Embed Size (px)
Citation preview


1page
International Organising Committee (Wess) 2
Local Organising Committee (Mss)
International Faculty 3
Local Faculty
Messages
• MinisterofHealthMalaysia 4
• Chairman,LocalOrganisingCommittee,MalaysiaSpineSociety 5
• President,WorldEndoscopicSpineSociety(WESS)& 6 InternationalCo-Chairman,InternationalOrganisingCommittee
• InternationalCo-Chairman,InternationalOrganisingCommittee 7
ProfessorDato’DrMohammadAbdulRazak–OutstandingLeadershipInSpine 8 Citation by Dr Sabarul A Mokhtar
ProgrammeSummary 9
DailyProgramme 10–13
Post-CongressWorkshop 14
CongressInformation 15
FloorPlan&TradeExhibition 16
Acknowledgements 17
Abstracts 18–56
• Symposia/Plenaries 18–37
• BestFreePaperPresentations1 38–43
• FreePapers2 44–49
• PosterPresentations 50–56
contentscontents
2page
InteRnAtIonAL oRGAnIsInG coMMIttee (Wess)InteRnAtIonAL oRGAnIsInG coMMIttee (Wess)
International Co-Chairmen JeanDestandau (France)
ShrinivasMRohidas(India)
LocAL oRGAnIsInG coMMIttee (Mss)LocAL oRGAnIsInG coMMIttee (Mss)
Advisor RRamanathan
Chairman MohammadAbdulRazak
Secretary SabarulAlfianbMokhtar
Treasurer KwanMunKeong
Scientific Committee AbdulHalimYusof(Chairman)
LimHengHing
MuralitharanPerumal
SawLimBeng
Social Paramaeshwarana/lKasipillai
Publications / Publicity NurulAzwaMohdNoor
Audio Visual ChrisChan
Committee Members AbdulMalikMohamedHussein
AzmiBaharuddin
ChoongLeongTong
MazwarSofiyan
ZairulAnuarbKamarulBahrin

3page
InteRnAtIonAL FAcULtYInteRnAtIonAL FAcULtY
AUSTRALIA
IanWangYiYuan
FRAnCe
JeanDestandau
IndIA
ShankarAcharya
PCDey
ArvindJayaswal
MohinderKaushal
ShrinivasMRohidas
IndoneSIA
AloysiusBambangDarwono
LuthfiGatam
JAPAn
Koji sato
KoReA
HyeunSungKim
SInGAPoRe
GabrielLiu
SPAIn
PeterSalgado
TAIWAn
Po-QuangChen
ThAILAnd
PraditPrateepvanich
USA
AnthonyYeung
AbdulHalimYusof
AbdulWahabGhani
ChoongLeongTong
KwanMunKeong
NizarAbdulJalil
MuralitharanPerumal
KSSivananthan
TanChorNgee
TohCharngJeng
LocAL FAcULtYLocAL FAcULtY

4page
ItgivesmegreatpleasuretopenthismessageinconjunctionwiththeInternationalMinimallyInvasiveSpineCongress,tobeheldinKualaLumpurfrom20thto 22nd March2014.
Inthespiritof1Malaysia,andasanationworkingtogetherforbetterhealth,Iampleased that this important congress is being ably co-organisedby theMalaysiaSpineSocietyandtheWorldEndoscopicSpineSociety,withtheparticipationofUniversitiKebangsaanMalaysia.
Thethemeof thiscongress,“TheTrendandFuturePractice”, is indeedahighlyaptoneandIampleasedthattheOrganisingCommitteehasassembledaneminentfacultyofexpertsfromaroundtheregionaswellasinternationally,tosharetheirtreasure trove of knowledge and expertise with congress participants, whowilllearnmore about treating patientswith spine pathologies and problems, aswellas update their understanding of the basic principles and how to overcome thedifficultiesencounteredinclinicalpractice.
Wishingyoueverysuccess,aswellasamemorableandfruitfulcongress.
MessAGeMessAGe
dATUK SeRI dR S SUbRAMAnIAM
MinisterofHealthMalaysia
5page
ItisarealpleasureformetowelcomeeverybodytothisCongressoftheMalaysiaSpineSociety(MSS)withWorldEndoscopicSpineSociety(WESS).Weareveryexcitedtohostdelegatesfromvariouspartoftheglobeforthisveryuniqueevent.
This is the first time in this region where various disciplines with differentapproachesarepresentingtheirviewsandtheirworkinacommonplatform.Wehaveinvitedpainspecialists,endoscopistsandminimally-invasivespinesurgeonsfromvariousrelatedspecialtiestodiscussanddebatefreelyontheirbesteffortsinmanagingbackpain.At thesametime,wewillalsofocusonthebasicconceptsandprinciplestoensurethatthesearenotlostinthemidstofinnovativeproceduresandtechniques.Wehopethatthedelegateswillstayflexibleandbereadytoadaptandtolookforbetteralternativesandwaysthatgiveoptimalshortandlongtermoutcome.
Iamsurethatyouwillgetinvaluableexposureandbestopportunityofenhancingnetworkingthatwillpromotefuturecooperationandcollaboration.
Wehaveallocatedaspecialforumthatcantrulydrivenewlearnerspassingthroughthelearningcurvebyinvitinggreatpersonalitiesandexpertstorelatetheirpersonaldifficulties and their trajectory during their early days of engaging with theirspecialisedtrade.
Lastly, may I welcome delegates to this beautiful country which is famous fordelicious and exciting foods, unbelievable sandywhite beaches, rain forest andexoticislandsandnottheleast,thegreathospitalityofMalaysianpeople.
MohAMMAd AbdUL RAzAK
Chairman,LocalOrganisingCommitteeMalaysiaSpineSociety
MessAGeMessAGe

6page
MessAGeMessAGe
Onbehalfof theorganiserandWorldEndoscopicSpineSociety(WESS), it isagreatprivilegeformetowelcomeallthedelegatesfromallovertheworldtothisevent.
IwouldliketothankthePresidentofMalaysiaSpineSociety(MSS)forhostingtheCongressandacceptingWESSasaco-hostforthisconference.
Wearealsofortunatetohavemanyexpertsaswellasdistinguishedspeakersfromallover theregion,comingtogether toshare theirknowledgeandexperienceonMISandalsothesharingofglobalchallenges.
ThethemeoftheCongress,“TheTrendandFuturePractice”,echoestheimportanceof respecting the natural body biomechanics and its functional purposes whiletreatingandremovingitspathologicpartsandthus,shouldthestandardoffuturepractice.We hope theCongresswill stimulate innovative thinking and helps toexplorenewfrontiersinreachingarealsolutionformanyunresolvedpathologies.Hence,webringexpertswithdifferentadoptedconceptsandapproachestogetherprovidingaspectrumandacontinuumofmanagement.
Malaysiaisabeautifulcountryanda“TrulyAsia”,andthedelegateswillsurelyenjoythestayandtheweather.
JeAn deSTAndAU
President,WorldEndoscopicSpineSociety(WESS)&InternationalCo-Chairman,InternationalOrganisingCommittee

7page
MessAGeMessAGe
Welcome toMIS InternationalCongress, held here inKualaLumpur,Malaysia.Thisisaspecialoccasionwhereexpertswhomanagedspineproblemsfromdifferentdisciplines from various part of the world meet: neurosurgeons, orthopaedicsurgeonsandpainspecialists.
Sharingofexperiencesfromdifferentperspectiveswithdifferentapproachesandusingvarioustechniqueswillsurelybeanexcitingprospect,anddefinitelywillhelpintheunderstandingandtreatingspinalpathologiesinmoreholisticandbroaderdimension.
Minimally invasive surgery isgoing tobegold standardandbenchmark innearfuturepractice.Withtheuseofendoscope,itoffersanewdepthandanenlightenedinsideviewintothenarrow,previouslynoteasilyreachable,corridorsofspine.
Themainhurdle in treatingdegenerative spinepathologies seems tobe treatingpathologiesatvariousstages,ages,withdifferentways.TheCongresswillhelpustoknowmoreaboutthesedifficultieswithunderstandingofbasicprinciples.Wewillensurethatthismeetingtakesplaceinaverycordiallyandfriendlyatmosphere,allowingfruitfulexchangesofinformationandopinions.
EnjoyyourstayinKualaLumpur.
ShRInIVAS M RohIdAS
InternationalCo-Chairman,InternationalOrganisingCommittee

8page
PRoFessoR DAto’ DR MoHAMMAD ABDUL RAZAK – oUtstAnDInG LeADeRsHIP In sPIne
MohamadBinAbdulRazakwasbornon16thNovember1953inthetownofKulaiofthesouthernstateofJohore,Malaysia.HereceivedearlyformaleducationatSekolahKebangsaanKulai,thenatSekolahMenengahSultanIbrahim,bothinKulai,Johore.HewentontoKualaLumpurtostudyattheprestigiousboardingschool,SekolahAlamShah.LittlethatheknewthefutureUniversitiKebangsaanMalaysiaMedicalCentrewastobebuiltastonethrowawayfromthisschool,thirtyyearslater.
HejoinedUniversitiKebangsaanMalaysia(UKM)asoneof thepioneerbatchof44medicalstudentsfortheMedicalFacultywhenitstartedthepremedicalcourse
attheScienceFaculty,atthemaincampusofUKM,atJalanPantaiBaru,KualaLumpur,inMay1973.TheFaculty latermovedtoHospitalKualaLumpurcampus, in1977.Hegraduatedwith theMedicalDegree(MD–UKM)in1979andstartedhisinternshipatHospitalKualaLumpur.HewasinthepioneerbatchoftheMastersofSurgery(Orthopaedics)programmeinUKMwhichwasinitiatedbythelateProfessorQuaziMIqbal.Aftercompletinghisorthopaedictraining,hejoinedthework-forceasasurgeon,academicianandresearcherintheDepartmentofOrthopaedicsandTraumatology,UniversitiKebangsaanMalaysia.Hewasadedicatedsurgeonandlovedbyhismedicalstudents.HewasalsotheCollegeMastersforthemedicalstudent’shostel,KolejTunDrIsmail.He later travelledabroad toUnitedKingdomforhissubspecialitytraininginspinesurgeryattheEdinburghUniversityandSouthportSpinalInjuriesCentresinLiverpool,from1991till1993.
Upon coming back from the UK, he was appointed as the Head for Department of Orthopaedics andTraumatology,UKM,till2002.Withinhistenureinthisoffice,hehadheldthepostofthePresidentoftheMalaysianOrthopaedicAssociation(1996-1998).HealsobuiltuptheMastersofOrthopaedicsprogrammeand initiatedwith fellowcolleagues inUniversityofMalayaandUniversitiSainsMalaysia, to form theConjointBoardofOrthopaedics(CBO)whichoverseethetrainingandexaminationoforthopaedicsurgeonsinthecountry.Later,hewasgiventheresponsibilityofbeingtheDirectoroftheUKMMedicalCentre,from2002till2009,untilcalleduponbythemaincampusofBangitobecometheDeputyVice-ChancellorofUKM.In2011,AllianzeUniversityCollegeofMedicalSciencesappointedhimastheVice-ChancellorafterservingUKMfornearly31years.
HeismarriedtoDatinRokiahwithfourchildren(ShawalFaizal,ShawalFirdaus,MohdAimanandSitiNurulAini),andthreegrandchildren.
Citation by Dr Sabarul A MokhtarCitation by Dr Sabarul A Mokhtar

9page
PRoGRAMMe sUMMARYPRoGRAMMe sUMMARY
dATeTIMe
20th MARCh 2014(ThURSdAy)
21st MARCh 2014(FRIdAy)
22nd MARCh 2014(SATURdAy)
0700–0800MeeT-The-exPeRTS
1 & 2MeeT-The-exPeRTS
3 & 4PoST-ConGReSS WoRKShoPS
(0830–1700)
Venue : Advanced Surgical Skills Centre (ASSC), universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur
Management of Lumbar Spine diseases: Live demonstration & Cadaveric Interventional Workshop
Cadaveric Workshop
Live Surgery
0800–0830oPenInG CeReMony
PLenARy 2
0830–0900SyMPoSIUM
5SyMPoSIUM
60900–0930 PLenARy 1
0930–1000SyMPoSIUM 1
Tea
1000–1030 beST FRee PAPeR
PReSenTATIonS 1
FRee PAPeRS
21030–1100 Tea
1100–1130SyMPoSIUM 2 SyMPoSIUM
7SyMPoSIUM
81130–1200
1200–1330Lunch SaTeLL I Te
SympoSIum[Jalinan Sejagat Sdn Bhd]
Lunch SaTeLL I TeSympoSIum
[Pfizer (Malaysia) Sdn Bhd]
LunchF r iday Prayers
1330–1400SyMPoSIUM 3
1400–1430
1430–1500SyMPoSIUM 4 SyMPoSIUM 9
1500–1530
1530–1600 Tea
FoRUM on MISS
1545–1815
CoMPAnyWoRKShoPS
1600–1630
1630–1700 Tea
1700–1800 WeSS AGM
1800–1900 1815–1915MSS AGM
1900–2200 1930–2200ConGReSS dInneR

10page
DAILY PRoGRAMMeDAILY PRoGRAMMe
Day 1 – 20Day 1 – 20ThTh MARCH 2014 (THURSDAY) MARCH 2014 (THURSDAY)
0700–0800 MeeT-The-exPeRTS 1 [Mss] KEDAH ROOM
K S Sivananthan / Sabarul Alfian b Mokhtar / Fazir Mohamad / Abdul Malik Mohamed Hussein
0700–0800 MeeT-The-exPeRTS 2 [Medtronic] SELANGOR ROOM
MASTMIDLFProcedureandCasePresentationOh Kim Soon / Shankar Acharya
0800–0900 oPenInG CeReMony oPenInG CeReMony SAbAH ROOM
0750–0800 Guestsanddelegatestobeseated. 0800–0805 ArrivalofYB Datuk Seri Dr S Subramaniam,MinisterofHealthMalaysia 0805–0810 WelcomebyProf Dato’ Dr Mohammad Abdul Razak,Chairman,LocalOrganisingCommittee 0810–0820 SpeechbyDr Shrinivas Rohidas,Vice-President,WorldEndoscopicSpineSociety(WESS) 0820–0850 SpeechbyYB Datuk Seri Dr S Subramaniam,MinisterofHealthMalaysia followedbyOpeningoftheCongress 0850–0900 OpeningofTradeExhibition
0900–0930 PLenARy 1 SAbAH ROOM
Chairperson: Harwant Singh
AvoidingandmanagingcomplicationsofminimallyinvasivespinesurgeryIan Wang Yi Yuen
0930–1030 SyMPoSIUM 1 SAbAH ROOM
Invasive Pain Management in Chronic back Pain: between evidence-based and Current Practice
Chairpersons: nizar Abdul Jalil / Muralitharan Perumal
Diagnosisandmanagementofprimaryandsecondarymyofascialpainsyndrome inbackpain [pg 18]
Pradit Prateepvanich
Discogenicpain:Isthereanysolution? [pg 18]
nizar Abdul Jalil
EvidenceininterventionalpainmanagementMuralitharan Perumal
Epidurolysisinfailedbacksurgerysyndrome:Doesitreallyworks?Peter Salgado
1030–1100 Tea
1100–1200 SyMPoSIUM 2 SAbAH ROOM
Image-Guided Spine InterventionChairpersons: Deepak Singh / Abdul Wahab Ghani
Epiduroscopyandepidurolysis:BasicprinciplesandtechnicalconsiderationPeter Salgado
Radiofrequencyneurolysis:Whoreallybenefits? [pg 19]
Abdul Wahab Ghani
Ultrasound-guidedneckandbackpaintherapy:Betteroption [pg 19]
Choong Leong Tong
Spinalcordstimulationinchronicbackpain [pg 20]
Toh Charng Jeng

