Embed Size (px)
Citation preview

A
cement in general dental An evaluation of a ranid setting glass ionomer
practice P. J. Knibbs, BDS* C. G. Plant, DDS, FDSt
Key words: Glass ionomer cement, performance assessment, restorative dentistry, setting time.
Abstract Forty-five general dental practitioners evaluated the clinical handling properties and performance of a newly formulated glass ionomer cement of the powderlwater type. Seven hundred and ninety restorations were placed and 457 were reviewed after seven months. This formulation set rapidly. Approximately 95 per cent of the restorations performed well over the period of assessment. The results of this trial were compared with those of a trial on an earlier glass ionomer cement. The main advantage of the new formulation was the improved handling properties, notably the speed of set. Misuse of the material was the major factor responsible for poor clinical performance.
(Received for publication October 1987. Awepted August 1988.)
Introduction Glass ionomer cement, an adhesive, tooth-coloured
material, has a number of applications in restora- tive dentistry. The material has been available to the profession for about 11 years and a number of proprietary materials are now in widespread use. The properties of the material have been reviewed’ and results of clinical studies have been reported.*
*Lecturer in Conservation, Department of Operative Dentistry, The Dental School, Newcastle upon Tyne, UK. ?Senior Lecturer in Conservarion, Department of Conservative Dentistry, The Dental School, Birmingham, UK.
An advance in technology enabled the polyacid component of the cement to be vacuum dried and incorporated in the powder component which required mixing with water or tartaric acid solution for reaction.’ This resulted in the improvement of handling properties and physical proper tie^.^-^
Further development produced a better control mechanism for the release of cations from the reac- tive glass, enabling a small glass particle to be used. A material developed in this way, Chemfil II,S was marketed in 1984. The manufacturers claimed that this formulation improved the setting time and physical properties when compared with previous materials. The performance of this material has been assessed in general practice by a single oper- ator. The material performed well and no restoration failed in the one year of study.’
The aims of this study were to assess the handling properties of Chemfil I1 when used by general dental practitioners; to evaluate the clinical perfor- mance of a large number of restorations placed by those practitioners; and to compare the material with its predecessor, Chemfil I,$ which had been assessed previously in a similar way.4
Materials and Methods The material was obtained from the manufacturer
soon after its release to the profession in 1984. It was packaged in the commercial container. This contained five single shade packs of 10 g powder, a powder measure, a water dispenser, a shade guide, a bottle of citric acid conditioner and the manufac- turer’s instructions for use. The material was recommended for several purposes:
SDeTrey Division, Dentsply Ltd, UK.
Australian Dental Journal 1989;34(5):459-65. 459
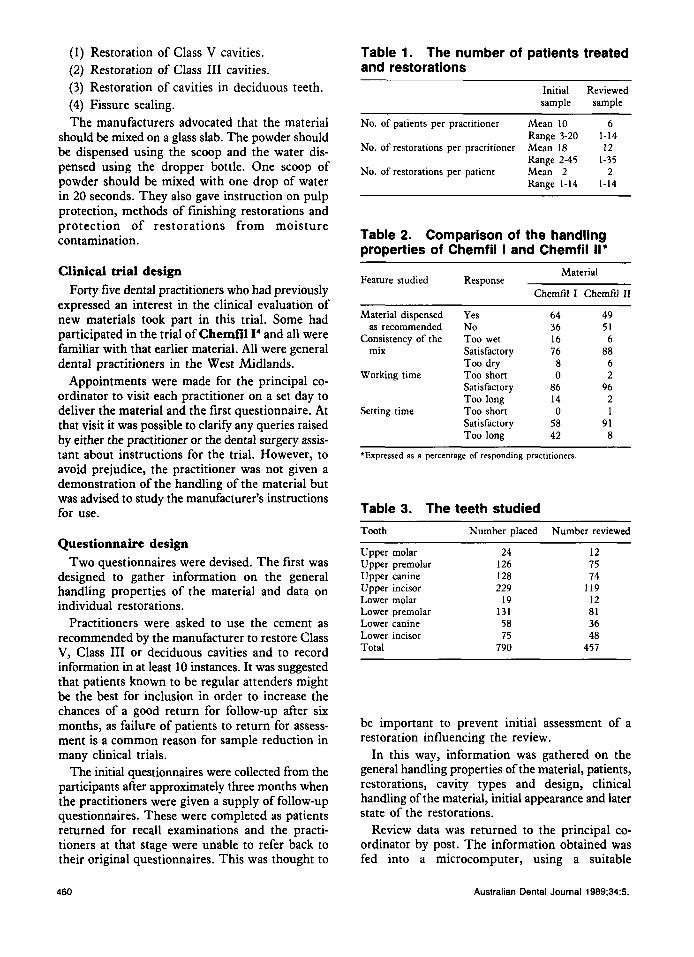
(1) Restoration of Class V cavities. (2) Restoration of Class I11 cavities. (3) Restoration of cavities in deciduous teeth. (4) Fissure sealing. The manufacturers advocated that the material
should be mixed on a glass slab. The powder should be dispensed using the scoop and the water dis- pensed using the dropper bottle. One scoop of powder should be mixed with one drop of water in 20 seconds. They also gave instruction on pulp protection, methods of finishing restorations and protection of restorations from moisture contamination.
