Embed Size (px)
Citation preview

Aneurysmal Aorto-RightVentricular TunnelSushil Kumar Singh, MCh,Sudhanshu Kumar Dwivedi, DM,Ambrish Kumar, MCh, Sudarshan Kumar Vijay, MD,Nitin Rajput, MCh, Vijyant Devenraj, MS, andJeevan Lal Sahni, MCh
Departments of Cardiothoracic and Vascular Surgery andCardiology, CSM Medical University, Lucknow, India
A successful closure of an aneurysmal aorto-right ven-tricular tunnel (ARVT) in a 16-year-old male patient isreported here. An attempt at device closure had failed inthis patient. Diagnosis was confirmed by Doppler echo-cardiography, 3-dimensional computed tomography, andcardiac catheterization. Surgical closure with a Dacronpatch (W.L. Gore & Associates, Flagstaff, AZ) at the aorticend and direct closure at the ventricular end was donesuccessfully with the patient under mild hypothermia.The postoperative echocardiogram showed a competentaortic valve with a closed ARVT.
(Ann Thorac Surg 2012;93:e21–2)© 2012 by The Society of Thoracic Surgeons
Aorto-right ventricular tunnel (ARVT) is a rare condi-tion; only 15 cases have been reported in the
English-language literature [1–6]. To our knowledge,aneurysmally dilatated (approximately 2 cm in diameter)ARVT has not been reported. This is a disease of earlychildhood with a high reported surgical mortality [1].New advancements in technology, leading to accuratepreoperative information about the malformation is thecause of better outcomes in recent times [1, 2]. We reporthere a case of successful surgical closure of aneurysmalARVT after a failed attempt at device closure.
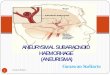
A 16-year-old male patient was admitted to our hospitalwith complaints of dyspnea and fatigue for the preceding 8years without any history of chest pain, cyanosis, or trauma.On examination, he had normal vital signs with skeletalfeatures suggestive of Marfan’s syndrome. Cardiac exami-nation revealed a grade 4/6 continuous murmur that wasmaximally heard over the right parasternal area in thefourth intercostal space. The electrocardiogram was normaland a chest roentgenogram showed a normal cardiotho-racic ratio with bilateral hilar prominence and increasedlung vascularity. Echocardiography revealed a large tunnel(2 cm in diameter) arising above the right aortic sinus and aturbulent jet with a velocity of 3.5 m/s coming from the freewall of the right ventricle. Cardiac computed tomographyangiography showed a tortuous dilatated tunnel of 1.85 cmdiameter originating from the right aortic root and termi-nating in the anterosuperior portion of the right ventricle.The right coronary artery was not visualized (Fig 1). Coro-nary angiography showed a normal left coronary artery; the
Accepted for publication Aug 24, 2011.
Address correspondence to Dr Singh, Cardiothoracic and Vascular Sur-
gery Department, CSM Medical University, Lucknow, India, Pin-226003;e-mail: [email protected].© 2012 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
right coronary artery was not visualized. The right sideof the heart was supplied entirely from branches arisingfrom the left coronary circulation. Aortic root injection con-firmed the tunnel and showed a left-to-right shunt withpulmonic to systemic blood flow of � 2:1 and pulmonaryartery systolic pressure of 50 mm Hg. Device closure wasunsuccessful. The patient was referred for surgicalintervention.
At operation through a median sternotomy, an aneu-rysmally dilatated, tortuous tunnel was visualized origi-nating above the aortic root, crossing the right atrioven-tricular groove, and terminating into the lateral wall ofthe right ventricle (Fig 2A) with continuous thrill over it.A standard mild hypothermic cardiopulmonary bypasswas instituted with antegrade coronary osteal bloodcardioplegia. Aortotomy showed a small right coronaryostium. The aortic end of the ARVT was approximately 2cm in diameter, well above the hinge line of the rightaortic leaflet and about 0.5 cm above the orifice of theright coronary artery (Fig 2B). A 2-mm probe was passedthrough the tunnel and its communication with the rightventricular cavity was confirmed.
Incision through the widest part of the tunnel showeda wide opening in the aortic root above the sinotubularjunction and a small right ventricular cavity opening(approximately 5 mm in diameter). A Dacron patch wasused to close the aortic end of the tunnel using continu-ous 4-0 Prolene suture (Ethicon, Somerville, NJ) throughaortotomy, taking care of the aortic valve leaflet and rightcoronary ostium. The right ventricular opening of thetunnel was oversewn with 4-0 Prolene suture (Ethicon)using pericardium.
