Embed Size (px)
Citation preview

J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 3 , N O . 1 1 , 2 0 1 7
ª 2 0 1 7 B Y T H E A M E R I C A N CO L L E G E O F C A R D I O L O G Y F O U N DA T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 2 4 0 5 - 5 0 0 X / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c e p . 2 0 1 7 . 0 5 . 0 1 4
Analyses of the Mode of TerminationDuring Diagnostic Ventricular Pacingto Differentiate the Mechanisms ofSupraventricular Tachycardias
Mitsunori Maruyama, MD, PHD,a Shunsuke Uetake, MD, PHD,a Yasushi Miyauchi, MD, PHD,aYoshihiko Seino, MD, PHD,a Wataru Shimizu, MD, PHDb
ABSTRACT
FrobD
rel
All
ins
vis
Ma
OBJECTIVES The goal of this study was to determine the diagnostic yield of analyzing the mode of termination during
ventricular overdrive pacing (VOP) to differentiate the mechanisms of supraventricular tachycardias (SVTs).
BACKGROUND The majority of the diagnostic criteria for VOP rely on successful entrainment, but termination of SVTs
is common during VOP.
METHODS We studied 225 SVTs with a 1:1 atrioventricular relationship, including 34 atrial tachycardias, 67 orthodromic
reciprocating tachycardias (ORTs) (including 4 ORTs using accessory pathways [APs] with decremental properties), and
124 atrioventricular nodal re-entrant tachycardias. The total pacing prematurity (TPP) needed to reset or terminate
the SVT was calculated by using a simplified method, and the post-pacing interval minus the tachycardia cycle length
(PPI – TCL) was predicted from the TPP.
RESULTS VOP terminated 87 SVTs (39%). No atrial tachycardias were terminated by VOP in this study. SVT termination
occurred after (n ¼ 71) or before (n ¼ 16) atrial resetting. The predicted PPI – TCL was highly correlated with the
measured PPI – TCL (r ¼ 0.96; p < 0.001). The TPP had diagnostic accuracy equivalent to the predicted PPI – TCL.
The TPP was measurable irrespective of the termination mode and correctly diagnosed ORTs with decremental APs.
All ORTs using septal APs and no atrioventricular nodal re-entrant tachycardias had a TPP <125 ms. Considering other
criteria evaluable in terminated SVTs, a combined criteria of a TPP <125 ms and atrial capture/termination within the
fusion period were specific for ORTs using free-wall APs, except for left anterolateral/lateral sites.
CONCLUSIONS The termination analyses were useful for differential diagnoses of SVTs terminated during VOP.
(J Am Coll Cardiol EP 2017;3:1252–61) © 2017 by the American College of Cardiology Foundation.
A correct differential diagnosis of paroxysmalsupraventricular tachycardia (SVT) is of clin-ical importance because catheter ablation
now offers a definitive cure for the majority of SVTs.Ventricular overdrive pacing (VOP) during an SVT isa key maneuver to distinguish the SVT mechanism.The electrogram sequence upon cessation of the
m the aDepartment of Cardiovascular Medicine, Nippon Medical Scho
epartment of Cardiovascular Medicine, Nippon Medical School, Tokyo, J
ationships relevant to the contents of this paper to disclose.
authors attest they are in compliance with human studies committe
titutions and Food and Drug Administration guidelines, including patien
it the JACC: Clinical Electrophysiology author instructions page.
nuscript received February 9, 2017; revised manuscript received May 8, 2
VOP (an atrial–ventricular or atrial–atrial–ventricularresponse) is useful for diagnosing atrial tachycardias(ATs) (1). In addition, several criteria obtained fromVOP provide important clues to distinguish ortho-dromic reciprocating tachycardia (ORT) by usingaccessory pathways (APs) from atrioventricular nodalre-entrant tachycardia (AVNRT). These criteria
ol Chiba Hokusoh Hospital, Chiba, Japan; and the
apan. The authors have reported that they have no
es and animal welfare regulations of the authors’
t consent where appropriate. For more information,
017, accepted May 30, 2017.

AB BR E V I A T I O N S
AND ACRONYM S
AP = accessory pathways
AT = atrial tachycardia
AVNRT = atrioventricular
nodal re-entrant tachycardia
ORT = orthodromic
reciprocating tachycardia
PCL = pacing cycle length
PPI = post-pacing interval
RVA = right ventricular apex
SVE = septal para-Hisian
ventricular electrogram
SVT = supraventricular
tachycardia
TCL = tachycardia cycle length
TPP = total pacing prematurity
VA = ventriculo-atrial
VOP = ventricular overdrive
pacing
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 3 , N O . 1 1 , 2 0 1 7 Maruyama et al.N O V E M B E R 2 0 1 7 : 1 2 5 2 – 6 1 Termination Analyses for Diagnoses of SVTs
1253
include the difference between the stimulus–atrial in-terval and tachycardia ventriculo-atrial (VA) interval,the difference between the post-pacing interval andtachycardia cycle length (PPI – TCL) (2,3), the differ-ence in the His-atrial intervals during VOP and thetachycardia (4), a constant QRS fusion (5), and ortho-dromic His-bundle or septal ventricular capture (6).These criteria rely on successful entrainment; howev-er, termination of the SVT during VOP is common.