Clinical trial design Forty five dental practitioners who had previously
expressed an interest in the clinical evaluation of new materials took part in this trial. Some had participated in the trial of Chemfil I4 and all were familiar with that earlier material. All were general dental practitioners in the West Midlands.
Appointments were made for the principal co- ordinator to visit each practitioner on a set day to deliver the material and the first questionnaire. At that visit it was possible to clarify any queries raised by either the practitioner or the dental surgery assis- tant about instructions for the trial. However, to avoid prejudice, the practitioner was not given a demonstration of the handling of the material but was advised to study the manufacturer’s instructions for use.
Questionnaire design Two questionnaires were devised. The first was
designed to gather information on the general handling properties of the material and data on individual restorations.
Practitioners were asked to use the cement as recommended by the manufacturer to restore Class V, Class I11 or deciduous cavities and to record information in at least 10 instances. It was suggested that patients known to be regular attenders might be the best for inclusion in order to increase the chances of a good return for follow-up after six months, as failure of patients to return for assess- ment is a common reason for sample reduction in many clinical trials.
The initial questionnaires were collected from the participants after approximately three months when the practitioners were given a supply of follow-up questionnaires. These were completed as patients returned for recall examinations and the practi- tioners at that stage were unable to refer back to their original questionnaires. This was thought to
Table 1. The number of patients treated and restorations
Initial Reviewed sample sample
~~
No. of patients per practitioner Mean 10 6 Range 3-20 1-14
Range 2-45 1-35
Range 1-14 1-14
No. of restorations per practitioner Mean 18 12
No. of restorations per patient Mean 2 2
Table 2. Comparison of the handling properties of Chemfil I and Chemfil II*
Material
Chemfil I Chemfil I1 Feature studied Response
Material dispensed Yes as recommended No
Consistency of the Too wet mix Satisfactory
Too dry Working time Too short
Satisfactory Too long
Setting time Too short Satisfactory Too long
64 36 16 76 8 0
86 14 0
58 42
49 51 6
88 6 2
96 2 1
91 8
*Expressed as a percentage of responding practitioners
Table 3. The teeth studied Tooth Number placed Number reviewed
Upper molar Upper premolar Upper canine Upper incisor Lower molar Lower premolar Lower canine Lower incisor Total
24 126 128 229
19 131 58 75
790
12 15 74
119 12 81 36 48
457
be important to prevent initial assessment of a restoration influencing the review.
In this way, information was gathered on the general handling properties of the material, patients, restorations, cavity types and design, clinical handling of the material, initial appearance and later state of the restorations.
