Embed Size (px)
Citation preview

13
An intuitive person-centred perspective on fibromyalgia syndrome and its management
A L F O N S E T. M A S I
Society is rapidly changing and most people experience considerable stresses in their perceived personal roles and work responsibilities (North- western National Life, 1992; Stresses and strains, 1992) which may lead to 'burn-out' or various illnesses (Masi, 1978, 1993). Stressful interpersonal dynamics are believed to be important factors in health versus illness (or disease), but are not well documented (McEwen and Stellar, 1993). Fibro- myalgia syndrome (FMS) is a complex, multifactorial disorder occurring in physically or psychologically susceptible persons (Yunus and Masi, 1993). Does this physically and psychologically mediated disorder result from a specific neurobiological diathesis, due to a particular biochemical defect? Alternatively, one might speculate that FMS is a reaction-pattern illness precipitated by psychological stresses (Dailey et al, 1990; see also Chapter 7), repetitive strain injuries (Littlejohn, 1989) or other personal impacts resulting from rapidly evolving social changes. Whichever is the more correct belief, the contributing factors are likely to be modulated in individuals by behavioural patterns, constitutional predispositions, and socioenvironmental circumstances (Masi and Yunus, 1990; Masi, 1993; McEwen and Stellar, 1993; see also Chapter 7). In this chapter it is proposed that FMS is a complex spectrum illness with multifactorial biomechanical, neuroendocrine, psychobehavioural and socioenvironmental determinants. Each one or several of these mechanisms might apply to a greater or lesser extent in any particular person and in an individualized manner.
Pressing social and political dynamics are also impacting upon the roles and responsibilities of physicians and other caregivers at many levels. Learning modes, research methods, practice settings and remuneration systems are all undergoing changes (Delbanco, 1992; Dougherty, 1992). Patient-doctor (or doctor-patient) relationships are consequently in flux (Dougherty, 1992). New designations such as client-caregiver or customer- provider indicate the many facets of this profoundly challenging relationship which may be emphasized. Regardless of the terminology in vogue, the patient's perspectives and needs are crucial and should be integrated effectively into a therapeutic relationship (Delbanco, 1992; Siegler, 1993).
In spite of global stresses on the general population and the healing professions, basic tenets of good medical care must be maintained. Proper
Bailli&e' s Clinical Rheumatology-- 957 Vol. 8, No. 4, November 1994 Copyright �9 1994, by Bailli~re Tindall ISBN 0-7020-1867-8 All rights of reproduction in any form reserved

958 A . T . MASI
therapy should include: (a) knowledge of the condition being treated; (b) an understanding or concept of its pathogenesis or biodynamics; and (c) a personalized (patient-centred), empathic approach to the patient's prob- lems or concerns (Masi and Yunus, 1990; Jackson, 1992; Masi, 1993; Zinn, 1993). These criteria may appear self-evident, since they reflect Hippocratic traditions (Temkin, 1991) as well as more modern medical teaching (Masi and Yunus, 1990; Delbanco, 1992; Dougherty, 1992; Zinn, 1993). However, achievement of such goals is often a great challenge and may become even more difficult in settings of restricted medical resources (Dougherty, 1992).
Personalized care is complex, both in its elements and in its overall goals (Masi and Yunus, 1990; Delbanco, 1992; Dougherty, 1992; Siegler, 1993). An intuitive, empirical perspective of biopsychosocial issues in FMS and their relevance to patient-centred management is offered in this chapter. The related, but separate, clinical entity of myofascial pain syndrome (MPS) is not addressed systematically, but is periodically referred to (Masi, 1993; see also Chapters 3, 9 and 10). Emphasis in this perspective is upon why a particular person may develop FMS (or related disorders), rather than a more traditional focus upon which factors might cause this condition. However, both approaches are considered to be appropriate and are encouraged for research and management goals.
HOLISTIC PERSPECTIVE OF FMS
Is FMS an accepted medical-psychological entity?
To start, a fundamental question might be whether or not FMS is a medical- psychological entity? Is it a valid diagnosis or disease (Mindham et al, 1992), both with respect to its nosological designations (Figure 1) or biophysio- logical mechanisms? If FMS is an accepted medical-psychological entity, can it be defined reliably and how might it best be managed? Alternatively, FMS might not be an accepted medical-psychological entity. Rather, it might be an heterogeneous mix of personal and physical complaints related to social incongruences or life's hardships, e.g. marital, occupational or social stresses, without fundamental biophysiological determinants. In this case, the problems might not be best addressed by primary medical or psycho- logical means, but rather by other social institutions or resources.
Presently, no absolute answers can be given to these enigmas and complex sociomedical issues as they might apply to one or another person (or patient). A combination of medical, psychological and sociological approaches may be appropriate in FMS and related dysfunctional disorders, depending upon the person and his or her circumstances. Hippocratic traditions over the ages (Temkin, 1991) have encouraged a broad commit- ment in medicine to relieve suffering from diverse illnesses, whether strictly defined or not. Under such precepts, FMS may be considered a medical entity, at least with respect to addressing its causes and the relief of suffering in this complex condition.

"/
1 1 .
959 AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS
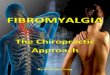
Figure 1. The blind physicians and the elephant: the neurologist (chronic tension headache), the gastroenterologist (irritable bowel syndrome), the otorhinolaryngologist (temporo- mandibular joint syndrome), the cardiologist (costochondritis), the rheumatologist (FMS), and the gynaecologist (primary dysmenorrhoea syndrome). Controversy also exists with respect to biophysiological mechanisms in FMS. From Block (1993, Rheumatic Disease Clinics o f North America 19: 61-78), with permission.
A biopsychosocial view of FMS and related dysfunctional syndromes
In any particular person suffering from FMS, the relative contributions of 'biological' predispositions (e.g. neuroendocrine, physical, physiological and psychological) versus 'socioenvironmental' stressful living factors (e.g. educational difficulties, environmental hardships, family and interpersonal problems, occupational demands or socioeconomic stresses) are not easily determined.
Dedication to healing and the relief of suffering are intrinsic goals in the spirit and ethics of medicine and its.allied health professions (Temkin, 1991; Dougherty, 1992; Siegler, 1993; Zinn, 1993). When persons suffering with FMS present to physicians or other professional caregivers with typical complaints, a 'patient-caregiver' relationship is likely to develop. In any one person, it is not known if social support systems (e.g. family, job counsel- lors, trusted relatives or friends) might or might not be more appropriate or effective than medical caregivers in helping to cope with the problems of FMS. Non-medical personal helpers might address various important aspects (or 'causes') of the patient's concerns and should be actively mobilized to assist with such problems. However, it is not likely that many such helpers would understand or be capable of taking the leadership direction in managing most of the complex 'clinical' manifestations of FMS, particularly the symptomatic, dysfunctional aspects or the illness concerns of the patient.
FMS is characterized by widespread musculoskeletal pains, i.e. articular

960 A . T . MASI
and para-articular, as well as dysfunctional symptoms in multiple systems of the body. On examination, the patient shows localized tenderness at multiple discrete soft tissue sites, i.e. 'tender points', which may be more or less generalized (Block, 1993; Yunus and Masi, 1993). Unlike in MPS (see Chapters 3, 9 and 10), 'trigger points', which radiate pain distantly, are not characteristically found in FMS in symptomatic areas or sites of localized tenderness. However, they may be present when radiation of pain occurs or when significant limitation in range of motion (ROM) is found. The cause and significance of tender points and trigger points in FMS and MPS are not known. Their precise differentiation must await further research (Hubbard and Berkoff, 1993; see also Chapters 3, 9 and 10). Tender points are 'markers' of FMS, but trigger points seem also to be dynamic factors in perpetuating the manifestations of MPS (see Chapter 10).
Regarding nomenclature, should this chronic, painful, multisystemic dysfunctional syndrome be designated strictly by its characteristic musculo- skeletal pain manifestations (i.e. be properly called 'fibromyalgia') or be designated by a term reflecting its composite constellation of varied symptoms and physical manifestations (i.e. be properly called 'fibromyalgia syndrome')? Another viewpoint (Cohen and Quinter, 1993) would consider that either diagnosis is tautologous without having an external validation of hyperalgesia. Such an objection raises the question of whether or not the fundamental problem is one of pain processing, specifically a disorder of secondary (referred) hyperalgesia (Arroyo and Cohen, 1993), or, alterna- tively, a more diffuse, ingrained bioneuropsychological diathesis. This chapter reviews both viewpoints, but favours the latter, broader concept of a more generalized syndrome than central hyperalgesia (Yunus, 1992).
The term 'fibromyalgia' is a more accurate designation than the earlier diagnosis of 'fibrositis', since pain and not inflammation is the characteristic feature in this disorder. Also, 'fibromyalgia' gives emphasis to peripheral, musculoskeletal manifestations and calls attention to such mechanisms in this disorder. Alternatively, the term 'fibromyalgia syndrome' also indicates the major musculoskeletal component, but implies a broader range of biophysiological manifestations involving other systems. The latter term, i.e. FMS, is preferred and used in this chapter to designate this complex condition.
Regardless of the true origins and mechanisms of FMS (or 'fibromyalgia'), its sufferers usually present via a 'medical process'. Patients often express concerns to caregivers about their future health and well-being as well as report various limiting dysfunctions in their personal lives. Current concepts argue for FMS to be viewed as a 'clinical syndrome' (Goldenberg, 1987; Wolfe, 1989; Masi and Yunus, 1990; Wolfe et al, 1990; Bennett, 1993; Wolfe and Hawley, 1993; Yunus and Masi, 1993). However, a broader socio- medical view of FMS, and the family of related dysfunctional spectrum syndromes (Masi and Yunus, 1990; see also Chapter 7), may offer a better understanding of the biodynamics (Masi, 1993). Thus, FMS may be considered to be a valid medical entity. It is prevalent in the population (Masi, 1993; Wolfe et al, 1993) and deserves priority research as well as practice commitment.

AN INTUITIVE PERSON'CENTRED PERSPECTIVE ON FMS 961
FMS is an i l lness, but not a disease!
Although FMS is an illness that can be reliably diagnosed at an acceptable level of consistency (Goldenberg, 1987; Wolfe, 1989; Masi and Yunus, 1990; Wolfe et al, 1990; MYOPAIN '92 Consensus Committee, 1993), it cannot be considered to be a pathophysiologically defined disease. No aetiological agent(s), specific physiological aberration(s) or organ tissue pathology have yet been demonstrated in FMS. Furthermore, FMS may be part of a severity or distribution gradient with regional (Figure 1) or diffuse 'rheumatisms' (Block, 1993), and overlapping with chronic fatigue syndrome or other functional systemic illnesses (see below).
A constellation of subjective symptoms characterize FMS: i.e. chronic widespread musculoskeletal aching pain, generalized stiffness, arousal sleep disturbances, persisting fatigue, a variety of systemic organ dysfunctions (including headache, bowel and bladder dysfunction), anxiety, depressive reactions or dysphoria. Objective findings include multiple, characteristic soft tissue tender points, which are essential to the diagnosis (Goldenberg, 1987; Wolfe, 1989; Masi and Yunus, 1990; Wolfe et al, 1990; MYOPAIN '92 Consensus Committee, 1993). FMS can be effectively diagnosed and reliably categorized (Yunus et al, 1989a; Wolfe et al, 1990), in spite of its broad range of manifestations.
Classification of FMS
Physicians manage their patients as individuals, with a unique disorder, yet we must communicate in terms of groups of patients sharing similar symptoms, signs and prognoses; this necessitates specific diagnoses and classification (Decker, 1983). In the American College of Rheumatology (formerly American Rheumatism Association) nomenclature and classifi- cation of arthritis and rheumatism (Decker et al, 1983), fibrositis and fibromyalgia are listed as generalized forms of 'D. Miscellaneous pain syndromes' within the major category 'IX. Extraarticular disorders'. This classifcation is retained in the current Primer on the Rheumatic Diseases (Schumacher, 1993).
Fibromyalgia is to be incorporated in the World Health Organization tenth revision of the International Classification of Diseases as number M 729.0 (MYOPAIN '92 Consensus Committee, 1993). A Fibromyalgia Consensus Conference was held at the MYOPAIN '92 Symposium in Copenhagen, August 20, 1992 (MYOPAIN '92 Consensus Committee, 1993), at which time a broad clinical description of fibromyalgia was drafted, consistent with current concepts (Goldenberg, 1987; Wolfe, 1989; Masi and Yunus, 1990; Wolfe et al, 1990). The American College of Rheumatology 1990 criteria for the classification of fibromyalgia (Wolfe et al, 1990) were recommended as an operational definition. In these criteria, a history of widespread musculoskeletal pain and multiple tender points are sufficient for classification, rather than also incorporating non-rheumatic items such as anxiety, irritable bowel syndrome and non-restorative sleep (Yunus et al, 1989a). Classification criteria and guidelines for diagnosis of FMS will likely