In contrast, some other VOP criteria, such as atrialcapture or tachycardia termination within the tran-sition zone of a QRS fusion (7), and the timing of theatrial capture relative to the advancement of theseptal para-Hisian ventricular electrogram (SVE) (8),were suggested to help differentiate ORT fromAVNRT even when the SVT was terminated duringVOP. However, it is not fully understood how effec-tively these criteria provide a final diagnosis of theterminated SVT. Recently, Kaiser et al. (9) showedthat PPI – TCL could be mathematically predicted ifVOP terminated the SVT after the resetting of theSVT. Furthermore, the pacing prematurity needed toreset or terminate an SVT may have a diagnostic valueequivalent to PPI – TCL (10), which is also potentiallyuseful in diagnosing terminated SVTs. The aim of thepresent study was to evaluate the diagnostic yield ofthe termination analyses in a cohort of patients withSVTs terminated during VOP.
METHODS
STUDY POPULATION. A total of 206 patients werestudied who presented to Nippon Medical SchoolChiba Hokusoh Hospital and Nippon Medical SchoolHospital for catheter ablation of SVT. The study wasapproved by our institutional review board. Patientswere included if they had SVTs with a 1:1 atrioven-tricular relationship and underwent VOP from theright ventricular apex (RVA) during the SVT at apacing cycle length (PCL) 10 to 40 ms shorter than theTCL. SVTs exhibiting spontaneous TCL oscillations>15 ms within 3 cycles before the onset of the VOPwere excluded from the study.
ELECTROPHYSIOLOGICAL STUDY AND CATHETER
ABLATION. After providing written informed con-sent, patients underwent an electrophysiologicalstudy that was performed under deep sedation.Twelve-lead surface electrocardiograms and intracar-diac electrograms from the high right atrium, coronarysinus, His-bundle region, and RVA were recorded anddigitally stored. All measurements were made by us-ing on-screen calipers. Intravenous isoproterenol(0.005 to 0.02 mg/kg/min) was administered if notachycardia was inducible or sustained at baseline.
When the sustained SVTs were terminatedduring VOP, multiple VOP attempts weremade, aiming at successful entrainment of theSVTs. The VOP results were classified as atermination response if the VOP terminatedthe SVT at least twice. Radiofrequency cath-eter ablation was performed with a nonirri-gated catheter for AVNRT and paraseptalAT/ORT or with an open-irrigated catheter fora nonseptal AT/ORT.DIAGNOSIS OF SVT. AT was diagnosed if theventricular activation was not linked to theatrial activation, which was demonstrated byatrial overdrive pacing from multiple atrialsites (differential atrial overdrive pacing)with a maximal difference in the post-pacingVA interval among the different atrial sites>20 ms (11). An atrial–atrial–ventricularresponse after VOP was considered diagnosticfor AT in a short-RP tachycardia but not in along-RP tachycardia because of the possibil-
ity of dual atrial responses (12). AT was excludedwhen any of the following were observed: 1) an atrial–ventricular response after VOP; 2) reproduciblespontaneous termination of the tachycardia withatrioventricular block; 3) occurrence of VA blockdespite perpetuation of the tachycardia; 4) tachy-cardia termination without capturing the atriumduring the VOP or ventricular extrastimulus; and 5)atrial cycle prolongation with atrial capture from aventricular extrastimulus (post-excitation).ORT was diagnosed if any of the following criteriawere satisfied: 1) an eccentric atrial activation duringthe tachycardia that was reproducible by ventricularpacing, with the earliest atrial activation beyond theleft posterolateral mitral annulus that excluded a“left-variant” AVNRT (13,14); 2) an increase in the VAinterval >20 ms with the development of ipsilateralbundle branch block (15); 3) resetting or reproducibletermination of the tachycardia with a ventricularextrastimulus applied when the His-bundle was re-fractory; 4) constant QRS fusion during VOP (5); 5)orthodromic His-bundle or septal ventricular captureduring VOP (6); 6) a PPI – TCL corrected by an atrio-ventricular nodal conduction delay <110 ms or astimulus–atrial interval minus tachycardia VAinterval <85 ms measured by VOP (2,3); and 7) ashorter His–atrial interval during the VOP than theHis–atrial interval during the tachycardia (4). ORTwas excluded if either spontaneous second-degreeatrioventricular block during the tachycardia or VAdissociation during VOP was observed.
AVNRT was diagnosed if the tachycardia wascapable of being induced and terminated by pacing,

Maruyama et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 3 , N O . 1 1 , 2 0 1 7
Termination Analyses for Diagnoses of SVTs N O V E M B E R 2 0 1 7 : 1 2 5 2 – 6 1
1254
and both AT and ORT were excluded. AVNRT wasconsidered typical when the septal VA intervalwas #70 ms and the earliest atrial activation was inthe His-bundle region.
