-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
1/25
Anemia Management in Chronic Kidney Disease and End-
Stage Renal Disease: Clinical Case Studies CME/CE
This activity is intended for nephrologists, primary care
providers, nurses, and nurse practitionerswho manage patients with
anemia associated with chronic kidney disease (CKD).
Goal
The goal of this activity is to summarize and interpret recent
clinical data on the use of currenterythropoiesisstimulating agents
(!"#s) in patients with CKD and endstage renal disease(!"$D) who
have anemia, including the role of iron supplementation and
emerging treatmentoptions. Decisionmaking that is %ased on uptodate
clinical data and evidence on managementinterventions will %e
encouraged.
Learning Objectives
&pon completion of this activity, participants will %e a%le
to'
. $eview the rationale for the recommended hemoglo%in targets in
patients with CKD andstrategies to minimize hemoglo%in cycling
. Consider the %enefits and challenges of !"# therapy in
hospitalized patients with !"$D
*. Descri%e the efficacy, safety, %enefits, and limitations of
current and emerging !"#therapies for patients with !"$D, including
the role of iron therapy
+. dentify strategies for incorporating current !"# therapies in
the management of patientswith !"$D and anemia
Credits Available
Physicians ma-imum of .AMA PRA Category 1 Credit(s)
Nurses .ANCC Contact Hour(s)(. contact hours are in the area of
pharmacology)
#ll other healthcare professionals completing continuing
education credit for this activity will %eissued a certificate of
participation.
/hysicians should only claim credit commensurate with the e-tent
of their participation in theactivity.
Accreditation Statements
For Physicians
0edscape, 11C is accredited %y the #ccreditation Council for
Continuing 0edical !ducation(#CC0!) to provide continuing medical
education for physicians.
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
2/25
0edscape, 11C designates this educational activity for a ma-imum
of .AMA PRA Category 1Credit(s). /hysicians should only claim
credit commensurate with the e-tent of theirparticipation in the
activity.
0edscape, 11C staff have disclosed that they have no relevant
financial relationships.
Contact This /rovider
For Nurses
0edscape, 11C is accredited as a provider of continuing nursing
education %y the #merican2urses Credentialing Center3s Commission
on #ccreditation.
#warded . contact hour(s) of continuing nursing education for
$2s and #/2s4 . contacthours are in the area of pharmacology.
#ccreditation of this program does not imply endorsement %y
either 0edscape, 11C or #2CC.
Contact This /rovider
5or 6uestions regarding the content of this activity, contact
the accredited provider for this C0!7C!activity noted a%ove. 5or
technical assistance, contact C0!8medscape.net
Instructions for Particiation and Credit
There are no fees for participating in or receiving credit for
this online educational activity. 5orinformation on applica%ility
and acceptance of continuing education credit for this activity,
pleaseconsult your professional licensing %oard.
This activity is designed to %e completed within the time
designated on the title page4 physiciansshould claim only those
credits that reflect the time actually spent in the activity. To
successfullyearn credit, participants must complete the activity
online during the valid credit period that is notedon the title
page.
5ollow these steps to earn C0!7C! credit9'
. $ead the target audience, learning o%:ectives, and author
disclosures.
. "tudy the educational content online or printed out.
*. ;nline, choose the %est answer to each test 6uestion. To
receive a certificate, you mustreceive a passing score as
designated at the top of the test. 0edscape !ducationencourages you
to complete the #ctivity !valuation to provide feed%ack for
futureprogramming.
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
3/25
# computer with an nternet connection.
nternet !-plorer =.- or higher, 5irefo- .- or higher, "afari .-
or higher, or any other ?*C
standards compliant %rowser.
#do%e 5lash /layerand7or an @T01 capa%le %rowser may %e re6uired
for video or audio
play%ack.
;ccasionally other additional software may re6uired such as
/ower/ointor#do%e
#cro%at $eader.
Authors and &isclosures
#s an organization accredited %y the #CC0!, 0edscape, 11C,
re6uires everyone who is in a
position to control the content of an education activity to
disclose all relevant financial relationships
with any commercial interest. The #CC0! defines >relevant
financial relationships> as financial
relationships in any amount, occurring within the past months,
including financial relationships
of a spouse or life partner, that could create a conflict of
interest.
0edscape, 11C, encourages #uthors to identify investigational
products or offla%el uses of
products regulated %y the &" 5ood and Drug #dministration,
at first mention and where
appropriate in the content.
Author's(
&aniel )* Coyne+ ,&
/rofessor of 0edicine, $enal Diseases, ?ashington
&niversity4 "taff /hysician, AarnesBewish
@ospital, "t. 1ouis, 0issouri
Disclosure' Daniel ?. Coyne, 0D, has disclosed the following
relevant financial relationships'
"erved as an advisor or consultant for' #%%ott 1a%oratories4
/harmacosmos4 sanofiaventis4
?atson /harmaceuticals, nc.4 2!;""erved as a speaker or a mem%er
of a speakers %ureau for' #%%ott 1a%oratories4 /harmacosmos4
?atson /harmaceuticals, nc.
;wns stock, stock options, or %onds from' 0erck Co., nc.
Dr. Coyne does not intend to discuss off-labeluses of drugs,
mechanical devices, %iologics, or
diagnostics approved%y the 5D# for use in the &nited
"tates.
Dr. Coyne does intend to discuss investigational drugs,
mechanical devices, %iologics, or
diagnostics not approved%y the 5D# for use in the &nited
"tates.
)riter's(
$obert ,ar- &ana+ ,A
http://get.adobe.com/flashplayer/http://office.microsoft.com/en-us/powerpoint/http://get.adobe.com/reader/http://get.adobe.com/reader/http://get.adobe.com/reader/http://get.adobe.com/flashplayer/http://office.microsoft.com/en-us/powerpoint/http://get.adobe.com/reader/http://get.adobe.com/reader/
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
4/25
0anaging /rincipal, "cientific Communications "ervices, !-ton,
/ennsylvania
Disclosure' Disclosure' $o%ert 0ark Dana, 0#, has disclosed the
followingrelevant financial relationships'"erved as an advisor or
consultant for' /fizer nc.;wns stock, stock options, or %onds from'
/fizer nc.4 0erck Co., nc.
.ames A* Shiffer+ $P!
0edical writer, 0arlton, 2ew Bersey
Disclosure' Bames #. "hiffer, $/@, has disclosed no relevant
financial relationships.
/ditor's(
Anne G* Le+ Pharm&+ $Ph
"cientific Director, 0edscape, 11C
Disclosure' #nne . 1e, /harmD, $/h, has disclosed no relevant
financial relationships.
C,/ $evie"er
Nafee0 1a"ahir+ ,&
C0! Clinical Director, 0edscape, 11C
Disclosure' 2afeez Eawahir, 0D, has disclosed no relevant
financial relationships.
