Embed Size (px)
Citation preview

© 2012 Lisa R. Nelson
AN INTRODUCTION TO HL7 CDA R2
In support of subject matter expertsparticipating to design CDA-based
electronic public health case reports
Lisa R. NelsonMarch, 2012

© 2012 Lisa R. Nelson
SESSION 1Why do I need to know about CDA R2

© 2012 Lisa R. Nelson
Why would I want to know about CDA R2?1. It will make it easier for us to collaborate2. This technology is emerging as a powerful communication
mechanism and you will be running into in other situations as well
3. Not too many people understand it, so this knowledge makes you a more valuable resource
4. The use of CDA shapes the answer to the question of what information do we need to collect. We need to understand and consider CDA when identifying the information that needs to be captured
5. You will be less frustrated, more efficient and more effective while doing this work if you understand how the information is going to be used and what form it will be molded into.
WIFM

© 2012 Lisa R. Nelson
Background and Significanceof the Research
Why?
Assessment of the Current Use of CDA R2 to Specify Electronic Public Health Case Reports

© 2012 Lisa R. Nelson
Over time, evolution happens.

© 2012 Lisa R. Nelson
Why is CDA R2 valuable?
Message
Transaction
Message
Transaction
CDA R2 Document
Database
Data
Applications Computers

© 2012 Lisa R. Nelson
Why is CDA R2 valuable?
Message
TransactionDatabase
Data
Applications Computers
Message
Transaction
CDA R2 Document

© 2012 Lisa R. Nelson
• CDA documents are “transaction agnostic”• The CDA specification focuses on standard ways to articulate
detailed, sometime voluminous information• Transactions are designed to be fast and sleek to facilitate the
workflow at hand• CDA documents are persistent and robust to facilitate the
accurate “recollection” of what happened in the past or has been planned to happen in the future
• CDA documents are data that is designed to be deposited – residual, at rest – a snapshot for posterity which allows you to iterate back over (playback) events as they happened in time.
• CDA documents act in concert with transactions to complement the task of communicating information
• Designed to work together
CDA documents don’t replace transactions, they augment them.

© 2012 Lisa R. Nelson
• A CDA document is a defined and complete information object that can exist outside of a messaging context and/or can be a payload within an HL7 message (see CDA Document Exchange in HL7 Messages (§ 3 )). Thus, the CDA complements HL7 messaging specifications.
• Any CDA exchange strategy must accommodate the following requirements: • All components of a CDA document that are integral to its state of wholeness (such as attested
multimedia) are able to be included in a single exchange package. • Content needing to be rendered if exchanging across a firewall where the links won't be traversable,
must be able to be included in a single exchange package. • Additional files associated with a CDA document to provide the recipient with the sender's rendering
suggestions (such as one or more style sheets) are able to be included in a single exchange package. • There is no need to change any of the references (e.g., a reference to attested multimedia in a
separate file) within the base CDA document when creating the exchange package. • There is no need to change any of the references (e.g., a reference to attested multimedia in a
separate file) within the base CDA document when extracting the contents of an exchange package. • There is no need to change any values of attributes of type XML ID when creating the exchange
package. • There are no restrictions on the directory structure used by receivers. Receivers can place the
components of the CDA document into directories of their choosing. • Critical metadata about the CDA instance needed for document management (e.g. document state,
document archival status) must be included in the exchange package.
Relationship of the CDA to HL7 Messaging Standards
© 2012 Lisa R. Nelson
• Application systems sending and receiving CDA documents are responsible for meeting all legal requirements for document authentication, confidentiality, and retention. For communications over public media, cryptographic techniques for source/recipient authentication and secure transport of encapsulated documents may be required, and should be addressed with commercially available tools outside the scope of this standard.
• The CDA does provide confidentiality status information to aid application systems in managing access to sensitive data. Confidentiality status may apply to the entire document or to specified segments of the document
Security, Confidentiality, and Data Integrity

© 2012 Lisa R. Nelson
Why is CDA R2 important to Public Health Case Reporting?
• A sustainable approach for standardization of information systems in public health
• Gathers more and better quality information, more efficiently
• Use existing information constructs
• Faster responsiveness to disease conditions
• Help shift focus from responding to illness, to improving prevention
Fighting communicable disease with communicable information.

© 2012 Lisa R. Nelson
Why is CDA R2 important to the Healthcare IT information ecosystem?
Information “orbits”
Individual
Care Providers& trusted
health and care resources
Public Health
A time-independent flow of information exchange between and among health stakeholders.
v
Care providersEducation, Media, HIEsEmergency responders

© 2012 Lisa R. Nelson
• This should be a picture of a CDA being created and then where it might go to be used and how it might get changed or added to along the way
• Concepts to introduce:
Lifecycle of a CDA document
Table 2: Value set for relatedDocument.typeCode (CNE) Code Definition
APND (append) The current document is an addendum to the ParentDocument.
RPLC (replace) The current document is a replacement of the ParentDocument.
XFRM (transform) The current document is a transformation of the ParentDocument.
ClinicalDocument.setID Represents an identifier that is common across all document revisions.
ClinicalDocument.versionNumber An integer value used to version successive replacement documents.

