Embed Size (px)
Citation preview

ELSEVIER Drug and Alcohol Dependence 38 (1995) 35-43
An examination of the cocaine relapse process
James R. McKay *, Megan J. Rutherford, Arthur I. Alterman, John S. Cacciola, Mara R. Kaplan
Department of Psychiatry, University of Pennsylvania, Philadelphia, PA, USA
Received 7 September 1994; accepted 30 December 1994
Abstract
Although empirical studies of the relapse process have been done with alcoholics, smokers, and opiate addicts, comparatively little information is available on the relapse process in cocaine abusers. This paper presents data from the Cocaine Relapse Inter- view (CRI), a structured interview that assesses factors associated with the onset, course, and termination of cocaine relapse episodes. In a sample of 95 cocaine dependent patients, the experiences that occurred with the greatest frequency immediately prior to relapse were wanting drugs, being alone, having money, and feeling extremely bored and lonely. Following the onset of the re- lapse, the most frequent experience was unpleasant affect, although positive reactions were also relatively common. The factors perceived as most important in terminating relapse were painful internal states, help-seeking behaviors, and other coping responses. Three types of relapse experiences, or pathways, were identified: (a) unpleasant affect - painful internal states prior to and throughout the relapse; (b) positive affect -positive affect and pleasant social experiences prior to relapse coupled with a relatively unproblematic course; and (c) sensation seeking - sensation seeking and interpersonal problems prior to relapse coupled with mixed emotional reactions and antisocial behavior during the relapse, and interpersonal problems at relapse termination.
Keywords: Cocaine; Relapse; Onset; Course; Termination; Typology
1. Introduction
Although treatments for drug abuse frequently pro- duce decreases in psycho-social and substance use prob- lem severity (Tims et al., 1991; Alterman et al., 1994), a significant percentage of substance abusers begin to abuse their drug of choice again relatively quickly (Hunt et al., 1971; Brownell et al., 1986). Cocaine abusers ap- pear to be particularly prone to relapse (Washton and Stone-Washton, 1990).
In the clinical literature, cocaine relapses have been linked to a number of factors, including negative mood, self-pity, impulsiveness, idealizing the cocaine high, a desire to test control over cocaine, entering high risk situations, relationship problems, untreated psychiatric disorders, and stressful life events (Wallace, 1989; Washton, 1989). A number of predictors of cocaine re-
* Corresponding author, University of Pennsylvania, Treatment Research Center, 3900 Chestnut St., Philadelphia, PA 19104, USA.
lapse have also been identified in prospective studies, in- cluding failure to complete treatment, psychopathology, absence of positive mood, lack of commitment to absti- nence, and low participation in self-help programs (Hall et al., 1991; Carroll et al., 1993; McKay et al., 1994a).
With other substances of abuse (e.g., alcohol, nico- tine, heroin), empirical analyses of relapse episodes have been undertaken through the use of detailed, retrospec- tive interviews. Marlatt and Gordon (1980) used this methodology to derive eight categories of relapse deter- minants, such as unpleasant and pleasant emotional states, interpersonal conflict, and social pressure to use. Retrospective interviews and questionnaires derived from these interviews have also been used to identify re- lapse precipitants of alcoholics in marital therapy, smokers, and opiate users (Shiffman, 1982; O’Connell and Martin, 1987; Baer and Lichtenstein, 1988; Maisto et al., 1988; Bradley et al., 1989; Heather et al., 1991). However, the experiences that immediately precede co- caine relapse episodes have not been systematically
0376-8716/95/%09.50 0 1995 Elsevier Science Ireland Ltd. All rights reserved SSDI 0376-8716(9S)OlO98-J

36 J. R. McKay et al. /Drug and Alcohol Dependence 38 (1995) 35-43
evaluated. Furthermore, there is little empirical infor- mation on the reactions and experiences of cocaine abusers after their initial use of cocaine during relapses, or the factors that contribute to the termination of relapses.
In this study, a structured interview was administered to a sample of 95 cocaine dependent patients to gather information on factors involved in the onset, course, and termination of cocaine relapses they had experienc- ed in the prior 18 months. This article presents data on experiences that were most common at each point of the relapse process. Relationships between experiences prior to relapse, experiences after the onset of the relapse, and factors in the termination of the relapse were also exam- ined in a preliminary attempt to identify different pathways through the cocaine relapse process.
2. Method
2.1. Subjects The subjects were 95 patients (65 men and 30 women)
who were participating in cocaine and alcohol treatment outcome studies at the University of Pennsylvania. All subjects met DSM-III-R criteria for cocaine depen- dence, based on a semi-structured diagnostic interview (SCID; Spitzer et al., 1989), and most subjects had histories of polydrug use. None of the subjects was receiving methadone. Virtually all the subjects were of lower socio-economic status, most were African-Amer- ican (83.2%), and 16.8% were white. All subjects were between the ages of 18 and 60. Additional demographic information was available on a subsample (N = 49) that was representative of the full sample in terms of gender and race’. Among subjects in the subsample, the mean age was 32.8 (S.D. = 7.4) and mean years of education was 11.8 (S.D. = 1.8); 26.5% were working 5 days or more per month; 6.1% were married, 38.7% were separated or divorced, and 55.1% had never married.
