Embed Size (px)
Citation preview

AACE 2017
Principles of Endocrine NeckSonography Course™
ANATOMY and ULTRASOUND PATHOLOGY
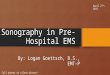
Neck Anatomy Derived from endodermal
tissue at base of tongue
Named after the thyroid cartilage (Greek: Shield)
1st gland to develop – day 24
Embryonal remnants form Thyroglossal duct; pyramidal lobe; lingual thyroid
Fuse with C-cells (neural crest origin)
C-cells scattered through posterior/superior lobes
Wharton 1656: “purpose is to… beautify the neck…particularly in females”

Thyroid Embryology
• Initial descent occurs anterior to
pharyngeal gut
• Connected to the base of tongue via
thyroglossal duct. Obliterates entirely in
7-10th week of gestation
• Remnants:
Thyroglossal duct cyst
Lingual thyroid (base of tongue)

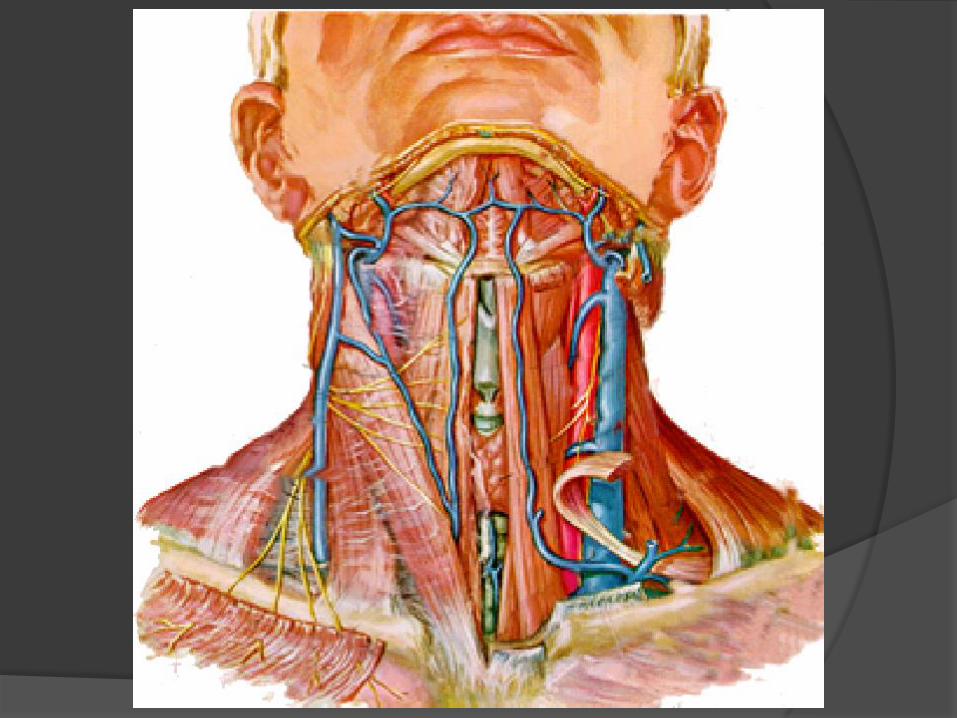
Thyroid Anatomy
• Largest endocrine
gland (20 - 25 g)
• Fills tracheo-
esophageal space
• Overlies RLN
bilaterally
• Parathyroids
typically lie at each
pole
Thyroid Ultrasonography
• Extension of physical exam
• To the thyroidologist as the stethoscope/
echocardiogram to the cardiologist
• “Real time” information to the clinician
• Very sensitive tool. Can detect nodules
only 2-3 mm in size. Lacks specificity

Thyroid Ultrasonography
Advantages
Painless
No radiation or contrast material
Less expensive than CT / MRI
May use in pregnancy
Most sensitive modality for thyroid
nodules
Best imaging for guided FNA
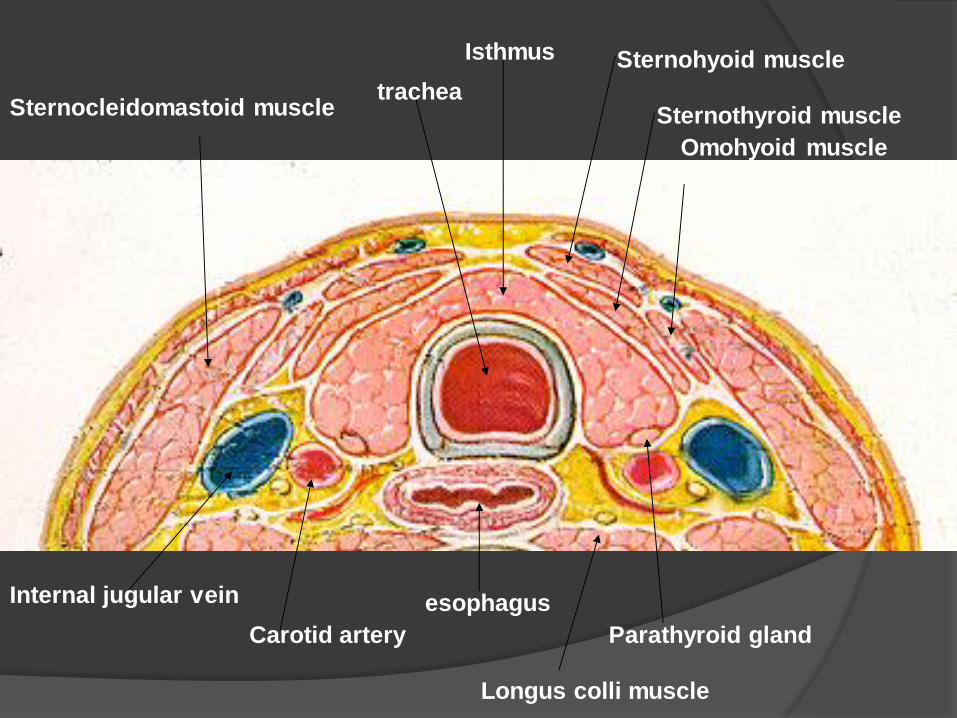
Isthmus Sternohyoid muscle
Sternothyroid muscle
Omohyoid muscle
tracheaSternocleidomastoid muscle
Internal jugular vein
Carotid artery
esophagus
Parathyroid gland
Longus colli muscle

Normal Thyroid – Composite View
CA
SCMStrap
TrachIJ
EsophLCM
R Lobe L Lobe

Normal Thyroid – R Transverse
High
Mid
Low

Normal Thyroid – L Transverse
High
Mid
Low

Appearance of
the Esophagus (post thyroidectomy)