© 2012 Lisa R. Nelson
Historical Events with a Public Health Information Dimension
• Typhoid Mary• AIDS Patient 0• 911• Katrina• Map pinpoints risk areas for Lyme• Tsunami in Japan• Costa Concordia sinks• Bad heart medicine kills hundreds in Pakistan

© 2012 Lisa R. Nelson
• Definitions• Principles• Conceptual frameworks• Goal: Develop our ability to communicate so that we can succeed at
a complex task which requires interdisciplinary collaboration
Overview

© 2012 Lisa R. Nelson
• Integration» Integrated electronic health records
• Interoperability» Syntactic Interoperability
– Structural Interoperability• Semantic Interoperability
Key Definitions
Why are these definitions important?
Discussions about what these concepts meanmove us toward a shared vision
of the goal for health information technology.

…a repository of information regarding the health of a subject of care in computer processable form, stored and transmitted securely, and accessible by multiple authorized users. It has a commonly agreed logical information model which is independent of EHR systems. Its primary purpose is the support of continuing efficient and quality integrated health care and it contains information which is retrospective, concurrent and prospective. (Sebastian Garde, Petra Knaup, Evelyn J.S. Hovenga, Sam Heard.. Towards Semantic Interoperability for Electronic Health Records: Domain Knowledge Governance for openEHR Archtypes. 2007) (International Organization for Standardization. ISO/TR 20514: Health informatics--Electronic health record--Definition, scope, and context. Geneva: ISO, 2005)– Patient-centered – related to one subject of care– Longitudinal – long-term, possibly covering an entire lifetime– Comprehensive – includes records from all types of events: all types of health care
events, not just one specialty– Both past, “present” and future oriented – includes information on goals, plans, orders
and evaluations, not just historical events
Integrated Electronic Health Records
Homework:Youtube.com “George Carlin time”http://www.youtube.com/watch?v=zaR3sVpTB98“There’s only the near future and the recent past. There is no ‘now’.”

© 2012 Lisa R. Nelson
Integration - Develop a pictorial version – with examples

© 2012 Lisa R. Nelson
• …the ability of two applications to share data, with no prior negotiations, such that decision support within each application continues to function reliably when processed against the received data. (HL7 CDA standard. Normative Web Edition, 2005, B.3)
1. Syntactic (data) interoperability: The structure and provenance of information or knowledge is understood by a (clinical) system. This comprises all (machine-readable) aspects of data representation. Syntax can be considered as the grammar to convey semantics and structure.
2. Structural interoperability/Semantic interpretability: The semantics of the information or knowledge provided is explicit and can be analysed by domain experts (clinicians). This involves (health) concept representation.
3. Semantic interoperability: Apart from comprising syntactic and structural interoperability, semantic interoperability requires that the information system understands the semantics of information request and those of information sources. Semantics is defined as the meanings of terms and expressions. Hence according to Veltman [29] semantic interoperability is “the ability of information systems to exchange information on the basis of shared, pre-established and negotiated meanings of terms and expressions.” (Garde, 2007)
Interoperability
© 2012 Lisa R. Nelson
Interoperability - Develop a pictorial version – with examples
© 2012 Lisa R. Nelson
The task at hand: designing public health case reports

© 2012 Lisa R. Nelson
Public Health Case Reports1. Acute Hepatitis B2. Anthrax3. Tuberculosis4. Tularemia5. Influenza6. Chlamydia trachomatis genital infection7. Coccidioidomycosis8. Haemophilus influenzae, invasive disease, all ages, serotypes9. Meningococcal disease, all serogroups10. Pertussis11. Salmonellosis12. Streptococcus pneumoniae, invasive disease13. Pesticide poisoning/exposure14. Toxic-shock syndrome15. West Nile virus
• December, 2011• 68 Nationally notifiable conditions• 8 Other diseases of interest• 76 Listed conditions for public health surveillance
2009 PHCR CDA prototype

© 2012 Lisa R. Nelson
* One of four specific public health case reports specified using current PHCR prototype design.
PHCR Relevant Diagnostic Tests and/or Laboratory Results
Anthrax PHCR Relevant Diagnostic Tests and/or Laboratory Results
Section Analysisacross the PHCR prototype set of documents
CCDContinuity of Care DocumentAll Sections:
PHCR Clinical Information
PHCR Social History
CCD ImmunizationPHCR EncountersPHCR Treatment Information
Anthrax PHCR Clinical Information
Anthrax PHCR Social History
Anthrax PHCR EncountersAnthrax PHCR Treatment Information
PHCRPublic Health Case ReportAll Sections:
Does the PHCR prototype design support data interoperability?How would a computer know?
Anthrax PHCRAnthrax Public Health Case ReportAll Sections:
Acute Hepatitis BTuberculosis
Tularemia
AlertsPayersAdvance DirectivesSupportProblemsFunctional StatusVital SignsMedicationsMedical EquipmentProceduresFamily HistorySocial HistoryResultsImmunizationEncountersPlan of Care
Note: Anthrax PHCR is not a specialization of PHCR. Each of these case report definitions is an extension of the base PHCR definition.

© 2012 Lisa R. Nelson
Entry Analysis for Social History Sections across the PHCR prototype set of documents
12
34
5
67*
89
1011 12*
13
14
PHCR
AcuteHepatitis B
Anthrax Tuberculosis
Tularemia
# Entry Template Name0 SocialHistoryObservation
1 GeotemporalHistoryObservation
2 MostRecentTimeArrivedInUSAObservation
3 RaceObservation
4 OccupationObservation
5 PregnancyObservation
6 JobRelatedBodyFluidExposureRiskFrequency
7* AccuteHepatitisBSocioBehavioralBooleanRiskFactor
8 AccuteHepatitisBActualBloodAndOrBodyFluidExposureObservation
9 AccuteHepatitisBPossibleExposureLocationAndType
10 AnthraxPossibleExposureLocationAndType
11 HIVStatusObservation
12* TuberculosisSocioBehavioralBooleanRiskFactor
13 TuberculosisPossibleExposureLocation
14 TularemiaPossibleExposureLocationAndType
List of Entries defined for the set of Social History Sections Social History Sections with Entries
0CCD
* Entry asserts conformance to the CCD Social History Observation entry.

