Embed Size (px)
Citation preview

An Employers’ Guide to Healthcare ConsumerismAn Employers’ Guide to
Healthcare Consumerism


INTRODUCTION ........................................................................................................................ 5
CH I Consumerism in Healthcare: The Next “Best Thing”?Why Consumerism? ........................................................................................................ 7Theory vs. Reality.......................................................................................................... 9How Are Providers Reacting? ........................................................................................ 11
CH II A New Way for the New MillenniumCurrent Drivers of Consumerism...................................................................................... 16Critical Success Factors ................................................................................................ 17
CH III Financing Vehicles to Promote Demand Control FSAs .......................................................................................................................... 20HRAs.......................................................................................................................... 20HSAs.......................................................................................................................... 22Strategies for Use of Accounts ...................................................................................... 24The Future? ................................................................................................................ 26
CH IV The Supply Side: Supportive Services & Programs Preventive Care: the Promise of Wellness ........................................................................ 27Disease Management: the Promise of Controlling Chronic Conditions .................................. 32Information Therapy and Other Tools .............................................................................. 34
CH V Information & Decision-Support: The Promise of Transparency1st Generation Decision-Support .................................................................................... 382nd Generation Decision-Support and Beyond .................................................................. 39
CH VI Plan Design: One Framework for ConsumerismRoadmap to Change .................................................................................................... 431st Generation Plan Design .......................................................................................... 442nd Generation Plan Design and Beyond ........................................................................ 45
CH VII Regulatory Issues: Enablers or ImpedimentsTax Policy Implementation ............................................................................................ 47The Promise of Tomorrow .............................................................................................. 49
CH VIII A European Perspective on Healthcare & the Impact of Consumer ChoicePerspective on Healthcare Financing .............................................................................. 53Supportive Policies, Tools and Processes in Europe............................................................ 54
CH IX Who Needs to Change & How Do We Make it Happen?What Do Physicians Need to Do? .................................................................................... 60What Do Consumers/Patients Need to Do? ...................................................................... 63What is the Role of Employers & Health Plans? ................................................................ 66What is the Role of Government? .................................................................................. 68
An Employers’ Guide to Healthcare Consumerism | 3
TABLE OF CONTENTS


In September, 2001, Wye River Group on Health Care (WRGH) published the Employers’ Guide to Patient-Directed Healthcare Benefits, widely viewed as a landmark document in helping to shepherd in a new eraof health benefits. This Guide defined a variety of models along a continuum of what was being referredto as defined contribution. Since that time, public policy and the marketplace have moved rapidly toenable the adoption of tools and policies to broaden these financing concepts to a model of medicalconsumerism.
We recognized even then the inherent pitfalls in viewing this movement as merely an alternative financ-ing mechanism, and were anxious to ensure that the concepts did not fall into the managed care trap ofthe 1990s, where managing costs took precedence over managing care. Alongside many others, WRGHhas worked to encourage honest evaluation of progress, and to facilitate public policy changes that opti-mize the advantages of prevention and consumer empowerment, while mitigating potential risks to theunderprivileged and those with chronic disease.
Encouraged by our allies in the healthcare, business, and public policy communities, WRGH and its affili-ate Foundation for American Health Care Leadership, once again worked with a broad array of intereststo develop An Employers’ Guide to Healthcare Consumerism.
This Guide is an effort to frame the promise of healthcare consumerism, which represents a true seachange in how all stakeholders view and participate in American healthcare, while being realistic aboutits challenges. Each chapter provides a perspective on different key elements for an effective transitionand explores the roles and reactions of payers, providers, and consumers.
Chapter I takes a step back in time to examine the trends that have influenced health policy and health-care delivery over the past 50 years. Next, the myths and realities about healthcare consumerism, asespoused by advocates and detractors, are considered. Finally, the chapter looks at the reaction of thosestakeholders who will strongly influence its success or failure—the provider community.
Chapter II defines what we mean by healthcare or medical consumerism and describes the drivers of themovement and how they are influencing the marketplace and public policy. This chapter further high-lights critical success factors for the future.
Chapter III provides a detailed description of the on-going evolution of the financing mechanisms, knownas personal care accounts, developed to enable greater individual choice and control. The implications forcurrent and emerging roles and interactions between employees and their employers are considered.
Chapter IV highlights the importance of seeing this movement as something beyond just developing newways to finance healthcare services. It focuses on the supply side of the healthcare equation and theimportance of improving the health of the entire population, by shifting the paradigm from illness careto prevention and chronic care management.
Chapter V makes the case for transparency. Cost and quality information must be readily available in acomprehensible form in order to help individuals evaluate care options in real time, before and after theyare sick.
INTRODUCTION
An Employers’ Guide to Healthcare Consumerism | 5

Chapter VI presents one framework for considering different generations of consumer-directed healthplans and the key components of each. Ideas under consideration by employers and health plans to meetnew challenges are described.
Chapter VII provides a detailed look at current regulatory enablers and barriers to constructive change.The chapter also provides an instructive analysis of what can and should be done to promote a con-sumer-driven marketplace with adequate consumer protections.
Chapter VIII looks at challenges and trends in healthcare consumerism in several European nations. Itoffers constructive insight into what learning is transferable to the US and why.
Chapter IX examines the social and behavioral changes that will be necessary to advance the consumermovement and avoid unnecessary pitfalls.
We are indebted to a number of individuals who drafted and edited various chapters of this book. RonBachman, President & CEO of HealthVisions, Inc and a former Senior partner with PricewaterhouseCoopersprovided a great deal of the content in CH II, III, IV, VI and VII. Terry Humo, Terry Humo BenefitCompliance, formerly with Marsh, contributed significantly to CH II and III and was primary author of CHVII. He also was a critical resource in ensuring general legal and regulatory accuracy. CatharinaMaulbecker, PhD, Vice President, Marketing & Sales, CAS, provided us with her insight into medical con-sumerism in European countries as primary author of CH VIII. CH V on transparency was drafted by ScottWerntz, Vice President of Product Development and Robert Sanchez, Product Development Director ofConsumer Engagement Initiatives with Caremark.
We are most grateful to Helen Lippman, our professional editor, who undertook this project on a verytight timeline, and Sooki Moon who once again applied her talents as a graphic artist to make the Guidevisually appealing. We also want to express our appreciation to Jessica Comola for providing the photo-graph appearing on the cover of this publication, as well as for her previous contribution of the coverphotograph on the January, 2005 Communities Shaping a Vision for America’s 21st Century Health andHealthcare, Phase II Progress publication.
Finally, a very special thanks to Caremark, Definity Health and Veritas Health Systems for underwritingdevelopment and publication of this Guide.
Jon R. Comola,Marcia L. Comstock, MD MPH
6 | Wye River Group on Healthcare

The goal of this Guide is to educate, inform, andcreate a “strawman” concept to spur developmentof supporting legislation, regulation, market prod-ucts, and implementation of consumerism con-cepts that create a better system for cost, quality,and access to health and healthcare.
For the most part, we take a positive perspective onthe current trends and the opportunities associatedwith Consumer-Driven Healthcare (CDHC).However,for balance, in this opening chapter we want to takea 20,000-foot look at both the myths and the reali-ties of consumerism in healthcare. We also want togive readers the perspective of the provider commu-nity, recognizing its critical importance in achievingthe overall objectives of CDHC.
In the first WRGH publication on this topic, AnEmployers’ Guide to Patient-Directed HealthcareBenefits, released in October 2001, we attempted toclarify the possibilities inherent in a “defined contri-bution” model. We described a continuum of financ-ing models that could move employers from theircurrent state to a more consumer-directed model,emphasizing greater individual choice and control.
This made sense at the time, since public policydebate was focused on concepts of “defined con-tribution” versus “defined benefit”. Many policyexperts feared that this movement represented away for employers to abandon their traditionalrole as interlocutors for the payment and manage-ment of medical services.
Consumerism’s staunchest proponents, on the otherhand, saw it as the answer to all that ails ourhealthcare system. Our goal was not to advocate,but rather to clarify terms and describe both prosand cons. Even then, we were careful to point outthat for CDHC to have lasting impact, it had to gofar beyond financing.
Building on our previous work, this Guide movesfurther along the continuum. It encompasses boththe financial and the delivery components of con-
sumerism in healthcare, using a uniform frameworkto define different “generations” of CDHC.
Why Consumerism?
In some ways, we can look at this direction inhealth benefits as part of a natural evolution—a“back to the future’” of sorts. Most observers areaware that employers’ prominent role in healthcaredid not occur through some master design, andrealize, as we do, that the employer role is notlikely to appreciably change anytime soon. Nearly160 million people in this country have employer-sponsored health benefits, and surveys suggestthat most of them are not looking for a majorchange. Organized labor and some traditional andhistorically paternalistic corporations are commit-ted to continuing to provide health and retirementbenefits, as is the federal government.
Simplistically speaking, you might consider theprogression this way. Between 1945 and 1970,there was a mutuality of interests among insurers,physicians and hospitals. This pact served thesestakeholders well by providing a vigorous flow ofdollars that enabled scientific progress in medi-cine, as well as financial security among all three groups.
In 1964 the Great Society movement swept thecountry, and its promise added more demands and public expectations through Medicare andMedicaid.
In the 1970s tensions began to mount as con-sumers’ appetite for the latest medical marvelsbegan to outstrip the system’s capacity to coverthe costs of care. In response to financial con-cerns of employers, Congress passed the HMO Actin 1974.
Initially, managed care seemed to be the answer tospiraling healthcare costs. It was envisioned as adramatic shift that placed the emphasis on preven-
Chapter I
Consumerism in Healthcare:The Next “Best” Thing?
An Employers’ Guide to Healthcare Consumerism | 7

tion and wellness and channeled patients to highquality/low cost providers. We now know that, inmost cases, managed care became synonymous withmanaged cost—and little else. The main problem:Managed care largely overlooked the fact that ourscience-based model in healthcare is geared to theindustry itself--not the consumer, or patient.Americans’ cultural abhorrence of “Big Brother” and“Mother, may I’” proved to be a major stickingpoint as well.
In the 1980s and 1990s, employers responded tothe growing financial pinch by applying commonbusiness practices to their relationships with thehealthcare industry—practices like competitivebidding, vendor contracts and supply and demandnegotiations. In one sense, consumerism mightalso fall under the rubric of a business practice,since it offers a way for employers to more accu-rately predict annual healthcare expenditures andlimit their financial risk.
It’s cultural first, last and always! The reason weare looking to the consumer now is simple—we’vetried everything else and repeatedly found thatAmericans react negatively to any entity that triesto substitute its priorities for those of the individ-ual. In our culture, rugged self-determination gen-erally wins over social responsibility and equity.
Consumerism may also be seen as the latestattempt to navigate the tensions between limitedresources and unlimited expectations. In otherwords, it’s about money! Ultimately, the healthreform debate gets down to this fundamental ques-tion: Who will control healthcare decisions, bureau-cracies or individuals? Since we cannot finance allthe services that might provide some benefit tosome people, hard choices need to be made. Andwho better to make those tough choices thanthose whose lives are directly affected?
The pluralistic nature of our country also meansthat there is increasing diversity in health-relatedattitudes and individual preferences, which varywithin communities and even over the lifespan ofa given person. This is another strong argument
for a healthcare system that’s capable of satisfyingindividual values rather than imposing a one-size-fits-all solution upon the U. S. population.
Economist James Robinson points out that what-ever approach we choose has to recognize thatunrealistic and rising expectations—largely drivenby direct to consumer advertising—are going headto head with an increasingly elastic definition ofhealth. More and more therapies that had beenviewed as cosmetic, optional or discretionary areseen by many as essential to their health.
But the jury is still out on the question of whetherCDHC—thought by some to be the next “best”thing—really is the right direction. Here are twoopposing viewpoints from two nationally knownhealth economists.
Can we adopt a model of consumerism fromother industries? Consumerism is a powerful forcethat has transformed industries like financial serv-ices, telecommunications, travel and entertain-ment in ways that could hardly have been predict-ed a decade ago. It has largely supported the 21stcentury notion of more choice, higher quality andlower cost. There is a sense that it is the duty ofthe system to figure out the equation.
This conundrum requires a fundamental shift inhow we view the value equation in healthcare. Forexample, the “higher quality, lower cost” theoryhas yet to be proven in healthcare, much to thechagrin of purchasers.
“Consumer cost-sharing may contribute to bottomup health system reform after the exhaustion ofgovernmental and corporate initiatives.” [JamesRobinson]
“…actuarial models in healthcare “conflict with asense of justice and social responsibility.” [VictorFuchs]
The big question that remains is, Will consumerismin healthcare amount to little more than a costshift or lead to a fundamental cultural shift?
In order to imagine the possibilities of a fully devel-oped consumer model in healthcare, consider someof these examples of its evolution in other indus-tries. The framework for stages or generations ofCDHC used here is described more fully in chapter V:
1st generation consumerism: “personalizedservice”—house calls; pharmacy delivery of med-
8 | Wye River Group on Healthcare
“Consumer cost-sharing may contribute to bottom up healthsystem reform after the exhaustion of governmental and
corporate initiatives.” [James Robinson]
“…actuarial models in healthcare “conflict with a sense ofjustice and social responsibility.” [Victor Fuchs]

ications; the milkman; full service gas stations;dry cleaning delivery.
2nd generation consumerism: “customer conven-ience”— stores open after 5 pm and on Sundays;the telephone company accepting payments at thegrocery store; multiple locations for paying bills orcustomer service booths; travel agents who negoti-ate for individuals.
3rd generation consumerism: “information access &technology”—credit card use over the telephone; 24hour access to account information over the tele-phone; fax machines; and, eventually, the Internet.
4th generation: “hybrid-customer convenience + oper-ational efficiency”—online checking; catalogueordering; online shopping; bartering on Ebay
Today’s consumerism has redefined our expectationsand created demand for things that look and feelmore like self-service. We pump our own gas. Webook our own travel online, print out boarding pass-es from our computers at home, and check our ownbaggage at the kiosk. Many of us scan and bag ourown groceries as well.
One can only imagine how far we will go in healthcare!
What are we trying to achieve? Are Americans look-ing for a utopian healthcare system? Can we agreeon what is a better system? Here are a few attemptsto define a vision.
A pluralistic system that empowers patients anddemands accountability from individuals and thehealth system, while adequately supporting theneeds of the disadvantaged. (from WRGH communi-ties initiative)
“Collaborative care” with an engaged patient and apartnering physician sharing expertise, as contrastedwith a more traditional model of a passive patientand a dominant physician seeking compliance withinstructions. (Thomas Bodenheimer, MD, ClinicalProfessor, Department of Family and CommunityMedicine, University of California at San Francisco.)
Knowledge-based care; patient centered; system ori-entation (Institute of Medicine)
To reiterate a point made earlier, today we have ascience-based model created to support the health-care industry. What we need is a humanistic-scien-tific model that is designed to support consumersand patients as well.
Evidence suggests that, if channeled correctly,consumerism has the potential to radically change ourdysfunctional healthcare system and move us towarda system characterized by value, accountability,operational transparency and partnerships.
The Theory Versus the Reality
Let’s focus a bit more narrowly on the purportedgoals of CDHC, looking at each of the following interms of theory vs. reality:
Put the patient-consumer at the center of health-care and create a true healthcare marketplace. Inessence, we are talking about giving patients theability and incentive to think differently abouthealth and healthcare, by providing greater systemtransparency of cost and quality information thatthey can use for comparison purposes.
In addition, we will promote and reward value-added innovation and increase system accountabil-ity. Here are some of the theories:
■ Enigma theory: The normal market incentivespresent in practically every other serviceindustry have not been present in healthcare.In what other industry is the consumer ofgoods not the purchaser? In what otherindustry does the supplier determine howmuch and what kind of product or service youneed? Where is the incentive for consumers toshop wisely or question value or for providersto reduce costs or utilization? Only the toyindustry is similar, since adults make purchas-es on behalf of kids!
■ Back to the future theory: Consumers havebeen shielded from the true cost of health-care for years. In 1960, over 55% of totalhealthcare spending was paid directly by con-sumers. That number has dropped to approxi-mately 17% now, although that’s a smallerpercentage of a vastly larger total. What’smore, the expenses that consumers paydirectly tend to be the least essential ones,
An Employers’ Guide to Healthcare Consumerism | 9
Evidence suggests that, if channeled correctly, consumerismhas the potential to radically change our dysfunctionalhealthcare system and move us toward a system characterized by value, accountability, operationaltransparency and partnerships.

like vision, dental, and over the counter med-icines. Clearly, this situation is changing assome cost elements, such as prescription drugcopays are rapidly increasing. In general,when consumers don’t feel the true cost ofcare, they over consume. In some ways this isback to the future! Remember fee for service;80/20 insurance; deductibles with caps?
■ Scrutiny theory: As patients become increas-ingly responsible for the cost of care, they’llbe much more discriminating about whatdiagnostics and therapeutics they request andreceive. and this will help address the problemof infinite demand.
■ Self empowerment theory: Providing thosewith employer-based coverage more choiceand control will allow individuals to shapetheir own healthcare benefit options. In man-aged care, dictating or mandating thesechoices for employees created resentment; incontrast, giving them more control can be animpetus for positive health system change.
■ Doctor-patient relationship theory:Consumer-directed healthcare will help patientsget the most out of the relationship they havewith their physician, because this new modelsupports a decision-making partnership.
But what about the realities?
■ Skin in the game reality: These theories willonly become reality if consumers are aware ofthe true cost of care, have a personal stake init and have enough information and confi-dence to make healthcare decisions. Much ofthe information needed is just not theretoday, especially on the value dimension.There are obstacles to understanding qualityor even the true price of health insurance orhealthcare services. Furthermore, not allpatients will be price sensitive and not allphysicians will joyfully embrace being interro-gated about cost and quality!
■ Competency reality: Even if the informationwere there, consumers vary enormously in theirability and willingness to navigate a complexhealthcare system. Providers, payers, hospitalsand health plans have an obligation to ensurethat as information quality improves, it ismade available in a relevant and usable form,especially for the disadvantaged. In addition,some say that consumer-directed plans are ask-
ing patients to ration their own care. The ques-tion is, When they are faced with financial risk,will they do a better job of making decisionsabout their own care than physicians did undermanaged care? That is not at all clear.
■ Emotional vs rational reality: Let’s face it, it’sonly human to want, hope for and seek agreater quality, and quantity, of life. When con-fronted with medical marvels the desire toachieve health optimization through any meanspossible makes the decision process less ration-al and much more emotional. This is a particu-lar risk when an individual is suddenly facedwith making a major healthcare decision with-out the benefit of time to research the optionsor to reflect on the consequences of each.
Consumerism will help contain healthcare costs.There is no consensus today on this point, althoughthe most common opinion is that the impact willprobably be minimal overall and occur through low-ered demand. The theories go something like this:
■ High deductible plans are less expensive.
■ Self managed accounts yield decreased admin-istrative costs for small employers.
■ There will be decreased use of “discretionary”care, estimated to account for approximatelyone-third of all healthcare spending.
■ There will be an increased use of generic med-ications.
■ The resulting development of more efficientcare networks to serve a price-sensitive publicwill lower costs.
■ Longer-term, lifestyle behavior changes willresult in decreased risk.
But the following facts need to be taken intoaccount.
■ Large deductibles but relatively low out ofpocket maximums will not tend to reduce uti-lization for individuals who experience anexpensive episode of care in a given year orfor those with chronic diseases. For thesepatients, the annual deductible will be metand stop-loss insurance coverage will providefor nearly all of the remaining expenses.
■ Since 5% of the population is responsible for
10 | Wye River Group on Healthcare

approximately 45% of costs, this populationwill require more aggressive and effective earlyintervention. Disease management programs willbe necessary to succeed in controlling medicalexpenditures for these high-cost patients.
■ If not properly designed, these models couldcost employers more by overcompensatinghealthy workers—the approximately 77% ofemployees who spend less than $500 per yearon healthcare. Thus, employers that provide$750 to each employee for a health savingsaccount (HSA) or other type of account willlose money on most employees.
■ Some research suggests that cost reductionscome from less use of necessary as well asunnecessary care. After all, who can accuratelydetermine what third of care is discretionary?Low and modest income families might feelfinancial pressure to cut their use of medicalservices under a consumer-directed model.Even advocates of CDHC admit that wealthierpeople will always get what they want becausethey have the means to pay for it. Some pointout, however, that the wealthy are a relativelysmall proportion of the population so it doesnot really matter what they do.
■ Some people question whether the lost rev-enue to government from not taxing employ-ees on the value of healthcare benefits isappropriate, as the largest tax savings flow tohigher income taxpayers while many individu-als remain with no health insurance.
■ A simulation based on consumer-directed plansprovided by Definity, one of the first nicheinsurers created to offer CDH plans, showedthat cost savings would accrue to both thehealthy (63% of the population) and the sickest5% of the population. But the rest would endup paying more than with traditional insurance.
■ People in the middle group may not moderatetheir spending because the relative effective-ness of many healthcare products and servicesis not clear.
Consumerism creates an opportunity to get morepeople insured and to allow individuals to savefor future needs. Advocates point to several waysthis might occur.
■ More small businesses will be able to providesome support for employees, as high
deductible or catastrophic policies can bepriced lower than standard plans.
■ New tax-free health savings accounts mightreduce small employer administrative costs.
■ The ability to accumulate funds in suchaccounts will help individuals plan for futurehealthcare needs—as a bridge to Medicare forearly retirees, for example. Proponents believethis opportunity to save is the real point, ratherthan the tax advantage. Accumulated funds mayalso help those who change jobs by enablingthem to afford to pay for COBRA policies.
But here, too, there is another side to the story.
■ High deductible insurance products have neverbeen very popular. Take-up rates have histori-cally been low and may remain so.
■ The plans could have an adverse impact on peo-ple with higher anticipated healthcare costs byfragmenting the risk pool. They complicate pool-ing of insurance risk between the consistentlyhealthy and the chronically ill. Self-insurance,experience rating and managed care ended thesubsidy of healthcare across employers.
■ To some, applying the actuarial model tohealthcare conflicts with their sense of justiceand belief in collective responsibility. There isconcern that there will not be sufficientfinancial subsidies for the poor.
■ Detractors point out that many of the unin-sured are in the 10-15% tax bracket and wouldnot find the tax advantages offered by HSAs acompelling reason to buy health insurance.
How Are Providers Reacting?
Through the power of their pens, physicians aloneare responsible for approximately 80% of health-care expenditures. Along with hospitals and otherproviders, they have historically adopted technolo-gy and added services in order to pursue two
An Employers’ Guide to Healthcare Consumerism | 11
The Goals of Medical Consumerism■ Put the patient-consumer at the center of healthcare■ Create a true healthcare marketplace■ Help contain healthcare costs■ Create an opportunity to get more people insured■ Allow individuals to save for future needs