Normal Thyroid – R Sagittal
Lateral
Mid
Medial

Thyroid Echogenicity
Normal thyroid: High intensity
homogeneous echo pattern
with little identifiable internal
architecture
Muscles located anteriorly
and anterolaterally are less
echogenic (“hypoechoic”)
Hashimoto’s thyroiditis - Note heterogeneous (hypoechoic) echotexture

Diffuse Goiter
Normal isthmus <0.5cm

Measurement of ThyroidWidth and Depth
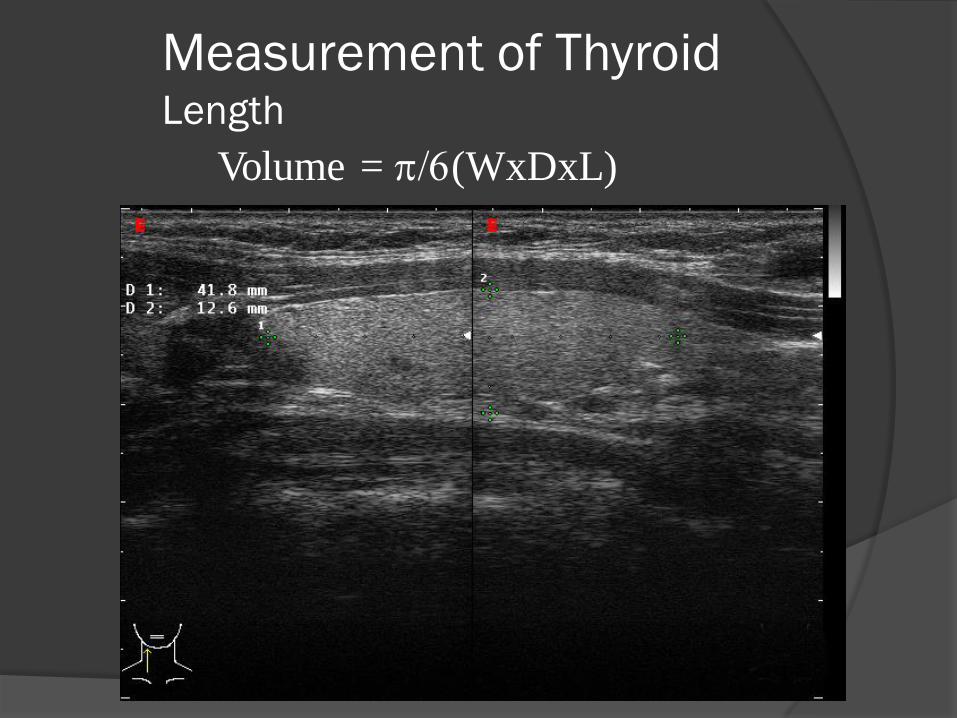
Measurement of ThyroidLength
Volume = p/6(WxDxL)

Pyramidal Lobe
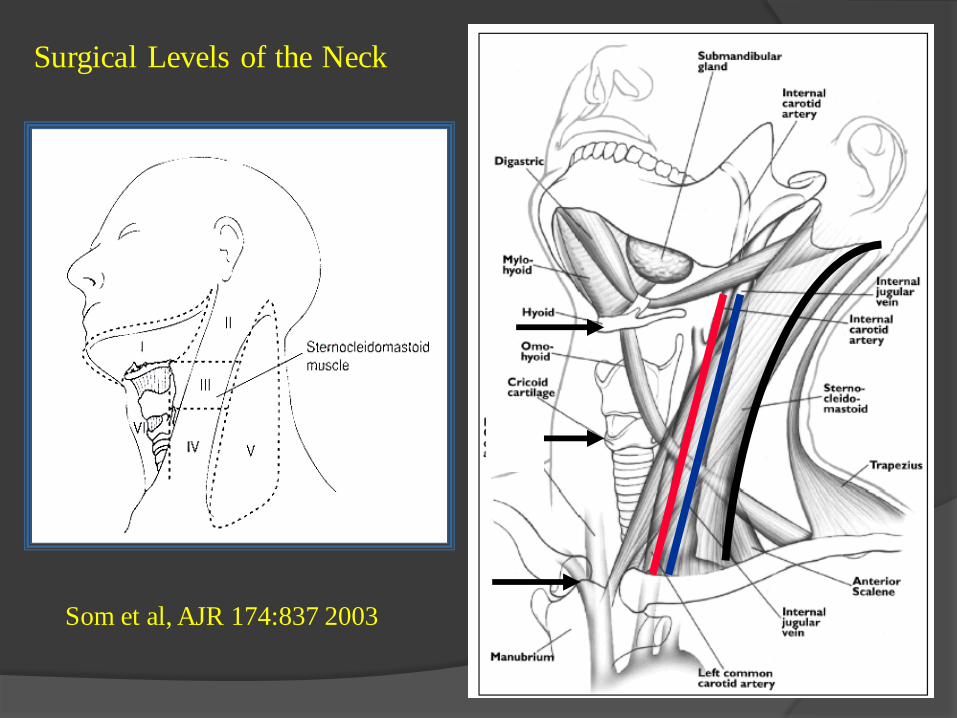
Som et al, AJR 174:837 2003
Surgical Levels of the Neck

Typical location of Parathyroid Glands
Summary
Ultrasound is an anatomic imaging tool, whose utility requires a thorough understanding of neck anatomy
Ultrasound does not generate pre-defined image planes, and is therefore highly operator dependent
Ultrasound is a functional imaging tool, through inquisition of blood flow patterns by Doppler
Ultrasound is a real-time imaging tool, which permits accurate localization of biopsy needles
Nodular Disease (more to come later)
Benign Malignant
Diffuse Goiter Iodine deficient Organification Defects Thyroiditis/Graves Riedel’s Struma Lymphoma, Metastatic Disease (nonthyroid primary)
Miscellaneous Malformations Vascular anomalies
Causes of Diffuse Thyroid Disease
Patterns of Hashimoto’s Thyroiditis
Nodules versus Pseudonodules
Doppler Evaluation of Thyrotoxicosis
Ultrasound Follow-up of Thyroiditis
Euthyroid- normal TSH, most common form
Atrophic
Goitrous
Typical Hashimoto’s US changes
50% with positive anti-TPO abs
Hypothyroid- high TSH
Atrophic, Fibrotic
Goitrous
90% with anti-TPO abs

