Embed Size (px)
Citation preview

PAIN IN LONG-TERM SURVIVORS OF BRAIN TUMOURS IN CHILDHOOD

AN EXPLORATION OF THE BURDEN OF PAIN AND HEALTH-
RELATED QUALITY OF LIFE OF LONG-TERM SURVIVORS OF BRAIN
TUMOURS IN CHILDHOOD
By TRISHANA NAYIAGER, B.Sc.H
A Thesis Submitted to the School of Graduate Studies in Partial Fulfilment of
the Requirements for the Degree Master of Science
McMaster University © Copyright by Trishana Nayiager, August 2013

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
ii
McMaster University MASTER OF SCIENCE (2013) Hamilton, Ontario
(Health Research Methodologies)
TITLE: An Exploration of the Burden of Pain and Health-Related Quality of Life
of Long-Term Survivors of Brain Tumours in Childhood
AUTHOR: Trishana Nayiager, B.Sc.H
SUPERVISOR: Dr Ronald D. Barr
Number of Pages: xii, 119

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
iii
ABSTRACT
Background: Health-related quality of life (HRQL) studies of survivors of brain
tumours in childhood have reported numerous areas of morbidity. The burden of pain is
identified inconsistently in this cohort, with limited exploration of this morbidity.
Objective: To explore the HRQL, with a focus on pain, in survivors greater than
10 years from diagnosis of a primary brain tumour in childhood or adolescence.
Methods: An exploratory cross-sectional study was undertaken using Health
Utilities Index (HUI) questionnaires. Pain was characterized using a coloured analogue
scale for self-perceived severity and a homunculus to identify the location of pain.
Comparison of the single-attribute HRQL scores for participants with and without pain
was undertaken. The stability of pain over a decade was established using available
HUI2/3 survey data of the same cohort with imputation for missing variables.
Results: Twelve males and 13 females out of 37 eligible subjects participated in
this study. Participants (mean time from diagnosis of 19.7 years) had mean multi-attribute
HRQL scores of 0.79 (SD of 0.23) for HUI2 and 0.69 (SD of 0.29) for HUI3. Thirteen
(52%) participants reported pain, with inter- and intra- individual differences in severity
and location of discomfort. Comparison of single-attribute HRQL scores for participants
with and without pain revealed considerably greater burdens of morbidity in sensation
and emotion in the former group. Pain also increased from the initial interview (10 years
prior) to the final interview.
Conclusion: As a group, long-term survivors of brain tumours in childhood have
diminished overall HRQL. However there is variability between subjects. Pain appeared
to be a persistent and significant burden in a subset of individuals, with those
experiencing pain reporting greater severity of morbidities in other attributes. The
findings of this study provide further insight into a poorly characterized phenomenon in
this survivor cohort and warrant further study.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
iv
ACKNOWLEDGEMENTS
I would like to recognize my mentor and supervisor, Dr Ronald Barr, for all of the
opportunities, guidance, constructive feedback and motivation that he has provided
throughout my Master’s program and on my thesis. These valuable learning experiences
have expanded my knowledge and have provided me with the confidence to be an active
researcher and to share my skills and enthusiasm for research with others. My committee
members have also been an integral part of this thesis. I sincerely appreciate having the
opportunity to work with Drs Anne Klassen, Eleanor Pullenayegum and Peter
Rosenbaum, who have shown me the importance of an inquisitive mind and I have grown
under their tutelage. I also thank Dr. David Feeny for his valuable and positive feedback
on my thesis and ideas for publications. Dr Uma Athale was also an important part of my
Master’s journey, with first encouraging me to apply to the HRM program and then
always having an open door to discuss course project ideas and encouragement to
continue to grow as a researcher.
In addition, I would like to acknowledge Joann Duckworth from the 3F clinic at
McMaster Children’s Hospital for her efforts to make this study a success, as well as
Dr Ziad Solh for assisting with patient-interviews and Charlene Rae for support with the
HUI questionnaires and databases. I would also like to thank the survivors who agreed to
participate on this study and for sharing their experiences with me.
These past 4 years would not have been as enjoyable without the (welcomed)
diversions and happy times provided by my friends, and the support from my colleagues
at work. The encouragement from my family kept me motivated to complete this thesis. I
am particularly grateful to my parents and sister for their continuous support,
understanding and helping make my life a little easier any time I asked, and for my
husband, Vik Venkatesh, for always believing in me, keeping a sense of humour and
never tiring from listening to me talk about health-related quality of life.
Finally, I would like to acknowledge H.U.Inc. for providing me with a student
grant to use the HUI2/3 questionnaires and for providing the programming to analyse the
responses, as well as to the b.r.a.i.n.child foundation who supported this study.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
v
TABLE OF CONTENTS LIST OF TABLES ........................................................................................ vii
LIST OF FIGURES ....................................................................................... ix
DECLARATION OF ACADEMIC ACHIEVEMENT ..................................... xii
INTRODUCTION ..................................................................................................... 1 Brain Tumours in Childhood ........................................................................................ 1
Survivorship and Outcomes of Patients with Brain Tumours in Childhood ......... 2
Quality of Life .............................................................................................................. 5
Health-Related Quality of Life ..................................................................................... 5
Measures of HRQL in Survivors of Brain Tumours in Childhood ..................... 11
Previous Assessments of HRQL of Survivors of Brain Tumours in Childhood . 17
Summary of the Studies Reviewed ................................................................ 26
METHODS .............................................................................................................. 31 Objective ..................................................................................................................... 31
Study Design ............................................................................................................... 31
Rationale ..................................................................................................................... 34
Cross Sectional Study Design .............................................................................. 34
Sample Selection ........................................................................................... 34
Measurement Instruments ............................................................................. 35
Proxy Reporting ............................................................................................ 41
Longitudinal Study Design .................................................................................. 41
Protocol ....................................................................................................................... 42
Procedures ............................................................................................................ 42
Subject Screening ................................................................................................ 43
Subject and Proxy Recruitment ........................................................................... 44
Consent Process ................................................................................................... 44
Administration of Questionnaires ........................................................................ 44
Non-Participants .................................................................................................. 46
Data Linkage ........................................................................................................ 46
Demographic and Clinical Information ............................................................... 46
Data Management ................................................................................................ 47
Scoring of HUI Questionnaire. ............................................................................ 47

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
vi
Analysis ...................................................................................................................... 47
Cross-Sectional Analysis ..................................................................................... 47
Description of Overall Cohort ...................................................................... 48
General Quality of Life Rating ..................................................................... 48
Health-Related Quality of Life...................................................................... 49
Proxy Reporting ............................................................................................ 49
Description of Participants Reporting Pain ................................................. 50
Burden of Pain by HRQL .............................................................................. 50
Longitudinal Analysis .......................................................................................... 51
Ethical Considerations ................................................................................................ 54
Research Ethics Board Approval ......................................................................... 54
Study Risks, Identification and Management ...................................................... 54
Study Benefits ...................................................................................................... 55
Confidentiality ..................................................................................................... 56
Consent ................................................................................................................ 57
RESULTS .................................................................................................... 58 Cross-Sectional Study- Time Point 3 (2011 and 2012) .............................................. 58
Overall Cohort ..................................................................................................... 58
Description of Participants........................................................................... 58
Sociodemographic Factors and General Quality of Life ............................. 60
Health-Related Quality of Life...................................................................... 63
Participants Reporting Pain ................................................................................. 68
Description of Participants with Pain .......................................................... 68
Proxy-Reporting for Participants with Pain................................................. 71
Health-Related Quality of Life of Participants with Pain ............................ 72
Longitudinal Analysis-Time points 2000/2001, 2005/2006 and 2011/2012 .............. 75
DISCUSSION .............................................................................................. 84 Cross-Sectional Results .............................................................................................. 85
Overall HRQL...................................................................................................... 85
Single Attribute Analysis ..................................................................................... 86
Pain in Survivors of Brain Tumours in Childhood and Adolescence ......................... 89
Limitations .................................................................................................................. 98
Implications of Findings ........................................................................................... 102
CONCLUSION .......................................................................................... 105
REFERENCES ........................................................................................... 106

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
vii
LIST OF TABLES
Table 1. Summary of study design and patient characteristics in studies reviewed .......... 79
Table 2. Summary of study methods and outcome. ........................................................... 29
Table 3. Summary of constructs used in the HUI2 Multi-Attribute System (aside from
fertility) (Torrance, 1996) .................................................................................. 38
Table 4. Summary of constructs used in the HUI3 Multi-Attribute System (Feeny, 1995)
........................................................................................................................... 38
Table 5. Clinical features of subjects eligible to participate in study at time point 3 (n=37)
........................................................................................................................... 59
Table 6 Self- and proxy- responses to direct questioning of overall health- related quality
of life ................................................................................................................. 63
Table 7. Measurement of concordance between self- and proxy- ratings for HUI2
attributes ............................................................................................................ 67
Table 8. Measurement of concordance between self- and proxy- ratings for HUI3
attributes ............................................................................................................ 67
Table 9. Number of days participants reported experiencing pain within a one-week
period ................................................................................................................. 68
Table 10. Clinical characteristics of participants with and without pain ........................... 69
Table 11. Reported location of pain as noted using homunculus and corresponding
intensity based on coloured analogue scale rating ............................................ 71
Table 12. Concordance between self- and proxy- reporting for pain as measured by
interventions to alleviate symptoms (HUI2). .................................................... 72
Table 13. Concordance between self- and proxy- reporting for pain as measured by
number of activities limited by pain (HUI3) ..................................................... 72
Table 14. Single-attribute utility scores for participants with (n=13) and without (n=12)
pain .................................................................................................................... 73
Table 15. Frequency of severity of morbidity by attribute, stratified by participants with
(n=13) and without (n=12) pain ........................................................................ 74

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
viii
Table 16. Minimum, maximum and mean pain utility scores reported at each time point
for HUI2 and HUI3. The prevalence of utility scores of equal to or greater than
0.80 are also presented ...................................................................................... 79
Table 17. Summary of the number of variables imputed for longitudinal analysis ........... 80
Table 18. Results of longitudinal analysis of the pain utility scores by linear mixed effects
model; fixed factor is time. Results presented are of pooled data (initial dataset
along with datasets with imputed missing values). T1= 2000/2001,
T2= 2005/2006, and T3= 2011/2012 survey time points. = increase in utility
score, = decrease in utility score ..................................................................... 81
Table 19. Results of longitudinal analysis of the multi-attribute utility scores by linear
mixed effects model; fixed factor is time. Results presented are of pooled data
(initial dataset along with datasets with imputed missing values).
T1= 2000/2001, T2= 2005/2006, and T3= 2011/2012 survey time points.
= increase in utility score, = decrease in utility score ................................... 82

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
ix
LIST OF FIGURES
Figure 1. Schematic diagram of study methods used to explore the health-related quality
of life in survivors of brain tumours in childhood over a ten-year period.
Measures include the HUI2/3 questionnaire, as well as additional investigations
to characterize the burden of pain experienced by the patient cohort.
Sociodemographic and quality of life information was also captured at time
point 3. ............................................................................................................... 33
Figure 2. A simplified human figure used to elucidate location of pain experienced by
participant. ......................................................................................................... 40
Figure 3. Summary of cross-sectional study procedures. .................................................. 43
Figure 4. Highest education level achieved as reported by participants (n=25). ............... 61
Figure 5. Mean overall quality of life as reported subjectively by participants as
remembered at times 5 years in the past, the present and predicted 5 years in
the future. ........................................................................................................... 62
Figure 6. Boxplot of median utility scores for cohort (n=24). ........................................... 63
Figure 7. Single attribute level data for HUI2 (2a) and HUI3 (2b) for overall cohort
(n=25). ............................................................................................................... 65
Figure 8. Impact of pain (n=13) as measured by a) Number of activities limited by pain,
and b) Interventions for relief of most severe pain in a 1 week period, for
participants reporting pain within the week prior to the interview. .................. 70
Figure 9. Overview of number of participants at each study time point\ as well as the
prevalence of pain (self-reported). .................................................................... 76
Figure 10. Median overall HRQL and pain utility scores over a 10 year period, measured
at five-year intervals. ......................................................................................... 78

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
x
LIST OF ABBREVIATIONS
ANOVA……………………………….…………….………………..Analysis of Variance
CAS…………………………………………………………..….Coloured Analogue Scale
CCSS………………………………………………..…..Childhood Cancer Survivor Study
CGSS………………………………………………..…..Canadian General Society Survey
CHQ………………………………………………...………….Child Health Questionnaire
CNS……………………………………………………………….Central Nervous System
HRQL………………………………………………………Health-Related Quality of Life
HUI……………………………………………………….……… Health Utilities Index ®
ICC……………………………………………………..Intra-Class Correlation Coefficient
JD……………………………………….……Neuro-Oncology Nurse (JoAnn Duckworth)
MCH……………………………………………………….McMaster Children’s Hospital
MMQL……………………………...……………Minneapolis Manchester Quality of Life
PedsQL………………………………………………...Pediatric Quality of Life Inventory
POGO……………………………………………….Pediatric Oncology Group of Ontario
QALY……………………………………………….…………Quality Adjusted Life Year
QOL………………………………………..………………………….…….Quality of Life
REB……………………………….…………………………….…..Research Ethics Board
SD…………..…………………………….…………………………….Standard Deviation
SF-36………………………………………,,………….Medical Outcomes Short Form-36

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
xi
TACQOL…… TNO-AZL Questionnaires for Children's Health-Related Quality of Life
T1…………………………………………………………...……Time point I (2000/2001)
T2………………………………………………………….…….Time point 2 (2005/2006)
T3……………………………………………………………..…Time point 3 (2011/2012)

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
xii
DECLARATION OF ACADEMIC ACHIEVEMENT
The following is a declaration that the content of this thesis has been completed by
Trishana Nayiager. The contributions of Drs R. Barr, A. Klassen, E. Pullenayegum and
P. Rosenbaum in the research processs, and Dr Solh and Ms. J. Duckworth in data
collection are acknowledged.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
1
INTRODUCTION
Brain Tumours in Childhood
Brain tumours, or neoplasms of the central nervous system (CNS), are among the
most commonly diagnosed solid tumours in children and adolescents. According to the
Canadian Cancer Statistics published in 2011, primary CNS tumours accounted for 16%
(n=1, 039) of all newly diagnosed cancers in patients under 19 years of age between 2003
and 2007 in Canada (excluding Quebec) (Canadian Cancer Society, 2011). These
proportions are similar to those observed in the US (Gurney et al., 2009).
Brain tumours are sub-categorized based on histology using the World Health
Organization or the International Classification of Childhood Cancer definitions
(Steliarova-Foucher, Stiller, Lacour & Kaatsch 2005; World Health Organization, 2000).
In order of decreasing incidence, the classifications are gliomas/astrocytomas,
medulloblastomas, ependymomas, and germ cell tumours. Most are diagnosed prior to the
seventh year of life; the incidence of astrocytoma also peaks around the early teen years
in addition to early childhood (Gurney, Smith & Bunin, 1999).
Histology, location of the primary tumour, age at diagnosis and extent of disease
are used to determine what therapeutic intervention should be used as well as the specific
treatment protocol to be employed (Pollack, 2008). An estimated 70% of pediatric CNS
tumours are malignant and require aggressive therapy, which may include surgery,
radiation and chemotherapy (Imbach, 2006). While treatment is required for survival, the

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
2
numerous assaults to the brain, including from the malignancy itself, as well as surgery,
chemotherapy and radiation, often result in unintended adverse effects on the patient
(Baron, Compton, Patel, Jacob & Harper, 2013). These complications are particularly
deleterious given the young age and consequently developing nature of the brain of these
patients. As such, it is not uncommon to observe immediate, long-term and chronic
morbidities relating to the primary diagnosis of a CNS tumour (Baron et al., 2013;
Pollack, 2008). Although there is no specified time for ‘late effects’, most investigators
include as late effects any deleterious outcomes that are chronic or develop at least five
years from diagnosis (Anderson et al., 2001A; Oeffinger , Eshelman, Tomlinson, Tolle &
Schneider, 2000).
Survivorship and Outcomes of Patients with Brain Tumours in Childhood
By definition, an individual is considered a cancer survivor from the time of
diagnosis through the remainder of his or her life (National Cancer Institute (NCI), 2012).
Prior to the 1980s, children and adolescents diagnosed with a brain tumour had a poor
prognosis. Technological advances leading to earlier diagnosis as well as improvement of
treatment have increased survival. The five-year relative survival estimate for patients
diagnosed with a CNS tumour (intracranial or intraspinal neoplasm) in childhood between
2002 and 2008 was 72.1% as noted by the National Cancer Institute in the USA (NCI,
2009).
However, survivors of CNS tumours in childhood are known to have significant
long-term morbidities (late effects). The medical sequelae of the disease and treatment
have been well-documented in the literature, with the most commonly cited issues being

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
3
cognitive deficits, short stature, osteopenia, endocrine deficiencies and second
malignancy. Several large multi-centre studies have reported a high prevalence as well as
severity of morbidity in this patient population. These late effects are noted to be greater
in survivors of CNS tumours compared to survivors of other childhood cancers. In many
cases, the survivor will develop combinations of these medical conditions (Oeffinger et
al., 2006). In addition, these patients are noted to have visual and auditory limitations,
and are often considered to be the group at highest risk for functional impairment
(Hudson et al., 2003; Mulhern, Hancock, Fairclough & Kun, 1992; Mulhern et al., 1999).
Location of the tumour and modalities of treatment have both been identified as
contributory to these late effects (Anderson, 2003).
The complications of treatment have implications for integration into society and
psychosocial development, with many survivors noted to have greater needs for
educational support, lower rates of graduation from high school and college, higher
likelihood of unemployment, less social supports, lower likelihood of getting married, and
psychological distress in comparison to their siblings as well as to other childhood cancer
survivors (Gurney et al., 2009). Numerous population-based studies undertaken in
Canada and the USA, as well as in European countries, have reported similar
sociodemographic outcomes (Armstrong et al., 2009; Barrera, Shaw, Speechley,
Maunsell & Pogany, 2005; Hays et al., 1992; Koch et al., 2004; Langeveld et al., 2003;
Lancashire et al., 2010; Mostow, Byrne, Connelly & Mulvihill, 1991).
It is apparent that survivors of brain tumours in childhood have numerous medical
complications as well as difficulties with education, employment and social adaptation.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
4
Specialized “survivorship clinics” are available to survivors of cancer in childhood. These
clinics consist of a multidisciplinary team of healthcare professionals who provide
systematic follow-up of survivors with the primary objective of health promotion,
education and monitoring of long-term consequences of therapy (Aziz, Oeffinger, Brooks
& Turoff, 2006; Pediatric Oncology Group of Ontario (POGO), 2006).
The Pediatric Oncology Group of Ontario (POGO) estimates that of the 80% of
children and adolescents who will survive their cancer approximately 60% will
experience a significant late effect of their disease or therapy (POGO, 2006). In addition
to providing a clinical service to survivors, these clinics facilitate research into cancer
survivorship. The Office of Cancer Survivorship at the National Cancer Institute defines
cancer survivorship research as encompassing “the physical, psychosocial, and economic
sequelae of cancer diagnosis and its treatment among both pediatric and adult survivors of
cancer”. The emphasis of the research is to increase understanding with the objective of
preventing and controlling adverse outcomes from the disease and treatment, as well as to
provide guidelines for optimal follow-up and care (NCI, 2012).
While concerted efforts have been made to appreciate the medical complications
and to characterize the sociodemographics of survivors of brain tumours in childhood and
adolescence, patient reported outcomes, such as measures of health-related quality of life
(HRQL), are gaining interest rapidly as an important outcome measure to appreciate the
capabilities as well as burden of morbidity experienced by survivors and to gain insight
into the lives of this patient population.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
5
Quality of Life
The concept of “quality of life” (QOL) encompasses an individual’s overall
perception of their well-being and incorporates multiple aspects of the person’s life,
including physical and psychological health, as well as independence, social
relationships, environment and beliefs including happiness and satisfaction (Center for
Disease Control, 2011). The World Health Organization (WHO) summarized QOL as an
“individual’s perception of their position in life in the context of the culture and value
systems in which they live and in relation to their goals, expectations, standards and
concerns” (WHOQOL Group, 1995).
Health-Related Quality of Life
Health related quality of life (HRQL) is a component of QOL that relates
specifically to the physical, social and mental health of an individual (Cella & Bonomi,
1995). Unlike the term “health”, which is often measured using objective or observable
measures such as blood pressure or ability to walk, HRQL refers to the perceived
physical, social and mental health of an individual within the context of a functional state
and, according to one particular approach, the value of that health state (Center for
Disease Control, 2011; Feeny, Furlong, Mulhern, Barr & Hudson, 1999). The focus on
the perceived health state of the individual based on their reported functional capabilities
is often described as a “narrow within the skin” approach to measuring HRQL (Ware,
Brook, Davies & Lohr, 1981).

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
6
Traditional outcomes of cancer therapy focus on mortality and morbidity
measures, such as event free survival, and overall survival (Heimans & Taphoorn, 2002).
In the past few decades, patient-reported outcomes, particularly HRQL, has been
embraced increasingly as an important measure of morbidity in clinical trials as well as in
population health studies (McHorney, 1999; Osoba, 2011).
The inclusion of HRQL measures in clinical trials allows researchers to
understand the burden of morbidity from disease and treatment within the context of an
individual’s life. When measured using reliable instruments validated to the patient
population, HRQL can provide valuable information on the design of new therapies by
providing an alternate outcome measure, such as whether patients felt better, or it can be
used to explore consequences of treatment that may not be otherwise measureable, and
should be considered when testing novel or comparing medical interventions (Feeny et
al., 1999). Clinicians can also use HRQL information to assist with treatment decisions
and treatment alternatives for patients (Feeny et al., 1999). The degree to which a
diagnosis or treatment will impact the daily functioning and overall well-being of an
individual is of particular importance in populations of people with chronic diseases,
which, by extension, can also include populations with long-term morbidities as a result
of disease or treatment (Patrick & Erickson, 1993).
HRQL is also an important outcome for understanding the perceived well-being of
a group of individuals, from specific disease groups to entire nations. The ability to
quantify the overall health status of a population provides valuable information to policy
makers and health administrators (Wennberg, 1990).

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
7
Measurement of HRQL is accomplished using self- or proxy- responses to capture
the perceived health of an individual and uses these responses to generate a meaningful
score that estimates the impact on overall QOL (Center for Disease Control, 2011). The
questionnaires, often structured as multiple items or questions with specific multiple-
choice responses, are designed to generate scores for key domains of health status. Feeny
et al. (1999) proposed that one way to conceptualize health is to summarize key attributes
(dimensions/domains) of health status including physical function, sensation, self-care
and dexterity, cognition, pain and discomfort, and emotional and psychological well-
being. These dimensions contribute collectively to the overall HRQL of the individual.
Based on the design of the questionnaire, it is possible to generate scores for each of the
individual domains as well as an overall HRQL score.
The resultant scores may be qualitative and describe the burden of morbidity using
adjectives, or be quantifiable, with the burden of morbidity falling within a structured
numerical scale allowing for analytical study. Scores from a reliable instrument that has
been validated in the patient population can be interpreted directly to identify areas of
particular morbidity, or can be referenced to another population, including those with
other diagnoses, healthy controls or even the same cohort at another point in time. This
indirect measurement of morbidity allows for comparison using statistical analyses or
absolute differences. Some instruments have previously established levels of meaningful
minimal clinically important differences.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
8
Given the varying definitions of HRQL and the complexity of measuring
perceived health in the context of daily living, multiple instruments have been created.
Although these instruments often incorporate similar principles of measuring physical,
psychological and social components to generate a measure of HRQL, the constructs used
to define HRQL are variable and scale dependent (Fayed, Schiariti, Bostan, Cieza &
Klassen, 2011). Most often HRQL measurement scales are divided into disease-specific
health outcomes or generic functioning measures (Feeny et al., 1999).
Disease-specific questionnaires are designed to focus on areas established or
hypothesized previously to be of relevance to the patient population under exploration.
This type of questionnaire is often sensitive to small changes in HRQL over time and has
considerable face validity. However, this type of instrument is limited in applicability as
scores cannot be compared to other disease populations (Khanna, 2006; King, Tsevat,
Moossy & Roberts, 2004; Tsevat et al., 1994).
Generic instruments, conversely, attempt to capture multiple areas of HRQL and
can be used across populations, including healthy and diseased groups, thus facilitating
comparisons between disease populations. In addition, this type of instrument does not
pre-suppose areas of morbidity and consequently provides a more global representation of
the capabilities of the population, which may be overlooked in disease-specific scales
(Dowie, 2002).

