Embed Size (px)
Citation preview

+ MODEL
Journal of Plastic, Reconstructive & Aesthetic Surgery (2014) xx, 1e2
CORRESPONDENCE AND COMMUNICATION
An important diagnosis for thehand surgeon: “The clenched fistsyndrome”
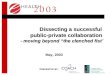
Figure 1 The patient with the clenched fist, all digits wereheld in a tight flexion at the metacarpal and interphalangeal
Dear Sir,
Clenched fist syndrome is a type of a psychiatric disorder inwhich the patients present with flexion contractures of thefingers without an organic etiology. An early recognitionand treatment is important in these patients, particularlyfor prevention of unnecessary diagnostic studies and ther-apies. To emphasize this, we present a 43-year old retiredsoldier with typical findings of this disorder.
The clenched fist syndrome (CFS) is a rare disorder ofthe hand associated with a tightly clenched fist after aminor trauma or surgery. It’s typically associated withpain, swelling and paradoxical stiffness.1e5 It may beencountered in all age groups and hand dominance is not afactor, at all.1 Awareness of these factitious disorders isimportant, not only for accurate diagnosis but also forchoosing the appropriate and supportive treatment op-tions. To emphasize the significance of this entity, here wepresent a case of a CFS in a patient with a pre-existingpsychiatric illness.
A 43-year-old, right hand-dominant man, presented witha 3-year history of progressive hand flexion contracture(Figure 1). On examination, all digits were held in a tightflexion at the metacarpal and interphalangeal joints,including the thumb. There were no tenderness on anyjoints, or any other lesions. However, the attempts topassively straighten the finger caused severe pain and thepatient stopped any degree of passive digital extension.Radiography of the hand revealed no abnormality. Elec-tromyography (EMG) and nerve conduction studies of theupper limp were unremarkable.
The patient was a retired soldier and the symptomswere found to start spontaneously after retirement. Thepatient had been consulted by several psychiatrists anddiagnosed with various illnesses including bipolar disorder,social phobia, and post-traumatic stress disorder.Following exclusion of an organic cause, psychiatricreevaluation and aggressive hand therapy were recomm-ended.
Please cite this article in press as: Basaran K, et al., An important diagof Plastic, Reconstructive & Aesthetic Surgery (2014), http://dx.doi.o
http://dx.doi.org/10.1016/j.bjps.2014.04.0271748-6815/ª 2014 British Association of Plastic, Reconstructive and Aesthetic
CFS is classified as a type of SHAFT syndrome which isdefined by Wallace and Fitzmore in 1978.1 The SHAFT syn-drome describes a ‘sad’, ‘hostile’, ‘angry’, ‘frustrated’,and ‘tenacious’ individual who may present with varyingdegrees of self inflicted trauma.1,2
SHAFT patients are categorized into two groups. Thefirst group inflicts physical harm on themselves, creatingfactitious injuries. The second group postures their limbs inattitudes that are not explainable anatomically.3 This lattergroup first named by Simmons and Vasile in 1980 as the“clenched fist syndrome”.2e4 CFS is usually intermingledand has been used synonymously with complex regionalpain syndrome (CRPS), but there are specific differences asdescribed by Simmons and Vasile.1,2,4 Characteristics thatare usually absent in CRPS, including a clenched fist withmacerated palm and paradoxical stiffness, are usuallypresent in clenched fist syndrome. Likewise pain with pas-sive flexion is usually absent in clenched fist syndromewhile it is usually present in CRPS.1
CFS is believed by many authors to be a conversionsyndrome.2 However, conversion disorder; a type of soma-toform disorder is unconsciously motivated and produced.In contrast, a factitious disorder is unconsciously motivatedand consciously produced.1,2
Factitious hand disorders can only be positively diag-nosed when the patient confesses, but still, diagnoses of
joints, including the thumb.
nosis for the hand surgeon: “The clenched fist syndrome”, Journalrg/10.1016/j.bjps.2014.04.027
Surgeons. Published by Elsevier Ltd. All rights reserved.

2 Correspondence and communication
+ MODEL
exclusion should be made.1 Identifying them requireslistening carefully to their history and complications. Theseconditions should particularly be considered in patientswith a dissociated history and a physical examination.2e4
Lack of positive findings in radiography, electromyographyand nerve conduction studies are useful for the diagnosis.
Differential diagnosis includes contractures seen inneurological diseases such as stroke and Parkinson’s dis-ease, complex regional pain syndrome (CRPS), Dupuytrendisease, multiple triggering, tendonitis, arthritis, ulnarneuroritis, median nerve compression, andcamptodactyly.1,2
In the case presented, the patient demonstratedtypical symptoms of a CFS such as paradoxical stiffnessand pain during passive extension. In addition, the patientalso described intermittent swelling periods prior toadmission, although it was not noted during physical ex-amination. Therefore, the diagnosis of CFS could be madeeasily.
Treatment of CF patients involve unclenching of thehand under general anesthesia if necessary and handtherapy which involves dynamic and static splinting,stretching, physiotherapy, and psychological support.Hypnosis has been suggested by Spiegel, Chase and Hoog-dium et al. previously.2 Surgical treatment is not indicated.Attempts to release contractures can even make a psychi-atric condition worse and amputation should be avoided.2,4
Prognosis varies with the psychiatric profile. In this case,the patient was reevaluated by a psychiatrist where he wasdiagnosed with an untreated post-traumatic stess disorderand depression. A supported psychotherapy and pharma-cotherapy were initiated. During follow-up, the patientimproved with aggressive hand physiotherapy includingstretching exercises and casting. Therefore, as demon-strated in our case, associated psychiatric conditions shouldbe handled by mental health professionals.1
Please cite this article in press as: Basaran K, et al., An important diagof Plastic, Reconstructive & Aesthetic Surgery (2014), http://dx.doi.o
In conclusion, awareness of these factitious disorderslike the “CFS” is important, not only for accurate diagnosisbut also for choosing appropriate and supportive treatmentoptions. Early recognition is also crucial to avoid progres-sively mutilating operations.
Conflict of interest/funding
None.
References
1. Eldridge MP, Grunert BK, Matloub HS. Streamlined classificationof psychopathological hand disorders: a literature review.Hand (N Y) 2008 Jun;3(2):118e28.
2. Weis T, Boeckstyns ME. The clenched fist syndrome: a pre-sentation of eight cases and an analysis of the medicolegalaspects in Denmark. J Hand Surg Eur Vol 2009 Jun;34(3):374e8.
3. Graham 3rd WP, Shearer AW, Mackay DR, Santo J, Stratis JP.SHAFT syndrome revisited. Ann Plast Surg 1999 Apr;42(4):411e6.
4. Simmons BP, Vasile RG. The clenched fist syndrome. J HandSurg Am 1980 Sep;5(5):420e7.
5. Wallace PF, Fitzmorris CS. The S-H-A-F-T syndrome in the upperextremity. J Hand Surg Am 1978 Sep;3(5):492e4.
Karaca BasaranAsli Datli
Muzaffer KurtBagcilar Research and Training Hospital, Merkez Mah.Mimar Sinan Cad, 6. Sokak, Bagcilar, Istanbul, Turkey
E-mail address: [email protected]
20 October 2013
nosis for the hand surgeon: “The clenched fist syndrome”, Journalrg/10.1016/j.bjps.2014.04.027