962 A .T . MASI
evolve as a result of future research and improved understanding of the genesis of this disorder.
Subclassification and subgrouping of FMS
FMS should be appropriately subclassified (Masi, 1993; MYOPAIN '92 Consensus Committee, 1993; Yunus and Masi, 1993). Primary FMS indicates the absence of other associated, contributory conditions such as rheumatoid arthritis or lupus. Concomitant FMS indicates an association with well-defined conditions such as rheumatoid arthritis or osteoarthritis which contribute partially to some of the manifestations, but are not believed to be the major underlying cause of the generalized manifestations. Secondary FMS is currently believed to occur rarely and results from a specific underlying condition such as hypothyroidism or polymyalgia rheumatica. In such cases, fibromyalgia manifestations should remit, by definition, when the primary disorder is effectively treated (Yunus and Masi, 1993).
A more problematic subcategory might be called 'induced FMS', indicat- ing that the onset of FMS followed various triggering or precipitating events such as repetitive strain injuries (Littlejohn, 1989), postaccident pain syndromes (Saskin et al, 1986) or infections, e.g. with Borrelia burgdorferi (Sigal, 1990). It is not known whether such affected persons would have developed FMS (by virtue of predisposing traits) without exposure to the 'trigger' or what factors influence the type of onset, i.e. 'overnight' versus gradual, or the course pattern of subsequent illness.
The question as to whether or not localized idiopathic rheumatic pain syndromes, e.g. neck, shoulder or low back disorders, represent incomplete forms of FMS (Masi and Yunus, 1986, 1990; Block, 1993; Yunus and Masi, 1993) or varieties of MPS (Masi, 1993; see also Chapters 3, 9 and 10) requires further investigation. For the present, it seems advisable to classify localized or regionalized forms separately from generalized forms of idio- pathic rheumatic pain syndromes.
At the Fibromyalgia Consensus Conference (MYOPAIN '92 Consensus Committee, 1993), recommendations were also made that future research should consider further patient subgroupings in order to increase com- parability among epidemiological and clinical studies. In addition to levels of severity (e.g. mild, moderate, severe), patients may be subgrouped according to presumed contributory factors or predispositions, e.g. joint- ligamentous hypermobility (Goldman, 1991), significant deconditioning (Bennett, 1989), chronic overuse or overload circumstances (Littlejohn, 1989), or psychosocial determinants (see Chapter 10). Other potential subgroups recognized in FMS are cold (Bennett, 1993) and histamine (see Chapter 10) sensitivity, as well as secondary hyperalgesia (Arroyo and Cohen, 1993). Subgrouping efforts may improve the accuracy of epidemio- logical (Masi, 1993) and clinical therapy (see Chapter 11) studies, as well as the efficacy of individual patient management (Masi and Yunus, 1990). Subsetting should be based upon reliably documented criteria and not arbitrarily useful clinical groupings: The entity of diffuse multifocal MPS

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 963
may stimulate FMS because of its widespread pain and multiple 'tender' or 'trigger' points, but may not persist after the regional muscular abnor- malities are corrected (see Chapter 10). This entity may be an associated disorder in a person who is predisposed to FMS, but who only manifests diffuse symptomatology when sleep patterns become chronically disturbed (see Chapter 10). Differentiation of FMS from diffuse multifocal MPS may guide therapeutic approaches. However, current clinical distinctions between these clinical entities may not be sufficiently precise to establish a valid subgroup. Criteria for future subgroups of FMS should include statistical correlations. Considerable future research is needed to clarify the complex issues of FMS subsetting.
Overlaps of FMS with related dysfunctional syndromes
Frequent overlaps occur between FMS and other functional disorders, e.g. irritable bowel syndrome, tension headache and primary dysmenorrhoea syndrome (Hudson and Pope, 1989; Yunus et al, 1989b; see also Chapters 7 and 8), as well as chronic fatigue syndrome (Goldenberg et al, 1990; see also Chapter 5). Further research is needed to more accurately define relation- ships among these other complex disorders of unknown aetiology. Whether they may best be designated collectively as either 'affective spectrum disorder' (Hudson and Pope, 1989; see also Chapter 8) or 'dysfunctional spectrum disorder' (see Chapter 7) is unresolved. Possible factors which might predispose an individual to one or another spectrum disorder need to be further investigated.
A PERSON-CENTRED PERSPECTIVE OF FMS
The aetiology and mechanisms of FMS remain unknown. Complex multi- factorial processes are believed to cause the disturbed physiological functioning in this syndrome (Bennett, 1989; Masi and Yunus, 1990; Masi, 1993; Yunus and Masi, 1993; see also Chapters 1 and 2). The 'causes' of FMS may vary among affected people (Masi, 1993; see also Chapter 7), i.e. different factors and mechanisms may play a relatively greater role in some people, or perhaps some families, than in others. Consideration of the individualized determinants of illness is essential to understanding the disorder, its management strategies and outcomes (Masi, 1993; see also Chapters 6 and 10) (Figure 2).
Causation concepts of illness versus disease
FMS is a more varied and multifactorial disorder than most epidemic diseases in which a specific aetiological agent or toxin is the major contribut- ing cause. In the latter diseases, an individual's psychosocial characteristics may not significantly alter their predisposition to illness or the outcome, as opposed to the dose of the aetiological agent or the person's immunity and

964 A.T. MASI
Constitutional- Hereditary Age, sex, r a c e ~ ~
MuscCircs~i~'~ I /"l~eumrUneO~giCa~e ~ . Physicalstatus ~ Physiologicalfunction _ _ " ~ ~
V Socio-Environrnental \ f Climate ~ [ I B~ tra:p~it S s ~ ~eastvermf UDPoCtmi~n ~ /~m~e y ~ /
| | Psych e - - - , - . . . . . .~ .~ [ - - \ ~tf Noxious agents l J ~ Sleep ~ ~ . ~ I PERSONA ~ /./ (e~. viruses) ] I
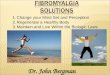
Figure 2. Factors contributing to health versus dysfunctional disorders: a personalized model. Numerous constitutional, psychological-behavioural and socioenvironmental factors con- tinuously affect the person through complex, integrated mechanisms. The constellations may enhance well-being and good function in certain persons or cause suffering and dysfunction in others, whether the problem results from abnormalities in a particular pathway ('box') or the external influences. Traditional, single-factor research approaches and analytic methodology are not likely to reveal the true dynamics of dysfunctional disorders. Personalized, integrated systems approaches offer greater promise in addressing such complex problems. From Masi (1993, Journal of Musculoskeletal Pain 1: 113-136), with permission.
tolerance status. In dysfunctional syndromes, physiological and psycho- logical patterns of reactivity to perturbing or aggravating factors may vary considerably among different persons and may influence their predispo- sition (see Chapters 4 and 7). Individualized physiological responsiveness to commonly prevalent, non-specific 'stress' factors (Dailey et al, 1990; North- western National Life, 1992; Stresses and strains, 1992) may contribute to a person's risk of or outcome from a dysfunctional illness (Figure 2).
In this chapter, it is assumed that complex combinations of physiological aberrations are more important contributors to FMS than any particular 'agent' or single 'metabolic defect'. Clinical manifestation in FMS seems to be best characterized as a chronic, generalized 'downside readjustment' in physiological fluctuations that most persons normally experience during daily or seasonal cycles, i.e. worse aching, pain, stiffness, sleep quality, affect and energy than normal (see Chapter 6). It is suspected that the complex, multifactorial physiological control mechanisms are operating in an integrated fashion, but that they have become dyssynchronized as a 'field' phenomenon. Such integrated deviations from normal would suggest a complex multifactorial imbalance rather than a 'single agent' aberration as the cause of FMS.
If such assumptions are true, then the disturbances in FMS would tend to be person specific. Hence, person-centred research and management would be more relevant in FMS than in diseases with major aetiological factors and only minor personalized contributors. Simply stated, in FMS, 'the person

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 965
may be the specific'. New paradigms of clinical judgement (Feinstein, 1994) and causation (Masi, 1993) are needed to address dysfunctional syndromes as opposed to diseases with specific pathophysiological aetiologies.
Multifactorial physiological aberrations from normal in the susceptible person
The various theories presented in this volume, especially the chronobio- logical concept (see Chapter 6), emphasize the critical importance of multi- factorial, biophysiological (not pathological) aberrations in FMS (and related disorders). Integrated study of the brain (and the mind), behaviour and somatic function over time promises to enhance research into the causes of FMS (Masi, 1993; see also Chapter 6). Also, comprehensive, patient- centred approaches are core to effective therapeutic interventions (see Chapters 6 and 10). In a systems model, aberrations in any physiological system may be within normal limits, but aggregate factors might still contribute to symptoms or dysfunction in the susceptible person.
Neurobiology of pain and its complex dynamics
A signal concept in these disorders is the effect of 'plasticity' in neurobio- logical (see Chapter 7) and even behavioural (see Chapter 5) phenomena. Such mechanisms could explain modulation (expansion or regression) of nociceptive and other fields that may influence pain or other symptoms. Pain is a multidimensional problem which involves (and likely affects) cognitive, motivational, behavioural, affective and spiritual, as well as nociceptive and neuropathic phenomena (Rummans, 1994). The nociceptive system is understood as serving dual functions. It provides a discriminative component of pain ('first pain'), which arrives rapidly in the central nervous system (CNS) by means of a lateral (newer) spinal neuronal pathway, and an affective-motivational component of pain ('second pain'), that arrives later and is subserved by the medial (more primitive) spinal system (Fields, 1987; Cross, 1994). The latter system gives rise to the unpleasant sensations with their affective reactions. The entire system responds to a variety of stimuli in the environment and to the physical and emotional needs of the organism (Cross, 1994).
Neural network 'plasticity' mechanisms may be generally analogous to other biological processes involved in task learning, muscular coordination or emotional development that characterize complex living organisms (Weiner, 1992), but not computer networks (Dreyfus, 1992, 1993/94). Organisms are functionally (if not structurally) modified by individualized biophysiological (Gabbard, 1992) and psychosocial (Post, 1992) stimuli, possibly by fundamental learning processes (Dreyfus, 1992, 1993/94) or stress-related physiological reactivity (Weiner, 1992).
In such plasticity and learning paradigms, one must consider not only the negative effects of stressful stimuli, but also the potential benefits of positive experiences in some individuals' lives. Positive relationships may be associated with recovery from or improvement in anxiety and depressive

966 A.T. MASI
disorders (Brown et al, 1992). A general thesis has been developed that pleasurable stimuli, including love, hope, faith, laughter and restful sleep, have healing and strengthening effects (Lehrman, 1993).
Biochemistry of emotions--a psychosomatic network
Neuroscience, immunological and physiological research are showing that emotions can be mediated by chemical processes in the brain as well as other cells in the body (Pert et al, 1985). Many neuropeptide mediators such as endorphins and their opiate receptors can also modulate pain sensation as well as the general stress reactivity of the body (see Chapter 7). Stress- related physiological changes are believed to alter affect as well as pain receptivity (see Chapter 7). The aggregated effects of biochemical and neuromediator processes can also influence physical behaviours and affect other physiological functions such as sleep (Moldofsky, 1989; see also Chapters 6 and 7).
Altered neuromediator pain modulation is proposed as the primary abnormality in FMS (Yunus, 1992; see also Chapter 7), perhaps as a result of constitutionally or genetically determined mechanisms (Russell et al, 1992; Yunus, 1992; see also Chapter 7). Accordingly, research may justifiably concentrate on the new medical frontier of neurochemical processes and their physiological ramifications. Such emphasis is technically and scientifically attractive and may lead to the discovery of either specific markers for FMS or its effective therapy, as with lithium in the case of manic-depressive disorder.
Recently, a gene mutation has been discovered in the mouse on chromo- some 5 (comparable in many functions to human chromosome 4) which affects the circadian rhythm in that animal (Vitaterna et al, 1994). Con- ceivably, comparable genetic controls might be discovered in humans and possibly be dysfunctional in FMS patients. Alternatively, multiple causes and exposures may be contributing to FMS, as is believed to be operating in the 'Gulf War syndrome', a blanket term for one or several illnesses (Milner et al, 1994). This syndrome complex is characterized by chronic fatigue, skin rashes, decreased concentration and memory, muscle and joint pain, dyspnoea and headache. The combination of physical (heat), psychological (fear of attacks) and toxic (chemical smoke) exposures experienced by Gulf War veterans is believed to have contributed to this group of disorders.
A fundamental question in FMS is whether a specific molecular aber- ration will be found which is intrinsic (inborn) or whether adaptive (learned) aberrations are disturbing the normal physiology and psychology. A classic model of disease would tend to favour the former viewpoint (i.e. a specific aetiological defect) whereas a systems model favours the latter concept (i.e. a multifactorial physiological dyssynchrony).
Biopsychosocial considerations on affect
Affect (Latin affectus disposition, affection, desire) generally connotes feelings and emotion as well as the psychological definition of 'the conscious