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
9
Generic instruments can be classified as either health profiles or preference-based
measures. Health profiles, which can be HRQL measures or measures of health status,
describe an individual’s function based on one or more domains. These domains may be
presented individually or consolidated as an overall summary score. Outcomes from
health status instruments are beneficial for describing the functioning capabilities of a
group.
Preference-based measures are also generic instruments. However, this type of
instrument provides a single utility score for a specific state of health, on an established
scale of 1 (perfect health) to 0 (equivalent to being dead). Similar to health profiles,
scores may be generated for individual domains, such as physical functioning, or
summarized as a single overall HRQL score. As these scores are referenced to a pre-
defined scale, the results obtained can be used to describe the functional capabilities of a
given population as well as allowing for direct comparison of HRQL scores to normal
(healthy) or even other non-related diseased populations.
Preference-based measures may use direct estimation methods, such as
willingness to pay, standard gamble or time trade-off, to generate a single score
corresponding to a health state of the domain under study (Feeny et al., 1999; Streiner &
Norman, 2008). This approach to preference-based measures simultaneously incorporates
the capabilities and limitations (or positive treatment outcomes and side effects) within a
single score.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
10
A second technique used in preference-based measures is indirect estimation. In
this scenario responses to items on the measurement scale are combined with pre-
determined weights of specific health states referenced to the general population (Streiner
& Norman, 2008). This results in a comprehensive health status utility score.
In addition to describing a population’s health, utility scores from preference-
based measures can be incorporated into clinical trial outcomes to generate quality-
adjusted life years (QALYs). This allows economists and policy-makers to compare
outcomes from different disease populations and facilitates decision-making processes for
funding of programs.
Selection of an appropriate measurement tool requires consideration of the study
objective and outcome, the property of the measurement scale as well as the patient
population. These factors include type of outcome, sensitivity of measurement scale, and
previous use in the targeted patient population to assess reliability and validity. In
addition, potential cognitive limitations of the subjects due to age or impairment must be
considered, as the length of the instrument, language-level, required method of
administration (interview or self-completion) and the use of proxy reporting will
influence the selection of the most appropriate instrument (Tao & Parsons, 2005). The
population under study must also find the scale acceptable with respect to the content and
length so that the respondent remains engaged long enough to complete the questionnaire
(Feeny et al., 1999; Streiner & Norman, 2008). Finally, as scales vary, the individual
HRQL dimensions and corresponding definitions for the selected questionnaire should

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
11
also be considered carefully to ensure that the study objective will be addressed
adequately and quantified with the given scale (Feeny et al., 1999).
Measures of HRQL in Survivors of Brain Tumours in Childhood
Survivors of brain tumours in childhood and adolescence have a high prevalence
of long-term, chronic morbidities as a consequence of the disease itself as well as the
treatment (Anderson et al., 2001A). These individuals have been identified to have a
much greater burden of long-term medical, neurocognitive and psychosocial sequelae
compared to survivors of other childhood cancers. This is particularly of relevance given
the increasing incidence of pediatric brain tumour diagnoses as well as increase in the
survival of affected children (Jemal et al., 2004; Smith et al., 2010).
Historically, the long-term sequelae of surviving a childhood brain tumour were
characterized by neuropsychological outcomes, measured by intelligence tests and
academic markers, and chronic medical complications, assessed by traditional health
outcome measures including physical examination and laboratory results (Anderson,
Northam, Hendy & Wrenhall, 2001B; Mulhern et al. 1992; Packer et al., 2003). Although
these late effects of disease and treatment were well documented in the literature, the
overall burden of morbidity as experienced by the survivors was not as well understood
(Barr et al., 1994). In addition, attempts to capture the QOL of individuals were often
undertaken as interviews to elicit sociodemographic characteristics, including marital
status, educational level achieved and employment details (Mostow et al, 1991). Further,
there was agreement that outcomes from surviving a brain tumour in childhood differed

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
12
from the experience of survivors of CNS tumours occurring in adult life (Twombly,
2009).
Over the past two decades there has been an increasing interest in the QOL, and
specifically health-related morbidity, as experienced by survivors of childhood brain
tumours (Mulhern et al., 1998). The characterization of HRQL as perceived by the
survivors is being recognized increasingly as important insights into the lives of these
patients, and provides clinicians guidance into the late effects experienced by survivors as
well as an alternate measure of the success of therapeutic protocols (Anderson et al.,
2001A). As such, retrospective and prospective studies frequently include HRQL
measures to assess the burden of morbidity experienced by such survivors, and to explore
the potential factors that contribute to a perceived health state as outcomes from
therapeutic interventions.
In addition, research has been dedicated to identifying commonly used
questionnaires in research and evaluating the psychometric properties of generic as well
as disease-specific instruments used to measure HRQL in survivors of brain tumours. A
systematic review was undertaken by Klassen et al to identify the most commonly used
HRQL measures in children with cancer and survivors of childhood cancers (Klassen,
Anthony, Khan, Sung, & Klaassen, 2011). The terms “quality of life”, “health-related
quality of life”, “quality adjusted life years”, “health status”, “functional status”, “well-
being”, or “patient reported outcome” were used to search Embase, MEDLINE,
CINAHL, EMBASE, PsycINFO, Cancerlit and Sociological Abstracts from inception to
May 29, 2011. The primary objective of this team’s systematic review was to identify

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
13
pediatric measures used in research to evaluate HRQL of patients and survivors of
childhood cancer. This review included studies of patients less than 30-years of age and
utilized unmodified HRQL questionnaire. The patient populations within the studies
could include multiple conditions provided that results were reported on childhood cancer
patients. Intervention studies or studies of hematopoietic or stem cell transplant study
subjects were excluded. The systematic review being undertaken by Klassen et al.’s team
closely aligned with the objectives of the current thesis. As such collaboration was
established and support was provided by T. Nayiager in the identification and review of
eligible articles published between June 15, 2009 and May 25, 2011, as an up-date to the
initial systematic review.
Of the 111 studies identified by the overall systematic review, 36 studies provided
results on survivors, or mixed on-treatment patients and survivors, of brain tumours,
either as a single population, or reported within a mixed cancer population. The measures
used most often in these studies were the PedsQL (n=12), the Health Utilities Index
(HUI) (n=9) and the Child Health Questionnaire (CHQ) (n= 6). Other measures included
the Minneapolis Manchester Quality of Life (MMQL) (n=4), the TNO-AZL
Questionnaires for Children's Health-Related Quality of Life (TACQOL) (n=3), the
Quality of Life- Cancer Survivors (n=2), the Assessment of Quality of Life (n=1), and the
KINDL (n=1). Two studies used more than 1 family of HRQL measures.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
14
In a separate search of PubMed using the terms “quality of life”, “survivors”,
“childhood”, “brain tumour,” with no restriction on age, it was determined that the Short-
Form-36 (SF-36) is a commonly used instrument in HRQL studies of adult survivors of
brain tumours in childhood. A synopsis of the PedsQL, HUI, CHQ and SF-36 is presented
below.
The PedsQL is a family of instruments used in children and adolescents with acute
and chronic health conditions, including patients undergoing treatment for, as well as
survivors of, childhood cancers (Varni, 2013). The 23-question parent (proxy) and patient
(self) reporting generic module measures four domains: physical functioning, emotional
functioning, social functioning and school functioning. These can be summarized into
two summary scores: a physical health summary score and a psychosocial health
summary score. The cancer-specific module can be used in combination with the generic
instrument. This disease-specific questionnaire explores health concepts pertaining to
cancer-specific aspects of HRQL, which include treatment and procedural anxiety,
cognitive ability, patient worry, physical self-appearance, and communication (Bhat et
al., 2005). The generic and cancer-specific measures have been found to be reliable and
valid in estimating the HRQL of children and adolescents with present and past histories
of CNS tumours (Bhat et al., 2005). A specific brain tumour questionnaire is also
available however this instrument is very similar to the cancer measure and appears to be
applicable only to patients undergoing treatment.
Although the PedsQL is used extensively in research with children, there are
conceptual and practical concerns about this family of instruments. A Canadian study of

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
15
the properties of the PedsQL, parent respondent, by Amin et al. (2012) involving children
undergoing treatment for cancer identified validity issues using Rasch analysis
(comparison of trait actually possessed versus level scored on scale), poor distribution
across response categories for over half of the items, and potential bias in reporting of
physical function by age, as well as differences in parent reporting based on the gender of
the child.
In addition to the limitations outlined above, others have pointed out that the
PedsQL uses negative phrasing exclusively, with respondents asked to identify problems
in the identified areas (Fayed et al., 2011). This presents a logistical problem as positive
factors are excluded and may not completely represent the HRQOL of the individual. In
addition, the negative questioning connotes an interest into limitations and disability but
not necessarily functioning (Fayed et al., 2011). The negative phrasing may also be
psychologically burdensome for the respondent (Waters et al., 2009).
The HUI is a set of generic multi-attribute health status and HRQL instruments
that capture the overall health status as well as individual single attribute of an
individual’s health. This family of questionnaires includes different versions dependent
on the type of administration (interview or self-completion), type of respondent (self,
proxy-relative, proxy-clinician), number of questions (15 or 42), type of construct used to
define the domains (HUI version 2 or HUI version 3) and language (available in > 20
versions). The HUI2 and HUI3 systems have been evaluated for their psychometric
properties. The design of the HUI3 system is noted to be theoretically and empirically
founded as the utility scores were ascribed and then validated in a random sample of

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
16
individuals within a community (Feeny et al., 2002). In addition, there is almost an even
divide of negative and positive phrasing of questions (Fayed et al., 2011). The
questionnaires have been used in a variety of populations, including epidemiological
studies (Orpana et al., 2009) and in a wide range of ages (>5 years) and disease types,
including children with cancer and survivors (Health Utilities Inc, 2011). A more
detailed description and review of the HUI family of instruments is presented in the
“Methods” section of this Thesis.
The CHQ is a generic multidimensional instrument that measures the physical and
psychosocial health of children and adolescents. A proxy (parent)-reported questionnaire
utilises 50 items to derive outcomes on individual scales, which can be aggregated further
into overall physical and psychosocial scores (Landgraf, Abetz & Ware, 1996). The proxy
(parental)-reported form (CHQ PF-50) has 10 individual scales: physical functioning, role
limits secondary to emotional/behaviour, role limits secondary to physical health
problems, bodily pain, mental health, self-esteem, general health, parental impact-time,
parental emotional impact and behaviour. Responses are captured on four to six point
Likert scales. A Dutch study of the reliability and validity of this tool in a general
population of children established that the CHQ-parent form 50 was able to distinguish
between healthy children and those with chronic conditions. The authors also
demonstrated internal consistency reliability between related items, and test-retest
reliability for all subscales aside from behaviour (Raat, Bonsel, Essink-Bot, Landgraf,
Gemke, 2002). This instrument has been used also in assessing patients 1 to 18 years of
age with cancer, including those with a history of brain tumours (Sung et al, 2003;

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
17
Sawyer, Antoniou, Toogood, & Rice M, 1999; Sands et al., 2001). The CHQ has also
been shown to correlate with constructs of the HUI2 and HUI3 questionnaires in
childhood cancer survivors (Nixon et al., 1999).
The SF-36 is a generic measurement scale that uses responses from 36-items to
define eight domains constituting HRQL: physical functioning, role-physical, bodily pain,
general health, vitality, social functioning, role-emotional and mental health (Ware, &
Gandek, 1998). These subscales can be used to generate two summary scores for physical
and mental health. Concordance with decreasing self-rated health and scores generated by
the SF-36 questionnaire has been established (Jenkinson, Wright, & Coulter, 1994). In
addition, large population-based studies of the SF-36 have generated country, age-group
and gender specific normative data (Hopman et al., 2000). This scale has also been
demonstrated to be valid and reliable in studies of adult survivors of childhood cancer
(Barr et al., 1999, Glaser et al., 1999, Reulen et al., 2006). The SF-36 has been used
previously in adolescents; however, there is limited information available about the
validity of the instrument in this age group (SF-36.org, n.d.).
Previous Assessments of HRQL of Survivors of Brain Tumours in Childhood
A literature review using keywords of “quality of life”, “health related quality of
life”, “health status”, “survivors”, “brain tumours” , and “child” was undertaken on
Medline to explore the capabilities and limitations of survivors of brain tumours in
childhood in high income countries. This review was restricted to studies that utilized
HRQL instruments; the scores could be based on either self- or proxy- reporting. There
was no restriction on age of survivors or minimum time from diagnosis. However,

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
18
subjects must have been diagnosed with a primary brain tumour during childhood or
adolescence (<21 years of age). Studies that included a mixed population of cancer types
or patients undergoing treatment as well as survivors were reviewed provided that
information on brain tumours survivors was presented independently. The objective of
this review was to provide a foundation of the previous work undertaken in the HRQL of
survivors of brain tumours.
McMaster Children’s Hospital (MCH) was one of the first institutions to
recognize the need for and subsequently develop a systematic measurement instrument to
capture the multi-attribute health status of survivors of childhood cancers, which was
piloted initially in brain tumour survivors to assess feasibility (Barr et al.,1994; Feeny,
Furlong, Boyle & Torrance, 1995). The instrument developed at MCH was based on the
HUI system and captured the global health status and severity of morbidity in subjects
using self- or proxy- reporting (Feeny et al., 1995). Descriptive and quantitative outcomes
from this small case series revealed a wide range of severity in morbidities experienced
by survivors of childhood brain tumours, with the recommendation that HRQL should be
a contributing measure of success in clinical trials (Barr, et al., 1999).
A second more comprehensive study was undertaken in the neuro-oncology
follow-up clinic at MCH between 1993 and 1995 (Barr et al., 1999). Forty-one
participants diagnosed with a brain tumour (irrespective of type, location and treatment),
mean age of 9.5 years (range of 1.7 to 17.9 years), mean time from diagnosis of 3.3 years
(range 0.2 to 8.6 years), underwent HRQL assessment using the 15-item HUI2/3
questionnaires. Questionnaires were completed by a nurse proxy as well as parent proxy;

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
19
subjects who were at least 9.5 years of age also completed a self-administered
questionnaire. The severity and number of areas of morbidity in this cohort, as captured
by the overall health utility score by the nurse reporting, ranged from 0.12 to 1.00
(median 0.92) for HUI2, and -0.27 to 1.0 (median 0.77) for HUI3, with negative scores
reflecting states of health worse than being dead. Over three-quarters of participants were
noted to have some level of morbidity (83% by HUI2 and 78% by HUI3). The authors
reviewed the frequency and severity of morbidity of the single attributes for the HUI2 and
HUI3 systems and noted that there was inter-subject variability in the degree of morbidity
within a single attribute.
The authors also noted that the most common morbidities reported were in
attributes predicted by clinical experience. The single-attribute utility scores for these
attributes observed were much lower than the HUI3 data available from the 1991
Canadian General Society Survey (CGSS), using the results for the youngest age group of
15 to 19 years. These attributes included vision (30% reporting limitations in brain
tumour survivors, versus 26% in CGSS), ambulation/mobility (19 % in brain tumour
survivors versus 0% in the CGSS), emotion (26% in brain tumour survivors versus 21%
in the CGSS) and cognition (68% in brain tumour survivors versus 24% in the CGSS).
In addition to these deficits, there was also an unexpected prevalence of pain
reported for this cohort of patients, as 32% of brain tumour survivors were noted by
nurse-reporting to have pain whereas the CGSS reported that 22% of individuals aged 15
to 19 years reported pain. The increased prevalence of pain was particularly surprising as
previous literature did not suggest issues with discomfort in this patient population;

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
20
however a study undertaken in survivors of adult brain tumours did note that almost 50%
of participants reported pain (Packer et al., 2003, Whitton, Rhydderch, Furlong, Feeny &
Barr, 1997).
A complementary study was undertaken in Nottingham, UK, during the same time
interval (Glaser et al., 1999). The patient population consisted of 30 survivors, mean age
at assessment of 10.5 years (range 6 to 16 years) and at a mean of 4.1 years from
diagnosis (range of 1 to 10 years). The 15-item HUI2/3 questionnaire, modified for the
UK population, was completed by parents, children, physiotherapists and physicians. The
results were similar to those reported in the McMaster study, with 79% of participants
noted to experience some morbidity by both HUI systems. Comparison at a single
attribute level identified similar areas of deficits, although the prevalence and degree of
severity varied between the two populations. Once again, an unexpected high prevalence
of pain was noted in this patient cohort, with approximately 30% reporting pain, which
was similar to the results observed by Barr et al, (1999) in Hamilton, Ontario.
The identified morbidities, as experienced by the individual patients in the context
of their daily lives, emphasized the need for further exploration of HRQL in survivors of
brain tumours in childhood. Subsequent studies, including those using alternate
measurement instruments, matched controls and large, population-based studies, also
identified burdens of morbidity in this patient cohort.
In a single institution in California, a cohort of 25 brain tumour patients actively
undergoing treatment and 109 post-therapy survivors ( median time from diagnosis of 3.2

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
21
years for overall cohort), as well as their parents, completed the PedsQL 4.0 generic
questionnaire (Bhat et al., 2005). In comparison to healthy children, patients (median age
of 11.3 years) reported statistically significantly worse HRQL in all of the subscales,
including physical health (which encompasses pain, measured as a single item within the
eight item physical function scale), emotional and social functioning. In keeping with
findings in the previous two studies, considerable variability between patients was noted.
A sub-analysis of the patient cohort revealed no evidence that patients further
from diagnosis reported better HRQL than those treated more recently. Although this was
determined by stratifying the patients based on time from diagnosis rather than following
a single cohort through time, this result was of particular interest as it was anticipated that
HRQL would improve with time for brain tumour survivors, as observed in children
diagnosed with other types of cancers (Varni, Burwinkle, Katz, Meeske & Dickinson,
2002).
One study undertaken at the Memorial Sloan Kettering Cancer Center attempted
to capture the influence of time on HRQL in a single cohort of patients as an outcome
measure of an interventional study (Sands et al., 2010). Survivors of malignant brain
tumours in childhood treated with the “Head Start 1” protocol consisting of myeloablative
chemotherapy, autologous stem cell rescue and either no or delayed cranial radiation
(Mason et al.,1998) were assessed in 1991 (N=25, mean time from diagnosis of 5.7 years)
and again in 1997 (N=19, mean time from diagnosis of 11.6 years). Parents of these
children (mean age of 8.1 years at T1 and 13.5 years at T2) completed the CHQ-PF50
questionnaire as a measure of HRQL at both time points, irrespective of the age of the

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
22
patient. Unlike previous studies, the findings noted that, as a group, physical and
psychosocial scores were within normal ranges at both time points, including bodily pain
(81% of patients in 1991 and 89.5% of patients in 1997) based on age-adjusted T-scores.
Although as a group there appeared to be little difference between the survivors and their
peers, a wide range of severity of disability was observed in these children. Interestingly,
the authors also recognized a trend to improvement of role limitations due to physical
functioning, but a significant decrease in general health between the two time points. This
suggests that HRQL may change over time as perceived by the parents of survivors of
brain tumours in childhood. Self-reporting may provide greater insight into the HRQL of
these individuals and the influence of time from diagnosis, particularly when these
survivors transition into adulthood.
The TACQOL measurement instrument is another tool that has been used in
children who have survived brain tumours and has demonstrated a burden of morbidity
experienced by this patient population. A study in the Netherlands of 38 children
surviving low grade astrocytomas, one of the most frequently occurring tumours that
require intervention, noted problems in physical, motor, cognitive, autonomy and social
domains as reported by parents (Aarsen et al.,2006). Children reported a slightly better
QOL, but still noted issues with motor, cognitive and social functioning. No specific
details regarding pain were reported; however this was incorporated in the physical
domain of the instrument. From the TACQOL questionnaire, the items directly soliciting
information regarding pain are in reference to stomach ache or abdominal pain, and colic.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
23
The challenges faced by survivors of brain tumours in childhood were also
appreciable in large surveillance studies investigating the HRQL of survivors of
childhood malignancies. The Childhood Cancer Survivor Study (CCSS), one of the
largest studies undertaken, included 26 institutions across Canada and the US and
explored the long-term outcomes of children and adolescents diagnosed with a
malignancy between 1970 and 1986, with the availability of matched sibling controls
(Packer et al., 2003). Armstrong et al. (2009) reviewed HRQL data for long term
survivors of brain tumours in childhood (N=1877, range of 5 to 34 years of survival after
diagnosis). The authors concluded that patients reported higher rates of impaired health
status than their siblings, in overall health as well as mental health, functional
impairment, activity limitation, pain and cancer-related anxiety, as measured by the SF-36
questionnaire and Cantril Ladder of Life (Armstrong et al., 2009). In keeping with the
smaller brain tumour specific studies presented earlier, pain was observed to be a
considerable morbidity in this study as measured by the SF-36, with brain tumour
survivors being 7.9 times more likely to report experiencing pain than their siblings.
A similar study of adult survivors of childhood cancer was undertaken in the UK
(Reulen et al., 2007). Retrospective analysis of the results demonstrated that CNS tumour
survivors were found to have a SF-36 summary scores substantially lower than the
population norms for mental health (difference of -0.1, 99% confidence interval of -2.2 to
-0.9) and physical health (lower scores at all ages, ranging from -4.1 (-6.0 to -2.5) to -7.5
(-8.9 to -3.1) , which includes pain. Patients with a history of CNS radiation also had
significantly lower physical component summary scores than survivors of leukemia, who

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
24
were used as the reference group in the study. Stratification by age also demonstrated that
individuals 25 years of age and older had increasing prevalence of physical health
limitations.
Population-based studies of childhood cancer survivors also revealed a significant
burden of morbidity, particularly in CNS tumour survivors. A cross-sectional Canada-
wide study of a random sample of childhood cancer survivors diagnosed before 20 years
of age between 1981 and 1990 and had survived at least five years from diagnosis were
identified from 12 pediatric oncology centres and provincial cancer registries (Pogany et
al., 2005). These individuals, as well as a cohort of the general population with no history
of cancer, completed mailed HUI3 questionnaires. CNS tumour survivors accounted for
362 of the 2152 participants with a history of cancer. Increased impairment in all
attributes contributing to HRQL was observed for cancer survivors as a group in
comparison to population controls. However, a particularly large burden of morbidity was
detected in survivors of CNS tumours in childhood. In comparison to other cancer
survivors as well as controls, patients with prior CNS tumours had amongst the lowest
overall HRQL, as determined by the percentage in the bottom quartile as well as mean
summary scores. CNS tumour survivors were noted to have greater impairment in
dexterity, ambulation, speech and cognition in comparison to other survivors. Single-
attribute mean scores of CNS tumour survivors demonstrated particularly high burdens of
morbidity in cognition, emotion and pain. Although the burden of pain would have
influenced the overall health status summary score, unlike the CCSS study, there did not
appear to be a large difference in the pain experienced by cancer survivors and controls.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
25
The percent of CNS tumour survivors reporting pain was less than that in the controls
(37% versus 44% respectively), but cancer survivors as a whole also reported less pain
than controls.
Another cross-sectional Canada-wide study of survivors of cancer in childhood
(N=1334, mean age 23 years, range of 15 to 37 years), who were greater than five years
from diagnosis, was undertaken in those diagnosed between 1981 and 1990, using the SF-
36 questionnaire (Maunsell et al., 2006). Again, CNS tumour survivors, in contrast to the
majority of other childhood cancer survivors (aside from those with bone tumours), had
lower overall HRQL scores than age- and gender-matched controls. Areas of greatest
deficiencies were general health, physical function, physical role, vitality, social function
and mental health. Unlike results from the CCSS study, but similar to the results seen by
Pogany et al. (2005), bodily pain and emotional role were not identified as statistically
different from controls.
The 15-item HUI3instrument was used in a prospective population-based cohort
study in Piedmont, Italy to assess the HRQL of long-term survivors (>five years from
diagnosis) of childhood cancer (Alessi et al., 2007). Long-term CNS tumour survivors
(n=133 out of 644 cancer survivors) as a group were identified to have the lowest overall
HRQL in comparison to all other cancer types. Further, CNS tumour survivors were over
represented (5 out of 11) in the group of individuals reporting an overall HRQL of lower
than 0.00 (worse than death). In addition, these adolescents and adults (age range of 15
years to > 35 years) with a history of primary CNS tumours had significant burdens of
morbidity, by both prevalence and severity, in the areas of cognition, pain, and vision.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
26
While most survivors did not indicate issues with emotion, those who did report
difficulties noted a severe impairment. Problems with ambulation and dexterity were also
identified by survivors, but these were not severe.
Summary of the Studies Reviewed
A preponderance of the studies reviewed reported a burden of morbidity amongst
survivors of brain tumours in childhood, which were often greater than those observed in
the normal population or in comparison to other childhood cancer survivors (Table 1 and
Table 2). Some of these studies also identified an unexpected burden of pain, which is not
well characterized. In addition, exploration of the influence of time on HRQL,
undertaken either by stratifying patients by time from diagnosis or following a cohort of
individuals over time, suggested that survivors of brain tumours in childhood may
experience greater difficulty as they progress through life after completing treatment
(Bhat et al., 2005; Sands et al., 2001).
There is still limited information available regarding the HRQL of long-term
survivors of brain tumours in childhood and adolescence. In addition, the change of
HRQL over time, particularly from childhood into adulthood, is relatively unknown. It
has been suggested that burdens of morbidity may influence other issues pertaining to
QOL, such as educational achievement and employability, and HRQL will change over
time (Zebrack & Zeltzer 2003; Zeltzer et al., 2009). Furthermore, it is important to
provide survivors the opportunity to self-report on their HRQL to best appreciate the
burden experienced by this population (Recklitis, O’Leary & Diller, 2003).