Review data was returned to the principal co- ordinator by post. The information obtained was fed into a microcomputer, using a suitable
460 Australian Dental Journal 1989;34:5.
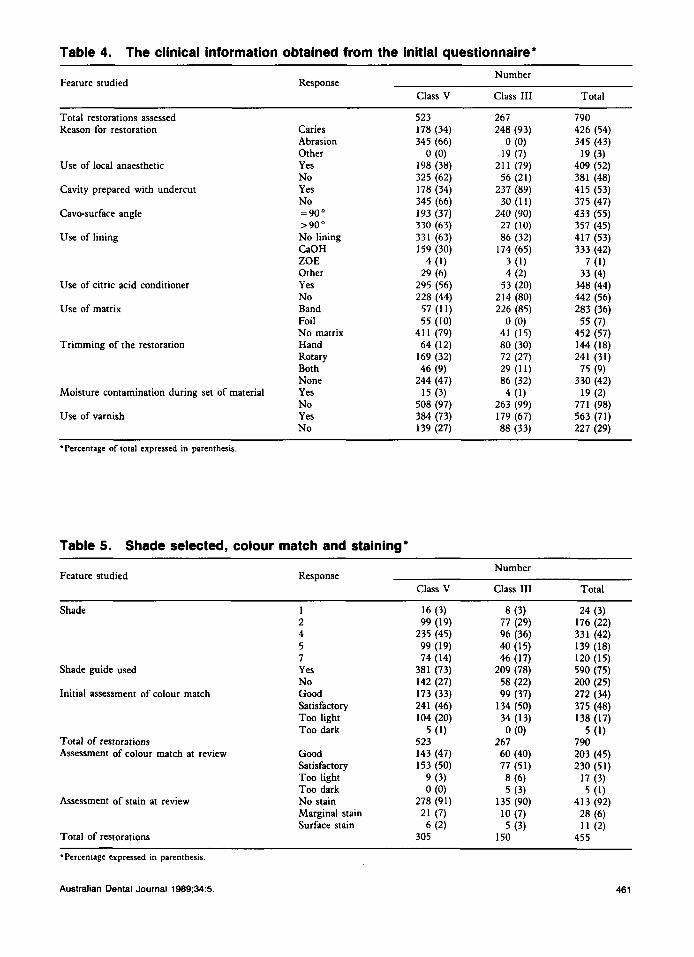
Table 4. The clinical information obtained from the initial questionnaire. Number
Class V Class I11 Total Feature studied Response
Total restorations assessed 523 267 790 Reason for restoration Caries 178 (34) 248 (93) 426 (54)
Abrasion 345 (66) 0 (0) 345 (43) Other 0 (0) 19 (7) 19 (3)
Use of local anaesthetic Yes 198 (38) 211 (79) 409 (52) No 325 (62) 56 (21) 381 (48)
Cavity prepared with undercut Yes 178 (34) 237 (89) 415 (53) No 345 (66) 30 (11) 375 (47)
Cavo-surface angle =90" 193 (37) 240 (90) 433 (55) >90" 330 (63) 27 (10) 357 (45)
ZOE 4 (1) 3 (1) 7 (1) Other 29 (6) 4 (2) 33 (4)
Use of lining No lining 331 (63) 86 (32) 417 (53) CaOH 159 (30) 174 (65) 333 (42)
Use of citric acid conditioner Yes 295 (56) 53 (20) 348 (44) No 228 (44) 214 (80) 442 (56)
Use of matrix Band 57 (11) 226 (85) 283 (36)
No matrix 411 (79) 41 (15) 452 (57) Trimming of the restoration Hand 64 (12) 80 (30) 144 (18)
Rotary 169 (32) 72 (27) 241 (31)
None 244 (47) 86 (32) 330 (42)
No 508 (97) 263 (99) 771 (98) Use of varnish Yes 384 (73) 179 (67) 563 (71)
No 139 (27) 88 (33) 227 (29)
Foil 55 (10) 0 (0) 55 (7)
Both 46 (9) 29 (11) 75 (9)
Moisture contamination during set of material Yes 15 (3) 4 (1) 19 (2)
'Percentage of total expressed in parenthesis.
