Embed Size (px)
Citation preview

Postgraduate Medical Journal (May 1970) 46, 265-271.
An epidemic of ECHO 6 virus infection
A. S. MARY J. H. SWALLOWM.B. Ch.B.(Bagdad), M.R.C.P.(Lond.) M.A., M.B.(Cantab), M.R.C.P.(Lond.)
Medical Registrar Consultant PhysicianChelmsford Group of Hospitals
SummaryFourteen cases of infection with ECHO 6 virus in theChelmsford area from August to December 1968 aredescribed. A comparative account of the seasonal,geographical and age incidence is given, and itsrelationship to certain epidemiological aspects isdiscussed.
Aseptic meningitis occurred in eleven patients,pharyngitis in seven and myalgia in five. One patientsuffered from pericarditis, a manifestation of thisinfection which has not hitherto been recognized.Another patient suffering from aseptic meningitisdeveloped nephritis during the course of the illness, anassociation which has not been reported with ECHO 6infection.A relapse occurred in one patient with meningitis.
No permanent ill-effects followed in any case.
IntroductionIt is almost 20 years since the first ECH virus
was recognized. During a search for polio-viruses,a virus was found in tissue culture which was notneutralized by antibodies to polio-viruses or toCoxsackie viruses, and which was incapable of pro-ducing illness in suckling mice or monkeys. Theseenteric viruses were then described as Orphanbecause they were not pathogenic to laboratoryanimals, and because their relationship to illness wasobscure. Subsequently they were defined as theEnteric (from their source), Cytopathogenic (fromthe changes produced in monkey and human cells intissue culture), Human (in origin) and Orphan groupof viruses (Science, 1955). To date thirty-one ECHOvirus types distinguished by antigenic propertieshave been recognized. However, some reclassifica-tion is taking place; thus, type 8 has been found tobe related to type 1, and types 10 and 28 are nowincluded in the reoviruses and rhinoviruses, respec-tively.ECHO type 6 is now well established as a not
uncommon cause of aseptic meningitis (Winkelsteinet al., 1957; Lepow et al., 1962; Peckham, 1964).Other syndromes attributed to infection with this
type are encephalitis, lymphadenopathy and muscleweakness (Winkelstein et al., 1957); skin rashes,respiratory infections, myalgia and a Bornholm-likeillness (Karzon & Barron, 1962; Peckham, 1964).The association with diarrhoea in children is not defi-nitely established (Sommerville, 1958; Kibrick,1965).During the latter half of 1968 a small epidemic of
ECHO 6 virus infection occurred in mid-Essex. Theaffected patients exhibited many of the recognizedsyndromes attributable to this infection, and somefeatures not previously described.
Ca ngmaterial/During the months of August to December 1968,fourteen patients were admitted to the acute medicaland paediatric wards of this hospital group, fromwhom ECHO 6 was isolated and in whom the clinicalillness was attributed to this infection. Ten patientswere males and four females; seven were adults andseven children (Table 1).
Virus isolation was achieved using standardlaboratory techniques. Specimens likely to be bac-teriologically sterile were inoculated directly on totissue culture material, while contaminated speci-mens, such as faeces, were suspended in bufferedsaline, centrifuged and treated with antibiotics. Inthe case of throat swabs and washings, sufficientamphotericin B solution was added to the culturemedium to give a final concentration of 2-5 ,g/ml.The cells used were monkey kidney cells, suppliedby the National Institute for Medical Research, andHela cells maintained in the laboratories. Tubeswere incubated for at least 2 weeks before they werediscarded as negative. When cytopathic changesoccurred in the second passage of a culture, thevirus was identified by a neutralization test, usingtyping sera provided by the Standards Laboratory,Central Public Health Laboratory, Colindale. Thesecovered all types of polio viruses, Coxsackie B types1-6, ECHO 6 virus and herpes simplex, but noattempt was made to isolate strains of Coxsackie Avirus, which would have required the inoculation ofsuckling mice.