2.2. Assessment instruments Information on the onset, course and termination of
cocaine relapses was gathered with the Cocaine Relapse Interview (CRI) (McKay et al., 1994b). The CR1 is a structured interview, administered by trained research technicians, that takes approximately 30 min to com- plete. The interview consists of six sections: (1) basic descriptive information about the relapse; (2) the ex- periences of the subject on the day of the relapse, prior to using cocaine; (3) the experiences of the subject dur- ing the week prior to the relapse; (4) the attributions of the subject about what caused the relapse; (5) the ex-
’ Complete demographic and problem severity data was not avail- able on the full sample because information that was necessary to match data from the Cocaine Relapse Interview (CRI) to other data collected on the subjects was not recorded on the CRIs until almost the midpoint of the study.
periences of the subject after the onset of the relapse; and (6) the perceptions of the subject of factors that con- tributed to the termination of the relapse. This article makes use of data from all sections except the attribu- tion for relapse section. Attributions for cocaine relapse and the relationship between attributions and experi- ences will be addressed in another article.
An abbreviated description of the CR1 and its de- velopment will be provided here, as the instrument is fully described elsewhere (McKay et al., 1994b; copies of this manuscript are available from the first author). For each section of the CRI, an initial pool of items was generated from prior research on reasons for use (Marlatt and Gordon, 1980, 1985; Annis and Martin, 1985; Maisto et al., 1988), the clinical literature (Wal- lace, 1989), and discussions with clinicians. After pilot testing, these items were placed in preliminary subscales, which were subjected to internal consistency analysis. Items in each subscale were retained or deleted on the basis of item-total correlations and changes in coeffi- cients alpha.
In the sections of the CR1 that assess experiences prior to the onset of relapse, thirty-six items were re- tained and included in seven subscales: Unpleasant Af- fect, Positive Affect, Interpersonal Problems, Pleasant Social Experiences, Social Pressure to Use, Sensation Seeking, and Lack of Self-help Involvement. Thirteen additional items that were not included in any of the subscales were included in Life Stress and Other Poten- tial Cues for Relapse categories. Subjects indicate whether they experienced the item on the day of their re- lapse, prior to using (0, no; 1, yes). Subjects also rate the degree to which each item was occurring during the week prior to the day the relapse began (0, not at all; 1, a little; 2, some; 3, a fair amount; 4, a lot).
In the section that assesses the initial reactions and ex- periences of subjects after the onset of the relapse (i.e., the ‘course’ of the relapse), twenty-three items were re- tained and included in six subscales: Help Seeking, Unpleasant Affect, Positive/Appetitive Reactions, In- terpersonal Problems, Self-Justification, and Antisocial Behavior. Four additional items were included in Other Experiences Following Initial Use category. Subjects in- dicate the degree to which they experienced any of the items after they had started using cocaine on the first day of the relapse (0, not at all; 1, a little; 2, some; 3, a fair amount; 4, a lot).
The section of the CR1 that assesses the perceptions of the subjects of the factors that contributed to ending the relapse is only administered to subjects who have either been abstinent for at least two weeks since the end of the relapse or who ended the relapse by going into an inpatient treatment facility. In this section, twenty-two items were retained and included in six subscales: Pain- ful Internal States, Help-Seeking Behaviors, Other Coping Responses, Interpersonal Problems, Confronta-

J. R. McKay et al. /Drug and Alcohol Dependence 38 (1995) 35-43 31
tion by Others, and Lack of Availability of Cocaine. Three additional items were included in Other Factors in Termination category. Subjects rate the degree to which they believe each factor contributed to stopping their relapse (0, not at all important; 1, played a minor role; 2, somewhat important role; 3, moderately strong role; 4, played a major role).
In each section of the CRI, subscales scores are calculated by summing the scores from all items in the subscale. Mean scores are determined by dividing the subscale score by the number of items in the subscale. Initial information on the psychometric properties of the CR1 is presented in McKay et al. (1994b). Most of the subscales in each section had coefficients alpha of between 0.60 and 0.90, and test-retest reliabilities typically exceeded 0.60. Correlations between the subscales in each section were generally less than 0.40. Validity analyses demonstrated that six of the seven subscales that assess experiences prior to relapse dif- ferentiated cocaine patients who had relapsed from those who maintained abstinence. Three of six subscales in each of the sections that assess experiences following initial use of cocaine and factors involved in relapse ter- mination differentiated relapsers from lapsers (i.e., those with brief relapse episodes).
Drug and psychiatric problem severity at intake to treatment was assessed with the Drug and Psychiatric composite scores from the Addiction Severity Index (ASI; McLellan et al., 1980). These scores range from 0.00 to 1.00, with higher scores indicating greater prob- lem severity. AS1 data were available on 49 of the 95 subjects.
2.3. Procedure Cocaine-dependent subjects who were already par-
ticipating in other research projects were approached and screened to determine eligibility for the cocaine re- lapse study. Over 95% of patients approached were will- ing to participate. For the purposes of this study, a relapse was defined as one day or more of cocaine use, surrounded by abstinent periods of at least two weeks in duration, during a period in which the subject was trying to not use cocaine. Potential subjects were asked if they had quit using cocaine at some point in the last 18 months and then started using again after two weeks or more of abstinence. Those who met this criterion were also asked if they could clearly remember the circums- tances surrounding their resumption of cocaine use. Pa- tients who met both of these criteria were invited to participate. In cases where subjects had more than one cocaine relapse episode in the past 18 months, they were interviewed about the episode that they remembered the most vividly. All patients in the study had blood alcohol levels of 0.04 or less, as determined by breath tests, at the time they were interviewed.