Table 5. Shade selected, colour match and staining-
Feature studied Number
Class 111 Total Response
Class V
Shade 1
4 5 7
Shade guide used Yes No
Initial assessment of colour match Good Satisfactory Too light Too dark
Good Satisfactory Too light Too dark No stain Marginal stain Surface stain
Total of restorations Assessment of colour match at review
Assessment of stain at review
Total of restorations
16 (3) 99 (19)
235 (45) 99 (19) 74 (14)
381 (73) 142 (27) 173 (33) 241 (46) 104 (20)
523 143 (47) 153 (50)
5 (1)
9 (3) 0 (0)
21 (7) 6 (2)
278 (91)
305
8 (3) 77 (29) 96 (36) 40 (15) 46 (17)
209 (78) 58 (22) 99 (37)
134 (50) 34 (13) 0 (0)
267 60 (40) 77 (51) 8 (6) 5 (3)
10 (7) 5 (3)
135 (90)
150
24 (3) 176 (22) 331 (42) 139 (18) 120 (15) 590 (75) 200 (25) 272 (34) 375 (48) 138 (17)
5 (1) 790 203 (45) 230 (51)
17 (3) 5 (1)
28 (6) 1 1 (2)
413 (92)
455
'Percentage expressed in parenthesis.
Australian Dental Journal 1989;34:5. 46 1
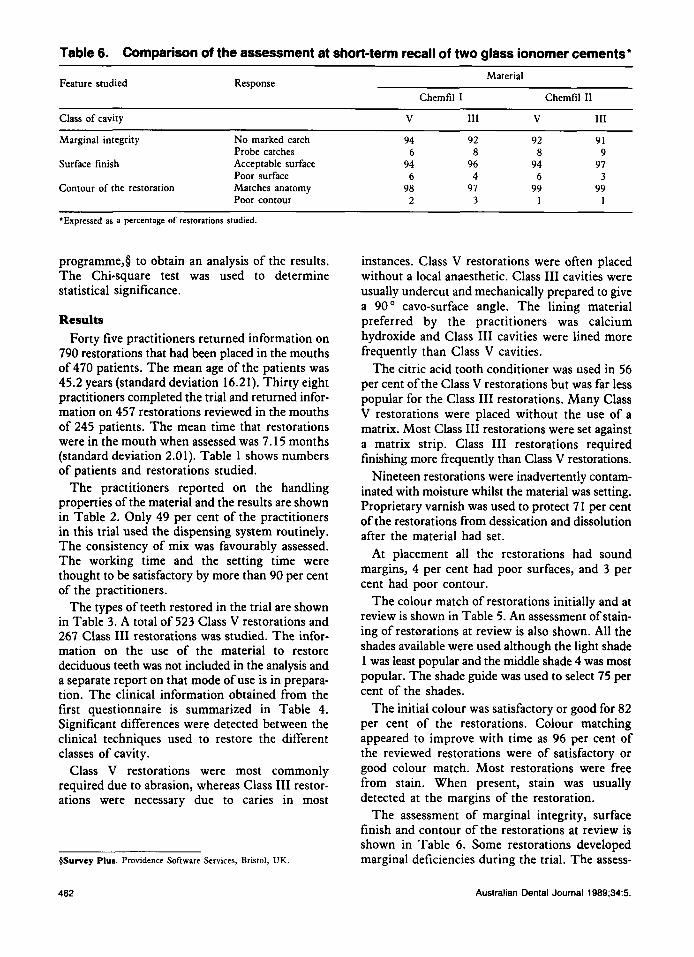
Table 6. Comparison of the assessment at short-term recall of two glass ionomer cements'
Feature studied Response Material
Chemfil I Chemfil I1 ~
Class of cavity V 111 V 111
Marginal integrity No marked catch 94 92 92 91 Probe catches 6 8 8 9
Surface finish Acceptable surface 94 96 94 97 Poor surface 6 4 6 3
Contour of the restoration Matches anatomy 98 97 99 99 Poor contour 2 3 1 1
'Expressed as a percentage of restorations studied
programme,§ to obtain an analysis of the results. The Chi-square test was used to determine statistical significance.
Results Forty five practitioners returned information on
790 restorations that had been placed in the mouths of 470 patients. The mean age of the patients was 45.2 years (standard deviation 16.21). Thirty eight practitioners completed the trial and returned infor- mation on 457 restorations reviewed in the mouths of 245 patients. The mean time that restorations were in the mouth when assessed was 7.15 months (standard deviation 2.01). Table 1 shows numbers of patients and restorations studied.