11page
DAILY PRoGRAMMeDAILY PRoGRAMMe
Day 1 – 20Day 1 – 20ThTh MARCH 2014 (THURSDAY) MARCH 2014 (THURSDAY) [conT’D] [conT’D]
1200–1330 Lunch SaTeLL I Te SympoSIum [JalinanSejagatSdnBhd] SAbAH ROOM
Chairperson: Abdul Halim Yusof
- Newdynamicstabilizationdeviceforthetreatmentofearlyandlatelumbar degenerativeproblems - Designofinterlaminardeviceandsurgicaltechnique
Aloysius Bambang Darwono
1330–1430 SyMPoSIUM 3 SAbAH ROOM
endoscopic Spine Surgery 1Chaipersons: Gilbert Mawera / Sabarul Alfian b Mokhtar
EvolutionofendoscopicspinesurgeryJean Destandau
Learningcurveinendoscopicspinesurgery:HowNOTtostopdoing [pg 21]
Mohinder Kaushal
Endoscopic/Microscopic&Interlaminar/Transforaminal:Mychoice [pg 22]
Shrinivas M Rohidas
Endoscopiclumbardiscectomy:Asimplifiedapproach [pg 23]
P C Dey
1430–1530 SyMPoSIUM 4 SAbAH ROOM
endoscopic Spine Surgery 2Chairpersons: P C Dey / Ahmad Tajuddin
Endoscopiclumbardecompression:Betweenprinciplesandpractices [pg 24-25]
Abdul Halim Yusof
Endoscopiccervicalspinesurgeries–Thebasicsandavoidingcomplications [pg 26-27]
Shrinivas M Rohidas
Endoscopicdiscsurgery:Afuturestandardpractice [pg 27]
Mohinder Kaushal
EndoscopicsurgeryforintraspinaltumoursJean Destandau
1530–1545 Tea
1545–1815 WORKSHOPSonMinimalInvasiveSpineProceduresMIS TLIF [Synthes DePuy] KEDAH ROOM
Ian Wang Yi Yuen
MIDLIF Sawbone Workshop [Medtronic] SELANGOR ROOM
Oh Kim Soon / Shankar Acharya
ultrasound guided nerve root and facet injection in cervical and lumbar spine SARAwAK ROOM [Abex Medical System]
1815–1915 MALAySIA SPIne SoCIeTy AGM MALAySIA SPIne SoCIeTy AGM SARAwAK ROOM
1930–2200 ConGReSS dInneR ConGReSS dInneR LAMAN wAu, KOMpLEKS KRAf, K L

12page
DAILY PRoGRAMMeDAILY PRoGRAMMe
0700–0800
0700–0800
MeeT-The-exPeRTS 3 [Wess] KEDAH ROOM
MeeT-The-exPeRTS 4 [Novamedika] SELANGOR ROOM
Soo-Bin Im
0800–0830 PLenARy 2 SAbAH ROOM
Chairperson: Ozlan Izma Kamil
Minimalinvasivespineprocedures:ThetrendandfutureAnthony Yeung
0830–0930 SyMPoSIUM 5 SAbAH ROOM
endoscopic Spine Surgery 3Chairpersons: Lim Heng Hing / nurul Azwa
Discectomyusingtransforaminaltechniques: TricksandpitfallsHyeun Sung Kim
StructuralpreservationPELDligamentum flavumsplittingHyeun Sung Kim
Transforaminalselectiveendoscopicdiscectomy
Anthony Yeung
SelectiveEndoscopicDiscectomy™,foraminal decompression,andnerveablationfor discogenicandaxialpain [pg 28-29]
Anthony Yeung
SyMPoSIUM 6 KEDAH ROOM
MIS-Instrumentation 1Chairpersons: Saw Lim Beng / Mazwar Sofiyan
Advancesofminimalinvasivespine stabilization [pg 29]
Koji Sato
Thetipsofminimallyinvasivespine stabilizationinlumbarspine [pg 30]
Koji Sato
Indirectdecompressioninspinalstenosis
[pg 31]
Tan Chor ngee
Ashortclinicaluseofcorticalscrewsfor lumbarspinefixation [pg 32]
Shankar Acharya
0930–1000 Tea
1000–1100 SAbAH ROOM beST FRee PAPeR PReSenTATIonS 1[pg 38 – pg 43]
Chairpersons: K Paramaeshwaran / Saw Lim Beng
KEDAH ROOM
FRee PAPeRS 2 [pg 44 – pg 49]
Chairpersons: Chong Chee Seang / Zairul Anuar
1000–1010 Minimallyinvasivemulti-levelposteriorlumbarinterbodyfusionusingarimmedheadtypepercutaneoustranspedicularscrew fixationsystem [pg 39] Hyeun Sung Kim
Accuracyandsafetyofflouroscopicguidedpercutaneouspediclescrewsinthoracicspine:Areviewof1120thoracicpediclescrews [pg 45] Chee Kidd Chiu
1010–1020 Confocallaserendomicroscopy:Ageneral descriptionofanewtechniqueforperformingrealtimeopticalbiopsiesinspinaltumorsurgery [pg 40] Cleopatra Charalampaki
Treatmentofdegenerativediscdiseasewithallogeneicmesenchymalstemcells [pg 46]
Ali noor M
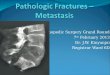
1020–1030 Minimallyinvasivespinesurgeryfor managementofspinalmetastasiswith progressiveneurologicaldeficits [pg 41]
Abrar Ahmed
Earlyexperiencewithendoscopicspinesurgery(Destandau’stechnique) [pg 47]
Arvind Malhotra
Day 2 – 21Day 2 – 21ST ST MARCH 2014 (FRiDAY)MARCH 2014 (FRiDAY)

13page
DAILY PRoGRAMMeDAILY PRoGRAMMe
Day 2 – 21Day 2 – 21ST ST MARCH 2014 (FRiDAY)MARCH 2014 (FRiDAY) [conT’D] [conT’D]
1030–1040 Minimalinvasivestabilizationofthedegenerativelumbarspine[pg 42]
Ardian Hana
Reductionofmoderatetohighgradespondylolisthesisaftercircumferentialreleasingtechniqueunderthemini-openPosteriorLumbarInterbodyFusion(PLIF)[pg 48]
Hyeun Sung Kim
1040–1050 Accuracyandsafetyoffluoroscopicguided percutaneouspediclescrewsinlumbarand sacralspine:Areviewof880screws[pg 43]
Chee Kidd Chiu
ConfocalLaserEndomicroscopic(CLE)characterizationanddifferentiationofspinalmetastasis [pg 49]
Cleopatra Charalampaki
1100–1200 SyMPoSIUM 7 SAbAH ROOM
osteoporosis & MISSChairpersons: Fazir Mohamad / Zamzuri Zakaria
Vertebralbodyaugmentationforosteoporotic compressionfractureusingexpandablepillarPo-Quang Chen
Vesselplastyandchallengesinosteoporoticspine[pg 33]
Aloysius Bambang Darwono
Minimalinvasivesurgery:Experiencein Indonesia[pg 34]
Luthfi Gatam
Vertebroplastyandkyphoplasty-Whatwehavelearned?K S Sivananthan
SyMPoSIUM 8 KEDAH ROOM
MIS-Instrumentation 2Chairpersons: Ahmad Sobri / Mohd Imran
IndicationandsafetyofMIStusing percutaneouspediclescrews[pg 35]
Kwan Mun Keong
MISinspinaldeformitysurgery[pg 36]
Arvind Jayaswal
Minimallyinvasivesurgeryintuberculous infectionofthespine[pg 37]
Arvind Jayaswal
MISSinsacro-pelvicfixationGabriel Liu
1200–1240 Lunch SaTeLL I Te SympoSIum [Pfizer(Malaysia)SdnBhd] SAbAH ROOM
Chairperson: Abdul Malik Mohamed Hussein Spinalinjuries&neuropathiesOzlan Izma Kamil
1240–1430 Lunch / F r iday Prayers
1430–1530 SyMPoSIUM 9 SAbAH ROOM
debate on Controversies in black disc (Case discussion)Chairpersons: Lim Heng Hing / Wong Chung Chek
Anthony Yeung
Abdul Wahab Ghani
Shrinivas M Rohidas
Shankar Acharya
1530–1630 FoRUM on MInIMAL InVASIVe SPIne (MIS) PRoCedUReS SAbAH ROOM
Chairperson: Abdul Malik Mohamed Hussein
how I Started and My MotivationPanelists: Jean Destandau / Anthony Yeung / Shankar Acharya
1630–1700 Tea
1700–1800 WeSS AGM WeSS AGM KEDAH ROOM

14page
Post-conGRess WoRKsHoPsPost-conGRess WoRKsHoPs
Day 3 – 22Day 3 – 22nD nD MARCH 2014 (SATURDAY)MARCH 2014 (SATURDAY)
MAnAGeMenT oF LUMbAR SPIne dISeASeS: LIVe deMonSTRATIon & CAdAVeRIC InTeRVenTIonAL WoRKShoP
(In conjunction with the International Minimally Invasive Spine (MIS) Congress Kuala Lumpur 2014)
Coordinator : Muralitharan Perumal
Committee : Lim Heng Hing
Sabarul Alfian b Mokhtar
nurul Azwa Mohd noor
Facilitators : Anthony Yeung (uSA)
Jean Destandau (France)
Peter Salgado (Spain)
0830–1700Organised by : Malaysian Society of Interventional Pain Practitioners (MSIPP)
Malaysia Spine Society (MSS)
Sponsored by : Perintis Medik Sdn Bhd
Sutra Medi-environ Sdn Bhd
Karl Storz endoskope
CAdAVeRIC WoRKShoP LIVe deMo
Session 1
Cadaveric Workshop on disc-Fx® for discectomy, nucleus Ablation and Thermal Annulus Modulation and for Facet Joint denervation
Session 1 (0900–1200)
endoscopic Spine Live SurgeryDemonstrator : Jean Destandau
Location : Advanced Surgical Skills Centre (ASSC), OT, universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur
Case1:LumbarPID
Case2:CervicalPID
Demonstrator : Anthony Yeung
Location : Advanced Surgical Skills Centre (ASSC), universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur
0830–0900 PresentationonsurgicaltipsforDisc-Fx®procedure
0900–0915 Q&A/Casediscussion
0915–1215 Hands-oninterventionalprocedures
1215–1300 Lunch Lunch
Session 2 Session 2 (1400–1700)
epiduroscopy & Adhesiolysis Live SurgeryDemonstrator : Peter Salgado
Location :
OT, universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur
1300–1330 PresentationonsurgicaltipsforDisc-Fx®procedure
1330–1345 Q&A/Casediscussion
1345–1645 Hands-oninterventionalprocedures
• Breakfast and tea will be made available.

15page
conGRess InFoRMAtIonconGRess InFoRMAtIon
CONGRESS VENUEShAnGRI-LA hoTeL KUALA LUMPUR11JalanSultanIsmail,50250KualaLumpur,MalaysiaTeLTeL(603)20268488FAxFAx(603)20321245
REGISTRATIONTheregistrationhoursare: 20thMarch2014(Thursday) 0700to1800hrs 21stMarch2014(Friday) 0730to1700hrs
CONGRESS DINNERTheCongressDinnerwillbeheldon20thMarch2014(Thursday),at1930hrs,atLamanWau,KompleksKraf,KualaLumpur.PleasebeattheLowerLobby,Shangri-LaHotel,KualaLumpur,asthebuswillleaveat1900hrs.
IDENTITY BADGESDelegatesarekindlyrequestedtowearidentitybadgesduringallsessionsandfunctions.
ENTITLEMENTSRegistereddelegateswillbeentitledtothefollowing:•Admissiontothescientificsessions,satellitesymposiaandtradeexhibition•Conferencebagandmaterials•CongressDinner•Lunches&Coffee/Tea
SPEAKERS AND PRESENTERSAllspeakersandpresentersarerequestedtocheckintotheSpeakerReadyRoomatleasttwohourspriortotheirpresentation.Therewillbehelpersondutytoassistwithyourrequirementsregardingyourpresentation.TheSpeakerReadyRoomislocatedattheSabahAnteRoom,Shangri-LaHotel,andtheoperatinghoursare: 20thMarch2014(Thursday) 0700to1700hrs 21stMarch2014(Friday) 0730to1600hrsAllpresentationswillbedeletedfromtheconferencecomputersafterthepresentationareover.
POSTERSPosterswillbedisplayedatBallroomFoyer.TheOrganisingCommitteebearsnoresponsibilityforthesafekeepingofposters.Anypostersnotcollectedbythecloseofthepostersessionwillbediscarded.
PHOTOGRAPHY & VIDEOTAPING POLICIESNophotographyorvideotapingofthepresentationsispermittedduringthescientificsessions.
MOBILE PHONEFortheconvenienceofalldelegates,pleaseensurethatyourmobilephoneissilencedduringtheconferencesessions.
DISCLAIMERWhilsteveryattemptwouldbemadetoensurethatallaspectsoftheConventionasmentionedinthispublicationwilltakeplaceasscheduled,
theOrganisingCommitteereservestherighttomakelastminutechangesshouldtheneedarises.

