high proportion of IBCT-WCT reports (Figure 22.4). Overall, paediatric error reports (IBCT, HSE, ADU, and anti-D immunoglobulin (Ig)) were 95/139 (68.3%) of total paediatric reports, similar to 2016, 101/136 (74.3%).
Errors categorised as primarily from the laboratory were 34/95 (35.4%) paediatric error reports (9 IBCT-WCT, 16 IBCT-SRNM, 2 HSE, 6 ADU, 1 anti-D Ig), compared to 409/1201 (34.1%) for total error reports. It is notable that reports of missed methylene-blue or solvent detergent-treated fresh frozen plasma (FFP) have decreased in 2017, Figure 22.3b. However, there continue to be reports of laboratory errors related to neonatal grouping and inadequate pre-transfusion testing despite these being the focus of the 2016 Annual SHOT Report (published 2017).
Clinical errors related to prescribing and administration are an ongoing concern, and this year there were 12 technical administration error reports. It is perhaps surprising that errors in weight-based prescribing for children are reported so regularly, given that most prescribing of drugs for children is done in this way.
The number of febrile, allergic and hypotensive reaction (FAHR, previously known as acute transfusion reactions (ATR)) reports has fluctuated over the last 10 years (Figure 22.3c). However, the proportion of FAHR to platelets is always high for paediatrics (primarily allergic) and the number of paediatric reports of reactions to platelets is 21/90 (23.3%) of the total reported to SHOT in 2017. This is similar to findings in the past (for example the 2008 Annual SHOT Report, published 2009), and suggests that there are a disproportionate number of platelet reactions in children. However, we do not have current denominator data about the number of platelet units transfused to the paediatric age group.
UCT=unclassifiable complications of transfusion; TRALI=transfusion-related acute lung injury; TAD=transfusion-associated dyspnoea; TACO=transfusion-associated circulatory overload; HTR=haemolytic transfusion reactions; FAHR=febrile, allergic and hypotensive reactions; HSE=handling and storage errors; ADU=avoidable, delayed or undertransfusion; IBCT-SRNM=incorrect blood component transfused-specific requirements not met; IBCT-WCT=IBCT-wrong component transfusion
18
23
31
16
7
36
1
1
1
2
3
82
225
225
243
426
284
42
92
20
3
11
0% 5% 10% 15% 20% 25% 30%
IBCT-WCT
IBCT-SRNM
ADU
HSE
Anti-D
FAHR
HTR
TACO
TAD
TRALI
UCT
Percentage of reports
% of total reports (1671)% of paediatric reports (139)
UCT=unclassifiable complications of transfusion; TRALI=transfusion-related acute lung injury; TAD=transfusion-associated dyspnoea; TACO=transfusion-associated circulatory overload; HTR=haemolytic transfusion reactions; FAHR=febrile, allergic and hypotensive reactions; HSE=handling and storage errors; ADU=avoidable, delayed or undertransfusion; IBCT-SRNM=incorrect blood component transfused-specific requirements not met; IBCT-WCT=IBCT-wrong component transfusion
Figure 22.1:
Percentages of
paediatric and total
reports in each
category

172
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
22. Paediatric Summary
Unclassified
16 to <18 years1 to <16 years>28 days to <1 year ≤28 days
1
2
1
11
15
2
5
2
6
8
1
1
2
1
7
29
14
14
2
7
4
4
3
1
1
2
1
167
36
31
41
Unclassifiable complications of transfusion (UCT)
Transfusion-associated dyspnoea (TAD)
Transfusion-associated circulatory overload (TACO)
Transfusion-related acute lung injury (TRALI)
Haemolytic transfusion reactions (HTR)
Handling and storage errors (HSE)
Anti-D immunoglobulin errors (Anti-D Ig)
Febrile, allergic and hypotensive reactions (FAHR)
Avoidable, delayed or undertransfusion (ADU)
Incorrect blood component transfused (IBCT)
a. Total paediatric reports subdivided by age
Figure 22.3: Trends in paediatric reports 2007-2017 a. Total paediatric reports subdivided by age
12 20 19 15 17 21 24 2741
28 301311 15 20 16 11 12 11
28
172330
43
6068 69
59 48
65
79
7469
18
16
19 1719
18
19
14
17 17
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
55
92
110122 119
110102
122
162
136 139
Unclassified
16 to <18 years1 to <16 years>28 days to <1 year ≤28 days
In 2007 only cases <16 years were included
b. Paediatric reports where specific requirements were not met (SRNM)
16
1114
9 10 11 108
13
75
5
7
5 3
88
4
9
10
3
3 2
4
1 2
3 4
5
11
15
15
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
1918
25
15 15
22 22
17
3332
23
Unclassified
Irradiated/CMV-screenedMB-FFP/SD-FFP/MB-cryoOther SRNM
MB-FFP=methylene-blue treated fresh frozen plasma; SD-FFP=solvent detergent-treated FFP; cryo=cryoprecipitate; CMV=cytomegalovirus
Figure 22.2:
Summary of
paediatric reports
by category and
age for 2017
Figure 22.3: Trends
in paediatric
reports 2007-2017

173
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
22. Paediatric Summary
c. Paediatric febrile, allergic and hypotensive reactions by component type
15
25
37
53
48
28
22
43
26
22
36
19
28
1913
815
5 612
6
7
18
14
17
26
11
12
21
18 15
21
3
83
2
2
7
2
2
112
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Unclassified
Red cellsPlateletsPlasmaGranulocytesMultiple components
Mildreactions excluded
1
1
1
1
Deaths due to transfusion n=0
There were 9 deaths in the 139 cases, all except 1 in neonates and young infants, a highly vulnerable group of transfused patients. None of these were related to the transfusions.
Major morbidity n=15
See the individual chapters for further information: 11 FAHR; 1 IBCT-WCT laboratory; 1 UCT; 1 TACO and 1 TRALI.
Incorrect blood component transfused (IBCT) n=41
IBCT-WCT=incorrect blood component transfused-wrong component transfused; IBCT-SRNM=IBCT-specific requirements not met; MB=methylene blue-treated; SD=solvent-detergent treated
3
1
4
7
4
11
4
1
5
1
2
3
7
3
10
1
3
4
1
2
1
4
15
3
5
23
9
9
18
≤28 days>28 days to <1 year1 to <16 years16 to <18 years
Others
MB- or SD-plasma
Irradiated
IBCT-SRNM Totals
Clinical
Laboratory
IBCT-WCT Totals
Cat
ego
ry o
f IB
CT
rep
ort
IBCT-WCT=incorrect blood component transfused-wrong component transfused; IBCT-SRNM=IBCT-specific requirements not met; MB=methylene blue-treated; SD=solvent-detergent treated
Figure 22.4:
Breakdown of
incorrect blood
transfusion reports
Error-related reports n=95

174
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
22. Paediatric Summary
Figure 22.5
Example of neonatal
emergency paedipack
identification
IBCT-wrong component transfused (WCT) n=18
IBCT-WCT clinical errors n=9
Adult emergency red cell units were used instead of neonatal red cells for 6 infants of different ages. Two occurred immediately following delivery of the babies. One was due to a change in the software of a blood refrigerator so the kiosk did not require the age of patient when accessing emergency blood. One was an infant, who should still have received neonatal/infant specification blood despite being outside the neonatal period.
Learning point
• Neonatal/infant specification blood has additional safety features in view of the particular vulnerability of the recipients. Therefore, it is not appropriate to resuscitate neonates with adult red cells unless there is no available paedipack. Mitigations put in place by hospitals to reduce the chance of selecting the incorrect component by clinical staff include having neonatal and adult red cell units placed in containers with visual identifiers to help staff distinguish between them (for example Fig 22.5)
With permission from Rachel Moss
There were 3 cases of incorrect procedure related to blood collection, sampling or administration. A wrong hospital number was used to collect blood for a neonate. The wrong sample was sent for another which grouped as B D-positive, whereas the correct group was O D-positive on the subsequent sample. (The baby was given O D-negative neonatal red cells in any case). Finally, a small volume of group O D-positive blood intended for another child was transfused to a group A D-positive child on the same day unit due to failure to follow the correct pre-administration bedside check.
IBCT-WCT laboratory errors n=9
Neonatal grouping procedural errors n=4
Two newborn babies were given group O fresh frozen plasma (FFP) issued after only a single grouping test (group O); in that situation they should have been given group AB. There were 2 cases of misinterpretation of neonatal grouping: a weak group A was misinterpreted as group O on two occasions (the second used only a rapid technique) and the baby was erroneously transfused with group O, incompatible FFP. In the other case, the group of a young infant for cardiac surgery was interpreted as A D-positive on one occasion and B D-positive on the other, and they were transfused (with group O red cells) before the error was noted.
D-mismatch errors n=3
Two D-negative babies were incorrectly given D-positive blood. One was delivered several weeks preterm due to severe fetal anaemia and was transfused with O D-positive red cells which the laboratory had already crossmatched against maternal plasma. The neonatal group was subsequently found to be A D-negative. Anti-D Ig was not given as it was felt unlikely that the baby would mount an immune response. The second D-negative infant was given O D-positive blood in an emergency due