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
27
MCH has a longstanding interest in the HRQL of survivors of brain tumours in
childhood. Given the unanticipated prevalence of pain identified in several studies, an
exploratory cross-sectional investigation was undertaken to capture the HRQL of
survivors more than 10 years from diagnosis using the HUI2/3 system, as well as
additional measures to better characterize the pain, including the potential relationship
with other morbidities experienced by this patient population. In addition, the stability
and severity of pain over time were explored using previously unpublished results of
previous HUI2/3survey data undertaken in the same cohort.

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
28
Stu
dy
L
oca
tio
n
Meth
od
olo
gy
P
arti
cip
an
ts
Yea
rs o
f
dia
gn
osis
Ag
e o
f su
rv
ivors a
t ti
me
of
su
rv
ey
Tim
e f
ro
m d
iag
no
sis
Barr
et
al.
,19
99
H
am
ilto
n,
ON
, C
an
ad
a
Pro
sp
ecti
ve
41
su
rviv
ors
of
bra
in
tum
ou
rs
19
93
-19
95
M
ean
of
9.5
years
(ra
nge
of
1.7
to
17
.9 y
ears
)
Mean
of
3.3
years
,
ran
ge o
f 0
.2 t
o 8
.6
years
Gla
ser
et
al.
,
19
99
No
ttin
gh
am
,
UK
Pro
sp
ecti
ve
28
su
rviv
ors
of
bra
in
tum
ou
rs
Un
kn
ow
n
Mean
of
10
.5 y
ears
(ra
nge
of
6 t
o 1
6 y
ears
)
Mean
of
4.1
years
,
ran
ge o
f 1
to
10
years
San
ds e
t a
l.,
20
01
New
Yo
rk,
NY
, U
SA
Pro
sp
ecti
ve,
lon
git
ud
inal
T1
= 2
5 s
urv
ivo
rs o
f
bra
in t
um
ou
rs
T2
=1
9 s
urv
ivo
rs o
f
bra
in t
um
ou
rs
19
91
-19
97
T
1=
mean
age o
f 8
.1 y
ears
(SD
2.3
4)
T2
= m
ean
age o
f 1
3.5
years
(S
D 2
.24
)
T1
= m
ean
of
5.7
years
, T
2=
mean
of
11
.6 y
ears
Bh
at
et
al.
, 2
00
5
Palo
Alt
o,
CA
, U
SA
Pro
sp
ecti
ve
10
9 s
urv
ivo
rs o
f
bra
in t
um
ou
rs
25
bra
in t
um
ou
r
pati
ents
on
-th
era
py
Un
kn
ow
n
Mean
11
.82
years
, S
D
5.3
9
Mean
of
4.2
6 y
ears
,
SD
of
4.4
1
Aars
en
et
al.
,20
06
N
eth
erl
an
ds
Pro
sp
ecti
ve
38
su
rviv
ors
of
low
gra
de a
str
ocyto
mas
19
94
-20
00
1
5 y
ears
(E
sti
mate
d b
ased
on
age o
f d
iagn
osis
+ #
years
in
fo
llo
w-u
p)
Mean
of
7.7
years
,
ran
ge 3
.7 t
o 1
1.4
years
Po
gan
y e
t a
l.,
20
06
Can
ad
a
Retr
osp
ecti
ve
36
2 s
urv
ivo
rs o
f
bra
in t
um
ou
rs (
ou
t o
f
21
52
mix
ed
can
cers
)
19
81
-19
90
6
3.8
% (
13
59
) w
ere
rep
ort
ed
to
be g
reate
r th
an
16
years
of
age (
all
su
rviv
ors
)
Gre
ate
r th
an
5 y
ears
Mau
nsell
et
al.
,
20
06
Can
ad
a
Pro
sp
ecti
ve
23
8 s
urv
ivo
rs o
f
bra
in t
um
ou
rs (
ou
t o
f
13
34
mix
ed
can
cers
)
19
81
-19
90
M
ean
of
23
years
(SD
5.2
) fo
r b
rain
tu
mo
ur
co
ho
rt
83
.5%
were
10
or
mo
re y
ears
fro
m
dia
gn
osis
Reu
len
et
al.
,
20
07
UK
R
etr
osp
ecti
ve
21
88
su
rviv
ors
of
bra
in t
um
ou
rs (
ou
t o
f
10
18
9 m
ixed
can
cer
su
rviv
ors
)
19
40
-19
91
M
ean
of
30
.4 y
ears
(all
su
rviv
ors
)
23
.5 y
ears
(E
sti
mate
d
based
on
mean
age
qu
esti
on
nair
e
co
mp
lete
d -
mean
age
at
dia
gn
osis
)
Ale
ssi
et
al.
,20
07
P
ied
mo
nt,
Italy
Pro
sp
ecti
ve
13
3 s
urv
ivo
rs o
f
bra
in t
um
ou
rs (
ou
t o
f
69
1 m
ixed
can
cers
)
19
67
-19
96
1
5 t
o g
reate
r th
an
35
years
(mean
no
t sp
ecif
ied
)
Gre
ate
r th
an
5 y
ears
(mean
no
t sp
ecif
ied
)
Arm
str
on
g e
t a
l.,
20
09
Can
ad
a a
nd
US
Retr
osp
ecti
ve
18
77
su
rviv
ors
of
bra
in t
um
ou
rs
19
70
-19
86
N
um
ber
of
part
icip
an
t (%
)
wit
h S
tud
y S
pecif
ied
Age
Ran
ge:
0 –
14
years
= 2
52
(1
3.4
)
≥ 5
years
Table
1. S
um
mar
y o
f st
ud
y d
esig
n a
nd p
atie
nt
char
acte
rist
ics
in s
tudie
s re
vie
wed
, ar
ranged
by a
scen
din
g o
rder
of
publi
cati
on d
ate

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
29
Stu
dy
Q
ues
tion
nair
e S
elf/
Pro
xy
*P
rim
ary
(if
ap
pli
cab
le)
HR
QL
Ou
tcom
es f
or S
urv
ivor
s of
Bra
in T
um
ou
rs i
n C
hil
dh
ood
Bar
r et
al.
,
1999
HU
I2/3
P
rox
y- n
urs
e*
Pro
xy-
par
ent
Sel
f (>
9.5
yea
rs)
-Ove
rall
mea
n H
UI2
sco
re o
f 0.9
2 (
range
of
0.1
2 t
o 1
.0)
-Ove
rall
mea
n H
UI3
sco
re o
f 0.7
7 (
-0.2
7 t
o 1
.0)
-Burd
ens
of
morb
idit
y, a
s m
easu
red b
y pre
vale
nce
, w
ere
note
d i
n
attr
ibut
es o
f co
gnit
ion, em
oti
on, se
nsa
tion
, vi
sion,
mobil
ity/
ambula
tion,
and p
ain
. P
ain w
as r
eport
ed i
n 2
7%
of
par
tici
pan
ts b
y H
UI2
and 3
2%
by
HU
I3
Gla
ser
et
al.
,1999
HU
I2/3
UK
P
rox
y- p
aren
t
Pro
xy-
ph
ysic
ian
Pro
xy-
ph
ysio
ther
apis
t*
Sel
f (w
ith h
elp o
f pl
ay
spec
iali
st f
or
<9 y
ears
)
-Ove
rall
mea
n H
UI2
sco
re o
f 0.7
8 (
range
of
0.3
6 t
o 1
.0)
-Ove
rall
mea
n H
UI3
sco
re o
f 0.6
6 (
range
of
0.1
7 t
o 1
.0)
-Burd
ens
of
morb
idit
y, a
s m
easu
red b
y pre
vale
nce
, w
ere
note
d i
n
attr
ibut
ed o
f em
oti
on, c
ogn
itio
n,
self
-car
e, p
ain.
Pai
n w
as r
eport
ed i
n
34%
of
par
tici
pan
ts b
y H
UI2
and 2
8%
by
HU
I3.
San
ds
et
al.
, 2001
CH
Q-P
F50
P
rox
y-par
ent
-Ph
ysic
al a
nd p
sych
oso
cial
sco
res
wit
hin
norm
al r
ange
of
pee
rs b
ased
on
adju
sted
T-s
core
s at
bot
h t
ime
poin
ts
-Dec
reas
ed g
ener
al h
ealt
h a
t T
2
-Wid
e ra
nge
of
seve
rity
of
dis
abil
itie
s at
T1 a
nd T
2.
Bodil
y pai
n w
as
report
ed a
t gr
eate
r th
an n
orm
al l
imit
s in
4 p
atie
nts
(16%
) at
T1 a
nd 2
pat
ient
s (1
0.5
%)
at T
2.
Bhat
et
al.
,
2005
Ped
sQL
(ge
ner
ic)
4.0
Pro
xy-
Par
ent*
Sel
f
-Dec
reas
ed p
hys
ical
hea
lth
(in
corp
ora
tes
pain
sco
re),
em
oti
ona
l an
d
soci
al f
unct
ionin
g in
com
pari
son t
o h
ealt
hy c
ontr
ols
-Incr
easi
ng
burd
ens
in c
om
munic
atio
n o
f il
lnes
s an
d d
ecre
ased
soci
al
funct
ionin
g as
pro
gres
s fu
rther
fro
m d
iagn
osi
s.
-Pai
n n
ot
expli
citl
y st
ated
to b
e a
burd
en
Aar
sen e
t
al.
, 2006
TA
CQ
OL
P
rox
y-par
ent
Sel
f (>
8 y
ears
)
-Dif
ficu
ltie
s w
ith p
hys
ical
(in
corp
ora
tes
pain
), m
oto
r, c
ogn
itiv
e,
auto
nom
y an
d s
oci
al d
om
ains
bas
ed o
n p
aren
t re
port
ing
-Dif
ficu
ltie
s w
ith m
otor,
cogn
itiv
e an
d s
oci
al f
unct
ionin
g bas
ed o
n
pat
ient
rep
ort
ing.
-Pai
n n
ot
expli
citl
y st
ated
to b
e a
burd
en
Table
2. S
um
mar
y o
f st
ud
y m
ethods
and o
utc
om
e of
studie
s re
vie
wed
, ar
ranged
by a
scen
din
g o
rder
of
publi
cati
on d
ate

M.Sc. Thesis- T. Nayiager; McMaster University– Health Research Methodologies
30
Stu
dy
Q
uest
ion
nair
e
Self
/Proxy
*P
rim
ary
(if
ap
pli
cab
le)
HR
QL
Ou
tcom
es
for S
urviv
ors
of
Brain
Tu
mou
rs
in C
hil
dh
ood
Pogan
y e
t
al.
, 2006
HU
I3
Sel
f -L
ow
er o
ver
all
HR
QL
sco
res
in b
rain
tum
our
surv
ivors
in c
om
par
ison t
o
contr
ols
as
wel
l as
oth
er c
ance
r su
rviv
ors
-Over
all
mea
n s
core
for
bra
in t
um
our
surv
ivors
of
0.7
5 (
SD
of
0.2
6)
-Are
as o
f gre
ates
t burd
ens
of
morb
idit
y b
y m
ean
HU
I sc
ore
wer
e
cognit
ion (
0.8
7),
em
oti
on (
0.9
2)
and p
ain (
0.9
3)
-Are
as o
f gre
ates
t burd
ens
in c
om
par
ison t
o o
ther
can
cer
surv
ivors
wer
e
cognit
ion, dex
teri
ty, sp
eech
and a
mbula
tion.
-37.3
% o
f C
NS
Tum
our
surv
ivors
rep
ort
ed e
xper
ienci
ng p
ain
Mau
nse
ll e
t
al.
, 2006
SF
-36
S
elf
-Low
er o
ver
all
HR
QL
sco
res
in b
rain
tum
our
surv
ivors
in c
om
par
ison t
o
age
and g
ender
mat
ched
contr
ols
, as
wel
l as
most
oth
er c
ance
r
surv
ivors
.
-Dec
reas
ed g
ener
al h
ealt
h, physi
cal
funct
ion, ph
ysi
cal
role
, vit
alit
y,
soci
al f
unct
ion a
nd m
enta
l hea
lth c
om
par
ed t
o c
ontr
ols
-Bodil
y p
ain r
eport
ed b
y C
NS
surv
ivors
was
not
found t
o b
e
signif
ican
tly d
iffe
rent
from
contr
ols
Reu
len e
t
al.
, 2007
SF
-36
S
elf
-Dec
reas
ed p
hysi
cal
sum
mar
y c
om
ponen
t sc
ore
on C
NS
surv
ivors
in
com
par
ison t
o g
ener
al p
opula
tion, as
wel
l as
leu
kem
ia s
urv
ivors
.
-Incr
ease
d p
hysi
cal
hea
lth l
imit
atio
ns
of
CN
S s
urv
ivors
wit
h a
ge
bas
ed
on s
trat
ific
atio
n
-Pai
n n
ot
expli
citl
y i
den
tifi
ed t
o b
e a
burd
en i
n C
NS
surv
ivors
Ale
ssi
et
al.
, 2007
HU
I3
Sel
f -W
ors
t o
ver
all
HR
QL
see
n i
n b
rain
tum
our
surv
ivors
in c
om
par
ison t
o
oth
er c
ance
r ty
pes
.
-Gre
ates
t m
orb
idit
y o
bse
rved
in d
om
ains
of
cognit
ion, pai
n a
nd v
isio
n.
-35.3
% o
f C
NS
surv
ivors
rep
ort
ed p
ain
-Sever
ity o
f pai
n i
den
tifi
ed t
o b
e gre
ater
in C
NS
surv
ivors
in c
om
par
ison
to s
urv
ivors
wit
h o
ther
mal
ignan
cies
Arm
stro
ng
et a
l.,
2009
SF
-36, C
antr
il
Lad
der
of
Lif
e
Sel
f
-Hig
her
rat
es o
f im
pai
rmen
t in
over
all
hea
lth, m
enta
l hea
lth, fu
nct
ional
impai
rmen
t, a
ctiv
ity l
imit
atio
n, pai
n a
nd c
ance
r-re
late
d a
nxie
ty i
n
com
par
ison t
o s
ibli
ngs.
-Rel
ativ
e ri
sk o
f pai
n f
or
CN
S s
urv
ivors
was
7.9
, 95%
CI=
5.5
in
com
par
ison t
o s
ibli
ngs
Table
2 c
onti
nued
. S
um
mar
y o
f st
ud
y m
ethods
and o
utc
om
e of
studie
s re
vie
wed
, ar
ranged
by a
scen
din
g
ord
er o
f publi
cati
on d
ate

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
31
METHODS
Objective
The primary objective of this study was to explore the prevalence and burden of
pain in a cohort of survivors of brain tumours in childhood who were at least ten years
from diagnosis. Secondary objectives included investigating the correlation of responses
between participant and participant-identified proxy reporting, determining other areas of
morbidity, and examining the trajectory of the prevalence and severity of pain over a
decade. The following hypotheses were generated a priori based on the literature
available and guided the design of this study:
1. In long-term survivors of brain tumours in childhood greater than 35% of
respondents will report pain as measured by the HUI2/3 questionnaire.
2. The expected correlation between proxy- and self- reported pain will be
less than 0.40 for both HUI2 and HUI3.
3. Other areas of increased morbidity will be identified in the overall cohort,
including in attributes of emotion and cognition.
4. Pain will be persistent in the overall cohort over a period of 10 years.
Study Design
The work presented in this thesis is part of a longitudinal prospective cohort study
that commenced in 2001 and attempted to characterize the change in HRQL, and in
particular pain, over a ten-year period. The initial study (2001/2002) identified survivors
who were diagnosed with a primary brain tumour in childhood at MCH at least two years
prior. At the commencement of the initial study, individuals who were less than five years

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
32
of age at the time or who had relapsed or had progression of the disease were excluded.
Eligible and consenting participants were followed at five-year intervals over a ten year
period (Figure 7). Participants as well as a proxy completed the HUI2/3 instrument as a
measure of HRQL at each of the three time points (2001/2002, 2005/2006 and
2011/2012). Self-reports of the presence of pain on at least one occasion in the week prior
to the survey resulted in additional questions (independent of the HUI system) to
characterize the pain. These additional questions included the exploration of the
frequency, location and intensity of the pain. The outcome of the results collected at the
2001/2002 and 2005/2006 time points have been presented previously by other authors
(Barr, 2006, Horsman et al., 2006, Horsman et al., 2007).
The work presented in this thesis is primarily from the last time point (2011/2012)
of the longitudinal study. The methodology and outcomes were approached as a cross-
sectional study with the intended purpose of exploring the HRQL, with a focus on pain,
of long-term survivors of a primary brain tumour in childhood at a single institution. In
addition to the HRQL instrument and pain measures, sociodemographic as well as overall
QOL were collected in order to provide a more complete understanding of this cohort.
The previous results from the longitudinal study provided an opportunity to explore the
persistence of pain over a decade in the same group of individuals. Imputation was
undertaken for data missing due to any reason for non-participation, aside from a subject
who died and was excluded from the longitudinal analysis. A summary of the methods
for this thesis is shown in Figure 1.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
33
Cohort identified and
eligibility confirmed
Subjects and proxies
contacted and consented
HUI2/3 Questionnaire administered
Responses entered into
database and coded
Demographic and clinical
data captured
Sociodemographic and Quality of Life data elicited
Description of entire
cohort -HRQL -Sociodemographics -General quality of life -Proxy reporting
Burden of morbidity for
group with pain -Description of burden
of pain -Comparison of groups with
and without pain
Data linkage to previous time points
by participant identifier
Identification of participants with pain
HRQL Single and Multi Attribute
scores generated
Master database created
for analysis
Protocol developed and ethics approval granted
Characterization of pain using coloured analogue scale,
and homunculus
Imputation of missing data
Longitudinal analysis of pain and
overall health-related quality of life
Figure 1. Schematic diagram of study methods used to explore the health-related quality of life
in survivors of brain tumours in childhood over a ten-year period. Measures include
the HUI2/3 questionnaire, as well as additional investigations to characterize the
burden of pain experienced by the patient cohort. Sociodemographic and quality of
life information was also captured at time point 3.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
34
Rationale
Cross Sectional Study Design
A cross-sectional study design was selected to address the primary objective of
exploring the burden of pain in long-term survivors of brain tumours in childhood. This
type of study design is well-suited to provide estimations of the prevalence and burden of
morbidity at a single point in time in a pre-specified population, and when the item of
interest is not well-described in the literature. Cross-sectional studies are limited in the
determination of attribution of outcomes to the primary disease. This is particularly the
case when there is a considerable period of time from the exposure to the outcome. As the
current study population was at least ten years from their primary brain tumour diagnosis,
this limitation is important. However, the objective of this study was to estimate and
describe the burden of pain in long-term survivors, rather than to determine causality. As
such, this study design was deemed appropriate for this context. This point is further
established by the collection of data being restricted to HRQL, sociodemographic
information and overall QOL, and not attempting to investigate potential causes of pain.
Sample Selection
A consecutive sample was undertaken, with recruitment restricted to a single
institution. This increased feasibility as well as decreased selection bias as all eligible
subjects were given the opportunity to participate, rather than a random sampling of
patients.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
35
All participants diagnosed with a brain tumour at least ten years prior at MCH,
irrespective of subsequent disease, and who had been receptive to previous similar HRQL
studies, were invited to participate in this study. Limited exclusion criteria allowed for the
inclusion of the maximum number of participants and provided an overview of this
patient population. In addition, it was recognized that the interviewer-administered
questionnaire could exclude potential participants and create a bias based on geographical
proximity to the hospital. As such all subjects were given the opportunity to undertake the
interview in-person or over the phone. Clinical information for the identified eligible
cohort was available and as such comparison for systematic differences between
participants and non-participants was undertaken.
Measurement Instruments
Measurement of HRQL of participants was undertaken using the interviewer-
administered Health Utilities Index (HUI®) questionnaire (HUI23S1E.40Q), which has
been validated previously in brain tumour survivors (Barr et al., 1999, Glaser et al.,
1999). The HUI family of instruments is used widely in clinical research, often for cross-
sectional studies, and these are referenced to the Canadian population in the Canadian
General Social Survey (Furlong et al., 2001). In addition, clinically important differences
of greater than 0.05 for single attribute utility scores, and 0.03 for multi-attribute scores
have been established previously and accepted by the clinical and research communities
(Horsman, Furlong, Feeny & Torrance, 2003).

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
36
The HUI2/3 interviewer-administered questionnaire is a single measurement
instrument comprised of 40 items that utilizes responses to generate single attribute
HRQL levels and utility scores as well as overall health status and HRQL. These
questions are based on capabilities at the time period of the questionnaire, which for this
project was defined as a one-week recollection period. This was beneficial as it provided
an estimate of the burden of morbidity at a point in time while accounting for possible
day-to-day variances, including weekdays and weekends. The HUI2 system provides
estimates of morbidity burden for seven specific attributes: sensation, mobility, emotion,
cognition, self-care, pain and fertility. The HUI3 system maps onto eight variables:
vision, hearing, speech, ambulation, dexterity, emotion, cognition and pain. These
attributes, aside from fertility, were considered in this study.
The HUI2/3 utilizes a branching-logic format to classify a person’s
comprehensive health status using algorithms corresponding to responses to questions
(Furlong, Feeny, Torrance & Barr, 1998). The mapping of questions onto attributes has
been established previously, based on prior studies and experience of the creators of the
HUI questionnaires (Furlong et al., 1998). The number of questions is dependent on the
attribute as well as the response. HUI3 vision, for example, requires responses to a set of
five questions, while ambulation capability is determined on responses to seven
questions. A response of “perfect” function would result in an automatic “not applicable”
score to subsequent questions relating to the same attribute. A response of functional
limitation requires responses to further questions in order to establish a level.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
37
In some cases there are overlaps between questions in the HUI2 and HUI3
systems. For example, those used to define HUI3 levels of vision, hearing and speech are
used in combination to generate the level for the HUI2 attribute of sensation. Similarly,
responses for HUI2 mobility are derived from responses that are used to generate levels
for HUI3 ambulation and dexterity. A detailed description of the responses and
corresponding levels can be found on Tables 1 through 8 in the HUI procedures manual
(Furlong et al., 1998). The levels generated can be converted to single- and multi-
attribute utility scores using multiplicative functions. These utility scores describe the
burden of morbidity within the context of relative desirability of a given functional state
(Furlong et al., 1998). The syntax for the algorithm to derive the single attribute levels as
well as single- and multi- attribute utility scores was made available through an in-kind
student grant for this project.
Single attribute level scores were determined. The levels are assigned a numerical
value, with 1 being no disability and the upper limit (severe morbidity) ranging from four
to six, depending on the attribute in question. The single attribute levels were categorized
into four previously established levels of disability: none, mild, moderate and severe
(Furlong et al., 1998). These disability levels are based on preference scores rather than
functional capacity, and as such have ordinal and not interval properties. The conversion
to the four descriptor levels for each attribute was undertaken as it allowed for easier
comprehension of the degree of disability, and for identification of areas with a high
prevalence of morbidity. Interval-level single attribute utility scores as well as multi-

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
38
attribute utility scores were also generated for both HUI2 and HUI3 systems, which
enabled parametric testing of hypotheses.
HUI2 and HUI3 are noted to have overlapping attributes. A previous study
undertaken in a cohort of pediatric brain tumour survivors demonstrated very good
agreement with respect to the frequency of morbidity for overlapping attributes (Barr et
al., 1999). However, the constructs differ between HUI2 and HUI3 (Table 3 and Table 4)
(Feeny et al., 1995). As such, these two systems are considered to be complementary, and
both were used in this study. The 2 systems were combined into a single questionnaire
using specific grouping and ordering of questions as recommended by HUInc.
Table 3. Summary of constructs used in the HUI2 Multi-Attribute System (aside from
fertility) (Torrance et al., 1996)
Attribute name # of Levels Construct
Sensation 4 See, hear and speak
Mobility 5 Walk, bend, lift, jump, and run
Emotion 5 Amount of worry
Cognition 4 Learning and remembering school work
Self-Care 4 Eat, bath, dress, and use the toilet.
Pain 5 Intervention for pain
Table 4. Summary of constructs used in the HUI3 Multi-Attribute System
(Feeny et al., 1995)
Attribute name # of Levels Construct
Vision 6 Read newsprint and recognize friend across street
Hearing 6 Hear conversation in group setting
Speech 5 Being able to be verbally understood
Ambulation 6 Walking
Dexterity 6 Use of hands and fingers
Emotion 5 Happiness
Cognition 6 Memory, ability to solve problems
Pain 5 Limitation of activity

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
39
Both HUI2 and HUI3 require the respondent to affirmatively identify
experiencing pain. However, each system measures pain in a different manner. The HUI2
construct for pain is based on the type of intervention, ranging from occasional pain
requiring limited non-prescription drugs or self-control of activities with no impact on
normal activities (level 2), to severe pain, not relieved with medications and disrupting
normal activities (level 5) (Torrance et al, 1996). The HUI3 pain construct is based on
activity limitation. Individuals with mild to moderate pain that does not limit activities are
considered a level 2, while participants with severe pain that limits most activities are
considered a level 5 (Feeny et al., 1995).The individual responses to each of the pain-
related questions provided further insight into pain experienced by individuals in this
cohort, in addition to the generation of attribute levels and utility scores.
In addition to the HUI questions, it was recognized that further exploration of pain
should also be undertaken to include identification of the location and intensity, as
assigned directly by the participant. As such, a simplified human figure (homunculus), as
show in Figure 2, was used for participants to identify the location of the pain. Further
exploration was undertaken using a coloured analogue scale (CAS) on which individuals
indicated the intensity of pain by the brightness of the colour red, which was then mapped
to a number on a scale of 0 (no pain) to 10 (worst pain ever experienced). This has been
used previously in participants with pain, and provides a direct quantitative value on a
subjective attribute (McGrath, 1996).

