Embed Size (px)
Citation preview

Journal of Plastic, Reconstructive & Aesthetic Surgery (2010) 63, 1091e1098
Anatomical study of latissimus dorsimusculocutaneous flap vascular distribution
Koichi Watanabe a, Kensuke Kiyokawa a,*, Hideaki Rikimaru a,Noriyuki Koga a, Koh-ichi Yamaki b, Tsuyoshi Saga b
a Department of Plastic and Reconstructive Surgery and Maxillofacial Surgery, Kurume University Schoolof Medicine, 67 Asahi-machi Kurume, Fukuoka 830-0011, Japanb Department of Anatomy, Kurume University School of Medicine, Fukuoka, Japan
Received 17 July 2008; accepted 18 May 2009
KEYWORDSLatissimus dorsimusculocutaneous flap;Vascular territory;Angiosome;Choke vessels;Safety elevation area offlap
* Corresponding author. Tel./fax: þE-mail address: [email protected]
1748-6815/$-seefrontmatterª2009Britdoi:10.1016/j.bjps.2009.05.042
Summary Background: The objective of the current study is to elucidate the three-dimen-sional vascular distribution as far as the peripheral areas of a latissimus dorsi musculocuta-neous flap and to establish a safe procedure for creating it.Methods: A lead oxide with gelatin-contrast agent was injected into fresh cadavers and theangiosomes in the muscle and skin were examined in detail.Results: In the muscle, three vascular territories were observed. The first vascular territory wasformed by the thoracodorsal artery, the perforating branches of the ninth intercostal artery andthose of the tenth intercostal artery located in the lateral part of the muscle. The second vascularterritory was formed by the perforating branches of the tenth intercostal artery located in themedial part of the muscle, those of the 11th intercostal artery and the subcostal artery. The thirdvascular territory was formed by perforating branches of the first and second lumbar arteries.
In the dorsal skin above the muscle, two vascular territories were observed. The first vascularterritory was formed by perforating cutaneous branches of the thoracodorsal artery, perforatingbranches of the ninth through 11th intercostal arteries and the scapular circumflex artery. Thesecond vascular territory was formed by perforating branches of the subcostal artery and the firstand second lumbar arteries.Conclusions: When using a latissimus dorsi musculocutaneous flap with the thoracodorsal arteryas a pedicle, the flap can be safely elevated as far as the inferior border of the 12th rib whereperforating branches of the subcostal artery are distributed. At the same time, skin above themuscle can be safely harvested up to the iliac crest. It is essential, however, that the skin paddleincludes perforating branches of the ninth intercostal artery or perforating branches of the 10thintercostal artery in the lateral part of the muscle.ª 2009 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
81 942 34 0834.e-u.ac.jp (K. Kiyokawa).
ishAssociationofPlastic,ReconstructiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.

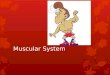
Figure 1 Latissimus dorsi muscle angiogram findings. Thereare three vascular territories in the latissimus dorsi muscle,with choke vessels between each of them. (a) Horizontalbranch of the thoracodorsal artery (b) Descending branch ofthe thoracodorsal artery (c) Perforating branches of the 9thintercostal artery in the medial part of the latissimus dorsimuscle (d) Perforating branch of the 9th intercostal artery inthe lateral part of the latissimus dorsi muscle (e) Perforatingbranch of the 10th intercostal artery in the lateral part of thelatissimus dorsi muscle (f) Perforating branches of the 10thintercostal artery (g) Perforating branches of the 11th inter-costal artery (h) Perforating branches of a subcostal artery (i)Perforating branches of the 1st lumbar artery (j) Perforatingbranch of the 2nd lumbar artery.