objectives: higher earnings and, better outcomes. Physicians see themselves, first and foremost and insome cases exclusively, as agents for patients. Assuch, they want to advocate for more resources tobe devoted to healthcare and have little interest inworking to balance the healthcare needs of indi-viduals with other national economic priorities.
Physician groups generally support the concept ofhealth savings accounts, but how it will all play outremains to be seen. Leading state medical societiesand the American Medical Association (AMA) havepromoted CDHC and health savings accounts (HSAs)as a more attractive option for helping to meethealthcare needs and as a means to strengthen thedoctor-patient relationship. CDHC, in their view,encourages greater communication and shared deci-sion-making. As one former AMA president was fondof saying, “Put the patient in the driver’s seat, withthe doctor riding shotgun.”
On the positive side, physicians point to the opportu-nity to maintain long-term relationships withpatients, even if jobs change or employers changeplans. They also tend to like the emphasis on preven-tive and behavioral services that support doctor-pre-scribed treatments and make for healthier patients.
Physicians also cite a number of administrativeadvantages to the consumerism model, the mainone being that it decreases “non value-added”bureaucratic oversight. Third party administrativehassle is perceived to be much less than that ofmanaged care. For one thing, generally CDHC doesnot require referrals.
Doctors also emphasize the potential of CDHC toinject more plan competition. After all, if employ-ees have a limited choice of plans, the plans havelittle incentive to be customer focused.
Many doctors appreciate the fact that CDHC mayhelp address some purchaser concerns about cost.
Finally, they like the fact that in some cases, thisapproach allows physicians to set their own fees.
And, at least they say.
But here, too, as in most aspects of CDHC, con-cerns and unknowns remain!
Physicians are a little leery of the “impatientpatient”— who demands better service and moreconvenience. It’s unclear, too, how doctors who didnot appreciate having their decisions questioned orsecond-guessed by managed care plans will respondto a similar interaction with their patients.
Indeed, patients are bound to ask more questionsabout cost and the necessity of various proceduresif they are paying the freight! Some doctors saythey’re not sure it’s good for patients to be wor-ried about the cost of care. They say, too, thatthey try not to make decisions based on cost and,in fact, have tried to ignore insurance status inmaking healthcare recommendations and decisionsin the past. When a patient with an HSA gets thebill for an office visit that seems too high for thetime spent with the physician, the doctor or officemanager needs to explain overhead and the valueof nurses and other support professionals.
Today, with the proliferation of on-line healthinformation, physicians are encounteringpatients with piles of unsorted informationdownloaded from the Internet, some of it usefuland reliable, much of it not. In order to makeCDHC work, physicians stress the need to makethe information available, accurate, relevant and understandable.
Because patients will be making more choices,physicians will need to carefully document thatthey have fully explained all treatment options. Ifa patient selects a less costly treatment andresults are less than optimal, it will be especiallycritical to have such documentation.
A much more fundamental concern expressed isthat CDHC plans could drive the “last nail in thecoffin” of primary care physicians. This approachmakes basic, routine healthcare services a com-modity. These are the types of services that peo-ple who have control over their healthcare dollarsare likely to limit. After all, why pay $70 to seean MD if you can see a nurse practitioner for $30, or go to the pharmacy for a routine bloodpressure or glucose check without an appointmentfor $10?
Lumenos, another firm offering CDHC-type cover-age, found that within six months of switching to
12 | Wye River Group on Healthcare
What Do Physicians Like about Medical Consumerism ■ More opportunity for long-term relationships■ Emphasis on prevention■ Less 3rd party hassle■ Potential for more plan competition■ Some opportunity to set fees

a consumer-directed health plan, there was a 6%reduction in physician visits. Although it is esti-mated that 20-25% of doctor visits are unneces-sary and that 30-35% of all healthcare is ineffec-tive or inefficient, at this point it is not alwaysclear which services or what care is unneeded orinefficient. It is also likely that people withchronic disease will view choices differently thantheir healthier counterparts.
One physician leader also expressed concern aboutbanks charging physicians transaction fees. Henoted that a large national bank that institutedmedical savings accounts is issuing a debit card toemployees. This makes it easier and quicker fordoctors to get paid and there is certainty that themoney will be there. However the transaction feeadds to administrative costs when CDHC is sup-posed to reduce cost.
The transition to a new way of doing business anda new relationship with patients and third partiesmay not be easy for practices that have becomeaccustomed to a steady flow of income from capi-tated contracts. Providers will need to institutevery transparent pricing information, but they donot want to see a “free for all” around negotiatingon price by patients who seek to save the moneyin their healthcare accounts.
There is also some concern about bad debt, depend-ing on how the plans are executed on the financingside. Doctors do not want to play the role of collec-tions agent, in the event that the HSA is depleted.
Finally, on the negative side, physicians are not atall sure that the money saved on the healthy lowutilizers will offset costs of care for those withserious illnesses and chronic disease. It is impor-tant to ensure that there are no disincentives forpreventive care in the design and that provisionsare made to promote coordination of care forthose who are chronically ill.
So far, there is little evidence that physicians’experience with patients who have high deductiblehealth insurance is different from their experiencewith those with more traditional insurance, butpenetration of CDHC is quite limited. Regardless ofthe issue of health savings accounts, the risingcost of health insurance premiums in general couldleave providers saddled with more uncompensatedcare as small employers—and more people over-all—are priced out of the market.
Then there are some areas where physicians are
unsure of the impact. CDHC puts a lot more deci-sion-making between the doctor and the patient. Itis likely that patients will pay more attention to thequality of care and service they receive. So physi-cians will have more incentive to invest in theirbusiness and will need to do so if they are to com-pete effectively. Many predict a lot more patientswill be willing to travel to providers in other citiesfor higher quality, lower cost procedures.
The reaction of the hospital industry: In general,hospital administrators are less sanguine thanphysicians about HSAs and high-deductible healthinsurance (HDHI) plans. Notwithstanding manyopportunities for an expanded role for this trustedand credible community asset, few experts seethem, in their current configuration, at the centerof the universe for healthcare in the 21st century.
Some experts express the opinion that the hospitalindustry is not well prepared for the convergenceof forces that will descend on it. Challenges aremany. Some of those cited by well-known CDHCadvocate Greg Scandlen in a recent edition ofHealth Care News include: lawsuits about tax-exemption status in exchange for care for indi-gent; the appearance of for-profits gauging self-pay patients; continuing patient safety concerns;the end of the specialty moratorium; a need togenerate top line growth, not just reduce expens-es; payment reductions; tiered benefits; and com-petition from off-shore facilities.
Scandlen points to a “restive” media portrayinghospitals as the latest in a long line of healthcarevillains that include greedy docs, evil insurancecompanies and profiteering pharmaceutical manu-facturers. He sees the media theme as “Hard work-ing consumers are being overcharged by dangerousand poorly run facilities that have conspired to retaina monopoly position in the healthcare system.”
He also believes that government is likely to inter-vene on behalf of hospitals only if communities or
An Employers’ Guide to Healthcare Consumerism | 13
What are Physicians’ concerns?■ Impatient, demanding, overly “netted” patients■ Issues of informed decision-making■ “Commoditization” of routine healthcare services■ Potential for transaction fees■ Need for transparency■ The needs of the chronically ill

beneficiaries across the state or country havebegun to be affected to the extent that it mightthreaten access to care.
In the face of all this, having to deal withpatients demanding price transparency, qualityinformation and customer convenience seems likeanother annoyance.
Hospitals do have some specific concerns aboutconsumerism. Industry leaders believe that somepatients, in an attempt to save dollars in theirhealth savings accounts, may delay seeking careuntil a problem costs more to treat. Another con-cern is that limited benefit plans often cap pay-ments for hospital bills at $5,000 or less, shiftingrisk to hospitals, which are required by law to atleast stabilize emergency cases. They believe thatmore patient responsibility for healthcare bills, inwhatever form, will add to the cycle of lower reim-bursement that leaves hospitals at a financial dis-advantage and will contribute to rising hospitalbad debt, higher credit risk and cost of collections.
The American Hospital Association (AHA) says ithasn’t done any official surveys, but a senior exec-utive stated that the perspectives of its memberson CDHC is all over the map. “With our small andrural members it is not anywhere near theirdopplers. In other places it depends on the level ofmarket penetration, which is still pretty low every-where. What the members are seeing are peoplewhose traditional coverage has taken a whack —higher co-pays and deductibles — and they can’tafford them.”
Many hospitals are preparing for a rise in high-deductible business by reviewing their financialaid and charity care polices and working tostreamline revenue cycle management. Hospitalofficials will try to identify patients right awaywho may have trouble paying instead of havingbills go to the collection process.
There appears to be a bit of schizophrenia on thesubject. Interviews conducted by the Center forStudying Health System Change with more than1,000 health system leaders in 12 communitiesrevealed significant skepticism about the ability ofmarket-based reforms to produce the type ofchanges that are urgently needed. But there wasalso deep concern about the potential for poorlyconceived government intervention and agreementabout “shared blame” for renewed healthcare infla-tion and receptivity to stronger market intervention.
There are even a few whispers of optimism.Hospital administrators and physicians like thefact that most plans build on the insurance com-pany’s existing provider network and negotiatedrates, showing that there is a level playing field.In fact, a recent hospital survey of insurersrevealed that 95% of HSA and HRA enrollment isin plans that build on existing networks. Finally,at least in theory, consumer-directed health planshave the potential to make patients more atten-tive to the details of care and costs, somethingmost providers recognize as crucial to addressinghealthcare challenges.
So far, the impact of high deductible plans onhospitals appears to be negligible. Some consult-ants say the fear of bad debt is overblown. Asmost of the costs of inpatient care will still becovered by insurance, hospital cash flow will bemostly unaffected.
What about other providers? Healthcare deliveryis, after all, about more than physicians and hos-pitals. Consider the perspectives of three otherprovider groups:
Dentists see this whole consumer movement asnothing new. Dental insurance is a relativelynewer benefit and much dental care has alwaysbeen paid out of pocket.
Nurses are strong supporters of patient-centrichealthcare in a broad sense, but most take noposition on financing issues since they don’t gen-erally bill directly for services. However, advancepractice nurses like nurse practitioners see signifi-cant opportunity to offer patients “better, morepersonal care for less money.”
Pharmacists also can play a valuable role in edu-cating and monitoring patients and in supportingself-care. But they certainly will want to be paidfor their services!
Conclusion: Clearly, the jury is still out withregard to the impact of consumer-directed health-care—and the truth of the matter is that there isno magic bullet. Even with the caveats outlined inthis chapter, however, medical consumerism hasthe potential to fix at least some of our nation’sbiggest healthcare challenges—and to move ustoward a more patient-centric, high quality andaffordable healthcare system.
14 | Wye River Group on Healthcare

Every decade seems to have produced a transfor-mation in how healthcare is administered in theUnited States. In the late 1940s and ‘50s it wasthe expansion of employer-sponsored healthcare.In the ‘60s it was the creation of Medicare andMedicaid and their impact on employer-based fee-for-service plans. In the ‘70s it was the passage ofERISA and the movement of large employerstoward self-insured arrangements. In the ‘80s itwas the expansion of managed care and the birthof the HMO. And in the 1990s it was the shift ofrisk to providers. True to form, the new millenni-um has seen another new paradigm —medicalconsumerism.
Essentially, managed care was grappling with onefundamental, structural problem with the U. S.healthcare system: how to control unlimiteddemand in the absence of individual consumer-level financial responsibility. The traditional man-aged care plan was based on a supply-controlmodel designed to control costs by limiting thesupply of care.
As costs continue their upward spiral, payers haverun out of room: They can no longer move employ-ees into tighter networks with more restrictionsand lower negotiated fees. Instead, they’re forcedto choose between two equally unpalatableoptions: Reduce benefits (i.e., increase deductibles,coinsurance amounts, and other out-of-pocketmedical costs) or lower pay (i.e., increase theemployee-paid portion of the premium.)
Employers do have another choice, however: Beginmoving toward consumerism in healthcare, whichrepresents a shift from a supply control model to ademand control model. Demand for services is lim-ited in every other part of our lives—in the formof costs, trade-offs and economic choices. Why notbring the power of the responsible, informed con-sumer to healthcare? Such a change is unprece-dented, complex and multi-dimensional—andgradual. It is not a revolution, but rather the startof an evolution.
Defining medical consumerism: Consumerism canbe defined as transforming employer-based healthbenefits into a model that puts economic purchas-ing power—and decision-making—in the hands ofparticipants. Employers supply the information anddecision support tools employees need to makeinformed choices, along with financial incentives,rewards, and other benefits that encourage benefi-ciaries to positively alter their health and health-care purchasing behaviors.
Why is this important? According to the Centersfor Disease Control and Prevention, 50% ofAmericans’ health status can be attributed directlyto their behavior, or lifestyle. Only 10% of overallhealth status is influenced by the healthcare
An Employers’ Guide to Healthcare Consumerism | 15
Chapter 2
A New Way for the New Millenium
Medical consumerism represents an unprecedented, complex, and multi-dimensional shift from a supply control model to a demand control model of healthcare.
Annual Change in Average Total Health Benefit Cost, 1987-2004
Note: Results for 1987-1998 are based on cost for active and retired employees combined. The change in cost from1998-2004 is based on cost for active employees only.
Source: Mercer’s National Survey of Employer-Sponsored Health Plans
1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
6.9%
18.6%
16.7%17.1%
12.1%
10.1%
8.0%
-1.1%
2.1% 2.5%
0.2%
6.1%7.3%
8.1%
11.2%
14.7%
10.1%
7.5%

system, yet that’s where most of the efforts arefocused.
Initially, the term “consumer-driven” (and similarterms, such as “consumer-centric,” “consumer-directed” and “patient-directed”) were associatedwith a health benefit design in which an employerestablished an account with a defined amount ofhealthcare dollars for each employee, and coupledthat contribution with catastrophic insurance. Asconsumerism has evolved, new generations ofthought have resulted in the addition of othercomponents. Stakeholders increasingly recognizethat affecting personal behavior, quality of careand, ultimately, cost, will require a creative, multi-faceted and flexible approach.
Today’s consumerism model is not limited to plandesign changes. Instead, it encompasses the broadspectrum of tools, incentives and plan design thathave the potential to positively impact health,healthcare purchasing and treatment decisions
Current Drivers of Consumerism
Under the current third-party reimbursement sys-tem, both the power of the marketplace and per-sonal decision-making are marginalized—and
attempts to modify behavior by using relativelysmall out-of-pocket deductibles, co-paymentsand/or coinsurance have had little effect ondemand. Many observers have concluded that costcontrol is impossible when patients are not awareof the true cost of healthcare services or able tojudge the quality of care delivered to them.Distorted purchasing decisions and uncontrollableinflation will remain problems in healthcare aslong as someone other than the patient is payingthe bill.
Clearly, using medical services is different thanpurchasing other consumer goods. But expertsestimate that up to 30% of care provided today is“discretionary” (i.e., either not medically neces-sary or available through less expensive, equallyeffective alternatives), and up to 25% is driven byunhealthy behaviors such as smoking, lack of exer-cise, and poor eating habits. Discretionary careand unhealthy behaviors alone are key drivers ofthe unmanageable cost hikes that are forcingemployer-payers to embrace CDHC.
As a result of the increase in healthcare costs andthe absence of quick solutions, the marketplaceand policy experts have once again re-evaluatedtheir approach. What emerged was the recognitionthat the individual user of health services couldbe encouraged to make better choices with theright incentives. More actively engaging con-sumers in decisions about their health and thecare they receive is expected to increase both thequality of that care and the level of patient satis-faction. This fundamental shift would put the con-sumer at the top of the decision tree, but to getthere will require a total revision of both the sys-tem and the consumer mentality.
The evolution began in 2000 - 2001, with theadvent of the concept of Consumer DirectedHealthcare. Several venture-capital backed entre-preneurial start-ups introduced health plan designsincorporating the consumer in innovative ways.Most of these included accounts that consumerscontrolled to pay for non-catastrophic care.
On June 26, 2002, the IRS issued guidelines thatapproved Health Reimbursement Arrangements(HRAs.) HRAs allow unused account balances tocarry over from year to year, financially benefitingthose willing to control discretionary healthcareexpenditures. HRAs make it possible for healthinsurance plans to simultaneously provide protec-tion and savings by allowing unused funds to be
16 | Wye River Group on Healthcare
Medical consumerism encompasses the broad spectrumof tools, incentives and plan design that have thepotential to positively impact personal behavior,
quality of care and healthcare costs.
Today’s Health Care Emvironment and Trends
Source: IFTF, Centers for Disease Control and Prevention
Access to Care Genetics Environment Behavior
Determinants 10% 20% 20% 50%
60%
50%
40%
30%
20%
10%
0%
Determinants of Health

rolled over. They may represent the most importantchange to affect healthcare benefits in 25 years.
The first CDHC products focused on plan designchanges, such as implementing HRAs in conjunc-tion with a high deductible plan. More recent pro-grams have expanded beyond plan design by inte-grating and aligning incentives around population-based health programs for example, wellness anddisease management. These newer designs moreeffectively address initial concerns that consumer-directed plans would be attractive only to theyoung and healthy and would penalize those withchronic conditions such as diabetes, asthma, orcongestive heart failure.
The Expanding CDHC MarketplaceAs consumer-centric healthcare evolved, severalissues surfaced regarding the tax treatment andcarryover provisions of spending accounts. TheIRS’ June 2002 ruling was undoubtedly responsiblefor major insurance companies such as Aetna,United, Humana and the Blues, joining start-ups—Definity Health, Destiny Health, Health Market andLumenos—as the major sellers of CDHC plandesigns. Although there were fewer than 500,000people enrolled in CDHC plans at the beginning of2003, enrollment as of January 1, 2005 was pro-jected to top 3.2 million.
Growth prospects for CDHC through 2010 are pro-jected at even higher levels.
Effective January 1, 2004, as a part of theMedicare Prescription Drug Improvement andModernization Act of 2003, the President signedinto law an important development for CDHC. Thelegislation created new tax-advantaged, fundedaccounts—Health Savings Accounts—to pay formedical expenses.
Some liken HSAs to medical IRAs or 401(k)s. Theycan be funded by employers or employees, theyare 100% vested (though in 401(K)s, employercontributions may not be fully vested the first fewyears) and they are portable. HSAs are the mosttax-advantaged savings vehicle ever passed intolaw by Congress. They are triple tax-advantaged,providing tax-free income to employees, accumu-lating tax-free, and not being taxable when fundsare withdrawn to cover eligible medical expenses.
With these new accounts, regulatory flexibility,additional proposed legislative initiatives and mar-ket-oriented IRS guidelines, CDHC and consumer
centric concepts are entering a new era. It is nowpossible for payers, insurers and providers to joinforces to create a healthcare system model thatpromotes better informed, more involved patientswho demand higher quality care at reasonablecost; greater cost transparency; and individualbehavioral changes that can simultaneously boosthealth and lower healthcare expenditures.
Critical Success Factors
The experience of early adopters of consumer-cen-tric plans has formed the basis for improved ver-sions of CDHC, creative new ideas and excitingproduct designs. Second generation products arenow available to employers, with more improve-ments rapidly on their way. Greater awareness inthe market and a growing number of believers are
An Employers’ Guide to Healthcare Consumerism | 17
Under 3rd-party reimbursement the power of the marketplace and personal decision-making are marginalized.A fundamental shift to medical consumerism would putthe consumer at the top of the decision tree, but to getthere will require a major shift in both system and consumer mentality.
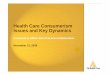
Figure 1 Forecast: US Consumer-Directed Health PlanAdoption, 2000 to 2010
2000 2002 `2004 2006 2008 2010Year
$500,000
$400,000
$300,000
$200,000
$100,000
$0
1-1 Consumer-directed heath plan revenues skyrocket
Total annual revenues from consumer-directed health plans, in premiums and premium equivalents paid by employers and employees
CDHP
PREM
IUM
(US$
mill
ions
)
Consumer-directed health plans will account for $80 billion in 2007, a sixfold increase over 2005.
!
Consumber-directed health plan premiu growth (US$ millions) for the yeare 2000 to 2010
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
$152 $393 $1,018 $2,568 $6,482 $16,186 $39,100 $87,750 $173,241 $289,502 $413,331

building a reservoir of thoughtful and creative newsolutions to old problems. National and regionalpayers have invested millions in new systems andproduct development. Second, third and evenfourth generation products are being developed,and transformation of employer-based health cov-erage is well underway.
It is the creative development, efficient delivery,efficacy and successful interaction of these ele-ments that will prove the success or failure ofconsumerism. It is not enough to deal only withhigh deductible plan designs associated with HRAsand HSAs. In the early stages of transformation,these designs may attract only 10-25% of theenrollee pool in an organization where they’reoffered. Even the most optimistic projections showthat consumer-driven high deductible plan designsare unlikely to capture more than 40-50% of thehealthcare market.
There are two basic requirements for a successfulconsumerism strategy. The consumer-centric pro-gram or options must:
■ Encourage and attract enrollment from thesickest members, as well as the healthy.
■ Work for those members who don’t want toget involved in decision-making as well as forthose who do.
By properly recognizing these core requirementsfor all plan options, concern about adverse selec-tion is mitigated.
18 | Wye River Group on Healthcare
The 5 Key Building Blocks of Medical Consumerism: ■ Personal Accounts (FSAs, HRAs, HSAs)■ Wellness/Prevention and Early Intervention Programs■ Disease Management and Case Management Programs■ Information and Decision Support Programs■ Incentive and Compliance Reward Programs
Note: The term “high deductible health plan” (lowercase) is used in a generic fashion to mean a higher than
normal front-end medical plan deductible (typically$1000 or more). Separate carve-out programs for
prescription drugs, or mental health may apply. Theterm “High Deductible Health Plan” (capital letters) or
“HDHP,” is a legal term as defined under the HSA legislation and means a plan meeting the design
requirements of the 2003 Medicare Improvement Act.
Basic Consumerism for Any Plan