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
40
Figure 2. A simplified human figure used to elucidate location of pain experienced
by participant.
One consideration regarding the HUI instruments is that these are restricted to
health-related capabilities only. Consequently, sociodemographic details were gathered to
provide a more complete understanding of this patient cohort. Questions were developed
by review of articles, as well as by consultation with an expert in the area (Hoven,
Lannering, Gustafsson & Boman, 2010, Zeltzer et al., 2008, S. Saigal (personal
communication, April 7, 2011)).
Cantril’s ladder is a measure of overall well-being, asking individuals to place
their present, past and future QOL, defined as life satisfaction, on a ladder with ten steps,
with the lowest rung representing the worst QOL (1) to the top rung (10) the best QOL
(Cantril, 1965). This self-anchoring tool has been used previously to estimate the
psychological well-being of survivors of childhood cancers, including those with brain
tumours (Zeltzer et al, 2009). Cantril’s Ladder was used in this study, with participants

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
41
being asked to rate their QOL on a scale of 1 to 10 at present, then reflecting on five years
ago, and then imagining it five years into the future. This provided a measure of
satisfaction with life in general at present, as well as providing insight into whether
participants felt life improved over time.
Proxy Reporting
Proxy reporting is used commonly in HUI2/3 measurements of HRQL, with the
parent or health-care provider as the alternative to self-reporting (Fluchel et al., 2008. Fu
et al., 2006). In this cross-sectional study (T3), subjects were asked to select an individual
who they felt knew them best. Given the age range of participants, it was felt more
appropriate to allow the subjects to select a proxy of their choosing as a parent responder
may not be able to provide information if the participant no longer lived at home. The use
of a subject-selected proxy in this study was exploratory in nature.
Longitudinal Study Design
Similar cross-sectional studies were undertaken in 2000/2001 and 2005/2006 for
this same cohort, using the eligibility criteria outlined previously. The availability of
HUI2/3 scores at these two previous time points provided the unique opportunity for the
exploration of the stability of pain over a decade using a linear mixed effects model for
longitudinal analysis. A repeated measures analysis is particularly attractive as it allows
for assessment of change over time at an individual and at a group level, while controlling
for within-subject correlations. This decreases the chance of committing a Type I error.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
42
Missing data are a concern for studies, particularly when a group of individuals is
followed over a length of time, as the exclusion of participants without data results in
reduction of sample size, and consequently power (Altman & Bland, 2007). This would
result in the increase chance of committing a Type II error. Imputation is an accepted
technique often used for missing survey data, and allows analysis of an entire set of data
(Stern et al., 2009). In order to decrease the potential for bias and to maximize the data
collected, scores were imputed for missing data of participants who responded “don’t
know” at any of the three time points, or had missing data due to non-participation for
reasons other than death, beyond time point 1. The increased degree of uncertainty of the
imputed values was accounted for by the generation of five sets of imputed data, which
were pooled along with the initial data set at the time of analysis. Linear mixed effects
models are able to handle imputed data sets.
Protocol
Procedures
Upon approval from the Research Ethics Board at Hamilton Health
Sciences/Faculty of Health Sciences, study procedures commenced. A summary of the
study procedures are depicted in Figure 3.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
43
Figure 3. Summary of cross-sectional study procedures.
Subject Screening
Initial screening of potential subjects was undertaken by the neuro-oncology nurse
(JD). Patient lists were reviewed to identify patients who were diagnosed with a primary
brain tumour at MCH between January 1985 and December 1998. Individuals with
disease that had relapsed or progressed were still eligible for participation, provided that
they were free of disease at the time of the study. In addition, eligible subjects must have
participated in previous HRQL studies that were undertaken at time points 1 (2000/2001)
and 2 (2005/2006) in order to have complete data sets.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
44
Subject and Proxy Recruitment
Subjects who met the inclusion criteria were then contacted by JD for a brief
introduction to the study. Interested individuals were given the option of meeting in-
person or having a follow-up phone call with a study team member for study consent and
questionnaire administration. Participants were also asked by the nurse if they would be
comfortable having someone respond about their health (proxy point of view), and if
acceptable, to identify an individual who “knew them well” who would be willing to
respond to the proxy questionnaire.
Consent Process
Follow-up phone calls, as well as in-hospital and community interviews, were
undertaken by a trained member of the research team. Consent was obtained through
review of the study question, as well as the procedures, potential risks, benefits and
voluntariness of participation. A written consent form was presented to the participant
and proxy if the meeting occurred in person, or mailed ahead of time to the participant for
consents that were obtained over the phone. All questions posed by the subject or proxy
were answered. Once all questions had been addressed and the individual affirmed
willingness to participate, consent was obtained in writing.
Administration of Questionnaires
Interviews were undertaken separately for subjects and proxies, with the person
not being interviewed being asked to relocate physically outside of hearing range. In
order to ensure a standardized approach, the instructions as well as the questions listed on

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
45
the questionnaire were read verbatim to the participant. Minimal additional instructions or
prompting were provided, with clarification being given only as requested by the
participant. Attempts were made to have the participant complete the questionnaire in its
entirety.
Participants reporting “yes” to pain were asked to complete two additional tasks:
(i) a homunculus (Figure 2) was used to identify locations of pain throughout the body,
with (ii) the intensity of pain experienced at each location indicated on a CAS.
Upon completion of the HUI2/3, participants were asked a set of
sociodemographic questions regarding educational level, living situation, relationship
status, children, employment and possession of a valid driver’s licence. All participants
were then asked to evaluate their life on a scale of 1 to 10 (10 being the “best”), at
present, as they remembered it five years ago, and how they felt it would be five years
ahead.
HUI2/3 interviews were then undertaken with the proxy, with the participant
asked to move out of the vicinity in which the interview was occurring.
Procedures were identical for subjects undertaking the questionnaire in person or
over the phone. However, in the latter circumstance, the consent form, copies of the CAS
with the participants instructed to draw a line indicating discomfort, and the homunculus
were completed by the participant at home and then returned to the study centre by mail
using a stamped, pre-addressed envelope. All participants were given or mailed copies of
the signed consent forms.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
46
Non-Participants
Patients who declined participation were not asked for proxy interviews, nor was
any further communication attempted for study purposes. Reasons for non-participation
were recorded if provided. Multiple attempts were made to contact all eligible subjects.
However, some participants were not contactable. Survival status for non-contactable
individuals was attempted through the Cancer Care Ontario registry, via POGO.
Data Linkage
The above procedures of screening and administration of the HUI2/3
questionnaire were undertaken at two previous time points: the first in 2000/2001, and
then again in 2005/2006. Unique patient identifiers allowed for data linkage and
facilitated a longitudinal analysis of this cohort of survivors of brain tumours in childhood
over a ten-year period. Given the length of time between surveys, separate Research
Ethics Board approvals as well as participant consents were obtained at each time point
with an indication made that data linkage would occur.
Demographic and Clinical Information
Demographic and clinical data, which included the age at diagnosis of the primary
tumour and the age at the time of interview; primary brain tumour subtype, location of
tumour, extent of surgery, nature of treatment; and relapse and progression, were
collected for all eligible subjects by JD. Data for consenting participants were provided
for analysis with study identifiers, while data for non-participants were provided without
any identifiers to enable comparison of the two groups.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
47
Data Management
Data was transcribed directly from the questionnaires onto spreadsheets on Excel
(v. 2010) by two investigators. Random checks were undertaken to confirm correct data
transcription. To ensure confidentiality, only non-identifying data were entered onto
spreadsheets. All analysis was undertaken using SPSS version 20.
Scoring of HUI Questionnaire.
The responses to each question were entered onto a database in Excel, then coded
and converted into SPSS. Using syntax provided by HUInc, single attribute utility scores
and multi-attribute utility scores were generated for HUI 2 and HUI3 systems. A second
database was created that included subject ID, as well as demographic, clinical,
sociodemographic, QOL and HRQL data. This dataset was used for analysis.
Analysis
Cross-Sectional Analysis
All data collected within this study were assumed to have a normal distribution
and were independent, unless stated otherwise. Descriptive statistics included measures of
central tendency and dispersion (mean and standard deviation for continuous variables;
frequency, median, mode and range for categorical variables). Comparisons between
groups for continuous variables were undertaken using parametric tests. Two-tailed
paired or independent t-tests were used to determine the mean difference. Levine’s Test
for Equality of Variances was used to test for homogeneity of variance. If the value was
significant (p < 0.05) an unequal variance t-test was used. If the value was not significant
M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
48
Student’s t-test was used (Ruxton, 2006). Non-parametric tests, including Chi-square,
Fisher’s exact test and odds ratios, were used to compare categorical data (Norman &
Streiner, 2007). A p-value of less than 0.05 was taken to indicate a statistically significant
difference for all tests, and resulted in the rejection of the null hypothesis (no difference
between groups). No adjustments were made for multiple testing as this is an exploratory
study.
Description of Overall Cohort
Demographic, sociodemographic and clinical characteristics of the participants at
the third time point were reviewed using descriptive statistics. Comparisons of
demographics of participants and non-participants were undertaken to explore potential
systematic differences between the two groups. Clinical data of participants were also
appraised critically for representativeness by reviewing published data on survivors of
brain tumours in childhood. Sociodemographic data were presented using descriptive
statistics and provided a comprehensive life status assessment of this cohort.
General Quality of Life Rating
Participants rated their general QOL subjectively for the present, 5 years prior
(past), and 5 years imagined into the future using Cantril’s Ladder. A one-way repeated
measures analysis of variance (ANOVA) was used to evaluate the perceived change in
QOL over time. This statistical method is superior to multiple paired t-tests as it allows
for the comparison of multiple groups, while accounting for within-subject correlation.
This decreases the chance of committing a Type I error. Listwise deletion occurred, with

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
49
participants with incomplete data excluded from the statistical analysis exercise.
Mauchly’s test of sphericity was reviewed, and the appropriate correction was applied, as
required. Pairwise comparison allowed for interrogation of change in QOL between time
points.
Health-Related Quality of Life
Results were generated using algorithms provided by HUInc and analyzed
independently for HUI2 and HUI3 systems. Overall multi-attribute scores (continuous
variable) were reviewed using descriptive statistics. Single attribute level scores were
categorized by disability using the HUI2 and HUI3 classification systems, using scheme
A (Furlong et al., 1998). The ordinal, single attribute level data were reviewed as
frequency and mode, and illustrated using a histogram. Attributes in which greater than
fifty percent of participants reported “mild” or worse difficulties were identified as areas
with a ‘high’ prevalence of morbidity.
Proxy Reporting
Responses from proxy respondents were evaluated for agreement (inter-rater
concordance). Single attribute level data were reviewed for percent exact agreement
based on four levels of disability: none, mild, moderate, severe, which have been
established previously (Feng, Bernier, McIntosh & Orpana, 2009). A two-way mixed
effects model, patient-random, instrument-fixed, intra-class correlation coefficient (ICC)
was used to analyse concordance for single- and multi-attribute utility scores. This
method of analysis is appropriate for continuous variables, and is an accepted measure of

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
50
inter-rater reliability. The resultant score is interpreted based on anchoring of 0 (no
agreement) and 1.0 (perfect agreement) and using the reference criteria outlined by
Altman (1991). Concordance was measured by ICC given the small sample size and the
potential for poor distribution across all cells of the contingency table.
Description of Participants Reporting Pain
Clinical and demographic details of the sub-group reporting pain were reviewed
using descriptive statistics. Formal statistical comparison of the characteristics between
the pain and no-pain groups was not undertaken due to the small sample size and,
consequently, lack of power to evaluate statistical significance.
The individual responses to pain-related questions on the HUI2/3 questionnaire, as
well as the location (homunculus) and intensity (CAS), were reviewed in order to
appreciate the burden of pain experienced by this cohort. Exploration of the possible
correlation between the maximum intensity of pain measured by the CAS and the single-
attribute HUI2 and HUI3 pain scores was undertaken using non-parametric correlation
tests. The CAS was multiplied by a factor of (-1) to allow for higher values to indicate
better health, in keeping with the HUI scores.
Burden of Pain by HRQL
Single-attribute utility scores for participants reporting pain and those reporting no
pain were compared for clinically significant differences using the pre-established criteria
of greater than 0.05 (Horsman et al., 2003). The mean scores of the two groups were also
analyzed for statistical significance using Student’s t-test. However, due to the small

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
51
sample size, results were interpreted with caution given that the result could be minimized
erroneously or over inflated.
The multi-attribute utility scores were described in relation to the results of the
single attribute scores. However, results were not compared directly between the pain and
no-pain groups due to the contribution of pain to the overall HRQL score.
Longitudinal Analysis
Longitudinal analysis occurred through data linkage by participant study
identifiers. The results from this cross-sectional study were combined with a database
containing scores of HRQL for cross-sectional studies undertaken 5 and 10 years prior
(Barr, 2006). The clinical and demographic data of the original cohort were reviewed and
described. The mean utility scores for each time point were used to generate a line graph,
and allowed for exploration of potential trends over time.
A linear mixed effects model was selected to analyse the change in the burden of
pain over time. This method is used commonly for correlated data, such as repeated
measures of survey respondents, as it allows for comparison of the means between groups
while decreasing the possibility of committing a type 1 error. A linear mixed effects
model describes a relationship between a response variable and covariates, using the
equation: Y=Xβ+ u +e, where Y, β, u and e are vectors, and X represents a design matrix.
In this study, the response or dependent variable was pain (Y) and the single fixed effect
was time (β), where X was a matrix relating the observations of pain to time, with the
addition of random effect capturing within-individual correlation (u) and residual error (ε)

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
52
(SPSS, 2005). This analysis was executed with the assumption that variances were
constant over the study period, and that there was normal distribution of the residuals and
random effects. This statistical method compares the mean utility score between the
baseline survey time point and subsequent survey time points (2000/2001 and 2005/2006
study), and provided information about the change of pain over time in this cohort.
A repeated measures ANOVA is also able to describe trends over a period of time.
However, this type of statistical method requires balanced, complete datasets for each
case. This requirement results in excluding cases with incomplete data, and has
implications for a potentially biased result if the remaining cases were not representative
of the entire population.
A linear mixed effects model is superior to a repeated measures ANOVA as it is
able to handle unbalanced data. However, the problem of missing data due to non-
participation and “don’t know” would also lead to a loss of power. As such, multiple
imputation using the fully conditional specification method with predictive mean
matching was undertaken for subjects in whom data were missing due to non-
participation at time point 2 or 3, or who responded “don’t know” at any time point.
(Rubin, 1987). Missing data was imputed five times using SPSS version 20, using
automatic method, with no defined constraints. The 5 complete data sets were pooled
along with the original data set for analysis to decrease the degree of uncertainty. All
assumptions were met for using imputation, namely that the data were missing at random,
it was appropriate to impute the data (excluding participants who died during the study

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
53
period), and imputation had been used previously for HUI data (Statistics Canada, 2007).
Imputation was undertaken at the utility score level, rather than at the question response
level due to the large number of variables (i.e. 41 questions x 3 time points). Linear
mixed effects models are able to handle imputed data.
The change in pain scores over time at a cohort level was evaluated for statistical
and clinical significance based on the results of the linear mixed effects modelling. The F-
values presented in the “Type III Tests of Fixed Effects” for the original and individual
imputed datasets were reviewed for statistical significance with respect to time. This
acted as an indicator of statistically significant changes of pain over the study period. If
indicated, further investigation was undertaken for pairwise comparisons of statistical
significance. The regression coefficients were examined also for estimates of clinically
significant differences, which was possible as this model only regressed onto one factor
(time).
For pairwise comparison, the linear mixed effects model was run twice, once with
T3 as the reference time point, to provide estimated differences for T1 to T3 (10 years)
and T2 to T3 (5 years). The second pairwise analysis used T1 as the reference, which
provided the estimated difference from T1 to T2 (5 years).
The persistence of pain at an individual level over the 10-year span of the study
was also of interest. The covariate matrix generated for the linear mixed effects model
allowed for the generation of ICCs by dividing the variance of the random effects by the

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
54
sum of the variance of the random effect and the variance of the residual. This provided
the degree of within-individual correlation of pain measured over the span of the study.
The above analysis was also undertaken for the multi-attribute utility scores as a
study of the change in overall HRQL over time in survivors of brain tumours in
childhood.
Ethical Considerations
Research Ethics Board Approval
Prior to the commencement of any study procedures, application was made to the
Hamilton Health Sciences/Faculty of Health Sciences Student Research Ethics Board
(REB). Submitted documents included the REB application, a copy of the protocol, which
outlined the study rationale, objectives and procedures, as well as consent forms for
subject and proxy respondents. Risks and benefits to subjects as well as society were
outlined in the application as well as the consent forms. The approved protocol was used
to guide study procedures, and any changes were approved formally by the REB prior to
implementation.
Study Risks, Identification and Management
The study was considered to be of minimal risk. Although the HUI2/3
questionnaire was designed carefully and used in the general population as well as with
patients having various diseases and conditions, it is possible that the questions could
make the participants feel vulnerable or emotional. Interviewers were trained to present
all questions and response choices as written using a neutral tone. Participants were

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
55
informed prior to the interview that if they felt upset or uncomfortable answering any of
the questions, the item could be skipped, or the interview could be discontinued. In
addition, participants were encouraged to contact the clinical team if they felt upset by the
questionnaire, or were concerned about their health. Reassurance was also provided that
the information from the research would not be referenced back to the individual
participant, nor would the information become a part of the participant’s medical record
or made available to the treating team.
Participants were also requested to identify a proxy to respond to the questionnaire
about the subject’s health. This was presented as optional to the subject to prevent placing
either the subject or proxy into an uncomfortable setting. In addition, participants
undertook the questionnaire first and were authorized to indicate if any questions should
be skipped by the proxy. Finally, responses from subjects and proxies were not made
available to either party.
Study Benefits
This study was judged to present minimal benefit to the individual participant.
However, it was extremely valuable in understanding and appreciating the health status of
long-term survivors of brain tumours in childhood. To the best of our knowledge, this
study was the first to measure HRQL in a cohort of brain tumour survivors over a ten-
year period, and was expected to provide important information to the clinical community
caring for patients with this type of cancer. In addition, this information is believed to be

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
56
relevant to counselling families with children diagnosed with brain tumours in regard to
their potential HRQL in the future, and understanding their child’s long-term needs.
Confidentiality
Efforts were made throughout the study to respect the confidentiality of study
subjects. JD was responsible for screening potential subjects as well as for the initial
contact to ascertain interest for participation. The names and contact information of
subjects expressing interest in the study were forwarded to the study team to arrange for
full consent and questionnaire administration. No additional attempts were made by team
members to contact subjects who had declined participation or were lost to follow-up.
Unique subject identifiers were used to identify the questionnaires, and were also used on
the study database; no names were captured.
Clinical and demographic data for the entire cohort were also abstracted by JD
from the medical charts and were entered into a database by study identifier only.
Minimal disease and demographic information was obtained for non-participants in order
to assess for systematic differences between the participants and those who did not
participate. Data presented for non-participants did not containing any identifying
information. The Pediatric Oncology Group of Ontario was queried for the status of
survivorship using POGO identifiers.
Consent forms, which contain the subjects’ names, were kept in a separate
location from the questionnaires. All hard-copies of patient-level data were kept securely

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
57
in a locked office at MCH, and databases with identifying information were kept on
secure, password-protected servers, and accessed through password-protected computers.
Consent
Consent forms were written in keeping with Good Clinical Practice, Tri-Council
Policy Statement, and REB requirements. The consent forms were amended as required to
reflect changes to the protocol, and approved by the REB prior to use. Separate consent
forms were created for subjects and for proxies.
Subjects were contacted initially by JD and provided a brief overview of the
study. All individuals expressing interest in the study were given the option to meet in
person or to have a consent form mailed to their home with a follow-up phone call by a
study team member. Prior to initiation of the interview, a study team member reviewed
the consent form with the subject and proxy and addressed any questions raised. The
consent form was signed by the subject or proxy respondent as well as by the study team
member. The original copy of the consent form was kept in a locked research office in a
file kept separate from the patient data, and a copy was given to the family immediately
or mailed back to the participant with a thank-you letter. Participants were encouraged to
contact the Principal Investigator, JD or the REB if they had any additional questions at
any point in time.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
58
RESULTS
Cross-Sectional Study- Time Point 3 (2011 and 2012)
Overall Cohort
Description of Participants
Recruitment to this study occurred between February 1, 2011 and March 31, 2012.
Of the 37 subjects identified as eligible for participation, 25 (67.6%) consented and
completed study requirements successfully. Reasons for non-participation included:
subject not interested in participating in the study and declined at time of contact by
neuro-oncology nurse (n=3), subject indicated interest in participation but could not be
contacted for subsequent interview (n=3), and subject lost to follow-up (n=6). Cancer
Care Ontario was queried through POGO for survival status of the participants classified
as lost to follow-up; no subjects were registered as having died in Ontario.
Twelve males and 13 females participated in the study. The mean age of the
cohort was 28 years (standard deviation (SD) of 4.1) at the time of the interview. Subjects
were between 13.2 years and 27.5 years from initial diagnosis (mean of 19.7, SD of 4.31).
Table 5 depicts the type of disease, initial clinical features, treatment and survival
status for this group. None of the participants were being treated actively for their brain
tumour at the time of the interview, although ten participants (40%) were noted to have
experienced a recurrence of the original tumour or a second malignancy.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
59
Table 5. Clinical features of subjects eligible to participate in study at time point 3(n=37)
Characteristic
Participants
(n=25)
Non-Participants
(n=12)
Brain tumour subtype
Astroglial tumour 16 (64%) 10 (83%)
PNET/Medulloblastoma 6 (24%) 0 (0%)
Ependymoma 1 (4%) 0 (0%)
Other 2 (8%) 2 (17%)
Site of primary tumour
Infratentorial- posterior fossa/cerebellum 13 (52%) 6 (50%)
Infratentorial- brain stem 2 (8%) 0 (0%)
Supratentorial-hemisphere/basal ganglia 5 (20%) 3 (25%)
Supratentorial- optic pathway 4 (16%) 0 (0%)
Other 1 (4%) 3 (25%)
Extent of resection
No surgery 1 (4%) 0(0%)
Biopsy only 2 (8%) 1 (8%)
Single resection 21 (84%) 11 (92%)
Multiple resections 1 (4%) 0 (0%)
Intervention
Observation only 1 (4%) 1 (8%)
Surgery only 6 (24%) 7 (58%)
Chemotherapy and/or radiation 18 (72%) 4 (33%)
Shunt (Yes) 5 (20%) 1 (8%)
Disease outcome*
Disease-Free/Stable-Disease Survival
Recurrence of any CNS Tumour
Progressive Disease
Non-CNS Second Malignancy
*At time of last contact, based on initial
tumour
15 (60%)
3 (12%)
3 (12%)
4 (16%)
10 (83%)
2 (17%)
0 (0%)
0 (0%)
Comparison of participant and non-participant groups revealed as few differences,
however these were not considered to be substantive; formal statistical comparison for
type of cancer and treatment received was not undertaken due to the small sample size.
Individuals diagnosed with PNET/medulloblastoma or ependymoma were represented
only in the participant group. Participants were also noted to have primary brain tumours

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
60
in numerous infratentorial and supratentorial sites, while non-participants did not have
primary tumours in the infratentorial-brain stem or supratentorial-optic pathway. There
was also a higher proportion of individuals who participated in the study who received
chemotherapy and/or radiation.
Interviews for consenting subjects occurred at MCH (n=15), in the community
(n=4) or by phone (n=6). All participants voiced an understanding of the tasks and were
able to undertake the interview-administered questionnaires. Two participants reported
visual impairment. For these participants the location of pain was determined on the basis
of description of the area on their body. One participant had difficulty with speaking but
was able to provide responses to questions through a sibling. Answers were confirmed
with the participant directly prior to being recorded. Another member of the family
provided the proxy-reporting.
Twenty-three participants identified proxies to answer the HUI questionnaire
designed for proxy-reporting of HRQL. The proxy’s relationship to the participant
included parent (n= 13), partner (n=9) and friend (n=1). Two proxies were not reachable
by phone despite multiple attempts.
Sociodemographic Factors and General Quality of Life
Review of the self-reported sociodemographic features of the sample revealed that ten
participants (40%) lived with a partner, thirteen (52%) lived with their parents and two
(8%) lived with others or alone. Three (12%) of the individuals not living with partners
reported being in a relationship.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
61
The majority of patients had completed at least a high school level of education,
as depicted in Figure 44. Eighteen (72%) of the 25 participants reported being employed
or currently in school, 5 (25%) were unemployed, and 2 (8%) were on sick leave or
disability. Slightly less than half (11 out of 25) reported having a driver’s licence.
When asked about overall general QOL on a scale of 1 to 10, with 10 being the
highest, participants reported scores ranging from 6 to 10 (mean of 8.46) at the time of the
interview. Two participants felt they could not predict how their life would be in five
years, and were excluded from further analysis. Figure 55 depicts the conjectured QOL at
five years prior, at the present time, and five years into the future; it can be seen that
participants had an overall favourable view of their future QOL.
Figure 4. Highest education level achieved as reported by participants (n=25).