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 967
subjective aspect of an emotion considered apart from bodily changes' (i.e. 'non-somatic mood') ( Webster' s New International Dictionary, Unabridged, 1981). Some scholars of affect distinguish 'emotion' and 'mood'. Emotions (especially acute) usually can be related to situational events, whereas most moods do not seem to be clearly related to specific referrents (Morris, 1989). However, mood is believed to be a product of natural selection. It serves an evolutionary purpose, regulating activity as a function of resources and effectiveness of current strategies (Lazarus, 1991). One may assume that affect results from an extraordinarily complex and integrative process involving endogenous homeostasis and introspective controls as well as interactive psychosocial feedback mechanisms. Affect may be a biopsycho- social product and, in turn, emotional and mood states influence essential activities, including behaviour, cognition, communication and physiological functions.
Developmental psychology, particularly that of parent-infant inter- actions, may hold clues to the processing of affect. Secure or insecure parent-infant attachments may lead to subsequent secure or insecure personalities and behaviours (Holmes, 1993). Similar principles of 'attach- ment theory' are also believed to apply to relationships between psycho- therapists and patients. Provision of a secure base is believed to be the common ingredient of various effective psychotherapies and may lead to a new interpersonal paradigm in psychotherapy (Holmes, 1993). Similar life- long biological effects of early nurturing versus separation have been observed within the sciences of ethology and animal behaviour (Weiner, 1992).
Research on 'human nature' has not yet evolved to a level of precise science. However, studies from anthropology and evolutionary psychology suggest that the human mind is influenced by specific instincts. In turn, instincts are believed to be 'trained' by experience and learning, which are triggered by outside stimuli. Thus, instincts are believed to be 'designed' by natural selection for the purposes of expression in certain environmental circumstances. This view holds that differences between people result from different environmental triggers acting upon common genetic substrates (Anon, 1993).
The 'nature-nurture' contributions to human (and other organism) biology are dynamically integrated. Thus, biological interactions should be considered to the fullest extent possible for better understanding of complex disorders (McEwen and Stellar, 1993; Shorter, 1993). A simplified model for affect might be, controlled life--~positive effect--~controlled life, and vice versa, uncontrolled life--~negative affect--~uncontrolled life. Under such a theory, favourable situations and circumstances would tend to engender advantageous emotions and moods, which tend to favour achievement of psychosocial goals. The opposite would also tend to be true within such a concept of reinforcing or modulating experiential loops.
A fundamental question, therefore, is what purpose or survival advantage may be served by negative affect? Sadness and low mood may be an unconscious 'survival' signal that the individual should not actively pursue a certain path (e.g. initiate certain aggressions). Also, such affect may alert

968 A.T. MASI
others to provide help and comforting. The dimensions of affect are vastly more mysterious and complex than the 'three neurone' pathways of noci- ception. Nevertheless, mood states are also believed to have important influence on the modulation of pain sensation (Morris, 1991).
Life stresses, social support and clinical depressionma psychosocial network
Analogous to the biopsychosomatic network of emotions, the social stress- illness (physical and psychological) process is highly complex and contro- versial (Antonovsky, 1987; Vilhjalmsson, 1993). Coping with conflicts and life's stresses characterize 'normal' human behaviour. The maintenance of personal equilibrium and coherence in such settings, with defined status and role sets ('purposefulness'), may not be perceived as stressful or a strain on the individual or her or his health. However, threatening or chaotic situations and loss of personal control, especially with identity crises ('helplessness'), can be distressful and may lead to physical or psychological disorders (Weiner, 1992; McEwen and Stellar, 1993). Social support (e.g. from significant others) may act as a stress modifier of clinical depression (Brown et al, 1992), but such influence is uncertain (Vilhjalmsson, 1993). Many biases exist in such studies. Persons with negative self-evaluations tend to seek or receive social support more frequently than others. Also, varied kinds of stressful situations under investigation have been analysed together. Nevertheless, availability of personal support seems to lower psychological distress and clinical depression (Brown et al, 1992), pre- sumably by conveying a sense of meaning and self-worth.
Little experimental research in FMS has been addressed towards actually modifying life stresses and determining outcomes following such actions, as opposed to observational interview studies which evaluate the patient's perceived psychological stresses or reactivities (Dailey et al, 1990; see also Chapter 7). Whether or not scientifically valid, 'double-blind', controlled trials in this area can be accomplished (e.g. in industry or clinical settings) remains to be determined. Nevertheless, stress reduction can be considered as part of an individual patient's management, within a patient-centred, comprehensive approach (see below).
CAUSAL THEORIES OF FMS
Peripheral musculoskeletal theories
According to peripheral, musculoskeletal theories of the origin of FMS, individuals may become predisposed because of microtrauma of muscles or deficient energy metabolism (Bennett, 1989; Zidar et al, 1990; see also Chapters 1, 2 and 7). Physical deconditioning may further aggravate such inherent tendencies (Bennett, 1989; see also Chapter 10). A vicious circle is proposed of pain---~inactivity--*deconditioning, which increases suscepti- bility to muscle trauma and pain, possibly perpetuated by growth hormone

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 969
deficiency (see Chapters 2 and 4). However, no specific defect of muscle metabolism or definite histopathology has been found in FMS (Yunus and Masi, 1993; Geel, 1994; see also Chapters 2 and 7). In a subset of FMS patients, it is inferred that peripheral musculoligamentous injury (trauma or repetitive strain) may initiate localized pain, which subsequently becomes regionalized or generalized through CNS plasticity mechanisms (Little john, 1989; see also Chapter 7).
Ligamentous hyperlaxity or joint hypermobility is another suspected musculoskeletal mechanism which may predispose to FMS (Goldman, 1991). In such situations, muscles are thought to overwork in order to compensate for the relative postural instability caused by the ligamentous laxity (Masi and Yunus, 1990). Physically deconditioned persons with ligamentous laxity are more likely to develop FMS than persons without either hyperlaxity or deconditioning (Masi and Yunus, 1990; Goldman, 1991). At the opposite physical extreme, I have noted a small minority of FMS patients with overly tight ('muscle bound') bodies, which may predispose to excessive muscle stiffness and pain, especially in cold environ- ments or when fatigued.
Muscle 'tension' and 'tone' disorders may contribute to FMS, but are not well defined (see Chapter 1). These phenomena and their mechanisms are very complex (Johansson and Sojka, 1991; Walsh, 1992). Increased muscle 'tension' connotes neurogenic contractions or spasm. This mechanism is not believed to be an important factor in FMS, since no electrodiagnostic evidence of active muscle contractions is found in FMS (Zidar et al, 1990; see also Chapter 1).
Increased muscle 'tone' (stiffness) is believed to occur in some FMS patients with or without pain. Tone is believed to be influenced by visco- elastic factors as well as by non-neurogenic, physiological contractures, i.e. shortening from painful decreased ROM rather than neurogenic con- tractions. As such, increased tone is electrically silent on electromyography (EMG) testing. However, tone may reflect active control of muscle spindle cells by the sympathetic system via gamma motoneurones (Zidar et al, 1990; Johansson and Sojka, 1991; Walsh, 1992; see also Chapter 3).
The sympathetic gamma motoneurone system may also contribute to the perpetuation of myofascial trigger points (Hubbard and Berkoff, 1993; see also Chapter 3). The neurobiology of the myofascial trigger point is reviewed in Chapter 3.
Cold environments can increase muscle tone as well as tightening, possibly via sympathetic reflexes (see Chapter 10). Increased muscle tone can also result in a prematurely fatigued, energy-poor muscle. Neither increased muscle tone nor tension alone are believed to be sufficient to cause pain, but may do so in the presence of sensitization mechanisms (see Chapter 1). Concepts of muscle 'tension' and 'tone' need to be further clarified, particularly as they may relate to FMS and MPS.
Chapter 10 considers exercises and other physical modalities which are directed at relieving increased muscle tone, stretching contractures, strengthening muscle capacity and re-establishing normal ROM and muscle balance.

970 A .T . MASI
Central theories
As opposed to 'peripheral' mechanisms, central theories propose an underlying CNS neuroendocrine diathesis in FMS which predisposes to decreased tolerance for pain (and other functional reactivities) and non- restorative sleep, with their many consequences. Such manifestations may possibly result from altered metabolism of serotonin or other neuro- transmitters (Moldofsky, 1989; Russell et al, 1992; Yunus, 1992; see also Chapter 7) or limbic dysfunction (see Chapter 5).
Altered interactions between several neurotransmitters and the hypothalamic-pituitary-adrenal axis have also been proposed to occur in FMS (Griep et al, 1993; see also Chapters 4 and 7). Such central factors might be responsible for abnormal peripheral pain modulation in FMS (Yunus, 1992; see also Chapter 7) as well as dysfunctional limbic system regulation of sleep and energy processes (see Chapter 5). Such aberrations may, secondarily, contribute to the non-restorative, arousal sleep disturb- ances (Moldofsky, 1989; Yunus and Masi, 1993; see also Chapters 6 and 7) and other affective-systemic manifestations of FMS (see Chapter 7).
Chronic dysregulation in CNS physiological pathways may lead to the aberrant sleep, frequent arousals, exaggerated fatigue and dysthymic patterns often seen in FMS over daily and seasonal cycles (see Chapter 6). The mechanisms of non-restorative sleep physiology and disturbed bio- rhythms in FMS are not known, but these aberrations seem to be almost universally present in active FMS. New concepts of sleep (Steriade et al, 1993) suggest that fundamental, complex regulatory dynamics and other chronobiological processes (see Chapter 6) are disturbed in FMS and related disorders (see Chapter 5).
Whether or not primary central neurobiological disturbances in pain control lead to secondary emotional or behavioural disorders, as found in FMS (see Chapter 7), is not presently known. Alternatively, if chronic psychosocial stresses can be transduced into neurobiological processing, as reviewed above (Gabbard, 1992; Post, 1992; Weiner, 1992; Holmes, 1993), then the individual's affect, behaviours, pain and general physiological reactivity to various stimuli might all become altered as part of a complex dysregulation. Questions remain as to the origin(s) of the altered central reactivities and the provoking stimuli.
Emotional psychological theories
A concept is proposed in Chapter 8 that FMS and its associated conditions constitute an 'affective spectrum disorder' family. These disorders are believed to be caused by common underlying biological diatheses and should be viewed as a cluster rather than as discrete entities.
Other theories relate a subgroup of FMS patients to intrinsic or secondarily acquired emotional dysfunctions, e.g. anxiety or depressive reactivity (Blumer and Heilbronn, 1982; Goldenberg, 1989b). Emotional disorders could promote enhanced sympathetic activity and exaggerated pain sensi- tivity as well as behaviourally related suffering and sick role modelling