Nurse Planner
Laurie /* Scudder+ &NP+ NP
2urse /lanner, Continuing /rofessional !ducation Department,
0edscape, 11C4 Clinical #ssistant
/rofessor, "chool of 2ursing and #llied @ealth, eorge ?ashington
&niversity, ?ashington, DC
Disclosure' 1aurie !. "cudder, D2/, 2/, has disclosed no
relevant financial relationships.
From ,edscae /ducation Nehrology
Anemia Management in Chronic Kidney Disease and End-Stage Renal
Disease: Clinical Case Studies CME/CEDaniel ?. Coyne, 0D
C0!7C! $eleased' F7F7F4 Galid for credit through F7F7F
The following testandteach case is an educational activity
modeled on the interactive grand
rounds approach. The 6uestions within the activity are designed
to test your current knowledge.
#fter each 6uestion, you will %e a%le to see whether you
answered correctly and will then read
evidence%ased information that supports the most appropriate
answer choice. /lease note that
these 6uestions are designed to challenge you4 you will not %e
penalized for answering the
6uestions incorrectly. #t the end of the case, there will %e a
short posttest assessment %ased on
material covered in the activity.
http://www.medscape.org/nephrologyhttp://www.medscape.org/nephrology
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
5/25
Case Study 234 &iagnosis and 5reatment of Anemia in
Predialysis Chronic
6idney &isease 77 Patient !istory
@T is a =yearold woman with previously diagnosed longterm type
dia%etes and su%se6uently
diagnosed chronic kidney disease (CKD), hypertension, and
anemia. "he is in the office for a
periodic followup and has %een compliant with her medications
for hypertension, dia%etes, and
hypercholesterolemia. "he denies cardiovascular (CG) symptoms,
including angina or dyspnea
during e-ertion. @ome measurements indicate that her %lood
pressure is well controlled. "he has
%een postmenopausal for years and reports no orthostatic
hypotension, gastrointestinal ()%leeding, or melena. "he had a
normal colonoscopy + years ago. "he reports recurring fatigue
during the past * months that has made it increasingly difficult
to perform her work as a sales
clerk. @er hemoglo%in (@%) values have slowly declined from F.H
g7d1 a year ago to I. g7d1
despite treatment with an oral iron supplement for = months,
which was discontinued months
ago. ;ther la%oratory values are as follows' sodium, + mmol714
potassium, +.H mmol714 car%on
dio-ide (C;), + mmol714 %lood urea nitrogen (A&2), +H mg7d14
creatinine, *. mg7d14 estimated
glomerular filtration rate (e5$), m17min4 white %lood cell
(?AC), . million7J14 hematocrit,
I.4 and platelets, H,FFF7J1.
?hat key clinical chemistry value or assessment information does
the clinician need
%efore proceeding to therapy with an erythropoiesisstimulating
agent (!"#) in this
patientL
Creactive protein
!C for left ventricular hypertrophy (1G@)
rondeficiency studies (serum ferritin, transferrin saturation
MT"#TN)
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
6/25
#c
Prevalence and Conse%uences of Anemia in C6&
The kidneys produce appro-imately IF of all !/;, the hormone
that stimulates the %one marrow
to produce red %lood cells. Thus, patients with !"$D or CKD
stage O * usually develop anemia
due to impaired renal secretion of !/;. #nemia can occur
insidiously soon after onset of CKD,
even prior to the 5$ P =F m17min diagnostic threshold of stage *
(moderate) CKD. #nemia
%ecomes progressively worse as kidney function declines and
progresses to !"$D. # recent
largescale study of predialysis CKD patients (2 Q ) in the
&nited "tates found that +R.R had
@% levels S g7d1 (the upper limit of normal) and H.I had levels
S F g7d1. MN# multinational
survey of predialysis patients (2 Q +***) found that =H had a @%
concentration S .F g7d1. MN
/revalence of CKD and attendant or coincidental anemia increases
with age. 5or e-ample, the
2ational @ealth and 2utrition !-amination "tudy (2@#2!" ) study
found that more than F of
#mericans = years of age and older are anemic, representing
perhaps * million individuals, with
H. of the cases due to renal insufficiency and an additional +
due to CKD plus anemia of
chronic disease.M*Niven the aging &" population and rapid
increase in diagnoses of type
dia%etes, the overall prevalence of CKD is likewise
increasing.
Aesides su%normal production of !/;, a common cause of anemia in
cases of CKD or !"$D is
iron deficiency resulting from any of several causes, as
discussed later in this article. nade6uate
iron or decreased iron availa%ility has %een shown to %e a
significant predictor of !"# resistance
or nonresponsiveness.M+NThus, for purposes of this initial
assessment of our patient, @T, clinicians
should o%tain a complete %lood count with differential and
platelet count, @% concentration, mean
corpuscular volume, mean corpuscular @% concentration, and tests
for iron deficiency' serum
ferritin level and serum T"#T level. The serum ferritin assay
reflects the %ody3s iron stores, while
the T"#T assesses the availa%ility of iron for erythropoiesis.
These standard tests may %e
supplemented with an assay for reticulocyte hemoglo%in content
(C@r), an early, direct
determination of iron availa%le for @% synthesis.
n treating CKDassociated anemia in this patient, what symptoms
or clinical risks are
most likely to improveL
Save and Proceed
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
7/25
$egression of 1G@
$eduction in heart failure risk
$eduction in stroke risk
$eduction in fatigue
There are multiple, wellknown conse6uences of untreated anemia
in the !"$D setting. 0ost
nota%ly are CG complications resulting from the added %urden
that CKD and anemia place on the
heart. #nemia in !"$D patients has %een shown to %e an
independent risk factor in de novo
cardiac failure and mortality.MN!ven in patients with
mildtomoderate renal insufficiency, studies
have shown a * increase in 1G@ risk for each F.g7d1 decrease in
@%. M=N#nemic !"$D patients
also e-perience fatigue, e-ercise intolerance, cognitive
impairment, and reduced immune function.!"$D patients treated with
!"#s have shown significant improvement in 6uality of life (;1)
into
the nearnormal activity range as measured %y increased Karnofsky
/erformance "tatus "cale
scores, reflecting the adverse impact of anemia on activities of
daily living. MRN# recent clinical trial
has shown that intravenous (G) iron therapy significantly
improved ;1 scores in irondeficient,
stage O * CKD patients not on dialysis, even in the a%sence of
!"# therapy.MHN n a persuasive
testimony to the de%ilitating effects of CKDassociated anemia, a
patient not receiving dialysis who
had a 5$ of m17min noted that none of the effects of his disease
truly slowed him down
>e-cept anemia, which in recent years has forced me toward
retirement and had prevented me
from virtually all e-ercise, even walking *F minutes per day to
protect my heart.>MINn effect, anemia
acts as a riskmultiplier in CKD patients, e-acer%ating e-isting
;1 limitations and contri%uting to
comor%idities such as hypertension and other forms of CG disease
and dia%etes.
