Embed Size (px)
Citation preview

Animal Models of InflammatoryBowel Disease
Lessons from Enteric Infections
LARS ECKMANN
University of California, San Diego, Department of Medicine, La Jolla,California 92093, USA
ABSTRACT: Mouse models of intestinal inflammation have played a keyrole in understanding the mechanisms that govern the inflammatoryresponse in the intestine, and in designing new therapeutic strategiesin the treatment of patients with inflammatory bowel disease (IBD).Most of these models use chemical challenges, whereas relatively few ro-bust models of intestinal inflammation caused by microbial infection areknown. Two common models of infectious murine colitis and typhlitis areinfection with the murine epithelial-adherent pathogen, Citrobacter ro-dentium, and infection of streptomycin-pretreated mice with Salmonellatyphimurium. Studies in these models have helped to define the interac-tions between bacterial pathogens and host immune defenses, thus broad-ening the understanding of host–microbial interactions in the intestinaltract. Furthermore, such models help to determine the physiologic con-sequences of neutralizing specific mediators and signaling pathways im-plicated in inflammation on antimicrobial host defense.
KEYWORDS: mucosal immunology; inflammation; microbial pathogene-sis; intestinal microbiota; animal models
INTRODUCTION
Inflammatory bowel disease (IBD) is characterized by chronic relapsing in-flammation of the intestine leading to diarrhea, abdominal pain, and weightloss. Patients with long-standing disease have an increased risk of develop-ing colorectal cancer. Ulcerative colitis (UC) and Crohn’s disease (CD) arethe two major manifestations of IBD, yet it has become increasingly clearover recent years that these are not homogeneous disease conditions. Rather,
Address for correspondence: Lars Eckmann, University of California, San Diego, Department ofMedicine 0665, 9500 Gilman Drive, La Jolla, California 92093-0665. Voice: 858-534-0683; fax: 858-822-6454.
e-mail: [email protected]
Ann. N.Y. Acad. Sci. 1072: 28–38 (2006). C© 2006 New York Academy of Sciences.doi: 10.1196/annals.1326.008
28

ECKMANN: ANIMAL MODELS OF IBD 29
genetic linkage studies and immunological phenotyping indicate that multiplesubgroups of IBD exist, which are likely to have different etiologies and exhibitdifferential responses to therapy.1,2
The notion that intestinal inflammation represents a common phenotypicpathway of several diseases with different etiologies arose initially from stud-ies in murine models of immune dysregulation, in which disruption of each ofseveral genes encoding proteins with distinct immunological functions causedintestinal inflammation.3–5 Subsequent studies have considerably expanded thelist of genes whose loss in mice is associated with the development of sponta-neous colitis or enteritis or increased susceptibility to experimental challengescausing these conditions.6 Furthermore, investigation of the mechanisms thatgovern immune responses to varying microbes and defined antigens in murinemodels have led to important insights into basic features of immune regula-tion. Most notably, mouse models were critical in developing the “Th1/Th2”paradigm that CD4 T cells can differentiate in a polarized manner into cellsthat express distinct cytokine profiles and stimulate specific immune effectormechanisms.7 These immunological concepts provided the intellectual frame-work to explore the mechanisms of immune dysregulation in IBD and gaverise to new treatment hypotheses for the disease. To give a recent example,based on the importance of IL-12 and/or IL-23 in mouse models of immune-driven intestinal inflammation,8 pilot studies in humans with IBD revealedthat blockade of IL-12p40 may be efficacious in treating CD.9 Together, theseconsiderations illustrate the critical importance of mouse models for under-standing the pathogenesis of human IBD, and for developing new therapeuticstrategies in preclinical trials.
Although intestinal inflammation is the central disease-causing feature ofIBD, and hence the process targeted by therapeutic interventions, this phys-iological host response normally serves a beneficial purpose in the defenseagainst enteric microbes. Absence of immune and inflammatory responsesrenders the host unable to defend itself against infection with food- and water-borne microbial pathogens. In contrast, these responses are not needed for nor-mal health and fertility in animals not exposed to microbial pathogens. Thus,investigation of the physiological functions of intestinal immunity and inflam-mation is important for understanding host defense against enteric pathogensand for designing effective vaccination strategies. Insights in this area are alsoimportant for developing novel treatment approaches in IBD, as they mighthelp to minimize the risk that a therapeutic intervention compromises criticalhost defenses against commonly encountered enteric pathogens. Furthermore,commensal enteric bacteria are involved in the development of intestinal in-flammation in many animal models, and are likely to contribute to the develop-ment of IBD in humans.10 Insights into the host responses to enteric bacteria,both pathogenic and commensal, are therefore likely to enhance the mecha-nistic understanding of IBD pathogenesis, which in turn is key for developingeffective preventive and therapeutic measures.