A final diagnosis was made based on a combinationof the tachycardia features, results of diagnosticpacing maneuvers, and the outcome of the catheterablation.
TOTAL PACING PREMATURITY AND PREDICTION OF
PPI – TCL. We measured the prematurity of the pac-ing needed to first reset or terminate the tachycardiaas the total pacing prematurity (TPP). The TPP wasdefined as the sum of the prematurity of each stim-ulus (TCL - PCL) until the first atrial resetting ortachycardia termination, calculated by the TCL-PCLmultiplied by the number (n) of stimuli needed toreset the atrium or to terminate the tachycardia (9).
TPP ¼ nðTCL-PCLÞ ¼ nTCL� nPCL
To prevent a potential error from minor variationsin the TCL and coupling of the first stimulus, and tomake the calculation simpler, we directly measuredthe nTCL and nPCL with on-screen calipers as thesum of the TCL and PCL, respectively (TCLsum andPCLsum) (Figures 1 to 3).
PPI – TCL could be predicted by subtracting theamount of the tachycardia advancement during thefirst atrial reset from the TPP (9).
Predicted PPI � TCL¼ TPP � tachycardia advancement
To exclude spontaneous termination during theVOP, we confirmed the reproducibility of the tachy-cardia termination by repeating the VOP and did notanalyze the data if the atrial rate displayed a pro-gressive slowing before the tachycardia termination.
OTHER DIAGNOSTIC CRITERIA FOR A TERMINATED
TACHYCARDIA DURING VOP. We examined thepresence or absence of atrial capture or tachycardiatermination within the “transition zone,” which wasreported to be useful for the diagnosis of ORTseven when the tachycardia was terminated duringVOP (7). Here, the transition zone was defined as thetime period from the beginning of the VOP with fusedQRS complexes and the first paced complex with astable QRS morphology. The “fusion period” wasdefined as the time period with fused QRS complexesbut not including the first stable QRS complex(Figure 1).
The number of stable QRS complexes required toreset the tachycardia was also counted. A number ofstable QRS complexes #1 were shown to be diagnosticfor ORT, similar to the transition zone criterion (16).
It was reported that atrial capture simultaneouswith or before advancement of the SVE helpeddifferentiate ORT by using a septal AP from AVNRTwhen the tachycardia terminated during VOP (8).Thus, the differential response of the SVE and atriumwas analyzed in septal ORTs and AVNRTs (Figure 1).
STATISTICAL ANALYSIS. Continuous variables areexpressed as the mean � SD and were compared byusing the Student’s t-test. A 1-way analysis of variancecombined with a Bonferroni procedure was used formultiple comparisons, and the Fisher exact test wasused to analyze the categorical data. The correlationwas examined by using a Pearson’s correlation. Ap value <0.05 was considered statistically significant.
RESULTS
PATIENT CHARACTERISTICS. A total of 225 SVTs in206 patients (including 34 ATs, 67 ORTs, and 124AVNRTs) were studied. The baseline patient charac-teristics are shown in Table 1. Male sex was moreprevalent in the ORT patients than in the AVNRT andAT patients. The mechanisms of AT were re-entrantin 21 and non-re-entrant in 13. The origins of 19 ATswere paraseptal regions (adenosine-sensitive re-entrant AT arising from near the atrioventricular node[n ¼ 11] or coronary sinus ostium [n ¼ 3], and non-re-entrant focal septal AT [n ¼ 5]). Three ATs wererelated to previous cardiac surgery. The mean cyclelength of AT was longer than that of ORT or AVNRT.In the ORTs, the locations of the APs were septal in 14(8 right APs [2 superoparaseptal APs, 1 midseptal AP,and 5 posteroseptal APs] and 6 left posteroseptalAPs), left free-wall in 48 (1 anterior APs, 13 antero-lateral APs, 21 lateral APs, 7 posterolateral APs, and 6posterior APs), and right free-wall in 5 (1 anterior AP,2 anterolateral APs, and 2 lateral APs). Four APs had adecremental conduction property, defined as a VAinterval during the tachycardia >40% of the TCL (17)(1 septal AP and 3 free-wall APs). Eighty-fiveAVNRTs were typical (slow–fast form) and 39 wereatypical (23 fast–slow form and 16 slow–slow form).
RESPONSES OF SVT TO VOP. Of 225 SVTs, VOPresulted in successful entrainment with 1:1 VA con-duction in 103 (46%), VA dissociation in 35 (15%), andtermination of the tachycardia in 87 (39%). Althoughthe TCL-PCL was similar among ORT, AVNRT, and AT,the responses to VOP substantially differed accordingto the cause of the SVT (Table 1). Because the ventricleis a critical part of ORT, VA dissociation neveroccurred with VOP during the ORT. VA dissociationwas frequently observed in ATs (85%) but was alsoseen in some AVNRTs (5%). In 55% of the ORT cases

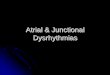
FIGURE 1 Measurements of the TPP and Other Diagnostic Criteria for SVTs Terminated During VOP
Tachycardia termination was classified into 2 types (type 1: termination after an atrial reset; type 2: termination without any perturbation of the
atrial cycle). The total pacing prematurity (TPP) was calculated as the difference between the sum of the tachycardia cycle length (TCLsum) and
pacing cycle length (PCLsum) until the atrium was captured (red) in type 1 or the tachycardia was terminated in type 2. The fusion period
indicates the time period with fused QRS complexes (F). The transition zone indicates the fusion period plus the first stable QRS complex (SM1).