3. Results
3.1. Descriptive information about cocaine relapses The cocaine relapse episodes of the subjects lasted an
average of 61.2 (S.D. = 66.9) days. During these relapses, cocaine was used on slightly more than half of the days (mean = 37.8, S.D.= 47.9). Twenty percent of the subjects had relapses that lasted one day. For relapses that lasted more than one day, the most fre- quent pattern of cocaine use was heavy use every day (42%) or a mix of heavy and abstinent days (18%). The most common route of administration was smoking (77%). Approximately half of the subjects were alone when their relapses began (45%), and about a third were with casual friends (28%) and/or acquaintances that they sometimes used drugs with (33%). Thirty-one percent of the subjects first thought seriously about using cocaine immediately before using, 24% an hour to a day before using, and 45% a day or more before using. More than half of the subjects reported they did not know for sure that they were going to use until an hour or less before the episode began (64%).
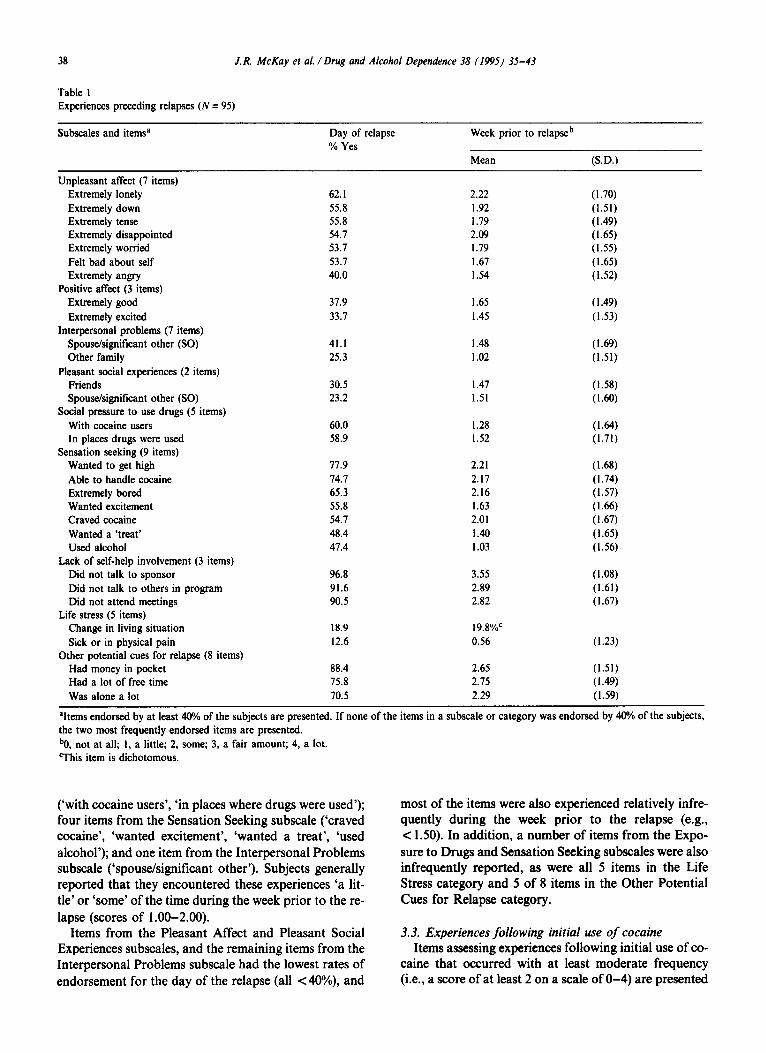
3.2. Onset of relapse Items that at least 40% of the subjects reported ex-
periencing on the day of their relapse, prior to using, are presented in Table 1. In cases where none of the items in a particular subscale or category was experienced by 40% of the subjects, the two most frequently reported items are presented*.
The following items pertaining to experiences the day of the relapse were endorsed by greater than 60% of the subjects: three items from the Sensation Seeking subscale (‘wanted to get high’, ‘able to handle cocaine’, and ‘was extremely bored’); one item from the Unplea- sant Affect subscale (‘was extremely lonely’); and three items from the Other Potential Cues for Relapse cate- gory (‘had money in pocket’, ‘had a lot of free time’, and ‘was alone a lot’). Not surprisingly, over 90% of the sub- jects also reported no self-help group involvement the day of their relapses. The reports of the subjects of ex- periences during the week prior to the day of the relapse generally yielded similar findings. Of all the items about experiences on the day of the relapse that were endorsed by more than 60% of the subjects, all were rated as hav- ing also occurred with at least moderate frequency ( 12 on a scale of O-4) during the week prior to the day of the relapse.