175
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
22. Paediatric Summary
to a transcription error by the biomedical scientist (BMS) when manually editing the blood group. On this occasion, it was decided to undertake an exchange transfusion and give anti-D Ig to remove the D-positive red cells (Case 10.1 in Chapter 10, Incorrect Blood Component Transfused (IBCT)). The baby died of their underlying condition. An older child with a D-variant was given 17 D-positive components as the requirement for D-negative blood was not flagged on the record.
Transplant-related blood group selection n=2
Blood was given that was ABO-compatible with a child recipient of a liver transplant but not D-compatible with the donor organ (Case 7.7 in Chapter 7, Laboratory Errors). An older child (group A) undergoing haemopoetic stem cell transplant (HSCT) was given group A red cells despite the protocol specifying group O, an error that was not preventable with the version of the laboratory information management system (LIMS) at the time.
IBCT-specific requirements not met (SRNM) n=23
Non-irradiated n=5
Four cases of missed irradiated components were due primarily to clinical error. A 1-month old baby who had received shared care in three hospitals and had received in-utero transfusions for haemolytic disease of the fetus and newborn did not receive irradiated blood. Non-irradiated cells were given for a young child in priming for a stem cell collection: the laboratory had been misinformed that irradiation was not required, and the error was not detected at the bedside check. Irradiated blood was not requested for a teenager who had received a purine analogue. An older teenager with DiGeorge syndrome was given non-irradiated red cells as the clinical staff did not request irradiated and the historical record was not checked in the laboratory. There was no adverse outcome. One child received non-irradiated platelets despite the requirement being stated on the LIMS.
Non-methylene blue/solvent-detergent plasma (MB/SD) n=3
A neonate was given standard cryoprecipitate having required resuscitation after birth following placental abruption. Local policy would have been to give fibrinogen concentrate in an emergency situation (although it is not licensed for this indication), as the laboratory did not stock MB cryoprecipitate due to infrequency of use. However, there was no alert in place for an age-related component choice for cryoprecipitate. Two teenagers were given standard FFP rather than MB/SD FFP in an emergency; in one the LIMS flag was ignored. It should be noted that some trauma centres where extended thawed standard FFP is held on standby choose to use pre-thawed standard FFP rather than MB/SD FFP in an emergency for paediatric patients as the fastest way of ensuring the child receives FFP.
Learning point
• There should be pre-agreed local policies in place for alternatives that may be used if specific components are not available in emergency situations
Others n=15
Inadequate pre-transfusion testing n=4
Three cases were reported related to neonates. Red cells were issued to a bleeding neonate where the maternal antibody status was unknown in an urgent situation. Later a retrospective crossmatch was not considered. For 2 cases, red cells were issued without serological crossmatch against the maternal sample, despite difficulties in neonatal grouping which should have precluded electronic issue. For an older child, a sample in an expired sample bottle was used for crossmatching.
Failure to use phenotyped blood n=9
A neonate was transfused with O D-negative paedipacks without checking the maternal sample. However, the mother had anti-f antibodies and antigen-negative units crossmatched against the maternal sample should have been used. Blood was issued without crossmatch for 2 infants where

176
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
22. Paediatric Summary
there was evidence of maternal anti-D. The requirement for K-negative red cells for a female infant was overlooked, but if she had been given the appropriate neonatal/infant component this would have been included in any case (New et al. 2016).
Three children with sickle cell disease received Rh-unselected units. In 1 case the laboratory was not informed of the sickle status of the child; another was due to a Blood Service error, and the child subsequently developed an allo anti-C; the 3rd child was transfused a unit of red cells that were not Rh- or K-matched. Another child with sickle cell disease on regular transfusion who required Fya-negative units was given units positive for Fya at a time when the historical records were unavailable due to a cyber-attack. A child with thalassaemia on regular transfusions developed anti-E following transfusion of an E-positive unit.
Missed HEV-screened components n=2
Two children who required hepatitis E-screened components due to their immunological status did not receive them as the laboratory had not been informed.
The underlying causes for many of the laboratory errors are discussed in more detail in Chapter 7, Laboratory Errors, including some paediatric cases illustrating principles of the laboratory errors.
Avoidable, delayed or undertransfusion (ADU) n=31
Over and undertransfusion in paediatric patients contributed 14/24 (54.2%) of all cases of over and undertransfusion.
Avoidable n=9
Transfusion based on the incorrect pre-transfusion result n=5
• A preterm neonate with a pre-transfusion haemoglobin (Hb) of 214g/L was given blood based on the Hb of another baby in the unit
• An infant with acute leukaemia was given a platelet transfusion despite the platelet count waiting confirmation on review of the blood film, which subsequently showed platelet clumps
• A young child was transfused red cells and platelets following an erroneous full blood count (FBC) result taken from a drip arm. Although the error was noted prior to transfusion, the prescription was not amended so the transfusions were given despite the true pre-transfusion results being Hb 101g/L, platelets 46x109/L
• A child with renal failure was transfused on the basis of an older pre-transfusion result (Hb 74g/L), rather than the more recent level of 103g/L, the error being detected by a relative
• A child in oncology received an unnecessary platelet transfusion. This was requested by the oncology centre due to thrombocytopenia, but when the child came to the shared care hospital for transfusion, the latest results were not checked
These cases illustrate the need for vigilance in checking pre-transfusion results and good communication, particularly with the additional complexity of shared care.
Avoidable use of O D-negative red cells n=4
O D-negative emergency units were used for transfusion in emergency neonatal surgery when the crossmatched units had been left out of temperature control in theatre for more than 30 minutes. O D-negative units were also used for a young child undergoing urgent replacement of an extracorporeal membrane oxygenation circuit. Although crossmatched blood was available (according to local policy, less than 4 days old to reduce the risk of hyperkalaemia), a 14-day-old O D-negative emergency unit was used. The other 2 cases were for neonates needing urgent provision of blood but where there would have been time to provide crossmatched units.

177
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
22. Paediatric Summary
Delays to transfusion n=8
Most of the delays to transfusion in the paediatric age group were in neonates (7 cases). Difficulties with laboratory systems contributed to 3 cases: an urgent FFP transfusion for a neonate with pulmonary haemorrhage was delayed because MB-FFP had not been added to the LIMS so could not be issued electronically; a red cell transfusion was delayed due to the absence of a unique identifying number on the pack compatibility label following a printing error; an urgent red cell transfusion was delayed following problems with printing from the LIMS and subsequent transcription errors on the manual transfusion paperwork.
Case 22.1: Emergency units in the satellite blood refrigerator became unavailable due to ‘misuse’ of the blood refrigerator
A neonate born with Hb 41g/L following a fetomaternal haemorrhage required emergency transfusion. A single unit of neonatal emergency blood was taken from the satellite blood refrigerator but the drawer and refrigerator doors were not closed by the staff member who went immediately to the neonate. The refrigerator process was therefore not completed and the remaining member of staff repeatedly selected the only option available to them: ‘press if tray empty’ until the refrigerator stated there was no emergency blood available. Approximately 15 minutes later the neonate required more blood so other units had to be obtained from the blood transfusion laboratory. The baby died 2 days later (it is not clear if the delay contributed).
The design of blood refrigerators needs to be such that in an emergency situation it is easy to access the units required.
Two neonatal exchange transfusions were delayed, one due to various factors including inadequate communication resulting in a delay in provision of K-negative blood by the Blood Service; the other to a delay in the request for and subsequent provision of blood suitable in the context of maternal C, D, E, K and Jka antibodies where there had been no antenatal monitoring. Finally, blood for a neonate was delayed due to investigations into an apparent antibody to a low frequency blood group, complicated by mislabelling of the initial maternal sample.
Overtransfusion n=13
Thirteen of 19 cases of overtransfusion occurred in paediatric patients.
Case 22.2: Unnecessary overtransfusion of a child with red cells following trauma required venesection
A child was punched in the abdomen and the next day seen in the emergency department with haemodynamic instability presumed due to intra-abdominal bleeding. As there was delayed access to the paediatric surgical team due to difficulties with telephone reception and although the Hb was 176g/L, the child was ‘resuscitated’ with two units of red cells. The Hb rose to 208g/L and the child was venesected.
Inadequate clinical assessment resulted in the patient being unnecessarily transfused.
Case 22.3: Lack of understanding causes overtransfusion of an infant
A young child with sepsis, skin necrosis and renal failure weighing 12kg was transfused with two adult units of red cells (approximately 560mL) for postoperative anaemia. The Hb rose from 70g/L before the transfusion to 177g/L after the transfusion. There were no serious sequelae.
This was a volume of 46.7mL per kg. The error in this case was due to the junior doctor’s lack of knowledge of how to prescribe blood components in paediatrics, it was noted in the procedural review that it was their first blood prescription outside adult medicine.
Case 22.4: Overtransfusion of red cells in a child during major haemorrhage
An infant with acute lymphoblastic leukaemia (ALL), weight 9kg, on enoxaparin, suffered major gastrointestinal bleeding with an unrecordable blood pressure and tachycardia of 190 beats per minute triggering activation of the major haemorrhage protocol. The child received 400mL of red cells

178
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
22. Paediatric Summary
(44mL/kg). The pre-transfusion Hb was 111g/L and post was 194g/L. In addition, the child received FFP, platelets and cryoprecipitate. The child was endoscoped, intubated and ventilated related to the major haemorrhage and not the overtransfusion of red cells.
Review of the case noted that it would have been appropriate to monitor the Hb at intervals on the blood gas analyser.
Case 22.5: Transcription error in the weight results in excessive red cell transfusion
A child weighing 33kg with sickle cell disease was overtransfused due to a transcription error with the wrong weight. The amount was challenged by nursing staff but they were advised to carry on as a haematology registrar had written the prescription. Nobody noticed the wrongly transcribed weight.
Lack of knowledge or mistakes in calculation of the prescription by weight was a common error, occurring in 8/13 cases. The errors included failure to prescribe in mL, and misunderstanding the way to calculate transfusion volume for children. The prescribing clinicians included surgeons and haematologists as well as paediatricians.
Undertransfusion n=1
One of 5 cases of undertransfusion occurred in a paediatric patient.
Case 22.6: A junior doctor’s order inappropriately overruled by registrar resulting in undertransfusion
A child weighing 22.5kg was oozing from a gastrostomy site and had Hb 77g/L. The junior doctor ordered one adult unit but the surgical registrar insisted on changing this to two paedipacks, despite advice from the BMS that the original request was more appropriate. The post-transfusion Hb was 71g/L and the child required a second transfusion of an adult unit resulting in an increase to 117g/L.
Learning point
• Clinical staff working in paediatrics need to have training in blood component prescribing in relation to patient weight to avoid potentially dangerous errors. Components should be prescribed in mL. This is particularly important for trainees who rotate from adult medicine. These errors are reported every year. Paediatric guidelines for transfusion should be readily available in all paediatric areas as recommended in recent British Society for Haematology (BSH) guidelines (New et al. 2016)
Paediatric errors related to transfusion pumps n=6 (including 3 from the handling and storage errors section)
There were 3 paediatric overtransfusion errors related to improper transfusion pump setup. Moreover, in the paediatric HSE section there were an additional 3 cases where the incorrect rate was set. Vigilance is needed, particularly in respect to checking rates and volumes administered to paediatric patients where inaccuracies can have significant consequences due to small circulating volumes.
Handling and storage errors (HSE) n=16
Cold chain errors n=2
Platelets were transfused to a neonate having been put in a refrigerator in error, not then queried by the neonatal staff. Red cells were transfused that had been in a refrigerator where the temperature rose to 6.5°C on several occasions without the alarm going off.
Excessive transfusion time n=2
Transfusions to two young infants took more than 5 hours, due to delays in re-cannulation. It is likely that other cases like this on neonatal units may be under-reported and lead to undertransfusions.
Technical administration errors n=12
In 4 cases, an incorrect giving set was used to transfuse red cells to an infant, with standard intravenous