Hyperthyroid- Hashitoxicosis
Goitrous with immune-mediated thyroid hormone spillage
Mild tenderness if any Typical echo heterogeneity with reactive LN’s +/- fibrosis Positive TG or anti-TPO abs and no thyroid stimulating
immunoglobulins High TG Modest vascularity compared to Graves’ gland
Transient TSH suppression
May have a history of previous hypothyroidism US shows typical Hashimoto’s changes in a normal sized or
enlarged gland

Hyperthyroid
Soft diffuse goiter
TSI elevated with anti-TPO abs negative or low titer
US shows hypervascular, hypoechoic, hyperplastic gland with less LN enlargement than Hashimoto’s
RAIU usually quite elevated
Associated eye and skin manifestations
Hypothyroid after RAI or gland burnout
Firm/rubbery, atrophied gland, often with nodules
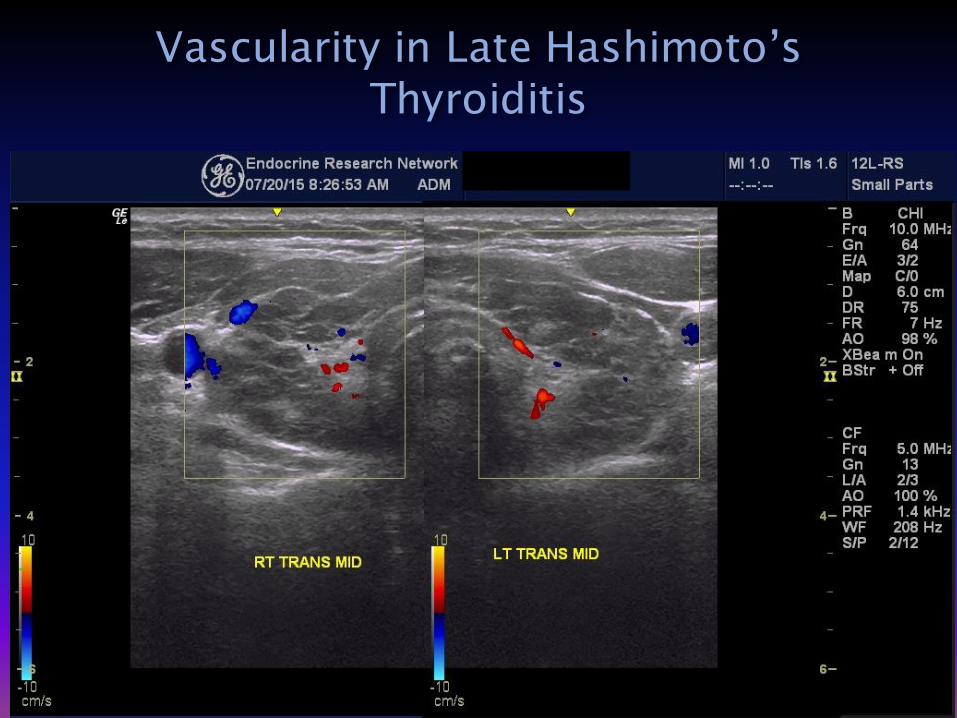
US shows densely hypoechoic, diffusely heterogenoeusappearance with hypovascularity, scarring/fibrosis
Graves Disease, Hashitoxicosis and Hashimoto’s
Graves’ and Hash exhibit different antibody profiles but commonly there is antibody overlap
Graves’ ultrasonographic appearance is classically an enlarged, hypervascular diffusely hypoechoic gland, but unadulterated Graves’ is infrequent
Typical Hashitoxicosis or Hashimoto’s ultrasonographic appearance is heterogeneous with scarring
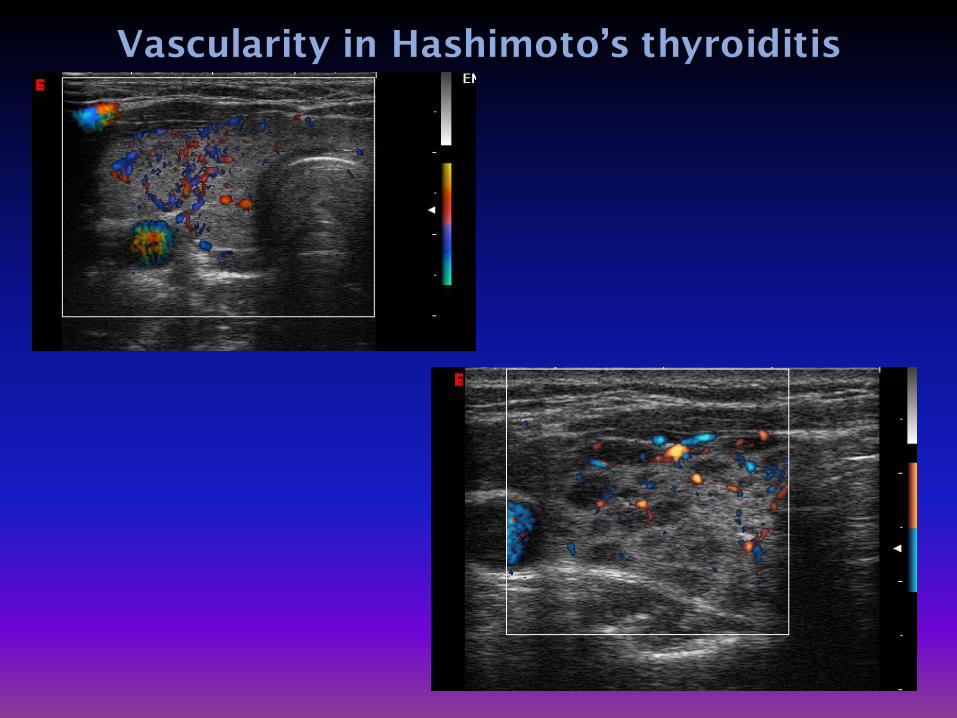
Vascularity– all patterns possible