1092 K. Watanabe et al.
Latissimus dorsi musculocutaneous flap is currently one ofthe most frequently used musculocutaneous flaps inreconstructive surgery. It has the advantages of enablingharvesting of large areas of muscle and skin with reliableblood supply, elevation of a scapular flap, anterior serratusmuscle and scapular bone as a combined flap1,2 and eleva-tion of an osteomusculocutaneous flap with attached ribbone.3,4 As a result, it is used for reconstruction of the headand neck,5,6 the chest7 and the upper arm,8 when used asa pedicled musculocutaneous flap, and various other areasof the body when used as a free musculocutaneous flap9
employing microvascular anastomosis. However, whenharvesting a pedicled latissimus dorsi musculocutaneousflap extending as far as the peripheral region in the vicinityof the iliac crest, we experienced cases in which bloodsupply to the skin paddle and muscle at the periphery of themusculocutaneous flap was insufficient. Considering thatmusculocutaneous flaps have a very reliable blood supply,this is not the case at their peripheral parts.
There are several reports regarding the blood supply oflattismus dorsi musculocutaneous flaps.10e14 However,there are no reports elucidating the three-dimensionalroute of blood flow from the thoracodorsal artery to thelatissimus dorsi musculocutaneous flap or whether bloodflow reaches the extremities of the muscle and skin paddle.Even now, when performing general microsurgery forreconstruction in cases of extensive loss on the limbs ortrunk, in cases of failed microsurgery and cases of salvageoperation, it is necessary to harvest latissimus dorsi mus-culocutaneous flaps up to the peripheral areas. In thecurrent study, we conducted micro-angiography12,15 onfresh cadavers with an objective of elucidating the three-dimensional vascular distribution of a latissimus dorsimusculocutaneous flap and establishing a reliable proce-dure for creating the flap.
Materials and methods
The use of autopsy cadavers
Prior to the sampling of tissue, informed consent wasobtained from the attending physician and the bereavedfamily for use of the cadaver in the study. The proceduresfor tissue sampling from autopsy cases and imaging are asindicated below.
1) Full-thickness, one-piece samples of the latissimusdorsi muscle, the skin overlying it and thoraco-abdom-inal wall below the seventh rib were taken from theback of six sides of six fresh cadavers.
2) The harvested tissue from the back was maintained ata temperature of 37 �C, about the same as bodytemperature, and physiological saline solution withheparin (1000 IU of heparin sodium mixed with 100 ml ofphysiological saline solution) at a temperature of 37 �Cwas used to thoroughly flush the intravascular space.
3) Using a 50-ml syringe, a lead oxide with gelatin-contrast agent with the same composition as that usedby Rees et al.16 and at a temperature of 50 �C wasinjected into the blood vessels with a moderate degreeof pressure.
4) After injecting the contrast agent, the tissue was storedfor about 24 h at 4 �C. When the contrast agent hadsolidified, radiographs of the latissimus dorsi muscle andthe skin were taken separately. The radiographs weretaken using computed radiography (Radiography system:Shimadzu X-ray High Voltage Genarator 150B-10, Imageprocessing: Fuki film Computed Radiography FCR-HQ).Following examination of the sampled tissue, soft radio-graph images of parts that required detailed examinationwere taken with a unit used for taking mammograms(Radiography system: Yokogawa Medical Systems Seno-graph 500t, Film: Kodak MIN-R 2000 (18� 24 cm)).
Whole-body injection of the cadavers
Whole-body injection of the contrast agent was performedon three fresh cadavers provided for anatomical trainingusing the procedures indicated below.
1) With the aim of injecting contrast agent into the arte-rial system, incisions were made in the common carotidarteries and the femoral arteries on both sides of thecadavers, and 18Fr oral aspiration catheters (TerumoSafeed aspiration catheters) were placed in them. Toreduce pressure on the venous system, 18Fr oral

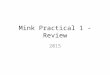
Figure 2 Dorsal skin angiogram findings. There are two angiosomes in the dorsal skin above the latissimus dorsi muscle, with chokevessels between them. (a) Circumflex scapular artery (b) Perforating branches of the thoracodorsal artery in the skin (c) Perforatingbranch of the 9th intercostal artery in the medial part of the latissimus dorsi muscle (d) Perforating branch of the 9th intercostal artery inthe lateral part of the latissimus dorsi muscle (e) Perforating branch of the 10th intercostal artery in the lateral part of the latissimus dorsimuscle (f) Perforating branches of the 10th intercostal artery (g) Perforating branches of the 11th intercostal artery (h) Perforatingbranches of the subcostal artery (i) Perforating branches of the 1st lumbar artery (j) Perforating branch of the 2nd lumbar artery.