The septal ventricular electrogram (SVE) was defined as the ventricular electrograms recorded in the His bundle region. Typical responses in
orthodromic reciprocating tachycardia (ORT) include atrial capture or termination within the fusion period and transition zone, simultaneous
with or before the SVE advancement (blue). In atrioventricular nodal re-entrant tachycardia (AVNRT) or atrial tachycardia (AT), atrial capture
typically occurs after the fusion period, transition zone, and SVE advancement. Termination after the fusion period, transition zone, and SVE
advancement suggests AVNRT with type 2 termination that excludes AT. The text provides additional details. ECG ¼ electrocardiogram;
HBE ¼ His-bundle electrogram; HRA ¼ high right atrium; RVA ¼ right ventricular apex; SVT ¼ supraventricular tachycardia; VOP ¼ ventricular
overdrive pacing.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 3 , N O . 1 1 , 2 0 1 7 Maruyama et al.N O V E M B E R 2 0 1 7 : 1 2 5 2 – 6 1 Termination Analyses for Diagnoses of SVTs
1255

FIGURE 2 Type 1 Termination in an ORT With a Right Posteroseptal AP
Shown are surface lead I, intracardiac bipolar electrograms recorded from the HRA, coronary sinus (CS), HBE, and RVA in ORT terminated during
VOP. In this example, the tachycardia termination occurred after the atrium was reset (type 1 termination) with the third ventricular stimulus
(S3). The TCLsum was measured with a digital caliper as a total of 3 atrial cycle lengths immediately before the atrial resetting, whereas the
PCLsum was measured as 3 pacing intervals (the interval from the ventricular electrogram just before the initiation of pacing to the resetting
stimulus [S3]). The TPP was simply calculated by subtracting the PCLsum from the TCLsum (1,110 ms�1,020 ms ¼ 90 ms). The amount of
tachycardia advancement at the first atrial reset was 20 ms. Predicted PPI – TCL was calculated as the TPP minus the tachycardia advancement
(90 ms�20 ms ¼ 70 ms). AP ¼ accessory pathway; Stim ¼ stimulus marker; other abbreviations as in Figure 1.
Maruyama et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 3 , N O . 1 1 , 2 0 1 7
Termination Analyses for Diagnoses of SVTs N O V E M B E R 2 0 1 7 : 1 2 5 2 – 6 1
1256
and 40% of AVNRT cases, the tachycardia terminatedduring the VOP. The VOP terminated 3 (75%) of 4ORTs with a decremental AP. There were no ATs thatterminated during the VOP. Hence, either ORT orAVNRT was responsible for the SVTs terminated byVOP in the subjects of this study.
FIGURE 3 Type 2 Termination in an ORT With a Left Anterior Decre
This example shows that the tachycardia was terminated without atrial
overdrive pacing (S4). The TCLsum and PCLsum were measured as the sum o
(TCLsum 1,120 ms – PCLsum 1,020 ms). Abbreviations as in Figures 1 and
Two modes of tachycardia termination wereobserved: 1) termination after an atrial reset (type 1:n ¼ 71 [82%]) (Figure 2); or 2) termination without anyperturbation of the atrial cycle (type 2: n ¼ 16 [18%])(Figure 3). During 3.1 � 1.2 (range: 2 to 7) attempts ofVOP, the type of termination was consistent in 34
mental AP
resetting (type 2 termination) after the fourth stimulus of ventricular
f 4 TCLs and 4 pacing intervals, respectively, and the TPP was 100 ms
2.

TABLE 1 Baseline Characteristics of the Study Patients
ORT (n ¼ 67) AVNRT (n ¼ 124) AT (n ¼ 34) p Value
Age, yrs 51 � 17 55 � 15 54 � 20 NS
Male 43 (64)* 40 (32) 11 (32) <0.01
Type of tachycardia Septal AP: 14 (21)Free-wall AP: 53 (79)
Typical: 85 (69)Atypical: 39 (31)
Re-entrant: 21 (62)Non-re-entrant: 13 (38)
TCL, ms 353 � 71 338 � 59 502 � 162† <0.01
TCL-PCL, ms 20 � 8 22 � 8 21 � 11 NS
Responses to VOP
1:1 VA conduction 30 (45)‡ 68 (55)§ 5 (15) <0.01
VA dissociation 0 6 (5) 29 (85)k <0.01
Termination 37 (55) 50 (40) 0¶ <0.01
Values are mean � SD or n (%). *p < 0.01 versus atrioventricular nodal re-entrant tachycardia (AVNRT) and atrialtachycardia (AT). †p < 0.01 versus orthodromic reciprocating tachycardia (ORT) and AVNRT. ‡p < 0.05 versusAT. §p < 0.01 versus AT. kp < 0.01 versus ORT and AVNRT. ¶p < 0.01 versus ORT and AVNRT.