Individually owned accounts to help pay for med-ical products and services have been an integralpart of the evolution of healthcare consumerism.Their key role has been to help promote individualresponsibility. It’s important to remember, howev-er, that the accounts are a tool, not an end inthemselves.
That realization can help employers and other plansponsors craft a benefit policy consistent withtheir business philosophy and objectives, under-stand developing federal and state healthcare poli-cies and design the best and most cost-effectivegroup plans possible within our ever-changinghealthcare environment.
Various types of individual medical accounts havedeveloped in the new millennium as part of theconsumerism movement. But neither the conceptof defined contribution healthcare benefits norindividual accounts for healthcare purchasing arenew. In fact, defined contribution health planshave been around for years under different names,but have attracted more attention as their abilityto control costs and to influence and reinforcepositive behavior has been recognized and betterunderstood.
Defined contribution healthcare was made possiblein the late 1970s through tax code provisionsauthorizing cafeteria plans and, specifically, med-ical flexible spending accounts (FSAs). Cafeteriaplans provide for employer and employee contribu-tions in defined amounts for individuals to use tobuy various benefits based on their priorities.
The FSA, one of the choices of a cafeteria plan,allows an individual to set aside tax-free employerand employee contributions to pay for medicalexpenses not otherwise reimbursed or coveredunder another medical benefits plan.
A feature of the FSA that eventually led to thedevelopment of a more consumer-oriented fundingdesign is the “use it or lose it” rule. Until recent-
ly, an individual had to use the FSA funds within adefined 12-month period or forfeit the money. Thetreasury department has recently added a 2-1/2month grace period, during which expenses maybe incurred and reimbursed from the FSA. Theproblem is that the “lose-it” feature has been anincentive for individuals to spend healthcare dol-lars remaining at year end, when the funds mightbe better saved for future medical care.
The Health Insurance Portability and AccountabilityAct of 1996 authorized a new individual savingsvehicle, the medical savings account (MSA). Thelegislation authorizing MSAs did so as a pilot proj-ect and limited their offering to small employers.These limitations, as well as negative pressure fromsome legislators, essentially doomed these earlyMSAs. They were not attractive from an underwrit-ing standpoint, and sponsors were reluctant totake on the administrative costs of setting upplans that potentially would be short-lived.
As pressure for more individual responsibility inhealthcare utilization and purchasing grew, theinsurance industry began to experiment with atype of self-funded plan that looked a lot like anFSA but allowed some accumulation of funds, orrollover. In 2002, Treasury gave its blessing to thehealth reimbursement arrangement. HRAs are indi-vidual employer-funded accounts in which unusedfunds can accrue and be used for future medicalneeds. This rollover feature carried the gene forthe evolution of healthcare consumerism, offeringindividuals a real incentive to take a more con-sumer-oriented approach to buying healthcareproducts and services.
The HRA still had two major drawbacks, however:a lack of assured portability and a lack of a mech-anism by which employees could make contribu-tions. Employers and other plan sponsors could, bydesign, allow individuals to take accumulated HRAfunds to new employers or into retirement, butwere not required to do so. While a few employersbuilt in these provisions, the general lack of guar-
Chapter III
Financing Vehicles to Promote DemandControl: Personal Care Accounts
An Employers’ Guide to Healthcare Consumerism | 19

20 | Wye River Group on Healthcare
anteed portability still needs to be addressed.Without it, the opposite of the intended effectcould occur: Any individual who plans to changejobs might have an incentive to spend an HRA bal-ance rather than lose it. Also, the prohibitionagainst individual contribution to the HRA under-mines the critical feature of individual responsibili-ty in purchasing healthcare. Employees with HRAsare still spending their employer’s money ratherthan their own— which means there’s less incen-tive to use the funds judiciously.
The health savings account (HSA), essentially asecond-generation MSA, addresses both concerns.HSAs may be funded through employer or employ-ee contributions, or both, but the funds belong tothe individual and thus are fully portable. This isnot to say that the HSA is the end of the evolu-tionary line in the development of individualaccounts, however. Certain features of the HSAand the HRA have resulted in a hybrid of the vari-ous health savings vehicles, which suggests thatthere still may be a better design.
More detailed discussion of the various accounts iswarranted to help employers understand how eachtype of account can further their business objectives,consistent with a consumerism approach to health-care. Ultimately, the goal for both business and con-sumers should be a healthier society, which in turnresults in a healthier, more productive workforce aswell as long-term control of healthcare costs.
Let’s look at specific features of the three mostsignificant accounts— the FSA, HRA and HSA.
Flexible Spending Accounts
Medical flexible spending accounts (FSAs) wereenacted as part of Tax Code section 125, the cafe-teria plan rules.
Medical FSAs are individual accounts that can befunded by employer and/or employee contribu-tions. They are available only to employees,although employees’ dependents may be benefici-aries. Employee contributions are made on a
salary-reduction, tax-favored basis.
Business partners, sole proprietors and 2% share-holders are not employees, therefore they cannotparticipate in FSAs.
Funds availability: FSA funds generally must beused within the 12-month plan year, althoughemployers can now authorize an additional 2-1/2month grace period through formal plan documentamendment. Funds not used within the allottedtime frame are lost.
Although employees typically contribute to an FSAeach pay period, employers under the “at risk”rule must make the entire plan year electionamount available at any time in the course of theyear. Thus, an employee who has made only onemonth’s contribution is entitled immediately tothe entire annual contribution, whether made byemployer or employee—provided the spendingmeets the fund criteria.
COBRA: FSA funds are portable only throughCOBRA continuation of coverage rules, and underlimited circumstances.
Reimbursable medical expense: Reimbursableexpenditures are limited to Tax Code section 213medical expenses and, under Treasury guidance,include certain over-the-counter products or serv-ices to treat specific conditions or injuries. FSAsmay not be used to pay health plan premiums.
Non-discrimination requirements: FSAs are sub-ject to cafeteria plan non-discrimination rules pro-hibiting contributions that favor highly compen-sated participants.
Health ReimbursementArrangements
Health reimbursement arrangements (HRAs) arefunded exclusively by employers and used to reim-burse employee medical expenses, including healthinsurance premiums. The contribution does notcount as part of the employee’s gross income.Excess funds at year-end may be rolled over forfuture medical expenses.
The program enables employers to define certainhealth benefit contributions and shift moreresponsibility for healthcare choices to employees.
Ultimately, the goal for both business and consumersfrom these accounts should be a healthier society, whichin turn results in a healthier, more productive workforce,
as well as long-term control of healthcare costs.

The HRA is defined as an arrangement that:■ Is paid for solely by employer contributions,
without any cafeteria plan style pre-tax,salary reduction or election;
■ Reimburses the employee, spouse or depend-ent for medical expenses as defined underSection 213 of the tax code, including premi-ums; and,
■ Provides reimbursements up to a maximumamount for a coverage period. Any unusedportion at the end of the coverage period iscarried forward, thereby increasing the maxi-mum reimbursement amount for the subse-quent coverage period.
Unlike FSAs, all funds do not have to be immedi-ately available to the individual, a feature thatprotects employers.
■ Funds must be used for medical expenses only,there is no opportunity to “cash out”;
■ Unused funds may be carried over for medicalexpenses in subsequent years;
■ Plans may provide for funds to carry over afterretirement or termination;
■ Premiums and other medical expenses may bereimbursed from the same HRA;
■ HRAs and FSAs may be provided simultaneously;■ When an individual is covered under both an
HRA and an FSA, plans may determine whichpays first; and,
■ HRAs are subject to COBRA and HIPAA.
The typical HRA scenario is for a plan sponsor tooffer a high-deductible, major medical insured orself-funded health plan, along with an HRA tohelp employees pay the deductible and other out-of-pocket expenses not covered by the major med-ical plan. The employer may establish a structurethat requires an individual to be covered under amajor medical health plan in order to be eligiblefor the HRA, but that is not required.
In fact, HRAs are being promoted as a way forsmall employers that otherwise cannot afford toprovide health benefits to offer the account alone.The theory is that by offering at least a minimalpackage, with a possible link to state-fundedhealth programs such as Children’s HealthInsurance Programs, employers will introduceemployees to the healthcare system and help themto learn to budget for healthcare needs and tootherwise take responsibility for some of thecosts. In addition, this consciousness-raising maylead to healthier behavior and lifestyle choices.
Who can receive reimbursement? The HRA is ahealthcare plan under tax code provisions thatallow reimbursements to be excluded from theemployee’s income, as provided under sections 105and 106 of the tax code. HRA reimbursements areavailable to employees, former employees, and theirspouses and dependents—but are not an option forthe self-employed. Retirees and terminated employ-ees may continue to receive HRA reimbursementseven if they do not elect COBRA coverage.
Reimbursable expenses defined: To avoid beingcounted as taxable income, HRA reimbursementsmust be used for medical expenses as defined underTax Code section 213—which includes long-termcare services. Such expenditures must be substanti-ated, a requirement similar to that of medical FSAs.Unlike FSAs, however, HRA funds may be used toreimburse premiums for a major medical plan.
There is a catch to this provision, though: If theplan requires the individual to be enrolled in amajor medical plan in order to participate in theHRA, the employer cannot impose a premium con-tribution requirement on the employee that islarger than the insurance cost without the HRA.IRS guidelines require that HRAs can only be fund-ed by the employer, and any extra salary deduc-tion above the cost of the major medical premiumwould be seen as an employee contribution to theHRA—which is not permitted.
There are also timing limitations on HRA reim-bursements: An HRA may not reimburse a medicalexpense incurred before the date that the accountis in existence—or before the employee enrolls.Nor can an HRA reimburse any medical expensethat is attributable to a deduction allowed in aprevious year.
Cafeteria plan prohibition: Because HRA contri-butions cannot be made on a pre-tax, salary-reduction basis, these accounts cannot be part of,or linked to, a cafeteria plan.
In another limit related to cafeteria plans, the HRAamount contributed by the employer cannot be linkedto any amount forfeited under an FSA. However, anindividual can have both an FSA and an HRA.
Order of payment: Generally, FSA funds cannot beused for a medical expense that is otherwisepayable or has been paid by another plan. If cov-erage is provided under both an HRA and an FSAfor the same medical expenses, the HRA funds
An Employers’ Guide to Healthcare Consumerism | 21

must be exhausted before FSA reimbursements areallowed. If the expense is not covered by the HRA,even though HRA funds still exist, then the FSAmay be used to reimburse the expense.
There is one caveat, however. Plan sponsors maysteer clear of that general rule by setting the pay-ment order through the plan document. If, beforethe FSA plan year begins, the sponsor specifies inthe plan document that FSA funds must beexhausted before an HRA will pay an expense cov-ered under both accounts, then reimbursementmay be made first from the FSA. The same expensecannot be paid by both accounts, of course.
Non-discrimination rules: HRA funding cannotfavor senior management. The tax code non-dis-crimination rules that prohibit offering morefavorable benefits to highly compensated individu-als apply to HRAs, since they are self-fundedplans. Thus, employers are required to make a flatcontribution to the HRA—$1,000 per participant,say—regardless of the employee’s status.
COBRA: COBRA rules apply to HRAs. An individualmay choose COBRA for just the major medical planor just the HRA, or both—unless the plan isdesigned so that the HRA is available only to thosecovered under the major medical plan.
Other matters: The tax code rules under sections419 and 419A regarding employer deductions andreserves for retiree medical coverage apply to HRAs.Also, the section 404 rules regarding when anemployer gets to take a deduction, i.e. when theexpense is paid, also apply to HRA reimbursements.
HIPAA’s nondiscrimination rules apply, too, includ-ing when HRAs are used to fund individual healthinsurance policies treated as a group health plan.In addition, HIPAA’s portability rules apply, requir-ing certificates of prior coverage to be issued.
ERISA’s requirements for welfare benefits plansapply, as well. This could create issues under planasset and trust rules, for example, depending onhow the HRA is structured—as a funded account ora notational credit. The normal ERISA health plandocument and other disclosure rules also apply.
Health Savings Accounts
HSAs were created by the Medicare prescriptionreform act signed by President Bush on Dec. 8,
2003, as a means of instilling a sense of personalresponsibility in healthcare purchasing—and help-ing Americans save for future qualified medicaland retiree expenses on a tax-free basis. Offeringof HSAs was authorized starting Jan. 1, 2004.
HSAs essentially are 2nd-generation medical sav-ings accounts. While available only to “eligibleindividuals,” anyone can contribute to them onbehalf of an individual. But HSAs are not stand-alone plans. They may be offered only in conjunc-tion with a high deductible health plan (HDHP)and are funding vehicles for medical expenses untilthe minimum required deductible is met under thehigh-deductible plan. HSAs also are designed to beused as a tool with other consumer-directed healthplan features that promote wellness.
To qualify as a high deductible plan, the annualdeductible must be at least $1,000 for individualcoverage and at least $2,000 for family coverage,adjusted for cost of living with a year 2003 base.However, there does not have to be a deductiblefor preventive care.
In HDHPs, the total deductible and other annualout-of-pocket expenses, other than for premiums,cannot exceed $5,000 for an individual and$10,000 for family coverage, with this exception:In network plans, the maximum allowable out-of-pocket expense may be exceeded due to highercosts for out-of-network services.
Individuals with an HSA and a high-deductibleplan may also have coverage for:
■ Workers’ compensation;■ Specified disease or illness coverage; and,■ Hospitalization per diem.
Any “eligible individual” may establish an HSA.The contributions belong to the account-holderand are completely portable. Every year, moneynot spent may remain in the account and gaininterest tax-free, just like an IRA. Unused amountsremain available for later years, unlike amounts inFSAs, which are forfeited if not used by the end ofthe year.
An “eligible individual” is someone who: ■ Is covered under a high-deductible health
plan;■ Is not entitled to benefits under Medicare;
and■ May not be claimed as a dependent on anoth-
er person’s tax return.
22 | Wye River Group on Healthcare

Tax-advantaged contributions can be made to anHSA in three ways:
■ The individual and family members can maketax-deductible contributions to the HSA evenif the individual does not itemize deductions;
■ The employer can make contributions that arenot taxable to either the employer or theemployee; and,
■ Employers with cafeteria plans can allowemployees to contribute untaxed wagesthrough a salary-reduction plan.
Funds distributed from the HSA are not taxed ifthey are used to pay qualifying medical expenses.Thus, an HSA essentially is a second-generationMSA with far fewer limitations. Any employer –including partners, sole proprietors and S corpora-tion 2% shareholders – may offer the accounts.Employers and employees may contribute, unusedfunds roll over for future years’ medical expenses,and individuals own the accounts. Plan rollovers–when changing employers, for instance—are lim-ited to one per year.
Preventive care: Although an HDHP generally cannot pay benefits until the high deductible is met, preventive care, and related treatment,such as removal of polyps found during a routinecolonoscopy, is an exception. Such services maybe covered by an HSA or through the HDHP beforethe deductible is met.
In addition, drugs or medications may be consid-ered preventive when taken by a person who hasrisk factors for a disease that has not yet mani-fested or to prevent recurrence of a disease.
Trust requirement: HSAs must be funded througha trust and used exclusively for qualified medicalexpenses. There must also be a plan documentthat limits contributions to no more than $4,500per year for individuals up to age 55. The maxi-mum contribution may be increased by $1,000 in2006 for those over 55. The contribution cap issubject to cost-of-living adjustments.
HSA assets cannot be commingled with other prop-erty, except in a common trust fund or commoninvestment fund, and are the property of the indi-vidual—not the employer that establishes thefunds. Thus, HSA funds are portable when an indi-vidual leaves an employer, regardless of the reason.
Tax treatment of HSAs: Contributions to and pay-ments from an HSA are excluded from taxable
income if they are used exclusively for qualifiedmedical expenses, within the following limits: Themaximum excludable contribution under a high-deductible plan is
■ $2,250 for an individual or the amount of theplan deductible, whichever is less; and$4,500, or the plan deductible, for a family.The dollar amounts date from 1997 and aresubject to annual cost-of-living increases.
Both the HDHP and HSA may be provided througha cafeteria plan. However, special provisions applyregarding HSAs provided through a cafeteria plan:
■ Accelerated contributions by the employer arenot required;
■ Individuals may make mid-year contributionand participation election changes at anytime; and,
■ Employers may incorporate negative elections.
Qualified medical expenses: Qualified medicalexpenses include diagnostic and curative services,mitigation and treatment of medical conditions orprevention of disease. They also include trans-portation primarily for and essential to medicalcare, and qualified long-term care services.
Prescription drugs may be covered, but over-the-counter drugs are not. Nor are health insurancepremiums qualified medical expenses for HSA pur-poses, with the following exceptions:
■ COBRA continuation coverage premiums;■ Premiums for long-term care insurance;■ Health plan premiums while an individual is
receiving unemployment compensation;■ Any health insurance other than a Medicare
supplemental policy if the person is age 65 orolder or meets certain disability requirementsunder the Social Security Act.
IRS guidance on HSAs also provides that an indi-vidual may use HSA funds to pay for medicalexpenses of a spouse or dependents, even whenthe spouse or dependent is covered under a non-HDHP. If HSA distributions cover expenses that arealso reimbursed through another health plan, theHSA distributions would be taxable. If a husbandand wife have separate HSAs, either spouse mayuse his or her account for medical expenses of the other.
A distribution does not have to be made in theyear the medical expense is incurred to be exclud-able from income, as long as the individual hasrecords to show: that funds were used exclusively
An Employers’ Guide to Healthcare Consumerism | 23

for qualified medical expenses; the expenses havenot been previously reimbursed from anothersource; and the expenses have not been taken asan itemized deduction in a prior year.
If an individual elects to pay qualified long-termcare insurance premiums with HSA funds made bysalary-reduction through a cafeteria plan, theexcludable distribution is limited to the annuallyadjusted amount allowed under tax code section213(d)(10). If the premium paid through the HSAdistribution exceeds the allowable LTC premium,the excess not only counts as taxable income, itmay be subject to a 10% tax penalty as well.
Similarly, taxes and 10% penalties are imposedwhen HSA funds are used for prohibited expenses,unless the payment is made after the account-holder becomes disabled or dies. In the event ofthe latter, the funds must go to a designated ben-eficiary’s account or be subject to taxes.
There is no penalty if funds are transferred toanother HSA within 60 days of payment from theoriginal HSA or in the case of a similar transferunder a divorce or separation document.
Special rules apply for married couples when bothhave HSA coverage. If one has family coverage,then the couple is regarded as having family cov-erage.
COBRA: HSAs are not subject to COBRA, althoughHDHPs are.
Non-discrimination: HSAs are subject to tax codenon-discrimination rules, which require employercontributions to be “comparable” for eligible indi-viduals. Contributions are considered comparable ifthey are either the same amount or the same per-centage of the deductible under the HDHP. Theremay be different contribution levels for full-timeand part-time employees, however.
The overriding question left is whether there canbe different contributions based on classificationsof employees, such as by years of service or byemployee “matching” contributions to HSAs.Comprehensive guidance from IRS allows some dif-ferent contribution schedules, but only throughcafeteria plans. Specific guidance is as follows:
■ Employers may not make matching contribu-tions that would result in some individualsreceiving different contributions than other
individuals based on the individuals’ contribu-tion rates. However, an employer may makematching contributions through a cafeteriaplan based on each individual’s contributionto it.
■ HSA distributions are not subject to nondis-crimination rules of section 105(h), whichapply to self-funded plans generally.
Unless contributions to an HSA are made under acafeteria plan, an employer may not base them onan individual’s participation in health assessments,disease management programs or wellness pro-grams.
Account administration: Employers may chargereasonable administrative fees for HSAs. Underaccount administration guidance HSA funds maybe placed in investments approved for IRAs (e.g.,bank accounts, annuities, certificates of deposit,stocks, mutual funds, or bonds) or in certain typesof bullion or coins. However, they may not beinvested in life insurance contracts or in col-lectibles. The HSA trust or custodial agreementmay restrict investments to certain types of per-missible funds.
Strategies For Use Of Accounts
The consumer-directed healthcare purchasingmovement is just the first step in a new approachto getting control of rapidly increasing healthcarecosts which emphasizes individual responsibility.
HRAs and HSAs, along with FSAs, should furtherthis objective by enabling employers and otherplan sponsors to define their liability at leastsomewhat, while putting more decision-making –and thus responsibility – in the hands of employ-ees. There are certain design considerations andmarket issues that will affect the success of suchconsumer-directed purchasing efforts.
While immediate cost-savings should not be thesole purpose of medical accounts associated withconsumer-directed health care, some immediatesavings may be achieved. Long-term savings aremore likely to result from healthy behavior andlifestyle choices that CDHC encourages throughdisease management, healthcare coaching andother wellness programs.
For HRAs and HSAs to bring immediate cost-sav-
24 | Wye River Group on Healthcare

An Employers’ Guide to Healthcare Consumerism | 25
ings, there must be high-deductible plans thatoffer sufficient premium discounts to providemeaningful savings to employers. For insuredmajor medical plans, cost savings will depend oncarriers’ willingness to offer products with adeductible that is high enough to sufficientlylower premiums and thus provide savings to plansponsors.
Then, there will be the issue of rising premiumsfor the high deductible plans to offset losses fromthe reduction in the market for lower-deductiblecoverage. It addition, there will have to be choic-es associated with major medical plans thatrequire individuals make informed decisions and becost-conscious in shopping for health coverage.
Employers that self-insure, on the other hand,have the flexibility to set their own deductiblelevels and are more likely to see advantages fromHRAs.
A plan sponsor may terminate its dental andvision plans and instead allow related expenses tobe reimbursed from the HRA, for example, thusreducing multiple plan administration costs. Forsmaller plan sponsors unable to otherwise providedental and vision coverage, an HRA could be intro-duced with the explanation that the purpose is toreimburse dental and vision as well as major med-ical expenses. The plan sponsor is thus able to tellemployees they are, in essence, receiving dentaland vision coverage—but to do so at minimal, ifany, extra cost to the employer.
Because of the potential relation of an HRAamount to a health plan funded at least in partthrough employee pre-tax salary reduction, a fixedlevel contribution to an HRA regardless of thechoice of health plan option may be needed. Therestill could be tiered HRA contributions, dependingon circumstances, such as one contribution levelfor single coverage and a second level for familycoverage.
Order of payment: Generally, under regulationsgoverning FSAs, a medical expense that’s reim-bursable under any part of the health plan—orany other health plan—may not be reimbursedfrom a medical FSA. Under normal IRS rules, ifcoverage is provided under both an HRA and aSection 125 FSA for the same medical expense, theHRA funds must be exhausted before reimburse-ments are permitted under the FSA. However, the2002 IRS ruling allowed reversal of the ordering
arrangements. Thus, a violation does not occur ifthe medical plan has contract language that isproperly written. A plan with a combination ofaccounts can not provide double reimbursements,of course.
Requiring FSA payment first may force individualsto be more judicious in their use of medical care.If the ultimate goal is to enable employees tosave toward post-retirement medical expenses,then requiring reimbursement to come from theFSA first may make more sense.
Cost-containment plan designs: Plan sponsorswill have to exercise care in creating incentivesfor participants to minimize healthcare spending.Providing rewards, such as bonuses, will have tobe unrelated to HRA or HSA balances.
Non-discrimination rules: The extent of ultimateemployer liability will depend in part on whetherthe plan allows accumulated HRA funds to beavailable after termination or retirement, or both.Plan sponsors may first want to allow such carry-over as a perk for senior management. However,the nondiscrimination rules must be considered.The plan may end up being discriminatory, eitherforcing plan sponsors to make the post-termina-tion coverage available to everyone or exposingsenior management to income tax liabilities.
Medical expenses limitation: The guidancespecifically limits HRA reimbursements to taxcode-defined medical expenses. A major medicalplan may cover treatment that does not meet thetax code definition of medical expense, such ascosmetic surgery that is not related to post-injuryor post-surgical reconstruction, in which case thereimbursement amount counts toward grossincome. Such expenses should not be reimbursedthrough an HRA.
COBRA: It is not clear from the guidance how pre-miums would be determined. Apparently, the samerules—that COBRA premiums are 102% of the fullannual employer contribution— would apply as formedical FSAs. An individual would not elect COBRAfor an HRA unless there had been carryover of
The consumer-directed healthcare purchasing movementis just the first step in a new approach to getting control of rapidly increasing healthcare costs whichemphasizes individual responsibility.