Case 3 'cont(
The clinician reviews @T3s medical history with her,
specifically asking a%out past occurrence of
stroke or other throm%otic events and cancer. The clinician
counsels @T a%out the practical
aspects of !"# therapy, including the necessity for fre6uent
parenteral administration and the
inconvenience associated with regular monitoring. #n occult
fecal %lood test is performed on site. #
%lood sample is o%tained to determine iron status.
#ll of the following clinical information is important in
deciding whether to use an !"# in
@T, a CKD patient, except'
Save and Proceed
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
8/25
/rior history of !"# use
@istory of stroke
/atient3s willingness to accept inconvenience and discomfort of
regular treatment
and monitoring$uling out iron deficiency as a primary cause of
anemia
$ationale and /vidence for 5reatment of Anemia
#nemia is easily diagnosed and relatively easy to correct, even
in patients with advanced kidney
disease. n doing so, clinicians should %e aware of relevant
treatment considerations. The first is
that circulating @% concentration, the principal %iomarker for
anemia, has a narrow reference range
that is often an elusive therapeutic target. Thus, maintaining
@% at target levels is dependent on
careful monitoring and dose ad:ustment of ironreplacement
therapy or !"#s. # second
consideration is that the optimal @% target in CKDassociated
anemia has %ecome somewhat
controversial %ecause of the outcomes of several largescale
randomized clinical trials ($CTs) that
evaluated treatment of anemia in CKD patients. The upshot of
these studies, which will %e
discussed %elow, is that the @% level achieved %y anemia therapy
may %e a source of %oth %enefit
and CG risk. Despite these therapeutic challenges, appropriate
treatment of CKD and anemia
together can su%stantially reduce CG risk, decrease transfusion
re6uirements, and improve ;1.
5or patients with stage * CKD and !"$D, !"#s are a cornerstone
of treatment. #vaila%ility of
!"#s with differing pharmacokinetic profiles ena%les
individualized treatment, specifically
regarding dose size and dosing intervals. #pproved initial and
maintenance dosing intervals are
shown in Ta%le . n practice, clinicians deviate widely from
these recommendations in nondialysis
CKD patients in order to individualize treatment. 5or e-ample,
epoetin is commonly given at
weekly or %iweekly intervals. Dar%epoetin alfa is often given at
intervals ranging from %iweekly to,
in some cases, monthly intervals on an offla%el %asis.
Table 1. Profile of FDA-Arove! Erythrooietin-"ti#ulating Agents
$1%&
Phar#aco'ineticProerties
(enericna#e
Tra!ena#e
FDA-Arove!!osingfre)uency
Co##onClinical*se
A!#inistration route
T+ , T+ ,"C T#a0
epoetinalfa
/rocritU,!pogenU
nitial' * timesweekly
0aintenance'individualized
nitial'weekly
0aintenance'
G or "C +.F.F
I.F.*
=.F+.F
Save and Proceed
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
9/25
weekly to *times weekly
individualized weekly to%iweekly
dar%epoetin alfa
#ranespU
nitial' weeklyor %iweekly
0aintenance'individualizedweekly to%iweekly
nitial'weekly or
%iweekly0aintenance' one doseevery +weeks
G or "C .* +H.H=I.=
+.F
SC = subcutaneous !" = intravenous #$ = p%as&a 'a%%ie
#&ax = ti&e to &axi&u& p%as&a
'a%%ie
"u%cutaneous ("C) administration of approved !"#s allows for
e-tended dosing intervals that
help reduce the inconvenience associated with in:ecta%le !"#
therapy. 5or e-ample, e-tended
dosing intervals for epoetin ranging from once weekly to once
every + or more weeks have %een
successful in maintaining @% levels V .F g7d1 in some patients.
MFNThe recommended approach is
to rule out iron deficiency as a primary cause of anemia prior
to !"# therapy, or to treat irondeficiency concurrently with !"#
therapy.
/SA Convenience Issues
Certain aspects of !"# therapy re6uire the for%earance of %oth
clinicians and !"$D patients. &"
5ood and Drug #dministration (5D#)approved !"#s (Ta%le ) are
photosensitive, highly la%ile
synthetic agents, re6uiring that they %e stored under
refrigeration and without shaking. 0ore
pro%lematic is the fre6uency of dosing needed for CKD therapy.
#s dosing fre6uency increases,
compliance inevita%ly declines. !poetin is approved for
administration * times weekly, though
dosing weekly or %iweekly is common in clinical practice.
Dar%epoetin has a longer halflife and
re6uires in:ection less fre6uently, at weekly or %iweekly
intervals depending on dialysis status.
Dar%epoetin is also occasionally used offla%el as a monthly
treatment. t should %e noted thatstudies have found that H of
predialysis CKD patients were a%le to maintain @% at O .F
g7d1 when epoetin was given at e-tended intervals from to more
than + weeks. MFN#n e-tended
dosing interval may %e of particular %enefit to patients who
selfadminister an !"#. !ach of the
three approved !"#s is indicated for selfadministration in
patients not on dialysis, a scenario that
makes it difficult to monitor compliance.
5he 5rial to $educe Cardiovascular /vents "ith Aranes 5heray
'5$/A5( and
Correction of !emoglobin and Outcomes in $enal Insufficiency
'C!OI$( Studies
The T$!#T study was an ongoing randomized, dou%le%lind,
multinational trial designed to
determine whether anemia therapy with dar%epoetin would reduce
mortality and CG events in
predialysis CKD patients with type dia%etes. 0ore than +FFF
patients with %aseline @% I.F.F
g7d1 not receiving !"# therapy were randomly assigned to achieve
a target @% of * g7d1 with
dar%epoetin therapy or place%o, with rescue dar%epoetin given
for @% P I g7d1. The primary
outcome was a composite endpoint of death, myocardial
infarction, acute myocardial ischemia,
congestive heart failure, and stroke. T$!#T was designed to
provide clinical guidance for the
future management of anemia in a highCGrisk population. t is the
largest $CT of anemia and
CKD conducted to date.
