Embed Size (px)
Citation preview

Brit. J. industr. Med., I966, 23, 83
The Anaemia of Lead Poisoning: A ReviewH. A. WALDRON
From the Medical Department, Vauxhall Motors Ltd., Luton, Beds.*
Lead intoxication has been recognized as a clinical entity since ancient times. Hippocrates (370 B.C.)was probably the first person to associate lead with clinical symptoms, since when the harmful effects oflead on the body have been well documented. Early observations culminated in the brilliant monographof Tanquerel des Planches (I839) in which the clinical aspects of the disease were completely outlined andmost of the early signs of the disease were mentioned. So complete was this work that virtually nothinghas been added to des Planches's observations since their publication.The earliest reference to lead anaemia was made in I83I by Laennec, who described thinness of the
blood and pallor of the tissues in cases of lead poisoning at necropsy. The first direct evidence of the effectof lead on red blood cells was presented by Andral and Gavarret (I840), who counted the number of redblood cells in cases of lead poisoning and found the count to be much lower than normal.
Since these early reports a great deal of work has been undertaken to try to discover the means by whichlead causes anaemia, but it is probably true to say that at the present time this mechanism is still not fullyunderstood. This review is an attempt to draw together at least some of the theories which have beenadvanced in the past and to present them, it is hoped, in an easily accessible manner for future workers inthis field.
Classification
The anaemia of lead poisoning is seldom severe,the haemoglobin level rarely falling below 6o% orthe red cell count below 4 x 106/c.mm. (Cantarowand Trumper, I944). There is a considerable varia-tion in the haemoglobin levels reported in theliterature in cases of lead poisoning but the anaemiais usually said to be hypochromic. Thus Griggs(I964), in a study of 20 men with lead poisoning,found the anaemia to be mild and hypochromic withmany reticulocytes and stippled cells present,although there was no correlation between thenumbers of these cells and the degree of anaemia.
Saita, Fiocchi, and Cattaneo (I952) made anextensive study of 41 cases of lead poisoning as aresult of which they were able to classify the anaemiainto three categories. In the pre-cinical stage theanaemia was normocytic and normochromic withhypochromia developing in the acute stage of thedisease. A few patients in the acute stage tended todevelop macrocytosis but as the disease moved intoa chronic stage, half the patients had a macrocytic,hypochromic anaemia. In the other half the
* Present address: 7 Elm Court, go Alcester Road,Moseley, Birmingham, I3.
Received for publication October 6, I965.
anaemia remained normocytic and normochromic.In children the anaemia is usually more severe and
more pronouncedly microcytic and hypochromic,perhaps because lead poisoning in children is oftenassociated coincidentally with a nutritional iron-deficiency disease (Watson, Decker, and Lichtman,I958).The anaemia of lead poisoning has many of the
characteristics of thalassaemia from which it must becarefully differentiated. This is of particular im-portance in the Mediterranean countries where theincidence of thalassaemia is high. Most of the workin this connexion has been carried out in France orItaly (Saita and Moreo, 1959; Roche, Lejeune,Tolot, Mouriquand, Baron, Goineau, and Soubrier,I960; Gaultier, Fournier, and Gervais, I962;Gerard, Guerrin, and Roussel, I964). Differentia-tion between the two states lies mainly in demon-strating the presence ofhaemoglobin A2. In patientswith thalassaemia this may be present in amountsup to io% whereas in the normal adult this type ofhaemoglobin amounts to less than 3%. Largeamounts (40 to 90%) of foetal haemoglobin (Hb F)are also present in thalassaemia. There have beenreports that Hb F is also found in cases of humanlead poisoning and in lead-poisoned rabbits(Buczkowski, I964), but Lovisetto, Sibour, and
83
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

Turco (I957) were unable to find it in I4 cases ofplumbism, and Wolman and Bongiovanni (I956) intheir review considered that only the normal adulthaemoglobin (Hb A) was present in lead poisoning.A finding of excessive urinary coproporphyrinexcretion will distinguish the patients with leadpoisoning from those with thalassaemia.Lead anaemia has many of the features of a
typical sideroblastic anaemia listed by MacGibbonand Mollin (I965), for example hypochromia, im-paired maturation and defective haemoglobinizationof red cells, raised serum iron, rapid plasma ironclearance with decreased cell uptake of 59Fe, anderythroblasts containing iron-staining inclusionbodies (sideroblasts). It is classified as a sidero-blastic anaemia by Mollin (I965).
Effects of Lead on Circulating Red Cells
Osmotic Fragility A great deal of the earlywork on the pathogenesis of the anaemia of leadpoisoning was carried out by Aub and his colleaguesand reported in a series of classic papers (Aub,Reznikoff, and Smith, 1924; Aub, Minot, Fairhall,and Reznikoff, I924; Aub, Fairhall, Minot, andReznikoff, I925; 1926). These authors found thatnormal washed or defibrinated red cells became moreresistant to hypotonic saline after exposure to leadchloride solution. Cells that had been exposed tosolutions of lead of concentrations as high as onepart per ioo,ooo did not haemolyse in o-I% salinewhereas normal cells were completely haemolysed in0-25% saline.These observations on the effects of lead on the
osmotic fragility of the red cell have been almostunanimously corroborated. Indeed the only dis-senting voice seems to be that of Sroczyn'ski whoinduced chronic and acute lead poisoning in rabbitsby injecting a o9% solution of alkaline lead acetateinto the marginal vein of the ear (Sroczynski, I959,I963) and found that red cells from both groups ofanimals showed a marked decrease in resistance tohypotonic saline solutions. The resistance wasdecreased more markedly in the acute group than inthe chronic group. Many other authors, however,have recorded a normal or increased resistance tohypotonic saline solutions (Pearse, I926; Velicogna,1933; Fullerton, 1952; Baron, 1954; Harris andGreenberg, I954; Crepet, Rubino, and Gobbato,I956; Rubino, Prato, and Fiorina, I956; Clarksonand Kench, I958b; Griggs and Harris, I958;Tishkoff, Granville, Rosen, and Dameshek, I958),and the findings of Aub and his colleagues may betaken as being well confirmed.
Fullerton (1952), in her study of eight patientswith plumbism, found that quantitative changes in
fragility curves were altered pari passu with anincrease in punctate basophil counts, but thisobservation has not been confirmed since. Thechanges in osmotic fragility induced by lead are, onthe whole, slight, although the osmotic fragility ofleaded red cells is more increased after sterile incu-bation for 24 hours (Harris, I963; Griggs, I964;Waldron, I964).The mechanism by which lead causes osmotic
changes in red cells is not as yet understood. Leadaffects the cation permeability of the cell membraneresulting in increased potassium loss (Joyce, Moore,and Weatherall, I954; Vincent and Blackburn,1958). At concentrations of ioo JM/l., K+ loss ismuch increased, the effect decreasing with time(Passow and Tillmann, I955). It is thought that theincreased osmotic resistance may indicate that morewater could enter the cells before a critical spheroidalform is reached and lysis occurs (Griggs, I964), andit may be possible to equate the changes in osmoticfragility with the alterations in permeability sincechanges in permeability may affect the waterrelations of the cell.
Mechanical Fragility Although Aub and hiscolleagues found that the osmotic fragility of theleaded red cell was decreased, they found, by con-trast, that the mechanical fragility was much in-creased. Thus, when leaded red cells were rotatedin a tonometer or centrifuged, haemolysis due to therolling of the red cells on the glass was markedlyincreased compared with normal red cells similarlytreated. Shaking the cell suspensions in a shakingmachine gave similar results. This double action oflead-decreasing the osmotic fragility whilst in-creasing the mechanical fragility-had also beenseen by Fici (I920, I92Ia and b).From their observations Aub et al. concluded that
leaded red cells were less able to withstand thedynamic trauma consequent upon passage throughthe capillaries and so broke up more readily thannormal cells, giving rise to the anaemia seen in leadpoisoning. This conclusion was in accord with thegeneral concensus of opinion at the time, since earlywork by Heubel (I87I) and Bouchard (I873), laterconfirmed by Rauch (I922), had indicated that leadanaemia was due to the destruction of circulating redcells.Aub and Reznikoff (1924) proposed that the
damage to the red cell envelope which broughtabout the increased mechanical fragility was causedby the liberation of free acid when lead combinedwith the inorganic phosphate of the red cells orplasma according to the following equation3PbCl2 + 2Na2HPO4 =
Pb3(PO4)2 + 4NaCl + 2HCI.
84 H. A. Waldron
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

The Anaemia of Lead Poisoning: A Review
This hypothesis was challenged by Maxwell andBischoff (1929a and b) after they had observedchanges in red cells after exposure to lead similar tothose described by Aub et al. but without theliberation of free acid. Maxwell and Bischoffbelieved that the injury to the cells might be due tothe formation of lead diglycerophosphate which ismore active than the tertiary phosphate. Morerecent work by Clarkson and Kench (1958a) hasindicated that lead interacts with red cells in a pro-cess involving the coagulation and flocculation of apeptized lead phosphate sol on the cell membrane.
Since Aub's original reports there has been aconsiderable division of opinion on the effect of leadon the mechanical fragility of the red cell. Goldblattand Goldblatt (I956) were of the opinion that thefall in numbers of red cells in lead poisoning wasalmost certainly due, in part at least, to an effect ofthe metal ion on the red cell envelope rendering itdeformed and more vulnerable to mechanical injury.Teisinger, Zumanova, and Zezula (1958) also statedthat the anaemia was caused by haemolysis due tothe action of lead on the cell membrane, butClarkson and Kench (I958b) concluded from theirstudies that in vivo lead would be unlikely to producedetectable damage to the circulating red cell due,they thought, to the protective action of excessphosphate in the plasma. They were of the opinionthat any damage caused to the red cells by leadwould be confined entirely to the formative stagesin the bone marrow. Baron (1954) found themechanical fragility of the red cells to be normal inIO cases of lead poisoning, and this was also thefinding of Rubino et al. (1956) in the i6 patientsthey studied. Sutherland and Eisentraut (1956)induced chronic plumbism in dogs by intraperi-toneal injection of lead acetate, and they noticed anincrease in mechanical fragility although this wasnot correlated with the degree of anaemia presentnor with the results of Coombs' test.An increase in mechanical fragility was reported
in cases of human plumbism by Harris and Green-berg (1954) and by Fratianne, Griggs, and Harris(I959), but later Griggs (I964) showed that themechanical fragility in IO patients with lead poison-ing did not vary considerably from the normal range.de Kretser and Waldron (I963) determined themechanical fragility index in a group of 68 leadworkers and found that the cells from these indi-viduals tended to be less fragile than normal.The reports of Harris and Greenberg (I954) and
Fratianne et al. (1959) do not contain experimentaldetails, and it is not possible to say whether theirexperiments were carried out with completely freshblood. Sutherland and Eisentraut (1956) also makeno mention of this point. de Kretser and Waldron
(I963) found that the mechanical fragility index ofred cells was markedly increased on standing, andthe disparity between their results and those of theearlier workers would be explained if the blood usedby the older workers was not fresh, i.e., had stoodfor more than one hour.There is also no mention in Harris's reports of
haemoglobin levels. de Kretser and Waldron (I963)showed that anaemia per se brought about an in-crease in the mechanical fragility of red cells andthey suggested that any increase in the mechanicalfragility of red cells in patients with plumbism mightbe a post hoc rather than a propter hoc phenomenon.There is general agreement, however, that sterile
incubation for 24 hours causes an increase in themechanical fragility of leaded red cells. In four ofthe io cases described by Griggs (I964), incubationcaused a more than normal increase in mechanicalfragility (i6-5%, I9-7%, 22-2%, and 26% comparedwith a mean control of io-5 ± 3-5%). Waldron(I964) confirmed this, but the changes found inleaded red cells were not enough to suggest that anincrease in mechanical fragility was a significantfactor in the production of lead anaemia.
Fratianne et al. (I959) were able to producechanges in normal red cells by incubating them forshort periods with lead chloride in vitro, but rela-tively high concentrations of lead had to be used,more than i5 ,tg. Pb++/ml. cells, according toGriggs (I964). Recently de Kretser and Waldron(I965) have found that below a concentration ofio pg. /ml. lead causes the mechanical fragility indexof normal red cells to be decreased, but above thisconcentration the mechanical fragility is increased,reaching a maximum at about 45 pg. Pb++/ml.With this in mind it is interesting to consider the
levels of lead found in the bone marrow. There issome evidence to suggest that the concentration oflead is much higher in the bone marrow than in theperipheral blood. Westermann, Pfitzer, and Jensen(I963) showed that in a group of patients with leadpoisoning with blood lead levels of o07 to 13 ,tg. /ml.,the corresponding marrow concentrations were 42to 92 ,tg. /ml. At these concentrations it may be thatlead does have some effect on the membrane of thedeveloping red cell. A number of glycolytic re-actions are thought to proceed in the cell membrane(Prankerd, I96I) and since some of these reactionsmay involve sulphydryl (-SH) group enzymes itwould not be unreasonable to expect lead to inhibitsome at least of these reactions in view of its knownaffinity for -SH groups (Wilkinson, I962). Anyinterference with the integrity of the red cellmembrane may well result in a shortened cell lifebut the evidence that this is indeed the case isequivocal to say the least.
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