prior years’ amounts that would make the electionworth the cost. For example, if an HRA balancehad accumulated to $4,500 for an arrangementwith a $1,000 annual contribution, the individualwould pay $1020 to have a right to reimbursementof $5,520 ($4,500 + $1020 = $5,520). Dependingon what the plan sponsor ultimately wants toachieve, there could be a limit on the maximumbuild-up.
The Future?
The concept of a 3rd generation personal careaccount (PCA) focuses on the impact of employeehealth on broader corporate metrics of productivi-ty, absenteeism, “presenteeism,” turnover, acci-dent rates, etc. PCAs will need to accommodateincentives and rewards for broader corporate ini-tiatives. For example, they could be structured sothat the funds are increased if an individual orgroup meets predetermined performance, safety, orsales standards. A mix of individual and groupawards would add a new dimension to the totalcompensation package, making PCAs the new “fre-quent flier” program.
4th generation PCAs would focus on the individualcharacteristics and lifestyle needs of each member.As employees become familiar with HRAs andbegin to accumulate sizeable sums, they will likelydemand more ownership and security of thefunds—with guaranteed portability, a feature thatwould have to be created with additional legisla-tion. Vesting issues and “notional interest” willbecome increasingly important to employees tosecure the value of their accounts. Eventually, too,demand will grow for more immediate use of thefunds for non-plan-qualified medical expenses(QMEs) and for paying health premiums.
Employees may also want the right to bolster theirHRA accounts by cashing in unused vacation orsick leave. Finally, PCAs will likely need to accom-modate personal lifestyle expenses such as variousalternative medical modalities. and, perhaps, theability to use debit/credit cards to cover Internetpurchases and cyber-office visits. The IRS willhave pressure to expand the definition of QME toencompass cosmetic surgery and other personalcare services.
26 | Wye River Group on Healthcare

As noted in Chapter I, medical consumerism isabout much more than financing vehicles. Theconcept, in its maturity, takes a broad look at theimportance of improving the health of the entirepopulation, not just at developing new ways tofinance healthcare services. If we are to optimizethe advantages of medical consumerism and miti-gate its potential drawbacks, there will need to bea significant shift in the focus of the delivery sys-tem from “sick” care to “health” care. The empha-sis must be on the continuum of care, from pre-vention and primary, or wellness, care to tertiarycare and disease management.
Preventive Care: The Promiseof Wellness
Consumer directed healthcare plans typically mini-mize barriers to obtaining preventive care. Themajority of CDHC designs include 100% coveragefor preventive care so that plan participants canfocus on maintaining good health and accumulat-ing funds for future medical needs. Extensive pre-ventive care coverage provides a greater potentialfor carryover of unused funds, since the cost ofpreventive services will not be deducted from HRAor HSA accounts.
Wellness care can be defined as a proactive,organized program providing lifestyle and med-ical/clinical assistance to help employees andtheir family members maintain good health.Wellness programs encourage voluntary behaviorchanges and support compliance with provenapproaches to maintain health, reduce health risksand enhance productivity.
As shown below, most employees (83%) fall intothe low and medium categories of healthcarespending. It is in an employer’s best interest tokeep employees in the low-user category by pro-viding preventive care and wellness-lifestyle sup-port. It is also important to minimize the cost of
acute conditions with early intervention and ofchronic conditions with wellness care and diseasemanagement. With consumerism, the power ofemployee self-interest and financial incentives areused to support lower costs and better health,both of which benefit the employer as well.
One of the unfulfilled promises of HMOs is thedelivery of member wellness and prevention. Underplans with first-dollar coverage, employee wellnessprograms were often inconsistent with the market-ing hype, and underutilized even when available.Employers feared that they would incur theexpense of wellness programs but that, because of high turnover, the benefits of such programswould accrue to other employers. Under CDHC HRA plans, the employer—not the HMO—decideswhat preventive care is covered and how much isreimbursed. And there is greater awareness of
Chapter IV
The Supply Side: Supportive Services & Programs
An Employers’ Guide to Healthcare Consumerism | 27
Employers can help keep employees in the low-user category by providing preventive care and wellness-lifestylesupport, and can minimize the cost of chronic conditionswith disease and care management.
Disease Management—How Does It Impact Employees and Family Members?

28 | Wye River Group on Healthcare
employer payback through increased productivityand better job performance.
Knowledge alone does not change tough healthbehaviors among the masses of people with littlemotivation. A person may have timely, accurate andscientific based knowledge on what needs to be done
to live healthier, but unless this knowledge is convert-ed into tangible and sustainable behavior change, thepromise of consumerism will never be fulfilled.
It is critical to address the gap between knowingand doing when designing a wellness program. Afull complement of tools is needed to educate andempower consumers and, ultimately, to change theirhealth habits and medical purchasing. Full servicewellness programs offer some or all of the following:
■ Health Risk Assessment ■ Health screenings■ Effective communication programs
– Health awareness– Program enrollment– Health education
■ Web-based software programs■ Printed materials when appropriate■ Collection and analysis of data
– Medical claims– Pharmacy claims– HRA data– HR data
■ Benchmarking and reporting■ The Prochaska Transtheoretical Model for
behavior change■ Health coaching
– Coaches from multiple disciplines– Extensive training around the science of
health behavior change– One-on-one patient-coach relationships
■ Health concierge services– Extensive knowledge of employer’s full
benefit plan– Ombudsman for all health and behavioral
health benefits– Customized research for local community support services
■ Incentives– Participation– Outcomes
■ Worksite fitness centers
IRS defined preventive care: Because the lawallows 100% coverage for preventive care, the IRShas authorized preventive care coverage at 100%for HSA eligible high-deductible health plans(HDHPs), without a need to meet the front-enddeductible. Wellness and preventive servicesapproved by the IRS as “safe harbor” benefitsinclude those listed in the chart.
Additional preventive care guidelines and safe har-bor definitions for HRAs were released in March2004 by the IRS.
Knowledge alone does not change tough health behaviors. It is critical to address the gap between
“knowing” and “doing”.
Wellness Preventive Care for HSAs
Safe Harbor Preventive Care Screening Services

An Employers’ Guide to Healthcare Consumerism | 29
July 2004 IRS guidelines further clarified preven-tive care as follows:Notice 2004-23 sets out a preventive care deductiblesafe harbor for HDHPs under section 223(c)(2)(C).Solely for this purpose, drugs or medications areconsidered preventive when taken by a person whohas risk factors for a disease but is asymptomatic orto prevent the recurrence of a disease.
For example, the treatment of high cholesterol withcholesterol lowering medications (e.g., statins) toprevent heart disease or the treatment of recoveredheart attack or stroke patients with angiotensin-converting enzyme (ACE) inhibitors to prevent arecurrence would constitute preventive care.
Drugs or medications used as part of preventivecare services specified in Notice 2004-23, includ-ing obesity, weight-loss and smoking cessationprograms also qualify. However, the preventivecare safe harbor under section 223(c)(2)(C) doesnot include any service or benefit, including med-ications, intended to treat an existing illness,injury, or condition.
Broader approaches to preventive care: 2nd generationInformation by itself will not move everyone tobetter care or better health. Second generationpreventive care programs provide incentives andawards. Because information alone is often inef-fective, 2nd generation preventive care plansreward participation in wellness programs orhealth risk appraisals, for example. In addition,employees who demonstrate specific desirablehealth habits may receive points that convert todiscounts, rebates, or improved coverage (e.g.non-smoking programs, health club membership,corporate sponsored runs, etc.).
An HRA with incentives offers individuals thepotential to address underlying health conditionsnot covered by traditional insurance. For example,a patient with high cholesterol and a family histo-ry of heart disease might find it extremely valu-able to have a CT scan to determine the degree ofcalcifications. Although this test is typically notcovered by insurance, the information it revealsmay help motivate the patient to comply with hismedication regimen. Similarly, depending on theCDHC design, consumers who believe in the valueof complementary and alternative medicine canpotentially benefit from an HRA in which individ-ual treatment choices can be covered based uponpatient preference.
These approaches combine personal responsibilitywith patient financial involvement to incentivizeprogram participation and foster compliance aswell as better personal health management. Thepossibilities are many and depend on what type ofbehavior an employer aims to encourage.Incentives that reinforce a culture of health, well-being, self help and shared responsibility can havea significant effect on outcomes.
Broader approaches to preventive care: 3rd generation The concept of 3rd generation preventive carefocuses on linking individual health to businessperformance metrics like productivity, attendance,and turnover. Thus, it emphasizes programsdesigned to maintain or improve the functionalityand performance of a particular population.Measurements are being established to link per-sonal safety, occupational hazards, accident pre-vention, prevention of worksite violence andstress, among others, to overall corporate produc-tivity and costs.
Calculating the return-on-investment (ROI) forpreventive care and wellness programs continuesto be challenging due to the multitude of vari-ables that influence health status and businessperformance. However, some employers are exam-ining the correlation between employee participa-tion in health promotion and wellness programsand direct medical costs and some business-unitoperational metrics. The link between health andother performance issues will continue to developas 3rd generation plans evolve.
Organizational stress: Stress costs U.S. business-es over $400 billion per year, according to theBureau of Labor Statistics. Indeed, stress has beenfound to be responsible for an estimated 22% ofhealthcare spending, 40% of employee turnover,
Second generation preventive care programs provideincentives and awards to enhance motivation to makechanges that will lead to improved health.
3rd generation preventive care links individual health to business performance metrics like productivity,attendance, and turnover.

and 50% of workers’ compensation, non-occupa-tional disability, absenteeism, and presenteeism.
Employers can design programs, however, to effec-tively address the effects of the demands andpressures on their employees. Stress managementprograms can help employees learn to use self-help tools, accept personal responsibility for solu-tions, master strategies to diminish the negativeimpact on their health and behavior, and do theirpart to establish a positive environment at homeand at work.
For many companies, 3rd generation stress man-agement programs can link healthcare, con-sumerism, and organizational quality, safety, anderror reduction. Depression in the workplace, amajor problem at many companies, needs to beaddressed as well.
Broader approaches to preventive care: 4th generation Personalized and individualized prevention andearly intervention will be the hallmark of 4th gen-eration medical consumerism. Personalized carewill utilize genomics, predictive modeling, andpush technology, and preventive care will includeboth lifestyle and clinical factors.
Preventive care is identified by the procedure(CPT) and diagnostic code submitted by a physi-cian. Preventive services are scheduled based onrecommendations by recognized experts, such asthe US Preventive Services Task Force, theAmerican Cancer Society, and the American Collegeof Obstetrics and Gynecology.
The charts below summarize the recommendedclinical screenings and immunizations for adultsage 18 and over. Beyond limiting preventive bene-fits to specific dollar amounts, which is a commonapproach, employers can safeguard against abuseby specifying the type of services and the frequen-cy with which they will be covered. The patientwill have little incentive to make multiple requestsfor benefits, as payment will be denied for servic-es that exceed the recommended limits.
By definition, a routine physical is a medical examperformed by a physician for a reason other thanto diagnose or treat a suspected or identifiedinjury or disease. Therefore, if the patient is ill orseeking treatment of a medical condition, the doc-tor cannot bill for a routine visit.
30 | Wye River Group on Healthcare
Recommended Clinical Screenings
Blood pressure Height & Weight Physical and mental status assessment including:
- Clinical breast exam - Clinical testicular exam - Complete skin exam
Serum Cholesterol/HDL Urinalysis screening Hemoglobin & Hematocrit Digital rectal examStool for occult Blood
High Risk Testing/Screenings • Tuberculin Testing • HIV Screening• Barium Enema• Colorectal Screening (includes colonoscopies and
sigmoidoscopies)
Immunizations
Tetanus-diphtheria (Td) booster every 10 yrs.
MMR for persons born after 1956 who lack evidence ofimmunity to measles
Varicella vaccine with no history of chickenpox.
High Risk Immunizations: • Hepatitis B - for adults at increased risk for hepatitis B • Pneumovax• Meningococcal• Hepatitis A
Age 18 – 39: One exam every 24 months

An Employers’ Guide to Healthcare Consumerism | 31
Recommended Clinical Screenings
Height & Weight Physical and mental assessment including:
- Clinical breast exam - Clinical testicular exam - Complete skin exam
Serum Cholesterol/HDL Urinalysis screening Hemoglobin & Hematocrit Digital Rectal Exam Stool for Occult Blood Baseline EKG; once between ages 40-64 Sigmoidoscopy; baseline at age 50-55 then every 3 – 5 years.
High Risk Testing/Screenings:• Tuberculin Testing • HIV Screening• Barium Enema• Colorectal Screening (includes colonoscopies and
sigmoidoscopies)
Immunizations
Varicella vaccine with no history of chickenpox.
Tetanus-diptheria (Td) booster every 10 years
High Risk Immunizations: • Hepatitis B - for adults at increased risk for hepatitis B • Pneumovax• Meningococcal• Hepatitis A
Age 40 – 64: One exam every 24 months
Recommended Clinical Screenings
Blood Pressure Height & Weight Physical and mental status assessment including:
- Clinical breast exam - Clinical testicular exam - Complete skin exam
Serum Cholesterol/HDL Urinalysis screening Hemoglobin & Hematocrit Digital Rectal Exam Stool for Occult Blood Sigmoidoscopy - every 3-5 years
High Risk Testing/Screenings:• Tuberculin Testing • HIV Screening• Barium Enema• Colorectal Screening (includes colonoscopies and
sigmoidoscopies)
Immunizations
Tetanus-diphtheria (Td) booster every 10 yrs.
MMR for persons born after 1956 who lack evidence ofimmunity to measles
Varicella vaccine with no history of chickenpox.
Influenza vaccine annually
High Risk Immunizations: • Hepatitis B - for adults at increased risk for hepatitis B • Pneumovax• Meningococcal• Hepatitis A
Age 65 & over: One exam every 12 months

Cancer screenings as preventive care
PSA: – Covers prostate specific antigen (PSA)screening of males age 40 and older nd men underage 40 who are at high risk for prostate cancer asa preventive service. Risk groups include African-Americans and those with a family history ofprostate cancer.
Note: Diagnostic PSA testing is also covered,regardless of preventive benefits, for men of allages with signs or symptoms of prostate cancer,and for follow-up of men with prostate cancer.
Mammogram: - Covers annual mammographyscreening for asymptomatic women age 40 andolder and younger women who are judged to be athigh risk by their primary care physician.
Note: Diagnostic mammography of women withsigns or symptoms of breast disease is coveredregardless of whether the woman has preventivebenefits.
Annual routine ob/gyn exams, including a Papsmear for all women, is covered.
Disease Management:The Promise of ControllingChronic Conditions Disease management (DM) is a proactive, organizedprogram providing lifestyle and medical/clinicalassistance to employees and their family memberswith chronic conditions. DM programs encouragevoluntary behavior changes and support compliancewith proven medical practices designed to stabilizeconditions, reduce health risks and enhanceindividual productivity.
Categorizing the covered population as non-users,low users, medium users, high users, and veryhigh users helps to find the most effective pro-grams and sources of savings. DM programs typi-cally target patients with chronic diseases such as
diabetes, asthma, and congestive heart failure, aswell as hypertension, depression, and back pain.Many employers also offer DM programs foremployees suffering from co-morbid complicationsof two or more conditions.
Such programs typically include an active outreachcomponent: Disease-specific educational materialsand reminders about adherence to various treat-ment guidelines are sent to patients. Nurses whoact as coaches on phone lines staffed 24/7 alsoplay a major role as patient advocates and educa-tors. Additional educational efforts are directedtowards providers, typically covering treatmentguidelines, research updates and updates on a par-ticular patient’s progress (or lack of progress) inadhering to a particular treatment regime.
The growth of disease management: As a rule,about 20% of the population generates about 68%of healthcare claims, while chronic conditionsaccount for about 16% of claims and representabout 41% of total plan payments. Clearly, a focuson chronic illness is likely to have a payoff interms of improving health and lowering costs.
There are currently 160 to 170 disease manage-ment companies in the United States, but manyare expected to consolidate over the next fewyears. According to the Disease ManagementAssociation of America (DMAA), the disease man-agement process:
■ Supports the physician-patient relationshipand plan of care.
■ Emphasizes preventing medical complicationsby following evidence based practice guide-lines and patient empowerment strategies.
■ Evaluates clinical, humanistic and economicoutcomes on an ongoing basis.
According to the Disease Management PurchasingConsortium, revenues for outsourced DM servicesgrew from $70 million in 1997 to about $500 mil-lion in 2001. The Boston Consulting Group proj-ects that this market could expand to $10 billionby 2010. A PricewaterhouseCoopers study foundthat 44% of large employers offered a DM programin 2000, up from 14% in 1995.
Three separate areas can be identified, with spe-cialty services and vendors for each. There seemsto be a growing demand for comprehensive singlevendor solutions.
■ Basic DM services target broad populations of
32 | Wye River Group on Healthcare
DM programs encourage voluntary behavior changes andsupport compliance with proven medical practices
designed to stabilize conditions, reduce health risks andenhance individual productivity.

patients with chronic conditions. But somespecialized firms focus on specific clinicalareas such as respiratory care, renal care, dia-betes, or high risk pregnancy, including:
AirlogixRMS Health ManagementDiabetixPadios Health ServiceCurrahee Health Solutions
■ DM companies specializing in multiple diseases, with an integrated approach, using case management of patients with co-morbidities:
LifeMasters Supported Self CareAmerican HealthwaysCorSolutionsSHPSHealth Dialogue- (offers patient support for making decisions about specific conditions like low back pain and prostate cancer.)
■ High-risk patient management targets patientswith complex conditions expected to be themost expensive within a population, ratherthan specific disease categories. Predictivemodeling is used to help identify patients whoneed this service. Examples of companies tak-ing this approach include:
StatusOneFutureHealthFranklin Health
2nd generation disease management:Specialized DM vendors have developed programsfor a dozen or more conditions. These 2nd genera-tion programs typically include incentives and afocus on self-care. Those with rewards for compli-ance with evidence-based treatment guidelines areproving to be effective.
Disease management program results are still pre-liminary, however, because of limited data and thedifficulty of definitively linking program participa-tion to outcomes among chronically ill patients.Some employers and health plans have demon-strated that specific DM programs improve patientcare and reduce medical service utilization, butevidence varies widely across health conditionsand the types of interventions. The most effectiveprograms combine information and support withfinancial incentives.
Although reported ROI can range from 1-to-1 to
5-to-1, most vendors guarantee savings at leastequal to the cost of the DM program.
Most DM programs are voluntary, so the decisionto participate is entirely up to the patient—andgetting people to do so has proven to be a majorchallenge. In some cases, data mining of prescrip-tion drug use and other health services can assistin determining the potential value of DM for anindividual. HIPAA and privacy concerns can beeffectively addressed while providing valuableinformation and self-help for DM candidates.
3rd generation disease management: Employeeproductivity, disability, unscheduled sick leave,workers’ compensation and the like are the focusof 3rd generation programs, in addition to healthand healthcare costs.
An important tool for discovering the key areasaffecting the business entity is to have all employ-ees participate in a Health Risk Assessment (HRA.)Aggregate information based on this type of popu-lation management tool can direct an employer’seducation, DM and worksite assistance efforts.
It is difficult to conceptually segment 3rd genera-tion disease management programs from otherefforts to positively affect human capital. Below isa spectrum of programs that promise to producesavings for the health benefit budget if they’reproperly integrated—and can go much further inproducing an efficient, optimally functioningorganization.
Another view of 3rd generation consumerism anddisease management opportunities is to integratepopulation management, disease management,case management and quality management.
4th generation disease management: The con-cept of 4th generation disease management focus-es on the individual. It looks at each beneficiary’slifestyle and clinical needs and the impact on hishealth and healthcare concerns. The 4th genera-tion disease management programs will useInternet based information and services, offermore personalized support and be more integratedinto the life of the patient via cyber connections. The future will include new tools that support per-sonalized disease management programs to assurethe delivery and impact of evidence based medi-cine. Imagine a world with a cyber-aide that con-tinuously searches the Internet for the latestinformation and research on your disease state.
An Employers’ Guide to Healthcare Consumerism | 33

Imagine a world with wireless connections forcontinuous streaming of vital signs, creating realtime test results that make it possible to monitortreatment progress.
In 4th generation DM programs, information will belinked on an interactive basis to actual care. Patientlifestyle and cultural differences will be accommo-dated. Consumers will receive holistic care, as theintegration of mind, body, and spirit develops. And,prescription drugs and other therapeutic treatmentswill be customized, based on the genomics andphysical characteristics of the patient.
For example, consider a 4th generation DM pro-gram that focuses on the individual and personal-ized profiling, with self-help direction for stressmanagement. Because of the historical stigma andbenefit limitations on mental healthcare, emotion-al issues like stress and depression have not beenadequately addressed. Yet we know that manyphysical symptoms and associated medical costshave a root cause of stress or depression which, ifaddressed directly and adequately, could mitigateboth health costs and problems.
Information Therapy andOther Tools
Cyber-health aides: Some aspects of personalizedhealthcare are already developing. The future willinclude mind-boggling decision support systemsand wireless connections that link each person toa personalized health and healthcare cyber-sup-port system. Such systems can be built to profileactivity and anticipate areas of interest.
In the future, we will likely be connected to serv-ices through monitors that will provide real timefeedback on health status, lifestyle, and healthconcerns. Healthcare cyber-feedback may providedaily results of calorie expenditures and suggest adietary menu for dinner, for instance. A personal-ized cyber-aide may seek out and suggest health-related vacation packages or personalized exerciseequipment through Internet searches or automaticcyber-auctions.
Predictive Modeling: Consumerism and relatedhealthcare programs are expanding into sophisti-cated predictive modeling programs that identifyproblem conditions and produce early warningnotices to patients. Genomics testing will add tothe personalized approaches as future scientificdevelopments occur. With the use of the Internetand web portals, vendors with disease manage-ment programs and predictive modeling now havea channel to rapidly communicate with thepatient.
Push technology: Push technology refers to aprocess of timely delivery of needed informationand self-help advice to consumers—before theyrequest it. The idea is to identify potential problems and suggest an appropriate course of action well before they become serious andcostly –conditions
34 | Wye River Group on Healthcare
• Holistic Health & Productivity Focus • Culture of Health & Wellbeing• Seamless Population Management• Shared Responsibility/Accountability• Organizational Alignment & Support• Data Driven Process Excellence
3rd Generation “Account Based” Benefits and Incentives Platform
Wellness Prevention DemandManagement/
EAP
DiseaseManagement
Case Management
AbsenceManagement
Optimizing Individual and Organizational Health & Performance
Disciplined Approach to Deliver Short Term and Long Term ROI

Electronic Medical Records: EMR, which manyhealthcare systems and providers are alreadyusing, will be the foundation for accurate, consis-tent, and integrated preventive care and medicaltreatments. The next decade will likely see thefederal government establish standards that makeit possible for hospitals and health systems acrossthe country to have instant access to patients’medical history through a national network ofelectronic medical records.
An Employers’ Guide to Healthcare Consumerism | 35
Optimizing Health & Performance

36 | Wye River Group on Healthcare

As healthcare benefits develop into modelsdesigned to meet individual needs, decision aidswill need to be coordinated with plan design toensure that the benefits provided are effective.Likewise, as accountability shifts to the consumer,decision-support tools must be developed withinput from the people who will use them. No twopeople are alike, nor are they at precisely thesame level of health literacy. So tools will need tobe customized— a “one size fits all” deliverymode will not work in tomorrow’s consumerhealthcare marketplace.
Americans are accustomed to being in control ofwhat and how they purchase products and servic-es. They seek to make informed choices, balancingquality against price, within their budgetary con-straints, taking into account the value of anyreward or incentive. While consumers generallyexpect to have this purchasing power, many peo-ple find healthcare decision-making—and personalaccountability—to be an intimidating prospect.The reason, of course, is that the stakes are sohigh.
The idea of making informed and cost-effectivehealthcare decisions is a new concept for mostconsumers, who recognize that doing so is consid-erably more complex than, say, buying a plasmatelevision. However, some non-medical purchasingdecisions are quite complex, yet most people areable to manage them. For instance, a first-timehome buyer has a lot to learn before making sucha significant purchase. Yet the idea of owning ahome motivates us to master the details, so wecan make a decision that best fits our needs.
With new consumer-based technologies that allowa comparison of product prices, quality and thereputations of the companies selling the products,consumers are better able to evaluate options.Given the right motivation, and appropriate infor-mation coupled with the right incentives, mostconsumers can learn to make wise healthcare deci-sions as well.
In order to successfully transition from restrictiveplan designs to consumer directed strategies in away that encourages choices that promote optimaloutcomes, plan sponsors need to provide con-sumers with more support and guidance than everbefore. As the rules of the road change, so mustthe vehicles.
The key to a consumer roadmap is a robust set ofdecision-support tools. In the managed care set-ting, consumer choice has mostly been governedby plan provisions, coupled with cost-share driversto preferred providers or services. Thus, consumershave had relatively few decisions to make. Because the limited choices found within a typicalmanaged care plan are strongly influenced by plandesign, consumer tools have focused primarily onpolicies and procedures, out-of-pocket cost com-parisons, condition-specific educational materials,and retail pharmacy and provider locators.
With CDHC models, consumer out-of-pocketexpenses are driven more by broad cost-sharestrategies and less by plan design. This requiresconsumers to shoulder more of the decision-mak-ing process and the financial responsibility associ-ated with those choices.
However, decision-support tools are not limited toCDHC plans. In an era of consumerism, traditionalplan providers have also learned that such toolsare instrumental in promoting optimal choices,
Chapter V
Information & Decision Support – The Promise of Transparency
An Employers’ Guide to Healthcare Consumerism | 37
To successfully transition from restrictive plan designs toconsumer directed strategies that promote optimal outcomes, plan sponsors need to provide consumers with more support and guidance than ever before.Decision-support tools must be developed with inputfrom the people who will use them. A “one size fits all”delivery mode will not work in tomorrow’s consumerhealthcare marketplace.