Mildly Hypoechoic and Heterogeneous
Micronodular
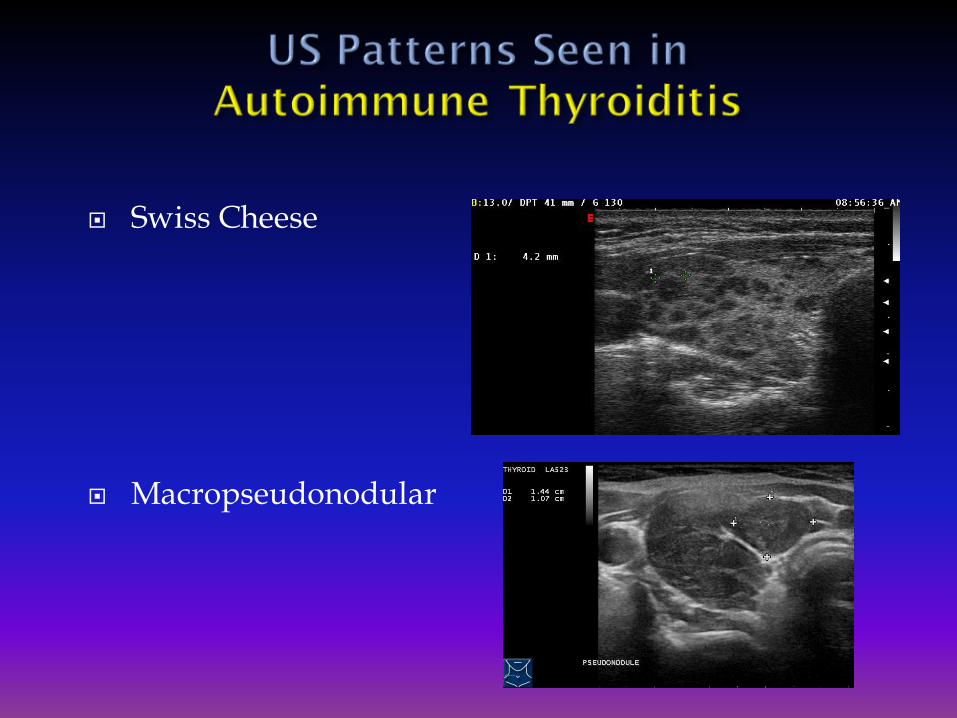
Swiss Cheese
Macropseudonodular

Profoundly hypoechoic and developing fibrosis
Hyperechoic
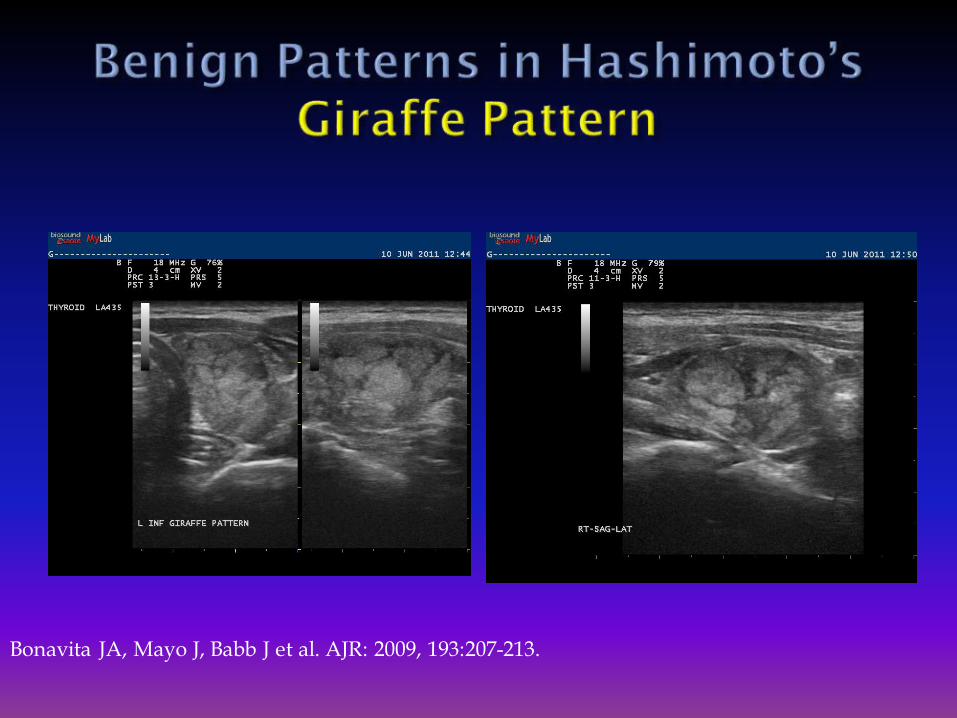
Bonavita JA, Mayo J, Babb J et al. AJR: 2009, 193:207-213.

Speckled – be careful here


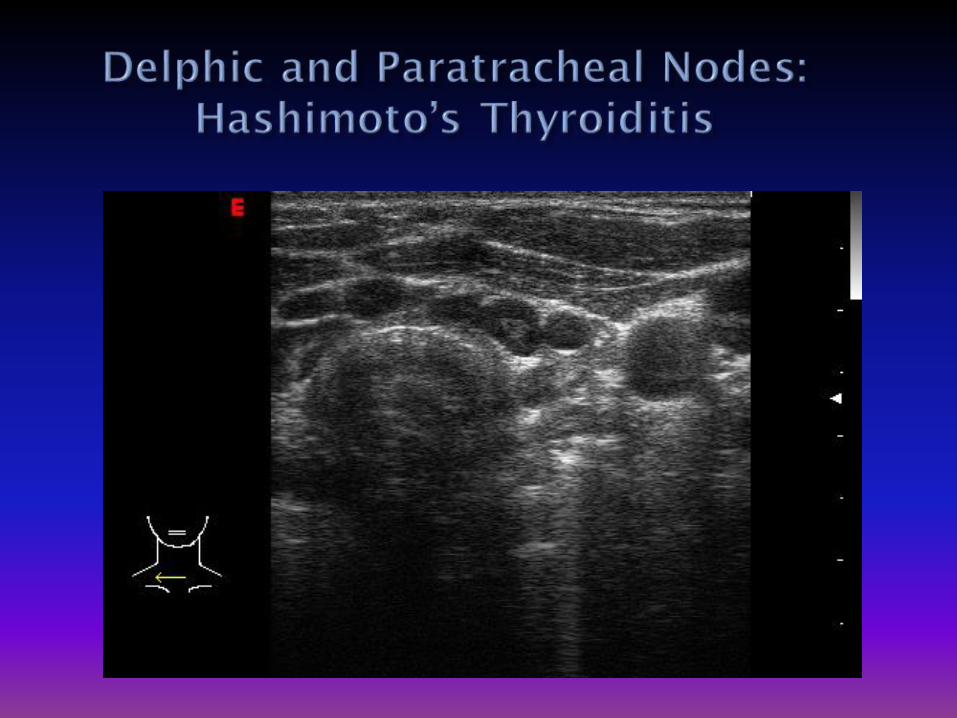
Multiple prominent nodes in central and lateral neck
Matted clustered nodes Often with abnormal shape and loss of hilar line
Location
Delphic area on and above the isthmus
Paratracheal nodes below the thyroid and at the lower poles

Typically enlarged gland with heterogeneity
May be hypoechoic or iso/hyperechoic
Increased blood flow in contrast to thyroiditis which usually has low flow
Detect nodules not felt on palpation and not seen on I-123 scan Cancer in Graves may have more aggressive biology
May be cost effective to do US in all GD patients
Cappelli C et al, Eur J Rad 2008; 65;99-103



Note the resemblance to speckled Hashimoto’s

Lymph nodeRight neckCompartment III


Note the resemblance to speckled Hashimoto’s

Note the resemblance to speckled Hashimoto’s

Bonavita JA, Mayo J, Babb J et al. AJR: 2009, 193:207-213.