copyright. on F
ebruary 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.46.535.265 on 1 M
ay 1970. Dow
nloaded from
266 A. S. Mary and J. H. Swallow
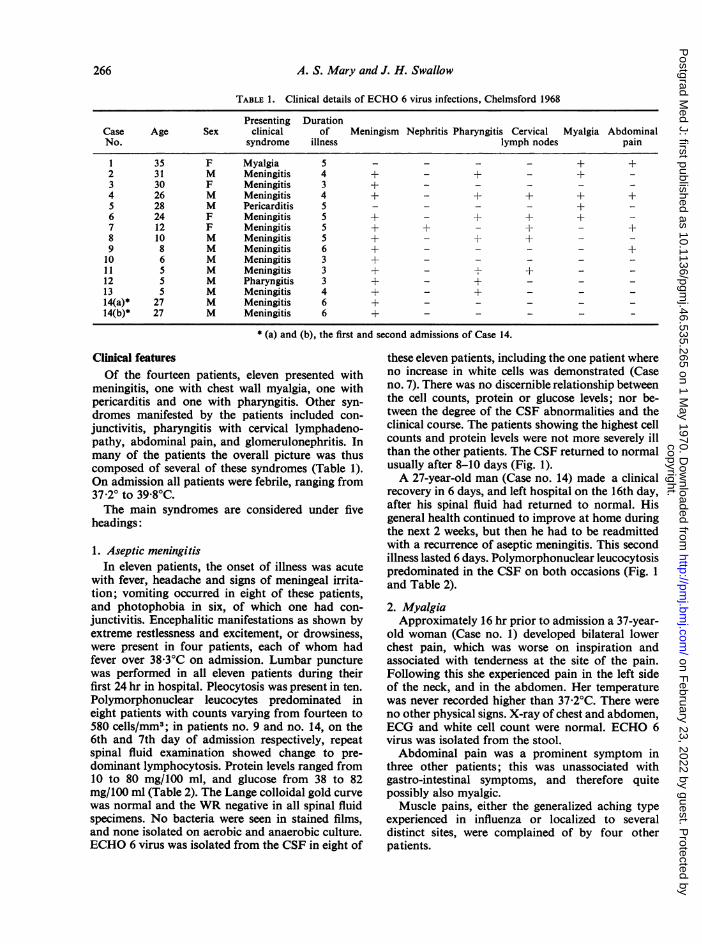
TABLE 1. Clinical details of ECHO 6 virus infections, Chelmsford 1968
Presenting DurationCase Age Sex clinical of Meningism Nephritis Pharyngitis Cervical Myalgia AbdominalNo. syndrome illness lymph nodes pain
1 35 F Myalgia 5 - - - - + +2 31 M Meningitis 4 + -+ - +-3 30 F Meningitis 3 +-4 26 M Meningitis 4 + - + + +5 28 M Pericarditis 5 - - - - +6 24 F Meningitis 5 +- + + +7 12 F Meningitis 5 + + - + - +8 10 M Meningitis 5 + - + -
9 8 M Meningitis 6 + - - - - +10 6 M Meningitis 3 +- -
11 5 M Meningitis 3 + - + - -
12 5 M Pharyngitis 3 + - + - - -
13 5 M Meningitis 4 + - + - - -
14(a)* 27 M Meningitis 6 +- -
14(b)* 27 M Meningitis 6 + - - -
* (a) and (b). the first and second admissions of Case 14.