H. A. Waldron
4f.~~~~~~~~~~~~.
4 0'4
f (a ':.<
:~~~~ ~~~~~~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~...
A*-.~~~*..:..!<,̂':>
.§......*t : 4 >. r.,
:>X,
, !,s>. @S:^k 4>i:
*! .t, d .
.. ,^ . P:|:* S k ; X; }> < t ; ...... o. r. t., >K .zF i.
*w;N m W; !Et °
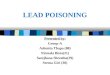
FIG. I. Photomicrograph of red cells incubated with lead (20 ,ug./ml. blood) showing distortion produced. Film fixed andstained with Leishman stain. x I,OOO.
However, large concentrations of lead have beenshown to produce morphological changes anddestruction of red cells when administered in vitroor in vivo. At concentrations of o i5M Pb++ haemo-lysis was observed microscopically in the sphericaland hexagonal crenate forms produced althoughsmaller crenate forms did not haemolyse (Vincent,I958). Incubating red cells with lead (20 ,tg.Pb++/ml. for 30 minutes) has been found by theauthor to produce morphological changes in redcells although haemolysis was not observed (Fig. i).The 'treatment' of malignancy with lead solutionsproduced some interesting reports on the effect oflead on circulating red cells. Brookfield (I928)investigated the effects of lead preparations used forsuch treatment on the blood of patients with cancer.The patients he studied were given 25 to 100 mg.Pb++ intravenously in one of two suspensions overa varying period of time. The effects varied frompatient to patient. Usually a positive van den Berghreaction was obtained after the first or second injec-tion and there was an increase in urobilin excretion.
Brookfield demonstrated that the red cell count wasdiminished after the injection of lead, in a few casesby -2I % in half an hour after the injection. Thered cell count rapidly returned to normal due toincreased marrow activity, indicated by an increasein reticulocytes. Morphologically the cells wereremarkably distorted with folding and clumping,some looking as though small pieces had been'bitten out of them with a punch', findings pre-viously reported by Maurel (I912) after blood fromrabbits and man had been treated with lead acetatein vitro. Gould, Kullman, and Shecket (I937)followed 17 cancer patients given a total of 535 to805 mg. Pb++ over a two- to four-week period and afurther five given I75 to 280 mg. over the sameperiod. A progressive anaemia was noted in i6 ofthe 22 patients. Bell, Williams, and Cunningham(1925) also found anaemia in cancer patients givenlead intravenously, and Bell (I930) found a reduc-tion of Io6 red cells in some patients one hour aftera single injection.
Results comparable to these are found in cases of
86
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

The Anaemia of Lead Poisoning: A Review
lead poisoning resulting from the ingestion of largedoses of lead, often single doses, taken either withsuicidal intent or by accident. There is a rapidlydeveloping anaemia in such cases (Laporte, Meyer,and Bousser, I939; Riedl, 1941; Strickland, 1948;Bastrup-Madsen, I950; Wade and Burnum, i955;Mellemgard and S0rensen, I955; Karpatkin, I96I)with occasional jaundice suggesting haemolysis(Karlog and M0oler, I958). A raised serum bilirubinwas observed by Crutcher (I963) in seven patientswith plumbism following the ingestion of lead-contaminated 'moonshine' whisky. This, hethought, gave support to the theory that lead causedhaemolysis. Davidson (1932) reported one case oflead poisoning due to drinking contaminated water;jaundice and a very raised serum bilirubin werenoticed due, partly at least, to increased blooddestruction. Jaundice was also found in one patientby Henderson (I952) and in a fatal case of a womanwho had taken lead as an abortifacient by Derobertand Hadengue (I947). Increased bilirubinaemiahas occasionally been reported in patients with leadpoisoning from other sources. Cantarow andTrumper (I944) found that levels ranging from I-0to 2-3 mg./Ioo ml. were not uncommon, and raisedlevels have also been reported by Heubel (I871),Schmidt-Kehl (I927), Klima and Seyfried (1937),Vigliani and Angeleri (I935), and Tishkoff et al.(I958) despite a note by Hijmans van den Bergh(I931) that the serum bilirubin is usually low ornormal in lead poisoning.
In an investigation of nine patients with industriallead poisoning, Maugeri (I940) found a raisedserum bilirubin and increased excretion of sterco-bilinogen and urobilinogen. He concluded that leadanaemia was haemolytic in type on the basis of thisstudy. Increased faecal urobilinogen excretion wasobserved in lead-poisoned guinea-pigs by Baikie(I954). Previous work by London, West, Shemin,and Rittenberg (I950) and Grinstein, Wikoff,Pimenta de Mello, and Watson (Ig5ob) using 15Nglycine had shown that faecal stercobilinogen wasderived in part from sources other than the haemo-globin of circulating red cells (at least I2% (Londonet al., I950); 40% in a case of untreated perniciousanaemia (London and West, ig5o) ) but, despite this,Baikie found that the increased urobilinogen excre-tion in the poisoned animals was closely correlatedwith the drop in haemoglobin, and he thought thathaemolysis played an important part in the patho-genesis of the anaemia of lead poisoning.
Simpson, Seaton, and Adams (I964), in anexhaustive study of a single case of lead poisoningin a lead burner presenting with neurological in-volvement, reported raised faecal and urinary uro-bilinogen excretion. Despite this, red cell fragility
studies were normal and the radio-chromium half-life of the cells was normal, and they did not thinkthat the urobilinogen excretion was due to hyper-haemolysis although they could suggest no alterna-tive explanation.Some further evidence for the haemolytic nature
of the anaemia of lead poisoning, however, was putforward by McFadzean and Davis (I949). In aprevious paper (McFadzean and Davis, I947) theyhad observed red cells containing iron-staining in-clusion granules in a number of acquired haemolyticconditions including lead poisoning. They extendedthis work using guinea-pigs poisoned with leadacetate and discovered many siderocytes in the bloodof these animals, the proportion being much higherin the bone marrow than in the peripheral blood.Splenectomy was performed on some of theanimals and it was found that this gave rise to avery considerable increase in the frequency ofstippling in the peripheral blood and in the numberof siderocytes present. After splenectomy the redcell count rose but there was no change in bonemarrow stippling. McFadzean and Davis (I949) sug-gested that lead was taken up by erythroblasts in themarrow as a result of which defective cells (sidero-cytes and stippled cells) were produced which weretaken up by the spleen and other parts of thereticulo-endothelial system and destroyed, thisaction by the spleen producing a haemolytic anaemia.There was some support for this theory in the workof Kin (I939) who had reported that the spleen andliver contained some specific chemical substancesable to decrease erythrocytes after the injection oflead acetate.
In their earlier paper, McFadzean and Davis(I947) had suggested that the iron granules foundwere produced by an abnormal mechanism ofhaemoglobin catabolism peculiar to haemolytic con-ditions. This part of their thesis was cast in doubtby the later work of Kaplan, Zuelzer, and Mouri-quand (I954) who found the presence of visible ironto be a normal phase in intracellular iron meta-bolism, associated with haemoglobin synthesisrather than breakdown. The later results ofMcFadzean and Davis (I949) were confirmed byPirrie (1952) using techniques similar to those ofMcFadzean and Davis. He also used trypan blueto block the reticulo-endothelial system of his in-toxicated animals and found that this, too, resultedin a greatly increased number of stippled cells in thecirculation. He found that the histological appear-ance of the spleens of the animals resembled thatseen in haemolytic anaemias in general, and hisconclusions as to the effect of lead on the erythronwere the same as those of McFadzean and Davis.Some doubt was cast on this hypothesis, however,
87
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