© 2012 Lisa R. Nelson
Value Set Usage Summary
Section Value SetA Immunizations
B Anthrax PHCR Relevant Diagnostic Tests AndOr Laboratory Data
C Anthrax PHCR Clinical Information Section
D Anthrax Social History Section
E PHCR Encounter Section
F Anthrax PHCR Treatment Information Section
Social History Obs Value Set

© 2012 Lisa R. Nelson
• Present the Case Definition and Position Material back to me– Add other materials if needed
• Think about identifying– Which of the 6 buckets (A-F) would I put this information in?– What are the specific Social History Observations needed to identify a
suspected, or confirmed case?– What Value set would apply here to articulate the possibilities?
Next Steps

© 2012 Lisa R. Nelson
The exploration team!
E X P L O R A T I O N

© 2012 Lisa R. Nelson
SESSION 2
Clinical Document Architecture – Release 2
What do I need to know about CDA R2 and why?
© 2012 Lisa R. Nelson
1. Understand the definition of Ontology and how formal definitions and relationships relate to the Clinical Document Architecture standard
2. Appreciate the time-line of advances in the development and use of CDA and the realities of early invention
3. Identify the six core principles of CDA4. Understand key qualities and attributes of the CDA standard5. Understand the different types of content modules and how they relate to each other6. Explain the different levels of conformance7. Understand concepts of templates and inheritance8. Understand what an OID is and the different ways it can be used9. Learn how CDA Documents have been specified in the past and what new tools are
being developed to support their definition and maintenance in the future10. Understand what code systems and value sets are and how they are used in content
module design11. Appreciate the different data structures that can combine to create an Entry and the
complexity/richness of the CDA standard12. Gain awareness of how HL7 RIM and v3 data types create the foundation for CDA13. Connect these concepts to the current Public Health Care Report design and the
specific content modeling needs for condition-specific case reports
Learning objectives
© 2012 Lisa R. Nelson
Understand the definition of Ontology and how definitions and relationships relate to
the Clinical Document Architecture standard
1

© 2012 Lisa R. Nelson
The philosophical study of being and knowing.
The metaphysical study of the nature of being and existence.
A rigorous and exhaustive organization of some knowledge domain that is usually hierarchical and contains all the relevant entities and their relations.
CDA formalizes information being communicated
mathematical formality
a bc d f
eg
A
A = {a, b, c, d, e, f, g}
{c | c setName}∈
Enumerated
Descriptive/Algebraic
{c | c setName}∉
The set of all c such that
c is a member of the set defined by setName
c is not a member of the set defined by setName
Inequalities can also be used.
A set of concepts and their relationships.
Definition from visualthesaurus.com
Expressing this information using natural languageAND…
© 2012 Lisa R. Nelson
Appreciate the time-line of advances in the development and use of CDA
and acknowledge the realities of early invention
2

© 2012 Lisa R. Nelson
• The Clinical Document Architecture-Release 2 standard• Developed by Health Level Seven (HL7) as part of HL7 v3• When?
– 1997 – CDA got started– 2000 - Release 1– 2005 - Release 2– 20?? - Release 3 – planned for 2010 (updated availability estimate not
established in 2012)
• Use of the Standard?– 2006 Continuity of Care Record introduced by ASTM– 2007 HL7 releases the Continuity of Care Document– Many other document implementations specified since then
What is CDA R2?

© 2012 Lisa R. Nelson
Defined CDA R2 Content Documents
LOINC Profile Name D11369-6 Immunization Content IHE 111488-4 Consultation Note HL7 211502-2, valueSet
XD-LAB (19 specialties: 1 doc template) IHE 3
11504-8 Operative Note HL7 411506-3 Progress Note HL7 511526-1 Anatomoic Pathology Struct Report IHE 611526-1 cancer APSR IHE 2711526-1 Xxxxxx cancer APSR (20 different docs) IHE 7-2618748-4* Cardiology Imaging Report Content IHE 2818748-4 Diagnostic Imaging Report HL7 2918842-5 Discharge Summary HL7 3018842-5 Medical Summaries Profile (Discharge) IHE 3126436-6 Antepartum Laboratory IHE 3228568-4 ED Physician Note IHE 3328570-0 Procedure Note HL7 3428651-8 eNursing Summary IHE 3534117-2 Antepartum History and Physical IHE 3634117-2 History and Physical IHE 3734117-2 History and Physical (H&P) Note HL7 3834133-9 Clinical Research Document IHE 39
34133-9 Continuity of Care Document (CCD) HL7 4034133-9 Drug Safety Content (is a CCD) IHE 4134133-9 Exchange of PHR Summary (Extract) IHE 4234133-9 Exchange of PHR Summary (Update)) IHE 4334133-9 HITSP C32 HL7 4434133-9 Medical Summaries Profile (Referral) IHE 4534746-8 Patient Plan of Care IHE 4634817-7 Early Hearing Care Plan IHE 4734895-3 Antepartum Education IHE 48
LOINC Profile Name D55751-2 Acute Hepatitis B PHCR HL7 4955751-2 Anthrax PHCR HL7 5055751-2 Tuberculosis PHCR HL7 5255751-2 Tularemia PHCR HL7 5355751-2 PHCR HL7 5157055-6 Antepartum Summary IHE 54
57056-4 Labor and Delivery History and Physical IHE 5557057-2 Labor and Delivery Summary IHE 56
57057-2Mother and Child Health - Birth and Fetal Death Reporting IHE 57
57058-0 Maternal Discharge Summary IHE 58
Any LOINC Code Medical Document IHE 59missing LOINC Emergency Department Referral IHE 60missing LOINC Unstructured Document HL7 61
Silent on LOINC Code Medical Summary IHE 62X-NN Nursing Note IHE 63
x-physician-cancer-rep
Physician Reporting to Public Health Cancer Registry IHE 64
X-TRIAGE Composite Triage&Nursing Note IHE 65X-TRIAGE Triage Note IHE 66XX-ETS EMS Transport Summary IHE 67XX-ITS Interfacility Transport Summary IHE 68
XX-NewbornDischargeSummary Newborn Discharge Summary IHE 69
XX-PostpartumVisitSummary Postpartum Visit Summary IHE 70XX-TRS Transport Record Summary IHE 71
71 Different document templates
14 - HL7 57 - IHE
1. Apparent overlap
2. Document “families”
3. Usage similarities
4. Focused on Public Health, Quality and Research
Findings
January 2012
Analysis
More under development in 2012-2013
Which documents hold info that could be useful to public and population health?