16page
FLooR PLAn & tRADe exHIBItIonFLooR PLAn & tRADe exHIBItIon
1 2
3 4
5 13
7 8
15 16
17 18 21
19 20 23
24 26
27
SABAH
KEDAH SELANGOR PERAK
PERLIS
CAR PARK
RESTROOM
DisplayTable
LOADING BAY
RESTROOM
CAR PARK
LIFT LOBBY
Recept ion
SURAU
STAGE
SABAHANTEROOM
BoardRoom A
BoardRoom B
BusinessCentre
BusinessSuite A
BusinessSuite B
BusinessSuite C
SARAWAK
Conference Hall
HospitalitySuite
(NovamedikaSdn Bhd)
Secretariat
Booth noBooth no companycompany1 EliLilly(M)SdnBhd2 BestContact(M)SdnBhd3 SutraMedi-EnvironSdnBhd4 MerckSharp&Dohme5 StrykerCorporation(M)SdnBhd7 Humedical(M)SdnBhd8 CarlZeissSdnBhd13 PerintisMedikSdnBhd15 TransmedicHealthcareSdnBhd16 IDSMedicalSystems(M)SdnBhd17 UMMI surgical18 MedtronicInternationalLtd19 SoringGmbH20 BBraunMedicalSupplies21 SiemensMalaysiaSdnBhd23 AntahSriRadinSdnBhd24 Johnson&JohnsonSdnBhd26 JalinanSejagatSdnBhd27 MundipharmaPharmaceuticalsSdnBhd
DisplayTable ResearchBooksAsiaPteLtd

17page
AcKnoWLeDGeMentsAcKnoWLeDGeMents
TheOrganisingCommitteeoftheInternationalMinimallyInvasiveSpine(MIS)Congress2014recordsitsdeepappreciationtothefollowingfortheirsupportandcontributions.
JalinanSejagatSdnBhd
Pfizer(Malaysia)SdnBhd
MedtronicInternationalLtd
PerintisMedikSdnBhd
StrykerCorporation(M)SdnBhd
AbexMedicalSystemSdnBhd
AntahSriRadinSdnBhd
BBraunMedicalSupplies
BestContact(M)SdnBhd
CarlZeissSdnBhd
EliLilly(M)SdnBhd
Humedical(M)SdnBhd
IDSMedicalSystems(M)SdnBhd
Johnson&JohnsonSdnBhd
MerckSharp&Dohme
MundipharmaPharmaceuticalsSdnBhd
NovamedikaSdnBhd
SiemensMalaysiaSdnBhd
SoringGmbH
SutraMedi-EnvironSdnBhd
TransmedicHealthcareSdnBhd
UMMI surgical
AstraZenecaSdnBhd
ResearchBooksAsiaPteLtd

18page
Diagnosis anD ManageMent of PriMary anD seconDary Myofascial Pain synDroMe in Back Pain
Pradit PrateepvanichMedical staff of Rehabilitation Medicine Department, Siriraj Hospital, Mahidol University, Thailand
Myofascial Pain Syndrome (MPS) defined as regional pain originated from trigger point is a common chronic pain problem in clinical practice. Identification of trigger point by manual palpation is fundamental for the diagnosis. Overlook in diagnosis of MPS is still a common phenomenon regarding to both pain and trigger point examination is non-specific symptom and sign respected. The pathophysiology of MPS is multifactor and overload principle of the muscle is one of the well accepted. This is why postural muscle particularly neck and back extensor muscle common to harbor myofascial trigger point. Furthermore some trigger points can present clinical picture closely to surgical condition for instance trigger point of scalene mimics thoracic outlet syndrome or cervical radiculopathy, quadratus lumborum trigger point similar to lumbar disc herniation, gluteus and piriformis trigger point usually produces pseudo-sciatica. This may be the reason why MPS is one of the common causes of failed back surgery. In general the treatment of MPS has two steps. First step is trigger point inactivation or eradication. As circulation at the trigger point is poor so systemic treatment such as oral medication usually loss of efficacy. Local treatment for example stretching, massage, acupuncture, trigger point injection found relatively more benefit. Second step is corrected perpetuating factor in case of secondary MPS as many causes of low back pain either active spondylosis, disc herniation, scoliosis can induce muscle spasm and consequence become trigger point in some. Treating the primary causes may convert the active trigger point to latent one or may not as trigger point is a self sustained muscle contraction in nature. In the later circumstance we need to treat both primary causes including eradicate the secondary MPS.
Discogenic Pain: is there any solution?Nizar A J
Pain Management Unit, Hospital Universiti Sains Malaysia, Kubang Kerian, Kelantan, Malaysia
Degeneration and disruption of the intervertebral disc can be the source of severe low back pain(LBP) and the associated physical dysfunction. IDET is a minimally invasive treatment option in the continuum of care between conservative nonoperative management and spinal surgery.To date, the evidence is fair for IDET and poor for discTRODE. Systemic review has shown that IDET produced 60-80% success rate in term of reduction in pain score and improvement in functional score. Alternatively, Pulse Radiofrequency(PRF) also appears to be effective, safe, minimally invasive treatment option to IDET in patients with chronic discogenic LBP. Recently, intradiscal Methyline Blue (MB) has created a phenomena as injection of this dye had shown to be effective for the treatment for discogenic back pain. Though its evidenced for only a short-term and may lose its effectiveness for long-term.
Based on the current researches trend, multimodal pain intervention approaches is the probably the way ahead for the best minimal invasive treatment for discogenic LBP.
SympoSium 1Invasive Pain Management in Chronic Back Pain: Between Evidence-Based and Current Practice
SympoSium 1Invasive Pain Management in Chronic Back Pain: Between Evidence-Based and Current Practice

19page
SympoSium 2Image-Guided Spine Intervention
SympoSium 2Image-Guided Spine Intervention
raDiofrequency neurolysis: Who really Benefits?Abdul Wahab Ghani
Ampang Puteri Specialist Hospital, Ampang, Selangor, Malaysia
The presentation will introduce the basic physic of RF lesioning and pulsing. The application of RFA/PRF in the management of spinal pain and other orthopaedic pain syndrome will be discussed. Techniques of facet RFA, discogenic pain treatment, SIJ RFA and Symplicity lesioning and PRF of Ganglion Impar etc will also be covered.
ultrasounD-guiDeD neck anD Back Pain theraPy: Better oPtionChoong Leong Tong
Rafflesia Medical Centre, Kota Kinabalu, Sabah, Malaysia
Imaging guided pararadicular and facet joint injections of the spine are to date mainly performed under CT or fluoroscopic guidance.
From the year 2006 onwards there has been reports exploring the use of Ultrasound imaging to guide pain blocks.
Reports demonstrate the feasibility in performing stellate ganglion block, third occipital nerve block, cervical and lumbar facet joint injections, lumbar medial branch block and periradicular injection.
The advantages of ultrasonography over fluoroscopy include lack of radiation exposure to both the patient (especially with repeated procedures) and the operator and real-time visualization of soft tissues (nerves, muscles, vessels, etc), visualization of needle tip advancement relevant to surrounding structures, and visualization of local anaesthetic spread.
An important consideration is that all cervical injection therapies can be technically challenging, as accidental puncture of paraspinal vessels may lead to severe and irreversible spinal complications. This is particularly relevant for cervical injections performed under fluoroscopic control, where the needle placement is more or less a blind flight until contrast agent is administered. Following current recommendations for cervical spinal injections, the application of contrast agent under real-time digital subtraction fluoroscopy should thus be performed to reduce the risk of unintentional injection in such paraspinal radicular vessels.
US-guided facet joint instillations can now be performed very efficiently under “bed-side” conditions, in outpatients setting. This saves time and resources, as US is comparatively inexpensive and broadly available, and does not imply any therapeutic compromises for the patient, as accuracy is sufficient for the purpose described.

20page
sPinal corD stiMulation in chronic Back PainToh Charng Jeng
Universiti Kebangsaan Malaysia, Bangi, Selangor, Malaysia
Chronic pain is defined as pain persisting beyond a period of normal tissue healing, and/or experienced every day for 3 months or more. Chronic pain has an enormous impact on our society. It is not only interfering with the physical function but also affecting the psychosocial well being of the patients. Chronic back pain can sometimes be very stubborn to medical therapy and interventional pain procedure or the therapies are unable to reduce the pain sufficient enough for the patient to have a productive life style. Therefore, spinal cord stimulation therapy can be the effective option for treating this group of patients. Spinal cord stimulation (SCS) is a technology using electrical neuromodulation in which one or more electrodes are placed in the epidural space of the spine. SCS therapy has been used to treat chronic pain for more than 40 years ago and continues to improve to give better pain control. The mechanism of action is still not fully understood yet, but the widely accepted theory is by “Melzac and Wall’s gate theory” in 1965. The success rate of the therapy is not consistent in all the centers and believed to be related to patients’ selection criteria. As we understand that pain sensation is not only transmitted to sensory cortex but also to the mood centre of the brain, and hence, the chronic back pain patient is not only suffering from pain sensation but also emotional disturbance. Therefore, I believe the outcome of the SCS therapy can further improve by using “biopsychosocial” approach in managing chronic back pain patients. Moreover, many studies have proved the effectiveness of this approach. Many studies has demonstrated that the mood disorder especially depression is closely related to the failure of SCS therapy; therefore strict patients selection and multidisciplinary team approach is the key to success in this therapy. SCS is not only able to improve the quality of life of chronic back pain patient. Furthermore, many studies have proved its cost-effectiveness as well. Lastly, I hope we can work together to provide the best treatment options for chronic back pain patients.
SympoSium 2Image-Guided Spine Intervention

21page
SympoSium 3Endoscopic Spine Surgery 1
learning curve in enDoscoPic sPine surgery: hoW not to stoP Doing
Mohinder KaushalTrinity Hospital and Medical Research Institute, Swastik Vihar, Zirakpur, Mohali, Punjab, India
IntroductIon
Compared with conventional microsurgical techniques, Endoscopic Discectomy and decompressions by Destandau’s Endospine syatem is a more minimally invasive technique for the surgical treatment of lumbar disc herniations and Spinal canal decompressions in canal stenosis. Its efficacy and safety have been confirmed by numerous studies. However, a steep learning curve with the use of such a complex technique is a major concern for the initial adoption of this technique. Many surgeons after initial enthusiasm give up techniques citing difficulty in mastering steep learning curve. Many studies have not been reported about how to shorten learning curve in this technique.
objectIve
To evaluate the learning curve of Destandau’s endospine system technique for the surgical treatment of lumbar disc herniation. Methods: In a series of 1000 patients operated by Author by this technique from November 2002 to November 2013 it was found that difficulty in triangulation, hand eye coordination, inadequate exposure to these techniques during residency, failure to practice on models and cadavers were main factors which led many surgeons to leave these techniques half way through. Author will discuss in his presentation how to shorten learning curve in these techniques.
results
In authors personal experience minimum of 30 patients were required to develop hand eye coordination and triangulation to overcome steep learning curve.
conclusIons
Excellent clinical and minimally invasive outcomes can be obtained in the surgical treatment of lumbar disc herniation and canal decompressions by Destandau’s endospine system. However, attention must be paid to certain details to minimize steep learning curve. Learning curve in these techniques can be minimized by attending workshops, cadaveric courses and working closely with experts and suitable patient selection can help shorten the learning curve and decrease the complications.
Key words
Endoscope, Learning curve, Endospine, Endoscopic laminotomy, radiculopathy

22page
enDoscoPic / MicroscoPic & interlaMinar / transforaMinal: My choice
Shrinivas M RohidasDr Rohidas‘s Centre for Minimally Invasive Spine & Neurosurgery Prakruti Clinic, Kolhapur, India
Almost all significant technical advances are initially met with skepticism, if not direct active resistance. This is true for microscopic, endoscopic techniques with various approaches.
Comparison of outcomes lumbar surgeries of different series is difficult because of different outcome rating scales, different approaches, different selection criteria, and outcomes interpretation. Hence we will discuss about the approach related issues for spine surgeon, not the comparison of results and complications.
Microscopic and endoscopic approaches are not foreign to each other, as both follows, a laminotomy, medial facetectomy, foraminotomy, nerve root decompression, retraction, and discectomy. For discectomy the technique remains same. But for nerve root compression by spinal stenosis with disc herniation, severe canal stenosis due to bony hypertrophy as well as soft tissue thickening endoscopic magnification, illumination in narrow corridors in side the spinal canal makes surgeons task easy. Endoscopes mobility, tubular retractor providing soft retraction in narrow corridors helps surgeon to target narrow corridors.
The concept of percutaneous endoscopic discectomy (PELD), has been evolving rapidly over past few years. However, although still in evolution, this technique has not been embraced by most of spine surgeons, mentioning its narrow indications of soft unmigrated disc herniations and absence of spinal stenosis. However with advancement in endoscope, camera, development of sturdy, small caliber surgical instruments coupled with application of laser technology this technique has really blossomed. Relative contraindications to this approach are disc protrusion without radiculopathy, severe canal stenosis, advanced lateral recess stenosis, radiculopathy due to spinal stenosis without disc herniation, and cauda equina. High level of iliac crest almost prevents the disc access at L5/S1 through transforaminal approach.
Endoscopic surgery through interlaminar approach is not foreign to surgeon as it is routine open or microscopic approach. There is a steep learning curve due to mobile system which is advantage once the steep learning curve has overcome. Same simple system can be used for lumbar disc herniation of any kind, stenosis of any grade, even in cervical anterior & posterior region with occasional thoracic herniations also.
As I am using this approach since 2002, I would like to share my results of 932 cases out of 990 lumbar endoscopic surgeries performed. In my set up I believe my choice of interlaminar approach is the best considering the social structure and other factors such as financial constraints and the stage at which our patients opt surgical treatment
My preference of interlaminar rather than transforaminal approach related more towards the types of pathologies of the spine that are seen my practice. Severe canal stenosis and huge protrusion discs are frequently seen. Beside that almost all the procedures can be done posteriorly through interlaminar. The minimal exposure of radiation and minimal inventory needed for the usage of the interlaminar system that I used are the added advantages. In fact there is no disposable items needed except for gauzes, patties, gelfoam and sutures.
Out of 932 cases, 596 were male and 336 female with age range from 14-82 yrs. 922 cases were done under general anesthesia, 2 under spinal anesthesia cases and 8 using local anesthesia. The commonest levels were L4/5, L5/S1 and L4/5 with L5/S1. Out of 423 cases of L4/5 level, in 114 discectomy was performed, in 274 cases discectomy with canal decompression was performed and in 35 cases only canal decompression without discectomy was performed. At L5/S1, out of 221 cases, discectomy was performed in 130 cases, discectomy with canal decompression in 90 cases and in 1 cases only canal decompression without discectomy was done. L4/5 and L5/S1 two levels were approached in 82 cases of which 50 cases a single incision is used
We had 93% excellent results with endoscopic discectomy, discectomy and canal decompression and bilateral canal decompression with unilateral approach. We used modified McNab’s criteria for evaluation. Good result in 3%, fair in 2% and poor result in 2% cases.
Why I choose endoscope instead of microscope? Two main reasons: endoscope is eye inside the body and its mobility. No turning of table and no obscuring of vision. My endoscope follow what I want to see and excellent vision can improve the success of surgery and minimize complications.
SympoSium 3Endoscopic Spine Surgery 1

23page
SympoSium 3Endoscopic Spine Surgery 1
enDoscoPic luMBar DiscectoMy: a siMPlifieD aPProach
Paresh Chandra DeyModern Ortho Clinic, Besides Kalinga Stadium, Bhubaneswar, Orissa, India
objectIves
Endoscopic discectomy is an established method for treatment of lumbar disc herniation. We have a series of 400 patients operated for lumbar discectomy by Destandau Endospine System.
MaterIal and Methods
A total of 400 patients suffering from lumbar disc herniations were operated between August 2008 and February 2013. Technique comprised localization of symptomatic level followed by insertion of an endospine system devise through a 15mm to 20mm skin and fascial incision. Endoscopic discectomy is then carried out by Endospine instruments by minimal invasive route. The results were evaluated by macnab’s criteria after a minimum follow up of 12 months and maximum up to 24 months.
results
Based on modified Macnab’s criteria, 96% patients had excellent to good, 3% had fair and 1% had poor results. The complications observed were discitis in two patients and dural tear in one patient and nerve root injury in one patient. 96% patient were able to return to light and sedentary work with an average delay of 18days and normal physical activities after 6 weeks.
conclusIon
Endoscopic Lumbar discectomy provides a safe, effective and minimal access corridor for lumbar discectomy. The technique also allows early post operative mobilization and faster return to work.
Key words
Endospine, Lumbar discectomy, laminotomy, radiculopathy.