The practitioners reported on the handling properties of the material and the results are shown in Table 2. Only 49 per cent of the practitioners in this trial used the dispensing system routinely. The consistency of mix was favourably assessed. The working time and the setting time were thought to be satisfactory by more than 90 per cent of the practitioners.
The types of teeth restored in the trial are shown in Table 3. A total of 523 Class V restorations and 267 Class 111 restorations was studied. The infor- mation on the use of the material to restore deciduous teeth was not included in the analysis and a separate report on that mode of use is in prepara- tion. The clinical information obtained from the first questionnaire is summarized in Table 4. Significant differences were detected between the clinical techniques used to restore the different classes of cavity.
Class V restorations were most commonly required due to abrasion, whereas Class I11 restor- ations were necessary due to caries in most
BSurvey Plus. Providence Software Services, Bristol, UK
462
instances. Class V restorations were often placed without a local anaesthetic. Class I11 cavities were usually undercut and mechanically prepared to give a 90' cavo-surface angle. The lining material preferred by the practitioners was calcium hydroxide and Class I11 cavities were lined more frequently than Class V cavities.
The citric acid tooth conditioner was used in 56 per cent of the Class V restorations but was far less popular for the Class I11 restorations. Many Class V restorations were placed without the use of a matrix. Most Class I11 restorations were set against a matrix strip. Class I11 restorations required finishing more frequently than Class V restorations.
Nineteen restorations were inadvertently contam- inated with moisture whilst the material was setting. Proprietary varnish was used to protect 71 per cent of the restorations from dessication and dissolution after the material had set.
At placement all the restorations had sound margins, 4 per cent had poor surfaces, and 3 per cent had poor contour.
The colour match of restorations initially and at review is shown in Table 5. An assessment of stain- ing of restorations at review is also shown. All the shades available were used although the light shade 1 was least popular and the middle shade 4 was most popular. The shade guide was used to select 75 per cent of the shades.
The initial colour was satisfactory or good for 82 per cent of the restorations. Colour matching appeared to improve with time as 96 per cent of the reviewed restorations were of satisfactory or good colour match. Most restorations were free from stain. When present, stain was usually detected at the margins of the restoration.
The assessment of marginal integrity, surface finish and contour of the restorations at review is shown in Table 6. Some restorations developed marginal deficiencies during the trial. The assess-
Australian Dental Journal 1989;34:5.
ments of surface finish and contour at review were of the same order as those at placement.
Three restorations gave rise to later symptoms. One Class I11 restoration placed in an undercut cavity was lost. Thirty one restorations were scored as poor in some respect at review. These poor resto- rations were placed by only 12 of the practitioners. The other 26 practitioners reported no poor restorations.
Discussion This trial was designed to show trends in the
performance of the material as it was used by general dental practitioners. The trial design lacked the precision of a controlled clinical trial. However, the large sample size partially compensated for this lack of precision. Trials of this type can provide a broad base of clinical information in a relatively short space of time.
Forty five practitioners entered the trial and 38 completed it. This was a fall-out of 16 per cent, higher than in previous trials of similar d e ~ i g n . ~ , ~ The second questionnaires in this trial were returned to the principal co-ordinator by post because he had left the West Midlands. This method of questionnaire collection has been shown to give higher fall-out9 than the method of personal visits used previo~sly.~." The usehlness of personal visits to practitioners was confirmed by this finding.
Statistically significant differences were detected between clinical techniques used to restore the different cavity types. Such findings confirmed obvious clinical differences between the treatment of lesions in various sites and merely served to confirm the usefulness of the material to treat both Class V and Class I11 lesions. This agrees with the findings of an assessment of Chemfil II as used by one operator in general dental practice.'
The handling properties of the new formulation compared well with the earlier material and the manufacturer's claim of a rapid set were confirmed by the practitioners in this trial. However, there was no apparent improvement in clinical performance, in the short term, of Chemfd II compared with Chemfil I (see Table 6). In vitro studies on solu- bility, surface finish and translucency 'led other workers to conclude that the newer formulation would give better clinical performance.s Compara- tive clinical studies over a longer period are needed to confirm these in w h o findings.