H. A. Waldron
by Douglas and Dacie (1953), who could find no
evidence that the spleen filtered off siderocytes but,despite this, Goldblatt (I955) still held that in leadpoisoning abnormal red cells produced in themarrow were rapidly taken up and destroyed by thespleen and other parts of the reticulo-endothelialsystem. Further doubts were cast by Bruschke(I959, I962) who, although confirming the experi-mental results of McFadzean and Davis (I949) andPirrie (I952), thought that the spleen did not remove
tile defective red cells but merely the iron-staininggranules. He referred to the earlier work of Crosby(1957) who had transfused blood containing many
siderocytes into patients with and without spleens.The transfused cells were tagged with 51Cr, and itwas found that in those patients with spleens thesiderotic granules gradually disappeared leaving thered cell membrane intact. There was furtherevidence to support Bruschke's contention in thework of Vorhaus and Turner (I957) who showedthat mature nucleated avian cells injected intoguiaea-pigs extruded their nuclei while in the spleenwithout undergoing apparent destruction, and alsoin the experiments of Jandl and Tomlinson (I958)who showed that lecithinized spherocytes were re-
tained in the spleen and returned to the circulationafter correction of their defects. Since the sinusoidsof the spleen are morphologically identical withthose of the bone marrow (Weiss, 1957) it is notunreasonable to assume, as Crosby (I959) suggests,that the spleen may provide a point at which defectsin circulating red cells are removed to compensatefor any inefficiencies in the mechanisms controllingthe release of newly formed red cells from the bonemarrow.
The evidence seems to suggest therefore thatMcFadzean and Davis (I949) and Pirrie (I952) mis-interpreted the results of their experiments. It ismore likely that siderocytes are 'matured' by thespleen (Bessis and Breton-Gorius, I962) with con-
sequent removal of siderotic granules, rather thandestroyed by it.
Inhibition of Haem and ProtoporphyrinSynthesis
Effect on Iron Metabolism Other theses havebeen advanced to account for the production ofanaemia by lead. Lourau (1946), for example, didnot think that lead caused destruction of red cellsbut, after conducting experiments with lead-poisoned rabbits, thought it prevented the syn-
thesis of an anti-pernicious factor by the inhibitionof an enzyme located in the gastro-intestinal tract(Lourau, 1947a, b, and c). This theory has attractedlittle attention, but one advanced by Rimington in
I938 has now become widely accepted. Rimingtonadvanced the hypothesis that lead interfered with aspecific enzyme system responsible for incorpora-ting iron into the protoporphyrin IX molecule toform haem. (He discounted the haemolytic actionof lead after finding normal faecal urobilinogenexcretion in lead-poisoned animals, but, as alreadydiscussed, this is not an altogether reliable index ofthe rate of degradation of circulating haemoglobin.)
If this hypothesis is correct, then one wouldexpect to find raised levels of erythrocyte proto-porphyrin and non-haemoglobin iron stores in casesof lead poisoning, and this is indeed the case.Raised erythrocyte protoporphyrin levels have beenreported by Roth (I935), Vigliani and Angeleri(I935), Vannotti and Imholz (I939), Watson (I950),Schmid, Schwartz, and Watson (I950), Pecora(I954), Larizza and Ventura (1954), Grazianni,Fusco, and Rossi (I954), Rutino and Prato (I955),Saita, Moreo, and Petrocchi (I956), Grazianni,Pecora, and Rossi (1956), Watson et al. (I958),Rubino, Pagliardi, Prato, and Giangrandi (I958),Rubino (I962), and Sano, Inoue, Harada, and Orita(I960), and raised serum iron values by Vannottiand Imholz (I939), Prader (1948), Grazianni et al.(I954), Larizza and Ventura (1954), Saita et al.(1956), Grazianni et al. (1956), Rubino et al. (I958),Tishkoff et al. (I958), Hutchison and Stark (I96I),David (I963), and Zegarski (I963). Vigliani andAngeleri (1935) found that the increase in proto-porphyrin was accompanied by a simultaneous risein serum bilirubin. They concluded that the por-phyrin was derived as a result of considerablehaemolysis. This view was discounted by Vannotti(I954) who thought that if any haemolysis werecaused by lead it would be insufficient to accountfor the rise in protoporphyrin found in leadpoisoning.There is no correlation between the levels of
protoporphyrin and serum iron (Saita et al., I956)but Zegarski (I963) found a distinct relation betweenurinary coproporphyrin excretion and serum ironvalues in 31 cases of lead poisoning.Some early opposition to Rimington's theory was
provided by Kench, Gillam, and Lane (I942) andlater by Lemberg and Legge (1949). These workersdrew attention to the disproportion betweenamounts of coproporphyrin III excreted in leadpoisoning and the degree of disappearance of haemo-globin in anaemic cases. Kench et al. (1942) per-formed a direct experiment on Kench and foundthat the daily intake of 20 mg. of lead acetate for38 days produced no change in blood haemoglobinlevels although the daily urinary coproporphyrinexcretion was raised from 22 pg. tO 268 jg. Theyconcluded that their results mitigated against
88
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

The Anaemia of Lead Poisoning: A Review
Rimington's theory despite finding a very raisedblood protoporphyrin level which the theorypredicts.Kench, Lane, and Varley (1952) were also critical
of Rimington's theory. They believed that theanaemia of lead poisoning was haemolytic incharacter and they based this conclusion mainly onthe finding of coproporphyrin I in the urine ofseven bath enamellers with lead poisoning. Theseauthors were the first to demonstrate copropor-phyrin I in the urine of patients with lead poisoning,it having been thought previously that only copro-porphyrin III was present in such persons (Grote-pass, I932; Watson, I936). The significance of thisfinding was that coproporphyrin I had previouslybeen found in excess only in haemolytic conditions(Watson, I937; Dobriner and Rhoads, I940;Watson and Larson, I947; Grinstein, Kamen,Wikoff, and Moore, I950; Rimington, I952), andRimington (I936) had advanced the theory that theurinary excretion of coproporphyrin I mightprovide an index of the rate of haemopoiesis.Kench et al. (I952) studied their workers for 130
days following cessation of exposure to lead. Theyfound that coproporphyrin I accounted for about30% of the total porphyrin excreted during thattime. In four cases the urine obtained on the 329thand 330th days after removal from exposure con-tained 42, 67, I 17, and 348 ,tg./l. of coproporphyrinI (constituting 20 to 47% of total porphyrin). Theymaintained that lead interfered with the maturationof the erythroid marrow cells giving rise to stippledcells broken down by the reticulo-endothelialsystem, the haemolytic action being confirmed bythe excess of coproporphyrin I excreted. It isquestionable, however, whether the excretion ofcoproporphyrin I nearly a year after exposure tolead had ceased would be due to abnormal destruc-tion (Goldblatt and Goldblatt, 1956). It is morelikely that these workers were seen in a stage ofactive regeneration of haemoglobin.
Coproporphyrin I has been demonstrated in theurine of cases of clinical plumbism and in lead-poisoned animals since Kench et al. (1952) firstreported it. Watson (I964) states that up to io%coproporphyrin I may be excreted in the urine ofcases of lead poisoning, and various proportions ofcoproporphyrin I were found by the author in I0lead workers having considerable exposure to lead,using techniques similar to those of Kench et al.(1952) (Table I). Holecek (I957) found smallamounts of coproporphyrin I, but unfortunately hisdata were qualitative only. Sumegi, Goreczky, andRoth (I956) found that 20 to 25% of the copropor-phyrin excreted in the urine of lead-poisonedrabbits was isomer I, and Weatherall (1952) thought
TABLE IURINARY COPROPORPHYRIN ANALYSIS IN IO CASES OF
INDusTRAL LEAD INTOXICATIONCase No. Total Copro- Isomer (%)
porphyrin (txg./l.)I III
I2345678910
I I05412251566485607
3047I397949499
5' 49IO 900 IOOIO 90II 890 IOO0 1000 10010 900 IOO
some of the coproporphyrin excreted by suchanimals might be isomer I (about io% on a qualita-tive basis) but later, in a further series of experi-ments, Comfort and Weatherall (I953) found onlyisomer III.The finding of coproporphyrin I in the urine
from cases of lead poisoning seems established, butthe work of Grinstein and his colleagues indicatesthat it is not there as a result of increased haemo-globin breakdown. In one series of experiments(Grinstein et al., I950a), 15N-labelled glycine wasadministered to dogs, and it was shown that boththe circulating haemoglobin and the excreted co-proporphyrin I contained a high proportion of 15N.Intravenous injection of the labelled haemoglobinfrom these dogs into other dogs treated with phenyl-hydrazine led to no significant increase of labelledcoproporphyrin I. This confirmed that the copro-porphyrin I excreted in the earlier experiment hadnot come from haemoglobin breakdown but hadbeen synthesized from the labelled glycine. Similarexperiments (Grinstein et al., 195ob) on lead-poisoned animals indicated that coproporphyrin IIIalso derived from ingested 15N glycine and not frompreformed haemoglobin. The results ofthese experi-ments confirmed earlier work by Bj6rkman (I941)who administered haemoglobin to lead-poisonedanimals with no subsequent effect on their porphyrinexcretion. Kark and Meiklejohn (I942) injectedhaemoglobin into two patients with lead poisoningand found an increase in plasma bilirubin identicalwith that found in normal subjects (Gilligan,Altschule, and Katersky, 1941). There was noincrease in porphyrin excretion and they were of theopinion that these results mitigated against thetheory that lead anaemia is haemolytic in character.Watson (I950) drew attention to experiments in
which there is a striking decrease of coproporphyrinin the red cells of lead-poisoned rabbits as theymature and leave the bone marrow (Schmid,
89
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

H. A. Waldron
Schwartz, and Watson, I950), although this may bepreceded by a transient increase (Schmid, Hanson,and Schwartz, 1952). Watson thought that theincrease in urinary porphyrin excretion was lesslikely to be due to destruction of the developingcells than to the liberation of porphyrin from intactcells, since an enormous number of cells would needto be destroyed to supply the amounts of copropor-phyrin excreted in the urine.
Despite a recent statement by Mann (I962) thatthe coproporphyrin excreted in the urine of casesof clinical plumbism is present as a result of haemo-globin breakdown, it seems extremely unlikely thatthis is, in fact, the case, and this must mitigateagainst the conclusions of Kench et al. (I952).
Further arguments for and against the validity ofRimington's theory have come from workers usingisotope techniques to study haem synthesis whohave also investigated the effects oflead on haem andprotoporphyrin formation. The results of thosestudies where fully quantitative data were given(Rimington, I95I; Dresel and Falk, I954, 1956a andb; Eriksen, I955; Goldberg, Ashenbrucker, Cart-wright, and Wintrobe, 1956; Kassenaar, Morell, andLondon, I957; Grinstein, Bannerman, and Moore,
I959; Klein, I962) are summarized in Table II.Various systems were used, but it will be seen thatgenerally lead did inhibit both haem and protopor-phyrin synthesis, the degree of inhibition dependingon the concentration of lead present and to someextent on the system used. Not all authors, how-ever, considered that the inhibition of haemsynthesis was due to the prevention of incorporationof iron into the protoporphyrin molecule. Dreseland Falk (1956a) thought that lead inhibited theformation of a precursor of haem rather than theincorporation of iron into protoporphyrin. (Anearlier finding by these authors (Falk and Dresel,1952) that lead stimulated free porphyrin synthesiswas considered to be due to an artefact in thesystem used.) Eriksen (I955) also thought that theinhibition of haem synthesis by lead was not due tothe mechanism proposed by Rimington but ratherto a diminished formation of the protein moiety ofhaem, and Aldrich, Labbe, and Talman (1955) wereof the opinion that such an effect of lead offereda better explanation of the widespread symptoms ofplumbism than that proposed by Rimington. Someevidence to support Eriksen's view is given in somerecent work of Trakatellis, Heinle, Montjar,
TABLE IISUMMARY OF EFFECTS OF LEAD ON HAEM AND PROTOPORPHYRIN SYNTHESIS
System Pb Conc. Inhibition (%)(M)
Haem
Rimington (I95I)
Dresel and Falk (I954)
Eriksen (I955)Dresel and Falk (1956a)
Dresel and Falk (1956b)
Goldberg et al. (1956)
Kassenaar et al. (I957)
Grinstein et al. (1959)
Klein (I962)
Chicken erythrocytesRinger-Tyrode soln.SalineHaemolysate of chicken erythrocytes
Rabbit and duck erythrocytesChicken erythrocytes
Haemolysate of chicken erythrocytes
Haemolysate of chicken erythrocytesHaem synthesis from protoporphyrinPhosphate buffer
Tris buffer
Duck erythrocytesPhosphate bufferHaemolysate of chicken erythrocytesIncorporation of 14C from glycineDuck erythrocytes
IO-4IO-4IO-5I0-410-4*lIO-53 X IO-5JO-6Io-53 X IO-5IO-4
10-2i-8
I0-4io-'10-4IO-5IO -6
5 X IO-4
IO-32 X IO-5*4 X IO-5*
90
40-5050
100
70-809
64I446-558473-89
I00
5090-1IOO
66
83
8o5730633083
77
350
'495I00
Concentrations of lead are given as lead acetate except when denoted *, when concentrations are given as Pb++.All syntheses are from glycine as substrate except where otherwise stated.
90
Author
Protoporphyrin
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