Clinical featuresOf the fourteen patients, eleven presented with
meningitis, one with chest wall myalgia, one withpericarditis and one with pharyngitis. Other syn-dromes manifested by the patients included con-junctivitis, pharyngitis with cervical lymphadeno-pathy, abdominal pain, and glomerulonephritis. Inmany of the patients the overall picture was thuscomposed of several of these syndromes (Table 1).On admission all patients were febrile, ranging from37-2° to 39-8°C.The main syndromes are considered under five
headings:
1. Aseptic meningitisIn eleven patients, the onset of illness was acute
with fever, headache and signs of meningeal irrita-tion; vomiting occurred in eight of these patients,and photophobia in six, of which one had con-junctivitis. Encephalitic manifestations as shown byextreme restlessness and excitement, or drowsiness,were present in four patients, each of whom hadfever over 38.3°C on admission. Lumbar puncturewas performed in all eleven patients during theirfirst 24 hr in hospital. Pleocytosis was present in ten.Polymorphonuclear leucocytes predominated ineight patients with counts varying from fourteen to580 cells/mm3; in patients no. 9 and no. 14, on the6th and 7th day of admission respectively, repeatspinal fluid examination showed change to pre-dominant lymphocytosis. Protein levels ranged from10 to 80 mg/100 ml, and glucose from 38 to 82mg/100 ml (Table 2). The Lange colloidal gold curvewas normal and the WR negative in all spinal fluidspecimens. No bacteria were seen in stained films,and none isolated on aerobic and anaerobic culture.ECHO 6 virus was isolated from the CSF in eight of
these eleven patients, including the one patient whereno increase in white cells was demonstrated (Caseno. 7). There was no discernible relationship betweenthe cell counts, protein or glucose levels; nor be-tween the degree of the CSF abnormalities and theclinical course. The patients showing the highest cellcounts and protein levels were not more severely illthan the other patients. The CSF returned to normalusually after 8-10 days (Fig. 1).A 27-year-old man (Case no. 14) made a clinical
recovery in 6 days, and left hospital on the 16th day,after his spinal fluid had returned to normal. Hisgeneral health continued to improve at home duringthe next 2 weeks, but then he had to be readmittedwith a recurrence of aseptic meningitis. This secondillness lasted 6 days. Polymorphonuclear leucocytosispredominated in the CSF on both occasions (Fig. 1and Table 2).2. MyalgiaApproximately 16 hr prior to admission a 37-year-
old woman (Case no. 1) developed bilateral lowerchest pain, which was worse on inspiration andassociated with tenderness at the site of the pain.Following this she experienced pain in the left sideof the neck, and in the abdomen. Her temperaturewas never recorded higher than 37-2°C. There wereno other physical signs. X-ray of chest and abdomen,ECG and white cell count were normal. ECHO 6virus was isolated from the stool.Abdominal pain was a prominent symptom in
three other patients; this was unassociated withgastro-intestinal symptoms, and therefore quitepossibly also myalgic.
Muscle pains, either the generalized aching typeexperienced in influenza or localized to severaldistinct sites, were complained of by four otherpatients.
copyright. on F
ebruary 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.46.535.265 on 1 M
ay 1970. Dow
nloaded from

An epidemic ofECHO 6 virus infection 267
m wo Co nO,t,
.c \°Zo\ 0o 0 0 00u00u0r(^'<^'000 0\ ·00
0 1-
c*- oo %oo Q%oo ooo_r-.
zc
d * ?> s* *
C 4 cO
tU 0
I~ . * +++*I++I+I 1++I.n
I °040^
e000000000 0
0 ,"
IU
copyright. on F
ebruary 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.46.535.265 on 1 M
ay 1970. Dow
nloaded from

268 A. S. Mary and J. H. Swallow
700
Ic ·\
nE IE 400-
7E b
u @
300oo I
200 t \
I -100 at \\ai
0 5 10 15 20 25 30Doys oafter odmission
FIG. 1. CSF pleocytosis in ECHO 6 virus meningitis. ---, Case 14., means of CSF cell counts. *, First lumbar puncture; 0, second lumbar
puncture; n, third lumbar puncture; A, fourth lumbar puncture.
3. PericarditisSome 16 hr prior to admission, a 28-year-old man
(Case no. 5) developed a dull ache across the frontof the chest, which was worse on movement and oninspiration. He also complained of headache andsweating, and was febrile on admission (38-2°C). Apericardial friction rub was never heard, but serialECG tracings showed transient ST elevation withupward coveing of this segment in standard leads 1and 2, aVL, and V5-6 (Fig. 2). There was noevidence to suggest development of a pericardialeffusion. Chest X-ray was normal. The pain andfever settled in 3 days. White cell count and repeatedASO titres were normal. No pathogenic organismswere isolated from sputum or blood. ECHO 6 viruswas isolated from his stool. There was no suggestionof pericarditis in any of the other patients.