Three restorations gave rise to later clinical symptoms, the nature of which was not stated. This low number helped to confirm the reported biolog- ical compatibility of this type of powderlwater glass
ionomer cement when used in the restorative mode." Calcium hydroxide was used to protect the pulp in many cases and in the light of current knowledge this practice of lining deeper cavities should continue.
The finding that only one restoration was lost, despite the lack of undercut in nearly half of the cavities, confirmed the adhesive properties of this material. The preparation of a 90' cavo-surface angle did not, in the short term, significantly influence marginal integrity at review. McLean and Wilson suggested that because the material is brittle in thin section, knife edge margins should be avoided.I1 Longer term assessment of the restora- tions in this study is required to provide more information about such features of cavity design.
The citric acid tooth conditioner was used in 56 per cent of the Class V cavities but only 20 per cent of the Class I11 cavities. The results of this short term study showed no apparent benefit in terms of restoration retention resulted from use of the condi- tioner. The manufacturer now recommends pretreatment of uncut dentine with a solution of polyacrylic acid to enhance adhesion.
Early glass ionomer cements were criticized for poor colour matching and translucency." The translucency of Chemfd I1 is superior to previous materials of similar form~lation.~ The findings of this study showed Chemfil I1 to have good colour matching and confirm its suitability for use in both Class V and Class I11 sites. The reported finding of improvement in colour match with time' was also noted in this study. The shade guide was used routinely by many practitioners. However, practi- tioners not using the shade guide reRoned the same levels of good or satisfactory colour matching as those who used the guide. Thus the study showed that the guide was useful to some but others could seemingly estimate shade matching satisfactorily without the guide.
Many Class V restorations were placed without the use of a matrix although most Class I11 restor- ations were set against a strip. The use or non-use of a matrix did not influence the assessment of surface finish at short term review although it has been shown that the best surface finish for this material was achieved by setting against a matrix strip.I3 The restorations placed with a matrix required trimming to remove excess more frequently than those placed with no matrix. This finding was statistically significant (P > 0.01).
Restorations scored as poor in any respect at review were grouped together and the data analysed to determine possible causes of failure. Features investigated were dispensing of the material;
Australian Dental Journal 1989;34:5. 463

methods of trimming; moisture contamination during the set of the material; and the use of the proprietary varnish to protect the set material from desiccation or dissolution. Significance was deter- mined using the Chi-square test.
It was found to be highly significant (P > 0.001) that restorations scored as poor at review had been of poor surface finish and contour at the time of placement. Thus poor findings at review did not represent deterioration of restorations in most cases but rather reflected poor quality initially. The provi- sion of poor restorations was also related to the operator either due to the standard of work or the severity of assessment because all of the poor restor- ations were placed by 12 practitioners; the other practitioners reporting no poor results.
The analysis showed that abuse of the material in various ways resulted in poor clinical perfor- mance. This was in agreement with a study of ASPA that stated glass ionomer cements gave poor performance if m i s ~ s e d . ' ~
Fewer practitioners routinely used the dispensing system than in the trial of C h e d i I. Failure to use the manufacturer's dispensing system in this trial produced a significantly high number of poor restor- ations (P > 0.01). These dispensing systems have limited acc~racy. '~ However, because the properties of powder/water glass ionomer cements were adver- sely effected by incorrect dispensingY6 the dispensing systems are to be preferred to unmeasured estimation of the constitutents. The findings did not show that moisture contamination during the set of the material resulted in later failure. Nevertheless, such contam- ination would alter the powdedwater ratio and in- corporate salivary constitutents into the set material. The need for adequate moisture control whilst using glass ionomer cement is obvious.
It is widely accepted that the set restoration should be protected against early moisture contami- nation or desiccation with a varnish, although such a procedure is only partially efficient with current varnishes.I6 Non-use of varnish in this study did not result in an increase of poor quality restorations at short term review.