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
62
Review of the ANOVA output to address the question of perceived QOL over
time revealed that Mauchly’s Test of Sphericity was significant (p<0.001), and as such,
Greenhouse-Geisser correction was applied. The resultant F-ratio of 59.78 was noted to
be significant (p=0.001), indicating that participants reported a difference in their QOL
over time. Pairwise comparisons of the time points revealed an anticipated improvement
in QOL to occur between the present and future (mean increase of 2.46, p=0.001). The
difference in the mean scores reported for the past to present (increase of 1.69) was not
significant.
Figure 5. Mean overall quality of life as reported subjectively by participants as
remembered at times 5 years in the past, the present and predicted 5 years in
the future.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
63
Health-Related Quality of Life
Overall utility scores were calculated for 24 of the 25 participants as one
individual reported “don’t know” for the HUI2 question relating to sensation, and the
HUI3 question relating to emotion. A burden of morbidity was prevalent in the cohort as
the mean multi-attribute utility score for HUI2 was 0.79 (SD of 0.23), median of 0.88
(minimum of 0.16 to maximum of 1.00 ), and for HUI3 was 0.69 (SD 0.29), median of
0.77 ( minimum of -0.19 to maximum 1.00). Overall utility scores can be seen in Figure
6. Nineteen of the 25 participants directly self-reported overall HRQL as “very good” or
“excellent” (Table 6).
Table 6. Self- and proxy- responses to direct reporting of overall HRQL
Response Subject (n=25) Proxy (n=22)
Excellent 10 (40%) 8 (36%)
Very good 9 (36%) 10 (45%)
Good 5 (20%) 3 (14%)
Fair 1 (4%) 1 (5%)
Poor 0 (0%) 0 (0%)
Figure 6. Boxplot of median utility scores for cohort (n=24).

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
64
Review of the single attribute level data (Figure 77) revealed that greater than
50% of the cohort indicated at least a mild burden of morbidity in the attributes of
cognition (60%0 and pain (52%) in both HUI2 and HUI3. Sensation difficulties were
noted in slightly less than half of the individuals (46%) as well as emotion (40%) as
measured by HUI2. The greatest variation in disability was reported in the attributes of
emotion and pain (HUI2) and cognition (HUI3) by single attribute utility scores. As a
group the highest burdens of morbidity were in attributes of mobility, emotion and pain
(HUI2), and dexterity, cognition and pain (HUI3). The results observed support
Hypothesis #3, which stated that in addition to pain, other areas of morbidity would be
identified, including attributes of emotion and cognition.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
65
*1 participant responded “Don’t know” therefore not included
Figure 7. Single attribute level data for HUI2 (2a) and HUI3 (2b) for overall cohort (n=25).
2a)
2b)

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
66
Twenty-three proxies responded to questions regarding the HRQL of long term
survivors. Four individuals were unable to answer at least one question despite being
encouraged to provide an answer. The mean multi-attribute utility score based on 19
proxies was 0.83 (range of 0.37 to 1.00) for HUI2, and 0.67 (range of 0.02 to 1.00) for
HUI3. Proxies were also asked to reflect on the overall HRQL of the subject. Eighteen
(81%) of the 22 proxies who responded perceived the subject’s HRQL to be “very good”
or “excellent” (Table 6).
Comparison of the overall utility score between self and proxy reported HRQL
was noted to be clinically significantly different for HUI2 (0.79 versus 0.83), but not for
HUI2 (0.69 versus 0.67).Evaluation of agreement between subject and proxy multi-
attribute utility scores was calculated for the 18 pairs who had complete data. The ICC for
the multi-attribute score for HUI2 was 0.745 (95% CI of 0.438 and 0.896), and 0.929
(95% CI of 0.822 to 0.973) for HUI3.
Percent exact agreement for single attribute scores was determined based on four
levels of disability: none, mild, moderate, severe, as defined by Health Utilities Index
Procedures Manual. Calculation of ICCs for single-attribute utility scores was also
undertaken to determine correlation of the self and proxy responses (Table 7 and Table
8) (Furlong et al. 1998). In both HUI2 and HUI3 there was poor agreement (ICC<0.5, and
low % exact agreement) for the attributes of emotion and pain. Cognition was also
identified to have poor concordance for HUI2 and HUI3 by exact agreement (65% and
48% respectively). This was also reflected in the ICC, where it was correlation for

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
67
cognition was calculated to be 0.28 for HUI2, however, was within an acceptable range
(0.75) for HUI3. Very good to perfect agreement by ICC was seen in the attributes of
self-care (HUI2), and hearing, speech, dexterity and ambulation (HUI3).
Table 7. Measurement of concordance between self- and proxy- ratings for HUI2
attributes
Attribute
Exact
agreement
4 levels
% Exact
Agreement
4 levels
ICC Utility scores
(95% CI lower, upper)
Sensation 17/20 85 0.828 (0.828, 0.971)
Mobility 18/23 78 0.743 (0.484, 0.882)
Emotion 10/19 53 ** (**, 0.423)
Cognition 15/23 65 0.280 (**, 0.615)
Self-Care 23/23 100 1.0 (1.0, 1.0)
Pain 11/22 50 0.444 (0.037, 0.724)
**Minimal correlation, undefined (King’s College London, 2013)
Table 8. Measurement of concordance between self- and proxy- ratings for HUI3
attributes.
Attribute
Exact
agreement
4 levels
% Exact
Agreement
4 levels
ICC Utility scores
(95% CI lower, upper)
Vision (n=23) 17/23 74 0.946 (0.877, 0.977)
Hearing (n=20) 20/20 100 1.0 (1.0, 1.0)
Speech (n=23) 22/23 96 0.955 (0.897, 0.981)
Ambulation (n=23) 22/23 96 0.869 (0.716, 0.942)
Dexterity (n=23) 21/23 91 0.869 (0.717, 0.942)
Emotion (n=20) 15/20 75 0.418 (** 0.720)
Cognition (n=23) 11/23 48 0.751 (0.498, 0.886)
Pain (n=22) 10/22 45 0.286 (**, 0.625)
**Minimal correlation, undefined (King’s College London, 2013)

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
68
Participants Reporting Pain
Description of Participants with Pain
Fifty-two percent (n=13) of participants reported experiencing pain or discomfort
at least once in the week prior to the interview, with most experiencing pain on less than
half of the days (Table 9). This finding supports Hypothesis #1 as the number of long-
term survivors reporting pain was greater than 35%.
Table 9. Number of days participants reported experiencing pain in week prior to
interview
# Days with Pain Frequency Cumulative Percent
7 Days 2 8%
6 Days 0 8%
5 Days 1 12%
4 Days 1 16%
3 Days 3 28%
2 Days 4 44%
1 Day 2 52%
0 Days 12
Clinical features and treatment of the primary brain tumour of participants with
and without pain are summarized in Table 10. Demographics of participants with pain
were found to be similar to those participants without pain with respect to age at
diagnosis (7.65 years versus 8.81 years) and age at time of interview (27.1 years versus
28.8 years). Nine males and 4 females reported pain. Survivors with pain were also
similar to their counterparts without pain with respect to life achievements (results not
shown), and a reported similar overall QOL (mean of 8.3 for the group with pain versus
8.6 for participants without pain). Formal statistical analysis was not undertaken due to
the small sample size.
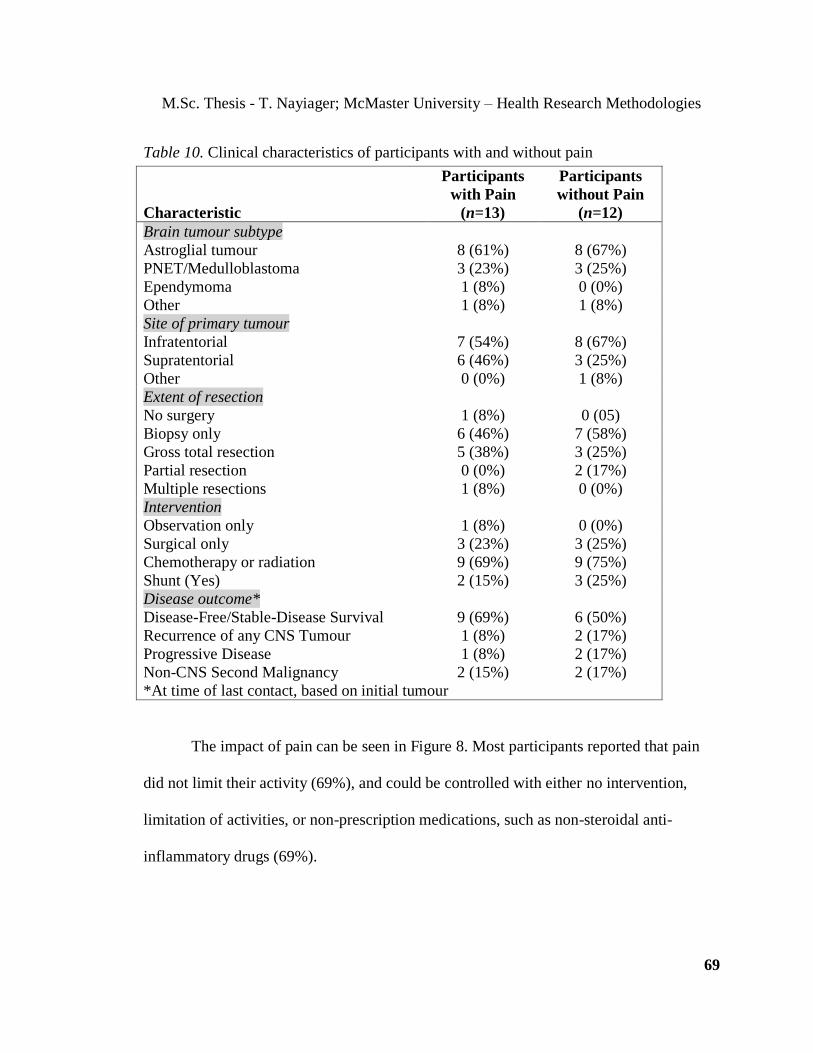
M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
69
Table 10. Clinical characteristics of participants with and without pain
Characteristic
Participants
with Pain
(n=13)
Participants
without Pain
(n=12)
Brain tumour subtype
Astroglial tumour 8 (61%) 8 (67%)
PNET/Medulloblastoma 3 (23%) 3 (25%)
Ependymoma 1 (8%) 0 (0%)
Other 1 (8%) 1 (8%)
Site of primary tumour
Infratentorial 7 (54%) 8 (67%)
Supratentorial 6 (46%) 3 (25%)
Other 0 (0%) 1 (8%)
Extent of resection
No surgery 1 (8%) 0 (05)
Biopsy only 6 (46%) 7 (58%)
Gross total resection 5 (38%) 3 (25%)
Partial resection 0 (0%) 2 (17%)
Multiple resections 1 (8%) 0 (0%)
Intervention
Observation only 1 (8%) 0 (0%)
Surgical only 3 (23%) 3 (25%)
Chemotherapy or radiation 9 (69%) 9 (75%)
Shunt (Yes) 2 (15%) 3 (25%)
Disease outcome*
Disease-Free/Stable-Disease Survival
Recurrence of any CNS Tumour
Progressive Disease
Non-CNS Second Malignancy
9 (69%)
1 (8%)
1 (8%)
2 (15%)
6 (50%)
2 (17%)
2 (17%)
2 (17%)
*At time of last contact, based on initial tumour
The impact of pain can be seen in Figure 8. Most participants reported that pain
did not limit their activity (69%), and could be controlled with either no intervention,
limitation of activities, or non-prescription medications, such as non-steroidal anti-
inflammatory drugs (69%).

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
70
Figure 8. Impact of pain (n=13) as measured by a) Number of activities limited by pain,
and b) Interventions for relief of most severe pain in a 1 week period, for
participants reporting pain within the week prior to the interview.
This cohort of long-term survivors reported varied locations of pain, throughout
the body and not solely restricted to the head, as can be seen in Table 11. Most common
areas of pain were lower extremities (n=12), head (n=6) and back (n=5). Lower
extremities and the back were also associated with the most extreme pain scores of 10.0
and 9.0 respectively, as measured by the CAS. Other areas of notable pain included
upper extremity (max 8.0) and abdomen (max 8.0). The pain intensity experienced in the
a)
b)

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
71
head was noted at a minimum of 3.4, and maximum of 6.8. Exploration of possible
correlation between maximum pain intensity for each participant as measured by the
coloured analogue scale and the single-attribute HUI2 and HUI3 pain scores using
Pearson’s correlation coefficient was 0.38 and 0.45, respectively.
Table 11. Reported location of pain as noted using homunculus and corresponding
intensity measured using coloured analogue scale ratings
Location
Frequency
reported
Median Pain
Intensity
Maximum Pain
Intensity
Head 6 3.4 6.8
Eyes 1 6.0 6.0
Back 5 3.5 9.0
Upper Extremity 4 2.8 8.0
Abdomen 2 6.3 8.0
Lower Extremity 12 4.4 10
Proxy-Reporting for Participants with Pain
There was fair concordance of self- and proxy-ratings of pain when measured by
activity limitation (HUI3, ICC of 0.286) and moderate concordance between self- and
proxy- ratings as measured by interventions to alleviate symptoms (HUI2, ICC of 0.444).
In keeping with hypothesis #2 the agreement between self- and proxy- reporting of the
severity of pain as measured by HUI3 was less than 0.4. However, agreement of severity
of pain by symptom relief (HUI2) was greater than 0.4, and therefore did not support
Hypothesis #2.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
72
Exact agreement by levels of severity of pain, as assigned by the 22 patient-proxy
pairs, was minimal. Review of the responses revealed that 50% of pairs reported the same
type of intervention to alleviate pain symptoms (Table12) and 45% had exact
concordance for the amount of activity limited by pain (Table13). Proxies more under-
reported the severity of pain experienced by the subject.
Table12. Concordance between self- and proxy-reporting for pain as measured by
interventions to alleviate symptoms (HUI2)
Proxy
None Mild Moderate Severe Total
Self
None 9 1 0 0 10
Mild 4 1 3 0 8
Moderate 0 1 1 0 2
Severe 0 0 2 0 2
Total 13 3 6 0 22
Table13. Concordance between self- and proxy-reporting for pain as measured by number
of activities limited by pain (HUI3)
Proxy
None Mild Moderate Severe Total
Self
None 9 1 0 0 10
Mild 4 1 1 2 8
Moderate 0 0 0 0 0
Severe 0 1 3 0 4
Total 13 3 4 2 22
Health-Related Quality of Life of Participants with Pain
As anticipated the multi-attribute utility scores of participants with pain
demonstrated lower overall HRQL than did scores in participants without pain for both
HUI2 (0.66 versus 0.94, significance of 0.001) and HUI3 (0.53 versus 0.88, significance
of 0.002). Although these values were noted to be statistically and clinically significant,

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
73
pain is included in the determination of the overall utility score, and therefore the value
could not be interpreted directly. As such, further investigation into the single attribute
utility scores was undertaken.
Participants with pain had equal or greater burden of morbidity than participants
without pain in all attributes measured by HUI2 and HUI3 (Table 14). Clinically
significant differences of greater than 0.05 between the two groups were noted in areas
measured by HUI2: sensation, mobility, self-care, and emotion, and by HUI3: vision,
speech, ambulation, dexterity and cognition. All participants noted to have severe burdens
of morbidity endorsed experiencing pain (Table 15).
Table 14. Single-attribute utility scores for participants with (n=13) and
without (n=12) pain. Attributes shaded in grey indicate clinical or statistical
significant difference between groups.
Attribute
Pain
(mean)
No Pain
(mean)
Clinically
Significant
Difference
(>0.05)
Statistically
Significant
Difference
(p<0.05)
HUI2
Sensation 0.83 0.99 -0.16 <0.01
Mobility 0.89 0.98 0.09 0.20
Emotion 0.75 0.97 -0.22 0.02
Cognition 0.94 0.90 0.04 0.15
Self-Care 0.92 1.00 -0.08 0.34
HUI3
Vision 0.89 1.00 -0.11 0.10
Hearing 0.99 1.00 -0.01 0.37
Speech 0.94 1.00 -0.06 0.23
Ambulation 0.86 1.00 -0.14 0.13
Dexterity 0.92 0.98 -0.06 0.49
Emotion 0.96 0.98 -0.02 0.61
Cognition 0.82 0.88 -0.06 0.45

Participants Participants Participants Participants
With
Pain
Without
Pain
With
Pain
Without
Pain
With
Pain
Without
Pain
With
Pain
Without
Pain
None None Mild Mild Moderate Moderate Severe Severe
HUI2
Sensation 3 10 6 1 4 0 0 0
Mobility 9 9 2 3 0 0 2 0
Emotion 5 9 3 2 3 0 2 0
Cognition 7 3 6 9 0 0 0 0
Self-Care 12 12 0 0 0 0 1 0
HUI3
Vision 6 11 5 1 0 0 2 0
Hearing 12 11 1 0 0 0 0 0
Speech 11 12 1 0 1 0 0 0
Ambulation 10 12 1 0 0 0 2 0
Dexterity 12 10 0 2 0 0 1 0
Emotion 9 10 3 0 1 1 0 0
Cognition 7 3 5 1 3 4 2 0
Table 15. Frequency of severity of morbidity by attribute, stratified by participants with (n=13) and
without (n=12) pain
M.S
c. Thesis - T
. Nayia
ger; M
cMaster U
niv
ersity –
Health
Research
Meth
odolo
gies
74

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
75
Although both systems measures cognition and emotion, the underlying constructs
used to define the attributes are different., and accordingly, differences in the scores of
these attributes were observed in this study. Emotion, as defined by “worry” on HUI2,
was compromised in the group experiencing pain, while emotion, as defined by
“happiness” on HUI3, was not. Similarly, cognition, as defined by “memory, thinking,
and solving day-to-day problems” on HUI3 was noted to be decreased in individuals with
pain, but not when defined as “learning and memory” on HUI2.
Longitudinal Analysis-Time points 2000/2001, 2005/2006 and 2011/2012
Longitudinal analysis was also undertaken to explore the burden of pain in the
same cohort at five-year intervals, over a 10-year time period. HUI utility scores collected
in 2011/2012 (time point of current study) (T3) were matched by participant ID to data
collected in 2005/2006(T2) and 2000/2001 (T1). The cross-sectional results from the
previous time points have been presented previously. Aside from one subject who died
between T1 and T2, the data from all subjects at each time point were used in the
longitudinal analysis. A summary of the number of participants accrued at each time
point, as well as the prevalence of pain reported at each time point, can be seen in
Figure 9.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
76
Figure 9. Overview of number of participants at each study time point\ as well as the
prevalence of pain (self-reported).
132 children diagnosed with a Brain Tumour
at McMaster Children’s Hospital between
January 1, 1985 and December 31, 1998
Initial Screening 59 subjects eligible
2000/2001 Cross-sectional study 40 participants 35% reported experiencing pain
73 Subjects excluded (screening by clinic nurse): Prior to initial study:
11 were alive but history of relapse or progressive disease 27 died after relapse or progression
16 died without relapse or progression
19 excluded based on age (<5 years), short interval from diagnosis (<2 years), not able to speak English or lost
to follow-up
19 Non-participants: 6 Declined participation 7 Non-responders
2 Unable to complete questionnaire
4 Lost to follow-up
2005/2006 Cross-sectional study 37 participants 27% reported experiencing pain
3 Non-participants: 1 Died between survey time points
2 Declined participation
2011/2012 Cross-sectional study 25 participants
52% reported experiencing pain
12 Non-participants: 3 Declined participation
3 Non-responders
6 Loss to follow-up

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
77
A total of 39 subjects who participated at the initials time point were included in
the longitudinal analysis. During the course of the study, 26 individuals were noted to be
disease free or have stable disease; 5 had recurrence of tumour, 3 had progressive disease,
and 5 had a second malignancy, including meningioma.
The median pain and median overall utility scores for the participants at each time
point are depicted in Figure 10. From the graph it appears that pain was fairly stable
between T1 and T2 and most individuals reported being pain-free or having pain that did
not limit their activity or that they required limited intervention for pain relief.
Irrespective of this stability of pain, the overall HRQL scores changed, with a decrease as
measured by the HUI2 and an increase by HUI3. An increase of pain by T3, as reflected
by the decrease in the utility score, was observed in the group as a whole. The overall
HRQL scores for both HUI2 and HUI3 were noted to decrease by T3, as would be
anticipated by the increased burden of pain reported by the group.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
78
Figure 10. Median overall HRQL and pain utility scores over a 10 year period, measured
at five-year intervals.
Additional examination of the original data at each time point was undertaken.
Table 16 highlights the minimum and maximum pain utility scores reported for each
system. Most participants were noted to have a pain utility score of equal to or over 0.80.
HUI2 Pain Utility Score
HUI3 Pain
Utility Score
HUI2 Overall
Utility Score
HUI3 Overall
Utility Score