4. PharyngitisA 5-year-old boy (Case no. 12) presented with
fever of 38'3°C, pharyngitis and meningism. The
white cell count was 13,200/mm3 with 83% poly-morphs. MSU, chest X-ray and CSF were normal.No pathogenic bacteria were cultured from throatswab, urine or CSF, but ECHO 6 virus was isolatedfrom both throat swab and faeces. One of thepatients presenting with aseptic meningitis (Caseno. 11) had a frank follicular tonsillitis with cervicallymphadenopathy; ECHO 6 virus was isolated fromthe throat swab. Pharyngitis was present in fiveother patients, three of whom had enlarged cervicallymph nodes. One patient had enlarged cervicallymph glands but no pharyngitis.
5. NephritisProteinuria was detected on routine urine testing
in a 12-year-old girl who presented with asepticmeningitis (Case no. 7). Laboratory examination ofa clean-catch specimen confirmed the proteinuria,and also showed the presence of microscopichaematuria and many epithelial cells in the deposit;no bacteria were seen or isolated on culture. Blood
copyright. on F
ebruary 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.46.535.265 on 1 M
ay 1970. Dow
nloaded from

An epidemic ofECHO 6 virus infection 269
bi·Bi:'r::.::
i·.i:iii'iii*eii.YHr.i..i.i..8Vi.gs.'lB7.?isi., Xi?(i:F:l: ·:':·::·::·:1:T:·:·:·':· ::;: i.F:si.:si ·····::s:s::n:: ·I::r:w::·;:...:::::!:::i:
:·:::I%
Ri: isifdilL8ie·:··:*·*::F s::8:8:fl:8::'.:W:8:'1:.:.::8:b: ::.:V::::l:Y':·*C:':S:s I·:;:.·:r:.:·:··:; :.::·:·: ·;:-·.· :.iBs-*II:i8I ;,:ii·i·u ·;;··,:·-*ar
^:"
:s::n:I:iisii2i2elBiliil.B.C..iliB:Cilb':'' :n:eim:gi*e9i.:i:.:ia::·:·:·-·8:i8is:b.:.;:s:pW:.i.... :Xa::R:r:bl;es:-rigi.iai.:.lseiiiiai...:·:::::.:a::s:a::s:-::.r:;:i..:b:::ii il..:iliaa:i;.i*i:gil:*'i8g:ii:i9i:v: ::%i-i·:i··.iBB:;siU:8
:a:n:Z%lggiieil;lgi.%igili..iplLaii;ib I:iibi.iBiL"i:sai..:i.isa·:·.:·i:r::::.:i:::.
·:.:::::!:::;::·::;::i::!! DiLillIit·'!·:i*iX:i::
.·..;.;.·.......::l::i:::i::*:::i::
jiiiiiiiiiiiii.:i.Yi::··:;.i;-·*::::-:s:
i;43i011il:::::,::i::::::::;:::;::::::,
%i.iEl.j.L$
FIG. 2. ECG showing changes of pericarditis.
urea was not elevated. The girl made a clinicalrecovery in 5 days, and repeated urine examinationthereafter was normal. Urine abnormalities were notdetected in any other patient.
In all patients the illness was of short duration,and all clinical abnormalities had disappeared withina week of admission. As mentioned above, onepatient (Case no. 14) showed a biphasic course.