30 ANNALS NEW YORK ACADEMY OF SCIENCES
MOUSE MODELS OF INFECTIOUS COLITIS
For several biological and practical reasons mice are the most commonlyused animal models for research in immunology and infectious diseases. Miceand humans are placental mammals with closely related genomes, since 99%of mouse genes have a homolog in the human genome and 80% of mousegenes have an ortholog in conserved syntenic intervals in the human genome(1:1 orthologs).11–13 Fewer than 1% of mouse genes (∼100 genes) have noapparent human homolog, although they could have functionally active, yetextremely diverged and thus unrecognizable, human counterparts. Further-more, many immunologic processes are similar in humans and mice, althoughsome differences exist in selected areas, such as the repertoire of antimicrobialpeptides of the �-defensin family.14 Mice can be engineered genetically to har-bor defined knockout or knockin mutations, and a plethora of research reagentsis available. Finally, mice are relatively small and have a short generation time,facilitating effective breeding and experimental schemes.
Murine infection models are widely employed for a range of infectiousagents, particularly those causing systemic infections. Somewhat surprisingly,very few good mouse models are available for investigating host defensesand inflammatory responses in the intestinal tract. Although intestinal infec-tion through oral gavage is effective for infecting the host with many entericpathogens, this route often does not lead to significant microbial colonizationor inflammation in the intestine. For example, oral infection of normal adultmice with the invasive gram-negative bacteria, Salmonella, leads to systemicinfection of spleen and liver, but causes only modest infection of the intestinaltract and very little intestinal inflammation.15 However, two intestinal infec-tion models, employing Citrobacter rodentium in normal mice and Salmonellatyphimurium in antibiotic-pretreated mice, have gained prominence over thelast few years, because infections are robust and cause significant intestinalinflammatory disease.
Citrobacter rodentium–Induced Colitis
C. rodentium (initially termed Citrobacter freundii biotype 4280) is a gram-negative murine pathogen that was first identified in veterinary medicine as themicrobial agent responsible for causing transmissible murine colonic hyperpla-sia in mouse breeding colonies.16,17 Subsequent studies revealed that the bacte-ria attach intimately to the colonic and cecal epithelium and form characteristicsubcellular lesions termed attaching and effacing (A/E) lesions.18 Similar le-sions are formed by two important human enteric pathogens, enteropathogenicEscherichia coli (EPEC) and enterohemorrhagic E. coli (EHEC).19,20 EPECcauses watery diarrhea worldwide, particularly in young children in developingcountries, while EHEC infection can lead to hemorrhagic colitis upon

ECKMANN: ANIMAL MODELS OF IBD 31
consumption of undercooked meat in developed countries.19,20 A/E lesions arecharacterized by localized destruction (effacement) of brush border microvilli,intimate attachment of the bacterium to the apical host cell membrane, andformation of an underlying pedestal-like structure in the host cell. The A/Elesion-forming pathogens generally do not invade deeper layers of the mu-cosa or spread systemically, making them predominantly mucosal pathogens.EHEC, but not EPEC or C. rodentium, elaborates specific enterotoxins, Shiga-like toxins, important in pathogenesis.20 C. rodentium shares other importantfunctional and structural similarities with clinical EPEC isolates. The bacterialgene coding for the outer membrane protein responsible for intimate attach-ment, intimin, is functionally homologous in C. rodentium and clinical EPECstrains.21 Furthermore, the murine and human infections with these pathogensare characterized by similar antibody responses to the bacteria. Taken together,these results suggest that C. rodentium is functionally similar to EPEC, thusmaking murine C. rodentium infection a model for human infections withEPEC.