38 | Wye River Group on Healthcare
regardless of plan structure. Empowered consumerslearn how to leverage any health plan to theirgreatest advantage, by learning the rules andseeking the path that best meets their needs withthe least out-of-pocket investment. In a properlyconstructed plan, the best path for the consumerwill also achieve optimal results for the plan spon-sor. In a consumerism model, plan participants gofrom being victims of benefit design to activedecision-makers, albeit within the boundariesestablished by the plan sponsor.
Let’s look at how decision support and informationhas changed and will need to evolve further inorder to be successful in CDHC.
1st Generation DecisionSupport : Account-Based Plans
The 1st generation of CDHC models focused onaccount-based benefits that placed more account-ability on the consumer. Most decision-supporttools in this setting were designed to help con-sumers make more cost-effective choices. The pri-mary goal was to reduce out-of-pocket expensesand plan costs through proactive and retrospectivecost awareness of medical services and prescrip-tions. These tools helped consumers to:
■ Compare costs of common services and treatments
■ Compare costs of prescription alternatives ■ Check tax-advantaged account balances■ Check plan benefit balances, i.e., deductible
and maximum out-of- pocket costs
Depending on the timing of healthcare utilization,cost-awareness tools are available through variouschannels, including call centers and online access.Retrospective cost-awareness tools are availablevia call centers, online, print communications, andtext messaging. Most CDHC plan providers havemade significant investments in these areas –often more than in the plan design technology
itself. In fact, decision-support tools are a vitalcomponent in successfully transitioning a popula-tion from managed care to a true consumer model.
To create an empowered consumer, plans mustprovide not only facts that encourage informeddecisions, but the means to conveniently accessinformation at the time of decision-making. Sinceindividuals differ in the ways they learn andassimilate information, a multi-pronged approachis necessary. Information should be providedthrough a variety of channels – and in a mannerthat is understandable to the consumer.
Online decision support tools: The Internet isthe most cost-effective and convenient channelfor providing information. True to the spirit ofconsumerism, Web tools have also evolved to edu-cate consumers about how to get the most out oftheir benefits – highlighting choices that encour-age cost-conscious behavior and align with plangoals. With these tools, consumers can:
■ Find in-network providers■ Access plan design summaries■ Look up formulary information■ Order prescriptions online ■ Obtain information about general health and
prescription drugs
Many plans have begun highlighting not onlymember out-of-pocket costs, but plan costs aswell. This tactic reveals the monetary value of thehealth benefit to plan participants and increasesawareness of the high costs of healthcare servicesthrough cost transparency. In an age in whichconsumers are becoming increasingly accustomedto Internet tools to find the highest quality prod-ucts for the lowest price, it’s a natural evolutionto carry this over to the healthcare arena.
Call center support: But a Web site alone doesnot create a consumer strategy. Prompted initiallyby CDHC niche players, mainstream health planshave begun to supplement Web tools with consult-ants at call centers. The staff at these call centersare often referred to as “advocates” or “coaches.”Their primary objective is to help consumers gaina better understanding of the nuances of plandesign and learn to balance cost and quality—issues that previously were hidden within complexplan policies and procedures.
Typically staffed by nurses, health educators orbenefit counselors, these call centers provide
Plans must provide not only facts that encourageinformed decisions, but the means to convenientlyaccess information at the time of decision-making.
A multi-pronged approach is necessary, with informationprovided through a variety of channels.

An Employers’ Guide to Healthcare Consumerism | 39
information pertaining to:
■ Provider choice – understanding fee schedulesof different providers within the network;
■ Procedural alternatives – evaluating cost andefficacy of various healthcare diagnostics andtreatments (e.g., understanding the differencebetween a CT scan and an MRI);
■ Symptom evaluation – determining when togo to the emergency room and when to waitfor a scheduled office visit;
■ Plan design – understanding the rules andhow to follow them;
■ General health and wellness coaching; and ■ Claims processing and appeals
Call centers are an effective means of providingconsumers one-on-one access to information thatcan help them calculate the cost/quality equationcentral to making the best healthcare choices.
Direct mail communications: Plan sponsors havea fiduciary obligation to communicate with mem-bers regarding benefits. And, although many planmembers have access to and are comfortable withthe Internet, there are still many people who arenot Web-savvy, do not own a computer or do nottrust online communications. Others prefer toreceive information by mail than to speak to astranger on the phone. This means that somedirect mail communications are still necessary.They may be used to:
■ Explain service costs and plan costs associat-ed with personal healthcare decisions;
■ Recommend generic or formulary alternativesto widely used prescription therapies;
■ Provide education about wellness and healthmaintenance targeted to individuals with spe-cific chronic conditions
2nd Generation DecisionSupport—and Beyond
As plan design strategies continue to demand moreconsumer accountability, participants will needmore sophisticated decision-support tools – particu-larly when it comes to balancing quality healthcarewith financial management. That’s where incentivesand disease management programs come in.
Over time, consumers’ sensitivity to both short-term and long-term costs will increase, including
the awareness that tactics which may offer partici-pants short-term savings could ultimately result inhigher costs to both the plan sponsor and to theindividual. For example, if a patient doesn’t takehis blood pressure medication to avoid paying theRx copay, the result could be a catastrophic med-ical event – clearly not a desirable outcome fromany perspective. Therefore, while plan sponsorsadopt account-based plan designs, many will alsobe adopting disease management and complianceprograms as a way to help consumers controlchronic conditions, improve their quality of life, increase their productivity and rein in healthcare costs.
Disease or care management programs are gearedto consumers who have been recently diagnosedwith a chronic condition as well as those whohave been living with a condition but are usingexcess healthcare resources due to poor self-man-agement. The objective is to provide individualizedguidance to patients who need this additionalsupport. Condition management programs educatepatients about their condition, help them manageit through lifestyle changes and help them complyto a treatment regimen and follow their physi-cian’s advice.
Plan sponsors are increasingly interested in med-ication compliance programs to decrease the likeli-hood of adverse events. The goal is to prevent theonset or recurrence of medical crises severeenough to require a visit to the emergency room.
The 2nd generation decision-support tools willinclude a blend of strategies to encourage con-sumer empowerment while promoting healthy out-comes. Successful plans will focus first on clinicalresults influenced by consumer choices, and thenon the financial impact associated with thosechoices. To strike this balance, plan sponsors candevelop strategies in four basic categories:
1 preventive care: Encouraging consumers to beproactive in reducing health risks, e.g., getroutine physical exams, regular exercise,adhering to drug therapy;
Consumers’ sensitivity to both short-term and long-termcosts will increase, including the awareness that tacticswhich may offer participants short-term savings couldultimately result in higher costs.

40 | Wye River Group on Healthcare
2 condition or disease management:Encouraging consumers with chronic condi-tions to adhere to their treatment regimen,e.g., taking antihypertensives as prescribed ormeasuring glucose levels routinely and under-going HgbA1c diabetes testing;
3 risk mitigation: Supporting individuals withincreased risk of adverse events in making thenecessary behavior changes, e.g., helpingsmokers with a family history of lung cancerto quit;
4 treatment management: Ensuring that con-sumers understand appropriate care options,e.g., an emergency room visit versus officevisit; a CT scan versus an X-ray, etc.
These programs use “push and pull” strategies toincentivize consumers to follow a self-care regi-men and follow their physician’s recommendations.Some mechanisms used to engage plan partici-pants include rewards and financial incentives forcompleting a health risk assessment or participat-ing in condition management or wellness pro-grams. Examples of incentives currently usedinclude:
■ Lower monthly healthcare premiums ■ Reduced co-pay or out-of-pocket costs■ Additional deposits in their Healthcare
Reimbursement Accounts ■ Airline miles■ Time off work■ Cash or gift certificates■ Vouchers for generic drugs or mail order pre-
scriptions
Individuals who could benefit from greater compli-ance and participation in a condition managementprogram can receive information and education ina variety of ways, depending on preference. Theymay choose:
■ Telephone counseling provided by nurse edu-cators;
■ Written correspondence via direct mail, phoneor text messaging, reminding them to refillmaintenance medications or to take importantclinical tests;
■ Brochures that provide detailed information
about lifestyle and management strategies fora specific condition;
■ Event-triggered communications informingparticipants that gaps in their care have beenidentified, along with recommendations onsteps to be taken;
■ Status reporting to treating physicians to helpcoordinate care; and
■ Electronic monitors that send a patient’s met-ric results, i.e., weight, blood pressure, glu-cose levels, etc., to a secure Internet site forreal-time monitoring.
Condition management and prevention programsare increasingly used not only to help beneficiar-ies stay healthier, but also to control and managetotal healthcare costs over the long haul. As plansponsors adopt consumer-directed strategies, theywill begin to integrate such programs as part of acomprehensive healthcare benefit offering, recog-nizing that the investment is likely to pay off inthe long run.
Health and performance: While condition man-agement programs focus on individuals who arealready living with a chronic condition, more plansponsors are adopting wellness programs as anoth-er tool to control rising costs. The goal is to keepemployees well and to cut costs for the consumersand the sponsors, by promoting healthy lifestylesand behavioral change. Some of the primary issuesthat wellness programs address are:
■ Disease prevention■ Stress management ■ Fatigue■ Absenteeism ■ Employee productivity
Wellness programs are less intrusive and generallydo not require as many resources as conditionmanagement programs. There are many tools thatcan be deployed that provide important informa-tion or convenient access to preventive servicesthat encourage consumers to take the necessarysteps to stay healthy. These tools can be interac-tive and fun and may have a financial incentivebuilt in. Some of the more popular tools include:
■ Discounts for gym membership■ Onsite wellness centers ■ Onsite clinics■ Onsite immunizations ■ General education via newsletters and
company intranets
Successful plans will focus first on clinical results influenced by consumer choices, and then on the
financial impact associated with those choices.

■ Online tools, e.g., calorie burn and smokingcost calculators, headache assessment
■ Online quizzes, e.g. , Vitamin ABCs, Fitness,and Emergency IQ
■ Employee volunteers who serve as wellnessambassadors
Before investing in any wellness program, a plansponsor should assess the employee population’smedical and pharmacy claims data to identify themost prevalent cost drivers—and ensure that pro-grams are developed that address specific needs.
Combining a wellness program and condition man-agement with a health plan design that offersfinancial incentives for making cost-effective deci-sions adds up to an effective arsenal of tools thatgive sponsors their best shot at managing health-care costs, promoting a healthy workforce andboosting productivity.
An Employers’ Guide to Healthcare Consumerism | 41
Before investing in any wellness program, a plan sponsorshould assess the employee population’s medical andpharmacy claims data to identify the most prevalentcost drivers.

42 | Wye River Group on Healthcare

The overall goal of a consumer-directed strategy isto provide medical plan designs that will assistconsumers in making more informed and cost-effective decisions about healthcare. The intent isto favorably affect both clinical outcomes and thecost of care. With plan design as the basic founda-tion, CDHC holds the promise of positive results,achieved through the following:
■ Breaking down barriers to good health byoffering first-dollar coverage for preventivecare, including drugs taken to prevent illnessor recurrence of a disease in high-risk individ-uals.
■ Supporting a healthy lifestyle and early inter-ventions at minimal cost to the members.Support can be in the form of information,decision support tools, change managementassistance, and incentives for adhering tohealthy habits.
■ Increasing the transparency of healthcarecosts to plan participants, who have frequent-ly been unaware of the true costs of medicalproducts and services because of managedcare’s relatively low copays. This can beachieved by switching from a design with lowcopays to a PPO plan, which typically relieson front-end deductibles and coinsurance, anda personal care account.
■ Reducing costs for “discretionary care.” CDHCdesigns promote wise consumption of health-care dollars via personal accounts and incen-tive programs. Reductions in cost are evidentin preliminary data from office visits, lab andX-rays.
■ Giving plan participants more control over andshared responsibility for managing their ownhealth and healthcare costs. When membershave such decision-making power as well asthe means to track their personal account bal-
ances, it is believed that they will learn tomake better choices.
■ Supporting the clinical and financial needs ofthose with chronic health problems. Offeringincentives in return for compliance canincrease the financial coverage availablethrough a basic CDHC model by supplementingthe funds put into an individual’s account.Taking advantage of such incentives anddoing what it takes to win awards will givebeneficiaries with serious conditions the pos-sibility of getting full or nearly full coveragethrough shared savings.
■ Supplying plan participants with the informa-tion they need to become well- informedhealthcare consumers. Those who are armedwith value- driven data make better decisions.
Roadmap to Change
There are significant issues for employers toaddress in order to establish a design foundationfor CDHC implementation. The most basic changeis the move from HMO, exclusive provider organi-zations (EPO), and point-of-service (POS) plandesigns to a preferred provider organization (PPO)model with deductibles and coinsurance. Highdeductible health plans used with individualaccounts require both a front-end deductible and amaximum out-of-pocket— legal requirements thatare inconsistent with a copayment design.
It may be possible, however, to use personal careaccounts with any plan design, as shown in thefollowing chart. The flexibility of HRAs allowsthem to be used with any plan design, as canFSAs, although the latter are limited by the use-it-or-lose-it requirement. FSAs and HRAs cannot beused to cover the health plan’s deductible.
One possible visual framework for the future of
Chapter VI
Plan Design – One Framework forConsumerism
An Employers’ Guide to Healthcare Consumerism | 43

healthcare benefits is the combination of different“generations” of consumerism and the five build-ing blocks:
■ Personal accounts (FSAs, HRAs, HSAs)■ Wellness/prevention and early intervention
programs■ Disease management and case management
programs■ Information and decision support programs■ Incentive and compliance reward programs
The first generation is primarily focused on plandesign and financing changes. The later genera-tions integrate the other critical elements foroverall success.
Regardless of the initial design selected, a medicalplan for a consumerism model ideally should haveaspects of each of these components built into itscore in order to achieve the desired effects ofconsumer involvement, changed behavior, financialsecurity and member satisfaction.
1st Generation Plan Designs
While consumerism can be built into any plandesign, the most adaptable are PPO plans. In par-ticular, 1st generation consumer plans focus on
the basic high deductible structures. The majorfocus of 1st generation CDHC is on reducing dis-cretionary expenditures.
CDHC with HRAs: Under the basic 1st generationCDHC model, members receive an annual allocationof HRA funds from their employers that they canuse to pay for covered services. These allocationsgenerally range from $500 to $1,000 per year for asingle employee and double that amount for fami-lies. Unused funds can be rolled over and added tothe next annual HRA deposit. If the HRA fund isexhausted, the member must meet a coverage gapbefore being able to use the high-deductible plan.Network discounts apply to all services regardlessof the source of payment.
First-dollar coverage is usually available for preven-tive services such as physicals, mammograms andwell-child care. HRA funds can be used to fill inplan deductibles or for copayments. If allowed bythe employer, HRAs can be used for IRS-qualifiedmedical expenses not covered by insurance, and topurchase additional health insurance—mostnotably, long-term care. The following is a tradi-tional CDHC plan design for a single employee.
HSA eligible high deductible health plans: Afterthe January 2004 effective date of the legislation,large employers began considering 1st generationHigh Deductible Health Plans. In order to realizethe tremendous tax advantages of an HSA, howev-er, they had to meet the strict plan requirementsimposed by Congress.
To qualify for an HSA, an individual must be cov-ered under an HDHP with a deductible of at least
44 | Wye River Group on Healthcare
A medical consumerism model ideally should haveaspects of each of these components built into its core.
Basic Plan Design Cost-sharing Differences
CDHC PPO with HRA Sample Design

An Employers’ Guide to Healthcare Consumerism | 45
$1,000 for individual coverage and $2,000 for fam-ily coverage and out-of-pocket caps of $5,000and $10,000, respectively. The individual and/orthe employer can make contributions to the HSAup to the plan’s deductible amount, but no morethan $2,600 for an individual or $5,150 for a fam-ily. The figures cited were for 2004; the deductibleand out-of-pocket amounts are inflation-adjustedeach subsequent year.
Below is a sample 1st generation HSA-eligible HDHPdesign. The $1,250 deductible, higher than required,forms the basis for the tax advantaged contributionsby either the employee or the employer. For employ-ees, the basic design shown below - without anemployer HSA contribution - is a very low cost planthat provides the security of catastrophic coverage.Employees can take the premium savings and estab-lish their own HSAs. Employers can also contributeto HSAs on behalf of their employees, but the totalof employee and employer deposits must complywith the legislated HSA cap.
Policyholders and covered spouses age 55 or olderhave a higher annual contribution limit, whichincreases incrementally: In 2004 the additionalamount was $500; in 2005 it increased to $600, andin 2006, it’s $700, and so on—until it reaches$1,000. However, employers contributing to HSAsmust make comparable contributions on behalf of allemployees with comparable coverage. And as long
as the funds are used to pay for qualified medicalexpenses, distributions from HSAs are not taxable.
2nd Generation Plan Designand Beyond
As large employers adopt CDHC options and createfull replacement plans, there will be a greaterdemand for customized designs. Most largeemployers consider their companies and theirworkforce to be unique. As CDHC develops accept-ance from a wide spectrum of employees, employ-ers will begin to fine tune the design options tofit their corporate metrics. Type of industry, geog-raphy, demographics, and work environment areamong the factors employers will use to determinehow to refine CDHC coverage.
2nd+ generation CDHC designs are likely to bemore flexible in determining what is chargedagainst the personal care account and what iscovered by the medical plan. For example, non-elective hospitalization could rapidly deplete anHRA account, which would remove the ability ofan HRA with a balance to roll over to serve as anincentive driving behavioral change. While 1stgeneration CDHC designs fail to take this intoaccount, designs that offer coverage for hospital-ization or other costly medical events without

46 | Wye River Group on Healthcare
reducing the funds in a personal care account maydevelop. Such an approach would ensure that PCAsthat support prudent day-to-day use of benefitsare not depleted by uncontrollable hospitalization,accidents or serious—and unexpected—illness.
Under CDHC models, prescription drugs costs gen-erally come out of the HRA account, even if thedrug is taken for preventive care or health mainte-nance. Coverage for preventive care and mainte-nance drugs will likely become more complex andtargeted as experience on behavioral changedevelops.
Future generation CDHC plan designs may be moretailored to the individual as well. For example, inorder to preserve the personal funds of a diabetic,the CDHP could be set up to deliver first-dollarcoverage for insulin and other required medica-tions. Complex CDHC plan designs based upon per-sonal health status may be a wave of the futurethat will change the way individual behavior isaffected.
However, 2nd+generation HSA-eligible HDHPoptions will require new enabling legislation.Since the 2003 Medicare Modernization Act definesa 1st generation HDHP, it is unlikely that we willsee significant changes on the political front thatwill alter the definition of HDHPs for quite sometime. Large employers tried to create design flexi-bility through recent IRS regulations. But regula-tors cannot create law, they can only interpret it,and many alternative HDHP designs that employ-ers were interested in were not acceptable basedon the July 2003 IRS guidance.
The most important—and unsuccessful—interpre-tations sought by large employers were coverageunder the HDHP deductible for prescription drugsand the use of HRA and FSA accounts for first dol-lar coverage without violation of the requirementsfor funding HSAs. Employers have also been con-cerned about the inability to dedicate their HSAcontributions exclusively to healthcare. Under finalregulations, employer-funded HSAs can be cashedout by employees, with a 10% penalty, plus recog-nition as taxable income.
There may be legislative initiatives in 2006 thataddress these and other design alternatives thatsupport flexibility in employer funding of HSAs.However, chances of passing enabling legislationare unlikely.
It is envisioned that 3rd generation plans willcontinue to build on enabling cultural change,placing an emphasis on health and performance,worksite health promotion and wellness, stressmanagement and performance. And 4th generationplans are expected to be personalized based onlifestyle and individual health, along withgenomics, push technology, information therapyand the like.
In the meantime, it is important that 2nd genera-tion CDHC plans have a greater degree of con-sumer engagement. Besides having a larger out-of-pocket “bridge,” HRAs and HSAs need to be estab-lished so that consumers can decide whether toseek reimbursement from the HRA or a distributionfrom the HSA. Such plan designs are starting totake root and are likely to move into the main-stream.
A real insurance model: Consumer directed planswith HSA funding follow other insurance models,such as car insurance or life insurance, where“good” behavior is rewarded by lower premiums orhigher savings. It remains to be seen whether anentirely market-based approach to consumer-directed spending is applicable for healthcare.
Some efficiencies may well be gained, however, bydifferentiating between the two healthcare com-ponents: the payment of risk insurance for the rarebut expensive events and the “health mainte-nance” cost for routine medical care and fromincentivizing consumer behavior accordingly.
We all understand that a third party will not payfor our windshield wipers to be replaced or for ouroil changes and tune-ups. For CDHC plans to flour-ish, Americans need to be equally certain that it isunrealistic to look to a third party to pay for rou-tine check-ups or our allergy medication as well.
Efficiencies may be gained by differentiating betweenthe payment of risk insurance for the rare but expensive
events and the cost for routine medical care.