24page
enDoscoPic luMBar DecoMPression: BetWeen PrinciPles anD Practices
Abdul Halim YusofSpine and Spinal Cord Rehabilitation Unit, Department of Orthopaedic
School of Medical Sciences Health Campus, Universiti Sains Malaysia, Kubang Kerian, Kelantan, Malaysia
bacKground
Surgical decompression is a standard and established procedure for spinal stenosis.Issues with the procedure are related to its approach and balancing between adequate decompression and preserving stability. Certain ‘facts’ based on biomechanical studies influenced the surgical procedures were probably not applied to the endoscopic procedures .
objectIves
1. To compare the early results of endoscopic decompression with the standard open technique
2. To identify cases that need no undergo fusion
3. To identify teething problems in early phase experience
Methods
From 2009 to 2013 174 consecutive patients were operated using Destandau translaminar technique of these. 9 cases were revision cases of the same levels.We use Karl Storz endoscopic system with a 4 mm HOPKINS® 00- telescope and 9mm working channel of ENDOSPINE® working insert The indications were predominantly severe claudication and radicular pain.They were undergone unilateral laminotomy and bilateral decompression.Mobilization as soon as tolerable
results
Total stenosis PID
2008 3 0 3
2009 20 12 8
2010 47 32 15
2011 71 57 14
2012 60 44 16
2013 39 29 10
The age ranged from 37 to 87 years (mean 58 y).
• Thedurationofsymptomsrangedfrom5monthstomorethan5yearsThewalkingtimepossibleaveragedlessthan20 minutes
• Early resultswereverypromisingwithaveragehospital stayof threedays,less than200ccofblood lossandnoinfection.The duration of surgery is about average of 1.5-2 hours per level and with three levels it took between 3.5-4 hours.
• Csaeswithspondylolisthesisorscoliosiswerenotcontraindicationsbutonepatientwithgrade2andhavemild-to-moderate back pain need subsequent fusion surgery .
• 2wereobese(120kg)weredonesuccessfullythroughsame23mmincision.
• PerioperativeComplicationsasintable2
SympoSium 4Endoscopic Spine Surgery 2

25page
Complication No of cases
1 Dural Tear 20
2 “Excess Bleeding” 4
3 Wrong Level 3
4 Transient new neurology 8
5 Spinal Headache 3
6 Worsening neurology 3
7 No improvement 2
8 Inadequate decompression 7
Advantages of endoscopic decompression over traditional open surgery other MISS
• Multiplelevelcanaldecompressionpossiblewithouttheneedforfusion
• Optimaldecompressionforbothsidesthroughunilateralapproachandstabilityismaintained
• Revisiondecompressionatthesamelevelispossible
• Earlyrehabilitation.
• Thefieldofvisioniswideanddirectincomparisontoothermini-invasivetechniques.
• Postoperativeinfectionalmostnil
• Smallsizeofthescarconstitutescosmeticadvantage.
• Minimalradiation:Onlyusedformarkingdisclevel.
• Obviousadvantageinobese&veryobesepatient
conclusIon
Endoscopic translaminar decompression using Destandau technique is effective in achieving adequate decompression and preserving stability with its excellent visual aids and endoscopic system provides early recovery and reduce the needs to do fusion.
Keywords
Endoscopic, spine, lumbar, decompression.

26page
enDoscoPic cervical sPine surgeries – the Basics anD avoiDing coMPlications
Shrinivas M RohidasDr Rohidas‘s Centre for Minimally Invasive Spine & Neurosurgery Prakruti Clinic, Kolhapur India
objectIve
We are using endospine in degenerative lumbar pathologies like disc herniation, radiculopathy due to disc hernia & bony canal & foraminal stenosis since 2002. After going through the initial steep learning curve we started using endospine for posterior foraminotomies & disc removal with canal decompression for cord compression since 2004. Since 2006 we started using Endospine for anterior cervical endoscopic microforaminotomy and cord decompression. We report the technique,s bothe anterior and posterior, indications and techniques to avoid complications.
Methods
Decompression of compressed cervical nerve root is a routine neurosurgical procedure. Most of the time it is achieved through an anterior approach and, also through posterior approach in specific conditions like disc hernia at C7/T1. From 2004 till today we have used posterior approach in 28 patients. Patient’s demographic and clinical presentations, surgical outcome data were recorded. Age of patients ranging from 20 to 70. Endoscopic posterior discectomy was performed in 9 patients. C4/5 level one case, C 5/6 level one case, C7/T1 level two cases, and C 6/7 level one case. Canal decompression for myeloradiculopathy was performed in 19 patients. C3/4 level in two cases, C 3/4/5 decompression in one case, C 5/6/7 was the common level performed in seven cases, C4/5 level in one case, C4/5/6 in four cases, C6/7/T1 in one case, C2/3/4 level in one case, and C3 to C6 and C3 to C7 decompression in one case each. In these 28 cases 8 had neck pain, 8 had motor weakness, radicular pain was in 14 patients, paraesthesia in 10 patients. 5 had motor wasting with 12 patients having myelopathy signs with spasticity. Out of 28, 23 patients had excellent results, 4 had good and 1 had fair results considering modified MacNab criteria. From ----- 2006 till today we used anterior cervical endoscopic approach (Jho’s technique), with Endospine for anterior cervical microforaminotomy, discectomy & cord decompression in 35 cases. Patient’s demographic and clinical presentations, surgical outcome data were recorded. 21 were male and 14 were female patients. Patient’s age ranged from 24 yrs to 65 yrs. There were 16 disc herniations at C5/6, followed by C4/5 in 10 patients, 4 nerve root compression at C6/7 level and 1 patient had C3/4 disc herniation leading to root compression. Out of these 3 had myeloradiculopathy at C4/5 and one each had myeloradiculopathy at C5/6 & C6/7 level. Three patients had two level nerve root compression at C3/4 & C4/5, C4/5 & C5/6, and C5/6 & C6/7. One patient had mass at C6 body and we took biopsy using this approach with endospine. 17 patients had neck pain, 13 had motor weakness, 25 had radicular pain, and 20 had paraesthesia. 5 had myeloradiculopathy with spasticity in LL’s, ataxia, KJ exaggerated, ankle clonus, with BJ and BR jerk inverted, Hoffman’s positive along with finger flexion positive. All the patients had sufficient around 6 months to one year conservative treatment. All underwent MRI of cervical spine with screening of whole spine. Plain xrays of cervical spine in AP, Lateral, in flexion and extension, Rt. and Lt. oblique were used to evaluate instability and bony foraminal compression due to foraminal osteophytes.
results
In posterior endoscopic cervical approach, out of 28, 23 patients had excellent results, 4 had good and 1 had fair results considering modified MacNab criteria. In anterior endoscopic cervical approach, 32 patients had excellent results, with good results in 2 patients, and 1 had fair result. Dural puncture was seen in one patient in each approach. Muscle piece with fibrin glue was used to seal the puncture. In anterior cervical approach 2 patients had Horner’s symdrome and 2 patient had transient recurrent laryngeal nerve paresis which recovered in 2 weeks to 8 weeks period completely. Pseudoaneyrysm of VA was reported in one case in anterior approach. This was a case demonstrated in one of the workshop & not included in the study but for the purpose to know the technique related complication we are mentioning this.
The complications can be reduced by selecting the cases for approach, and by exact knowledge of endoscopic anatomy through small incision. To remove flavum use of through cut punch can be very helpful. In cervical region pulling of flavum can be dangerous in rupturing epidural veins which can bleed profusely. Through cut punch helps in minimizing trauma to veins. Bipolar cautery can be used. Opposite canal decompression in both the approaches can be safely done with help of ultrasonic bone dissectors of various types. It reduces surgeons stress while working in these narrow corridors. Bleeding from vertebral artery in anterior approach should not be tackled with bipolar cautery. Rather we use surgicell packing over vertebral artery venous plexus which helps in reducing oozing from VA.
SympoSium 4Endoscopic Spine Surgery 2

27page
SympoSium 4Endoscopic Spine Surgery 2
conclusIon
Endospine in cervical However basically region can be used for both anterior as well as posterior approaches. Endospine has a very steep learning curve. Posterior approach is ideal for C7/T1 approach as to approach it anteriorly may be difficult. Posterior approach is better for multilevel cervical cord compression as up to three level can be approached through single incision. Endospine with Jho’s approach is a better technique for disc preserving functional spine surgery. Cord decompression also can be achieved with anterior approach. Use of endospine with posterior and anterior, Jho’s approach should be by experienced surgeon to avoid complications like dural injury.
Key words
Cervical disc herniation, cervical foraminotomy, Jho’s technique, endospine, intervetebral disc, radiculopathy.
enDoscoPic Disc surgery: a future stanDarD PracticeMohinder Kaushal
Trinity Hospital and Medical Research Institute, Swastik Vihar, Zirakpur, Mohali, Punjab, India
objectIve
Surgical treatment of Lumbar disc prolapse in most centres is still open discectomy facilitated by microscope or loupe magnification and illumination. This review describes Endoscopic discectomy by posterior interlaminar approach and transforaminal endoscopic spine system by HD-video technology.
Methods
The method of Interlaminar and transforaminal endoscopic discectomy is described and an electronic literature search performed to identify papers reporting clinical outcomes. International data were translated where necessary and proceedings’ abstracts included. In addition, papers held by the authors and colleagues in personal libraries were carefully cross-referenced to the obtained database.
results
Analysis of the data supports the use of a Interlaminar approach and transforaminal endoscopic approach to the lumbar intervertebral disc and suggests that outcomes following surgery are at least equivalent to those following microdiscectomy. Significant cost-savings in terms of inpatient stay may be generated. Main drawback of transforaminal endoscopic technique observed was its limited indications in various type of disc herniations and stenosis.
conclusIon
Based on current evidence there are good arguments supporting a more widespread adoption of interlaminar and transforaminal endoscopic surgery for the treatment of lumbar disc. However careful patient selection and application of correct endoscopic spinal technique is important for successful clinical outcome.
28page
SympoSium 5Endoscopic Spine Surgery 3
selective enDoscoPic DiscectoMy™, foraMinal DecoMPression, anD nerve aBlation for
Discogenic anD axial PainAnthony T Yeung
Desert Institute for Spine Care, Phoenix, Arizona University of New Mexico School of Medicine, Albuquerque, New Mexico, USA
IntroductIon
Non-operative therapeutic regimens often fail to achieve satisfactory and effective relief inpatients with disabling chronic discogenic and axial back pain. State-of-the-art Transforaminal Endoscopic Minimally Invasive surgical options range from intradiscal electrothermal therapy, disc and foraminal decompression, to dorsal rhizotomy, and culminating in lumbar fusion. MIS endoscopic techniques in the literature feature visualized intradiscal procedures that incorporate selective endoscopic discectomy™ with thermal annuloplasty for discogenic back pain, then endoscopic medial branch, lateral branch, and dorsal ramus rhizotomy for axial back pain.
study desIgn/settIng
Endoscopic techniques utilized by ATY as part of an endoscopic spine system developed with Richard Wolf GmbH is reviewed. A 1997 IRB approved study of endoscopic spine surgery for the spectrum of painful degenerative conditions of the lumbar spine evolved, and carried on to the present time. The study first determined that laser assisted and radiofrequency thermal modulation can provide pain relief from discogenic lumbar pain. The clinical outcome of a retrospective study of 113 consecutive patients with minimal 2 year follow-up was reported in Spine, October 2004. Outcome measurements were by modified MacNab surgeon rating and a patient satisfaction questionnaire. VAS and Oswestry was added in 2001. Patient selection included positive evocative discography for concordant pain, pre-operatively and/or intraoperatively, correlated with an abnormal discogram pattern. At surgery, chromo-discography with diluted indigo carmine dye stained the degenerative nucleus pulposus blue, targeting the blue stained degenerative tissue for endoscopic removal. The annulus was the treated by bipolar radiofrequency guided by endoscopic visualization after disc decompression. Disc material, embedded in the annulus, was removed. A second phase prospective study was initiated in 2006 utilizing the endoscope for visualized thermal ablation of the branches of the Dorsal Ramus. In the process, medial. Intermediate and lateral branches of the dorsal ramus could be visualized. Only the medial branches are targets for thermal ablation in the pain management literature. Foraminal decompression for stenosis was facilitated by instrument development of endoscopic trephines, kerrisons and high speed burrs.
FIndIngs
Endoscopic surgical decompression was discovered to be more effective than fluoroscopically guided IDET and pulsed radiofrequency for axial back pain. The painful discs mostly had inflammatory or granuation tissue associated with annular tears. The degenerative nucleus pulposus is removed mechanically with pituitary rongeus and shavers, then the granulation and inflammatory tissue seen adjacent to the annular tears are thermally modulated by flexible radiofrequency electrodes. The annular defects are endoscopically observed to be altered by radiofrequency treatment. In medial branch, lateral branch and dorsal ramus rhizotomy, The nerves may of may not be consistently visualized, but ablation of the soft tissue at the base of the spinous process is sufficient to bring back pain relief in 90% of patients who get at least 70% improvement from preliminary anesthetic and steroid injections.
results
In the SED with thermal annuloplasty group that included a variety of degenerative discs from early to late stage degenerative disc disease and lumbar spondylosis. Eighty-three patients 83/113 (73.5%) were in the satisfactory outcome group. Thirty patients (26.5%) were determined to have poor results because of only minimal or partial improvement, but additional surgery was required after two years. The specific reasons were as follows: eight patients had subsequent lumbar fusion; seven patients had repeat lumbar endoscopic surgery; and three patients had lumbar laminectomy. Twelve patients in the poor category elected to have no further back surgery and chose to live with their residual pain. Of the eighteen patients who had secondary back surgery, ten reported improvement after the subsequent operation. The satisfied group of patients would select the lumbar endoscopic surgery again in the future given the knowledge gained from their endoscopic experience was 91%. No patient was worse.

29page
In the endoscopic medial branch and dorsal ramus Rhizotomy study, 48/50 had positive benefit from the rhizotomy at least equal to but mostly better than the pain relief they obtained with their medial branch facet injection. There was 100% patient satisfaction. 10/50 has regressed but none were worse. Some patients claimed to have 100% relief of their pre-operative back pain. Others also reported relief of sciatica. Pre- and post op Vas and Oswestry scores were tabulated, demonstrating significant improvement. No patient was worse.
After the preliminary study, better patient stratification and selection by their response to diagnostic and therapeutic transforaminal steroid block and medial branch blocks brought the Good/ excellent results to over 90%.
conclusIon
The treatment rationale for selective endoscopic discectomy and thermal annuloplasty is superior to disc decompression alone. The inclusion of endoscopic discectomy removes a source of chemical sciatica, the deteriorating nucleus, but also removes the nuclear tissue embedded in the annular tear. Inflammatory tissue is thermally ablated under endoscopic visualization. Case examples will illustrate the patho-anatomy and its response to endoscopic decompression, ablation and irrigation. Thermal ablation of branches of the dorsal ramus is also effective for alleviating low back pain, and can be combined with endoscopic decompression. The results appear to be at least equivalent to traditional surgical techniques but patient satisfaction is higher and surgical morbidity is less.
aDvances of MiniMally invasive sPine staBilizationKoji Sato
Department of Orthopedic and Spine Surgery, Nagoya Daini Red Cross Hospital, Nagoya, Japan
The MISt is a trend. Of course, MISt is not a special indication for all spine disease. MIS-PLIF/TLIF is popular procedure for lumbar spinal canal stenosis. Recently, we can do MIS-long fixation for metastasis spine tumor, trauma, mild infection, and so on. Mild injury for the tissue is in relation to short recovery daily life of patient. The advantage of MISt is low blood loss, short operation time, short recovery time, a little infection rate, small fee for treatment, etc. The disadvantage of MISt is severe learning curve, irradiation exposure time, less volume of bone graft, extradural hematoma, and so on. It may be good for the adjacent disease. I did MISt technique since 2005. I talk about the advantage of MISt from our data.
SympoSium 6MIS-Instrumentation 1

30page
the tiPs of MiniMally invasive sPine staBilization in luMBar sPine
Koji SatoDepartment of Orthopedic and Spine Surgery, Nagoya Daini Red Cross Hospital, Nagoya, Japan
The MISt is a trend. We need the time to get MISt skill. This procedure is a different method of convention approach. Percutaneous pedicle screw (PPS) is more oblique trajectory through the longismus muscle. We use spine navigation system for the right place of implant, to get the orientation, and for the education. MEP spinal monitoring is safety goods for the keyhole surgery. There are some ideas for long fixation, MIS-Galveston, 1st sacral PPS, etc. We have some training program for these procedures. These are pig animal laboratory, cadaver workshop, and operation visitation program. We are welcome to visit our hospital.
SympoSium 6MIS-Instrumentation 1