Oral C. rodentium infection of normal adult mice causes transient coloniza-tion of cecum and colon, which peaks after 1 week, and is cleared over theensuing 2–3 weeks (FIG. 1). Bacterial colonization is limited to the intestinalmucosa, with only a few bacteria reaching systemic sites or the bloodstream.22
After bacterial eradication, mice are resistant to a secondary bacterial chal-lenge.23 Infection is normally accompanied by only modest morbidity (weightloss, diarrhea) and minimal mortality in adult mice, although significantmorbidity, such as retarded growth, and high mortality can occur in suck-
FIGURE 1. Time course of C. rodentium infection in normal mice. Adult C57BL/6mice were infected orally with 5 × 108 C. rodentium. At the indicated times after infec-tion, fecal pellets were collected, weighed, and homogenized. Homogenates were plated inserial dilutions on selective agar plates (MacConkey) and incubated overnight, after whichcolonies were counted. The dotted line indicates the sensitivity of the assay.

32 ANNALS NEW YORK ACADEMY OF SCIENCES
FIGURE 2. C. rodentium-induced colitis in normal mice. Paraffin sections of the colonof adult C57BL/6 mice, either uninfected (A) or 2 weeks after oral C. rodentium infection(B), were prepared and stained with hematoxylin/eosin. Infected mice show marked crypthyperplasia and mixed inflammatory cell infiltration of mucosa and submucosa.
ling mice.24 Infection leads to crypt hyperplasia, loss of goblet cells, andmucosal infiltration with lymphocytes, macrophages, neutrophils, and mastcells in colon and cecum16,17,23 (FIG. 2). The lymphocytic host response to C.rodentium is characterized by mucosal infiltration with CD3+ T cells, par-ticularly the CD4+ subset.25 In addition, the cytokines interleukin-12 (IL-12)and gamma-interferon (IFN-� ) are upregulated in the colon of infected mice,indicating a bias toward a T helper cell-type 1 immune response.26 T cells areimportant for clearance of C. rodentium, since mice with deficient �� T cellsor CD4 T cells cannot control infection and exhibit high morbidity and mor-tality.22,27 Moreover, mice develop IgG and IgA antibody responses to severalbacterial proteins involved in virulence, including intimin, EspA, EspB, andTir,28 and B cells are absolutely required for bacterial clearance.23,27 Despite

ECKMANN: ANIMAL MODELS OF IBD 33
the mucosal localization of the bacteria, secretory IgA or IgM antibodies,which are the dominant isotypes in mucosal secretions, play no role in hostdefense against C. rodentium, whereas IgG antibodies confer modest passiveimmune protection against oral challenge.23 These data suggest that IgG acts asan immune effector against the bacteria, although it is not clear how circulatingIgG can fulfill this function against luminal bacteria. B cells may also act asimmune sensor cells during infection, perhaps in antigen presentation, as sug-gested by the marked delay in normal mucosal responses in B cell–deficientmice compared to normal mice after infection.23
Besides T and B lymphocytes, cells and mediators of innate immunity playa role in host defense against C. rodentium. The acute inflammatory cytokine,tumor necrosis factor (TNF)-�, is induced upon infection, and is required foreffective clearance.29 We found recently that IL-6, a multifunctional cytokineinvolved in B cell functions and the acute-phase response, is upregulated inthe colon of infected mice. IL-6 deficiency leads to markedly delayed bacterialeradication, and greater infection-associated mucosal inflammation, suggest-ing that IL-6 exerts mucosa-protective functions in this model. This is in con-trast to the findings in T cell–dependent models of experimental colitis, whereIL-6 ablation was shown to attenuate inflammation.30,31 Furthermore, signal-ing through the lymphotoxin � receptor is required for effective host defenseagainst C. rodentium.32 In its absence, mice fail to eradicate infection normallyand exhibit more severe colitis, findings which caution that treatment of IBDwith agents directed against the lymphotoxin � receptor signaling pathwayis likely to render patients more susceptible to infection with certain entericpathogens.32 Among innate immune cells, a role for mast cells has been demon-strated in host defense against C. rodentium. Thus, mast cell–deficient miceshow more severe colonic inflammation and increased bacterial disseminationinto systemic sites, leading to higher mortality after C. rodentium infection thanthat in wild-type animals.33 Neutrophil numbers also increase in the colon afterinfection, but their involvement in host defense is not clear at present.