Other laboratory findingsBloodA polymorphonuclear leucocyte count of 8000/
mm3 was found in seven patients; one patient hadneutropenia (Case no. 3). An ESR of 16mm or above(1 hr Westergren) was recorded in seven patients(Table 2).Virus isolation
Isolations from stools were mostly from specimenscollected during the 1st week of the illness, though inone patient ECHO 6 virus was isolated 14 days afteradmission to hospital. From the CSF most isolationswere from the fluid obtained at lumbar punctureduring the first 24 hr in hospital (Table 3).DiscussionThe peak incidence of ECHO 6 virus infection in
Chelmsford occurred in the autumn. This seasonalpattern corresponded with that seen in England andWales during 1968, and to a lesser extent in 1967when there was no national epidemic (Tables 4 and5 and Fig. 3). No ECHO 6 virus was isolated in theChelmsford area during 1967. The incidence ofECHO 6 virus infection in New York in 1955 hadan earlier peak, in July and August (Karzon &
TABLE 3. Virus isolation
Case CSF Faeces ThroatNo. swab
1 0 + 02 + ++ 03 + + 04 + + 05 0 + 06 - ++ 07 + 0 08 + + 09 - +10 + + +11 - 0 +12 - + +13 ++ + +14 (a)* + + + 014 (b)* - 0 0
+, virus isolated once; + +, virus isolatedtwice; -, virus not isolated; 0, isolation notattempted.* (a) and (b), the first and second admissionsof case 14.
Barron, 1962). The seasonal pattern shown in thenational and Chelmsford figures (Fig. 3) canspeculatively be attributed to the increased ease ofviral transmission occasioned by more frequentperson-to-person contact in closed places at the startof the cold weather, while the fall in incidence overthe next several weeks may relate to the acquisitionof immunity and disappearance of ECHO 6 viruscarriers. During the period when these patients wereobserved, a considerable number of individuals wereseen in the same hospital group with similar syn-dromes but from whom no pathogens were isolated,which raises the distinct possibility of a higherincidence of ECHO 6 virus infection than was
copyright. on F
ebruary 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.46.535.265 on 1 M
ay 1970. Dow
nloaded from

270 A. S. Mary J. H. Swallow
140 -
(o)
80-
10
Z 20-
10(b)
April Moy June July Aug. Sept. Oct. Nov. Dec. Jon. Feb. March
FIG. 3. Seasonal incidence of ECHO 6 virus isolation. (a) England and Wales, 1967( --- ) and 1968 ( -- ). (b) Chelmsford 1968.
TABLE 4. Respiratory, cardiac and neurological infections due to ECHO 6 virus 1968
Total Jan. Feb. Mar. Apr. May June July Aug. Sept. Oct. Nov. Dec.
RespiratoryEngland and Wales* 42 4 2 3 3 5 8 17Chelmsford 1 1
CardiacEngland and Wales* 3 1 2Chelmsford 1 1
CNSEngland and Wales* 302 2 3 1 3 11 12 51 52 70 97Chelmsford 12 1 1 6 3 1
* Permission to use these figures was given by the Central Public Health Laboratory, Colindale.
TABLE 5. ECHO 6 virus infections 1967 and 1968
Total Jan. Feb. Mar. Apr. May June July Aug. Sept. Oct. Nov. Dec.
England and Wales 1967* 87 12 6 6 1 1 5 4 6 15 20 11England and Wales 1968* 539 7 4 3 3 4 15 21 66 68 107 1391 102Chelmsford 1968 14 - - - - - - - 2 2 6 3 1
*Permission to use these figures was given by the Central Public Health Laboratory, Colindale.
positively identified. As in the epidemic of asepticmeningitis due to ECHO 6 virus infection in NewYork (Karzon & Barron, 1962), children wereespecially affected in Chelmsford, six boys and onegirl. This is possibly due to immunity in adultsacquired following exposure to infection in earlierlife.
There was a contact history between Cases 11 and12, who were 5-year-old playmates. The intervalbetween the onsets of their illnesses was 3-4 days,which accords with the incubation period suggestedin other outbreaks (Winkelstein et al., 1957). It isnot certain, of course, whether these boys wereinfected from a common source. No other episodes
copyright. on F
ebruary 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.46.535.265 on 1 M
ay 1970. Dow
nloaded from

An epidemic ofECHO 6 virus infection 271
of illness occurred in the families of these or anyother patients in the series around the period coveredby this epidemic. The rate ofECHO 6 virus isolationin healthy contacts of clinically affected patients ishigher than in the general population at the sametime (Karzon & Barron, 1962). The first of these twochildren presented with aseptic meningitis (Caseno. 11), and the second with an upper respiratorytract infection (Case no. 12), thus demonstratingthe recognized variability in clinical syndromes thatcan be caused by the same strain of ECHO virus.