Anatomical study of latissimus dorsi flap 1093
aspiration catheters were also placed in the femoralveins on both sides.
2) Intra-arterial perfusion with 10 l of physiological salinesolution with heparin (500 IU of heparin sodium mixedwith 500 ml of physiological saline solution) ata temperature of 40 �C was performed to thoroughlyflush the intravascular space.
3) Using a 50-ml syringe, a lead oxide with gelatin-contrast agent with the same composition as that usedby Rees et al.16 and at a temperature of 50 �C wasinjected into the common carotid arteries and femoralarteries on both sides from four locations.
4) The injected cadavers were kept in a 30% formalin bathfor about 1 month to preserve the tissue.
5) After completion of the above procedures, the sameprocedure used in the above-mentioned 1e4 was usedto take radiographs of samples of the back of the chestwall and abdominal wall, including the latissimus dorsimuscle and the overlying dorsal skin.
Results
Latissimus dorsi muscle blood circulation
Three vascular territories were observed in the latissimusdorsi muscle (Figure 1).
After entering the latissimus dorsi muscle from the axil-lary region, the thoracodorsal artery was seen to bifur-cate.11 One of the bifurcations, a horizontal branch runningparallel to the superior border of the latissimus dorsi muscle,
was directly connected as a result of perforating branches ofthe ninth intercostal artery in the medial part of thelatissimus dorsi muscle and true anastomosis. The otherbifurcation, a descending branch running parallel to thelateral border of the latissimus dorsi muscle, was directlyconnected as a result of perforating branches of the ninthand tenth intercostal arteries in the lateral part of thelatissimus dorsi muscle and true anastomosis.14 In otherwords, the first vascular territory in the latissimus dorsimuscle was a vascular network formed by direct anastomosisof the thoracodorsal artery (horizontal branch, descendingbranch), perforating branches of the ninth intercostal arteryand perforating branches of the tenth intercostal arterypresent in the lateral part of the latissimus dorsi muscle.
The second vascular territory was a vascular networkformed by direct anastomosis of perforating branches ofthe tenth intercostal artery present in the medial part ofthe latissimus dorsi muscle, perforating branches of the11th intercostal artery and perforating branches of thesubcostal artery.17e19
The third vascular territory was a sparse area of vascularnetwork composed of perforating branches of the first andsecond lumbar arteries.
Choke vessels were present between the above-mentioned first and second, and second and third vascularterritories.
Dorsal skin blood circulation
Two vascular territories were observed in the dorsal skinoverlying the latissimus dorsi muscle (Figure 2).

Figure 3 Three-dimensional vascular configuration of a latissimus dorsi musculocutaneous flap. TDA: Thoracodorsal artery Th9:Perforating branches of the 9th intercostal artery Th10: Perforating branches of the 10th intercostal artery Th11: Perforatingbranches of the 11th intercostal artery Th12: Perforating branches of a subcostal artery L1: Perforating branches of the 1st lumbarartery L2: Perforating branches of the 2nd lumbar artery L3: Perforating branches of the 3rd lumbar artery. (a) Lateral part oflatissimus dorsi muscle and skin sagittal section angiogram findings. There are choke vessels between Th10, Th11 and Th12 in thelatissimus dorsi muscle and between Th11 and Th12 in the skin. (b) Three-dimensional schema of an angiosome in a latissimus dorsimusculocutaneous flap.
