Embed Size (px)
Citation preview

www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2011) 46, 252–255
Pediatric surgical images
An unusual presentation of a congenital intrahepaticarterioportal fistula in an infant with Down syndromeJames N. Bogert a, D. Dean Potter a,⁎, Sheri Crowb,Grace M. Arteaga b, Deborah K. Freese c
aDivision of Pediatric Surgery, Mayo Clinic Rochester, Rochester, MN 55905, USAbDivision of Pediatric Critical Care, Mayo Clinic Rochester, Rochester, MN 55905, USAcDivision of Pediatric Gastroenterology and Hepatology, Mayo Clinic Rochester, Rochester, MN 55905, USA
Received 28 June 2010; revised 10 August 2010; accepted 11 August 2010
0d
Key words:Intrahepatic arterioportalfistula;
Congenital fistula;Portal hypertension;Down syndrome;Vascular malformation
Abstract Congenital intrahepatic arterioportal fistula is a rare entity that most often presents withsymptoms of portal hypertension and malabsorption. We discuss a patient who presented withdistributive shock, congestive heart failure, pulmonary hypertension, ascites, and a history ofsevere constipation.© 2011 Elsevier Inc. All rights reserved.
Congenital intrahepatic arterioportal fistula (IAPF) is arare entity that most often presents with symptoms of portalhypertension and malabsorption [1]. We discuss a patientthat presented with distributive shock, congestive heartfailure, pulmonary hypertension, ascites, and a history ofsevere constipation.
1. Case report
A 79-day-old Amish boy was transferred to our institutionintubated for septic shock. He was a term infant that was bornat home without complication. On day of life 3, he wasbriefly hospitalized for dehydration and hyperbilirubinemia.He was treated as an outpatient for pneumonia and
⁎ Corresponding author. Tel.: +1 507 284 8391; fax: +1 507 284 0058.E-mail address: [email protected] (D.D. Potter).
022-3468/$ – see front matter © 2011 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2010.08.016
constipation at 1 month of age. His parents could not recallthe timing of his first bowel movement; however, he stoolednormally until 1 month of age when he became ill withpneumonia. Since that time, his ongoing constipation hadbeen treated with several home remedies including goat'smilk and a special mixture of cow's milk and corn starch.Approximately 48 hours before admission, he became febrilewith a loss of appetite. He was taken to an outside emergencyroom where his temperature was 41.2°C with an oxygensaturation of 70% in room air. He was intubated andtransferred to our pediatric intensive care unit. He had noimmunizations. He takes no other medications at home.
Physical examination was significant for stigmata oftrisomy 21 including flat nasal bridge, protruding tongue,and epicanthal folds. There was no jaundice, and his stoolwas guaiac positive. His abdominal examination revealedhepatomegaly with a liver 3 cm below the costal margin,marked distention, and a fluid wave. The rectum and analorifice were normally positioned, and digital stimulationresulted in forceful expulsion of stool. Diagnostic paracent-esis found the ascites to be sterile.

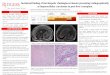
Fig. 2 Transfemoral common hepatic artery angiogram definingthe arterioportal fistula. (1) Common hepatic artery, (2) gastrodu-odenal artery; (3) dilated left hepatic artery, (4) right hepatic arterywith decreased peripheral perfusion. Arrows indicates filling of leftportal veins via the fistula.
253IAPF presentation in an infant with Down syndrome
Treatment for a presumed diagnosis of Hirschsprung-associated enterocolitis was started, which included intrave-nous antibiotics, frequent colonic irrigations, and a rectalbiopsy when he stabilized. Laboratory studies were consis-tent with sick euthyroid and adrenal insufficiency. Supple-mentation with thyroxine and methylprednisolone improvedhis condition. Echocardiography demonstrated a largeatrioseptal defect with left to right shunt, severe right atrialand right ventricular enlargement, and near systemicpulmonary hypertension. His sepsis improved within 24hours of steroid supplementation; however, his pulmonaryhypertension and ascites proved to be refractory. Aggressivediuresis resolved his ascites; however, his hepatomegalypersisted. A full-thickness rectal biopsy demonstratedganglion cells ruling out Hirschsprung disease. Feedingswere resumed resulting in normal bowel movements, andtotal parenteral nutrition was discontinued. The severepulmonary hypertension improved marginally with maximalmedical management. Further evaluation of his persistentpulmonary hypertension included a computed tomographyscan of the chest, which revealed findings suggestive ofIAPF (Fig. 1). Subsequent ultrasonography demonstrated 2separate left hepatic artery to left portal vein fistulae withretrograde flow in the left portal vein and antegrade flow inthe right portal vein and the main portal vein. An angiogramwas obtained confirming this anatomy (Fig. 2), and thefistulae were coil embolized (Fig. 3). He has since done wellwith no further evidence of recurrent arterioportal fistulae.His pulmonary hypertension has been treated with sildenafil.Recent echocardiography showed improvement in hiscardiac status with persistent large atrial septal defect(ASD) and atrioventricular (AV) canal defect. The rightventricular enlargement is improved; however, the RVSPremains 60 mm Hg. He underwent repair of his congenitalheart disease without complication. Repeat imaging of thecoiled IAPF is pending.