Note the resemblance to speckled Hashimoto’s
Echogenicity of “nodule” similar to the unaffected thyroid parenchyma
No vascular shadow / ring / halo
Nodule shrinks with time and continued observation
Margins vague or absent
“Nodule” often not seen well in in one of the two views
Linear fibrosis often seen around “nodule”, and in the rest of the thyroid


There may be a higher prevalence of PTC in patients with Hashimoto’s Thyroiditis
The heterogeneous echotexture may make identifying nodules more difficult
In general, sonographic appearance of PTC in CLT is same as seen in normal thyroids
May be tendency towards denser calcification
If there is doubt, perform FNA Gul K, Dirikoc A, Kiyak G et al. Thyroid 2010; 20:873-8.Fiore E, Rago T, Latrofa F, et al. Endocr Relat Cancer. 2011;18(4):429-37
Anderson L, Middleton W, et al. AJR: 195, 216-222, 2010.Ohmori N, Miyakawa M, Ohmori K, et al. Intern Med 2007;46(9):547-50

Autoimmune thyroiditis is very common and has myriad forms Hypoechoic and heterogeneous US pattern is the most
common
Autoimmune thyroiditis represents a broad spectrum of thyroid disease
Thyroid nodules are common in autoimmune glands and knowing which ones to biopsy is key to being a competent thyroidologist
Thyroid cancer is not uncommon in autoimmune glands
Progressive growth of a goiter or of (pseudo)nodules should raise suspicion for a neoplastic process
Rare form of autoimmune thyroiditis
May present as a systemic disease characterized by fibrosis and lymphocytic infiltration of the retroperitoneum, mediastinum, biliary system, and orbits
Only 30% are hypothyroid
Some have hypocalcemia due to infiltration of parathyroids
Considered to be the most severe manifestation of IgG4 disease
Avoid surgery, except for diagnostic biopsy or debulking when needed
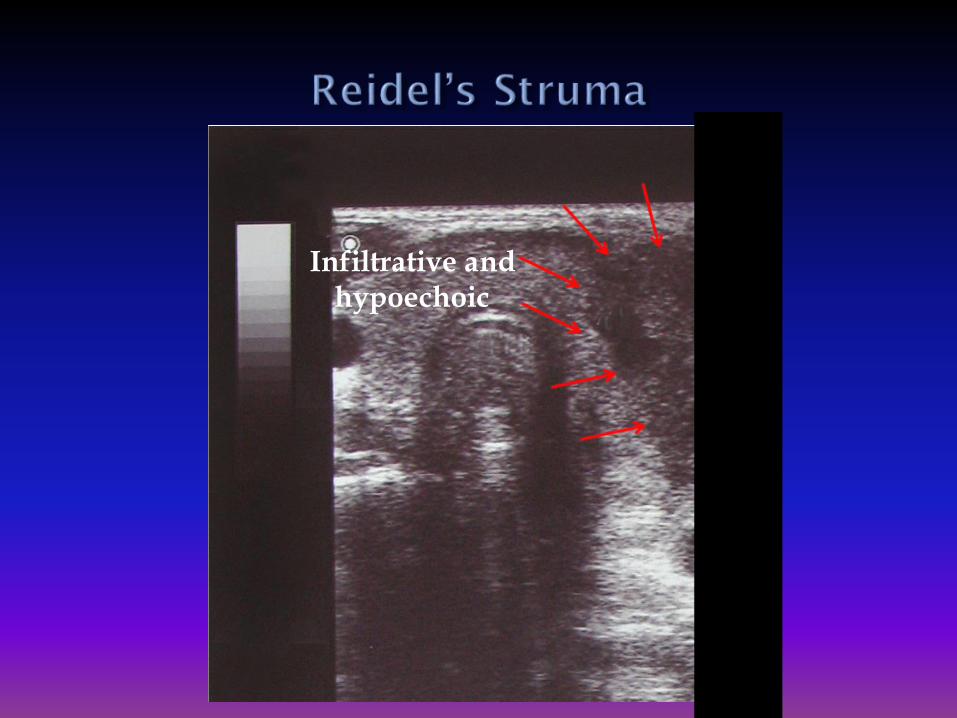
Infiltrative and hypoechoic

Diffuse or focal hypoechoic areas with irregular boundaries
Hold off on FNA if clinical suspicion suggests non-Hashimotoid thyroiditis- RTC 6-8 weeks Hyperthyroid Fever, past viral infection (6-8 weeks) and thyroid
tenderness suggest sub-acute (findings will resolve)
In thyrotoxic patient the absence of flow suggests thyroiditis, but high intensity flow can be seen in either Graves or thyroiditis of any causality
Extremely tender gland- often dramatic
Varying degree of goiter Preexisting and inflammatory
Systemic toxicity- FUO common Can masquerade as endocarditis, vasculitis
Transient thyrotoxic phase
Subsequent hypothyroid phase 95% recovery
Often focal, or multifocal
Painless, postpartum variants

At presentation
Six month follow-up

Six Weeks Later

Doppler used to help differentiate Type 1 vs Type 2 Amiodarone Induced Thyrotoxicosis
Graves’ Disease – Thyroid Inferno
Destructive Thyroiditis –
Usually Low Vascularity
Can Doppler be used to distinguish painless/postpartum thyroiditis from Graves’?