Experiences that were reported by 40-60% of the sub- jects on the day of their relapses included six items in the Unpleasant Affect subscale (‘disappointed’, ‘down’, ‘tense’, ‘worried’, ‘felt bad about self, ‘angry’); two items from the Social Pressure to Use Drugs subscale
2 Complete versions of Tables I, 2, and 3 with all CR1 items in- cluded are available from the first author.
38 J. R. McKay et al. /Drug and Alcohol Dependence 38 (1995) 35-43
Table 1 Experiences preceding relapses (N = 95)
Subscales and item? Day of relapse % Yes
Week prior to relapseb
Mean (S.D.)
Unpleasant affect (7 items) Extremely lonely 62.1 2.22 (1.70) Extremely down 55.8 I .92 (1.51) Extremely tense 55.8 1.79 (1.49) Extremely disappointed 54.7 2.09 (1.65) Extremely worried 53.7 1.79 (1.55) Felt bad about self 53.7 1.67 (1.65) Extremely angry 40.0 1.54 (1.52)
Positive affect (3 items) Extremely good 37.9 1.65 ( 1.49) Extremely excited 33.7 1.45 (1.53)
Interpersonal problems (7 items) Spouse/signiIicant other (SO) 41.1 1.48 (1.69) Other family 25.3 I .02 (1.51)
Pleasant social experiences (2 items) Friends 30.5 I .47 (1.58) Spouse/significant other (SO) 23.2 1.51 (1.W
Social pressure to use drugs (5 items) With cocaine users 60.0 1.28 (I.64 In places drugs were used 58.9 1.52 (1.71)
Sensation seeking (9 items) Wanted to get high 77.9 2.21 (1.68) Able to handle cocaine 74.7 2.17 (1.74) Extremely bored 65.3 2.16 (1.57) Wanted excitement 55.8 1.63 (1.W Craved cocaine 54.7 2.01 (1.67) Wanted a ‘treat’ 48.4 1.40 (1.65) Used alcohol 47.4 1.03 (1.56)
Lack of self-help involvement (3 items) Did not talk to sponsor 96.8 3.55 (1.08) Did not talk to others in program 91.6 2.89 (1.61) Did not attend meetings 90.5 2.82 (1.67)
Life stress (5 items) Change in living situation 18.9 19.8%c Sick or in physical pain 12.6 0.56 (1.23)
Other potential cues for relapse (8 items) Had money in pocket 88.4 2.65 (1.51) Had a lot of free time 75.8 2.75 (1.49) Was alone a lot 70.5 2.29 (1.59)
‘Items endorsed by at least 40% of the subjects are presented. If none of the items in a subscale or category was endorsed by 40% of the subjects, the two most frequently endorsed items are presented. bO, not at all; 1, a little; 2, some; 3, a fair amount; 4, a lot. This item is dichotomous.
(‘with cocaine users’, ‘in places where drugs were used’); four items from the Sensation Seeking subscale (‘craved cocaine’, ‘wanted excitement’, ‘wanted a treat’, ‘used alcohol’); and one item from the Interpersonal Problems subscale (‘spouse/significant other’). Subjects generally reported that they encountered these experiences ‘a lit- tle’ or ‘some’ of the time during the week prior to the re- lapse (scores of 1.00-2.00).
Items from the Pleasant Affect and Pleasant Social Experiences subscales, and the remaining items from the Interpersonal Problems subscale had the lowest rates of endorsement for the day of the relapse (all <40%), and
most of the items were also experienced relatively infre- quently during the week prior to the relapse (e.g., c 1.50). In addition, a number of items from the Expo- sure to Drugs and Sensation Seeking subscales were also infrequently reported, as were all 5 items in the Life Stress category and 5 of 8 items in the Other Potential Cues for Relapse category.
3.3. Experiences following initial use of cocaine Items assessing experiences following initial use of co-
caine that occurred with at least moderate frequency (i.e., a score of at least 2 on a scale of O-4) are presented

J. R. McKay er al. /Drug and Alcohol Dependence 38 (199s) 35-43 39
Table 2 Experiences following initial use of cocaine during relapse (N = 94)
Subscales and items” Mean b (S.D.)
Help seeking (4 items) Told others about your lapse I .22 (1.53) Went to self-help meetings 0.76 (1.46)
Unpleasant affect (4 items) Guilt feelings about initial cocaine use 3.50 (1.19) Feelings of having failed or ‘blown it’ 3.22 (1.29) Feelings of depression following initial use 2.83 (1.42) Feelings of anxiety following initial use 2.38 (1.W
Positive/appetitive reaction (4 items) Increased craving following initial use 2.35 (1.67) Enjoyed it so much you wanted more 2.24 (1.80)
Interpersonal problems (4 items) With other family because of initial use I.55 (1.76) With spouse/lover because of initial use I.51 (1.76)
Self-justification (4 items) Believed that you could control your cocaine use 2.49 (1.63) Had desire to say ‘to hell with it’ and take more cocaine 2.48 (1.66) You got away with initial use, so you could get away with more 2.28 (1.71)
Antisocial behavior (3 items) Had legal problems 0.55 (1.25) Engaged in illegal activities 0.33 (0.99)
Other experiences following initial use (4 items) Believed that any use meant you would relapse 2.41 (1.72) Used other drugs or alcohol I.59 (1.66)
%ems with scores of 2.00 or greater are presented. If none of the items in a subscale or category received a score of 2.00, the two items with the highest scores are presented. bO, not at all; I, a little; 2, some; 3, a fair amount; 4, a lot.
