Embed Size (px)
DESCRIPTION
Lisa Quinn Executive Director Performance and Assurance. Annual Plan 2014 - 2019. Major change from last year Integrated strategic and operational planning process for 2014 i.e. CCGs, Foundation Trusts, non Foundation Trusts and Local Government (via Health and Wellbeing Boards) - PowerPoint PPT Presentation
Citation preview

Annual Plan 2014 - 2019
Lisa Quinn
Executive Director Performance and Assurance

Annual Plan requirements
• Major change from last year
• Integrated strategic and operational planning process for 2014 i.e. CCGs, Foundation Trusts, non Foundation Trusts and Local
Government (via Health and Wellbeing Boards)
• Initial guidance issued and a 2 year and 5 year plan is required-but precise requirements still not clear
• Guidance on precise requirements and content due out week commencing 16th December
• The Trust’s Plans will continue to reflect IBP (October 2012) and Transformation of Services

Provisional Timetable-Key Dates• 10th December 2013-Joint Council of Governors/Board of Directors• w/c 16th December 2013-Monitor Guidance, Templates and Tools
issued• 13th January 2014-Initial high level plan submitted to Monitor• 20th March 2014-Council of Governors Full Meeting (review of draft
2 year plan)• 26th March 2014-Board of Directors approval of 2 year plan• 4th April 2014-Submission of final 2 year plan to Monitor• 15th May 2014-Council of Governors Full Meeting (to sign off 5 year
plan)• 28th May 2014-Board of Directors approval of 5 year plan• 20th June 2014-Submission of 5 year plan• 15th July 2014-Council of Governors Full Meeting (review of
Summary Annual Plan)• Annual Members Meeting-Circulation of Summary Annual Plan

Annual Plan Working Group
Thank you to all of those that volunteered to be members.
• Council of Governors Representatives/constituency: Austen O’Malley-Public Marion Moore-Service User Grahame Ellis-Staff Ann Clark-Carer
• Meetings-monthly January 2014-June 2014
• Chair - Steve Brooks, Head of Commercial Support

Questions

Council of GovernorsTransforming Services
10 December 2013

The environment in which we work:
• We have to improve quality for the patient
• We have to reduce our overall cost of doing so by 20%
• We aim to improve clinical effectiveness thus reducing reliance on inpatient beds
• We have to create sustainable services, delivered by sustainable organisations, operating in a sustainable system
Quality
Cost
Sustainability
-20%
Strategic Direction

What we are told nationally:
• ‘Call to Action’ and ‘Closing the Gap’ reports highlight that the NHS needs to radically transform to meet the current quality, safety and financial challenges
‘The NHS… needs to develop and implement bold and transformative long
term strategies and plans for their services, otherwise they will become
financially unsustainable and the safety and quality of patient care will decline’
Joint letter to the NHS and Local Authorities, 4th November 2013

What our partners have told us:
• We have to get much better at what we do and how we do it
• We have to get better at listening and acting on what people are telling us
• We have to be consistently good across all our services
• We need to get the patient quickly into the right services and then deliver the best outcome possible
GPsCommissioners
Local
Authorities
3rd Sector
Other providers

What patients and carers have told us:
• They want high-quality, safe care close to home
• They want inpatient services to be of a high standard
• They want services designed and operated around the needs of patients
• They want the patient to be truly ‘at the centre’
• They want to gain and re-gain independence, as far as possible
Patient

The Service Model
Request for Help
Initial ResponseInitial evaluation regarding nature, risk, complexity and urgency of the problem
Discharge
PICU Crisis Beds
Low Security Intermediate beds
Acute WardChallenging Behaviour
Assessment
Intensive Home
TreatmentEtc.
Very severe & complex
non-psychotic
Psychosis DementiaNeuro -
disabilityLearning Disability
Children & YoungPeople
Mild -severe non -
psychotic
Signposting to principal service pathway for assessment and formulation Scaffolding
Information & Advice
In the Community
At Home
SubstanceMisuse
More Intensive Packages of Care
Crisis Assessment
Challenging Behaviour Assessment Formulation
& Treatment Planning
Specialist Ward Environment
Acute Ward
Intermediate Facility
Crisis Bed
Intensive Home Treatment
Low Security
Medium Security
Psychiatric Intensive Care
Treatment Intensity
Hospital
Hom
e

SMR Principles• You should reach us, quickly and simply• The earlier the better• To get the right help and care, safely and easily• From our flexible and skilled workforce• In collaboration with you and your carers and partnership
organisations• So that you can gain / re-gain independence, as far as
possible• By making smooth and sustainable steps forward• Reaching us again, simply and quickly