Salmonella-induced Colitis in Streptomycin-Treated Mice
Salmonella are gram-negative food-borne enteric bacterial pathogens thatcan cause diarrheal disease or severe systemic infection in humans. Manydifferent species exist, which fall into two major groups: Salmonella ty-phi, the cause of systemic typhoid fever, and nontyphoid Salmonella (e.g.,S. typhimurium, S. dublin) that cause mostly intestinal disease, although thelatter can also cause systemic disease.34 Human intestinal disease induced bynontyphoid Salmonella is characterized by acute neutrophilic mucosal inflam-mation. In contrast, oral infection of mice with these bacteria causes no majorintestinal disease, but rather systemic infection resembling typhoid fever inhumans. Only in the end stages of disseminated Salmonella infection in mice

34 ANNALS NEW YORK ACADEMY OF SCIENCES
can significant mucosal inflammation and destruction be observed in smallintestine and colon. This lack of mucosal disease upon Salmonella infectioncan be partly overcome by treating mice with an oral antibiotic, such as strepto-mycin or kanamycin, before oral infection with Salmonella.35,36 The antibioticsdiminish the normal intestinal microbiota, allowing the inoculated Salmonellato colonize the lumen of cecum and colon more effectively than without an-tibiotic conditioning. Consequently, Salmonella grow to high density in theintestine within a day, which is accompanied by marked mucosal inflamma-tion over the same time period.36 Thus, conditioning by oral antibiotics breaksthe colonization resistance normally conferred by the microbiota35 and allowsorally inoculated Salmonella to establish intestinal infection rapidly and causeinfection-associated colitis and typhlitis in normal mice. Similar results havebeen obtained after infection of germ-free mice with S. typhimurium, underlin-ing the importance of the normal microbiota in limiting Salmonella-inducedintestinal inflammation in mice.37
Intestinal inflammation in the model is characterized by rapid crypt loss,epithelial erosions and goblet cell loss, mucosal and submucosal infiltrationwith acute inflammatory cells, particularly neutrophils, and marked edema,in the cecum and, to a lesser degree, in the colon.36,38(FIG. 3). The model isespecially useful for examining the early (4–72 h) intestinal events that occurafter oral Salmonella infection, while the overwhelming intestinal infectionprobably causes severe, presumably lethal systemic disease at later stages (5–7 days), although this has not reported in detail. The Salmonella infectiouscolitis/typhlitis model has been used to examine the role of specific bacterialvirulence factors in causing intestinal disease, and the importance of hostfactors in intestinal defense against Salmonella. For example, studies in thismodel have shown that flagella, appendages of the outer bacterial membranerequired for motility, are required for effective colonization and induction ofintestinal inflammation.39 This effect appears to be mostly related to bacterialchemotaxis, since nonflagellated bacteria failed to get close to the epithelium.39
Furthermore, the adaptor molecule MyD88, which is required for signalingthrough most toll-like receptors, was shown to be important for inducing colitisafter infection with bacterial mutants lacking the Salmonella pathogenicityisland (SPI)-2 secretion system, but not those lacking the SPI-1 system.40
Virulence factors of the SPI-2 locus are important for bacterial survival inmacrophages, while those of the SPI-1 locus are primarily involved in invasionof the intestinal epithelium.38 Thus, SPI-2-dependent intracellular proliferationof the bacteria triggers MyD88-dependent innate immune responses in theintestinal tract.40
CONCLUSIONS
Mouse models of infectious colitis can help to determine the interactionsbetween bacterial pathogens and host immune defenses, thus broadening the

ECKMANN: ANIMAL MODELS OF IBD 35
FIGURE 3. Salmonella-induced intestinal inflammation. Adult C57BL/6 mice weregiven 20 mg streptomycin orally, and infected 24 h later with S. typhimurium 14028 by oralgavage. Paraffin sections of the cecum 48 h after infection (B), or from uninfected controlmice (A), were prepared and stained with hematoxylin/eosin. Infected mice exhibit extensivecrypt hyperplasia, epithelial erosions at the surface, and edema and mixed inflammatorycell infiltration of mucosa and submucosa.