CDA document classes across the health information ecosystem2006 - 2011
68 notifiable conditions
ConsCDA
CDA R2
PHCR
© 2012 Lisa R. Nelson
CCD/C32
CCR
XPHRExtr
XPHRUpd
APSR
CancerAPSR
20 types of Cancer APSR documentsAnthrax
PHCR
MedDoc
MedSum
XDSMSReferral
XDSMSDischarge
EDReferral
PRPH-CA
19 types of Lab Report documents with a single document templateXD-
LAB
Inheritance from CCD is not at the document level. Some section and some entry structures are inherited from CCD.
For PHCR,
Discharge
H&P
H&P
APL
APE
APHP
CTNN TN NN EDPN
ENS
IC
Un-structdoc
CRD
LDHP
Hep BPHCR
Tula-remiaPHCR
Tuber-culosisPHCR
ProgressNote
EHCP
LDS
MCH
DSC
Con-Sultnote
Diag ImgingRpt.
Proce-dureNote
Oper-ativeNote
MDS NDS
PPOC
PPVS
ETS
ITS TRS
More in progress through various IHE Domains and HL7 Working Groups
Gartner Hype Cycle

© 2012 Lisa R. Nelson
Identify the six core principles of CDA
3

© 2012 Lisa R. Nelson
1. Persistence – A clinical document continues to exist in an unaltered state, for a time period defined by local and regulatory requirements (NOTE: There is a distinct scope of persistence for a clinical document, independent of the persistence of any XML-encoded CDA document instance).
2. Stewardship – A clinical document is maintained by an organization entrusted with its care.
3. Potential for authentication - A clinical document is an assemblage of information that is intended to be legally authenticated.
4. Context - A clinical document establishes the default context for its contents.
5. Wholeness - Authentication of a clinical document applies to the whole and does not apply to portions of the document without the full context of the document.
6. Human readability – A clinical document is human readable.
The Six Core Principles of CDA R2?

© 2012 Lisa R. Nelson
Understand key qualities and attributes of the CDA standard
4

© 2012 Lisa R. Nelson
• An XML-based markup standard specifying the encoding, structure, and semantics of clinical documents for exchange
• Part of the HL7 version 3 standard– based on the HL7 Reference Information Model (RIM) and the HL7
Version 3 Data Types– developed using the HL7 Development Framework (HDF)
• The structured part relies on the use of code systems (such as from SNOMED CT, LOINC and HL7) and value sets to represent concepts
• Specifies that the content of the document consists of a mandatory textual part (which ensures human interpretation of the document contents) and optional more highly structured parts (for software processing)
• Doesn’t specify how the documents should be transported – “transaction agnostic”
Qualities and Attributes of CDA R2

© 2012 Lisa R. Nelson
Understand the different types of content modules and how they relate to each other
5

A document is a set of content modules
The hierarchy is expressed using the nesting mechanisms of XML.
Each content module has a context which is implied through the nesting or may be explicitly stated for the author, informant and subject.
Uber-section
Entry-part
Basic Hierarchy
© 2012 Lisa R. Nelson
DocumentConformance Rules
Header

© 2012 Lisa R. Nelson
• Sections are human readable clinical information• Entries are machine readable clinical information which give computers
access to the same information that is accessible to human readers.– The entries can be used to derive the narrative text (typeCode=DRIV) OR– The entries can be components of the narrative text (typeCode=COMP) (the default)
• In some cases, computable linkages exist between the machine readable entries and the corresponding narrative text.– Although the principle behind the linkage to support human readability is documented
in the CDA R2 standard, the standard does not mandate that this guideline be followed.– Some implementations require it and others are silent on the issue.
What is the relationship between sections and entries?
Let A = the clinical information contained in the narrative text of a section
Let B = the clinical information contained in the encoded entries of that section
By principles 3 and 6 of CDA R2 , B <= A
!
The same informationmeans the semantic meaning of the information is equivalent for the intended uses