Arises in thyroid already affected by Hashimoto’s thyroiditis
Ultrasonographic appearance deeply hypoechoic.
Appearance not significantly different than in Hashimoto’s
Rapid growth of goiter should raise suspicion
Diagnosis by cytology and flow cytometry

Image courtesy of Woody Sistrunk, MD, FACE

NODULAR LYMPHOMA

Malformations
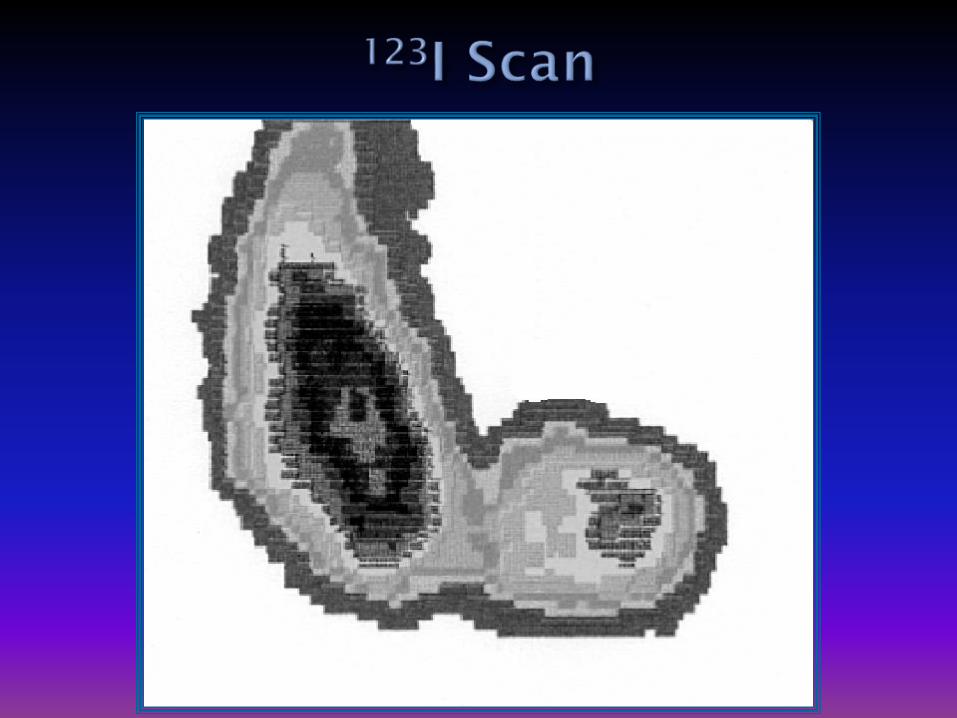
Hemiagenesis
Thyroglossal Duct Cyst
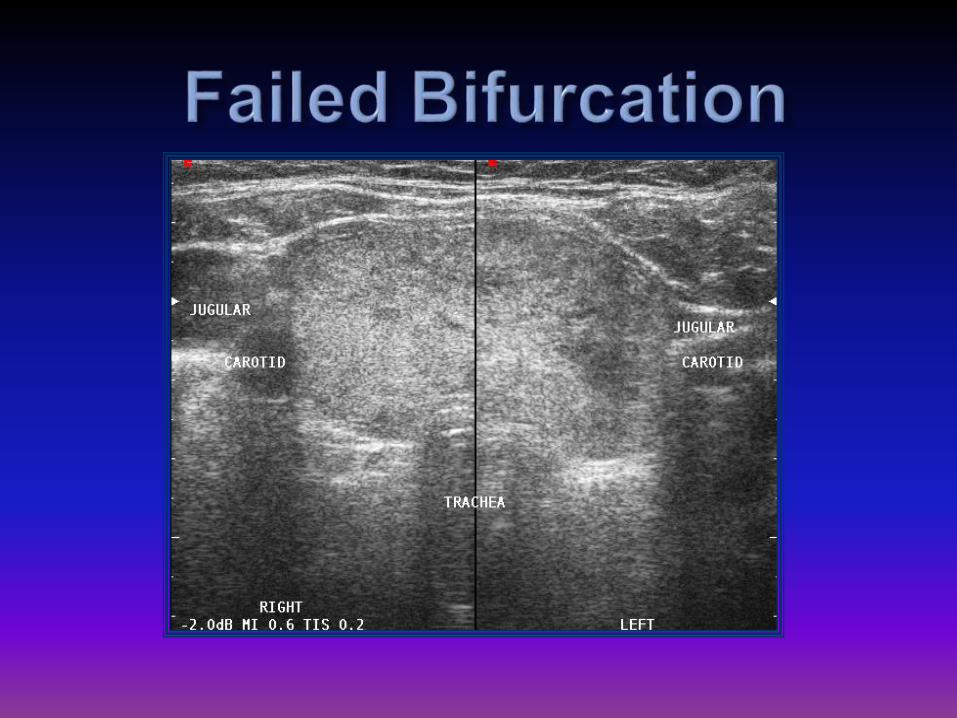
Vascular
Varicosities
Hemangioma
Anatomical Variants

Hemiagenesis of Left Lobe
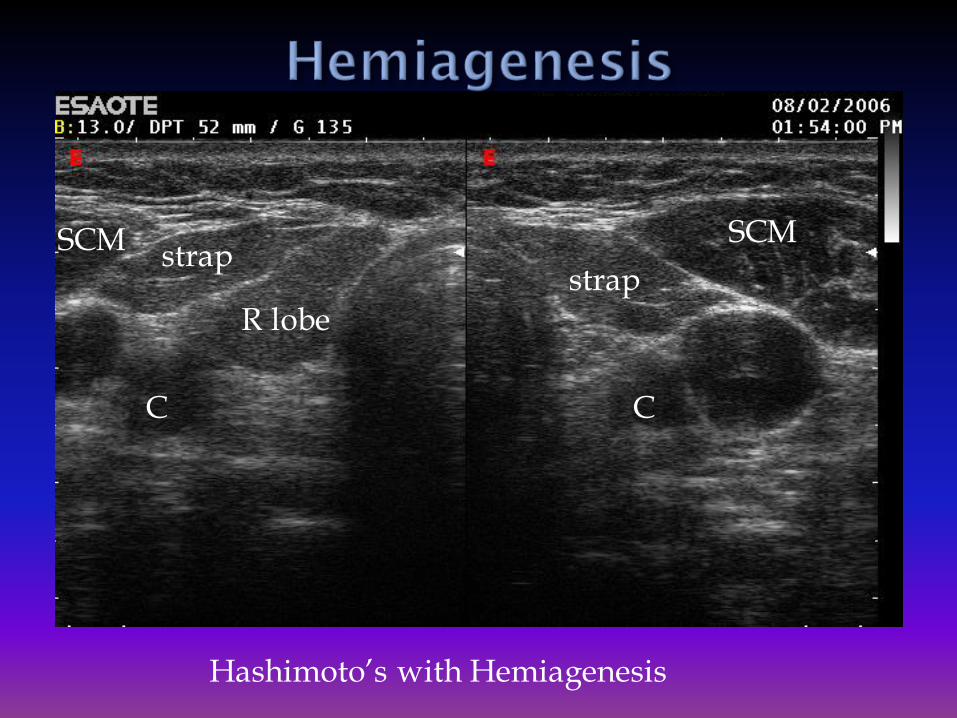
SCM SCM
C C
strapstrap
R lobe
Hashimoto’s with Hemiagenesis