The need to realign and balance resources:
• We spend in inpatient areas to the detriment of community services
• A few patients consume much of the resource
• Many in-patients perhaps don’t need to be, but we lack the necessary community services to support them out of hospital
• We need to balance resources to maximise quality over cost
Inpatient Services
Community Services
£92.2MNTW Whole
costs
£84.8MNTW Whole
costs
At any time, 3% of patients are consuming 52% of resources

Principal Community Pathways

Principal Community PathwaysA programme to design and implement new, evidence-based community pathways for adults and older people.
Our ambition is high and is matched by the expectations of service users and carers. The new pathways will:
• Significantly improve quality for the patient
• Double current productive time of community services by redesigning current systems
• Enhance the skills of our workforce
• Improve ways of working and interfaces with partners
• Reduce reliance on inpatient beds and enable cost savings
This is not achievable in isolation and to be successful we need it to be part of integrated work with partners
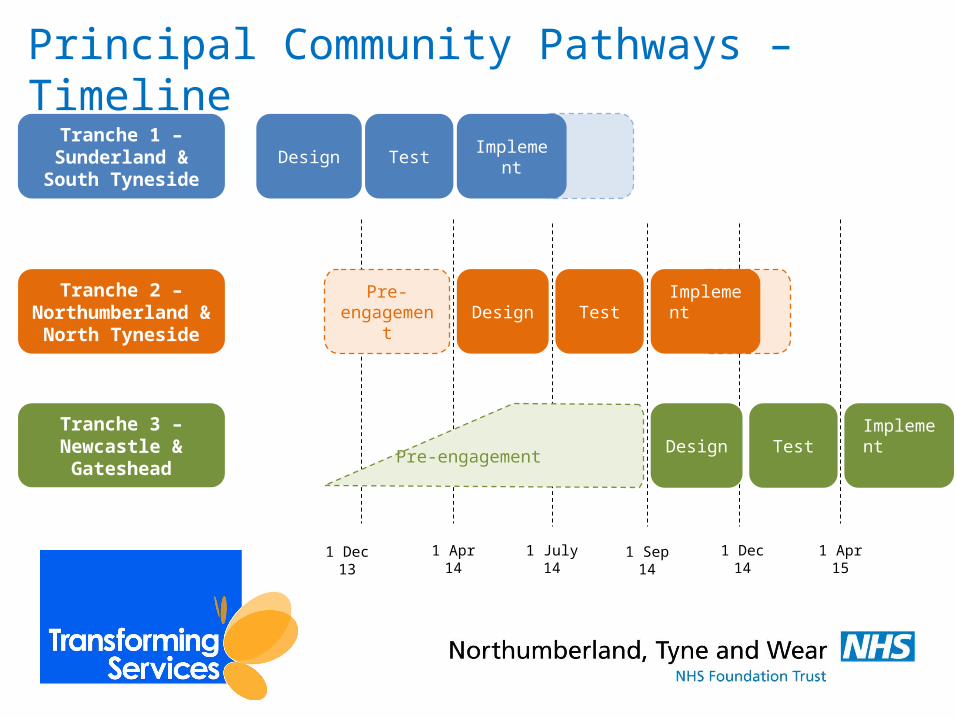
Principal Community Pathways – Timeline
1 Dec 13
Design Test Implement
Design Test
1 Apr 14 1 July 14
Implement
1 Sep 14 1 Dec 14
Pre-engagement
Design Test Implement
Pre-engagement
1 Apr 15
Tranche 2 – Northumberland &
North Tyneside
Tranche 3 – Newcastle & Gateshead
Tranche 1 – Sunderland & South
Tyneside

Principal Community Pathways – How people have been involved
So far 362 people have attended the 27
clinical and supporting systems workshops,
these have included: GPs, Local Authority
staff, Acute Trust staff, Community and
voluntary sector staff, CCG staff, NTW staff
and most importantly our service users and carers.
• Our Trust-wide Service User and Carer Reference Group has been involved throughout
• We have presented our plans to various groups including HealthNet and South Tyneside GP Education Forum
• We’ve been ‘walking the wall’ with all of our stakeholders and have so far run sessions for over 800 people – with more to follow

So what is so different?