The primary results of T$!#T, reported in FFI, indicated that
use of dar%epoetin in patients with
dia%etes, CKD, and moderate anemia did not reduce risk for the
primary outcomes' death or a CG
or renal event.MN#dditionally, the annualized risk for stroke
(@$ .I4 I C, .*H.=H4 P P .FF)
was nearly dou%le in dar%epoetintreated patients vs the place%o
group, . vs .. #
su%se6uent analysis %y T$!#T investigators found that those
patients who had a poor initial
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
10/25
hematopoietic response to dar%epoetin had higher rates of CG
events. MNn contrast, those patients
with a good initial response to dar%epoetin did not have
increased CG events compared with the
place%o group, though they also did not show any reduction in CG
events. The T$!#T study and
the recent analysis confirm that treatment with !"# does not
reduce CG risk in nondialysis patients
and may increase the risk for some CG events. #lthough cancer
mortality was not significantly
different %etween dar%epoetin and place%o groups, T$!#T patients
with cancer history at %aselinehad a significantly greater cancer
mortality rate vs patients without a history of malignancy
(+7HH
vs 7=F4P Q .FF).MN
Current data %roadly indicate that CG disease is the leading
cause of death in CKD patients. The
C@;$ study,M*Na previous largescale $CT involving predialysis
CKD patients treated with epoetin
to achieve target @% levels of either .* g7d1 or *. g7d1, found
an increased risk with higher @%
target in a composite CG endpoint of death, stroke, myocardial
infarction (0), and heart failure.
The increased CG risk in the C@;$ study was driven %y a higher
rate of death and heart failure
associated with higher @% targeting. Thus, while these large
trials differ in design and the o%served
CG risks from !"# use designed to achieve higher @% levels, they
are harmonious on the point
that targeting higher @% does not reduce risks.
"ome %enefits do appear to accrue from anemia treatment in CKD,
including improvements in
fatigue in select patients and a reduction in likelihood of
transfusion. Dar%epoetintreated patients
in the T$!#T study had a ++ lower risk for %lood transfusions vs
the place%o group, +.H vs
+. (@$ F.=4 I C, F.+IF.=4 P P .FF).MN Dar%epoetintreated
patients also had a week
improvement in their 5#CT5atigue score of +. W F. points vs .H W
F.* points (PQ .FF)
compared with the place%o group. #n increase of * or more
points, considered to %e clinically
relevant, occurred in +.R of dar%epoetintreated patients vs +I.
of place%o patients (PQ .
FF), @owever, other ;1 factors related to energy and physical
functioning were not significantly
different %etween groups.
#le-ander /risant, a healthcare policy advisor and the CKD
patient 6uoted in the preceding
section, provided an elo6uent commentary on the pitfalls of
overreliance on onesizefitsall
guidelines derived from evidence%ased trials such as T$!#T.
#fter %eing placed on a regimen of
FF Jg of "C dar%epoetin administered %iweekly, >the results
have %een electrifying,> he reported
in a recent issue of theA&erican *ourna% o +idney
,iseases.MIN 5ollowing treatment, his @% level
rose to V g7d1 for the first time in more than years, allowing
him to e-ercise * times weekly
and virtually eliminating H years of sta%le angina. Commenting
specifically on the implications of
T$!#T, he offered the following recommendation to clinicians'
treat the patient as an individual.
@is response was e-ceptional, as evidenced %y the %linded trial
results in the T$!#T and C@;$
studies, %ut led to an important point' ?hether e-amining trial
results like T$!#T or guidelines
recommendations like those from the Kidney Disease ;utcome
uality nitiative (KD;) or
Kidney Disease' mproving lo%al ;utcomes (KD;), clinicians should
consider the particular
patient3s risks and %enefits of !"# therapy. f choosing to treat
with an !"#, monitor individual
response to determine whether further treatment is really
providing a lasting %enefit.
C@;$ was an $CT that evaluated the a%ility of epoetin to correct
anemia in more than +FF CKD
patients. /articipating patients were treated at epoetin doses
designed to achieve an @% level of
either *. g7d1 or .* g7d1 during a median treatment period of =
months. The group assigned
to the @% target level of *. g7d1 had a significantly higher
risk for CGassociated events (@$
.*+4 I C, .F*.R+4 P Q .F*).M*N!-cess CG events included
mortality and heart failure %ut not
stroke. mprovements in ;1 were similar in %oth treatment groups.
1imitations of C@;$ were its
openla%el design and high rate (*H.*) of early withdrawal for
reasons other than primary
endpoints.M+N"tudy investigators concluded that an @% target of
.* g7d1 rather than *. g7d1 is
an appropriate target to correct anemia in CKD patients. This is
consistent with the .F.F g7d1
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
11/25
range recommended %y the KD; guidelines and the 5D#approved goal
of maintaining @%
%etween F.F and .F g7d1 when using an !"#. # su%se6uent
metaanalysis of $CTs of !"#
usage in CKD patients with anemia concluded that patients in the
higher @% target group had a
significantly greater risk for allcause mortality ($$ .R4 I C,
.F.*4 P Q .F*).MN
5he Normal !ematocrit Study 'N!S(
The 2@" preceded T$!#T and C@;$ and differed from the later $CTs
in that it evaluated
anemia treatment in chronic dialysis patients (2 Q **) with
pree-isting CG disease. #ll
participants had a %aseline hematocrit of at least *F and were
then randomly assigned to receive
epoetin to maintain hematocrit of *F or raise it to +. /atients
randomly assigned to the lower
hematocrit target had a *F lower risk for mortality and nonfatal
heart attacks. 2@" for the first
time contradicted the conventional wisdom that aggressive
correction of anemia in patients
receiving dialysis was %oth %eneficial and without risk.M=N
6&O8I and F&A Guidelines for !emoglobin 5arget
$esults of the preceding trials are generally interpreted as
indicating that () adherence to the 5D#guideline of maintaining @%
levels S g7d1 is advisa%le for minimizing risk for CG
complications
from anemia therapy in CKD, and () little or no incremental
improvement in ;1 occurs %y
targeting a higher @% level. nformed %y largescale $CT results,
the KD; ?ork roup has
issued an evidence%ased clinical practice recommendation that
CKD patients %oth on and not on
dialysis who are receiving !"# therapy should generally have an
@% target in the range of .F
.F g7d1. &se of the word >generally> can %e
interpreted as allowing some latitude for
individualization of therapy. #dditionally, the guidelines
acknowledged that use of !"# was a
patientspecific decision. The ?ork roup has also issued a
clinical practice guideline stating that
CKD patients %oth on and not on dialysis who are receiving !"#
therapy should have an @% target
S *.F g7d1 in the a%sence of sufficient evidence of %enefit from
maintaining higher @% levels. MRN#n
interesting perspective on the KD; guidelines is the o%servation
that some ?ork roupmem%ers represent corporate interests and may
have a proindustry %ias that favors increased use
of !"#s.MFN
The 5D# @% targetrange lower limit for approved !"#s differs
somewhat from the KD; range
and recommendations. 1a%eling for 5D#approved !"#s recommends
>individualized dosing to
achieve and maintain hemoglo%in levels within the range of F to
g7d1.>MHFN The 5D# la%eling
also states that for patients una%le to achieve an @% of F.F.F
g7d1 after * months of increasing
!"# dose, clinicians should reduce the !"# dose to the lowest
necessary to avoid transfusions.