© 2012 Lisa R. Nelson
• Allergy Section– <text>
<content ID="noallergy" styleCode="bold">Active Drug Allergy: The patient has an adverse reaction to LEXAPRO(Escitalopram) which involved Hallucinations. The problem began on October 18, 2011. </content></text>
– Entry: – <entry>
<act classCode="ACT" moodCode="EVN">[stuff removed] <entryRelationship inversionInd="false" typeCode="SUBJ"> <observation classCode="OBS" moodCode="EVN"> [stuff removed]
– <code code="419199007" codeSystem="2.16.840.1.113883.6.96" codeSystemName="SNOMED-CT" displayName="Allergy to substance"/> <text> <reference value="#noallergy"/> </text>[stuff removed]
<value code="160244002" codeSystem="2.16.840.1.113883.6.96" codeSystemName="SNOMED-CT" displayName="No known allergies" xmlns:xsi="http://www.w3.org/2001/XMLSchema-instance" xsi:type="CD"> <originalText> <reference value="#noallergy"/> </originalText> </value> </observation> </entryRelationship> </act> </entry>
Example – Scenario 1
© 2012 Lisa R. Nelson
• Text shows 2 allergies• Entries for 2 allergies• Secenrio 3:• Entry for 1 allergy• Text for 2 allergies• Scenario 4:• Entries for 2 allergies• Text for 1 allergy
Scenario 2

© 2012 Lisa R. Nelson
Explain the different levels of conformance
6
© 2012 Lisa R. Nelson
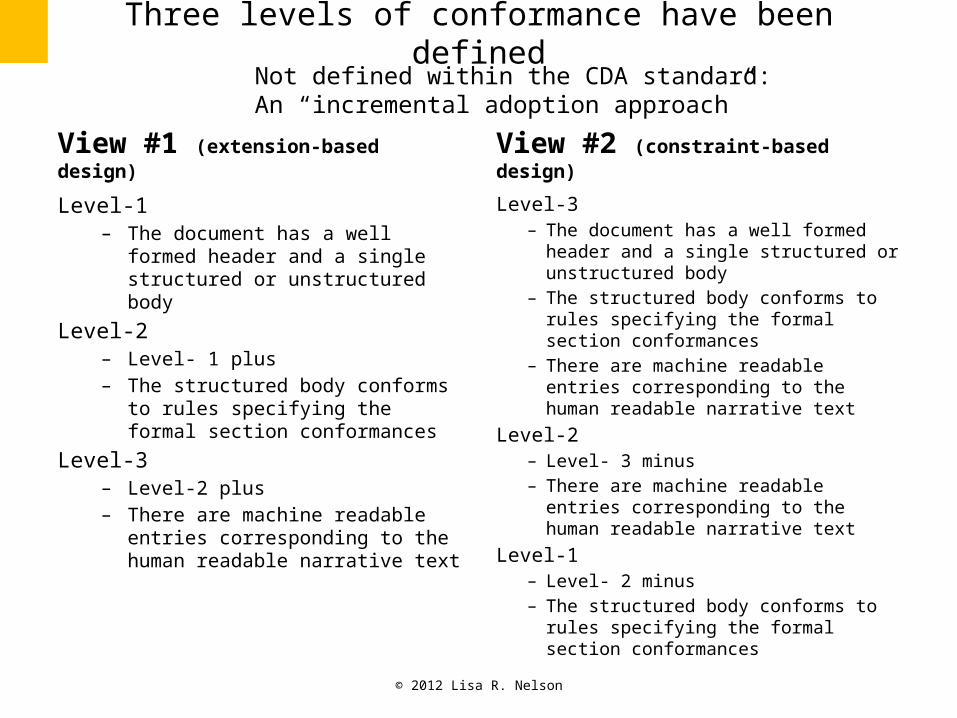
Three levels of conformance have been defined
View #1 (extension-based design)
Level-1 – The document has a well formed
header and a single structured or unstructured body
Level-2 – Level- 1 plus – The structured body conforms to
rules specifying the formal section conformances
Level-3 – Level-2 plus – There are machine readable entries
corresponding to the human readable narrative text
View #2 (constraint-based design)
Level-3– The document has a well formed header
and a single structured or unstructured body
– The structured body conforms to rules specifying the formal section conformances
– There are machine readable entries corresponding to the human readable narrative text
Level-2 – Level- 3 minus– There are machine readable entries
corresponding to the human readable narrative text
Level-1 – Level- 2 minus– The structured body conforms to rules
specifying the formal section conformances
Not defined within the CDA standard:An “incremental adoption approach”

© 2012 Lisa R. Nelson
Understand concepts of templates and inheritance
7
© 2012 Lisa R. Nelson
• Templates are a structure used to define conformance rules• Templates are a set of conformance rules• Templates provide an expedient way to adopt preciously
defined conformance rules, and further constrain them– A parent template allows all the rules that apply to a previous content
module to be inherited by a new content module as it is being defined– Additional templates are then added to include additional
conformance constraints which differentiate the new modules definition from one that has already been defined
– Templates can be used at all levels of content modules
• Templates are used to automate validation of content documents
What are content module templates and how are they used?
© 2012 Lisa R. Nelson
Understand what an OID is and the different ways it can be used
Understand what code systems and value sets are and how they are used in content module design
8 (&10)