The Anaemia of Lead Poisoning: AReview9Axelrod, and Jensen (i965). These authors addedlead acetate in a concentration of 5-7 x 10-5M to asystem of rat reticulocytes and found that leadcaused a very rapid breakdown of polysomes (40%in one hour, 72% in five hours). Since thepolysomesare known to be able to synthesize the polypeptidechains of haemoglobin (Burka and Marks, I964),Eriksen's conclusions seem well founded.
Other workers, however, are firm in their supportof Rimington's original hypothesis. Baron (I954)considered that the failure to incorporate iron intoprotoporphyrin was the most important cause oflead anaemia. Sano (1958a) and Heilmeyer (I959)both reported that lead blocked iron incorporationinto protoporphyrin, but Sano thought that the in-hibition of iron incorporation into the porphyrinring was a secondary effect of lead. In a later work(Sano, 1958c) in which high erythrocyte protopor-phyrin levels were found both with normal red cellcounts and haemoglobin levels and with anaemia, hesuggested that lead caused a hypersynthesis of por-phyrin taking a course different from that of normalhaem formation. Gajdos-T6rbk, Gajdos, andBenard (I958), using cells from rabbits treated withphenylhydrazine, found that lead (as lead acetate)completely inhibited the enzyme responsible forthis incorporation (haem synthetase), probably byincorporating with free sulphydryl groups necessaryfor the activation of the enzyme (Schwartz, Cart-wright, Smith, and Wintrobe, I959). This findingwas in accordance with the earlier work of Benard,Gajdos, and Gajdos-Torok (I958) who had shownthat virtually no radio-iron was incorporated in vitrointo the haemoglobin in red cells from lead-poisonedrabbits although protoporphyrin synthesis still tookplace. Later, Gajdos and Gajdos-Torok (1958)found that iron was not incorporated into protopor-phyrin in vivo using rabbits with experimental leadpoisoning.
Although there seems no doubt that lead inhibitshaem synthesis-by whatever means-in vitro,there is some evidence to suggest that its effect in
vivo may not be the same as that observed in vitro.Caccuri, Pecora, Fati, and Vecchione (I958) foundthat the addition of homogenized tissue fromanimals with lead poisoning to a system of intactred cells and glycine stimulated the synthesis ofprotoporphyrin. Later, using the same system butwithout the homogenized tissue, they found that theaddition of lead nitrate completely inhibited thesynthesis of protoporphyrin (Pecora, Fati, andVecchione, I960). They advanced the theory,earlier put forward by Pecora (I954), that the effectof lead on protoporphyrin synthesis in vitro wasdifferent from that in vivo. In a more recent paperPecora and his colleagues (Pecora, Fati, Mole, andPesaresi, I963) reported a study on the effect of leadon delta-aminolaevulinic acid dehydrogenase (ALA-d) prepared from the bone marrow of rabbits.Weak concentrations of lead (IO-4 to IO-11M) stimu-lated protoporphyrin synthesis but inhibited it at aconcentration of Io-2M. This they regarded as con-clusive evidence that lead stimulates protoporphyrinsynthesis in vivo since, they said, lead is found inlow concentrations in the bone marrow. The workof Westermann et al. (I963), however, suggests thatlead is present in high concentrations in the bonemarrow and this must throw some doubt on theconclusion of Pecora and his colleagues.
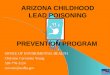
It is worth noting at this point that earlier stagesin haem synthesis are also affected by lead (Fig. 2),notably the production of ALA from porphobilino-gen, but it is not proposed to comment on this inthis paper. The subject has been well dealt with byHaeger-Aronsen (I960) in her excellent monograph,and more recently by Chisolm (I964).
Extracellular iron metabolism is unaffected bylead. Iron is cleared from the plasma of patientswith lead poisoning at a rapid or normal rate (Beck,Lanini, and Beraud, I955; Boyett and Butterworth,I962; Simpson et al., I964). This is not always soin children. Watson et al. (I958) found abnormallylow serum iron values in I3 children with leadpoisoning. The total iron-building capacity of the
Succinyl CoA)- ALA >- PBG > Uro C--Copro > Fe Haem
FIG. 2. Scheme showing main steps in haem synthesis. Solid arrows indicate stages inhibited by lead; broken arrowsindicate stages at which inhibition is thought to take place, but evidence is inconclusive.
ALA = delta-aminolaevulinic acid; PBG = porphobilinogen; Uro = uroporphyrinogen;Copro = coproporphyrinogen; Proto = protoporphyrinogen.
9I
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

H. A. Waldron
serum was variable, but the mean value for thegroup was normal (285 pg./Ioo ml.). Leikin andEng (I963), however, who studied plasma ironclearance in seven children with lead poisoning,found that in the three with the longest history ofexposure the plasma iron clearance time was pro-longed and the rate of incorporation of iron into theblood cells was decreased. The four children withshorter exposure were found to have normal orincreased iron-turnover results. These studies con-firmed that extracellular iron metabolism is normalin lead poisoning but, with long exposure, erythroidhyperplasia may result in a decreased turnover ofiron. An increase in plasma iron clearance has beennoted in animals with lead poisoning by Paolino,Resegotti, Sartoris, and Infelise (I963).
Sroczynski, Jonderko, and Watras (I964) pro-duced additional evidence that lead impairs the rateof incorporation of iron into mature and immaturered cells. Using 59Fe they found that lead preventedthe incorporation of iron into the red cells of lead-poisoned rabbits although this inhibition wasapparently prevented by the administration ofethylene diamine tetracetate (EDTA). Lead hasalso been found to impair the incorporation of ironinto circulating red cells in cases of human leadpoisoning (Boyett, Pittman, and Butterworth, I960;Boyett and Butterworth, I962). In their case of leadpoisoning, Simpson et al. (I964) found that, al-though iron passed normally to the marrow, only4o09% was utilized as against a normal utilization of68 to 86%.
Jandl, Inman, Simmons, and Allen (I959) showedthat the uptake of 59Fe by human reticulocytes wasalmost completely inhibited by the addition of5 X I0-4M Pb++ but only slightly diminished(-2o-6%) by I0-4M Pb++. The incorporation of59Fe into haemoglobin, however, was almost entirelyprevented, with the consequence that the amount ofiron in the red cell membrane was greatly increased.Reticulocytes from bled rabbits incubated withI0-4M Pb++ showed only a moderate diminution incellular uptake of 59Fe but there was a strikingincrease in the amount of iron in the stromalfraction of the hydrolysed centrifuged cells. Thisconfirmed earlier work by Bessis and Breton-Gorius(1957c) who had also demonstrated an accumulationof iron in the stroma of immature red cells in casesof plumbism.
Allen and Jandl (I960) extended their earlierwork using washed rabbit reticulocytes. They foundthat when iron was taken up by these cells it wasfirst associated with various particulate fractions(stroma, mitochondria, and microsomes) beforebeing gradually released into the soluble cytoplasmto become incorporated into a transient non-
haemoglobin protein phase and then into haemo-globin. They found that lead allowed iron toaccumulate in the particulate fractions but that itblocked the entry into the non-haemoglobin phaseand into haemoglobin. This work was confirmedby Gajdos-Torok, Gajdos, and Benard (I960) andlater by Lothe and Falbe-Hansen (I963). Lotheand Falbe-Hansen found that haemoglobin synthesisin lead-poisoned rabbits was greatly diminished,although haemoglobin precursors could still take upiron. They concluded that lead blocked the transferof iron from a ferritin phase, not associated with thestroma, to an electrophoretically fast-moving frac-tion associated with the mitochondria. Greenough,Peters, and Thomas (I962) studied the effects oflead on intracellular iron metabolism in vitro usinga system derived from dog and human bone marrow.A minor fraction was isolated from this system whichappeared to be a precursor of haemoglobin. Leadacetate (Io-4M) did not block incorporation of ironinto this fraction but it did block the entry of ironinto haemoglobin. Korst, Frenkel, and Wilhelm(I962), using short-term marrow culture techniques,found that serum from anaemic animals increasedthe uptake of iron by the marrow cells, but uptakewas inhibited by lead. Cooper (cit Griggs, I964)prepared mitochondria from the reticulocytes ofanaemic rabbits and found that lead inhibited themitochondrial uptake of iron. This result is some-what at variance with the evidence obtained usingthe electron microscope which indicates that ironstores are increased in the mitochondria in leadpoisoning. These electron microscope studies haveshown that the mitochondria of normoblasts andreticulocytes are morphologically changed in casesof human lead poisoning and in animals intoxicatedexperimentally. There is general agreement that thestores of intracellular iron are increased but someconfusion has arisen over the site of these increasediron stores. Thus, although several reports clearlyindicate the presence of iron within the mito-chondria of the normoblast (Bessis, I958; Bessis andBreton-Gorius, I957a, b, c, d, 1959; Pernis andBairati, I959; Pernis, Bairati, and Guibileo, I959;Pernis,Vigliani, Depretis,Beard and Karlsbad, I964),Griggs (I964) states categorically that this is not so,iron is not found within the mitochondria, and hequotes a personal communication from Bessis (I963)in support of this. Indeed, in an article by Bessisand Breton-Gorius (I962), after describing thecharacteristic alterations of the mitochondria, theseauthors state, 'We have not seen any iron inside themitochondria'.
Later work, however, leaves no doubt that iron isfound within the mitochondria. Bessis and Jensen(I965) say that two types of non-haem iron may be
92
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