To know where you should be going and why, ithelps to know where you’ve been and what hasbrought you to the present place. This conceptholds true for new directions and progress inrestructuring the American healthcare system ingeneral, and in developing health savings vehiclesin particular.
As a critical element in understanding the currentsituation, it is necessary to examine the relation-ship between national healthcare policy andnational tax policy. They go hand in hand, some-times smoothly and sometimes with one pullingon and straining the other.
To achieve the most effective and efficient health-care system, tax policy should be used as a tool toencourage implementation of health policy, notthe other way around. An obvious example is thetax deduction employers get for providing grouphealth coverage and the exclusion from individualincome tax for the value or cost of coverage.
Thus, healthcare coverage and health promotionshould be the goals of tax policy. The more peoplewho can be covered as a result of effective taxpolicy and health policy, the greater the risk-shar-ing, which ultimately helps keep costs down.
Tax Policy Implementation
Various savings accounts for medical care havedeveloped as tax policy tools through the TaxCode. (For a detailed discussion of the mainaccounts, see Chapter III). Following is a discus-sion of the tax policies as reflected in the keytypes of savings accounts for healthcare.
Flexible spending accounts: Health flexiblespending accounts (FSAs) allow for employer andemployee contributions to a personal account formedical expenses not paid for through anotherhealth plan. Expenses reimbursable through anFSA include deductibles and co-pays as well as
treatment that is excluded from group health plancoverage.
The FSA concept originally was intended, in part,to provide an element of choice within a cafete-ria plan financing structure. Individuals weregiven a defined amount of employer funds, com-bined with their own contribution, and theopportunity to select from a menu of benefitsthose that best met the needs of the employeeor the employee’s family. From a consumerismstandpoint, the FSA did allow choice and instilledsome modicum of individual responsibility inbudgeting certain, albeit limited, healthcare dol-lars. Tax policy was used to encourage coverage,as reflected in allowing both employer andemployee to make tax-free contributions to the FSA.
However, one feature caused the FSA to live up toits name as a spending account. Under cafeteriaplan rules, there can be no deferral of compensa-tion from one plan year to another. Thus, the“use-it-or-lose-it” rule results in forfeiture of FSAbalances at the end of the year—or the end of agrace period that employers now may include ifthey so choose. The result of this rule has been toprohibit long-term medical savings and to encour-age end-of-year spending on medical products orservices that may not be necessary.
In this case, tax policy seems to have drivenhealth policy in an inefficient and costly direction.This feature helped redirect efforts toward a moreefficient type of savings account that addressed acouple of the defining FSA issues.
Medical savings accounts: MSAs eliminated theend-of-year spending problem inherent in FSAs byallowing the rollover of unused balances from yearto year. Funds can build up, thus enabling individ-uals to save healthcare dollars.
A limiting feature of the MSA, however, is that theemployer or the employee – but not both – can
Chapter VII
Regulatory Issues – Enablers orImpediment?
An Employers’ Guide to Healthcare Consumerism | 47

contribute in the same year. Plus, the MSA mustbe offered with a high-deductible health plan.That means the MSA is likely underfunded in termsof meeting the HDHP premium and/or deductible.
Neither the employer nor employee may want, orbe able to afford, to fund the MSA to the degreenecessary for the individual to buy adequate insur-ance coverage. In addition, the MSA was designedfor—and is limited to —small employers whoseemployees tend to be lower paid. Thus, MSAs havehad limited success. Again, tax policy drove healthpolicy, rather than vice versa, and limited theMSA’s availability and effectiveness.
The healthcare market still saw the need for amedical savings vehicle that allowed for accountfunds rollover and would overcome the affordabili-ty flaw of the MSA. However, a full-blown savingsvehicle that could be funded tax-free by bothemployers and employees and allow the rollover ofunused funds could only be done by federalstatute –not an easily or rapidly attained goal.
In time, however, the market took the initiative,driven by two concepts: the need to contain rap-idly escalating healthcare costs and the relatedneed to address the public attitude of entitlementto all the medical care one desires, with theexpectation that a third party should pay for thatunlimited care.
To get such a savings vehicle, the TreasuryDepartment and IRS were persuaded to interpretthe Tax Code in such a way that self-fundedaccounts with a roll-over provision were allowed,and that large as well as small employers couldoffer.
Health reimbursement arrangements: HRAs,which came next, addressed some problems inher-ent in the MSA, but still faced major tax policybarriers that impede health policy. These includelimited financing sources and the related problemof limited ability to force a change in the entitle-ment attitude. However, the market did addressthe latter in the form of wellness programs.
Treasury and IRS rules for HRAs allow onlyemployer contributions. Account funds, like thoseof FSAs and MSAs, can be used for medical expens-es only, including health plan premiums. Fundsremaining at year-end may be carried forward and– at the employer’s option – move beyond theemployment relationship. Here, to a greater
degree, healthcare policy is achieved despite taxpolicy.
While HRAs developed with the idea that individu-als would also have high deductible health plansand thus reduce employer coverage costs, manyemployers have been willing to contribute in orderto foster the concept of individual responsibility.The hope is that individuals will become morecognizant of the costs of medical products andservices, in part by being forced to make choiceswith HRA dollars that can be used to pay premi-ums as well as deductibles, co-pays and othermedical expenses – or saved for future medicalneeds.
Employers may condition HRA eligibility on indi-vidual participation in any of a number of wellnessprograms. Included are health risk assessmentsand programs that address specific behavioral ormedical conditions. Examples include participationin smoking cessation programs, adherence totreatment regimens, and the use of healthcarecoaches to help individuals manage chronic disease.
In another development, some smaller employ-ers—or those otherwise financially unable to pro-vide traditional group health coverage—haveoffered HRAs alone. This is not an option withMSAs, which must be provided in conjunction with HDHPs.
Stand-alone HRAs offer at least minimal coveragefor those who might otherwise have no coverageat all. By doing so, they help introduce theseemployees, often low-wage workers, to the reali-ties of the healthcare system, and to engage themin medical decision-making. HRA funds may beused to help pay for coverage under state (public)or private healthcare programs and can start theprocess of behavioral change, by helping individu-als learn to accept responsibility for their healthand the healthcare choices they make.
However, tax policy still impedes healthcare poli-cy. The Tax Code prohibition against employeetax-free contributions to HRAs has left manyemployers dissatisfied. Many believe that employ-ees who have no personal contribution at stakeare not as judicious as they might be if the moneycame out of their pocket. Financially strappedemployers that looked to HDHPs as a way to saveon premiums still had to contribute to the HRAsto help make coverage affordable.
48 | Wye River Group on Healthcare

An Employers’ Guide to Healthcare Consumerism | 49
Flaws notwithstanding, this type of account doesplant the seeds of individual responsibility. Inaddition, the HRA was a major step forward in fos-tering congressional and administrative awarenessof the need for a more practical health savingsaccount.
Health savings accounts: Ultimately, tax policywas changed to address a critical flaw in the HRAand to promote a key healthcare policy feature.The result: the HSA.
Employers and employees may contribute concur-rently to HSAs on a tax-free basis, addressing lim-ited funding issues, allowing rollovers of unusedaccounts, and encouraging better healthcare deci-sion-making by consumers in part through theemployee contribution. Consumerism got a realboost through some convergence of tax andhealthcare policy.
HSAs do allow employee contributions and thusencourage individual responsibility. They do allowemployers to contribute at the same time – thusaiding access. And they do allow rollovers andthus further promote individual responsibility. Onthe other hand, HSAs do not require employer con-tributions— and thus encourage HSA offering byproviding options for employers who object toemployees’ use of healthcare funds for non-med-ical purposes.
The Promise of Tomorrow
Despite the progress made, tax policy still presentsimpediments to health policy, as reflected in thefollowing issues:
■ HSAs are not required to be structured ashealth plans and their funds may be used fornon-medical expenses.
■ HSAs are available only in conjunction withhigh deductible health plans, a provision thatlimits access to those who can afford group orindividual health coverage.
■ The non-discrimination rules in the Tax Codehave—through regulatory complexity— limit-ed implementation or increased administrativecosts of wellness programs.
■ HSA funds generally may not be used to payfor healthcare premiums or coverage (self-funded plans). Thus, tax policy limits accessby excluding individuals who cannot affordboth the premium and the high deductible.
These limitations beg the question: What kind ofaccount, or what combination of accounts, isneeded to achieve optimal healthcare policy?
First, there has to be a clearly defined optimalhealthcare policy. Then, there must be a fiscalcommitment to achieve it. With such a commit-ment, tax policy would have to follow (rather thanlead) to help us achieve that optimal vision. That,in turn, would require tax policy to be consistentwith healthcare policy.
The current funding of healthcare has created arti-ficial segmentation of healthcare coverage, both inthe private and public sectors.
In the private sector, coverage from birth toadulthood is typically provided by the parents’employer(s). That is the first financing segment.Once an individual enters the working world, hisor her coverage is provided by a different employ-er— the second financing segment. The third seg-ment comes post active employment, when theindividual is covered through employer-sponsoredretiree coverage, individual coverage, or Medicare.The fourth segment may involve long-term care orassisted living, and the fifth and final segmentoften involves hospice care. These segments arenot necessarily distinct and may overlap—or evenbe skipped, but do serve to illustrate the segmen-tation principle.
On the public side, a child may be coveredthrough a state Children’s Health InsuranceProgram, then as an adult through Medicaid, andfinally as a senior through Medicare.
Yet, health and healthcare are continuums. Healthneeds and risks vary, but typically arise primarilyin later years. The artificial segmentation offinancing does not provide a means of buildingassets for those most medically costly later years.To the contrary, risk funding may be cut off witheach segment. Thus, when an individual reachesthe most costly segments under the financing seg-mentation structure, funding to pay for care isessentially starting anew.
Retirement (non-healthcare) savings are structuredto enable a somewhat better spread of the fundingover many more years. Yet, the problem remainsthat Americans, in general, do a poor job of sav-ing. There is one asset, though, that can moreeasily be prefunded even in a period of lowincome and a culture of poor saving—and that

50 | Wye River Group on Healthcare
asset is personal health. Doing everything possibleto protect that asset – through health promotionand a healthy lifestyle, – is the least expensiveway to build assets for retirement. A person whois healthy during much of his adult life minimizesmedical problems and delays the onset of chronicconditions. That same individual remains produc-tive longer, holding high healthcare costs at bayuntil late in life. Thus, there is considerable returnon an investment in personal health.
What is needed to accommodate such a continuumof healthcare, promote healthy lifestyles and helpbuild assets for the later years? In the context ofsavings vehicles for healthcare, the answer lies inan individual account from cradle to grave.
In the broader context, programs could be estab-lished that allow for one contribution distributedactuarially, to address varying needs: lower costcoverage in the earlier, low-risk years, with excesscontributions/balances designated for accounts tobe used to buy coverage or pay directly for med-ical services in later years. There may be years,such as while raising families, where fewer dollarscan be set aside for health accounts. But thoseyears may be offset in later years when depend-ents are gone and earnings are greater. Catch-upcontributions with greater amounts in excess ofthe premium – which would be actuarially deter-mined – could be set aside for the most costlyyears as the end of life nears.
The continuum of coverage could include, in addi-tion to the savings vehicles, contributions desig-nated for group or individual coverage, long-termcare premiums, Medicare, assisted living, and end-of-life care.
The account for tomorrow: While the heading ofthis chapter refers to regulatory issues and thepromise of tomorrow, that promise must be basedin law. Allowing for the optimal healthcare savingsaccount requires more than regulatory authority:Congress and the President must address theissues.
In this regard, healthcare policy must come beforetax policy, so that the latter serves as a tool tohelp implement the former, rather than the otherway around.
Because healthcare policy must be developed inthe context of the real working world, it mustinclude factors such as the continuum of healthand healthcare needs, employment status, pay rate,fluctuations in income, and, healthcare affordabili-ty. What kind of account, or what combination ofaccounts, is needed to achieve our aim?
First, let’s consider the objectives:
■ Access ■ Individual responsibility■ Health promotion■ A personal financial stake in health and
healthcare purchasing■ Healthcare quality■ Cost control
Then, let’s look at the shape needed for a healthfinancing vehicle to support those objectives. Areview of the history of savings accounts forhealth suggests that the savings vehicle of tomorrow should have most or all of the followingfeatures:
■ A lifetime of care (cradle to grave);■ Coverage for medical expenses only;■ A stand-alone option;■ Individual accounts;■ Tax-free contributions from anyone, to include
pre-tax salary-reduction;■ Establishment by any employer or individual;■ High-contribution limits that encourage long-
term savings and promote catch-up in higher-income years;
■ Premiums or coverage payable from theaccount for health care, long-term care, well-ness, nursing homes and assisted livingarrangements, hospice and other end-of-lifearrangements;
■ Rollover of funds;■ Full portability;■ Promotion of wellness programs in the broad
context, to include risk assessments, diseasemanagement and other healthcare coaching,behavioral modification, and exercise andnutrition education and promotion;
■ Design flexibility; and,■ More flexibility under non-discrimination
rules.
The current funding of healthcare has created artificialsegmentation of healthcare coverage, both in the
private and public sectors. Yet, health and healthcare are continuums.

Administrative issues: There are administrativecost savings and efficiencies from a single savingsvehicle under a defined and set national policy.Any healthcare funding account necessarily impli-cates costs from implementation and compliance.
Establishing a set national healthcare policy thatis implemented through coordinated tax policy canhelp minimize administrative costs. Having a setdirection can mean fewer changes in course, thusless revamping of administration systems.Consistency in the regulatory environment similar-ly can mean reduced costs in education, trainingand implementation of new requirements.
An Employers’ Guide to Healthcare Consumerism | 51
Healthcare policy must come before tax policy, so thatthe latter serves as a tool to help implement the former,rather than the other way around.

52 | Wye River Group on Healthcare

The term “consumer driven,” as defined in theUnited States by Professor Regina Herzlinger ofHarvard Business School, can be applied to health-care when patients have unrestricted choice ofproviders and are exposed to the true costs oftheir own medical care.
In many European healthcare systems, consumershave long been accustomed to a relatively unre-stricted choice of health insurance provider, cover-age levels and co-payment ratios, in a model char-acteristic of consumer-driven care. European con-sumers in many systems have transparency regard-ing medical costs incurred, but do not bear thefull financial risk.
In January 2004, the U.S. enacted a new law pro-moting CDHC in its financing and healthcare deliv-ery systems. .A relatively new concept here, theconsumer-driven healthcare system is based onprivate HSAs , a model that’s not used in Europe.Instead, all European healthcare systems are builtaround the principles of solidarity and universalcoverage, but in many cases do carry limited riskassumption by consumers, coupled with relativelyunrestricted choice of providers and care levels.
We believe that the tools and processes developedto support consumer-driven care across Europeshould be applicable to the needs of the newlyempowered owners of HSAs in the United States.
Perspective on HealthcareFinancing
At 45% of total healthcare costs, the U.S. govern-ment’s portion of the country’s total healthcaretab is less than that of 12 other developed coun-tries, with a per capita GDP of more than $20,000(See the chart below.) In all 12, the governmentcontributes more than 50% of total healthcarecosts.
What’s the major difference between the UnitedStates and these countries in terms of healthcarespending? In this country, a much larger portion(36%) of total healthcare funding comes from theprivate sector, via private insurance paid for pri-marily by employers who voluntarily provide med-ical benefits to their employees. No otherOrganisation for Economic Co-operation andDevelopment (OECD) country has as high a level ofprepaid private insurance, which shields the con-sumer from direct exposure to the financing ofhealthcare.
Rising healthcare costs in the early 1990s stimu-lated the development of a number of managedcare initiatives. These almost eliminated increasesin healthcare costs between 1994 and 1997.
Chapter VIII
A European Perspective on Healthcare &the Impact of Consumer Choice
An Employers’ Guide to Healthcare Consumerism | 53
The US has the highest share of private insurancelevels for healthcare
Share of health expenditure in basket of nations with GDP/pc > $2002
Private
20 000, percent
Other**
Out-of-pocket*
Prepaid
Social Insurance/Government
Health spending %GDP Life expectancy at birth % population > 60 yrs
* Includes uninsured in the US, ** other private funds Source: WHO, OECD Health Data © C. Maulbecker Armstong, Consulting.
14.6 11.2 8.8 9.5 9.6 7.6 8.5 9.7 10.9 7.9 8.8 7.7 9.277 81 79 81 80 80 80 79 82 77 79 81 16.3 22.6 18.7 16.9 17.4 21.8 24.7 20.5 24.4 25 20.7 20.6 23.2
US Switzerland
Netherlands
Australia
Canada
SpainItaly
FranceGermany
JapanDenmark
UK Sweden
45 58 65 68 70 71 75 76 78 82 83 84 85
38
14
5 17 5 2 1 2 1 1 2
319 20
15 24 2110 11 16 15 3
10
187
134 1
13 9 2 210
15

54 | Wye River Group on Healthcare
However, since 1998, healthcare costs have risenat double digit annual rates, reaching 16% in2004 of the nation’s gross domestic product(GDP). That’s far higher than the percentage ofGDP that healthcare expenditures comprise inthese 12 developed nations. Yet U.S. employershave seen their share of healthcare costs rise at acompounded annual growth rate of 6.7%, fasterthan all other employee benefit components.(McKinsey Quarterly, January 2004). It is worthnoting that medical outcomes, at least in terms oflife expectancy, are comparable, if not better, insome other nations with similar demographics.
Not surprisingly, American employers are increas-ingly unable to offer comprehensive, fully fundedhealthcare benefits or to absorb the cost increas-es. As a result, many are forced to design andshop for new health benefits and to increase co-payment levels and deductibles. Large employershave seen unions and employee groups protest thereduction in health benefits, and some small andmedium-sized employers may end up opting out ofoffering health benefits, labor market permitting.
In a recent Wall Street Journal poll, 61% of therespondents rated reliable health benefits as moreimportant than higher salaries. U.S. employers arethe major payers of health insurance and thushave a big stake in improving the efficiency of thehealthcare system or changing the funding struc-ture so that more costs are shared with employeesor the government. The consumer-driven health-care movement and the Health Savings Accountlegislation that took effect in January 2004addresses both needs.
We believe that consumer-driven healthcare will beinfluenced more by technological and healthcaresystem innovations than by the private insurancereform in conjunction with the health savingsaccounts.” (Global “Consumer Driven” HealthcareMoving beyond the first generation private accounts;Feb 2005 W.R. Boyles, C. C. Maulbecker Armstrong:www.hsamarkets.com) This is why we would like tofocus more on technology and system innovationsthan on the financing in taking a closer look atinternational healthcare systems.
Supportive Policies, Tools andProcesses in Europe
All EU systems are converging around commondenominators, such as more “power to patient”organizations, cost-control measures and the useof informatics to enhance cost-effectiveness.What’s more, European Union regulatory bodies arehaving an increasing impact on national health-care systems. In 1998, two landmark court rulingsin favor of the free movement of goods and servic-es within the EU markets were applied to health-care: In the Kohl and Decker judgments(c-120/95and C158/), two EU citizens won the right to bereimbursed by their national social security systemfor treatments— in this case, for spectacles andorthodonture. So-called “medical tourism,” drivenby consumers seeking to access the best possiblecare in both inpatient and outpatient settings,has become common in Europe ever since. (Dr. C.Maulbecker; Economics and Finance – Consumerpressure, medical tourism and healthcare costs;Economist Healthcare Europe – 4Q1998)
Financial responsibility drives change: Generally,in all healthcare systems with high consumerengagement—through co-payments, for example—there is a high demand for participation as stake-holders and for changes to enhance efficiencies. A2004 EU survey showed that 1/3 of consumers arewilling to spend their own money for healthcare,and are asking for better access to health-relatedinformation (Impatient for Change, EuropeanAttitudes to Healthcare Reform, published 2005 by the Stockholm Network ISB 1-95476-630-0,http://www.healthpowerhouse.com) Higher con-sumer engagement driven by greater financialresponsibility through Health Savings Accounts isexpected to have a similar effect in this country.
Among European countries, Switzerland has thehighest co-payment levels, at 31%. Switzerlandhas also been the most aggressive EU country inworking to change its healthcare system. A com-prehensive health reform movement beginning in1994, with a second wave in 1998, introducedPhysician Practice Organizations, DRG-based hospi-tal compensations and mail order pharmacy sys-tems. (Opportunities for PPMCs in Switzerland,Managed Care, July 1998).
While this may seem very similar to the U.S. man-aged care models, there is an important difference:Consumers select and pay for their health insurance.
Consumer driven healthcare will be driven more bytechnological and healthcare system innovations than
by the private insurance reform in conjunction with the health savings accounts.