179
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
22. Paediatric Summary
(IV) sets being erroneously used. The filter in a blood giving set has a pore size of 170 to 200 microns, quite different to the filter in a standard IV set which is much smaller. The correct filter will remove any aggregates prior to transfusion into the patient. In 1 case for transfusion to a young child acutely bleeding with a head injury, no set was used at all; the pack was punctured with needle and syringe and the blood was given directly by peripheral venous access.
Incorrect pump settings were reported for 3 cases. In 2 of these, the pump rate was set using the figure for the volume to transfuse. Platelets were transfused using an infusion device for a young child, against local policy stating that they should only be given by free flow.
Case 22.7: Blood from two packs mixed in a syringe for an infant transfusion
An infant was prescribed 58mL red cells. Two paedipacks from the same donor were ordered from the laboratory. The nurse administering the blood mixed both bags into a 50mL syringe and started the transfusion. The remaining 8mL were left in the medication tray out of a temperature-controlled environment and without a label ready to be administered after completion of the first 50mL. Once the error was noted, the 8mL were discarded.
Blood from more than one pack should never be mixed in a syringe, or left unlabelled and separated from the original donation pack. This case illustrates the need for competency assessment in the blood administration process.
Case 22.8: A teenager on haemodialysis received rapid red cell infusion as line not clamped
Prior to haemodialysis for a teenager, the dialysis lines were primed with blood. However, the line was not clamped before starting dialysis, so the patient received one unit of red cells in the first 5 minutes. The staff member giving the transfusion had never given blood before and the unit was extremely busy with a high patient to staff ratio.
Flow rates on dialysis and apheresis machines can be rapid and small children may require red cell priming of apheresis machines, it is essential that staff operating such machines are fully trained.
Anti-D Ig n=7
All were errors in giving anti-D Ig to older teenagers related to pregnancy (see Chapter 14, Adverse Events Related to Anti-D Immunoglobulin (Anti-D Ig)).
Febrile, allergic and hypotensive reactions (FAHR) n=36
The number of cases in this category (previously ‘Acute transfusion reactions’) increased in 2017 (Figure 22.3c). As has usually been the case for paediatrics, in contrast to adults, platelet reactions are the largest group (Figure 22.6a).
• Red cells: 12/36 (33.3%) reports. One child with a febrile reaction required admission and there were 2 severe allergic reactions
• Platelets: 21/36 (58.3%) reports. The majority of reactions (17/21) were allergic, of which 8 were severe (Figure 22.6b) including 2 from patients transfused with platelets pooled in platelet additive solution (PAS). There was a single moderate hypotensive reaction in a young child who had sepsis and pneumonia. Overall, there were 18 reports associated with apheresis platelets and 3 with pools in PAS. This is in line with the recommendation that paediatric patients should be transfused with apheresis platelets where possible. One of the apheresis platelet reports was associated with washed platelets in PAS, requested as the patient had previously had anaphylaxis following human leucocyte antigen (HLA)-matched platelets. One patient had also received contrast agent in association with a scan, a possible alternative precipitant of the reaction. In 20 patients where the underlying diagnosis was given, all were haematology/oncology/HSCT patients except 1 with
Transfusion reactions n=44

180
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
22. Paediatric Summary
pneumonia. For recommendations related to FAHR in association with platelets see Chapter 16, Febrile, Allergic and Hypotensive Reactions (FAHR)
• Plasma components/products: 2/36 (5.6%) reports. Both were moderate mixed allergic/febrile reactions to Octaplas®, one occurring during a plasma exchange. There were no reports of reactions to MB plasma in 2017
• Granulocytes: 1/36 (2.8%) reports. There was a moderate mixed/febrile reaction to granulocytes transfused to a neutropenic teenager with leukaemia and sepsis
a. Comparison of proportions of adult and paediatric FAHR related to different components
Unclassified
Multiple components (8)Granulocytes (1)Plasma (18)Platelets (90)Red cells (167)
155
12
69
21
16 218
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Adult Paediatric
b. Percentages of reaction types for each component for paediatric reports
5
27
4
9
13
2
810
11
2 1
5
1 1
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Red cells Platelets Plasma Granulocytes Total
HypotensiveMixed allergic/febrileAnaphylactic/severe allergicModerate allergicFebrile
Figure 22.6:
Paediatric
febrile, allergic
and hypotensive
reaction (FAHR)
reports

181
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
22. Paediatric Summary
Haemolytic transfusion reactions (HTR) n=1
A child <10 years old with multiple comorbidities including postoperative bleeding was noted to have anti-Jka in a pre-transfusion sample following two transfusions in the previous 2 weeks. She had evidence of a delayed transfusion reaction on blood tests and this may have contributed to her low Hb (see Chapter 19, Haemolytic Transfusion Reactions (HTR)).
Transfusion-associated circulatory overload (TACO) n=1
Case 22.9: Probable TACO in a child with newly-diagnosed leukaemia
A young child with probable newly diagnosed ALL was admitted with bleeding and coagulopathy. Prior to diagnostic procedures and line insertion the child was given platelets and cryoprecipitate, and platelets rose to >100x109/L. The child also required hyperhydration to reduce the risk of tumour lysis syndrome. As the line was oozing overnight further platelets were transfused as the instructions in the notes had said to transfuse platelets if bleeding (and had omitted to say ‘if platelets <50’). This was despite the child being in significant positive fluid balance at the time. Subsequently the child became acutely unwell, requiring oxygen and admission to the paediatric intensive care unit (PICU) for non-invasive ventilation. The child responded to diuretics and was diagnosed with TACO.
The case illustrates the vulnerability of children at the time of leukaemia diagnosis and the need for careful consideration of TACO particularly while receiving hyperhydration as well as transfusion. However, reports of TACO in children are uncommon, with only 1/92 total SHOT reports in 2017 of TACO in the paediatric age group, possibly due to under-recognition or uncertainty in diagnosis (De Cloedt et al. 2018).
Transfusion-associated dyspnoea (TAD) n=1
This was a reaction following a granulocyte transfusion in a teenager with fever and sepsis on treatment for acute myeloid leukaemia. Following transfusion, the patient reported chest tightening, and the oxygen saturations dropped (see Chapter 18c, Transfusion-Associated Dyspnoea (TAD) for full details). The same patient had a FAHR after the previous transfusion.
Transfusion-related acute lung injury (TRALI) n=2
There were 2 reports. A child <10 years of age with acute leukaemia had acute respiratory deterioration and hypotension requiring ventilation, which occurred within 30 minutes of a platelet transfusion. The clinical condition improved following adrenaline and furosemide. A teenager on PICU following a liver transplant was transfused red cells for a Hb of 61g/L and 4 hours later had respiratory deterioration with non-specific chest X-ray changes. Both cases are reported in detail in Chapter 18a, Transfusion-Related Acute Lung Injury (TRALI), and the overall conclusion was that they can be considered as confirmed cases of TRALI.
New or unclassifiable complications of transfusion (UCT) n=3
There were 3 cases of transfusion-associated necrotising enterocolitis (TANEC) reported in preterm babies (see Chapter 20, New or Unclassifiable Complications of Transfusion (UCT) for details). For one, symptoms of NEC developed shortly after transfusion, whereas the other two were 12-24 hours later.
Near miss (NM) n=72 and right blood right patient (RBRP) n=13
See Chapter 12, Near Miss Reporting (NM) and Chapter 8, Right Blood Right Patient (RBRP) for full details, including 44 cases of incorrect identification between mother and baby (n=36) or between neonatal twins (n=8). Overall 43/44 were wrong blood in tube errors.
References
BSH New HV, Berryman J et al. Guidelines on transfusion for fetuses, neonates and older children. Br J Haematol 2016;175:784-828.
De Cloedt L, Emeriaud G et al. Transfusion-associated circulatory overload in a pediatric intensive care unit: different incidences with different diagnostic criteria. Transfusion 2018;58(4):1037-1044.