found inside the abnormal sideroblast from thebone marrow of lead-poisoned animals or frompatients with lead poisoning-ferritin, similar tothat found in normal cells, and an abnormal type ofiron which they term ferruginous micelles. Theferruginous micelles are dust-like or they occur inplaques having no constant formation. Ferritin isfound within the mitochondria whereas it is foundonly in the cytoplasm of normal cells. The fer-ruginous micelles are found only within the mito-chondria. In an even more recent report (Jensen,Moreno, and Bessis, I965), the abnormalities foundin the normoblasts are concisely described: mito-chondria are found in abundance, they are greatlyenlarged, dilated, devoid ofnormal cristae, and oftencontain large amounts of ferritin or ferruginousmicelles. Ferritin is also found within the cyto-plasm. (The morphological changes in the mito-chondria described by Jensen et al. (I965) have alsobeen seen in mitochondria prepared from the liver
of swine fed with lead acetate over a three- to six-month period by Watrach (I964).)
In rat experiments where phenylhydrazine andlead are used there is an abundance of iron withinthe mitochondria, but iron may also be foundoccasionally in the mitochondria of animals fedphenylhydrazine alone (Jensen, I965, personalcommunication).
Jensen (I965, personal communication) statesthat in I963 Bessis was aware that iron was found inthe mitochondria, and it seems therefore thatGriggs' (i964) statement is at fault. The statementin the review by Bessis and Breton-Gorius (I962)quoted above may have resulted from an error intranslation. The true picture is that there is nodoubt that iron is found in excess in the normoblastand that a portion of the ferritin is found within theintercristal spaces of the mitochondria.
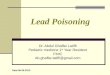
Several stages of haem synthesis are known to befacilitated by intact mitochondria (Sano, I958b;Sano, Inoue, Tanabe, and Koike, I959; Bessis andJensen, I965) and it has been suggested that theymay function as an intermediate in intracellulariron metabolism (Cooper, Webster, and Harris,I963) (Fig. 3). They are probably necessary forthe continued transfer of iron from extracellularsites to normoblasts or reticulocytes (Jandl et al.,I959; Morgan and Laurell, I963). Thus the electronmicroscopic findings of altered and damaged mito-chondria described above may well have a correla-tion with impaired haem synthesis.
The Coombs' Test in Lead Poisoning
The most comprehensive study on the Coombs'test in lead poisoning was performed by Sutherland
Succinate +Glycine
ALAPBGUroCopro
93
FETransferrin
FEFerritin
FerruginousMicelles
Haem
FIG. 3. Stages of haem synthesis dependent on intact mito-chondria. Continuous lines indicate stages at leastpartially dependent on intact mitochondria (based onBessis and Jensen, I965).
and Eisentraut (I956). They produced acuteplumbism in six dogs by injecting them with leadacetate either intravenously or intraperitoneally. Infive of the six dogs so treated a positive Coombs'reaction developed within 24 hours. The sixth dogreceived less lead acetate than the others and it wasadministered intraperitoneally in this case, butnevertheless a positive Coombs' test was obtainedafter 13 days.A further ii dogs were given chronic plumbism
and all eventually developed a positive Coombs'test, but the reaction was observed only in the upperlayer ofred cells after centrifugation. Since reticulo-cytes and stippled cells tend to be concentrated inthe upper layers of centrifuged blood cells, Suther-land and Eisentraut suggested that reticulocytesmay retain free globulin on the cell membrane whichwould account for the positive Coombs' reaction.This suggestion was confirmed in a later study byJandl (I960).Ten lead workers were examined by Sutherland
and Eisentraut; all had a negative Coombs' reactionwhen whole blood was tested. Blood was obtainedfrom a further I9 lead workers and this test was
performed after the cells had been allowed to sedi-ment. Positive reactions were obtained in the uppercells in 79% of the cases; the reaction in the lowercells or with whole blood was always negative.Pernis and Finulli (I960) also found a positiveCoombs' test in the upper layer of sedimented cellsfrom lead workers.
In cases of human lead poisoning the results are
usually negative, although Crutcher (I963) did findpositive reactions in three of eight cases ofplumbismresulting from the drinking of 'moonshine' whisky.
The Anaemia of Lead Poisoning: A Review
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

The reactions were negative when repeated I0 daysafter treatment with EDTA. Tishkoff et al. (I958)found a negative reaction in two patients with leadpoisoning, and negative findings were reported insingle cases by Fullerton (1952), Karpatkin (I96I),Lane and Lawrence (I96I), and Simpson et al.(I964).
Jandl and Simmons (1957) reported that theaddition of lead in vitro did not cause normal redcells to become agglutinable to Coombs' serum, andit seems likely that positive reactions will occur onlyin cases of lead poisoning where there is a greatlyincreased number of reticulocytes or stippled cellspresent.
Red Cell Survival in Lead Poisoning
Relatively few studies on the red cell survivaltime in experimental or human lead poisoning havebeen made. The quantitative data given in theliterature are summarized in Table III. The mostcomprehensive study has been made by Rubino,Prato, and Fiorina (I959), and it will be seen that inseveral cases significantly lower values than normalwere obtained using both radio-chromium taggingand the method of Seip (I953).
Griggs and Harris (I958) showed that cellsremoved from two of four patients with lead poison-ing had a significantly shorter half-life (TO), 20 days,than the normal, 27 tO 34 days. Hutchison andStark (I96I) found one very low Ti in the threecases they studied. After treatment with EDTA theTi returned to normal (Goldberg, I960). Combris-son, Desoille, and Albahary (I964) found low Tivalues in three of seven human subjects but a con-
sistently normral value in 78 rabbits given acute andchronic plumbism experimentally. Cells frompoisoned animals survived normally when trans-fused into control animals.
Leikin and Eng (I963) reported erythrocytesurvival times in seven children with lead poisoning.The TI was reduced in five of the seven patients,the shortest survival times being seen in thosechildren with the shortest exposure to lead. Noneof the children studied had a concurrent irondeficiency syndrome.
Other abnormally low survival times have beenreported by Sheets et al. (195i), by Crepet et al.(1956) using Ashby's technique (I92I), and byKaplan (1954). Karpatkin (I96I) and Simpson et al.(I964) both found normal survival times in thesingle cases they described.
Survival times of normal red cells incubated withlead in vitro and then reinfused into the donor havebeen reported (Fratianne et al., 1959; Rubino et al.,1959). In two of the four experiments performed
by Fratianne et al., moderately shortened survivaltimes were found, whereas in all three cases reportedby Rubino et al. shortened T values were obtained.Although there seems no doubt that in some cases
of lead poisoning a shortened red cell life span isfound, Rubino (I962) says that anaemia will notresult until the life span is less than 40 days. Abovethis value compensatory erythropoiesis is sufficientto prevent anaemia developing.There is no conclusive evidence to explain how
lead produces a shortened life span in red cells, butit seems likely to be due to an effect on the develop-ing red cells in the bone marrow, where the con-centration of lead is higher than in the peripheralblood, rather than on the cell membrane of thecirculating cell, as has sometimes been suggested.
Stippled Cells: Effect of Lead on Erythro-poietic Cells in Bone Marrow
Stippled cells are an invariable but by no meansconstant accompaniment of lead poisoning. Theenumeration of the number of stippled cells in theperipheral blood has been advocated as a means ofcontrolling exposure to lead (Lane, I93I, I949;McCord, Holden, and Johnston, 1935) but nowa-days stippling is generally regarded as an unreliableindex of lead absorption (Griggs, I964). The degreeof stippling does not correlate well with the in-tensity of exposure and is found in a wide varietyof other haematological disorders, e.g., in manyhaemolytic anaemias, thalassaemia, leukaemia, andafter exposure to aniline, arsenic, benzene, carbonmonoxide, and copper. The stippled cell countshows considerable diurnal variation (Minden andOpitz, I957; King and Thompson, I96I), and awide variation in the number of cells showingpunctate basophilia may be found on different filmsfrom the same blood sample (Bruckner, 1927;Brookfield, I928; Dustin, 1943, I944) dependinglargely on the speed of drying of the film, slowlydrying films containing more stippled cells thanquickly drying films. Incubating blood with NewMethylene Blue (0-25% for 5 minutes) also increasesthe number of stippled cells present (Jensen et al.,I965).
Since Behrend (I899) first described the appear-ance of stippled cells in lead poisoning, much workhas been undertaken to establish the causation andcharacter of the stippled material. Grawitz (I900,I906) thought that it was of cytoplasmic origin sincethe staining reaction of the granules was differentfrom that of nuclear substances. This seemed toconfirm the earlier views of Ehrlich (i885), Smith(I89I), and Foa (I889), although Askanazy (I907)
H. A. Waldron94
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

TABLE IIISUMMARY OF RED CELL SURvIVAL TiMEs IN CASES OF LEAD POISONING
Author Technique Survival Time(days)
Sheets et al. (I95I)Crepet et al. (I956)
Griggs and Harris (I958)
Rubino et al. (1959)
Rubino et al. (I959)
Fratianne et al. (I959)
Goldberg (I960)
Hutchison and Stark (I96I)
Leikin and Eng (I963)
Combrisson et al. (I964)
Simpson et al. (I964)
AshbyAshby
51Cr
5"Cr
Transfusion of cells from patients with plumbism intocompatible normals. Original survival times inbrackets.
50 ml. blood incubated with I50 tg. lead acetate for6o min. Reinfused into donor.
Seip
Seip
5"CrNormal cells incubated with lead chloride, reinfused
into donor
51CrAfter treatment with EDTA51Cr
51CrChildren
5"Cr
5"Cr
25 (TO)9555267020 (TI)20252927* (TI)25-5*I7.5*24-5*20*12I8-5I7i8 (20) (TI)i6 (12)20 (i8-5)I9 (TO)i820-5
426o55
II38i9373
8317
'35II99922II0
405095
I8222628I8I62632I8t'320
I52522232820242024I8i62I26
Normal
55-60
I20
27-34
25-31
IIO
IIO
(TI)
(TO)
(TO)
30
Not given
Not given
Unless otherwise stated, auto-survival times were determined.
*Also described by Crepet et al. (I956). tAlso described by Goldberg (I960).
(TI)
25-28
(TO)
20-32
(TI) 25-30
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