1094 K. Watanabe et al.
The first vascular territory was a vascular networkformed by direct anastomosis of perforating cutaneousbranches of the thoracodorsal artery, perforating branchesof the ninth, tenth and 11th intercostal arteries and thescapular circumflex artery.20
The second vascular territory was a vascular networkformed by direct anastomosis of perforating branches ofthe subcostal artery and perforating branches of the firstand second lumbar arteries.
Choke vessels were present between the above-mentioned first and second vascular territories.
In the skin, caudally from the iliac crest where there isno latissimus dorsi muscle, there was another vascularterritory completely distinct from the second vascularterritory consisting of a vascular network formed by
anastomosis of the perforating branches of the third lumbarartery and perforating cutaneous branches from the glutealmuscle.
Latissimus dorsi musculocutaneous flap three-dimensional vascular distribution
Blood supply from the thoracodorsal artery to the firstvascular territory in the latissimus dorsi muscle wasprimarily via perforating branches of the ninth intercostalartery and perforating branches of the tenth intercostalartery located in the lateral part of the latissimus dorsimuscle, with blood flowing directly to the first vascularterritory in the skin. It is the first vascular territory of the

Figure 4 Case 1 71-year-old male. Right pedicled latissimus dorsi musculocutaneous flap grafted to reconstruct the anterior wallof the cervical oesophagus after formation of an external pharyngeal fistula following surgery for hypopharyngeal cancer (a).Latissimus dorsi musculocutaneous flap created to include perforating branches of the 10th intercostals artery in the skin paddle,with the entire latissimus dorsi muscle harvested up to the vicinity of the iliac crest (b). Anterior wall of the cervical oesophagusreconstructed with a latissimus dorsi musculocutaneous flap skin paddle, with sufficient covering by the latissimus dorsi muscu-locutaneous flap muscle. Reticular, split-thickness skin graft also performed on the rear surface of the latissimus dorsi. After surgery,the skin paddle took completely but there was partial necrosis of the muscle and the split-thickness skin graft did not take (c, d).
Anatomical study of latissimus dorsi flap 1095
latissimus dorsi muscle and the dorsal skin that form the 1stvascular territory of the latissimus dorsi musculocutaneousflap. The second vascular territory of a latissimus dorsimusculocutaneous flap was in the muscle from the edge ofthe first vascular territory to the inferior border of the 12thrib and in the skin extending to the iliac crest. Here, bloodflow in the first vascular territory was through choke vesselslocated in the muscle and skin (Figure 3a and b).
Discussion
The first report of a latissimus dorsi musculocutaneous flapwas by Tansini21 in 1906. In 1912, d’Este22 reported thereconstruction of the chest wall using a latissimus dorsimusculocutaneous flap. With the consequent developmentof microsurgery, the same musculocutaneous flap was usedas a free flap for reconstruction in various areas of thebody.9 In recent years, ingenious new ways to use the flaphave been developed, with methods of creating flaps fora wide range of applications, such as latissimus dorsi
perforator-based flaps reported by Angrigiani et al.23 andSpinelli et al.,24 and a split latissimus dorsi flap reported byTobin et al.25
However, even with a latissimus dorsi musculocutaneousflap, which is often used since it is a safe flap with a stableblood supply, we have experienced a case where, despitecomplete adherence of the skin paddle, partial necrosis ofjust the underlying muscle occurred (Figure 4). From thisexperience, it was conjectured that even with a latissimusdorsi musculocutaneous flap, depending on how it iscreated, blood supply to the peripheral areas of the flap isnot necessarily stable and that the regions of adhesion ofmuscle and skin paddle differ. In other words, even fora latissimus dorsi musculocutaneous flap, which is known tohave an extremely stable blood supply, there is actually noclear understanding of the three-dimensional vasculardistribution up to the peripheral area of the flap. In thecurrent study, we examined in detail the three-dimensionalvascular distribution of the thoracodorsal artery, which isa nutrient vessel for the latissimus dorsi muscle, andperforating branches of the costal, subcostal and lumbar

Figure 5 Case 2 72-year-old male. Reconstruction conducted with a pedicled latissimus dorsi musculocutaneous flap followingthe development of a cervical fistula after a total glossectomy, laryngectomy and mandibulectomy. The latissimus dorsi muscu-locutaneous flap skin paddle included perforating branches of the 10th intercostal artery present at the lateral border of thelatissimus dorsi, and was long, extending to the lumbar region. Muscle was harvested up to the inferior border of the 12th rib (a, b).After surgery, both the musculocutaneous flap skin paddle and muscle took completely (c, d).