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
79
Table 16. Minimum, maximum and mean pain utility scores reported at each time point
for HUI2 and HUI3. The prevalence of utility scores of equal to or greater than
0.80 is also presented
Timepoint
2000/2001 2005/2006 2011/2012
# of Participants 39* 37 25
% pain 35 27 52
HUI 2 Pain Utility Score
Min/Max 0.00/1.00 0.42/1.00 0.00/1.00
Mean 0.93 0.96 0.90
# with utility
≥0.80 (%) 32 (82%) 32 (86%) 21 (84%)
HUI 3 Pain Utility Score
Min/Max 0.48/1.00 0.00/1.00 0.00/1.00
Mean 0.95 0.93 0.85
# with utility
≥0.80 (%) 34 (89%) 33 (89%) 21 (84%)
*1 participant did not respond to pain question for HUI3 system (n=38)
Of the 25 individuals who provided responses at all 3 time points, 36% (9/25)
reported no pain at all three survey administrations, while 40% reported pain on more
than one occasion.
Exploration of pain over time was also undertaken using statistical analysis. A
complete data set was generated using imputed data for missing values. A description of
the imputation procedures can be found in the “Methods” section of this Thesis. The
number of values imputed at each time point can be seen in Table 17. The imputed
datasets along with the original data were pooled for analysis.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
80
Table 17. Summary of the number of variables imputed for longitudinal analysis
Analysis of change in pain over time by HUI2 was facilitated using a linear mixed
effects model. F-values of the original and the imputed data sets were not significant, as
determined by a p-value of >0.05. As anticipated the pairwise comparison of the five-year
interval changes (2000/2001 to 2005/2006, and 2005/2006 to 2011/2012) as well as the
change over ten years (2000/2001 to 2011/2012), were not statistically significant (Table
18). In addition, these time points were also noted to be clinically similar with an increase
of pain utility score (interpreted as a decrease of burden of pain) by 0.029 at T2, and a
slight decrease (0.032) of the utility score between T2 and T3.
Time-
point Attribute
# of
Values
Available
# of Value
Imputed-
Missing-
Participants
# of Values
Imputed-
Non-
Participants
# of
Values
Used in
Analysis
2000/
2001
HUI2- Pain 39 0 0 39
HUI2- Overall 37 2 0 39
HUI3- Pain 38 1 0 39
HUI3-Overall 37 2 0 39
2005/
2006
HUI2- Pain 36 1 2 39
HUI2- Overall 33 4 2 39
HUI3- Pain 36 1 2 39
HUI3-Overall 33 4 2 39
2011/
2012
HUI2- Pain 25 0 14 39
HUI2- Overall 24 1 14 39
HUI3- Pain 25 0 14 39
HUI3-Overall 24 1 14 39

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
81
Table 18. Results of longitudinal analysis of the pain utility scores by linear mixed effects
model; fixed factor is time. Results presented are of pooled data (initial dataset
along with datasets with imputed missing values).
T1= 2000/2001, T2= 2005/2006, and T3= 2011/2012 survey time points.
= increase in utility score, = decrease in utility score
HUI
System
Time
point Estimate
St.
Error
Stat.
Sig.
Clinical
Sig.
(>0.05)
95% Confidence
Interval
Lower
Bound
Upper
Bound
HUI2
T1 to T2 0.029 0.0286 0.315 No -0.085 0.027
T2 to T3 0.032 0.030 0.286 No -0.027 0.061
T1 to T3 0.003 0.030 0.910 No -0.055 0.061
HUI3
T1 to T2 0.021 0.529 0.692 No 0.088 0.357
T2 to T3 0.202 0.062 0.002 Yes 0.078 0.326
T1 to T3 0.223 0.066 0.002 Yes 0.089 0.357
In contrast, the F-values resulting from the HUI3 pain utility scores over time was
statistically significant (p<0.05) for the five datasets containing imputed data; the original
dataset comparing T1 and T2 to T3 was not significant, with a p-value of 0.071. Review
of the pairwise comparison revealed both statistically and clinically significant increases
in the burden of pain between the five-year period of 2005/2006 and 2011/2012 (decrease
of utility score by 0.20, standard error 0.06, significance p<0.01). This marked decrease
in pain utility score was also noted over the ten-year study period (estimated decrease of
0.223, standard error 0.07, significance of p<0.01).
Generation of ICCs was also undertaken to provide an estimate of the stability of
pain at an individual level. The within-individual correlation for pain was fair, with the
ICC calculated at 0.41 as measured by HUI2 and 0.40 by HUI3. It can be interpreted that,
although pain is a consistent burden of morbidity in this cohort, only a few participants
experience a persistent level of pain at each time point.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
82
Finally, the overall HRQL over time was also investigated for this cohort. The
median overall utility scores for the original data at each time point can be seen in 10. It
was noted that, although the pain score contributes to the generation of the overall utility
score, the line graph revealed that the mean HRQL utility scores and the pain utility
scores did not follow the same trajectory.
Analysis of the linear mixed effects model results using pooled data from the
original and imputed datasets for the HRQL mean utility scores by HUI2 revealed
significance of the F-value in some but not all of the datasets generated. Pooled pairwise
comparisons of the initial time point to the subsequent time points were not statistically
significant (Table 19). However, there was a clinically significant increase in HRQL
between T1 and T2, but marked decrease between T2 and T3.
Table 19. Results of longitudinal analysis of the multi-attribute utility scores by linear
mixed effects model; fixed factor is time. Results presented are of pooled data
(initial dataset along with datasets with imputed missing values).
T1= 2000/2001, T2= 2005/2006, and T3= 2011/2012 survey time points.
= increase in utility score, = decrease in utility score.
HUI
System
Time
point Estimate
St.
Error
Stat.
Sig.
Clinical
Sig.
(>0.03)
95% Confidence
Interval
Lower
Bound
Upper
Bound
HUI2
T1 to T2 0.031 0.03 0.304 Yes -0.089 0.028
T2 to T3 0.068 0.041 0.121 Yes -0.020 0.155
T1 to T3 0.037 0.040 0.358 Yes -0.045 0.119
HUI3
T1 to T2 0.017 0.065 0.793 No -0.148 0.113
T2 to T3 0.173 0.068 0.015 Yes 0.036 0.310
T1 to T3 0.155 0.066 0.021 Yes 0.024 0.287

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
83
This decrease between 2005/2006 and 2011/2012 was even more pronounced in
the HUI3 multi-attribute scores, with significant differences seen statistically and
clinically (regression estimate of -0.173, standard error of 0.068, statistical significance of
p=0.015). The change over the ten years also reflected this decrease in HRQL over the
long-term (regression estimate of -0.155 from time point 1 to time point 3, standard error
of 0.066, significance of p=0.021). There was no perceivable change between T1 and T2.
The within-individual correlations for the overall HRQL were calculated to be 0.48 for
HUI2, and 0.37 for HUI3.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
84
DISCUSSION
Surviving a brain tumour in childhood is not without consequence with multiple
medical late effects cited in the literature. Given the precarious balance between
interventions required for cure and the ensuing long-term sequelae, HRQL has gained
increasing recognition as an important outcome in pediatric oncology research studies
(Schwartz & Sprangers, 2003). This current exploratory study undertaken in 25 survivors
of brain tumours diagnosed in childhood or adolescence provides insight into the HRQL
of long-term survivors of CNS malignancies.
Of the 31 eligible participants contacted, 81% (N=25) completed the interviewer-
administered HUI2/3 questionnaires, which is noteworthy given that survivors were all
greater than ten years from their initial diagnosis. The high rate of participation is not
uncommon in oncologic studies; survivors of cancer are not to be responsive to research
and specifically, welcoming the opportunity for self-reporting of health (Turner et al.,
2009). Of the individuals who did participate the majority provided responses to all items
on the HUI2/3 questionnaires. This is felt to be partially attributable to the use of
interviewer-administered questionnaires as previous studies of childhood cancer survivors
have noted that this population has a propensity to respond “don’t know” or leave
responses blank to mailed questionnaires relating to HRQL (Ness et al., 2005).
Formal comparison between disease and treatment characteristics of participants
and non-participants was not undertaken due to the small sample size. On review,
participants appeared to have received more intensive intervention by means of radiation

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
85
and chemotherapy. However, the proportions of brain tumour sub-types, site of primary
tumour, extent of resection and mode of therapeutic intervention were diverse and similar
to the patient characteristics reported in the CCSS, which was a large, North-American
multi-centre study of long-term survivors of cancer in childhood and adolescence,
including those with brain tumours (Packer et al., 2003).
Cross-Sectional Results
Overall HRQL
As a group long-term survivors of brain tumours in childhood and adolescence
were found to experience a compromised overall HRQL, with a resultant overall HUI2
mean score of 0.79 (SD 0.23), median of 0.88, and HUI3 mean score of 0.69 (SD 0.29),
median of 0.77. This cohort of survivors reported greater burdens of morbidity, including
a clinically significant difference of >0.03, than is observed in the general population. A
US population-based report of the HRQL of adults aged 18-44 revealed a HUI2 mean
score of 0.89 (median of 0.92) and HUI3 score of 0.86 (median of 0.93) (Luo, Johnson,
Shaw, Feeny & Coons, 2005). Of note, the US-based study oversampled Hispanic and
non-Hispanic Blacks to be representative of the ethnic composition of the US. Therefore
comparisons the study cohort and the population based data should be approached
cautiously. A smaller, population-based study was undertaken in Canada using the HUI3
questionnaire (Pogany et al., 2006). Individuals between the ages of 20 and 37 without a
history of cancer had a mean score of 0.85, which is once again higher (and clinically
significant different) than the mean score observed in our cohort of long-term survivors

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
86
of brain tumours. In both the US and Canadian studies the assessment was by self-
completion, which may have had an influence on the responses.
With respect to other childhood cancer survivor studies, the mean HUI scores
observed in the current study were within the range of scores reported in other studies of
survivors of childhood brain tumours and using the HUI family of instruments (Alessi et
al., 2007; Barr et al., 1999; Glaser et al., 1999).
The overall mean HRQL score from this study was noticeably lower than the
median, which prompted further investigation. Examination of the distribution of the
individual patient scores revealed that there was a wide range in the overall utility scores,
including one report of a “very poor” HRQL of 0.16 as measured by the HUI2 system and
“as significant as a state that is worse than being dead” (-0.19) by the HUI3 system. It
would appear that a sub-group of individuals within this cohort experience considerable
morbidity even many years after diagnosis.
Single Attribute Analysis
A high prevalence of morbidity in attributes of cognition, pain, sensation and
emotion was observed in our cohort of survivors of brain tumours in childhood. This was
consistent with Hypothesis #1, which anticipated a high prevalence of participants
reporting pain, and Hypothesis #3, which noted additional areas of morbidity, in
particular in cognition and emotion. Further, participants also reported a high burden
(severity) of morbidity in areas of physical functioning, including the attributes of
mobility, ambulation, dexterity and vision, as well as in areas of executive functioning,

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
87
demonstrated by the scores in emotion and cognition. Pain was also established to be a
prevalent and considerable burden among those interviewed.
The breadth of physical and other morbidities observed, although well
documented in the literature, is not fully understood. Many survivors experience
functional deficits that do not match the area of the primary brain tumour. It has been
postulated that, although a tumour may occur in a single area of the brain, there is overlap
in function and therefore decreased ability in one area has ramifications for other
capabilities. Baron Nelson et al. (2013) provide the example of cognition, which relies on
the processes of thinking, memory, perception and language. As HRQL attempts to
capture the functional capabilities of an individual within the context of daily living, it is
possible that the deficits observed could be a result of any number of limitations within a
complex process required to perform the desired function. That is, the measure of the
specific morbidity could be confounded by deficits in other areas.
The HUI2/3 system explores functional capabilities of an individual. This may
require multiple cognitive processes in addition to the attribute under investigation.
Therefore this measure may be particularly sensitive to burdens in functional capabilities
and as such evaluates a process of abilities as opposed to a single observable attribute. For
example, “vision” is measured based on the response to the question “Have you been able
to see well enough to recognize a friend on the other side of the street without glasses or
contact lenses?” This question requires that the respondent utilise multiple faculties in

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
88
addition to sight, including memory, perception and thinking, as the item also specifies
that the individual is able to distinguish between a friend and a stranger.
Unlike most survivors of non-CNS malignancies in childhood, as noted previously
and once again established in this study, there continues to be a high prevalence of
morbidity detected many years after diagnosis in survivors of brain tumours in childhood.
This was observed in the study by Alessi et al (2007) in which the overall HRQL scores
for childhood leukemia survivors greater than 15 years of age was 0.85 in comparison to
CNS tumour survivors who had a score of 0.73, as measured by the HUI3 questionnaire.
Pogany et al., (2006) also identified survivors of childhood brain tumours to have poorer
health utility scores in comparison to most other primary cancer survivors, again
measured using the HUI3. Reulen et al., (2007) also found that long-term survivors of
brain tumours in childhood treated with radiotherapy scored significantly lower physical
component score than survivors of leukemia and most other cancers (aside from survivors
of bone tumours and neuroblastoma treated with radiotherapy. It is possible that in
children with brain tumours, the assault to the young brain at a time of crucial
development may result in cognitive limitations. Functional impairment that may also
become increasingly apparent as the brain develops, and even more so as these
individuals attain an age associated with expectations of increasing independence,
potential demands on physical activity, and integration into society (Anderson et al.,
2001B; Radcliffe et al., 1992, Mulhern & Palmer, 2003; Sands et al., 2001). The
increased limitations may also contribute to previous observations that survivors of brain
tumours are at greater risk than other childhood cancer survivors of having difficulty with

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
89
educational achievement, employment and social supports, and maintaining relationships
(Armstrong et al., 2009; Barrera et al., 2005; Gurney et al., 2009; Hays et al., 1992; Koch
et al., 2004; Langeveld et al., 2003; Lancashire et al., 2010; Mostow, et al., 1991).
Pain in Survivors of Brain Tumours in Childhood and Adolescence
In keeping with Hypothesis #1 pain was reported in greater than 35% of
respondents. This establishes a burden of pain in long-term survivors with over half of the
participants reporting experiencing pain the week prior to the interview. Interestingly,
discomfort was not limited to the head, but was also identified to be present in various
locations through the body. The presence of pain in survivors of CNS tumours in
childhood has been reported inconsistently. Previous studies have noted the presence of
pain, including an increased prevalence in comparison to normal controls and other
cancer survivors, while others have found no pain, or pain at levels similar to childhood
cancer survivor and non-cancer comparison groups (Alessi et al., 2007; Armstrong et al.,
2009; Barr et al., 1999; Glaser et al., 1999; Pogany et al., 2006).
It is possible that the discrepancies between the burden of pain observed in
various studies, including this current study, could be attributed partially to the use of
self- or proxy-reporting (Sands et al., 2001). This is related to Hypothesis #2, which
stated that expectation of correlation between self- and proxy- reported pain would be fair
(less than 0.4). In this study it was observed that there was only fair correlation of pain
when measured by activity limitation (HUI3), and slightly above fair when measured by
interventions to alleviate pain (HUI2).

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
90
In keeping with other studies it was observed in the current study that overtly
observable attributes, such as mobility, had good correlation between the proxies (parent,
spouse or friend) and the participants, while less observable attributes, such as emotion
and pain, had poorer correlation, particularly when it came to severity of the morbidity
(Barr et al, 1999; Bhat et al., 2005; Glaser et al., 1999). Interestingly, in the current study
there was poor agreement between participants and proxies in attributes that, as a group,
were identified by participants to have increased burden of morbidity. It is possible that
“very good” to “perfect” health is easier to rate than the degree of poor health. This was
seen in the attribute of pain in which the presence or absence of morbidity was identified
correctly by most proxies (17 out of 22); however, only 45 to 50% of proxies were able to
identify the severity of pain correctly as measured by the amount of activity limitation
and by the type of intervention to alleviate symptoms. Of the five discordant pairs, four
proxies under-reported the presence of pain in the participants. The results are also in
keeping with poor prediction of pain by spouses of chronic pain sufferers (Sorbi et al.,
2006).
The questionnaire itself may also be instrumental in the reporting of pain by the
subject. From literature reviewed for this thesis, studies that utilized the HUI family of
instruments to explore HRQL were more likely to explicitly provide results for pain as
well as identify pain as a concern for long-term survivors of brain tumours in childhood
(Alessi et al., 2007; Barr et al, 1999; Glaser et al., 1999; Pogany et al. 2006). The current
study, which also used the HUI system of instruments, also identified pain as a burden in
this cohort. The increased reporting of pain may be a result of the wording of the

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
91
questions by the HUI family of questionnaires as participants were requested to report
whether they experienced any pain or discomfort within the past week. In addition, the
interpretation of pain or discomfort was made by the respondent and did not preclude any
location within the body or type of pain experienced. Further pain was not defined by the
interviewer nor was any attempts made at that time, by a health care professional or
member of the research team to differentiate between the pain or symptoms reported by
the subject. This is different from the CCSS in which participants responded to a question
framed around being informed by a doctor or health care professional that they were
experiencing pain in very specific areas of the body (Lu et al., 2011). The response to the
CCSS questionnaire is contingent on the experience of pain being identified through
routine medical care, as well as for the participant to recall a discussion with a member of
the health care team. Also, the HUI family of questionnaires provides a single attribute
score for pain, which may facilitate the reporting of pain.
Further, certain studies attempted to explore HRQL and pain using novel or
disease-specific questionnaires. Consequently enquiry into pain was often limited to
specific body areas preconceived to be a problem, such as the head or abdomen, which
may have limited the exploration of pain and thus resulted in under-reporting (Lu et al.,
2011; Streiner & Norman, 2008). The results of the current study, which utilised generic
questionnaires, concurred with the possibility of this limitation as it was demonstrated
that survivors of brain tumours in childhood experienced pain in multiple areas of the
body, including but not limited to the head.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
92
In addition, many survivors of brain tumours in childhood have received radiation
therapy to the brain, which is associated with long-term cognitive dysfunction (Lawrence
et al., 2010). As such, it is possible that measurement instruments with increased
complexity may result in under-reporting of pain due to limited comprehension of the
question itself. The HUI2/3 items related to pain had an average Flesch-Kincaid grade
level of 6.7 (minimum of 4.1, maximum of 9.1), which, coupled with interviewer
administration, would increase the possibility of the brain tumour survivors being able to
understand and respond to the questions.
In the current study of survivors of brain tumours in childhood it was observed
that 52% of participants reported experiencing pain on at least one occasion in the past
week. However, of those reporting pain, the majority expressed that the pain did not
occur daily, and that the most severe pain experienced within the past week restricted
none or very few of their daily activities and either did not require any intervention or
could be controlled with over-the-counter medications or self-control of activities. While
participants report limited requirements for therapeutic intervention for their pain, it is
unclear whether their pain was managed effectively. Further exploration into the type of
pain and the potential role of counselling regarding methods to control pain, needs to be
pursued.
Further exploration of pain and the association with other attributes of HRQL
revealed a more complex picture and potentially a greater understanding of the actual
burden experienced by this subgroup. Individuals reporting discomfort were found to

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
93
have equal or greater burdens of morbidity in all attributes compared to their pain-free
counterparts. Areas of clinically significant difference included those of physical
functioning, cognitive processing and fretfulness. The most conspicuous difference was
the increased worry and fretfulness, as measured by the HUI2 attribute of emotion. As a
group, however, participants with pain had mean single attributes of greater than 0.8 for
all attributes aside from the HUI2 emotion score of 0.75.The most remarkable finding,
however, was that all individuals reporting a severe burden of morbidity in any attribute
also endorsed experiencing pain. In addition, participants with pain comprised 71% of
individuals noting a moderate level of morbidity measured at a single attribute level.
The increased difficulties with movement, sensation and dexterity are not
unexpected in individuals with pain and this was supported by the increased prevalence of
extremity pain, particularly of the lower extremities, reported by participants. Further,
30% of survivors with pain directly endorsed discomfort limiting at least some of their
daily activities. The greater morbidity in physical functioning in survivors with
symptomatic pain may be a result of the neurological complications, such as peripheral
neuropathy and motor dysfunction, as well as neurosensory system difficulties, including
visual deficits, which have been described as common long-term consequences in
survivors of CNS tumours (Deliganis, Geyer & Berger, 1996; Gayre, Scott, Feuer,
Saunders & Siatkowski, 2001; Packer et al., 2003; Sonderkaer et al., 2003). These
medically significant late effects are thought to be related to both tumour involvement
and therapeutic intervention, including radiation, platinum-based chemotherapy and
antibiotics (Turner et al., 2009).

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
94
It is also possible that neurosensory changes may influence pain independently,
and, more specifically, the perceptions of pain. As such, individuals identified to have
greater neurological morbidity may also experience a heightened sense of pain. This is
postulated to be a potential mechanism of the chronic pain that is often observed in
patients with a history of traumatic brain injury (Nampiaparampil, 2008; Sherman,
Goldberg & Bell, 2005).
The presence of pain may also influence neurocognitive functioning; in the
current study, long-term survivors reporting pain also self-reported difficulty with
memory, thinking and solving of day-to-day problems. The negative impact of pain on
neurocognitive processing has been demonstrated in studies of patients with and without
known histories of assaults to the brain or neurologic disorders (Hart, Martelli & Zasler,
2000). Specifically, areas of attentional capacity, processing speed and psychomotor
speed were identified as the most significantly affected areas in these individuals (Hart et
al., 2000). Grigsby, Rosenberg & Busenbark (1995) also found that individuals with
chronic pain performed more poorly with respect to information processing compared to
individuals with traumatic brain injury.
Neuropsychological late effects, including mood irregularities such as anxiety and
depression, are well-documented in the literature for patients with a history of CNS
malignancy in childhood and have been attributed to tumour type, location and extent, as
well as treatment (Turner et al., 2009; Gragert & Ris, 2010). Pain also may play a role in
emotional morbidity, defined by worry, as this was found to be a clinically significantly

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
95
greater burden in individuals with pain than in those without pain in the current study.
This finding is in keeping with observations of decreased emotional functioning,
including heightened anxiety, reported in pain sufferers, and is well-described in the
literature and considered one of six essential domains included in the evaluation of
chronic pain in clinical studies (Turk et al., 2003).
Somewhat surprisingly emotion as measured by happiness did not differ
significantly between the two groups. Diminished happiness was not identified as a
significant burden for the overall cohort, which is unlike the CCSS that demonstrated
increased depression and decreased expectation of future life satisfaction in brain tumour
survivors (Zebrack & Zeltzer, 2003; Zeltzer et al., 2008). The self-reported happiness
experienced by the participants in the current study may be a consequence of the self-
affirmed overall HRQL, with 24 of the 25 participants reporting at least “good” HRQL,
and the optimism seen by the anticipated increase in general QOL over time. Other
studies, including those involving children diagnosed with cancer, have also reported
favourable outlooks by participants despite living with health conditions or disabilities;
this phenomenon is given the term “disability paradox” to explain the appearance of
moderate correlation between health status and QOL (Albrecht & Devlieger, 1999;
Phipps & Srivastava, 1997; Phipps et al., 2001).
Correlation between direct reporting of maximum pain intensity at each location
as measured by the coloured analogue scale and pain measured by intervention for
symptom relief (HUI2 system) and activity limitation (HUI3 system) was moderate, with

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
96
ICCs of 0.38 and 0.45, neither of which was statistically significant. The strength of the
correlation observed suggests that the numerous measures of pain severity may be related
but not redundant. As pain is a subjective, multi-faceted process, the measurement of
perceived intensity, activity limitation and level of intervention can be seen as
complementary in the measure of pain. This idea of multiple domains to capture pain is
emphasised in the IMMPACT consensus statement which provides guidance on the
measurement of chronic pain in clinical trials (Turk et al., 2003). Other suggested core
domains include emotional and physical functioning, which were areas that were also
identified to be significantly different between participants with and without pain.
Sociodemographics, including social adjustments, and life and career pursuits,
have been shown in previous studies to be compromised in individuals with brain
tumours in comparison to healthy controls as well as to survivors of non-CNS
malignancies (Lannering, Marky, Lundberg & Olsson, 1990; Pang et al., 2008). Although
patients with pain had greater burdens related to their HRQL, there were similar
distributions of social integration and adaptation including reported living situation,
relationship status, ability to drive, educational level achieved and employment/student
status as in their pain-free counterparts. Exploration of the severity of pain and
distribution of sociodemographics was not undertaken due to the sample size. However,
at a cursory overview it appears that there may be alternate factors that influence the
variability seen within this cohort. Posited theories for variability include maladaptation
and transition into adulthood as a consequence of health care needs and neurocognitive
morbidities (Turner et al., 2009).