Table 3 Perceptions of factors involved in the termination of cocaine relapse (N = 75)
Subscales and items” Mean b (S.D.)
Painful internal states (2 items) Felt bad emotionally Felt bad physically
Help-see-king behavior (6 items) Asked for help Told others you were using again
Other coping responses (5 items) Knew things would get worse if you continued Just decided to stop Used prayer and other spiritual supports (e.g., meditation)
Interpersonal problems (4 items) Had problems with lover/spouse Had problems with other family members
Confronted by others (3 items) Confronted by others about the seriousness of your problem People you cared about gave you an ultimatum
Lack of availability of cocaine (2 items) Ran out of money Couldn’t get any more cocaine
Other factors in termination (3 items) Used other drugs or alcohol to come off cocaine Had legal problems
3.43 (1.07) 2.56 (1.57)
2.49 (1.87) 2.32 (1.80)
3.65 (I .02) 3.15 (1.34) 2.43 (1.74)
1.65 (1.83) 1.64 (1.77)
2.05 (1.77) 2.03 (1.76)
1.49 0.80
I .07 0.97
(1.73) (1.49)
(1.51) (1.57)
‘Items with scores of 2.00 or greater are presented. If none of the items in a subscale or category received a score of 2.00, the two items with the highest scores are presented. bO, not at all important; I, played a minor role; 2, somewhat important role; 3, moderately strong role; 4, played a major role.

40 J.R. McKay et al. /Drug and Alcohol Dependence 38 (1995) 35-43
Table 4 Correlations between experiences prior to relapse, and experiences after initial cocaine use and termination factors
Experiences the week prior to relapse
Unpleasant affect
Positive affect
Pleasant social exneriences
Interpersonal problems
Social pressure
Sensation seeking
Experiences after initial cocaine use Help seeking -0.07 Unpleasant affect 0.50*** Positive/appetitive 0.16 Interpersonal problems 0.28** Self-justification 0.19 Antisocial behavior 0.10
Factors in termination of relapse Painful internal states 0.312; Helpseeking behavior 0.01 Other coping responses -0.10 Interpersonal problems 0.18 Confronted by others 0.20 Lack of cocaine 0.04
0.09 0.23* -0.04 -0.04
0.32*+ 0.29’: -0.01 0.09
0.21* 0.20 -0.03 0.06
0.00 0.19 0.02 0.15 0.25’ -0.09 0.32** 0.38*** -0.05
-0.07 0.23* 0.46*** 0.05 0.19 0.34** 0.31** 0.09 0.01
0.03 0.21; 0.19 0.42*** 0.12 0.27**
0.05 0.21* 0.39*** 0.16 0.39*** 0.23;
0.07 0.16 0.13 0.19 0.16 0.13 0.35** 0.17 0.29* 0.34** 0.24* 0.16
0.02 0.34*** 0.56*** 0.14 0.56*** 0.35***
*P < 0.05; **p < 0.01; ***P < 0.001.
in Table 2. In cases where none of the items in a particu- lar subscale or category received a score of 2, the two most frequently reported items are presented. The most common experience following the initial use of cocaine was unpleasant affect, including guilt, depression, and feelings of having failed. However, positive/appetitive reactions to the first use were also common (e.g., ‘in- creased craving following initial use’, ‘enjoyed it so much you wanted more’), as were attempts at self- justification (e.g., ‘believed you could control your co- caine use’). Items from the Help Seeking, Interpersonal Problems, and Antisocial Behavior subscales were reported relatively infrequently, as were withdrawal symptoms and problems at work.
3.4. Factors involved in terminating relapses Of the 95 subjects, 75 had been abstinent for at least
two weeks following the relapse episode at the time of their interview and were therefore eligible to provide in- formation on how they were able to end their relapses. Items assessing factors in termination that occurred with at least moderate frequency (i.e., a score of at least 2 on a scale of O-4) are presented in Table 3. In cases where none of the items in a particular subscale or category received a score of 2, the two most frequently reported items are presented. The highest rated items were from the Painful Internal States, Help-Seeking Behaviors, and Other Coping Responses subscales. Conversely, subjects tended to give relatively low ratings to external factors, such as those assessed by the Interpersonal Problems, Confrontation by Others, and Lack of Availability of Cocaine subscales, and the legal problems item.
3.5. Different pathways through the relapse process To more fully explore the nature of the relapse pro-
cess, analyses were done to examine relationships be- tween factors in the onset, course, and termination of relapses. In these analyses, subscales from the sections of the CR1 that pertain to the onset of relapse (e.g., the Day and Week sections) were correlated with subscales scores from the Experiences Following Initial Use of Cocaine and the Factors Involved in Terminating Relapses sections. Results from the Day and Week sec- tions were similar. Therefore, for the sake of brevity, only results from the Week section will be discussed. These correlations are presented in Table 43.