Fig. 1 Abdominal computed tomography with arterial phaseintravenous contrast demonstrating differential filling of the leftlobe of the liver as compared with the right lobe suggesting anarterioportal fistula. Note the enlarged, ectatic vessels in theumbilical fissure.
2. Discussion
Intrahepatic arterioportal fistulas are rare in children. Themajority are acquired secondary to other conditionsincluding trauma, iatrogenic injury (such as liver biopsy),tumors, and aneurysms [2]. Intrahepatic arterioportal fistulaeare congenital in 15% of patients [2]. These lesions mostoften present with watery diarrhea, malaise, ascites, andfailure to thrive [3]. The mean age of presentation is 3 years[4]. Our case represents a complex and atypical presentationof this condition. Our patient presented with the stigmata of
Fig. 3 Post–coil embolization common hepatic artery angio-gram. (1) common hepatic artery, (2) gastroduodenal artery, (3)dilated left hepatic artery with coli in place, (4) right hepatic arterywith improved distal perfusion. Arrow indicates filling of the distalleft hepatic arterial branches.

254 J.N. Bogert et al.
trisomy 21, sepsis, ascites, congestive heart failure withpulmonary hypertension, and constipation. The constellationof trisomy 21, sepsis, and constipation caused us to first treathim empirically for Hirschsprung-associated enterocolitis.However, rectal biopsies ruled out this diagnosis. Theetiology of our patient's constipation is perplexing. He didnot meet the criteria for hypothyroidism by repeated thyroid-stimulating hormone (TSH) testing; however, early labora-tory studies lead us to treat him empirically for hypothy-roidism. These medications have subsequently been stopped.Recent work has shown that some children with Downsyndrome whose thyroid function tests are within normallimits benefit from thyroid supplementation, suggesting akind of functional hypothyroidism [5]. In addition, deficien-cies in selenium and zinc may lead to decreased circulatinglevels of triiodothyronine and thyroxine [6]. We did notmeasure selenium or zinc levels when our patient presentedto our intensive care unit, but these minerals werereplenished with total parenteral nutrition (TPN). We believethat the etiology of his constipation was multifactorial andincluded functional hypothyroidism, possibly nutritionaldeficiencies secondary to cow's milk, and Down syndrome.
We believe that the etiology of his sepsis resulted fromsignificant diversion of blood through the IAPF (Fig. 4)creating a low flow state to themesenteric vessels and intestinalischemia as evidenced by guaiac positive stool. The addition ofhyperosmolar home remedies to treat his constipation mayhave promoted bacterial overgrowth and exacerbated theintestinal ischemia. This intestinal ischemia led to a breakdownof the blood-enteric barrier, which led to microbial transloca-tion resulting in sepsis [7]. With antibiotic therapy andexcellent intensive care unit support, his bowel functionrecovered and he began to have normal bowel movements.
Significant ascites, which was initially attributed to ourpatient's congenital heart disease and severe pulmonaryhypertension, is a common finding in children with
Fig. 4 Coronal computed tomography with arterial phaseintravenous contrast. Note the dramatic narrowing of the abdominalaorta immediately distal to the takeoff of the celiac trunk (arrow).
congenital IAPF. This is secondary to portal hypertension,which results from portal venous overflow though thehepatic artery to portal venous shunt [3]. Untreated IAPF canresult in upper gastrointestinal hemorrhage secondary tovarices from portal hypertension.