AP ¼ accessory pathway; TCL ¼ tachycardia cycle length; TCL-PCL ¼ the difference between the TCL andpacing cycle length; VOP ¼ ventricular overdrive pacing; VA ¼ ventriculoatrial.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 3 , N O . 1 1 , 2 0 1 7 Maruyama et al.N O V E M B E R 2 0 1 7 : 1 2 5 2 – 6 1 Termination Analyses for Diagnoses of SVTs
1257
(39%) SVTs, both types of termination were observedin 5 (6%) SVTs, and successful entrainment wasfinally obtained in 48 (55%) SVTs. Either type oftermination was observed when the tachycardia wasterminated with conduction block in the retrogradelimb (type 1 [n ¼ 17], type 2 [n ¼ 16]), whereasonly type 1 termination occurred when the tachy-cardia was terminated with conduction block in theanterograde limb (n ¼ 54). In ORTs with a decre-mental AP, all the terminations were type 2, whereasonly 3 (9%) of 34 ORTs with a nondecremental APexhibited type 2 termination (p < 0.01). In AVNRT,the incidence of type 2 termination was higherin atypical AVNRTs than in typical AVNRTs (54% vs.8%; p < 0.01).
PREDICTED PPI – TCL. PPI – TCL was able to be pre-dicted by the formula shown in the Methods section ifthe SVT was successfully entrained or terminatedafter atrial resetting (i.e., 1:1 VA conduction or type 1termination). Figure 4A shows a correlation betweenthe predicted PPI – TCL and measured PPI – TCLcorrected by an atrioventricular nodal conductiondelay (3) in 103 successfully entrained SVTs. Thepredicted PPI – TCL was highly correlated with thecorrected PPI – TCL derived from actual measure-ments (r ¼ 0.96; p < 0.001).
In 71 SVTs with type 1 termination during VOP,all AVNRT cases had a predicted PPI – TCL >110 ms(range: 132 to 286 ms), and all ORT cases usinga septal AP had a predicted PPI – TCL <110 ms(range: 25 to 94 ms) (Figure 4B), as in the previousstudy identifying a measured corrected PPI – TCL>110 ms in AVNRTs and <110 ms in septal ORTs (3).Seven of 22 ORT cases with type 1 termination usinga left free-wall AP (4 left anterolateral APs, 1 leftlateral AP, and 2 left posterolateral APs) had apredicted PPI – TCL >110 ms, probably because theselocations of the AP were relatively remote from thepacing site, at the RVA. The prediction of PPI – TCLwas not feasible in ORT using a decremental APbecause all of them exhibited type 2 termination(Figure 3).
TPP. The predicted PPI – TCL was not available fortype 2 termination, whereas the calculation of theTPP was possible independently of the type oftachycardia termination. In 87 SVTs terminated dur-ing VOP, all AVNRT cases had a TPP >125 ms (range:140 to 331 ms), and all ORT cases using a septal AP hada TPP <125 ms (range: 40 to 104 ms) (Figure 5). Similarto PPI – TCL, 9 of 26 terminated ORT cases using a leftfree-wall AP (4 left anterolateral APs, 3 left lateralAPs, and 2 left posterolateral APs) had a TPP >125 ms.
The TPP results were consistent within the same SVTeven when different responses to VOP were observedduring multiple VOP attempts.
COMPARISONS OF THE DIAGNOSTIC PERFORMANCE
AMONG THE CRITERIA FOR ORT IN TERMINATED
SVT. The present study confirmed that the criterion(atrial capture or tachycardia termination within thetransition zone) had a favorable sensitivity andspecificity for a diagnosis of ORT (Table 2). Thenumber of stable QRS complexes required to resetthe tachycardia was 0.5 � 0.7 in ORT and 3.7 � 1.9in AVNRT (p < 0.01). The diagnostic yield of thecriterion (the number of stable QRS complexes #1)was substantially the same as the transition zonecriterion for a diagnosis of ORT. These criteria werenot diagnostic for ORTs due to 11 false-positivesin AVNRT cases (Figure 6). Because all the false-positives in the AVNRT cases exhibited atrial cap-ture at the timing of the first stable QRS complex,the criteria redefined as atrial capture or tachycardiatermination within the fusion period, and theabsence of a stable QRS complex, were specific forORT, although the sensitivity was substantiallydiminished.
Calvo et al. (8) reported that atrial capture simul-taneous with or preceding the SVE advancement wasspecific for ORT using a septal AP. Because this cri-terion is not applicable to ORT using a free-wall AP,its availability was limited. Of 14 septal ORTs, 6 false-negatives were noted (5 left posteroseptal APs and 1right posteroseptal AP with a decremental conductionproperty). When combined with other criteria, anadditional diagnostic yield by using the SVE criterioncould not be found.