The pattern of correlations suggested that there were three fairly distinct pathways through the relapse pro- cess. The first pathway is centered around unpleasant af- fect. Higher Unpleasant Affect scores prior to relapse were associated most strongly with Unpleasant Affect following initial use of cocaine and with Painful Internal States at termination. This relapse process was labeled the Unpleasant Affect pathway. The second pathway is characterized by generally positive experiences prior to and during relapse, and self-initiated coping behaviors at termination. Higher Positive Affect and Pleasant So- cial Experiences scores prior to relapse were associated most strongly with positive/appetitive reactions follow- ing initial use of cocaine and with coping responses at
3 Due to low rates of participation in self-help programs prior to relapse, correlations were not performed between the Lack of Self- Help Involvement subscale and subscales from the Experiences Following Initial Use of Cocaine and Factors Involved in Terminating Relapse sections.

J.R. MeKay et al. /Drug and Alcohol Dependence 38 (1995) 35-43 41
termination. This relapse process was labeled the Posi- tive Affect pathway. However, it should be noted that pleasant social experiences prior to relapse were also positively associated with termination due to interper- sonal problems.
The third pathway is characterized by sensation seek- ing, interpersonal difficulties, and antisociality. Higher Sensation Seeking and Social Pressure to Use scores in the week prior to relapse were associated most strongly with self-justification, positive/appetitive reactions, anti- social behavior, and unpleasant affect after initial use of cocaine. Higher Interpersonal Problems scores prior to relapse were also associated with antisocial behavior after initial use of cocaine, as well as with continued in- terpersonal problems. Sensation Seeking, Social Pres- sure to Use, and Interpersonal Problems scores prior to relapse were associated most strongly at termination with interpersonal problems and confrontation by others. This relapse process was labeled the Sensation Seeking pathway.
Several additional analyses were performed to ex- amine correlates of these pathways. To determine membership in each pathway, the mean scores of the subjects on the subscale from each pathway that assessed experiences during the week prior to relapse were averaged. These average scores were z-scored, to control for differences between the pathways in average scores (Unpleasant Affect = 1.87; Positive Affect = 1.53; Sensation Seeking = 1.04). Subjects were placed in one of the three pathways on the basis of which z-score was the highest (N = 36 in Unpleasant Affect, N = 37 in Positive Affect, and N = 21 in Sensation Seeking).
Subjects in each pathway did not differ on age or education. Women were somewhat under-represented in the Sensation Seeking pathway (23.8%), compared to the Positive Affect (32.4%) and Unpleasant Affect (36.1%) pathways, although the difference was not signi- ficant. African-American subjects were over-represented in the Positive Affect pathway (97.3%), compared to the Unpleasant Affect (75%) and Sensation Seeking (71.4%) pathways (x2 (2) = 8.98, P < 0.05). Being alone at the beginning of a relapse was more common in the Unplea- sant Affect pathway (67.7%), compared to the Sensation Seeking (40.0%) and Positive Affect (38.7%) pathways (x2 (2) = 6.61, P < 0.05). Impulsive relapses (i.e., first serious thoughts of relapse within two hours of using) were most common in the Positive Affect pathway (56.8%), followed by the Sensation Seeking (42.9%) and Unpleasant Affect (27.8%) pathways (x2 (2) = 6.29, P < 0.05). Higher Sensation Seeking pathway scores were correlated with more days of cocaine use during the re- lapse (r = 0.25, P = 0.02). In the subsample with AS1 data, higher Positive Affect pathway scores were cor- related with lower drug severity composite scores at treatment intake (r = -0.36, P = 0.01). Higher Unplea- sant Affect pathway scores were associated with higher
psychiatric severity composite scores at the level of a trend (r = 0.26, P = 0.07).
4. Discussion
This article presented descriptive information and correlational data on the cocaine relapse process. The experiences that were most likely to precede cocaine relapse were wanting drugs, having a lot of free time, being alone, having money, feeling extremely bored and lonely, and not participating in self-help programs. Interpersonal problems, pleasant affect, and pleasant social experiences were somewhat less common prior to relapse. These results suggest that the majority of cocaine abusers in the study relapsed when they had the motivation (desire for drugs coupled with boredom and loneliness), the means (money), and the opportunity (free and unsupervised time).
A strong association between unpleasant affect and relapse has also been reported in studies of other addic- tive behaviors, including alcoholism and smoking (Shiff- man, 1982; Marlatt and Gordon, 1985; Baer and Lichtenstein, 1988; Maisto et al., 1988). However, two recent prospective studies failed to find a relationship between negative mood and subsequent relapse to alco- hol, opiates, or nicotine (Hall et al., 1990), or to cocaine (Hall et al., 1991). With cocaine, the absence of positive mood, rather than presence of negative mood, predicted relapse (Hall et al., 1991). Although prospective designs are less vulnerable to distortions in memory, they pre- sent other methodological problems. For example, unless subjects are interviewed immediately prior to re- lapse, it is not clear whether the factors assessed at one point in time that are found to predict future relapses are actually occurring at the time of the relapses. The limitations of both prospective and retrospective designs suggest that further research is needed to improve and perhaps combine existing methodologies, and to develop new creative approaches for the study of relapse.