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FI~IS 971
(Blumer and Heilbronn, 1982; Fordyce, 1988; Goldenberg, 1989b; Masi and Yunus, 1990; Morris, 1991; see also Chapters 7 and 10). The fundamental emotional aberrations which may contribute to FMS or related syndromes in certain individuals are not known. However, they are not believed to be simply variations of depressive illness or somatoform disorders (Blumer and Heilbronn, 1982; Goldenberg, 1989b; Morris, 1991; see also Chapter 7).
Dysfunctional syndromes may result from varied and individualized experiential trauma or disturbances to the host (Weiner, 1992; McEwen and Stellar, 1993; Shorter, 1993). After an acute injury or a subacute dys- functional stage, some individuals, but not others, may progress to chronic pain and disability (see Chapter 10). Such poor outcomes may possibly be due to 'ingraining' of neurophysiological dyssynchronies that do not restore to normal. To what extent differences in risk and outcome of FMS are the result of intrinsic, preconditioned emotional, physical and physiological factors or the person's degree of social support or rehabilitative resources is not known.
Simplified framework to encompass causation theories in FMS
Proposed mechanisms in fibromyalgia may be analysed within an hierarchical framework at various phenomenological levels. Three theories (Blumer and Heilbronn, 1982; Bennett, 1989; Moldofsky, 1989) are outlined in Table 1. Such comparisons may help to build an integrated picture of FMS from which more critical analyses can proceed within particular patient subgroups (Masi, 1993) or help to target management plans (Masi and Yunus, 1990).
Pain and suffering is a fundamental human reaction to a broad spectrum of injury and socioenvironmental stresses (Fordyce, 1988; Morris, 1991). Each theory of FMS should explain the chronic, exaggerated pain (Cohen and Quintner, 1993) and other dysfunctions in this disorder (see Chapter 7). It does not seem likely that FMS is either a hyperalgesic diathesis alone or simply a 'somatic' expression of 'psychic' pain (Btumer and Heilbronn, 1982). Rather, it seems that the outlined hypotheses are spectral represen- tations of different mechanisms which overlap and which are likely to apply in varying degrees and extents to. different patients. Multiple determinants seem to be operating in FMS at different 'hierarchical' levels within the affected person.
Complex interactions of multiple factors operating at various levels fit better into a general systems theory model (Leigh and Reiser, 1992; Weiner, 1992; Boyd and Noble, 1993; McEwen and Stellar, 1993) than a direct cause-effect disease model (Masi and Yunus, 1986; Masi, 1993). The interacting mechanisms are likely to be synergistic, individualized and regulated by complex neurohumoral control systems (see Chapters 5 and 7).
PERSON-CENTRED CHALLENGES IN FMS
In conceptualizing FMS, attention needs to be given to the particular person and how various factors may or may not affect that individual's complex

972 A . T . M A S I
o
%
0
q~
o~
oo , ~
0 r
c~
" ~ ~ ~
~.~ ~ ~ �9 ~ ~ N ~ ~:~'~ ~
o = .= ~.
~== .- - ~ ~ o ~ ,~ .~
o 0
~ ~ ~ ~ o o ~
o = ~, ~ ~ ~ ~ ~
0
'ID
0
0
�9
I!

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 973
physiology and functioning at various levels. Valid subgrouping or sub- setting of patients (see above) may facilitate proper aggregation of data, in order to assist clinical judgement (Feinstein, 1994) or target management (Masi, 1993).
Systems model of FMS and subsetting
Systems models (Masi, 1993) are a better concept for dysfunctional syndromes generally than are the classical disease paradigms of primary aetiological agents, host constitutional susceptibilities and environmental determinants (Masi and Yunus, 1986). Causal mechanisms would seem less likely to be proved in dysfunctional syndromes than in pathological diseases of yet unknown aetiology such as rheumatoid arthritis and lupus. However, in dysfunctional syndromes, important contributory factors relevant to a particular individual may be identified, or at least suspected. Such presumed determinants can help to categorize patients within appropriate subgroups (e.g. secondary fibromyalgia)or subsets of primary FMS (Figure 3).
Further research is needed to determine whether or not FMS is truly a 'spectral' syndrome consisting of definable subsets (Figures 1 and 3). The implications of defined subsets for research and therapy are profound. Assuming that one could identify valid subsets of FMS patients with different combinations (or relative intensities) of determinants that influence the onset or course, then management could be more effectively individualized and targeted to a particular patient's contributory factors and reactivities (Figures 2 and 3).
- Endocrine ~ ~ ] - OA - Inflammatory - RA, SLE, CTDs - Post-traumatic f ~ - Other disorders
Socio-environmental factors: Neuroendoorine factors: - H o m e - j o b stresses - Cold intolerance - Litigation pending - Low energy-easy fatigue - Unemployed, unproduct ive - N e u r o a u t o n o m i c imbalance - Unrealistic roles ~ . j - Non-restorative sleep
Bin-mechanical factors: Psychological factors: - Hyperlaxity - Affective spectrum disorders - Over-use, over-load - Anxiety disorders - Physically decondit ioned - Depression - 'Tight-body' ~ . j - Helplessness behaviours
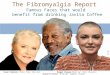
Figure 3. Classification and subsetting of FMS: a personalized perspective to target determi- nants. Criteria need to be established scientifically for valid subsetting in order to identify more homogeneous groups of FMS patients for targeted research and therapy. OA = osteoarthritis; RA=rheumato id arthritis; SLE=systemic lupus erythematosus; CTDs=connective tissue disorders. From Masi (1993, Journal of Musculoskeletal Pain 1: 113-136), with permission.

974 A . T . MASI
Methodological challenges of a systems concept model
The ultimate extension of a multifactorial systems approach to FMS (or other dysfunctional illnesses) is to classify each patient uniquely in terms of her or his set of relevant determinants (Leigh and Reiser, 1992). One is reminded of the admonition that, 'there are no diseases, only sick people'. Empirical illness paradigms (Evidence-Based Medicine Working Group, 1992; Leigh and Reiser, 1992; Sadler and Hulgus, 1992; Wartman, 1992; Boyd and Noble, 1993) intellectually conflict with more scientific concepts of disease caused by specific aetiological agents (Odegaard and Inui, 1992; Masi, 1993). Analogous dilemmas have persisted since the time of Hippocrates between different doctrinal approaches to therapy (Temkin, 1991).
The full spectrum of issues impacting upon a person's health can be overwhelming for both the patient and physician. If strictly addressed, they can cause enormous methodological difficulties in clinical problem solving (Sadler and Hulgus, 1992), teaching (Evidence-Based Medicine Working Group, 1992) and research, i.e. 'multidisciplinary madness' (Wartman, 1992). Innovative and creative ideas, hypotheses and methodologies are needed to address these complex challenges (Wartman, 1992; Feinstein, 1994).
Research needs to resolve tensions between nineteenth century vintage biomedical models of disease (i.e. 'agent-host-environment') and twenty- first century conceptualizations of dysfunctional syndromes (i.e. 'systems theory') (Odegaard and Inui, 1992). Investigators in FMS have the opportunity to take leadership roles in this new scientific challenge and modern dilemma (Feinstein, 1994). Better understanding of the mechan- isms of FMS, its improved management and possible future preventive measures promise to apply also to related functional disorders, which collectively constitute the majority of primary care demands (Odegaard and Inui, 1992).
Neurophysiology of learning and behaviours versus artificial intelligence
When reduced to their final biological pathways, affect, behaviours, learn- ing, pain, psychological reactivity and thinking, whether normal or abnormal, are associated with biochemical processes in the brain. New imaging methods are revealing basic information on how the brain functions. Positron emission tomography has shown that dramatic changes occur in blood flow to the frontal cortex during a new reading task as opposed to after 15 min of practice (Posner, 1993). A rhetorical question is raised: 'how can we any longer separate organic structures from their experience in the organism's history?' (Posner, 1993).
The biology of stressful experiences from a mainly animal experimental viewpoint has recently been reviewed in detail (Weiner, 1992). Dramatic life-long, behavioural and physiological changes are documented after non- physical, experiential perturbations, especially when incurred at early developmental stages. Analogous observations in humans have been

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 975
reviewed above. One may, therefore, suspect that long-lasting neurobio- logical effects may result from perturbed physiological reactivity to life's stresses.
Neurophysiology and cognitive psychology are also being linked by directly studying the dynamics of neuronal populations involved in a variety of cognitive processes (Georgopoulos et al, 1993). A learning model is proposed: problems--~human behaviour-~psychological process--~brain events-->new problems. Learning and cognition processes seem to involve existing, weakly interconnected neurones as well as mechanisms of synaptic strengthening (pathway facilitation).
Interactions between cells in the motor cortex are analogous to those observed in massively interconnected artificial computer networks perform- ing the same computations. Importantly, however, the brain functions as an example of 'organic intelligence', i.e. it is able to adapt to changing stimuli (Weiner, 1992). The brain is able to program itself, based upon past experience, possibly by 'synaptic strengthening' processes. This quantum leap of adaptive self-programming has not yet been achieved in computer science or artificial intelligence (Dreyfus, 1992).
A hierarchical learning model of intellectual skills acquisition for personal performance is summarized in Table 2. It emphasizes the fundamental role of intuitive responsiveness, rather than calculative rationality, in reaching the highest levels of skilled performance (Dreyfus, 1992, 1993/94). In this model, intuition is stated to be the highest level of integrative learning and information processing. Analogous hierarchical processes may occur in emotional development and maturation, which are even less quantifiable. Personal responsibility and involvement seem to be common virtues that need to be developed in order to achieve the higher levels of intellectual skills and emotional maturation (which are mutually reinforcing).
Logistical challenges of a patient-centred management approach
A patient-centred, comprehensive (or 'multidisciplinary') approach to ill- ness management mainly requires a reorientation in attitudes, perspectives and strategies, rather than acquisition of new knowledge (Masi and Yunus, 1990; Siegler, 1993; Zinn, 1993; Frankel, 1994). More active attention needs to be addressed towards disordered functional, physical, physiological, psychological and social dynamics in patient assessment and management rather than the current emphasis on biotechnological and 'pathological' aspects. The patient is approached and evaluated as a 'whole person' and is encouraged to learn and understand the dynamics of her or his illness, in order to become more active in self-care (Masi and Yunus, 1990; Burckhardt et al, 1994; see also Chapters 10 and 12). Over time, the patient assumes increasing responsibility for maintaining an individualized manage- ment programme, with the goal of improved physical, psychological and social functioning, under the guidance and support of the primary caregiver.
Physicians and other caregivers can be unduly challenged (or 'stressed') in this approach, especially during busy work schedules. Logistical difficulties from scheduling demands can be compounded by unfairly limited

976 A.T. MASI
r e i m b u r s e m e n t fo rmulas . T i m e - c o n s u m i n g p e r s o n a l suppo r t of and car ing for pa t i en t s o f t en p rov ide less f inancial r e w a r d than p e r f o r m i n g p r o c e d u r e s o r expens ive t echno log ica l examina t ions . P ro fess iona l d e m a n d s and e c o n o m i c obs tac les to p e r s o n a l i z e d car ing a re rea l and u n f o r t u n a t e l y p r e v a l e n t p r o b l e m s . H o w e v e r , these inequi t ies shou ld be a d d r e s s e d by a p p r o p r i a t e r e fo rms ( D o u g h e r t y , 1992). Idea l ly , t hey shou ld no t be a l l owed to obs t ruc t effect ive p a t i e n t - d o c t o r r e la t ionsh ips and the i r key va lues .
Mul t id i sc ip l ina ry pa in m a n a g e m e n t or r ehab i l i t a t i on cen t res m a y be he lp fu l for comp lex pa t i en t s ( Jensen et al, 1991; F l o r e t al, 1992), a l though such c o m p r e h e n s i v e services a re cost ly ( M a r u t a et al, 1990) and not wide ly ava i l ab le (Brad ley , 1994). T e a m w o r k and c o o r d i n a t e d c o m m u n i c a t i o n s n e e d to be e s t ab l i shed in p rov id ing effect ive in ter - or mu l t id i sc ip l ina ry services (see C h a p t e r 10).
Table 2. A hierarchical learning model of skills acquisitions for personal performance.
Stage 1:
Stage 2:
Stage 3:
Stage 4:
Stage 5:
Rules and priorities determine actions The novice learns simplified characteristics of the challenge and acts in a non-
involved 'rule-following' stance. Such a response is analogous to a heuristically programmed computer based upon knowledge of good practice and good judgement in a field.
Coping experiences modify situational behaviours Based upon previous coping experiences, the advanced beginner learns to
recognize new situational distinctions in interactions or tasks and modifies behaviours from precise rules to meet the special circumstances. Resistance or fear of accepting personal responsibility at this stage can lead to stagnation or even regression of skills.
Perspectives of importance facilitate decision making With even further experience, the competent person acquires a sense of what is
important in any particular situation. Such skills facilitate decision making, based upon 'calculative rationality'. At this stage, a detached mode of analysis can progress to a more advanced, emotionally involved level of performance, e.g. inspired.
Intuitive responses gradually replace calculative rationality Positive and negative experiences strengthen and inhibit the proficient learner's
reactivities, allowing situational discriminations and associated intuitive responses to gradually replace strictly explicit and logical rules and principles. Concern and involvement in this stage seems to promote intuitive assimilation of experiences (and responses) in the brain (mind) in an atheoretical way, which is not simply rational or computer programmable. When goals become obvious, doubt diminishes in complex circumstances.
Intuitive, compelling sense of the one best action The wise expert or grandmaster in most complex situations experiences a
compelling sense of the issues and the one best move. This 'Solomon sense' derives mainly from intuition (i.e. vast, cumulative, assimilated experience) rather than from analysis and comparison of alteratives, i.e. calculative rationality.
Modified from Dreyfus (1993/94).