© 2012 Lisa R. Nelson
What is an OID?
• An OID is an Object Identifier – it is a unique number, by design
• Content templates are identified with OIDS– The OID is called the templateId– Example: 2.16.840.1.113883.10.20.1 (Asserts: This is an HL7 CCD document)– Example: 2.16.840.1.113883.10.20.15.2.15 (Asserts: This is an
AnthraxPhcrClinicalInformation Section)– Example: 2.16.840.1.113883.10.20.15.3.37 (Asserts: This is an
AnthraxTherapeuticRegimen Entry)
• OIDs are used to uniquely identify other things too– Code Systems are sets of codes that are arranged systematically
• Examples: LOINC, SNOMED CT, HL7 Code Systems• Example: 2.16.840.1.113883.6.96 (Asserts use of the SNOMED CT code system)
– Value Sets are sets of codes from one or more Code Systems• Example: The set of codes used to encode concepts of gender• Example: 2.16.840.1.114222.4.11.926 (Asserts use of the HL7 value set for
Administrative Gender)

© 2012 Lisa R. Nelson
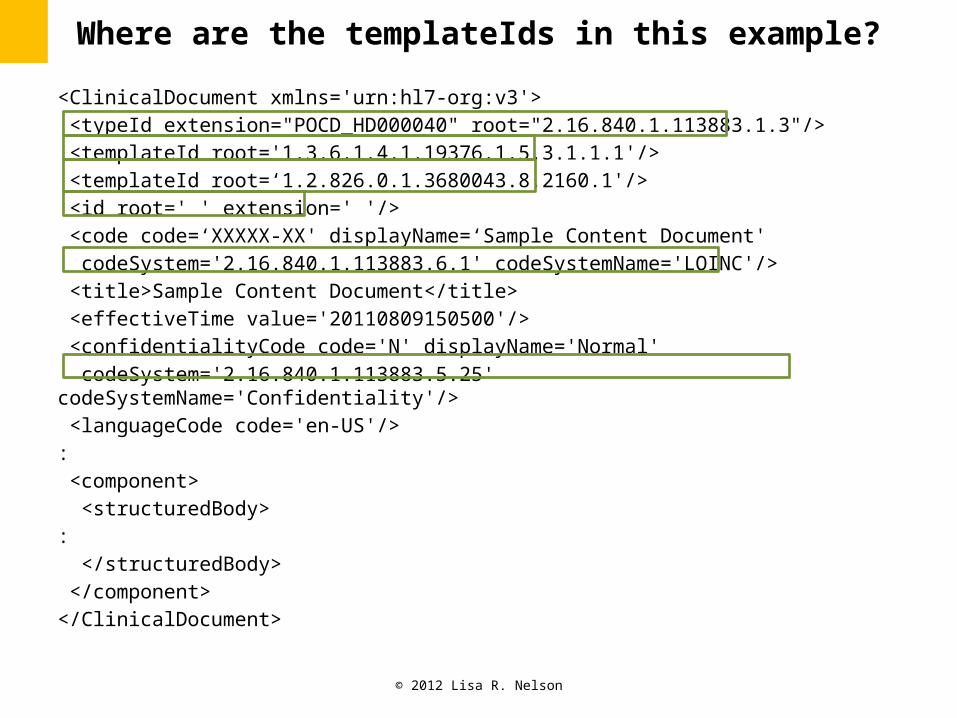
<ClinicalDocument xmlns='urn:hl7-org:v3'> <typeId extension="POCD_HD000040" root="2.16.840.1.113883.1.3"/> <templateId root='1.3.6.1.4.1.19376.1.5.3.1.1.1'/> <templateId root=‘1.2.826.0.1.3680043.8.2160.1'/> <id root=' ' extension=' '/> <code code=‘XXXXX-XX' displayName=‘Sample Content Document' codeSystem='2.16.840.1.113883.6.1' codeSystemName='LOINC'/> <title>Sample Content Document</title> <effectiveTime value='20110809150500'/> <confidentialityCode code='N' displayName='Normal' codeSystem='2.16.840.1.113883.5.25' codeSystemName='Confidentiality'/> <languageCode code='en-US'/> : <component> <structuredBody> : </structuredBody> </component> </ClinicalDocument>
Where are the template Ids in this example?
© 2012 Lisa R. Nelson
<ClinicalDocument xmlns='urn:hl7-org:v3'> <typeId extension="POCD_HD000040" root="2.16.840.1.113883.1.3"/> <templateId root='1.3.6.1.4.1.19376.1.5.3.1.1.1'/> <templateId root=‘1.2.826.0.1.3680043.8.2160.1'/> <id root=' ' extension=' '/> <code code=‘XXXXX-XX' displayName=‘Sample Content Document' codeSystem='2.16.840.1.113883.6.1' codeSystemName='LOINC'/> <title>Sample Content Document</title> <effectiveTime value='20110809150500'/> <confidentialityCode code='N' displayName='Normal' codeSystem='2.16.840.1.113883.5.25' codeSystemName='Confidentiality'/> <languageCode code='en-US'/> : <component> <structuredBody> : </structuredBody> </component> </ClinicalDocument>
Where are the templateIds in this example?

© 2012 Lisa R. Nelson
Learn how CDA Documents have been specified in the past and what new tools are being developed
to support their definition and maintenance in the future
9