Case 3 'cont(
Discontinuance of oral iron therapy coincided with the patient3s
symptoms of fatigue and declining@% level. @T was found to have a
serum iron of H+ Jg7d1, a serum ferritin level of + ng7m1 and a
T"#T of . Dar%epoetin therapy was initiated at a dosage of * Jg
"C weekly, consistent with
the product3s recommended starting dose of F.+ Jg7kg.
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
12/25
?hat is the %est option for @T who is on !"# therapy %ut whose
@% level increases
a%ove the normal range to *.H g7d1L
Keep the !"# dose at the current level for an additional
weeks
"top !"# therapy4 resume at a lower dose when @% is P g7d1
$educe the !"# dose %y F
$educe the !"# dose %y
Challenges Associated )ith Current 5reatment Otions
# fundamental challenge facing clinicians in the management of
patients with renal insufficiency is
that, in general, controlled @% levels vary significantly over
time despite continuous !"# treatmentand ade6uate iron
availa%ility. This is principally %ecause intercurrent events and
varying sensitivity
to !"# alter @% levels %eyond our narrow therapeutic target
range. !-cessive alterations in !"#
dose, inade6uate time %etween !"# dose changes, and fluctuating
iron ade6uacy may also
contri%ute to this varia%ility. This phenomenon is termed @%
cycling (shortterm varia%ility in @%
level) and can %e e-acer%ated %y using currently availa%le
in:ecta%le !"#s at long dosing
intervals. t should %e noted that @% varia%ility is more
fre6uent and pronounced in dialysis
patients, such as the individual who will %e discussed in case ,
than in CKD stage * and +
patients not on dialysis.
!emoglobin 5arget $ange and Cycling
There is wide varia%ility of @% levels around the target range
of .F.F g7d1 and S * g7d1 in
!"#treated patients. 5or e-ample, a recent study found that more
than =F of !"#treated
patients receiving hemodialysis re6uired %etween = and I dose
ad:ustments per year to maintain
an @% target range of .F.F g7d1. MRN# trial of patients on
hemodialysis who were treated with
dar%epoetin found that !"# dose ad:ustments (increases or
decreases) were re6uired %y RF of
patients receiving dialysis during a Fweek titration period and
%y F during an Hweek
maintenance period.MRN# 5resenius 0edical Care 2orth #merica
largescale study of !"$D
patients (2 V =,FFF) found that only *H.+ of participants had @%
levels %etween .F and .F
g7d1.MNThe recommended approach to managing varia%le @% levels
in CKD patients is to
administer !"# dose titrations in increments of and to monitor
@% levels at least once
monthly after each ad:ustment.
Save and Proceed
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
13/25
The great ma:ority of patients on dialysis who are receiving !"#
therapy e-perience hemoglo%in
cycling or periodic changes V . g7d1 in @% levels, followed %y
reversion to the appro-imate
prefluctuation level over a period of H weeks or more. n one
study of patients receiving
hemodialysis, the mean num%er of @% e-cursions was *. W . per
year, with a mean @%
amplitude of . W F.HI g7d1 per e-cursion. MN0ore than IF of
patients in the study e-perienced
at least @% cycle. The aforementioned 5resenius study found that
I of !"$D patients movedfrom %elow to a%ove the @% target range or
vice versa during the *month tracking period. MNn
other words, the @% level in most !"$D patients is 6uite
varia%le due to physiologic factors (eg,
inflammation, chronic infection, %lood loss, iron status,
dietary intake, !/; resistance) or
iatrogenic causes (eg, effects of !"# or iron therapy, including
dose ad:ustments and withholding,
hospitalization, inade6uate dialysis, dialysis volume removal).
/erhaps the most clinically relevant
concern associated with @% cycling is treatmentrelated
>overshoots,> a rapid rise in @% defined %y
the 5D# as V g7d1 within a week period. The failure to find
incremental %enefit of @% levels V
g7d1 and the potential risks of @% levels outside the KD; target
range place added emphasis
on fre6uent monitoring and therapeutic dose ad:ustment on an
individualized %asis to offset the
impact of @% cycling.
#n important caveat applies to !"# dose ad:ustments' #de6uate
time must have elapsed %etween
ad:ustments to determine their ultimate effect on @% level.
$eacting to an overshoot %y a%ruptly
discontinuing treatment, for e-ample, can result in an a%rupt
drop in @% concentration to a level
well %elow the target range. # good rule of thum% is that !"#
dose should %e decreased %ut not
withheld when the @% level e-ceeds .F g7d1, dose ad:ustments
should %e in increments or
decrements, a +week interval should %e allowed to elapse %etween
dose ad:ustments, and
monitoring should %e done on at least a monthly %asis. &sing
this approach, it is not uncommon for
=H weeks to elapse %efore the desired @% level is reached while
at the same time e-cessive
e-cursions outside the target range are minimized. Ta%le
summarizes !"# dosead:ustment
guidelines in CKDassociated anemia.
Table . (ui!ance for E"A Dose A!2ust#ents in C3D or E"4D
Patients
#d:ust the !"# dose to maintain the @% level within the desired
range %ut not V .F
g7d1
#d:ust !"# dose in increments or decrements to avoid
overcompensating for @%
levels outside the target range
#llow a +week interval %etween !"# dose ad:ustments for
hematopoietic response to
occur
0onitor @% level on at least a monthly %asis to maintain target
@% level4 more fre6uent
monitoring may %e indicated after !"# dose changes
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
14/25
?hich statement a%out iron deficiency in a CKD patient with
anemia such as @T is trueL
#ll CKD patients with anemia have iron deficiency
;ral iron therapy should always %e administered %efore G iron is
given
Correction of iron deficiency will increase the response to !"#
therapy
ron therapy and !"#s should not %e given concurrently
Iron 5heray
0any CKD patients have a%solute iron deficiency, usually defined
as serum ferritin levels P FF
ng7d1 and T"#T P F. This can result from any of several causes,
including inade6uate dietary
intake, %lood loss, occult gastrointestinal malignancy, or
chronic inflammation. CKD is a
proinflammatory disease often due to chronic in:ury to the
kidneys, dia%etesassociated vascular
in:ury, malignancy, autoimmune disease, or infection. f an iron
deficiency e-ists, it must %e
corrected %efore a patient with CKD or on dialysis can respond
to !"# therapy. nitial treatment for
iron deficiency is usually with oral iron therapy for * months
or more. G iron therapy is generally
given as a single initial dose followed %y testing for ferritin
levels and T"#T and retreatment as
necessary. !"# therapy can %egin when la%oratory values indicate
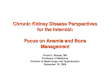
that the iron deficiency has%een treated successfully (5igure
).