later advanced the theory that the granules werenuclear fragments.There was much controversy among early
workers whether stippling represented a regenera-tive or a degenerative change. Engel (I900)thought it was a regenerative change because of theappearance of stippled cells in the embryo. Thisview was supported by Askanazy (I907), Konig(I9I0), Naegeli (193i), and Young and Osgood(I935). Those who championed the opposite viewwere Weidenreich (1903), Jolly (I907), and Grawitz,Key, and Pappenheim (I9I9). These last authorsbased their conclusions principally on the fact thatthey were unable to demonstrate stippled cells inthe bone marrow of lead-poisoned animals. Key(I924) was also unable to find stippled cells in thebone marrow of lead-poisoned animals, and Bell etal. (I925) could not detect stippled cells even in themarrow of animals which had died from leadpoisoning. Since then, however, many workers havesucceeded in demonstrating punctate basophils inthe marrow from cases of human and animal leadpoisoning (Young and Osgood, 1935; Klima andSeyfried, I937; Duvoir, Pollet, Gaultier, andMenetrier, I938; de Weerdt, I939; Thaddea, 1940;Bentsath and Varga, I940; Henning and Keilhack,1940; Kopasz, I943; Albahary, 1944-45; Movitt,I945; Saita, I946; Leitner, 1949; McFadzean andDavis, I949; Fullerton, I952; Pirrie, 1952; Morel,Roche, and Baron, 1954; Beritic and Vandekar, I956;David, I959). Albahary (I944-45) gave lead acetateintravenously to volunteers and found stippled cellsin the marrow before they appeared in the peripheralblood. Generally, more stippled cells are found inthe bone marrow than in the peripheral blood, sug-gesting that lead exerts its effect primarily on redcell precursors in the bone marrow rather than onthe circulating red cell.
Brookfield (I928) thought that stippled cells wereyoung cells altered by a degenerative process, andhe produced some evidence to confirm the earlierwork of Schwarz and Hefke (1923), Bruckner andSpatz (I926, I927), and Bruickner (I927) thatstippling as such is not present while the blood cellsare circulating but appears only after the blood hasbeen shed. He was unable to demonstrate stipplingin fresh blood as some earlier workers had done(Dietrich, I9I0; Ferrata and Boselli, I910). Later,Dustin (1943, 1944) confirmed Brookfield's workand indicated that stippling occurs only when cellscontaining the necessary precursors are subjected tocertain manipulations prior to microscopic examina-tion.
Ferrata (I933) thought that the stippled materialwas derived from the red cell membrane but Whitbyand Britton (I933) were of the opinion that stippled
cells were reticulocytes in which the basophilicmaterial had been altered by the lead. This viewwas corroborated by Haenel (I949) and by Baikieand Pirrie (1958) who also thought that the stippledcell was a modified reticulocyte. Sroczyn'ski (I962),however, stated that stippled cells were not reticulo-cytes, but later work by Jensen et al. (I965) indi-cated that there was almost certainly some relation-ship between the two types of cell.McFadzean and Davis (I947, I949) found that
stippled cells frequently contained iron-staininginclusion bodies which they thought were related tothe basophilic stippling of plumbism althoughDoniach, Gruneberg, and Pearson (I943) had pre-viously reported that there was no such relationship.Dacie and Doniach (1947) demonstrated that thesiderotic granules in red cells may be basophilic butthey noticed that red cells showing classical punctatebasophilia gave a negative iron-staining reaction.Pirrie (1952) reported that a varying proportion ofthe basophilic granules of stippled cells gave a posi-tive iron-staining reaction, but Douglas and Dacie(I953) found that few, if any, of the granules ofdiffuse punctate basophilia were iron-containing. Insome pathological states, however, erythroblastsshowing coarse basophilia may give a positive iron-staining reaction (Sundberg and Broman, I955).Beritic, Grgic, and Sirec (I957) found no correlationbetween the incidence of stippled cells and iron-containing cells, although basophilic granules werefrequently found in siderocytes and sideroblasts. Ina later paper, Beritic (I963) was able to demonstratethree distinct types of cell in patients with leadpoisoning: those containing basophilic, iron-nega-tive granules only, those containing iron-positive,non-basophilic granules only, and those containingboth types of granule. This paper considerablyclarified the confused situation, Beritic concludingthat since the two types of granule were constantlyfound together, it was justifiable to conclude thatboth phenomena were intimately related to the samemetabolic disturbance. He stressed, however, thatthe iron-positive granules were not to be regardedas cytochemical variants of the iron-negativegranules.The comprehensive studies of Dustin (I943,
1944) indicated that the basophilic granules werecomposed of ribonucleoproteins, and the electronmicroscope studies of Sano (I955) showed that thestipple material might be aggregates of ribonucleicacid (RNA) around the mitochondria. He latershowed (Sano, 1958a) that the oxygen consumptionof stippled cells was much greater than that ofmature cells, thus confirming the results of Baikieand Valtis (1954). RNA was also found in stippledcells by Sroczyn'ski (I962) and David (I963).
96 H. A. Waldron
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

The Anaemia of Lead Poisoning: A Review
Bessis and Breton-Gorius (I962) thought that thealtered mitochondria found in the normoblasts inlead poisoning might constitute the basophilicgranulation, but recent papers by Jensen and hiscolleagues (Jensen and Moreno, I964; Jensen et al.,I965) indicate that the stipple granules are com-
posed of altered ribosomes and do not include mito-chondria. After extensive electron microscopestudies they concluded that the three morphologicalentities, reticulocytes, diffuse polychromasia, andbasophilic stippling, were largely the result ofdifferent manipulations in preparation for optical or
electron microscopy, and this accounted for themultiplicity of conclusions reported regarding thenature of the stipple material. They confirmed theresults of Beritic (I963) regarding siderocytes andstippled cells and showed that non-haem iron was
not an essential component of basophilic stippling.Lead has been shown to produce definite morpho-
logical changes in the erythroid cells of the bonemarrow. The occurrence of stippled cells in themarrow has been mentioned above. In additionmany authors have noted the presence of megalo-blasts (or macroblasts) in lead-poisoned animals(Dumas, I903; Ophuls, I9I5; Seiffert and Arnold,I928; Speransky and Sklianskaja, I928; Fontanaand Stazzi, I933; Klima and Seyfried, 1937;
Sroczyniski, I962) and in cases of human plumbism(Cadwalader, I906; Pellegrini, 1935; PelaezRedondo, I941; Garta, 1949; Heilmeyer andBegemann, I95I) although Beritic and Vandekar(I956) in an extensive study of I9 cases of leadpoisoning were unable to find megaloblastosis in a
single instance. Instead, they discovered a greatpreponderance of polyploid erythroblasts, mostlybi-nuclear (incidence 2-2 to I3-7%), and they sug-
gested that these cells may have been confused withmegaloblasts by earlier workers. Beritic andVandekar were apparently the first authors todescribe polyploid erythroblasts in lead poisoning,and their finding was subsequently confirmed byDavid (i959).Nuclear changes have been noted by several
authors (Cadwalader, I906; Leitner, I945; deWeerdt, 1939; Rohr, I949; Fulerton, I952; Beriticand Vandekar, I956; Moeschlin, 1957; David,I959), the most complete description of the changesobserved being that given by Beritic and Vandekar.They believed that the nuclear alterations wereclosely related to the polyploidy they observed.They thought that the fusion of chromosomes didnot permit the nucleus of the late normoblast tocomplete its division, but instead a plurinuclearerythroblast with karyorrhexis resulted.
Abnormalities in mitosis have been noted by otherauthors (Morel et al., I954; Kienle, 1943; Omel-
janienko, 1954). In a series of animal experimentsRondanelli, Gorini, Colombi, and Verga (I958)found that lead had a definite mitostatic activity onerythroblast nuclei at metaphase. They consideredthat this antimitotic effect of lead might be anelement in the pathogenesis of the anaemia of leadpoisoning.
Conclusion
It seems probable that there is no single factorresponsible for the production of the anaemia of leadpoisoning. Much of the evidence which has beenput forward to show that the anaemia is haemolyticin character is equivocal, although there can be nodoubt that high concentrations of lead can producemorphological changes in mature circulating redcells both in vitro and in vivo.On the other hand, there seems no doubt that lead
has a profound effect on red cell precursors in thebone marrow, producing morphological changes andalso causing defective haemoglobinization by in-hibiting haem synthesis, and any changes inducedin the peripheral red cells may be the results of thisprimary action on erythroblastic cells in themarrow.
It is true to say that the precise cause of theanaemia of lead poisoning is still not known, but, inthe author's opinion, the answer is likely to be foundin the effect of lead on a complex of enzymes, boththose responsible for haem synthesis and thoseconcerned with glycolysis.
REFERENCES
Albahary, C. (I944-45). Sang., I6, 341.Aldrich, R. A., Labbe, R. F., and Talman, E. L. (I955).
Amer. J7. med. Sci., 230, 675.Allen, D. W., and Jandl, J. H. (I960). Blood, IS, 7I.Andral and Gavarret (I840). Ann. Chim. et Phys., 75, 309.Ashby, W. (I921). J. exp. Med., 34, 127.Askanazy, S. (1907). Z. klin. Med., 64, 288.Aub, J. C., Fairhall, L. T., Minot, A. S., and Reznikoff, P.
(1925). Medicine, 4, I.-, and (1926). Lead Poisoning. Williams
& Wilkins, Baltimore., Minot, A. S., Fairhall, L. T., and Reznikoff, P. (1924).
J. Amer. med. Ass., 83, 588.and Reznikoff, P. (I924). J. exp. Med., 40, I89.
, , and Smith, D. E. (I924). Ibid., 40, 151.Baikie, A. G. (1954). Blood, 9, 46I.
and Pirrie, R. (I958). Scot. med. J., 3, 264.and Valtis, D. J. (I954). Brit. J'. exp. Path., 35, 434.
Baron, J. (1954). Thesis, Lyons.Bastrup-Madsen, P. (I950). Lancet, 2, 171.Beck, E., Lanini, G., and B6raud, T. (I955). Helv. med.
Acta, 22, 442.
97'
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