31page
SympoSium 6MIS-Instrumentation 1
inDirect DecoMPression in sPinal stenosisTan Chor Ngee
Department of Orthopaedics & Traumatology, Hospital Putrajaya, Putrajaya, Malaysia
Conventional spinal decompression often required removal of the bony structures like the lamina and facet joint. Intraoperative examination of the various neural tissues is necessary in order to make a satisfactory decompression. However the morbidity of the muscle retraction and bony together with ligamentous resection needed to gain access to the disc space is a distinct disadvantage. The posterior approach to the disc space also requires direct retraction of the cauda equina and hence the risk for nerve root injury or dural tear.
The original abdominal approach to the anterior column access obviates some of the approach related disadvantages of posterior approaches. However it is not without its own challenges.
The 1st direct lateral approach to the lumbar spinal pathologies was presented in Brazil in 2001. Over the years, there were improvement made on the types of retractors, neuromonitoring system and its instrumentation.
Indirect decompression by direct lateral, transpsoas and retroperitoneal approach to the lumbar disc space is achieved by “internal discectomy” and placement of a large interbody cage on the anterior column of the spine. The result of the restoration of disc height is thought to induce a degree of ligamentotaxis, especially the posterior ligaments and causing an increase in canal area. If the canal narrowing is due to disc bulge or frank herniation, by increasing the disc height will result in stretching and tightening of the annulus fibers, decreasing the amount of disc bulge and further aiding in indirect decompression.
Foraminal height is restored in a mechanical manner as the disc space is elevated.
In cases of stenosis secondary to spondylolisthesis, fusion with lateral surgery will have some degree of correction of the listhesis which in turn will reduce the patients symptoms. If the radiculopathy is caused by scoliosis, placement of the interbody cage will help to correct the deformity and lead to foraminal decompression.
In this review, we include only single and double levels disease. In between 2011 to end of 2012, we have performed lateral approach surgeries on 62 patients. 34 were female and 28 were male patients. The primary diagnosis for the cases include Grade 1 spondylolisthesis (4), spinal stenosis(6), DDD(5) and HNP(4). Their age ranges from 54 to 76 years old. 20 patients had single level surgery and 42 patients had 2 levels surgery. 57 cases were at L45, 40 cases at L34 and 7 level at L23. No blood transfusion was needed to all the patients. Visual analog score pre operation was 7.8 and 2.5 post operation. The mean pre operation Oswestry Disability index was 55% and post operation was 9.8%. The mean pre operation disc height was 8.2mm and post operation value was 13.5mm. The average corrected height was 5.35mm. Mean value for pre operation intervertibral foraminal height was 18.3mm and post operation mean value was 22.1mm.
Transient left thigh numbness was seen in 32 patients, all had complete recovery after 6-10weeks except in 1 patient.
2 patients had subsidence that resulted in incomplete symptomatic recovery. One of these two patients had fracture of vertebral endplate which was not detected intraoperatively and result in early subsidence. Both had posterior percutaneous pedicle screws fixation.
One patient had post operation infection(psaos abscess) that was initially treated with antibiotic and subsequently had surgical debridement with cages removed and tricortical bone graft insertion.
In this review, we think that lateral direct, transpsoas and retroperitonel approach is an effective and safe option for solving carefully selected spinal pathologies.
32page
a short clinical use of cortical screWs for luMBar sPine fixation
Shankar AcharyaConsultant Orthopaedic & Spine Surgeon, Sir Ganga Ram Hospital Rajinder Nagar, New Delhi, India
IntroductIon
Lumbar pedicle screws have been inserted with the traditional end on technique. But the trajectory required for the approach requires a substantial dissection and blood loss. Use of cortical screws with mediolateral screw insertion is a step forward for placement of screws in a minimally invasive fashion.
MaterIal and Methods
There were a total of 8 cases during the last 18 months with a followup of atleast 9 months. The average age of the patients was 55 years and all were lumbar degenerative cases.
results
The average number of level fixed was 2.5, average blood loss 135ml, average operative time was 3.5 hours. TLIF at one level was done in 5 cases. There were one intraoperative complication of CSF leak related to decompression and not screw placement. There were no postoperative complications like implant failure, screw loosening or TLIF cage back out. The VAS score was average 2.3, 24 hours after the surgery.
conclusIon
The high operative time reflects the early learning curve for this procedure. The current cost of the implants also is a big concern. But the low blood loss and low post-operative pain reflects the minimally invasive nature of the lumbar cortical screws. To conclude lumbar cortical screws are an effective alternative to end on pedicle screws requires further clinical experience.
SympoSium 6MIS-Instrumentation 1

33page
vesselPlasty anD challenges in osteoPorotic sPine Darwono A Bambang
Department of Orthopaedic Surgery, Gading Pluit Hospital, Indonesia Medical Faculty, Tarumanagara University Jakarta, Indonesia
IntroductIon
Vertebroplasty and Kyphoplasty are used to treat stable VCFs in Osteoporotic Spine with a risk of certain cement leakage. Regarding cement leakage the new technique Vesselplasty use a non stretchable PET container to prevent leakage of the injected cement and then left as an implant body expander. Instead of PMMA, the new SrHA cement (osteoinductive and osteoconductive with less 65° C heat production) is to be used. Sr is reported to have a dual effect of action: stimulation of osteoblast differentiation and inhibition of osteoclast formation. The animal study in Hong Kong shows a new bone formation at the interface of SrHA. To treat unstable VCFs combined with multiple stenosis, kyphotic and degenerative de novo scoliosis, the new innovative Vessel-lock system is used. The purpose of this study is to review the theory, surgical techniques, 5 years results using this new technique and compare the effect of SrHA and PMMA cement in osteoporotic spine.
MaterIals and Methods
A non randomized prospective study to treat VCFs using Vesselplasty with PMMA and SrHA cement. This new technique is a percutaneous non fusion technique to restore VCFs., and prevent leakage risk of cement. This system allows the delivery of a non-stretchable Cement Container (CC) into the vertebral body in deflated configuration, then inflated by injecting viscous cement into the CC, and left as an implant body expander. Comparison of the effect of SrHA and PMMA is done using VAS, X-ray and CT-scan: just after treatment, 3 months and 6 months. Vessel-lock system with SrHA is used to treat a complex case (Osteoporotic VCFs, multiple stenosis, kyphotic and degenerative scoliosis) by open surgery.
results
250 cases with a total of 298 VCFs ( VT3 – VL 5 ) have been treated using this new technique, consist of 178 PMMA and 120 SrHA cases. The same excellent result is achieved with PMMA and SrHA just after reatment, also 3 and 6 months afterwards. The difference is recorded at 6 months after treatment: a new bone formation is seen by Ct-scan at the interface of SrHA, while none of PMMA. The 11 preliminary cases of Vessel-lock with SrHA are reported also.
conclussIon
SrHA cement is superior compare to PMMA in the osteoporotic spine. The Vesselplasty is acting as implant body expander. It’s allows the restoration of the vertebral body height, with the advantage in controlling volume of the injected cement, pressure inside CC, and preventing the leakage of cement. The Vessel-Lock with SrHA is used to solve the unstable and complex cases of VCFs.
SympoSium 7Osteoporosis & MISS
34page
SympoSium 7Osteoporosis & MISS
MiniMal invasive surgery: exPerience in inDonesiaLuthfi Gatam
Indonesian Spine Society (ISS) Spine Section, Indonesian Orthopaedic Association-IOA (PABOI)
Orthopaedic and Traumatology Department, Fatmawati General Hospital, Jakarta Timur, Indonesia
Orthopaedic Spine SurgeonSpinal surgery is not without risk. Conventional surgery often requires large exposure. Large exposure results in muscular denervation, intramuscular pressure increment, ischemia, necrosis, and revascularization injury causing to iatrogenic injury. Minimal invasive surgery is a possible panacea for this problem. In Indonesia, we have started minimal invasive surgery since 2000. Various minimal invasive surgeries have been performed, including intra discalelectrothermal therapy, microendoscopic discectomy, video assisted microdiscectomy, percutaneous endoscopic lumbar discectomy, radiofrequency ablation, and minimal invasive spinal stabilization and fusion.
Among 47 patients who had undergoneintra discalelectrothermal therapy, we found that decrease in 12 month visual analog scale was significant for single level (p=0.00) but not multilevel intra discalelectrothermal therapy (p=0.09). We also compared 41 cases of video assisted micro discectomy to 29 cases of microendoscopic discectomy and found that micro endoscopic discectomy leaded to significant 3 month postoperative visual analog scale (p=0.0101), 3 month postoperative functional activity score (p=0.0023), shorter hospital stay (p=0.0149). Compared to conventional spinal stabilization and fusion, minimal invasive stabilization and fusion leaded to lesser blood loss (p=0.037) but similar postoperative oswestry disability index (p=0.072), postoperative visual analog scale (p=0.089), first sitting visual analog scale (p=0.329), first walking visual analog scale (p=0.860), hospital stay (p=0.521), and duration of surgery (p=0.322).
Minimal invasive surgery offers many benefits compared to conventional surgery. It might be a panacea for iatrogenic injury due to excessive exposure.
Keywords
minimal invasive surgery, intra discalelectrothermal therapy, microendoscopic discectomy, video assisted micro discectomy, minimal invasive stabilization and fusion

35page
inDication anD safety of Mist using Percutaneous PeDicle screWs
Kwan Mun KeongDepartment of Orthopaedic Surgery, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia
Pedicle screw has been shown to have superior biomechanical properties as compared to other conventional modes of instrumentations. Various pedicle screw insertion techniques have been recommended. However all of these techniques require an open surgery. Recently a new technique of percutaneous instrumented stabilization of thoracolumbar spine has been introduced. This new system allow multiple levels fixation spanning from thoracic, lumbar and/ or sacral region percutaneously, using the Minimally Invasive Stabilization (MISt) technique.
The absolute indications for percutaneous pedicle screws stabilization are spinal metastases, spinal infection, damage control spine surgery for poly trauma and osteoporotic fracture. The indication for this technique is expanding gradually. With the advent of lateral access fusion surgery, the use of this technique has already been explored as an option to manage difficult cases i.e. degenerative scoliosis. However, the safety of this technique especially in Asian population has to be determined due to the smaller pedicle dimension.
A total of 155 patients, who had undergone posterior stabilization of the thoracolumbar spine using percutaneous pedicle screw technique (MISt) from two spine centers: University Medical Centre, Hamburg-Eppendorf, Germany and University Malaya Medical Centre, Malaysia was recruited into this study. There were 83 consecutive European patients and 72 consecutive Asian patients selected with the mean age of 58.3 ± 16.1 (Europeans: 61.7 ± 15.2, Asians: 54.3 ± 16.3). There were no difference in the gender distribution between Europeans and Asians. Overall, the main etiology was neoplasia. Other etiologies were infections, degeneration, trauma and osteoporotic fractures. CT scan was used to assess the following pedicle perforations; medial, lateral, superior, inferior as well as anterior perforations. Only Grade 2 and 3 medial perforations were considered a critical perforation as these perforations may result in neurological injury.
A total of 1138 screws were evaluated with the average screw perforation rate was 10.6% (Europeans: 10.0%, Asians: 11.3%). Majority 8.5% (97 screws) were only grade 1 perforations with 1.8% (21 screws) with grade 2 perforations and 0.3% (3 screws) with grade 3 perforations. In the European group, the grade 1, grade 2 and grade 3 perforation rates were 7.9% (46 screws), 1.9% (11 screws) and 0.2% (1 screw) respectively. In the Asian patients, grade 1, grade 2 and grade 3 perforation rates were 9.1% (51), 1.8% (10) and 0.4% (2). (Table 1). There is no statistically different between the perforation rates between the 2 groups of patients. The incidence of Medial grade 2 and 3 perforations (Critical Perforation) was very low. In the European group, there was only one grade 2 and one grade 3 perforations whereas in the Asian group there was only one grade 2 perforation. The perforation rate was noted to be highest in T1 (37.5%) followed by T4 (32.0%).
In conclusion, percutaneous pedicle screw stabilization in thoraco-lumbar spine has provided a new option for the management of many spinal pathologies and this technique is safe in the Asian population despite having a smaller pedicle dimension.
table 1: comparison between the perforation rates between the european and the asian patients
european asian total
Number of Percutaneous Pedicle Screws 579 559 1138
Overall Screws Perforation Rate 10.0% (58) 11.3% (63) 10.6% (121)
Grade 1 perforation 7.9% (46) 9.1% (51) 8.5% (97)
Grade 2 perforation 1.9% (11) 1.8% (10) 1.8% (21)
Grade 3 perforation 0.2% (1) 0.4% (2) 0.3% (3)
SympoSium 8MIS-Instrumentation 2

36page
Mis in sPinal DeforMity surgeryArvind Jayaswal
Department of Orthopaedics, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India
IntroductIon
With encouraging results of minimally invasive techniques in spine surgery especially low grade listhesis and trauma etc, various surgeons are spreading their indication to the field of deformity correction. The benefits of less blood loss and less postoperative pain and faster recovery may be extended to patients with spinal deformity using minimally invasive pedicle screw fixation surgery. Isolated case series of incorporation of these techniques using Percutaneous multi level pedicular screw Rod system in adult deformity are reported in the literature but no study is yet reported utilizing it in Adolescent Idiopathic Scoliosis(AIS).
Methods
23 patients with average age of 32.6yrs (16-42yrs) underwent MISS spinal deformity correction at our institute. 5 patients had tuberculosis of the lumbar spine (4 underwent 2 level Percut. Ped.screws + MISS TLIF and one patient had 3 level percut fixations +MISS TLIF), 6 patients had spinal trauma (MISS in stable Burst # with Spanning Percut.ped screws with distraction & transpedicular bone grafting or Vert. augmentation with Kyphoplasty) and 12 patients had scoliosis (11patients with AIS and one with neuromuscular scoliosis). All patients were evaluated for blood loss, operative time, deformity correction and complications. The average followup was 14months (8-20m).
results
The average pre-op segmental kyphosis in the T.B.group was 18.6º(12-28º) which corrected to -6º(-2 to -11º) of lordosis post-operatively, in the trauma group the preoperative kyphosis of 19.4º(15-22º) which corrected to -1º(-5 to +3º) and in the scoliosis group the preoperative cobb’s angle was 62º(58-66º) which corrected to 17º(14-19º) postoperatively. The average blood loss was 500ml (100-700ml) and the operative time varied from 190min to 410min which decreased with each subsequent procedure, signifying the learning curve. No patient had worsening of neurology or surgical site infection, but there were minor intra-operative problems with extender pullout in 2 cases.
conclusIon
Patients with flexible deformity were chosen for these procedures respecting the learning curve. The major advantage observed was in the low blood loss and the operative time reduced with each subsequent procedure. We conclude that minimally invasive surgery is feasible in spinal deformity with modern multilevel Percutaneous pedicle screw-rod systems with results comparable to open surgery with acceptable complications. However, long term follow results are awaited before these procedures can be considered as effective alternatives to open spinal deformity corrective surgeries.
SympoSium 8MIS-Instrumentation 2