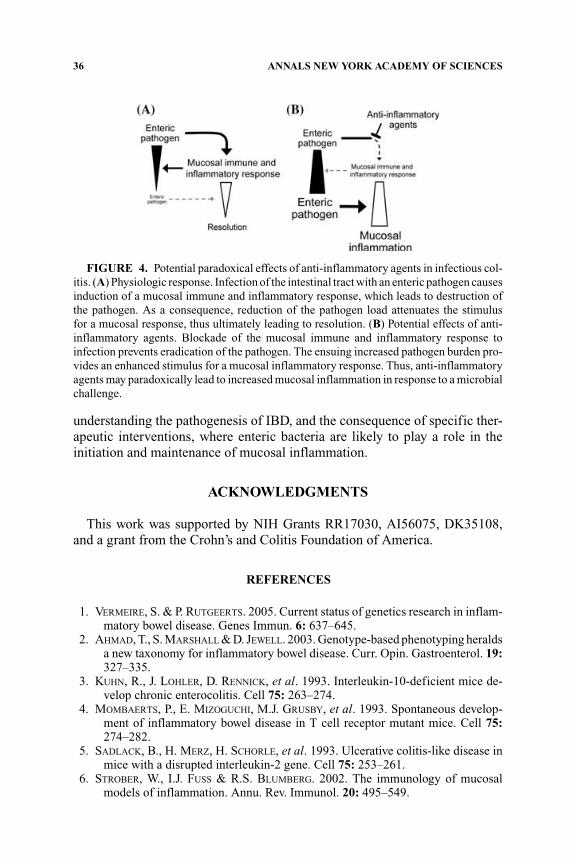
understanding of host–microbial interactions in the intestinal tract. Further-more, such models help to define the physiologic consequences of neutraliz-ing specific mediators and signaling pathways on antimicrobial host defense.These insights are important for assessing potential untoward side effects thatnovel pharmacological interventions might have in patients with IBD. In thisregard, it is important to realize that microbial infection as the proximal causeof mucosal inflammation is a dynamic stimulus that changes in response to hostdefenses (FIG. 4). Interventions designed to inhibit a particular proinflamma-tory pathway in the host may, paradoxically, exacerbate mucosal inflammation,because the pathway might be required for effective host defense against in-fection, so that its loss results in a greater microbial load and thus a strongerstimulus for mucosal inflammation. Such considerations may also apply to
36 ANNALS NEW YORK ACADEMY OF SCIENCES
FIGURE 4. Potential paradoxical effects of anti-inflammatory agents in infectious col-itis. (A) Physiologic response. Infection of the intestinal tract with an enteric pathogen causesinduction of a mucosal immune and inflammatory response, which leads to destruction ofthe pathogen. As a consequence, reduction of the pathogen load attenuates the stimulusfor a mucosal response, thus ultimately leading to resolution. (B) Potential effects of anti-inflammatory agents. Blockade of the mucosal immune and inflammatory response toinfection prevents eradication of the pathogen. The ensuing increased pathogen burden pro-vides an enhanced stimulus for a mucosal inflammatory response. Thus, anti-inflammatoryagents may paradoxically lead to increased mucosal inflammation in response to a microbialchallenge.
understanding the pathogenesis of IBD, and the consequence of specific ther-apeutic interventions, where enteric bacteria are likely to play a role in theinitiation and maintenance of mucosal inflammation.
ACKNOWLEDGMENTS
This work was supported by NIH Grants RR17030, AI56075, DK35108,and a grant from the Crohn’s and Colitis Foundation of America.
REFERENCES
1. VERMEIRE, S. & P. RUTGEERTS. 2005. Current status of genetics research in inflam-matory bowel disease. Genes Immun. 6: 637–645.
2. AHMAD, T., S. MARSHALL & D. JEWELL. 2003. Genotype-based phenotyping heraldsa new taxonomy for inflammatory bowel disease. Curr. Opin. Gastroenterol. 19:327–335.
3. KUHN, R., J. LOHLER, D. RENNICK, et al. 1993. Interleukin-10-deficient mice de-velop chronic enterocolitis. Cell 75: 263–274.
4. MOMBAERTS, P., E. MIZOGUCHI, M.J. GRUSBY, et al. 1993. Spontaneous develop-ment of inflammatory bowel disease in T cell receptor mutant mice. Cell 75:274–282.
5. SADLACK, B., H. MERZ, H. SCHORLE, et al. 1993. Ulcerative colitis-like disease inmice with a disrupted interleukin-2 gene. Cell 75: 253–261.