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
97
Exploration of pain at five-year intervals over a 10-year period established that
pain is a persistent burden in survivors of brain tumours in childhood. Review of the raw
data revealed that pain was endorsed by 35% of participants at the first time point and,
although decreased at the second interview (27%), increased to 52% at the third interview
when all individuals were deemed to be long-term survivors of brain tumours in
childhood. Irrespective of the trend, 40% (n=10) of the 25 individuals who participated at
all survey time points reported the presence of pain on at least 2 of the 3 interview time
points. This suggests that a subgroup of survivors experience on-going pain.
Analysis of the pain utility scores, using imputation and longitudinal analytic
techniques, supported the hypothesis of the continued prevalence of pain in the study
cohort over time. This burden of morbidity was found to be relatively stable between the
first two time points (5-year period), as measured by HUI2 and HUI3 systems. However,
between the interviews at 2005 (T2) and 2010 (T3), although there was no increase in
interventions to alleviate discomfort, there was a significantly increased amount of
activity limitation. Accordingly, the within-individual correlation of pain over time,
interpreted with an ICC, was fair. This would suggest that an individual with a history of
a CNS malignancy in childhood may experience variability in the presence and severity
of pain in survivorship.
The overall HRQL utility score, which incorporates the attribute of pain, also
decreased between the second and third time points. The HUI3 system appeared to be
more sensitive than HUI2 to the increased morbidity experienced by the cohort with a

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
98
statistically and clinically significant decrease of HRQL over a 10-year period (regression
estimate of -0.155 from time point 1 to time point 3, standard error of 0.066, significance
of p=0.021). The within-individual correlations for overall HRQL for the ten-year study
perdiod were calculated to be 0.48 for HUI2 and 0.37 for HUI3. Interpreted as an ICC,
this would suggest that the overall HRQL of individual long-term survivors of brain
tumours in childhood varies over time for many of the survivors. This could be a
reflection of a change in health status according to the ability of the individual or by a
change in life requirements. This is consistent with the theory that the impact of
morbidities increases or becomes more apparent as cancer survivors age and assimilate to
adult life (Anderson et al., 2001B; Radcliffe et al., 1992, Mulhern & Palmer, 2003; Sands
et al., 2001).
While pain contributes directly to the overall HRQL, in this study it was also
demonstrated to influence morbidity in other areas and as such have a greater impact on
the HRQL than is readily observed. This could explain the different rates of change of
pain and HRQL over time. It is also possible that the other attributes change
independently over time. However, this was not explored and is beyond the realm of this
project.
Limitations
There are several limitations of the current study. It is possible that the burden of
morbidity experienced by long-term survivors of brain tumours may be over-estimated
due to selection bias. Participation in this study was limited to individuals who were

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
99
contactable and therefore either traceable through the health care system, such as being
actively seen in the brain tumour survivor clinic or family doctor’s office, or reachable
through the last listed telephone contact. It is conceivable that patients with less morbidity
are more likely to move away from home and consequently may be more difficult to
reach. As such, the recruitment strategy may select indirectly subjects with greater
morbidity. A sensitivity analysis (best-case, worst-case scenarios) could be undertaken to
assess the influence of the missing data on the overall results. In addition, once an
individual was deemed a “non-participant” they were not approached again at a later time
point for participation. This could further bias the results. It may have been appropriate to
re-approach the individuals at the later time points even if they had not participated
previously in the study. A comparison of the characteristics of the participants versus
non-participants at each time point may also be beneficial to see if there are systematic
differences between the two groups.
Although review of the initial diagnostic characteristics of participants and non-
participants were suggestive of more intensive treatment of individuals who participated
in the study and, by extension, suggestive of increased levels of morbidity, the
demographic and disease characteristics as well as therapeutic interventions of
participants were similar to those seen in the large, multi-centre CCSS (Packer et al.,
2003). Therefore the results obtained in this study are thought to be representative of
survivors of CNS tumours in childhood. In addition, morbidities observed in this study
were similar to those reported in previous studies. Other reasons for non-participation

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
100
include individuals who were not able to schedule a time for the interview, as well as
those who felt the study would result in increased distress.
The possibility also exists that the true prevalence of pain is overestimated in this
study. On the HUI2/3 system participants are required to assess retrospectively pain
experienced the week prior without investigation into pain beyond this period or the type
of pain being reported (Furlong et al., 1998). While episodes of acute pain have been
found to be recalled accurately within a one-week period, this method of retrospectively
assessing pain has been found to potentially bias chronic pain sufferers to the over-
reporting of pain (Singer, Kowalska, & Thode, 2001; Sorbi et al., 2006). The use of
momentary assessments, such as electronic pain diaries, which are completed in real time
throughout the identified period, may provide a better representation of the discomfort
experienced by the cohort under study, particularly if survivors of childhood brain
tumours experience chronic pain (Morren, van Dulmen, Ouwerkerk & Bensing, 2009). As
the burden of pain in long-term survivors of brain tumours becomes better understood,
more comprehensive, but costlier and more intensive measures, such as those used in
chronic pain studies, can be justified for use.
Another consideration is the potential response shift when applied to longitudinal
analysis. QOL measurement is founded on the assumption that an individual’s values do
not change and, as such, changes in health would be reflected by the HRQL outcomes
(Schwartz & Sprangers, 1999). However, “response shift” is the change in an individual’s
values and perceptions, often in response to a change in health status, and may result in

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
101
alteration of values (Sprangers & Schwartz, 1999). This is often reported within the
context of medical conditions, with patients asserting good self-reported health status
despite medically worsening health. In the current study, all but one participant endorsed
“good” overall HRQL when questioned directly; however, analysis of the multi-attribute
health status scores as well as the single attribute scores indicated otherwise. This
discrepancy may be accounted for by response shift bias.
In addition, it can be postulated that, as healthy individuals age, there would be an
increase in pain over time, and therefore the increase in pain over a decade observed in
the current study may be a reflection of this ‘developmental’ phenomenon. However, the
contribution of the natural aging process to the burden of pain, as well as any normal
intra-individual variation, would not be expected to reach the degree of change observed
in this study. Furthermore, at the last time point of the survey, all patients were less than
40 years old, and therefore would not be anticipated to experience age-related changes in
morbidity as demonstrated by the overall health status reference values for Canada and
the USA (Fryback et al., 2007; Luo et al., 2005; Pogany et al., 2006).
Finally, this study is limited by small sample size, which has implications on the
power to detect differences. This was an exploratory study and therefore statistical results
should be interpreted with caution. Although this study is limited by the small sample
size, as noted previously, the overall participant characteristics and morbidities observed
are similar to those seen in other studies (Aarsen et al., 2006; Alessi et al., 2007;

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
102
Armstrong et al., 2009; Barr et al., 1999; Bhat et al., 2005; Maunsell et al., 2006; Pogany
et al., 2006).
Implications of Findings
The current cross-sectional and longitudinal studies undertaken at MCH
established that pain is a common and persistent phenomenon in survivors of brain
tumours in childhood. While it is unclear whether the pain experienced by this cohort is a
result of the disease, treatment or consequences of other late effects, there appears to be a
distinct relationship between pain and morbidity in other attributes contributing to HRQL,
as individuals experiencing pain also reported increased levels of other morbidities.
The burden of pain in long-term survivors of brain tumours in childhood has been
reported inconsistently in the literature. It is possible that study design, including the
questions selected to delineate pain, the questionnaire, the primary respondent and time
from diagnosis may influence the discrepancies seen. In the present study, results suggest
that pain is a chronic burden in this cohort of individuals, with implications for other
areas of compromised HRQL.
This finding has important implications for the clinical surveillance of survivors.
Given the high prevalence of pain, clinicians following patients with a history of CNS
malignancy in childhood should be aware of pain when individuals present with other
more easily visualized or reportable burdens of morbidity, such as increased anxiety and
compromised dexterity. Conversely, clinicians could use the reporting of pain as a
screening question to identify and further explore other areas of morbidity in survivors.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
103
It should also be considered that the presence of pain in conjunction with other
morbidities may have health-related implications. For example, decreased mobility
secondary to pain may put patients at an increased risk of osteopenia (Barr 1998). In
addition, given the diversity in the location of pain, it is possible that survivors of brain
tumours in childhood may not relate the present discomfort to their initial malignancy. It
would therefore be important for clinicians to enquire about both anticipated and
generalized pain, rather than discomfort limited strictly to the head.
The identification of pain by long-term survivors of brain tumours in childhood
may also provide insight into other potential late effects that may not be well described
yet. This is of particular importance as this patient cohort continues to age and may have
changes in the type and severity of morbidity with either a decline or improvement in
their HRQL.
This current study, while small in size, is in keeping with previous studies that
revealed a burden of pain in long-term survivors of brain tumours. Additionally serial
follow-up of the study cohort over a 10-year period revealed a persistence of pain over
time. Future work needs to be undertaken to explore the pathology of the pain, including
the type of pain experienced, what it could be attributed to, why individuals continue to
be burdened by discomfort many years after treatment, as well as the diversity of the
location of pain throughout the body. This may provide insight into potential
interventions to control the pain. It would also be of interest to explore whether survivors
attribute the pain to their malignancy and subsequent treatment or to another source. This