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 977
Outcome and prognosis of FMS
Person-centred, comprehensive approaches to managing FMS dysfunctions may offer greater benefits to patients and society (Rosen et al, 1985; Maruta et al, 1990; Masi and Yunus, 1990) than conventional treatment modes (Geel, 1994) such as would be employed in controlled therapy trials (see Chapter 11). However, scientifically valid investigations are needed to draw conclusions about relative merits. For example, low dose tricyclic anti- depressants (TCAs) and selective antidepressant agents (Goldenberg, 1989a), aerobic physical conditioning (McCain, 1989) and cognitive- behavioural therapy (Bradley, 1989; Burckhardt et al, 1994) (see also Chapters 11 and 12) have all been shown to offer modest benefits in carefully controlled clinical trials.
Recent findings suggest somewhat improved outcomes with a combi- nation of therapies within the context of multidisciplinary outpatient treatment programmes in FMS (Burckhardt et al, 1994; see also Chapter 12), MPS (see Chapter 9) and chronic pain generally (Maruta et al, 1990; Jensen et al, 1991; Flor et al, 1992). Improvements in patient sub- jective (60-64%) and tender point (48%) ratings were reported for such comprehensive approaches in FMS (see Chapter 12). Interestingly, psycho- logical profiles revealed no significant differences in relation to therapeutic outcomes in one comprehensive management programme (see Chapter 12).
Personalized prognostic factors are now being recognized in FMS. In one large series (Goldenberg et al, 1992), negative outcome factors included psychological distress, current depression, feelings of helplessness, not working or disability, and pending legal action. Whether the negative outcomes could have been improved in a comprehensive or personalized multidisciplinary treatment programme remains to be determined. Never- theless, available findings would seem to support the value of patient subgrouping and multidisciplinary care, in either individualized or clinical trial therapy programmes (Masi and Yunus, 1990; MYOPAIN '92 Con- sensus Committee, 1993).
PATIENT-CENTRED APPROACHES TO THE MANAGEMENT OF FMS
An intuitive, empirical approach to personalized management of FMS has been detailed elsewhere (Masi and Yunus, 1990). This chapter can only briefly outline some elements and mention some clinically relevant aspects in the long term, reinforcing management process. The broad spectrum of management considerations offered are especially relevant in dealing with complex or therapy-resistant patients (Table 3). Many aspects will likely not need to be utilized in milder or moderately difficult cases, but behaviours should be assessed in all patients (see Chapter 10). Further details on these approaches are covered within the preceding chapters of this volume and other detailed clinical references (Goldenberg, 1989a; Bennett, 1993; Wolfe and Hawley, 1993; Yunus and Masi, 1993; Rachlin, 1994).

978 A . T . MASI
Diagnosis and patient assessment
The clinical diagnosis of FMS can be made reliably on the basis of a careful his tory and physical examinat ion. A min imum of labora tory , radiographic or o ther technical p rocedures is needed to exclude confounding condit ions. A n incidental f requency of positivity for ant inuclear ant ibodies (a round 10% or less) in low or mode ra t e titre is found in FMS; the significance is u n k n o w n , but these patients rarely develop lupus (Yunus et al, 1993).
A personal ized, percept ive history by a concerned listener can reveal the basic personal i ty traits and 'coping styles' of the pat ient (see Chap te r 10) and can be therapeut ic (Masi and Yunus , 1990; Zinn, 1993). Careful evaluat ion can fur ther de termine and identify the scope and severity of physical cont r ibutory factors that will need to be addressed in the manage- men t plan (see Chap te r 10). This detailed evaluat ion step is vital for p lanning a m a n a g e m e n t p r o g r a m m e and building a therapeut ic relat ionship (Block, 1993; Frankel , 1994). T he exper ienced physician can demons t ra t e
Table 3. Outline of considerations in the management of FMS,
1. Firmly establish the diagnosis and convince the patient of its benign nature.
2. Educate the patient about the nature of fibromyalgia and its major interacting, multifactorial mechanisms.
3. Reassure the patient that improved function and quality of life usually may be achieved, although discomfort may persist.
4. Offer emotional support and guide the patient in behavioural modifications, i.e. remedying aggravating factors and enhancing relieving ones, with focus on performance goals rather than pain or suffering.
5. Remedy physical perpetuating or aggravating factors, e.g. unfitness, occupational strains, poor posture, ligamentous laxity, obesity or muscle tensing with body cooling.
6. Regularly perform specific stretching exercises, e.g. for neck, shoulders or lower back, as needed for symptom relief and prior to conditioning exercises, as well as utilize massage and other physical measures, e.g. hot showers, baths or other hydrotherapy.
7. Promote physical conditioning with prescribed, graduated exercises.
8. Improve sleep quality, including hygiene measures initially and medication with a low dose tricyclic antidepressant before bedtime, if needed. Trials of newer serotonergic/ noradrenergic drugs may be useful in both sleep and pain control. Tender points persist but symptoms decrease. However, pain control is sufficient.
9. Trial of simple analgesic agents, e.g. salicylates or non-steroidal anti-inflammatory drugs, as needed.
10. Inject disabling and particularly symptomatic tender points with local anaesthetics and corticosteroid preparations, and consider other physical measures to relieve such local problems.
11. Provide psychological support and consider consultation, if necessary.
12. Help the patient commit herself or himself to major management responsibility for self-rehabilitation, pain control and improved function.
From Masi and Yunus (1990), with permission.

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 979
confidence-building professional competence in the careful evaluation of FMS as well as relieve the anxieties of patients who may be suspecting 'undetected' life-threatening or crippling conditions.
Patient education
This essential process can actually start while taking the medical history and performing the physical examination. The patient as well as the doctor can explore and discover possible contributory factors to FMS, e.g. non- restorative sleep, emotional or physical stresses, expressed maladaptive behaviours, postural abnormalities, and obesity or other potential structural predispositions.
Didactic patient education, i.e. explaining simplified mechanisms which may be operating in the development of FMS, can be most helpful. The patient usually benefits from an improved understanding of the benign nature of FMS with regard to health and longevity. Also, explaining the dynamics of contributory factors in the syndrome and the means of coping with such personalized factors is likely to decrease their impact upon symptoms and function (i.e. cognitive-behavioural therapy). Increased patient understanding usually decreases anxiety and enhances compliance with the management programme.
Patient self-management education programmes are designed to: (a) assess needs; (b) develop a coping programme; and (c) evaluate outcome (Burckhardt et al, 1994; see also Chapters 10 and 12). A major goal of education is to refocus attention away from symptoms to improved function and quality of life (see Chapter 10). Better patient understanding of the dynamics of FMS and learning improved coping behaviours may be some of the most valuable means of improving the quality of life with the disorder (Bradley, 1989; see also Chapter 12).
A small minority subgroup of patients are described as cognitively or emotionally deficient and might not be expected to assume independent self-management responsibility (see Chapter 10). However, I have only rarely encountered such patients in a private practice referral setting.
An informal 'daily journal' or more systematic 'graphs' of major activities, including exercises, stressors and symptom levels, can benefit the highly symptomatic patient by pinpointing personal or extrinsic aggravating factors and providing positive feedback on how to manage them better. Patients can become fearful when pain exacerbates. They may believe that the process will enter a 'progressive' phase, especially if precipitating factors which may be contributing to a temporary 'flare up' are not recognized. Also, patients are relieved to know that their symptoms and feelings have an explanation and can be medically explained. As one patient said, 'The best weapon against fear is knowledge'.
Reassurance
This aspect can start with a 'kind and human' attitude. Frustration, insecurities and feelings of inadequacy often accompany dysfunctional

980 A .T . MASI
illnesses. Both caregivers and significant others can often reduce such feelings by displaying a measure of acceptance, human kindness and concern for the patient, i.e. empathy (Jackson, 1992; Zinn, 1993). Sense of dignity and self-respect is often low in persons with fibromyalgia. This can be exacerbated by the negative attitudes or disbelief of caregivers and signifi- cant others. Improved self-esteem and acceptance are essential in helping patients to better cope with chronic symptoms and dysfunctions. In this way, patients are not led to believe that they are alone in dealing with their problems. Patients often state that, 'having a doctor who cares does help how I feel'. Also, they express appreciation for a mutually respectful doctor- patient relationship.
Patients often need help and reassurance in gaining self-acceptance and in relieving guilt related to the limitations of their condition. Severely symptomatic, primary FMS patients can experience symptoms and dys- functions in many systems, which often raises fears in the sufferer of dire medical consequences. The therapist should attempt to allay such unneces- sary concerns and convince the patient that findings which are clinically attributable to FMS are part of that condition.
Experienced therapists can usually demonstrate reassuring and compas- sionate attitudes without spending inordinate amounts of time (Masi and Yunus, 1990; Zinn, 1993; Frankel, 1994), especially by inviting the patient's perspective (Delbanco, 1992). The direct benefit-to-cost ratio of 'caring and kindness' in FMS (Masi and Yunus, 1990) and helping the patient to define personalized goals (see Chapter 10) may be as favourable as any other modality, but no controlled evidence is available.
Emotional support
Perhaps the greatest controversy concerning FMS is the nature of its relationship to emotional and psychological disorders (Blumer and Heil- bronn, 1982; Goldenberg, 1989b; Hudson and Pope, 1989; Yunus et al, 1989b; Wolfe et al, 1993; see also Chapters 7 and 8). Clearly, FMS is not simply a psychological aberration, in the sense of 'psychogenic rheumatism' (Masi and Yunus, 1990; Yunus and Masi, 1993; see also Chapter 7). The admonition that 'It's all in the head', is unfair, inaccurate and usually damaging when applied to FMS. Patients often have great sensitivity and aversion to such labels and perceptions. Many times, patients will build unreasonable defences to guard against suggestions of emotional stresses or dysfunctions, fearing that such manifestations might be interpreted as weaknesses or inadequacies in their character or personality.
Emotional problems such as anxiety and depression are common in the population at large, but seem to be further increased in community samples of people with FMS (Wolfe et al, 1993). These disorders are usually mild in FMS and consistent in nature with those seen in patients with other chronic pain syndromes (Yunus and Masi, 1993; see also Chapter 7). A minority of FMS patients referred to medical centres have an increased frequency of past or current major depression (Goldenberg, 1989b; Hudson and Pope, 1989; see also Chapter 8). Therefore, patients and physicians should be

A N INTUITIVE P E R S O N - C E N T R E D PERSPECTIVE O N FMS 981
prepared to realistically address assessment and management of any co- existing emotional problems. Anxieties, depressive reactions, maladaptive behaviours or the uncommon somatization tendencies may be encountered in FMS. Such patients might constitute a subgroup in the spectrum of FMS (Figure 3) that can be targeted for investigation and management of psycho- logical factors.
Mechanisms leading to somatization disorder are outlined in Chapter 5 and in other work (Fordyce, 1988; Shorter, 1993). These tendencies involve increased anxiety, enhanced preoccupation with illness and misinterpre- tation of bodily variations as somatic concerns. Somatization disorder may persist for a lifetime and its expressions may reflect psychological distress. Approaches to this and other challenging emotional disorders should be handled in a personalized, sensitive and structured manner. Psychiatric consultation or referral may be considered (see below).
Usually emotional problems in FMS and MPS are reactions to common situational stresses and interpersonal frustrations and may not be difficult to manage. Patients often need reassurance and support in these circumstances in order to achieve mutual respect in relationships (i.e. gain personal 'strengths') rather than focus upon issues of control (i.e. 'power') or non- control (i.e. 'helplessness') (Masi and Yunus, 1990). Stress and time management education can be helpful, as well as assertiveness training. A concerted effort should be made by the patient to simplify life circumstances and establish realistic priorities. Patients can often be improved with support and guidance of various therapists (which may include family and friends) without psychotropic medications. Community support groups can also be beneficial, as they offer a source of companionship, expression, reinforcement and resource information.
The more distressed or complex patient, e.g. those with maladaptive behaviours (see Chapter 10), major depression or somatization tendencies, may benefit from referral to specialized or multidisciplinary therapy centres (Maruta et al, 1990; Masi and Yunus, 1990; Jensen et al, 1991; Flor et al, 1992; Bradley, 1994). Emotional distress affects symptoms and function, but not the number of tender points (Yunus and Masi, 1993), further supporting the concept that FMS is not simply a psychological aberration.
Treatment of aggravating physical factors
An astute history and skilled examination will usually detect and gauge the importance of physical contributory factors (Masi and Yunus, 1990; see also Chapter 10), as listed in Table 3 and discussed above. Physical contributory factors tend to be relatively more prominent in variants of FMS such as repetitive strain injury (Littlejohn, 1989), in limited FMS (see Chapter 10) and in MPS (see Chapter 9), than in primary FMS (Masi and Yunus, 1990). In resistant cases, specialist consultation, e.g. with physiotherapists, physiatrists, sports or occupational medicine physicians, can be considered to help remedy aggravating physical factors. Conservation of body heat by 'dressing defensively' in cool environments is one of the most important and often overlooked beneficial physical measures. Maintenance of core body