182
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
23. Haemoglobin Disorders: Update
Author: Paula Bolton-Maggs
Forty-five incidents were reported. The majority were instances where the specific requirements were not met n=15, clinical errors in 4 and laboratory errors in 11, followed by haemolytic transfusion reactions n=14, 13/14 in patients with sickle cell disease (SCD). There were no deaths directly related to complications of transfusion; one woman with SCD died (Case 19.1 Chapter 19, Haemolytic Transfusion Reactions (HTR)) due to complications of SCD. The median age was 22, range 2 to 70 years; only 10 were over 40 years of age, in contrast to the median and ranges of the transfused population overall reported to SHOT: median 50 years, range 0 to 101.
Major morbidity occurred in 6 patients with SCD where transfusion was complicated by hyperhaemolysis. These are discussed in Chapter 19, Haemolytic Transfusion Reactions (HTR). There were 3 additional cases of major morbidity in febrile, acute and hypotensive reactions (FAHR) where the patients were admitted following their reactions.
a) Sickle cell disease n=193
14.5%
5.7%3.6%
38.3%
35.8%
1
1
2
7
11
28
69
74
TTITAD
TACOIBCT
ADUFAHR
SRNM
HTR 1.0% 0.5% 0.5%
FAHR=febrile, allergic or hypotensive reactions; ADU=avoidable, delayed or under or overtransfusion; IBCT=incorrect blood component transfused; SRNM=specific requirements not met; TACO=transfusion-associated circulatory overload; TAD=transfusion-associated dyspnoea; HTR=haemolytic transfusion reactions; TTI=transfusion-transmitted infection
Figure 23.1:
Cumulative data for
adverse events in
transfusion for patients
with haemoglobin
disorders 2010 to 2017
Haemoglobin Disorders: Update23

183
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
23. Haemoglobin Disorders: Update
b) Thalassaemia n=50
8.0%
26.0%
42.0%
12.0%
10.0%
2.0%
1
5
6
21
13
4
TACOIBCT
ADUFAHR
SRNM
HTR
FAHR=febrile, allergic or hypotensive reactions; ADU=avoidable, delayed or under or overtransfusion; IBCT=incorrect blood component transfused; SRNM=specific requirements not met; TACO=transfusion-associated circulatory overload; TAD=transfusion-associated dyspnoea; HTR=haemolytic transfusion reactions; TTI=transfusion-transmitted infection
Careless practice n=4
Delay was reported for an exchange transfusion for a young pregnant woman with sickle cell disease but the clinical area did not inform the laboratory of the pregnancy so cytomegalovirus (CMV)-screened antigen-matched units had to be re-ordered. The patient had her day-case admission rearranged. The prescriber was a registrar in haematology.
An avoidable transfusion occurred in a thalassaemia patient on regular transfusions because the pre-transfusion haemoglobin (Hb) 116g/L, was not reviewed until the second unit was in progress. The authoriser had written up three units to be transfused ‘because this was the amount she usually received’.
A child with SCD was overtransfused due to transcription of the wrong patient weight. Another child had a wrong transfusion rate set up (to give the total volume in 1 hour).
Specific requirements not met n=15
Clinical causes n=4
In all 4 instances (all SCD) the clinicians did not inform the laboratory, in 3 cases that these were patients with SCD and in the other that the patient was pregnant. In 2/3 cases there were serial errors that could have been detected including the correct diagnosis on subsequent requests that the laboratory failed to notice. The pregnant patient received 26 CMV-unscreened units in a series of exchange transfusions. Although ‘CMV-screened’ was included on some requests the reporter noted that their laboratory information system was not able to flag CMV requirements for pregnancy in addition to the requirements for SCD.
Laboratory causes n=11
A young child in sickle crisis developed an alloantibody after receiving a unit crossmatched by the Blood Service which was not matched for the extended Rh phenotype despite full phenotype information available from the red cell immunohaematology (RCI) laboratory report.
A woman in her 60s with SCD and subarachnoid haemorrhage was admitted to a hospital where she was not previously known. Another hospital was contacted for further information; she was known to

184
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
23. Haemoglobin Disorders: Update
have three historical antibodies not currently detectable but there was a verbal communication error resulting in transfusion of inappropriate antigen-positive red cells. The information was also available from Specialist Services Electronic Reporting using Sunquest ICE (Sp-ICE) but the biomedical scientist (BMS) did not have access to this as she had not been competency-assessed and this incident occurred overnight. Shortage of resources was cited. As a result of this incident all BMS staff now have access to Sp-ICE, and any antibodies identified there can be added to the laboratory information management system (LIMS).
The remaining incidents were mostly caused by failure to note the clinical information, failure to search for historical transfusion results, or simple errors in red cell selection. The majority showed more than one error with a maximum of six in one case, i.e. there were other opportunities to detect the first error (failure to note the SCD on the request form in a patient new to that hospital where transfusion was urgent).
Wrong transfusions n=2
A child with beta thalassaemia was transfused with the wrong unit. Two nurses checked the unit against the prescription and medical records. The blood was run through a giving set and then the nurses repeated the procedure for another unit destined for a second patient. They then took one unit to the bedside, checking the name and date of birth against the prescription. The transfusion was connected and begun before one of the nurses checked the unit label and realised this was the wrong patient. Fortunately, although ABO-non-identical (patient group A, unit group O), this was not an incompatible transfusion.
This was a basic failure to perform the procedure correctly. The unit must be checked with the patient identification (ID), not the prescription. This was a serious error. As a result, all day-unit staff were retrained and the two staff involved were prevented from performing the bedside checks until competency had been re-assessed.
A child with SCD was identified as having a D-variant but this was not entered properly into the LIMS so that 17 D-positive components were given for elective transfusions. As a result, the laboratory checked the extended genotype file for any similar cases, updated flags and all BMS staff are to be given access to Sp-ICE.
Febrile/acute allergic/hypotensive transfusion reactions n=8
(7 SCD, 1 beta thalassaemia)
The age range was 6-34 years. Four of the 7 patients with SCD were on exchange transfusion programmes. After the reaction a child under 10 years of age with complex antibodies was changed from an exchange programme to top ups.
Haemolytic transfusion reactions n=14
Thirteen of these were in patients with SCD, 1 with beta thalassaemia. One woman in her 40s died related to complications of SCD following caesarean section (Case 19.1 in Chapter 19, Haemolytic Transfusion Reactions (HTR)). She also had hyperhaemolysis.
Near miss n=2
A unit of red cells was recalled by the specialist laboratory as it was not Jkb-negative. Communication was poor but the unit was changed to a compatible one prior to transfusion to a woman in her 20s with SCD.
The second case was a teenager with SCD in whom excessive transfusion was avoided in a sickle crisis by rechecking the unexpectedly low Hb result and adjusting the authorised volume.

185
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
23. Haemoglobin Disorders: Update
Commentary
People with SCD are at risk of serious transfusion complications including haemolysis resulting in death (Chubar and Bisharat 2017). To reduce the risk of alloimmunisation patients should have a full red cell phenotype recorded at diagnosis and in England can be fully genotyped including Rh variants which enables more appropriate red cell selection (Rees et al. 2018). Every transfusion should have a clear indication (Chinchilla Langeber et al. 2018), and good communication with the transfusion laboratory is essential. Delayed haemolytic transfusion reactions with hyperhaemolysis are serious and difficult to manage (Pirenne et al. 2017). Patients should be monitored for early recognition of this complication so that urgent measures can be taken to manage it. Confusion is caused by the similarity between features of haemolytic reactions and the symptoms of SCD complications.
Revised standards for the clinical care of adults with SCD in the UK have been published (May 2018) (Sickle Cell Society 2018). These can be downloaded from the Sickle Cell Society website.
References
Chinchilla Langeber S et al. When a transfusion in an emergency service is not really urgent: hyperhaemolysis syndrome in a child with sickle cell disease. BMJ Case Rep 2018;doi/10.1136/bcr-2017-223209.
Chubar E and Bisharat N. Fatal delayed haemolytic transfusion reaction in a patient without previous transfusions but with an obstetric history of 13 pregnancies. BMJ Case Rep 2017;doi/10.1136/bcr-2017-222343.
Pirenne F, Bartolucci P and Habibi A. Management of delayed hemolytic transfusion reaction in sickle cell disease: Prevention, diagnosis, treatment. Transfus Clin Biol 2017;24(3):227-231.
Rees DC, Robinson S and Howard J. How I manage red cell transfusions in patients with sickle cell disease. Br J Haematol 2018;180(4):607-617.
Sickle Cell Society. Standards for the clinical care of adults with sickle cell disease in the UK. 2nd Edition:2018 www.sicklecellsociety.org.

ANNUAL SHOT REPORT 2017
186 Acknowledgements
Acknowledgements
The Steering Group takes this opportunity to thank the following individuals and organisations for their contributions without which the publication of this 21st Annual SHOT Report would not have been possible:
• The Blood Services of the United Kingdom for funding and support
• The Royal College of Pathologists to which SHOT is affiliated
• The Blood Services of the United Kingdom for the provision of data relating to the issue of blood components:
– Miss Helen Livingstone, National Product Manager-WB, NHSBT
– Ms Amanda Stewart, Principle Transfusion Data Analysis Manager, SNBTS
– Mr Edward Stack, Management Information Analyst, SNBTS
– Mrs Chloe George, Head of Manufacturing & Distribution, WBS
– Mrs Pauline Gowdy, Hospital Services Manager, NIBTS
– Mrs Martina McCalmont, Senior Biomedical Scientist, Hospital Services Department, NIBTS
– Mr Andy Rowley, Therapy Area Lead, Critical Care - UK and Republic of Ireland, Octapharma Ltd for data relating to SD-FFP (Octaplas®)
• The expert group who reviewed TRALI cases:
– Dr Neil Soni, Chelsea and Westminster Hospital
– Dr Cliff Morgan, Royal Brompton Hospital
– Dr Tom Latham, NHSBT Bristol
– Dr Nay Win, NHSBT Tooting
– Dr Peter Davis, Bristol University Hospitals NHS Foundation Trust
– Dr Rob Webster, Consultant Haematologist, NHSBT Sheffield
• Clinical and scientific staff, in hospitals and reference laboratories, who have contributed to the clinical and laboratory investigation of cases
• Toast Design Consultancy Ltd for maintenance of the SHOT website
• Dendrite Clinical Systems for the update of the online reporting system
• Lisa Parker, SHOT Administration Office Manager
• ARC-UK Technologies for design and production of the report
• Hospital Transfusion Teams for submitting case reports to the scheme