1096 K. Watanabe et al.
arteries in the latissimus dorsi muscle and dorsal skin, withthe aim of establishing a method of creating safe latissimusdorsi musculocutaneous flaps.
In a report related to the blood circulation of flaps byMcGregor et al.26 in 1973, flaps were classified for the firsttime as being an axial pattern flap, which includesa nutrient artery, or a random pattern flap, which does notinclude one. The blood circulation of soft tissue was clari-fied in a report by Taylor et al.12 in 1987 that first intro-duced the concept of the angiosome (anatomical vascularterritory), which receives nutrition through a single-sourceartery and is bordered by extremely fine blood vessels,called choke vessel, that gradually become narrower.Nakajima et al.27 as well reported on the changes in bloodcirculation, including choke vessels, that occur whenelevating a flap. This referred to the elevation of an axialpattern flap, when the blood flow to the flap is from anaxial nutrient vessel only, which is a pedicle, while thevascular pedicles of adjacent vascular territories areoccluded. At this time, a pressure gradient is formedbetween the vascular territory supplied with nutrients bythe axial nutrient vessel and adjacent vascular territories.
This pressure gradient causes the choke vessels betweenadjacent vascular territories to dilate, resulting in bloodflowing from the axial nutrient vessel to the adjacentvascular territories, and the linking of blood flow.As a result, new blood circulation is created for the flap.This linking of blood flow occurs between the first vascularterritory directly supplied by the axial nutrient vessel and,through choke vessels, the adjacent second vascular terri-tory. However, linking of blood flow does not occurbetween the second and third vascular territories con-nected by choke vessels, and there is no blood flow fromthe axial nutrient vessel, which is a pedicle. In this case,the range of safe adhesion of the flap is up to the secondvascular territory, with a high possibility of partial necrosiswhen elevating a flap that includes the third vascularterritory.28,29
To clarify blood circulation when elevating a flap, thelocation of the choke vessels in the area used for the flapmust be verified and the vascular territory must be clearlyestablished. Furthermore, the location and blood circula-tion of choke vessels in the muscle, skin and subcutaneoustissue of the musculocutaneous flap and the connecting

Anatomical study of latissimus dorsi flap 1097
pathways between them must be verified three-dimen-sionally, and a ‘three-dimensional angiosome’ must bedetermined for the flap. This enables determination of therange for safe harvesting of the muscle and skin paddle forthe musculocutaneous flap, and the perforating cutaneousbranches (connecting pathways between skin and muscle)necessary in the skin paddle. Based on the above, Rikimaruet al.15 elucidated the three-dimensional vascular distri-bution of a pectoralis major musculocutaneous flap anda safe method for creating one.
If the concept of a three-dimensional angiosome isapplied to the latissimus dorsi musculocutaneous flap, thenthere are three vascular territories in a latissimus dorsimuscle, with the third vascular territory located caudallyfrom the inferior border of the 12th rib. This is in accordancewith the results we obtained with clinical cases in whichnecrosis of the muscle in the peripheral parts of latissimusdorsi musculocutaneous flaps occurred (Figure 4). Our resultsagreed with those reported by Taylor et al.12 These resultspoint to the possibility that in actual clinical practice, lat-issimus dorsi muscle located caudally from the inferiorborder of the 12th rib does not have to be included ina musculocutaneous flap.