37page
SympoSium 8MIS-Instrumentation 2
MiniMally invasive surgery in tuBerculous infection of the sPineArvind Jayaswal
Department of Orthopaedics, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India
IntroductIonTubercular Infection is still prevalent in a large population in the developing countries – specially in the Asia pacific region , Africa etc which are still endemic zones as per the WHO grading. Tubercular spondylitis a major cause of deformity of the spine and neurological deficit affecting all ages. Though majority of patients are managed with antitubercular chemotherapy alone, surgery is required for spinal instability and deteriorating neurology. Anterior and Antero-lateral decompression of the cord are two popular surgical procedures with good time tested results. However, the morbidity associated with open thoracotomy makes surgical anterior decompression to be undertaken with caution. Posterior and posterolateral decompressions which avoid thoracotomy, have gained popularity with advent of good posterior spinal instrumentation. The Minimally Invasive Surgeries aim to further decrease the morbidity associated with each of the open procedures without compromising on the surgical goals. Video Assisted Thoracoscopic Surgery (VATS) has changed this clinical scenario in thoracic spine with decreased morbidity associated with anterior decompressions. Various procedures can be done using VATS to address specific clinical scenario, starting from simple drainage of abscess not responding to chemotherapy, debridement and decompression with grafting for deteriorating neurology and anterior instrumentation using VATS to address spinal instability. VATS decompression can be combined with Percutaneous pedicle screw Stabilization to address spinal instability.
In the Lumbar spine, percutaneous pedicle screw instrumentation can be combined with Transforaminal decompression ( TLIF ) using Minimally Invasive tubular rectractors with Interbody fusion or MINI ALIF with anterior debridement and anterior column support.
These procedures have not been reported extensively in literature and we share our results and outcome of these procedures. 23 patients(13 male,10 female), mean age 38.2yrs with single level Spondylodiscitis(T4-T11)treated with VATS and 15 patients (9males, 6 females) with mean age of 32.5 yr (21- 45yr)who underwent minimally invasive posterior pedicle screw instrumentation were part of the study conducted from Mar 2003 to Dec 2009 at AIIMS. Ten of the patient among fifteen had lumbosacral tuberculosis who underwent two level instrumentation with decompression and TLIF (Medtronic Sextant), while five of the patient underwent multilevel percutaneous posterior fixation with posterolateral decompression with interbody fusion (Medtronic Longitude). The indication of surgery was either progressive neurological deficit or instability. All the patients were evaluated for blood loss, duration of surgery, VAS scores, improvement in kyphosis and fusion status. Improvement in neurology was documented and functional outcome was judged by ODI.
resultsThe mean blood loss in VATS category was 780ml (330-1180ml) and operative time averaged 228min (102-324min) while the mean blood loss was 625 ml (range 350- 800ml) with average duration of surgery of 4hr 15min;255min (180-345min) in percutaneous posterior instrumentation group. The average preoperative VAS scores of 7.5 improved to 3.5 on 14th postoperative day. Similarly the improvement in ODI scores was also significant at the last follow-up in all the patients. The average pre-op kyphosis in VATS group was 38°(22°-58°) which was corrected to 30°(range 22°-42°),while in percutaneous pedicle screw group the pre-operative segmental kyphosis of 48° (26° to 64°) improved to 12°(8°- 16°) at immediate post-operative period and maintained at 13.5° at final follow-up (71.8% correction). Sixteen patients who underwent VATS had definite fusion, six had Grade II and failure of fusion was seen in one, on the other hand patients undergoing percutaneous pedicle system,Grade I(definite)fusion was seen in 53.33 %(n=8), Grade II fusion(probably) in40%(n=6) and GradeIII fusion(probably not) in one patient.
Complications occurred in seven patients who underwent VATS. One patient suffered with pseudarthrosis/doubtful fusion with screw loosening in percutaneous group. Patient responded to IInd line AKT and at the end of one year good fusion was appreciated. No other complication was seen in any of the patients.
conclusIonThe authors have been using Thoracoscopic debridement, decompression and anterior instrumentation for thoracic Spondylodiscitis while Minimally Invasive Percutaneous Pedicle screw system for thoracolumbar and Lumbar tuberculosis. Minimally invasive spine procedures are challenging, require expertise and have a steep learning curve. The time taken for the procedures comes down with every subsequent case. Good fusion rate with encouraging functional results can be obtained in Caries spine with minimally invasive techniques while reducing the approach related morbidity.

38page
BP 1 MINIMALLY INVASIVE MULTI-LEVEL POSTERIOR LUMBAR INTERBODY 39 FUSION USING A RIMMED HEAD TYPE PERCUTANEOUS TRANSPEDICULAR SCREW FIXATION SYSTEM
Hyeun Sung Kim1, Se Jin Jeong1, Hyung Jun Ahn1, Ki Hyun Jeon1, Woo Jin Choi1, Kwan Tae Kim1, Keun Soo Jang2, Seok Won Kim2, Chang Il Ju2, Seung Myung Lee2, Ho Shin2
1Department of Neurosurgery, Hurisarang Spine Hospital, Daejeon City, Republic of Korea 2Department of Neurosurgery, College of Medicine, Chosun University, Gwangju City, Republic of Korea
BP 2 CONFOCAL LASER ENDOMICROSCOPY: A GENERAL DESCRIPTION OF 40 A NEW TECHNIQUE FOR PERFORMING REAL TIME OPTICAL BIOPSIES IN SPINAL TUMOR SURGERY
Cleopatra Charalampaki, Christian Eyth, Mirwais Morgan, Alhadi IgressaHospital Merheim, University of Witten-Herdecke, Cologne, Germany
BP 3 MINIMALLY INVASIVE SPINE SURGERY FOR MANAGEMENT OF SPINAL 41 METASTASIS WITH PROGRESSIVE NEUROLOGICAL DEFICITS
Abrar Ahmed, Sanjoy BiswasApollo Gleneagles Hospitals, Kolkata, West Bengal, India
BP 4 MINIMAL INVASIVE STABILIZATION OF THE DEGENERATIVE LUMBAR SPINE 42Ardian Hana, Christophe Berthold, Vimal Gunness, Guy MatgéNational Neurosurgical Department, Centre Hospitalier de Luxembourg, Luxembourg
BP 5 ACCURACY AND SAFETY OF FLOUROSCOPIC GUIDED PERCUTANEOUS 43 PEDICLE SCREWS IN LUMBAR AND SACRAL SPINE: A REVIEW OF 880 SCREWS
Chee Kidd Chiu1, Mun Keong Kwan1, Chris Yin Wei Chan1, Christian Schaefer3, Nils Hansen-Algenstaedt2
1Department of Orthopaedic Surgery, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia 2OrthoCentrum Hamburg, Parkklinik Manhagen, Germany 3Department of Orthopaedic Surgery, University Medical Centre, Hamburg-Eppendorf, Germany
BEST FREE PAPER PRESENTATIONS 1

39page
BEST FREE pApER pRESENTATioNS 1BP 1
MiniMally invasive Multi-level Posterior luMBar interBoDy fusion using a riMMeD heaD tyPe Percutaneous
transPeDicular screW fixation systeMHyeun Sung Kim1, Se Jin Jeong1, Hyung Jun Ahn1, Ki Hyun Jeon1, Woo Jin Choi1,
Kwan Tae Kim1, Keun Soo Jang2, Seok Won Kim2, Chang Il Ju2, Seung Myung Lee2, Ho Shin2
1Department of Neurosurgery, Hurisarang Spine Hospital, Daejeon City, Republic of Korea 2Department of Neurosurgery, College of Medicine, Chosun University, Gwangju City, Republic of Korea
Minimally invasive percutaneous screw fixation allows for significantly less blood loss and tissue disruption than open surgery. However, there are technical limitations of multi-level posterior pedicle screw fixation performed using the percutaneous technique.
objectIve
To present the outcome of minimally invasive multi-level posterior lumbar interbody fusion (PLIF) using a rimmed head type percutaneous transpedicular screw fixation system with a vertical axis and detachable extender.
Methods
42 patients that had mini-open PLIF using the percutaneous screw fixation system (Apollon system®, Solco medical South Korea) were studied. The clinical outcome was assessed using the visual analog scale (VAS) and Low Back Outcome Score (LBOS). In addition, achievement of radiological fusion, intra-operative blood loss, the postoperative midline surgical scar and procedure related complications were analyzed.
results
The mean age of the patients was 59.1 (range, 23 to 78 years). Two levels were involved in 32 cases and three levels in 10 cases. The mean follow-up period was 25.3 months. The mean LBOS prior to surgery was 34.5, which improved to 49.1 at the final follow up. The mean pain score (VAS) prior to surgery was 7.5, which decreased to 2.9 at the last follow up. The mean estimated blood loss was 238ml (140-350mL) for the two level procedures and 387ml (278-458mL) for three levels. The postoperative midline surgical scar was 6.27cm for two levels and 8.25cm for three level procedures. Complications included two cases of asymptomatic medial penetration of the pedicle border and one case with a deep wound infection. However, there were no signs of neurological deterioration or fusion failure.
conclusIon
Multilevel minimally invasive PLIF could be performed using the rimmed head type percutaneous transpedicular screw fixation system with a vertical axis and detachable screw extender which made rod manipulation easier to perform.
Key words
Minimallyinvasivesurgery•Interbodyfusion•Percutaneousscrewfixation•rimmedheadtype.
40page
confocal laser enDoMicroscoPy: a general DescriPtion of a neW technique for PerforMing real
tiMe oPtical BioPsies in sPinal tuMor surgery Cleopatra Charalampaki, Christian Eyth, Mirwais Morgan, Alhadi Igressa
Hospital Merheim, University of Witten-Herdecke, Cologne, Germany
IntroductIon
Early detection and evaluation of spinal tumors during surgery is crucial for accurate resection. Currently cryosections during surgery are regularly performed. Confocal laser endoscopy (CLE) is a novel technique permitting in vivo histologic imaging with miniaturized endoscopic probes at excellent resolution.
objectIves
To evaluate the use of CLE in vivo diagnosis of different types and models of intraspinal neoplasia
To evaluate its intraoperative usability for better resection of intra- and extramedulary tumors.
Methods
Fresh surgical resection specimen of human spinal tumors were examined to test the signal intensity and adequate contrast for CLE imaging after topical application of 0.1ml acriflavine. Reproducible and specific histomorphologic criteria was the ex vivo histopathologic gold standard staining.
results
CLE yielded high-quality histomorphology of normal tissue and tumors. Different fluorescent agents revealed distinct aspects of tissue and cell structure (nuclear pattern, axonal pathways, hemorrhages). CLE discrimination of neoplastic from healthy tissue was easy to perform based on tissue and cellular architecture and resemblance with histopathology was excellent.
conclusIon
Confocal endomicroscopy is a recent method for diagnosis of various neurosurgical disorders. It provides real-time images to aid in the diagnosis and management for these conditions. CLE also achieves a more targeted optical biopsy of the abnormal tissue to expedite the therapeutic planning and decisions regarding surgical intervention. Future trends in confocal endomicroscopy include the wide spread use of molecular imaging with labeled peptides to aid in a more accurate diagnosis of malignancies and for therapeutic planning.
BEST FREE pApER pRESENTATioNS 1BP 2

41page
BEST FREE pApER pRESENTATioNS 1BP 3
MiniMally invasive sPine surgery for ManageMent of sPinal Metastasis With Progressive neurological Deficits
Abrar Ahmed, Sanjoy BiswasApollo Gleneagles Hospitals, Kolkata, West Bengal, India
objectIves
To evaluate clinical outcomes and complications after minimally invasive decompression and stabilization in patients with progressive neurological deficit
Methods
It is a non randomized prospective study performed between January 2010 until Dec 2013 by a single spine surgeon. Twenty patients having progressive neurological deficits pertaining to metastasis spine were operated. There were 15 males and five female patients. Median age was 45 years (range-30yrs to79 yrs) All patients had biopsy proven primary oncological diagnosis. Patients with renal cell carcinioma and thyroid carcinoma had preoperative embolization. All patients had percutaneous pedicular screw stabilisations and minimally invasive cord decompression. They were followed up at three monthly intervals. All the patients were given adjuvant chemotherapy and/or radiotherapy in postoperative period
results
Median surgical time was 132 minutes with average blood loss of 180 ml (range 100-450ml) All the patients had percutaneous pedicular screw insertion followed by minimally invasive posterolateral or anterolateral decompressions. All patients improved by one to two Frankel grades. One patient had superficial wound necrosis at site of previous radiotherapy. There was one death due to metastatic encephalopathy, hypercalcemia,and malignant ascitis VAS score improved from average of 6.9 to 1.6.
conclusIon
Percutaneous stabilization and decompression is an effective procedures in patients with multiple comorbidities because of primary malignancy and its treatment. These procedures are associated with minimal discomfort, less blood loss, minimal complications and perioperative morbidities and should be preferred treatment modality in metastasis with progressive neurological deficits.

42page
MiniMal invasive staBilization of the Degenerative luMBar sPine
Ardian Hana, Christophe Berthold, Vimal Gunness, Guy MatgéNational Neurosurgical Department, Centre Hospitalier de Luxembourg, Luxembourg
bacKground
Short arthrodesis is preferred to mobilise patients quickly in order to enable them a return to work as soon as possible, mainly in critical economic environment.
objectIves
To review surgical treatment of the instability of the lumbar column by means of minimal invasive surgery between 2011 and 2013.
Methods
Patients have been operated between 9/2011 and 9/2013 were reviewed. Approach is a minimal invasive TLIF under microscope. The percutaneous osteosynthesis is performed under frontal and lateral fluoroscopy. A complete removal of the disc is followed by the implantation of a banana cage with bone graft. Patients are mobilized on the first postoperative day.
results
There were 38 patients – stand-alone-cage 6 cases, cage – fixator in 25 cases, only fixator in 7 cases. There were unilateral foraminal stenosis in 28 cases and bilateral foraminal stenosis in 10 cases.Postoperatively there was one case of L5 radicular paresis and three cases of transient radicular dysesthesia. One reoperation was necessary because of secondary dislocation of screws. 89% of the patients could return to their normal activities within 4-8 weeks.
conclusIons
Minimal invasive surgery is satisfactory from a technical point of view. A cage and bilateral fixation is not always mandatory. We have to adapt the technique to patients pathology. The results up to date are promising with a rapid recovery of the patients and a fast return to work in 89% within 4-8 weeks.
BEST FREE pApER pRESENTATioNS 1BP 4

43page
BEST FREE pApER pRESENTATioNS 1BP 5
accuracy anD safety of flouroscoPic guiDeD Percutaneous PeDicle screWs in luMBar anD sacral sPine:
a revieW of 880 screWs Chee Kidd Chiu1, Mun Keong Kwan1, Chris Yin Wei Chan1,
Christian Schaefer3, Nils Hansen-Algenstaedt2
1Department of Orthopaedic Surgery, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia 2OrthoCentrum Hamburg, Parkklinik Manhagen, Germany
3Department of Orthopaedic Surgery, University Medical Centre, Hamburg-Eppendorf, Germany
IntroductIon
Minimally invasive lumbar spinal stabilization using percutaneous pedicle screws technique has become very popular in the recent years. The indications of this new technique have been expanding each day. However the knowledge regarding the accuracy and safety is still lacking especially in our Asian patients.
objectIve
To determine the accuracy and safety of fluoroscopic guided percutaneous pedicle screw technique. The safety of this technique was assessed by the rates, grades and directions of perforations.
Methods
CT scans of patients who had spinal surgery from January 2008 to December 2012 using percutaneous pedicle screws were selected to be evaluated from two spine centers: University Medical Centre, Hamburg-Eppendorf, Germany and University Malaya Medical Centre, Malaysia. There were 203 subjects with the mean age of 58.8±16.0 recruited for this study. A total of 880 percutaneous pedicle screws were analyzed. The screws with perforations were divided into according to the directions of perforation i.e. medial, lateral, superior, inferior and anterior) and the severity of the perforation were graded accordingly using Rao’s classification.
results
Of the 880 screws evaluated, 793 pedicle screws (90.1%) were inserted into the pedicle perfectly. There were 87 screws with perforation with the overall perforation rate of 9.9%. There were 65 (7.4%) grade 1 perforations, 18 (2.0%) grade 2 perforations and 4 (0.5%) grade 3 perforations. All the grade 3 perforations did not result in any complications and therefore it was left in-situ. The perforation rate was noted to be highest in S1 (19.4%), and L5 (14.9%).
The directions of perforations were: medial 1.4% (12 screws), lateral 5.7% (50 screws), anterior 2.7% (24 screws), superior 0.5% (4 screws) and inferior 0.2% (2 screws). Out of the 12 screws with medial perforation, there were 83.3% (10 screws) grade 1 perforations, 8.3% (1 screw) grade 2 perforations and 8.3% (1 screw) grade 3 perforations. All of the grade 2 and 3 medial perforations did not result in any neurological complication. For anterior perforations, there were 95.8% (23 screws) grade 1 perforations and 3.6% (1 screw) grade 3 perforations. The 3 anterior perforations did not require any revision as it did not impinge on important anterior structures.
conclusIons
Fluoroscopic guided percutaneous pedicle screws fixation in lumbar and sacral spine is safe and accurate.
Keywords
pedicle screw, minimally invasive, percutaneous, fluoroscopic guided, safety, accuracy, perforation.