982 A . T . MASI
PATIENT E D U C A T I O N GUIDE
For ou r patients with f ibromyalgia syndrome
Stretching exercises for your neck and shoulders
These exercises can help relieve pain and stiffness in your neck and shoulders. Start them gradually, and do not force the movements if they cause pain. Mild discomfort lastinc a few minutes after exercise is normal.
Sit or stand erect, with hands touching or clasped behind the neck, elbows gently stretched back in line with shoulders. Turn head slowly to right, over to the shoulder, and hold for 3 seconds. Repeat on left side.
With hands relaxed at side, bend your head slowly to the right, trying to touch your shoulder wi th your ear. Pause, return to center, pause again, then repeat on the left side.
Standing or sitting erect, arms relaxed at sides, roll shoulders up and forward, then down and as far back as you can, breathing deeply. Lower to starting position as you breathe out. Relax. Repeat several times.
Prepared by Alfonse T. Masi, M.D., DR.P.H, University of fllinois, Peoria
Rotate your head up, to the right, down, and to the left, in a wide circle, 3 times clockwise and then 3 times counterclockwisq Pause.
Do all of these steps in the order described to complete 1 set. Do 3 sets each morning and evening, or more often as needed. A hot shower or bath or a heating pad can be used to relax tight m usctes before you exercise.
Special instructions for you: if exercises worsen your pain or you have any questions, call this office:
THE .~NIIIN~.OF Volume 11, Number 8 - August 1994 M U ~ - ~ ' I r ~ L M I = D ~ N I~ Copyright �9 1994 by Cliggott Publishing Co.
Figure 4. Neck and shoulder stretching exercises. Reproduced with the kind permission of The Journal of Musculoskeletal Medicine (Masi, 1994).

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 983
PATIENT EDUCATION GUIDE
For our patients with fibromyalgia syndrome
Exercises for low back pain and stiffness
Moderate exercise is important to keep your back muscles toned and flexible. Be sure to start exercising gradually and not overdo it. Some mild discomfort for a few minutes after exercise is normal. If your back feels stiff, a hot bath or shower or use of a heating pad will help to relax your muscles just before you exercise.
Knees to shoulders Lie on a firm but comfortable surface in the position shown, with a small pillow beneath your head (A). Raise one knee toward your shoulder, fold hands over it, and gently pull it toward your shoulder, keeping the other knee bent and shoulders fiat on the floor (B). Hold for a count of 10, return to starting position, and relax. Repeat with the other knee. Then bring both knees to the shoulders with ankles crossed (C).
Repeat the 3 steps of this exercise 5 to 10 times twice dally as a regular habit, or more often if pain or 9 t i f f n e s s ~ ~
B
Flat back Lie on back as shown (A). Tighten the muscles of your belly and buttocks at the same time to flatten you r back against the floor (B). Hold for a count of 1 O, then relax Repeat 10 times.
) \
m Prepared by Alfonse T. Masi, M.D., DR.P.H. UniverSity of Illinois, Peoria
Special instructions for you:
If exercises worsen your pain or you have any questions, call this office:
THE J(Xm~AL OF MUSCULOSKELETAL MEDICINE
Volume 11, Number 8 �9 August 1994 Copyright �9 1994 by Cliggott Publishing Co.
Figure 5. Lower back exercises. Reproduced with the kind permission of The Journal o f Musculoskeletal Medicine (Masi, 1994).

984 A . T . MASI
temperature helps decrease elevated muscle tone (see above) (Masi and Yunus, 1990) and may even decrease the tendency to early fatigue which follows muscle tightening.
Home stretching exercises and massage
Patients describe home stretching exercises as one of the most relaxing measures in FMS, albeit temporary, especially when performed after the application of warmth (bath or heating pad). Similarly gratifying statements are expressed about massage therapy. These modalities help to decrease pain and soreness by relaxing muscles and relieving tightness. When tight muscles are used resistively, they may incur microtrauma, which is decreased by preceding 'warm-up' stretching. Hot showers, baths and other forms of heated hydrotherapy complement muscle stretching and relaxing manoeuvres.
Importantly, patients with hypermobile joints and lax, weak muscles may still need stretching as well as strengthening exercises (Masi and Yunus, 1990; see also Chapter 10). The rationale is to re-establish that person's own full ROM and antagonistic muscle balance. In this manner, pain and fatigue are relieved by stretching-out contracted, weak muscles. Thus, pain is first relieved with stretching exercise programmes; such patients then usually also need muscle conditioning and strengthening in order to increase their muscle bulk and reserve (see Chapter 10). Such patients, usually ecto- morphic young women, are believed to be a subgroup of FMS (Figures 3-5).
Promotion of physical conditioning
Fatigue is a major and prominent manifestation of FMS, as it is in chronic fatigue syndrome (see Chapter 5). Fatigue is a complex manifestation, having behavioural, emotional and non-restorative sleep aspects, besides physical deconditioning. It should be actively addressed with carefully graduated physical measures (McCain, !989; see also Chapter 11), improvement of sleep quality (Moldofsky, 1989; see also Chapters 6 and 11) and behavioural modifications (Fordyce, 1988; Bradley, 1989; see also Chapter 12).
Aerobic conditioning exercises, when properly graduated and tolerated, can be helpful in FMS (McCain, 1989; see also Chapter 11). The more severe patient may not tolerate such routines and more modest exercise goals should be set, at least initially. Warm water aerobic exercises are usually best tolerated, especially if any phobias can be overcome.
Strengthening exercises should be included at a later phase of a physical conditioning programme and in graded stages, as tolerated (Masi and Yunus, 1990; see also Chapter 10). Preliminary stretching and warm-up is mandatory to diminish the likelihood of flare-ups in FMS. Isotonic resistance exercises are recommended (Geel, 1994), especially in patients with thin muscles and hyperlaxity syndromes (see Chapter 10). Further aspects of exercise training, physiotherapy and rehabilitation have been reviewed elsewhere (Rachlin, 1994; see also Chapter 10).

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 985
Improvement of sleep quality and use of serotonergic/ noradrenergic agents
The problem of non-restorative sleep in FMS is complex and incompletely understood (Moldofsky, 1989; see also Chapter 6). However, it seems to be one of the most important factors, if not the central aberrant pathway, in this disorder (Table 1). Usually, the difficulty in FMS is not in falling asleep, i.e. insomnia, but rather in staying asleep and awakening feeling rested and refreshed. Contributory factors include 'alpha-delta arousals', restless legs syndrome (RLS), periodic limb movement disorder (PLMD) (replacing the older term, nocturnal or sleep myoclonus), bruxism and sleep apnoea, but the sleep disturbance is most commonly 'for no known specific reason' (Moldofsky, 1989; see also Chapters 6, 7 and 9).
Subjectively, one of the most gratifying aspects of FMS management is the global improvement in the minority of patients whose sleep quality can be enhanced by various 'sleep hygiene' (Hauri, 1993) or drug measures (see Chapter 11). Such patients often indicate that a succession of 'deep-sleep nights' can have a very positive effect in lessening pain and improving ability to cope. Sometimes, improved sleep can be achieved with as little as 10 mg (or even 5 mg) of a tricyclic antidepressant prescribed 1 or 2 h before bed (Masi and Yunus, 1990; see also Chapter 11). Importantly, the drug is not operating as an antidepressant (Masi and Yunus, 1990), but rather as a regulator of the arousal sleep disturbance, in some, as yet, incompletely defined manner.
Specific contributory factors to disturbed sleep, as indicated above, should be addressed by other approaches. In RLS and PLMD, low dosage clonazepam (e.g. 1 mg or less, at hour of sleep) has been found to be useful (Clough, 1987; Krueger, 1990). Other medications used in RLS include carbamazepine and levodopa (Clough, 1987), whereas in PLMD, baclofen, temazepam and imipramine given at night-time have been recommended (Kreuger, 1990). TCAs may aggravate PLMD (Krueger, 1990). Dextropro- poxyphene (propoxyphene USP) in low dosage has also been recommended for these disorders. Some patients have tried rotation of helpful drugs on a nightly or weekly basis as a means of preserving efficacy.
Low dose TCAs have antihistaminic effects. TCAs seem to counteract the disturbing hyperarousal mechanisms in FMS (possibly histamine mediated) and help promote deeper sleep. These drugs may have an antihistaminergic effect in the limbic system (see Chapter 5) as well as a reuptake blocking effect on brain serotonin (Masi and Yunus, 1990; Potter et al, 1991; Russell et al, 1992; Yunus and Masi, 1993; see also Chapter 7). Importantly, the serotonergic/noradrenergic reuptake blocking and enhancing agents may be operating to alleviate pain and other symptoms in FMS via more direct mechanisms than through sleep modulation alone (see Chapters 7 and 11). More research is needed on the pharmacodynamic effects of these agents in FMS.
Morning grogginess and sedation side-effects of TCAs (as well as dry mouth and others) can be a significant problem, especially with higher doses (see Chapter 11). Careful dose titration (i.e. the minimum tolerated and

986 A . T . MASI
effective dose) or drug substitution within the TCA family or among the non-stimulating antihistamines (e.g. diphenhydramine) can sometimes improve compliance. Highest priority should be given to managing sleep problems in FMS with behavioural measures and selected drugs.
Low dose TCAs are usually not effective for anxiety or insomnia. Such symptoms may require separate behavioural, anxiolytic or short-acting hypnotic therapy. Sleep hygiene measures may be helpful; these include alleviation of various physical or situational factors that can interfere with restful sleep (Hauri, 1993). In problem patients, referral to a sleep centre for diagnosis and therapy may be considered (Hauri, 1993). Further reading on this complex, multifaceted area of disturbed sleep in FMS is recommended (Goldenberg, 1989a; Moldofsky, 1989; see also Chapter 6).
Peri- or postmenopausal women should be surveyed for status of hormone replacement therapy, which can affect sleep and general well-being. Various other precautions and measures should be taken to help improve sleep, as outlined elsewhere (Masi and Yunus, 1990; Yunus and Masi, 1993).
Use of simple analgesics and non-steroidal anti-inflammatory drugs
Paracetamol (acetaminophen USP), aspirin and non-steroidal anti- inflammatory drugs are often used in FMS patients with equivocal results (Masi and Yunus, 1990; see also Chapter 11). Controlled therapy trial data do not demonstrate consistent or convincing evidence of benefit (see Chapter 11). Also, side-effects must be considered. Nevertheless, some patients do express modest temporary relief (e.g. 'takes the edge off'), possibly due to relieving post exercise soreness (see Chapter 10).
Narcotic analgesics are not indicated in the day-to-day, chronic manage- ment of FMS because of their limited benefit and addictive potentials. They may have specific indications for acute, new pains, e.g. back or neck strains, for limited intervals. Occasional, reliable patients may be prescribed a bedtime dose of a mildly potent and infrequently addicting narcotic agent such as dextropropoxyphene hydrochloride if it is shown to facilitate and improve sleep, as might be the case in RLS or PLMD. Further research is needed on the limited, specific indication of mild, narcotic analgesics in FMS. It goes without saying that the motivations and trustworthiness of the patient must be evaluated when these agents are either requested or prescribed.
Systemic use of glucocorticoids is not believed to be effective in FMS (Masi and Yunus, 1990; Bennett, 1993; see also Chapter 11).
Elimination of disabling tender points
Therapy of 'tender' points in FMS or 'trigger' points in MPS (but which sometimes also occur in FMS) is an essential element of the management programme in some patients, as indicated elsewhere (Rachlin, 1994; see also Chapters 3, 9 and 10). Various techniques, e.g. manipulative stretching, 'spray and stretch', or injection, may be used effectively to treat myofascial trigger points (Rachlin, 1994; see also Chapter 10). The main indications for