FIGURE 5 TPP in All SVT Cases Terminated During the VOP
Note that a cutoff level (125 ms) distinguished ORT using a septal
AP and AVNRT, as with PPI – TCL. Some ORTs using a left free-
wall AP displayed a TPP >125 ms. Abbreviations as in Figures 1
and 2.
FIGURE 4 Predicted PPI – TCL
(A) A high correlation between the measured corrected PPI – TCL and predicted PPI – TCL in SVTs with successful entrainment. (B) Predicted
PPI – TCL in SVTs with type 1 termination. Because the AT was not terminated by the VOP, the data from SVTs other than AT (ORT using a septal
or free-wall AP and AVNRT) are shown. The text provides additional details. Abbreviations as in Figures 1 and 2.
Maruyama et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 3 , N O . 1 1 , 2 0 1 7
Termination Analyses for Diagnoses of SVTs N O V E M B E R 2 0 1 7 : 1 2 5 2 – 6 1
1258
When the TPP criterion was combined with thecriterion of the fusion period (or no stable QRS com-plex), the sensitivity for diagnosing ORT was maxi-mized, although it remained specific (Table 2). Allfalse-negatives with the combined criteria wereobserved in patients with ORTs using an AP beyondthe left posterolateral mitral annulus (6 anterolateralAPs and 7 lateral APs) that did not require a differ-entiation from AVNRT.
DISCUSSION
Because the RVA is closer to the re-entrant circuit ofORT, PPI – TCL measured at the RVA should be asmaller value in ORT than it would for AVNRT orAT. A corrected PPI – TCL <110 ms is specific forORT (3), but it cannot be measured when VOP ter-minates the SVT. The incidence of SVT terminationduring VOP is reported to be 8% to 56% (7,8,16,18)and was 39% in this study. As shown in a recentstudy (9), PPI – TCL was accurately predicted,provided that the atrium was reset during VOP.Thus, the prediction of PPI – TCL is feasible whenthe mode of the SVT termination is type 1, and itsdiagnostic values in the terminated SVT are consis-tent with the values in the SVT that is successfully

TABLE 2 Performance of Ventricular Overdrive Pacing Maneuvers for Diagnosing ORT in
All the Study Patients
Availabilityof Criteria Sensitivity Specificity PPV
Atrial capture or tachycardia terminationwithin the transition zone (7)
84 91 91 85
Atrial capture or tachycardia terminationwithin the fusion period
84 58 100 100
Atrial capture simultaneous with or beforeSVE advancement (8)
61 57 100 100
TPP <125 ms 84 75 100 100
Atrial capture or tachycardia terminationwithin the fusion period or TPP <125 ms
84 81 100 100
Values are %.
ORT ¼ orthodromic reciprocating tachycardia; PPV ¼ positive predictive value; SVE ¼ septal ventricularelectrogram; TPP ¼ total pacing prematurity.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 3 , N O . 1 1 , 2 0 1 7 Maruyama et al.N O V E M B E R 2 0 1 7 : 1 2 5 2 – 6 1 Termination Analyses for Diagnoses of SVTs
1259
entrained (2,3). Furthermore, we found that the TPP,obtained by using our simplified method, had a diag-nostic value similar to PPI – TCL for the ORT diagnosis,but the TPP was measurable irrespective of the modeof the SVT termination. Bennett et al. (17) describedthat the PPI – TCL criterion was invalid in approxi-mately 50% of ORT cases with a decremental APbecause a conduction delay in the AP caused aprolongation of PPI – TCL. In this study, 3 of 4 ORTswith a decremental AP displayed type 2 terminationduring VOP, in which a conduction block in the APwas responsible for the tachycardia termination.Interestingly, the TPP correctly differentiated all theORTs with decremental APs. This finding suggeststhat the TPP might be less affected by a decrementalconduction property because it should reflect thecharacteristics of the conducting path from the pacingsite to the tachycardia circuit rather than that of thetachycardia circuit itself. Figure 7 represents howthe TPP and PPI – TCL were demonstrated in SVTs witha prominent decremental conduction property inthe retrograde limb of the tachycardia circuit. Thisexample exhibits a prolongation of the atrial cycle atthe first atrial reset (i.e., post-excitation), resulting ina longer predicted PCL-TCL than the TPP. Hence, theTPP might be a better criterion than PPI – TCL in ORTsusing decremental APs.