In theories of relapse (Marlatt and Gordon, 1985; Brownell et al., 1986), lapses are likely to progress into full-blown relapses when substance abusers make cer- tain attributions for their use (e.g., internal, stable, and global) and/or fail to engage in coping behaviors of some sort. In the present study, the combination of high scores on ‘feelings of having failed or blown it’ and ‘believed that any use meant you would relapse’ provid- ed some evidence of an abstinence violation effect (Marlatt and Gordon, 1985). Data from the CR1 also suggests that the course of lapse/relapse episodes may be influenced by the degree to which the substance abuser enjoys the initial use of cocaine and engages in self- justification and other forms of denial. Although sub- jects in our sample did experience unpleasant affect following their initial use of cocaine, positive/appetitive

42 J. R. McKay et al. /Drug and Alcohol Dependenee 38 (1995) 35-43
reactions and self-justification were also common. In- dividuals who have these latter reactions are probably less likely to engage in coping behaviors that interrupt the relapse process.
Correlations between experiences prior to relapse, ex- periences following onset of relapse, and factors in ter- mination of relapse were suggestive of three pathways through the relapse process. In the Unpleasant Affect pathway, cocaine abusers who relapsed following unpleasant affect continued to experience dysphoria, which in turn appears to have provided an incentive to terminate the relapse. The correlates of this pathway were being alone at the time of the relapse and relapsing in a relatively non-impulsive manner, and there was some indication that the pathway was associated with greater psychiatric severity at admission to treatment. For these individuals, relapse may have represented a failed attempt at reducing painful internal states (i.e., self-medication).
The Positive Affect pathway, on the other hand, was characterized by positive experiences prior to relapse and a relatively unproblematic relapse course. The pri- mary correlates of this pathway were lower drug prob- lem severity at admission to treatment and relapsing in a relatively impulsive manner. In addition, virtually all of the subjects in this pathway were African-American. The characteristics of this pathway and its correlates suggest that it may represent a less severe type of relapse experience. Cocaine users who experience positive mood and pleasant social interactions prior to relapse may be higher functioning and have healthier social support networks, both of which could increase the likelihood that they would either seek out help or engage more ac- tively in other coping responses after relapsing.
The Sensation Seeking pathway involved sensation seeking and interpersonal stressors prior to relapse, a mixture of self-justification, positive/appetitive reac- tions, unpleasant affect, and antisocial behavior follow- ing initial use, and termination through external factors. Higher Sensation Seeking pathway scores were also cor- related with more days of cocaine use during the relapse. This type of relapse might be viewed as highly treatment resistant, due to externalizing by the substance abuser and lack of internal controls on behavior, coupled with self-justification of use. The combination of both posi- tive/appetitive and unpleasant affect following initial use suggests that this pathway may be more heterogeneous than the other two pathways. It is also possible that there is a connection between the Sensation Seeking pathway and ‘Cluster B’ personality disorders (nar- cissistic, borderline, and antisocial), which are characterized by emotional lability, sensation seeking, and acting out. The relationship between the three pathways and Axis I and II disorders will be examined in future research.
Several potential limitations of this study should be
acknowledged. First, retrospective self-reports were used to gather data on the relapse process. The validity of such reports has been questioned, due to cognitive and motivational factors such as forgetting, time distor- tions and biases, and the need to present oneself in a favorable light (Bradley, 1978; Zuckerman, 1979; McKay et al., 1989; Ross, 1989; Squire, 1989; Henry et al., 1994). However, Henry et al. (1994) have suggested that retrospective reports can be useful for testing hypotheses that involve comparing individuals in a dis- tribution In regard to the present study, this suggests that retrospective reports can be used to compare the re- lative frequency of different experiences throughout the relapse process and to examine relationships between factors in the onset, course, and termination of relapse.
Second, the presence of an experience prior to a re- lapse, even if it is relatively specific to relapse, does not necessarily imply causality. Third, the relatively large correlations that were observed across Onset, Course, and Termination sections with certain subscales (e.g., Unpleasant Affect) may indicate a certain consistency in the experiences of some individuals throughout the re- lapse process, but it could also simply reflect a response set. Fourth, some of the analyses to examine potential correlates of each pathway should be interpreted cautiously, as data were only available from a little over half of the subjects in the full sample. However, this sub- sample was representative of the full sample in terms of both gender and race. Finally, virtually all the subjects in the present study were low SES, and most were unemployed. It is therefore not clear to what extent the findings would generalize to other populations. Ad- ditional studies with a wider range of subjects, including employed and higher SES individuals, are needed to determine generalizability.
Acknowledgements
This research was supported by National Institute on Drug Abuse grants DA08399 to James R. McKay, Ph.D. and DA05 186 to Charles P. O’Brien, M.D., Ph.D. We thank two reviewers for their comments on an earlier version of this article.
References
Alterman, A.I., McLellan, A.T., O’Brien, C.P., August, D.S., Snider, EC., Droba, M., Comish, J.W., Hall, C.P., Raphaelson, A.H. and Schrade, F. (1994) Effectiveness and costs of inpatient versus day hospital treatment for cocaine dependence. J. Nerv. Ment. Dis. 182, 157-163.
Annis, H. and Martin, G. (1985) Inventory of Drug Taking Situations, Addiction Research Foundation, Toronto, Ontario.
Baer, J.S. and Lichtenstein, E. (1988) Classification and prediction of smoking relapse episodes: an exploration of individual differences. J. Consult. Clin. Psychol. 56, 104-I 10.