Save and Proceed
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
15/25
Figure 1. $ecommended use of erythropoietinstimulating agents to
manage anemia in patients
with chronic kidney disease.
"ome patients do not respond even after several months of !"#
therapy with increment dose
increases. n the Dialysis /atients3 $esponse to G ron with
!levated 5erritin (D$G!) trial,
hemodialysis patients with refractory anemia had a faster and
larger @% response when treated
with mg of G ferrous gluconate for H consecutive hemodialysis
sessions. M*NThus, concurrent
G iron therapy can %e %eneficial in anemic patients on dialysis
who are receiving recommended
!"# dosages (5igure ).
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
16/25
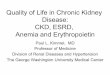
Figure . !valuation and treatment of iron deficiency for chronic
kidney disease patients receiving
erythropoiesisstimulating agents.
Clinicians should note that peripheral iron indices such as
serum ferritin and T"#T only have
moderate accuracy in predicting response to iron therapy.M+Nf
%oth T"#T and ferritin levels are low,
the likelihood of iron deficiency is high. #t higher levels,
these values have a relatively poorer
correlation with iron deficiency and response to !"# therapy.
;nly when the T"#T is truly high, ie,
at the F level, can iron deficiency %e definitively ruled out.
Thus, some patients with a ferritin
level in the FF*FF ng7m1 range and a T"#T level in the F*F range
may still %e iron
deficient and capa%le of %enefitting from a dose of G iron.
Case 34 Conclusion and &iscussion
The patient had an @% level of F.H g7d1 within weeks after
initiating !"#, and reported that her
fatigue was much reduced. @er ferritin level increased to *RF
mg7m1 and her T"#T level increased
to *F at + weeks after %eginning !"# therapy. "he maintained an
@% level %etween F.H and
g7d1 for the ne-t = months of treatment with no e-cursions a%ove
g7d1. G iron treatment was
not used %ecause her pretreatment iron levels were accepta%le
and consistent with ade6uate iron
stores. ;ver time while on !"# therapy, @T may %ecome iron
deficient, characterized %y higher
!"# dose re6uirements or lower @% and falling T"#T or ferritin
level. &se of oral or G iron at that
time may %e appropriate.
/merging /SA 5heraies
!poetin was the original synthetic endogenous !/; approved %y
the 5D# as an !"# in IHI.
Dar%epoetin, the secondgeneration !"# introduced in FF, has a
similar mode of action and
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
17/25
safety and efficacy profiles, %ut it re6uires much less fre6uent
dosing due to its longer halflife,
particularly following "C administration (Ta%le ). These !"#s
have replaced transfusions as first
line therapy for treatmentresponsive anemia in patients with
CKD. Aesides avoiding transfusion,
!"# therapy3s demonstrated %enefits include improved ;1 and
survival. n addition, there is
some evidence that !"#s may slow progression of renal disease
and provide cardioprotection
when @% levels are maintained within the F.F.F g7d1 treatment
target range.MFN#lthough theseearly !"#s are the current standard
of care and have transformed treatment of anemia in CKD,
the following e-perimental or newly emerging agents promise to
further increase our a%ility to
manage this aspect of renal insufficiency.
f our patient, @T, developed anti%odymediated pure red cell
aplasia (/$C#) related to
her !"# therapy, which of the following investigational agents
appears to %e most
promising for treatment of anemiaL
Continuous erythropoietin receptor activator (C!$#)
@ypo-iainduci%le factor (@5) sta%ilizers
@epcidin activators
/eginesatide
Peginesatide
/eginesatide (@ematideX) is an investigational !"# now %eing
tested in phase * clinical trials
involving patients with chronic renal failure, including trials
in patients receiving dialysis
(!0!$#1D and ) and in patients not receiving dialysis (/!#$1 and
). MN/eginesatide is a
novel, synthetic !"# that is immunologically unrelated to
endogenous human !/;. /ure red cell
aplasia (/$C#) is a rare %ut potential side effect of currently
availa%le !"#s, where%y the patient
develops neutralizing anti%odies to the recom%inant !/; analogs.
This nullifies the activity of the
!"# as well as endogenously produced !/;, leaving the individual
severely anemic and
dependent on %lood transfusions. !/; anti%odies do not
crossreact with peginesatide. #s a
result, peginesatide has shown the a%ility to increase and
maintain @% levels in patients with
/$C#, avoiding a rare %ut serious adverse effect of !"#s that
contain synthetic !/; analogs. n
Save and Proceed
http://www.medscape.org/viewarticle/736963_4http://www.medscape.org/viewarticle/736963_4
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
18/25
addition, peginesatide has the advantages of oncemonthly
administration, greatly reducing the
fre6uency and inconvenience of treatment, as well as storage at
room temperature.
n a phase trial, peginesatide maintained @% levels in patients
with CKD previously treated with
dar%epoetin. n the /!#$1 studies of patients not receiving
dialysis, peginesatide had mi-ed
results. #lthough peginesatide had e6uivalence to dar%epoetin in
increasing @%, higher rates ofmortality and CG events were
reported, and /!#$1 showed a higher percentage of patients
receiving transfusions. n the !0!$#1D studies of patients
receiving dialysis, peginesatide had
safety and efficacy e6uivalence to epoetin, including
transfusion rates.
Continuous /rythrooietin $ecetor Activator
Continuous erythropoietin receptor activator (C!$#) is the
generic designation for a third
generation !"# class in which the !/; analog is pegylated, a
drug delivery formulation that alters
pharmacokinetics so that the clinically active agent has an
e-tended halflife. n the case of
C!$#s, pegylation allows e-tended dosing intervals. 0etho-y
polyethylene glycolepoetin %eta is
the firstinclass C!$#, licensed as 0iceraU%y $oche in FFH for
oncemonthly treatment of CKD
associated anemia, including in patients receiving dialysis. n a
recent phase * study, metho-y
polyethylene glycolepoetin %eta maintained target @% levels more
successfully than dar%epoetin
at oncemonthly dosing intervals, despite dose increases with
dar%epoetin. M=N# noteworthy aspect
of the study was that the early withdrawal rate was + in the
metho-y polyethylene glycol
epoetin %eta group vs +F for dar%epoetin, with the difference
primarily due to a higher rate of
insufficient therapeutic response in the dar%epoetin patients.
The !"#s had compara%le safety
profiles. 0etho-y polyethylene glycolepoetin %eta is approved
for use in the !uropean &nion %ut
has yet to %e marketed commercially in the &nited "tates due
to patent disputes. #n interesting
aspect of C!$# therapy is that some clinicians may actually
prefer shorteracting !"#s so that the
dose response can %e more closely controlled in order to
minimize the potential for adverse side
effects.