The patient was weaned from bypass uneventfully.Thrill disappeared on palpation. His course in the inten-sive care unit was uneventful and he was dischargedfrom the hospital on the sixth postoperative day. Echocar-diography before discharge and 6 months later at follow-uprevealed a competent aortic valve and no residual commu-
Fig 1. Three-dimensional reconstructed image from multislice com-puted angiography showing large tortuous tunnel arising from rightaortic sinus (X) with single coronary artery taking origin from leftaortic sinus (Y).
nication between the aorta and right ventricle.
0003-4975/$36.00doi:10.1016/j.athoracsur.2011.08.061

ttfsaltttnf
itrao
s
opa
ssaRrtco
dt
e22 CASE REPORT SINGH ET AL Ann Thorac SurgAORTO-VENTRICULAR TUNNEL 2012;93:e21–2
Comment
Aortoventricular tunnel is a rare congenital extracardiacchannel that connects the ascending aorta above thesinotubular junction to the cavity of the left or (lesscommonly) right ventricle. Bharati and associates [3]described a postmortem specimen in which a tunnelarising above the right sinus of Valsalva connected withthe right ventricle. Lin and associates [1] reviewed 10cases of ARVT published in the English-language litera-ture (excluding their own); 4 more cases have recentlybeen reported [2–6], including 1 with transcatheter clo-sure of ARVT [2]. Associated defects, usually involvingthe proximal coronary arteries or the aortic or pulmonaryvalves, are present in nearly half of cases [2].
The pathogenesis of ARVT is unknown. The explana-tion given for aorto–left ventricular tunnel by Bove andSchwartz [7] might be pertinent to this case, ie, (1) theunnel represents an anomalous coronary artery; (2) theunnel represents a dissecting aneurysm related to Mar-an’s syndrome; (3) it is due to an abnormally formedupravalvular ridge. The cushion that forms the facingortic and pulmonary sinuses with their respective valvareaflet normally become separated by an extracardiacissue plane. The coronary arteries, initially encased byhis cuff of myocardium, grow through it to connect withhe aortic sinuses. Failure of this tissue plane to developormally might then result in a tunnel above 1 of the
acing aortic sinuses [8].Differential diagnosis with ruptured sinus of Valsalva
nto the right ventricle was ruled out in our case becausehe opening in our patient lies above the supravalvularidge and hence above the sinus of Valsalva. A coronaryrtery fistula was excluded because the coronary arteryrigin and distribution were normal.This vascular channel functions like a left-to-right
Fig 2. (A) Aneurysmal aorto-rightventricular tunnel (X). (B) Suctionthrough incision over tunnel (X),aortic end of tunnel (Y), and rightcoronary artery ostium (Z).
hunt at the ventricular level, and complications can
ccur in the form of volume overload of both ventricles,ulmonary vascular disease, spontaneous rupture, orneurysm formation [2].This is a disease of early childhood with high reported
urgical mortality. Lin and associates [1] reported only 5urvivors of 9 patients who underwent operation. Oper-tive closure is the mainstay of treatment for this anomaly.ecently, successful device closure of the tunnel has been
eported [2]. Device closure was attempted in our institu-ion also but failed. Detailed anatomy of the tunnel andoronary anatomy is important for successful surgicalutcome.This case of ARVT, in which the tract was aneurysmally
ilatated, was successfully repaired with a patchechnique.
References
1. Lin BS, Zhang XH, Jiang YZ, Zhang BM, Gao D, Song J.Diagnosis and surgical treatment of adult aortico-right ven-tricular tunnel. Ann Thorac Surg 2010;89:2024–6.
2. Poptani VA, Thakkar BM, Nehal H, Patel NH. Transcatheterclosure of a rare case of aorto-right ventricular tunnel withsingle coronary artery. J Invasive Cardiol 2010;22:611–4.
3. Bharati S, Lev M, Cassels DE. Aortico-right ventricular tun-nel. Chest 1973;63:198–202.
4. Pinaud F, Pezard P, Merheb M, Sibileau E, Baufreton C.Congenital aorto-right ventricular fistula in an adult. EurHeart J 2009;30:2116.
5. Bratsas A, Vlachopoulos C, Kotoulas G, Makris T, StefanadisC. Snakelike aortic right ventricular tunnel with anomalousorigin of left main coronary artery in an adult woman. J AmColl Cardiol 2010;56:11.
6. Li J, Wang H, Zheng M. Diagnosis of aortic-right ventriculartunnel by dual-source computed tomography. Eur J Cardio-thorac Surg 2011;39:609.
7. Bove KE, Schwartz DC: Aorto-left ventricular tunnel. Am JCardiol 1967;19:696–709.
8. McKay R, Anderson RH, Cook AC. The aorto-ventriculartunnels. Cardiol Young 2002;12:563–80.