© 2012 Lisa R. Nelson
How are classes of CDA R2 content documents defined?
IHE Content Profiles and HL7 Implementation Guides
establish the specification for a class of CDA documents
Or a family of CDA documents
The rules are recorded and identified using unique numbers
called template IDs
Example: Public Health Case Report
164 pages
Validation comes after the construction of the “pros” –
through human discernment of issues.
Document validation tools are manually built
as a secondary step
© 2012 Lisa R. Nelson
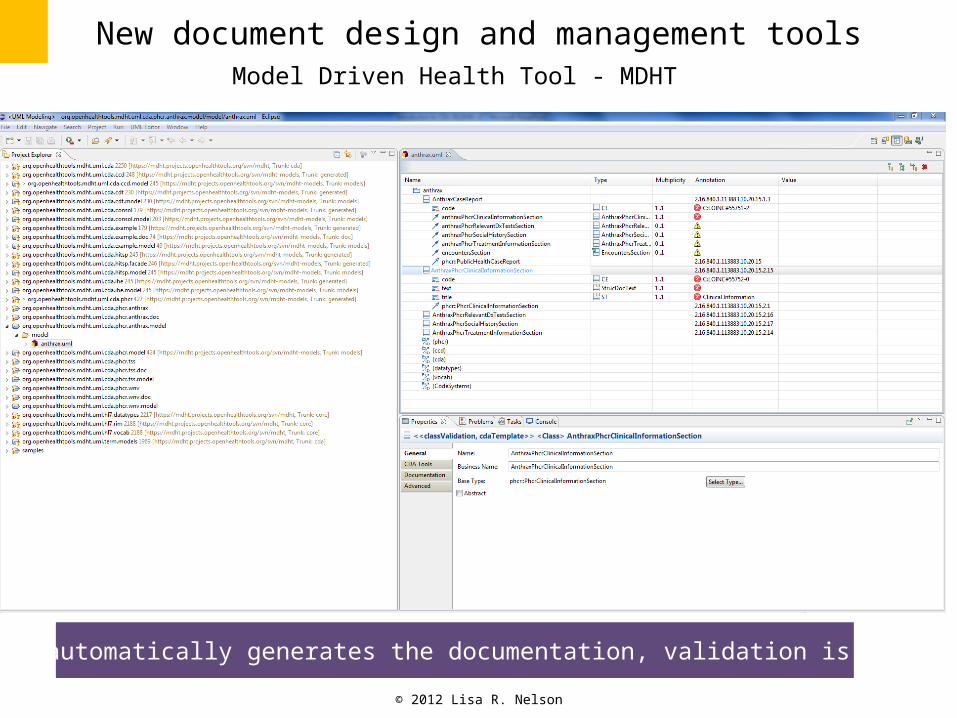
New document design and management toolsModel Driven Health Tool - MDHT
The model automatically generates the documentation, validation is built-in.

© 2012 Lisa R. Nelson
https://www.projects.openhealthtools.org/sf/projects/mdht/

© 2012 Lisa R. Nelson
Understand what code systems and value sets are and how they are used in content module design
Appreciate the different data structures that can combine to create an Entry and the complexity/richness of the
CDA standard
Gain awareness of how HL7 RIM and v3 data types create the foundation for CDA
10-12
© 2012 Lisa R. Nelson
• Demonstration:– Examine some of the content structure definitions– Use Oxygen to review the XML of a PHCR sample– Use Excel to look at a sample value set– Use MDHT to show the Anthrax PHCR definition
What do sections and entries look