Pericarditis has been recorded in infections withECHO virus types 1 and 9 (Kibrick, 1964), but nothitherto with type 6. A 12-year-old girl (Case no. 7)who presented with aseptic meningitis, developed amild nephritis during the course of this illness.Acute glomerulonephritis has been reported tooccur during the course of infection with ECHOvirus type 9 in two cases (Yuceoglu, Berkovich &Minkowitz, 1966) but not previously in associationwith type 6 infection. Diarrhoea has been reportedin ECHO type 6 epidemics (Karzon & Barron, 1962;Peckham, 1964); but, in comparison with childrensuffering from respiratory infection as control,Sommerville (1958) encountered only a slight excessof ECHO virus isolation in children with diarrhoea.Only one of our patients had diarrhoea. Nausea andvomiting occurred in ten of our fourteen patients,but these symptoms were essentially part of themeningitic illness, rather than primarily gastro-enterological.As in previous epidemics of ECHO type 6 virus
infection, our patients had illnesses of only moderateseverity from which they rapidly recovered withoutsequelae. The severity and course of the illness werenot related to the haematological or cerebrospinalfluid abnormalities. One patient (Case no. 14 showeda biphasic course, which has previously been ob-served by Karzon & Barron (1962). The explanationfor this variability in response to infection is notunderstood; Webb (1968) suggests that host im-munity may be the determining factor.The virus is most commonly isolated from the
stool, followed by throat swab and then CSF(Winkelstein et al., 1957; Karzon & Barron, 1962;Peckham, 1964). The stool was the commonestsource of ECHO 6 virus in this series. It would seemprobable that ECHO 6 virus infection is transmitted,like the enteric infections, by faecally contaminatedfood or drink. The longest period during which viruswas isolated from the stools of any of our cases was14 days, similar to the 17 days in the 1955 New YorkECHO 6 virus epidemic (Karzon & Barron, 1962).
AcknowledgmentsWe wish to thank Dr R. Pilsworth, Director of the Public
Health Laboratory, Chelmsford, and the Medical ConsultantStaff of the Chelmsford Group of Hospitals, for allowing usto study their patients, and Miss B. J. Wall, Chief Technicianof the Public Health Laboratory, Chelmsford, for hertechnical assistance.
ReferencesKARZON, D.T. & BARRON, A.L. (1962) An epidemic of aseptic
meningitis syndrome due to ECHO virus type 6. Pediatrics,29, 409, 418 and 432.
KIBRICK, S. (1964) Current status of Coxsackie and ECHOviruses in human disease. Progress in Medical Virology, 6,27.
LEPOW, M.L., CARVER, D.H., WRIGHT, Jr, H.T., WOODSW.A. & ROBBINS, F.C. (1962) A clinical, epidemiologic andlaboratory investigation of aseptic meningitis during thefour-year period 1955-1958. New England Journal ofMedicine, 266, 1181.
PECKHAM, C.S. (1964) ECHO virus infections in England andWales, 1959-63. Monthly Bulletin of the Ministry of Healthand The Public Health Laboratory Service, 23, 217.
SOMMERVILLE, R.G. (1958) Enteroviruses and diarrhoea inyoung persons. Lancet, ii, 1347.
WEBB, H.E. (1968) Factors in the host-virus relationshipwhich may affect the course ofan infection. British MedicalJournal, 4, 684.
WINKELSTEIN, W., KARZON, D.T., BARRON, A.L. & HAYNER,N. (1957) Epidemiological observation on an outbreak ofaseptic meningitis due to ECHO virus type 6. AmericanJournal of Public Health, 47, 741.
YUCEOGLU, A.M., BERKOVICH, A. & MINKOWITZ, S. (1966)Acute glomerulonephritis associated with ECHO virustype 9 infection. Journal of Paediatrics, 69, 603.
SCIENCE (1955) Committee on the ECHO viruses: entericcytopathogenic human orphan viruses. 122, 1187.
copyright. on F
ebruary 23, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.46.535.265 on 1 M
ay 1970. Dow
nloaded from