Every Swiss citizen purchases his or her own cov-erage, and a selection of private health plans com-pete for members. The government subsidizes lowincome families, not by providing coverage forthem but by giving them the funds to purchasehealth insurance themselves. All health insurersmust offer a standardized mandatory basic pack-age. Plans can only differentiate by the premiumsthey set for this standard coverage and throughancillary private insurance modules offering addi-tional healthcare services.
Independent brokers and online portals providetransparency: There are companies, includinginsurance brokers and online portals, that adviseSwiss consumers on the most cost efficient healthplan based on individual needs. A website,www.comparis.ch, calculates which of four possi-ble co-payment levels is best for a Swiss citizen,based on age, gender and locale. Consumers canswitch insurers annually without penalty.
Since consumers have the freedom to go to anyprovider they choose, there is no need to changedoctors when changing health insurer. This pro-vision supports continuity of care—and manySwiss families have had the same doctors fordecades.
Prevention, wellness, health programs andinformation: One way insurers compete witheach other for Swiss consumers is to have a rangeof prevention and wellness offerings, such asnutrition counseling, spa weekends, fitness class-es, or alternative medicine treatments. Privatelyinsured Swiss patients have a “Gesundheitskonto”(a health spending account) that can be used tocover the cost of fitness programs, including yogaand swimming classes, for example. Money spentby the consumer for such services is subsidized at50% by the health insurer. Facts about nutrition,complementary medicine and preventive careappear in monthly magazines sent to all customersand are available on the insurer’s Web site andtelephone information centers. To facilitate costefficient decision making, the health plans offerfree second opinion programs and 24-hour tele-phone help lines.
Partially financed coverage in Germany:Germany, similar to the United States, has a largepart of its population (70 million) covered byhealth insurance that’s partially paid by employ-ers, but based in the nation’s statutory sicknessfunds. Those whose earnings fall below a specified
level are required to be covered by the public sick-ness funds. While in Germany, unlike inSwitzerland, employers often pay 50% of the pre-mium for membership in a public sickness fund,the consumer still has many such funds to choosefrom. Premium levels in these public health fundsare dependent upon income level.
Once they’re covered by a sickness fund or privateinsurance, consumers have a free choice of physi-cians, and few service limitations.
Increased co payment: Germany has increased thelevel of self payment from 13% in 1992 to 16% in2002. This has coincided with ongoing reform thatis gradually adding user charges to the publichealth insurance system, and creating a muchlarger movement of insured between the differentsickness funds and private health insurances.German consumers increasingly pay part of thecost for medical care received, as the followingexamples illustrate:
■ Consumers pay 10% of the prescription drugprice, within a preset range of minimums andmaximums. Generic drug use has increased inresponse to the additional out-of-pocketexpense, which is similar to what happenedwhen Medical Savings Accounts with highdeductibles were introduced in South Africa.(S. Matisonn, NCPA Policy Report # 254);
■ A one-time co-payment “entrance fee” of 10Euros per quarter, which steers patients to aGP first, with free referrals thereafter, savedthe German sickness fund 4 billion Euros in2004—enough to make them profitable again.This highlights the power of low co-payments,while still retaining choice. The Germanpatient who wishes to forgo seeing a GP firstcan pay another 10 Euros to go directly to aspecialist without a referral.
Nationwide information, prevention and well-ness: Last year the German Federal Ministrydeducted 2.5 Euros for every life covered by thesickness funds in order to pay for a nationwidehealth information prevention program. In addi-tion, targeted disease management programs withmore than 1 million enrollees are funded with alifetime approach, rather than the common fee-for- service model.
Another key to the German healthcare program isthe position of patient advocate. Created in 2004within the German Federal Ministry of Health, the
An Employers’ Guide to Healthcare Consumerism | 55

advocate received 400,000 e-mails that yearalone. Patient advocates function together withthe IQWIG (www.iqwig.de), a new institute forquality and cost efficiency in the German health-care system, and serve as information sources forpatients and providers. Patient organizations aswell as providers can request research into healthrisk assessments and cost-benefit analyses of ther-apeutic guidelines, drugs and medical devices.
Investment in technology: This year Europeancitizens from 25 countries will receive thehealth insurance card shown here, whichoffers direct access to pan-European med-ical care and reimbursement.
This electronic insurance card is the firststep that EU health ministers have takentowards an integrated e-health platform:
“It is well recognised that medical errors and acci-dents cost thousands of lives as well as millions ofeuro every year. It is also acknowledged that e-health tools such as electronic [prescriptions] andreal-time decision support - when coupled with inte-grated, interoperable electronic health records - canreduce significantly the number of such accidentsand errors,” attendees at a recent European confer-ence concluded. “Yet patient safety will not be theonly benefit of an integrated e-health infrastruc-ture. Efficient e-health tools developed for the useof health professionals will facilitate more flexibleand collaborative work within and between healthinstitutions as well as between traditional health-care spheres, such as primary and secondary careand home care.”
Some European countries, such as the UK, Franceand Germany, have already begun introducing cen-tralized Electronic Medical Records. In 2006, 80million Germans will begin to be linked with theirproviders, pharmacies and health insurers.
A larger role in the evaluation of new drugs andtechnologies: The benchmark in Europe for healthrisk assessments combined with cost effectivenessconsiderations is the NICE (National Institute of
Clinical Excellence) in the UK. New technologiesare evaluated at a cost per Quality Adjusted LifeYear (QALY) level based on a comprehensive costbenefit analysis. NICE manages the entry of newtechnologies into the market as well as the exit ofold technologies.
Patient representation at all levels: In morecentrally organized healthcare systems, such asthe UK or Denmark, the government has beendriving health system reform. Patient bodies arepart of the decision making in most EU systems.At the European level, the International Allianceof Patient Organization (www.IAPO.org) works withthe legislature to insure patient representation.Patient representatives are, for example, involvedin the evaluation of new drugs or medical devicesat the EMEA (European Agency for the Evaluationof Medicinal Products) unlike its U.S. counterpart,the FDA.
Patients as stakeholders are integral to the evalua-tion of new technologies and in the setting ofreimbursement levels in Germany. German patientorganizations are represented in all decisions onwhether a new procedure is to be admitted forreimbursement. In addition, Germany employs ahighly regulated framework to determine whichnew technologies to adopt and at which reim-bursement levels. The process is based on healthtechnology assessments and requires the approvalof all stakeholders: the health insurance industry,provider representatives, patient organizations andthe German health ministry.
The other major difference between the UnitedStates and Europe is that in Europe, access to newtechnologies is also evaluated for its cost effec-tiveness; conversely, the United States does notdetermine whether to approve innovations basedon cost criteria. In Europe, once a product or pro-cedure is approved, there is no limit in its usagefor all health consumers.
Conclusion: Given the boundaries of solidarityand equality, European healthcare systems aregradually introducing risk assumption, more choicesupported by technology, and health informationto their healthcare systems. Patient organizationsare engaged in healthcare policy decisions and are empowered to safeguard the interest of consumers.
The government or large payer groups bargainwith providers on behalf of the consumers. More
56 | Wye River Group on Healthcare
Given the boundaries of solidarity and equality,European healthcare systems are gradually introducingrisk assumption, more choice supported by technology,
and health information to their healthcare systems.

recently the European Union, national governmentbodies, as well as insurers are using technology toenhance access to health information and improvedata management through centralized data sharingand the introduction of electronic medical records.
It is in those three areas—risk sharing, patientrepresentation, and health information provisionand management through technology—that U.S.healthcare policymakers and employers would bewise to compare and learn from international con-sumer driven approaches as they develop theirstrategies here.
An Employers’ Guide to Healthcare Consumerism | 57
U.S. healthcare policymakers can learn from internationalexperience in risk sharing, patient representation, andhealth information management through technology.

58 | Wye River Group on Healthcare

Now that we’ve looked at consumerism in health-care from a variety of angles, we want to concludethis report with our thoughts on what needs tohappen—and who needs to do what— in order toreap the benefit and mitigate the liabilities inher-ent in CDHC. To reiterate a point made in the firstchapter, experience suggests that having eitherthe public sector, in the form of government, orthe private sector, in the form of employers andhealth plans, arbitrate the tension between limit-ed resources and unlimited expectations is incom-patible with American culture.
The best healthcare system in the world could beone that provides empowered consumers with theright balance of physical health, psychosocialhealth, lifestyle, and genetic profile. But who paysfor what? How do we address the disconnects?
There is a fundamental conflict between our con-cerns about cost and our demands for choice andfreedom. People do not want to make trade-offs inhealthcare. Although Americans generally acceptthem in the market sector, healthcare is widelyviewed in a societal model. Furthermore, polls tellus most people don’t really believe trade-offs arenecessary; rather, the public believes that greedand waste in the system are responsible for therising cost of care. Therefore, any actions designedto motivate the public to be more cost-efficient inthe use of healthcare resources must address thisperception.
We are experiencing an upward cycle of scientificand technological abilities which will have a majorimpact on cost. Just as with electronics, health-related technologies make specific products andservices cheaper, but also drive market penetrationand the development of better and more expensivetechnologies to replace them.
Scientific and technological advances will alsohave a major impact on values and ethics. It willbecome clear that the system is unlikely to find away to pay for every available and potentially ben-
eficial treatment. The struggle will be to definewhich treatments and therapeutics should be cov-ered by insurance and which should be seen aslifestyle enhancements that people should pay forout of pocket, if desired.
As noted in the first chapter, the definition ofhealth is increasingly elastic. In essence, a con-sumer-driven healthcare system will allow each ofus, given adequate resources, to choose what wewant to have—and for how much.
How can we ensure that this “brave new world” ofconsumer-focused healthcare is designed in a waythat will optimize health? Clearly, to move fromwhere we are today to a more desirable futurestate will require a lot more than finance mecha-nisms such as HSAs, HRAs and MSAs. Savingsaccounts are merely a tool that helps create anenvironment in which a discussion of cost andvalue, benefits and tradeoffs can occur. This is nota warm and fuzzy conversation, and realistic ornot, people want to think of their healthcare aswarm and fuzzy. It will take a fundamental shift inattitudes and behavior on the part of the Americanpublic, and significant business model changes ofall healthcare organizations. Change is hard.
We should remember that at the end of the day,medical care principally revolves around the doc-tor-patient relationship, and ultimately that rela-tionship determines both the cost and quality ofcare. The role of all other players in the healthcaresystem is to support that relationship.
As a result, the primary focus of efforts to changemust be physicians and consumer-patients. And
An Employers’ Guide to Healthcare Consumerism | 59
Chapter IX
Who Needs to Change & How Do We Make It Happen?
Having either the public sector or the private sectorarbitrate the tension between limited resources andunlimited expectations seems to be incompatible withAmerican culture.

60 | Wye River Group on Healthcare
what is needed from these key players’ requires adifficult shift in thinking, a fundamental culturalshift from where we’ve been.
What Do Physicians Need ToDo?
In some ways, it’s really quite simple: Physiciansneed to redesign their practice to be more cus-tomer-focused. This is a huge departure from mostcontemporary business models, including adoptionof practices such as evidence-based medicine(EBM) and shared decision-making. After all, it isnot a pretty picture when a 21st century consumerencounters a 19th century physician!
Many providers have not yet realized how dramaticthe impact of putting consumers in the driver’sseat is likely to be on their business. The focus ofcare for most physicians has always been thepatient. But the pursuit of that focus has beenfrom a provider-centered model. In contrast, apatient-centered model is one in which the physi-cian leads the way to a greater or lesser extentbut is attuned to the patient’s perspectives, whichare incorporated into the care process.
In designing their practice to be more patient-focused, doctors will have to learn how to com-pete on the basis of value in a more transparentmarketplace. Such a marketplace will demand
greater attention to clinical quality, service, pro-ductivity and responsiveness. In the new worldof patient-centered care, people will not be will-ing to wait the average of 38 minutes to see thedoctor as they are required to do today. Theywill demand much more convenience, continuityof care and comprehensiveness of services. Theywill expect their physicians to collaborate withother health and social service professionals toensure that their needs are met. Consumers willdrive changes in the provider community, andsome providers are understandably anxious about this!
We hear a lot about EBM today, but how do wedefine this? Paul Keckley of Vanderbilt Universityoffers a useful description of three dimensions:
■ Science—What works best given what weknow today as a result of population-basedpeer-reviewed research;
■ Clinician training and experience—academictraining, CME and credentialing; practice set-ting, locality; and
■ Patient preferences, understanding and values.
Currently, this isn’t happening. Providers are well-rewarded for redundancy and waste and oftenpenalized for cost-efficient care. We need ahealthcare system that is accountable for resultsand based on values, not procedures.
Jack Wennberg and his colleagues at Dartmouthwere pioneers in demonstrating the huge andunwarranted variations in practices that result inthree unacceptable patterns:
■ Underuse of effective care and servicesshown to work and that patients want.Physicians provide preventive, acute andchronic care called for in the medical litera-ture just 55% of the time. (McGlynn, 2003)
■ Misuse of preference-sensitive care, wheremore than one approach is reasonable andpatient values should be considered.Patients who are informed about treatmentoptions tend to choose more conservative,lower cost care.
■ Overuse of supply sensitive care and servic-es driven by providers. High cost areas ofthe country, where there is a greater supply ofphysicians, hospital beds, etc., spend up totwice as much on healthcare than low-cost
What Do Physicians Need to Do? ■ Create customer-focused practices■ Practice evidence-based medicine■ Engage in shared decision-making
Many providers have not yet realized how dramatic theimpact of putting consumers in the driver’s seat is likely
to be on their business. Doctors will have to learn how to compete on the basis of value in a more
transparent marketplace.
A consumer-driven healthcare system will allow each ofus, given adequate resources, to choose what we want
to have—and for how much.

areas. But people don’t get more preventivecare, nor do they have better outcomes or livelonger. And they aren’t more satisfied withtheir care. Instead, they get more visits andtests, longer hospital stays and more proce-dures—especially futile care at the end oflife! (Fisher 2003)
There is more evidence than ever that the practiceof medicine is anything but pure science today. Ina Harris Poll conducted in March 2005, only 29%of U. S. adults reported that they or a familymember had received a second medical opinionfrom a doctor in the past five years. (Of the 71%who did not get a second opinion, 46% said itwasn’t necessary and 39% said they trusted theirdoctor.) Among those who did get a second opin-ion, 50% said they did it because they wanted asmuch information as possible. What’s more, in46% of these cases, the diagnosis was differentfrom the original, and in two thirds of thesecases, treatment was different as a result! Thatcertainly suggests work needs to be done toimprove the quality of clinical science as well asthe quality of clinical decision-making!
The late John Eisenberg, former head of theAgency for Healthcare Research and Quality(AHRQ) put it this way: “… there is sufficient evi-dence to suggest that most clinicians’ practices donot reflect the principles of evidence-based medi-cine but rather are based upon tradition, their mostrecent experience, what they learned years ago inmedical school, or what they have heard from theirfriends….”.
When the rules of clinical practice are not clear,variation results from subjective opinion, practicepreferences and hospital capacity.
Why is there all this variation and what can bedone? The fact is, physicians simply can’t keep upwith the rapid changes in science. Surveys con-clude that the average physician spends approxi-mately two hours a week reading scientific jour-nals, and many doctors are overwhelmed by thevolume of material confronting them. There are10,000 randomized controlled trials publishedannually in primary care alone!
Most physicians also have little incentive to makea concerted effort to practice evidence-based med-icine because they are not confident that healthplans will pay for it. In fact, health insurers maynot be in agreement with best practices. In addi-
tion, most physician groups fear the widespreadapplication of EBM because it challenges their professional turf.
It is clear that at least some consumer advocatesalso fume about what the docs call “cookbookmedicine.” However, as we have already pointedout, it is apparent that not all physicians knowhow to cook. So perhaps a good cookbook is nec-essary, if not sufficient, to improve healthcarequality.
As an example of a consumer advocacy group thatechoes physician concerns, the Citizen’s Council onHealth Care, a non-profit group in Minnesota thatpromotes individual patient and practitioner con-trol of health care decisions, describes EBM as“technocrats taking over the practice of medicine.”They express concern about rigid standards of careimposed on patients, restrictions on professionalfreedom and judgment, rationing of healthcareservices and the politicization of medicine.(http://www.cchconline.org/pdfreport/EBM_Report_-_Ex_Summary.pdf)
Its members cite numerous problems with avail-able evidence. Some are certainly issues that needto be considered but others reflect the advocacygroup’s own biases. We should be cautious aboutthe wholesale undermining of change, as clearlythere are known and unknown risks. It is impor-tant to not let the desire for perfection keep usfrom moving forward.
There is a good deal of enthusiasm in some quar-ters for pay for performance, or P4P strategies, asa means of gaining provider cooperation withstandardization and practice guidelines. P4P wasgiven an important professional endorsement in2001 in an IOM report, Crossing the QualityChasm, which stated that private and public pur-chasers must modify their payment mechanisms to“recognize quality, reward quality, and supportquality improvement.” In a consumer-driven socie-ty, the idea of paying for performance resonateswith patients, and currently there are at least 100
An Employers’ Guide to Healthcare Consumerism | 61
Considerable work needs to be done to improve the qual-ity of clinical science as well as the quality of clinical decision-making. When the rules of clinical practice are not clear, variation results from subjectiveopinion, practice preferences and hospital capacity.

62 | Wye River Group on Healthcare
different pilots and programs sponsored by insur-ers, government agencies, employer groups andCongress.
However, despite all of this irrational, unexplainedand unwarranted practice variation, there is notoverwhelming enthusiasm even in the medicalcommunity for rewarding physicians for practicingEBM, even when standards are clear. Last year, theAMA board chair and current President-electdenounced P4P as a “scam designed by multimil-lionaire CEOS of health insurance companies” tocut reimbursement by taking advantage of gulliblephysicians. (AMNews, Wm Plested, Mar 1, 2004)
What do consumers think of this approach? HarrisInteractive released a survey in June 2005 thatfound the public to be only moderately supportiveof having health plans pay more to doctors forhigher quality (38% of those surveyed said yes,17% said no, and 32% were indifferent)—withone caveat: If P4P lowered their health insurancecosts, 67% would be in favor. The more educatedthe respondent, the more he or she was likely tofavor P4P. Consumers are somewhat supportive ofmeasures that are associated with prevention andpromoting patient compliance, but less so ofmeasures of quality based on a particular diseaseor technology metrics.
The promise of shared decision-making: Thethird leg of the successful consumer-driven health-care model is shared decision-making. Thisrequires a fundamental change in attitude andbehavior by many physicians. Unfortunately, thenews is rather grim when it comes to the scientificresearch on just how frequently and how deeplythe average doctor gets into shared decision mak-ing with the average patient.
One study (Braddock, et al., JAMA 1999) of over3,000 medical decisions involved in 1,000 visitslooked at six key elements of informed consent orshared decision-making:
■ Decision itself was raised and discussed; ■ Some discussion of alternatives;
■ Discussion took place about pros and cons;■ Discussion of any uncertainties■ Attempt made to assess the patient’s under-
standing of the decision or its implications■ Some exploration of patient preferences.
Only 9% of all the decisions reflected even a fairlylimited degree of shared decision-making. And notone out of 3,000 included all six elements. Theone element that is probably the most important,both in terms of developing and strengthening thedoctor-patient relationship and leading to a high-er likelihood of patient compliance, is a discussionand an exploration of the patient’s understanding.That element was the least frequently noted of thesix elements, appearing only 2% of the time.
Perhaps part of the reason for these results relatesto the fact that there are a number of prerequi-sites for shared decision-making that don’t oftenseem to exist today:
■ Trust, something that is hard to achieve with-out a long-term doctor-patient relationship;
■ Good communication skills, which, in general,are not taught to physicians;
■ Adequate time, certainly more than the aver-age 5 minute, 48 second office visit;
■ Incentives, which are not provided in terms ofcompensation; and
■ Commitment and conviction from both par-ties, as to the value and the need.
Many opine that one needs to experience it toappreciate the value of shared decision-making.
So it is perhaps not surprising that it rarely hap-pens. Today’s healthcare organizations and health-care settings all too often produce non-compliantpatients and demoralized clinicians, neither ofwhich is conducive to the kind of shared decision-making we think would be ideal.
Interestingly, physicians have no better trackrecord when it comes to taking the initiative tocounsel patients about lifestyle changes thanpatients do in adopting them. The rationale theygive for not doing so relates to a number of fac-tors. They don’t know how, they don’t have time,they aren’t paid for it, are among the reasonscited for not communicating well. But in reality,the number one reason is skepticism. They don’tthink it will make any difference—they don’tbelieve patients will change!
Only 9% of all the healthcare decisions reflected even alimited degree of shared decision-making, perhaps
because many prerequisites for shared decision-makingdon’t often exist today.

What Do Consumer/PatientsNeed To Do?
With regard to the other side of that key equationin healthcare, what is it that consumer- patientsneed to do differently?
According to economist Jamie Robinson, there aresome significant challenges when it comes to thecentral role of consumers. He points out that “Thenatural role for the consumer in a market economyis to make informed, price-sensitive choices basedon personal preferences and subject to individualbudgetary constraints. This paradigm is poorlymatched to the special features of health care.”
However, as with the physician role, we will sug-gest three “simple” steps that would go a longway toward enhancing the effectiveness of theconsumer role in healthcare decision making. First,consumers need to take personal responsibility forpracticing healthy lifestyles. Second, they need toshop effectively for the best care. Third, they needto be compliant with their providers recommenda-tions for therapy and treatment.
Is this realistic today? Obviously, there are a num-ber of challenges that even the most well-inten-tioned patient might have with these demands.Let’s look at each more carefully.
Take responsibility for practicing healthylifestyles: One of the principle tenets of CDHC ispersonal responsibility. But we know there isstrong resistance to this notion from some advo-cacy groups who see it as blaming the patient ortrying to make the patient accountable for factorsthat are beyond her control.
Yet, it is realistic to say that when it comes today-to-day decisions about exercise, diet, smokingcessation, and other health behaviors it’s the doc-
tor who advises but the patient who decides. Andlest we think this is a trivial matter, consider thisstatistic: According to the CDC, 50% of healthcarecosts are directly related to individual behavior.
If we look at the need for behavioral change inthe context of future healthcare needs, there aresome sobering facts. We are all getting older—asindividuals and as a population. And many of usare getting fatter. As a result, we are facing animpending tsunami of chronic care needs whichwill be extremely costly. Obesity, as a key under-pinning of chronic disease, explains almost asmuch of the healthcare cost increases as tobacco,and leads to a huge increase in risk of death frommany causes. So this is a big deal from a financialpoint of view, and as such, has received a gooddeal of attention from the national media.
Why are we getting fatter? It’s a simple matter ofenergy balance, or rather lack of it. We are facinga “perfect storm” for obesity. We are eating moreand we’re eating out more. In 1970, a third of thefood budget was consumed outside the home. Bythe late 90’s, it rose to almost half, and now thenumber is well over 50%. Everything is beingsuper-sized—we are a super-size society! As acountry, we are producing 4,000 calories per per-son, per day. No wonder 35% of the populationare obese or severely obese—numbers that havealmost doubled in the last 25 years.
When we highlight the need for consumers to takemore personal responsibility for their healthhabits, however, we’re not just talking about ener-gy balance and obesity. We are talking about tak-ing responsibility as a society and as individualsfor wellness and health promotion. At the heart ofthis is a need for comprehensive, effective behav-ioral change programs, which will be increasingly
An Employers’ Guide to Healthcare Consumerism | 63
What Do Consumer-Patients Need To Do? ■ Take responsibility for practicing
healthy lifestyles■ Shop for the best care■ Comply with treatment
recommendations
Physicians have no better track record when it comes totaking the initiative to counsel patients about lifestylechanges than patients do in adopting them.
When it comes to day-to-day decisions about lifestylehabits, it’s the doctor who advises but the patient who decides.