Congential IAPFs are commonly large and involvemultiple arteries and veins. Despite the significant size ofthe fistulae, patients rarely present with congestive heartfailure and/or pulmonary hypertension. This is thought to becaused by the resistance of flow in the hepatic capillary bed,which limits the shunt between the fistulae and the right heart[3,4]. The exception to this occurs in patients with a patentductus venosum that allows a high flow shunt between thearterial circulation and venous system [4]. Our patient hadcongestive heart failure and pulmonary hypertension thatwas not secondary to his IAPF because of the absence of apatent ductus venosum. Multiple echocardiograms havedemonstrated important structural anomalies commonlyassociated with trisomy 21, but no ductus venosus. Inaddition, Doppler ultrasound examinations and angiogramshave failed to identify a patent ductus venosus.
Congenital IAPFs can be classified based on theiranatomy and likely response to embolization [4]. Type 1(unilateral) lesions involve only one of the hepatic arteries.Type 2 (bilateral) lesions involve both hepatic arteries.Finally, type 3 (complex) lesions involve at least one hepaticartery as well as another nonhepatic artery [4]. Type 1 lesionsare successfully treated with embolization. Embolization canbe attempted in type 2 lesions; however, surgical ligationmay be needed in the event of an embolization failure. Type3 lesions are generally not amenable to embolization. Ourpatient's lesion involved 2 separate fistulae both from the lefthepatic artery to the left portal vein. This represented a type 1lesion, and coil embolization was successfully used. Closefollow-up is important because new fistulae that werepreviously undetectable may appear after embolization ofthe main fistula. It is not uncommon for serial embolizationsto be required in the treatment of these lesions [4].
It has been postulated that patients with Down syndromehave a decreased risk for congenital vascular malformationsbecause of the presence of VEGF inhibitors on chromosome21 [8]. The paucity of case reports in the literature describingvascular malformations in Down syndrome patients wouldappear to support this. As the above case demonstrates, thesemalformations do occur in patients with Down syndrome andcan produce devastating effects. Further evaluation of therelationship between Down syndrome and vascular mal-formations is warranted.
3. Conclusion
Intrahepatic arterioportal fistulae are rare entities inchildren that commonly present with ascites, upper gastro-intestinal bleeding, and diarrhea. Our patient presented with

255IAPF presentation in an infant with Down syndrome
distributive shock, ascites, heart failure, constipation, andhematochezia. Initially, his problems appeared to beexplained by the combination of congenital heart diseaseand Hirschsprung enterocolitis. However, it was thecombination of his complex congenital heart disease andIAPF that resulted in bowel ischemia and bacterialtranslocation. The known effects of trisomy 21 on thegastrointestinal tract likely caused him to have paradoxicalconstipation. Fortunately, his IAPF was amenable to coilembolization, and follow-up is ongoing to identify anyenlarging fistulae.
References
[1] Tannuri ACA, Tannuri U, Lima FR, et al. Congenital intrahepaticarterioportal fistula presenting as severe undernutrition and chronicwatery diarrhea in a 2-year-old girl. J Pediatr Surg 2009;44(10):E19-22.
[2] Vauthey JN, Tomczak RJ, Helmberger T, et al. The arterioportal fistulasyndrome: clinicopathologic features, diagnosis, and therapy. Gastro-enterology 1997;113(4):1390-401.
[3] Heaton ND, Davenport M, Karani J, et al. Congenital hepatoportalarteriovenous fistula. Surgery 1995;117(2):170-4.
[4] Norton SP, Jacobson K, Moroz SP, et al. The congenital intrahepaticarterioportal fistula syndrome: elucidation and proposed classification. JPediatr Gastroenterol Nutr 2006;43(2):248-55.
[5] van Trotsenburg AS, Vulsma T, van Rozenburg-Marres SL, et al. Theeffect of thyroxine treatment started in the neonatal period ondevelopment and growth of two-year-old Down syndrome children: arandomized clinical trial. J Clin Endocrinol Metab 2005;90(6):3304-11[Epub 2005 Mar 8].
[6] Thiel R, Fowkes SW. Down syndrome and thyroid dysfunction: shouldnutritional support be the first-line treatment? Med Hypotheses 2007;69:809-15.
[7] Bateman SL, Seed PC. Procession to pediatric bacteremia and sepsis:covert operations and failures in diplomacy. Pediatrics 2010;126(1):137-50.
[8] Greene AK, Kim S, Rogers GF, et al. Risk of vascular anomalies withDown syndrome. Pediatrics 2008;121(1):e135-40.