Unlike the muscle, the skin above the latissimus dorsihas two vascular territories. Consequently, the skin paddleof a latissimus dorsi musculocutaneous flap can be safelyharvested from the inferior edge of the second vascularterritory, which extends up to the iliac crest. This is also inaccordance with clinical cases in which there was safeadhesion of a long skin paddle harvested up to the iliaccrest (Figure 5). The first vascular territory in the skinabove the latissimus dorsi muscle is directly supplied withblood by the first vascular territory in the muscle, princi-pally by perforating branches of the ninth intercostalartery, and perforating branches of the tenth intercostalartery located in the lateral part of the latissimus dorsimuscle. Together with the first vascular territory in themuscle, a first three-dimensional angiosome (vascularterritory) of the latissimus dorsi musculocutaneous flap iscreated. Blood supply to this first vascular territory fromthe thoracodorsal artery flows through the choke vessels inthe muscle and subcutaneous tissue into the second three-dimensional angiosome (vascular territory) of the latissimusdorsi musculocutaneous flap (Figure 3b). Consequently, toensure that blood flow reaches the second vascular terri-tory of the latissimus dorsi musculocutaneous flap, partic-ularly to the skin at the peripheral area over the iliac crest,the first essential step is to ensure that blood flow to theentire first vascular territory of the flap is sufficient. Toachieve this, the skin paddle must include perforatingbranches of the ninth intercostal arteries and perforatingbranches of the tenth intercostal artery located in thelateral part of the latissimus dorsi muscle. It is important tosecure a connecting pathway for blood flow from the firstvascular territory of the muscle to that of the skin. If bloodsupply to this territory is sufficient, blood supply is possiblethrough choke vessels to the extremities of the secondvascular territory (Figure 5).
From the above, important points concerning the actualcreation of a safe latissimus dorsi musculocutaneous flapduring clinical practice are as follows. When designing theskin paddle, use Doppler examination to verify that the
perforating branches of the ninth intercostal artery andperforating branches of the tenth intercostal artery in thelateral part of the latissimus dorsi muscle are included,which is essential, and do not extend the range beyond theiliac crest. For the muscle, harvest up to the inferior borderof the 12th rib (Figure 5). It is believed that adopting theseprocedures will assure the continued creation of safelatissimus dorsi musculocutaneous flaps with stable bloodsupply.
Conflict of interest
None.
Funding
None.
References
1. Harii K, Ono I, Ebihara S. Closure of total cheek defects withtwo combined myocutaneous free flaps. Arch Otolaryngol1983;108:303e7.
2. Allen RJ, Dupin CL, Dreschnack PA, et al. The latissimus dor-si/scapular bone flap (the ‘‘latissimus/bone flap’’). PlastReconstr Surg 1994;94:988e96.
3. Schmidt DR, Robson MC. One-stage composite reconstructionusing the latissimus myocutaneous flap. Am J Surg 1982;144:4470.
4. Maruyama Y, Urita Y, Ohnishi K. Rib-latissimus dorsi osteo-myocutaneous flap in reconstruction of a mandibular defect.Br J Plast Surg 1985;38:234e7.
5. Quillen CG. Latissimus dorsi myocutaneous flaps in head andneck reconstruction. Plast Reconstr Surg 1979;63:664e70.
6. Chowdhuryn CR, McLean NR, Griffithes KH, et al. The repair ofdefects in the head and neck region with the latissimus dorsimyocutaneous flap. J Laryngol Otol 1988;102:1127e32.
7. Morgan RF, Edgerton MT, Wanebo HJ, et al. Reconstruction offull thickness chest wall defects. Ann Surg 1988;207:707e16.
8. Doi K, Sakai K, Ihara K, et al. Reinnervated free muscletransplantation for extreme reconstruction. Plast ReconstrSurg 1993;91:872e83.