Multinodular Goiter ???
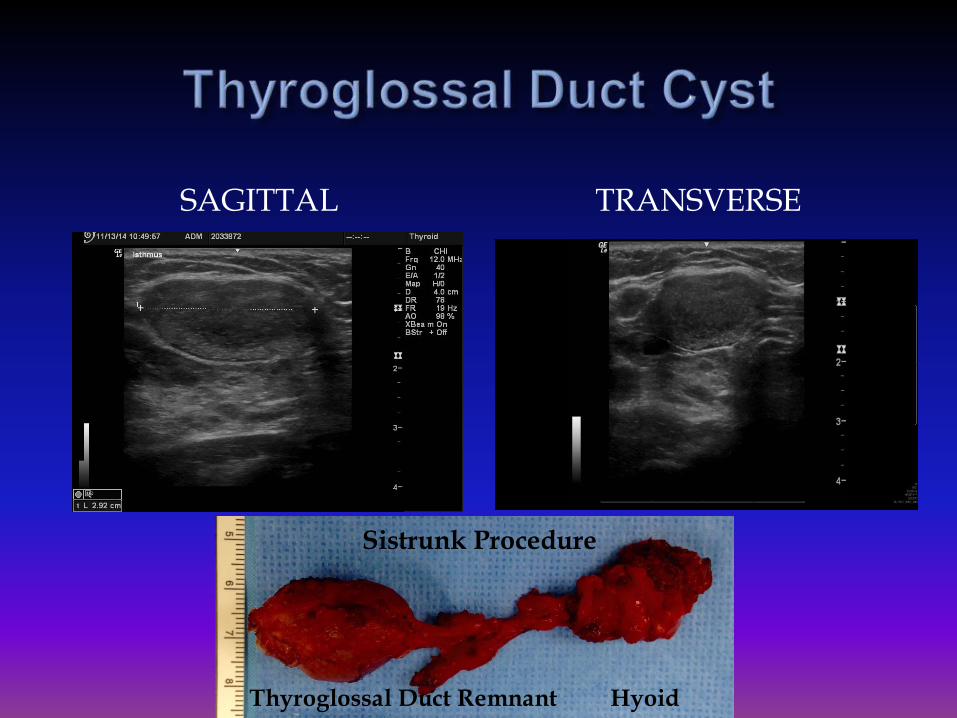
SAGITTAL TRANSVERSE
Thyroglossal Duct Remnant Hyoid
Sistrunk Procedure
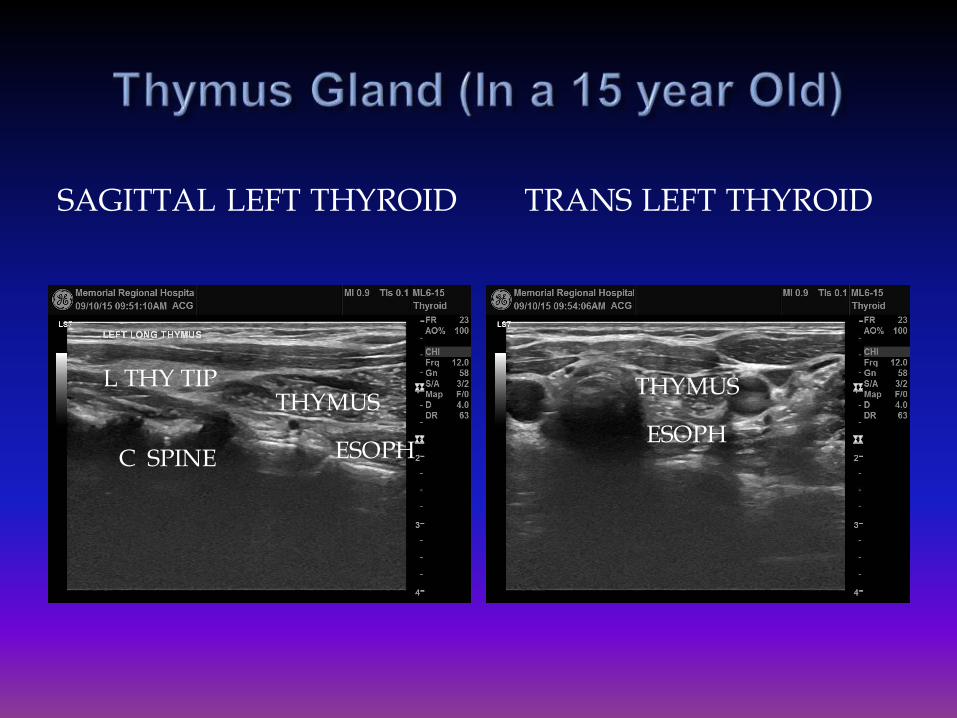
SAGITTAL LEFT THYROID TRANS LEFT THYROID
L THY TIPTHYMUS
ESOPHC SPINE
THYMUS
ESOPH