!yo9ia7Inducible Factor Stabili0ers
@5 is a key regulator of !/; gene e-pression. @5 responds to
changes in cellular or circulating
o-ygen levels. f %lood o-ygen levels decline, as in anemia or at
highaltitude environments, @5 is
activated from renal cells and !/; production rapidly increases.
$ecently, @5 has %ecome a
therapeutic target for treatment of anemia in CKD patients.
&nder normal conditions, @5 is
meta%olized %y prolylhydro-ylase. &nder hypo-ic conditions,
prolylhydro-ylase is inhi%ited
%ecause it uses o-ygen, thus sta%ilizing @5 e-pression. 5= and
5+I MRN(developed %y
5i%roen, nc) are oral @5 sta%ilizers that function as
prolylhydro-ylase inhi%itors (/@s) and
are %eing evaluated in phase trials as oral agents given or *
times weekly. $esponse time
occurs in * weeks. ;f particular interest was the a%ility of 5=
to stimulate erythropoiesis
compara%le to dar%epoetin therapy, %ut with only modest
increases in plasma !/; levels. MHNThis
was attri%uted to /@ upregulation of other erythropoiesis
pathways, particularly iron mo%ilization.
This activity would potentially allow erythropoiesis even in
!"$D patients with negligi%le kidney
function. ;ne safety concern with this class of drugs is whether
they would e-acer%ate cancer
%ecause @5 is angiogenic and is constitutively e-pressed %y some
cancers.
5heraeutic $ole of !ecidin
The hormone hepcidin is the predominant negative regulator of
iron a%sorption from the intestine
and iron release from macrophages for purposes of o-ygen
transport. This homeostatic
mechanism ena%les tight control of iron, simultaneously avoiding
to-ic effects of iron overload
while meeting physiologic demands for iron use. nflammation,
hypo-ia, and anemia all suppresshepcidin production, removing its
inhi%itory effect on iron a%sorption and iron release from
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
19/25
macrophages.MIN &nderstanding hepcidin synthesis pathways
may contri%ute to an alternative
treatment of anemia, specifically %y means of hepcidin
antagonists, which would increase iron
availa%ility. This would provide a therapeutic option separate
from !"# treatment, thus avoiding
the occasional adverse side effects of !"#s, such as
hypertension and anti!/; immune
response.
/PO&:$/ ;ioum
Treatment of anemia in patients with CKD typically involves "C
administration of !"#s at regular
intervals followed %y fre6uent la%oratory tests to monitor @%
concentration. The !/;D&$!
Aiopump (0edgenics4 Gienna, Girginia) is a sustained !/; drug
delivery system for CKD patients.
!/;D&$! is an autologous dermal %iopump capa%le of sustained
secretion of !"#s at
therapeutic levels. # small tissue e-plant is harvested directly
from the patient3s dermis under local
anesthetic. The %iopump is produced %y e- vivo introduction of
the !/; gene into cells of the
e-plant, which then e-presses and secretes !/;. The %iopump is
su%se6uently implanted
su%cutaneously %ack to the patient in order to provide
continuous delivery of a known amount of
!/;. /hase and clinical trials, as yet unpu%lished, have
demonstrated sustained !"# therapy
for greater than months in CKD patients implanted with the
%iopumps. M*FN
Case
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
20/25
;n the %asis of the information provided, what is the most
likely e-planation for 0/3s
anemiaL
nade6uate !"# therapy
nfectionrelated inflammation
;ccult %lood loss
nterventionalprocedure related %lood loss
#ll of the a%ove
Anemia ,anagement in !ositali0ed Patients on &ialysis
@ospitalization is common in patients on dialysis and fre6uently
e-acer%ates CKDassociated
anemia. @ospitalization rates vary depending on the severity of
CKD and certain comor%idities. 5or
e-ample, 0edicare patients with stage * CKD had allcause
hospitalization rates that were I
higher than those of patients with stage CKD. 0edicare patients
with CKD also had hospital
admission rates for all causes, CG disease, and infection that
were *H+= higher than for non
CKD patients.M*N
/atients on dialysis who have prehospitalization @% levels
within the KD; target range often
have depressed @% levels during or after hospitalization. The
posthospitalization decrease in @%
levels can %e significant and prolonged. 5or e-ample, one study
found that hospitalized dialysis
patients (2 Q =) had @% levels at discharge and for months
thereafter that were significantly
lower (F.R W F. vs .+ W F. g7d14 PP .F) than at months prior to
admission.M*NThe
prolonged decrease in @% levels occurred despite an increase in
mean epoetin dosage (H vs
H &7kg7week4 P P .FFF) during the month period after
discharge.
5actors associated with su%normal or declining @% levels after
hospitalization include pree-isting
anemia, high prehospitalization !/; re6uirements, inade6uate or
interrupted !"# administrationduring hospitalization, e-tended
stays, and diagnosis of congestive heart failure or other CG
Save and Proceed
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
21/25
disease. ;ther causes of anemia in hospitalized patients on
dialysis include fre6uent or high
volume %lood sampling, %leeding, surgery or other sources of
%lood loss, inflammation or
infection of arteriovenous grafts or fistulas, and poor wound
healing. n older patients on dialysis,
%lood loss can often result from lesions such as gastric ulcers,
diverticulitis, colonic
hemorrhoids, or fissures. Treatment with anticlotting agents
such as clopidogrel can increase %lood
loss from these sources of lowgrade occult %leeding. nflammation
may also occur duringillnesses. This can lead to increased hepcidin
levels which in turn reduce iron %ioavaila%ility. M**N
nflammation may also hinder the response to !"# therapy. #ny of
these pree-isting conditions
can %e predictive of the need for increased !"# dosing during or
after hospitalization.
Case < 'cont(
&pon return to his dialysis unit + weeks later, 0/3s epoetin
dose is increased from ,FFF to
H,RF unit7week, a dose increase. The dosing fre6uency for the
FFmg G iron therapy is
increased to once weekly. # hemoccult test performed to
determine whether there was occult
%lood loss is negative. @emoglo%in, serum ferritin, and T"#T
levels are determined + weeks after
discharge to assess anemia status. The @% level at that time is
F.+ g7d1, ferritin level is I+
ng7m1, and T"#T level is +.
#ssuming that your @% target is g7d1, what would %e the most
appropriate
intervention for 0/ at this pointL
#dminister FFF mg oral iron over * weeks
ncrease his !"# dose another
Aoth of the a%ove
Continue present therapy and reevaluate in + weeks
?hen preadmission @% levels are within the KD; target range,
patients receiving dialysis clearly
are at a lower risk of having @% concentration fall
precipitously %elow the g7d1 anemia threshold
during and after hospitalization. Thus, it is advisa%le to
maintain @% in the target range for dialysis
patients through prudent use of !"# and iron therapy. iven the
long interval %etween !"# dose
Save and Proceed
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
22/25
changes and hematopoietic response, a dose increase should
generally occur only once during
most hospitalizations, and only after a +week interval has
elapsed since the last increase.