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 987
tender point injections in FMS are: (a) disabling pain (e.g. interfering with essential functions such as driving or sleep); (b) helping to re-establish a full ROM (which needs to be maintained by stretching); and (c) elimination of active pain radiation (as with 'trigger' point injections in MPS) (Masi and Yunus, 1990; Rachlin, 1994; see also Chapters 9 and 10).
Injection therapy generally tends to be more effective with acute or limited syndromes (see Chapters 9 and 10), perhaps following trauma, occupational strains or injuries, than in most FMS patients. The techniques of injection (Masi and Yunus, 1990; Rachlin, 1994; see also Chapter 9) are important and should be mastered by the therapist. However , injection therapy alone, without a centrally effective drug and attention to the entire musculoskeletal or personal problems, usually does not succeed in FMS.
Psychological support Office psychotherapy may range from behavioural guidance, emotional support and general reassurance to the use of anxiolytic or antidepressant drugs in varying dosages. Physicians and other caregivers can choose the level of care consistent with their skills and practice logistics. Non-drug therapy may be performed effectively by a physician's associate staff or by referral to a clinical psychologist or psychiatrist interested in chronic pain problems. A small minority of FMS patients are expected to need referral for psychiatric assessment or therapy; my personal guidelines are given in Table 4.
Various other community resources may he considered, including patient support groups, stress and time management courses to build self-control and confidence, as well as hospital group therapy programmes for anxiety and depression syndromes. Occasionally, one may see a reverse, negative reaction in family or group networks, wherein some individuals may
Table 4. Guidelines for referral of FMS patients to the psychiatric services.
1. Affective0 emotional or psychiatric comorbidity manifestations which independently satisfy DSM-IIIR criteria*, i.e. not considering symptomatology of FMS.
2. Significant maladaptive functioning at home or work that interferes with roles and responsibilities and which is disturbing or disrupting relationships, considering both the symptoms and dysfunctions of FMS and the patient's reactions to them.
3. Deteriorating affective, emotional or psychological coping with the symptoms or dysfunctions of FMS, in spite of best management attempts of primary physician and patient.
4. Opportunities for multidisciplinary management of emotional or psychological problems in patients with a stable but unsatisfactory course, utilizing psychiatrist, clinical psychologist, behavioural therapist and social worker resources.
5. Physician's insecurity in managing a high intensity of patient's emotional or psychological complaints/demands or about the level of psychopharmacological drug therapy needed.
* As in American Psychiatric Association (1987).

988 A . T . MASI
compete with others over 'who has more pain'. Patients should be guided into positive relationships which focus upon enhanced function and not on providing sympathy to the sufferer.
Low dosage anxiolytics, TCAs and newer serotonin reuptake inhibitors (e.g. fluoxetine hydrochloride, sertraline hydrochloride and paroxetine) are easy to administer, are usually well tolerated and can be symptomatically useful for mild affective disorders in FMS. In the minority of psychologically disturbed patients, psychiatric consultation may be preferable for more aggressive behavioural and drug therapy.
Self-management and rehabilitation
The culmination of a person-centred approach is to assist and support the patient in assuming major management responsibility for the control of pain, improved function and general self-rehabilitation (Masi and Yunus, 1990; see also Chapter 10. This objective has been more simply stated by a patient: 'being helped to regain control in my life and participate in my wellness'.
Most patients are willing to accept this role, especially with support of their network of family, friends and loved ones, and particularly when environmental circumstances (e.g. living conditions and occupation) are favourable. All patients should be encouraged to be active participants in their own care and rehabilitation. They may use modalities such as biofeed- back or transcutaneous electrical nerve stimulation which again allows them to feel some sense of control over the pain. Patients should understand that FMS may not be cured and that some degree of chronic discomfort usually continues, but that most patients can expect to achieve a satisfying and productive quality of life. Patients should also learn not to be too demanding of themselves and pace their activities within reasonable limits.
A minority of patients cannot effectively assume management responsi- bility, often because of chronic emotional disorders (e.g. significant anxiety, major depression or somatization) or maladaptive behaviours (e.g. 'help- lessness'), and are likely to have a less good outcome (Goldenberg et al, 1992; see also Chapter 10). Patients failing standard therapy may require structured, multidisciplinary care (Maruta et al, 1990; Masi and Yunus, 1990; Jensen et al, 1991; Flor et al, 1992; Bradley, 1994; see also Chapters 9 and 10). Such comprehensive pain or rehabilitation centres are few (Brad- ley, 1994), but have psychiatric, clinical psychology, behavioural therapy and social services, besides either pain management or rehabilitation resources.
Complex FMS patients often feel loss of control in their lives, which is frightening. Unless a commitment can be made and maintained to achieve positive attitudes and 'take control', self-management is unlikely to succeed. Pain behaviours must be translated into well behaviours (see Chapter 10). If all efforts of the patient and therapists fail to achieve rehabilitation and gainful employment is not possible, then the FMS sufferer may be con- sidered a candidate for disability assistance (Monsein, 1994).

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 989
CONCLUDING REMARKS
Complex multifactorial mechanisms are believed to operate in the causation of FMS and related functional disorders. A person-centred, general systems model is believed to be more appropriate for conceptualization of FMS than the classical 'agent-host-environment' model. A person-centred systems model helps to focus on individualized determinants rather than on generic aetiological pathways, which tend to be emphasized in classical diseases and may or may not apply to a particular FMS patient.
Physicians can choose to participate in as full or as limited a role in the management of FMS as seems appropriate to a mutually satisfying, suppor- tive doctor-patient relationship, without intimidation or frustration of one by the other. Nevertheless, unless the full scope of the therapy were pro- vided the process might not be controlled. A person-centred perspective and approach to this disorder (regardless of the intensity of responsibility assumed) promises to facilitate communications and defuse tensions.
The patient and physician may elect to become an 'expert team of two' (Masi and Yunus, 1990) or additional members can participate in a multidi- sciplinary, comprehensive team management programme (see Chapters 9 and 12) as appropriate. The complexity of the management programme needs to match the complexity of the patient, bothin FMS (Masi and Yunus, 1990) and MPS (see Chapters 9 and 10).
A consensus is beginning to emerge that promising outcomes in FMS and MPS can result from individualized, multidisciplinary, long-term approaches to management (Rosen et al, 1985; Masi and Yunus, 1990; MYOPAIN '92 Consensus Committee, 1993; see also Chapters 9, 10 and 12). Self-management education and related non-drug techniques are essential ingredients in achieving the subjective goals of self-efficacy and enhanced quality of life (see Chapter 12). Short-term controlled therapy trials with single modalities have shown modest degrees of efficacy from many different interventions, but only in small proportions of patients (see Chapter 11). Long-term, multidisciplinary studies are needed, addressing specific person-centred problems (Goldenberg et al, 1992). Such methodo- logical strategies are very complex and costly and have not yet been implemented in FMS. The large investments in comprehensive, prolonged treatment programmes will need to be evaluated in terms of improved 'social outcomes' and economic cost-benefit ratios, as well as subjective measures.
Effectiveness of FMS management may be related to the physician's astuteness in perceiving the major contributory factors in a particular patient's disorders (such as are outlined in Table 1 and Figures 2 and 3). Equally important in achieving a successful physician's (or team) role is skill and success in motivating patients to strive for personalized, self- management goals whenever possible.
The caring physician who knows the patient well and has cultivated a therapeutic relationship (a 'healing physician') is believed to achieve superior outcomes in FMS (Masi and Yunus, 1990). However, no documen- tation is yet available for the validity of this impression. It cannot rest upon

990 A.T. MASI
infe rence or tes t imony, bu t ra ther requires a d o c u m e n t e d ev idence f rom proper ly designed, cont ro l led trials ( M Y O P A I N '92 Consensus Commi t t ee , 1993). Proof of such concepts would s t imulate r enewed emphas is in medi- cine on the person and a greater i nves tmen t in pe r son-cen t red car ing (Masi and Yunus , 1990; Kirsner , 1992; Siegler, 1993; Z i nn , 1993; F ranke l , 1994).
Acknowledgements
Sincere gratitude is expressed to Debbie Harper for outstanding contributions to preparing this manuscript. Appreciation is offered to Margaret Walsh, for her secretarial assistance, Jo Dorsch and Walter Wilkins, for their diligent library research support, all staff of UICOM-P, as well as to Jon Spacht, for expert graphics and photography services, at the Methodist Medical Center of Illinois. Many descriptions of symptoms and dysfunctions resulting from FMS reflect statements made by various patients, who kindly reviewed and commented upon the manu- script. Colleagues and co-authors of this volume are also recognized for their review of this chapter and expert critiques.
REFERENCES
Ahles TA, Yunus MB & Masi AT (1987) Is chronic pain a variant of depressive disease? The case of primary fibromyalgia syndrome. Pain 29: 105-111.
American Psychiatric Association (1987) Diagnostic and Statistical Manual of Mental Dis- orders, 3rd edn, revised. Washington, DC: American Psychiatric Association.
Anon (1992) Fibromyalgia: the Copenhagen declaration. Lancet 340: 663-664. Anon (1993) Evo-economics: Biology meets the dismal science. The Economist December 25:
93-95. Antonovsky A (1987) Unraveling the Mystery of Health. San Francisco: Jossey-Bass. Arroyo JF & Cohen ML (1993) Abnormal responses to electrocutaneous stimulation in
fibromyalgia. Journal of Rheumatology 20: 1925-1931. Beighton P, Grahame R & Bird H (1989) Hypermobility of Joints, 2nd edn, 182 pp. London:
Springer-Verlag. Bennett RM (1989) Beyond fibromyalgia: ideas on etiology and treatment. Journal of
Rheumatology 16 (supplement 19): 185-191. Bennett RM (1993) The fibromyalgia syndrome: myofascial pain and the chronic fatigue
syndrome. In Kelley WM, Harris ED Jr, Ruddy S & Sledge CB (eds) Textbook of Rheumatology, 4th edn, pp 471-483. Philadelphia: WB Saunders.
Block SR (1993) Fibromyalgia and the rheumatisms: common sense and sensibility. Rheumatic Diseases Clinics of North America 19: 61-78.
Blumer D & Heilbronn M (1982) Chronic pain as a variant of depressive disease: the pain- prone disorder. Journal of Nervous and Mental Disease 170: 381-406.
Boyd CAR & Noble D (eds) (1993) The Logic of Life: The Challenge of lntegrative Physiology, 226 pp. Oxford: Oxford University Press.
Bradley LA (1989) Cognitive-behavioral therapy for primary fibromyalgia. Journal of Rheumatology 16 (supplement 19): 131-136.
Bradley LA (1994) Behavioral interventions for managing chronic pain. Bulletin on the Rheumatic Diseases 43(2): 2-5.
Brown GW, Lemyre L & Bifulco A (1992) Social factors and recovery from anxiety and depressive disorders. British Journal of Psychiatry 161: 44-54.
Burckhardt CS, Mannerkorpi K, Hedenberg L & Bjelle A (1994) A randomized, controlled clinical trial of education and physical training for women with fibromyalgia. Journal of Rheumatology 21: 714-720.
Clough C (1987) Restless legs syndrome. British Medical Journal 294: 262-263. Cohen ML & Quintner JL (1993) Fibromyalgia syndrome, a problem of tautology. Lancet 342:
906-909.