Access
Single point of access for service users, carers and referrers, open 24/7
Service Users and carers are able to self-refer to services within the scope of Principal Community Pathways
Referrals are accepted by telephone, letter, email and fax
Clear single point for obtaining advice and information, including clinical advice
Wider hours of operation for community services
Service User is contacted within 24hrs of referral being received and offered choice of venue and time for appointment.
Service User is asked how they would prefer to be contacted in the future e.g. letter/phone/email/text/Skype.
There are no waiting lists for patients
Opportunity for easier and more streamlined route back into services should this be required following discharge
Multiple points + times of access.
Referral Source + methods vary area to area.
Bouncing.
No standardisation of allocation meetings.
Access to clinical advice variable quality + recording variable
Service users are often sent an appointment letter after the allocation meeting, with no choice of day, time or venue
Community services operate 9 to 5 in most areas
Most contact with service users is by letter, limited use of phone calls and text messaging reminders.
Many teams have waiting lists for assessment and for treatment
Multiple routes for re-engagement into services by historical service users, no clear route back in
Current State Future State

Assessment & FormulationFirst appointment date is within 7 days of referral being received (agreed)
Service User offered a choice of appointment days/times/venues
Service Users given information and invited to tell us a little about their life using a “introduction to me” before assessment to feel more prepared
Service User can choose to receive a text message or phone call to remind them of the appointment
Where clinic appointment is required, Service User is greeted by front of house staff where demographic information is checked and an explanation of their visit is provided
Where required, Service Users will also receive a full baseline physical health check.
Where appropriate, carers involved throughout the assessment and formulation process
Service user and carers will leave with a plan and a clear understanding of what will happen next
First appointment date may be several weeks after referral being received
Limited choice of appointment days/times/venues
Service Users often unprepared for the assessment, giving rise to anxiety and is a cause of DNAs
Very limited use of reminders of appointments, often just one appointment letter sent out with no follow up
Mixed availability of reception services at clinical venues, and mixed customer service skills
Limited access to physical health check facilities, many service users not offered this option
Current State Future State

Treatment
Service Users continue to have the choice of text message or phone call reminders for appointments
Service Users receive treatment in the form of clinical interventions and /or medication as agreed in their treatment plan and in line with NICE guidance with clear review points to monitor/change care where appropriate
Service Users will have access to Peer Support Workers as well as community workers to help them with benefits, housing, social issues
Service Users will receive treatment and care in the most suitable environment
Service Users, Carers and other professionals will be able to call a review
Care plans will be developed collaboratively with the patient/carers where appropriate
Service Users often only receive a single letter about an appointment, without options to receive reminders
Service Users receive mixed levels of treatment in the form of clinical interventions and/or medication, as agreed in their treatment plan
Service Users have mixed access to community support to help them with benefits, housing, social issues
Service Users receive treatment and care in a range of environments which are not always the most suitable
Care planning is not always developed collaboratively with the Service User/carers
Current State Future State

Discharge
The term ‘discharge’ will only be used when the service user is leaving NTW services in their entirety – otherwise, the terms ‘transfer’ and ‘transition’ will be used
Discharge process is part of treatment and the Service User will feel prepared for the discharge.
Any disputed issues will be resolved prior to last meeting.
Service User will agree a discharge plan including how to ‘stay well’ and what steps they should take in the event of a relapse
Carers will be involved throughout discharge planning
Service Users are often ‘discharged’ by one part of NTW while care continues to be provided by another part, which is confusing to them, carers and referrers
Discharge planning is not a standardised approach
Often service users return to NTW because of unresolved issues in the wider world (social issues, housing, benefits, welfare), for which they receive varied levels of support across services
Service Users do not always have a clear plan of how to ‘stay well’ and what steps they should take in the event of a relapse
Carers are not always involved in discharge planning, and their needs are not always directly considered
Current State Future State

Mark’s
Story

MarkMark is 38yrs old and has struggled with low mood and paranoid thoughts all of his life. He had a difficult upbringing, his Dad beat him from a young age and would always pick fights and criticise him. Mark left home at 16 years old. He spent many years on the street, took a lot of drugs and was in and out of prison for a few years.
He was staying in B&Bs but has recently got a place in a supported living block. He finds it difficult as he feels paranoid most of the time and thinks people are talking about him. He hears the voice of his Dad continuously – criticising him and telling him how useless he is. He used to take ODs or get as smashed as he could to stop the voice, he was always in A+E or being brought in by the police but nowadays he tends to just withdraw to his room. He smokes a lot of weed which sometimes relaxes him.
He has seen a psychiatrist in the past and they put him on a tablet. It made him feel blank and tired and it put weight on him which he hated, so he stopped taking it. He sees his GP quite regularly for this and that. He’s been referred back to the mental health team a few times but only seen a CPN once for 20 mins and finds it difficult to get in touch with him. He admits he’s missed a few appointments. He really wants to stop the voice and improve his mood but he thinks nobody’s bothered about him because he doesn’t cause trouble anymore.
His doctor asks him to rate his mood on a scale of 1 to 10. It’s 1.