187
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
Author: Chris Robbie
Introduction
The United Kingdom (UK) Blood Safety and Quality Regulations 2005 (as amended) (BSQR) require that serious adverse events (SAE) and serious adverse reactions (SAR) related to blood and blood components are reported by blood establishments, hospital transfusion laboratories and facilities to the MHRA, the UK Competent Authority (CA) for blood safety. This requirement is enabled by the serious adverse blood reactions and events (SABRE) reporting system. All data in this report are correct as of 22 January 2018.
Key message
• Assessment of some serious adverse blood reactions and events (SABRE) reports support anecdotal evidence from reporters at regional meetings, SHOT Symposia and other conferences that staffing, workload and skill-mix problems are affecting laboratories’ performance in meeting the requirements of the Blood Safety and Quality Regulations (BSQR). This also reflects the findings of the UK Transfusion Laboratory Collaborative (UKTLC) surveys. However, it is not always evident from the root-cause analyses that the error reported is linked to staffing, workload and skill-mix problems in the laboratory. Reporters are encouraged to continue to thoroughly investigate serious adverse events (SAE) and serious adverse reactions (SAR) and report not just how an error occurred, but to report why it occurred. Reporters must aim to address all root causes and contributory factors to allow the Medicines and Healthcare Products Regulatory Agency (MHRA) and SHOT to gather as much information as possible related to the apparent staffing and workload problems experienced by laboratories
Summary
In the second full year of MHRA and SHOT viewing all reports and deciding which meet the individual organisation’s reporting requirements, more SAE and SAR have been reported in 2017 than in 2016. The European Commission recognises that high numbers of reports may indicate a healthy reporting culture in a member state compared with a member state that does not report any at all (EU 2016). More detailed analysis shows the rate of increase in SAR is greater than the increase in the numbers of SAE and that the increase in SAE comes mainly from Blood Establishments rather than hospital reports.
Many SAE reports indicated the pressures that laboratories are under related to staffing, workload and skill-mix problems. MHRA inspection data indicate that more hospital blood compliance reports (BCR) were assessed as ‘high risk’ in 2016/17 and one of the main findings at inspections was related to resource failings by Hospital Trust/Health Board senior management (not laboratory management).
The total number of SAE received from hospitals (i.e. excluding blood establishment SAE) remains similar to previous years, although there are differences in the reporting patterns in some categories. There has been anecdotal evidence from reporters that they are being discouraged from reporting, or are not able to report at all. While this may be true in some cases, it would appear that most reporters are able to actively engage in UK haemovigilance. This is evidenced by the increase in total number of reports received and the fact that all except 31 SABRE accounts have made at least one report since January 2017 (see Figure 2.1 in Chapter 2, Participation in UK Haemovigilance).
Medicines and Healthcare Products Regulatory Agency (MHRA) Report 24

188
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
A question therefore arises, why has the level of hospital transfusion laboratory SAE reporting not increased to reflect the evidence of staffing, workload, skill-mix and resource problems? Are reporters prevented from reporting due to time or senior management pressure, or have quality management systems (QMS) been made robust enough to prevent adverse events from becoming serious, or resolved at the time they occurred?
Denominator data
Comparing SAE data to a previous year’s data can be very complex. It is not as simple as, say, comparing the number of reactions to the number of donations transfused since one component can only cause one reaction. SAE can occur at any step in the vein-to-vein processes and it is not possible to calculate a finite number of steps where an error can occur. Therefore, there is no relationship in the number of SAE to any kind of denominator data.
Furthermore, the perception of what might make an event ‘serious’ can be subjective, and changes to a reporting organisation’s personnel can therefore have an effect on the numbers of SAE reported.
SABRE report data
Table 24.1 and Figure 24.1 display the total number of SABRE confirmation reports that were submitted and satisfy the European Commission reporting criteria for SAR and SAE since 2008. Since even old data are live, and subject to amendment. Table 24.1 has been updated to reflect changes to historic reports.
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
SAE 790 968 889 810 931 705 762 764 1027 1076
SAR 436 501 549 444 343 345 346 262 464 508
Total 1226 1469 1438 1254 1274 1050 1108 1026 1491 1584
0
200
400
600
800
1000
1200
1400
1600
1800
2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Serious adverse eventSerious adverse reactionTotal
This is the second full year that data have been available to both organisations following changes to the UK Haemovigilance system made in October 2015. Although comparisons can be made between 2016 data and 2017 data it is not possible to identify any trends.
Table 24.1:
Submitted SABRE
confirmation
reports 2008–2017
Figure 24.1:
Submitted SABRE
confirmation
reports 2008-2017

189
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
The total number of reports has increased by about 6% compared to last year, however that is a result of an increase in SAR by about 9% and SAE by about 5% meaning most of the increase in reports has come from SAR reporting. In fact, further assessment of SAE figures shows that the majority of the increase in SAE (49) reports has come from blood establishments, SAE reports n=66 in 2016 and n=109 in 2017, +43.
Serious adverse events
Definition: Any untoward occurrence associated with the collection, testing, processing, storage and distribution, of blood or blood components that might lead to death or life-threatening, disabling or incapacitating conditions for patients or which results in, or prolongs, hospitalisation or morbidity.
HSE=handling and storage errors
11
3
717
251
41
22
16
11
1
1
1
1
0 100 200 300 400 500 600 700 800
Other
Storage/HSE
Whole blood collection
Distribution/HSE
Processing
Testing of donations
Materials
Apheresis collection
Equipment failure
Human error
Other
Product defect
HSE=handling and storage errors
Similar to previous years there is no real change in the proportions of each category of reported SAE. ‘Other’ and ‘storage’ categories contain the most reports, and human error remains the main root cause.
Storage data n=255 (+20)
Storage remains the second largest individual error category and includes all BSQR reportable storage SAE in both the laboratory and clinical areas. For a breakdown of handling and storage errors (HSE) in the laboratory and the clinical area, please see the relevant sections of the Laboratory Errors (Chapter 7) and HSE (Chapter 9) chapters. The MHRA has subclassified ‘storage’ reports further to try and identify specific error subtypes, Table 24.2. For a description of the subcategories used, see Appendix 24.1.
Storage subclassification 2017 (+/-2016) 2016 position
Component expiry 74 (+8) 2
Incorrect storage of component 68 (-17) 1
Sample expiry 46 (+14) 3
Return to stock error 19 (+4) 4
Failure to action alarm 19 (+12) 7
Storage temperature deviation 8 (-4) 5
Security 8 (+3) 8
30-minute rule 7 (-1) 6
Miscellaneous 6 (+1) 9
Total 255 (+20) x
Figure 24.2:
2017 SAE
confirmation
reports by
deviation and
specification
Table 24.2:
SAE storage error
subclassification
2017

190
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
Despite still being the second most commonly reported storage SAE, reports of incorrect storage of component have decreased since last year. These errors can occur when any component is placed in an incorrect storage location whether in the laboratory or in clinical areas.
Failure to action alarm has seen an increase in number of reports from 7 to 19 and 11/19 were found to be due to inadequate processes. Factors involved in these reports included equipment not adequate for the task e.g. the temperature monitoring computer logging out, processes not being adequately designed to fully describe what actions to take and processes not being designed to be sufficiently robust to work out-of-hours when fewer laboratory and clinical staff are available to take the required actions.
The first and third most common storage SAE are related to component and sample expiry. These are SAE where components have time-expired and have not been removed from the supply chain in a timely manner or where the component is still in date but the patient sample has expired. Although different errors, the systems in place to manage these situations are often linked and so have been assessed in greater detail below. Collectively these errors account for n=120/1076, 11.2% of all SAE reported.
QMS=quality management system
29
18
14
4
4
3
19
9
6
5
22
2
2
1
Inadequate process
Procedural steps omitted/wrong procedure performed
Procedure performed incorrectly
Inadequate QMS-staffing and workload
Inadequate training
Ineffective training
Incorrect procedure
Lapsed/no training Sample expiryComponent expiry
QMS=quality management system
Last year the most common cause for these errors was inadequate processes and it remains the case this year. There are several measures that laboratories can take to manage expiring components and samples which include:
• Checks at various times of the day depending on staffing levels and workload
• Physical checks of storage locations where practical
• Interrogation of the laboratory information management system (LIMS) to produce lists of expiring components
• Removal of close-to-expiry components from clinical areas to allow a final check by laboratory staff if the component is required
Whatever methods are used, it is imperative that the process is properly designed to identify expiring components and to prevent them from being transfused. The design of the process must take into account whether staff are able to perform the task in a timely manner when there might be competing pressures from other tasks, and procedures must be written to include detailed instructions as to what checks to perform and how to perform them to facilitate training of new staff.
Figure 24.3:
Sample and
component expiry by
specification 2017

191
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
Case 24.1: Red cell units left in refrigerator long after their de-reservation date
A number of units of red cells were left in the blood refrigerator at an off-site private hospital beyond their de-reservation dates. Two of those units were left for more than a week beyond their de-reservation date and therefore could have been transfused when the sample was no longer valid. The patient for whom those two units had been issued had known blood group antibodies.
The investigation identified multiple factors that resulted in an inadequate process for managing the use of off-site refrigerators. The paperwork did not alert staff to when units had reached their de-reservation dates and the need to be removed. Training had been left to medical laboratory assistants (MLA) who had not used the standard operating procedures (SOP) as training material, relying on ‘word-of-mouth’, and vital aspects of the process had been forgotten and not relayed. The corrective measures included re-design of the paperwork and re-education of staff involved in both the process and noted the importance of adequate training.
Other n=726 (+8)
Since ‘other’ is the largest category of SAE reports, the MHRA haemovigilance team has created subcategories to further analyse this type of error, Table 24.3. For a description of subcategories, see Appendix 24.2.
Other subcategory 2017 (+/- 2016) 2016 position
Incorrect blood component issued (IBCI) 175 (-17) 1
Sample processing error (SPE) 123 (-11) 2
Component labelling error (CLE) 114 (+8) 4
Pre-transfusion testing error (PTTE) 104 (-6) 3
Component collection error (CCE) 94 (+16) 5
Data entry error (DEE) 71 (+13) 6
Failed recall (FR) 18 (+1) 7
Unspecified (UNSPEC) 9 (+7) 10=
Component available for transfusion past de- reservation (CATPD) 5 (+2) 9
Expired component available for transfusion (ECAT) 5 (+3) 10=
Incorrect blood component ordered (IBCO) 5 (-9) 8
Handling damage (HD) 2 (0) 12
Incorrect blood component accepted (IBCA) 1 (+1) 13
Total 726 (+8) x
175
123
114
104
94
71
18
9
5
5
5
2
1
Incorrect blood component issued (IBCI)
Sample processing error (SPE)
Component labelling error (CLE)
Pre-transfusion testing error (PTTE)
Component collection error (CCE)
Data entry error (DEE)
Failed recall (FR)
Unspecified (UNSPEC)
Incorrect blood component ordered (IBCO)
Component available for transfusion past dereservation (CATPD)
Expired component available for transfusion (ECAT)
Handling damage (HD)
Incorrect blood component accepted (IBCA)
Table 24.3:
SABRE reports,
subcategory ‘other’
2017
Figure 24.4:
SABRE reports
subcategory ‘other’
2017