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
104
would provide insight to the treatment and supportive care measures that are offered to
children with newly diagnosed brain tumours as well as to survivors of CNS malignancies
in childhood and adolescence. Furthermore the additional morbidity experienced by
individuals experiencing pain, particularly the identified increased worry and fretfulness
observed, warrants further study, including by qualitative and exploratory methods to
better understand the potential relationship between these morbidities.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
105
CONCLUSION
In conclusion, long-term survivors of brain tumours in childhood experience
morbidity in physical and cognitive function, as measured by the HUI2/3 HRQL systems.
Pain was reported frequently by participants in this study and had deleterious impacts on
their overall health status as well as on the single attributes that contribute to HRQL. In
addition, self-reporting should be used for assessing patients particularly when the goal is
to measure less readily observable attributes, including pain. The cross-sectional and
longitudinal studies that were undertaken provide further validation that pain is indeed a
genuine phenomenon in survivors of brain tumours, and survivorship clinics should be
aware of and interrogate patients regarding this late effect. Further work needs to be
undertaken to better describe the daily pain and possible pathology resulting in the
persistent discomfort experienced by patients with a history of CNS tumours in
childhood.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
106
REFERENCES
Aarsen, F.K., Paquier, P.F., Reddingius, R.E., Streng, I.C., Arts, W.F., Evera-Preesman,
M., & Catsman-Berrevoets. C.E. (2006). Functional outcome after low-grade astrocytoma
treatment in childhood. Cancer, 106(2):396-402.
Albrecht, G.L., & Devlieger, P.J. (1999). The disability paradox: high quality of life
against all odds. Soc Sci Med. 48(8):977-88.
Alessi, D., Dama, E., Barr, R., Mosso, M.L., Maule, M., Magnani, C., Pastore, G., &
Merletti. F. (2007). Health-related quality of life of long-term childhood cancer survivors:
a population-based study from the Childhood Cancer Registry of Piedmont, Italy. Eur J
Cancer, 43(17):2545-52.
Altman, D.G. (1991). Practical statistics for medical research. London: Chapman & Hall.
Altman, D.G., & Bland, J.M. (2007). Missing Data. BMJ, 334-424
Amin, L., Rosenbaum, P., Barr, R., Sung, L., Klaassen, R.J., Dix, D.B., & Klassen, A.
(2012). Rasch analysis of the PedsQL: an increased understanding of the properties of a
rating scale. J Clin Epidemiol, 65(10):1117-23. doi: 10.1016/j.jclinepi.2012.04.014.
Anderson, D.M., Rennie, K.M., Ziegler, R.S., Neglia, J.P., Robinson, L.R., & Gurney,
J.G. (2001A). Medical and neurocognitive late effects among survivors of childhood
central nervous system tumors. Cancer, 92(10):2709-19.
Anderson, N.E. (2003). Late complications in childhood central nervous system tumour
survivors. Curr Opin Neurol, 16(6):677-683.
Anderson, V., Northam, E., Hendy, J., & Wrenhall, J. (2001B). Developmental
neuropsychology- a clinical approach. Hove, East Sussex, UK: Psychology Press, 2001
Armstrong, G.T., Liu, Q., Yasui, Y., Huang, S., Ness, K.K., Leisenring, W., Hudson,
M.M., Donaldson, S.S., King, A.A., Stovall, M., Krull, K.R., Robison, L.L., & Packer
R.J. (2009). Long-term outcomes among adult survivors of childhood central nervous
system malignancies in the Childhood Cancer Survivor Study. J Natl Cancer Inst,
101(13):946-58. doi: 10.1093/jnci/djp148.
Armstrong, G.T., Liu, Q., Yasui, Y., Huang, S., Ness, K.K., Leisenring, W., Hudson,
M.M., Donaldson, S.S., King, A.A., Stovall, M., Krull, K.R., Robison, L.L., & Packer
R.J. (2009). Long-term outcomes among adult survivors of childhood central nervous
system malignancies in the Childhood Cancer Survivor Study. J Natl Cancer
Inst;101(13):946-58. doi: 10.1093/jnci/djp148.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
107
Aziz, N.M., Oeffinger, K.C., Brooks, S., & Turoff, A.J. (2006) Comprehensive long-term
follow-up programs for pediatric cancer survivors. Cancer,107(4):841-8.
Baron Nelson M., Compton, P., Patel, S.K., Jacob, E., & Harper, R. (2013). Central
Nervous System Injury and Neurobiobehavioral Function in Children With Brain
Tumors: A Review of the Literature. Cancer Nurs, 36(2):E31-47. doi:
10.1097/NCC.0b013e31825d1eb0.
Barr, R. (2006, June). Health status and health-related quality of life in survivors of brain
tumors in childhood – a focus on pain. Poster presented at the International Conference
on Long-Term Complications of Treatment of Children and Adolescents for Cancer,
Niagara-on-the Lake, Ontario
Barr, R., Pai, M., Weitzman, S., Feeny, D., Furlong, W., Rosenbaum, P., & Torrance, G.
(1994). A multiattribute approach to health-status measurement and clinical management
illustrated by an application to brain-tumors in childhood. Int J Oncol, 4(3):639-48.
Barr, R.D., Simpson, T., Webber, C.E., Gill, G.J., Hay, J., Eves, M., & Whitton, A.C.
(1998). Osteopenia in children surviving brain tumours. Eur J Cancer, 34(6):873-7.
Barr, R.D., Simpson, T., Whitton, A., Rush, B., Furlong, W.J., & Feeny, D.H. (1999).
Health-related quality of life in survivors of tumours of the central nervous system in
childhood – a preference-based approach to measurement in a cross-sectional study. Eur J
Cancer, 35: 248-255.
Barrera, M., Shaw, A.K., Speechley, K.N., Maunsell, E., & Pogany, L. (2005).
Educational and social late effects of childhood cancer and related clinical, personal, and
familial characteristics. Cancer, 104(8):1751-60.
Beebe, D.W., Ris. M.D., Armstrong, F.D., Fontanesi, J., Mulhern, R., Holmes, E., &
Wisoff, J.H. (2005). Cognitive and adaptive outcome in low-grade pediatric cerebellar
astrocytomas: evidence of diminished cognitive and adaptive functioning in National
Collaborative Research Studies (CCG 9891/POG 9130). J Clin Oncol, 23(22):5198-204.
Bhat, S.R., Goodwin, T.L., Burwinkle, T.M., Lansdale, M.F., Dahl, G.V., Huhn, S.L.,
Gibbs, I.C., Donaldson, S.S., Rosenblum, R.K., Varni, J.W., & Fisher, P.G. (2005).
Profile of daily life in children with brain tumors: an assessment of health-related quality
of life. J Clin Oncol, 23(24):5493-500.
Boman, K.K., Hovén, E., Anclair, M., Lannering, B., & Gustafsson, G. (2009). Health
and persistent functional late effects in adult survivors of childhood CNS tumours: a
population-based cohort study. Eur J Cancer, 45(14):2552-61.
Canadian Cancer Society’s Steering Committee on Cancer Statistics. Canadian Cancer
Statistics 2011. Toronto, ON: Canadian Cancer Society; 2011.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
108
Cantril, H. (1965). The Pattern of Human Concerns. New Brunswick, N.J. Rutgers
University Press.
Cella, D.F., & Bonomi, A.E. (1995). Measuring quality of life: 1995 update. Oncology
(Williston Park), 9 (suppl): 47-60
Center for Disease Control. (2011). Health-Related Quality of Life (HRQOL). Retrieved
from http://www.cdc.gov/hrqol/concept.htm. Accessed September 10, 2012.
Davis, E., Nicolas, C., Waters, E., Cook, K., Gibbs, L., Gosch, A., & Ravens-Sieberer, U.
(2007). Parent-proxy and child self-reported health-related quality of life: using
qualitative methods to explain the discordance. Qual Life Res, 16(5):863-71.
Deliganis, A.V., Geyer, J.R., & Berger, M.S. (1996). Prognostic significance of type 1
neurofibromatosis (von Recklinghausen Disease) in childhood optic glioma.
Neurosurgery, 38(6):1114-1118
Dowie, J. (2002). Decision validity should determine whether a generic or condition-
specific HRQL measure should be used in health care decisions. Health Economics, 1:21-
22.
Eiser, C., Eiser, J.R., & Stride, C.B. (2005). Quality of life in children newly diagnosed
with cancer and their mothers. Health Qual Life Outcomes, 3: 29.
Fayed, N., Schiariti, V., Bostan, C., Cieza, A., & Klassen, A. (2012). Health status and
QOL instruments used in childhood cancer research: deciphering conceptual content
using World Health Organization definitions. Qual Life Res, 20(8):1247-58. doi:
10.1007/s11136-011-9851-5.
Feeny, D., Furlong, W., Boyle, M., & Torrance, G.W. (1995). Multi-attribute health
status classification systems: health utilities index. Pharmacoeconomics, 7:490-502.
Feeny, D., Furlong, W., Mulhern, R.K., Barr, R.D., & Hudson, M. A. (1999). A
framework for assessing health-related quality of life among children with cancer. Int J
Cancer Suppl,12:2-9.
Feeny, D., Furlong, W., Torrance, G.W., Goldsmith, C.H., Zhu, Z., DePauw, S., Denton,
M., & Boyle, M. (2002). Multiattribute and single-attribute utility functions for the health
utilities index mark 3 system. Med Care, 40(2):113-28.
Feng, Y., Bernier, J., McIntosh, C., & Orpana, H. (2009). Validation of disability
categories derived from Health Utilities Index Mark 3 scores. Health Reports, 20(2):43-
50.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
109
Fluchel, M., Horsman, J.R., Furlong, W., Castillo, L., Alfonz, Y., & Barr, R.D. (2008).
Self and proxy-reported health status and health-related quality of life in survivors of
childhood cancer in Uruguay. Pediatr Blood Cancer, 50(4):838-43.
Fryback, D. G, Dunham, N.C., Palta, M., Hanmer, J., Buechner, J., Cherepanov, D.,
Herrington, S. A., Hays, R.D., Kaplan, R. M., Ganiats, T.G., Feeny, D., & Kind, P.
(2007). US Norms for Six Generic Health-Related Quality-of-Life Indexes From the
National Health Measurement Study. Medical Care, 45(12):1162-1170.
Fu, L., Talsma, D., Baez, F., Bonilla, M., Moreno, B., Ah-Chu, M., Pena, A., Furlong,
W., & Barr, R.D. (2006). Measurement of health-related quality of life in survivors of
cancer in childhood in Central America: feasibility, reliability, and validity. J Pediatr
Hematol Oncol, 28(6):331-41.
Furlong, W.J., Feeny, D.H., & Torrance, G.W. (1998). Health Utilities Index (HUI®)
Procedures Manual: Algorithm for determining HUI Mark 2 (HUI2) / Mark 3 (HUI3)
health status classification level, health states, single-attribute level utility scores and
overall health-related quality of life utility scores from 40-item interviewer-administered
health status questionnaires, Health Utilities Inc.
Furlong, W.J., Feeny, D.H., Torrance, G.T., & Barr, R.D. (2001) The Health Utilities
Index (HUI®) system for assessing health-related quality of life in clinical studies. Ann
Med, 33: 375-384.
Gayre, G.S., Scott, I.U., Feuer, W., Saunders, T.G., & Siatkowski, R.M. (2001) Long-
term visual outcome in patients with anterior visual pathway gliomas. J Neuroophthalmol.
21(1):1-7.
Glaser, A.W., Furlong, W., Walker, D.A., Fielding, K., Davies, K., Feeny, D.H., & Barr,
R.D. (1999). Applicability of the Health Utilities Index to a population of childhood
survivors of central nervous system tumours in the UK. Eur J Cancer, 35: 256-261.
Goldbeck, L., & Melches, J. (2005). Quality of life in families of children with congenital
heart disease. Qual Life Res, 14(8):1915-24.
Gragert, M.N., & Ris, M.D. (2011). Neuropsychological late effects and rehabilitation
following pediatric brain tumor. J Pediatr Rehabil Med, 4(1):47-58.
Grigsby, J., Rosenberg, N.L., & Busenbark, D. (1995). Chronic pain is associated with
deficits in information processing. Percept Mot Skills. 81(2):403-10.
Gurney, J.G., Krull, K.R., Kadan-Lottick, N., Nicholson, H.S., Nathan, P.C., Zebrack, B.,
Tersak, J.M., & Ness, K.K. (2009). Social outcomes in the Childhood Cancer Survivor
Study cohort. J Clin Oncol, 27(14):2390-5.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
110
Gurney, J.G., Smith, M.A., & Bunin, G.R. (1999). CNS and miscellaneous intracranial
and intraspinal neoplasms. In: Ries LA, Smith MA, Gurney JG, et al., eds.: Cancer
incidence and survival among children and adolescents: United States SEER Program
1975-1995. Bethesda, Md: National Cancer Institute, SEER Program. NIH Pub.No. 99-
4649., Chapter 3, pp 51-63
Hart, R.P., Martelli, M.F., & Zasler, N.D. (2000). Chronic pain and neuropsychological
functioning. Neuropsychol Rev, 10(3):131-49.
Hays, D.M., Landsverk, J., Sallan, S.E., Hewett, K.D., Patenaude, A.F., Schoonover, D.,
Zilber, S.L., Ruccione, K., & Siegel, S.E. Educational, occupational, and insurance status
of childhood cancer survivors in their fourth and fifth decades of life. J Clin Oncol. 1992
Sep;10(9):1397-406.
Health Utilitis Inc. (2011). References. Retrieved from http://www.healthutilities.com/.
Accessed May 31, 2013.
Heimans, J.J., & Taphoorn, M.J. (2002). Impact of brain tumour treatment on quality of
life. J Neurol, 249(8):955-60.
Hopman, W.M., Towheed, T., Anastassiades, T., Tenenhouse, A., Poliquin, S., Berger,
C., Joseph, L., Brown, J.P., Murray, T.M., Adachi, J.D., Hanley, D.A., &
Papadimitropoulos, E. (2000). Canadian normative data for the SF-36 health survey.
Canadian Multicentre Osteoporosis Study Research Group. CMAJ,163(3):265-71.
Horsman, J.R., Furlong, W.J., Feeny, D.H., & Torrance, G.W. (2003). The Health
Utilities Index (HUI®): Concepts, measurement properties and applications. Health Qual
Life Outcomes (electronic journal) (Vol. 1: 54, October 16, 2003), at
http://www.hqlo.com/content/1/1/54
Horsman, J., Duckworth, J., Rae, C., Furlong, W., Hsu, T., Spitzer, R., & Barr, R. (2007
October). Proxy-Rater Reliability in a Follow-Up Study of Health Status in Childhood
Brain Tumour Survivors using the Health Utilities Index Mark 3 (HUI3). Poster presented
at the 14th
Annual Conference of the International Society of Quality of Life Research,
Toronto, Ontario.
Horsman, J.R., Furlong, B., Spitzer, R., Hsu, T., Duckworth, J., & Barr, R.D. (2006
October). Reliability and Validity of Health Utilities Index (HUI®) Scores for Survivors
of Brain Tumours in Childhood in Canada: Agreement between patients and parents.
Poster presented at the 9th
Annual European Congress of International Society for
Pharmacoeconomics and Outcomes Research, Copenhagen, Denmark.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
111
Hovén, E., Lannering, B., Gustafsson, G., & Boman, K.K. (2011). The met and unmet
health care needs of adult survivors of childhood central nervous system tumors: a
double-informant, population-based study.The met and unmet health care needs of adult
survivors of childhood central nervous system tumors: a double-informant, population-
based study. Cancer, 15;117(18):4294-303. doi: 10.1002/cncr.26020.
Hudson, M.M., Mertens, A.C., Yasui, Y., Hobbie, W., Chen, H., Gurney, J.G., Yeazel,
M., Recklitis, C.J., Marina, N., Robison, L.R., Oeffinger, K.C. & Childhood Cancer
Survivor Study Investigators. (2003). Health status of adult long-term survivors of
childhood cancer: a report from the Childhood Cancer Survivor Study. JAMA,
290(12):1583-92.
Imbach, P. (2006). Pediatric Oncology: A Comprehensive Guide. In P. Imbach, T. Kuhne
& R. Arceci (Eds). Brain Tumours (pp 95-117). Germany: Springer-Verlag Berlin
Heidelberg
Jemal, A., Clegg, L.X., Ward, E., Ries, L.A., Wu, X., Jamison, P.M., Wingo, P.A., Howe,
H.L., Anderson, R.N., & Edwards, B.K. (2004). Annual report to the nation on the status
of cancer 1975-2001, with a special feature regarding survival. Cancer, 101, 3-27.
Jenkinson, C., Wright, L., & Coulter, A. (1994). Criterion validity and reliability of the
SF-36 in a population sample. Qual Life Res, 3(1):7-12.
Johnson, D.L., McCabe, M.A., Nicholson, H.S., Joseph, A.L., Getson, P.R., Byrne, J.,
Brasseux, C., Packer, R.J., & Reaman, G. (1994). Quality of long-term survival in young
children with medulloblastoma. J Neurosurg, 80(6):1004-10.
Jurbergs, N., Russell, K.M., Long, A., & Phipps, S. (2008). Adaptive style and
differences in parent and child report of health-related quality of life in children with
cancer. Psychooncology, 17(1):83-90.
Kadan-Lottick, N.S., Dinu, I., Wasilewski-Masker, K., Kaste, S., Meacham, L.R.,
Mahajan, A., Stovall, M., Yasui, Y., Robison, L.L., & Sklar, C.A. (2008). Osteonecrosis
in adult survivors of childhood cancer: a report from the childhood cancer survivor study.
J Clin Oncol, 26(18):3038-45.
Khanna, D. (2006). Health-related quality of life: a primer with a focus on scleroderma.
Scleroderma Care Res, 3:3-13
King, J.T. Jr, Tsevat, J., Moossy, J.J., & Roberts, M.S. (2004). Preference-based quality
of life measurement in patients with cervical spondylotic myelopathy. Spine,
29(11):1271-80.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
112
King’s College London. (2013). Statistics Advisory Service. Frequently Asked Questions
No. 9 Retrieved from
http://www.kcl.ac.uk/iop/depts/biostatistics/advisory/faqs9.aspx#a9_5. Accessed May 31,
2013.
Klassen, A.F., Anthony, S.J., Khan, A., Sung, L., & Klaassen, R. (2011). Identifying
determinants of quality of life of children with cancer and childhood cancer survivors: a
systematic review. Support Care Cancer. 2011 Sep;19(9):1275-87. doi: 10.1007/s00520-
011-1193-x. Epub 2011 May 25
Kleihues, P., Burger, P.C., & Scheithauer, B.W. (1993). The new WHO classification of
brain tumours. Brain Pathol, 3(3):255-68.
Koch, S. V., Kejs, A.M.T., Engholm, G., Johansen, C., & Schmiegelow, K. (2004).
Educational attainment among survivors of childhood cancer: a population-based cohort
study in Denmark. Br J Cancer, 91(5): 923–928.
Kopec, J.A., Williams, J.I., To, T., & Austin, P.C. (2000). Measuring population health:
correlates of the Health Utilities Index among English and French Canadians. Can J
Public Health, 91(6):465-70.
Kramárová, E., & Stiller, C.A. (1996). The international classification of childhood
cancer. Int J Cancer, 68(6):759-65.
Lancashire, E.R., Frobisher, C., Reulen, R.C., Winter, D.L., Glaser, A., & Hawkins,
M.M. (2010). Educational attainment among adult survivors of childhood cancer in Great
Britain: a population-based cohort study. J Natl Cancer Inst. 102(4):254-70.
Landgraf, J.M., Abetz, L., & Ware, J.E. (1996). The Child Health Questionnaire (CHQ): a
user's manual. The Health Institute, New England Medical Center, Boston.
Landis, J.R., & Koch, G.G. (1977). The measurement of observer agreement for
categorical data. Biometrics, 33(1):159-74.
Langeveld, N.E., Ubbink, M.C., Last, B.F., Grootenhuis, M.A., Voûte, P.A., & De Haan,
R.J. (2003). Educational achievement, employment and living situation in long-term
young adult survivors of childhood cancer in the Netherlands. Psychooncology,
12(3):213-25.
Lannering, B., Marky, I., Lundberg, A., & Olsson, E. (1990). Long-term sequelae after
pediatric brain tumors: their effect on disability and quality of life. Med Pediatr Oncol,
18(4):304-10.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
113
Lawrence, Y.R., Li, X.A., el Naqa, I., Hahn, C.A., Marks, L.B., Merchant, T.E., &
Dicker, A.P. (2010). Radiation dose-volume effects in the brain. Int J Radiat Oncol Biol
Phys, 76:S20-7.
Levinson, W., & Roter, D. (1995). Physicians' psychosocial beliefs correlate with their
patient communication skills. J Gen Intern Med, 10(7):375-9.
Lu, Q., Krull, K.R., Leisenring, W., Owen, J.E., Kawashima, T., Tsao, J.C., Zebrack, B.,
Mertens, A., Armstrong, G.T., Stovall, M., Robison, L.L., & Zeltzer, L.K. (2011). Pain in
long-term adult survivors of childhood cancers and their siblings: a report from the
Childhood Cancer Survivor Study. Pain, 152(11):2616-24. Epub 2011 Sep 9.
Luo, N., Johnson, J.A., Shaw, J.W., Feeny, D., & Coons, S.J. (2005). Self-reported health
status of the general adult U.S. population as assessed by the EQ-5D and Health Utilities
Index. Med Care, 43(11):1078-86.
Mason, W.P., Grovas, A., Halpern, S., Dunkel, I.J., Garvin, J., Heller, G., Rosenblum, M.,
Gardner, S., Lyden, D., Sands, S., Puccetti, D., Lindsley, K., Merchant, T.E., O'Malley,
B., Bayer, L., Petriccione. M.M., Allen, J., & Finlay, J.L. (1998). Intensive chemotherapy
and bone marrow rescue for young children with newly diagnosed malignant brain
tumors. J Clin Oncol, 16:210-221.
Maunsell, E., Pogany, L., Barrera, M., Shaw, A.K., & Speechley, K.N. (2006). Quality of
life among l ng-term adolescent and adult survivors of childhood cancer. J Clin Oncol,
24(16):2527-35.
McGrath, P.A., Seifert, C.E., Speechley, K.N., Booth, J.C., Stitt, L., & Gibson, M.C.
(1996). A new analogue scale for assessing children’s pain: An initial validation study.
Pain, 64: 435-443.
McHorney, C.A. (1999). Health status assessment methods for adults: past
accomplishments and future challenges. Annual Rev Public Health, 20:309-35.
Morren, M., van Dulmen, S., Ouwerkerk, J., & Bensing, J. (2009). Compliance with
momentary pain measurement using electronic diaries: a systematic review. Eur J Pain,
13(4):354-65
Mostow, E.N., Byrne, J., Connelly, R.R., & Mulvihill, J.J. (1991). Quality of life in long-
term survivors of CNS tumors of childhood and adolescence. J Clin Oncol, 9(4):592-9.
Mulhern, R.K., & Palmer, S.L. (2003). Neurocognitive late effects in pediatric cancer.
Curr Probl Cancer, 27: 177–197.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
114
Mulhern, R.K., Hancock, J., Fairclough, D., & Kun, L. (1992). Neuropsychological status
of children treated for brain tumors: a critical review and integrative analysis. Med
Pediatr Oncol, 20(3):181-91.
Mulhern, R.K., Kepner, J.L., Thomas, P.R., Armstrong, F.D., Friedman, H.S., & Kun,
L.E. (1998). Neuropsychologic functioning of survivors of childhood medulloblastoma
randomized to receive conventional or reduced-dose craniospinal irradiation: a Pediatric
Oncology Group Study. J Clin Oncol, 16: 1723–1728.
Mulhern, R.K., Reddick, W.E., Palmer, S.L., Glass, J.O., Elkin, T.D., Kun, L.E., Taylor,
J., Langston, J., & Gajjar, A. (1999). Neurocognitive deficits in medulloblastoma
survivors and white matter loss. Ann Neurol, 46(6):834-41.
Nampiaparampil, D.E. (2008). Prevalence of chronic pain after traumatic brain injury: a
systematic review. JAMA, 300(6):711-9
National Cancer Institute. (2007). The Childhood Cancer Survivor Study: An Overview.
Retrieved from http://www.cancer.gov/cancertopics/coping/ccss. Accessed November 11,
2012.
National Cancer Institute. (2009). SEER Cancer Statistics Review 1975-2009- Table 29.6
5-Year Relative Survival (Percent), 2002-2008 By International Classification of
Childhood Cancer(ICCC)b Selected Group and Subgroupc and Sex and Age. Retrieved
from
http://seer.cancer.gov/csr/1975_2009_pops09/browse_csr.php?section=29&page=sect_29
_table.06.html. Accessed March 11, 2013.
National Cancer Institute. (2012). About Cancer Survivorship Research: Cancer
Survivorship Definitions. Cancer Control and Population Sciences: Office of Cancer
Survivorship. Retrieved from http://cancercontrol.cancer.gov/ocs/definitions.html.
Accessed October 20, 2012.
Ness, K.K., Mertens, A.C., Hudson, M.M., Wall, M.M., Leisenring, W.M., Oeffinger,
K.C., Sklar, C.A., Robison, L.L., & Gurney, J.G. (2005). Limitations on physical
performance and daily activities among long-term survivors of childhood cancer. Ann
Intern Med, 143(9):639-47.
Nixon Speechley, K., Maunsell, E., Desmeules, M., Schanzer, D., Landgraf, J.M., Feeny,
D.H., Barrera, M.E. (1999). Mutual concurrent validity of the child health questionnaire
and the health utilities index: an exploratory analysis using survivors of childhood cancer.
Int J Cancer Suppl, 12:95-105.
Norman, G.R., & Streiner, D.L. (2007). Biostatistics: The Bare Essentials (3rd edition).
Hamilton, Canada: B.C. Decker.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
115
Oeffinger, K.C., Eshelman, D.A., Tomlinson, G.E., Tolle, M., & Schneider, G.W. (2000).
Providing primary care for long-term survivors of childhood acute lymphoblastic
leukemia. J Fam Pract, 49(12):1133-46.
Oeffinger, K.C., Mertens, A.C., Sklar, C.A., Kawashima, T., Hudson, M.M., Meadows,
A.T., Friedman, D.L., Marina, N., Hobbie, W., Kadan-Lottick, N.S., Schwartz, C.L.,
Leisenring, W., & Robison, L.L. (2006). Childhood Cancer Survivor Study. Chronic
health conditions in adult survivors of childhood cancer. N Engl J Med, 355(15):1572-82.
Osoba, D. (2011). Health-Related Qualithy of Life and Cancer Clinical Trials. Ther Adv
Med Oncol. 2011 March; 3(2): 57–71. doi: 10.1177/1758834010395342
Packer, R.J. (2008). Childhood brain tumors: accomplishments and ongoing challenges. J
Child Neurol,23(10):1122-7.
Packer, R.J., Gurney, J.G., Punyko JA, Donaldson, S.S., Inskip, P.D., Stovall, M., Yasui,
Y., Mertens, A.C., Sklar, C.A., Nicholson, H.S., Zeltzer, L.K., Neglia, J.P., & Robison,
L.L. (2003). Long-term neurologic and neurosensory sequelae in adult survivors of a
childhood brain tumor: childhood cancer survivor study. J Clin Oncol, 21: 3255–3261
Pang, J.W., Friedman, D.L., Whitton, J.A., Stovall, M., Mertens, A.C., Robison, L.L., &
Weiss, N.S. (2008). Employment status among adult survivors in the Childhood Cancer
Survivor Study. Pediatr Blood Cancer, 50(1):104-10.
Patrick, D.L., & Erickson, P. (1993). Health status and health policy: quality of life in
helth care evaluation and resource allocation. New York: USA: Oxford University Press.
Pediatric Oncology Group of Ontario. (2006). Provincial Pediatric Oncology AfterCare
Program. Retrieved from http://www.pogo.ca/care/aftercareclinics. Accessed October 20,
2012.
Penn, A., Lowis, S.P., Stevens, M.C., Shortman, R.I., Hunt, L.P., McCarter, R.J., Curran,
A.L., & Sharples, P.M. (2011). A detailed prospective longitudinal assessment of health
status in children with brain tumors in the first year after diagnosis. J Pediatr Hematol
Oncol, 33(8):592-9.
Phipps, S., & Srivastava, D.K. (1997). Repressive adaptation in children with cancer.
Health Psychol. 16(6):521-8.
Phipps, S., Steele, R.G., Hall, K., & Leigh, L. (2001). Repressive adaptation in children
with cancer: a replication and extension. Health Psychol, 20(6):445-51.
Pogany, L., Barr, R.D., Shaw, A., Speechley, K.N., Barrera, M., & Maunsell, E. (2006).
Health status in survivors of cancer in childhood and adolescence. Qual Life Res.
15(1):143-57.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
116
Pollack, I.F. (2008). Diagnostic and therapeutic stratification of childhood brain tumors:
implications for translational research. J Child Neurol, 23(10):1179-85.
Raat, H., Bonsel, G.J., Essink-Bot, M.L., Landgraf, J.M., & Gemke, R.J. (2002).
Reliability and validity of comprehensive health status measures in children: The Child
Health Questionnaire in relation to the Health Utilities Index. J Clin Epidemiol, 55(1):67-
76.
Radcliffe, J., Packer, R.J., Atkins, T.E., Bunin, G.R., Schut, L., Goldwein, J.W., &
Sutton, L.N. (1992). Three- and four-year cognitive outcome in children with noncortical
brain tumors treated with whole-brain radiotherapy. Ann Neurol, 32(4):551-4.
Recklitis, C., O’Leary, T., & Diller, L. (2003). Utility of routine psychological screening
in the childhood cancer survivor clinic. J Clin Oncol; 21(5):787-792
Reulen, R.C., Winter, D.L., Lancashire, E.R., Zeegers, M.P., Jenney, M.E., Walters, S.J.,
Jenkinson, C., & Hawkins, M.M. (2007). Health-status of adult survivors of childhood
cancer: a large-scale population-based study from the British Childhood Cancer Survivor
Study. Int J Cancer, 121(3):633-40.
Reulen, R.C., Zeegers, M.P., Jenkinson, C., Lancashire, E.R., Winter, D.L., Jenney, M.E.,
& Hawkins, M.M. (2006). The use of the SF-36 questionnaire in adult survivors of
childhood cancer: evaluation of data quality, score reliability, and scaling assumptions.
Health Qual Life Outcomes, 4:77.
Rubin, D.B. (1987). Multiple Imputation for Nonresponse in Surveys. New York, USA:
Wiley.
Rubin, D.B. (1996). Multiple imputation after 18+ years. Journal of the American
Statistical Association, 91, 473-489.
Ruxton, G. (2006). The unequal variance t-test is an underused alternative to Student's t-
test and the Mann--Whitney U test. Behavioral Ecology, 17;4: 688-690.
Sands, S. A., Kellie, S. J., Davidow, A. L., Diez, B., Villablanca, J., Weiner, H. L.,
Pietanza, M. C., Balmaceda, C. & Finlay, J. L. (2001). Long-term quality of life and
neuropsychologic functioning for patients with CNS germ-cell tumors: from the First
International CNS Germ-Cell Tumor Study. Neuro Oncol, 3(3): 174–183.
Sawyer, M., Antoniou, G., Toogood, I., & Rice, M. (1999). A comparison of parent and
adolescent reports describing the health-related quality of life of adolescents treated for
cancer. Int J Cancer Suppl; 12:39-45.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
117
Schwartz, C.E., & Sprangers, M.A. (1999). Methodological approaches for assessing
response shift in longitudinal health-related quality-of-life research. Soc Sci Med,
48(11):1531-48.
SF-36.org. FAQ's. Retrieved from http://www.sf-36.org/faq/condition.aspx?id=4.
Accessed October 27, 2012
Sherman, K.B., Goldberg, M., & Bell, K.R. (2006). Traumatic brain injury and pain. Phys
Med Rehabil Clin N Am, 17(2):473-90, viii.
Singer A.J., Kowalska A., & Thode H.C. Jr. (2001) Ability of patients to accurately recall
the severity of acute painful events. Acad Emerg Med; 8(3):292-5.
Smith, M.A., Seibel, N.L., Altekruse, S.F., Ries, L.A., Melbert, D.L., O'Leary, M., Smith,
F.O., & Reaman, G.H. (2010). Outcomes for children and adolescents with cancer:
challenges for the twenty-first century. J Clin Onco; 28(15):2625-34. doi:
10.1200/JCO.2009.27.0421. Epub 2010 Apr 19.
Sonderkaer, S., Schmiegelow, M., Carstensen, H., Nielsen, L.B., Muller, J., &
Schmiegelow, K. (2003). Long-term neurological outcome of childhood brain tumors
treated by surgery only. J Clin Oncol, 21(7):1347-1351.
Sorbi, M.J., Peters, M.L., Kruise, D.A., Maas, C.J., Kerssens, J.J., Verhaak, P.F., &
Bensing, J.M. (2006). Electronic momentary assessment in chronic pain I: psychological
pain responses as predictors of pain intensity. Clin J Pain, 22(1):55-66.
Sprangers, M.A., & Schwartz, C.E. (1999). Integrating response shift into health-related
quality of life research: a theoretical model. Soc Sci Med, 48(11):1507-15.
SPSS. (2005). Linear Mixed-Effects Modeling in SPSS: An Introduction to the MIXED
Procedure. Retrieved from
http://www.spss.ch/upload/1126184451_Linear%20Mixed%20Effects%20Modeling%20i
n%20SPSS.pdf. Accessed Octobor 20, 2012.
Statistics Canada. (2007). National Population Health Survey: Health Institutions
Component, Longitudinal (NPHS). Retrieved from
http://www23.statcan.gc.ca/imdb/p2SV.pl?Function=getSurvey&SDDS=5003&lang=en
&db=imdb&adm=8&dis=2#b5. Accessed August 6, 2012.
Orpana, H.M., Ross, N., Feeny, D., Bentson, M., Bernier, J. & Kaplan, M.S. (2009). The
Natural History of Health-Related Quality of Life: A 10-year Cohort Study. Health
Reports, 20 (1): 29-35.
Steliarova-Foucher, E., Stiller, C., Lacour, B., & Kaatsch, P. (2005). International
Classification of Childhood Cancer, third edition. Cancer, 103(7):1457-67.

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
118
Sterne, J.A., White, I.R., Carlin, J.B., Spratt, M., Royston, P., Kenward, M.G., Wood,
A.M., & Carpenter, J.R. (2009). Multiple imputation for missing data in epidemiological
and clinical research: potential and pitfalls. BMJ, 338:2393.
Streiner, D.L., & Norman, G.R. (2008). Health Measurement Scales: A Practical Guide to
their Development and Use. (4th edition). New York, USA: Oxford University Press.
Sung, L., Greenberg, M.L., Doyle, J.J., Young. N.L., Ingber, S., Rubenstein, J., Wong, J.,
Samanta, T., McLimont, M., & Feldmanm B.M. (2003). Construct validation of the
Health Utilities Index and the Child Health Questionnaire in children undergoing cancer
chemotherapy. Br J Cancer; 88(8):1185-90.
Tao, M.L., & Parsons, S.K. (2005). Quality-of-Life Assessment in Pediatric Brain Tumor
Patients and Survivors: Lessons Learned and Challenges to Face. Journal of Clinical
Oncology, 23 (24): 5424-5426
The WHOQOL Group (1995). The World Health Organization Quality of Life
Assessment (WHOQOL): Position paper from the World Health Organization. Soc Sci
Med, 41:1403-1409
Torrance, G.W ., Feeny, D.H., Furlong, W.J., Barr, R.D., Zhang, Y., & Wang Q. (1996).
Multiattribute Utility Function for a Comprehensive Health Status Classification System:
Health Utilities Index Mark 2. Medical Care; 34 (7): 702-722.
Trudel, J.G., Rivard, M., Dobkin, P.L., Leclerc, J.M. & Robaey P. (1998). Psychometric
properties of the Health Utilities Index Mark 2 system in paediatric oncology patients.
Qual Life Res, 7(5):421-32.
Tsevat, J. (2000). What do utilities measure? Med Care, 38 (suppl):II 160-II 164
Tsevat, J., Weeks, J.C., Guadagnoli, E., Tosteson, A.N., Mangione, C.M., Pliskin, J.S.,
Weinstein, M.C., & Cleary, P.D. (1994). Using health-related quality-of-life information:
clinical encounters, clinical trials, and health policy. J Gen Intern Med, 9(10):576-82.
Turk, D.C., Dworkin, R.H., Allen, R.R., Bellamy, N., Brandenburg, N., Carr, D.B.,
Cleeland, C., Dionne, R., Farrar, J.T., Galer, B.S., Hewitt, D.J., Jadad, A.R., Katz, N.P.,
Kramer, L.D., Manning, D.C., McCormick ,C.G., McDermott, M.P., McGrath, P.,
Quessy, S., Rappaport, B.A., Robinson, J.P., Royal, M.A., Simon, L., Stauffer, J.W.,
Stein, W., Tollett, J., & Witter, J. (2003). Core outcome domains for chronic pain clinical
trials: IMMPACT recommendations. Pain, 106(3):337-45.
Turner, C.D., Rey-Casserly, C., Liptak, C.C., & Chordas, C. (2009). Late effects of
therapy for pediatric brain tumor survivors. J Child Neurol, 24(11):1455-63

M.Sc. Thesis - T. Nayiager; McMaster University – Health Research Methodologies
119
Twombly, R. (2009). Pediatric brain tumor survivors, physicians, and researchers face
long-term challenges. J Natl Cancer Inst, 101(13):908-10.
Varni, J.W. (2013). The PedsQL- Measurement Model for the Pediatric Quality of Life
Inventory. Retrieved from http://www.pedsql.org/about_pedsql.html. Accessed October
22, 2012
Varni, J.W., Burwinkle, T.M., Katz, E.R., Meeske, K., & Dickinson, P. (2002). The
PedsQL in pediatric cancer: reliability and validity of the Pediatric Quality of Life
Inventory Generic Core Scales, Multidimensional Fatigue Scale, and Cancer Module.
Cancer, 94(7):2090-106.
Ware, J.E., Jr., Brook, R.H., Davies, A.R. & Lohr, K.N. (1981). Choosing measures of
health status for individuals in general populations. Amer. J. publ. Health, 71, 620-625 .
Ware, J.E. Jr, & Gandek B. (1998). Overview of the SF-36 Health Survey and the
International Quality of Life Assessment (IQOLA) Project. J Clin Epidemiol, 1(11):903-
12.
Waters, E., Davis, E., Ronen, G.M., Rosenbaum, P., Livingston, M., & Saigal, S. (2009).
Quality of life instruments for children and adolescents with neurodisabilities: how to
choose the appropriate instrument. Dev Med Child Neurol, 51(8):660-9. doi:
10.1111/j.1469-8749.2009.03324.x.
Wennberg, J.E. (1990). Outcomes research, cost containment, and the fear of health care
rationing. N Eng J Med, 323:1202-4
Whitton, A.C., Rhydderch, H., Furlong W, Feeny, D., & Barr, R.D. (1997). Self-reported
comprehensive health status of adult brain tumour patients using the Health Utilities
Index. Cancer, 80: 258-265.
World Health Organisation. (1992). International Classification of Diseases for Oncology,
3rd Edition (ICD-O-3). Geneva, Switzerland: World Health Organisation.
Zebrack, B.J., & Zeltzer, L.K. (2003). Quality of life issues and cancer survivorship. Curr
Probl Cancer, 27: 198-211.
Zeltzer, L.K., Lu, Q., Leisenring, W., Tsao, J.C., Recklitis, C., Armstrong, G., Mertens,
A.C., Robison, L.L., & Ness, K.K. (2008). Psychosocial outcomes and health-related
quality of life in adult childhood cancer survivors: a report from the childhood cancer
survivor study. Cancer Epidemiol Biomarkers Prev, 435-46.
Zeltzer, L.K., Recklitis, C., Buchbinder, D., Zebrack, B., Casillas, J., Tsao, J.C., Lu, Q.,
& Krull, K. (2009). Psychological status in childhood cancer survivors: a report from the
Childhood Cancer Survivor Study. J Clin Oncol, 27(14):2396-404.





