It was highly significant (P > 0.001) that restor- ations trimmed either by hand or with rotary instruments were more likely to be poor at review than untrimmed restorations. An explanation may be that most restorations were trimmed too soon after the set of the material. The mean time when restorations were trimmed was 5.95 minutes (stan- dard deviation 13.06). Pearson and Knibbs, in a study on methods of finishing Chemfil 11, recom- mended that finishing should be done after a delay of 24 h 0 ~ r s . I ~
Poor quality of surface finish at the time of place- ment was highly significant (P>O.OOl) in the tendency of restorations to accumulate extrinsic stain. This finding highlights the importance of producing restorations with smooth surfaces.
Conclusions The newly formulated glass ionomer cement,
Chemfil 11, set rapidly and this speed of set was thought to be an advantage by general practitioners.
The material performed well when used by general dental practitioners to restore Class V and Class I11 cavities. Over 90 per cent of the restora- tions had intact margins, good surface finish, no evidence of contour loss and were colour matched well to the tooth when assessed about six months after placement.
The clinical performance of the material was similar, in the short term, to that of its predecessor, Chemfil I.
Poor quality restorations at review were gener- ally the result of misuse of the material at the time of placement.
Acknowledgements We wish to thank the general practitioners who
participated in the trial for their work and their hospitality and DeTrey Division of Dentsply Ltd for their financial support.
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
Walls AWG. Glass polyalkenoate (glass-ionomer) cements: a review. J Dent 1986;14:231-46. Knibbs PJ. Glass ionomer cements: Ten years of clinical use. J Oral Rehabil 1988;15:103-15. McLean JW, Wilson AD, Prosser HJ. Development and use of water hardening glass ionomer luting cements. J Prosthet Dent 1984;52: 175-81. Knibbs PJ, Plant CG, Shovelton DS. An evaluation of an anhydrous glass ionomer cement in general dental practice. Br Dent J 1986;160:170-3. Atkinson AS, Pearson GJ. The evolution of glass ionomer cements. Br Dent J 1985;159:335-7. Prosser HJ, Powis DR, Wilson AD. Glass ionomer cements of improved flexural strength. J Dent Res 1986;65:146-8. Knibbs PJ, Plant CG. A clinical assessment of a rapid setting glass ionomer cement. Br Dent J 1986;161:323-6. Knibbs PJ, Plant CG, Shovelton DS. The performance of a zinc polycarboxylate luting cement and a glass ionomer luting cement in general dental practice. Br Dent J
Vlietstra JR, Plant CG, Shovelton DS, Bradnock G. The use of glass ionomer cement in deciduous teeth. Follow-up survey. Br Dent J 1978;145:164-6.
1986; 160: 13-5.
464 Australian Dental Journal 1989;34:5

10. Plant CG, Browne RM, Knibbs PJ, Britton AS, Sorahan T. Pulpal effects of glass ionomer cements. Int Endod J 1984; 17:51-9.
11. McLean JW, Wilson AD. The clinical development of the glass ionomer cement. 111. The erosion lesion. Aust Dent
12. Crisp S, Abel G, Wilson AD. The quantitative measure- ment of the opacity of aesthetic dental filling materials. J Dent Res 1979;58:1585-96.
13. Pearson GJ, Knibbs PJ. Finishing an anhydrous glass ionomer cement (an in vitro and in vivo study). Restorative Dent 1987;3:35-9.
14. Smales RJ, Clinical use of ASPA glass ionomer cement. Br Dent J 1981;151:58-60.
15. Wong TCC, Bryant RW. Glass ionomer cements: dispensing and strength. Aust Dent J 1985;30:336-40.
16. Earl MSA, Hume WR, Mount GJ. Effect of varnishes and other surface treatments on water movement across the glass ionomer cement surface. Aust Dent J 1985;30:298-301.
J 1977;22:190-5.
Address for correspondenceheprints: Department of Operative Dentistry,
The Dental School, Framlington Place,
Newcastle upon Tyne, NE2 4BW, UK.
Australian Dental Journal 1989;34:5 465





