192
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
The total number of reports that fall into the ‘other’ category is similar to last year and the relative proportions of incidents in each subcategory also remains similar. However, there are some marked differences in reporting patterns. There have been reductions in the number of reports associated with incorrect blood components issued (IBCI) and pre-transfusion testing errors (PTTE). These are processes which, although they involve manual steps and human factors, can be controlled by LIMS, equipment, education and training. A reduction in these SAE could be a result of:
• Better controls in LIMS
• Improvements in processes and procedures
• Improved understanding of the processes and procedures
• Changes to the provision of HEV-screened blood (i.e. no longer reported as all cellular components are HEV-screened)
Increases have been seen in component labelling errors (CLE) and data entry errors (DEE). These are processes which are not easily controlled by equipment and electronic processes, and rely more heavily on manual steps and concentration. Conversely, there is a reduction in sample processing errors (SPE), which rely heavily on laboratory staff noticing discrepancies in labelling, forms and LIMS. Reduction in these incidents could be a result of:
• Improved sample collection processes
• Improvements to laboratory environments and reduction of distractions
• Highlighting the importance of thorough checking and concentration
There has also been an increase in component collection errors (CCE). These can occur when laboratory staff hand over components at collection, but typically involve clinical staff and porters collecting components from storage locations. Often these are the result of lapses of concentration, but analysis also suggests that staff are often poorly trained in collection processes, whether they involve electronic systems or not, and system bars and warnings are ignored or over-ridden.
Human error category and human factors
Human factors are all the things which can influence how a human behaves. These will either lead to an action being successful, or it will lead to human error and can be organisational, job-related or related to the individual concerned.
To better understand human error, the SABRE team has developed subcategories which can be applied to the report narratives to help understand the human factors involved. For a description of these categories, see Appendix 24.3. Table 24.4 shows the breakdown of reports in the human error subcategories.
Human error subcategory Total (+/- 2016)
Procedure performed incorrectly 291 (+22)
Procedural steps omitted/wrong procedure performed 237 (+54)
Inadequate process 211 (+16)
Ineffective training 119 (+1)
Inadequate QMS – staffing and workload 80 (-23)
Inadequate training 46 (0)
Incorrect procedure 40 (-9)
Lapsed/no training 25 (+4)
Inadequate supervision 9 (-13)
Total 1058 (+52)
Table 24.4:
SABRE reports,
human error
subcategory 2017

193
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
QMS=quality management system
291
237
211
119
80
46
40
25
9
Procedure performed incorrectly
Procedural steps omitted/wrong procedure performed
Inadequate process
Ineffective training
Inadequate QMS—staffing and workload
Inadequate training
Incorrect procedure
Lapsed/no training
Inadequate supervision
QMS=quality management system
NOTE: These numbers should be used as guidance only. The quality of these data are limited by a number of factors:
• The root causes of incidents are usually the result of many contributory factors. The subcategory chosen reflects the most likely reason for the main SAE category
• The subcategory chosen is based on the information in the report. A limited investigation or a report which does not provide the MHRA with enough information may not be subcategorised appropriately
The distribution of categories remains similar to last year. Procedures performed incorrectly, missed steps, or wrong procedures followed account for the most of all SAE attributed to human error. These are typically errors resulting from slips or lapses of concentration by individuals after other aspects of the quality system have been ruled out.
Staff should be able to cope with a certain pressure of workload and distractions, and simply being busy should not be used as an excuse for errors. The quality of work is the responsibility of individual staff and they should take time to ensure they ‘get it right first time’. Staff should be encouraged to prioritise their workload and use the support mechanisms available when they need to, such as delaying non-urgent work, or calling staff for extra support from other laboratories.
It would be wrong to suggest that over half of the SAE are the result of poor concentration. Staff are reported to be under pressure from poor staffing levels, inadequate skill mixes and high workloads. Distractions can also affect concentration and can come from interruptions by other staff, telephone calls, equipment breaking down or not being available and multitasking. Quality systems should be designed to be robust and help prevent staff from falling victim to slips and lapses. This will include, but is not limited to:
• Adequate working environment (e.g. lighting, space, equipment, logical design)
• Adequate staffing and skill mix
• Appropriate workloads
• Robust processes
• Accurate procedures
• Adequate training
• Access to information and expertise
• Leadership and supervision
Figure 24.5:
SABRE reports,
human error
subcategory, 2017

194
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
Many report narratives hold staff solely responsible for the errors made. While in some cases this may be true, poor quality investigations and reports overlook the systems factors that led to staff behaving and acting in a way that resulted in error. The MHRA will often contact reporters to clarify details of their SABRE reports and discuss improvements to quality systems which may help prevent errors, but this cannot be done for every single report. It is possible that many of the SAE reports which fall into the ‘procedure performed incorrectly’ and the ‘procedural steps omitted/wrong procedure performed’ categories could be assigned to different subcategories with a more detailed SAE report.
Reports that indicate staff error as the primary cause of the SAE without a thorough investigation may account for fewer reports being assigned the category ‘quality system – staffing and workload’. Fewer reports in this category compared to last year should not be seen as an improvement in staffing and workload problems. The 80 reports indicated above were assessed to directly result from staffing and workload problems, however, many of the SAE reports that occurred in the other subcategories may have been indirectly related to staffing and workload problems. For example, a sample and form were sent to the laboratory with a different address to the one recorded on the LIMS. This sample was sent towards the end of the day during a busy time and the discrepancy was not noticed due to rushing the checking process. There was no valid reason for rushing the process, despite being busy; however, rearranging the workflow at this busy time could alleviate the pressure on the staff and their perception that they need to rush to complete the work.
Top 5 SAE
‘Procedure performed incorrectly’ and ‘procedural steps omitted/wrong procedure performed’ account for over half the SAE reported and can affect any type of SAE. Since managing these types of error has been discussed above, the top 5 types of error have been assessed considering the remaining root cause types only.
SAE deviation subcategory Specification subcategory
Incorrect blood component issued (IBCI) Inadequate process
Pre-transfusion testing error (PTTE) Inadequate process
Sample processing error (SPE) Inadequate process - staffing and workload
Component collection error (CCE) Ineffective training
Incorrect blood component issued (IBCI) Ineffective training
The following cases are included to illustrate what might be considered by way of corrective and preventive action (CAPA) to address the root causes. They are not meant to represent actual investigation processes and CAPA for all similarly categorised incidents, but are representative of many of the reports received, and are clearly designed to focus on improvements to systems, practice and transfusion laboratories.
Case 24.1: Incorrect blood component issued (IBCI) – inadequate process (Case 10.8 in Incorrect Blood Component Transfused (IBCT), Chapter 10)
Five units of group O fresh frozen plasma (FFP) were issued and transfused to a group A patient. A telephone request was taken and the correct patient’s name and hospital number were written down. The investigation revealed that the wrong hospital number was copied and pasted from a different patient record and used to populate the LIMS and the wrong blood group and sample accession number obtained. These incorrect details were then transcribed to the telephone request form. Units of the incorrect group were thawed and issued to the patient. This error could have been discovered sooner when the porter came to collect the units because the porter recognised that the patient details on the label did not match the details on the collection form. The discrepancy was not thoroughly investigated and the units were re-issued to the correct patient without noticing the discrepant group.
When the units arrived at the bedside, although checks were made, it was assumed that group O FFP was compatible with the patient whose blood group was A. A further request for cryoprecipitate was processed by a different biomedical scientist (BMS) and it was only at this point that the mistake was noticed.
Table 24.5:
Top 5 SAE with
human error
subcategory

195
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
The hospital transfusion team could have concluded the root cause of the SAE to be a lapse in concentration that occurred when the wrong details were selected and transcribed, however they conducted a thorough investigation and wrote a comprehensive investigation report which highlighted numerous QMS failures. More importantly, however, they were able to identify CAPA which targeted exactly the root causes and make significant improvements to their QMS.
Contributory factors identified included:
• The current version of the LIMS was old and did not allow staff to move easily between programmes. A project to implement a new LIMS had stalled a number of times
• The telephone request form did not include a verification step to ensure the correct information had been recorded
• Although there were instructions in the SOP to use each programme in the LIMS the SOP did not detail how to enter the hospital number, and more importantly to verify that the correct hospital number and other details had been used
• The blood component issue SOP did not detail that verification checks of the manual information on the telephone request form matched the details entered on the LIMS
• There was no SOP to detail the return of incorrectly issued components and their re-issue
• When re-issuing the FFP, it was assumed that the correct blood group had been issued to the wrong patient, and there was no check that the component issued was suitable for the correct patient
• When the FFP was issued to the correct patient, warnings that the incorrect group had been issued were not heeded and the LIMS did not prevent their issue
• There was a knowledge gap regarding compatibility of FFP groups by the administrator
• There were procedural steps omitted by operators and missed by the laboratory supervisor
The investigating team also considered staffing/workload and skill-mix factors, but concluded that these were not factors in the event.
In addressing these factors and other issues arising from the investigation, the hospital transfusion laboratory staff were able to:
• Re-state their need for a new LIMS and revive the project to implement the new one
• Re-evaluate their processes and re-design them
• Re-write SOP to include missing instructions and steps
• Re-assess competence of staff and re-train where necessary
• Review new-starter and trainee BMS capacity proportional to number of appropriately trained staff available to undertake supervision
• Review adequate staffing levels and develop procedures for escalating unmanageable workloads
In all, 28 recommendations were identified to improve the QMS.
Case 24.2: Pre-transfusion testing error (PTTE) – inadequate process
A sample used for crossmatch and issue of red cells was 8 days old. The investigation revealed that old samples were not being discarded early enough in the day.
The CAPA to resolve this error was simply to change the process to discard old samples earlier and to update the LIMS system to recognise and not process samples that are too old.