© 2012 Lisa R. Nelson
Connect these concepts to the current Public Health Care Report design and the specific content modeling needs
for condition-specific case reports
13
© 2012 Lisa R. Nelson
* One of four specific public health case reports specified using current PHCR prototype design.
PHCR Relevant Diagnostic Tests and/or Laboratory Results
Anthrax PHCR Relevant Diagnostic Tests and/or Laboratory Results
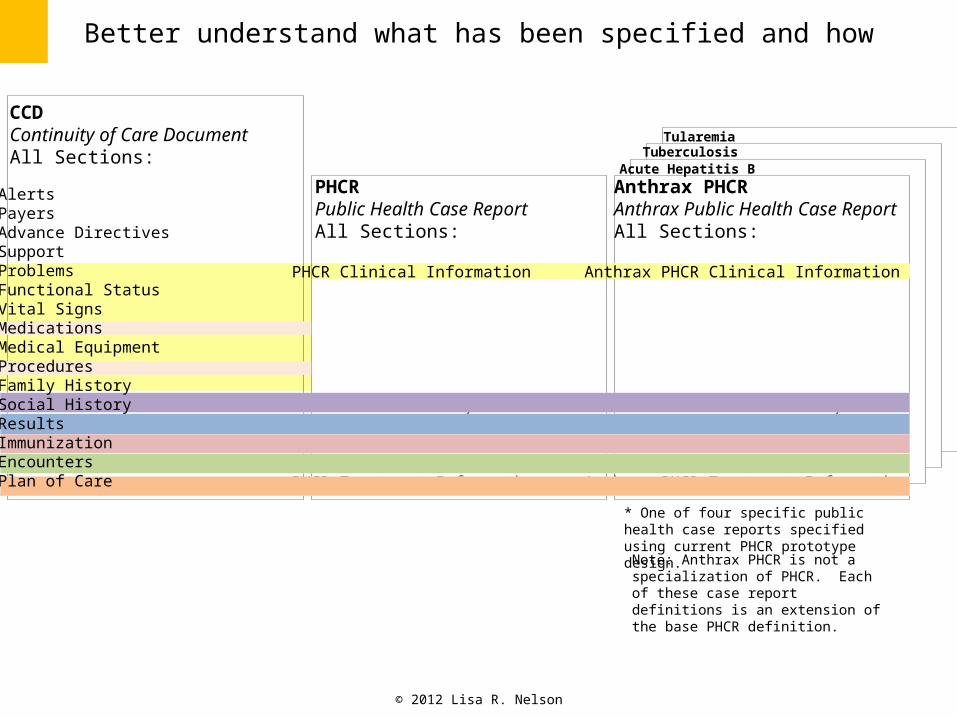
Better understand what has been specified and how
CCDContinuity of Care DocumentAll Sections:
PHCR Clinical Information
PHCR Social History
CCD ImmunizationPHCR EncountersPHCR Treatment Information
Anthrax PHCR Clinical Information
Anthrax PHCR Social History
Anthrax PHCR EncountersAnthrax PHCR Treatment Information
PHCRPublic Health Case ReportAll Sections:
Anthrax PHCRAnthrax Public Health Case ReportAll Sections:
Acute Hepatitis BTuberculosis
Tularemia
AlertsPayersAdvance DirectivesSupportProblemsFunctional StatusVital SignsMedicationsMedical EquipmentProceduresFamily HistorySocial HistoryResultsImmunizationEncountersPlan of Care
Note: Anthrax PHCR is not a specialization of PHCR. Each of these case report definitions is an extension of the base PHCR definition.
© 2012 Lisa R. Nelson
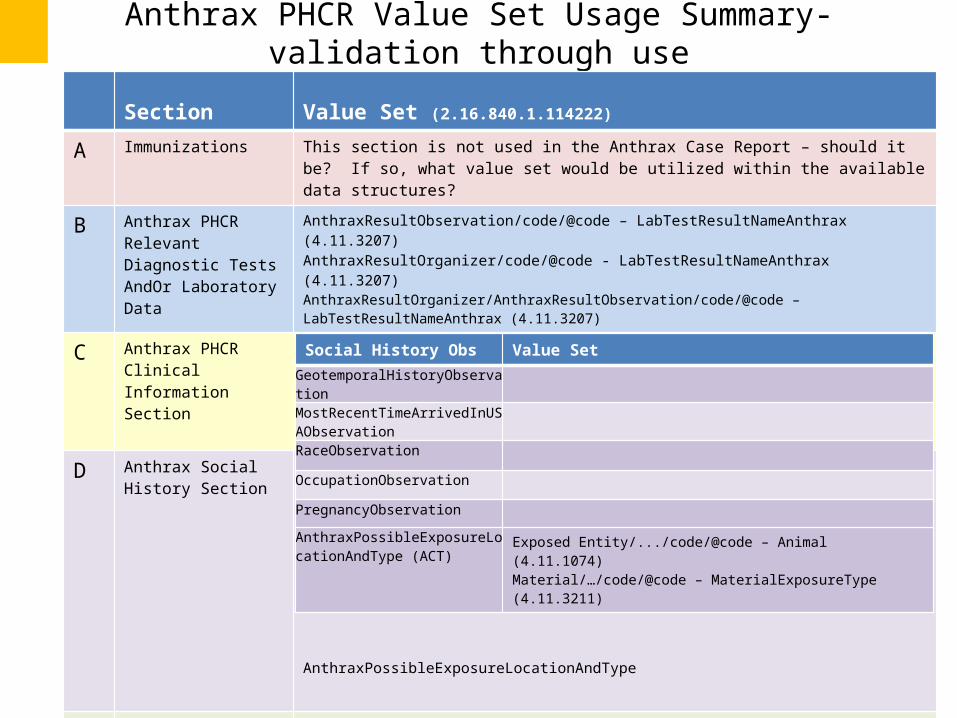
Anthrax PHCR Value Set Usage Summary- validation through use
Section Value Set (2.16.840.1.114222)
A Immunizations This section is not used in the Anthrax Case Report – should it be? If so, what value set would be utilized within the available data structures?
B Anthrax PHCR Relevant Diagnostic Tests AndOr Laboratory Data
AnthraxResultObservation/code/@code – LabTestResultNameAnthrax (4.11.3207)AnthraxResultOrganizer/code/@code - LabTestResultNameAnthrax (4.11.3207)AnthraxResultOrganizer/AnthraxResultObservation/code/@code – LabTestResultNameAnthrax (4.11.3207)
C Anthrax PHCR Clinical Information Section
AnthraxCaseObservation/value/@code – DiseaseTypeAnthrax (4.11.3220)AnthraxSignsAndSymptoms/value/@code – SignsAndSymptomsAnthrax (4.11.3212)
D Anthrax Social History Section
AnthraxPossibleExposureLocationAndType
E PHCR Encounter Section The entries in this section do not use value sets.
F Anthrax PHCR Treatment Information Section
AnthraxTherapeuticRegimen/value/@code – DiseaseTypeAnthrax (4.11.3220)AnthraxTreatmentGiven/…/material/code@code - MedicationTreatmentAnthrax (4.11.3216) AnthraxTreatmentNotGiven/…/material/code@code - MedicationTreatmentAnthrax (4.11.3216)
Social History Obs Value SetGeotemporalHistoryObservation
MostRecentTimeArrivedInUSAObservationRaceObservation
OccupationObservation
PregnancyObservation
AnthraxPossibleExposureLocationAndType (ACT)
Exposed Entity/.../code/@code – Animal (4.11.1074)Material/…/code/@code – MaterialExposureType (4.11.3211)

© 2012 Lisa R. Nelson
• Attempt to fit the information into the provided form (5-6 sections)– What are the specific Social History Observations needed to identify a
suspected, or confirmed case?– What Value set would apply here to articulate the possibilities?– Where do we see gaps for Anthrax?– What happens when we try to model TSS (w/ no prior IG)?– What are the strengths and weaknesses of the approach?– What can we learn from this?
• (request) Present the Case Definition, Position Statement and other material back to me– Add other materials/perspectives as needed– Show me the view of this from the Epidemiologist’s point of view
Next Steps

© 2012 Lisa R. Nelson
END OF DECK