Atrial capture or tachycardia termination withinthe transition zone and a number of stable QRScomplexes #1 correctly diagnosed the majority ofORTs even when VOP terminated the SVT. However,because atrial capture was also observed at thetiming of the first stable QRS complex in 11 (9%)AVNRTs (Figure 6), we could not make a definitivediagnosis by using only the transition zone criterion.In agreement with our results, the later study notedatrial resetting within the transition zone in 6% to7% of AVNRT cases (18). Excluding the first stableQRS complex from the transition zone (i.e., fusionperiod without any stable QRS complexes) made thecriteria diagnostic for ORT. However, a modificationof the criteria lowered their sensitivity to 58%.When the modified criteria were combined with theTPP criterion, the sensitivity for diagnosing ORTincreased to 81% with a 100% specificity (Table 2).The combined criteria did not make a correct diag-nosis only in ORT with a left anterolateral or leftlateral AP. In general, the differential diagnosisbetween AVNRT and ORT with this location of theAP has little problem, because a left deviation ofthe atrioventricular node does not exceed theposterolateral mitral annulus (13,14). In addition,the combined criteria were available unless VA
dissociation occurred during the VOP. Because VAdissociation excludes ORT, inclusion of the termi-nation analysis in the diagnostic evaluation wouldallow us to practically distinguish most ORTs fromthe other SVTs.
In the present series, VOP did not terminate AT. Asa general rule, AT is excluded when the tachycardia isterminated without atrial resetting (i.e., type 2termination). Thus, a TPP >125 ms diagnoses AVNRTwith type 2 termination. In contrast, if the tachy-cardia is terminated after atrial resetting (i.e., type 1termination), AT may underlie the mechanism of theSVT. Nonetheless, our results show that VOP rarelyterminates AT, suggesting that the occurrence of thetachycardia termination by VOP per se support adiagnosis other than AT.
STUDY LIMITATIONS. This study was retrospectivein design, and the diagnostic criteria have not beenevaluated prospectively. Although inaccurate resultswere observed exclusively in the left anterolateraland left lateral free-wall APs in this study, diagnosisusing termination analyses has potential limitationsin ORTs with APs remote from the pacing site.Furthermore, the number of ORTs with decrementalAPs in our study was too small. Hence, a long TPPshould be interpreted with caution if it conflictswith other electrophysiological findings. Our resultsare not applicable to SVTs terminated spontaneouslyduring VOP. For that reason, we only included SVTsthat were sustained at least before the VOP andwere terminated reproducibly by VOP. Moreover,cases with a gradual lengthening of the TCL justbefore the tachycardia termination were notanalyzed to avoid an incidental termination duringthe VOP.

FIGURE 7 Entrainment of a Fast–Slow Form AVNRT With VOP
Upon cessation of pacing, a pseudo atrial–atrial–ventricular response was observed due to a prominent decremental conduction in the
retrograde limb of the re-entrant circuit. The atrial cycle was prolonged at the first resetting, whereby the predicted PPI – TCL (173 ms) became
longer than the TPP (151 ms). Furthermore, the measured corrected PPI – TCL (211 ms) was longer than the predicted PPI – TCL, which may be
attributable to a greater conduction delay during successive paced beats after the first resetting. Abbreviations as in Figure 1.
FIGURE 6 Atrial Capture Within the “Transition Zone” in Typical AVNRT With Type 1 Termination
The atrium was reset with the seventh ventricular stimulus when the QRS morphology first became stable (asterisk). Thus, the atrial resetting
occurred beyond the “fusion period” but within the “transition zone” by its definition. The TPP was 158 ms (TCLsum 2,534 ms – PCLsum 2,376 ms),
which was compatible with AVNRT. Abbreviations as in Figure 1.
Maruyama et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 3 , N O . 1 1 , 2 0 1 7
Termination Analyses for Diagnoses of SVTs N O V E M B E R 2 0 1 7 : 1 2 5 2 – 6 1
1260

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: An electro-
physiological diagnosis of SVT may be challenging when the SVT
is terminated during diagnostic pacing. The termination analyses
help differentiate the SVT mechanisms and facilitate a
successful ablation.
TRANSLATIONAL OUTLOOK: Prospective evaluations in a
large-scale cohort are needed to establish the utility of the
termination analyses for differential diagnoses of SVTs
terminated during diagnostic pacing.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 3 , N O . 1 1 , 2 0 1 7 Maruyama et al.N O V E M B E R 2 0 1 7 : 1 2 5 2 – 6 1 Termination Analyses for Diagnoses of SVTs
1261
CONCLUSIONS
The termination analyses are useful for differentialdiagnoses of SVTs terminated during VOP. VOP rarelyterminates AT. Combining the TPP with the modifiedresetting criteria during VOP accurately distinguishedORT from the other SVTs.
ACKNOWLEDGMENT The authors thank Mr. JohnMartin for his linguistic assistance with the manuscript.
ADDRESS FOR CORRESPONDENCE: Dr. MitsunoriMaruyama, Department of Cardiovascular Medicine,Nippon Medical School, Chiba Hokusoh Hospital, 1715Kamakari, Inzai-city, Chiba 2701694, Japan. E-mail:[email protected].
RE F E RENCE S
1. Knight BP, Zivin A, Souza J, et al. A techniquefor the rapid diagnosis of atrial tachycardia in theelectrophysiology laboratory. J Am Coll Cardiol1999;33:775–81.