44page
FREE PAPERS 2
FP 1 ACCURACY AND SAFETY OF FLOUROSCOPIC GUIDED PERCUTANEOUS 45 PEDICLE SCREWS IN THORACIC SPINE: A REVIEW OF 1120 THORACIC PEDICLE SCREWS
Chee Kidd Chiu1, Mun Keong Kwan1, Chris Yin Wei Chan1, Rezza Zamani3, Nils Hansen-Algenstaedt2
1Department of Orthopaedic Surgery, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia 2OrthoCentrum Hamburg, Parkklinik Manhagen, Germany 3Department of Orthopaedic Surgery, University Medical Centre, Hamburg-Eppendorf, Germany
FP 2 TREATMENT OF DEGENERATIVE DISC DISEASE WITH ALLOGENEIC 46 MESENCHYMAL STEM CELLS
Ali Noor M1, Mohd Noor M N2 1Ampang Puteri Specialist Hospital, Kuala Lumpur, Malaysia 2Department of Orthopaedics, University Kebangsaan Malaysia, Kuala Lumpur, Malaysia
FP 3 EARLY EXPERIENCE WITH ENDOSCOPIC SPINE SURGERY 47 (DESTANDAU’S TECHNIQUE)
Arvind MalhotraGovernment Medical College & Hospital, Chandigarh, Punjab India
FP 4 REDUCTION OF MODERATE TO HIGH GRADE SPONDYLOLISTHESIS 48 AFTER CIRCUMFERENTIAL RELEASING TECHNIQUE UNDER THE MINI-OPEN POSTERIOR LUMBAR INTERBODY FUSION (PLIF)
Hyeun Sung Kim1, Se Jin Jeong1, Hyung Jun Ahn1, Ki Hyun Jeon1, Woo Jin Choi1, Kwan Tae Kim1, Keun Soo Jang2, Seok Won Kim2, Chang Il Ju2, Seung Myung Lee2, Ho Shin2
1Department of Neurosurgery, Hurisarang Spine Hospital, Daejeon City, Republic of Korea 2Department of Neurosurgery, College of Medicine, Chosun University, Gwangju City, Republic of Korea
FP 5 CONFOCAL LASER ENDOMICROSCOPIC (CLE) CHARACTERIZATION AND 49 DIFFERENTIATION OF SPINAL METASTASIS
Cleopatra Charalampaki, Christian Eyth, Mirwais Morgan, Alhadi IgressaNeurosurgical Department, Hospital Merheim, University of Witten-Herdecke, Cologne, Germany

45page
FREE pApERS 2FP 1
accuracy anD safety of flouroscoPic guiDeD Percutaneous PeDicle screWs in thoracic sPine:
a revieW of 1120 thoracic PeDicle screWs Chee Kidd Chiu1, Mun Keong Kwan1, Chris Yin Wei Chan1,
Rezza Zamani3, Nils Hansen-Algenstaedt2
1Department of Orthopaedic Surgery, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia 2OrthoCentrum Hamburg, Parkklinik Manhagen, Germany
3Department of Orthopaedic Surgery, University Medical Centre, Hamburg-Eppendorf, Germany
IntroductIon
Minimally invasive spinal stabilization using percutaneous pedicle screws technique has become popular in the recent years. The indications of this new technique have been expanding each day. However the knowledge regarding the accuracy and safety is still lacking in the English literature, especially the safety of this technique in the thoracic spine region.
objectIve
To determine the accuracy and safety of fluoroscopic guided percutaneous pedicle screw technique. The safety of this technique was assessed by the rates, grades and directions of perforations.
Methods
CT scans of patients who had spinal surgery from January 2008 to December 2012 using percutaneous pedicle screws were selected to be evaluated from two spine centers: University Medical Centre, Hamburg-Eppendorf, Germany and University Malaya Medical Centre, Malaysia. There were 208 subjects with the mean age of 59.2±15.5 recruited for this study. A total of 1120 percutaneous thoracic pedicle screws were analyzed. The screws with perforations were divided into according to the directions of perforation i.e. medial, lateral, superior, inferior and anterior and the severity of the perforation were graded accordingly using Rao’s classification.
results
Of the 1120 screws evaluated, 1020 pedicle screws (91.1%) were inserted into the pedicle perfectly. There were 100 screws with perforation with the overall perforation rate of 8.9%. There were 86 (7.7%) grade 1 perforations, 13 (1.2%) grade 2 perforations and 1 (0.1%) grade 3 perforations. The grade 3 perforation was directed anteriorly and did not result in any complications and therefore it was left in-situ. The perforation rate was noted to be highest in T1 (33.3%), and T4 (18.6%).
The directions of perforations were: medial 4.3% (48 screws), lateral 2.1% (24 screws), anterior 2.5% (28 screws), superior 0.2% (2 screws) and inferior 0.5% (6 screws). Out of the 48 screws with medial perforation, there were 89.6% (43 screws) grade 1 perforations and 10.4% (5 screws) grade 2 perforations. All of the grade 2 medial perforations did not result in any neurological complication. For anterior perforations, there were 85.7% (24 screws) grade 1 perforations, 10.7% (3 screws) grade 2 perforations and 3.6% (1 screw) grade 3 perforations. None of the grade 2 or 3 anterior perforations required any revision as it did not impinge on important anterior structures.
conclusIons
Fluoroscopic guided percutaneous pedicle screws fixation in thoracic spine is safe and accurate.
Keywords
thoracic, percutaneous pedicle screw, minimally invasive, fluoroscopic guided, safety, accuracy.

46page
FREE pApERS 2FP 2
treatMent of Degenerative Disc Disease With allogeneic MesenchyMal steM cells
Ali Noor M1, Mohd Noor M N2 1Ampang Puteri Specialist Hospital, Kuala Lumpur, Malaysia
2Department of Orthopaedics, University Kebangsaan Malaysia, Kuala Lumpur, Malaysia
objectIve
To evaluate the use of allogenic mesenchymal stem cells in the treatment of degenerative disc disease
Method
15 patients with degenerative disc disease (DDD) were treated with percutaneous disc nucleoplasty followed by infiltration of allogenic mesenchymal stem cells (AMSC). The patients had either Cervical or Lumbar DDD. Several patients had prolapsed discs. Most had multi-level disc pathology.
All patients had been treated previously with an adequate period of conservative management and continued to experience severe pain and neurology. All patients were treated with percutaneous disc nucleoplasty followed by an infusion of allogenic mesenchymal stem cells.
results
The patients were followed up for a period of 24 to 36 months. All patients showed good to excellent pain relief on the VAS. There were no adverse reactions or complications. Several of the patients had MRI scans done 24 to 36 months after treatment. All the treated discs did not show deterioration of the discs. One Cervical disc prolapse showed spontaneous fusion of disc.
These early results are encouraging.

47page
early exPerience With enDoscoPic sPine surgery (DestanDau’s technique)
Arvind MalhotraGovernment Medical College & Hospital, Chandigarh, Punjab, India
bacKground
Functional surgery is a surgery where the pathologic tissue is removed while retaining the stability of spine. Endoscopic spine surgery through interlaminar approach using Destandau technique has the capability of achieving it
objectIve
To review retrospectively cases done using the method including intraoperative complications and outcome of the surgery
MaterIals and Methods
Patients diagnosed of lumbar disc herniations were operated after failure of conservative treatment between January 2010 and December 2013 were reviewed. Technique comprised localization of symptomatic level followed by insertion of an endospine system devise through a 15 mm skin and fascial incision. Endoscopic discectomy is then carried out by conventional micro disc surgery instruments by minimal invasive route. The results were evaluated by Macnab’s criteria after a minimum followup of 12 months and maximum up to 24 months.
results
Based on modified Macnab’s criteria, 90% patients had excellent to good, 8% had fair, and 2% had poor results. The complications observed were discitis and dural tear in five patients. 90% patients were able to return to light and sedentary work with an average delay of 3 weeks and normal physical activities after 2 months.
conclusIon
Endoscopic discectomy provides a safe and minimal access corridor for lumbar discectomy. The technique also allows early postoperative mobilization and faster return to work.
FREE pApERS 2FP 3

48page
FREE pApERS 2FP 4
reDuction of MoDerate to high graDe sPonDylolisthesis after circuMferential releasing technique unDer
the Mini-oPen Posterior luMBar interBoDy fusion (Plif)Hyeun Sung Kim1, Se Jin Jeong1, Hyung Jun Ahn1, Ki Hyun Jeon1, Woo Jin Choi1,
Kwan Tae Kim1, Keun Soo Jang2, Seok Won Kim2, Chang Il Ju2, Seung Myung Lee2, Ho Shin2
1Department of Neurosurgery, Hurisarang Spine Hospital, Daejeon City, Republic of Korea 2Department of Neurosurgery, College of Medicine, Chosun University, Gwangju City, Republic of Korea
Surgical reduction of spondylolisthesis is always challenging. The aim is to be safe and minimizing the risk of any neurologic deficit and while maximise the reduction using mini-open, posterior-lumbar interbody fusion under circumferential releasing technique.
objectIves
To present the results of reduction of moderate to high grade Spondylolisthesis after circumferential releasing technique under the mini-open posterior lumbar interbody fusion(PLIF)
MaterIal & Methods
50 cases of spondylolisthesis ( 42 cases included in Grade II, 5 cases included in Grade III and 3 cases included in Grade IV ) underwent mini-open PLIF with percutaneous screwing under epidural anesthesia using the percutaneous screw system. A circumferential releasing technique was performed according to the following sequence: 1. Intraoperative postural reduction position; 2. facet joint mobilization decompression; 3. Segmental Mobilization by wide distraction of restricted disc space; 4. Increasing sacral slope by pressure compression and rod compression during rod tightening; and 5. Increasing the anterior disc height by angled lumbar interbody fusion cage. The clinical results were evaluated by degree of slippage reduction, degree of disc height restoration, degree of lumbar lordosis restoration, degree of segmental angle restoration, and degree of postoperative neurological complications.
results
The degree of slippage rate preoperative was 37.98% to postoperative 9.3%. The height of disc space was preoperative 5.5mm to postoperative 12.1mm. The preoperative lumbar segmental angle preoperative was 430 to postoperative 48.20 and focal segmental kyphotic angle was preoperative 10.10 to postoperative 15.90. There was no motor weakness after operation. Even though 3 cases (6%) had transient, mild, motor weakness and 7 cases (14%) had transient sensory change.
conclusIon
Maximal reduction of spondylolisthesis under is achieved in the cases of a moderate to high grade of spondylolisthesis using the circumferential segmental releasing technique with minimal complications.

49page
confocal laser enDoMicroscoPic (cle) characterization anD Differentiation of sPinal Metastasis
Cleopatra Charalampaki, Christian Eyth, Mirwais Morgan, Alhadi IgressaNeurosurgical Department, Hospital Merheim, University of Witten-Herdecke, Cologne, Germany
IntroductIon
Metastatic tumors are among the most common mass lesions in the vertebral bodies. Histopathological criteria for differentiation of metastasis originate from their morphological appearance in HE stains.
PurPose
To investigate the accuracy of the CLE technique in analyzing histological patterns of different metastasis originated from different organs.
To assess the accuracy of diagnosis of the primary tumor according the confocal endoscopic histopathological patterns in comparison with the HE stains of the original tumor.
Methods
Intraoperative CLE technique were used to analyze different tissues originated from different organs of the body. The samples were stained with topical application of 0.1ml acriflavine. Then the analysis of the CLE technique biopsies taking from the primary tumor of origin were done, and compared those with the CLE pictures generated from the brain metastasis. Reproducible and specific histomorphologic criteria were criteria for the histopathologic gold standard staining.
results
45 samples of biopsied tissue from different primary tumors were analyzed. Every type of metastasis could be defined with the CLE technique. The CLE pictures showed the same histomorphological findings as in the HE staining. Furthermore, we achieved a high accuracy of the confocal image of the metastasis compared with the confocal image of the primary tumor. The differentiation and classification under CLE view of the metastasis and also the affiliation to the organ of origin in every patient was possible.
conclusIon
With the CLE technique it is possible to characterize and define lesions as metastasis regarding their histological confocal appearance. Furthermore, we were able to differentiate metastasis in vivo from each other, and in the future it might be able to define the organ of origin according to histomorphological architecture of the confocal image.
FREE pApERS 2FP 5

50page
PP 1 OUTCOMES FOLLOWING AGGRESSIVE SURGICAL RESECTION OF INTRAMEDULLARY 51 SPINAL CORD TUMORS (IMSCT) WITH INTRA-OPERATIVE NEURO-MOINTORING R Tiruchelvarayan1, M H Tang1, S Perera1, Y L Lo2 1Department of Neurosurgery, National Neuroscience Institute, Singapore General Hospital, Singapore 2Department of Neurology, National Neuroscience Institute, Singapore General Hospital, Singapore
PP 2 BASIS OF POLICY OF SURGERY TREATMENT OF LUMBAR DISCOGENIC CONFLICT 52 Artem DydykinMunicipal Angarsk Emergency Hospital, Angarsk, Irkutsk Region, Russia
PP 3 ANTERIOR CERVICAL DISCECTOMY AND FUSION-IMPROVING SURGICAL 53 TECHNIQUES AND MINIMISING INVASIVENESSRajendra Tiruchelvarayan, Foong Wei ShengDepartment of Neurosurgery, National Neuroscience Institute, Singapore General Hospital, Singapore
PP 4 BODY MASS INDEX (BMI) AS A PREDICTIVE FACTOR OF THORACIC 54 INSUFFICIENCY SYNDROME IN ADOLESCENT IDIOPATHIC SCOLIOSIS (AIS)Joehaimey Johari1, Mohd Ariff S4, Azriani A R3, Sobri Nor2
1Department of Orthopaedics, Hospital Sultanah Nurzahirah, Kuala Terengganu, Terengganu, Malaysia 2Department of Orthopaedics, Hospital Raja Perempuan Zainab II, Kota Bharu, Kelantan, Malaysia 3Department of Community Medicine, School of Medical Sciences, Universiti Sains Malaysia Health Campus, Kubang Kerian, Kelantan, Malaysia 4Department of Orthopaedic, International Islamic University Malaysia, Kuantan, Pahang, Malaysia
PP 5 LUMBAR FUSION SURGERY – IMPROVEMENTS IN SURGICAL TECHNIQUES 54 TO MINIMISE THE INVASIVENESS Rajendra TiruchelvarayanDepartment of Neurosurgery, National Neuroscience Institute, Singapore General Hospital, Singapore
PP 6 APICAL VERTEBRAE VS LUNG FUNCTION IN ADOLESCENT IDIOPATHIC 55 SCOLIOSIS (AIS) Joehaimey J1, Mohd Ariff S4, Azriani A R3, Ahmad Sabri O2, Ahmad Tajudin A1, Sobri Nor2, Andrew Lam1, Mohd Imran Yusof5 1Department of Orthopaedics, Hospital Sultanah Nurzahirah, Kuala Terengganu, Terengganu, Malaysia 2Department of Orthopaedics, Hospital Raja Perempuan Zainab II, Kota Bharu, Kelantan, Malaysia 3Department of Community Medicine, School of Medical Sciences, Universiti Sains Malaysia Health Campus, Kubang Kerian, Kelantan, Malaysia 4Department of Orthopaedic, International Islamic University Malaysia, Kuantan, Pahang, Malaysia 5Department of Orthopaedics, School of Medical Sciences, Universiti Sains Malaysia Health Campus, Kubang Kerian, Kelantan, Malaysia
PP 7 CAUDA EQUINA SYNDROME TREATED WITH ENDOSCOPIC SURGERY – 56 A REPORT ON SERIES OF 7 CASESMahmoud Marzouq, Abdul Halim YusofSpine and Spinal Cord Rehabilitation Unit, Department of Orthopaedic, School of Medical Sciences Universiti Sains Malaysia Health Campus, Kubang Kerian, Kelantan, Malaysia
POSTER PRESENTATIONS