H. A. Waldron
Behrend (I899). Dtsch. med. Wschr., 25, Vereins-BeilageNo. 42, 254.
Bell, W. B. (1930). Some Aspects of the Cancer Problem.Bailliere, Tindall and Cox, London.Williams, W. R., and Cunningham, L. (I925). Lancet,2, 793-
B6nard, H., Gajdos, A., and Gajdos-Torok, M. (1958).C. R. Soc. Biol. (Paris), 152, 296.
Bentsath, A., and Varga, S. (1940). Dtsch. med. Wschr., 66,1194.
Beritic, T. (i963). Brit. J. Haemat., 9, i85.Grgic, Z., and Sirec, A. (1957). Proc. XII Int. Congr.Occup. Health, Helsinki, I957.and Vandekar, M. (I956). Blood, II, II4.
Bessis, M. (1958). Bull. Acad. nat. Med. (Paris), 142, 629.and Breton-Gorius, J. (I9s7a). C. R. Acad. Sci. (Paris),244, 2846.
and (1957b). Rev. Hemat., 12, 43.and (I957c). Sem. Hop. Path. et Biol., 33, 4II.and (1957d). C. R. Soc. Biol. (Paris), 151, 275.and (I959). Blood, 14, 423.and- (i962). Ibid., i9, 635.
- and Jensen, W. N. (i965). Brit. J'. Haemat., II, 49.Bjorkman, S. E. (194I). Acta med. scand., Io8, 568.Bouchard, C. (i873). C. R. Soc. Biol. (Paris), 5 Ser., 5, 358.Boyett, J. D., and Butterworth, C. E. (i962). Amer. J7. Med.,
32, 884.Pittman, J. A., and Butterworth, C. E. (ig60). Clin.Res., 8, 52.
Brookfield, R. W. (I928). J. Path. Bact., 31, 277.Bruckner, H. (1927). Arch. Hyg. (Berl.), 98, 95.
and Spatz, R. (I926). Ibid., 97, 277.and (1927). Arb. Reichs gesundh.-Amte, 58, 49I.
Bruschke, G. (i959). Dtsch. Gesundh.-wes., 14, 1059.(i962). Folia Haemat. (Lpz.), 78, 286.
Buczkowski, M. (I964). Int. Arch. Gewerbepath. Gewerbehyg.,20, 537.
Burka, E. R., and Marks, P. A. (I964). J7. molec. Biol., 9, 439.Caccuri, S., Pecora, L., Fati, S., and Vecchione, C. (I958).
Arch. Mal. prof., 19, 34I.Cadwalader, W. P. (I906). Bull. Ayer. clin. Lab., I, no. 3, p.
44-Cantarow, A., and Trumper, M. (I944). Lead Poisoning.
Williams and Wilkins, Baltimore.Chisolm, J. J. (I964). J. Pediat., 64, 174.Clarkson, T. W., and Kench, J. E. (I958a). Biochem. J7., 69,
432.and (I958b). Brit.J_. industr. Med., I5, 1I5.
Combrisson, A., Desoille, H., and Albahary, C. (I964). Proc.XIV Int. Cong. Occup. Health, Madrid, I963, Vol. 2,
P. 755-Comfort, A., and Weatherall, M. (953). Biochem.J., 54, 247.Cooper, R. G., Webster, L. T., and Harris, J. W. (I963). 7.
clin. Invest., 42, 926.Crepet, M., Rubino, G., and Gobbato, F. (I956). Proc. 2Ist
Cong. Nat. di Med. del Lavoro.Crosby, W. H. (I957). Blood, 12, i65
(I959). Ibid., 14, 399.Crutcher, J. C. (I963). Ann. intern. Med., 59, 707.Dacie, J. V., and Doniach, I. (I947). J. Path. Bact., 59, 684.David, A. (I959). Arch. Gewerbepath. Gewerbehyg., 17, 329.
(I963). Caso. Lek. ces., 102, 69.Davidson, L. S. P. (I932). Quart. Jr. Med., I, 543.de Kretser, A. J., and Waldron, H. A. (I963). Brit. J. industr.
Med., 20, 3I6.and (I965). Ibid., in press.
Derobert, L., and Hadengue, A. (I947). Ann. Med. lIg., 27,I30.
de Weerdt, W. (1939). Rev. belge, Sci. med., II, 297.Dietrich, A. (I9Io). Folia haemat. (Lpz.), 9, 297.
Dobriner, K., and Rhoads, C. P. (1940). Physiol. Rev., 20,4i6.
Doniach, I., Gruneberg, H., and Pearson, J. E. G. (I943).J. Path. Bact., 55, 23.
Douglas, A. S., and Dacie, J. V. (I953). clin. Path., 6, 307.
Dresel, E. I. B., and Falk, J. E. (I954). Biochem. ., 56, I56.and (I956a). Ibid., 63, 72.
- and (1956b). Ibid., 63, 8o.Dumas, R. (1903). Arch. gin. Mid., 192, 2567.Dustin, P. (I943). Arch. Biol. (Liege), 55, 475.
(I944). Ibid., 55, 285.Duvoir, M., Pollet, L., Gaultier, M., and M6ndtrier, J.
(1938). Sang., 12, 906.Ehrlich, P. (i885). Charite-Ann., I0, I36.Engel, C. S. (I900). Berl. klin. Wschr., 37, 455.Eriksen, L. (I955). Scand. J. clin. Lab. Invest., 7, 8o.Falk, J. E., and Dresel, E. I. B. (I952). IIe Congr. int.
Biochimie, Paris, I952. Resumis de Communications,p. 8.
Ferrata, A. (1933). Le Emopatie, Vol. I., part I. SocietaEditrice Libraria, Milan.
and Boselli, S. (IgIo). Folia haemat. (Lpz.), 10, 451.
Fici, V. (I920). Folia med. (Napoli), 6, 587.(192ia). Ibid., 7, 82.(192ib). Ibid., 7, 20I.
Foa, P. (I889). Beitr. path. Anat., 5, 253.Fontana, A., and Stazzi, S. (I933). Clin. med., 14, 3 1.
Fratianne, R. B., Griggs, R. C., and Harris, J. W. (1959).Clin. Res., 7, 384.
Fullerton, J. M. (I952). Brit. med. J., 2, II7.Gajdos, A., and Gajdos-Torok, M. (1958). Sang., 29, 444.Gajdos-Torok, M., Gajdos, A., and B6nard, H. (1958). C. R.
Soc. Biol. (Paris), 152, I689.and (ig60). Ibid., 154, 508.
Garta, I. (i949). Wien. klin. Wschr., 6i, 6io.Gaultier, M., Fournier, E., and Gervais, P. (i962). Bull.
Soc. med. H6p. (Paris), 113, 863.G&rard, A., Guerrin, F., and Roussel, P. (i964). Arch. Mal.
prof., 25, 346.Gilligan, D. R., Altschule, M. D., and Katersky, E. M.
(1941). . clin. Invest., 20, I77.Goldberg, A. (ig60). Proc. 2e Colloque Int. de Biol. de Saclay.
Ashenbrucker, H., Cartwright, G. E., and Wintrobe,M. M. (I956). Blood, II, 82I.
Goldblatt, M. W. (1955). Brit. J. industr. Med., 12, I.
and Goldblatt, J. (1956). In Industrial Medicine andHygiene, Vol. 3. Ed. Merewether, E. R. A. Butter-worth, London.
Gould, S. E., Kuilman, H. J., and Shecket, H. A. 0937).Amer. J3. med. Sci., 194, 304.
Grawitz, E. (I900). Berl. klin. Wschr., 37, i8i.(I906). Klinische Pathologie des Blutes, 3rd ed. Leipzig.Key, J. E., and Pappenheim, A. (I9I9). Folia haemat.(Lpz.), 24, 86.
Grazianni, G., Fusco, M., and Rossi, L. (1954). Folia med.(Napoli), 37, 643.Pecora, L., and Rossi, L. (1956). Ibid., 39, 217.
Greenough, W. B., Peters, T., and Thomas, E. D. (i962).J. clin. Invest., 41, III6.
Griggs, R. C. (i964). Progr. Hemat., 4, I17.and Harris, J. W. (1958). Clin. Res., 6, I88.
Grinstein, M., Bannerman, R. M., and Moore, C. V. (1959).Blood, 14, 476.Kamen, M. D., Wikoff, H. M., and Moore, C. V.(I95oa). J. biol. Chem., i82, 715.
Wikoff, H. M., Pimenta de Mello, R., and Watson, C. J.(I95ob). Ibid., I82, 723.
Grotepass, W. (1932). Hoppe-Seylers Z. physiol. Chem., 205,
193.
98
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