2. Michaud GF, Tada H, Chough S, et al. Differen-tiation of atypical atrioventricular node re-entranttachycardia from orthodromic reciprocatingtachycardia using a septal accessory pathway bythe response to ventricular pacing. J Am CollCardiol 2001;38:1163–7.
3. Gonzalez-Torrecilla E, Arenal A, Atienza F, et al.First postpacing interval after tachycardiaentrainment with correction for atrioventricularnode delay: a simple maneuver for differentialdiagnosis of atrioventricular nodal reentranttachycardias versus orthodromic reciprocatingtachycardias. Heart Rhythm 2006;3:674–9.
4. Ho RT, Mark GE, Rhim ES, Pavri BB,Greenspon AJ. Differentiating atrioventricularnodal reentrant tachycardia from atrioventricularreentrant tachycardia by DeltaHA values duringentrainment from the ventricle. Heart Rhythm2008;5:83–8.
5. Ormaetxe JM, Almendral J, Arenal A, et al.Ventricular fusion during resetting and entrain-ment of orthodromic supraventricular tachy-cardia involving septal accessory pathways.Implications for the differential diagnosis withatrioventricular nodal reentry. Circulation 1993;88:2623–31.
6. Nagashima K, Kumar S, Stevenson WG, et al.Anterograde conduction to the His bundle duringright ventricular overdrive pacing distinguishesseptal pathway atrioventricular reentry fromatypical atrioventricular nodal reentrant tachy-cardia. Heart Rhythm 2015;12:735–43.
7. AlMahameed ST, Buxton AE, Michaud GF. Newcriteria during right ventricular pacing to deter-mine the mechanism of supraventricular tachy-cardia. Circ Arrhythm Electrophysiol 2010;3:578–84.
8. Calvo D, Avila P, Garcia-Fernandez FJ, et al.Differential responses of the septal ventricle andthe atrial signals during ongoing entrainment: amethod to differentiate orthodromic reciprocatingtachycardia using septal accessory pathways fromatypical atrioventricular nodal reentry. CircArrhythm Electrophysiol 2015;8:1201–9.
9. Kaiser DW, Hsia HH, Dubin AM, et al. The pre-cise timing of tachycardia entrainment is deter-mined by the postpacing interval, the tachycardiacycle length, and the pacing rate: theoretical in-sights and practical applications. Heart Rhythm2016;13:695–703.
10. Maruyama M, Yamamoto T, Abe J, et al.Number needed to entrain: a new criterion forentrainment mapping in patients with intra-atrialreentrant tachycardia. Circ Arrhythm Electro-physiol 2014;7:490–6.
11. Maruyama M, Kobayashi Y, Miyauchi Y, et al.The VA relationship after differential atrial over-drive pacing: a novel tool for the diagnosis of atrialtachycardia in the electrophysiologic laboratory.J Cardiovasc Electrophysiol 2007;18:1127–33.
12. Ho RT, Frisch DR, Pavri BB, Levi SA,Greenspon AJ. Electrophysiological featuresdifferentiating the atypical atrioventricular node-dependent long RP supraventricular tachycardias.Circ Arrhythm Electrophysiol 2013;6:597–605.
13. Otomo K, Okamura H, Noda T, et al. “Left-variant” atypical atrioventricular nodal reentrant
tachycardia: electrophysiological characteristicsand effect of slow pathway ablation within coro-nary sinus. J Cardiovasc Electrophysiol 2006;17:1177–83.
14. Lockwood D, Nakagawa H, Jackman WM.Electrophysiologic characteristics of atrioventric-ular nodal reentrant tachycardia: implications forreentrant circuits. In: Zipes DP, Jalife J, editors.Cardiac Electrophysiology: From Cell to Bedside.5th ed. Philadelphia, PA: Saunders, 2009:615–46.
15. Knight BP, Ebinger M, Oral H, et al. Diagnosticvalue of tachycardia features and pacing maneu-vers during paroxysmal supraventricular tachy-cardia. J Am Coll Cardiol 2000;36:574–82.
16. Dandamudi G, Mokabberi R, Assal C, et al.A novel approach to differentiating orthodromicreciprocating tachycardia from atrioventricularnodal reentrant tachycardia. Heart Rhythm 2010;7:1326–9.
17. Bennett MT, Leong-Sit P, Gula LJ, et al.Entrainment for distinguishing atypical atrioven-tricular node reentrant tachycardia from atrioven-tricular reentrant tachycardia over septal accessorypathways with long-RP tachycardia. Circ ArrhythmElectrophysiol 2011;4:506–9.
18. Rosman JZ, John RM, Stevenson WG, et al.Resetting criteria during ventricular overdrive pac-ing successfully differentiate orthodromic reentranttachycardia from atrioventricular nodal reentranttachycardia despite interobserver disagreementconcerning QRS fusion. Heart Rhythm 2011;8:2–7.
KEY WORDS ablation, diagnosis,orthodromic reciprocating tachycardia,supraventricular tachycardia