196
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
Case 24.3: Sample processing error (SPE) - inadequate process - staffing and workload
A crossmatch sample was received with an incorrectly spelt last name and used to issue 2 units of red cells before the discrepancy was noticed. This was also reported to be a repeat error for the laboratory.
As discussed above, SPE are often a result of slips and lapses of concentration. However, there is much evidence in SABRE reports to indicate that staffing and workload pressure are directly affecting the ability of staff to work safely, causing them to rush and either skip steps in a procedure or not identify often slight discrepancies. In this particular report, the reporter identified that a recent increase in workload, as a result of severe staff shortages, was affecting staff morale by increasing stress in the laboratory. The reporter also indicated that these staff shortages had led to a delay in being able to thoroughly investigate the error.
More worryingly the reporter stated that often staff were being encouraged NOT to report SAE to SABRE. Anecdotal evidence given to the MHRA during meetings and other discussions have also indicated that laboratory managers are being encouraged to give false information on the BCR. If any SABRE reporter finds themselves in this position they should remind them of their legal responsibilities under the BSQR. Also, the MHRA will assess any information provided by whistleblower, https://www.gov.uk/guidance/contact-mhra#whistleblower-referrals.
Case 24.4: Component collection error (CCE) – ineffective training
A patient had platelets and plasma allocated. The patient required plasma, but the porter incorrectly collected the platelets, failing to perform the correct checks other than the patient name. Although the porter had been trained, it was the first time they had collected anything other than red cells and they had got confused between the two components. Instead of stopping and contacting the laboratory for advice, they continued to collect the wrong component.
When delivering training, not only must it cover all aspects of the task, but must also cover what to do if things do not go to plan. Often staff may not perform tasks regularly, and the training may have been delivered some time before they need to carry out a procedure. It is not unreasonable to assume that staff may have forgotten some of the aspects of that training. It may seem like common sense that someone should ask for help or advice when stuck, but staff must be reminded of this when they are being trained. Also, if staff having forgotten some of their training this may be an indication that training needs to be delivered more frequently for some tasks and for some staff groups.
Case 24.5: Incorrect blood component issued (IBCI) – ineffective training
A patient born after 1 January 1996 was issued and transfused with 8 units of FFP instead of Octaplas® (solvent-detergent FFP). The member of staff thought they were following the correct protocol as they incorrectly thought Octaplas® (or methylene blue-treated FFP) should be issued to patients under the age of 16.
As a result of this, a specific requirements flag was added to the patient’s record. Report narratives suggest that some LIMS do not prevent staff from overriding flags and warnings and components have been issued with incorrect specific requirements. The addition of flags is important, but should not be considered in isolation as effective CAPA to prevent IBCI errors.
Figure 24.6 shows the ‘other’ subcategory and root cause for all SAE other than procedural steps omitted/wrong procedure performed and procedure performed incorrectly.

197
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
See Figure 24.4 for key to category abbreviations
35
6
7
27
12
7
7
4
2
11
20
11
12
1
6
1
1
4
1
8
1
8
8
1
1
1
10
6
2
8
2
1
1
1
16
7
4
15
20
2
3
2
1
1
4
1
1
5
1
0 10 20 30 40 50 60 70 80 90 100
IBCI
SPE
CLE
PTTE
CCE
DEE
FR
UNSPEC
CATPD
ECAT
IBCO
HD
IBCA Inadequate processInadequate QMS—staffing and workload Inadequate supervisionInadequate trainingIncorrect procedureIneffective trainingLapsed/no training
See Figure 24.4 for key to category abbreviations
Blood establishment reporting n=109 (+43)
The majority of SAE reports originate from hospital transfusion laboratories. Although reports from blood establishments are included in the main analysis, the specific nature of the SAE reports from blood establishments are lost in the greater numbers of reported hospital transfusion laboratory SAE. Figure 24.7 displays the reported blood establishment SAE in 2017.
1
41
26
16
12
8
1
3
1
0 10 20 30 40 50
Whole blood collection
Other
Processing
Testing of donations
Distribution/HSE
Storage/HSE
Apheresis collection
Equipment failureHuman errorProduct defect
HSE=handling and storage errors
The SAE reported from blood establishments demonstrate an almost identical pattern to last year, except that they have reported in much greater numbers, with errors at donation remaining the single biggest category. The reason for the sharp rise in the number of SAE reports from blood establishments is unclear, but could simply be greater awareness of what should be reported.
Figure 24.6:
‘Other’ subcategory
root causes
Figure 24.7:
Blood
establishment
SAE category by
specification

198
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
Assessment of the ‘other’ category, Figure 24.8, once again shows that failed recalls are the main error. SAE in the ‘incorrect blood component issued’ and ‘pre-transfusion testing errors’ demonstrate that blood establishment laboratories are liable to making similar errors to hospital laboratories,
See Figure 24.4 for key to category abbreviations
8
8
6
1
1
1
1
FR
IBCI
PTTE
UNSPEC
CLE
DEE
ECAT
See Figure 24.4 for key to category abbreviations
Serious adverse reactions (SAR)
Definition: an unintended response in a donor or in a patient that is associated with the collection, or transfusion of blood or blood components that is fatal, life-threatening, disabling or incapacitating, or which results in or prolongs hospitalisation or morbidity…blood establishments and the person responsible for the management of a hospital blood bank shall notify the Secretary of State (Competent Authority) of any serious adverse reactions observed during or after transfusion which may be attributable to the quality or safety of blood or blood components:
(i) Collected, tested, processed, stored or distributed by the blood establishment, or
(ii) Issued for transfusion by the hospital blood bank
Blood products
Adverse reactions involving blood products (i.e. licensed medicines such as anti-D Ig, Octaplas®, or coagulation factor concentrates should be reported to the MHRA via the Yellow Card scheme (http://yellowcard.mhra.gov.uk).
Summary of SAR report data
To avoid any confusion the MHRA will only supply, in this Annual SHOT Report, total SAR numbers reported to Europe, Table 24.6.
Imputability score
NA 0 1 2 3
SAR reports by imputability score 7 76 185 181 59
Figure 24.8:
Blood
establishment
SAE ‘other’,
‘human error’ by
subcategory
Table 24.6:
SAR reports,
by imputability,
reported to SABRE
in 2017 n=508

199
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
76
185 181
59
7
0 1 2 3 Not assessable
Imputability level
MHRA inspection activity on hospital blood banks 2016-2017
Author: Graham Carroll
A total of 299 blood compliance reports (BCR) were submitted for review for the reporting period 01 April 2016 to 31 March 2017. Twenty-seven hospital blood banks (HBB) including 6 control sites were selected for inspection; this included sites under the oversight of the Inspection Action Group (IAG) and Compliance Management Team (CMT) following previous inspections.
Inspection outcomes
Inspections for the reporting period 01 April 2016 to 31 March 2017 are performed in the following year, i.e. from 01 April 2017 to 31 March 2018. At the time of writing, a total of 19 inspections had been performed at 18 sites, and the numbers of deficiencies are as follows:
Critical Major Other
0 42 76
Five HBB had significant deficiency findings related to their operations and were escalated to the CMT. This is a significant increase over the previous year. Common deficiency groups identified from these inspections included:
• Senior management not fulfilling their responsibilities
• Non-conformances/incidents/events and CAPA implementation
• Change control management
• Self-inspection
• Resourcing and training
• Failure to complete previous commitments
• Data integrity failures
An overview of the compliance management escalation processes used by the good manufacturing practice (GMP) inspectorate, including information on the IAG and CMT referral processes, is available from the MHRA inspectorate blog: https://mhrainspectorate.blog.gov.uk/2017/02/06/overview-of-compliance-management-escalation-processes-used-by-the-gmp-inspectorate/.
Figure 24.9:
SAR reports,
by imputability,
reported to SABRE
in 2017
Table 24.7:
MHRA inspection
deficiencies

200
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
QMS=quality management system; CAPA=corrective and preventive actions
11111
233
45
66
79
17
Laboratory operationsPremises/equipment
Transport/distributionTraceability
Outstanding commitmentsRecall
Self-inspectionDocument control/data integrity
Qualification/validationManagement review
CAPA implementationQMS implementation
Personnel (inadequate resource)/trainingChange control
Incidents/non-conformances
QMS=quality management system; CAPA=corrective and preventive actions
QMS=quality management system; CAPA=corrective and preventive actions
12222
4444
5666
91313
CAPA implementationQMS implementationManagement review
Transport/distributionTraceability
Incidents/non-conformancesChange controlSelf-inspection
Qualification/validationOutsourced activitiesPremises/equipment
RecallComputerised systems
Personnel (inadequate resource)/trainingLaboratory operations
Document control/data integrity
QMS=quality management system; CAPA=corrective and preventive actions
Summary of significant issues identified at inspected sites
Senior management responsibilities
Senior management has the ultimate responsibility to ensure an effective quality system is in place, that it is adequately resourced and that roles, responsibilities, and authorities are defined, communicated and implemented throughout the organisation. In a number of cases, senior management was not adequately monitoring the performance of the QMS to ensure that it was effective and adequately resourced. Examples of this included:
• Management meetings were not performed at the specified frequency
• Reports reviewed by senior management lacked appropriate metrics to detect that the QMS was not functioning correctly
• Meeting minutes were not prepared, or did not identify actions to be taken (including timelines and responsibilities) to address poor performance of the QMS
Figure 24.10:
Categories of major
deficiencies found
Figure 24.11:
Categories of other
deficiencies found

201
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
In some inspections, the number of systems found to be deficient indicated that there were insufficient resources to maintain an effective QMS at the same time as ensuring service delivery. Further investigation identified failings such as:
• A quality manager who was available for less than 0.1 whole time equivalent (WTE) for transfusion
• A laboratory manager with overall responsibility for quality but insufficient time to fulfil this responsibility due to required time on the bench
• No resource plan to define the required resource levels to support operational delivery and the quality system
Non-conformances/incidents/events and CAPA implementation
Incident investigations continue to be an area of concern. Example deficiencies include:
• No defined timeframes for raising, assessing, investigating, and closing incidents
• Failing to record incidents in the QMS
• Poor risk-management practices, such as not considering potential harm or detectability when determining the risk level, and not having an immediate criticality assessment when an incident occurs
• Late, incomplete or missing investigation of the root cause(s) of an incident
• Attributing incidents to human error without a documented assessment of potential process, procedural and system causes
The lack of effective investigation of incidents has a knock-on effect on CAPA implementation. An effective investigation process should ensure that CAPA are appropriate and address the root cause(s) of the incident; the CAPA process should also ensure that actions taken are effective. Issues with CAPA processes included:
• Significant numbers of overdue CAPA
• No tracking of the number of CAPA currently open, and progress towards completion
• Lack of effectiveness checks
Change-control management
Given the criticality of the testing performed by transfusion laboratories, it is concerning that issues with the control of changes continue to be cited in a high number of major deficiencies. Examples of system weaknesses included:
• Change controls not raised for significant changes, such as new equipment, new processes, software version changes for critical systems, and headcount reduction
• Lack of effective tracking and oversight of ongoing change controls
• Risks that had been identified were not addressed before implementation of changes
• Failures and deviations during execution of validation testing were not assessed or addressed before implementation of changes
• No review after implementation of changes to determine whether the change had been effective, and also to confirm that the change had not adversely impacted on other activities