Bradley, G.W. (1978) Self-serving biases in the attributional process:

J. R. McKay et al. /Drug and Alcohol Dependence 38 (199s) 35-43 43
a re-examination of the fact or fiction question. J. Personality Sot. Psychol. 36, 56-71.
Bradley, B.P., Phillips, G., Green, L. and Gossop, M. (1989) Cir- cumstances surrounding the initial lapse to opiate use following detoxification. Br. J. Psychiatry 154, 354-359.
Brownell, K.D., Marlatt, G.A., Lichtenstein, E. and Wilson, G.T. (1986) Understanding and preventing relapse. Am. Psychol. 41, 765-782.
Carroll, K.M., Power, M.D., Bryant, K. and Rounsaville, B.J. (1993) One-year follow-up status of treatment-seeking cocaine abusers: psychopathology and dependence severity as predictors of out- come. J. Nerv. Ment. Dis. 181, 71-79.
Hall, S.H., Havassy, B.E. and Wasserman, D.A. (1990) Commitment to abstinence and acute stress in relapse to alcohol, opiates, and ni- cotine. J. Consult. Clin. Psychol. 58, 175-181.
Hall, SM., Havassy, B.E. and Wasserman, D.A. (1991) Effects of commitment to abstinence, positive moods, stress, and coping on relapse to cocaine use. J. Consult. Clin. Psychol. 59, 526-532.
Heather, N., Stallard, A. and Tebbutt, J. (1991) Importance of sub- stance cues in relapse among heroin users: comparison of two methods of investigation. Addict. Behav. 16, 41-49.
Henry, B., Moffitt, T.E., Caspi, A., Langley, J. and Silva, P.A. (1994) On ‘remembrance of things past’: a longitudinal evaluation of the retrospective method. Psychol. Assess: J. Consult. Clin. Psychol. 6, 92-101.
Hunt, W., Bamet, L. and Branch, L. (1971) Relapse rates in addiction programs. J. Clin. Psychol. 27, 455-456.
Maisto, S.A., O’Farrell, T.J., Connors, G.J., McKay, J.R. and Pelcovits, M. (1988) Alcoholics’ attributions of factors affecting their relapse to drinking and reasons for terminating relapse events following marital therapy. Addict. Behav. 13, 79-82.
Marlatt, G.A. and Gordon, J.R. (1980) Determinants of relapse: im- plications for the maintenance of behavior change. In: Behavioral Medicine: Changing Health Lifestyles (Davidson, P.O. and David- son, SM., eds.), pp. 410-452. Brunner/Mazel, NY.
Marlatt, G.A. and Gordon, J.R. (1985) Relapse Prevention, Guilford, New York.
McKay, J.R., Alterman, A.I., McLellan, A.1. and Snider, E. (1994a) Treatment goals, continuity of care, and outcome in day hospital
substance abuse rehabilitation program. Am. J. Psychiatry 151, 254-259.
McKay, J.R., O’Farrell, T.J., Maisto, S.A., Connors, G.T. and Funder, DC. (1989) Biases in relapse attributions made by alco- holics and their wives. Addict. Behav. 14, 513-522.
McKay, J.R., Rutherford, M.J., Alterman, AI. and Cacciola, J.S. (1994b) Development of the cocaine relapse interview: an initial re- port. Submitted for publication.
McLellan, A.T., Luborsky, L., Woody, G.E. and O’Brien, C.P. (1980) An improved diagnostic evaluation instrument for substance abuse patients: The Addiction Severity Index. J. Nerv. Ment. Dis. 168, 26-33.
O’Connell, K.A. and Martin, E.J. (1987) Highly tempting situations associated with abstinence, temporary lapse, and relapse among participants in smoking cessation programs. J. Consult. Clin. Psychol. 55, 367-371.
Ross, M. (1989) Relation of implicit theories to the construction of personal histories. Psychol. Rev. 96, 341-357.
Shiffman, S. (1982) Relapse following smoking cessation: a situational analysis. J. Consult. Clin. Psychol. 50, 71-86.
Spitzer, R.L., Williams, J.B., Gibbon, M. and First, M.B. (1989) Structured Clinical Interview for DSM-III-R, Biometrics Research Department, New York State Psychiatric Institute, New York.
Squire, L. (1989) On the course of forgetting in very long-term memory. J. Exp. Psychol: Learn. Memory Cognition IS, 241-245.
Tims, F.M., Fletcher, B.W. and Hubbard R.L. (1991) Treatment out- comes for drug abuse clients. In: NIDA Research Monograph 106 (Pickens, R.W., Leukefeld, C.G. and Schuster, CR., eds.), pp. 93-l 13. USDHHS, Rockville, MD.
Wallace, B.C. (1989) Psychological and environmental determinants of relapse in crack cocaine smokers. J. Substance Abuse Treat. 6, 95-106.
Washton, A.M. (1989) Cocaine Addiction, Norton, New York. Washton, A.M. and Stone-Washton, N. (1990) Abstinence and relapse
in outpatient cocaine addicts. J. Psychoactive Drugs 22, 135-147. Zuckerman, M. (1979) Attribution of success and failure revisited, or
the motivational bias is alive and well in attribution theory. J. Per- sonality 47, 245-287.





