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 991
Cross SA (1994) Symposium on pain management--Part I. Pathophysiology of pain. Mayo Clinic Proceedings 69: 375-383.
Dailey PA, Bishop GD, Russell IJ & Fletcher EM (1990) Psychological stress and the fibrositis/fibromyalgia syndrome. Journal of Rheumatology 17: 1380-1385.
Decker JL & the Glossary Subcommittee of the ARA Committee on Rheumatologic Practice (1983) American Rheumatism Association nomenclature and classification of arthritis and rheumatism. Arthritis and Rheumatism 26: 1029-1032.
Delbanco TL (1992) Enriching the doctor-patient relationship by inviting the patient's perspective. Annals of lnternal Medicine 116: 414-418.
Dougherty CJ (1992) Ethical values at stake in health care reform. Journal of the American Medical Association 268: 2409-2412.
Dreyfus HL (1992) What Computers Still Can't Do. Cambridge, MA: MIT Press. Dreyfus HL (1994) What computers still can't do. The Key Reporter 59: 4--9. Evidence-Based Medicine Working Group (1992) Evidence-based medicine: a new approach
to teaching the practice of medicine. Journal of the American Medical Association 268: 2420-2425.
Feinstein AR (1994) Clinical judgement revisited: the distraction of quantitative models. Annals of lnternal Medicine 120: 799-806.
Fields HL (1987) Pain. New York: McGraw-Hill. Flor H, Fydrich T & Turk DC (1992) Efficacy of multidisciplinary pain treatment centers: a
meta-analytic review. Pain 49: 221-230. Fordyce WE (1988) Pain and suffering: a reappraisal. American Psychologist 43: 276-283. Frankel RM (1994) The secret to good patient care. Hospital Physician 30(5): 45-49. Gabbard GO (1992) Psychodynamic psychiatry in the 'Decade of the brain'. American Journal
of Psychiatry 149: 991-998. Geel SE (1994) The fibromyalgia syndrome: musculoskeletal pathophysiology. Seminars in
Arthritis and Rheumatism 23: 347-353. Georgopoulos AP, Taira M & Lukashin A (1993) Cognitive neurophysiology of the motor
cortex. Science 260: 47-52. Goldenberg DL (1987) Fibromyalgia syndrome: an emerging but controversial condition.
Journal of the American Medical Association 257: 2782-2787. Goldenberg DL (1989a) Treatment of fibromyalgia syndrome. Rheumatic Diseases Clinics of
North America 15: 61-71. Goldenberg DL (1989b) Psychiatric and psychologic aspects of fibromyalgia syndrome.
Rheumatic Diseases Clinics of North America 15: 105-114. Goldenberg DL, Simms RW, Geiger A e t al (1990) High frequency of fibromyalgia in patients
with chronic fatigue seen in a primary care practice. Arthritis and Rheumatism 33: 381-387. Goldenberg DL, Brodeur CA, Smith Set al (1992) Prognostic factors in fibromyalgia. Arthritis
and Rheumatism 35 (supplement): $113. Goldman JA (1991) Hypermobility and deconditioning: important links to fibromyalgia/
fibrositis. Southern Medical Journal 84:1192-1196. Griep EN, Boersma JW & deKloet ER (1993) Altered reactivity of the hypothalamic-
pituitary-adrenal axis in the primary fibromyalgia syndrome. Journal of Rheumatology 20: 469-474.
Hauri PJ (1993) Consulting about insomnia: a method and some preliminary data. Sleep 16: 344--350.
Holmes J (1993) Attachment theory: a biological basis for psychotherapy? British Journal of Psychiatry 163: 430-438.
Hubbard DR & Berkoff GM (1993) Myofascial trigger points show spontaneous needle EMG activity. Spine 18: 1803-1807.
Hudson JI & Pope HG Jr (1989) Fibromyalgia and psychopathology: is fibromyalgia a form of affective spectrum disorder? Journal of Rheumatology 16 (supplement 19): 15-22.
Jackson SW (1992) The listening healer in the history of psychological healing. American Journal of Psychiatry 149: 1623--1632.
Jensen MP, Turner JA, Romano JM & Karoly P (1991) Coping with chronic pain: a critical review of the literature. Pain 47: 249-283.
Johansson H & Soika P (1991) Pathophysiological mechanisms involved in genesis and spread of muscular tension in occupational muscle pain and in chronic musculoskeletal pain syndromes. Medical Hypotheses 35: 196-203.

992 A . T . MASI
Kirsner JB (1992) Living with Hippocrates in a changing medical world, with particular reference to the patient-physician relationship. Archives of Internal Medicine 152: 2184-2188.
Krueger BR (1990) Restless legs syndrome and periodic movements of sleep. Mayo Clinic Proceedings 65: 999-1006.
Lazarus RS (1991) Emotion and Adaptation. New York: Oxford University Press. Lehrman NS (1993) Pleasure heals. The role of social pleasure-love in its broadest sense--in
medical practice. Archives of Internal Medicine 153: 929-934. Leigh H & Reiser MF (1992) The Patient: Biological, Psychological and Social Dimensions of
Medical Practice, 3rd edn, 496 pp. New York: Plenum Press. Littlejohn GO (1989) Fibrositis/fibromyalgia syndrome in the workplace. Rheumatic Diseases
Clinics of North America 15: 45-60. Maruta T, Swanson DW & McHardy MJ (1990) Three-year follow-up of patients with chronic
pain who were treated in a multidisciplinary pain management center. Pain 41: 47-53. Masi AT (1978) An holistic concept of health and illness: a tricentennial goal for medicine and
public health. Journal of Chronic Diseases 31: 563-572. Masi AT (1993) Aspects on the epidemiology and criteria of myofascial pain and fibromyalgia:
concepts of illness in populations as applied to dysfunctional syndromes. Journal of Musculoskeletal Pain 1: 113-136.
Masi AT (1994) Management of fibromyalgia syndrome: a person-centered approach. Journal of Musculoskeletal Medicine 11: (in press).
Masi AT & Yunus MB (1986) Concepts of illness in populations as applied to fibromyalgia syndromes. American Journal of Medicine 81(3A): 19-25.
Masi AT & Yunus MB (1990) Fibromyalgia--which is the best treatment? A personalized, comprehensive, ambulatory, patient-involved management programme. BailliOre's Clinical Rheumatology 4: 333-370.
McCain GA (1989) Nonmedicinal treatments in primary fibromyalgia. Rheumatic Diseases Clinics of North America 15: 73-90.
McEwen BS & Stellar E (1993) Stress and the individual: Mechanisms leading to disease. Archives of lnternal Medicine 153: 2093-2101.
Milner IB, Axelrod BN, Pasquantonio J & Sillanpaa M (1994) Is there a Gulf War syndrome? Journal of the American Medical Association 271: 661.
Mindham RHS, Scadding JG & Cawley RH (1992) Diagnoses are not diseases. British Journal of Psychiatry 161: 689-691.
Moldofsky H (1989) Sleep and fibrositis syndrome. Rheumatic Diseases Clinics of North America 15: 91-103.
Monsein M (1994) Disability evaluation and management of myofascial pain. In Rachlin ES (ed.) Myofascial Pain and Fibromyalgia: Trigger Point Management. St Louis: Mosby.
Morris WN (1989) Mood: The Frame of Mind. New York: Springer-Verlag. Morris DB (1991) The Culture of Pain. Berkeley, CA: University of California Press. MYOPAIN '92 Consensus Committee (1993) Consensus document on Fibromyalgia: The
Copenhagen Declaration. Journal of Musculoskeletal Pain 314: 295-312. Northwestern National Life (1992) Employee Burnout: Causes and Cures, part 1: Employee
Stress Levels, a Research Report, pp 1-13. Minneapolis, HN: Northwestern National Life Insurance Company.
Odegaard CE & Inui TS (1992) A 1992 manifesto for primary physicians. Pharos of Alpha Omega Alpha Honor Medical Society 55: 2-6.
Pert CB, Ruff MR, Weber RJ & Herkenham M (1985) Neuropeptides and their receptors: A psychosomatic network. Journal of Immunology 135: 820S-826S.
Posner MI (1993) Seeing the mind. Science 262: 673-674. Post RM (1992) Transduction of psychosocial stress into the neurobiology of recurrent affective
disorder. American Journal of Psychiatry 149: 999-1010. Potter WZ, Rudorfer MV & Manji H (1991) The pharmacologic treatment of depression. New
England Journal of Medicine 325: 633-642. Rachlin ES (ed.) (1994) Myofascial Pain and Fibromyalgia: Trigger Point Management. St
Louis: Mosby. Rosen NB, Sharoff K & Khanna V (1985) The dysfunctional pain patient--returning to work: a
preliminary report. Maryland Medical Journal 34: 605-608. Rummans TA (1994) Symposium on pain management. Introduction. Mayo Clinic Proceedings
69: 373-374.

AN INTUITIVE PERSON-CENTRED PERSPECTIVE ON FMS 993
Russell IJ, V~er0y H, Javors Met al (1992) Cerebrospinal fluid biogenic amine metabolites in fibromyalgia/fibrositis syndrome and rheumatoid arthritis. Arthritis and Rheumatism 35: 550-556.
Sadler JZ & Hulgus YF (1992) Clinical problem solving and the biopsychosocial model. American Journal of Psychiatry 149: 1315-1323.
Saskin P, Moldofsky H & Lue FA (1986) Sleep and posttraumatic rheumatic pain modulation disorder (fibrositis syndrome). Psychosomatic Medicine 48: 319-323.
Schumacher HR (1993) Classification of the rheumatic diseases. In Schumacher HR, Klippel JH & Koopman WJ (eds) Primer on the Rheumatic Diseases, 10th edn, pp 82-86. Atlanta: Arthritis Foundation.
Shorter E (1993) From the Mind into the Body: The Cultural Origins of Psychosomatic Symptoms. Toronto: University of Toronto Press.
Siegler M (1993) Falling off the pedestal: What is happening to the traditional doctor-patient relationship: Mayo Clinic Proceedings 68: 461-467.
Sigal LH (1990) Summary of the first 100 patients seen at a Lyme disease referral center. American Journal of Medicine 88: 57%581.
Steriade M, McCormick DA & Sejnowski TJ (1993) Thalamocortical oscillations in the sleeping and aroused brain. Science 262: 67%685.
Stresses and strains (Anon) (1992) The Economist August 15th: 43. Temkin O (1991) Hippocrates in a world of Pagans and Christians. Baltimore: Johns Hopkins
Press. Vilhjalmsson R (1993) Life stress, social support and clinical depression: a reanalysis of the
literature. Social Science and Medicine 37: 331-342. Vitaterna MH, King DP, Chang AM et al (1994) Mutagenesis and mapping of a mouse gene,
clock, essential for circadian behavior. Science 264: 719-725. Walsh EG (1992) Muscles, masses and motion. The physiology of normality, hypotonicity,
spasticity and rigidity. Clinics in Developmental Medicine 125: Oxford: MacKeith Press. Wartman SA (1992) Multidisciplinary madness: the trials and tribulations of the MD-PhD.
Pharos of Alpha Omega Alpha Honor Medical Society 55: 2-6. Websters Third New International Dictionary (1981) Merriam-Webster Inc. Weiner H (1992) Perturbing the Organism: The Biology of Stressful Experience, 357 pp.~
Chicago: The University of Chicago Press. Wolfe F (1989) Fibromyalgia: the clinical syndrome. Rheumatic Diseases Clinics of North
America 15: 1-18. Wolfe F & Hawley DJ (1993) Fibromyalgia. In Kelley WN, Harris ED Jr, Ruddy S & Sledge CB
(eds) Textbook ofRheumatology, 6th edn, pp 2-16. Philadelphia: WB Saunders. Wolfe F, Smythe HA, Yunus MB et al (1990) The American College of Rheumatology 1990
criteria for classification of fibromyalgia: report of the Multicenter Criteria Committee. Arthritis and Rheumatism 33: 160-172.
Wolfe F, Ross K, Anderson J & Russell IJ (1993) The prevalence and characteristics of fibromyalgia in the general populatioia. Arthritis and Rheumatism 36 (supplement): $48.
Yunus MB (1992) Towards a model of pathophysiology of fibromyalgia: aberrant central pain mechanisms with peripheral modulation. Journal of Rheumatology 19: 846-850.
Yunus MB & Masi AT (1993) Fibromyalgia, restless legs syndrome, periodic limb movement disorder, and psychogenic pain. In McCarty DJ & Koopman WJ (eds) Arthritis andAllied Conditions: A Textbook ofRheumatology, 12th edn, pp 1383-1405. Philadelphia: Lea & Febiger.
Yunus MB, Masi AT & Aldag JC (1989a) Preliminary criteria for primary fibromyalgia syndrome (PFS). Multivariate analysis of a consecutive series of PFS, other pain patients, and normal subjects. Clinical and Experimental Rheumatotogy 7: 63-69.
Yunus MB, Masi AT & Aldag JC (1989b) A controlled study of primary fibromyalgia syndrome: clinical features and association with other functional syndromes. Journal of Rheumatology 16 (supplement 19): 62-71.
Yunus MB, Hussey FX & Aldag JC (1993) Antinuclear antibodies and connective tissue disease features in fibromyalgia syndrome: a controlled study. Journal of Rheumatology 20: 1557-1560.
Zidar J, Bfickman E, Bengtsson A & Henriksson KG (1990) Quantitative EMG and muscle tension in painful muscles in fibromyalgia. Pain 40: 249-254.
Zinn W (1993) The empathic physician. Archives of Internal Medicine 153: 306-312.