202
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
Self-inspection
Self-inspection is an important mechanism to identify weaknesses and implement improvements. Inspections have identified issues with audits not being performed and non-conformances not being recorded promptly. Where audits are not performed in accordance with the pre-determined programme, this should be documented in the quality system so that an investigation can be performed to assess the impact and determine the root cause.
Resourcing and training
A capacity plan should be put in place to demonstrate that the staffing level is sufficient to cover the workload including out-of-hours working and effective implementation of the QMS. Where a shortfall is identified, senior management should take action to ensure sufficient resource will be made available. Job descriptions and organisation diagrams should be in place and made available to all staff.
It is expected that staff are trained in their duties, the QMS, and good practice. The effectiveness of training should be periodically assessed. Inspections identified overdue reassessment of laboratory staff as well as porters collecting and transporting blood components. An example was also noted of cleaners who were given unsupervised access to laboratory areas but who had not received GMP training. GMP awareness training for contract service providers including contract cleaners and transport providers is required as their work can have an impact on patient safety and component quality.
Failure to complete previous commitments
MHRA inspections are closed on the basis of the commitments given to address any deficiencies identified. Closure indicates that the inspector (or CMT/IAG if applicable) have accepted the commitments given; any delay or change to these commitments should be proactively communicated to the MHRA. Examples identified at inspection included significant delays to projects, failure to complete document reviews, and removing additional resources once the inspection was closed.
Failure to adhere to commitments given, or to proactively communicate changes to the MHRA, is seen as a high-risk factor as it can be indicative of a poor-quality culture in the organisation. In a number of cases this failure has led to the direct involvement of Chief Executive Officers (CEO) and an escalation to compliance management processes within the MHRA.
Data integrity
Poor documentation practice and data integrity was the most cited ‘other’ deficiency but was also cited in major deficiencies in a number of inspections. Examples included:
• False and misleading information was presented to the inspector, including falsified dates, images of signatures which had been applied by another party, and modification of screenshots. It should be noted that depending on the impact of the data, provision of false and misleading information can result in critical deficiencies being cited
• Poor documentation practices such as uncontrolled deletions, obliteration and overwriting in documents reviewed during the inspection, impeding the ability to reconstruct an activity from the available records
• No mechanism to ensure that staff were aware of changes in procedures at the time they became effective
• Legacy procedures still in place with no overall clarifying index or document to demonstrate which local QMS documents were regarded as live for the transfusion area
• Emergency login details for electronic systems were openly available
It is important to apply the basic ALCOA principle to all data, whether written or electronic. ALCOA means that data are Attributable, Legible, Contemporaneous, Original and Accurate.

203
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
Traceability
The expectation is that the fate of every unit of blood or blood component is known and documented. The traceability of blood components remains a concern, with a major deficiency cited for significant failures to ensure that the fate of all blood components was confirmed. Specific concerns included:
• Poor overall traceability compliance
• No clear plans or actions taken to address poor compliance
• Failure to escalate risks to the appropriate level in the organisation
• Ineffective systems to monitor traceability compliance, such as groups not meeting at the specified frequency
• Traceability compliance deteriorating during the implementation of an electronic traceability system
The final point above is an important reminder that introducing an electronic system cannot, in itself, solve issues with traceability compliance. The traceability system relies on adequate and timely resources, effective training, robust record keeping and an effective system for reporting and investigating non-compliance.
Security of blood components
Storage areas should provide properly secure and segregated storage. Examples of deficiencies in security included:
• Security bypass mechanisms being open for all users
• Electronic systems not being maintained to ensure that access rights were removed for users who had left the organisation, changed roles or were no longer up to date with their training
Laboratory operations
At a number of inspections, deviations were cited for operations in the laboratory which were not consistent with good practice. Examples included:
• No formal justification available for the sample preparation centrifuge speed adopted; in addition, procedures still referenced the previous speed
• Prepared solutions within the laboratory were ineffectively labelled to identify the contents, details of preparation, and expiry
• Cause of internal quality control (IQC) failures were not consistently documented
Changes for 2017–2018
Inspections for the reporting period 01 April 2017 to 31 March 2018 will be performed in the following year, i.e. from 01 April 2018 to 31 March 2019. In response to the compliance trends identified during 2016–2017, the MHRA have notified HBB of changes to the BCR and inspection programme.
Following the adoption of the Good Practice Guidelines for blood establishments into UK law, from 01 April 2018 the MHRA will inspect blood establishments and hospital blood banks against these guidelines. All deficiencies identified at inspections (including other deficiencies) will be referenced to these guidelines, and references to EU GMP will no longer be required.
Information and guidance
For further information on the MHRA and the regulation of blood please refer to the MHRA website: https://www.gov.uk/topic/medicines-medical-devices-blood/blood-regulation-safety.
The MHRA blood forum was launched in June 2016 as a tool to help those involved in blood component collection, processing, testing and distribution to comply with the EU Blood Directives, UK

204
ANNUAL SHOT REPORT 2017 REACTIONS IN PATIENTS
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
Statutory Instruments and good practice requirements. It provides the ideal opportunity for extended communication between peers and allows users to put forward their comments and get ‘real-life’ examples of ways in which they can manage robust quality procedures that ensure compliance and which dovetail with their own business needs and resources.
http://forums.mhra.gov.uk/forumdisplay.php?60-Blood-Forum.
Appendices
Appendix 24.1: Storage subcategoriesComponent expiry A component has time expired and not been removed from the storage location
according to laboratory procedures
Incorrect storage of component A component has not been stored in the correct location
Sample expiry A sample has expired and the component has not been removed from the supply chain for the original patient
Return to stock error A component has been returned to the supply chain in error instead of being quarantined or discarded
Failure to action alarm A storage location alarm has been activated but not actioned according to the procedure
Storage temperature deviation The storage temperature has gone out of specification without an alarm being activated
Security A storage location is accessible to staff or public who are not authorised to do so
30-minute rule Red cells are returned to a refrigerator after 30 minutes have elapsed contrary to local procedures for return of unused red cells
Miscellaneous Any other storage event affecting the quality and safety of blood or blood components
Appendix 24.2: Other subcategoriesIncorrect blood component issued (IBCI)
Blood issued which does not meet the patient’s specific requirements
Sample processing error (SPE) Sample incorrectly receipted into the laboratory that should have been rejected
Component labelling error (CLE) Typically, transposition of labels
Pre-transfusion testing error (PTTE)
Any error in the process of testing patient samples and the interpretation of results
Component collection error (CCE) Any error in the collection of components from storage locations, or the handover of components on collection from the laboratory
Data entry error (DEE) Transcription errors of data, including both electronic and hand-written data
Failed recall (FR) Failure to recall components in a timely manner
Unspecified (UNSPEC) Any error affecting the quality and safety of components not specified elsewhere
Component available for transfusion past de-reservation (CATPD)
Expired components which were incorrectly collected, prior to their scheduled re-stock by the laboratory
Expired component available for transfusion (ECAT)
Any component issued for a patient, where the component expires prior to the planned transfusion
Incorrect blood component ordered (IBCO)
Components ordered from a blood establishment that do not meet the patient’s specific requirements
Handling damage (HD) Damage to a component affecting its quality and safety
Incorrect blood component accepted (IBCA)
Blood accepted into a laboratory for a specific patient where the specific requirements have not been matched

205
REACTIONS IN PATIENTS ANNUAL SHOT REPORT 2017
24. Medicines and Healthcare Products Regulatory Agency (MHRA) Report
Appendix 24.3: Human error subcategoriesProcedure performed incorrectly Failure to carry out a step(s) correctly
Procedural steps omitted/wrong procedure performed
Missing a key step or not following the procedure
Inadequate process Inadequate design of a process
Incorrect procedure Process not properly described in the SOP
Ineffective training Training not understood by operator
Inadequate training Training process not fit for purpose
Lapsed or no training Carrying out a procedure without any formal training
Inadequate QMS – staffing and workload
Staffing levels below the minimum level, or unacceptably high workload has resulted in staff making errors. It is also important to consider an appropriate skill-mix when deciding on minimum staffing levels
Inadequate supervision Errors have been made by trainees or inexperienced members of staff and should have been noticed by adequate supervision
References
BSQR. Blood Safety and Quality Regulations. (SI 2005/50, as amended) http://www.legislation.gov.uk/uksi/2005/50/contents/made [accessed 3 April 2018].
EU: Summary of the 2016 annual reporting of serious adverse reactions and events for blood and blood components (page 12) https://ec.europa.eu/health/sites/health/files/blood_tissues_organs/docs/2016_sare_blood_summary_en.pdf [accessed 3 April 2018].
Good Practice Guidelines for blood establishments https://www.edqm.eu/en/good-practice-guidelines-blood-establishments [accessed 3 April 2018].

If you would like more information on SHOT please contact:
The SHOT Office, Manchester Blood Centre, Plymouth Grove, Manchester M13 9LL
Telephone: 0161 423 4208Email: [email protected]: www.shotuk.org
All SHOT publications must be considered as bound by the copyright statement within the SHOT Annual Report
working with
Affiliated to the Royal College of Pathologists
ANNUAL SHOT REPORT 2017
AN
NU
AL
SH
OT
RE
PO
RT
2017
SE
RIO
US HAZARDS OF TRANSFU
SION
AN
NU
AL SHOT REPORT 21ST A
NNIV
ER
SA
RY
YEARS