51page
poSTER pRESENTATioNS PP 1
outcoMes folloWing aggressive surgical resection of intraMeDullary sPinal corD tuMors (iMsct) With
intra-oPerative neuro-Mointoring R Tiruchelvarayan1, M H Tang1, S Perera1, Y L Lo2
1Department of Neurosurgery, National Neuroscience Institute, Singapore General Hospital, Singapore 2Department of Neurology, National Neuroscience Institute, Singapore General Hospital, Singapore
IntroductIon
IMSCTs can result in severe neurological deficits if untreated. Traditionally they were either biopsied or excised subtotally, but this may lead to early recurrence and progressive neurological impairment. To improve outcomes, more radical tumour resection guided by intra-operative monitoring (IOM) is being performed. In this single-surgeon series, we analyse outcomes following optimal resection of IMCSTs in conjunction with IOM. Methods All patients who underwent IMSCT resection between 2006-2012 at the Singapore General Hospital Neurosurgery Department were included in this study. IOM with somatosensory evoked potential and motor evoked potential were utilized intraoperatively. Neurological status were compared pre- and post-operatively with long-term follow-up on outcomes. MRI imaging was used pre and post operatively to assess extent of tumor resection
results
13 consecutive patients (5 males, mean age 36 years, range 12-60) were included in this study. Radical resection was performed for 11 patients; the remaining 2 had biopsies and partial debulking as frozen section showed high-grade astrocytomas. Histology revealed 6 cases of ependymoma, 5 of astrocytoma and one of haemangioblastoma and neuroenteric cyst. 1 patient had wound infection that was treated successfully. There were no cases of cerebro-spinal fluid leak. Two patients had pre-existing spinal deformity, and underwent posterior instrumented fusion concomitantly. The neurological state improved or remained stable in 11 (85%) patients; 2 patients had immediate postoperative neurological deterioration which improved subsequently with physiotherapy. Favourable functional outcomes were observed in the majority of patients during follow-up. Patients with high-grade tumours were treated with adjuvant radiotherapy though they showed poorer long-term outcomes. Mean follow-up duration was 3.2 years from operation.
conclusIon
Radical resection of IMSCTs with IOM leads to a favourable functional outcome in selected group of patients.

52page
Basis of Policy of surgery treatMent of luMBar Discogenic conflict
Artem DydykinMunicipal Angarsk Emergency Hospital, Angarsk, Irkutsk Region, Russia
Surgical removal of herniated disk in the lumbar area is the most frequent elective surgery in all neurosurgical hospitals in the Russian Federation.
As a rule, ray-tracing method of diagnostics, such as X-ray CT or MRI are used for visualization to select surgery method. However, their results are not always unambiguous.
PurPose
Design of selection principle of the type of surgery treatment of lumbar discogenic radiculitis conflict.
MaterIal and Methods
272 patients were operated on hernia of lumbar spine for the period from 2011 till 2013. Diagnostics was carried out on the basis of clinical presentation, CT-myelography and MRI. CT-myelography was used in 33% of cases.
Stable condition of posterior longitudinal ligament (PLL) and was determined with indirect indicators of CT-myelography and MRI data.
In all the cases standard back intralaminar approach was executed. During intraoperational examination posterior longitudinal ligament perforation of 63 patients was detected, thus in this case standard microdiscectomy was carried out. Paracentetic poli-canal laser decompression of disc herniation was carried out for 209 patients with intact posterior longitudinal ligament. In all cases partial ligamentum flavum resection and foraminotomy if needed were carried out.
results and dIscussIon
Result analysis of preoperational and intraoperational examination indicated, that in 22 (34,9 %) of 63 cases CT-myelography and MRI didn’t present significant data about the condition of posterior longitudinal ligament.
Constant regress of neurologic symptomatology was detected in 164 (78,4%) cases in the group of patients operated by laser technology.
conclusIon
In the case of kept intact of PLL it is reasonable to carry out laser decompression of contained herniation, if posterior longitudinal ligament is damaged microdiscectomy is carried out. Preserved posterior longitudinal ligament decreases risk of pain syndrome recurrence.
poSTER pRESENTATioNS PP 2

53page
poSTER pRESENTATioNS PP 3
anterior cervical DiscectoMy anD fusion-iMProving surgical techniques anD MiniMising invasiveness
Rajendra Tiruchelvarayan, Foong Wei ShengDepartment of Neurosurgery, National Neuroscience Institute, Singapore General Hospital, Singapore
bacKground / objectIves
Traditional ACDF methods were move invasive,with harvesting of iliac crest bone graft.Long incision were used, and patients had to use a rigid cervical collar post-operatively for fusion. New surgical techniques have improved surgical results and safety. In suitable patients, the senior author also used hybrid cervical fusion(1 level fusion with 1 level disc replacement), to allow for motion preservation.
Methods
This was a single surgeon series(RT), a retrospective study of patients undergoing ACDF(1,2 and 3 levels) in the Singapore General Hospital, Department of Neurosurgery from 2007 to September 2013. The author used techniques such as: interbody cage/plates, microscope use with microsurgical techniques, neuro-monitoring,and hybrid surgery when indicated.This was compared with a previous ACDF series 2002-2006 in the same unit, using traditional techniques (Iliac crest bone graft harvesting with collar usage).
results
From 2007 to 2013, there was an improvement in surgical results, with less complications. There were 97 patients. There were: Single level ACDF(46), 2-level ACDF(35), 3 level(8), Hybrid(1 level fusion with 1 level disc replacement)(8). Most patients presented with cervical myelopathy and cord compression, and some presented with radiculopathy-nerve root compression.The overall surgical results were good. No cases of cage/implant dislodgement requiring surgery. No patients had permanent neurological defecits. Two patients had partial worsening of limb power, but this improved gradually with physiotherapy. All other patients had improvement/preservation of motor power. There was 1 case of superficial wound infection(1%), and this was treated successfully with antibiotics. There was 1 case of a superficial neck subcutaneous hematoma, which was evacuated with no other issues. There were 2 cases of transient recurrent laryngeal nerve palsy, and these improved gradually. From the earlier series 2002-2006(45 patients), the complication rate was higher.
conclusIon
Improvements in surgical techniques have resulted in better surgical outcomes.

54page
BoDy Mass inDex (BMi) as a PreDictive factor of thoracic insufficiency synDroMe in aDolescent iDioPathic scoliosis (ais)
Joehaimey Johari1, Mohd Ariff S4, Azriani A R3, Sobri Nor2
1Department of Orthopaedics, Hospital Sultanah Nurzahirah, Kuala Terengganu, Terengganu, Malaysia 2Department of Orthopaedics, Hospital Raja Perempuan Zainab II, Kota Bharu, Kelantan, Malaysia
3Department of Community Medicine, School of Medical Sciences, Universiti Sains Malaysia Health Campus, Kubang Kerian, Kelantan, Malaysia
4Department of Orthopaedic, International Islamic University Malaysia, Kuantan, Pahang, Malaysia
Among the reported complications of scoliosis is restrictive lung disease. Resting metabolic rate is increased when the pulmonary function is impaired. Reduction in patients’ body mass index (BMI) may be an important indicator of thoracic insufficiency syndrome. The objective of this retrospective study was to determine the correlation between spinal deformity, pulmonary function and BMI. All patients with adolescent idiopathic scoliosis (AIS) aged between 13 to 24 years, confirmed cases of AIS, and admitted at Hospital Raja Perempuan Zainab II for surgical interventions from year 2000 to 2013 were selected. Spinal deformity were determined by measuring the spinal curve angle using the Cobb angle on anterior-posterior radiographs. Pre-operative pulmonary function were evaluated using the forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1). Pearson correlation was performed to analyse the correlation between spinal deformity and pulmonary function with BMI. Thirty-eight patients were recruited. The mean age of patients was 16.7 years (SD = 6.04). Significant positive fair correlations between BMI and pre-operative FEV1 (p=0.009; r=0.417), and FVC (p=0.018; r=0.38) were observed. However, the correlation between BMI and Cobb angle was not significant (p=0.363). In conclusion, BMI was affected by poor lung function in AIS patients and can be used as a predictive factor of thoracic insufficiency syndrome.
poSTER pRESENTATioNS PP 4
poSTER pRESENTATioNS PP 5
luMBar fusion surgery – iMProveMents in surgical techniques to MiniMise the invasiveness
Rajendra TiruchelvarayanDepartment of Neurosurgery, National Neuroscience Institute, Singapore General Hospital, Singapore
bacKground / objectIvesLumbar fusion surgery has previously been associated with long skin incisions, significant pain post-operatively and associated morbidity. MIS Surgery can lessen some of the morbidity. In some spine cases, tubular retractors can be used, but in certain cases such as lumbar spine tumors, they cannot be used. Other improvements in surgical techniques can decrease the invasiveness of surgery eg: Usage of microscopes/microsurgical techniques, Spine Navigation, and these can improve patient outcomes.
MethodsThis study is a retrospective series by a single spine neurosurgeon in Singapore General Hospital. There were a total of 23 patients. The indications for lumbar fusion included: Degenerative Spine disease(8)(eg.TLIFs) and Spine Tumors(15 cases)(Benign and malignant). The duration of the study was from 2008 to 2013. Improved techniques such as Spine Navigation were used. The author also used laminotomy(at the end of surgery-replacing the lamina which was still attached to the supraspinous ligaments at 1 end), instead of laminectomy in tumor cases.
resultsThe overall results were good. All patients had preservation or gradual improvement of neurological lower limb power. There were no cases of pedicle screw related neural damage, and all patients(100%) achieved fusion. Patients were mobilized soon after surgery, and were discharged from hospital. Only 1 patient had an inadvertent dural tear intra-operatively, and this was repaired successfully. Two patient had wound infections, and these were treated successfully with drainage and antibiotics.
In conclusion, for lumbar fusion surgery, improvements in surgical techniques such as spine navigation, microsurgical techniques, and the usage of laminotomy have improved the surgical outcome.

55page
aPical verteBrae vs lung function in aDolescent iDioPathic scoliosis (ais)
Joehaimey J1, Mohd Ariff S4, Azriani A R3, Ahmad Sabri O2, Ahmad Tajudin A1, Sobri Nor2, Andrew Lam1, Mohd Imran Yusof5
1Department of Orthopaedics, Hospital Sultanah Nurzahirah, Kuala Terengganu, Terengganu, Malaysia 2Department of Orthopaedics, Hospital Raja Perempuan Zainab II, Kota Bharu, Kelantan, Malaysia
3Department of Community Medicine, School of Medical Sciences, Universiti Sains Malaysia Health Campus, Kubang Kerian, Kelantan, Malaysia
4Department of Orthopaedic, International Islamic University Malaysia, Kuantan, Pahang, Malaysia 5Department of Orthopaedics, School of Medical Sciences, Universiti Sains Malaysia Health Campus,
Kubang Kerian, Kelantan, Malaysia
A retrospective record review was conducted among patients with adolescent idiopathic scoliosis (AIS) aged 13 to 24 years, admitted to our institution for surgical intervention from 2000 to 2013. A total of 38 patients were studied to determine apical veretebrae location and lung function. The curvature of spinal deformity was measured by Cobb method on anterior-posterior radiographs. The forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV 1) were used to evaluate their pre operative pulmonary function. Simple linear regression was performed to analyse the relationship between Cobb angle and pre operative pulmonary function. Kruskal-Wallis and Mann Whitney tests were used to compare the lung function according to the severity of the deformity and different levels of affected spinal vertebra. A total of 38 patients were studied that involved thoracic and thoracolumbar scoliosis. The median FVC was significantly higher in those with affected apical vertebrae located at L1, L2 and L3 levels (median =92; IQR= 30) than those with apical vertebra at T6, T7 and T8 (median =68.5; IQR= 36) (p=0.008). The median FVC was also significantly higher in those with affected apical vertebra located at L1, L2 and L3 (median =92; IQR =30) than those with affected T9-T12 (median =74; IQR= 19 (p=0.003). In conclusion, impairment of lung function was seen in more severe spinal deformity and more proximally located curve.
poSTER pRESENTATioNS PP 6

56page
poSTER pRESENTATioNS PP 7
cauDa equina synDroMe treateD With enDoscoPic surgery– a rePort on series of 7 cases
Mahmoud Marzouq, Abdul Halim YusofSpine and Spinal Cord Rehabilitation Unit, Department of Orthopaedic, School of Medical Sciences,
Universiti Sains Malaysia Health Campus, Kubang Kerian, Kelantan, Malaysia
bacKground
Cauda Equina Syndrome is an emergency situation usually caused by massive disc herniation.
Minimally invasive surgery is said to be contraindicated in these cases. However using Karl Storz endoscopic system with a 4 mm HOPKINS® 0º- telescope and 9mm working channel of ENDOSPINE® working insert through translaminar approach we reported a case series of 7 cases succesfully operated.
objectIves
• Toshareexperienceofoperatingcaudaequinasyndromeduetomassivedischerniation
• Toevaluatetheresults
• Tonoteanyspecialprecautions
results
7 cases 6 males and one female. All gave history of heavy lifting.
No Pt Age Diagnosis Occupation Blood loss Complications Associations Urinary function
recovery
1 HWM 37 PID L4/5 CES Mechanic 200 No Yes
2 ZAR 28 PID L4/L5 CES unemployed 150 No Previous laminectomy & psy problems
No
3 MRM 27 PID L54L5 CES Lorry driver 150 Dural tear Yes (almost)
4 MD 59 PID L4L5 CES Director 50 No Had RF disc therapy 2 days prior to CES
Yes but had ED
5 AA 37 PID L4/L CES House wife 400 Dural tear Osification of Ligamentum Flavum
No
6 MZI 28 L4/L5 & L3/L4 CES
student 180 No Yes
7 AD 39 PID L3/L4 CES Lorry driver 120 No Developmental stenosis Yes
conclusIon
Cauda Equina Syndrome can be managed by endoscopic surgery. Need to alert for any associated developmental stenosis.