6. STROBER, W., I.J. FUSS & R.S. BLUMBERG. 2002. The immunology of mucosalmodels of inflammation. Annu. Rev. Immunol. 20: 495–549.

ECKMANN: ANIMAL MODELS OF IBD 37
7. ELSON, C.O., Y. CONG, V.J. MCCRACKEN, et al. 2005. Experimental models ofinflammatory bowel disease reveal innate, adaptive, and regulatory mechanismsof host dialogue with the microbiota. Immunol. Rev. 206: 260–276.
8. NEURATH, M.F., I. FUSS, B.L. KELSALL, et al. 1995. Antibodies to interleukin 12abrogate established experimental colitis in mice. J. Exp. Med. 182: 1281–1290.
9. MANNON, P. J., I.J. FUSS, L. MAYER, et al. 2004. Anti-interleukin-12 antibody foractive Crohn’s disease. N. Engl. J. Med. 351: 2069–2079.
10. SARTOR, R.B. 2004. Therapeutic manipulation of the enteric microflora in inflam-matory bowel diseases: antibiotics, probiotics, and prebiotics. Gastroenterology126: 1620–1633.
11. LANDER, E.S., L.M. LINTON, B. BIRREN, et al. 2001. Initial sequencing and analysisof the human genome. Nature 409: 860–921.
12. VENTER, J.C., M.D. ADAMS, E.W. MYERS, et al. 2001. The sequence of the humangenome. Science 291: 1304–1351.
13. WATERSTON, R.H., K. LINDBLAD-TOH, E. BIRNEY, et al. 2002. Initial sequencingand comparative analysis of the mouse genome. Nature 420: 520–562.
14. PATIL, A., A.L. HUGHES & G. ZHANG. 2004. Rapid evolution and diversification ofmammalian alpha-defensins as revealed by comparative analysis of rodent andprimate genes. Physiol. Genomics 20: 1–11.
15. HEFFERNAN, E.J., J. FIERER, G. CHIKAMI, et al. 1987. Natural history of oralSalmonella dublin infection in BALB/c mice: effect of an 80-kilobase-pair plas-mid on virulence. J. Infect. Dis. 155: 1254–1259.
16. BARTHOLD, S.W., G.L. COLEMAN, P.N. BHATT, et al. 1976. The etiology of trans-missible murine colonic hyperplasia. Lab. Anim. Sci. 26: 889–894.
17. LUPERCHIO, S.A. & D.B. SCHAUER. 2001. Molecular pathogenesis of Citrobacterrodentium and transmissible murine colonic hyperplasia. Microbes Infect. 3:333–340.
18. SCHAUER, D.B. & S. FALKOW. 1993. Attaching and effacing locus of a Citrobacterfreundii biotype that causes transmissible murine colonic hyperplasia. Infect.Immun. 61: 2486–2492.
19. KAPER, J.B., J.P. NATARO & H.L. MOBLEY. 2004. Pathogenic Escherichia coli. Nat.Rev. Microbiol. 2: 123–140.
20. WELINDER-OLSSON, C. & B. KAIJSER. 2005. Enterohemorrhagic Escherichia coli(EHEC). Scand. J. Infect. Dis. 37: 405–416.
21. FRANKEL, G., A.D. PHILLIPS, M. NOVAKOVA, et al. 1996. Intimin from en-teropathogenic Escherichia coli restores murine virulence to a Citrobacter ro-dentium eaeA mutant: induction of an immunoglobulin A response to intiminand EspB. Infect. Immun. 64: 5315–5325.
22. BRY, L. & M.B. BRENNER. 2004. Critical role of T cell-dependent serum antibody,but not the gut-associated lymphoid tissue, for surviving acute mucosal infectionwith Citrobacter rodentium, an attaching and effacing pathogen. J. Immunol. 172:433–441.
23. MAASER, C., M.P. HOUSLEY, M. IIMURA, et al. 2004. Clearance of Citrobacterrodentium requires B cells but not secretory immunoglobulin A (IgA) or IgMantibodies. Infect. Immun. 72: 3315–3324.
24. BARTHOLD, S.W., G.L. COLEMAN, R.O. JACOBY, et al. 1978. Transmissible murinecolonic hyperplasia. Vet. Pathol. 15: 223–236.