The Anaemia of Lead Poisoning: A Review
Haeger-Aronsen, B. (I960). Scand. clin. La5. Invest., 12,
SuppI. 47.Haenel, U. (I949). Acta haemat. (Basel), 2, 298.Harris, J. W. (i963). The Red Cell, Production, Metabolism,
Destruction: Normal and Abnormal. Harvard Univer-sity Press, Cambridge, Mass.
and Greenberg, M. S. (I954). Clin. Res. Proc., 2, 55.Heilmeyer, L. (i959). Dtsch. med. Wschr., 84, 176i.
and Begemann, H. (I95i). Blut und Blutkrankheiten.Springer, Berlin.
Henderson, L. L. (I952). Arch. intern. Med., 89, 967.Henning, N., and Keilhack, H. (I940). Dtsch. med. Wschr.,
66, 323.Heubel, E. (i871). Pathogenese und Symptome der chronischen
Bleivergiftung. Hirschwald, Berlin.Hijmans van den Bergh, A. A. (I93I). Wien. med. Wschr.,
8i, 1359.Holecek, V. (I957). Brit. . industr. Med., 14, I98.Hutchison, H. E., and Stark, J. M. (i96i). J. clin. Path.,
14, 548.Jandil, J. H. (ig60). J. Lab. clin. Med., 55, 663.
Inman, J. K., Simmons, R. L., and Allen, D. W. (I959).J. clin. Invest., 38, i6i.
and Simmons, R. L. (i957). Brit. J7. Haemat., 3, I9.and Tomlinson, A. S. (i958). J. clin. Invest., 37, 1202.
Jensen, W. N., and Moreno, G. (i964). C. R. Acad. Sci.(Paris), 258, 3596.
, and Bessis, M. (i965). Blood, 25, 933.Jolly, J. (I907). Arch. Anat. micr., 9, 133.Joyce, C. R. B., Moore, H., and Weatherall, M. (i954). Brit.
J. Pharmacol., 9, 463.Kaplan, E. (i954). Amer. J7. Dis. Child., 88, 808.
Zuelzer, W. W., and Mouriquand, C. (i954). Blood,9, 203.
Kark, R., and Meiklejohn, A. P. (i942). J. clin. Invest., 21,9I.
Karlog, 0., and Moller, K. 0. (1958). Acta pharmacol.(Kbh.), I5, 8.
Karpatkin, S. (i96i). Arch. environm. Hlth, 2, 679.Kassenaar, A., Morell, H., and London, I. M. (I957). J.
biol. Chem., 229, 423.Kench, J. E., Gillam, A. E., and Lane, R. E. (1942). Biochem.
J., 36, 384.Lane, R. E., and Varley, H. (1952). Brit. J. industr.Med., 9, 133.
Key, J. A. (1924). Amer. J7. Physiol., 70, 86.Kienle, F. (I943). Die Sternalpunktion in der Diagnostik.
Thieme, Leipzig.Kin, S. 0939). J. med. Coll. Keijo, 9, IOI.King, E., and Thompson, A. R. (i96i). Ann. occup. Hyg.,
3, 247-Klein, J. R. (i962). Amer. J. Physiol., 203, 97I.Klima, R., and Seyfried, H. (i937). Folia haemat. (Lpz.),
57, 283.Konig, H. (igio). Ibid., 9, 278.Kopasz, E. (I943). Ibid., 67, 292.Korst, D. R., Frenkel, E. P., and Wilhelm, J. E. (i962). In
Erythropoiesis, ed. L. D. Jacobsen and M. Doyle.Grune and Stratton, New York.
Laennec, R. T. H. (i83i). Traite de L'auscultaticn mediate,3rd ed. Chaude, Paris.
Lane, R. E. (I93i). 7. industr. Hyg., 13, 276.(I949). Brit. J. industr. Med., 6, 125.
Lane, C. Rickword, and Lawrence, A. (i96i). Brit. med. J.,
2, 939.Laporte, A., Meyer, A., and Bousser, J. (I939). Bull. Soc.
mid H6p. Paris, 55, 955.Larizza, P., and Ventura, S. (1954). Medicina (Parma), 4, I.
Leikin, S., and Eng, G. (i963). Pediatrics, 31, 996.
Leitner, S. J. (I945). Die intravitale Knochenmarksunter-suchung: Die Hdmatologie im Lichte der Sternal-punktion. Schwabe, Basel.
- (I949). Bone Marrow Biopsy. Eng. trans. rev. and ed.C. J. C. Britton and E. Neumark. Churchill, London.
Lemberg, R., and Legge, J. W. (i949). Hematin Compoundsand Bile Pigments. Interscience Publishers, New York.
London, I. M., and West, R. (1950). J. biol. Chem., 184, 359.
, Shemin, D., and Rittenberg, D. (I950). Ibid.,184, 351.
Lothe, K., and Falbe-Hansen, I. (i963). Clin. Sci., 24, 47.
Lourau, M. (I946). Sang., 1I7, 5I7.(I947a). Ibid., i8, 96.(I947b). Bull. Soc. Chim. biol. (Paris), 29, 34.
(I947c). Ibid., 29, 53I.Lovisetto, P., Sibour, F., and Turco, G. L. (I957). Boll. Soc.
ital. Biol. sper., 33, 149.McCord, C. P., Holden, F. R., and Johnston, J. (I935).
Amer. J. publ. Hlth, 25, Io89.McFadzean, A. J. S., and Davis, L. J. (1947). Glasg. med. .,
28, 237.and- (i949). Quart. J. Med., I8, 57.
MacGibbon, B. H., and Mollin, D. L. (i965). Brit. J.
Haemat., II, 59.Mann, T. S. (i962). Scot. med. J'., 7, 36.Maugeri, S. (I940). Med. d. Lavoro, 31, 97.Maurel, E. (I912). C. R. Soc. Biol. (Paris), 73, 550.Maxwell, L. C., and Bischoff, F. (I929a). J. Pharmacol. exp.
therap., 36, 279.and (1929b). Ibid., 37, 413.
Mellemgard, K., and Sorensen, G. (I955). Ugeskr. Lceg.,117, I27.
Minden, H., and Opitz, H. (1957). Arch. Gewerbepath.Gewerbehyg., 15, 230.
Moeschlin, S. (I957). Schweiz. med. Wschr., 87, I09I.Mollin, D. L. (I965). Brit. J. Haematol., I, 4I.Morel, P., Roche, L., and Baron, J. (I954). Arch. Mal. prof.,
15, 308.Morgan, E. H., and Laurell, C.-B. (I963). Brit. J. Haemat.,
9, 47I-Movitt, E. R. (1945). Amer. J. clin. Path., 15, 557.Naegeli, 0. (I93I). Blutkrankheiten und Blutdiagnostik, 5th
ed. Springer, Berlin.Omeljanienko, L. M. (I954). Thesis, Moscow.Ophuls, W. (I9I5). Amer. J. med. Sci., I50, 5i8.Paolino, W., Resegotti, L., Sartoris, S., and Infelise, V.
(I963). Minerva med., 54, 527.Passow, H., and Tillmann, K. (1955). Pflugers Arch. ges.
Physiol., 262, 23.Pearse, H. E. (I926). Arch. intern. Med., 37, 715.Pecora, L. (I954). Folia med. (Napoli), 37, 82.
Fati, S., and Vecchione, C. (I960). Ibid., 43, 685., Mole, R., and Pesaresi, C. (I963). Proc. XIV
Int. Congr. Occup. Health, Madrid, I963, Vol. III,p. Io68.
Pelaez Redondo, J. (194I). Rev. Clin. esp., 2, 426.Pellegrini, G. (1935). Rif. med., 51, 589.Pernis, B., and Bairati, A. (I959). Med. d. Lavoro, 50, 447.
, and Giubileo, M. (1959). Ibid., 50, 358.and Finulli, M. (I960). Ibid., 51, 48I.Vigliani, E. C., Depretis, Beard, R., and Karlsbad, G.(I964). Proc. XIV Int. Cong. Occup. Health, Madrid,I963, Vol. II, p. 798.
Pirrie, R. (I952). J. Path. Bact., 64, 2II.Prader, A. (I948). Schweiz. med. Wschr., 78, 273.Prankerd, T. A. J. (I96I). The Red Cell. Blackwell, Oxford.Rauch, H. (I922). Z. ges. exp. Med., 28, 50.Riedl, L. (I941). Wien. med. Wcshr., 9I, 697.Rimington, C. (I936). Onderstepoort J. vet. Res. Sci., 7, 567.
(I938). C. R. Trav. Lab. Carlsberg (Sir. chim.), 22, 454.
99
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from

H. A. Waldron
(I95I). In Ciba Foundation Conference on Isotopes inBiochemistry. Churchill, London.
(I952). Acta med. scand., 143, I6I.Roche, L., Lejeune, E., Tolot, F., Mouriquand, C., Baron,
J., Goineau, M., and Soubrier, J. (i96o). Arch. Mal.prof., 21, 329.
Rohr, K. (1949). Das menschliche Knochenmark, 2nd ed.Thieme, Stuttgart.
Roth, E. (i935). Z. klin. Med., x29, I23.Rondanelli, E. G., Gorini, P., Colombi, R., and Verga, L.
(1958). Haematologica, 43, 1077.Rubino, G. F. (i962). Panminerva med., 4, 340.
and Prato, V. (I955). G. Accad. Med. Torino, II8, 23.,and Fiorina, L. (I956). Folia med. (Napoli), 39,
I 1I7., and (1959). Ibid., 42, I.
Pagliardi, E., Prato, V., and Giangrandi, E. (1958).Brit. J7. Haemat., 4, I03.
Saita, G. (1946). Med. d. Lavoro, 37, 207.Fiocchi, F., and Cattaneo, E. (I952). Med. d. Lavoro,43, 99-
and Moreo, L. (1959). Ibid., 50, 37.-, and Petrocchi, L. (1956). Folia med. (Napoli),
39, 217.Sano, S. (i955). Acta haemat. jap., I8, 631.
(1958a). Ibid., 21, SuppI. 2.
(1958b). Ibid., 2I, I57.(1958c). Acta haemat. jap., 21, 337.Inoue, S., Harada, A., and Orita, Z. (I960). Acta Sch.med. Univ. Kioto, Jap., 36, I82.
Tanabe, Y., and Koike, S. (1959). Science, I29,275.
Schmid, R., Hanson, B., and Schwartz, S. (1952). Proc. Soc.exp. Biol. (N.Y.), 79, 459.Schwartz, S., and Watson, C. J. (1950). Ibid., 75, 705.
Schmidt-Kehl, L. (1927). Arch. Hyg. (Berl.), 98, I.Schwartz, H. C., Cartwright, G. E., Smith, E. L., and
Wintrobe, M. M. (i959). Blood, 14, 486.Schwarz, L., and Hefke, H. (I923). Dtsch. med. Wschr., 49,
212.
Seiffert, G., and Arnold, A. (I928). Arch. Hyg. (Berl.), 99,272.
Seip, M. (i953). Acta med. scand., SuppI. 282.Sheets, R. F., Janney, C. D., Hamilton, H. E., and DeGowin,
E. L. (i95i). J. clin. Invest., 30, I272.Simpson, J. A., Seaton, D. A., and Adams, J. F. (i964). J.
Neurol. Neurosurg. Psychiat., 27, 536.Smith, T. (I89I). Trans. Ass. Amer. Phycns., 6, 263.Speransky, J., and Sklianskaja, R. (I928). Folia haemat.
(Lpz.), 36, 289.Sroczyiski, J. (i959). Postepy Hig. Med. d6sw., I3, 74I.--(962). Pol. Arch. Med. wewntt, 32, 673.
- (i963). Postepy Hig. Med. d6sw., 17, 585., Jonderko, G., and Watras, J. (i964). Proc. X Congr.
Int. Soc. Haematol., Stockholm, i964.Strickland, S. C. (I948). N. S. med. Bull., 27, 206.Sumegi, I., Goreczky, L., and R6th, I. (I956). Acta morph.
Acad. Sci. hung., 7, i83.Sundberg, R. D., and Broman, H. (I955). Blood, I0, I60.Sutherland, D. A., and Eisentraut, A. M. (1956). Ibid., ii,
1024.Tanquerel des Planches, L. (I839). Traitis des maladies de
plomb, ou saturnines. Paris.Teisinger, J., Zumanova, R., and Zezula, I. (1958). A. M. A.
Arch. industr. Hlth, 17, 295.Thaddea, S. (1940). Dtsch. med. Wschr., 66, 992.Tishkoff, G. H., Granville, N. B., Rosen, R., and Dameshek,
W. (1958). Acta Haemat. (Basel), 19, 32I.Trakatellis, A. C., Heinle, E., Montiar, M., Axelrod, A. E.,
and Jensen, W. N. (i965). Arch. Biochem., in press.Vannotti, A. (I954). Porphyrins. Hilger and Watts, London.- and Imholz, A. (I939). Z. ges. exp. Med., Io6, 597.Velicogna, A. (I933). Med. d. Lavoro, 24, I.
Vigliani, E. C., and Angeleri, C. (1935). Clin. med. ital.,66, 5.
Vincent, P. C. (I958). Aust. J7. exp. Biol. med. Sci., 36, 589.and Blackburn, C. R. B. (I958). Ibid., 36, 47I.
Vorhaus, E. F., and Turner, J. C. (1957). Blood, 12, 469.Wade, J. F., and Burnum, J. F. (I955). Ann. intern. Med.,
42, 251.Waldron, H. A. (i964). J. clin. Path., 17, 405.Watrach, A. M. (i964). J. Ultrastruct. Res., l0, I77.Watson, C. J. (I936). J. clin. Invest., 15, 327.
(I937)- Ibid., I6, 383.(I950). Arch. intern. Med., 86, 797.(i964). In Diseases of Metabolism. Ed. G. Duncan,5th ed., pp. 850-887. Saunders, Philadelphia.
- and Larson, E. A. (I947). Physiol. Rev., 27, 478.Watson, R. J., Decker, E., and Lichtman, H. C. (1958).
Pediatrics, 21, 40.Weatherall, M. (I952). Biochem. J., 52, 683.Weidenreich, F. (I903). Ergebn. Anat. Entwickl.-Gesch.,
139 I.
Weiss, L. (I957). J. biophys. biochem. Cytol., 3, 599.Westerman, M. P., Pfitzer, E. A., and Jensen, W. N. (i963).
Clin. Res., II, 201.Whitby, L. E. H., and Britton, C. J. C. (1933). Lancet, i,
II73.Wilkinson, J. H. (i962). An Introduction to Diagnostic
Enzymology, Arnold, London.Wolman, I. J., and Bongiovanni, A. M. (I956). Amer. J3.
med. Sci., 232, 688.Young, R. H., and Osgood, E. E. (I935). Arch. intern. Med.,
55, I86.Zegarski, W. (i963). Acta biol. Med. Soc. Sci. Gedan., 7, 33.
IOO
on June 9, 2020 by guest. Protected by copyright.
http://oem.bm
j.com/
Br J Ind M
ed: first published as 10.1136/oem.23.2.83 on 1 A
pril 1966. Dow
nloaded from