64 | Wye River Group on Healthcare
important to the future of healthcare, givenchronic disease trends and demographics.
Whether we are looking at lifestyle behaviors andprimary prevention or self-management of chronicdisease, we should recognize the importance ofscientific behavioral change models and tailor pro-grams to meet individual stages. Otherwise, wewon’t motivate people to change and the impactis likely to be minimal. To make this whole CDHCmovement work, we need to really understand howconsumers view their role in health care decision-making and how they feel about making choicesand possibly changing their lifestyles.
A few months ago, WRGH commissioned a HarrisInteractive survey to explore some of the attitudesof the public around these issues. We found thatalthough most Americans are aware that a healthylifestyle can improve and/or prevent many medicalproblems, they are generally unwilling to requirepeople who are overweight or who do not exerciseregularly to pay more for their coverage and care.This suggests that payers should rely on a systemof incentives that emphasize rewards for healthybehaviors rather than punishment for unhealthyhabits. One possible exception to this rule issmoking, as the public appears more willing torequire smokers to pay more for their health insurance and medical care.
When it comes to perceptions about the quality of healthcare, the public holds mixed views.Americans appreciate that there are great differ-ences in the quality of care provided by differenthospitals and physicians for serious medical prob-lems. However, they are not willing to pay morefor access to higher-quality hospitals or physi-cians. This may well be related to the fact thatmost Americans feel satisfied with their currentphysicians and would not change them if cost orother limitations were not an issue. With this inmind, insurers will need to use well-designedincentives to drive consumers to higher-qualityproviders.
There is considerable data that shows fewAmericans are preparing financially for their futurehealthcare needs. Given rising health care costs, itis significant that a large majority of adults saythey would be willing to work an extra two orthree years in order to ensure that they haveenough money to pay for their healthcare inretirement. However, older adults – includingthose in their pre-retirement years – are less likely
than younger adults to be willing to do so.
Shop for the “best” care: Effective healthcare isall about decisions: decisions about healthy orunhealthy behavior; whether and when and whereto seek care; about drugs, tests, and surgeries. Tomake good decisions, consumers must have accessto personalized care management tools or decisionaids for guided self-care management. By decisionaids’ we mean self-administered information toolsthat prepare patients to make informed decisionsabout medical tests or treatments. Their role is toprovide a higher level of awareness about expect-ed outcomes, and they are designed to work with-in the framework of a clinician-patient relation-ship and help encourage patient participation.
Tools come in variety of forms, including videosand DVDs, Internet-based guides, online interac-tive tools, decision boards, books, and CD/ROMs.All share the ability to help the patient gain abetter understanding of options, risks and treat-ment alternatives. But this information has to beeasily available, clearly presented, relevant andtimely. In other words it must be “pushed” to thepatient at the time of need. Information Therapy(IX), such as that promoted by HealthWise, is thetimely prescription and availability of evidence-based health information to meet individuals’ spe-cific needs and support sound decision-making.
We know that many people do want informationand want to be involved. A RAND study released inMarch 2005 showed that more than 60% ofAmericans had searched for information to helpthem make sound treatment decisions in the last 12months. One-third of the 4,300 people polled saidthe information they found affected their treatmentchoice or the choice of healthcare facility. Of thosewho had not needed to do so, 94% said they wouldsearch for information if they or a family memberneeded medical care. And 52% said they alonewanted to make the final decisions, whereas 38%wanted to make it with their physicians.
However, the results of another survey were a lit-tle less encouraging when it comes to progress onconsumer engagement. It showed that despitetheir interest in being involved, most people donot think they are in a position to affect the costor quality of the care they receive.
Nonetheless, providing information and realigningincentives to support quality care does lead tohigher consumer satisfaction, better healthcare

An Employers’ Guide to Healthcare Consumerism | 65
outcomes and greater affordability. So there isboth a need and a demand for clinical decision-support tools to improve patient satisfaction and quality.
As part of the study, RAND also looked at existingliterature of how treatment decision tools affectbehavior and found that patients using aids aremore likely to make more conservative choices,—and more detailed information has an even greaterimpact. Theoretically, at least, this should resultin some cost savings without any perception bypatients that they are being denied care.
Some providers are taking significant steps to sup-port patients’ use of online information. Accordingto the Center for Information Therapy, GroupHealth Cooperative, Puget Sound, is on the cuttingedge of guiding patients through online medicalinformation and is using IT to transform patients’experience with healthcare.
For the majority of people who don’t have accessto a fully integrated HMO or don’t want to, AARPlaunched its Health Guide to help patients throughthe health information maze. It provides easy tounderstand, scientifically valid health informationpresented in the way that patients deal withhealth care problems. AARP sees its Health Guideas a launching pad for providing more services,such as maintaining electronic medical records.
How are consumers using information that’s avail-able? What do we know about the way consumersare currently using cost and quality informationon providers? CDHC is helping to bring cost trans-parency to health care sooner than many expertswould ever have predicted. Access to cost esti-mates for drugs, tests, and surgical procedures isincreasingly a reality. Cost transparency for hospi-tal comparisons is rapidly improving, even thoughit is still evolving and not ideal. Transparency for most physician rates, however, is still someyears away.
Transparency of quality information is on a similartrajectory. Partly as a result of pay for qualityefforts by both private payers and CMS, many hos-pitals now report quality metrics that are publishedand available for use in decision support tools.
Efforts are being made to address this problem. InApril 1, 2005, for example, CMS began postingquality performance data for the nation’s hospitalson its new “Hospital Compare” Web site.
Cooperation among representatives from differentsectors is important. One model might be theConsumer-Purchaser Disclosure Project, a non-prof-it partnership of consumer and labor organiza-tions, public and private purchasers and employergroups. Its goal is to make it possible by January2007 for Americans to be able to “select hospitals,physicians, physician groups/delivery systems andtreatments based on public reporting of nationallystandardized measures for clinical quality, con-sumer experience, equity and efficiency.”
Still, folks argue about whether consumers arecapable of using such information. And consumersare a bit schizophrenic about it, too. We learnedfrom our December 2004 Harris survey that aneffective approach to getting Americans moreinvolved in healthcare decision-making will needto ensure that the healthcare system is easy forthem to understand and navigate. This is impor-tant in helping consumers become more comfort-able using information sources other than thosethey have traditionally relied on. Nearly two out ofthree Americans feel that they would become moreinvolved in decision-making if the healthcare sys-tem were easier to navigate. Reflecting a tradi-tional reliance on physicians for making decisionsabout treatments or selecting specialists or hospi-tals on their behalf, over a third of consumers saythey would still follow their doctor’s advice even if it conflicted with reliable information fromanother knowledgeable source.
Despite their interest in being involved inhealthcare decisions, most people do not thinkthey are in a position to affect the cost or quality of the care they receive.
Despite their interest in being involved in healthcaredecisions, most people do not think they are in a position to affect the cost or quality of the care they receive.
In October 2002, a Harris poll found that althoughhealthcare quality ratings were available to an increasingnumber of U.S. consumers, the information led very fewto alter their use of healthcare. But at the time, ratingsadvocates said that the information available wasn’t presented well, complicating consumers’ efforts to makegood use of the reports.

Be compliant with therapy: The third fundamen-tal requirement from consumers is to comply withrecommended interventions, be they preventive ortherapeutic. Yet, the statistics on compliance withphysician recommendations, whether related todiagnostic testing, prescriptions or lifestylechanges are not encouraging. Patients fail to com-ply with directives for a whole host of reasons,many related to lack of understanding or trust,that is, a poor doctor-patient relationship.
It’s quite clear from decades of research that with-out really good behavioral health communicationprograms in place, as a group, patients really don’tadhere very well, particularly when it comes tocomplex or long-term regimens. It’s particularlydifficult when treatment is multifaceted and thereare no symptoms.
Low health literacy affects 40 million Americansand is estimated to contribute 30-54 billion dol-lars in additional healthcare charges. The IOM sayshalf of healthcare providers believe patients donot adhere to treatment because of language bar-riers, cognitive impairment, lack of knowledge orcultural issues. Other types of non-compliancerelate to the regimen itself, which may be diffi-cult, complicated, or disruptive of lifestyles. Athird type of non-compliance is intentional. Thepatient makes a conscious decision to alter orstop treatment.
Some experts have pointed out that the problemis compounded by the fact that doctors consis-tently underestimate the degree of non-compli-ance among their patients and overestimate theirability to identify it as an issue.
In summary, it is unrealistic to think patients in aconsumer-centric healthcare model currently haveenough information to make good decisions. Butit is coming! Robust, reliable, trustworthy infor-mation isn’t yet there on price and certainly noton quality. Patient coaches or patient navigators,especially for the disadvantaged and chronicallyill, are going to be a critical component in ensur-ing that these strategies are truly useful.
What is the Role of Employersand Health Plans?
Most of this guide is focused on how the role ofemployers and health plans is changing. So wewill not belabor many of the points already made.
As we pointed out in an earlier chapter, thedebate over health reform gets down to the funda-mental question over who will control healthcaredecisions - bureaucracies or individuals. Thosewaiting for the “big bang” might reconsider.Whatever change occurs will preserve the currentpillars that support our system. The change will bean evolution, not a revolution, and it will bepainful. In fact, most leaders we’ve talked to rec-ognize that change is imminent and that allstakeholders in healthcare will need to carefullyredefine and articulate their value proposition.
Understandably, a principle interest of employer pur-chasers is cost control, although many of the strate-gies that can help address costs are supportive ofemployees and also can enhance productivity. Theycan also help the consumer get the most out of therelationship they have with their physician.
Communicate the need for and advantages ofthe new model and serve as “information bro-kers”: Today, employers have the opportunity toavoid the mistakes of the managed care movementby taking a longer-term strategic view of their rolein supporting their employees’ health. Someemployers may seize the consumerism movementas a quick fix to rein in escalating costs by shift-ing them onto their employees and just give lip-service to CDHC. But smart employers will not fallinto that trap. Instead, they will recognize theopportunity to reposition themselves as trusted,honest brokers of information and as active cata-lyst for healthy lifestyles. In order to be success-ful, they will embrace all the facts of CDHC, moveslowly, focus on communication, and truly empow-er and support their employees.
66 | Wye River Group on Healthcare
Without really good behavioral health communicationprograms in place, patients really don’t adhere very
well, particularly when treatment is complex and thereare no symptoms.
What Can Employers and Plans Do?■ Serve as information brokers■ Base prevention and disease
management programs on behavioralchange model
■ Reward provider for quality

For some employers, this means setting aside thepaternalism and control that marked the old wayof doing business, in favor of supporting theunderlying cultural changes necessary to empowereach employee with the right incentives to takeownership of his or her health. It means activelysupporting employees with credible informationon doctors and hospitals. It means educatingthem about prevention and self-care for the mostprevalent diseases. It means being thoughtful inbenefit design, ensuring that no one is disenfran-chised. It means ensuring that those with chronicillness are effectively linked to disease manage-ment and primary case management programs.And it means ensuring strong incentives are builtinto plans for prevention and wellness. In short,it is a whole new world, as described in detail inearlier chapters.
But the difficulty in putting CDHC theory intopractice should not be underestimated. There is noquestion that there will be some unintended con-sequences that must be monitored and addressed.Critical details that will require sustained atten-tion if the benefits are to outweigh the risks areoften glossed. No single design, such as highdeductible health insurance, is suited to everyone.Non value-added infrastructure will be subjectedto the most intense scrutiny possible—that of theconsumer and marketplace. Many of the issues areundoubtedly familiar to the reader and have beendiscussed earlier in the guide.
Benefit design is key to ensuring that needed careis not avoided. Accounts need to initially be fund-ed with sufficient resources and incentives forconsumers to seek appropriate preventive andchronic care. Information and a personal supportsafety net are critical components of successfuldesign.
Plans need to facilitate movement by providingaccess to existing networks and on-line informa-tion tools.
Design and provide comprehensive programs inprevention and disease management based onbehavioral change model: The importance of bet-ter management of those individuals with multiplechronic conditions is discussed in detail in chapterIV. Here, we will just reiterate some key points.
During the 1970s we began to think about healthpromotion and disease prevention as an alterna-tive to only curing and repairing. Somewhat later
we began to recognize that tertiary prevention, orso-called disease management, was where wecould really save money and improve care. Giventhat 5% of the population accounts for approxi-mately 45% of costs, identifying and targetingthis group with aggressive case management andcare coordination is absolutely critical to cost-containment strategies.
Studies have shown that when someone else paysfor disease management, participation rates areexcellent. Under consumer directed plans, employ-ers should ensure that there are no financial orlogistical barriers to disease management for thatsegment of their population who can most benefit.Employers should also consider additional incen-tives, such as providing additional contributionsto the employee’s HSA or HRA in exchange for par-ticipation. Disease and case management is on thecusp of widespread acceptance among consumersand employers, but integrating it across the spec-trum of consumer products such as HSAs or HRAsis still evolving.
A combination of traditional disease management,focused on diseases like heart failure or diabetes,which pay off in the short-term, coupled withtobacco cessation, which provides a big longer-term pay off, make sense. Some programs focus onmembers’ total health profile and identify andwork with those likely to develop multiple expen-sive conditions down the line.
Change reimbursement mechanisms to rewardquality: Purchasers and payers need to incentivizetotal system redesign. They need to pay for out-comes, results, integrated care, and IT.
The P4P momentum is driven by a number of factors, including CDHC. In a consumer-based society, the idea of paying for performance theoretically resonates with patients. But aspointed out earlier, they are less than excitedabout it, both because they are reflecting some of their doctors’ complaints and because theyaren’t convinced of the kind of tangible benefitsthey want for themselves.
An Employers’ Guide to Healthcare Consumerism | 67
The difficulty in putting CDHC theory into practiceshould not be underestimated. Critical details are oftenglossed over by advocates and unintended consequencesmust be expected and addressed.

68 | Wye River Group on Healthcare
In addition to the skepticism of physicians andthe rallying of patients behind them, there areother reasons to wonder how effective P4P will beif payers don’t develop a common agenda.
Despite the hopes and interests of some pur-chasers, the current generation of P4P is notdesigned to reap cost savings, particularly sincemost of the quality measures it targets are meas-ures of underuse.
Although it was estimated a couple of years agothat by 2006, 80% of plans would use P4P strate-gies, the reality is much lower. If only a few ofthe many payers that a provider contracts with arepaying for performance, or if each focuses on adifferent measurement set, the effects are diluted.Some private-sector employers have begun align-ing efforts through healthcare quality improve-ment coalitions such as the Leapfrog Group andBridges to Excellence, which offer standardizedprograms of performance measurement, reporting,and reward.
Given the overall focus of employers on cost con-trol, it is significant that a recent CommonwealthFund Health Care Opinion Leaders Survey foundsignificant consensus on the most promising waysto do so from all sectors: academia/research; busi-ness, insurance, healthcare industry, labor/con-sumer advocacy organizations, and government .And their views support the recommendations out-lined above.
All respondents agreed that to get value for themoney we are spending, we need to change theway we pay for care, streamline administration,and foster collaboration.
The strategies rated as the most effective ways tocontrol costs are:
■ Rewarding more efficient and high qualitycare;
■ Improving disease management services forpatients with high-cost conditions;
■ Enhancing primary case management andapplying evidence-based guidelines to deter-mining when a test or procedure should bedone; and
■ Increasing collaboration among private insur-ers, Medicare, and Medicaid to adopt commonpayment methods and rates and streamlineadministrative costs.
What are the specific implications of CDHC for
health plans themselves? Health plans see HSAs asboth an opportunity and a potential threat. At thisstage, most health plans are partnering with banksto offer accounts, in some cases because they fearthat banks will cannibalize their business.
These plans pose a major challenge to payer infor-mation systems because of a complex array ofservice-specific elements: co-pays, three-tier drugpricing, provider network choices, etc. Core claimsand membership systems have to be modified.Auto-adjudication rates are down because many ofthese claims require manual intervention. Somepayers have outsourced IT functions because it istoo costly to build these applications themselves.
What is the Role ofGovernment?
The politics of healthcare represents the last bigopportunity for broad social change. For many,this translates into a politically polarized vision—those who want to see government run and fundhealthcare versus those who believe in a marriageof markets and public sector. This is a terriblyunfriendly environment in which to bring aboutsystem wide change!
Healthcare pollsters repeatedly confirm the gapbetween what people say they want and whatelected officials recognize and act on. This gapand political polarization with regard to health-care has only gotten worse. However, with health-care consumerism, there is reasonable alignmentof political interests. The basic model of robustinformation plus incentives is a political consen-sus point, which has been advocated by suchpolitical polar opposites as Ralph Nader and NewtGingrich. Gingrich promotes “information-richdecision support and health management tools,”
What Can Government Do?■ Use its leverage as purchaser■ Recognize its leadership role■ Improve technology assessment■ Support clinical effectiveness research■ Support IT standards development■ Tests CDHC models in public programs■ Create more flexible accounts

a concept that is not much different than RalphNader’s call for information about physician fees,drug-prescribing habits, and so forth. Nader oncesaid, “That this country tolerates the very worstalong with the very best quality of medical care,the poorly trained doctor along with the well-trained, those who overcharge along with those whocharge reasonable fees, can best be explained bethe total lack of information consumers have about doctors.”
So what are some constructive steps that govern-ment can take? As the payer of roughly 60% ofthe healthcare bill facing the impending swellingof the Medicare budget to care for an aging popu-lation, the government certainly has the incentiveto use its most powerful tool—its leverage as pur-chaser. Government as a purchaser, similar to pri-vate-sector purchasers, should consider supportingmodels of reform that allow the reimbursementsystem to align with the quality agenda.
There are a number of examples in which the current Bush administration is looking to do justthat. Integrated services, information, social sup-port, logistics, complex case management andmeasurement, and standards are cornerstones toconstructive change. Today CMS is advancing manyof these ideas through pilots and demonstrationprojects, such as P4P demos and Voluntary ChronicCare Improvement pilots
The leadership role of CMS is central to furtheringthis goal as private payers historically have emu-lated many of CMS’s significant payment reforms—for example, the prospective payment system. Theycould also support P4P by contributing patientdata (stripped of identifiers) to an all-payer dataset from which more reliable performance evalua-tion could be conducted because of the largerdenominators.
Government should create improved technologyassessment in order to speed the time it takes toget real innovation into practice. Currently it takesbetween 12 and 15 years for known improvementsto become mainstream practice.
Government should drive improvements in medicaleffectiveness through clinical outcomes researchand improved assessment and evaluation of theappropriate uses of new technology to mitigatevariations in physician practices.
Government and business should help create and
disseminate information by supporting the devel-opment of standards for information on qualitymeasurement, enabling consumers to makeinformed decisions and ensuring technology com-patibility and data confidentiality.
Government should test CDHC models in publicprograms, such as Medicaid and Medicare. Morepilots and demos are needed, like the self-determi-nation Cash & Counseling Medicaid, which showedthat even elderly, disabled patients and those withdevelopmental disabilities can make choices whichmeet their needs.
Government also has formal and informal powersthrough administrative law, regulation, executiveorders, legislation and the bully pulpit to havesignificant influence over the direction of healthcare.
On the savings account front, the fundamentalneed is for more flexibility, as discussed inChapter VII.
With FSAs, unused funds should be allowed torollover until retirement, both within the FSA andinto other tax-deferred accounts such as HSAs,IRAs, and 401(K)s. They would also be moreattractive if workers could make contributionsmore than once a year. Workers whose employersdon’t t provide health savings accounts should bepermitted to purchase through a third-partyadministrator.
Some say, too, that employees should be able towithdraw HRA funds as cash—after paying taxeson them— and that these funds they should beportable. If employees don’t perceive that theywill benefit from prudent consumption of health-care services, they have less incentive to makewise choices. Restrictions on who can contributeand the ability to tie contributions to salaryreduction or deferred compensation serve no useful purpose.
The design of HSAs codified in tax law in unneces-sarily restrictive ways. For example, employerscannot establish low deductibles for drug coverageor wellness programs. Nor can they create
An Employers’ Guide to Healthcare Consumerism | 69
The politics of healthcare represents the last big opportunity for broad social change.

70 | Wye River Group on Healthcare
accounts designed specifically for those withchronic disease. MSAs in South Africa have thatflexibility, with varying deductibles. A plan mighthave no deductible for hospital care on the theorythat patients have no discretion about when andwhether it’s needed, but have a $1000 or higherdeductible for outpatient care. Similarly, thedeductible on drugs for a patient with chronic dis-ease could be eliminated because skimping onmedications could lead to higher costs later.
HSAs currently have a maximum out-of-pocketexpenditure limit of $5,000 for an individual and$10,000 for a family. A person with a preexistingchronic condition might not be able to get an HSAbecause his yearly out-of-pocket costs exceed themaximum. People should be allowed to depositpre-tax funds into HSAs even if they want to self-insure for higher amounts—or cannot obtaininsurance at all.
Many also advocate for more flexibility in modelsof employer-sponsored insurance—allowingemployees to purchase personal and portableinsurance that is individually owned, for example.Different households should be accommodated.Employees who turn down employer-sponsoredinsurance because they are covered under a spouseshould get higher wages instead. And part-timeemployees should be able to choose betweenhigher wages or health insurance.
Others have focused their recommendations onways to make these plans more equitable. Here aresome suggestions from different sources:
■ Limit the maximum out of pocket exposure toa small percentage of income, for example,5%
■ Adjust individuals’ HSA contributions based onmedical condition, self-management behaviorand income
■ Develop (and authorize regulations for) newCDHC/HSA plan features that exempt evi-dence-based disease management therapiesand preventive services from high-deductibleHSA requirements
■ Permit employers to lower deductibles forlower-wage workers
■ Exempt primary care and preventive servicesfrom the deductible
■ Permit greater flexibility in plan design■ Set an income ceiling on eligibility for HSAs■ Guarantee choice of a comprehensive health
plan to workers covered under employer plans
Making all the changes proposed here may seemlike a daunting—or even impossible—process. Buthealth system change, like all societal changes, isa process of evolution rather than revolution—andevery one of us can take steps that bring us closerto an equitable consumer-directed healthcare system now.

© Copyright 2006 by the Wye River Group on Healthcare, Inc.
All right reserved. No part of this work covered by the copyrights herein may be reproduced or copied in any formor by any means – graphic, electronic or mechanical, including photocopying, recording, taping or informationand retrieval systems for distribution without written permission of the publisher.
Price: US $45.00Plus $1.75 shipping and handling
Order from WRGHP.O. Box 1682Austin, TX. 78767Telephone: 512-472-2005E-mail: [email protected]: www.wrgh.org
Make checks payable to: WRGH
(Add appropriate tax for deliveries made in CA, DC, GA, KS, KY, MD, MN, MS, ND, NE, TX).
This publication is designed to provide accurate and authoritative information in regard to the subject mattercovered. It is sold with the understanding that the publisher is not engaged in rendering legal, accounting orother professional service. If legal advice or other expert assistance is required, the services of a competentprofessional person should be sought.