25. HIGGINS, L.M., G. FRANKEL, G. DOUCE, et al. 1999. Citrobacter rodentium infectionin mice elicits a mucosal Th1 cytokine response and lesions similar to those inmurine inflammatory bowel disease. Infect. Immun. 67: 3031–3039.

38 ANNALS NEW YORK ACADEMY OF SCIENCES
26. SIMMONS, C.P., N.S. GONCALVES, M. GHAEM-MAGHAMI, et al. 2002. Impaired re-sistance and enhanced pathology during infection with a noninvasive, attaching-effacing enteric bacterial pathogen, Citrobacter rodentium, in mice lacking IL-12or IFN-gamma. J. Immunol. 168: 1804–1812.
27. SIMMONS, C.P., S. CLARE, M. GHAEM–MAGHAMI, et al. 2003. Central role for Blymphocytes and CD4+ T cells in immunity to infection by the attaching andeffacing pathogen Citrobacter rodentium. Infect. Immun. 71: 5077–5086.
28. GHAEM-MAGHAMI, M., C.P. SIMMONS, S. DANIELL, et al. 2001. Intimin-specific im-mune responses prevent bacterial colonization by the attaching-effacing pathogenCitrobacter rodentium. Infect. Immun. 69: 5597–5605.
29. GONCALVES, N.S., M. GHAEM-MAGHAMI, G. MONTELEONE, et al. 2001. Critical rolefor tumor necrosis factor alpha in controlling the number of luminal pathogenicbacteria and immunopathology in infectious colitis. Infect. Immun. 69: 6651–6659.
30. YAMAMOTO, M., K. YOSHIZAKI, T. KISHIMOTO, et al. 2000. IL-6 is required for thedevelopment of Th1 cell-mediated murine colitis. J. Immunol. 164: 4878–4882.
31. KITAMURA, K., Y. NAKAMOTO, S. KANEKO, et al. 2004. Pivotal roles of interleukin-6 in transmural inflammation in murine T cell transfer colitis. J. Leukoc. Biol.76: 1111–1117.
32. SPAHN, T.W., C. MAASER, L. ECKMANN, et al. 2004. The lymphotoxin-beta re-ceptor is critical for control of murine Citrobacter rodentium-induced colitis.Gastroenterology 127: 1463–1473.
33. WEI, O.L., A. HILLIARD, D. KALMAN, et al. 2005. Mast cells limit systemic bacterialdissemination but not colitis in response to Citrobacter rodentium. Infect. Immun.73: 1978–1985.
34. FIERER, J. & M. SWANCUTT. 2000. Non-typhoid Salmonella: a review. Curr. Clin.Top. Infect. Dis. 20: 134–157.
35. QUE, J.U. & D.J. HENTGES. 1985. Effect of streptomycin administration on col-onization resistance to Salmonella typhimurium in mice. Infect. Immun. 48:169–174.
36. BARTHEL, M., S. HAPFELMEIER, L. QUINTANILLA-MARTINEZ, et al. 2003. Pretreat-ment of mice with streptomycin provides a Salmonella enterica serovar Ty-phimurium colitis model that allows analysis of both pathogen and host. Infect.Immun. 71: 2839–2858.
37. STECHER, B., A.J. MACPHERSON, S. HAPFELMEIER, et al. 2005. Comparison ofSalmonella enterica serovar Typhimurium colitis in germfree mice and micepretreated with streptomycin. Infect. Immun. 73: 3228–3241.
38. COOMBES, B.K., B.A. COBURN, A.A. POTTER, et al. 2005. Analysis of the contribu-tion of Salmonella pathogenicity islands 1 and 2 to enteric disease progressionusing a novel bovine ileal loop model and a murine model of infectious entero-colitis. Infect. Immun. 73: 7161–7169.
39. STECHER, B., S. HAPFELMEIER, C. MULLER, et al. 2004. Flagella and chemotaxisare required for efficient induction of Salmonella enterica serovar Typhimuriumcolitis in streptomycin-pretreated mice. Infect. Immun. 72: 4138–4150.
40. HAPFELMEIER, S., B. STECHER, M. BARTHEL, et al. 2005. The Salmonellapathogenicity island (SPI)-2 and SPI-1 type III secretion systems allowSalmonella serovar typhimurium to trigger colitis via MyD88-dependent andMyD88-independent mechanisms. J. Immunol. 174: 1675–1685.