9. Watson JS, Graig RDP, Orton CI. The free latissimus dorsimyocutaneous flap. Plast Reconstr Surg 1979;64:299e305.
10. Bartlett SP, May WM, Yaremchuk MJ. The latissimus dorsimuscle: a fresh cadaver study of the primary neurovascularpedicle. Plast Reconstr Surg 1981;67:631e6.
11. Roswell AR, Eisenberg N, Davies DM, et al. The anatomy of thethoracodorsal artery within the latissimus dorsi muscle.Br J Plast Surg 1986;39:206e9.
12. Taylor GI, Palmer JH. The vascular territories (angiosomes) ofthe body: experimental study and clinical applications.Br J Plast Surg 1987;40:113e41.
13. El-Maasarany SH, Sharaf E, Moustafa F, et al. Anatomical basisof latissimus dorsi myocutaneous flap: clinical applications.Surg Radiol Anat 1989;11:197e203.
14. Yang D, Morrris SF. Differences in intramuscular vascularconnections of human and dog latissimus dorsi muscles.Ann Thorac Surg 1999;67:489e93.
15. Rikimaru H, Kiyokawa K, Inoue Y, et al. Three-dimensionalanatomical vascular distribution in the pectoralis major myo-cutaneous flap. Plast Reconstr Surg 2005;115:1342e52.
16. Rees MJW, Taylor GI. A simplified lead oxide cadaver injectiontechnique. Plast Reconstr Surg 1986;77:141e5.

1098 K. Watanabe et al.
17. Beer GM, Lang A, Manestar M, et al. The bipedicle and bipartitelatissimus dorsi free and perforator flap: an anatomic study.Plast Reconstr Surg 2008;118:1162e70.
18. Hamdi M, Spano A, van landuty K, et al. The lateral intercostalartery perforators: anatomical study and clinical application inbreast surgery. Plast Reconstr Surg 2008;121:389e96.
19. Hamdi M, Van Landuty K, de Frene B, et al. The versatility ofthe inter-costal artery perforator (ICAP) flaps. J Plast ReconstrAesthet Surg 2006;59:644e52.
20. Schaverien M, Saint-Cyr M, Arbique G, et al. Three- and four-dimensional arterial and venous anatomies of the thoracodorsalartery perforator flap. Plast Reconstr Surg 2008;121:1578e87.
21. Tansini I. Sopra il mino nuovo processo di amputazion dellamammella. Gazz Med Ital 1906;57:141.
22. d’Este S. La technique de l’amputation la mammele pourcarcinone mammaire. Rev Chir (Paris) 1912;45:164.
23. Angrigiani C, Grillio D, Siebert J. Latissimus dorsi muscu-locutaneous flap without muscle. Plast Reconstr Surg 1995;96:1608e14.
24. Spinelli HM, Fink JA, Muzaffar AR. The latissimus dorsi perfo-rator-based faciocutaneous flap. Ann Plast Surg 1996;37:500e6.
25. Tobin GR, Schusterman M, Peterson GH, et al. The intramus-cular neurovascular anatomy of the latissimus dorsi muscle:the basis for splitting the flap. Plast Reconstr Surg 1981;67:637e41.
26. McGregor IA, Morgan G. Axial and random pattern flaps.Br J Plast Surg 1973;26:202e13.
27. Nakajima H, Maruyama Y, Koda E. The definition of vascularterritories with prostaglandin E1-the anterior chest,abdomen and thigh-inguinal region. Br J Plast Surg 1981;34:258e63.
28. Callegari PR, Taylor GI, Caddy CM, et al. An anatomical reviewof the delay phenomenon: experimental studies. PlastReconstr Surg 1992;89:397e407.
29. Taylor GI, Corlette RJ, Caddy CM, et al. An anatomical reviewof the delay phenomenon: clinical applications. Plast ReconstrSurg 1992;89:408e16.