Mark
Process step
Mark is able to ring one number.
The single point of access service is available 24/7
Mark is contacted within 24hrs of referral being received and offered choice of venue and time for appointment.
Mark’s GP is able to contact the same number for support or advice about Mark’s care
NTW will work in collaboration with social care, and 3rd sector partners to support Mark
Mark is provided with information about what to expect from his visit to NTW
Mark will be sent a ‘introduction to me’ pack where he can prepare for his first assessment
If deemed necessary Mark will also receive a full baseline physical health check.
Mark’s care plan will be developed collaboratively with him
Mark’s discharge planning commences at this point
Mark will receive treatment in line with NICE guidance.
Treatment package tailored to his needs.
Mark will have access to Peer Support Workers and Recovery College to help him with important issues.
Mark can request a Review at any point.
Mark’s GP will have access to an advice line where they can speak directly to an NTW psychiatrist or pharmacy about any issues in relation to Mark’s care.
Upon discharge Mark will agree a discharge plan including how to ‘stay well’
Mark’s discharge plan will also include what steps he should take in the event of a relapse
Mark’s GP will also receive a copy of this plan along with any early warning signs and initial management plan

Augmenting Services

Total beds per 100,000 of population within the Mental Health Care Packages & Pathways consortium

What does this mean for inpatient services?Our aim for in-patient services is to ensure that when service users need to be in hospital, they are looked after in •an appropriate environment, •which is properly staffed, and •delivers effective interventions which are focussed on recovery •supporting people to step down out of hospital, as soon as their needs allow

Elm House
Monkwearmouth
Brooke House
Rose Lodge
CAV
Northgate
QE
The Grange
St Nicholas
St Georges
Male AcuteFemale AcutePICULDOPS (func.)
URGENT
OP Organic
PLANNED
Stepped Care
S Tyneside DH
Cherry Knowle
Bed Model Current State(42 Wards April 2013)

What does this mean for inpatient services?
• Overall, across the Trust we are looking to reduce in-patient provision for adults and older people’s services from the current level of 723 beds to around 425.

Ward Grouping Count Ward TypeAssessment 8PICU 1 or 2Organic 6Stepped Care 5LD 1Complex Care 2Frail Group 2
Male Assessment
Female Assessment
PICU
LD
Male HDU
Female HDU
Complex Care
Moving On
Organic
A group of senior clinicians suggested that the following suite of wards, with the appropriate enablers in place, could be a starting point for a discussion about the future of NTW inpatient services
Functional Frail
Key

Male Assessment
Female Assessment
PICU
LD
Male HDU
Female HDU
Complex Care
Moving On
Organic
Senior NTW clinical staff agree the co-location of certain “ward types” makes clinical sense
Functional Frail
Key
Functional Frail / Organic
Functional / Complex Services

St Nicholas
St Georges
Monkwearmouth
Hopewood Park
Option W(26 Wards)
Male Assessment
Female Assessment
PICU
LD
Male HDU
Female HDU
Complex Care
Moving On
Organic
Functional Frail
Rose Lodge

St Nicholas
St Georges
Monkwearmouth
Hopewood Park
Option X(26 Wards)
Male Assessment
Female Assessment
PICU
LD
Male HDU
Female HDU
Complex Care
Moving On
Organic
Functional Frail
Rose Lodge

St Nicholas
St Georges
Monkwearmouth
Hopewood Park
Option Y(26 Wards)
Male Assessment
Female Assessment
PICU
LD
Male HDU
Female HDU
Complex Care
Moving On
Organic
Functional Frail
Rose Lodge

St Georges
Monkwearmouth
Hopewood Park
Option Z(26 Wards)
Male Assessment
Female Assessment
PICU
LD
Male HDU
Female HDU
Complex Care
Moving On
Organic
Functional Frail
Rose Lodge

The travel issue…• Across NTW it is not unusual for people to travel to the
right inpatient services.• Every patient is asked about travel for them and their
carers/family on admission• Wards have a number of resources available to help
families and patients, including ward cars, access to information on grants for families etc.
• We are working on ways to ensure local staff can keep in touch without too much travel

The staff perspective
• NTW does not anticipate making any compulsory redundancies as a result of this change
• There will be separate staff consultations in due course
• Affected staff will have access to TED – the Transitional Employment and Development Approach

Proposal for public involvement and consultation 2014Phase 1 – FDP delivery schemes for 2014/15•Newberry closure•Hebron closure•Newcastle dementia (castleside)•Greentrees - Interim•Rehabilitation South of Tyne (Brooke House and Elm House)•Rehabilitation North of Tyne (The Grange and Church View) Potentially interim

Proposal for public involvement and consultation 2014
Phase – Inpatient Beds Consultation •Options W, X, Y, Z•6 local authority areas (NB South Tyneside TBC)•i.e. all adult and older peoples assessment and treatment beds, dementia and LD•Exclude rehabilitation beds

Proposal for public involvement and consultation 2014Timing
Preparation: December 2013
Phase 1: January – March 2014
Phase 2: Mid May – August 2014
Implement phase 1 from April 2014
Implement phase 2 from April 2015

Questions?





