Case
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
23/25
. 5oley $2, /arfrey /", @arnett BD, et al. The impact of anemia
on cardiomyopathy,
mor%idity, and and mortality in endstage renal disease. #m B
Kidney Dis. II=4H'*=.
#%stract
=. 1evin #, Thompson C$, !thier B, et al. 1eft ventricular mass
inde- increase in early renal
disease' impact of decline in hemoglo%in. #m B Kidney Dis.
III4*+'*+.#%stract
R. 0oreno 5, #racil 5B, /[rez $, et al. Controlled study on the
improvement of 6uality of life
in elderly hemodialysis patients after correcting endstage renal
diseaserelated anemia
with erythropoietin. #m B Kidney Dis. II=4R'+H=.#%stract
H. #garwal $, $izkala #$, Aastani A, et al. # randomized
controlled trial of oral versus
intravenous iron in chronic kidney disease. #m B 2ephrol.
FF=4='++++.#%stract
I. /risant #. T$!#T versus treatment' # patient3s view of a
scientific interpretation. #m B Kid
Dis. FF4'#*#*.
F. ?ish BA, Coyne D?. &se of erythropoiesisstimulating
agents in patients with anemia of
chronic kidney disease' overcoming the pharmacological and
pharmacoeconomic
limitations of e-isting therapies. 0ayo Clin /roc.
FFR4H'*R*HF.#%stract
. /feffer 0#, Aurdmann !#, Chen C
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
24/25
I. #ranespU(dar%epoetin alfa) 5or n:ection. /rescri%ing
information. #mgen nc. $evised
0ay FF.
F. !/;!2U(!poetin alfa) 5;$ 2B!CT;2. /rescri%ing information.
#mgen nc. $evised
5e%ruary FF.
. 1acson ! Br, ;fsthun 2, 1azarus B0. !ffect of varia%ility in
anemia management on
hemoglo%in outcomes in !"$D. #m B Kidney Dis.
FF*4+'+.#%stract
. 5ish%ane ", Aerns B". @emoglo%in cycling in hemodialysis
patients treated with
recom%inant human erythropoietin. Kidney nt.
FF4=H'**R*+*.#%stract
*. Coyne D?, Kapoian T, "uki ?, et al. 5erric gluconate is
highly efficacious in anemic
hemodialysis patients with high serum ferritin and low
transferrin saturation' results of the
Dialysis /atients3 $esponse to G ron with !levated 5erritin
(D$G!) "tudy. B #m "oc
2ephrol. FFR4H'IRIH+.#%stract
+. "tancu ", A^rsan 1, "tanciu #, et al. Can the response to
iron therapy %e predicted in
anemic nondialysis patients with chronic kidney diseaseL Clin B
#m "oc 2ephrol.
FF4'+FI+=.
. #ffyma- and Takeda announce phase * trials meet primary
endpoints for investigational
drug, hematide(T0)7peginesatide, to treat anemia in chronic
renal failure with some
differences noted in secondary analyses. Bune , FF. M/ress
release.N #vaila%le at'
http'77www.takeda.com7press7article]*=.html#ccessed Banuary H,
F.
=. Carrera 5, 1ok C!, de 5rancisco #, et al. 0aintenance
treatment of renal anaemia in
haemodialysis patients with metho-y polyethylene glycolepoetin
%eta versus dar%epoetin
alfa administered monthly' a randomized comparative trial.
2ephrol Dial Transplant.
FF4'+FFI+FR.#%stract
R. Aesara% #, @ulter @2, Klaus ", et al. 5+I, a novel oral @5
prolyl hydro-ylase
inhi%itor, elevates hemoglo%in in anemic stage *7+ CKD patients.
/rogram and a%stracts
of the +*rd #nnual 0eeting "cientific !-position of the #merican
"ociety of 2ephrology
(#"2) $enal ?eek4 2ovem%er =, FF4 Denver, Colorado. /oster
"#5C+=.
H. Aunn @5. 2ew agents that stimulate erythropoiesis. Alood.
FFR4FI'H=HHR*.#%stract
I. /ak 0, 1opez 0#, a%ayan G, anz T, $ivera ". "uppression of
hepcidin during anemia
re6uires erythropoietic activity. Alood.
FF=4FH'*R*F*R*.#%stract
*F. Aesara% #, 2issenson #$, "chwartz D, et al. !rythropoiesis
sustained months %y the
!/;D&$! %iopump in patients with chronic kidney disease'
further results of phase 7
proof of concept trial. /rogram and a%stracts of the +*rd #nnual
0eeting "cientific
!-position of the #merican "ociety of 2ephrology (#"2) $enal
?eek4 2ovem%er =,
FF4 Denver, Colorado. /oster 5 5CRF.
*. &nited "tates $enal Data "ystem. FF #tlas of CKD and
!"$D. Gol , #tlas of CKD,
Chapter +, 0or%idity and 0ortality. #vaila%le at'
http'77www.usrds.org7atlas.htm. #ccessed
Decem%er , FF.
http://www.medscape.org/medline/abstract/12500228http://www.medscape.org/medline/abstract/12500228http://www.medscape.org/medline/abstract/16105069http://www.medscape.org/medline/abstract/17267740http://www.takeda.com/press/article_36525.htmlhttp://www.medscape.org/medline/abstract/20522670http://www.medscape.org/medline/abstract/17032916http://www.medscape.org/medline/abstract/16882706http://www.usrds.org/atlas.htmhttp://www.medscape.org/medline/abstract/12500228http://www.medscape.org/medline/abstract/16105069http://www.medscape.org/medline/abstract/17267740http://www.takeda.com/press/article_36525.htmlhttp://www.medscape.org/medline/abstract/20522670http://www.medscape.org/medline/abstract/17032916http://www.medscape.org/medline/abstract/16882706http://www.usrds.org/atlas.htm
-
7/25/2019 Anemia Management in Chronic Kidney Disease and
End
25/25
*.















![Anemia of Chronic Disease-1.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/.../his127_slide_anemia_of_chronic_disease.pdf · Anemia of Chronic Disease (ACD) = Anemia of Chronic Inflammation](https://img.dokumen.tips/doc/110x75/5c00539409d3f24d2c8b7d4b/anemia-of-chronic-disease-1ppt-read-only-ocwusuacidocwusuacidhis127slideanemiaofchronic.jpg)