Muscle
Biopsy Proven Scar Tissue
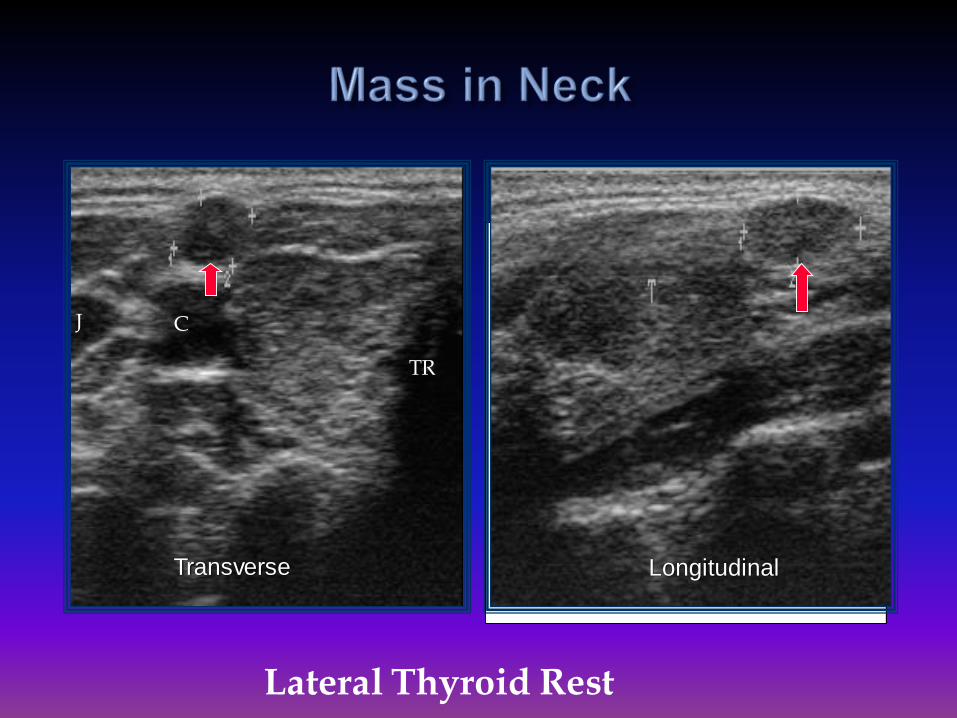
Transverse Longitudinal
C
TR
J
Lateral Thyroid Rest
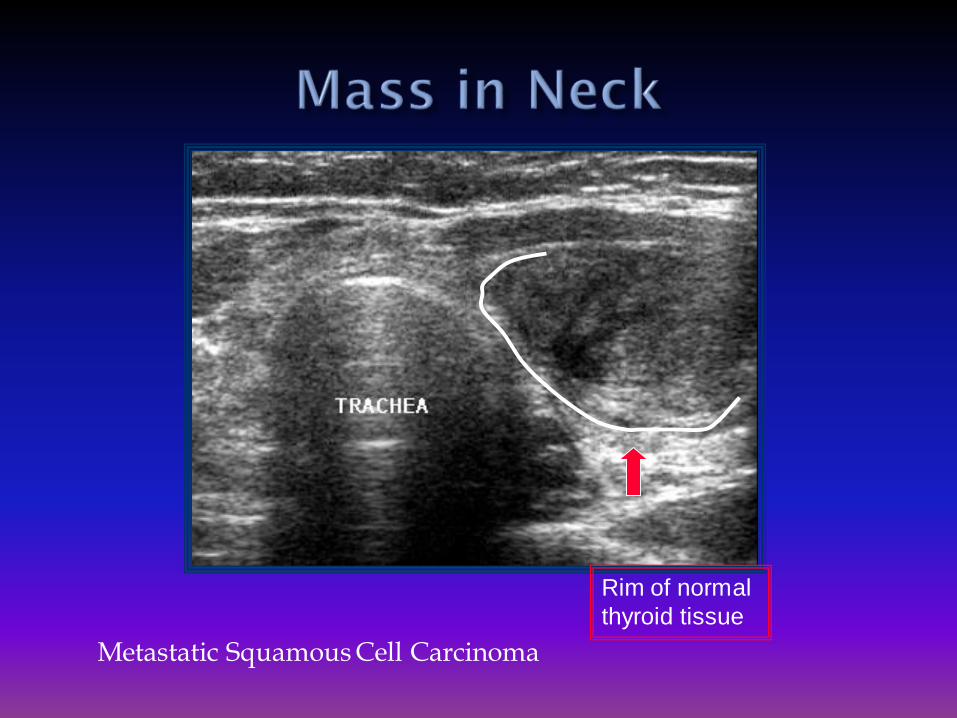
Rim of normal
thyroid tissue
Metastatic Squamous Cell Carcinoma
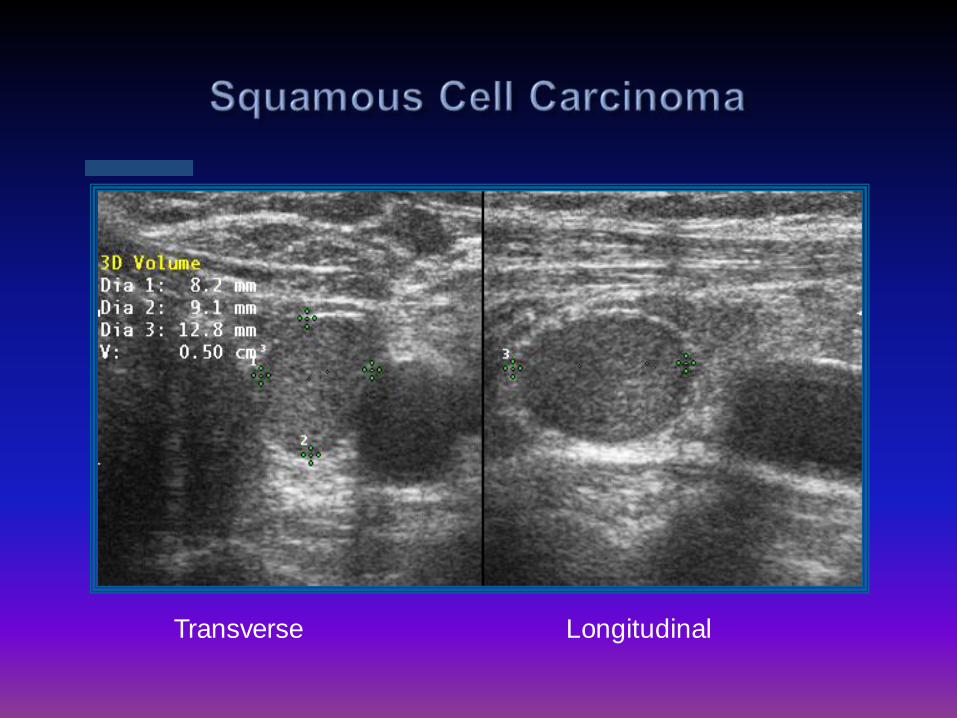
Transverse Longitudinal




Hemangioma

Tubercle of Zuckerkandl
Superior Parathyroid
Gland
Tubercle of Zuckerkandl




Transverse Longitudinal

Diffuse Thyroid Disease is a common finding in Clinical Thyroidology
AITD often mimics nodular thyroid disease
Careful ultrasound can help distinguish nodules that need FNA from those that can be observed
Doppler findings are variable, but may be helpful in the evaluation of thyrotoxicosis